Construction workers build, repair, maintain, renovate, modify and demolish houses, office buildings, temples, factories, hospitals, roads, bridges, tunnels, stadiums, docks, airports and more. The International Labour Organization (ILO) classifies the construction industry as government and private-sector firms erecting buildings for habitation or for commercial purposes and public works such as roads, bridges, tunnels, dams or airports. In the United States and some other countries, construction workers also clean hazardous waste sites.
Construction as a proportion of gross domestic product varies widely in industrialized countries. It is about 4% of GDP in the United States, 6.5% in Germany and 17% in Japan. In most countries, employers have relatively few full-time employees. Many companies specialize in skilled trades—electricity, plumbing or tile setting, for instance—and work as subcontractors.
The Construction Labour Force
A large portion of construction workers are unskilled labourers; others are classified in any of several skilled trades (see table 1). Construction workers include about 5 to 10% of the workforce in industrialized countries. Throughout the world, over 90% of construction workers are male. In some developing countries, the proportion of women is higher and they tend to be concentrated in unskilled occupations. In some countries, the work is left to migrant workers, and in others, the industry provides relatively well-paid employment and an avenue to financial security. For many, unskilled construction work is the entry into the paid labour force in construction or other industries.
Work Organization and Labour Instability
Construction projects, especially large ones, are complex and dynamic. Several employers may work on one site simultaneously, with the mix of contractors changing with the phases of the project; for example, the general contractor is present at all times, excavating contractors early, then carpenters, electricians and plumbers, followed by floor finishers, painters and landscapers. And as the work develops—for instance, as a building’s walls are erected, as the weather changes or as a tunnel advances—the ambient conditions such as ventilation and temperature change too.
Construction workers typically are hired from project to project and may spend only a few weeks or months at any one project. There are consequences for both workers and work projects. Workers must make and remake productive and safe working relationships with other workers whom they may not know, and this may affect safety at the work site. And in the course of the year, construction workers may have several employers and less than full employment. They might work an average of only 1,500 hours in a year while workers in manufacturing, for example, are more likely to work regular 40 hour weeks and 2,000 hours per year. In order to make up for slack time, many construction workers have other jobs—and exposure to other health or safety hazards—outside of construction.
For a particular project, there is frequent change in the number of workers and the composition of the labour force at any one site. This change results both from the need for different skilled trades at different phases of a work project and from the high turnover of construction workers, particularly unskilled workers. At any one time, a project may include a large proportion of inexperienced, temporary and transient workers who may not be fluent in the common language. Although construction work often must be done in teams, it is difficult to develop effective, safe teamwork under such conditions.
Like the workforce, the universe of construction contractors is marked by high turnover and consists mainly of small operations. Of the 1.9 million construction contractors in the United States identified by the 1990 Census, only 28% had any full-time employees. Just 136,000 (7%) had 10 or more employees. The degree of contractor participation in trade organizations varies by country. In the United States, only about 10 to 15% of contractors participate; in some European countries, this proportion is higher but still involves less than half of contractors. This makes it difficult to identify contractors and inform them of their rights and responsibilities under pertinent health and safety or any other legislation or regulations.
As in some other industries, an increasing proportion of contractors in the United States and Europe consists of individual workers hired as independent contractors by prime- or sub-contractors who employ workers. Ordinarily, an employing contractor does not provide subcontractors with health benefits, workers’ compensation coverage, unemployment insurance, pension benefits or other benefits. Nor do prime contractors have any obligation to subcontractors under health and safety regulations; these regulations govern rights and responsibilities as they apply to their own employees. This arrangement gives some independence to individuals who contract for their services, but at the cost of removing a wide range of benefits. It also relieves employing contractors of the obligation to provide mandated benefits to individuals who are contractors. This private arrangement subverts public policy and has been successfully challenged in court, yet it persists and may become more of a problem for the health and safety of workers on the job, regardless of their employment relationship. The US Bureau of Labor Statistics (BLS) estimates that 9% of the US workforce is self-employed, but in construction as many as 25% of workers are self-employed independent contractors.
Health Hazards on Construction Sites
Construction workers are exposed to a wide variety of health hazards on the job. Exposure differs from trade to trade, from job to job, by the day, even by the hour. Exposure to any one hazard is typically intermittent and of short duration, but is likely to reoccur. A worker may not only encounter the primary hazards of his or her own job, but may also be exposed as a bystander to hazards produced by those who work nearby or upwind. This pattern of exposure is a consequence of having many employers with jobs of relatively short duration and working alongside workers in other trades that generate other hazards. The severity of each hazard depends on the concentration and duration of exposure for that particular job. Bystander exposures can be approximated if one knows the trade of workers nearby. Hazards present for workers in particular trades are listed in table 2.
Table 2. Primary hazards encountered in skilled construction trades.
Each trade is listed below with an indication of the primary hazards to which a worker in that trade might be exposed. Exposure may occur to either supervisors or to wage earners. Hazards that are common to nearly all construction-heat, risk factors for musculoskeletal disorders and stress-are not listed.
The classifications of construction trades used here are those used in the United States. It includes the construction trades as classified in the Standard Occupational Classification system developed by the US Department of Commerce. This system classifies the trades by the principal skills inherent in the trade.
|
Occupations |
Hazards |
|
Brickmasons |
Cement dermatitis, awkward postures, heavy loads |
|
Stonemasons |
Cement dermatitis, awkward postures, heavy loads |
|
Hard tile setters |
Vapour from bonding agents, dermatitis, awkward postures |
|
Carpenters |
Wood dust, heavy loads, repetitive motion |
|
Drywall installers |
Plaster dust, walking on stilts, heavy loads, awkward postures |
|
Electricians |
Heavy metals in solder fumes, awkward posture, heavy loads, asbestos dust |
|
Electrical power installers and repairers |
Heavy metals in solder fumes, heavy loads, asbestos dust |
|
Painters |
Solvent vapours, toxic metals in pigments, paint additives |
|
Paperhangers |
Vapours from glue, awkward postures |
|
Plasterers |
Dermatitis, awkward postures |
|
Plumbers |
Lead fumes and particles, welding fumes |
|
Pipefitters |
Lead fumes and particles, welding fumes, asbestos dust |
|
Steamfitters |
Welding fumes, asbestos dust |
|
Carpet layers |
Knee trauma, awkward postures, glue and glue vapour |
|
Soft tile installers |
Bonding agents |
|
Concrete and terrazzo finishers |
Awkward postures |
|
Glaziers |
Awkward postures |
|
Insulation workers |
Asbestos, synthetic fibres, awkward postures |
|
Paving, surfacing and tamping equipment operators |
Asphalt emissions, gasoline and diesel engine exhaust, heat |
|
Rail- and track-laying equipment operators |
Silica dust, heat |
|
Roofers |
Roofing tar, heat, working at heights |
|
Sheetmetal duct installers |
Awkward postures, heavy loads, noise |
|
Structural metal installers |
Awkward postures, heavy loads, working at heights |
|
Welders |
Welding emissions |
|
Solderers |
Metal fumes, lead, cadmium |
|
Drillers, earth, rock |
Silica dust, whole-body vibration, noise |
|
Air hammer operators |
Noise, whole-body vibration, silica dust |
|
Pile driving operators |
Noise, whole-body vibration |
|
Hoist and winch operators |
Noise, lubricating oil |
|
Crane and tower operators |
Stress, isolation |
|
Excavating and loading machine operators |
Silica dust, histoplasmosis, whole-body vibration, heat stress, noise |
|
Grader, dozer and scraper operators |
Silica dust, whole-body vibration, heat noise |
|
Highway and street construction workers |
Asphalt emissions, heat, diesel engine exhaust |
|
Truck and tractor equipment operators |
Whole-body vibration, diesel engine exhaust |
|
Demolition workers |
Asbestos, lead, dust, noise |
|
Hazardous waste workers |
Heat, stress |
Construction Hazards
As in other jobs, hazards for construction workers are typically of four classes: chemical, physical, biological and social.
Chemical hazards
Chemical hazards are often airborne and can appear as dusts, fumes, mists, vapours or gases; thus, exposure usually occurs by inhalation, although some airborne hazards may settle on and be absorbed through the intact skin (e.g., pesticides and some organic solvents). Chemical hazards also occur in liquid or semi-liquid state (e.g., glues or adhesives, tar) or as powders (e.g., dry cement). Skin contact with chemicals in this state can occur in addition to possible inhalation of the vapour resulting in systemic poisoning or contact dermatitis. Chemicals might also be ingested with food or water, or might be inhaled by smoking.
Several illnesses have been linked to the construction trades, among them:
- silicosis among sand blasters, tunnel builders and rock drill operators
- asbestosis (and other diseases caused by asbestos) among asbestos insulation workers, steam pipe fitters, building demolition workers and others
- bronchitis among welders
- skin allergies among masons and others who work with cement
- neurologic disorders among painters and others exposed to organic solvents and lead.
Elevated death rates from cancer of the lung and respiratory tree have been found among asbestos insulation workers, roofers, welders and some woodworkers. Lead poisoning occurs among bridge rehabilitation workers and painters, and heat stress (from wearing full-body protective suits) among hazardous-waste clean-up workers and roofers. White finger (Raynaud’s syndrome) appears among some jackhammer operators and other workers who use vibrating drills (e.g., stoper drills among tunnellers).
Alcoholism and other alcohol-related disease is more frequent than expected among construction workers. Specific occupational causes have not been identified, but it is possible that it is related to stress resulting from lack of control over employment prospects, heavy work demands or social isolation due to unstable working relationships.
Physical hazards
Physical hazards are present in every construction project. These hazards include noise, heat and cold, radiation, vibration and barometric pressure. Construction work often must be done in extreme heat or cold, in windy, rainy, snowy, or foggy weather or at night. Ionizing and non-ionizing radiation is encountered, as are extremes of barometric pressure.
The machines that have transformed construction into an increasingly mechanized activity have also made it increasingly noisy. The sources of noise are engines of all kinds (e.g., on vehicles, air compressors and cranes), winches, rivet guns, nail guns, paint guns, pneumatic hammers, power saws, sanders, routers, planers, explosives and many more. Noise is present on demolition projects by the very activity of demolition. It affects not only the person operating a noise-making machine, but all those close-by and not only causes noise-induced hearing loss, but also masks other sounds that are important for communication and for safety.
Pneumatic hammers, many hand tools and earth-moving and other large mobile machines also subject workers to segmental and whole-body vibration.
Heat and cold hazards arise primarily because a large portion of construction work is conducted while exposed to the weather, the principal source of heat and cold hazards. Roofers are exposed to the sun, often with no protection, and often must heat pots of tar, thus receiving both heavy radiant and convective heat loads in addition to metabolic heat from physical labour. Heavy equipment operators may sit beside a hot engine and work in an enclosed cab with windows and without ventilation. Those that work in an open cab with no roof have no protection from the sun. Workers in protective gear, such as that needed for removal of hazardous waste, may generate metabolic heat from hard physical labour and get little relief since they may be in an air-tight suit. A shortage of potable water or shade contributes to heat stress as well. Construction workers also work in especially cold conditions during the winter, with danger of frostbite and hypothermia and risk of slipping on ice.
The principal sources of non-ionizing ultraviolet (UV) radiation are the sun and electric arc welding. Exposure to ionizing radiation is less common, but can occur with x-ray inspection of welds, for example, or it may occur with instruments such as flow meters that use radioactive isotopes. Lasers are becoming more common and may cause injury, especially to the eyes, if the beam is intercepted.
Those who work under water or in pressurized tunnels, in caissons or as divers are exposed to high barometric pressure. Such workers are at risk of developing a variety of conditions associated with high pressure: decompression sickness, inert gas narcosis, aseptic bone necrosis and other disorders.
Strains and sprains are among the most common injuries among construction workers. These, and many chronically disabling musculoskeletal disorders (such as tendinitis, carpal tunnel syndrome and low-back pain) occur as a result of either traumatic injury, repetitive forceful movements, awkward postures or overexertion (see figure 1). Falls due to unstable footing, unguarded holes and slips off scaffolding (see figure 2) and ladders are very common.
Figure 1. Carrying without appropriate work clothing and protective equipment.
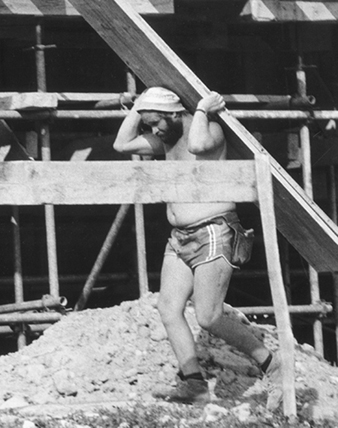
Figure 2. Unsafe scaffolding in Kathmandu, Nepal, 1974

Jane Seegal
Biological hazards
Biological hazards are presented by exposure to infectious micro-organisms, to toxic substances of biological origin or animal attacks. Excavation workers, for example, can develop histoplasmosis, an infection of the lung caused by a common soil fungus. Since there is constant change in the composition of the labour force on any one project, individual workers come in contact with other workers and, as a consequence, may become infected with contagious diseases—influenza or tuberculosis, for example. Workers may also be at risk of malaria, yellow fever or Lyme disease if work is conducted in areas where these organisms and their insect vectors are prevalent.
Toxic substances of plant origin come from poison ivy, poison oak, poison sumac and nettles, all of which can cause skin eruptions. Some wood dusts are carcinogenic, and some (e.g., western red cedar) are allergenic.
Attacks by animals are rare but may occur whenever a construction project disturbs them or encroaches on their habitat. This could include wasps, hornets, fire ants, snakes and many others. Underwater workers may be at risk from attack by sharks or other fish.
Social hazards
Social hazards stem from the social organization of the industry. Employment is intermittent and constantly changing, and control over many aspects of employment is limited because construction activity is dependent on many factors over which construction workers have no control, such as the state of an economy or the weather. Because of the same factors, there can be intense pressure to become more productive. Since the workforce is constantly changing, and with it the hours and location of work, and many projects require living in work camps away from home and family, construction workers may lack stable and dependable networks of social support. Features of construction work such as heavy workload, limited control and limited social support are the very factors associated with increased stress in other industries. These hazards are not unique to any trade, but are common to all construction workers in one way or another.
Evaluating Exposure
Evaluating either primary or bystander exposure requires knowing the tasks being done and the composition of ingredients and by-products associated with each job or task. This knowledge usually exists somewhere (e.g., material safety data sheets, MSDSs) but may not be available at the job site. With continually evolving computer and communications technology, it is relatively easy to obtain such information and make it available.
Controlling Occupational Hazards
Measuring and evaluating exposure to occupational hazards requires consideration of the novel manner in which construction workers are exposed. Conventional industrial hygiene measurements and exposure limits are based on 8-hour time-weighted averages. But since exposures in construction are usually brief, intermittent, varied but likely to be repeated, such measures and exposure limits are not as useful as in other jobs. Exposure measurement can be based on tasks rather than shifts. With this approach, separate tasks can be identified and hazards characterized for each. A task is a limited activity such as welding, soldering, sanding drywall, painting, installing plumbing and so on. As exposures are characterized for tasks, it should be possible to develop an exposure profile for an individual worker with knowledge of the tasks he or she performed or was near enough to be exposed to. As knowledge of task-based exposure increases, one may develop task-based controls.
Exposure varies with the concentration of the hazard and the frequency and duration of the task. As a general approach to hazard control, it is possible to reduce exposure by reducing the concentration or the duration or frequency of the task. Since exposure in construction is already intermittent, administrative controls that rely on reducing the frequency or duration of exposure are less practical than in other industries. Consequently, the most effective way to reduce exposure is to reduce the concentration of hazards. Other important aspects of controlling exposure include provisions for eating and sanitary facilities and education and training.
Decreasing exposure concentration
For reducing exposure concentration, it is useful to consider the source, the environment in which a hazard occurs and the workers who are exposed. As a general rule, the closer controls are to a source, the more efficient and effective they are. Three general types of controls can be used to reduce the concentration of occupational hazards. These are, from most to least effective:
- engineering controls at the source
- environmental controls that remove the hazard from the environment
- personal protection provided to the worker.
Engineering controls
Hazards originate at a source. The most efficient way to protect workers from hazards is to change the primary source with some sort of engineering change. For example, a less hazardous substance can be substituted for one that is more hazardous. Non-respirable synthetic vitreous fibres can be substituted for asbestos, and water can be substituted for organic solvents in paints. Similarly, non-silica abrasives can replace sand in abrasive blasting (also known as sand blasting). Or a process can be fundamentally changed, such as by replacing pneumatic hammers with impact hammers that generate less noise and vibration. If sawing or drilling generates harmful dusts, particulate matter or noise, these processes could be done by shear cutting or punching. Technological improvements are reducing the risks of some musculoskeletal and other health problems. Many of the changes are straightforward—for example, a two-handed screwdriver with a longer handle increases torque on the object and reduces stress on the wrists.
Environmental controls
Environmental controls are used to remove a hazardous substance from the environment, if the substance is airborne, or to shield the source, if it is a physical hazard. Local exhaust ventilation (LEV) can be used at a particular job with a ventilation duct and a hood to capture the fumes, vapours or dust. However, since the location of tasks that emit toxic materials changes, and because the structure itself changes, any LEV would have to be mobile and flexible in order to accommodate these changes. Mobile truck-mounted dust collectors with fans and filters, independent power sources, flexible ducts and mobile water supplies have been used on many job sites to provide LEV for a variety of hazard-producing processes.
The simple and effective method for controlling exposure to radiant physical hazards (noise, ultraviolet (UV) radiation from arc welding, infrared radiant (IR) heat from hot objects) is to shield them with some appropriate material. Plywood sheets shield IR and UV radiation, and material that absorbs and reflects sound will provide some protection from noise sources.
Major sources of heat stress are weather and hard physical labour. Adverse effects from heat stress can be avoided through reductions in the workload, provision of water and adequate breaks in the shade and, possibly, night work.
Personal protection
When engineering controls or changes in work practices do not adequately protect workers, workers may need to use personal protective equipment (PPE) (see figure 3). In order for such equipment to be effective, workers must be trained in its use, and the equipment must fit properly and be inspected and maintained. Furthermore, if others who are in the vicinity may be exposed to the hazard, they should either be protected or prevented from entering the area.
Figure 3. Construction worker in Nairobi, Kenya, without foot protection or hard hat

The use of some personal controls can create problems. For instance, construction workers often perform as teams and thus have to communicate with each other, but respirators interfere with communication. And full-body protective gear can contribute to heat stress because it is heavy and because body heat is not allowed to dissipate.
Having protective gear without knowing its limitations can also give workers or employers the illusion that the workers are protected when, with certain exposure conditions, they are not protected. For instance, there are no gloves currently available that protect for more than 2 hours against methylene chloride, a common ingredient in paint strippers. And there are few data on whether gloves protect against solvent mixtures such as those containing both acetone and toluene or both methanol and xylene. The level of protection depends on how a glove is used. In addition, gloves are generally tested on one chemical at a time and rarely for more than 8 hours.
Eating and sanitary facilities
A lack of eating and sanitary facilities may also lead to increased exposures. Often, workers cannot wash before meals and must eat in the work zone, which means they may inadvertently swallow toxic substances transferred from their hands to food or cigarettes. A lack of changing facilities at a worksite may result in transport of contaminants from the workplace to a worker’s home.
Injuries and Illnesses in Construction
Fatal injuries
Because construction involves a large proportion of the workforce, construction fatalities also affect a large population. For instance, in the United States, construction represents 5 to 6% of the workforce but accounts for 15% of work-related fatalities—more than any other sector. The construction sector in Japan is 10% of the workforce but has 42% of the work-related deaths; in Sweden, the numbers are 6% and 13%, respectively.
The most common fatal injuries among construction workers in the United States are falls (30%), transportation accidents (26%), contact with objects or equipment (e.g., struck by an object or caught in machinery or materials) (19%) and exposure to harmful substances (18%), most of which (75%) are electrocutions from contact with electrical wiring, overhead power lines or electrically powered machinery or hand tools. These four types of events account for nearly all (93%) fatal injuries among construction workers in the United States (Pollack et al. 1996).
Among trades in the US, the rate of fatal injuries is highest among structural steel workers (118 fatalities per 100,000 full-time equivalent workers for 1992–1993 compared to a rate of 17 per 100,000 for other trades combined) and 70% of structural steel worker fatalities were from falls. Labourers experienced the greatest number of fatalities, with an annual average number of about 200. Overall, the rate of fatalities was highest for workers 55 years and older.
The proportion of fatalities by event differed for each trade. For supervisors, falls and transportation accidents accounted for about 60% of all fatalities. For carpenters, painters, roofers and structural steel workers, falls were most common, accounting for 50, 55, 70 and 69% of all fatalities for those trades, respectively. For operating engineers and excavating machine operators, transportation accidents were the most common causes, accounting for 48 and 65% of fatalities for those trades, respectively. Most of these were associated with dump trucks. Fatalities from improperly sloped or shored trenches continue to be a major cause of fatalities (McVittie 1995). The primary hazards in the skilled trades are listed in table 2.
A study of Swedish construction workers did not find a high overall work-related mortality rate, but did find high death rates for particular conditions (see table 3).
Table 3. Construction occupations with excess standardized mortality rates (SMRs)and standardized incidence rates (SIRs) for selected causes.
|
Occupation |
Significantly higher SMRs |
Significantly higher SIRs |
|
Bricklayers |
- |
Peritoneal tumour |
|
Concrete workers |
All causes,* all cancers,* stomach cancer, violent death,* accidental falls |
Lip cancer, stomach and larynx cancer,*a lung cancerb |
|
Crane drivers |
Violent death* |
- |
|
Drivers |
All causes,* cardiovascular* |
Lip cancer |
|
Insulators |
All causes,* lung cancer, pneumoconiosis, violent death* |
Peritoneal tumour, lung cancer |
|
Machine operators |
Cardiovascular,* other accidents |
- |
|
Plumbers |
All cancers,* lung cancer, pneumoconiosis |
All cancers, pleural tumour, lung cancer |
|
Rock workers |
All causes,* cardiovascular,* |
- |
|
Sheet metal workers |
All cancers,* lung cancer, accidental falls |
All cancers, lung cancer |
|
Woodworkers/carpenters |
- |
Nose and nasal sinus cancer |
* Cancers or causes of death are significantly higher in comparison to all other occupational groups combined. “Other accidents” includes typical work-related injuries.
a The relative risk for larynx cancer among concrete workers, compared to carpenters, is 3 times higher.
b The relative risk for lung cancer among concrete workers, compared to carpenters, is almost double.
Source: Engholm and Englund 1995.
Disabling or lost time injuries
In the United States and Canada, the most common causes of lost time injuries are overexertion; being struck by an object; falls to a lower level; and slips, trips and falls on the same level. The most common category of injury is strains and sprains, some of which become sources of chronic pain and impairment. The activities most often associated with lost time injuries are manual materials handling and installation (e.g., installing dry-wall, piping or ventilation duct-work). Injuries occurring in transit (e.g., walking, climbing, descending) are also common. Underlying many of these injuries is the problem of housekeeping. Many slips, trips and falls are caused by walking through construction debris.
Costs of Injuries and Illness
Occupational injuries and illnesses in construction are very costly. Estimates for the cost of injuries in construction in the US range from $10 billion to $40 billion annually (Meridian Research 1994); at $20 billion, the cost per construction worker would be US$3,500 yearly. Workers’ compensation premiums for three trades—carpenters, masons and structural iron workers— averaged 28.6% of payroll nationally in mid-1994 (Powers 1994). Premium rates vary enormously, depending on trade and jurisdiction. The average premium cost is several times higher than in most industrialized countries, where workers’ compensation insurance premiums range from 3 to 6% of payroll. In addition to workers’ compensation, there are liability insurance premiums and other indirect costs, including reduced work crew efficiency, clean-up (from a cave-in or collapse, for instance) or overtime necessitated by an injury. Such indirect costs can be several times the workers’ compensation award.
Management for Safe Construction Work
Effective safety programmes have several features in common. They are manifest throughout organizations, from the highest offices of a general contractor to project managers, supervisors, union officials and workers on the job. Codes of practice are conscientiously implemented and evaluated. Costs of injury and illness are calculated and performance is measured; those that do well are rewarded, those that do not are penalized. Safety is an integral part of contracts and subcontracts. Everybody—managers, supervisors and workers—receives general, site-specific and site-relevant training and re-training. Inexperienced workers receive on-the-job training from experienced workers. In projects where such measures are implemented, injury rates are significantly lower than on otherwise comparable sites.
Preventing Accidents and Injuries
Entities in the industry with lower injury rates share several common characteristics: they have a clearly defined policy statement that applies throughout the organization, from top management to the project site. This policy statement refers to a specific code of practice that describes, in detail, the hazards and their control for the pertinent occupations and tasks at a site. Responsibilities are clearly assigned and standards of performance are stated. Failures to meet these standards are investigated and penalties imposed as appropriate. Meeting or exceeding standards is rewarded. An accounting system is used that shows the costs of each injury or accident and the benefits of injury prevention. Employees or their representatives are involved in establishing and administering a programme of injury prevention. Involvement often occurs in the formation of a joint labour or worker management committee. Physical examinations are performed to determine workers’ fitness for duty and job assignment. These exams are provided when first employed and when returning from a disability or other layoff.
Hazards are identified, analysed and controlled following the classes of hazards discussed in other articles in this chapter. The entire work site is inspected on a regular basis and results are recorded. Equipment is inspected to ensure its safe operation (e.g., brakes on vehicles, alarms, guards and so on). Injury hazards include those associated with the most common types of lost-time injuries: falls from heights or at the same level, lifting or other forms of manual materials handling, risk of electrocution, risk of injury associated with either highway or off-road vehicles, trench cave-ins and others. Health hazards would include airborne particles (such as silica, asbestos, synthetic vitreous fibres, diesel particulates), gases and vapours (such as carbon monoxide, solvent vapour, engine exhaust), physical hazards (such as noise, heat, hyperbaric pressure) and others, such as stress.
Preparations are made for emergency situations and emergency drills are conducted as needed. Preparations would include assignment of responsibilities, provision of first aid and immediate medical attention at the site, communication at the site and with others off the site (such as ambulances, family members, home offices and labour unions), transportation, designation of health care facilities, securing and stabilizing the environment where the emergency occurred, identifying witnesses and documenting events. As needed, emergency preparedness would also cover means of escape from an uncontrolled hazard such as fire or flood.
Accidents and injuries are investigated and recorded. The purpose of reports is to identify causes that could have been controlled so that, in the future, similar occurrences can be prevented. Reports should be organized with a standardized record-keeping system to better facilitate analysis and prevention. To facilitate comparison of injury rates from one situation to another, it is useful to identify the pertinent population of workers within which an injury occurred, and their hours worked, in order to calculate an injury rate (i.e., the number of injuries per hour worked or the number of hours worked between injuries).
Workers and supervisors receive training and education in safety. This education consists of teaching general principles of safety and health, is integrated into task training, is specific for each work site and covers procedures to follow in the event of an accident or injury. Education and training for workers and supervisors is an essential part of any effort to prevent injuries and disease. Training about safe work practices and procedures have been provided in many countries by some companies and trade unions. These procedures, include lockout and tagout of electrical power sources during maintenance procedures, use of lanyards while working at heights, shoring trenches, providing safe walking surfaces and so on. It is also important to provide site-specific training, covering unique features about the job site such as means of entry and exit. Training should include instruction about dangerous substances. Performance or hands-on training, demonstrating that one knows safe practices, is much better for instilling safe behaviour than classroom instruction and written examination.
In the United States, training about certain hazardous substances is mandated by federal law. The same concern in Germany led to development of the Gefahrstoff-Informationssystem der Berufsgenossenschaften der Bauwirtschaft, or GISBAU, programme. GISBAU works with manufacturers to determine the content of all substances used on construction sites. Equally important, the programme provides the information in a form to suit the differing needs of health staff, managers and workers. The information is available through training programmes, in print and on computer terminals at work sites. GISBAU gives advice about how to substitute for some hazardous substances and tells how to safely handle others. (See the chapter Using, storing and transporting chemicals.)
Information about chemical, physical and other health hazards is available at the work site in the languages that workers use. If workers are to work intelligently on the job, they should have the information necessary to decide what to do in specific situations.
And finally, contracts between contractors and subcontractors should include safety features. Provisions could include establishing a unified safety organization at multi-employer work sites, performance requirements and rewards and penalties.