- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Health Effects and Disease Patterns
Leather Tanning
The major International Standard Industrial Classification (ISIC) group for the leather and fur processing is 323. In the United States, the Standard Industrial Classification (SIC) group for leather and leather manufacturing products industry is SIC 311 (OMB 1987). This group includes establishments engaged in tanning, currying and finishing hides and skins, as well as establishments manufacturing finished leather and artificial leather products and some similar products made of other materials. Leather converter, belting and chamois leather are also included in SIC 311. In addition, parts of SIC 23 (i.e., SIC 2371 and 2386) include establishments involved in the manufacturing of coats, garments, accessories and trimmings made of fur and establishments involved in sheep-lined clothing.
There are many varieties of leather with different characteristics depending upon the animal species and the specific part of the body of the animal from which the hide is obtained. Hides are made from cattle or horse skins; fancy leather from the skin of the calf, pig, goat, sheep and so on; and reptile leather from crocodile, lizard, chameleon and so on.
Employment in the leather and leather manufacturing products industry has been associated with various diseases caused by biological, toxicological and carcinogenic agents. The specific disease associated with exposure in the leather industry depends upon the extent to which the worker is exposed to the agent(s), which is dependent upon the occupation and work area within the industry.
For the tanning process, the epidermis of the hide is first removed and only the dermis transformed into leather. During this process, infection is a constant hazard, since the hide serves as a medium for numerous micro-organisms. Colonies of fungi may develop, specifically Aspergillus niger and Penicillus glaucum (Martignone 1964). To avoid the development of fungi, chlorinated phenols, specifically pentachlorophenol, have been widely used; unfortunately, such chemicals have been found to be toxic to the worker. Yeasts of three genera (Rhodotorula, Cladosporium and Torulopsis) have also been found (Kallenberger 1978). Tetanus, anthrax, leptospirosis, epizootic aphtha, Q fever and brucellosis are examples of diseases that workers could contract during the tanning process due to infected hides (Valsecchi and Fiorio 1978).
Skin disorders such as eczema and contact (allergic) dermatitis have also been diagnosed among leather tanners exposed to preservatives applied to the hides (Abrams and Warr 1951). The leather tanning and finishing process has been shown to have the highest incidence of dermatoses of any working group in the United States (Stevens 1979). Irritations of the mucous membranes of the throat and nose and perforations of the nasal septum may also occur after inhaling chromic acid fumes liberated during the chrome-tanning process.
Tannery workers have the potential for exposure to numerous known or suspected occupational carcinogens, including hexavalent chromium salts, benzidine-based azo dyes, organic solvents (e.g., benzene and formaldehyde), pentachlorophenol, N-nitroso compounds, arsenic, dimethylformamide and airborne leather dusts. These exposures may result in the development of various site-specific cancers. An excess of lung cancer has been observed in studies carried out in Italy (Seniori, Merler and Saracci 1990; Bonassi et al. 1990) and in a case-control study carried out in the United States (Garabrant and Wegman 1984), but this result is not always supported by other studies (Mikoczy, Schutz and Hagmar 1994; Stern et al. 1987; Pippard and Acheson 1985). Chromium and arsenicals were mentioned as possible contributors to the lung cancer excess. A significantly increased risk of soft tissue sarcoma has been observed in at least two separate tannery studies, one in Italy and one in the United Kingdom; the investigators of both studies suggest that the chlorophenols used at the tanneries may have produced these malignancies (Seniori et al. 1989; Mikoczy, Schutz and Hagmar 1994).
A threefold statistically significant excess in pancreatic cancer mortality was noted in a Swedish case control study (Erdling et al. 1986); a 50% increase in pancreatic cancer was also noted in another study examining three Swedish tanneries (Mikoczy, Schutz and Hagmar 1994) and in a study of an Italian tannery (Seniori et al. 1989). Despite the excess risk of pancreatic cancer, no specific environmental agent was identified, and dietary factors were considered a possibility. An excess risk of testicular cancer was observed among leather tanners from the finishing department of one tannery; all three workers with testicular cancer had worked during the same time period and were exposed to dimethylformamide (Levin et al. 1987; Calvert et al. 1990). An excess risk of sinonasal cancer among leather tannery workers was observed in a case-control study in Italy; chromium, leather dust and tannins were indicated as possible aetiological agents (Comba et al. 1992; Battista et al. 1995). However, IARC research in the early 1980s found no evidence of an association between leather tanning and nasal cancer (IARC 1981). The results of a study of the Chinese leather tanning industry showed a statistically significant excess morbidity from bladder cancer among those tanners ever exposed to benzidine-based dyes, which increased with duration of exposure (Chen 1990).
Accidents are also a leading cause of disability in leather tannery workers. Slips and falls on wet and greasy floors are common, as are knife cuts from the trimming of hides. In addition, the machines used to process the hides are capable of crushing and inflicting bruises, abrasions and amputations. For example, United States Bureau of Labor Statistics (BLS) data for 1994 have shown an incidence rate in SIC 311 for injuries and illnesses combined of 19.1 per 100 full-time workers and an incidence rate for injuries alone of 16.4. These results are over 50% higher than the all-manufacturing incidence for illnesses and injuries combined, 12.2 per 100 full-time workers, and the incidence of 10.4 for injuries alone (BLS 1995).
Footwear
The handling and processing of leather in the manufacturing of shoes and boots may entail exposures to some of the same chemicals used in the tanning and finishing processes as cited above, giving rise to similar diseases. Furthermore, different chemicals used may also produce other diseases. Exposures to the toxic solvents used in adhesives and cleaners and to airborne leather dusts are of particular concern. One solvent of specific concern is benzene, which can produce thrombocytopenia; depression of the red blood cell, platelet and white cell counts; and pancytopenia. Benzene has largely been eliminated from the footwear industry. Peripheral neuropathy has also been found among workers in shoemaking factories due to n-hexane in the adhesives. This, too, has largely been substituted for by less toxic solvents. Electroencephalographic changes, liver damage and behavioural alterations have also been reported in connection with exposure to solvents in shoeworkers.
Benzene has been judged to be a human carcinogen (IARC 1982), and various investigators have observed excess leukaemias among workers exposed to benzene in the shoe industry. One study included the largest shoe manufacturing facility in Florence, Italy, consisting of over 2,000 employees. The study results revealed a fourfold excess risk of leukaemia, and benzene was cited as the most likely exposure (Paci et al. 1989). A follow-up to this study showed an over fivefold risk for those shoe workers employed in jobs where benzene exposure was substantial (Fu et al. 1996). A study in the United Kingdom examining mortality among males employed in shoe manufacturing found an elevated risk for leukaemia among workers handling glues and solvents which contained benzene (Pippard and Acheson 1985). Various studies of shoe industry workers in Istanbul, Turkey, have reported an excess risk of leukaemia from exposure to benzene. When benzene was later replaced by petrol, the absolute number of cases and risk of leukaemia dropped considerably (Aksoy, Erdem and DinCol 1974; 1976; Aksoy and Erdem 1978).
Various types of nasal cancer (adenocarcinoma, squamous-cell carcinoma and transitional-cell carcinoma) have been associated with employment in shoe manufacture and repair. Relative risks in excess of tenfold have been reported from studies in Italy and the United Kingdom (Fu et al. 1996; Comba et al. 1992; Merler et al. 1986; Pippard and Acheson 1985; Acheson 1972, 1976; Cecchi et al. 1980) but not in the United States (DeCoufle and Walrath 1987; Walker et al. 1993). The elevated nasal cancer risks were almost entirely accounted for by employees “heavily” exposed to leather dust in the preparation and finishing rooms. The mechanism by which exposure to leather dust may increase the risk of nasal cancer is not known.
Excesses of digestive and urinary tract cancers, such as bladder (Malker et al. 1984; Morrison et al. 1985), kidney (Walker et al. 1993; Malker et al. 1984), stomach (Walrath, DeCoufle and Thomas 1987) and rectal (DeCoufle and Walrath 1983; Walrath, DeCoufle and Thomas 1987) cancers, have been found in other studies of shoe workers but have not been consistently reported and have not been linked with particular exposures in the industry.
Ergonomic hazards causing work-related musculoskeletal disorders (WRMDs) are major problems in the shoe manufacturing industry. These hazards are due to the specialized equipment used and hands-on work requiring repetitive movements, forceful exertions and awkward body postures. BLS data show men’s footwear to be one of the “industries with the highest rates of nonfatal illness disorders associated with repeated trauma” (BLS 1995). The incidence rate for the total footwear industry for illnesses and injuries combined was found to be 11.9 per 100 workers, with 8.6 being the incidence rate for injuries alone. These rates are slightly less than the incidence rates for all manufacturing. WRMDs in the shoe manufacturing industry include conditions such as tendinitis, synovitis, tenosynovitis, bursitis, ganglionic cysts, strains, carpal tunnel syndrome, low-back pain and cervical spine injuries.
Fur Workers
Fur processing involves the activities of three categories of workers. Fur dressers flesh and tan skins; fur dyers then colour or tint the skins with natural or synthetic dyes; and finally fur service workers grade, match and bale dressed furs. Dressers and dyers are exposed to potential carcinogens including tannins, oxidative dyes, chromium and formaldehyde, whereas fur service workers are potentially exposed to residual tanning materials while handling previous dressed furs. Very few epidemiological studies have been conducted on fur workers. The only comprehensive study among these workers revealed statistically elevated risks of colo-rectal and liver cancer among the dyers, lung cancer among the dressers and cardiovascular diseases among the service workers as compared to overall rates in the United States (Sweeney, Walrath and Waxweiler 1985).
Footwear Industry
Adapted by P. Portich from the article in the 3rd edition of this Encyclopaedia by F.L. Conradi.
The term footwear covers a vast range of products made from many different materials. Boots, shoes, sandals, slippers, clogs and so forth are made wholly or partly of leather, rubber, synthetic and plastics materials, canvas, rope and wood. This article deals with the footwear industry as generally understood (i.e., based on traditional manufacturing methods). The manufacture of rubber boots (or their synthetic equivalents) is essentially a section of the rubber industry, which is covered in the chapter Rubber industry.
Shoes, boots and sandals made from leather, felts and other materials have been made by hand over the centuries. Fine shoes are still made wholly or partly by hand, but in all the industrialized countries there are now large mass-production plants. Even so, some work may still be given out to be done as home work. Child labour continues as one of the more serious problems in the footwear industry, although several countries have taken action against child labour with the help of various international programmes in this area.
Boot and shoe plants usually locate close to leather-producing areas (i.e., near cattle-raising country); some slipper and light-shoe making developed where there was a plentiful supply of felts from the textile trade, and in most countries the industry tends to be localized in its original centres. Leathers of different type and quality, and some reptile skins, formed the original materials, with a tougher quality skin for the soles. In recent years leather has been increasingly displaced by other materials, in particular rubber and plastics. Linings may be made of wool or polyamide (nylon) fabric or sheepskin; laces are made of horsehair or synthetic fibres; paper, cardboard and thermoplastics are used for stiffening. Natural and coloured wax, aniline dyes and colouring agents are used in finishing.
Economic and other factors have transformed the footwear industry in recent years. Tennis shoe manufacturing is one of the major growth sectors of the industry and has moved from production in predominantly one country to worldwide production, especially in developing countries in Asia and South America, in order to increase production and reduce costs. This migration of production to developing countries has also occurred in other sectors of the footwear industry.
Processes
There may be over a hundred operations in the making of a shoe, and only a brief summary is possible here. Mechanization has been applied at all stages, but the pattern of the hand process has been closely followed. Introduction of new materials has modified the process without changing its broad outline.
In the making of the uppers (tops of shoes), the leather or other material is sorted and prepared, and the uppers are then cut out on stitching (or dinting) presses by shaped, loose-knife tools. The parts, including the linings, are then “closed” (i.e., sewn or stuck together). Perforating, eyeletting and button-holing may also be carried out.
For making the bottom stock, soles, insoles, heels and welts, pieces are cut out in revolving presses using loose-knife cutters, or in sole-moulding presses; heels are made by compression of leather or wood strips. The stock is trimmed, shaped, scoured and stamped.
The uppers and bottom stock are assembled and then stitched, glued, nailed or screwed together. These operations are followed by shaping and levelling between rollers. The final finishing of the shoe includes waxing, colouring, spraying, polishing and packaging.
Among the raw materials used in the manufacturing process, the most important from the point of view of occupational hazards are the adhesives. These include natural solid and liquid adhesives and adhesive solutions based on organic solvents.
Hazards and Their Prevention
The intensive use of flammable liquids constitutes a considerable fire hazard, and the widespread use of presses and assembling machines has introduced an increased risk of mechanical accidents into this industry. The main health hazards are toxic solvents, high atmospheric dust concentrations, ergonomic risks and noise from the machines.
Fire
The solvents and sprays used in adhesives and finishing materials may be highly flammable. Precautions include:
- using the lowest flash point solvents possible
- using good general ventilation and local exhaust ventilation in spray booths and drying racks to reduce the concentration of flammable vapours
- removing combustible residues from cabinets and workbenches and provide closed containers for solvent-containing and oily wastes
- maintaining unobstructed exits and gangways
- minimizing the amount of stored flammable liquids; keep them in approved containers, cabinets and storage rooms
- ensuring that all electrical equipment and wiring near flammable solvents meets appropriate electrical codes
- grounding adequately polishing machines and other sources of static electricity.
Accidents
Many of the operating parts of the machines present serious hazards, in particular presses, stampers, rollers and knives. The loose-knife cutters at stitching and revolving presses can cause serious injury. The appropriate precautions minimally include two-hand controls (a photo-electric cell device for automatically cutting power may be preferable), the reduction of stroke rate to a safe level in relation to the size of the cutter, and the use of well-designed, stable cutters of adequate height, with flanges fitted perhaps with handles. Sole-moulding and heel presses should be guarded to prevent hand access. Stamping machines can cause burns as well as crushing injuries unless hand access is prevented by guarding. Nips of rollers and knives of milling and shaping machines should be fitted with suitable machinery guarding. The shading and polishing wheels of finishing machines and the spindles on which they are mounted should also be guarded. There should be an effective lockout/tagout programme for repair and maintenance work.
Health hazards
Organic solvents can cause acute and chronic effects on the central nervous system. Benzene, which was formerly used in adhesives and solvents, has been replaced by toluene, xylene, hexane, methyl ethyl ketone (MEK) and methyl butyl ketone (MBK). Both n-hexane and MBK can cause peripheral neuropathy and should be replaced by heptane or other solvents.
Outbreaks of a disease known popularly as “shoemakers’ paralysis” have appeared in a number of factories, presenting a clinical picture of a more or less severe form of paralysis. This paralysis is of the flaccid type, it is localized in the limbs (pelvic or thoracic) and gives rise to osteo-tendinous atrophy with areflexia and no alteration in superficial or deep sensitivity. Clinically, it is a syndrome resulting from functional inhibition or injury of the lower motor neurons of the voluntary motor system (pyramidal tract). The common outcome is neurological regression with extensive proximo-distal functional recuperation.
Good general ventilation and exhaust ventilation at the point of origin of the vapours should be provided to maintain concentrations well below maximum permissible levels. If these levels are observed, the fire risk will also be diminished. Minimizing the amount of solvent used, enclosure of solvent-using equipment and closing solvent containers are also important precautions.
Finishing machines produce dust, which should be removed from the atmosphere by exhaust ventilation. Some of the polishes, stains, colours and polychloroprene glues may carry a dermatitis risk. Good washing and sanitary facilities should be maintained and personal hygiene encouraged.
The increased intensive use of machines and equipment creates a significant noise hazard, necessitating source control of the noise or other preventive measures to prevent hearing loss. There should also be a hearing conservation programme.
Prolonged work on nailing machines which produce high levels of vibration may produce “dead hand” (Raynaud’s phenomenon). It is advisable to restrict the time spent at these machines.
Low-back pain and repetitive strain injuries are two musculoskeletal diseases that are major problems in the footwear industry. Ergonomic solutions are essential for prevention of these problems. Pre-placement and periodic medical examinations linked to workplace hazards are an effective factor for protection of employees’ health.
Environmental and Public Health Hazards
Earth Summit 1992, held in Rio de Janeiro, dealt with environmental concerns, and its proposals for future action, known as Agenda 21, could transform the footwear industry with its emphasis on recycling. In general, however, most waste materials are disposed of in landfills. Without proper precautions, this can result in contamination of the ground and groundwater.
Although home work has social advantages in decreasing unemployment and in the formation of cooperatives, the problems of ensuring proper precautions and working conditions in the home are enormous. In addition, other family members can be at risk if they are not already involved in the work. As discussed previously, child labour remains a serious problem.
Fur Industry
Adapted from the article by the author that appeared in the 3rd edition of this Encyclopaedia. Acknowledgements to Gary Meisel and to Tom Cunningham of the United Food and Commercial Workers Union for reviewing and adapting this article
Rudimentary means of preserving furs have been used since very early times and are still practised in many parts of the world. Typically, after the pelt is scraped and cleaned by washing, the skin is impregnated with animal oil, which serves to preserve it and make it more pliable. The pelt may be beaten or chewed after the oil treatment in order to effect better impregnation by the oil.
In the modern fur industry, pelts are obtained from fur farmers, trappers or hunters. At this stage they have been stripped from the carcass, flesh and fatty deposits have been removed by scraping and the pelts have been stretched and air dried. The fur industry grades the pelts according to factors such as the general condition of the pelt, fur length, curl and patterning. The pelts go through a series of treatment steps, called fur dressing, to preserve them (see figure 1). The furs may also be dyed. Fur dressing and dyeing are done in batches, with the pelts usually being transferred from one step to another using hand carts.
Figure 1. Flow chart of fur dressing
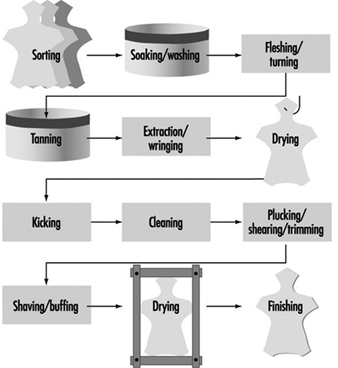
Fur Dressing
First, the pelts are sorted, stamped with an identifying mark, and cut open using knives and snippers. They are then soaked in salt water in tubs or barrels for several hours to re-soften them (see figure 2). Rotating paddles are often used to help this soaking. Sometimes formic acid, lactic acid or sulphuric acid is used in the soaking step. The excess water is then removed in revolving drums.
Figure 2. Soaking department in a fur-processing works

Office du film du Quebec
Next, the underside of the pelt is drawn across razor-sharp round-knife fleshing machines by workers known as fleshers (figure 3). Hand turning (turning the pelt inside out) and trimming with knives is also done. This operation removes the loose connective tissue from the underside of the skin. The object is to remove, as far as possible, any tissue which is not involved in the attachment of the fur, thus producing the maximum degree of lightness and flexibility of the pelt.
Figure 3. Machine fleshing of lamb skins

Office du film du Quebec
The pelts are now ready for tanning and are soaked in alum solution in pits or tubs. As with soaking, paddles are used. The alum solution is usually acidified somewhat with hydrochloric or sulphuric acid. The alum treatment may be carried out in either an aqueous or an oil solution. Excess liquid is extracted and the pelts are dried in special drying rooms to set the skin collagen.
The tanned pelts are then treated with an oil solution in a kicking machine or similar type of machine to force the oil into the skin. They are then cleaned in rotating drums containing sawdust, which absorbs moisture and excess oil.
Pelts contain guard hairs as well as the softer fur fibres. The guard hairs are stiffer and longer than the fur fibres and, depending on the type of fur and the final product desired, these hairs may be either partially or totally removed by machine or by hand plucking. Some pelts also require shearing or trimming with knives (see figure 4).
Figure 4. Shearing operation on Canadian beaver pelts

Office du film du Quebec
Other steps can include shaving or “paring out” with round-knife fleshers, buffing with buffing machines, drying and finishing. The latter can include degreasing, stretching, cleaning, buffing, brushing and lusterizing with lacquers and resins.
Dyeing
Although dyeing of furs was at one time not looked upon favourably, it is now an accepted part of fur preparation and is practised extensively. This can be done at the same time as tanning or in a subsequent step. The usual procedure involves treatment of the pelts with a weak alkaline solution (e.g., sodium carbonate) to remove dirt and oil residues. The pelts are then soaked in a mordant solution (e.g., ferric sulphate), after which they are steeped in dye solution until the desired colour is obtained. They are then repeatedly rinsed and drum-dried with the aid of sawdust.
Many other chemicals may be used in dyeing, including ammonia, ammonium chloride, formaldehyde, hydrogen peroxide, lead acetate or nitrate, oxalic acid, sodium perborate,
p-phenylenediamine dyes, benzidine dyes and so forth.
Fur Garment Manufacture
Before being made into garments, pelts may be cut and “let out”. This involves making a series of closely spaced diagonal or V-shaped slits in the skin, after which the pelt is pulled in order either to lengthen or to broaden it as needed. The pelt is then re-sewn (see figure 5). This type of operation requires great skill and experience. The pelts are next thoroughly moistened and then laid out and tacked on a board according to a chalked-on pattern, left to dry and sewn together. Finally, lining and other finishing steps complete the garment.
Figure 5. Operators engaged in the machine sewing of skins

Office du film du Quebec
Hazards and Their Prevention
Accidents
Some of the machines used in fur processing present serious hazards unless sufficient guarding is maintained: in particular, all drums should be protected with an interlocking gate and the centrifuges used for extraction of moisture should be fitted with interlocking lids; fur clipping and fur cutting machines should be totally enclosed except for the feed and discharge openings.
Vats should be covered or effectively railed to prevent accidental immersion. Falls on wet and slippery floors can be largely prevented by maintenance of sound, impervious surfaces, well-drained and frequently cleaned. Dyeing vats should be surrounded by drainage channels. Accidents caused by hand tools can be reduced if the handles are well designed and the tools well maintained. In the fur manufacturing sector, sewing machines require similar protection to those used in the garment trade (e.g., guarding of driving mechanisms and of needles).
Health Hazards
The use by the fur industry of such a large proportion of pelts from animals bred in captivity has considerably reduced the likelihood of transmission of animal diseases to fur workers. Nevertheless, anthrax may occur in workers handling carcasses, skins, hides or hairs from infected animals; a vaccine may be administered to all likely to have contact. All concerned should be aware of the risk and trained to report any suspicious symptoms immediately.
Various chemicals used in the fur industry are potential skin irritants. These include alkalis, acids, alum, chromates, bleaching agents, oils, salt and the compounds involved in the dyeing process, which comprise various types of dyes as well as mordants.
Unpacking of bales which have been treated with dusting powder in their countries of origin, drumming, plucking, unhairing and shearing can all produce irritant dust. In dye houses and dye kitchens, where salts of lead, copper and chromium (and possibly carcinogenic dyes) are weighed and cooked, there is also a risk of ingestion of toxic dusts. Injurious vapours may arise from degreasing solvents and fumigating chemicals. There is also the possibility of development of contact sensitization (allergy) to some of these chemicals or to the dust from one or more of the types of fur being handled.
The main protection against the hazards of dust and vapours is the provision of local exhaust ventilation; good general ventilation is also necessary throughout the process. Good housekeeping is important to remove dust. Personal respiratory protective equipment may be necessary for short-term jobs or in addition to local exhaust at particularly dusty operations. Particular attention should be paid to potential confined space hazards in pits and vats used for soaking/washing, tanning and dyeing.
Protective clothing appropriate to the process is necessary at most stages of fur processing. Rubber hand protection, foot and leg protection and aprons are required for wet processes (e.g., at the dye and mordant vats) and as a protection against acids, alkalis and corrosive chemicals. Good sanitary and washing facilities, including showers, should be provided. Bleaches and strong alkali soaps should not be used for hand cleansing.
Ergonomic problems can result from manual lifting and moving of materials, especially pushing hand carts, and manual loading and unloading of pelts (particularly when wet). Automation of these processes can help solve these problems. Repetitive motions in fur garment manufacture are also a source of ergonomic problems.
Heat stress diseases can occur while working in the drying room. Preventive measures include adequate exhaust of hot air and supply of cool air, limiting exposure time, readily accessible drinking water and training in the recognition of heat stress symptoms and in first aid measures.
Noise can be a problem with many of the machines used, especially in drums and combing, shearing and lusterizing machines.
Pre-placement medical examination can assist in the prevention of dermatitis by proper placement of employees with a history of sensitivity. Medical supervision is desirable; well maintained first-aid provisions in the charge of trained personnel are essential. Strict attention to hygiene, ventilation and temperature are necessary in the many small workrooms in which much of the making of fur garments is done.
Tanning and Leather Finishing
Some text was revised from the article authored by V.P.Gupta in the 3rd edition of this Encyclopaedia.
Tanning is the chemical process that converts animal hides and skins into leather. The term hide is used for the skin of large animals (e.g., cows or horses), while skin is used for that of small animals (e.g., sheep). Hides and skins are mostly by-products of slaughterhouses, although they may also come from animals that have died naturally or been hunted or trapped. Tanning industries are usually located near stock-raising regions; however, hides and skins may be preserved and transported prior to tanning, so the industry is widespread.
The tanning process consists in strengthening the hide’s protein structure by creating a bond between the peptide chains. The hide is composed of three layers: epidermis, dermis and subcutaneous layer. The dermis consists of about 30 to 35% protein, which is mostly collagen, with the remainder being water and fat. The dermis is used to make leather after the other layers have been removed using chemical and mechanical means. The tanning process uses acids, alkalis, salts, enzymes and tanning agents to dissolve fats and non-fibrous proteins and chemically bond the collagen fibres together.
Tanning has been practised since prehistoric times. The oldest system of tanning relies on the chemical action of vegetable material containing tannin (tannic acid). Extracts are taken from the parts of plants that are rich in tannin and processed into tanning liquors. The hides are soaked in pits or vats of increasingly strong liquors until they are tanned, which may take weeks or months. This process is used in countries with low levels of technology. This process is also used in developed countries to produce firmer, thicker leather for shoe soles, bags, cases and straps, although process changes have been introduced to shorten the time needed for tanning. Chemical tanning using mineral salts such as chromium sulphate was introduced during the late 19th century and has become the primary process to produce softer, thinner leather for goods such as handbags, gloves, garments, upholstery and shoe uppers. Tanning may also be accomplished using fish oils or synthetic tannins.
There is great variation in the scale and types of tanning facilities. Some tanneries are highly mechanized and use closed automatic systems and many chemicals, whereas others still use largely manual work and natural tanning substances with techniques essentially unchanged over the centuries (see figure 1). The type of product required (e.g., heavy-duty leather or fine flexible leathers) influences the choice of tanning agents and the finishing required.
Figure 1. Manual working methods in an Afghanistan tannery

Process Description
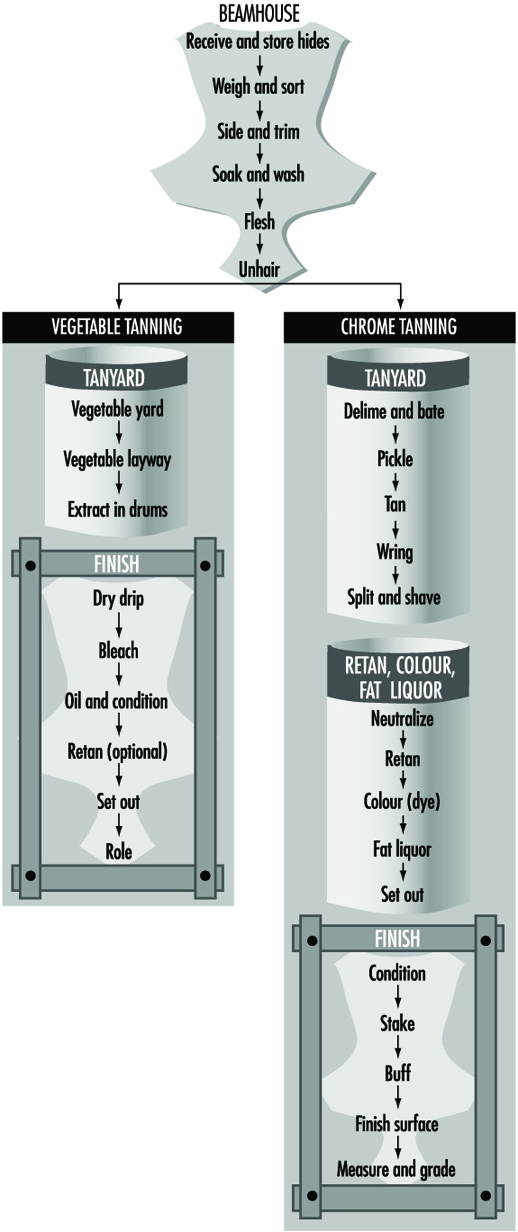
Leather production can be divided into three stages: preparation of the hide for tanning, which includes processes such as the removal of hair and adherent flesh; the tanning process; and the finishing process. Finishing includes mechanical processes to shape and smooth the leather and chemical treatments to colour, lubricate, soften and apply a surface finish to the leather (see figure 2). All of these processes may take place in one facility, although it is common for leather finishing to be conducted at locations different from tanning in order to take advantage of transportation costs and local markets. The implication is that it affects the likelihood of cross-contamination among the processes.
Figure 2. Typical processes for leather tanning & finishing
Curing and shipment. Because raw hides and skins decay rapidly, they are preserved and disinfected prior to shipment to the tannery. The hide or skin is flayed from the carcass and then preserved by curing. Curing can be accomplished by a variety of means. Curing by drying is suitable in regions where hot and dry climatic conditions prevail. Drying consists of stretching the hides on frames or spreading them on the ground in the sun. Dry-salting, another method of curing hides, consists of rubbing the fleshy side of the hide with salt. Brine curing, or brining, consists of submerging the hides in a solution of sodium chloride to which naphthalene may have been added. Brining is the most common form of preservation in developed countries.
Prior to shipment, hides are generally treated with DDT, zinc chloride, mercury chloride, chlorophenols or other agents for disinfection. These substances may represent hazards both at the site of curing and on receipt at the tannery.
Preparation. The cured hides and skins are prepared for tanning by several operations, collectively referred to as beamhouse operations. First the hides are sorted, trimmed and then washed in vats or drums. Disinfectants such as bleaching powder, chlorine and sodium acid fluoride in the water prevent putrefaction of hides. Chemicals such as caustic soda, sodium sulphide and surfactants are added to the water to accelerate soaking of dry-salted or dried hides.
The soaked hides and skins are then limed by immersing in milk of lime to loosen the epidermis and hair roots and to remove other unwanted soluble proteins and fats. In another method, a depilatory paste of lime, sulphide and salt is applied to the flesh side of the skins in order to save hair and wool. The limed hides are unhaired to remove the loosened hairs and defleshed. Epidermal debris and fine hair roots are mechanically removed by the scudding operation.
These operations are followed by deliming and bating with buffering salts, such as ammonium sulphate or ammonium chloride, and the action of proteolytic enzymes neutralizes the high alkalinity of limed hides. In pickling, hides are placed in an acid environment consisting of sodium chloride and sulphuric acid. The acid is necessary because chrome-tanning agents are not soluble under alkaline conditions. Vegetable-tanned hides do not need to be pickled.
Many of the beamhouse operations are carried out by processing the hides in solutions using large pits, vats or drums. Solutions are piped or poured into the containers and later emptied through pipes or into open drainage channels in the work area. The chemicals may be added to the containers by pipes or manually by workers. Good ventilation and personal protective equipment are needed to prevent respiratory and dermal exposure.
Tanyard. Various substances may be used for tanning, but the main distinction is between vegetable and chrome tanning. Vegetable tanning may be carried out either in pits or in rotating drums. Rapid tanning, in which high concentrations of tannins are used, is carried out in rotating drums. The chrome-tanning process most often used is the one-bath method, in which the hides are milled in a colloidal solution of chromium (III) sulphate until tanning is complete. A two-bath chrome-tanning process was used in the past, but this process involved potential exposure to hexavalent chromium salts and required more manual handling of the hides. The two-bath process is now considered obsolete and is rarely used.
Once tanned, the hide is further processed to shape and condition the leather. The hide is removed from the solution and excess water is removed by wringing. Chrome leather must be neutralized after being tanned. Splitting is the longitudinal division of wet or dry leather that is too thick, for articles such as shoe uppers and leather goods. Roll machines with cutting blades are used to further reduce the leather to the thickness required. A large amount of dust may be released when the leather is split or shaved while dry.
Re-tanning, colouring and fat-liquoring. After tanning, most leathers except sole leathers undergo colouring (dyeing). Generally, colouring is performed in a batch mode; and re-tanning, colouring and fat liquoring operations are all performed in sequence in the same drum with intermediate steps of washing and drying. Three major types of dyes are used: acid, basic and direct. Blends of dyes are used in order to obtain the exact shade desired, so the composition is not always known except by the supplier. The purpose of fat-liquoring is to lubricate leather to give it strength and flexibility. Oils, natural fats, their transformation products, mineral oils and several synthetic fats are used.
Finishing. After drying, vegetable tanned leather is subjected to mechanical operations (setting and rolling) and given a final polish. The finishing process for chrome leather includes a series of mechanical operations and, normally, the application of a covering layer to the leather surface. Staking is a mechanical beating operation used to make the leather soft. To improve the final appearance, the grain side of the leather is buffed using a sanding drum. This process generates a tremendous amount of dust.
A final surface finish is applied, which may contain solvents, plasticizers, binders and pigments. These solutions are applied by pads, flow coating or spraying. Some tanneries employ hand labour to apply the finish using pads, but this is usually carried out by machines. In flow coating, the solution is pumped into a reservoir above the conveyor carrying the leather and flows down onto it. In most cases, painted or sprayed leathers are not dried in ovens, but on trays on shelves. This practice provides a wide evaporating surface and contributes to air pollution.
Hazards and Their Prevention
Infectious hazards. In the early stages of the beamhouse operations, there may be some risk of infection due to zoonoses from the raw hides. Anthrax was a recognized hazard among workers engaged in handling hides and skins, particularly dry and dry-salted hides. This hazard has been virtually eliminated in tanneries due to disinfection of hides prior to shipment to the facilities. Colonies of fungi may develop on leathers and on the surface of the liquors.
Injuries. Slippery, wet and greasy floors form a serious hazard in all parts of a tannery. All floors should be of impervious material, have an even surface and be well drained. Good maintenance and housekeeping are essential. Mechanized transfer of hides and skins from one operation to another and proper drainage of liquors from vats and drums will help to reduce spillage and manual-handling ergonomic problems. Open pits and vats should be fenced to prevent injuries due to drowning and scalds.
There are many hazards connected with the operating parts of the machines—for example, injuries caused by revolving drums, in-running rollers and knives. Efficient guarding should be provided. All transmission machinery, belts, pulleys and gear wheels should be guarded.
Several operations involve manual lifting of the hides and leather, which represents an ergonomic hazard. Noise associated with the machinery is another potential hazard.
Dust. Dust is produced in a variety of tanning operations. Chemical dust can be produced during the loading of hide-processing drums. Leather dust is produced during mechanical operations. Buffing is the major source of dust. The dust in tanneries may be impregnated with chemicals, as well as fragments of hair, mould and excrement. Effective ventilation is needed for dust removal.
Chemical hazards. The large variety of acids, alkalis, tannins, solvents, disinfectants and other chemicals can be respiratory and skin irritants. Dusts of vegetable tanning materials, lime and leather and chemical mists and vapours arising in the various processes may be responsible for causing chronic bronchitis. Several chemicals may cause contact dermatitis. Chrome ulceration may occur in chrome tanning, especially on the hands. Exposures in the beamhouse operations are mainly to sulphur compounds such as sulphides and sulphates. Since these are alkaline substances, there is a potential to generate hydrogen sulphide gas if these substances contact acids.
Potential cancer-causing agents used in leather tanning and finishing include hexavalent chromium salts (in the past), aniline and azo dyes, vegetable tannins, organic solvents, formaldehyde and chlorophenols. The International Agency for Research on Cancer (IARC) evaluated the leather tanning industry in the early 1980s and concluded that there was no evidence to suggest an association between leather tanning and nasal cancer (IARC 1981). Case reports and epidemiological studies since the IARC evaluation have indicated increased risk for cancers among leather tanning and finishing workers—including lung cancer, sinonasal cancer and pancreatic cancer associated with leather dust and tanning (Mikoczy et al. 1996) and bladder cancer and testicular cancer associated with dyes or solvents in the finishing process (Stern et al. 1987). None of these associations is clearly established at this time.
General Profile
Animal furs and leather from tanned animal hides and skins have been used to make clothing for thousands of years. Fur and leather remain important industries today. Fur is used to produce a variety of outer garments, such as coats, jackets, hats, gloves and boots, and it provides trim for other types of garments as well. Leather is used to make garments and can be employed in the manufacture of other products, including leather upholstery for automobiles and furniture, and a wide variety of leather goods, such as watch straps, purses and suitcases. Footwear is another traditional leather product.
Fur-producing animals include aquatic species such as beaver, otter, muskrat and seal; northern land species such as fox, wolf, mink, weasel, bear, marten and raccoon; and tropical species such as leopard, ocelot and cheetah. In addition, the young of certain animals such as cattle, horse, pig and goat may be processed to produce furs. Although most fur-bearing animals are trapped, mink in particular is produced on fur farms.
Production
The major sources of leather are cattle, pigs, lambs and sheep. As of 1990, the United States was the largest producer of bovine hides and skins. Other significant producers include Argentina, Australia, Brazil, China, France, Germany (former Federal Republic) and India. Australia, China, India, Islamic Republic of Iran, New Zealand, the Russian Federation, Turkey and the United Kingdom are major producers of sheepskins. Goatskins are largely produced in China, India and Pakistan. The major producers of pigskin are China, Eastern Europe and the former USSR.
An analysis prepared by Landell Mills Commodities Studies (LMC) for the International Labour Organization (ILO) shows that the international market for hides is increasingly dominated by a few large producing countries in North America, Western Europe and Oceania, which allow free exportation of hides in any form. The tanning industry in the United States has been shrinking steadily since 1981, while most surviving tanneries in northern Europe have diversified in order to reduce dependence on the footwear-leather market. Worldwide footwear production has continued to shift primarily to Southeast Asia (ILO 1992).
Several factors influence the overall demand for leather throughout the world: the level, rate of growth and distribution of income; the price of leather compared to alternative materials; and changes in consumers’ preference for leather over alternative materials for a variety of products.
The fastest growing end-use sector in the leather industry has been leather upholstery, which accounted for about one-third of the world’s high-quality bovine leather production in 1990. Over one-third of all upholstery leather is destined for the vehicle industry and, according to LMC forecasts, the prospects for this subsector are fairly bright. The proportion of cars with leather upholstery has increased substantially through the 1990s.
The demand for leather garments is determined primarily by income and fashion, while fashion particularly influences the changing demand for specific types of leather. For example, a strong demand for the softer, more supple sheepskin leather in fashion garments motivated the production of the fashionable garment nappa from sheepskins and cattle hides.
The major producers of mink pelts in 1996 were Canada, the Russian Federation, the Scandinavian countries and the United States.
Between 1980 and 1989, leather employment increased in China, Hungary, India, Indonesia, the Republic of Korea, Uruguay and Venezuela and decreased in Australia, Colombia, Kenya, the Philippines, Poland and the United States. Leather employment also fell in Denmark, Finland, Norway and Sweden. In Botswana leather employment declined sharply in 1984, then experienced a steep increase, doubling the 1980 level by 1988.
There are several issues which will affect future production and employment in the leather, footwear and fur industries. New technology, the relocation of footwear production to developing countries and environmental regulations in the tanning industry will continue to affect the skills and the health and safety of workers in these industries.
Health Effects and Environmental Issues
Health Problems and Disease Patterns
Garment production workers are at risk for the development of WRMDs; occupational asthma; contact and irritative dermatitis; eye, nose and throat irritative symptoms; lung, nasopharyngeal and bladder cancers; and noise-induced hearing loss. Additionally, as some processes in this industry involve exposure to heated plastic fumes, metal dust and fumes (especially lead), leather dust, wool dust and hazardous solvents such as dimethyl formamide, the illnesses associated with these exposures may also be seen among garment workers. Electromagnetic field exposures generated by sewing machine motors are an area of increasing concern. Associations have been reported between maternal employment in apparel production and adverse reproductive outcomes.
Table 1 summarizes the spectrum of occupational diseases which may be seen in the clothing and finished textile industry.
Table 1. Examples of occupational diseases which may be seen in garment workers
|
Condition |
Exposure |
|
Musculoskeletal disorders |
|
|
Carpal tunnel syndrome, forearm tendinitis, |
Force |
|
Asthma |
Formaldehyde |
|
Cancer |
|
|
Bladder cancer |
Dyes |
|
Lung, nasopharyngeal cancer |
Formaldehyde |
|
Hearing loss |
Noise |
|
Skin |
|
|
Contact and irritative dermatitis |
Formaldehyde, textile dyes |
|
Lead poisoning |
Lead |
Musculoskeletal disorders. Garment production involves the performance of monotonous, highly repetitive and high-speed tasks, often requiring non-neutral and awkward joint postures. These exposures place garment workers at risk of developing WRMDs of the neck, upper extremities, back and lower extremities (Andersen and Gaardboe 1993; Schibye et al. 1995). It is not uncommon for garment workers to develop multiple WRMDs, often with both soft-tissue disorders, such as tendinitis, and concomitant nerve entrapment syndromes, such as carpal tunnel syndrome (Punnett et al. 1985; Schibye et al. 1995).
Sewing machine operators and hand sewers (sample-makers and finishers) perform work which requires repetitive hand and wrist movements, typically performed with non-neutral postures of the fingers, wrist, elbows, shoulders and neck. Therefore, they are at risk for developing carpal tunnel syndrome, ganglion cysts, forearm tendinitis, epicondylitis, shoulder disorders including bicipital and rotator cuff tendinitis, rotator cuff tears and neck disorders. Additionally, sewing machine operation typically requires prolonged sitting (often in seats without backrests and in workstations that necessitate leaning forward from the waist), intermittent lifting and repetitive use of foot pedals. Thus, sewing machine operators may develop WRMDs of the low back and lower extremities.
Cutters, whose work requires lifting and carrying of fabric rolls as well as operation of hand-held or computer-operated cutting machines, are also at risk for development of musculoskeletal disorders of the neck, shoulder, elbow, forearm/wrist and low back. Pressers are at risk for developing tendinitis and related disorders of the shoulder, elbow and forearm, and may also be at risk for developing related nerve entrapment disorders.
In addition to ergonomic/biomechanical factors, rapid piece-rate production systems and work organizational factors described more fully in the previous section may contribute to musculoskeletal disorders among workers in the clothing industry. In one study of garment workers, duration of employment in piece-work was found to be associated with an increased prevalence of severe disability (Brisson et al. 1989). Consequently, prevention of work-related musculoskeletal disorders may require both workplace ergonomic modifications and attention to work organization issues, including piece-work.
Chemical hazards. Resin-treated fabrics used in permanent press clothing may release formaldehyde. Exposures are greatest during cutting, because off-gassing is greatest when fabric bolts are first unrolled; during pressing, as heating promotes the liberation of formaldehyde from residual amounts of resins; in production areas in which large quantities of fabric are being used; and in warehouse and retail areas. Many garment shops are poorly ventilated and afford poor control of ambient temperatures. With increased temperature, off-gassing is greater; with poor ventilation, increasing ambient concentrations of formaldehyde can accumulate. Formaldehyde is a well-recognized acute irritant of the eyes, nose, throat and upper and lower airways. Formaldehyde may be a cause of occupational asthma due to either irritative effects or allergic sensitization (Friedman-Jimenez 1994; Ng et al. 1994).
Formaldehyde exposure has been associated in a number of studies with the development of lung and nasopharyngeal cancers (Alderson 1986). Additionally, formaldehyde exposure can result in both allergic contact and irritative dermatitis. Garment workers may develop a chronic, eczema-like dermatitis of the hands and arms which is likely related to sensitization to formaldehyde. The irritative and other non-allergic health effects of formaldehyde can be minimized by the implementation of proper ventilation systems and product substitution where feasible. Allergic sensitization, however, can occur at lower levels of exposure. Once a garment worker has developed allergic sensitization, removal from exposure may be necessary.
Workers in the finished textile industry may sustain exposure to organic solvents. Solvents such as perchlorethylene, trichlorethylene and 1,1,1-trichlorethane are frequently used in finishing departments for stain removal. Health effects due to such exposures may include central nervous system depression, peripheral neuropathy, dermatitis and, less commonly, liver toxicity. Dimethyl formamide (DMF) is a particularly hazardous solvent which has been employed to waterproof fabric. Its use in one such setting resulted in an outbreak of occupational hepatitis among exposed garment workers (Redlich et al. 1988). DMF use should be avoided both due to its hepatotoxicity and because it has been found to be associated with testicular cancer in two distinct occupational settings. Similarly, benzene may still be used in some clothing industry settings. Its use should be scrupulously avoided.
Physical hazards; electromagnetic fields. Recent reports have indicated that operation of a sewing machine may result in high exposures to electromagnetic fields (EMFs). The health effects of EMFs are not yet well understood and are the subject of current debate. However, one case-control study, which utilized three separate data sets from two countries (United States and Finland), found a strong association in all three data sets between occupational EMF exposure and Alzheimer’s disease among sewing machine operators and others classified as having sustained medium and high EMF exposures (Sobel et al. 1995). A case-control study of maternal occupation and acute lymphoblastic leukaemia (ALL) in Spain found an increased risk of ALL in offspring of mothers working at home during pregnancy, with most performing sewing machine operation. Although the authors of the study initially speculated that maternal exposure to organic dust and synthetic fibres might be responsible for the observed increase, the possibility of EMF exposure as a possible aetiological agent was raised (Infante-Rivard et al. 1991). (See the chapter Radiation, non-ionizing for further discussion.)
Other occupational illnesses and hazards. Garment workers have been shown in a number of studies to be at increased risk for the development of asthma (Friedman-Jimenez et al. 1994; Ng et al. 1994). In addition to potentially increased risk of lung and nasopharyngeal cancer due to formaldehyde exposure, garment workers have been found to have an increased risk of bladder cancer (Alderson 1986). Lead poisoning has been observed among clothing workers involved in production of metallic buttons. Warehouse and distribution workers may be at risk of developing the illnesses associated with exposure to diesel exhaust.
Worldwide, the high proportion of women and children employed in the garment industry, combined with the predominance of sub-contracting and industrial home work, has created an ideal field for exploitation. Sexual harassment, including non-consensual sexual activity with its attendant health problems, is a serious problem in the clothing industry worldwide. Child workers are particularly vulnerable to the health effects of toxic exposures and to the effects of poor workplace ergonomics due to their developing bodies. Working children are also highly vulnerable to workplace accidents. Lastly, two recent studies have found associations between work in the apparel industry during pregnancy and adverse reproductive outcomes, suggesting the need for further investigation in this area (Eskenazi et al. 1993; Decouflé et al. 1993).
Public Health and Environmental Issues
The apparel and other finished textile products industry is, generally, an industry which yields relatively little environmental contamination via discharges into air, soil or water. However, off-gassing of formaldehyde can persist at the retail level in this industry, creating the potential for development of formaldehyde-related allergic, irritative and respiratory symptomatology among both sales people and customers. Additionally, some of the special processes utilized in the garment industry, such as rubberizing and production of lead-based adornments, can pose more serious threats of environmental contamination.
In recent years, growing concerns about the potential adverse health effects associated with exposure to formaldehyde and other fabric treatments has lead to development of a “green” industry. Apparel and other finished textile products are typically sewn from natural rather than synthetic fibre-based materials. Additionally, these natural products are generally not treated with crease-resistant and other finishing agents.
The crowded, often squalid, conditions in the garment industry create ideal conditions for transmission of infectious diseases. In particular, tuberculosis has been a recurrent public health issue among workers in the garment industry.
Accidents in Clothing Manufacture
Adapted from 3rd edition, Encyclopaedia of Occupational Health and Safety
Small enterprises in unsuitable domestic premises used for clothing manufacture often present a serious fire hazard. In any workroom, large or small, there is much combustible material, and combustible waste will accumulate unless very strict control is exercised. Some of the materials used are particularly flammable (e.g., foam resins used for lining and padding and fine particulate coir). Adequate means of escape, adequate fire extinguishers and training in procedures in case of fire are necessary. Maintenance and good housekeeping not only assist in preventing fires and limiting their spread, but are essential where goods are transported mechanically.
In general, the accident frequency and severity rates are low, but the trade produces a multiplicity of minor injuries that can be prevented from becoming more serious by immediate first aid. Band knives can cause serious wounds unless effectively protected; only that part of the knife necessarily exposed for cutting should be left unguarded; the circular knives of portable cutting machines should be similarly protected. If power presses are used, adequate machinery guarding, preferably fixed, is necessary to keep hands out of the danger area. The sewing machine presents two main hazards—the driving mechanisms and the needle. In many places, long lines of machines are still driven by underbench shafting. It is essential that this shafting be effectively guarded by enclosure or close railing; many entanglement accidents have occurred when workers stooped under benches to retrieve materials or to replace belts. Several different types of needle guard, which keep fingers out of the area of risk, are available.
The use of garment presses involves a serious risk of crushing and burning. Two-handed controls are widely used but are not entirely satisfactory: they may be subject to misuse (e.g., operation by the knee). They should always be set to make this impossible and to prevent operation by one hand. Guards which prevent the pressure head from closing on the buck if anything (most importantly, the hand) comes within the area are to be used. All presses, with their steam and pneumatic supplies, require frequent inspection.
All portable electrical power tools require careful maintenance of the earthing arrangements.
Recent developments in plastics welding (to replace seaming and so on) and in the making of foam backs usually involve the use of an electric press, sometimes operated by treadle, sometimes by compressed air. There is a risk of physical trapping between the electrodes and also of electrical burns from high-frequency current. The only sure safety measure is to enclose the dangerous parts so that the electrode cannot operate when the hand is in the danger area: double-handed control has not proved satisfactory. Seaming machines must incorporate built-in safety designs.
Major Sectors and Processes
Overall Processes
In general, the processes involved in the production of clothing and other finished textile products have changed little since the inception of the industry. Although the organization of the production process has changed, and continues to change, and some technological advances have upgraded machinery, many of the safety and health hazards in this industry remain the same as those facing the earliest apparel workers.
The major health and safety concerns in the apparel industry are related to general conditions of the work environment. Poorly designed workstations, tools and equipment, combined with piece-rate compensation systems and the progressive bundle system of production, pose serious risks of musculoskeletal injury and stress-related conditions. Garment shops are often housed in buildings that are poorly maintained and inadequately ventilated, cooled, heated and lit. Overcrowding, together with improper storage of flammable materials, frequently creates serious fire hazards. Poor sanitation and lack of proper housekeeping measures contribute to these conditions.
Major advances have been made in the design and production of well-designed, ergonomic sewing workstations that include adjustable sewing tables and chairs and take into consideration proper positioning of equipment and tools. These workstations are widely available and are in use in some facilities, mostly large manufacturing establishments. However, only the largest, best-capitalized facilities are able to afford these amenities. Ergonomic redesign is also possible in other clothing manufacturing operations (see figure 1).The majority of apparel production, however, still takes place in small, ill-equipped contracting operations where, in general, little attention is paid to workplace design, working conditions and health and safety hazards.
Figure 1. A sequin-manufacturing facility

Source: Michael McCann
Product design and sample-making. The design of clothing and other textile products is overseen by apparel manufacturers, retailers or “jobbers”, with the design process performed by skilled designers. Apparel jobbers, manufacturers or retailers are frequently responsible only for the design, sample production and marketing of the product. While the jobber or manufacturer takes responsibility for specifying all details of the garment’s production, purchases the fabric and trims items to be used, the actual large-scale production work is typically performed by independent contracting shops.
Sample-making, in which small numbers of sample garments are made to be used to market the product and to be sent to contracting shops as examples of the finished product, also takes place on the jobber’s premises. Samples are produced by highly skilled sewing machine operators, sample-makers, who sew the entire garment.
Pattern-making and cutting. Garment design must be broken down into pattern parts for cutting and sewing. Traditionally, cardboard patterns are made up for each piece of the garment; these patterns are graded by the sizes to be made. From these patterns, paper-cutting markers are created, which are used by the garment cutter to cut out the pattern pieces. In more modern plants, cutting markers are made up and graded for size on a computer screen, then printed on a computerized plotter.
In the cutting phase, fabric is first spread into multiple piles on a cutting table, the length and width of which is determined by production demands. This is most often performed by an automatic or semi-automatic spreading machine which unrolls the bolts of fabric along the length of the table. Plaid or print fabrics may be laid out by hand and pinned to assure that plaids for prints will match. Markers are then laid down on the fabric to be cut.
Fabric for apparel production is usually cut using hand-held band saw cutting tools (see figure 2). Small parts may be cut using a die press. Advanced cutting technology includes robotic cutting, which automatically follows patterns made on a computer.
Figure 2. A clothing factory in the Philippines

There are several hazards associated with fabric cutting. Although the blade on the cutting tool is guarded, this guard must be correctly set in order to afford the necessary protection to the hand positioning the material. Guards should always be used and correctly positioned. As an additional protection it is recommended that cutting machine operators wear a protective glove, preferably of metal mesh. Besides posing the risk of accidental cuts, cutting fabric also presents ergonomic risks. Supporting and manoeuvering a cutting machine, while stretching across the cutting table, can present a risk of neck, upper-extremity and back disorders. Finally, many cutters have a tendency to work with the cutting machine at ear level, often exposing themselves to excessive noise with the attendant risk of noise-induced hearing loss.
Handling rolls of fabric, which can weigh up to 32 kg and must be lifted above the head onto a rack for spreading, also poses an ergonomic hazard. Proper material-handling equipment can eliminate or reduce these risks.
Sewing machine operation. Typically, cut fabric pieces are sewn together on sewing machines operated by hand. The traditional “progressive bundle system”, in which bundles of cut pieces progress from one sewing machine operator to the next, with each operator performing a different single operation, continues to prevail in the industry, despite significant changes in work organization in many shops. This type of work organization breaks the production process down into many different operations, each consisting of a very short cycle repeated hundreds of times by one operator during the course of a workday. This system, combined with piece-rate pay compensation that rewards speed above all else and affords workers very little control over the production process, creates a potentially very stressful work environment.
The majority of the sewing machine workstations currently in use are designed without the comfort, health or convenience of the sewing machine operator in mind (see figure 3). Because sewing machine operators generally work in a seated position at poorly designed workstations, performing the same operation during the entire course of the workday, the risk of developing musculoskeletal disorders is high. The poor postures resulting from the conditions described above, combined with highly repetitive, time-pressured work, has resulted in high rates of work-related musculoskeletal disorders (WRMDs) among sewing machine operators and other workers in the industry.
Figure 3. Woman using a sewing machine without a needle guard

Advances in sewing workstation design, such as adjustable chairs and worktables, create the potential for reduction of some of the risks associated with sewing machine operation. However, while these workstations and chairs are widely available, their price often places them out of reach of all but the most profitable enterprises. Additionally, even with better-designed workstations, the risk factor of repetition remains.
Changes in the organization of work and the introduction of teamwork, in the form of modular or flexible manufacturing, offer an alternative to the traditional, Taylorist production process and may serve to alleviate some of the health risks involved in the traditional system. In a teamwork system sewing machine operators work in a group to produce an entire garment, often shifting frequently between machines and jobs.
In one of the most popular team systems, workers work standing up, rather than seated, and move frequently from machine to machine. Cross-training for a variety of jobs enhances workers’ skills, and workers are given more control over production. Changes from an individual piece-rate system of pay to hourly pay or to a group incentive system, as well as increased emphasis on monitoring quality throughout the production process, may help to eliminate some factors that put workers at risk of developing WRMDs.
Some newer manufacturing systems, while technologically advanced, may actually contribute to increased risk of WRMD. So-called unit production systems, for example, are designed to mechanically convey cut goods on an overhead conveyor from worker to worker, thus speeding up the progress of the goods and eliminating much of the material handling previously performed by the sewing machine operators or by floor workers. While these systems often increase production by speeding up the line, they eliminate the already small rest time that was afforded to the operator between cycles, resulting in increased fatigue and repetition.
When instituting any alternative production system, care should be taken to evaluate risk factors and design the new system with ergonomics in mind. For example, when workers will be trained to do a variety of jobs, jobs should be combined to stress differing parts of the body and not overtax any one muscle or joint. Care should be taken to ensure that equipment and machinery can be adapted to fit all the workers in the team.
Whenever any new equipment is purchased, it should be easily adjustable by the workers themselves, and training should be provided on how to make adjustments. This is particularly important in the apparel industry, where mechanics are often not readily available to adjust equipment to properly fit workers.
Recent studies have raised concerns about sewing machine operators’ exposure to high levels of electromagnetic fields (EMFs) generated by sewing machine motors. These studies have indicated that there may be an association between increased levels of Alzheimer’s disease (Sobel et al. 1995) and other chronic diseases found among sewing machine operators and the operators’ exposure to high levels of EMFs.
Finishing and pressing. Once sewn, the completed garment is ironed by pressers and checked for loose threads, stains and other defects by finishers. Finishers perform a variety of hand work, including clipping loose threads, hand sewing, turning and hand pressing. Ergonomic hazards are a problem for workers who finish, ticket, pack and distribute apparel. They often perform highly repetitive tasks, frequently involving working with the hands and arms in awkward and unhealthy postures. Seating and workstations for these workers are rarely adjustable or designed for comfort or health. Finishing workers, including pressers, often work standing and in static positions, despite the fact that many of the jobs could be equipped with chairs, stools or sit-stand chairs, and workers could alternate between standing and sitting. Table tops could be adjusted to the proper height for the operator and could be tilted to enable the operator to work in a more comfortable position. Padded table edges and properly designed and sized tools could eliminate some stresses on hands, wrists and arms.
Pressing the sewn product is performed either using a hand iron or a buck press. Sewn products may also be steamed using a hand steamer or a steam tunnel. Presses and irons may present risks of burns, as well as ergonomic hazards. While most presses are designed with two-handed controls, eliminating the possibility of getting the hand stuck in the press, some old machines still exist which do not have these safety features. Working a pressing machine also presents the risks of shoulder, neck and back injury caused by frequent overhead reaching and by constant standing and operating the foot pedals. While the job can be made safer by a more highly automated machine and by proper positioning of the worker at the machine, the current machinery makes it difficult to eliminate the high stress.
Ticketers, who use ticketing guns to place tags on finished garments, are at risk of hand and wrist injury from this highly repetitive operation. Automatic, as opposed to manual, ticketing guns can help decrease the force needed to perform the operation, greatly reducing stress and strain on the fingers and hands.
Distribution. Workers in apparel distribution centres are exposed to all the hazards of other warehouse workers. Manual material handling accounts for many of the injuries in warehouse operations. Particular hazards include lifting and overhead work. Designing the distribution workplace with the proper handling of materials in mind, such as placement of conveyors and worktables at appropriate heights, can help prevent many injuries. Mechanical material-handling equipment, such as fork-lifts and hoists, can help prevent injuries caused by having to perform awkward or heavy lifts.
Chemical exposure. Workers at every stage of apparel production may be exposed to the chemicals used in fabric finishing; the most common of these is formaldehyde. Used to make fabric permanent press and colour-fast, formaldehyde is released into the air from fabric in the form of a gas. Workers may also have skin exposure to formaldehyde as they handle the fabric. The amount of formaldehyde released from fabric depends on a variety of factors, including the amount used in finishing, the finishing process used and the ambient heat and humidity. Exposure to formaldehyde can be prevented by allowing the fabric to off-gas in a well-ventilated area before it is handled and by providing good ventilation in the work areas, particularly where fabric is exposed to high heat and humidity (e.g., in pressing operations). Workers who experience skin problems from handling formaldehyde-treated fabric can wear gloves or protective cream. Finally, textile manufacturers should be encouraged to develop safer alternative fabric treatments.
Special Processes
Pleating. The pleating process is used to place creases or pleats into fabric or garments. This process uses high temperatures and high humidity to put folds into various types of fabric. Pleaters are exposed to these conditions of high heat and humidity, which may cause the release of greater quantities of substances used to finish the fabric than may otherwise be released under conditions of normal temperature and humidity. Stiffening agents may be added to fabrics that are to be pleated to facilitate the fabric’s ability to hold the crease. Steam boxes and steam chambers expose the pleated fabric to steam under pressure.
Rubberizing/waterproofing. To create a rubberized or waterproof finish, fabrics may be coated with a waterproof substance. These various coatings, which may be a type of rubber, are often thinned with solvents, including those that pose serious health risks to exposed workers. These coatings may include benzene or dimethylformamide, as well as other solvents. Workers are exposed to these chemicals when they are mixed or poured, often by hand, or in large vats in poorly ventilated areas. Workers can also be exposed as they pour the mixtures on the fabric to coat it. Hazardous exposures should be minimized by substitution of less toxic substances and by providing adequate ventilation at the point of use. In addition, mixing and pouring operations should be contained and automated, where possible.
Computer use. Computers are increasingly used in the apparel industry, from computer-aided design/computer-aided manufacturing (CAD/CAM) systems in the design, marking and cutting processes to the tracking of goods in the warehousing and shipping operations. Hazards associated with computer usage are discussed elsewhere in this Encyclopaedia.
Buttons, buckles and other adornments. Buttons, buckles and other fasteners on apparel or sewn products are most often manufactured in facilities separate from those that produce apparel. Buttons may be manufactured from a variety of materials, and the material used will determine the production process. Most commonly, buttons and buckles are made from moulded plastic or metals, including lead. During the production process, the heated raw materials are poured into moulds and then cooled. Workers may be exposed to toxic chemicals or metals during this moulding process. After cooling, workers may be exposed to the dust generated when the products are polished or ground. These exposures can be prevented by providing adequate ventilation during this finishing process or by containment of these operations. Other adornments, such as sequins, beads and so on, are produced from plastics and metals, either stamped or moulded, and may expose the production workers to the hazards of their components.
Sewn plastic products and plastic accessories. Various items such as shower curtains, tablecloths and protective raingear are made of sewn, or joined, plastics. Where goods are sewn from sheet plastic, the hazards are similar to those of other sewn items. However, working with large stores of plastic material creates a unique fire safety hazard, since the heating and burning of plastic creates a release of toxic materials that can be very dangerous. Extreme care should be taken in the area of fire prevention and protection where large amounts of plastic materials are used or stored.
In addition to being sewn, plastics can also be joined together by heat or electromagnetic radiation. When plastics are heated they release their components and they may expose workers to these toxics. When electromagnetic radiation is used to join or seal plastics, care must be taken not to expose workers to dangerous levels of this radiation.
Work Organization
The piece-rate system, where workers are paid according to the number of units they produce, is one which is still widely used in the production of apparel and sewn products. The continued use of the piece-work system of compensation poses both stress-related and musculoskeletal health risks to workers in the apparel industry. As discussed above, alternative compensation systems, as well as alternative production systems, may make apparel production a more attractive, less stressful and less hazardous option for workers entering the workforce.
A teamwork system, which gives workers more control over the production process, as well as the opportunity to work with others, may be less stressful than the traditional progressive bundle system. However, these team systems may also cause additional stress if they are set up so that workers are responsible for enforcing work rules against their co-workers. Some types of group compensation systems which penalize an entire team for the slowness or absenteeism of any of its members may create tension and stress within the group.
Home work is the system of sending out work to be done in the home of a worker. It is very common in the apparel industry. Work may be sent home with a factory worker at the end of the workday to be done in the evening or the weekend; or, work may be sent directly into the worker’s home, bypassing the factory altogether.
The home-work system is often synonymous with exploitation of workers. Home work cannot easily be regulated by agencies that enforce labour standards, including laws governing child labour, health and safety, minimum wage and so on. In many instances home workers are paid substandard wages and forced to furnish, at their own expense, equipment and tools needed for production. Children in the home may be drawn into doing home work, regardless of their age or ability to work safely, or at a detriment to their schooling or leisure time. Health and safety hazards may abound in homeworking situations, including exposure to dangerous chemicals, fire and electrical hazards. Industrial machinery may present hazards to small children in the home.
Oil and Fat
Adapted from 3rd edition, “Encyclopaedia of Occupational Health and Safety”.
The term oils and fats is generally applied to the triglycerides of fatty acids in plant seeds and animal tissues. Oils and fats constitute one of the three main types of organic materials regarded as the building materials of living organisms, the other two being proteins and carbohydrates.
More than 100 varieties of oil-bearing plants and animals are exploited as sources of oils and fats. The most important vegetable sources are: the olive, coconut, peanut, cotton seed, soya bean, rapeseed (canola oil), mustard seed, flax or linseed, palmfruit, sesame, sunflower, palm kernel, castor bean, hemp seed, tung, cocoa, mowrah, corn and babassu.
The main animal sources are beef cattle, pigs and sheep, the whale, cod and halibut.
Edible oils and fats provide a concentrated source of food energy, serve as carriers of fat-soluble vitamins and also furnish the essential fatty acids which are of vital importance to metabolism. Oils and fats constitute the major raw materials for soaps and detergents, paints, lacquers and varnishes, lubricants and illuminants such as candles. They are also used in the manufacture of linoleum and oiled fabrics, in the manufacture of fixatives and mordants in the tanning of leather, and as feedstock for chemical synthesis.
Processing
Initial processing depends upon the raw material; for example, animal fats are rendered in steam-jacketted vessels, seeds are cleaned, milled and separated and nut-meats are flaked. The fats or oils are extracted by pressing or treatment by solvents, and further processing depends upon the end use. Olives may be pressed several times, but no further treatment is usually required. For other edible oils and fats, processing may comprise a number of different stages, including refining, deodorization, hydrogenation, solidification or emulsification.
Raw oils and fats contain impurities, some of which are objectionable because they darken the oil, cause it to foam and smoke on heating, impart an undesirable flavour or odour or affect processing. Refining, which consists of neutralization and bleaching, removes most of these impurities. Neutralization removes fatty acids and gummy phosphatides by alkali and degumming treatments. The raw materials are bleached by absorption on natural or activated bleaching earths; however, heat bleaching may be employed. Oil temperature does not normally exceed 100 °C during refining.
Deodorization removes the odoriferous compounds by steam distillation at high temperature and low absolute pressure.
Liquid oils and soft fats are converted into firm plastic fats by hydrogenation, which also helps prevent rancidity due to oxidation. In this process, the oil is reacted with hydrogen at a temperature of 180 ºC or more in the presence of a catalyst, usually finely divided nickel. The hydrogen is fed in at a pressure of between 2 and 30 atmospheres, depending upon the desired end-product.
If the oil or fat is to be marketed in plastic or emulsion form, further processing is required. Many proprietary brand oils and fats are blended, and shortenings are solidified to yield granules by controlled gradual cooling (fractionation) and separation of crystallized fractions at various temperatures based on their melting points. An alternative method produces a texturized product by rapid chilling in special equipment called a votator.
Hazards and Their Prevention
Hydrogen presents a high risk of explosion and fire in the hydrogenation process. Burning oils and fats may emit highly irritant fumes such as acrolein. The solvents, such as hexane, used for the extraction of oils are highly flammable, although they are commonly used in closed systems. Precautions against fire and explosion include:
- elimination of all sources of ignition
- use of explosion-proof equipment and spark-proof tools
- prohibition of smoking
- ensuring fire exits are not blocked and are well maintained
- provision of appropriate fire extinguishers
- development of procedures for spills and leaks of hydrogen and flammable solvents
- training of staff in firefighting procedures.
Electrical installations present a risk of electrical shock in damp and steamy conditions. All equipment, conductors and so on should be suitably protected with special attention to any portable equipment or lights. Ground fault circuit interrupters should be installed on electrical equipment in wet or steamy areas.
Injuries from moving machinery parts can be prevented by efficient and well maintained machinery guarding. Particular attention should be given to crushing machinery, filling and drum-seaming machines and nips between belts, drums and pulleys of conveyors. Lockout/tagout procedures should be used when maintaining and repairing equipment. Risks of explosion and leakage in steam plant should be prevented by regular inspection and maintenance procedures.
Excessive noise from equipment should be minimized by engineering controls if possible. Employees exposed to excessive noise should wear appropriate hearing protectors, and there should be a hearing conservation programme.
Manual handling of drums may cause musculoskeletal strains and injuries to hands and toes. Mechanical handling equipment should be used when possible. There should be training in correct methods of handling and lifting, foot and hand protection, and checking of containers for sharp edges. Badly stacked drums may fall and cause serious injury; supervision and training in stacking and destacking will reduce the risk involved.
Falls may occur on slippery floors and staircases, and can be prevented by well maintained non-slip floor surfaces, regular cleaning and good housekeeping, and wearing of non-slip footwear.
Burns may be caused by sodium hydroxide during handling of drums for refining and from spurts of liquid caustic when drums are opened; by hot oil or spent catalyst during cleaning of filter presses; from acids; and from steamlines and steam leaks. Protective clothing, boots, aprons and gloves will prevent many injuries; face shields are necessary to protect the eyes from splashes of corrosive or hot material.
Oils are processed at high temperatures, and physical discomfort can result, especially in the tropics, unless effective measures are taken. Muscle cramps, exhaustion and heat strokes may occur. Radiant heat should be reduced by lagging or insulating the vessels and steam pipes. Efficient mechanical ventilation should provide frequent changes of air. Workers should have frequent access to liquids and frequent breaks in cool areas.
Entering bulk tanks for repair or cleaning can be a confined space hazard. Employees should be trained in confined space procedures, such as testing of the confined space air and emergency rescue procedures. A minimum of two workers should be present.
Solvents used for the extraction of fats and oils may present toxic risks. Benzene should not be used, and the least toxic solvent practicable should be substituted (e.g., substitution of heptane for hexane). LEV is required to remove solvent vapours at the point of origin, or closed systems should be used.
Dermatitis may be caused by handling of oils, fats and solvents. Provision and use of adequate washing and sanitary facilities is essential; barrier creams and protective clothing also aid in prevention.
In peanut oil processing plants, under suitable conditions of moisture and temperature, press-cakes can be contaminated by moulds of Aspergillus flavus, which contain aflatoxins. Workers exposed to heavy aflatoxin contamination in workroom air have been found to develop acute or subacute liver damage and to present an increased prevalence of tumours.
Rendering of animals to produce animal fats and animal feed can also involve biological hazards. Although most animals and animal materials used as a source for rendering are healthy or from healthy animals, a small percentage comes from animals that have been road-killed or have died of unknown causes and perhaps are diseased. Some animal diseases, such as anthrax and brucellosis, can also affect humans. Workers in slaughterhouses and rendering plants may be at risk. In the United Kingdom, people called knackers make their living going around the countryside picking up dead animals and rendering them in their backyards. They could be at greater risk because of the greater likelihood of their exposure to diseased animals and the crude conditions they work under.
The past rendering of sheep organs, including brains, as a source for cattle feed has resulted in bovine spongiform encephalopathy (“mad cow disease”) in some British cows where the sheep had a brain disease called scrapie. It appears that some humans have developed this disease from eating beef from cows with mad cow disease.
Periodic medical examination of workers, selection, training and supervision are aids in prevention of both accidents and occupational diseases.
Sugar-Beet Industry
This is an update of the article prepared by the European Committee of Sugar Manufacturers (CEFS) for the 3rd edition of the “Encyclopaedia of Occupational Health and Safety”.
Processing
The process of producing sugar from beets consists of many steps, which have been improved continuously throughout the more than century-old history of the sugar-beet industry. Sugar-beet processing facilities have become modernized and use current technology as well as current safety measures. Workers are now trained in using modern and sophisticated equipment.
The sugar content of the beets ranges from 15 to 18%. They are first cleaned in a beet washer. They are then cut in beet slicers and the “cossettes” thus obtained are conveyed via a scalder into the diffuser, where most of the sugar contained in the beets is extracted in hot water. The desugarized cossettes, called “pulps”, are pressed mechanically and dried, mostly by heat. The pulps contain many nutrients and are used as animal feed.
The raw juice obtained in the diffuser, in addition to sugar, also contains non-sugar impurities which are precipitated (by adding lime and carbon dioxide) and then filtered. The raw juice thus becomes thin juice, with a sugar content of 12 to 14%. The thin juice is concentrated in evaporators to 65 to 70% dry matter. This thick juice is boiled in a vacuum pan at a temperature of about 70 °C until crystals form. This is then discharged into mixers, and the liquid surrounding the crystals is spun off. The low syrup thus separated from the sugar crystals still contains sugar which can be crystallized. The desugaring process is continued until it is no longer economical. Molasses is the syrup left after the last crystallization.
After drying and cooling, the sugar is stored in silos, where it can be kept indefinitely if adequately air conditioned and moisture controlled.
The molasses contains approximately 60% sugar and, together with the non-sugar impurities, constitutes valuable animal feed as well as an ideal culture medium for many micro-organisms. For animal feed, part of the molasses is added to the sugar-exhausted pulps before they are dried. Molasses is also used for the production of yeast and alcohol.
With the help of other micro-organisms, other products can be made, such as lactic acid, an important raw material for the food and pharmaceutical industries, or citric acid, which the food industry needs in great quantities. Molasses is also used in the production of antibiotics such as penicillin and streptomycin, and also of sodium glutamate.
Working Conditions
In the highly mechanized sugar-beet industry, the beet is transformed into sugar during what is known as the “campaign”. The campaign lasts from 3 to 4 months, during which time the processing plants operate continuously. Personnel work in rotating shifts around the clock. Additional workers may be added temporarily during peak periods. Upon completion of the beet processing, repairs, maintenance and updates are done in the facilities.
Hazards and Their Prevention
Sugar beet processing does not produce or involve working with toxic gases or airborne dusts. Parts of the processing facility may be extremely noisy. In areas where the noise levels cannot be brought down to the threshold limits, hearing protection needs to be provided and a hearing conservation programme instituted. However, for the most part, occupationally related illnesses are rare in the sugar-beet processing plants. This is partially due to the fact that the campaign is only of 3 to 4 months duration per year.
As in most food industries, contact dermatitis and skin allergies from cleaning agents used to clean vats and equipment can be a problem, requiring gloves. When entering vats for cleaning or other reasons, confined space procedures should be in effect.
Care must be taken when entering silos of stored granular sugar, due to the risk of engulfment, a hazard similar to that of grain silos. (See the article “Grain, grain milling and grain-based consumer products” in this chapter for more detailed recommendations.)
Burns from steam lines and hot water are a concern. Proper maintenance, PPE and employee training can help prevent this type of injury.
Mechanization and automation in the sugar-beet industry minimize the risk of ergonomic disorders.
Machinery must be regularly checked and routinely maintained and repaired as required. Safety guards and mechanisms must be kept in place. Employees should have access to protective equipment and devices. Employees should be required to participate in safety training.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."