- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Bakeries
Adapted from 3rd edition, “Encyclopaedia of Occupational Health and Safety”.
The manufacture of foodstuffs from starches and sugars is done in bakeries and biscuit-, pastry- and cake-making establishments. The safety and health hazards presented by the raw materials, the plant and equipment and the manufacturing processes in these plants are similar. This article deals with small-scale bakeries and covers bread and various related products.
Production
There are three main stages in breadmaking—mixing and moulding, fermentation and baking. These processes are carried out in different work areas—the raw materials store, the mixing and moulding room, cold and fermentation chambers, the oven, the cooling room and the wrapping and packaging shop. The sales premises are frequently attached to the manufacturing shops.
Flour, water, salt and yeast are mixed together to make dough; hand mixing has been largely replaced by the use of mechanical mixing machines. Beating machines are used in the manufacture of other products. The dough is left to ferment in a warm, humid atmosphere, after which it is divided, weighed, moulded and baked (see figure 1).
Figure 1. Bread production for a supermarket chain in Switzerland
 Small-scale production ovens are of the fixed-hearth type with direct or indirect heat transfer. In the direct type, the refractory lining is heated either intermittently or continuously before each charge. Off-gases pass to the chimney through the adjustable orifices at the rear of the chamber. In the indirect type, the chamber is heated by steam passing through tubes in the chamber wall or by forced hot-air circulation. The oven may be fired by wood, coal, oil, town gas, liquefied petroleum gas or electricity. In rural areas, ovens with hearths heated directly by wood fires are still found. Bread is charged into the oven on paddles or trays. The oven interior can be illuminated so that the baking bread can be observed through the chamber windows. During baking, the air in the chamber becomes charged with water vapour given off by the product and/or introduced in the form of steam. The excess usually escapes up the chimney, but the oven door may also be left open.
Small-scale production ovens are of the fixed-hearth type with direct or indirect heat transfer. In the direct type, the refractory lining is heated either intermittently or continuously before each charge. Off-gases pass to the chimney through the adjustable orifices at the rear of the chamber. In the indirect type, the chamber is heated by steam passing through tubes in the chamber wall or by forced hot-air circulation. The oven may be fired by wood, coal, oil, town gas, liquefied petroleum gas or electricity. In rural areas, ovens with hearths heated directly by wood fires are still found. Bread is charged into the oven on paddles or trays. The oven interior can be illuminated so that the baking bread can be observed through the chamber windows. During baking, the air in the chamber becomes charged with water vapour given off by the product and/or introduced in the form of steam. The excess usually escapes up the chimney, but the oven door may also be left open.
Hazards and Their Prevention
Working conditions
The working conditions in artisanal bakehouses can have the following features: night work starting at 2:00 or 3:00 a.m., especially in Mediterranean countries, where the dough is prepared in the evening; premises often infested with parasites such as cockroaches, mice and rats, which may be carriers of pathogenic micro-organisms (suitable construction materials should be used to ensure that these premises are maintained in an adequate state of hygiene); house-to-house bread delivery, which is not always carried out in adequate conditions of hygiene and which may entail an excess workload; low wages supplemented by board and lodging.
Premises
Premises are often old and dilapidated and lead to considerable safety and health problems. The problem is particularly acute in rented premises for which neither the lessor nor the lessee can afford the cost of renovation. Floor surfaces can be very slippery when wet, although reasonably safe when dry; non-slip surfaces should be provided whenever possible. General hygiene suffers owing to defective sanitary facilities, increased hazards of poisoning, explosions and fire, and the difficulty of modernizing heavy bakehouse plant owing to the terms of the lease. Small premises cannot be suitably divided up; consequently traffic aisles are blocked or littered, equipment is inadequately spaced, handling is difficult, and the danger of slips and falls, collisions with plant, burns and injuries resulting from overexertion is increased. Where premises are located on two or more storeys there is the danger of falls from a height. Basement premises often lack emergency exits, have access stairways which are narrow, winding or steep and are fitted with poor artificial lighting. They are usually inadequately ventilated, and consequently temperatures and humidity levels are excessive; the use of simple cellar ventilators at street level merely leads to the contamination of the bakehouse air by street dust and vehicle exhaust gases.
Accidents
Knives and needles are widely used in artisanal bakeries, with a risk of cuts and puncture wounds and subsequent infection; heavy, blunt objects such as weights and trays may cause crush injuries if dropped on the worker’s foot.
Ovens present a number of hazards. Depending on the fuel used, there is the danger of fire and explosion. Flashbacks, steam, cinders, baked goods or uninsulated plant may cause burns or scalds. Firing equipment which is badly adjusted or has insufficient draw, or defective chimneys, may lead to the accumulation of unburnt fuel vapours or gases, or of combustion products, including carbon monoxide, which may cause intoxication or asphyxia. Defective electrical equipment and installations, especially of the portable or mobile type, may cause electric shock. The sawing or chopping of wood for wood-fired ovens may result in cuts and abrasions.
Flour is delivered in sacks weighing up to 100 kg, and these must often be lifted and carried by workers through tortuous gangways (steep inclines and staircases) to the storage rooms. There is the danger of falls while carrying heavy loads, and this arduous manual handling may cause back pain and lesions of intervertebral discs. The hazards may be avoided by: providing suitable access ways to the premises; stipulating a suitable maximum weight for sacks of flour; using mechanical handling equipment of a type suitable for use in small undertakings and at a price within the range of most artisanal workers; and by wider use of bulk flour transport, which is, however, suitable only when the baker has a sufficiently large turnover.
Flour dust is also a fire and explosion hazard, and proper precautions should be taken, including fire and explosion suppression systems.
In mechanized bakeries, dough which is in an active state of fermentation may give off dangerous amounts of carbon dioxide; thorough ventilation should therefore be provided in confined spaces wherever the gas is likely to accumulate (dough chutes and so on). Workers should be trained in confined-space procedures.
A wide variety of machines are used in bread manufacture, particularly in industrial bakeries. Mechanization can bring serious accidents in its wake. Modern bakery machines are usually equipped with built-in guards whose correct operation often depends upon the functioning of electrical limit switches and positive interlocks. Feed hoppers and chutes present special hazards which can be eliminated by extending the length of the feed opening beyond arm’s length to prevent the operator from reaching the moving parts; hinged double gates or rotary flaps are sometimes used as feeding devices for the same purpose. Nips on dough brakes can be protected by either fixed or automatic guards. A variety of guards (covers, grids and so on) can be used on dough mixers to prevent access to the trapping zone while permitting insertion of additional material and scraping of the bowl. Increasing use is made of bread-slicing and wrapping machines with alternating saw blades or rotary knives; all moving parts should be completely enclosed, interlocking covers being provided where access is necessary. There should be a lockout/tagout programme for maintenance and repair of machinery.
Health Hazards
Bakehouse workers are usually lightly clothed and sweat profusely; they are subject to draughts and pronounced variations in ambient temperature when changing, for example, from oven charging to cooler work. Airborne flour dust may cause rhinitis, throat disorders, bronchial asthma (“baker’s asthma”) and eye diseases; sugar dust may cause dental caries. Airborne vegetable dust should be controlled by suitable ventilation. Allergic dermatitis may occur in persons with special predisposition. The above health hazards and the high incidence of pulmonary tuberculosis amongst bakers emphasize the need for medical supervision with frequent periodic examinations; in addition, strict personal hygiene is essential in the interests of both workers and the public in general.
Grain, Grain Milling and Grain-based Consumer Products
Grain goes through many steps and processes to be prepared for human consumption. The major steps are: collection, consolidation and storage at grain elevators; milling into an intermediate product such as starch or flour; and processing into finished products such as bread, cereal or snacks.
Grain Collection, Consolidation and Storage
Grains are grown on farms and moved to grain elevators. They are transported by truck, rail, barge or ship depending on the location of the farm and the size and type of elevator. Grain elevators are used to collect, classify and store agricultural products. Grains are separated according to their quality, protein content, moisture content and so on. Grain elevators consist of bins, tanks or silos with vertical and horizontal continuous belts. Vertical belts have cups on them to carry the grain up to weighing scales and horizontal belts for distribution of the grain into bins. Bins have discharges on the bottoms which deposit grain on a horizontal belt which conveys the product to a vertical belt for weighing and transportation or return to storage. Elevators can have capacities ranging from just a few thousand bushels at a country elevator to millions of bushels at a terminal elevator. As these products move towards processing, they may be handled many times through elevators of increasing size and capacity. When they are ready to be transported to another elevator or processing facility, they will be loaded into either truck, railcar, barge or ship.
Grain Milling
Milling is a series of operations involving the grinding of grains to produce starch or flour, most commonly from wheat, oats, corn, rye, barley or rice. The raw product is ground and sifted until the desired size is reached. Typically, milling involves the following steps: raw grain is delivered to a mill elevator; grain is cleaned and prepared for milling; grain is milled and separated by size and grain part; flour, starch and by-products are packaged for consumer distribution or bulk transported to be used in various industrial applications.
Grain-based Consumer Products Manufacturing
Bread, cereal and other baked goods are produced using a series of steps, including: combining raw ingredients, batter production and processing, product forming, baking or toasting, enrobing or frosting, packaging, casing, palletizing and final shipment.
Raw materials are often stored in bins and tanks. Some are handled in large bags or other containers. The materials are transported to processing areas using pneumatic conveyors, pumps or manual material-handling methods.
Dough production is a step where raw ingredients, including flour, sugar and fats or oils, and minor ingredients, such as flavorings, spices and vitamins, are combined in a cooking vessel. Any particulate ingredients are added along with puréed or pulped fruits. Nuts are usually husked and cut to size. Cookers (either continuous process or batch) are used. Processing of the dough into intermediate product stages can involve extruders, formers, pelletizers and shaping systems. Further processing can involve rolling systems, formers, heaters, dryers and fermentation systems.
Packaging systems take the finished product and encase it in a paper or plastic individual wrapping, place individual products in a box and then pack boxes on a pallet to prepare for shipment. Manual pallet stacking or product handling is used along with fork-lift trucks.
Mechanical Safety Issues
Equipment safety hazards include points of operation which can abrade, cut, bruise, crush, fracture and amputate. Workers can be protected by guarding or isolating the hazards, de-energizing all power sources prior to performing any maintenance or adjustment on the equipment and training workers in proper procedures to follow when working on the equipment.
The machines used to mill and convey products can be particularly dangerous. The pneumatic system and its rotary valves can cause severe finger or hand amputations. The equipment must be locked out while maintenance or clean-up is being performed. All equipment must be properly guarded and all workers need to be trained in proper operating procedures.
Processing systems have mechanical parts moving under automatic control which can cause severe injury, especially to fingers and hands. Cookers are hot and noisy, usually involving steam heating under pressure. Extrusion dies can have hazardous moving parts, including knives moving at high speed. Blenders and mixing machines can cause severe injuries and are particularly dangerous during clean-up between batches. Lockout and tagout procedures will minimize risk to workers. Slitter knives and water knives can cause severe lacerations and are especially dangerous during change-outs and adjustment procedures. Further processing can involve rolling systems, formers, heaters, dryers and fermentation systems, which present additional hazards to the extremities in the form of crushing and burn injuries. Manual handling and opening of bags can result in cuts and bruises.
Packaging systems have automated moving parts and can cause crushing or tearing injuries. Maintenance and adjustment procedures are particularly hazardous. Manual pallet stacking or product handling can cause repetitive strain injuries. Fork-lift trucks and hand pallet movers are also dangerous, and poorly stacked or secured loads can fall on nearby personnel.
Fire and Explosion
Fire and explosion can destroy grain-handling facilities and injure or kill workers and others who are in the facility or nearby at the time of explosion. Explosions require oxygen (air), fuel (grain dust), an ignition source of sufficient energy and duration (spark, flame or hot surface) and confinement (to allow pressure build-up). Typically, when an explosion occurs at a grain handling facility, it is not a single explosion but a series of explosions. The primary explosion, which can be quite small and localized, can suspend dust in the air throughout the facility in concentrations sufficient to sustain secondary explosions of great magnitude. The lower explosion limit for grain dust is approximately 20,000 mg/m3. Prevention of fire and explosion hazards can be accomplished by designing plants with minimal confinement (except for bins, tanks and silos); controlling dust emissions into air and accumulations on floors and equipment surfaces (enclosing product streams, LEV, housekeeping and grain additives such as food-grade mineral oil or water); and controlling the explosion (fire and explosion suppression systems, explosion venting). There should be adequate fire exits or means of escape. Firefighting equipment should be strategically located, and workers should be trained in emergency response; but only very small fires should be fought because of the explosion potential.
Health Hazards
Dust can be created when grain is moved or disturbed. Although most grain dusts are simple respiratory irritants, the dusts from unprocessed grain can contain moulds and other contaminants which can cause fever and allergic asthma reactions in sensitive persons. Employees tend not to work for prolonged times in dusty areas. Typically, a respirator is worn when needed. The highest dust exposures occur during loading/unloading operations or during major cleaning. Some research has indicated pulmonary function changes related to dust exposure. The current American Conference of Governmental Industrial Hygienists (ACGIH) TLVs for occupational exposure to grain dust are 4 mg/m3 for oat, wheat and barley and 10 mg/m3 for other grain dust (particulates, not otherwise classified).
Respiratory protection is often worn to minimize dust exposure. Approved dust respirators can be very effective if worn properly. Workers need to be trained in their proper use, maintenance and limitations. Housekeeping is essential.
Pesticides are used in the grain and grain-processing industries to control insects, rodents, birds, mould and so on. Some of the more common pesticides are phosphine, organophosphates and pyrethrins. Potential health effects can include dermatitis, dizziness, nausea and long-term problems with liver, kidney and nervous system functions. These effects occur only if employees are overexposed. Proper use of PPE and following safety procedures will prevent overexposure.
Most grain-processing facilities apply pesticides during shut-down times, when there are few employees in the buildings. Those workers present should be on the pesticide application team and receive special training. Re-entry rules should be followed to prevent overexposure. Many locations heat the entire structure to about 60 ºC for 24 to 48 hours in lieu of using chemical pesticides. Workers may also be exposed to pesticides on treated grain being brought to the truck cargo facility in trucks or rail cars.
Noise is a common problem in most grain-processing plants. The predominant noise levels range from 83 to 95 dBA, but can exceed 100 dBA in some areas. Relatively little acoustical absorption can be used due to the need for cleaning of equipment used in these facilities. Most floors and walls are made of cement, tile and stainless steel to allow easy cleaning and to prevent the facility from becoming a refuge for insects. Many employees move from area to area and spend little time working in the noisiest areas. This reduces personal exposure considerably, but hearing protection should be worn to reduce noise exposure to acceptable levels.
Working in a confined space such as a bin, tank or silo can present workers with health and physical hazards. The greatest concern is oxygen deficiency. Tightly sealed bins, tanks and silos can become oxygen deficient due to inert gases (nitrogen and carbon dioxide to prevent pest infestation) and biological action (insect infestation or mouldy grain). Prior to any entry into a bin, tank, silo or other confined space, the atmospheric conditions inside the confined space need to be checked for sufficient oxygen. If oxygen is less than 19.5%, the confined space must be ventilated. Confined spaces should also be checked for recent pesticide application or any other toxic material which may be present. Physical hazards in confined spaces include engulfment in the grain and entrapment in the space due to its configuration (inward sloping walls or entrapment in equipment inside the space). No worker should be in a confined space such as a grain silo, bin or tank while grain is being removed. Injury and death can be prevented by de-energizing and locking out all equipment associated with the confined space, ensuring that workers wear harnesses with lifelines while inside the confined space and maintaining a supply of breathable air. Prior to entry, the atmosphere inside a bin, silo or tank should be tested for the presence of combustible gases, vapours or toxic agents, and for the presence of sufficient oxygen. Employees must not enter bins, silos or tanks underneath a bridging condition, or where build-up of grain products on the sides could fall and bury them.
Medical Screening
Potential employees should be given a medical examination focusing on any pre-existing allergies and checking liver, kidney and lung function. Special examinations may be required for pesticide applicators and workers who use respiratory protection. Evaluations of hearing need to be made to assess any hearing loss. Periodic follow-up should seek to detect any changes.
Cocoa Production and the Chocolate Industry
Cocoa is indigenous to the Amazon region of South America, and, during the first years of the twentieth century, the southern region of Bahia provided the perfect conditions for its growth. The cocoa-producing region of Bahia is composed of 92 municipalities and Ilheus and Itabuna are its main centres. This region accounts for 87% of the national production of cocoa in Brazil, currently world’s the second largest producer of cocoa beans. Cocoa is also produced in about 50 other countries, with Nigeria and Ghana being major producers.
The vast majority of this production is exported to countries like Japan, the Russian Federation, Switzerland and the United States; half of this is sold as processed products (chocolate, vegetable fat, chocolate liquor, cocoa powder and butter) and the rest is exported as cocoa beans.
Process Overview
The industrial method for processing cocoa involves several stages. It begins with the storage of the raw material in adequate sheds, where it undergoes fumigation to prevent the proliferation of rodents and insects. Next, the process of cleaning the grains begins in order to remove any foreign objects or residues. Then all cocoa beans are dried out to extract excess moisture until an ideal level is reached. The next stage is the cracking of the grains in order to separate the skin from the core, followed by the roasting stage, which consists of the heating of the inner part of the grain.
The resulting product, which is in the shape of small particles known as “nibs”, is subject to a process of grinding (crushing), thus becoming a liquid paste, which in turn is strained and solidified in refrigeration chambers and sold as paste.
Most grinding companies normally separate the liquor through a process of pressing it until the fat is extracted and converted into two final products: cocoa butter and cocoa cake. The cake is packed in solid pieces while the cocoa butter is filtered, deodorized, cooled in refrigeration chambers and later packaged.
Hazards and Their Prevention
Although, the processing of cocoa is usually automated in such a way that it requires little manual contact and a high level of hygiene is maintained, the great majority of the employees in the industry still are exposed to a variety of occupational risks.
Noise and excessive vibration are problems found throughout the production line since, in order to prevent the easy access of rodents and insects, closed sheds are built with the machinery suspended on metal platforms. These machines must be subjected to proper maintenance and adjustment routines. Anti-vibratory devices should be installed. Noisy machinery should be isolated or noise reduction barriers should be used.
During the fumigation process, tablets of aluminium phosphate are utilized; as these come in contact with humid air, phosphine gas is released. It is recommended that grains remain covered for periods of 48 to 72 hours during and after these fumigation sessions. Air sampling should be done before re-entry.
The operation of grinders, hydraulic presses and drying machinery generate a great deal of heat with the high levels of noise; the high heat is intensified by the type of construction of the buildings. However, many safety measures can be adopted: use of barriers, isolation of the operations, implementation of schedules of working hours and breaks, availability of liquids to drink, use of adequate attire and the appropriate acclimatization of the employees.
In the areas of finished products, where the average temperature is 10 °C, staff members should wear appropriate clothing and have working periods of 20 to 40 minutes. The process of acclimatization is also important. Rest breaks in warm areas are necessary.
In the operations of product reception, where storage of raw materials and all finished products are packaged, ergonomically inadequate procedures and equipment are common. Mechanized equipment should replace manual handling where possible since moving and carrying loads can cause injuries, heavy articles can hit employees and injuries can result from the use of machinery without proper guards.
Procedures and equipment should be evaluated from an ergonomic point of view. Falls due to slippery floors are also a concern. In addition, there are other activities, like the cracking of the grains and the grinding and production of cocoa powder, where there are high levels of organic dust. Adequate dilution ventilation or local exhaust systems should be installed; processes and operations isolated and segregated as appropriate.
A rigorous programme of environmental risks prevention is highly recommended, in addition to the regular system of fire prevention and safety, adequate guarding of machinery and good standards of hygiene. Signs and informational bulletins should be posted in highly visible places and equipment and devices for the personal protection should be distributed to each worker. In maintaining machinery, a lockout/tagout programme should be instituted to prevent injuries.
Dairy Products Industry
Dairy products have formed an important element in human food since the earliest days when animals were first domesticated. Originally the work was done within the home or farm, and even now much is produced in small-scale enterprises, although in many countries large-scale industries are common. Cooperatives have been of great importance in the development of the industry and the improvement of its products.
In many countries, there are strict regulations governing the preparation of dairy products—for example, a requirement that all liquids be pasteurized. In most dairies, milk is pasteurized; sometimes it is sterilized or homogenized. Safe, high-quality dairy products are the goal of manufacturing plants today. While recent advances in technology allow for more sophistication and automation, safety is still a concern.
Liquid or fluid milk is the basic raw material for the dairy products industry. The milk is received via tanker trucks (or sometimes in cans) and is unloaded. Each tanker is checked for drug residues and temperature. The milk is filtered and stored in tanks/silos. Temperature of the milk should be less than 7 °C and held for no more than 72 hours. After storage, the milk is separated, the raw cream is stored in house or shipped elsewhere and the remaining milk is pasteurized. The raw cream temperature should also be less than 7 °C and held for no more than 72 hours. Before or after pasteurization (heating to 72°C for 15 seconds), vitamins may be added. If vitamins are added, proper concentrations must be administered. After pasteurization, the milk goes into a storage tank. The milk is then packaged, refrigerated and entered into distribution.
In the production of cheddar cheese, the incoming raw milk is filtered, stored, and the cream separated as discussed above. Before pasteurization, the dry and non-dairy ingredients are blended with the milk. This blended product is then pasteurized at a temperature greater than 72 °C for over 15 seconds. After pasteurization, the starter media (which has also been pasteurized) is added. The cheese-milk mixture then enters the cheese vat. At this time colour, salt (NaCl), rennet and calcium chloride (CaCl2) may be added. The cheese then enters the drain table. Salt may also be added at this time. Whey is then expelled and put into a storage tank. A metal detector can be used prior to filling to detect any metal fragments present in the cheese. After filling, the cheese is pressed, packaged, stored and entered into the distribution chain.
For the formation of butter, the raw cream from milk separation is either stored in house or received via trucks or cans. The raw cream is pasteurized at temperatures over 85 °C for over 25 seconds and placed in storage tanks. The cream is pre-heated and pumped into the churn. During churning, water, colour, salt and/or starter distillate may be added. After churning, the buttermilk that is produced is stored in tanks. The butter is pumped into a silo and subsequently packaged. A metal detector may be used prior to or after packaging to detect any metal fragments present in the butter. After packaging, the butter is palletized, stored and entered into the distribution chain.
In the production of dry milk, the raw milk is received, filtered and stored as previously discussed. After storage, the milk is preheated and separated. The raw cream is stored in house or shipped elsewhere. The remaining milk is pasteurized. The temperature of the raw cream and raw skim should be less than 7 °C and held for no more than 72 hours. The raw skim milk is pasteurized at a temperature over 72 °C for 15 seconds, evaporated by drying between heated cylinders or by spray drying and stored in tanks. After storage, the product enters a drying system. After drying, the product is cooled. Both the heated and cool air used must be filtered. After cooling, the product enters a bulk storage tank, is sifted and packaged. A magnet may be used prior to packaging to detect any ferrous metal fragments greater than 0.5 mm in the dry milk. A metal detector may be used prior to or after packaging. After packaging, the dry milk is stored and shipped.
Good Manufacturing Practices
Good manufacturing practices (GMPs) are guidelines to assist in the day-to-day operation of a dairy plant and to ensure the manufacture of a safe dairy product. Areas covered include premises, receiving/storage, equipment performance and maintenance, personnel training programmes, sanitation and recall programmes.
Microbiological, physical and chemical contamination of dairy products is a major industry concern. Microbiological hazards include Brucella, Clostridium botulinum, Listeria monocytogenes, hepatitis A and E, salmonella, Escherichia coli 0157:H7, Bacillus cereus, Staphylococcus aureus and parasites. Physical hazards include metal, glass, insects, dirt, wood, plastic and personal effects. Chemical hazards include natural toxins, metals, drug residues, food additives and inadvertent chemicals. As a result, dairies do extensive drug, microbiological and other testing to ensure product purity. Steam and chemical cleaning of equipment is necessary to maintain sanitary conditions.
Hazards and Their Prevention
Safety hazards include slips and falls caused by wet or soapy floor and ladder surfaces; exposures to unguarded machinery such as pinch points, conveyors, packing machines, fillers, slicers and so forth; and exposure to electrical shock, especially in wet areas.
Aisles should be kept clear. Spilled materials should be cleaned immediately. Floors should be covered with non-slip material. Machinery should be adequately guarded and properly grounded, and ground fault circuit interrupters should be installed in wet areas. Proper lockout/tagout procedures are necessary to ensure that the possibility of unexpected start-up of machines and equipment will not cause injury to plant personnel.
Thermal burns can occur from steam lines and steam cleaning and from leaks or line breaks of high-pressure hydraulic equipment. Cryogenic “burns” can occur from exposure to liquid ammonia refrigerant. Good maintenance, spill and leak procedures and training can minimize the risk of burns.
Fires and explosions. Leaking ammonia systems (the lower explosive limit for ammonia is 16%; the upper explosive limit is 25%), dry milk powder and other flammable and combustible materials, welding and leaking high-pressure hydraulic equipment can all result in fires or explosions. An ammonia leak detector should be installed in areas with ammonia refrigeration systems. Flammable and combustible materials must be stored in closed metal receptacles. Spraying of milk powder should meet appropriate explosion-proof requirements. Only authorized personnel should perform welding. Compressed-gas cylinders should be regularly examined. Precautions should be taken to prevent the mixture of oxygen with flammable gases. Cylinders should be kept away from sources of heat.
Frostbite and cold stress can occur from exposure in the freezers and coolers. Adequate protective clothing, job rotation to warmer areas, warm lunchrooms and provision of hot drinks are recommended precautions.
Exposures to high noise levels can occur in processing, packaging, grinding and plastic model blow-moulding operations. Precautions include isolation of noisy equipment, proper maintenance, wearing of hearing protectors and a hearing conservation programme.
When entering confined spaces—for example, when entering sewer pits or cleaning tanks—ventilation must be provided. The area should be free from equipment, product, gas and personnel. Impellers, agitators and other equipment should be locked out.
Lifting of raw materials, pulling cases of product and packaging of products are associated with ergonomic problems. Solutions include mechanization and automation of manual operations.
A wide variety of chemical exposures can occur in the dairy products industry, including exposure to:
- ammonia vapours due to leaks in ammonia refrigeration systems
- corrosive chemicals (e.g., phosphoric acid used in the manufacture of cottage cheese, cleaning compounds, battery acids and so on)
- chlorine gas generated by inadvertent mixing of chlorinated sanitizer with acids
- hydrogen peroxide generated during ultra-high-temperature packaging operations
- ozone (and ultraviolet) exposure from UV light used in sanitizing operations
- carbon monoxide generated by the action of caustics reacting with milk sugar in clean-in-place (CIP) operations in milk evaporators
- carbon monoxide generated from propane or gasoline lift trucks, gas-fired heaters or gas-fired carton heat sealers
- chromium, nickel and other welding fumes and gases.
Employees should be trained and aware of handling practices for hazardous chemicals. Chemicals must be labelled properly. Standard operating procedures should be established and followed when cleaning up spills. LEV should be provided where necessary. Protective clothing, safety goggles, face shields, gloves and so on must be available for use and subsequently maintained. An eye wash facility and a quick drench shower should be accessible when working with corrosive materials.
Biological hazards. Employees may be exposed to a variety of bacteria and other microbiological hazards from the unprocessed raw milk and cheeses. Precautions include proper gloves, good personal hygiene and adequate sanitary facilities.
Poultry Processing
Economic Importance
Chicken and turkey production has increased dramatically in the United States since the 1980s. According to a US Department of Labor report this has been due to a change in consumer eating patterns (Hetrick 1994). A shift from red meat and pork to poultry is due in part to early medical studies.
The rise in consumption correspondingly has spurred an increase in the number of processing facilities and growers and a large rise in levels of employment. For example, the United States poultry industry experienced an increase in employment of 64% from 1980 to 1992. Productivity, in terms of pounds yield per worker, increased 3.1% due to mechanization or automation, as well as an increase in line speed, or birds per work hour. However, in comparison to red meat production, poultry production is still very labour intensive.
Globalization is also ocurring. There are production and processing facilities jointly owned by US investors and China and breeding, grow-out and processing facilities in China export product to Japan.
Typical poultry line workers are relatively unskilled, less educated, often members of minority groups and much lower paid than workers in the red meat and manufacturing sectors. Turnover is unusually high in certain aspects of the process. Live hanging, deboning and sanitation jobs are particularly stressful and have high turnover rates. Poultry processing by its nature is a largely rural-based industry found in economically depressed areas where there is a labour surplus. In the United States many processing plants have an increasing number of Spanish-speaking workers. These workers are somewhat transient, working in the processing plants part of the year. As the region’s crops near harvest, large segments of the workers move outdoors to pick and harvest.
Processing
Throughout the processing of chicken, rigid sanitation requirements must be met. This means that floors must be washed down periodically and often and that debris, parts and fat must be removed. Conveyors and processing equipment must be accessible, washed down and sanitized also. Condensation must not be allowed to accumulate on ceilings and equipment over exposed chicken; it must be wiped down with long-handled sponge mops. Overhead, unguarded radial-blade fans circulate the air in the processing areas.
Because of these sanitation requirements, guarded rotating equipment often cannot be silenced for noise-abatement purposes. Consequently, in the majority of the processing plant’s production areas, there is high noise exposure. A proper and well-run hearing conservation programme is necessary. Not only should initial audiograms and annual audiograms be given, but periodic dosimetry should also be done to document exposure. Purchased processing equipment should have as low an operating noise level as possible. Particular care needs to be taken in educating and training the workforce.
Receiving and live hang
The first step in processing involves off-loading of the modules and destacking the trays onto a conveyor system to the live hang area. Work here is in almost complete darkness, since this has a quieting effect on the birds. The conveyor belt with a tray is at about waist level. A hanger, with gloved hands, must reach and grab a bird by both thighs and hang its feet in a shackle on an overhead conveyor travelling in the opposite direction.
The hazards of the operation vary. Aside from the normal high level of noise, the darkness and the disorienting effect of opposite running conveyors, there is the dust from flapping birds, suddenly sprayed urine or faeces in the face and the possibility of a gloved finger being caught in a shackle. Conveyor lines need to be equipped with emergency stops. Hangers are constantly striking the backs of their hands against neighboring shackles as they pass overhead.
It is not uncommon for a hanger to be required to hang an average of 23 (or more) birds per minute. (Some positions on the hanger’s lines require more physical motions, perhaps 26 birds per minute.) Typically, seven hangers on one line may hang 38,640 birds in 4 hours before they get a break. If each bird weighs approximately 1.9 kg, each hanger conceivably lifts a total of 1,057 kg during the first 4 hours of his or her shift before a scheduled break. The hanger’s job is extremely stressful from both a physiological and psychological standpoint. Reducing workload could lessen this stress. The constant grabbing with both hands, pulling in and simultaneously lifting a flapping, scratching bird at shoulder or head height is stressful to the upper shoulder and neck.
The bird’s feathers and feet can easily scratch a hanger’s unprotected arms. The hangers are required to stand for prolonged periods of time on hard surfaces, which can lead to lower-back discomfort and pain. Proper footwear, possible use of a rump rest stand, protective eyewear, single-use disposable respirators, eyewash facilities and arm guards need to be available for the hanger’s protection.
An extremely important element to ensure the worker’s health is a proper job conditioning programme. For a period of up to 2 weeks, a new hanger must be acclimated to the conditions and slowly work up to a full shift. Another key ingredient is job rotation; after two hours of hanging birds, a hanger may be rotated to a less strenuous position. The division of labour among the hangers may be such that frequent short rest breaks in an air conditioned area are essential. Some plants have tried double crewing to allow crews to work for 20 minutes and rest for 20 minutes, to reduce the ergonomic stressors.
The health and comfort conditions for the hangers are somewhat dependent on the outside weather conditions and the conditions of the birds. If the weather is hot and dry, the birds carry with them dust and mites, which easily become airborne. If the weather is wet, the birds are harder to handle, the hangers’ gloves readily become wet and the hangers must work harder to hold onto the birds. There have been recent developments in reusable gloves with padded backs.
The impact of airborne particulates, feathers, mites and so on may be lessened with an efficient local exhaust ventilation (LEV) system. A balanced system using the push-pull principle, which uses down-draft cooling or heating, would benefit the workers. Additional cooling fans placed about would upset the efficiency of a balanced push-pull system.
Once hung in the shackles, the birds are conveyed to be initially stunned with electricity. The high voltage does not kill them but forces them to hang limply as a rotating wheel (bicycle tyre) guides their neck against a counter-rotating circular cutting blade. The neck is partially severed with the bird’s heart still beating to pump out the remainder of blood. There must be no blood in the carcass. A skilled worker must be positioned to slice those birds the kill machine misses. Because of the excessive amount of blood, the worker must be protected by wearing wet gear (a rain suit) and eye protection. Eye washing or flushing facilities must be made available also.
Dressing
The conveyor of birds then passes through a series of troughs or tanks of circulating hot water. These are called scalders. Water is usually heated by steam coils. The water is usually treated or chlorinated to kill bacteria. This phase allows the feathers to be easily removed. Care must be taken when working around the scalders. Often piping and valves are unprotected or poorly insulated and are contact points for burns.
As the birds exit the scalders, the carcass is passed through a U-shaped arrangement which pulls the head off. These parts are usually conveyed in flowing water troughs to a rendering (or by-products) area.
The line of carcasses passes through machines which have a series of rotating drums fixed with rubber fingers which remove the feathers. The feathers drop into a trench below with flowing water leading to the rendering area.
Consistency in bird weight is extremely critical to all aspects of the processing operation. If the weights vary from load to load, the production departments must adjust their processing equipment accordingly. For example, if lighter-weight birds follow heavier birds through the pickers, the rotating drums may not get all the feathers off. This causes rejects and rework. Not only does it add to the processing costs, but it causes additional ergonomic hand stresses, because someone has to hand pick the feathers using a pincer grip.
Once through the pickers, the line of birds passes through a singer. This is a gas-fired arrangement with three burners on each side, used to singe the fine hairs and feathers of each bird. Care must be taken to assure that the gas piping’s integrity is maintained due to the corrosive conditions of the picking or dressing area.
The birds then pass a hock cutter to sever the feet (or paws). The paws may be conveyed separately to a separate processing area of the plant for cleaning, sizing, sorting, chilling and packaging for the Asian market.
The birds must be rehung on different shackles before they enter the evisceration section of the plant. The shackles here are configured slightly differently, usually longer. Automation is readily available for this part of the process (see figure 1). However, workers need to provide back-up if a machine jams, to rehang dropped birds or to manually cut the feet off with pruning shears if the hock cutter fails to sever properly. From a processing and cost standpoint, it is critical that every shackle be filled. Rehang jobs involve exposure to highly repetitive motions and work involving awkward postures (raised elbows and shoulders). These workers are at increased risk for cumulative trauma disorders (CDTs).
Figure 1. Multi-cut machines reducing repetitive manual work

If a machine goes down or gets out of adjustment, a great deal of effort and stress is applied to get the lines running, sometimes at the expense of workers’ safety. When climbing to access points on the equipment, a maintenance worker may not take the time to get a ladder, instead stepping on top of wet, slippery equipment. Falls are a hazard. When any such equipment is purchased and installed, provisions must be made for easy access and maintenance. Lockout points and shut-offs need to be placed on each piece of equipment. The manufacturer must consider the environment and hazardous conditions under which their equipment must be maintained.
Evisceration
As the conveyor of birds pass out of dressing into a physically separate part of the process, they usually pass through another singer and then through a rotating circular blade which cuts out the oil sac or gland on each bird’s back at the base of the tail. Often such equipment’s blades are free rotating and need to guarded properly. Again, if the machine is not adjusted according to the bird’s weight, workers must be assigned to remove the sac by slicing it off with a knife.
Next, the conveyor line of birds passes through an automatic venting machine, which pushes up on the abdomen slightly while a blade cuts open the carcass without disturbing the bowel. The next machine or part of the process scoops into the cavity and pulls out the unbroken viscera for inspection. In the United States, the next few processing steps may involve government inspectors who check for growths, air sac disease, faecal contamination and a series of other abnormalities. Usually one inspector checks for only two or three items. If there is a high rate of abnormalities, the inspectors will slow the line down. Often the abnormalities do not cause total rejects, but specific parts of the birds may be washed or salvaged from the carcass to increase yield.
The more rejects, the more manual rework involving repetitive motion due to cutting, slicing and so on the production workers must perform. Government inspectors are usually seated on mandated adjustable elevating stands, whereas production workers called helpers, to their left and right, stand on grating or may use an adjustable sit stand if provided. Foot rests, adjustable height platforms, sit stands and job rotation will help relieve the physical and psychological stresses associated with this part of the process.
Once past the inspections, the viscera are sorted as they pass through a liver/heart or giblet harvester. The separated intestines, stomachs, spleens, kidneys and gall bladders are discarded and flushed into a flowing trench below. The heart and liver are separated and pumped to separate sorting conveyors, where workers inspect and pick by hand. The remaining intact livers and hearts are pumped or carried to a separate processing area to be bulk-packed by hand or later recombined in a giblet pack for stuffing by hand into the cavity of a whole bird for sale.
Once the carcass clears the harvester, the bird’s crop is augured out; each body cavity is probed by hand to pull out the remaining viscera and gizzard if necessary. The worker uses each hand in a separate bird as the conveyor passes in front. A suction device is often used to vacuum out any remaining lungs or kidneys. Frequently, due to the bird’s habit of ingesting small pebbles or pieces of litter during grow-out, a worker will reach into the bird’s cavity and receive painful puncture wounds in the tips of the fingers or under the finger nails.
The small wounds, if not treated properly, run the risk of serious infection since the bird’s cavity still is not cleaned of bacteria. Since tactile sensitivity is necessary for the job, there are no gloves yet available to prevent these frequent incidents. A tight-fitting surgeon’s type glove has been tried with some success. The line pace is so fast that it does not allow the worker to carefully insert his or her hands.
Finally, the carcass’s neck is removed by machine and harvested. The birds go through a bird washer which uses chlorinated spray to wash out excess viscera inside and outside each bird.
Throughout the dressing and evisceration, workers are exposed to high levels of noise, slippery floors and high ergonomic stress on kill, scissor and packaging jobs. According to a NIOSH study, rates of CTDs documented in poultry plants can range from 20 to 30% of workers (NIOSH 1990).
Chiller operations
Depending on the process, necks are pumped to a open-surfaced chiller tank with rotating arms, paddles or augers. These open tanks pose a serious threat to the safety of the worker during operation and need to be properly guarded by removable covers or grills. The tank’s cover must allow for visual inspection of the tank. If a cover is removed or lifted, interlocks must be provided to shut off the rotating arms or auger. The chilled necks are either bulk-packed for later processing or taken to the giblet wrap area for recombining and wrapping.
Once through evisceration, the conveyor lines of birds are either dropped into large, open-surfaced horizontal chilling tanks or, in Europe, pass through refrigerated, circulating air. These chillers are fitted with paddles which slowly rotate through the chiller, bringing down the bird’s body temperature. The chilled water is highly chlorinated (20 ppm or greater) and aerated for agitation. Bird carcass residence time in the chiller may be up to an hour.
Due to the high levels of free chlorine released and circulated, workers are exposed and may experience symptoms of eye and throat irritation, coughing and shortness of breath. NIOSH conducted several studies of eye and upper respiratory irritation in poultry processing plants, which recommended that levels of chlorine be monitored and controlled closely, that curtains be used to contain the liberated chlorine (or an enclosure of some sort should surround the open surface of the tank) and that an exhaust ventilation system should be installed (Sanderson, Weber and Echt 1995).
The resident time is critical and a matter of some controversy. Upon exiting evisceration, the carcass is not completely clean, and the skin pores and feather follicles are open and harbour disease-causing bacteria. The main purpose of the trip through the chiller is to chill the bird quickly to reduce spoilage. It does not kill bacteria, and the risk of cross contamination is a serious public health issue. Critics have called the chiller bath method “faecal soup”. From a profit perspective, a side benefit is the fact that the meat will absorb the chiller water like a sponge. It adds almost 8% to the market weight of the product (Linder 1996).
Upon exiting the chiller, the carcasses are deposited on a conveyor or shaker table. Specially trained workers called graders inspect the birds for bruises, skin breaks and so on and rehang the birds on separate shackle lines travelling in front of them. Downgraded birds may travel to different processes for parts recovery. Graders stand for prolonged periods handling chilled birds, which can result in numbness and hand pain. Gloves with liners are worn not only to protect the hands of workers from the chlorine residue, but also to provide some degree of warmth.
Cut-up
From grading the birds travel overhead to different processes, machines and lines in an area of the plant called second or further processing. Some machines are hand fed with two-handed trips. Other, more modern European equipment, at separate stations, may remove the thighs and wings and split the breast, without being touched by the worker. Again, consistency in bird size or weight is critical to the successful operation of this automated equipment. Rotating circular blades must be changed every day.
Skilled maintenance technicians and operators must be attentive to the equipment. Access to such equipment for adjustment, maintenance and sanitation needs to be frequent, requiring stairs, not ladders, and substantial work platforms. During blade changing, handling needs to be cautious because of the slipperiness due to fat build-up. Special cut- and slip-resistant gloves with the fingertips removed protect most of the hand, while the tips of the fingers can be used to manipulate the tools, bolts and nuts used for replacement.
Evolving consumer tastes have affected the production process. In some cases, the products (e.g., drumstick, thighs and breasts) are required to be skinless. Processing equipment has been developed to efficiently remove skin so workers do not have to do so by hand. However, as automated processing equipment is added and lines are rearranged, conditions become more crowded and awkward for workers to get around, manoeuvre floor jacks and carry totes, or plastic tubs, of iced product weighing over 27 kg over slippery, wet floors.
Depending on the customer demand and product mix sales, workers stand facing fixed-height conveyors, selecting and arranging product on plastic trays. The product travels in one direction or drops from a chute. The trays arrive on overhead conveyors, descending so the workers can grab a stack and set them in front for easy reach. Product defects may be either placed on a counter-flow conveyor below or hung in a shackle travelling in the opposite direction overhead. Workers stand for prolonged periods of time almost shoulder to shoulder, perhaps separated only by a tote into which defects or waste are dropped. Workers need to be provided with gloves, aprons and boots.
Some products may be bulk-packed in cartons covered with ice. This is called ice pack. Workers fill cartons by hand onto scales and manually transfer them to moving conveyors. Later in the ice pack room, ice is added, cartons recovered and the cartons removed and stacked manually on pallets ready for shipment.
Some workers in cut-up are also exposed to high levels of noise.
Deboning
If the carcass is destined for deboning, the product is tanked out in large aluminium bins or cardboard boxes (or gaylords) mounted on pallets. Breast meat must be aged for a certain number of hours before processing either by machine or hand. Fresh chicken is difficult to cut and trim by hand. From an ergonomic standpoint, meat ageing is a key point in helping to reduce repetitive motion injuries to the hand.
There are two methods used in deboning. In the manual method, once ready, carcasses with only the breast meat remaining are dumped into a hopper leading to a conveyor. This section of the line’s workers must handle each carcass and hold them against two horizontal, in-running textured skinner rolls. The carcass is rolled over the rolls as the skin is pulled away and down to a conveyor below. There is a risk of workers becoming inattentive or distracted and having their fingers pulled into the rollers. Emergency stop (E-stop) switches need to be provided within easy reach of either the free hand or knee. Gloves and loose clothing cannot be worn around such equipment. Aprons (worn snugly) and protective eyewear must be worn due to the possibility of bone chips or fragments being thrown.
The next step is performed by workers called nickers. They hold a carcass in one hand and make a slice along the keel (or breastbone) with the other. Sharp, short-bladed knives are normally used. Stainless steel mesh gloves are usually worn over a latex- or nitrile-gloved hand holding the carcass. Knives used for this operation do not need to have a sharp point. Protective eye wear needs to be worn.
The third step is performed by the keel pullers. This may be done manually or with a jig or fixture where the carcass is guided over an inexpensive “Y” fixture (made out of stainless steel rod stock) and pulled toward the worker. The working height of each fixture needs to be adjusted to the worker. The manual method simply requires the worker to use a pincer grip with a gloved hand and pull the keel bone out. Protective eyewear must be worn as described above.
The fourth step requires hand filleting. Workers stand shoulder to shoulder reaching for breast meat as it travels on shackle trays in front of them. There are certain techniques that must be observed for this part of the process. Proper job instruction and immediate correction when errors are observed are necessary. Workers are protected with a chain or mesh glove on one hand. In the other, they hold an extremely sharp knife (with a tip that may be too sharply pointed).
The work is fast paced, and workers who get behind are pressured to take short cuts, such as reaching across in front of the associate next to them or reaching for and/or stabbing a piece of meat travelling by out of their reach. Not only does the knife puncture reduce the quality of the product, but it also results in serious injury to fellow workers in the form of lacerations, which are often subject to infection. Protective plastic arm guards are available to prevent this frequent type of injury.
As the fillet meat is replaced on the conveyor shackle, it is picked off by the next section of workers, called trimmers. These workers must trim excess fat, missed skin and bones out of the meat using sharp and adjusted shears. Once trimmed, the finished product is either tray packed by hand or dropped into bulk bags and placed into cartons for restaurant use.
The second method of deboning involves automatic processing equipment developed in Europe. As with the manual method, bulk boxes or tanks of carcasses, sometimes with wings still attached, are loaded into a hopper and chute. Carcasses may then be picked manually and placed into segmented conveyors, or each carcass must be placed manually onto a shoe of the machine. The machine moves rapidly, carrying the carcass through a series of fingers (to remove skin), cutting blades and slitters. All that remains is a meatless carcass that is bulked out and used elsewhere. Most of the manual line’s positions are eliminated, except for the trimmers with scissors.
Deboning workers are exposed to serious ergonomic hazards from the forceful, repetitive nature of the work. In each of the deboning positions, especially filleters and trimmers, job rotation may be a key element to reducing ergonomic stresses. It must be understood that the position a worker rotates to must not use the same muscle group. A weak argument has been made that filleters and trimmers may rotate to each other’s position. This should not be allowed, because the same gripping, twisting and turning methods are used in the hand not holding the tool (knife or scissors). It may be argued that the muscles holding a knife loosely for twisting and turning while making fillet cuts are used differently when opening and closing scissors. However, twisting and turning of the hand is still required. Line speeds play a critical role in the onset of ergonomic disorders on these jobs.
Overwrap and chilling
After the product is tray packed in either cut-up or deboning, the trays are conveyed to another step in the process called overwrap. Workers retrieve specific product in trays and feed the trays into machines which apply and stretch printed clear wrap over the tray, tuck it under and pass the tray over a heat sealer. The tray may then pass through a washer, where it is retrieved and placed in a basket. The basket containing a particular product is placed on a conveyor where it passes into a chiller area. Trays are then sorted and stacked either manually or automatically.
Workers in the overwrap area stand for prolonged periods of time and are rotated so the hands they use to pick up the product trays are rotated. Normally the overwrap area is relatively dry. Cushioned mats would reduce leg and back fatigue.
Consumer demand, sales and marketing can create special ergonomic hazards. At certain times of the year, large trays are packed with several pounds of product for “convenience and cost savings”. This added weight has contributed to additional repetitive motion-related hand injuries simply because the process and conveying system is designed for one-handed pick-up. A worker simply does not have the strength necessary for repeated one-handed lifts of overweight trays.
The clear plastic wrap used in the packing may release slight amounts of monomer or other decomposition products when heated for sealing. If complaints arise concerning the fumes, the manufacturer or supplier of the film should be called in to help assess the problem. LEV may be necessary. The heat-sealing equipment needs to be maintained properly and its E-stops checked for proper operation at the beginning of each shift.
The chilling room or refrigeration area poses a different set of fire, safety and health risks. From a fire standpoint, the product packaging poses a risk since it is usually highly combustible polystyrene. The wall’s insulation is usually a polystyrene foam core. Chillers should be properly protected with pre-action dry sprinkler systems designed for extraordinary hazard. (Pre-action systems employ automatic sprinklers attached to piping systems containing dry air or nitrogen as well as a supplemental detection system installed in the same area as the sprinklers.)
Once the baskets of trays enter the chiller, workers must physically pick up a basket and lift it to shoulder height or higher to a stack on a dolly. After so many baskets are stacked, workers are required to assist each other to stack the baskets of product higher.
Temperatures in the chiller may run as low as –2 °C. Workers should be issued and instructed to wear multilayered clothing or “freezer suits” along with insulated safety-toed footwear. Dollies or stacks of baskets must be physically handled and pushed to various areas of the chiller until called for. Often, workers attempt to save time by pushing several stacks of trays at one time, which can result in muscle or lower-back strain.
Basket integrity is an important aspect of both product quality control and worker safety. If broken baskets are stacked with other full baskets stacked on top, the entire load becomes unstable and is easily tipped over. Product packages fall on the floor and become dirty or damaged, resulting in rework and extra manual handling by workers. Stacks of baskets may also fall on other workers.
When a particular product mix is called for, baskets may be destacked manually. Trays are loaded onto a conveyor with a scale which weighs them and attaches labels marked with the weight and codes for tracking purposes. Trays are packed manually in cartons or boxes sometimes lined with impermeable liners. Workers often have to reach for trays. As in the case of the overwrap process, larger, heavier packages of product can cause stress to the hands, arms and shoulders. Workers stand for prolonged periods in one spot. Antifatigue mats can reduce leg and lower-back stresses.
As the cartons of packages pass down a conveyor, liners may be heat sealed while CO2 is injected. This, along with continued refrigeration, prolongs product shelf life. Also, as the carton or case continues its progress, a scoop of CO2 nuggets (dry ice) is added to prolong shelf life on its way to a customer in a refrigerated trailer. However, CO2 has inherent hazards in enclosed areas. The nuggets may either be dropped by the chute or scooped out of a large, partially covered bin. Though the exposure limit (TLV) for CO2 is relatively high, and continuous monitors are readily available, workers also need to learn its hazards and symptoms and wear protective gloves and eye protection. Proper warning signs should also be posted in the area.
Cartons or cases of trayed product usually are sealed with hot-melt adhesive injected onto the cardboard. Painful contact burns are possible if adjustments, sensors and pressures are improper. Workers need to wear protective eyewear with side shields. The application and sealing equipment needs to be completely de-energized, with pressure bled off, before adjustments or repairs are made.
Once the cartons are sealed, they may either be manually lifted from the conveyor or run through an automatic palletizer or other remotely operated equipment. Due to the high rate of production, the potential for back injuries exists. This work is usually performed in a cold environment, which has a tendency to lead to strain injuries.
From an ergonomic standpoint, carton retrieval and stacking is easily automated, but investment and maintenance costs will be high.
Thigh deboning and ground chicken
No part of the chicken is wasted in modern poultry processing. Chicken thighs are bulk-packed, stored at or near freezing and then further processed, or deboned, either with scissors or pneumatically actuated hand-operated trimmers. Like the breast deboning operation, thigh deboning workers must remove excess fat and skin with scissors. Work area temperatures may be as low as 4 to 7 °C. Despite the fact that trimmers may wear liners with gloves, their hands are sufficiently chilled to restrict blood circulation, thereby magnifying the ergonomic stresses.
Once chilled, the thigh meat is further processed by adding flavours and grinding under a CO2 blanket. It is extruded as ground chicken patties or bulk.
Deli processing
Necks, backs and remaining carcasses from breast deboning are not wasted, but dumped into large paddle grinders or mixers, pumped through chilled mixers and extruded into bulk containers. This is usually sold or sent for further processing into what is called “chicken hot dogs” or “frankfurters”.
The recent development of convenience foods, which require little processing or preparation in the home, has resulted in high-value-added products for the poultry industry. Select pieces of meat from breast deboning are placed in a rotating vessel; solutions of flavouring and spices are then mixed under vacuum for a prescribed length of time. The meat gains not only flavour but weight as well, which improves the profit margin. The pieces are then packaged individually in trays. The trays are sealed under vacuum and packed off in small cases for shipment. This process is not time dependent, so workers are not subjected to the same line speeds as others in cut-up. The final product must be handled, inspected and packed carefully so it presents well in the stores.
Summary
Throughout poultry plants, wet processes and fat can create very dangerous floors, with a concurrent high risk of slipping and falling hazards. Proper cleaning of floors, adequate drainage (with protective barriers placed on all floor holes), proper footwear (waterproof and anti-slip) provided to workers and anti-slip floors are key to preventing these hazards.
In addition, high levels of noise are pervasive in poultry plants. Attention must be paid to engineering measures that decrease noise levels. Earplugs and replacements must be provided, as well as a full hearing conservation programme with annual hearing exams.
The poultry industry is an interesting blend of labour-intensive operations and high-tech processing. Human sweat and anguish still characterize the industry. The demands for increased yield and higher line speeds frequently overshadow efforts to properly train and protect the workers. As the technology improves to help eliminate repetitive-motion injuries or disorders, the equipment must be carefully maintained and calibrated by skilled technicians. The industry generally does not attract highly skilled technicians because of the mediocre pay levels, extremely stressful working conditions and often autocratic management, which also often resists positive changes that can be achieved with pro-active safety and health programming.
Meatpacking/Processing
Sources of meat slaughtered for human consumption include cattle, hogs, sheep, lambs and, in some countries, horses and camels. The size and production of slaughterhouses vary considerably. Except for very small operations located in rural areas, animals are slaughtered and processed in factory-type workplaces. These workplaces are usually subject to food-safety controls by the local government to prevent bacterial contamination that can cause foodborne illnesses in consumers. Examples of known pathogens in meat include salmonella and Escherichia coli. In these meat processing plants the work has become very specialized, with almost all the work being done on production disassembly lines where the meat moves on chains and conveyors, and each worker does only one operation. Almost all the cutting and processing is still done by workers. Production jobs can require between 10,000 and 20,000 cuts a day. In some large plants in the United States, for example, a few jobs, such as carcass splitting and bacon slicing, have been automated.
Slaughtering Process
The animals are herded through a holding pen to slaughter (see figure 1). The animal must be stunned before being bled, unless slaughtered in accordance with Jewish or Muslim rites. Usually the animal is either knocked to an unconscious state with a bolt stunner gun or with a stunner gun utilizing compressed air that drives a pin into the head (the medulla oblongata) of the animal. After the stunning or “knocking” process, one of the animal’s hind legs is secured by a chain hooked onto an overhead conveyor which transfers the animal to the next room, where it is bled by “sticking” the jugular arteries in the neck with a sharp knife. The bleeding-out process follows, and the blood is drained through pipes for processing on floors below.
Figure 1. Beef slaughtering flow chart
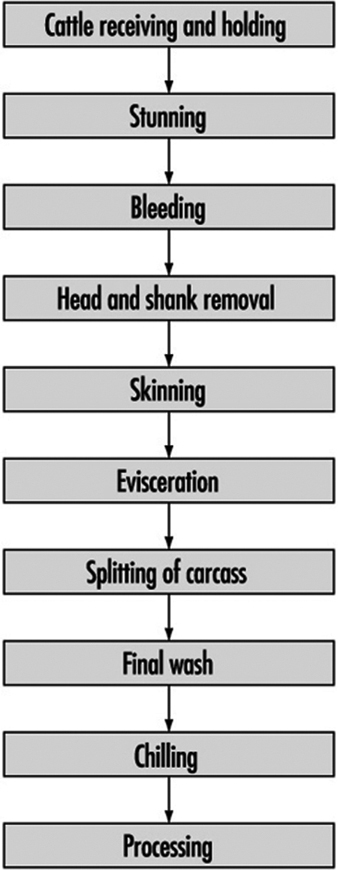
The skin (hide) is removed by a series of cuts with knives (new air-powered knives are being used in the larger plants for some hide-removal operations) and the animal is then suspended by both hind legs from the overhead conveyor system. In some hog operations, the skin is not removed at this stage. Rather the hair is removed by sending the carcass through tanks of water heated to 58 ºC and then through a dehair machine that rubs the hair off the skin. Any remaining hair is removed by singeing and finally shaving.
The front legs and then the viscera (intestines) are removed. The head is then cut and dropped, and the carcass is split in half vertically along the spinal column. Hydraulic band saws are the usual tool for this job. After the carcass is split, it is rinsed with hot water, and may be steam vacuumed or even treated with a newly developed pasteurization process being introduced in some countries.
Government health inspectors usually inspect after the head removal, the viscera removal and the carcass splitting and final wash.
After this, the carcass, still hanging from the overhead conveyor system, moves to a cooler for chilling over the next 24 to 36 hours. The temperature is usually about 2 ºC to slow bacterial growth and inhibit spoilage.
Processing
Once chilled, the carcass halves are then cut into front and hind quarters. After this, pieces are further divided into prime cuts, depending on customer specifications. Some quarters are processed for delivery as the front or hind quarters without any further significant trimming. These pieces can weigh from 70 to 125 kg. Many plants (in the United States, the majority of plants) conduct further processing of the meat (some plants do only this processing and receive their meat from slaughterhouses). Products from these plants are shipped in boxes weighing approximately 30 kg.
Cutting is done by hand or powered saws, depending on the cuts, usually following trimming operations to remove skin. Many plants also use large grinders for grinding hamburger and other ground meats. Further processing can involve equipment including bacon presses, ham tumblers and extruders, bacon slicers, electric meat tenderizers and smoke houses. Conveyor belts and screw augers are often used to transport product. Processing areas are also kept cool, with temperatures in the 4 °C range.
Offal meats, such as liver, hearts, sweetbreads, tongues and glands, are processed in a separate area.
Many plants also treat the hides before sending them to a tanner.
Hazards and Their Prevention
Meatpacking has one of the highest rates of injury of all industries. A worker may be injured by the moving animals as they are led through the holding pen into the plant. Adequate training must be given to workers on handling live animals, and minimal worker exposure in this process is advised. Stunner guns may prematurely or inadvertently discharge while workers try to still the animals. Falling animals and nervous system reactions in stunned cattle that cause jerking present hazards to workers in the area. Further, many operations utilize a series of hooks, chains and conveyor tram rails to move the product between processing steps, posing the hazard of falling carcasses and product.
Adequate maintenance of all equipment is necessary, especially equipment used to move meat. Such equipment must be checked frequently and repaired as needed. Adequate safeguards for knocking guns, such as safety switches and making sure there is no blow back, must be taken. Workers involved in knocking and sticking operations must be trained on the hazards of this job, as well as provided with guarded knives and protective equipment to prevent injury. For sticking operations this includes arm guards, mesh gloves and special guarded knives.
Both in the slaughter and further processing of animals, hand knives and mechanical cutting devices are used. Mechanical cutting devices include head splitters, bone splitters, snout pullers, electric band and circular saws, electric- or air-powered circular-blade knives, grinding machines and bacon processors. These types of operations have a high rate of injury, from knife cuts to amputations, because of the speed at which workers operate, the inherent danger of the tools being used and the often slippery nature of the product from fat and wet processes. Workers can be cut by their own knives and by other workers’ knives during the butchering process (see figure 2).
Figure 2. Cutting and sorting meat without protective equipment in a Thai meat packing factory
The above operations require protective equipment, including protective helmets, footwear, mesh gloves and aprons, wrist and forearm guards and waterproof aprons. Protective goggles may be required during boning, trimming and cutting operations to prevent foreign objects from entering workers’ eyes. Metal mesh gloves must not be used while operating any type of powered or electrical saw. Powered saws and tools must have proper safety guards, such as blade guards and shut-off switches. Unguarded sprockets and chains, conveyor belts and other equipment can pose a hazard. All such equipment must be properly guarded. Hand knives should also have guards to prevent the hand holding the knife from slipping over the blade. Training and adequate spacing between workers is necessary to conduct operations safely.
Workers maintaining, cleaning or unjamming equipment such as conveyor belts, bacon processors, meat grinders and other processing equipment are subject to the hazard of the inadvertent start-up of equipment. This has caused fatalities and amputations. Some equipment is cleaned while running, subjecting workers to the hazard of getting caught in the machinery.
Workers must be trained in safety lockout/tagout procedures. Implementation of procedures that prevent workers from fixing, cleaning or unjamming equipment until the equipment is off and locked out will prevent injuries. Workers involved in locking out pieces of equipment must be trained on procedures for neutralizing all energy sources.
Wet and treacherously slippery floors and stairs throughout the plant pose a serious hazard to workers. Elevated work platforms also pose a falling hazard. Workers must be provided with safety shoes with non-slip soles. Non-slip floor surfaces and roughened floors, approved by local health agencies, are available and should be used on floors and stairways. Adequate drainage in wet areas must be provided, along with proper and adequate housekeeping of floors during production hours to minimize wet and slippery surfaces. All elevated surfaces must also be properly equipped with guard rails both to prevent workers from accidental falls and to prevent worker contact and materials falling from conveyors. Toe boards should also be used on elevated platforms, where necessary. Guardrails should also be used on stairways on the production floor to prevent slipping.
The combination of wet working conditions and elaborate electrical wiring poses a hazard of electrocution to workers. All equipment must be properly grounded. Electrical outlet boxes should be provided with covers which effectively protect against accidental contact. All electrical wiring should be checked periodically for cracking, fraying or other defects, and all electrical equipment should be grounded. Ground fault circuit interrupters should be used where possible.
Lugging of carcasses (which can weigh up to 140 kg) and repetitive lifting of 30 kg boxes of meat ready for shipping can cause back injuries. Cumulative trauma disorders such as carpal tunnel syndrome, tendinitis and tenosynovitis are widespread in the industry. In the United States, for example, meatpacking operations have higher rates of these disorders than any other industry. The wrist, elbow and shoulder are all affected. These disorders can arise from the highly repetitive and forceful nature of the assembly line work in the plants, the use of vibrating equipment in some jobs, the use of dull knives, the cutting of frozen meat and the use of high-pressure hoses in cleaning operations. Prevention of these disorders comes through ergonomic redesign of equipment, use of mechanical assists, vigilant maintenance of vibrating equipment to minimize vibration, and improved worker training and medical programmes. Ergonomic redesign measures include:
- lowering overhead conveyors to reduce repetitive overhead throws on production lines (see figure 3)
- moving horizontal platforms that allow workers to split animals with a minimum of reaches
- providing sharp knives with redesigned handles
- building mechanical assists that reduce the force of a job (see figure 4)
- increased staffing on high-force jobs, assuring properly sized hand tools and gloves and careful design of packing areas to minimize twisting when lifting, as well as to minimize lifting from below the knees and above the shoulders
- vacuum hoists and other mechanical lifting devices to reduce lifting of boxes (see figure 5).
Figure 3. With conveyer belts located beneath worktables, workers can push finished products through a hole in the table instead of having to throw meat over their heads

United Food & Commercial Workers, AFL-CIO
Figure 4. Having paddle bones pulled out by the force of an attached chain rather than manually lessens musculoskeletal hazards

United Food & Commercial Workers, AFL-CIO
Figure 5. The use of vacuum hoists for lifting boxes allows workers to guide boxes rather than load them by hand

United Food & Commercial Workers, AFL-CIO
Aisles and walkways should be dry and free of obstacles so that carrying and transporting heavy loads can be done safely.
Workers should be trained or proper use of knives. Cutting frozen meat should be avoided completely.
Early medical intervention and treatment for symptomatic workers is also desirable. Because of the similar nature of the stressors on jobs in this industry, job rotation must be used with caution. Job analyses must be carried out and reviewed to assure that the same muscle tendon groups are not used in different tasks. In addition, workers must be adequately trained in all jobs in any planned rotation.
Machines and equipment found in meatpacking plants produce a high level of noise. Workers must be provided with ear plugs, as well as hearing examinations to ascertain any potential hearing loss. Further, sound-dampening equipment should be used on machinery where possible. Good maintenance on conveyor systems can prevent unnecessary noise.
Workers can be exposed to toxic chemicals during the cleaning and sanitizing of equipment. Compounds used include both alkaline (caustic) and acid cleaners. These can cause dryness, allergic rashes and other skin problems. Liquids can splash up and burn the eyes. Depending on the type of cleaning compound used, PPE—including eye, face and arm coverings, aprons and protective footwear—must be provided. Hand and eye washing facilities should also be available. High-pressure hoses used to transport hot water for disinfecting equipment can also cause burns. Adequate worker training on the use of such hoses is important. Chlorine in the water used to wash the carcasses can also cause eye, throat and skin irritation. New anti-bacterial rinses are being introduced on the slaughter side to decrease bacteria that can cause foodborne illnesses. Adequate ventilation must be provided. Special care to assure that the strength of the chemicals does not exceed manufacturers’ instructions must be taken.
Ammonia is used as a refrigerant in the industry, and ammonia leaks from pipes are common. Ammonia gas is irritating to the eyes and skin. Mild to moderate exposure to the gas can produce headaches, burning in the throat, perspiration, nausea and vomiting. If escape is not possible, there may be severe irritation of the respiratory tract, producing cough, pulmonary oedema or respiratory arrest. Adequate maintenance of refrigeration lines is key to preventing such leaks. In addition, once an ammonia leak is detected, monitoring and evacuation procedures must be carried out to prevent dangerous exposures.
Carbon dioxide (CO2) in the form of dry ice is used in the packaging area. During this process, CO2 gas may escape from these vats and spread throughout the room. Exposure can cause headaches, dizziness, nausea, vomiting and, at high levels, death. Adequate ventilation must be provided.
Blood tanks present hazards associated with confined spaces if the plant does not utilize a closed piping and processing system for the blood. Toxic substances emitted from decomposing blood and lack of oxygen pose serious hazards to those having to enter and/or clean tanks or work in the area. Prior to entry, the atmosphere must be tested for toxic chemicals, and the presence of adequate oxygen must be assured.
Workers are exposed to infectious diseases such as brucellosis, erysipeloid, leptospirosis, dermatophytoses and warts.
Brucellosis is caused by a bacterium and is transmitted by the handling of infected cattle or swine. Persons infected by this bacterium experience constant or recurring fever, headaches, weakness, joint pain, night sweats and loss of appetite. Limiting the number of infected cattle slaughtered is one key to preventing this disorder.
Erysipeloid and leptospirosis are also caused by bacteria. Erysipeloid is transmitted by infection of skin puncture wounds, scratches and abrasions; it causes redness and irritation around the site of infection and can spread to the bloodstream and lymph nodes. Leptospirosis is transmitted through direct contact with infected animals or through water, moist soil or vegetation contaminated by the urine of infected animals. Muscular aches, eye infections, fever, vomiting, chills and headaches occur, and kidney and liver damage may develop.
Dermatophytosis, on the other hand, is a fungal disease and is transmitted by contact with the hair and skin of infected persons and animals. Dermatophytosis, also know as ringworm, causes the hair to fall out and small, yellowish cuplike crusts to develop on the scalp.
Verruca vulgaris, a wart caused by a virus, can be spread by infectious workers who have contaminated towels, meat, fish knives, work tables or other objects.
Other diseases that are found in meatpacking plants in some countries include Q fever and tuberculosis. The primary carriers of Q fever are cattle, sheep, goats and ticks. Humans are usually infected by inhaling aerosolized particles from contaminated environments. Typical symptoms include fever, malaise, severe headache and muscular and abdominal pain. The incidence of toxoplasma antibodies amongst abattoir workers is high in certain countries.
Dermatitis is also common in meatpacking plants. Exposure to blood and other animal fluids, exposure to wet conditions, and exposure to cleaning compounds used for cleaning/sanitation in facilities can lead to skin irritation.
Infectious diseases and dermatitis can be prevented with personal hygiene that includes ready and easy access to sanitation and hand-washing facilities that contain soap and disposable hand towels, the provision of proper PPE (which may include protective gloves as well as eye and respiratory protection where exposure to airborne animal body fluids is possible), the use of some barrier creams to provide limited protection against irritants, worker education and early medical care.
The kill floor, where the slaughtering, bleeding and splitting of the animal is done, can be especially hot and humid. A properly working ventilation system that removes the hot, humid air and prevents heat stress should be used. Fans, preferably overhead or roof fans, increase air movement. Beverages should be provided to replace fluids and salts lost through sweating, and frequent rest breaks, in a cool area, should be allowed.
There is also a distinctive smell in slaughterhouses, due to a mixture of odours such as those of wet leather, blood, vomit, urine and faeces of animals. This smell spreads throughout the kill floor, offal, rendering and hide areas. Exhaust ventilation is necessary to remove the odours.
Refrigerated work environments are essential in the meatpacking industry. Processing and transporting meat products generally require temperatures at or below 9 °C. Areas such as freezers may require temperatures to go as low as –40 °C. The most common cold-related injuries are frostnip, frostbite, immersion foot and trenchfoot, which occur in localized areas of the body. A serious consequence of cold stress is hypothermia. The respiratory system, the circulatory system and the osteoarticular system can also be affected by overexposure to the cold.
To prevent the consequences of cold stress and reduce the hazards of cold working conditions, workers should wear appropriate clothing, and the workplace should have proper equipment, administrative controls and engineering controls. Multiple layers of clothing provide better protection than single thick garments. Cooling equipment and air distribution systems should minimize air velocity. Unit coolers should be placed as far away from workers as possible, and wind deflectors and barriers should be used to protect workers from windchill.
Environmental Protection and Public Health Issues
Overview
The food industry is directly dependent on the natural environment for a supply of raw materials to produce contaminant-free products for human consumption. Due to the extensive processing of a great volume of materials, potential impact on the environment is considerable. This is also true of the beverage industry.
Environmental concern with respect to the food industry focuses more on organic pollutant loadings than on the impact of toxic substances. If pollutant loadings are inadequately prevented or controlled, they will strain community pollution control infrastructure or produce negative impacts on local ecosystems. Production techniques that control product losses serve the double function of improving yield and efficiency while at the same time reducing potential waste and pollution problems.
While the availability of potable water is essential, the food-processing industry also requires very large volumes of water for a wide variety of non-consumption uses, such as for initial cleaning of raw material, fluming, blanching, pasteurizing, cleaning of processing equipment and cooling of finished product. Water uses are identified by quality criteria for different applications, with the highest quality uses often requiring separate treatment to assure complete freedom from odour and taste and to ensure uniform conditions.
The processing of very large volumes of material introduces a potentially great solid waste problem in the production phase. Packaging waste has been the subject of increasing concern with regard to the post-consumer phase of a product’s life cycle. In certain branches of the food industry, processing activities are also associated with potential air emissions and odour control problems.
Despite considerable variation among specific industry sub-sectors, approaches to the prevention and control of pollution share many general characteristics.
Water Pollution Control
The food-processing industry has a raw waste effluent before treatment that is extremely high in soluble organic matter. Even small, seasonal plants are likely to have waste loads comparable to those of populations of 15,000 to 25,000, with large plants approximating the population-equivalent waste load of a quarter of a million people. If a stream or waterway receiving effluent is too small and organic waste too large in volume, the organic waste will utilize the dissolved oxygen in the process of being stabilized and will pollute or degrade the water body by reducing the dissolved oxygen value below that required by normal aquatic organisms. In most cases the waste from food-processing plants is amenable to biological treatment.
The strength of wastewater varies considerably according to plant, specific process and raw product characteristics. From an economic point of view, it is normally less costly to treat a high-strength, low-volume waste than a large-volume, diluted waste. For this reason, effluent with a high biological oxygen demand (BOD), such as the blood of chickens or meat, should be kept out of poultry and meatpacking plant sewers to reduce pollution load, and retained in containers for separate disposal in a by-products or rendering plant.
Waste streams with extreme pH (acidity) values should be carefully considered because of their effect on biological treatment. The combination of acid and basic waste streams may result in neutralization, and, where possible, cooperation with adjacent industries may be very beneficial.
The liquid portion of food-processing waste is normally screened or separated after settling, as a preliminary step in any treatment process, so that these wastes can be disposed of as garbage or combined with other solids in a by-products recovery programme.
The treatment of wastewater can be accomplished by a variety of physical, chemical and biological methods. As secondary processes are more expensive, maximum use of primary treatment is critical in reducing loads. Primary treatment includes processes such as settling or plain sedimentation, filtration (single, dual and multi-media), flocculation, flotation, centrifugation ion exchange, reverse osmosis, carbon absorption and chemical precipitation. Settling facilities range from simple settling ponds to sophisticated clarifiers designed specifically for the particular waste stream characteristics.
The use of biological secondary treatment to follow primary treatment is frequently a necessity to reach wastewater effluent standards. As most food and beverage industry wastewaters contain mainly biodegradable organic pollutants, biological processes used as secondary treatment seek to reduce the BOD of the waste stream by mixing higher concentrations of organisms and oxygen in the waste stream to provide rapid oxidation and stabilization of the waste stream prior to their discharge back to the environment.
Techniques and combinations of techniques may be adapted to address specific waste situations. For example, for dairy wastes, anaerobic treatment to remove the major portion of the pollutant load, with aerobic post-treatment to further reduce the residual BOD and chemical oxygen demand (COD) down to low values and remove nutrients biologically, has proven to be effective. The biogas mixture of methane (CH4) and CO2 that is produced from anaerobic treatment can be captured and used as an alternative to fossil fuels or as a source for electrical power generation (typically 0.30 m3 biogas per kg of COD removed).
Other secondary methods that are widely used include the activated sludge process, aerobic trickling filters, spray irrigation and the use of a variety of ponds and lagoons. Odour nuisances have been associated with ponds of inadequate depth. Odours from anaerobic processes can be removed by the use of soil filters that can oxidize objectionable polar gases.
Air Pollution Control
Air pollution from the food industry generally revolves around the question of objectionable odours rather than toxic air emissions, with a few exceptions. For this reason, for example, many cities have regulated the location of slaughterhouses under their health codes. Isolation is one obvious way to reduce community complaints about odours. However, this does not remove the odour. Odour control measures such as absorbers or scrubbers may sometimes be necessary.
One major health concern in the food industries is leaks of ammonia gas from refrigeration units. Ammonia is a severe eye and respiratory irritant, and a major leak into the environment could require evacuation of local residents. A leak control plan and emergency procedures are necessary.
Food processes that use solvents (e.g., edible oil processing) may emit solvent vapours into the atmosphere. Closed systems and recycling of solvents is the best method of control. Industries such as sugar-cane refining, which use sulphuric acid and other acids, may release sulphur oxides and other contaminants into the atmosphere. Controls such as scrubbers should be used.
Solid Waste Management
Solid waste can be quite considerable. Tomato waste for canning, for example, may represent 15 to 30% of total quantity of product processed; with peas and corn, waste is in excess of 75%. By isolating solid wastes, the concentration of soluble organics in wastewater may be reduced and the drier solid wastes may be more easily used for by-product or feeding purposes and as fuel.
Utilization of process by-products in a manner that provides income will reduce the total cost of waste treatment and eventually the cost of the final product. Waste solids should be evaluated as sources of food for plants and animals. A growing emphasis has been devoted to the development of markets for by-products or for the compost produced by converting waste organic materials to an innocuous humus. Table 1 provides examples of uses for by-products from the food industry.
Table 1. Examples of uses for by-products from the food industry
|
Method |
Examples |
|
Anaerobic digestion |
Digestion by mixed bacteria population to yield methane and CO2 |
|
Animal feed |
Directly, after pressing or drying, as fodder ensiling or as supplement |
|
Composting |
Natural microbiological process in which organic components decompose under controlled aerobic conditions |
|
Edible fibre |
Method for utilizing organic solids by filtering and hydration |
|
Fermentation |
Combination of starch, sugar and alcohol-bearing substances |
|
Incineration |
Burning of biomass as fuel |
|
Pyrolysis |
Transformation of nut shells and fruit pits into charcoal briquets |
|
Soil amendment |
Fertilizing of soils with low nutrient and organic matter content |
Source: Adapted from Merlo and Rose 1992.
Water Reuse and Effluent Reduction
Extensive dependence on water by food-processing industries has encouraged the development of conservation and reuse programmes, especially in locations of water scarcity. Reuse of process water can provide substantial reductions in both water consumption and waste load, with reuse in many lower-quality applications not requiring biological treatment. However, any potential for anaerobic fermentation of organic solids must be avoided so that corrosive, odourous decomposition products do not affect equipment, work environment or product quality. Bacterial growth can be controlled by disinfection and by changing environmental factors such as pH and temperature.
Table 2 presents typical water reuse ratios. Factors such as the location of sprays, water temperature and pressure are key factors influencing the volume of water required for processing operations. For example, water used as a cooling medium to cool cans and for air conditioning may later be used for primary washing of vegetables and other products. The same water later may be used for fluming waste material, and finally a portion of it may be used to cool ashes in the powerhouse.
Table 2. Typical water reuse ratios for different industry sub-sectors
|
Sub-sectors |
Reuse ratios |
|
Beet sugar |
1.48 |
|
Cane sugar |
1.26 |
|
Corn and wheat milling |
1.22 |
|
Distilling |
1.51 |
|
Food processing |
1.19 |
|
Meat |
4.03 |
|
Poultry processing |
7.56 |
Water conservation techniques and waste prevention techniques include the use of high-pressure sprays for clean-up, elimination of excessive overflow from washing and soaking tanks, substitution of mechanical conveyors for water flumes, use of automatic shut-off valves on water hoses, separation of can cooling water from the composite waste flow and recirculation of can cooling water.
Pollution loads at processing plants can be reduced through modified processing methods. For example, most pollution load generated from fruit and vegetable processing originates in the peeling and blanching operations. By moving from conventional water or steam blanching to a hot gas blanching process, pollution loads can be reduced by as much as 99.9%. Similarly, dry caustic peeling can cut BOD by more than 90% in comparison to conventional peeling processes.
Energy Conservation
Energy needs have risen with the increased sophistication of the food industry. Energy is required for a wide a variety of equipment such as gas-fired ovens; dryers; steam boilers; electrical motors; refrigeration units; and heating, ventilation and air-conditioning systems.
As the cost of energy has risen, there has been a trend to install heat recovery equipment to conserve energy and to investigate the feasibility of alternative energy sources in various food-processing situations such as cheese processing, food dehydration and water heating. Energy conservation, waste minimization and water conservation are all mutually supportive strategies.
Consumer Health Issues
The increasing separation of the consumer from the food- production sector that has accompanied urbanization globally has resulted in a loss of the traditional means used by the consumer to ensure the quality and safety of food, making the consumer dependent on a functional and responsible food-processing industry. Increased dependence on food processing has created the possibility of exposure to pathogen-contaminated food from a single production facility. To provide protection from this threat, extensive regulatory structures have been established, especially in the industrialized countries, to protect public health and to regulate the use of additives and other chemicals. Harmonization of regulations and standards across borders is emerging as an issue to ensure the free flow of food among all the world’s countries.
Dairy industry wastewater treatment
The dairy industry is made up of a large number of relatively small plants supplying products such as milk, cheese, cottage cheese, sour cream, ice cream, whey solids and lactose.
The dairy industry has long been a proponent of aerobic biological wastewater treatment. Many dairy plants have invested heavily in activated sludge, biotower, sequencing batch reactor and package treatment systems. Interest in water and energy conservation has led many dairy facilities to reduce water consumption. This trend, with the presence of normally high-strength wastewater streams in dairy plants, has resulted in the design and construction of numerous anaerobic wastewater treatment systems.
Health Effects and Disease Patterns
Health effects found in food processing are similar to those found in other manufacturing operations. Respiratory disorders, skin diseases and contact allergies, hearing impairment and musculoskeletal disorders are among the most common occupational health problems in the food and beverage industry (Tomoda 1993; BLS 1991; Caisse nationale d’assurance maladie des travailleurs salariés 1990). Thermal extremes are also a concern. Table 1 shows rankings of the three most common occupational diseases in this industry in selected countries.
Table 1. Most common occupational diseases in the food and drink industries in selected countries
|
Country |
Year |
Occupational diseases |
|||
|
Most common |
Second most common |
Third most common |
Other |
||
|
Austria |
1989 |
Bronchitis, asthma |
Hearing impairment |
Skin diseases |
Infections transmitted by animals |
|
Belgium (food) |
1988 |
Diseases induced by inhalation of substances |
Diseases induced by physical agents |
Skin diseases |
Infections or parasites from animals |
|
Belgium (drink) |
1988 |
Diseases induced by physical agents |
Diseases induced by chemical agents |
Diseases induced by inhalation of substances |
– |
|
Colombia |
1989 |
Hearing impairment |
Respiratory disorders (asthma) |
Musculoskeletal disorders |
Skin diseases |
|
Czechoslovakia |
1988 |
Respiratory disorders |
Musculoskeletal disorders |
Digestive disorders |
Circulatory disorders, skin diseases |
|
Denmark |
1988 |
Physical coordination disorders |
Skin diseases |
Hearing impairment |
Infections, allergies |
|
France |
1988 |
Asthma and other respiratory disorders |
Strains in various parts of body (knees, elbows) |
Septicemia (blood poisoning) and other infections |
Hearing impairment |
|
Poland |
1989 |
Respiratory disorders |
Skin diseases |
Infections |
Hearing impairment |
|
Sweden |
1989 |
Musculoskeletal disorders |
Allergies (contact with chemical agents) |
Hearing impairment |
Infections |
|
United States |
1989 |
Disorders associated with repeated trauma |
Skin diseases |
Diseases due to physical agents |
Respiratory conditions associated with toxic agents |
Source: Tomoda 1993.
Respiratory System
Respiratory problems can largely be classified as rhinitis, which affects the nasal passages; broncho-constriction in the major airways; and pneumonitis, which consists of damage to the fine structures of the lung. Exposure to airborne dust from various foodstuffs, as well as chemicals, may lead to emphysema and asthma. A Finnish study found chronic rhinitis common among slaughterhouse and pre-cooked foods workers (30%), mill and bakery workers (26%) and food processing workers (23%). Also, food processing workers (14%) and slaughterhouse/pre-cooked foods workers (11%) suffered from chronic coughs. The causative agent is flour dust in bakery workers, while temperature variations and various kinds of dust (spices) are believed to cause disease in other branches.
Two studies in the former Yugoslavia found a much higher prevalence of chronic respiratory symptoms than in a control group. In a study of spice workers the most common complaint (57.6%) was dyspnea or breathing difficulty, followed by nasal catarrh (37.0%), sinusitis (27.2%), chronic cough (22.8%) and chronic phlegm and bronchitis (19.6%). A study of animal food processing workers found that in addition to the animal food processing ingredients, exposure included powdered coriander, garlic dust, cinnamon dust, red paprika dust and dust from other spices. Non-smokers studied showed a significantly higher prevalence of chronic phlegm and chest tightness. Smokers had a significantly higher prevalence of chronic coughs; chronic phlegm, chronic bronchitis and chest tightness were also observed. The frequency of acute respiratory symptoms associated with the working day was high for the exposed group, and respiratory ventilatory capacity of smokers was significantly lower than predicted. The study therefore concluded an association exists between exposure to animal food dust and the development of respiratory disorders.
Industrial injury compensation in the United Kingdom recognizes occupational asthma from the handling of enzymes, animals, grains and flour. Exposure to cinnamic aldehyde from tree bark and sulphur dioxide, a bleaching agent and fumigant, cause a high prevalence of asthma in cinnamon workers in Sri Lanka. Dust exposure is minimal for the workers who peel the bark, but workers in the local buyers’ stores are exposed to high levels of dust and sulphur dioxide. A study found 35 of 40 cinnamon workers complained of chronic coughs (37.5%) or suffered from asthma (22.5%). Other abnormalities included weight loss (65%), skin irritation (50%), hair loss (37.5%), eye irritation (22.5%) and rashes (12.5%). For workers who work under similar high concentrations of airborne dust of vegetable origin, asthma is highest in cinnamon workers (22.5%, compared with 6.4% in tea workers and 2.5% in kapok workers). Smoking is not believed to be directly related to the coughs, since similar symptoms occurred in 8 non-smoking women and 5 men who smoked about 7 cigarettes a day. Irritation of the respiratory mucosa by cinnamon dust causes the coughing.
Other studies examined the relationship between respiratory disorders and the allergens and antigens originating in foodstuffs, such as egg protein and seafood products. While no specific workplace dust could be linked to the various acute and chronic respiratory disorders among the exposed workers, the results of the studies indicate a strong association between the disorders and the work environment.
Use of microbiology has long been a part of food production. In general, most of the micro-organisms used in the food and drink industries are considered to be harmless. Wine, cheese, yogurt and sour dough all use a microbial process to yield a usable product. Production of proteins and enzymes increasingly use biotechnological techniques. Certain species of aspergillus and bacillus produce amylases that convert starches into sugar. Yeasts turn starch into acetone. Tricoderma and Penicillium produce cellulases that break down cellulose. As a result, spores of fungi and actinomycetes are widely found in food processing. Aspergillus and Penicillium are frequently present in the air in bakeries. Penicillium is also found in dairy and meat processing plants; during the maturation of cheeses and sausages, there can be abundant surface growth. Cleaning steps, prior to sale, disperse them into the air, and workers may develop allergic alveolitis. Occupational asthma cases have association with many of these organisms, while some are suspected of causing infection or carrying mycotoxins. The enzymes trypsin, chymotrypsin and protease are associated with hypersensitivity and respiratory disease, particularly among laboratory workers.
In addition to the airborne particulate originating from foodstuffs and microbial agents, inhalation of hazardous chemical substances used as reagents, refrigerants, fumigants and sanitizers may cause respiratory and other disorders. These substances are found in solid, liquid or gaseous form. Exposure at or above recognized limits often results in skin or eye irritation and respiratory disorders. Headaches, salivation, burning of the throat, perspiration, nausea and vomiting are symptoms of intoxication due to overexposure.
Ammonia is a colourless gas refrigerant, cleaning agent and fumigant for foodstuffs. Exposure to ammonia can result in corrosive burns or blistering of skin. Excessive and prolonged exposure can produce bronchitis and pneumonia.
Trichloroethylene, hexane, benzene, carbon monoxide (CO), carbon dioxide (CO2) and polyvinyl chloride (PVC) are frequently found in food and beverage plants. Trichloroethylene and hexane are used for olive oil extraction.
CO, a colourless, odourless gas, is difficult to detect. Exposure occurs in smokehouses that are poorly ventilated or while working in grain silos, wine fermentation cellars or where fish are stored. Dry-ice freezing or chilling, CO2-freeze tunnels and combustion processes expose workers to CO2. Intoxication symptoms of overexposure to CO and CO2 include headache, dizziness, drowsiness, nausea, vomiting and, in extreme cases, even death. CO also can aggravate heart and respiratory symptoms. The acceptable exposure limits, set by several governments, permit 100 times greater exposure to CO2 than CO to trigger the same response.
PVC is used for packaging and food-wrap materials. When PVC film is heated, thermal degradation products cause irritation to the eyes, nose and throat. Workers also report symptoms of wheezing, chest pains, breathing difficulties, nausea, muscle pains, chills and fever.
Hypochlorites, acids (phosphoric, nitric and sulphuric), caustics and quaternary ammonium compounds are frequently used in wet cleaning. Microbiology labs use mercury compounds and formaldehyde (gas and formalin solution). Disinfection in the lab uses phenolics, hypochlorites and glutaraldehyde. Irritation and corrosion to eyes, skin and lungs occur with excessive exposure and contact. Improper handling can release highly toxic substances, like chlorine and sulphur oxides.
The National Institute for Occupational Safety and Health (NIOSH) in the United States reported worker breathing difficulties during washing of poultry with super-chlorinated water. The symptoms included headaches, sore throat, tightness in the chest and difficulty breathing. Chloramine is the suspected agent. Chloromines can form when ammonia-treated water or amine-treated boiler water contacts hypochlorite solutions used in sanitation. Cities have added ammonia to water to prevent the formation of halomethanes. Air sample methods are not available for chloramines. Chlorine and ammonia levels are not predictive as indicators of exposure, as testing found their levels to be well below their limits.
Fumigants prevent infestation during storage and transport of food raw materials. Some fumigants include anhydrous ammonia, phostoxin (phosphine) and methyl bromide. The short duration of this process makes respiratory protection the cost-effective strategy. Proper respiratory protection practices should be observed when handling these items until air measurements of the area are below applicable limits.
Employers should take steps to assess the level of toxic contamination at the workplace and ensure that exposure levels do not exceed limits found in safety and health codes. Contamination levels should be measured frequently, especially following changes in processing methods or the chemicals used.
Engineering controls to minimize the risk of intoxication or infection have two approaches. First, eliminate the use of such materials or substitute a less hazardous material. This may involve replacing a powdered substance with a liquid or slurry. Second, control the exposure through reducing the level of air contamination. Workplace designs include the following: total or partial enclosure of the process, suitable ventilation systems and restricted access (to reduce exposed population). An appropriate ventilation system is instrumental in preventing the dispersal of spores or aerosols throughout the workplace. Substitution of vacuum cleaning or wet cleaning for compressed-air blow-out of equipment is critical for dry materials that could become airborne during cleaning.
Administrative controls include worker rotation (to reduce exposure period) and off-shift/weekend hazardous task work (to reduce exposed population). Personal protective equipment (PPE) is the least favoured exposure control method due to high maintenance, availability issues in developing countries and the fact that the worker must remember to wear it.
PPE consists of splash goggles, face shields and respirators for workers mixing hazardous chemicals. Worker training on use and limitations, plus equipment fitting, must occur for the equipment to adequately serve its purpose. Different types of respirators (masks) are worn depending on the nature of the work and the level of the hazard. These respirators range from the simple half facepiece for dust and mist, through chemical air purifying of various facepiece types, up to self-contained breathing apparatus (SCBA). Proper selection (based on hazard, face-fit and maintenance) and training assure effectiveness of the respirator in reducing exposure and the incidence of respiratory disorders.
Skin
Skin problems found in the food and drink industries are skin disease (dermatitis) and contact allergies (e.g., eczema). Due to sanitation requirements, workers are constantly washing their hands with soap and using hand-dip stations that contain quaternary ammonium solutions. This constant wetting of the hands can reduce the lipid content of the skin and lead to dermatitis. Dermatitis is an inflammation of the skin as a result of contact-exposure to chemicals and food additives. Work with fats and oils can clog the pores of the skin and lead to acne-like symptoms. These primary irritants account for 80% of all occupational dermatitis seen.
There is growing concern that workers may become highly sensitized to microbial proteins and peptides generated by fermentation and extraction, which can lead to eczema and other allergies. An allergy is a hypersensitive response of any type that is greater than that which normally occurs in response to antigens (not-self) in the environment. Allergic contact dermatitis is rarely seen before the fifth or seventh day after exposure is initiated. Hypersensitivity occupational dermatitis is also reported for work with enzymes, such as trypsin, chymotrypsin and protease.
Chlorinated solvents (see “Respiratory system” section above) stimulate the epidermal cells to undertake peculiar growth patterns. This keratin stimulation may lead to tumour formation. Other chlorinated compounds found in soaps for antibacterial purposes can lead to photosensitivity dermatitis.
Reduction of exposure to causative agents is the principle preventive method for dermatitis and contact allergies. Adequately drying foodstuffs prior to storage and clean-condition storage can control airborne spores. PPE such as gloves, masks and uniforms keep workers from direct contact and minimize the risk of dermatitis and other allergies. Latex glove materials can cause allergic skin reactions and should be avoided. Proper application of barrier creams, where permitted, can also minimize contact with the skin irritant.
Infectious and parasitic diseases of animal origin are the occupational diseases most specific to the food and drink industries. The diseases are most common among meat-packing and dairy workers as a result of direct contact with infected animals. Agricultural workers and others are also at risk due to their contact with these animals. Prevention is particularly difficult since the animals may not give any overt signs of disease. Table 2 lists the types of infections reported.
Table 2. Types of infections reported in food and drink industries
|
Infections |
Exposure |
Symptoms |
|
Brucellosis (Brucella melitensis) |
Contact with infected cattle, goats and sheep (Northern and Central Europe and North America) |
Constant and recurring fever, headaches, weakness, joint pain, night sweats and loss of appetite; can also give rise to symptoms of arthritis, influenza, asthenia and spondylitis |
|
Erysipeloid |
Contact of open wounds with infected pigs and fish (Czechoslovakia) |
Localized redness, irritation, a burning sensation, pain in the infected area. It can spread to the bloodstream and lymph nodes. |
|
Leptospirosis |
Direct contact with infected animals or their urine |
Headaches, aching muscles, eye infections, fever, vomiting and chills; in more serious cases, kidney and liver damage, plus cardiovascular and neurological complications |
|
Epidermycosis |
Caused by a parasitic fungus on the skin of animals |
Erythema and blistering of skin |
|
Dematophytosis (ringworm) |
Fungal disease through contact with skin and hair of infected animals |
Localized hair loss and small crusts on the scalp |
|
Toxoplasmosis |
Contact with infected sheep, goats, cattle, pigs and poultry |
Acute stage: fever, muscle pain, sore throats, headaches, swollen lymph nodes and enlarged spleen. Chronic infection leads to development of cysts in the brain and muscle cells. Foetal transmission causes still- and premature births. Full-term babies can have brain and heart defects and may die. |
|
Papilloma viral lung cancers |
Regular contact with live animals or animal flesh coupled with exposure to polycyclic aromatic hydrocarbons and nitrites |
Lung cancers in butchers and slaughterhouse workers studied in England, Wales, Denmark and Sweden |
The fundamental principle for preventing the contraction and spread of infectious and parasitic skin diseases is personal hygiene. Clean washrooms, toilets and shower facilities should be provided. Uniforms, PPE and hand towels need to be washed and in some cases sterilized frequently. All wounds should be sterilized and dressed, regardless of how slight, and covered with protective gear until healed. Keeping the workplace clean and healthy is just as important. This includes the thorough washing of all equipment and surfaces that contact animal flesh after each workday, the control and extermination of rodents and the exclusion of dogs, cats and other animals from the workplace.
Vaccination of animals and inoculation of workers are measures many countries take to prevent infectious and parasitic diseases. Early detection and treatment of diseases with antibacterial/anti-parasitic drugs is essential to contain and even eradicate them. Workers should be examined as soon as any symptoms, such as recurring coughs, fever, headaches, sore throats and intestinal disorders, appear. In any case, workers should undergo medical examinations at established frequencies, including pre-placement/post-offer baseline exams. In some countries, authorities must be notified when examination detects work-related infection in the workers.
Noise and Hearing
Hearing impairment occurs as a result of continuous and prolonged exposure to noise above recognized threshold levels. This impairment is an incurable illness causing communication disorders and is stressful if the work demands concentration. As a result, psychological and physiological performance can deteriorate. There is also an association between high noise level exposure and abnormal blood pressure, heartbeat, respiration rate/volume, stomach and intestinal spasms and nervous disorders. Individual susceptibility, exposure duration and noise frequency plus intensity are factors that determine the exposure risk.
Safety and health codes vary from country to country, but worker exposure to noise is usually limited to 85 to 90 dBA for 8 continuous hours, followed by a 16-hour recovery time below 80 dBA. Ear protection should be made available at 85 dBA and is required for workers with a confirmed loss and for 8-hour exposures at or above 90 dBA. Annual audiometric testing is recommended, and in some countries required, for this exposed population. Noise measurements with a meter such as the American National Standards Institute (ANSI) Type II sound meter should be taken at least every 2 years. Readings should be repeated whenever equipment or process changes could increase the ambient noise levels.
Ensuring that noise exposure levels are not hazardous is the primary strategy for noise controls. Good manufacturing practices (GMPs) dictate that control devices and their exposed surfaces be cleanable, do not harbour pests and have necessary approvals to contact food or be ancillary to food production. The methods adopted also depend on the availability of financial resources, equipment, materials and trained staff. One of the most important factors in noise reduction is the design of the workplace. Equipment should be designed for low noise and low vibration. Replacing metal parts with softer materials, like rubber, can reduce noise.
When new or replacement equipment is purchased a low-noise type should be selected. Silencers should be installed at air valves and exhaust pipes. Noise-producing machines and processes should be enclosed to reduce to a minimum the number of workers exposed to high noise levels. Where permitted, noise-proof partitions and noise-absorbing ceilings should be installed. Removal and cleaning of these partitions and ceiling tiles need to be included in the maintenance costs. The optimum solution is usually a combination of these measures, adapted to the needs of each workplace.
When engineering controls are not feasible or when it is impossible to reduce noise below harmful levels, PPE should be used to protect the ears. Protective equipment availability and worker awareness is important to prevent hearing impairment. In general, a selection of plugs and earmuffs will lead to greater acceptance and wearing.
Musculoskeletal System
Musculoskeletal disorders were also reported in the 1988–89 data (see table 1]). Data in the early 1990s noted more and more workers reporting occupational musculoskeletal disorders. Plant automation and work whose pacing is regulated by a machine or conveyor belt occurs today for more workers in the food industry than ever before. Tasks in automated plants tend to be monotonous, with workers performing the same movement all day long.
A Finnish study found that nearly 40% of survey participants reported performing repetitive work all day. Of those performing repetitive work, 60% used their hands, 37% used more than one part of the body and 3% used their feet. Workers in the following occupational groups perform repetitive work for two-thirds or more of their working hours: 70% of cleaners; 67% of slaughterhouse, pre-cooked food and packaging workers; 56% of warehouse and transport workers; and 54% of dairy workers.
Ergonomic stresses arise because most food products come from natural sources and are not uniform. Meat handling requires workers to handle carcasses of varying sizes. With the introduction of poultry sold in parts in the 1960s, more birds (40%, up from less than 20%) were cut into parts. Workers must make many cuts using sharp tools. Changes in US Department of Agriculture (USDA) inspection procedures now permit average line speeds to increase from 56 to 90 birds per minute. Packaging operations may involve repetitive hand and wrist motions to place finished items undamaged into trays or packs. This is especially true for new products, as the market may not justify high-volume operations. Special promotions, including recipes and coupons, may require that an item be manually inserted into the package. Ingredient packaging and workplace layout may require lifting beyond the action limits recommended by occupational health agencies.
Repetitive strain injuries (RSIs) include inflammation of the tendon (tendinitis) and inflammation of the tendon sheath (tenosynovitis). These are prevalent among workers whose jobs require repetitive hand movements, like meatpacking workers. Tasks that repeatedly combine the bending of the wrist with gripping, squeezing and twisting motion can cause carpal tunnel syndrome (CTS). CTS, characterized by a tingling sensation in the thumb and first three index fingers, is caused by inflammation in the wrist joint creating pressure on the nerve system in the wrist. Misdiagnosis of CTS as arthritis can result in permanent numbness and severe pain in the hands, elbows and shoulders.
Vibration disorders also accompany an increased level of mechanization. Food workers are no exception, although the problem may not be as serious as for certain other industries. Food workers using machines such as band saws, mixers and cutters are exposed to vibration. Cold temperatures also increase the probability of vibration disorders to the fingers of the hand. Five per cent of the participants in the Finnish study noted above were exposed to a fairly high level of vibration, while 9% were exposed to some level of vibration.
Excessive exposure to vibration leads, among other problems, to musculoskeletal disorders in the wrists, elbows and shoulders. The type and degree of disorder depend on the type of machine, how it is used and the level of oscillation involved. High levels of exposure can result in growth of a protuberance on the bone or the gradual destruction of the bone in the joint, resulting in severe pain and/or limited mobility.
Rotation of workers with a view to avoiding repetitive motions may reduce the risk by sharing the critical task across the team. Teamwork by task rotation or two-person handling of awkward/heavy ingredient bags can reduce the stress on a single worker in material handling. Tool maintenance, especially knife sharpening, also plays an important role. An ergonomic team of management and production workers can best address these issues as they arise.
Engineering controls focus on reduction or elimination of the 3 primary causes of musculoskeletal problems—force, position and repetition. The workplace should be analysed to identify needed changes, including workstation design (favouring adjustability), working methods, task automation/mechanical assists and ergonomically sound hand tools.
Adequate training should be provided to workers using knives on keeping the knife sharp to minimize force. Also, plants must provide adequate knife-sharpening facilities and avoid the cutting of frozen meat. Training encourages workers to understand the cause and prevention of musculoskeletal disorders. It reinforces the need to use correctly the tools and machines specified for the task. It should also encourage workers to report medical symptoms as soon as possible. Elimination of more invasive medical intervention by restriction of duties and other conservative care, is effective treatment of these disorders.
Heat and Cold
Thermal extremes exist in the food work area. People must work in freezers with temperatures of –18 °C or below. Freezer clothing helps insulate the worker from the cold, but warm break rooms with access to warm liquids must be provided. Meat-processing plants must be kept at 7 to 10 °C. This is below the comfort zone and workers may need to wear additional clothing layers.
Ovens and steam cookers have radiant and moist heat. Heat stress can occur during season changes and heat waves. Copious amounts of fluids and salting of foods may relieve the symptoms until the worker can acclimatize, usually after 5 to 10 days. Salt tablets are not recommended due to complications of hypertension or gastrointestinal upset.
Food Industry Processes
This article is adapted from the 3rd edition “Encyclopaedia of Occupational Health” articles “Food industries”, by M Malagié; “Frozen food industry”, by G. Jenson; and “Canning and food preserving”, by J.C. Graham, which were revised by Donald L. Smith.
The term food industries covers a series of industrial activities directed at the processing, conversion, preparation, preservation and packaging of foodstuffs (see table 1). The raw materials used are generally of vegetable or animal origin and produced by agriculture, farming, breeding and fishing. This article provides an overview of the complex of food industries. Other articles in this chapter and Encyclopaedia deal with particular food industry sectors and particular hazards.
Table 1. The food industries, their raw materials and processes
|
Industry |
Materials processed |
Storage requirements |
Processing techniques |
Preserving techniques |
Packaging of finished products |
|
Meat processing and preserving |
Beef, lamb, pork, poultry |
Cold stores |
Slaughtering, cutting up, boning, comminuting, cooking |
Salting, smoking, refrigeration, deep-freezing, sterilization |
Loose or in cans, cardboard |
|
Fish processing |
All types of fish |
Cold stores or salted loose or in barrels |
Heading, gutting, filleting, cooking |
Deep-freezing, drying, smoking, sterilization |
Loose in refrigerated containers or in cans |
|
Fruit and vegetable preserving |
Fresh fruit and vegetables |
Processed immediately; fruits may be stabilized with sulphur dioxide |
Blanching or cooking, grinding, vacuum- concentration of juices |
Sterilization, pasteurization, drying, dehydration, lyophilization (freeze drying) |
Bags, cans or glass or plastic bottles |
|
Milling |
Grains |
Silos may be fumigated in storage |
Grinding, sifting, milling, rolling |
Drying cooking or baking |
Silos (conveyed pneumatically), sacks or bags to other processes, or boxed for retail trade |
|
Baking |
Flour and other dry goods, water, oils |
Silos, super sacks and bags |
Kneading, fermentation, laminating surface treatments of seasoning |
Baking, cutting surface treatments and packaging |
Packaged for wholesale trades, restaurants and retail markets |
|
Biscuit making |
Flour, cream, butter, sugar, fruit and seasoning |
Silos, super sacks and bags |
Mixing, kneading, laminating moulding |
Baking, cutting surface treatments and packaging |
Bags, boxes for institutional and retail trades |
|
Pasta manufacture |
Flour, eggs |
Silos |
Kneading, grinding, cutting, extrusion or moulding |
Drying |
Bags, packets |
|
Sugar processing and refining |
Sugar beet, sugar cane |
Silos |
Crushing, maceration, vacuum concentration, centrifuging, drying |
Vacuum cooking |
Bags, packets |
|
Chocolate making and confectionery |
Cocoa bean sugar, fats |
Silos, sacks, conditioned chambers |
Roasting, grinding, mixing, conching, moulding |
– |
Packets |
|
Brewing |
Barley, hops |
Silos, tanks, conditioned cellars |
Grain milling, malting, brewing, filter pressing, fermentation |
Pasteurization |
Bottles, cans, barrels |
|
Distilling and manufacture of other beverages |
Fruit, grain, carbonated water |
Silos, tanks, vats |
Distillation, blending, aeration |
Pasteurization |
Barrels, bottles, cans |
|
Milk and milk products processing |
Milk, sugar, other constituents |
Immediate processing; subsequently in ripening vats, conditioned vats, cold store |
Skimming, churning (butter), coagulation (cheese), ripening |
Pasteurization, sterilization or concentration, desiccation |
Bottles, plastic wrapping, boxes (cheese) or unpacked |
|
Processing of oils and fats |
Groundnuts, olives, dates, other fruit and grain, animal or vegetable fats |
Silos, tanks, cold stores |
Milling, solvent or steam extraction, filter pressing |
Pasteurization where necessary |
Bottles, packets, cans |
The food industry today has become highly diversified, with manufacturing ranging from small, traditional, family-run activities that are highly labour intensive, to large, capital-intensive and highly mechanized industrial processes. Many food industries depend almost entirely on local agriculture or fishing. In the past, this meant seasonal production and hiring of seasonal workers. Improvements in food processing and preservation technologies have taken some of the pressure off workers to process food quickly to prevent spoilage. This has resulted in a decrease in seasonal employment fluctuations. However, certain industries still have seasonal activities, such as fresh fruit and vegetable processing and increases in production of baked goods, chocolate and so forth for holiday seasons. Seasonal workers are often women and foreign workers.
The world’s food product output has been increasing. World exports of food products in 1989 totalled US$290 billion, a 30% increase over 1981. Industrialized market economy countries had a 67% share of this export. Much of this increase can be attributed to an increased demand for processed food and drink, especially in developing countries where the market has not yet been saturated.
This increase in output of food and drink products, however, has not resulted in increased employment because of intensified competition, which has resulted in decreased employment in many food industries, especially in industrialized countries. This is due to increased productivity and mechanization in many of these industries.
Demographic pressure, uneven distribution of agricultural resources and the need to insure preservation of food products to facilitate their better distribution explain the rapid technical evolution in the food industries. Constant economic and marketing pressures drive the industry to provide new and different products for market, while other operations may make the same product in the same way for decades. Even highly industrialized facilities often resort to seemingly archaic techniques when starting new products or processes. In practice, to satisfy population requirements, there is a need not only for a sufficient quantity of foodstuffs, which presupposes an increase of production, but also strict control of sanitation to obtain the quality essential to maintain the health of the community. Only modernization of techniques justified by production volumes in a stable production environment will eliminate manual handling hazards. In spite of the extreme diversity of the food industries, the preparation processes can be divided into handling and storage of raw materials, extraction, processing, preservation and packaging.
Handling and Storage
Manipulation of the raw materials, the ingredients during processing and the finished products is varied and diverse. The current trend is to minimize manual handling by mechanization, through “continuous processing” and automation. Mechanical handling may involve: self-propelled in-plant transport with or without palletization or super or bulk sacks (often containing several thousand pounds of dry powder material); conveyor belts (e.g., with beets, grain and fruit); bucket elevators (e.g., with grain and fish); spiral conveyors (e.g., with confectionery and flour); air fluming (e.g., for unloading grain, sugar or nuts and for transport of flours).
Storage of raw materials is most important in a seasonal industry (e.g., sugar refining, brewing, grain processing and canning). It is usually done in silos, tanks, cellars, bins or cold stores. Storage of the finished products varies according to their nature (liquid or solid), the method of preserving and the method of packaging (loose, in sack or super sack, in bundles, boxes or bottles); and the respective premises must be planned to suit the conditions of handling and preserving (traffic aisles, ease of access, temperature and humidity suited to product, cold-storage installations). Commodities may be held in oxygen-deficient atmospheres or under fumigation while in storage or just before shipment.
Extraction
To extract a specific food product from fruit, cereals or liquids, any of the following methods may be used: crushing, pounding or grinding, extraction by heat (direct or indirect), extraction by solvents, drying and filtration.
Crushing, pounding and grinding are usually preparatory operations—for example, the crushing of cocoa beans and the slicing of sugar beet. In other cases it may be the actual extraction process, as in flour milling.
Heat can be used directly as a means of preparation by extraction, as in roasting (e.g., cocoa, coffee and chicory); in manufacturing it is usually used directly or indirectly in the form of steam (e.g., extraction of edible oils or extraction of sweet juice from thin slices of beet in the sugar industry).
Oils can be extracted equally well by combining and mixing the crushed fruit with solvents that are later eliminated by filtering and reheating. The separation of liquid products is carried out by centrifuging (turbines in a sugar refinery) or by filtering through filter presses in breweries and in oil and fat production.
Production Processes
Operations in processing food products are extremely varied and can be described only after individual study of each industry, but the following general procedures are used: fermentation, cooking, dehydration and distillation.
Fermentation, obtained usually by addition of a micro-organism to the previously prepared product, is practiced in bakeries, breweries, the wine and spirits industry and the cheese products industry. (See also the chapter Beverage industry.)
Cooking occurs in many manufacturing operations: canning and preserving of meat, fish, vegetables and fruits; ready-to-serve meat-processing plants (e.g., chicken nuggets); in bakeries, biscuit making, breweries; and so on. In other cases, cooking is done in a vacuum-sealed container and produces a concentration of the product (e.g., sugar refining and tomato-paste production).
Besides the drying of products by the sun, as with many tropical fruits, dehydration can be carried out in hot air (fixed dryers or drying tunnels), by contact (on a drying drum heated by steam, such as in the instant-coffee industry and the tea industry), vacuum drying (often combined with filtering) and lyophilization (freeze drying), where the product is first frozen solid and then dried by vacuum in a heated chamber.
Distillation is used in the making of spirits. The fermented liquid, treated to separate grain or fruit, is vaporized in a still; the condensed vapour is then collected as liquid ethyl alcohol.
Preservation Processes
It is important to prevent any deterioration of food products, as much for the quality of the products as for the more serious risk of contamination or threat to the consumers’ health.
There are six basic methods of food preservation:
- radiation sterilization
- antibiotic sterilization
- chemical action
- dehydration
- refrigeration.
Briefly, the first three methods destroy microbial life; the latter merely inhibit growth. Raw ingredients such as fish and meat, fruit or vegetables are taken fresh and preserved by one of the above methods, or a mixture of different foods are processed to form a product or dish, which is then preserved. Such products include soups, meat dishes and puddings.
Food preservation goes back to the last Ice Age, about 15,000 BC, when Cro-Magnon humans discovered for the first time a way of preserving food by smoking it. The evidence for this lies in the caves at Les Eyzies in the Dordogne in France, where this way of life is well portrayed in carvings, engravings and paintings. From then to the present day, although many methods have been used and still are, heat remains one of the principal cornerstones of food preservation.
High-temperature processes can destroy bacteria, depending on the cooking temperature and duration. Sterilization (mainly used in canneries) involves submitting the already canned product to the action of steam, generally in a closed container such as an autoclave or continuous cooker. Pasteurization—the term is particularly reserved for liquids such as fruit juice, beer, milk or cream—is carried out at a lower temperature and for a short time. Smoking is carried out mainly on fish, ham and bacon, assuring dehydration and giving a distinctive flavor.
Ionizing radiation sterilization is used heavily on spices in some countries to reduce wastage and spoilage. “Radiation pasteurization” using much lower doses enables the refrigerated shelf life of many foods to be considerably extended. However, sterilizing canned foods with radiation requires such high dosage that unacceptable flavours and odours result.
Ionizing radiation has two other well recognized uses in the food industry—the screening of food packs for foreign matter and monitoring to detect underfilling.
Microwave sterilization is another type of electromagnetic emission that is currently finding use in the food industry. It is used for rapidly thawing raw frozen ingredients before further processing, as well as for heating frozen cooked foods in 2 to 3 minutes. Such a method, with its low moisture content loss, preserves the appearance and flavour of the food.
Drying is a common preservation process. Sun drying is the oldest and most widely used method of food preservation. Today foodstuffs may be dried in air, superheated steam, in vacuum, in inert gas and by direct application of heat. Many types of dryers exist, the particular type being dependent on the nature of the material, the desired form of finished product and so on. Dehydration is a process in which heat is transferred into the water in the food, which is vapourized. The water vapour is then removed.
Low-temperature processes involve storage in a cold store (the temperature determined by the nature of the products), freezing and deep-freezing, which allows foodstuffs to be preserved in their naturally fresh state, by various methods of slow or rapid freezing.
With freeze drying, the material to be dried is frozen and placed in a sealed chamber. The chamber pressure is reduced and maintained at a value below 1 mm Hg. Heat is applied to the material, the surface ice heats up and the resultant water vapour is drawn off by the vacuum system. As the ice boundary recedes into the material, the ice sublimes in situ and the water percolates to the surface through the pore structure of the material.
Intermediate-moisture foods are foodstuffs that contain relatively large amounts of water (5 to 30%) and yet do not support microbial growth. The technology, which is difficult, is a spin-off from space travel. Open-shelf stability is achieved by suitable control of acidity, redox potential, humectants and preservatives. Most developments to date have been in foods for pet animals.
Whatever the preservation process, the food to be preserved has first to be prepared. Meat preservation involves a butchery department; fish needs cleaning and gutting, filleting, curing and so on. Before fruit and vegetables can be preserved they have to be washed, cleaned, blanched, perhaps graded, peeled, stalked, shelled and stoned. Many of the ingredients have to be chopped, sliced, minced or pressed.
Packaging
There are many methods of packaging food, including canning, aseptic packaging and frozen packaging.
Canning
The conventional method of canning is based on the original work of Appert in France, for which in 1810 the French government awarded him a prize of 12,000 francs. He preserved food in glass containers. In Dartford, England, in 1812, Donkin and Hall set up the first cannery using tinned iron containers.
Today the world uses several million tonnes of tinplate annually for the canning industry, and a substantial amount of preserved food is packed into glass jars. The process of canning consists of taking cleaned food, raw or partly cooked but not intentionally sterilized, and packing it into a can that is sealed with a lid. The can is then heated, usually by steam under pressure, to a certain temperature for a period of time to allow penetration of the heat to the centre of the can, destroying the microbial life. The can is then cooled in air or chlorinated water, after which it is labelled and packed.
Changes in processing have occurred over the years. Continuous sterilizers cause less damage to cans by impact and allow cooling and drying in a closed atmosphere. Foods can also be heat preserved in retortable pouches. These are bags of small cross-sectional area made from laminates of aluminium and heat-sealable plastics. The process is the same as for conventional canning, but better taste properties are claimed for the products because sterilization times can be reduced. Very careful control of the retorting process is essential to avoid damage to the heat seals with subsequent bacterial spoilage.
Aseptic packaging
There have been recent developments in the aseptic packaging of food. The process is fundamentally different from conventional canning. In the aseptic method the food container and closure are sterilized separately, and the filling and closing are done in a sterile atmosphere. Product quality is optimal because heat treatment of the foodstuff can be controlled precisely and is independent of the size or material of the container. Of concern is employee exposure to the sterilizing agents. It is likely that the method will become more widely used because overall it should result in energy savings. To date most progress has been made with liquids and purées sterilized by the so-called HTST process, in which the product is heated to a high temperature for a few seconds. Developments on particulate foodstuffs will follow. One likely benefit in food factories will be the reduction of noise if rigid metallic containers are replaced. Such containers may also cause problems by contaminating preserved food with lead and tin. These are minimized by new-type two-piece containers drawn from lacquered tinplate and three-piece containers with welded instead of soldered side seams.
Frozen packaging
The frozen food industry utilizes all methods of deep-freezing fresh food at temperatures below their freezing point, thus forming ice crystals in the watery tissues. The food may be frozen raw or partially cooked (e.g., animal carcasses or made-up meat dishes, fish or fish products, vegetables, fruits, poultry, eggs, ready-made meals, bread and cakes). Frozen perishable products can be transported over long distances and stored for processing and/or sale when demand arises, and seasonal products can be available at all times.
Food for freezing must be in prime condition and prepared under strict hygienic control. Packaging materials should be vapour- and aroma-proof and resistant to low temperatures. The quality of the product depends on the rate of freezing: if too slow, the structure of the food may be damaged by large ice crystals and enzymatic and microbiological properties destroyed. Small items, such as shrimps and peas, can be frozen quickly, which makes for an improvement in quality.
The various methods of freezing include: air freezing, blast freezing, fluid-bed freezing, fluid freezing, contact freezing, liqui-freezing and dehydro-freezing.
Air freezing in its simplest form involves placing food in trays on shelves in a cold store at approximately –30 ºC for a time varying from a few hours to 3 days, depending on size. Blast freezing, a more complicated technique, uses a rapidly circulating stream of cold air, sometimes combined with cold spirals, which removes heat by means of radiation. Temperatures range between –40 and –50 ºC, and the maximum air speed is 5 m/s. Blast freezing may be carried out in tunnel freezers, often equipped with conveyors to carry the food through to cold-storage rooms. When the freezer is adjacent to the cold store, the tunnel is often closed with an air curtain instead of doors.
Fluid-bed freezing is used for chopped or sliced vegetables, peas and so on, which are placed on a perforated belt through which a stream of air is blown. Each item is coated with ice and thus retains its shape and separateness. The frozen vegetables may be stored in large containers and repackaged when needed in small units. In fluid freezing (one of the oldest known methods) the food, usually fish, is immersed in a strong solution of brine. Salt may penetrate unwrapped goods and even wrappings, affecting the flavour and hastening rancidity. This method had declined in use but is now gaining ground again as more effective plastic wrapping materials are developed. Poultry is frozen by a combination of the fluid- and air-freezing methods. Each bird, packed in polyethylene or similar material, is first sprayed or immersed in a fluid to freeze its outer layer; the inside is afterwards frozen in a blast freezer.
Contact freezing is the common method for foodstuffs packed in cartons, which are placed between hollow shelves through which a cooling fluid is circulated; the shelves are pressed flat against the cartons, usually by hydraulic pressure.
In liqui-freezing, the product is placed on a conveyor belt which is passed through a tank of liquid nitrogen (or occasionally liquid carbon dioxide) or through a tunnel where liquid nitrogen is sprayed. Freezing occurs at a temperature as low as –196 ºC, and not every type of product or wrapping can withstand this cold. Dehydro-freezing, which removes some of the water before freezing, is used for certain vegetables and fruits. A considerable reduction of weight is achieved, involving lower transport, storage and wrapping costs.
During cold storage, the product must be kept at a temperature of –25 to –30 ºC, and good air circulation must be maintained. Transport of frozen goods has to be in refrigerated wagons, lorries, ships and so on, and during loading and unloading, the goods must be exposed to as little heat as possible. Usually, firms producing frozen food also prepare the raw material, but sometimes this treatment is carried out in separate establishments. In beef and poultry operations, carbon dioxide is often used to cool and preserve product during shipping.
Hazards and Their Prevention
Injury hazards
The most common causes of injuries in the food industry are hand tools, especially knives; operation of machinery; collisions with moving or stationary objects; falls or slips; and burns.
Injuries caused by knives in meat and fish preparation can be minimized by design and maintenance, adequate work areas, selection of the right knife for the job, provision of tough protective gloves and aprons and correct training of workers on both the sharpening and the use of the knife. Mechanical cutting devices also pose a hazard, and good maintenance and adequate training of workers is critical to prevent injuries (see figure 1).
Figure 1. Carving frozen whale meat on a band saw without adequate machine guarding and electrical precautions, Japan, 1989
L. Manderson
Although accidents involving transmission machinery are relatively infrequent, they are likely to be serious. Risks related to machines and handling systems must be studied individually in each industry. Handling problems can be addressed by close examination of injury history for each particular process and by use of appropriate personal protection, such as foot and leg protection, hand and arm protection and eye and face protection. Risks from machinery can be prevented by secure machinery guarding. Mechanical handling equipment, especially conveyors, is widely employed, and particular attention should be paid to in-running nips on such equipment. Filling and closing machines should be totally enclosed except for the intake and discharge openings. The intakes of conveyor belts and drums, as well as pulleys and gearing, should be securely protected. To prevent cuts in canning, for example, effective arrangements for clearing up sharp tin or broken glass are required. Serious injury due to the inadvertent start-up of transmission machinery during cleaning or maintenance can be avoided by strict lockout/tagout procedures.
Falling accidents are most often caused by:
- The state of the floor. Accidents are possible when floors are uneven, wet or made slippery by the type of surface; by products; by fatty, oily or dusty waste; or, in cold rooms, from humid air condensing on the floors. Anti-slip floors help to prevent slips. Finding the proper surface and cleaning regimen, along with good housekeeping and proper footwear, will help prevent many falls. Curbs around machines containing water will prevent water flowing onto the floor. Good drainage should be provided to remove rapidly any accumulating liquids or spillage that occurs.
- Uncovered pits or drainage channels. Maintenance of covers or barricading of the hazard is necessary.
- Work at heights. Provision of safe means of access to equipment and storage areas, sound ladders and fall protection (including body harnesses and lifelines) can prevent many hazards.
- Steam or dust. Operations that generate steam or dust may not only make the floor slippery but also prevent good visibility.
- Insufficient or inconsistent lighting. Illumination needs to be bright enough for employees to be able to observe the process. The perception of inadequate lighting occurs when warehouses appear dark compared to production areas and people’s eyes do not adjust when moving from one light level to the other.
Burns and scalds from hot liquors and cooking equipment are common; similar injuries arise from steam and hot water used in equipment cleaning. Even more serious accidents can occur due to explosion of boilers or autoclaves due to lack of regular examination, poor employee training, poor procedures or poor maintenance. All steam equipment needs regular and careful maintenance to prevent major explosion or minor leaks.
Electrical installations, especially in wet or damp places, require proper grounding and good maintenance to control the common hazard of electrical shock. In addition to proper grounds, outlets protected with ground fault interrupters (GFIs) are effective in protecting from electrical shock. Proper electrical classification for hazardous environments is critical. Often flavours, extracts and dusty flammable powders such as grain dust, corn starch or sugar (thought of as foodstuffs rather than hazardous chemicals) may require classified electrical equipment to eliminate ignition during process upsets or excursions. Fires may also occur if welding is done around explosive/combustible organic dusts in grain elevators and mills. Explosions may also occur in gas or oil-fired ovens or cooking processes if they are not installed, operated or maintained correctly; provided with the essential safety devices; or if proper safety procedures are not followed (especially in open flame operations).
Strict product sanitation control is vital at all stages of food processing, including in slaughterhouses. Personal and industrial hygiene practices are most important in guarding against infection or contamination of the products. The premises and equipment should be designed to encourage personal hygiene through good, conveniently situated and sanitary washing facilities, showerbaths when necessary, provision and laundering of suitable protective clothing and provision of barrier creams and lotions, where appropriate.
Strict equipment sanitation is also vital to all stages of food processing. During the regular operation of most facilities, safety standards are effective to control equipment hazards. During the sanitation cycle, equipment must be opened up, guards removed and interlock systems disabled. A frustration is that the equipment is designed to run, but clean-up is often an afterthought. A disproportional share of the most serious injuries happen during this part of the process. Injuries are commonly caused by exposure to in-running nip points, hot water, chemicals and acid or base splashes, or by cleaning moving equipment. Dangerous high-pressure hoses which carry hot water also pose a hazard. Lack of equipment-specific procedures, lack of training and the low experience level of the typical new employee pressed into a cleaning job can add to the problem. The hazard is increased when equipment to be cleaned is located in areas that are not easily accessible. An effective lockout/tagout programme is essential. Current best practice to help control the problem is designing of clean-in-place facilities. Some equipment is designed to be self-cleaning by use of high-pressure spray balls and self-scrubbing systems, but too often manual labour is required to address trouble spots. In the meat and poultry industries, for example, all cleaning is manual.
Health hazards
Infections and infectious or parasitic diseases spread by animals or the waste products of animals used in manufacture are common occupational problems in the food industry. These zoonoses include anthrax, brucellosis, the leptospiroses, tularemia, bovine tuberculosis, glanders, erysipeloid, Q fever, foot-and-mouth disease, rabies and so on. Some food handlers may be subject to a wide variety of skin infections, including anthrax, actinomycosis and erysipeloid. Certain dried fruits are infested with mites; this can affect workers in sorting operations.
Apart from specific prophylactic vaccination against infectious diseases, proper gloves, good personal hygiene and the sanitary facilities to enable this (which are a prerequisite of any food industry as a protection to the product) are the most valuable preventive measures. Good washing facilities, including showers, and appropriate protective clothing are essential. Efficient medical care, especially for treatment of minor injuries, is an equally important requirement.
Contact dermatitis and allergies of the skin or respiratory system caused by organic products, animal or vegetable, are also common. Primary dermatitis can be caused by irritants such as acids, alkalis, detergents and water used in cleaning; friction from fruit picking and packing; and the handling of sugar, which is much used in food manufacture. Secondary sensitization results from the handling of many fruits and vegetables. Organic dusts from grain or flour can also cause respiratory diseases (e.g., “baker’s asthma”) and must be controlled. Too often the food industry considers the ingredients they use to be merely ingredients, rather than chemicals that can have health effects when employees are exposed to either industrial strengths or industrial quantities of “normal” household kitchen ingredients.
Cumulative trauma disorders
Many of the meat, poultry, fish and food processing plants involve highly repetitious and forceful work. The very nature of the products is such that manual labour often is needed to manipulate product when inspecting or loading fragile products into packaging or during the scale-up of a product before high-volume equipment is purchased or installed. Further, handling of boxes for shipping can cause back injuries. Three things to watch for are tasks involving extreme postures, high forces or high levels of repetition. Combinations of more than one factor make the problem more critical. Early detection and treatment of affected workers is desirable. Ergonomic redesign of equipment and other changes discussed in specific articles in this chapter will decrease the incidence of these hazards.
Refrigerants such as anhydrous ammonia, methyl chloride and other halogenated aliphatic hydrocarbons used in freezing and cold storage bring risks of poisoning and chemical burns. Emergency planning in addition to the normal fire planning is important. Training of workers in evacuation procedures is also necessary. Escape-type respiratory protection may be needed during evacuation from some areas of the facility. For some chemicals, sensors in the building are used to provide early warning to all employees through a central alarm system to signal the need to evacuate. Worker reactions to increases in ammonia levels must be taken seriously, and affected workers must be evacuated and treated. Ammonia leaks warrant strict attention and contiuous monitoring. Evacuation may be required if levels start to rise, before dangerous levels are reached. A central assembly point should be selected so that those who are evacuated are not in danger of being downwind of the refrigerant leak. Chemical protective clothing will be needed to aggressively approach the system leak to contain the release. Anhydrous ammonia and the less frequently used refrigerants, such as propane, butane, ethane and ethylene, are also flammable and explosive. Leaks from pipes are usually due to inadequate maintenance and can be prevented with adequate attention. Adequate measures should be taken for explosion prevention and firefighting.
Pesticides, fumigants and other hazardous materials must be kept under strict control and used only according to the manufacturer’s guidance. Organophosphate pesticides should only be used when accompanied with biological monitoring to assure the control of exposure.
The traditional tin/lead soldering of the side seam of a food can and the awareness of the problem of lead levels in food products have resulted in studies of environmental lead levels in can-making units and blood lead levels in workers. Evidence has shown both to be raised, but neither the environmental threshold limit value (TLV) nor the currently acceptable blood lead levels have ever been found to be exceeded. Thus, the results are consistent with a “low risk” lead process.
Carbon dioxide, used in cooling refrigerated products that are to be shipped, must also be kept under strict controls. Adequate ventilation must be provided over dry ice bins to prevent the gas from causing ill effects.
Exposure to cold can range from handling and storage of raw materials in winter or in processing and store rooms cooled with “still air”, to extremes of cold in air-blast refrigeration of raw materials, as in the ice cream and frozen foods industry. Cold-store workers may suffer impairment of health through exposure to cold if adequate protective clothing is not supplied. Exposure to cold is most critical for employees with sedentary jobs in very cold environments. Barriers should be used to deflect cold breezes from workers standing near fans used to circulate air. Job rotation to more active or warmer locations is advisable. In large tunnel freezing plants, it may be fatal for workers to stay in the rapidly moving stream of air, even if dressed in polar clothing. It is particularly important to prohibit entry into a tunnel freezer in operation and to make effective interlocking arrangements or use confined-space entry protocol to ensure that freezers cannot be started up while workers are still inside them. Warm lunchrooms and provision of hot drinks will mitigate the effects of cold work.
Heat, often combined with high humidity in cooking and sterilizing, can produce an equally intolerable physical environment, where heat stroke and heat exhaustion are an issue. These conditions are found especially in processing that entails evaporation of solutions, such as tomato paste production, often in countries where hot conditions already prevail. It is also prevalent on kill floors of slaughterhouses. Effective ventilation systems are essential, with special attention to condensation problems. Air conditioning may be necessary in some areas.
A serious health hazard in most modern plants, especially with canning, is exposure to noise. Putting additional high-speed machines in a limited space continues to drive noise levels up, despite best efforts to keep them below 85 dBA. The manufacture, conveying and filling of cans at speeds of up to 1,000 per minute leads to exposure of operators to a noise level of up to 100 dBA at frequencies ranging from 500 to 4,000 Hz, a dose equivalent of about 96 dBA, which if uncontrolled will lead in many cases to noise-induced deafness over a working lifetime. Certain engineering techniques can lead to some noise reduction; these include sound-absorbent mounting, magnetic elevators, nylon-coated cables and speed-matching in can conveyor systems. However, some radical change in the industry, such as the use of plastic containers, is the only hope for the future of producing a reasonably noise-free environment. At present, a hearing conservation programme based on audiometric examinations, hearing-protection equipment and education should be instituted. Noise refuges and personal ear protection should be provided.
Where ionizing radiation is used, the full precautions applicable to such work (e.g., radiation protection, hazard monitoring, health screening and periodic medical examinations) are necessary.
Medical supervision of workers is desirable; many food factories are small and membership in a group medical service may be the most effective way of securing this.
Health and safety committees that effectively involve the entire organization, including production operators, in the development of plant programmes is the key to a safe operation. Too often the food industry is not considered to be particularly hazardous, and a feeling of complacency develops. Often materials used are ones that people are familiar with and hence individuals may not understand the hazards that can arise when industrial strengths or quantities are employed. Plant employees who understand that safety rules and procedures are in place to protect their health and safety and not simply to meet government requirements are key to the development of a quality safety programme. Management must establish practices and policies that will allow employees to develop those beliefs.
Environmental and Public Health Issues
Because the pulp and paper industry is a large consumer of natural resources (i.e., wood, water and energy), it can be a major contributor to water, air and soil pollution problems and has come under a great deal of scrutiny in recent years. This concern appears to be warranted, considering the quantity of water pollutants generated per tonne of pulp (e.g., 55 kg of biological oxygen demand, 70 kg of suspended solids, and up to 8 kg of organochlorine compounds) and the amount of pulp produced globally on an annual basis (approximately 180 million tonnes in 1994). In addition, only about 35% of used paper is recycled, and waste paper is a major contributor to total worldwide solid waste (about 150 million of 500 million tonnes annually).
Historically, pollution control was not considered in the design of pulp and paper mills. Many of the processes used in the industry were developed with little regard for minimizing effluent volume and pollutant concentration. Since the 1970s, pollution abatement technologies have become integral components of mill design in Europe, North America and other parts of the world. Figure 1 illustrates trends over the period 1980 to 1994 in Canadian pulp and paper mills in response to some of these environmental concerns: increased use of wood waste products and recyclable paper as fibre sources; and decreased oxygen demand and chlorinated organics in wastewater.
Figure 1. Environmental indicators in Canadian pulp and paper mills, 1980 to 1994, showing use of wood waste and recyclable paper in production, and biological oxygen demand (BOD) and organochlorine compounds (AOX) in wastewater effluent.
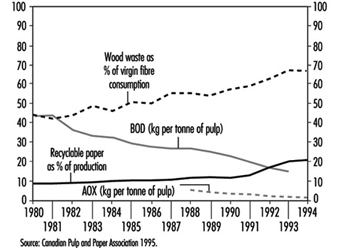
This article discusses the major environmental issues associated with the pulp and paper process, identifies the sources of pollution within the process and briefly describes control technologies, including both external treatment and in-plant modifications. Issues arising from wood waste and anti-sapstain fungicides are dealt with in more detail in the chapter Lumber.
Air Pollution Issues
Air emissions of oxidized sulphur compounds from pulp and paper mills have caused damage to vegetation, and emissions of reduced sulphur compounds have generated complaints about “rotten egg” odours. Studies among residents of pulp mill communities, in particular children, have shown respiratory effects related to particulate emissions, and mucous membrane irritation and headache thought to be related to reduced sulphur compounds. Of the pulping processes, those with the greatest potential to cause air pollution problems are chemical methods, in particular kraft pulping.
Sulphur oxides are emitted at the highest rates from sulphite operations, especially those using calcium or magnesium bases. The major sources include batch digester blows, evaporators and liquor preparation, with washing, screening and recovery operations contributing lesser amounts. Kraft recovery furnaces are also a source of sulphur dioxide, as are power boilers which use high-sulphur coal or oil as fuel.
Reduced sulphur compounds, including hydrogen sulphide, methyl mercaptan, dimethyl sulphide and dimethyl disulphide, are almost exclusively associated with kraft pulping, and give these mills their characteristic odour. The major sources include the recovery furnace, digester blow, digester relief valves, and washer vents, though evaporators, smelt tanks, slakers, the lime kiln and waste water may also contribute. Some sulphite operations use reducing environments in their recovery furnaces and may have associated reduced sulphur odour problems.
Sulphur gases emitted by the recovery boiler are best controlled by reducing emissions at the source. Controls include black liquor oxidation, reduction in liquor sulphidity, low-odour recovery boilers and proper operation of the recovery furnace. Sulphur gases from digester blow, digester relief valves and liquor evaporation can be collected and incinerated - for example, in the lime kiln. Combustion flue gases can be collected using scrubbers.
Nitrogen oxides are produced as products of high-temperature combustion, and may arise in any mill with a recovery boiler, power boiler or lime kiln, depending on the operating conditions. The formation of nitrogen oxides can be controlled by regulating temperatures, air-fuel ratios and residence time in the combustion zone. Other gaseous compounds are minor contributors to mill air pollution (e.g., carbon monoxide from incomplete combustion, chloroform from bleaching operations, and volatile organics from digester relief and liquor evaporation).
Particulates arise mainly from combustion operations, though smelt-dissolving tanks can also be a minor source. More than 50% of pulp mill particulate is very fine (less than 1 μm in diameter). This fine material includes sodium sulphate (Na2SO4) and sodium carbonate (Na2CO3) from recovery furnaces, lime kilns and smelt-dissolving tanks, and NaCl from burning by-products of logs which have been stored in salt water. Lime kiln emissions include a significant amount of coarse particulates due to entrainment of calcium salts and sublimation of sodium compounds. Coarse particulate may also include fly ash and organic combustion products, especially from power boilers. Reduction of particulate concentrations can be achieved by passing flue gases through electrostatic precipitators or scrubbers. Recent innovations in power boiler technology include fluidized bed incinerators which burn at very high temperatures, result in more efficient energy conversion, and allow burning of less uniform wood waste.
Water Pollution Issues
Contaminated wastewater from pulp and paper mills can cause death of aquatic organisms, allow bioaccumulation of toxic compounds in fish, and impair the taste of downstream drinking water. Pulp and paper wastewater effluents are characterized on the basis of physical, chemical or biological characteristics, with the most important being solids content, oxygen demand and toxicity.
The solids content of wastewater is typically classified on the basis of the fraction that is suspended (versus dissolved), the fraction of suspended solids that is settleable, and the fractions of either that are volatile. The settleable fraction is the most objectionable because it may form a dense sludge blanket close to the discharge point, which rapidly depletes dissolved oxygen in the receiving water and allows the proliferation of anaerobic bacteria which generate methane and reduced sulphur gases. Although non-settleable solids are usually diluted by the receiving water and are therefore of less concern, they may transport toxic organic compounds to aquatic organisms. Suspended solids discharged from pulp and paper mills include bark particles, wood fibre, sand, grit from mechanical pulp grinders, papermaking additives, liquor dregs, by-products of water treatment processes and microbial cells from secondary treatment operations.
Wood derivatives dissolved in the pulping liquors, including oligosaccharides, simple sugars, low-molecular-weight lignin derivatives, acetic acid and solubilized cellulose fibres, are the main contributors to both biological oxygen demand (BOD) and chemical oxygen demand (COD). Compounds which are toxic to aquatic organisms include chlorinated organics (AOX; from bleaching, especially kraft pulp); resin acids; unsaturated fatty acids; diterpene alcohols (especially from debarking and mechanical pulping); juvabiones (especially from sulphite and mechanical pulping); lignin degradation products (especially from sulphite pulping); synthetic organics, such as slimicides, oils and greases; and process chemicals, papermaking additives and oxidized metals. The chlorinated organics have been of particular concern, because they are acutely toxic to marine organisms and may bioaccumulate. This group of compounds, including the polychlorinated dibenzo-p-dioxins, have been the major impetus for minimizing chlorine use in pulp bleaching.
The amount and sources of suspended solids, oxygen demand and toxic discharges are process-dependent (table 1). Due to the solubilization of wood extractives with little or no chemical and resin acid recovery, both sulphite and CTMP pulping generate acutely toxic effluents with high BOD. Kraft mills historically used more chlorine for bleaching, and their effluents were more toxic; however, effluents from kraft mills which have eliminated Cl2 in bleaching and use secondary treatment typically exhibit little acute toxicity if any, and subacute toxicity has been greatly reduced.
Table 1. Total suspended solids and BOD associated with the untreated (raw) effluent of various pulping processes
|
Pulping Process |
Total Suspended Solids (kg/tonne) |
BOD (kg/tonne) |
|
Groundwood |
50–70 |
10–20 |
|
TMP |
45–50 |
25–50 |
|
CTMP |
50–55 |
40–95 |
|
Kraft, unbleached |
20–25 |
15–30 |
|
Kraft, bleached |
70–85 |
20–50 |
|
Sulphite, low-yield |
30–90 |
40–125 |
|
Sulphite, high-yield |
90–95 |
140–250 |
|
De-inking, non-tissue |
175–180 |
10–80 |
|
Waste paper |
110–115 |
5–15 |
Suspended solids have become less of a problem because most mills utilize primary clarification (e.g., gravity sedimentation or dissolved air flotation), which removes 80 to 95% of the settleable solids. Secondary wastewater treatment technologies such as aerated lagoons, activated sludge systems and biological filtration are used for reducing BOD, COD and chlorinated organics in the effluent.
In-plant process modifications to reduce settleable solids, BOD and toxicity include dry debarking and log conveying, improved chip screening to allow uniform cooking, extended delignification during pulping, changes to digestion chemical recovery operations, alternative bleaching technologies, high-efficiency pulp washing, fibre recovery from whitewater and improved spill containment. However, process upsets (particularly if they result in intentional sewering of liquors) and operational changes (particularly the use of unseasoned wood with a higher percentage of extractives) may still cause periodic toxicity breakthroughs.
A relatively recent pollution control strategy to eliminate water pollution entirely is the “closed mill” concept. Such mills are an attractive alternative in locations that lack large water sources to act as process-supply or effluent-receiving streams. Closed systems have been successfully implemented in CTMP and sodium-base sulphite mills. What distinguishes closed mills is that liquid effluent is evaporated and the condensate is treated, filtered, then reused. Other features of closed mills are enclosed screen rooms, counter-current washing in the bleach plant, and salt control systems. Although this approach is effective at minimizing water pollution, it is not yet clear how worker exposures will be affected by concentrating all contaminant streams within the mill. Corrosion is a major issue facing mills using closed systems, and bacteria and endotoxin concentrations are increased in recycled process water.
Solids Handling
The composition of solids (sludges) removed from liquid effluent treatment systems varies, depending on their source. Solids from primary treatment principally consist of cellulose fibres. The major component of solids from secondary treatment is microbial cells. If the mill uses chlorinated bleaching agents, both primary and secondary solids may also contain chlorinated organic compounds, an important consideration in determining the extent of treatment required.
Prior to disposal, sludges are thickened in gravity sedimentation units and mechanically dewatered in centrifuges, vacuum filters or belt or screw presses. Sludges from primary treatment are relatively easy to dewater. Secondary sludges contain a large quantity of intracellular water and exist in a matrix of slime; therefore they require the addition of chemical flocculants. Once sufficiently dewatered, sludge is disposed of in land-based applications (e.g., spread on arable or forested land, used as compost or as a soil conditioner) or incinerated. Although incineration is more costly and can contribute to air pollution problems, it may be advantageous because it can destroy or reduce toxic materials (e.g., chlorinated organics) that could create serious environmental problems if they were to leach into the groundwater from land-based applications.
Solid wastes can be generated in other mill operations. Ash from power boilers can be used in road beds, as construction material and as a dust suppressant. Waste from lime kilns can be used to modify soil acidity and improve soil chemistry.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."