- You are here:
-
Home

-
Contents (2)
-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
-
Storage
- Grandjean, Philippe

Brophy, Mary O.
Address: 5954 Smith Road, North Syracuse, New York 13212
Country: United States
Phone: 1 (315) 479-3441; Fax:
E-mail: mbrophy@sescva.esc.edu
Past position(s): Environmental Toxicologist, Syracuse Research Corporation; Research Assistant, Professor, SUN4 Health Science Center, Medical School
Education: PhD, 1979, University of Michigan; CIH; CPE
Areas of interest: Ergonomics; risk assessment
Funeral Services
General Profile
Assuming a world population of 5 billion, between one-quarter and one-half of a million people die each day. Many of the dead are infants or children, but eventually everyone who is born will also die. Despite the diversity in culture and religious beliefs surrounding death, the bodily remains of each person must be disposed of. In general, the two main methods of disposing of human remains consist of burial and cremation. Both of these disposal methods often have been applied to the untreated human remains. Many cultures, however, have developed funeral rites that prescribe some treatment of the dead body. Simpler rites may include the washing of the external surface with herbs and spices to slow or mask the onset of decay and the smell associated with dead tissue. More sophisticated rites include intrusive procedures such as embalming and removal of internal organs. Embalming usually involves replacement of blood with an embalming or preserving fluid. The Egyptians were among the first culture to develop and practice embalming of the dead. Embalming has been extensively practiced in the twentieth century throughout Western Europe and North America. Embalming may be followed either by burial or cremation. Outside of Western Europe and North America, burial or cremation is usually not preceded by embalming.
Funeral Processes
The preparation and burial of a deceased person can involve many processes, including:
- washing the surface of the body with various preparations
- dressing the body in burial clothes
- autopsies, in certain circumstances, which involve intrusive procedure, such as dissection and analysis of blood and body tissues
- embalming and removal of internal organs
- application of cosmetics to cover up visible damage if the body is to be viewed
- transporting the body to place of burial or cremation
- lifting of body and casket, and lowering it into the grave
- digging and filling of the grave
- possible exhumation of the body and subsequent autopsy.
Three types of hazard are always associated with the handling of deceased humans: microbial, psychological and ergonomic. A fourth type of hazard - chemical exposure - is introduced when embalming is performed. In the United States many states have enacted laws that require a body to be embalmed if the deceased person will be viewed in a open casket.
Microbial Hazards
Death is often caused by disease. After death the germs that caused the disease may continue to live in the deceased person and can infect the people handling the dead body.
Contagious diseases such as the plague and smallpox have been spread by improper handling of victims who died from the diseases. The route of exposure must be considered when evaluating the microbial hazard associated with the handling of dead bodies. Many diseases are spread by touching a source of contamination and then introducing that disease-causing organism, or pathogen, to one’s mucous membranes by rubbing the eyes or nose, or by ingesting the pathogen. Some diseases can be contracted simply by inhaling the pathogen. Inhalation can be a special hazard during exhumation, when the remains are dry, or during procedures that aerosolize parts of the human body, such as sawing through the bone of a deceased person. The contagion of diseases is further exacerbated when procedures with sharp instruments are used in funeral rites. Such practices introduce the possibility of parenteral exposure.
Microbial hazards can be classified in many different ways, including the type of disease-causing organism, the type of disease, the severity of the disease and the route of infection. Perhaps the most useful way of discussing microbial hazards encountered by funeral workers is by route of infection. The routes of infection are ingestion, inhalation, touch or surface contact and parenteral, or puncture of a body surface.
Ingestion as a route of exposure can be controlled by proper personal hygiene - that is, always washing hands before eating or smoking, and by keeping food, drink or any object that will be put in the mouth (such as cigarettes) out of areas of possible contamination. This is important for controlling chemical exposure as well. In addition to careful personal hygiene, wearing impermeable gloves when handling the dead can reduce the probability of infection.
Inhalation exposure occurs only when disease-causing organisms become airborne. For funeral workers the two primary ways that pathogens can become airborne are during an exhumation or during autopsy procedures in which a saw is used to cut through bone. A third possibility of aerosolizing a pathogen - tuberculosis, for example - is when air is forced out of the lungs of a corpse during handling. Although the epidemics of the past have included plague, cholera, typhoid, tuberculosis, anthrax and smallpox, only the organisms causing anthrax and smallpox appear capable of surviving any length of time after burial (Healing, Hoffman and Young 1995). These pathogens would be found in any of the soft tissues, not the bones, and particularly in soft tissues that have become mummified and/or dried out and friable. The anthrax bacterium can form spores that remain viable for long periods, especially under dry conditions. Intact smallpox viruses taken from the tissues of bodies buried in the 1850s were identified under the electron microscope. None of the viruses grew in tissue culture and they were deemed to be non-infective (Baxter, Brazier and Young 1988). Smallpox virus has remained infective, however, after 13 years in dry storage under laboratory conditions (Wolff and Croon 1968). An article appearing in the Journal of Public Health (UK) during the 1850s reports concern about smallpox infectivity from remains buried two hundred years earlier in Montreal, when smallpox was widespread in the New World (Sly 1994).
Perhaps a more probable source of inhalation exposure during exhumation are fungal spores. Whenever old material of any sort is disturbed, protection against the inhalation of fungal spores should be provided. Disposable high efficiency particulate (HEPA) respirators, developed primarily for protection against tuberculosis and lead dust, are quite effective against fungal spores as well. In addition to microbial concerns, the possibility of exposure to wood dust and/or lead needs to be evaluated before any exhumation proceeds.
The primary route of infection for tuberculosis is inhalation. The incidence of tuberculosis has increased during the last quarter of the twentieth century, primarily due to decreased public health vigilance and the emergence of bacterial strains that are resistant to several groups of antibiotics. A recent study conducted at Johns Hopkins School of Public Health (Baltimore, Maryland, US) indicates that 18.8% of embalmers demonstrated positive results to tuberculin skin tests. Only 6.8% of people employed in the funeral business who are not embalmers demonstrated positive results to the same test. The lower rate of reactivity is similar to the general public (Gershon and Karkashion 1996).
Hepatitis B virus (HBV) and the human immunodeficiency virus (HIV) are infective if they come in contact with mucous membranes or are introduced into the bloodstream through a cut or puncture. A study of funeral service practitioners in Maryland indicated that 10% had a mucous membrane exposure within the past 6 months and 15% reported a needle stick within the past 6 months (Gershon et al. 1995). Other US studies reported that between 39 and 53% of morticians had a needle stick within the past 12 months (Nwanyanwu, Tubasuri and Harris 1989). In the United States, the reported prevalence of HBV is between 7.5 and 12.0% in unvaccinated funeral directors, and 2.6% or less in vaccinated funeral workers. The reported vaccination rate varies between 19 and 60% of morticians in the United States. Although there is a vaccine for HBV, there is currently no vaccine for HIV.
HIV and HBV are infective only when the virus comes into contact with the mucous membranes or is introduced into the bloodstream of another human. The virus is not absorbed through intact skin. Mucous membranes include the mouth, nose and eyes. These viruses can be introduced into the bloodstream through a cut or abrasion in the skin, or by puncturing or cutting the skin with an instrument that is contaminated with the virus. Hands that are cracked due to dryness or a hangnail may provide routes of entry for these viruses. Therefore, to prevent transmission of these diseases it is important to provide a barrier impermeable to body fluids, to avoid splashing contaminated fluids on the eyes, nose or mouth, and to prevent puncturing or cutting the skin with an instrument contaminated with HIV or HBV. Use of latex gloves and a face shield can often provide this protection. Latex gloves, however, have a limited shelf life depending on the amount of sunlight and heat to which they have been exposed. In general, the latex should be stress tested if the gloves have been stored for more than a year. Stress testing involves filling the glove with water and observing if any leaks develop during a minimum of two minutes. Some countries in the West, such as the United States and Great Britain, have adopted the idea of universal precautions, which means that every corpse is treated as if it were infected with HIV and HBV.
Psychological Hazards
In many cultures the family of the deceased prepares the body of their dead relative for burial or cremation. In other cultures a specialized group of individuals prepares the bodies of the dead for burial or cremation. There is a psychological effect on the living when they are involved in handling dead bodies. The psychological effect is real regardless of the procedures used in the funeral rites. Recently there has been an interest in identifying and evaluating the effects of performing funeral rites on those who actually perform them.
Although the psychological hazards of being a professional funeral worker have not been extensively studied, the psychological effects of dealing with the human remains of traumatic death have been recently analyzed. The main psychological effects appear to be anxiety, depression and somatization (the tendency to report physical ailments), as well as irritability, appetite and sleep disturbances, and increased alcohol use (Ursano et al. 1995). Post-traumatic stress disorder (PTSD) occurred in a significant number of individuals who handled the victims of traumatic deaths. Immediately after a disaster in which human remains were handled by rescue workers, between 20 and 40% of the rescue workers were considered to be in a high risk category, as demonstrated by psychological testing, but only about 10% of the rescue workers were diagnosed with PTSD. The psychological effects were still present in rescue workers one year after the disaster, but the incidence was greatly reduced. Adverse psychological effects, however, have been detected in individuals several years after the traumatic event.
Many of these studies were performed on military personnel. They indicate that generalized stress rates are higher in inexperienced individuals who were not volunteers, and that there was an increased incidence of stress indicators up to one year after a traumatic incident. Empathy or self-identification of the mortuary worker with the deceased appeared to be associated with an increased level of psychological stress (McCarroll et al. 1993; McCarroll et al. 1995).
One study evaluated the causes of death in 4,046 embalmers and funeral directors in the United States between 1975 and 1985, and reported a proportionate mortality ratio (PMR) of 130 for suicide. The PMR is a ratio of the actual number of suicides in the embalmers and funeral directors divided by the number of suicides that would be expected in a group of individuals comparable in age, race and sex who are not embalmers or funeral directors. This ratio is then multiplied by 100. The purpose of this study was to assess the risk of cancer in morticians, and the suicide statistic was not elaborated any further.
Ergonomics
A deceased human adult is heavy and usually must be carried to a designated place of burial or cremation. Even when mechanical means of transportation are used, the dead body must be transferred from the place of death to the vehicle and from the vehicle to the burial or cremation site. Out of respect for the dead person, this transfer is usually performed by other humans.
Morticians are required to move corpses many times during the course of body preparation and funerals. Although there were no studies found that addressed this issue, low-back pain and injury is associated with prolonged repetitive lifting of heavy objects. There are lifting devices available which can assist with these types of lifts.
Chemical Hazards
Embalming procedures introduce a number of potent chemicals into the workspace of funeral workers. Perhaps the most widely used and toxic of these is formaldehyde. Formaldehyde is irritating to the mucous membranes, the eyes, the nasal lining and the respiratory system, and has been associated with mutagenic cell changes and the development of cancer, as well as occupational asthma. During the past several decades the occupational exposure level associated with no adverse effects has been consistently lowered. Current 8-hour time-weighted average permissible exposure limits range from 0.5 ppm in Germany, Japan, Norway, Sweden and Switzerland to 5 ppm in Egypt and Taiwan (IARC 1995c). Formaldehyde levels between 0.15 and 4.3 ppm, with instantaneous levels as high as 6.6 ppm, have been reported for individual embalmings. An embalming typically takes between 1 and 2 hours. Additional formaldehyde exposure is associated with the application of embalming creams and drying and hardening powders, and during spills.
Rats that have been chronically exposed to 6 to 15 ppm of formaldehyde (Albert et al. 1982; Kerns et al. 1982; Tobe et al. 1985), or repeatedly exposed to 20 ppm for 15-minute periods (Feron et al. 1988), have developed nasal carcinomas (Hayes et al. 1990). The IARC reports limited epidemiological evidence for an association between formaldehyde exposure in industry and the development of human nasal and pharyngeal cancers (Olsen and Asnaes 1986; Hayes et al. 1986; Roush et al. 1987; Vaughan et al. 1986; Blair et al. 1986; Stayner et al. 1988). Several studies of morticians, however, have reported an increased incidence of leukaemias and brain tumours (Levine, Andjelkovich and Shaw 1984; Walrath and Fraumeni 1983). In addition to the carcinogenic effects, formaldehyde is irritating to the mucous membranes and has been considered a strong sensitizer in the development of adult-onset asthma. The mechanism or mechanisms by which formaldehyde precipitates asthma are even less well characterized than its role in the development of cancer.
Other potentially toxic chemicals used in embalming fluids include phenol, methanol, isopropyl alcohol and glutaraldehyde (Hayes et al. 1990). Glutaraldehyde appears to be even more irritating than formaldehyde to the mucous membranes, and affects the central nervous system at levels well above 500 ppm. Methanol also affects the central nervous system and, in particular, the vision system. Phenol appears to affect the nervous system as well as the lungs, heart, liver and kidneys, and is absorbed quite rapidly through the skin. Our understanding of the toxicology of, and our ability to perform risk assessment for, exposure to multiple chemicals simultaneously are not sufficiently sophisticated to analyse the physiological effects of the mixtures to which embalmers and funeral directors are exposed. Blair et al. (1990a) thought that the increased incidence of leukaemias and brain tumours reported in professional, but not industrial, workers was a result of exposure to chemicals other than formaldehyde.
Recent advances in the design of dissecting tables indicate that local downdrafting of vapours significantly reduces the exposure of individuals working in the vicinity (Coleman 1995). Wearing gloves while performing procedures that require skin contact with embalming fluids and creams also reduces the hazard. There has been some concern, however, that some of the latex gloves on the market may be permeable to formaldehyde. Therefore, protective gloves should be selected carefully. In addition to the immediate concerns about the hazards of formaldehyde exposure, evidence has been accumulating that leachate from cemeteries may lead to formaldehyde contamination of groundwater.
Exhumation of bodies may also involve chemical exposures. Although used sporadically for centuries, lead was commonly used to line coffins beginning in the eighteenth and continuing into the nineteenth century. Inhalation of wood dust is associated with respiratory problems, and fungus-contaminated wood dust is a double-edged sword. Arsenic and mercury compounds were also used as preservatives in the past and could present a hazard during exhumation.
Hazards in Sewage (Waste) Treatment Plants
Without treatment of waste the current concentration of people and industry in many parts of the world would very quickly make portions of the environment incompatible with life. Although reduction of the amount of waste is important, the proper treatment of waste is essential. Two basic types of waste enter a treatment plant, human/animal waste and industrial waste. Humans excrete about 250 grams of solid waste per capita per day, including 2000 million coliform and 450 million streptococci bacteria per person per day (Mara 1974). Industrial solid waste production rates range from 0.12 tons per employee per year at professional and scientific institutions to 162.0 tons per employee per year at sawmills and planing mills (Salvato 1992). Although some waste treatment plants are exclusively dedicated to handling one or the other type of material, most plants handle both animal and industrial waste.
Hazards and Their Prevention
The goal of waste water treatment plants is to remove as much of the solid, liquid and gaseous contaminants as possible within technically feasible and financially achievable constraints. There are a variety of different processes that are used to remove contaminants from waste water including sedimentation, coagulation, flocculation, aeration, disinfection, filtration and sludge treatment. (See also the article “Sewage treatment” in this chapter.) The specific hazard associated with each process varies depending on the design of the treatment plant and the chemicals used in the different processes, but the types of hazard can be classified as physical, microbial and chemical. The key to preventing and/or minimizing the adverse effects associated with working in sewage treatment plants is to anticipate, recognize, evaluate and control the hazards.
Figure 1. Manhole with cover removed.
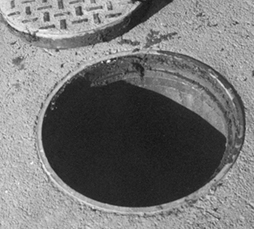
Mary O. Brophy
Physical hazards
Physical hazards include confined spaces, inadvertent energizing of machines or machine parts and trips and falls. The result of an encounter with a physical hazards can often be immediate, irreversible and serious, even fatal. Physical hazards vary with the design of the plant. Most sewage treatment plants, however, have confined spaces which include underground or below grade vaults with limited access, manholes (figure 1) and the sedimentation tanks when they have been emptied of liquid content during, for example, repairs (figure 2). Mixing equipment, sludge rakes, pumps and mechanical devices used for a variety of operations in sewage treatment plants can maim, and even kill, if they are inadvertently activated when a worker is servicing them. Wet surfaces, often encountered in sewage treatment plants, contribute to slipping and falling hazards.
Figure 2. Empty tank in a sewage treatment plant.

Mary O. Brophy
Confined-space entry is one of the most common and one of the most serious hazards faced by sewage treatment workers. A universal definition of a confined space is elusive. In general, however, a confined space is an area with limited means of entry and egress that was not designed for continuous human habitation and that does not have adequate ventilation. Hazards occur when the confined space is associated with a deficiency of oxygen, the presence of a toxic chemical or an engulfing material, such as water. Decreased oxygen levels can be the result of a variety of conditions including the replacement of oxygen with another gas, such as methane or hydrogen sulphide, the consumption of oxygen by the decay of organic material contained in the waste water or the scavenging of oxygen molecules in the rusting process of some structure within the confined space. Because low levels of oxygen in confined spaces cannot be detected by unaided human observation it is extremely important to use an instrument that can determine the level of oxygen before entering any confined space.
The earth’s atmosphere consists of 21% oxygen at sea level. When the percentage of oxygen in breathing air falls below about 16.5% a person’s breathing becomes more rapid and more shallow, the heart rate increases and the person begins to lose coordination. Below about 11% the person experiences nausea, vomiting, inability to move and unconsciousness. Emotional instability and impaired judgement may occur at oxygen levels somewhere between these two points. When individuals enter an atmosphere with oxygen levels below 16.5% they may immediately become too disoriented to get themselves out and eventually succumb to unconsciousness. If the oxygen depletion is great enough individuals can become unconscious after one breath. Without rescue they can die within minutes. Even if rescued and resuscitated, permanent damage can occur (Wilkenfeld et al. 1992).
Lack of oxygen is not the only hazard in a confined space. Toxic gases can be present in a confined space at a concentration level high enough to do serious harm, even kill, despite adequate oxygen levels. The effects of toxic chemicals encountered in confined spaces are discussed further below. One of the most effective ways to control the hazards associated with low oxygen levels (below 19.5%) and atmospheres contaminated with toxic chemicals is to thoroughly and adequately ventilate the confined space with mechanical ventilation prior to allowing anyone to enter it. This is usually done with a flexible duct through which outside air is blown into the confined space (see figure 3). Care must be taken to ensure that fumes from a generator or the fan motor are not also blown into the confined space (Brophy 1991).
Figure 3. Air moving unit for entering a confined space.
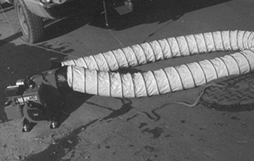
Mary O. Brophy
Sewage treatment plants often have large pieces of machinery to move sludge or raw sewage from one place in the plant to another. When repairs are made on this type of equipment the entire machine should be de-energized. Furthermore, the switch to re-energize the equipment should be under the control of the person performing the repairs. This prevents another worker in the plant from inadvertently energizing the equipment. Development and implementation of procedures to achieve these goals is called a lockout/tagout programme. Mutilation of body parts, such as fingers, arms and legs, dismemberment and even death can result from ineffective or inadequate lockout/tagout programmes.
Sewage treatment plants often contain large tanks and storage containers. People sometimes need to work on top of the containers, or walk by pits that have been emptied of water and may contain an 8 to 10 foot (2.5 to 3 m) drop (see figure 4). Sufficient protection against falls as well as adequate safety training should be provided for the workers.
Microbial hazards
Microbial hazards are primarily associated with the treatment of human and animal waste. Although bacteria are often added to alter the solids contained in waste water, the hazard to sewage treatment workers comes primarily from exposure to micro-organisms contained in human and other animal waste. When aeration is used during the sewage treatment process these micro-organisms can become airborne. The long term effect on the immune system of individuals exposed to these micro-organisms for extended periods of time has not been conclusively evaluated. In addition, workers who remove solid refuse from the influent stream before any treatment is begun are often exposed to micro-organisms contained in material splashing onto their skin and making contact with the mucous membranes. The results of encountering micro-organisms found in sewage treatment plants for extended periods of time are often more subtle than resulting from acute intense exposures. Nevertheless, these effects can also be irreversible and serious.
The three main categories of microbes relevant to this discussion are fungi, bacteria and viruses. All three of these can cause acute illness as well as chronic disease. Acute symptoms including respiratory distress, abdominal pains and diarrhoea have been reported in waste treatment workers (Crook, Bardos and Lacey 1988; Lundholm and Rylander 1980). Chronic diseases, such as asthma and allergic alveolitis, have been traditionally associated with exposure to high levels of airborne microbes and, recently, with microbial exposure during the treatment of domestic waste (Rosas et al. 1996; Johanning, Olmstead and Yang 1995). Reports of significantly elevated concentrations of fungi and bacteria in waste treatment, sludge dewatering and composting facilities are beginning to be published (Rosas et al. 1996; Bisesi and Kudlinski 1996; Johanning Olmstead and Yang 1995). Another source of airborne microbes is the aeration tanks which are used in many sewage treatment plants.
In addition to inhalation, microbes can be transmitted through ingestion and through contact with skin that is not intact. Personal hygiene, including washing hands before eating, smoking and going to the bathroom, is important. Food, drink, eating utensils, cigarettes and anything that would be put into the mouth should be kept away from areas of possible microbial contamination.
Chemical hazards
Chemical encounters at waste treatment plants can be both immediate and fatal, as well as protracted. A variety of chemicals are used in the process of coagulation, flocculation, disinfection and sludge treatment. The chemical of choice is determined by the contaminant or contaminants in the raw sewage; some industrial waste requires somewhat exotic chemical treatment. In general, however, the primary hazards from chemicals used in the coagulation and flocculation processes are skin irritation and eye injury due to direct contact. This is especially true of solutions which have a pH (acidity) less than 3 or greater than 9. The disinfection of effluent is often achieved by using either liquid or gaseous chlorine. Use of liquid chlorine can cause eye injury if splashed into the eyes. Ozone and ultraviolet light are also used to achieve disinfection of the effluent.
One way to monitor the effectiveness of sewage treatment is to measure the amount of organic material which remains in the effluent after treatment is complete. This can be done by determining the amount of oxygen that would be required to biodegrade the organic material contained in 1 litre of liquid over a period of 5 days. This is referred to as the 5-day biological oxygen demand (BOD5).
Chemical hazards in sewage treatment plants arise from the decomposition of organic material which results in the production of hydrogen sulphide and methane, from toxic waste dumped down the sewer lines and from the contaminants produced by operations performed by the workers themselves.
Hydrogen sulphide is almost always found in waste treatment plants. Hydrogen sulphide, also known as sewer gas, has a distinctive, unpleasant smell, often identified as rotten eggs. The human nose, however, quickly becomes accustomed to the smell. People who are exposed to hydrogen sulphide often lose their ability to detect its odour (i.e., olfactory fatigue). Furthermore, even if the olfactory system is able to detect hydrogen sulphide, it is not able to accurately judge its concentration in the atmosphere. Hydrogen sulphide biochemically interferes with the electron transport mechanism and blocks the utilization of oxygen at the molecular level. The result is asphyxiation and ultimately death due to the lack of oxygen in the brainstem cells that control the breathing rate. High levels of hydrogen sulphide (greater than 100 ppm) can, and often do, occur in the confined spaces found in sewage treatment plants. Exposure to very high levels of hydrogen sulphide can result in almost instantaneous suppression of the respiratory centre in the brainstem. The US National Institute for Occupational Safety and Health (NIOSH) has identified 100 ppm of hydrogen sulphide as immediately dangerous to life and health (IDLH). Lower levels of hydrogen sulphide (less than 10 ppm) are almost always present in some areas of sewage treatment plants. At these lower levels hydrogen sulphide can be irritating to the respiratory system, be associated with headaches and result in conjunctivitis (Smith 1986). Hydrogen sulphide is produced whenever organic matter decays and, industrially, during the production of paper (Kraft process), the tanning of leather (hair removal with sodium sulphide), and the production of heavy water for nuclear reactors.
Methane is another gas produced by the decomposition of organic matter. In addition to displacing oxygen, methane is explosive. Levels can be reached which result in an explosion when a spark or source of ignition is introduced.
Plants that handle industrial waste should have a thorough knowledge of the chemicals used in each of the industrial plants that utilize their services and a working relationship with the management of those plants so that they are promptly informed of any changes in processes and waste contents. Dumping of solvents, fuels and any other substance into sewer systems presents a hazard to treatment workers not only because of the toxicity of the material dumped but also because the dumping is unanticipated.
Whenever any industrial operation, such as welding or spray painting, is performed in a confined space special care must be taken to provide sufficient ventilation to prevent an explosion hazard as well as to remove toxic material produced by the operation. When an operation performed in a confined space produces a toxic atmosphere it is often necessary to equip the worker with a respirator because ventilation of the confined space may not ensure that the concentration of the toxic chemical can be maintained below the permissible exposure limit. Selection and fitting of a proper respirator falls within the purview of industrial hygiene practice.
Another serious chemical hazard in sewage treatment plants is the use of gaseous chlorine to decontaminate the effluent from the plant. The gaseous chlorine comes in a variety of containers weighing from 70 kg to roughly 1 tonne. Some of the very large sewage treatment plants use chlorine delivered in railroad cars. Gaseous chlorine is extremely irritating to the alveolar portion of the lungs, even in levels as low as a few ppm. Inhalation of higher concentrations of chlorine can cause inflammation of the alveoli of the lung and produce the adult respiratory distress syndrome, which has a 50% death rate. When a sewage treatment plant utilizes large amounts of chlorine (1 tonne and greater) the hazard exists not only for the plant workers but for the surrounding community as well. Unfortunately, the plants that use the largest amounts of chlorine are often located in large metropolitan centres with high density of people. Other methods of decontamination of sewage treatment plant effluent are available, including ozone treatment, the use of liquid hypochlorite solution and ultraviolet irradiation.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."