- You are here:
-
Home

-
Contents (2)
-
Part XVII. Services and Trade
-
Transport Industry and Warehousing
- Storage

Kogi, Kazutaka
Address: The Institute for Science of Labour (ISL), 2-8-14 Sugao, Miyamae-ku, Kawasaki 216
Country: Japan
Phone: 81 44 977 2121
Fax: 81 44 977 7504
Past position(s): Director, Working Conditions and Environment Department, International Labour Office; Chief, Occupational Safety and Health Branch, International Labour Office
Education: MD, 1958, University of Tokyo Faculty of Medicine; Dr Med Sci, 1990, Okayama University
Areas of interest: Assessment of fatigue; shift work; participatory ergonomics; low-cost improvements
Sleep Deprivation
Healthy individuals regularly sleep for several hours every day. Normally they sleep during the night hours. They find it most difficult to remain awake during the hours between midnight and early morning, when they normally sleep. If an individual has to remain awake during these hours either totally or partially, the individual comes to a state of forced sleep loss, or sleep deprivation, that is usually perceived as tiredness. A need for sleep, with fluctuating degrees of sleepiness, is felt which continues until sufficient sleep is taken. This is the reason why periods of sleep deprivation are often said to cause a person to incur sleep deficit or sleep debt.
Sleep deprivation presents a particular problem for workers who cannot take sufficient sleep periods because of work schedules (e.g., working at night) or, for that matter, prolonged free-time activities. A worker on a night shift remains sleep-deprived until the opportunity for a sleep period becomes available at the end of the shift. Since sleep taken during daytime hours is usually shorter than needed, the worker cannot recover from the condition of sleep loss sufficiently until a long sleep period, most likely a night sleep, is taken. Until then, the person accumulates a sleep deficit. (A similar condition—jet lag—arises after travelling between time zones that differ by a few hours or more. The traveller tends to be sleep-deprived as the activity periods in the new time zone correspond more clearly to the normal sleep period in the originating place.) During the periods of sleep loss, workers feel tired and their performance is affected in various ways. Thus various degrees of sleep deprivation are incorporated into the daily life of workers having to work irregular hours and it is important to take measures to cope with unfavourable effects of such sleep deficit. The main conditions of irregular working hours that contribute to sleep deprivation are shown in table 1.
Table 1. Main conditions of irregular working hours which contribute to sleep deprivation of various degrees
|
Irregular working hours |
Conditions leading to sleep deprivation |
|
Night duty |
No or shortened night-time sleep |
|
Early morning or late evening duty |
Shortened sleep, disrupted sleep |
|
Long hours of work or working two shifts together |
Phase displacement of sleep |
|
Straight night or early morning shifts |
Consecutive phase displacement of sleep |
|
Short between-shift period |
Short and disrupted sleep |
|
Long interval between days off |
Accumulation of sleep shortages |
|
Work in a different time zone |
No or shortened sleep during the “night” hours in the originating place (jet lag) |
|
Unbalanced free time periods |
Phase displacement of sleep, short sleep |
In extreme conditions, sleep deprivation may last for more than a day. Then sleepiness and performance changes increase as the period of sleep deprivation is prolonged. Workers, however, normally take some form of sleep before sleep deprivation becomes too protracted. If the sleep thus taken is not sufficient, the effects of sleep shortage still continue. Thus, it is important to know not only the effects of sleep deprivation in various forms but also the ways in which workers can recover from it.
Figure 1. Perfomance, sleep ratings and physiological variables of a group of subjects exposed to two nights of sleep deprivation
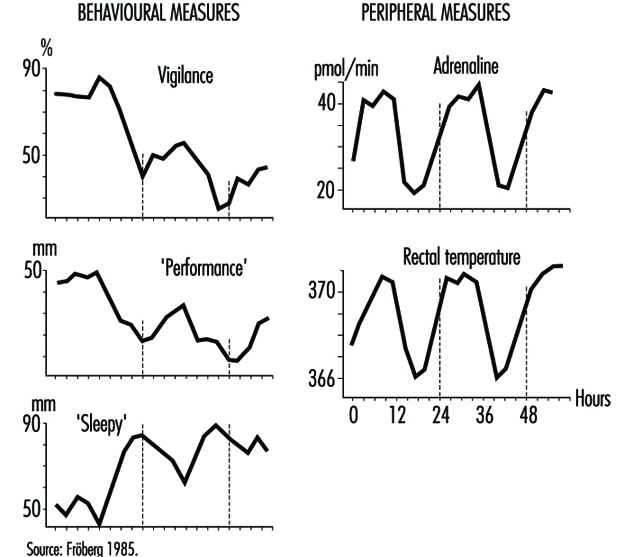
The complex nature of sleep deprivation is shown by figure 1, which depicts data from laboratory studies on the effects of two days of sleep deprivation (Fröberg 1985). The data show three basic changes resulting from prolonged sleep deprivation:
- There is a general decreasing trend in both objective performance and subjective ratings of performance efficiency.
- The decline in performance is influenced by the time of day. This cycling decline is correlated with those physiological variables which have a circadian cycling period. Performance is better in the normal activity phase when, for example, adrenaline excretion and body temperature are higher than those in the period originally assigned to a normal night’s sleep, when the physiological measures are low.
- Self-ratings of sleepiness increase with time of continuous sleep deprivation, with a clear cyclic component associated with time of day.
The fact that the effects of sleep deprivation are correlated with physiological circadian rhythms helps us to understand its complex nature (Folkard and Akerstedt 1992). These effects should be viewed as a result of a phase shift of the sleep-wakefulness cycle in one’s daily life.
The effects of continuous work or sleep deprivation thus include not only a reduction in alertness but decreased performance capabilities, increased probability of falling asleep, lowered well-being and morale and impaired safety. When such periods of sleep deprivation are repeated, as in the case of shift workers, their health may be affected (Rutenfranz 1982; Koller 1983; Costa et al. 1990). An important aim of research is thus to determine to what extent sleep deprivation damages the well-being of individuals and how we can best use the recovery function of sleep in reducing such effects.
Effects of Sleep Deprivation
During and after a night of sleep deprivation, the physiological circadian rhythms of the human body seem to remain sustained. For example, the body temperature curve during the first day’s work among night-shift workers tends to keep its basic circadian pattern. During the night hours, the temperature declines towards early morning hours, rebounds to rise during the subsequent daytime and falls again after an afternoon peak. The physiological rhythms are known to get “adjusted” to the reversed sleep-wakefulness cycles of night-shift workers only gradually in the course of several days of repeated night shifts. This means that the effects on performance and sleepiness are more significant during night hours than in the daytime. The effects of sleep deprivation are therefore variably associated with the original circadian rhythms seen in physiological and psychological functions.
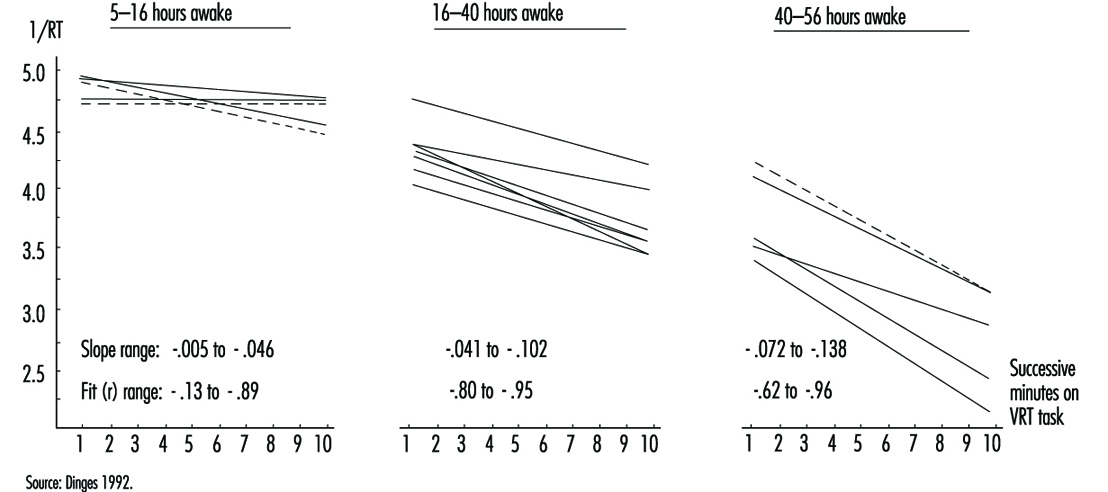
The effects of sleep deprivation on performance depend on the type of the task to be performed. Different characteristics of the task influence the effects (Fröberg 1985; Folkard and Monk 1985; Folkard and Akerstedt 1992). Generally, a complex task is more vulnerable than a simpler task. Performance of a task involving an increasing number of digits or a more complex coding deteriorates more during three days of sleep loss (Fröberg 1985; Wilkinson 1964). Paced tasks that need to be responded to within a certain interval deteriorate more than self-paced tasks. Practical examples of vulnerable tasks include serial reactions to defined stimulations, simple sorting operations, the recording of coded messages, copy typing, display monitoring and continuous inspection. Effects of sleep deprivation on strenuous physical performance are also known. Typical effects of prolonged sleep deprivation on performance (on a visual task) is shown in figure 2 (Dinges 1992). The effects are more pronounced after two nights of sleep loss (40-56 hours) than after one night of sleep loss (16-40 hours).
Figure 2. Regression lines fit to response speed (the reciprocal of response times) on a 10-minute simple, unprepared visual task administered repeatedly to healthy young adults during no sleep loss (5-16 hours), one night of sleep loss (16-40 hours) and two nights of sleep loss (40-56 hours)
The degree to which the performance of tasks is affected also appears to depend on how it is influenced by the “masking” components of the circadian rhythms. For example, some measures of performance, such as five-target memory search tasks, are found to adjust to night work considerably more quickly than serial reaction time tasks, and hence they may be relatively unimpaired on rapidly rotating shift systems (Folkard et al. 1993). Such differences in the effects of endogenous physiological body clock rhythms and their masking components must be taken into account in considering the safety and accuracy of performance under the influence of sleep deprivation.
One particular effect of sleep deprivation on performance efficiency is the appearance of frequent “lapses” or periods of no response (Wilkinson 1964; Empson 1993). These performance lapses are short periods of lowered alertness or light sleep. This can be traced in records of videotaped performance, eye movements or electroencephalograms (EEGs). A prolonged task (one-half hour or more), especially when the task is replicated, can more easily lead to such lapses. Monotonous tasks such as repetitions of simple reactions or monitoring of infrequent signals are very sensitive in this regard. On the other hand, a novel task is less affected. Performance in changing work situations is also resistant.
While there is evidence of a gradual arousal decrease in sleep deprivation, one would expect less affected performance levels between lapses. This explains why results of some performance tests show little influence of sleep loss when the tests are done in a short period of time. In a simple reaction time task, lapses would lead to very long response times whereas the rest of the measured times would remain unchanged. Caution is thus needed in interpreting test results concerning sleep loss effects in actual situations.
Changes in sleepiness during sleep deprivation obviously relate to physiological circadian rhythms as well as to such lapse periods. Sleepiness sharply increases with time of the first period of night-shift work, but decreases during subsequent daytime hours. If sleep deprivation continues to the second night sleepiness becomes very advanced during the night hours (Costa et al. 1990; Matsumoto and Harada 1994). There are moments when the need for sleep is felt to be almost irresistible; these moments correspond to the appearance of lapses, as well as to the appearance of interruptions in the cerebral functions as evidenced by EEG records. After a while, sleepiness is felt to be reduced, but there follows another period of lapse effects. If workers are questioned about various fatigue feelings, however, they usually mention increasing levels of fatigue and general tiredness persisting throughout the sleep deprivation period and between-lapse periods. A slight recovery of subjective fatigue levels is seen during the daytime following a night of sleep deprivation, but fatigue feelings are remarkably advanced in the second and subsequent nights of continued sleep deprivation.
During sleep deprivation, sleep pressure from the interaction of prior wakefulness and circadian phase may always be present to some degree, but the lability of state in sleepy subjects is also modulated by context effects (Dinges 1992). Sleepiness is influenced by the amount and type of stimulation, the interest afforded by the environment and the meaning of the stimulation to the subject. Monotonous stimulation or that requiring sustained attention can more easily lead to vigilance decrement and lapses. The greater the physiological sleepiness due to sleep loss, the more the subject is vulnerable to environmental monotony. Motivation and incentive can help override this environmental effect, but only for a limited period.
Effects of Partial Sleep Deprivation and Accumulated Sleep Shortages
If a subject works continuously for a whole night without sleep, many performance functions will have definitely deteriorated. If the subject goes to the second night shift without getting any sleep, the performance decline is far advanced. After the third or fourth night of total sleep deprivation, very few people can stay awake and perform tasks even if highly motivated. In actual life, however, such conditions of total sleep loss rarely occur. Usually people take some sleep during subsequent night shifts. But reports from various countries show that sleep taken during daytime is almost always insufficient to recover from the sleep debt incurred by night work (Knauth and Rutenfranz 1981; Kogi 1981; ILO 1990). As a result, sleep shortages accumulate as shift workers repeat night shifts. Similar sleep shortages also result when sleep periods are reduced on account of the need to follow shift schedules. Even if night sleep can be taken, sleep restriction of as little as two hours each night is known to lead to an insufficient amount of sleep for most persons. Such sleep reduction can lead to impaired performance and alertness (Monk 1991).
Examples of conditions in shift systems which contribute to accumulation of sleep shortages, or partial sleep deprivation, are given in table 1. In addition to continued night work for two or more days, short between-shift periods, repetition of an early start of morning shifts, frequent night shifts and inappropriate holiday allotment accelerate the accumulation of sleep shortages.
The poor quality of daytime sleep or shortened sleep is important, too. Daytime sleep is accompanied by an increased frequency of awakenings, less deep and slow-wave sleep and a distribution of REM sleep different from that of normal night-time sleep (Torsvall, Akerstedt and Gillberg 1981; Folkard and Monk 1985; Empson 1993). Thus a daytime sleep may not be as sound as a night sleep even in a favourable environment.
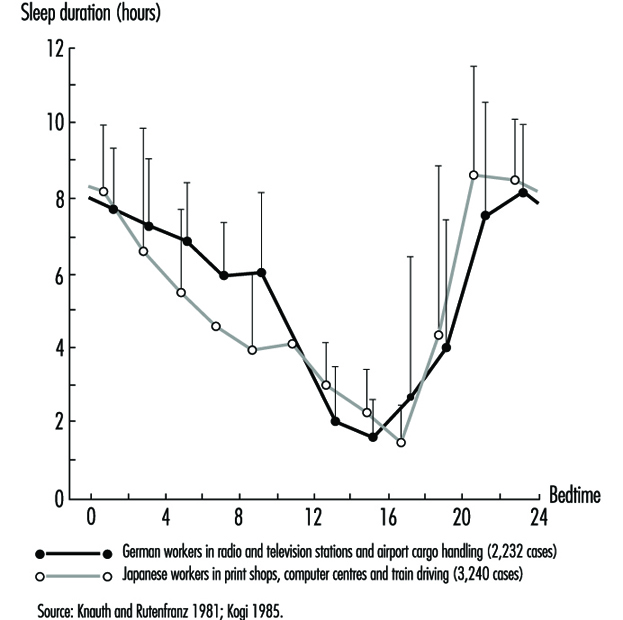
This difficulty of taking good quality sleep due to different timing of sleep in a shift system is illustrated by figure 3 which shows the duration of sleep as a function of the time of sleep onset for German and Japanese workers based on diary records (Knauth and Rutenfranz 1981; Kogi 1985). Due to circadian influence, daytime sleep is forced to be short. Many workers may have split sleep during the daytime and often add some sleep in the evening where possible.
Figure 3. Mean sleep length as a function of the time of sleep onset. Comparison of data from German and Japanese shift workers.
In real-life settings, shift workers take a variety of measures to cope with such accumulation of sleep shortages (Wedderburn 1991). For example, many of them try to sleep in advance before a night shift or have a long sleep after it. Although such efforts are by no means entirely effective to offset the effects of sleep deficit, they are made quite deliberately. Social and cultural activities may be restricted as part of coping measures. Outgoing free-time activities, for example, are undertaken less frequently between two night shifts. Sleep timing and duration as well as the actual accumulation of sleep deficit thus depend on both job-related and social circumstances.
Recovery from Sleep Deprivation and Health Measures
The only effective means of recovering from sleep deprivation is to sleep. This restorative effect of sleep is well known (Kogi 1982). As recovery by sleep may differ according to its timing and duration (Costa et al. 1990), it is essential to know when and for how long people should sleep. In normal daily life, it is always the best to take a full night’s sleep to accelerate the recovery from sleep deficit but efforts are usually made to minimize sleep deficit by taking sleep at different occasions as replacements of normal night sleeps of which one has been deprived. Aspects of such replacement sleeps are shown in table 2.
Table 2. Aspects of advance, anchor & retard sleeps taken as replacement of normal night sleep
|
Aspect |
Advance sleep |
Anchor sleep |
Retard sleep |
|
Occasion |
Before a night shift |
Intermittent night |
After a night shift |
|
Duration |
Usually short |
Short by definition |
Usually short but |
|
Quality |
Longer latency of |
Short latency |
Shorter latency for |
|
Interaction with |
Disrupted rhythms; |
Conducive to |
Disrupted rhythms; |
To offset night sleep deficit, the usual effort made is to take daytime sleep in “advance” and “retard” phases (i.e., before and after night-shift work). Such a sleep coincides with the circadian activity phase. Thus the sleep is characterized by longer latency, shortened slow-wave sleep, disrupted REM sleep and disturbances of one’s social life. Social and environmental factors are important in determining the recuperative effect of a sleep. That a complete conversion of circadian rhythms is impossible for a shift worker in a real-life situation should be borne in mind in considering the effectiveness of the recovery functions of sleep.
In this respect, interesting features of a short “anchor sleep” have been reported (Minors and Waterhouse 1981; Kogi 1982; Matsumoto and Harada 1994). When part of the customary daily sleep is taken during the normal night sleep period and the rest at irregular times, the circadian rhythms of rectal temperature and urinary secretion of several electrolytes can retain a 24-hour period. This means that a short night-time sleep taken during the night sleep period can help preserve the original circadian rhythms in subsequent periods.
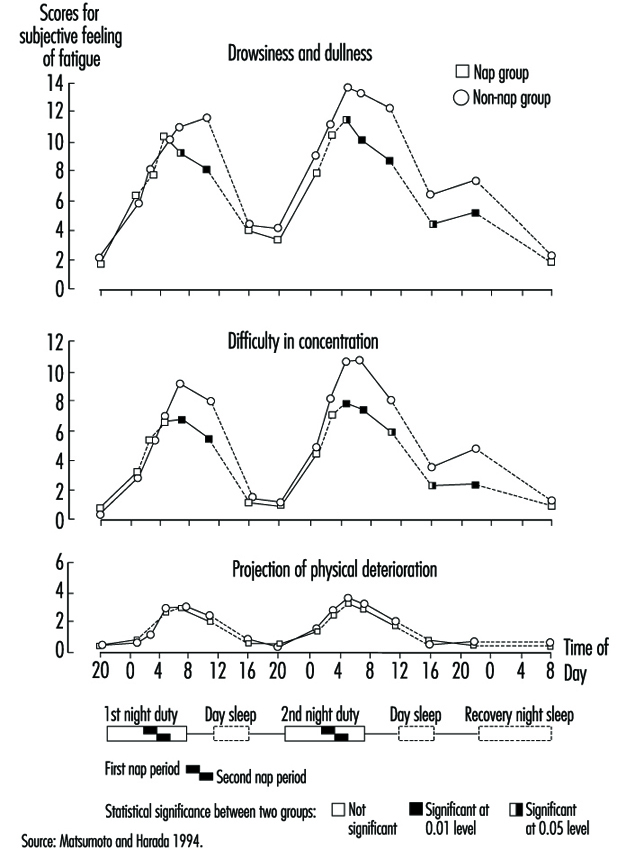
We may assume that sleeps taken at different periods of the day could have certain complementary effects in view of the different recovery functions of these sleeps. An interesting approach for night-shift workers is the use of a night-time nap which usually lasts up to a few hours. Surveys show this short sleep taken during a night shift is common among some groups of workers. This anchor-sleep type sleep is effective in reducing night work fatigue (Kogi 1982) and may reduce the need of recovery sleep. Figure 4 compares the subjective feelings of fatigue during two consecutive night shifts and the off-duty recovery period between the nap-taking group and the non-nap group (Matsumoto and Harada 1994). The positive effects of a night-time nap in reducing fatigue was obvious. These effects continued for a large part of the recovery period following night work. Between these two groups, no significant difference was found upon comparing the length of the day sleep of the non-nap group with the total sleeping time (night-time nap plus subsequent day sleep) of the nap group. Therefore a night-time nap enables part of the essential sleep to be taken in advance of the day sleep following night work. It can therefore be suggested that naps taken during night work can to a certain extent aid recovery from the fatigue caused by that work and accompanying sleep deprivation (Sakai et al. 1984; Saito and Matsumoto 1988).
Figure 4. Mean scores for subjective feelings of fatigue during two consecutive night shifts and the off-duty recovery period for nap and no-nap groups
It must be admitted, however, that it is not possible to work out optimal strategies that each worker suffering from sleep deficit can apply. This is demonstrated in the development of international labour standards for night work that recommend a set of measures for workers doing frequent night work (Kogi and Thurman 1993). The varied nature of these measures and the trend towards increasing flexibility in shift systems clearly reflect an effort to develop flexible sleep strategies (Kogi 1991). Age, physical fitness, sleep habits and other individual differences in tolerance may play important roles (Folkard and Monk 1985; Costa et al. 1990; Härmä 1993). Increasing flexibility in work schedules in combination with better job design is useful in this regard (Kogi 1991).
Sleep strategies against sleep deprivation should be dependent on type of working life and be flexible enough to meet individual situations (Knauth, Rohmert and Rutenfranz 1979; Rutenfranz, Knauth and Angersbach 1981; Wedderburn 1991; Monk 1991). A general conclusion is that we should minimize night sleep deprivation by selecting appropriate work schedules and facilitate recovery by encouraging individually suitable sleeps, including replacement sleeps and a sound night-time sleep in the early periods after sleep deprivation. It is important to prevent the accumulation of sleep deficit. The period of night work which deprives workers of sleep in the normal night sleep period should be as short as possible. Between-shift intervals should be long enough to allow a sleep of sufficient length. A better sleep environment and measures to cope with social needs are also useful. Thus, social support is essential in designing working time arrangements, job design and individual coping strategies in promoting the health of workers faced with frequent sleep deficit.
Workers' Accident Compensation in Japan
Summary of Coverage and Goal
Coverage
Hazards covered
The workers’ accident compensation insurance system in Japan is under the control of the government, based on the Workmen’s Accident Compensation Law (1947). It gives workers insurance benefits in order to protect them promptly and fairly against injuries, diseases, disabilities or deaths incurred “because of duty”. The definition of “because of duty” is not stipulated by the provisions in related laws. The criteria used by the government administration make it clear, however, that the system is applied to injuries, disabilities or deaths that result from employment, namely “during the duty situation in which workers are under the control of an employer according to work contracts” and “due to an accident or a circumstance caused by this duty situation”. Thus the system is applied to all the injuries, disabilities and deaths incurred while workers are working or commuting to work. It is also applied to “diseases or disorders to workers engaged in work with hazards that can harm health from sudden or chronic action of such hazards”. These because-of-duty diseases include those caused by injury resulting from employment and occupational diseases caused by physical, chemical and biological agents or specific forms of work performance, and those apparently caused by work.
Industries and workers covered
The workmen’s accident compensation insurance system is applied compulsorily to all workers who are employed in enterprises to which the Labour Standards Law is applied and receive wages. They include those regularly or temporarily employed, daily-wage workers, and both full-time and part-time workers, irrespective of the size of enterprises.
All industries are covered by the system, except part of the agriculture, forestry and fishery industries. The exceptions are agricultural undertakings individually owned and employing less than five workers, forestry undertakings not employing regular workers, and fishery undertakings employing less than five workers and operating in sea areas without significant accident. Government employees, local government employees and sailors are covered by separate workmen’s compensation systems.
Types of payment
The following types of insurance benefits are available for on-the-job injuries and diseases:
- medical benefit: in principle, medical treatment (in exceptional cases cash reimbursement for treatment expenses)
- temporary disability benefit: when unable to work and earn wages because of treatment
- injury and disease compensation pension: when not recovered one-and-a-half years after starting to receive treatment and the extent of disabilities remains at a certain level
- physical handicaps compensation benefit: according to the degree of physical handicap the workers are left with
- bereaved family compensation benefit: to the spouse, children, parents, grandchildren, grandparents or brothers and sisters who had been supported by the income of the workers concerned
- expenses for funeral rites
- nursing compensation benefit: for full-time or occasional nursing in the case of a grade 1 or grade 2 physical handicaps compensation pension or an injury and disease compensation pension.
For injury, disease, disability or death incurred during commuting, the following benefits are paid: (a) medical benefit; (b) temporary disability benefit; (c) injury and disease pension; (d) physical handicaps benefit; (e) bereaved family benefit; (f) funeral rites benefit; and (g) nursing benefit. The details of these benefits are the same as in the case of on-the-job accidents or occupational diseases.
The income benefits are calculated on the basis of the average daily wage of the workers concerned. The temporary disability benefit amounts to 60 of the average daily wage and is given starting from the fourth day of absence from work, together with the temporary disability special supplement equivalent to 20% of the average daily wage (the employer must pay compensation equivalent to 60% of the average wage for the first three days). The amount of injury and disease compensation pension, given when workers do not recover within one-and-a-half years, ranges from 245 to 313 days of the average daily wage. The physical handicaps benefit ranges from 131 to 313 days of the average daily wage. The amount of the bereaved family compensation lump sum ranges from 153 to 245 days of the average daily wage.
The temporary disability benefit, the pension and the lump sum benefit are subject to the sliding scale system which reflects the movement of wages. In cases where the average pay of all the workers for a quarter of the year surpasses 110% or falls short of 90% of the average pay for the quarter to which the day belongs when the worker concerned was injured or taken ill, the average daily wage used for the calculation of temporary disability benefit is automatically revised according to the fluctuating average pay rate. Similar calculations are done for pension and lump sum benefits when the average pay of all the workers for a year surpasses or falls short of the average pay for the year in which the worker concerned died or became ill.
Other aspects
Welfare services
The purpose of the Workmen’s Accident Compensation Insurance is to advance the welfare of workers by promoting return to work or social life of the victims, to give support to them and their bereaved families and to secure proper working conditions. Therefore the system has separate provisions for various welfare services and some preventive measures. Some of these services are managed by the Labour Welfare Services Association, to which the insurance system supplies the funds. Welfare services include the establishment and management of employment injury hospitals, spinal cord impediment centres, rehabilitation workshops, housing loans, relief funds for education and long-term family nursing, installation and operation of special care facilities for workers suffering from employment injuries, home help services and nursing device leasing.
Extension of coverage
Employers of small and medium-sized enterprises and self-employed persons to whom it is appropriate to give the same protection as workers considering the nature of their business may be covered by the workers’ compensation insurance. Entry into the insurance system is allowed to employers of small and medium-sized enterprises which entrust insurance procedures to a labour insurance business association, as well as to the self-employed who join an organization capable of executing insurance procedures.
Workers who are dispatched overseas by employers in Japan or dispatched as representatives for overseas small and medium-sized enterprises are covered.
Description of the System
History
The need for compensating workers for on-the-job injury was first noted by the Factory Law (1911) and the Mine Law (1905). These laws stipulated that employers were responsible for providing sufferers of industrial injuries with assistance. The Health Insurance Law (1922) covered short-term injuries incurred on or outside the job by workers engaged in enterprises to which these laws were applicable. The coverage was later extended to long-term injuries and to civil engineering, construction and transportation workers. A new stage began when the two principal laws described below were enacted in 1947, following the termination of the Second World War. The Labour Standards Law introduced for the first time the idea of employers’ liability and compensation in place of “assistance” in the case of employment injury. The Workmen’s Accident Compensation Insurance Law set up insurance within the jurisdiction of the newly established Ministry of Labour. The insurance system has been improved by repeated revisions of the law. It operates as a system independent from the social security programmes of the country.
Types of insurance coverage
Workmen’s Accident Compensation Insurance is a state insurance system administered by the government. The scope of the insurance extends to all on-the-job accidents and diseases and commuting accidents. It covers both medical and cash income benefits. The medical and rehabilitation costs for workers suffering from injuries or diseases covered by this system are paid by the insurance, a separate treatment not covered by health insurance schemes.
Employers covered by Workmen’s Accident Compensation Insurance are no longer liable for compensation stipulated by the Labour Standards Law for cases compensated by this insurance. However, there are collective agreements that provide for supplementary compensation beyond the levels provided by the state insurance. Furthermore, there are a number of private enterprises that join the compensation insurance schemes managed by private insurance companies.
Disputes about the amount of supplementary compensation for victims of occupational injuries and disease and their families are often brought before the court.
All types of employment and commuting injuries are covered. As for diseases, there is a list of occupational diseases attached to Article 35 of the Enforcement Ordinance of the Labour Standards Law (revised in 1978). The list is comprehensive and covers in effect all types of work-related diseases. The following nine categories are mentioned:
- diseases caused by injury resulting from employment
- diseases caused by physical agents (13 items)
- diseases caused by specific forms of work performance in which an extreme physiological tension is involved (5 items)
- diseases caused by chemical substances and others (8 items)
- pneumoconiosis caused by work in places where dust is dispersed, and diseases complicated by pneumoconiosis stipulated by the Enforcement Ordinance of the Pneumoconiosis Law (1960)
- diseases caused by bacteria, viruses and other pathogenic organisms (5 items)
- diseases caused by carcinogenic substances or agents, or work performed in a carcinogenic manufacturing process (18 items)
- other diseases designated by the Minister of Labour
- other diseases apparently caused by work.
Role of social partners
Development of compensation principles
Workmen’s Accident Compensation Insurance started as an insurance system financed wholly by employers. Partial payment by the government began in 1960, when long-term injury and disease compensation was adopted and lump sum payment was replaced with annuity payment for the physically handicapped. In 1965, government subsidies were introduced for the expenses of administering the workers’ compensation insurance and for insurance payments. This was accomplished by serial amendments of the Workmen’s Accident Compensation Law, which in the beginning was applicable only to enterprises regularly employing five or more workers, except part of the agriculture, forestry and fishery industries. Any such enterprise is obliged to automatically join the insurance system as soon as its business starts. Administration of the insurance system is supervised by the Bureau of Labour Standards of the Ministry of Labour. Penalties are applied in the case of violations. Thus the roles of employers and workers are basically what they were at the beginning of the system.
The benefits received by the injured workers and the bereaved families have been improved by several modifications of the law. These modifications improved long-term benefits and bereaved family compensation pensions, introduced the sliding scale of payments as determined by wage level changes, extended benefits to all commuting accidents, and established the special supplement system and the labour welfare services in 1976. In 1981, the adjustment rules between the workers’ compensation insurance benefit and the civil damage compensation were established. Nursing compensation benefits are being introduced.
Deciding whether an injury or disease is because of work duty is based on administrative interpretations. Those who are not satisfied with the decisions may demand an examination or arbitration by a Workmen’s Accident Compensation Insurance examiner appointed by the Minister of Labour. If they are not satisfied with the examiner’s decision, they may demand a re-examination of their case by the Labour Insurance Council. Those who are dissatisfied with the council’s decision can file a suit in court.
Mechanism for updating
The terms of operation of the insurance system are approved by the Council of Workmen’s Accident Compensation Insurance, in which employers, workers and academia are represented. The development of the system and modifications of insurance benefits are examined by the council. As a result, the Workmen’s Accident Compensation Insurance Law was revised several times as mentioned above.
Decisions of the appeal and the civil court systems concerning compensation cases contribute to updating of benefit levels and criteria.
Finances
The government collects the insurance premium from employers. The premium is calculated by multiplying the total wages payable to all the workers in the enterprise in the insurance year by the premium rate. This premium rate is determined for each category of enterprise, taking into account the past accident rates and other factors. A merit system is applied in determining the premium rate for different industries. The premium rates as of April 1992 for different industries are given in table 1.
Table 1. Premium rates of workmen’s accident compensation insurance in Japan (April 1992)
|
Industry |
Types of undertaking |
Premium rate |
|
Forestry |
Felling and transport of wood |
0.142 |
|
Others |
0.041 |
|
|
Fishery |
Sea fishery (except below) |
0.067 |
|
Fishery by stationary nets or by culture |
0.042 |
|
|
Mining |
Coal mining |
0.111 |
|
Metal and non-metal mining |
0.099 |
|
|
Others other than below |
0.040-0.072 |
|
|
Petroleum or natural gas mining |
0.010 |
|
|
Construction |
New construction or power plants and tunnels |
0.149 |
|
New construction of railroads |
0.068 |
|
|
New construction of roads |
0.049 |
|
|
Others |
0.025-0.038 |
|
|
Manufacturing |
Ceramics |
0.020-0.027 |
|
Wood products |
0.026 |
|
|
Ship building and repair |
0.023 |
|
|
Metal products |
0.022 |
|
|
Foundry |
0.021 |
|
|
Others |
0.006-0.018 |
|
|
Transport |
Ship loading/unloading |
0.053 |
|
Other kinds of cargo handling in ports |
0.029 |
|
|
Freight handling other than above |
0.019 |
|
|
Traffic and transportation |
0.007 |
|
|
Supply of electicity, gas, water or heat |
0.006 |
|
|
Others |
Cleaning,, cremation or meat-processing |
0.014 |
|
Others |
0.006-0.012 |
Special exceptional measures to increase or decrease the premium rate determined throughout the merit system are to be applicable starting in 1997 to small and medium-sized enterprises that have taken special measures to secure the safety and health of workers.
The injured workers or bereaved families are expected to provide the information necessary for demanding the insurance payment. The workers who receive the medical benefit for commuting injuries must have contributed to the expenses up to the limit of two hundred yen for the first medical treatment.
Prevention
Some preventive measures are undertaken as part of the labour welfare services within the Workmen’s Accident Compensation Insurance. These include:
- establishing and managing occupational health centres; and
- supporting industrial safety and health associations.
As a result, a variety of preventive activities are supported by means of the insurance funds.
Summary of Cost Experience
The changes in the numbers of enterprises and workers covered by the workers’ compensation system and the total annual amount of insurance payments are indicated in table 2. It should be noted that sliding scales of pension rates were first applied in 1983 and that the lowest and highest limits of average daily wage of temporary disability benefit for those who need prolonged care were established in 1990. The table shows that the number of workers covered by the insurance system has been steadily increasing, but that the number of cases receiving insurance payments has decreased since 1988.
Table 2. Enterprises and workers where the workmen’s accident compensation insurance was applicable and amount of benefits in Japan
|
Fiscal year (April-March) |
Number of applicable |
Number of applicable workers (thousand) |
Amount of insurance benefits |
Number of |
|
1960 |
808 |
16,186 |
27,172 |
874 |
|
1965 |
856 |
20,141 |
58,372 |
1,341 |
|
1970 |
1,202 |
26,530 |
122,019 |
1,650 |
|
1975 |
1,535 |
29,075 |
287,640 |
1,099 |
|
1980 |
1,840 |
31,840 |
567,288 |
1,099 |
|
1985 |
2,067 |
36,215 |
705,936 |
902 |
|
1986 |
2,110 |
36,697 |
724,260 |
859 |
|
1987 |
2,177 |
38,800 |
725,922 |
847 |
|
1988 |
2,270 |
39,725 |
733,380 |
832 |
|
1989 |
2,342 |
41,249 |
741,378 |
818 |
|
1990 |
2,421 |
43,222 |
753,128 |
798 |
|
1991 |
2,492 |
44,469 |
770,682 |
765 |
|
1992 |
2,542 |
45,832 |
791,626 |
726 |
|
1993 |
2,577 |
46,633 |
799,975 |
696 |
|
1994 |
2,604 |
47,008 |
806,932 |
675 |
In 1994, 25% of the total insurance benefits were for medical benefits, 14% for temporary disability benefits, 6% for physical handicaps compensation lump sum, 39% for pension and 14% for special grants. The distribution of the insurance benefits by industry is given in table 3.
Table 3. Payment of insurance benefits by industry in Japan
|
Industry |
Applicable plants1 |
Applicable workers1 |
Amount of insurance benefits2 |
|||
|
Number |
(%) |
Number |
(%) |
(Thousand yen) |
(%) |
|
|
Forestry |
26,960 |
(1.0) |
126,166 |
(0.3) |
33,422,545 |
(4.2) |
|
Fishery |
6,261 |
(0.3) |
56,459 |
(0.1) |
3,547,307 |
(0.4) |
|
Mining |
6,061 |
(0.2) |
55,026 |
(0.1) |
58,847,081 |
(7.3) |
|
Construction |
666,500 |
(25.6) |
5,886,845 |
(12.5) |
268,977,320 |
(33.6) |
|
Manufacturing |
544,275 |
(20.9) |
11,620,223 |
(24.7) |
217,642,629 |
(27.2) |
|
Transportation |
70,334 |
(2.7) |
2,350,323 |
(5.0) |
64,536,818 |
(8.1) |
|
Supply of electricity, gas, water or heat |
1,962 |
(0.1) |
188,255 |
(0.4) |
1,344,440 |
(0.2) |
|
Others |
1,281,741 |
(49.2) |
26,724,978 |
(56.9) |
151,657,177 |
(19.0) |
|
Total |
2,604,094 |
(100%) |
47,008,275 |
(100%) |
799,975,317 |
(100%) |
1 As of end of the 1994 fiscal year.
2 As of end of the 1993 fiscal year.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."