- You are here:
-
Home

-
Contents (2)
-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
-
Storage
- Urban, Jill P.G.

Sauter, Steven L.
Address: National Institute for Occupational Safety and Health, 4676 Columbia Parkway MS C-24, Cincinnati, Ohio 45226-1998
Country: United States
Phone: 1 (513) 533-8383
Fax: 1 (513) 533-8596
E-mail: SLS4@niobbs1.em.cdc.gov
Past position(s): University of Wisconsin, Department of Preventive Medicine
Education: PhD, Industrial Psychology, University of Wisconsin
Areas of interest: Job stress; psychosocial factors and occupational health
Musculoskeletal Disorders
There is growing evidence in the occupational health literature that psychosocial work factors may influence the development of musculoskeletal problems, including both low back and upper extremity disorders (Bongers et al. 1993). Psychosocial work factors are defined as aspects of the work environment (such as work roles, work pressure, relationships at work) that can contribute to the experience of stress in individuals (Lim and Carayon 1994; ILO 1986). This paper provides a synopsis of the evidence and underlying mechanisms linking psychosocial work factors and musculoskeletal problems with the emphasis on studies of upper extremity disorders among office workers. Directions for future research are also discussed.
An impressive array of studies from 1985 to 1995 had linked workplace psychosocial factors to upper extremity musculoskeletal problems in the office work environment (see Moon and Sauter 1996 for an extensive review). In the United States, this relationship was first suggested in an exploratory research by the National Institute for Occupational Safety and Health (NIOSH) (Smith et al. 1981). Results of this research indicated that video display unit (VDU) operators who reported less autonomy and role clarity and greater work pressure and management control over their work processes also reported more musculoskeletal problems than their counterparts who did not work with VDUs (Smith et al. 1981).
Recent studies employing more powerful inferential statistical techniques point more strongly to an effect of psychosocial work factors on upper extremity musculoskeletal disorders among office workers. For example, Lim and Carayon (1994) used structural analysis methods to examine the relationship between psychosocial work factors and upper extremity musculoskeletal discomfort in a sample of 129 office workers. Results showed that psychosocial factors such as work pressure, task control and production quotas were important predictors of upper extremity musculoskeletal discomfort, especially in the neck and shoulder regions. Demographic factors (age, gender, tenure with employer, hours of computer use per day) and other confounding factors (self-reports of medical conditions, hobbies and keyboard use outside work) were controlled for in the study and were not related to any of these problems.
Confirmatory findings were reported by Hales et al. (1994) in a NIOSH study of musculoskeletal disorders in 533 tele-communication workers from 3 different metropolitan cities. Two types of musculoskeletal outcomes were investigated: (1) upper extremity musculoskeletal symptoms determined by questionnaire alone; and (2) potential work-related upper extremity musculoskeletal disorders which were determined by physical examination in addition to the questionnaire. Using regression techniques, the study found that factors such as work pressure and little decision-making opportunity were associated both with intensified musculoskeletal symptoms and also with increased physical evidence of disease. Similar relationships have been observed in the industrial environment, but mainly for back pain (Bongers et al. 1993).
Researchers have suggested a variety of mechanisms underlying the relationship between psychosocial factors and musculoskeletal problems (Sauter and Swanson 1996; Smith and Carayon 1996; Lim 1994; Bongers et al. 1993). These mechanisms can be classified into four categories:
- psychophysiological
- behavioural
- physical
- perceptual.
Psychophysiological mechanisms
It has been demonstrated that individuals subject to stressful psychosocial working conditions also exhibit increased autonomic arousal (e.g., increased catecholomine secretion, increased heart rate and blood pressure, increased muscle tension etc.) (Frankenhaeuser and Gardell 1976). This is a normal and adaptive psychophysiological response which prepares the individual for action. However, prolonged exposure to stress may have a deleterious effect on musculoskeletal function as well as on health in general. For example, stress-related muscle tension may increase the static loading of muscles, thereby accelerating muscle fatigue and associated discomfort (Westgaard and Bjorklund 1987; Grandjean 1986).
Behavioural mechanisms
Individuals who are under stress may alter their work behaviour in a way that increases musculoskeletal strain. For example, psychological stress may result in greater application of force than necessary during typing or other manual tasks, leading to increased wear and tear on the musculoskeletal system.
Physical mechanisms
Psychosocial factors may influence the physical (ergonomic) demands of the job directly. For example, an increase in time pressure is likely to lead to an increase in work pace (i.e., increased repetition) and increased strain. Alternatively, workers who are given more control over their tasks may be able to adjust their tasks in ways that lead to reduced repetitiveness (Lim and Carayon 1994).
Perceptual mechanisms
Sauter and Swanson (1996) suggest that the relationship between biomechanical stressors (e.g., ergonomic factors) and the development of musculoskeletal problems is mediated by perceptual processes which are influenced by workplace psychosocial factors. For example, symptoms might become more evident in dull, routine jobs than in more engrossing tasks which more fully occupy the attention of the worker (Pennebaker and Hall 1982).
Additional research is needed to assess the relative importance of each of these mechanisms and their possible interactions. Further, our understanding of causal relationships between psychosocial work factors and musculoskeletal disorders would benefit from: (1) increased use of longitudinal study designs; (2) improved methods for assessing and disentangling psychosocial and physical exposures; and (3) improved measurement of musculoskeletal outcomes.
Still, the current evidence linking psychosocial factors and musculoskeletal disorders is impressive and suggests that psychosocial interventions probably play an important role in preventing musculoskeletal problems in the workplace. In this regard, several publications (NIOSH 1988; ILO 1986) provide directions for optimizing the psychosocial environment at work. As suggested by Bongers et al. (1993), special attention should be given to providing a supportive work environment, manageable workloads and increased worker autonomy. Positive effects of such variables were evident in a case study by Westin (1990) of the Federal Express Corporation. According to Westin, a programme of work reorganization to provide an “employee-supportive” work environment, improve communications and reduce work and time pressures was associated with minimal evidence of musculoskeletal health problems.
Psychosocial and Organizational Factors
In 1966, long before job stress and psychosocial factors became household expressions, a special report entitled “Protecting the Health of Eighty Million Workers—A National Goal for Occupational Health” was issued to the Surgeon General of the United States (US Department of Health and Human Services 1966). The report was prepared under the auspices of the National Advisory Environmental Health Committee to provide direction to Federal programmes in occupational health. Among its many observations, the report noted that psychological stress was increasingly apparent in the workplace, presenting “... new and subtle threats to mental health,” and possible risk of somatic disorders such as cardiovascular disease. Technological change and the increasing psychological demands of the workplace were listed as contributing factors. The report concluded with a list of two dozen “urgent problems” requiring priority attention, including occupational mental health and contributing workplace factors.
Thirty years later, this report has proven remarkably prophetic. Job stress has become a leading source of worker disability in North America and Europe. In 1990, 13% of all worker disability cases handled by Northwestern National Life, a major US underwriter of worker compensation claims, were due to disorders with a suspected link to job stress (Northwestern National Life 1991). A 1985 study by the National Council on Compensation Insurance found that one type of claim, involving psychological disability due to “gradual mental stress” at work, had grown to 11% of all occupational disease claims (National Council on Compensation Insurance 1985)
* In the United States, occupational disease claims are distinct from injury claims, which tend to greatly outnumber disease claims.
These developments are understandable considering the demands of modern work. A 1991 survey of European Union members found that “The proportion of workers who complain from organizational constraints, which are in particular conducive to stress, is higher than the proportion of workers complaining from physical constraints” (European Foundation for the Improvement of Living and Working Conditions 1992). Similarly, a more recent study of the Dutch working population found that one-half of the sample reported a high work pace, three-fourths of the sample reported poor possibilities of promotion, and one-third reported a poor fit between their education and their jobs (Houtman and Kompier 1995). On the American side, data on the prevalence of job stress risk factors in the workplace are less available. However, in a recent survey of several thousand US workers, over 40% of the workers reported excessive workloads and said they were “used up” and “emotionally drained” at the end of the day (Galinsky, Bond and Friedman 1993).
The impact of this problem in terms of lost productivity, disease and reduced quality of life is undoubtedly formidable, although difficult to estimate reliably. However, recent analyses of data from over 28,000 workers by the Saint Paul Fire and Marine Insurance company are of interest and relevance. This study found that time pressure and other emotional and personal problems at work were more strongly associated with reported health problems than any other personal life stressor; more so than even financial or family problems, or death of a loved one (St. Paul Fire and Marine Insurance Company 1992).
Looking to the future, rapid changes in the fabric of work and the workforce pose unknown, and possibly increased, risks of job stress. For example, in many countries the workforce is rapidly ageing at a time when job security is decreasing. In the United States, corporate downsizing continues almost unabated into the last half of the decade at a rate of over 30,000 jobs lost per month (Roy 1995). In the above-cited study by Galinsky, Bond and Friedman (1993) nearly one-fifth of the workers thought it likely they would lose their jobs in the forthcoming year. At the same time the number of contingent workers, who are generally without health benefits and other safety nets, continues to grow and now comprises about 5% of the workforce (USBLS 1995).
The aim of this chapter is to provide an overview of current knowledge on conditions which lead to stress at work and associated health and safety problems. These conditions, which are commonly referred to as psychosocial factors, include aspects of the job and work environment such as organizational climate or culture, work roles, interpersonal relationships at work, and the design and content of tasks (e.g., variety, meaning, scope, repetitiveness, etc.). The concept of psychosocial factors extends also to the extra-organizational environment (e.g., domestic demands) and aspects of the individual (e.g., personality and attitudes) which may influence the development of stress at work. Frequently, the expressions work organization or organizational factors are used interchangeably with psychosocial factors in reference to working conditions which may lead to stress.
This section of the Encyclopaedia begins with descriptions of several models of job stress which are of current scientific interest, including the job demands-job control model, the person- environment (P-E) fit model, and other theoretical approaches to stress at work. Like all contemporary notions of job stress, these models have a common theme: job stress is conceptualized in terms of the relationship between the job and the person. According to this view, job stress and the potential for ill health develop when job demands are at variance with the needs, expectations or capacities of the worker. This core feature is implicit in figure 1, which shows the basic elements of a stress model favoured by researchers at the National Institute for Occupational Safety and Health (NIOSH). In this model, work-related psychosocial factors (termed stressors) result in psychological, behavioural and physical reactions which may ultimately influence health. However, as illustrated in figure 1, individual and contextual factors (termed stress moderators) intervene to influence the effects of job stressors on health and well-being. (See Hurrell and Murphy 1992 for a more elaborate description of the NIOSH stress model.)
Figure 1. The Job Stress Model of the National Institute for Occupational Safety and Health (NIOSH)
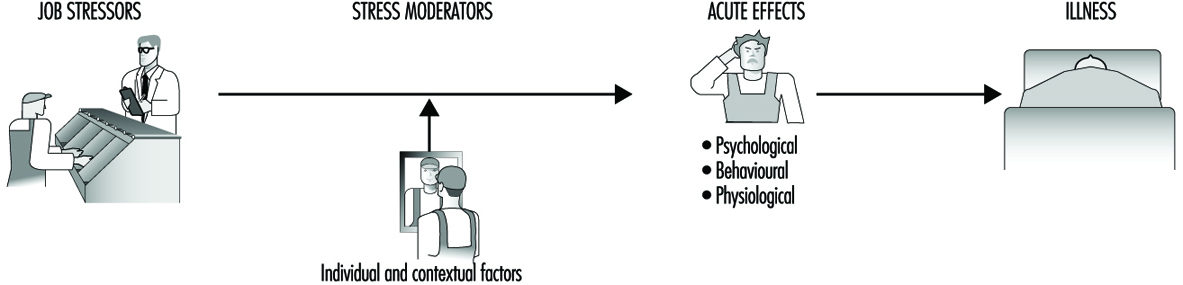
But putting aside this conceptual similarity, there are also non-trivial theoretical differences among these models. For example, unlike the NIOSH and P-E fit models of job stress, which acknowledge a host of potential psychosocial risk factors in the workplace, the job demands-job control model focuses most intensely on a more limited range of psychosocial dimensions pertaining to psychological workload and opportunity for workers to exercise control (termed decision latitude) over aspects of their jobs. Further, both the demand-control and the NIOSH models can be distinguished from the P-E fit models in terms of the focus placed on the individual. In the P-E fit model, emphasis is placed on individuals’ perceptions of the balance between features of the job and individual attributes. This focus on perceptions provides a bridge between P-E fit theory and another variant of stress theory attributed to Lazarus (1966), in which individual differences in appraisal of psychosocial stressors and in coping strategies become critically important in determining stress outcomes. In contrast, while not denying the importance of individual differences, the NIOSH stress model gives primacy to environmental factors in determining stress outcomes as suggested by the geometry of the model illustrated in figure 1. In essence, the model suggests that most stressors will be threatening to most of the people most of the time, regardless of circumstances. A similar emphasis can be seen in other models of stress and job stress (e.g., Cooper and Marshall 1976; Kagan and Levi 1971; Matteson and Ivancevich 1987).
These differences have important implications for both guiding job stress research and intervention strategies at the workplace. The NIOSH model, for example, argues for primary prevention of job stress via attention first to psychosocial stressors in the workplace and, in this regard, is consistent with a public health model of prevention. Although a public health approach recognizes the importance of host factors or resistance in the aetiology of disease, the first line of defence in this approach is to eradicate or reduce exposure to environmental pathogens.
The NIOSH stress model illustrated in figure 1 provides an organizing framework for the remainder of this section. Following the discussions of job stress models are short articles containing summaries of current knowledge on workplace psychosocial stressors and on stress moderators. These subsections address conditions which have received wide attention in the literature as stressors and stress moderators, as well as topics of emerging interest such as organizational climate and career stage. Prepared by leading authorities in the field, each summary provides a definition and brief overview of relevant literature on the topic. Further, to maximize the utility of these summaries, each contributor has been asked to include information on measurement or assessment methods and on prevention practices.
The final subsection of the chapter reviews current knowledge on a wide range of potential health risks of job stress and underlying mechanisms for these effects. Discussion ranges from traditional concerns, such as psychological and cardiovascular disorders, to emerging topics such as depressed immune function and musculoskeletal disease.
In summary, recent years have witnessed unprecedented changes in the design and demands of work, and the emergence of job stress as a major concern in occupational health. This section of the Encyclopaedia tries to promote understanding of psychosocial risks posed by the evolving work environment, and thus better protect the well-being of workers.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."