- You are here:
-
Home

-
Contents
-
Part X. Industries Based on Biological Resources
-
Paper and Pulp Industry
- Major Sectors and Processes
Safety and Ergonomics in Airframe Manufacturing
Safety Management
The airframe manufacturing industry’s safety management systems have reflected the evolutionary process of safety management within the traditional manufacturing setting. The health and safety programmes tended to be highly structured, with the company executives directing health and safety programmes and a hierarchical structure reflective of the traditional command and control management system. The large aircraft and aerospace companies have staffs of safety and health professionals (industrial hygienists, health physicists, safety engineers, nurses, physicians and technicians) that work with line management to address the various safety risks that are found within their manufacturing processes. This approach to line control safety programmes, with the operational supervisor responsible for the daily management of risks, supported by a core group of safety and health professionals, was the primary model since the establishment of the industry. The introduction of detailed regulations in the early 1970s in the United States caused a shift to a greater reliance on the safety and health professionals, not only for programme development, but also implementation and evaluation. This shift was a result of the technical nature of standards that were not readily understood and translated into the manufacturing processes. As a result, many of the safety management systems changed to compliance-based systems rather than injury/illness prevention. The previously integrated line control safety management programmes lost some of their effectiveness when the complexity of regulations forced a greater reliance on the core safety and health professionals for all aspects of the safety programmes and took some of the responsibility and accountability away from line management.
With the increasing emphasis on total quality management throughout the world, the emphasis is again being placed back on the manufacturing shop floor. Airframe manufacturers are moving to programmes that incorporate safety as an integral component of a reliable manufacturing process. Compliance takes on a secondary role, in that it is believed that while focusing on a reliable process, injury/illness prevention will be a primary objective and the regulations or their intent will be satisfied in establishing a reliable process. The industry as a whole currently has some traditional programmes, procedural/engineered-based programmes and emerging applications of behaviour-based programmes. Regardless of the specific model, those demonstrating the greatest success in injury/illness prevention require three critical components: (1) visible commitment by both management and the employees, (2) a clearly stated expectation of outstanding performance in injury/illness prevention and (3) accountability and reward systems, based on both endpoint measures (such as injury/illness data) and process indicators (such as per cent safety behaviour) or other proactive prevention activities that have equal weighting with other critical organization goals. All of the above systems are leading to a positive safety culture, which is leadership driven, with extensive employee involvement in both the process design and process improvement efforts.
Physical Safety
A substantial number of potentially serious hazards can be encountered in the airframe manufacturing industry largely because of the sheer physical size and complexity of the products produced and the diverse and changing array of manufacturing and assembly processes utilized. Inadvertent or inadequately controlled exposure to these hazards can produce immediate, serious injuries.
Table 1. Aircraft and aerospace industry safety hazards.
| Type of hazard | Common examples | Possible effects |
| Physical | ||
| Falling objects | Rivet guns, bucking bars, fasteners, hand tools | Contusions, head injuries |
| Moving equipment | Trucks, tractors, bicycles, fork-lift vehicles, cranes | Contusions, fractures, lacerations |
| Hazardous heights | Ladders, scaffolding, aerostands, assembly jigs | Multiple serious injuries, death |
| Sharp objects | Knives, drill bits, router and saw blades | Lacerations, puncture wounds |
| Moving machinery | Lathes, punch presses, milling machines, metal shears | Amputations, avulsions, crush injuries |
| Airborne fragments | Drilling, sanding, sawing, reaming, grinding | Ocular foreign bodies, corneal abrasions |
| Heated materials | Heat-treated metals, welded surfaces, boiling rinses | Burns, keloid formation, pigmentation changes |
| Hot metal, dross, slag | Welding, flame cutting, foundry operations | Serious skin, eye and ear burns |
| Electrical equipment | Hand tools, cords, portable lights, junction boxes | Contusions, strains, burns, death |
| Pressurized fluids | Hydraulic systems, airless grease and spray guns | Eye injuries, serious subcutaneous wounds |
| Altered air pressure | Aircraft pressure testing, autoclaves, test chambers | Ear, sinus and lung injuries, bends |
| Temperature extremes | Hot metal working, foundries, cold metal fabrication work | Heat exhaustion, frostbite |
| Loud noises | Riveting, engine testing, high-speed drilling, drop hammers | Temporary or permanent loss of hearing |
| Ionizing radiation | Industrial radiography, accelerators, radiation research | Sterility, cancer, radiation sickness, death |
| Non-ionizing radiation | Welding, lasers, radar, microwave ovens, research work | Corneal burns, cataracts, retinal burns, cancer |
| Walking/working surfaces | Spilled lubricants, disarranged tools, hoses and cords | Contusions, lacerations, strains, fractures |
| Ergonomic | ||
| Work in confined spaces | Aircraft fuel cells, wings | Oxygen deprivation, entrapment, narcosis, anxiety |
| Forceful exertions | Lifting, carrying, tub skids, hand tools, wire shop | Excess fatigue, musculoskeletal injuries, carpal tunnel syndrome |
| Vibration | Riveting, sanding | Musculoskeletal injuries, carpal tunnel syndrome |
| Human/machine interface | Tooling, awkward posture assembly | Musculoskeletal injuries |
| Repetitive motion | Data entry, engineering design work, plastic lay up | Carpal tunnel syndrome, musculoskeletal injuries |
Adapted from Dunphy and George 1983.
Immediate, direct trauma can result from dropped rivet bucking bars or other falling objects; tripping on irregular, slippery or littered work surfaces; falling from overhead crane catwalks, ladders, aerostands and major assembly jigs; touching ungrounded electrical equipment, heated metal objects and concentrated chemical solutions; contact with knives, drill bits and router blades; hair, hand or clothes entanglement or entrapment in milling machines, lathes and punch presses; flying chips, particles and slag from drilling, grinding and welding; and contusions and cuts from bumping against parts and components of the airframe during the manufacturing process.
The frequency and severity of injuries related to the physical safety hazards have been reduced as the industry’s safety processes have matured. The injuries and illnesses related to ergonomically related risks have mirrored the growing concern shared by all manufacturing and service-based industries.
Ergonomics
The airframe manufacturers have a long history in the use of human factors in developing critical systems on their product. The pilots’ flight deck has been one of the most extensively studied areas in product design history, as human factors engineers worked to optimize flight safety. Today, the fast-growing area of ergonomics as it pertains to injury/illness prevention is an extension of the original work done in human factors. The industry has processes that involve forceful exertions, awkward postures, repetitiveness, mechanical contact stress and vibration. These exposures can be exacerbated by work in confined areas such as wing interiors and fuel cells. To address these concerns, the industry is using ergonomists in product and process design, as well as “participatory ergonomics”, where cross-functional teams of manufacturing employees, supervision and tooling and facility designers are working together to reduce ergonomic risks in their processes.
In the airframe industry some of the key ergonomic concerns are the wire shops, which require many hand tools to strip or crimp and require strong grip forces. Most are being replaced by pneumatic tools that are suspended by balancers if they are heavy. Height-adjustable workstations to accommodate males and females provide options to sit or stand. Work has been organized into cells in which each worker performs a variety of tasks to reduce fatigue of any particular muscle group. In the winglines, another key area, padding of tooling, parts or workers is necessary to reduce mechanical contact stress in confined areas. Also in the wingline, height-adjustable work platforms are utilized instead of stepladders to minimize falls and place workers in neutral posture to drill or rivet. Riveters are still a major area of challenge, as they represent both a vibration and forceful exertion risk. To address this, low-recoil riveters and electromagnetic riveting are being introduced, but due both to some of the performance criteria of the products and also the practical limitations of these techniques in some aspects of the manufacturing process, they are not universal solutions.
With the introduction of composite materials both for weight and performance considerations, hand lay-up of composite material has also introduced potential ergonomic risks due to the extensive use of hands for forming, cutting and working the material. Additional tools with varying grip size, and some automated processes, are being introduced to reduce the risks. Also, adjustable tooling is being used to place the work in neutral posture positions. The assembly processes bring about an extensive number of awkward postures and manual handling challenges that are often addressed by the participatory ergonomics processes. Risk reductions are achieved by increased use of mechanical lifting devices where feasible, re-sequencing of work, as well as establishing other process improvements that typically not only address the ergonomic risks, but also improve productivity and product quality.
Employment Injuries Insurance and Compensation in Israel
Summary of Coverage and Goal
Coverage
The workers’ accident compensation system in Israel is controlled and managed by the National Insurance Institute and is based on the National Insurance Law, Consolidated version (1995-5755), Chapter 5, “Employment Injuries Insurance”.
Insured persons and conditions of insurance
The workers’ accident compensation system is applied compulsorily to all employers to insure their employees (except for policemen, jailers and defence employees)—those regularly or temporarily employed, for daily or monthly wages, full time or part time, including: self-employed persons, vocational trainees, foreign residents employed in Israel, working prisoners, persons undergoing vocational rehabilitation, Israeli residents working abroad for an Israeli employer (under certain conditions), and persons whose salary is determined by law (such as Knesset members, judges, mayors), regardless of the age or nationality of the workers.
Hazards covered
This law grants benefits in order to protect the workers promptly and fairly against work-related accidents, occupational disease, disability or death.
If an insured person dies as a result of an employment injury (work accident or occupational disease), his or her relatives—widow/widower, orphans, parents and any other relatives (hereinafter called dependants)—under special conditions are entitled to employment injury benefits.
The term employment injury is applied to injuries, disabilities or deaths resulting from employment. The term work accident means an accident “which occurred in the course and as a consequence of the work and/or on behalf of the worker’s employer”. The definition in the case of a self-employed person is different and is “in the course and in consequence of the pursuit of his occupation”.
The insurance applies also to an accident that occurred to the insured person while driving, riding or walking to the workplace from home, or from the place he or she stayed overnight, or from work to home, or from one workplace to another, even if the harm caused to the employee occurred because of road hazards, so long as the demands or needs of the employee’s work constitute the main reason for the employee’s presence at the scene of the accident.
The insurance also applies to occupational diseases, defined in article 2 of Employment Injuries Insurance.
Occupational disease is defined as a disease contracted as a consequence of work or while acting on behalf of the employers, or, in the case of a self-employed person, in consequence of the pursuit of his or her occupation.
The occupational diseases are specified in a list recognized by the Institute and published in the Bylaws (regulations).
The list includes those diseases caused by injury resulting from employment and diseases caused by physical, chemical or biological agents or specific forms of work performance, and those apparently caused by work.
All employees are covered by the insurance, without exception. Every employer must insure his or her workers under each category.
Insurance coverage is mandatory also on the Government as employer, and includes all public employers.
Eligibility
Who is eligible
- An insured person who suffers a work injury (work accident or occupational disease) is entitled to injury allowance.
- An insured person who becomes an invalid as a result of a work injury is eligible for a pension or grant.
- An insured person with a 10 per cent or higher medical disability is eligible for vocational rehabilitation. For the way the extent of the disability is determined, see below.
Conditions of entitlement for work injury benefits
Injury allowance is granted to the insured person who was injured at work or became ill with occupational disease and as a result is unable to do either the original job or any other suitable work, and did not work in fact.
Work Invalidity Benefits Grant or Pension (hereinafter called disability benefits) are paid as long as the disability has been recognized as being due to a work accident and the insured person remains disabled as a result of the injury.
The results of the injury are evaluated by comparing the fitness of the person injured at work with the fitness of a healthy person of the same age and sex. The tests determining degree of disability are a combination of the fixed percentages for each injury, taking subjective consideration into account; the loss of a particular limb is of greater weight in certain professions.
The degree of disability is determined by medical boards, of which there are two categories:
- boards of the first instance
- appeal boards.
The boards first determine the causal connection between the work accident (injury or occupational disease) that had to be recognized for disability purposes and the degree of the causal connection. The medical boards are independent of the body that confronts them. The medical boards are quasi-legal bodies and give rulings rather than implementing administrative action. Being quasi-legal bodies, the medical boards are subject to the control of the labour courts.
Dependants’ benefits (pensions or grants)
To be entitled to dependants’ pension, a widow must be 40 years old or over, or have a child living with her, or be unable to support herself; a widower must have a child living with him. Definition of child: Child of the insured person up to the age of 18, and up to the age of 22 in certain cases.
Vocational rehabilitation
To be entitled to vocational rehabilitation, the insured person, due to work injury, must be unable to perform the previous work or job, or any other suitable work, and be in need of and suited for vocational rehabilitation.
Insurance contributions by the self-employed
Arrears in insurance contributions rule out eligibility or reduce the rate of monetary benefits. A self-employed person not registered as such in the National Insurance Institute at the time of the injury is not eligible for benefits.
Types of benefits (payments)
The insured person is entitled to two main types of benefits under the National Insurance Law in the event of work injuries or disease:
Benefits in kind
Benefits in kind include medical attention, convalescence facilities, and medical and vocational rehabilitation.
Medical attention includes hospitalization, medications and supply, repair and replacement of orthopaedic and therapeutic appliances. The medical attention in general is provided to the extent necessitated by the work injury and its effects during the life of the insured. In fact, the medical attention is supplied on behalf of the Institute by the approved Sick Funds, recognized as approved medical service. Vocational rehabilitation is provided by the Institute either directly or through the services of other bodies.
Benefits in cash
Injury allowance: This is payment for a period of incapacity to work as a result of work injury, for a maximum period of 182 days beginning the day after the injury, calculated by day, on the basis of 75% of wages liable for insurance contributions in the quarter-year prior to the injury. The daily injury allowance has a maximum limit (see table 1).
Table 1. Recipients of work injury benefits in Israel
|
Period |
Dependants’ pension1 |
Permanent disability pensions1 |
Injury benefits1 |
Period |
||||||
|
Number of days paid for |
Number of injured |
|||||||||
|
Self- |
Employees |
Self- |
Employees |
Self- employed |
Employees |
Self-employed |
Employees |
|||
|
1965 |
891 |
150 |
1,766 |
132,948 |
747,803 |
6,455 |
54,852 |
1965 |
||
|
1975 |
2,134 |
508 |
4,183 |
237,112 |
1,067,250 |
10,819 |
65,291 |
1975 |
||
|
1980 |
382 |
2,477 |
950 |
6,592 |
23,617 |
1,017,877 |
10,679 |
63,234 |
19802 |
|
|
1985 |
445 |
2,841 |
1,232 |
8,640 |
165,635 |
921,295 |
6,619 |
50,302 |
1985 |
|
|
1986 |
455 |
2,883 |
1,258 |
8,760 |
169,035 |
964,250 |
6,472 |
51,351 |
1986 |
|
|
1987 |
470 |
2,911 |
1,291 |
9,078 |
183,961 |
1,026,114 |
6,959 |
50,075 |
1987 |
|
|
1988 |
468 |
2,953 |
1,229 |
9,416 |
172,331 |
1,004,906 |
6,683 |
47,608 |
1988 |
|
|
1989 |
481 |
2,990 |
1,375 |
9,824 |
240,995 |
1,126,001 |
8,259 |
51,197 |
1989 |
|
|
1990 |
490 |
3,022 |
1,412 |
10,183 |
248,234 |
1,159,645 |
5,346 |
51,367 |
1990 |
|
|
1991 |
502 |
3,031 |
1,508 |
10,621 |
260,440 |
1,351,342 |
8,470 |
55,827 |
1991 |
|
|
1992 |
520 |
3,078 |
1,566 |
11,124 |
300,034 |
1,692,430 |
9,287 |
64,926 |
1992 |
|
|
1993 |
545 |
3,153 |
1,634 |
11,748 |
300,142 |
1,808,848 |
8,973 |
65,728 |
1993 |
|
|
1994 |
552 |
3,200 |
1,723 |
12,520 |
351,905 |
2,134,860 |
9,650 |
71,528 |
1994 |
|
|
1995 |
570 |
3,260 |
1,760 |
12,600 |
383,500 |
2,400,000 |
9,500 |
73,700 |
1995 |
|
1 For disability and dependants’ pension, the annual figure is the number of recipients in April for each year. For injury benefits it is the total number of recipients during the year.
2 As of 1980, the annual figure given under payment disability pensions is a monthly average of recipients.
Injury allowance is not paid for the first two days after the day of injury, unless the injured person was not capable of working for at least 12 days.
Work disability benefit (work disability pension): This covers those with a disability of 20% and over—a monthly pension according to the degree of medical disability, at a rate proportionate to wages and degree of disability. Recipients of disability pensions who belong to low-income groups receive an additional “income support” supplement (see table 1).
Work disability grant: This covers those with a disability of 5 to 19%—a one-time grant equivalent to the daily injury allowance 21 ´ the percentage disability.
Special pension: This covers those with a disability of 75% and over, and those with a disability of 65 to 74% who have difficulty in walking; provides financial aid for personal expenses and transportation, up to a maximum determined by law.
Special grant: This covers those with a disability of 75% and over, and those with a disability of 65 to 74% with difficulty in walking; provides aid in purchasing a car (under special conditions), aid in solving housing problems and acquiring special accessories needed due to the disability.
Vocational rehabilitation payment: This covers aid in diagnosis and professional guidance, rehabilitation allowance during period of studies (as a supplement to disability pension) and various expenses connected with studies, such as travel, tuition and learning materials; in special cases, a grant is given for the purchase of work tools.
Benefits to dependants
Dependants’ pension: This amounts to 40 to 100% of the full pension that the insured person would have been entitled to, had he or she been 100% disabled—taking into consideration the number of children. Recipients of dependants’ pensions who belong to low-income groups receive an additional “income support” supplement (see table 1).
Dependants’ grant: This goes to a widow who has no children at home and who was not yet 40 years of age upon the death of the insured spouse—a grant equivalent to 36 months of dependant’s pension.
Marriage grant: This goes to a widow or widower who remarries—a grant equivalent to 36 monthly pension payments, paid in two instalments—the first one right after remarriage, the second two years after remarriage (right to survivor’s benefit expires).
Vocational rehabilitation: This covers vocational studies, in the form of vocational training, payment of maintenance allowance during period of study, and various expenses connected with studies.
Maintenance allowance for orphans: This goes to a child who spends most of his or her time studying in high school or in vocational training—9% of the average wage as it was on 1 January, subject to a means test of the parent. Maintenance allowance is updated by the rate of the compensation paid in the course of the year.
Bar-Mitzvah grant: This goes to a boy reaching the age of 13 and a girl reaching the age of 12, at the rate of 2/3 of the average wage as it was on 1 January, updated by the rate of the compensation paid in the course of the year.
Grant following decease: At the decease of a disabled person who had a disability of 50% or over, to whom a disability pension had been paid, or at the decease of a disabled person who was at least 65 years of age (man) or 60 years of age (woman), or at the decease of a person who had received a dependant’s allowance—a lump sum equal to the average wage as it was on 1 January preceding the day of decease, updated by the rate of the compensation paid in the course of the year, to the spouse of the deceased (or in absence thereof, to child). To recipients of income supplement, the grant is equal to 150% of the average wage as stated.
Other aspects
Rehabilitation
The main scope of the Employment Injuries Insurance is to advance the welfare of the injured persons by encouraging them to return to work. Therefore the Institute supports the services of vocational rehabilitation to the disabled persons with a medical disability of 10% or more. Furthermore, the disabled is entitled to any extra income from work without affecting his or her right to the disability pension from the Institute.
Extension of coverage
As mentioned above, persons insured by the Institute include those who are not workers in the narrow meaning of this word, such as self-employed, vocational trainees and so on.
Description of the system
History
The first labour law promulgated during the British Mandate in Palestine (1922 to 1948) was the Workmen’s Compensation Ordinance 1922. This was replaced in 1947 by a more modern law based on the English Law of 1925. The main advantage of these laws was that through their interpretation the English innovations in the field of workers’ compensation were introduced in Israel.
The laws mentioned above were in force until 1 April 1954, when the Knesset passed the National Insurance Law 1954. This law authorized the National Insurance Institute to act according to the provisions of the law. The National Insurance Law was the first comprehensive social security law to include a wide range of National Insurance and statutory allowance programmes which were almost non-existent until the National Insurance Law came into effect.
The Law included three main branches of insurance benefits:
- old age and survivors’ insurance
- employment injury insurance
- maternity insurance.
Through the years, the National Insurance Law has been amended many times. The main amendments connected with workers’ compensation are:
- including the self-employed in the insurance system (1957)
- “work accident” was expanded to include accidents occurring while walking or driving to work.
Types of coverage
Workers’ compensation insurance for employment injury is administered by the National Insurance Institute. The insurance covers both cash benefits and benefits in kind for work accidents. Employers who contribute to the insurance of the employees are no longer liable under the law of Torts. However, they may be liable in case of negligence. Benefits paid by the National Insurance are deducted from the compensation received by the employee.
Besides covering work injuries, the Institute covers occupational diseases. There is a list of occupational diseases attached as the second appendix to Regulations 44 and 45 of the Regulations of Work Accidents Insurance. The list is almost comprehensive and in effect covers 49 types of work-related diseases. The system of recognition for occupational diseases is a mixed system. This includes the occupational diseases listed, but other diseases of occupational origin can, subject to certain conditions, also be compensated.
According to the National Insurance Law, “occupational disease” means a disease defined by the Law (Chapter 85) as an occupational disease and contracted as a consequence of work or on behalf of his or her employment or, in the case of a self-employed person, as a consequence of his or her occupation.
Some compensation principles
The main role of the Workers’ Compensation Law is that the injured person is entitled to the benefits granted by the law, whether his or her employer contributed to the Institute or not, and the injured worker is eligible to file a claim for these benefits.
The Claims Officer of the Institute is empowered by the Board of the National Insurance to decide whether an injury or work-related disease claim is valid. If claimant is dissatisfied with the decision, he or she can file a suit with the Labour Court and have the right to appeal to the National Labour Court of Appeal.
The applicant in the proceedings in the labour courts, in accordance with professional decision, is granted free legal aid by the National Insurance Institute.
Mechanism for updating benefits
Employment Injury Benefits are adjusted from the 91st day in relation to the increase of the average wage on 1 January following the payment and during the year in relation to the wage increase received by workers due to inflation.
Injury Allowance (182 days) is taxable at source. Disability and long-term benefits are updated according to the cost of living increment and according to the changes that took place in the average wage as it was on 1 January. Disability and long-term benefits are not taxable.
When an insured person reaches entitlement to old-age pension (65 years for men, 60 for women), he or she can choose between the two forms of benefits.
Finance—Contributions
All employers must contribute for their employees. Where an insured person is employed by several employers, each of them shall contribute as it he were the only employer. Self-employed and persons who are neither employees nor self-employed must contribute for themselves. The employer contributes to the National Insurance Institute. The average rate until 31 March 1970 ranged between 0.5 per cent and 3.0 per cent, and from 1 April 1971, between 0.7 and 4.0 per cent. From 1 October 1981 the minimum rate was 0.7 per cent and the maximum 2.4 per cent. From 1 July 1986, the standard rate of insurance contributions (0.7 per cent) has been determined without regard to the extent of risk in the various industries, as it was before 1986. As of 1 April 1987, the level of rates has been decreased due to low labour costs.
The rates of monthly contribution in the case of an employee shall be the percentage of the amount of his or her monthly income. In the case of other persons, the percentage shall be based on quarterly income.
The contributions are subject to maximum and minimum income of the insured. The maximum income for collection of contribution is calculated as four times the average wage for employees and for non-employees.
There are in the National Insurance Law certain exemptions from payment of contributions, such as an employee who received injury benefits for the time he or she received the benefits.
Prevention
The National Insurance Law does not concern itself with work-related accident prevention. Paragraph 82 of the National Insurance Law refers to injuries caused by negligence of the insured person. Sanctions are applied in the form of non-payment of benefits where the insured is unable to work for less than ten days.
The National Insurance Institute contributes to associations in the field of accident prevention, such as the Institute of Occupational Safety and Hygiene.
The National Insurance Institute maintains a fund to support the financing of activities aimed at preventing work accidents, such as research and the development of experimental means broadly applicable in areas such as safety, engineering, medicine, and industrial chemistry and hygiene.
Prevention, Rehabilitation and Compensation in the German Accident Insurance System
Foundations and Development
The statutory accident insurance system was introduced as an independent branch of social security by the accident insurance law of 1884 and has existed since 1885. It has the following legal responsibilities:
- The accident insurance system, using all appropriate means, should assist in preventing work-related accidents and occupational diseases. In the future, this role should be expanded.
- In the event of a workplace accident or the onset of an occupational illness, the system has the task of providing comprehensive compensation for injury or damages. In this capacity, the primary goal is to restore the health of the insured to the extent possible and to re-integrate the insured into occupational and social life (medical, occupational and social rehabilitation). Permanent health problems, furthermore, are to be compensated through annuity payments. If the case results in death, the survivors receive pensions and other monetary benefits.
In the course of its development, the system has been continually amended and expanded in many respects. This refers in particular to the enterprises covered (all-inclusive since 1942), the groups insured (e.g., the inclusion of schoolchildren, students and kindergarteners in 1971), the types of claims (1925 extension to include commuting accidents, accidents that occur while operating equipment at work, and occupational diseases) and indexation of monetary benefits (comprehensive since 1957). The continual improvement of measures, methods and practices for prevention and rehabilitation is also of great significance.
Structure and Organization
The implementation of accident insurance is currently conferred by law upon 110 accident insurance carriers (Berufgenossenshaften). These are organized in the public law, mostly as “corporations of public law”. Three domains are to be distinguished:
- industrial accident insurance (including insurance for accidents at sea) with 35 carriers organized by industrial branch (e.g., mining, chemical, trade or health-care system)
- agricultural accident insurance, with 21 regionally organized carriers
- accident insurance for the public sector with 54 carriers that correspond for the most part to governmental divisions (federal, state and municipal groups, with separate funds for the postal service, railways and fire departments).
The most significant sector—industrial accident insurance—is given the most attention in the following discussion. As corporations of public law, the (Berufgenossenshaften) come under governmental administration and, as such, are part of the legal system . On the other hand, they are independent and self-governing in many respects. Both organs of self-administration, the assembly of representatives and the board of directors for each carrier are composed in equal proportion of employer and employee representatives chosen through elections. They make the decisions necessary to apply accident insurance within the legal framework. Whereas the preconditions for and scope of insurance benefits are regulated by law in individual cases, the accident insurance system preserves considerable self-administrative, decision-making latitude in setting premiums and especially in the area of prevention, which the self-administration fills out with concretizing and organizational regulations. The administrative organs of the (Berufgenossenshaften) also decide questions of organization, personnel and budget. Supervision by government authorities ensures that the decisions of the self-administration and administrative personnel are in accordance with the law.
Trends in Accident Rates and Finances
The number of work-related and commuting accidents decreased continuously over many years—until the increase due to the incorporation of the new federal state in 1991. The trend for the industrial accident insurance system can be summarized as follows: the accident rate—that is, the frequency of reportable work-related and commuting accidents per 1,000 full-time workers—decreased to less than half between 1960 and 1990. This positive trend can be even more clearly demonstrated in the case of severe accidents leading to compensation through annuities: a drop of nearly two-thirds in the accident rate. Fatal accidents fell by approximately three-quarters. Occupational diseases diverge from this trend and showed no uniform pattern of change during this time period. As new occupational diseases were progressively added to the list of occupational diseases, the number of cases of occupational diseases has increased, both with respect to prevention and rehabilitation.
The general decrease in the number and severity of accident insurance cases favourably affected costs. On the other hand, the following factors contributed to the increase in costs: indexing of monetary benefits, the general increase in health care costs, the expansion of persons insured, the broadening of insurance coverage—especially for occupational diseases—and the efforts to improve and intensify preventive and rehabilitative measures of the system. Altogether, the expenditures rose less than the salary base that is used to calculate the premiums. The average industrial accident insurance premium decreased from 1.51% in 1960 to 1.36% in 1990. As a result of the costs associated with German reunification, the average premium rose to 1.45% in 1994.
The distribution of costs for the three areas of responsibility (prevention, rehabilitation and financial compensation) have shifted in the following manner from 1960 to 1994:
- The costs of prevention increased from 2.6 to 7.1%. This is attributable to the steady improvement, intensification and expansion of preventive measures of the system.
- The portion of rehabilitation costs (including payments) rose from 20.4 to 31.2%. In this area, the increase of costs in the health-care industry cannot be absorbed by the decrease in accident frequency alone.
- The portion of costs for annuities and pensions decreased from 77% to 61.7%. Despite indexation of annuities and pensions, this did not increase to the same extent as did the rehabilitation costs.
In other branches of the German social security system, the burden of premiums rose considerably during this time. On average, the cost of premiums for all branches of social insurance in the German Federal Republic was DM25.91 per DM100 wages in 1960; this figure rose to DM40.35 per DM100 paid by 1994. The portion of the average accident insurance premium to the premium burden of the total social insurance system decreased from 5.83% in 1960 to 3.59% in 1994. The proportion of accident insurance to the gross national product remained at approximately 0.5%. Thus only in the area of accident insurance could the economy be relieved to a certain extent of social taxes.
A decisive cause for this positive trend was the decrease in frequency and severity of accidents, as depicted above. In addition, the accident insurance system has succeeded, by further developing rehabilitation practice, in preventing or minimizing long-term disabilities in many cases. As a result, annuity cases have been almost constant despite the 40% increase in persons insured over that time period.
The decrease in the frequency of accidents can be traced to many causes and developments—the modernization of production methods (especially automation) and the structural shift from the production sector to the service and communications industries; the efforts at prevention undertaken by the accident insurance system have made a substantial contribution to this financial and humanitarian achievement.
Basic Principles and Features of the German Accident Insurance System
The system is supposed to provide comprehensive social security to individuals afflicted by work-related accidents or occupational diseases. It also relieves those who are responsible for such accidents and diseases in the plants from the burden of liability to the injured. The following basic principles can be traced to these twin objectives of the system, which have marked it since its inception:
The liability of employers for industrial injuries is replaced by a public-law obligation of the accident insurance system to provide benefits (“relief of employers’ liability”). Any civil damage suits by the insured against the business owner or other company employees are precluded.
Business owners alone make payments to the accident insurance system, as they bear responsibility for industrial hazards and are relieved of liability risks by the accident insurance system.
Insurance benefits, based on the principle of compensation for injury, substitute for civil liability claims against the employers.
Insurance benefits are provided independent of formal proof of the insurance relationship and independent of employer notification to the accident insurance carrier. A more reliable and effective safeguard is thereby provided for all persons legislatively covered by insurance protection.
The insurance benefits are provided, as a general principle, regardless of who is at fault and without suit by the entitled person. The employment relationship is thereby freed from disputes over the question of fault.
As an important supplement to the task of providing insurance benefits, the accident insurance system is responsible for preventing work-related accidents and occupational diseases. The system frees the employer from liability, but not from responsibility for organizing a safe and healthy work environment. The close connection of prevention with rehabilitation and financial compensation is of fundamental importance.
The basic organizational principles have already been discussed above (organized as a corporation of public law with the power of self-administration and structured according to industrial branch).
The relationship of the various areas of responsibility to one another is marked by two principles: The primary goal must be to keep the number of insurance cases as low as possible through appropriate preventive measures (“priority of prevention over compensation”). In the event of an insurance claim, the primary goal must be to rehabilitate the injured party medically, occupationally and socially to the extent possible. Only then shall any remaining disabilities be compensated in the form of monetary payments (“rehabilitation before annuity”).
The following sections will show how these basic principles operate within the specific areas of responsibility of the accident insurance system.
Prevention
The task of prevention is based upon the following considerations: the accident insurance system, which bears the costs of work-related accidents and occupational diseases within the framework of rehabilitation and compensation, should first of all have the ability to prevent the occurrence of injuries insofar as possible. Employers should be aware that they remain responsible for health and safety in the workplace, even though their direct liability to the employees has been replaced by the accident insurance system. The connection between accident insurance and accident prevention should make clear to the parties involved—particularly the employers—that capital investment in workplace safety pays off, primarily in the humanitarian sense, by preventing human suffering, but also in an economic sense, through the reduction of accident insurance premiums and company costs resulting from injuries. Structuring the industrial accident insurance system by branches and involving the concerned parties within the framework of self-administration results in a high degree of practical preventive experience, as well as acceptance and motivation by those affected. This close connection between accident insurance and prevention distinguishes the German system from the systems of most other nations, which generally provide for the inspection of workplace safety by government officials. Such workplace safety authorities also exist in Germany in addition to the technical monitoring service of the accident insurance carriers. The two institutions complement and cooperate with one another. The responsibilities of the government supervisory authorities (factory inspection) go beyond those of the technical monitoring service of the accident insurance carriers (regulation of work hours, protection of especially high-risk groups such as juveniles and pregnant women, environmental protection).
The accident insurance system’s prevention mandate stipulates only the basic premises, allowing the self-administration of the carriers considerable latitude in the particulars—especially with respect to special features within specific branches that are applied to the individual plants or to the entire facility and by general regulations.
The most important aspects of the system’s conception of prevention include the following:
The (Berufgenossenshaften) are required to issue accident prevention instructions on specific danger areas. These instructions must be regarded as law by the employers and insured persons. Compliance with these instructions can be enforced by the carriers through sanctions (fines). These regulations are based on industrial experience and will be continually adjusted to the requirements of technical development.
Each carrier maintains its own specialized monitoring service, which advises and oversees the businesses. These are staffed by specially trained monitors—especially engineers and scientists—and are supported by experts in other disciplines according to the branch of industry being served. The authority of the monitoring services ranges from giving advice on binding regulations to closing down part of a plant in the case of an acute threat to health.
The carriers provide company doctors and safety specialists with advice, training, informational literature and work assistance. These internal work safety experts are important consultants for the monitoring services. This industry-specific cooperation strives to uncover accident dangers and work-related health hazards in advance, and to enable appropriate protective measures.
The monitoring services for the carriers check whether the employers comply with their obligation to engage company doctors and safety experts. Some trade associations maintain their own doctors and experts, to which their member companies can turn in cases where they have not arranged for their own.
The training and continuing education of the individuals assigned to implement occupational safety measures in the plants is mostly in the hands of the carriers. The training programmes are adapted to the needs of the individual branches of industry. They target and are differentiated according to the various levels of plant responsibility. Many accident insurance companies run their own training centres.
Accident insurance carriers address questions concerning workplace safety to the employers and managers, keeping them informed and motivated to improve prevention. Attention to small and middle-sized businesses has recently become the focus of preventive efforts.
The carriers’ technical monitoring services also advise the employees on health and safety risks in their workplaces. Cooperation with the workers’ councils, which represent the interests of the employees within the company, takes on greater significance in this connection. The employees should participate in organizing the working environment, and their experiences should be made use of. Practical solutions to safety problems can often be found by strengthening the participation of the employees. Improving safety can promote the employees’ motivation and job satisfaction, and have a positive effect on productivity.
The carriers’ technical monitoring services routinely inspect factories and investigate cases of accidents or occupational diseases. They then make many individual measurements corresponding to the dangers present, in order to work out necessary protective measures. The results of these measurements, of the analysis of the workplace and of the problems, together with knowledge derived from occupational medical care, are compiled using modern data-processing methods and are used throughout all plants to further promote prevention.
The carriers maintain specialized testing sites in which particular kinds of equipment and safety features are tested. Through this and through the advice of manufacturers and operators of technical equipment, the carriers obtain detailed information which they translate into the practical work of prevention in the plants and which they also introduce into national, European and international standards.
The (Berufgenossenshaften) have themselves conducted, initiated or financially promoted many need- and use-oriented research projects to advance knowledge in the field of safety and health protection.
In the interests of the employers as well as the employees, all the accident prevention work of the carriers aims to organize workplace safety and health measures as efficiently and economically as possible. Implementation strategies must also be practical. The effectiveness of preventive work is also monitored.
Scope of Insurance Protection
The insured
Employees who are working or in training are insured persons under the accident insurance system. Insurance protection is awarded regardless of age, sex, marital status, nationality, level of remuneration or length of employment. Insurance coverage is also guaranteed in the event that the business has not yet registered with the accident insurance carrier or has not paid premiums.
Homeworkers and persons who are active as employees in home industries are mandatorily covered, as are persons who receive rehabilitation measures from a social insurance carrier, and employers in some branches. All other employers can voluntarily insure themselves through the system.
In the agricultural accident insurance system, the employees, agricultural employers and employers’ spouses who work are obligatorily covered.
In the governmental accident insurance system, many groups are insured in addition to employees (but not the civil service and soldiers). These include students, schoolchildren and kindergarteners. Persons who are active in the interest of the public good and prisoners who work are also covered. A large portion of those insured by the government programme enjoy premium-free coverage, financed by federal, state and local governments.
The insurance cases
Insurance cases, or incidents, in the accident insurance system are workplace accidents and occupational diseases. Accidents which occur during the use or operation of equipment and commuting accidents also count as work-related accidents. The decisive criteria for insurance cases are as follows:
- membership in an insured group
- bodily injury resulting from a sudden work-related accident
- exercise of an activity covered by insurance at the time of the accident or at the time of injury to health; covered activities are those closely connected to the employment relationship
- an accident or an injury to health caused by an activity covered by insurance.
Fault on the part of the insured does not invalidate a claim. But if the only substantive causes of the accident are from the private sphere, then coverage will not apply—for example, an accident while an individual is under the influence of alcohol or as the result of a violent dispute. No insurance coverage is applicable to injuries which, though they occurred in the course of an insured activity, nonetheless arose as the result of a pre-existing health problem; this applies mostly to heart attacks and slipped disks.
Occupational diseases (those that are medically known to be caused by particular effects that certain groups are exposed to in their work to a higher degree than the general public) are included on an official list. If new information exists regarding an illness that does not appear on the list, the carriers can compensate the illness as an occupational illness.
Notification and statistical recording of insurance cases
In general, the benefits of accident insurance do not need to be applied for by the injured party, but are to be furnished at the initiative of the carriers. This presumes that cases are reported in some other way—employers, doctors and hospitals are obliged to inform carriers. This is the basis for a comprehensive statistical recording of occurrences of accidents and occupational diseases.
Rehabilitation
The system has the legal responsibility to provide comprehensive medical, occupational and social rehabilitation benefits upon the occurrence of an accident or the onset of an occupational disease. The objective of this mandate is, insofar as possible, to restore the health and the reintegration of the injured into work and society. Alongside the aforementioned principle of “rehabilitation before annuity”, the system provides all rehabilitation benefits of an accident insurance carrier “from one hand”. This guarantees a speedy and consistent rehabilitation programme, coordinated to the individual’s health, level of education and personal situation. The carrier is not confined to paying benefits and ensuring the care of the injured. Rather, the carrier optimizes the rehabilitation with specially qualified and equipped doctors and hospitals, through establishing carriers’ own clinics—especially for the care of severe burn victims and spinal cord and skull and brain injuries—as well as through observation, attendant care and, when necessary, corrective steering of the rehabilitation process. The following particulars apply:
Medical rehabilitation
The carriers must ensure that proper treatment begins as rapidly as possible after the incident. If necessary, this should include care from specialized physicians or occupational medical care. Physicians should participate in the treatment who are specialized due to training in accident medicine and have experience as surgeons or in orthopaedics, are equipped with a technical medical practice, and are prepared to fulfil certain duties with respect to the insurance carrier, particularly submitting forms and expert opinions.
After an incident occurs, injured persons should immediately go to a physician who is on contract with the carrier and who must prove the above-mentioned qualifications. They are empowered by the carrier to begin further treatment and to decide whether general treatment or special treatment—in cases of serious injuries—should be provided.
In the case of especially severe injury, the accident insurance system exacts the highest requirements in treating the injured person. Therefore, the insurance carriers authorize only specially qualified hospitals to undertake this treatment. These hospitals are subject to special guidelines and supervision.
The carriers use certain doctors to monitor and direct the treatment, who are required to supervise the treatment, to make reports to the carrier and, if necessary, to propose further rehabilitation measures.
The treatment and medical rehabilitation benefits are fully assumed by the accident insurance system (without copayment by the insured). This fulfils the injury compensation principle of the system.
Occupational rehabilitation
If medical rehabilitation alone cannot render injured persons capable of returning to their jobs, then the carrier must provide for occupational rehabilitation. The law provides for rehabilitation that conforms to the circumstances of each individual case (severity of disability, level of education, occupational qualifications and inclinations, age of the injured). The rehabilitation can result in measures specific to the plant, such as adapting the workplace to the disability; assistance in obtaining a position in the plant where the accident took place or in another plant; or financial support for the employer who is prepared to provide employment. Occupational training, including retraining for an entirely new occupation, is also covered.
As the system is responsible for providing medical as well as occupational rehabilitation, necessary occupational rehabilitation measures can be planned and started during the medical rehabilitation with the participation of the injured and the physicians. This task is performed by occupational counsellors—specially qualified and experienced employees of the carriers. They visit the severely injured while they are still hospitalized, attend to the insured persons, especially in searching out and selecting appropriate and promising rehabilitation measures, and stay with them until they are reintegrated into working life.
Social rehabilitation
Medical and occupational rehabilitation are essential preconditions to injured persons’ ability to resume living as much as possible as they did before the injury. Beyond this, however, it must also be assured that those suffering long-term health effects can not only resume work, but also social, family and cultural life as well. To this end, the carrier also provides social rehabilitation benefits; for example, vehicle assistance to promote mobility, handicapped sports to help promote health and participation in social life, household assistance or creating and equipping an apartment adapted for handicapped individuals.
Monetary benefits
During rehabilitation, the injured have a claim to continued payment of wages by the employer in the first period of the inability to work as a result of the incident (at least six weeks by the union contract). Then the carrier must provide “replacement pay” during the period of the medical rehabilitation. The disability payment corresponds, generally, to the net salary at the time of the incident—with deductions for the employees’ contribution to social security and unemployment insurance (at present almost 13 per cent). During occupational rehabilitation, a transitional wage replacement benefit is paid, which is somewhat less than the disability payment. These benefits are paid throughout the duration of the medical and occupational rehabilitation so that the insured and their families are financially secure. Continued payment of premiums to the other branches of the social security system prevents any gaps in insurance coverage.
Financial Compensation through Annuities
Insurance annuities
Insured persons receive annuities as compensation for remaining health problems from a work-related accident or occupational illness. These pensions are granted only at the close of the rehabilitation process and assume a definite decrease in earning capacity (generally 20%) for a minimum time period (beyond 13 weeks after the work-related accident). The annuities are calculated according to the degree of decrease in earning capacity and the annual earned income.
The principle of “abstract injury rating” applies in determining the degree of decrease in earning capacity. Accordingly, the loss of earning power on the general labour market and not the concrete loss of earnings (lost wages) caused by a work-related accident or occupational disease is taken into account. Measuring the decrease in earning capacity depends primarily on the severity of the health problem, which is in turn assessed by the expert opinion of a physician. This helps to minimize administrative costs and also keeps the burden on the insured and their employers to a minimum. In most cases, the abstract injury rating for annuities works out so that the insured are not in a worse overall economic position after the insurance incident than before. In many cases, indeed, a certain improvement of position results so that the annuities contribute in fact toward compensating for immaterial damages. The principles of the abstract injury rating and of “rehabilitation before annuity” work against the danger of an “annuity mentality” developing among the insured. The insured are motivated, despite any continuing health problems, to seek gainful employment.
The principle of the abstract injury rating is supplemented by factors of concrete damage assessment to ensure that appropriate compensation is made in all cases.
Annual earned income is the second basis upon which annuities are computed. By this is meant the sum of all wages and self-employed income an insured person earned during the year preceding the insurance incident. The annual earnings should reflect the standard of living that the insured had attained at the time of the workplace accident.
Under certain conditions, disability annuities can be fully or partially indemnified.
Survivors’ pensions and other death benefits
Widows, widowers and orphans—and under specific conditions also parents—have a claim for survivors’ pensions upon the death of insured individuals from work-related accidents and illnesses. The function of these pensions is to replace support lost through death. The computation is, as in the case of injury annuities, based upon the earned income. It is graduated according to the survivors’ need (especially widows with versus without children; children orphaned by one or both parents). Earned income and earned replacement income is taken into account in the case of survivors’ pensions, with the exception of orphans under 18 years of age. In the latter case the principle of loss replacement is applied: only those actually dependent upon support receive the benefits to the requisite and proportionate extent.
Along with survivors’ pensions, costs of conveyance and burial costs are guaranteed.
Widow and widower pensions are granted until remarriage; in the event of remarriage a settlement of two times the yearly annuity is paid.
Financing and Law on Premiums
There exist considerable differences among the three branches of the accident insurance system (industrial, agricultural and governmental) on financing and the law on premiums. The following discussion deals only with industrial accident insurance.
The costs of the industrial accident insurance system are financed almost exclusively by premiums from employers. Additional income received from indemnity claims against third parties (especially for traffic accidents), capital gains, late charges and fines is of relatively little significance. It should be emphasized that the industrial accident insurance system functions without financial assistance from the government. Revenues are raised and utilized solely to fulfil the legal obligation—attempting to turn a profit is forbidden.
Premiums for individual businesses are calculated based upon the employees’ wages that are subject to premium (or of the income from work or the insurance amount of the employer). The law on premiums takes particularly into account the occurrence of accidents and the attendant threat of accident in the branches of industry and individual businesses. Three levels are distinguished:
The first level of premium is conferred by collecting one or more branches of industry into an industrial insurance carrier as a common risk group. For example, more, and more severe, insurance incidents occur in the construction industry than in precision tool manufacture. Thus the premiums for a construction carrier are considerably higher on average than those for a carrier in precision tool manufacture.
At the second level, at the level of each individual carrier, the industrial branches included in this carrier—the bricklayers, roofers and janitors in the construction industry, for example—are classified according to the costs of accidents in the different risk groups. The general allocation of branches of industry into risk groups produces risk tables for each carrier. Each individual business is assessed by the carrier according to risk group on the basis of the risk tables. Different constituent parts of a business are assigned to various corresponding risk groups. The risk tables are actualized on the basis of five-year statistical surveys of accident frequency and costs. By means of the risk groups, the amount of the premiums for the individual branches of industry grouped within the same trade association are differentiated.
At the third step, the premiums are once again modified at the level of the individual enterprises. Here the criteria can be the number, severity and cost of the work-related accidents (excluding commuting accidents) over the last 1 to 3 business years. The insurance carrier can reduce the premium of an enterprise with a below-average incidence of accidents, or impose a premium surcharge in the case of an above-average incidence of accidents. The carriers are authorized to rule independently on the further detail (imposing surcharges or granting premium reductions, or combining the two).
Graduating the premiums for the various branches of industry and the individual enterprises according to accident trends is supposed to make the employers aware that the cost of accident insurance premiums also depends on efforts at—and the success of— prevention, and to spur efforts in this direction.
The accident insurance system is financed by a procedure of retroactive apportionment to cover costs. The amount to be apportioned is the excess expenditure over income, calculated retroactively for every budget year. The apportionment debit is divided among the individual member companies of the respective insurance carriers according to the premium computations (risk group of the company, total wages paid in that premium year and, if applicable, the premium surcharge or reduction). Naturally, ongoing costs must be financed in advance. This comes from collecting working funds and from pre-paid premiums. In order to compensate for long-term fluctuations in premiums, the accident insurance carriers must build reserve funds. These funds are preferentially invested in establishments that serve to fulfil the tasks of the accident insurance system—for example, training facilities or accident-care hospitals.
As accident insurance premiums cannot be calculated by the employer, the insurance carrier does the calculation and notifies the employer.
In the German accident insurance system, which is organized by industrial branch, structural changes in the economy can lead to an indefensibly heavy financial burden for some insurance carriers. This is especially the case for the coal mining industry. The number of working coal miners has declined substantially in the last decades, but the insurance carrier for mining must nonetheless pay annuities which date from a period when several times as many miners were employed. To remedy this extreme, no longer sustainable increase in the burden of premiums for that branch of industry, a method for sharing the burden among the various insurance carriers was introduced through legislation in 1968. The other insurance carriers are obliged to raise an additional apportionment to fill the financial gaps among those insurance carriers that have a right to equalization. Legislators thereby extended the fundamental notion of solidarity, which applies within each individual accident insurance carrier, to all industrial enterprises.
Workers' Compensation: Trends and Perspectives
Workers’ compensation systems (WCSs) were created to provide payment for medical care and rehabilitation services for workers sustaining work-related injuries and impairments. They also provide income maintenance for the injured workers and their dependants during the period of disability. They were patterned after the systems maintained by guilds and provident associations in which members made contributions to funds which then were disbursed to members unable to work because they had been injured on the job. Once their usually slender savings were exhausted, the only alternative for workers who were not members of such systems was to rely on charity or to bring suit against the employer, alleging that the injury resulted from the latter’s wilful action or negligence. Such lawsuits were rarely successful for a variety of reasons, including:
- the employee’s inability to command the requisite legal talent and his or her lack of resources compared to those of the employer
- the difficulty of overcoming the employer’s defence that the accident causing the injury was either an “act of God” or the result of the worker’s own ineptitude or negligence, rather than that of the employer
- the inability of the worker to wait out the often long time period required to adjudicate civil actions.
WCSs are “no-fault” systems requiring only that the worker file the claim as required and provide information demonstrating that the injury/disability was “work related” as defined in the legislation or regulations creating the WCSs in the particular jurisdiction. The requisite financial support is promptly available, supplied by funds accumulated by a government agency. These funds come from taxes on employers, from mandatory insurance mechanisms sustained by premiums paid by the employers, or from varying combinations of the two. The organization and operation of WCSs are described in detail in the previous chapter by Ison.
Despite gaps and deficiencies that have been addressed by legislative amendments and regulatory revisions over the past century, WCSs have worked fairly well as a social system providing for the needs of workers injured in the course of their employment. Their initial focus was on accidents (i.e., unexpected occurrences in the workplace or on the job), which are more easily identified than occupational diseases. The immediacy of the association between the occurrence and the injury makes the relationship to the workplace more or less simple to establish within the framework of the relevant laws and regulations. As a result, safety organizations have tried to develop, with more or less success, an epidemiology of accidents defining the kind of individuals, jobs and workplace circumstances associated with particular types of injuries. This led to the development of a sizeable safety industry devoted to studying various types of work-related injuries and identifying approaches to their prevention. Employers were constrained to adopt these preventive measures in the hope of escaping the burden of the costs of preventable accidents. These costs have been expressed in terms of workplace disruptions, temporary or permanent loss of productive workers, and escalating workers’ compensation taxes and/or insurance premiums paid by employers. An added inducement has been the passage in many countries of occupational safety and health legislation that enforces the requirement that employers adopt the appropriate accident prevention measures through the use of worksite inspections and various forms of penalties for lapses in compliance.
This arrangement has not worked very well, however, in the area of occupational disease. There, the relationship between the workplace hazard and a worker’s illness is often much more subtle and more complicated, reflecting the frequently long latency period between exposure and the initial signs and symptoms, and the confounding effects of influences such as the worker’s lifestyle and behaviour (e.g., cigarette smoking) and the coincidental development of non-work-related diseases. (The latter may, however, be influenced, aggravated or even precipitated by workplace exposures that under certain circumstances may bring them under the jurisdiction of a WCS.)
This article will focus initially on the validity of two related hypotheses:
- WCSs are able to develop preventive programmes based on adequate workplace risk assessments formulated through analysis of data derived from compensated cases of injuries and diseases; and
- WCSs are able to provide potent financial incentives (e.g., premium rating or bonus malus) to persuade employers to mount effective preventive programmes (Burger 1989).
In short, the nature and extent of risk on the job or in the workplace may be derived by analysis of workers’ compensation data using such variables as the presence of potentially noxious agents (chemical, physical, biological and so on), the characteristics of the workers involved, the circumstances at the time of the exposure (e.g., its nature, amount and duration), the pathophysiological effects on the worker, the extent and reversibility of the resulting disease or impairment, and the distribution of such cases among jobs, workplaces and industries. Identification and rating of the potential risks would lead to the development of programmes to eliminate or control them. Implementation of these programmes would lead to a reduction of work-related injuries and diseases, which would not only be beneficial to the workers, but would also reduce the direct and indirect financial burdens that otherwise would have to be borne by the employer.
We intend to show that the connections between compensated cases, risk evaluations, effective prevention efforts and lowering of employers’ financial burdens are not as simple as is usually believed. In addition, we will discuss a number of proposals offered by occupational physicians, lawyers and ergonomists to improve our knowledge of risks, enhance safety in the workplace and introduce more justice into WCSs.
Results of Studies
Value of the compensation insurers’ database
According to Léger and Macun (1990), the value of an accident database depends on the extent to which it allows safety performance to be measured, the causes of accidents to be identified, and the exposure to risk of subgroups within the working population to be determined. Accurate and effective accident statistics have great value for the design of effective accident prevention programmes by employers, labour organizations and government inspectors.
What data are compiled?
Statistics are limited to the accidents and illnesses defined by compensation laws and regulations and, therefore, recognized by WCSs. There is much variation among the cases so recognized within any given country or jurisdiction, between different countries and jurisdictions, and over time.
For example, in France the statistics compiled by the Institut national de recherche et de sécurité (INRS) are based on a list of occupational diseases coupled with a list of sectors at risk. In Switzerland, occupational diseases are categorized by the LAA (law on accident insurance) according to their association with conditions prevailing at the worksite. There, two categories are defined: in the first, a list of noxious agents accompanied by a list of diseases is provided; in the second, a list of diseases based on having demonstrated a strong possibility of causality between exposure and illness is provided.
Definitions of occupational accidents also vary. In Switzerland, for example, commuting accidents are not considered occupational, while all events occurring at the worksite, whether or not they are related to the work activity (e.g., burns resulting from cooking lunch), are encompassed by the definition of “occupational accidents”.
Accordingly, the number of cases recognized and tabulated in a particular jurisdiction is determined by the relevant legal definitions of accidents and diseases covered by the WCS. This may be illustrated by the Swiss statistics on occupational hearing loss, which was recognized as an occupational disease during the 1955-60 period. As soon as it was recognized, there was a marked increase in the number of reported cases, which produced a comparable increase in the total number of cases of occupational disease attributable to physical agents. Then, over the following years, the numbers of these cases tended to decrease. This did not mean that occupational hearing loss was any less of a problem. Since hearing loss develops slowly over time, once the initial backlog of cases hitherto not officially recognized had been recorded, the number of new cases tabulated each year reflected the constant association between noise exposure and the risk of hearing loss. Currently, we are witnessing another marked increase in the number of reported cases caused by physical agents, reflecting the recent official recognition of musculoskeletal disorders, commonly called “ergonomic disorders”, which include tenosynovitis, epicondylitis, rotator cuff problems, carpal tunnel syndrome and others.
Reporting of Cases
It is evident in all countries that many cases of accidents or diseases considered to be work-related are not reported, either deliberately or by omission. Reporting is generally the employer’s responsibility. However, as some authors have shown, it may be to the employers’ advantage not to report, thereby not only avoiding the administrative bother, but also preserving the reputation of the enterprise as a good place to work and preventing the accumulation of claims that might result in an increase in their workers’ compensation insurance premiums or taxes. This is particularly true for cases that do not involve any lost work time as well as those that are treated by an employee health service at the worksite (Brody, Letourneau and Poirier 1990).
It is the physician’s responsibility to recognize and report cases of occupational injury and disease and to notify the patient of his or her rights to compensation. However, some cases are not reported because they are treated by general practitioners who do not recognize the work-related nature of a health problem. (A knowledge of occupational and legal aspects of health care should be an integral element of medical education. International organizations such as the ILO should encourage the inclusion of such subjects in undergraduate as well as postgraduate training for all health professionals.) Even when they do make the connection, some physicians are reluctant to accept the burden of the necessary paperwork and the risk of being required to testify in administrative procedures or hearings if the worker’s claim for compensation is contested. In some jurisdictions, the fact that statutory or scheduled fees for treating workers’ compensation cases may be lower than the physician’s customary charges may be another disincentive to proper reporting.
The reporting of cases also depends on how much workers know about their rights and the WCS under which they are covered. Walters and Haines (1988), for example, surveyed a sample of 311 unionized and non-unionized workers in a highly industrialized area of Ontario, Canada, to assess their use and knowledge of the “internal responsibility system”. This was created by local legislation to encourage employees and employers to resolve health and safety problems at the plant level. While 85% felt that their working conditions might harm their health, only one-fifth reported time lost from their jobs due to a work-related health problem. Thus, despite beliefs about the damaging effects of their work on their health, only relatively few used the rights and resources provided in the legislation. Their descriptions of their refusals to work and their worries about the health effects of their work contained very few references to the “internal responsibility system” provided by the legislation. In fact, the main contact they reported was with their supervisor rather than the designated health and safety representatives.
Awareness of the legislation was greater among unionized workers, the researchers found, and was more often associated with taking actions relating to occupational health and safety (Walters and Haines 1988).
On the other hand, some workers make claims for compensation even if the injury or disease is not related to their work, or continue to claim benefits even when they are capable of returning to work. Some studies have shown that liberal compensation coverage may even be an incentive for filing claims. According to Walsh and Dumitru (1988), in fact, “improved benefits may result in additional claim filing and injuries”. These authors, using the example of back injuries (which constitute 25% of workers’ compensation claims in the United States) note that “workers are more demanding of time off for injury when compensation is comparable to earned wages”, adding that “the system of disability compensation in the United States does increase the frequency of certain types of disability claims and contributes to delayed recovery from LBP” and that “compensation factors may delay recovery, prolong symptoms, and reinforce sick role behaviour”.
Similar observations were made by Judd and Burrows (1986), based on a study of a representative sample of Australian workers in which, in the course of one year, 59% “have been away from work for more than two months, and 38% for longer than six months.” It is suggested that “the medical and legal services may result in this high rate of prolonged invalidism” and that “recovery appears to be against the victim’s best interest, at least for the settlement of compensation”.
Admissibility of Cases
As noted above, national statistics reflect changes in the admissibility of types of cases. Examples include adding a new disease to the list of compensable diseases, as in the case of hearing loss in Switzerland; extending coverage to new types of workers, as in the changes in wage scale limits in South Africa; and extending coverage to new types of businesses.
Unlike accidents, occupational diseases are not readily compensated. A study of a large sample of workers who had lost at least one month off the job was conducted in francophone Switzerland. It confirmed that accidents were largely accepted as work-related and compensated promptly, but only a small percentage of illnesses were accepted (Rey and Bousquet 1995). The end result in cases of illness is that it is the patients’ health insurance rather than the WCS that pays the medical charges. This does not increase the cost to the employers (Rey and Bousquet 1995; Burger 1989). (It should be noted that where, as in the United States, the employer also bears the cost of general health insurance, the cost may be even greater since the fees allowed by WCSs are often lower than those charged by private health-care providers.)
Yassi (1983) wrote a report on a lecture given by Prof. Weiler, in Toronto. Some of Weiler’s remarks, quoted by Yassi, are worth mentioning here:
the Workmen’s Compensation Act worked fairly well in compensating for disability due to accidents—the same cannot be said for occupational diseases—Whereas, even in the most difficult cases of injury due to accident, the cheque was in the mail within a month or so, the average time for adjudicating cancer claims is about seven months (idem for respiratory disease claims). Only a small percentage of claims for injuries is rejected (around 2 per cent); in contrast the rejection rate for claims for serious diseases is well over 50 per cent.
Particularly striking is the under-reporting of occupational cancer cases: “Less than 15 per cent of the estimated number of occupational cancers are reported to the Board.”
The necessity of demonstrating a causal relationship between a disease and the job (e.g., a recognized toxic agent, or a disease on the accepted list) is a major obstacle for workers trying to receive compensation. Currently in most industrialized countries, the WCSs compensate less than 10% of all occupational disease cases, and most of these are relatively minor illnesses such as dermatitis. And in most of the 10% that are ultimately compensated, the basic question of compensability first had to be litigated (Burger 1989).
Part of the problem is that the legislation in the particular jurisdiction creates what have been called “artificial barriers” to compensation for occupational diseases. These include, for example, a requirement that to be compensable a disease must be peculiar to the workplace and not “an ordinary disease of life”, that it be listed on a specific schedule of diseases, that it not be an infectious disease, or that disease claims must be filed within a restrictive period starting with the time of exposure rather than the time the presence of the disease is recognized (Burger 1989).
Another deterrent has been the growing awareness that many occupational diseases are multifactorial in origin. This sometimes makes it difficult to pinpoint an occupational exposure as the cause of the disease or, conversely, allows those who would deny the worker’s claim to hold that non-occupational factors were responsible. The difficulty of proving an exclusive workplace cause-and-effect relationship has placed an often overwhelming burden of proof on the disabled worker (Burger 1989).
Mallino (1989), discussing scientific aspects of artificial barriers toward compensation, states that
Most of these artificial barriers have little or no relation to modern medical science which has concluded that most occupational diseases are multicausal in nature and have relatively long latency periods from the time of initial exposure to the actual manifestation of disease.
In most cases of traumatic injury or death, the cause and effect relation is clear: a worker loses a hand in a stamping machine, falls from a scaffold, or is killed in a grain elevator explosion.
For many of these diseases, such as work-related cancers, it is often difficult, if not impossible, to determine a specific cause and then link it specifically to a particular workplace exposure or set of exposures.
Moreover, risk-facing equality does not exist, and it is highly problematical to assess the degree and nature of occupational hazard solely on the basis of compensated cases. Past compensation experience in individual sectors of employment usually forms the basis on which insurers rate the risks associated with employment and calculate the premiums to be assessed on the employers. This provides little incentive for preventive programmes, even though industries such as mining or forestry are known to be dangerous.
More fruitful, however, is the notion discussed by Morabia (1984) of “homogeneous groups”. Grouping similar workers across sectors demonstrates quite clearly that risk is more related to skill level than to the type of industry, as such.
Inequalities among Workers Facing Job Hazards
Risk inequality is measured by several variables:
Effect of skill level
Differences in risk exposure between skilled and unskilled workers are independent of the company’s type of production and are not limited just to the type of workplace and exposure to toxic agents (Rey and Bousquet 1995). In Canada, for example, Laflamme and Arsenault (1984) found that the frequency of accidents among different categories of production workers is not randomly distributed. Less skilled, manual labourers—a minority of the workforce—suffered the highest proportion of accidents.
Moreover, injuries were not distributed by chance either; in unskilled piece-paid workers, the frequency of lumbar injuries is higher than in other groups, as well as other locations. Unskilled workers, in the type of work organization described by Laflamme and Arsenault (1984), concentrated risk factors. Differences in risk exposure with other groups of workers were exacerbated by what appeared to be an implicit “political” attitude in which preventive measures were more likely to be focused on the skilled workers, an organizational arrangement that was inherently discriminatory to the detriment of the unskilled workers, among whom the risks were concentrated.
Effect of work experience
The most vulnerable workers are those with the least experience on the job, be they newly hired or subject to frequent job changes. For example, data from INRS and CNAM (Conservatoire national des arts et métiers) in France show that temporary workers have 2.5 times the accident rate of permanent employees. This difference is attributed to their lack of basic training, less experience in the particular job, and inadequate preparation for it. In fact, the researchers note, the temporary workers represent predominantly a population of young, inexperienced workers who are exposed to high risks in workplaces without effective preventive programmes.
Moreover, accidents happen most frequently during the first month of employment (François and Liévin 1993). The US Navy found that the highest incidence of injury among shore-based personnel occurred during the first few weeks on the job. Approximately 35% of all hospitalizations occurred during the first month of a new job assignment; this frequency then decreased sharply and continued to decline as time on the assignment increased. A similar tendency was displayed by personnel on sea duty, but the rates were lower, presumably reflecting more time in the navy (Helmkamp and Bone 1987). The authors compared their data to that of a 1979 report from the US Bureau of Labor Statistics of the National Safety Council and found similar results. Moreover, they noted that the above-mentioned phenomenon varies only slightly with increasing age. While young workers are at highest risk for accidents for reasons noted above, the “new-to-the-job” factor remains important at all ages.
Effects of type of wage scheme
The way workers are paid may influence the frequency of accidents. In his critical review of publications on incentive wages, Berthelette (1982) notes that the piece-work method of pay is associated with a higher risk of accidents. In part, this can be explained by the incentive to “cut corners” and ignore job risks, by overwork, and the accumulation of fatigue. This negative effect of the piece-work incentive was also recognized by Laflamme and Arsenault (1984) in the furniture industry, as well as by Stonecipher and Hyner (1993) in other industrial activities.
The “healthy worker effect” (HWE)
There is ample evidence of the beneficial health effects of work and the negative health impact of unemployment. The HWE, however, does not connote that work is good for health. Rather it signifies that the working population is healthier than the population as a whole. This reflects the difficulty of those who are chronically ill, severely disabled or too old in obtaining and holding jobs, and the fact that those who are least able to cope with job risks are soon forced to abandon their jobs, leaving a workforce of the healthiest and most fit workers.
The HWE is defined by epidemiologists as a submortality (or, also, as a submorbidity) of workers compared to the mortality or morbidity of the whole population. For epidemiologists who use firms as a field for studying a disease, such an effect needs to be minimized. In his article on HWE, Choi (1992) considers not only the reasons, but also the methods, for decreeing this selection bias.
From the point of view of ergonomists, non-occupational factors, such as lower financial resources and family problems, may also enter into the picture, in addition to occupational factors such as lack of professional incentives and fear of not measuring up to one’s job requirements. If a worker voluntarily leaves a job very quickly—a few days or weeks after starting—the possibility that age has rendered the worker less capable of facing the demands of the job must be considered.
For example, the diminishing incidence of low-back pain (LBP) with age does not imply that older workers are necessarily more resistant to back pain. Instead, it suggests that those with a predisposition to backache (e.g., those with anatomical defects, poor musculature and/or poor physical condition) have discovered that bad backs are not compatible with heavy lifting and have migrated to other types of work (Abenhaim and Suissa 1987).
In the study by Abenhaim and Suissa, data were obtained from the Workmen’s Compensation Board of Quebec from a sampling of 2,532 workers who had lost at least one day of work due to back pain. The 74% of compensated workers who were absent from work less than one month accounted for 11.1% of lost workdays, while the 7.4% of workers who were absent more than six months accounted for 68.2% of the lost workdays. The latter group of workers (0.1% of the workforce) were responsible for 73.2% of the medical costs and 76% of compensation and indemnity payments (a total amount of 125 million dollars (1981). Each of these cost approximately 45,000 Canadian dollars. The high incidence rate found in men (85% of the cases) could be explained by the presence of a larger population of men in those tasks with a greater probability of back injury. Other explanations are less likely, such as a higher vulnerability of men or a greater proportion of men filing compensation claims. Abenhaim and Suissa state:
The increase-decrease pattern of back pain with age is most probably due to the healthy worker effect; workers would be more likely found in back-threatening tasks before age 45 years and would quit these jobs after they become older... The results of the study are at variance with the belief in industrialized countries that the major portion of this type of medical expense is due to ‘uncontrolled’ multiple periods of absence from work due to back pain with ‘no objective signs.’ The more socially significant cases are among those with long duration of absence and heavy medical assistance. Prevention and occupational health and safety policies should bear this finding in mind.
In brief, numerous factors not taken into account in tabulating the statistics of occupational injuries and diseases can modify the fundamental underpinnings of the data and completely transform the conclusions reached by workers’ compensation officials and others. This has particular relevance for those using these data as the basis for designing programmes to control particular hazards and ranking the urgency of their implementation.
Life and work events; stress
Stress is a major factor in the causation of work-related injuries and diseases. Stress in the workplace, whether arising out of the job or brought to the workplace from life at home and/or in the community, can affect behaviour, judgement, physical capabilities and coordination, leading to accidents and injuries, and there is growing evidence that it may affect the immune system, increasing the susceptibility to disease. In addition, stress has a significant influence on the response to rehabilitation therapy as well as on the extent and duration of any residual disability.
In attempting to account for the increased rate of accidents during the weeks immediately following a transfer from shore duty to sea and vice versa, Helmkamp and Bone (1987) suggested that the stress created by the transition and the changes in patterns of living may have been a contributing factor. Similarly, Von Allmen and Ramaciotti (1993) noted the influence of both job-related and off-the-job psychosocial factors in the development of chronic back problems.
In a 27-month prospective study among air traffic controllers, levels of social stress were dramatically related to the occurrence of accidents. The 25% of the study group of 100 workers who reported high levels of stress developed a total morbidity rate 69% greater than that of the workers reporting low stress levels, and an 80% greater chance of incurring an injury (Niemcryk et al. 1987).
It is not surprising, therefore, that at least in the United States there has been a proliferation of workers’ compensation claims attributing disability to alleged occupation stress. Even though such claims are still not allowed in many jurisdictions, their rate of increase has probably been exceeded only by the surge of recent claims for repetitive injuries such as carpal tunnel syndrome, and other ergonomic disorders.
Claims based on alleged stress offer another illustration of the “artificial barriers” to compensation noted above. For example, some of the jurisdictions in the United States (mainly the individual states) do not accept any claims based on stress: some will accept them only if the stressor is a sudden, discrete or frightening or shocking event, and some require the stress to be “unusual” (i.e., in excess of the stress of everyday life or employment). Some jurisdictions allow stress claims to be adjudicated on their merits, while there remain some where neither statutes or case-law have yet established sufficient consistency to constitute a guideline. Accordingly, it appears, the worker’s chance of success with a claim based on stress is as much a factor of where the claim is filed and adjudicated as the merits of the claim (Warshaw 1988).
Perception of risk
Before employers decide to improve working conditions, and before workers choose to work more safely, they must be convinced that there is a risk to be guarded against. This must be personally perceived; “textbook knowledge” is not very persuasive. For example, non-unionized workers are less likely to complain about potential work hazards because they tend to be less well informed about them (Walters and Haines 1988).
Risk-taking, the willingness of individuals to accept danger in the workplace, depends to a large extent on the culture of the organization. One can find a blasé attitude with risk-taking encouraged (Dejours 1993), or a more prudent approach (Helmkamp and Bone 1987).
Where there is a low accident rate and workers have never witnessed a serious accident, and especially where there is no union to sensitize workers to latent hazards, there may in effect be a denial of risk. On the other hand, where workers are aware of risks of serious injuries or even fatalities, they may demand supplemental hazard pay (Cousineau, Lacroix and Girard 1989). Deliberate risk-taking may, therefore, be stimulated by the desire or need for the extra pay.
Attitudes toward risk-taking on the job generally reflect the workers’ attitudes toward prevention in their personal lives. Stonecipher and Hyner (1993) noted that salaried employees had significantly higher levels of participation in health screening programmes and pursuing a healthy lifestyle compared to wage (paid on an hourly basis) workers, who tended to be less well educated and lower paid. Thus, low-skilled, low-wage workers who, as noted above, are prone to higher rates of accidents and injuries are also more likely to indulge in excessive use of tobacco and alcohol, have poor dietary habits and be less likely to take advantage of preventive health services. As a result, they appear to be in double jeopardy.
Organizational culture and risk levels in the enterprise
Characteristics of the organizational culture in the enterprise may influence the perception of risks in the workplace and, therefore, actions to control them. These include:
Size of the enterprise
Risks of occupational injuries and diseases are inversely related to the size of the enterprise. In Switzerland, for example, the smallest enterprises outside of the high-tech industries (up to ten employees) account for a very high percentage of the cases of occupational diseases recognized by the CNA (Caisse nationale suisse d’assurance en cas d’accidents—Swiss national accident insurer). In contrast to the larger enterprises, these small shops have less of a chance of recruiting the best trained, the most experienced and, from the standpoint of their health, the hardiest workers. Their owners and managers are less likely to be knowledgeable about workplace hazards and to have the time and financial resources to address them. They are inspected much more rarely and have greater difficulty than their larger counterparts in obtaining access to the technical assistance and specialist services they may need (Gressot and Rey 1982).
Rejection of responsibility
In Switzerland the employer is responsible for the safety of the worker and the worker is required to abide by the safety systems established at work. Unfortunately, the law and reality are not the same. A study of Swiss workplaces with 100 or more employees disclosed a tendency for each of the involved parties to deny responsibility for the accident and blame the other. Thus, employers pointed to the employee’s alcoholism or disregard of safety rules as the culprit, while the employees blamed workplace deficiencies and ineffective management. In addition, the industries rated most dangerous by the insurance companies tend to understate the risks (Rey et al. 1984).
Prevention of compensation cases reduces employers’ costs
In theory, the WCS is designed to reward employers who successfully mount effective prevention programmes and lower the frequency and severity of injuries and illnesses by reducing the workers’ compensation taxes or premiums levied on them. But this hypothesis is often not validated in practice. The costs of the prevention programmes may exceed the premium reduction, particularly when the premiums are based on a percentage of total payroll during a period when there have been significant wage increases. Further, the reduction may be meaningful only in very large organizations where premiums rates may be based on the experience of the individual company, in contrast to smaller organizations who pay “manual” rates that reflect the experience of a group of companies in a particular industry or geographic area. In the latter case, a single company’s improvement may be more than offset by the unfavourable experience of other companies in the group.
There is also the reality that although the number and severity of accidents and injuries may be reduced, the premiums are driven up by the escalating costs of medical care and by more generous payments for disability, particularly in the industrialized countries.
Theoretically—and this often happens—the costs of the prevention programme are more than recouped by continuation of the premium “rebates” as the improved compensation experience persists, and by avoidance of the indirect costs of work-related injuries and illnesses. The latter may be expressed in terms of workplace disruptions, absenteeism and lost production; these may be greater than the costs of workers’ compensation.
Attitudes of employers and managers
Most employers are genuinely concerned about the health and welfare of their employees and, in many larger organizations, this concern is often explicitly stated in formal policy statements. Too many managers, however, are much more concerned about their own status with respect to pay increases or bonuses and advancement within the organization. Competition among segments of the organization for awards and other recognition for holding down the number of injuries and illness often leads to concealment of accidents and denial of workers’ claims for compensation.
An important factor is that while preventive programmes require an upfront expenditure of money and other resources, notably staff time and effort and consultants’ fees, their payoff is often delayed or masked by unrelated rare events. This becomes a significant barrier when the enterprise is financially stretched and forced to restrain expenditures or even reduce them. The delayed payoff may also be critical for plant managers and other executives whose performance is judged by the “bottom line” at the end of the fiscal year or other accounting period. Such an executive may readily be tempted to defer investing in a safety programme until he or she has been promoted to a higher position in the organization, leaving this problem for a successor.
Labour-management collaboration
Labour-management collaboration is critical to the success of programmes to prevent work-related injuries and illnesses. Ideally, a joint labour-management committee will be created to identify problems, design programmes to address them and monitor their implementation.
Too often, however, such collaboration is prohibited or at least made difficult when relations between the employer and the union become inordinately adversarial. For example, employers sometimes resist union “intrusions” into workplace operations and activities and resent the union’s militancy in sensitizing their members to potential workplace hazards and encouraging them to pursue workers’ compensation claims on what the employer may regard as insufficient or inappropriate grounds. Unions, on the other hand, often feel compelled to be aggressive in advancing the interests of their members against what they regard as the lack of interest of the employers.
Suggested Reforms
Reform of the WCSs is not a simple matter. It necessarily involves a number of parties (e.g., workers and their representatives, owners of enterprises and employers, government agencies, compensation insurance carriers, legislators) each of whom has vested interests to protect. However, the high stakes involved—the health, well-being and productivity of workers and their dependants—make WCS reform a matter of more than a little urgency. Included among some of the reforms that have been suggested are the following:
Making statistics and their analysis reliable and compatible
There is currently an effort underway to make statistics internationally comparable. A single formula for European countries is one laudable example. There are directives that correspond to current practices, looking at the frequency or severity of cases by industrial sector, by physical or chemical agent, or by the conditions surrounding the accident.
The formula is not a radical departure from current practices such as those of the Swiss CNA, and thus one can hardly expect that the biases discussed above will be avoided. In Switzerland, however, the authorities have reacted favourably to the new requirements for the involvement of safety and health specialists at the enterprise level, particularly to the idea that information on risk should not rest solely on insurance company statistics, but rather should also have access to precise epidemiological studies.
It appears that in Europe, the member countries of the community have decided to adhere to the principle of a uniform formula for data collection. In the United States, however, a recent study showed that the creation of a data bank on insured cases does not have the same chance of success, according to Johnson and Schmieden (1992), despite the size of the insured pool and the expenses incurred by the insurance companies.
In the United States, workers’ compensation is big business, with almost 91.3 million workers covered in 1988, and nearly $34 billion paid out in benefits to workers at a cost to employers of over $43 billion for that year. Currently, workers’ compensation costs are increasing more rapidly than other health-care costs, a fact that seems to have escaped the notice of many employers who have been focusing on the escalation of employee health insurance costs, which many assume is partially or totally responsible. A unified database seems much less likely to be developed in the United States, in contrast to the European countries. Nevertheless, it has been suggested that, as a starting point, making the currently available workers’ compensation data more accessible to those who should be interested in it by having health science resource centres and libraries collect and disseminate it would be useful (Johnson and Schmieden 1992). Their survey on 340 relevant libraries in the United States and in Canada indicates that only about half of them do provide information services on this topic; only 10% foresaw a future need for a collection in this field, while most respondents indicated no need or did not answer. With increasing concern about the rapid rise in workers’ compensation costs, it seems reasonable to expect that employers, insurers and their consultants would press for the development of such data resources.
It should be noted that this is not the first time that such an initiative has been undertaken in North America. Following the 1981 report of the Joint Federation-Provincial Inquiry Commission into Safety in Mines and Mining Plants in Ontario, it was recommended that a database be developed that would:
- formulate clear and unambiguous definitions of which accidents are to be included
- profile each reportable accident (how, when, where, why, severity of injury and so on) and each worker (age, sex, type of job, length of service and so on)
- provide background data on the characteristics of the work force as a whole (e.g., skill levels, training and experience) along with data on production levels, hours of work and so on.
In interpreting the available statistics, indices defined in thresholds of time off from work should be emphasized and greater weight given to indices that are less amenable to social and economic influences (Léger and Macun 1990).
Separating compensation from prevention
It has been contended that the purpose of the WCSs should be limited to the collection and distribution of funds for the workers’ compensation benefits prescribed in the relevant legislation, while prevention of workers’ injuries and diseases is an extraneous matter that should be relegated elsewhere.
Mikaelsson and Lister (1991), for example, suggest that abuse of the WCS in Sweden makes the validity of the Swedish accident and illness data very questionable and not at all useful as a basis for designing preventive programmes. The Swedish WCS, they contend, invites multiple appeals and permits arbitrariness. Its costs have been rising rapidly largely because compensation is often granted without substantial evidence of a relationship of the injury or disease to the job, while the rules of evidence discourage a meaningful search for the actual cause.
Because the issue of causation is obscured or bypassed entirely, the Swedish data present a misleading picture of occupational injuries and diseases. The reported incidence of some diseases may be inflated (e.g., low-back pain) while causes of other disease may be entirely overlooked.
Let us stress here that the new Swedish law on compensation, under the influence of the multiplication of claims, particularly for low-back pain (LBP), is going backward. As it now operates, the Swedish WCS offers no incentives for employers to identify and eliminate the actual causes of occupational diseases and injuries. The meaningful investigation of the nature, extent and control of occupational hazards could be assigned to other agencies designated under other provisions of Swedish law (see “Country Case Study: Sweden” on page 26.26).
Burger (1989) goes one step further, suggesting that all occupational injuries and illness should be compensated without any preconditions and that the WCSs be subsumed in the general social insurance programme. On the other hand, he states, if the test of causal relationship is to be retained for coverage by the WCSs, that test should be performed, rigorously observing all the traditional criteria for the validity and quality of medical-scientific information.
Merge compensation medicine with general health care
In some jurisdictions, treatment of individuals with compensable injuries and illness is restricted to physicians and other health professionals who have been credentialed as having the knowledge and skill to deal with such problems. This, it is hoped, will ensure the quality of their care.
In some instances, this has had just the reverse effect. The great majority of workers’ compensation injuries are relatively minor and require little care beyond first aid, presenting little in the way of interesting challenges to the physician. In jurisdictions where statutory fees established for the care of such cases are lower than those that are customary in the area, there is an economic incentive to increase the number and extent of treatments. For example, when caring for a cut or laceration in New York State in the United States, the Workers’ Compensation Fee Schedule allows a supplementary fee of $1 for each suture up to a maximum of ten; thus, one sees wounds closed with ten sutures regardless of their length and even when adhesive “butterflies” might suffice. Also, to be convenient to workplaces, physicians’ offices and polyclinics treating workers’ compensation cases are often located in industrial districts that are generally not among the most prepossessing parts of town. As a result of such factors, compensation medicine often does not rank very high among the fields of medical practice.
Further, from another perspective, in areas where there are shortages of medical facilities and personnel, occupational injuries and diseases must perforce be treated in the nearest available physician’s office or polyclinic, where sophistication in the care of work-related health problems may be minimal. This is a particular problem in non-urban, non-industrialized areas and for enterprises too small to have their own employee health service.
At the opposite pole from those who would separate prevention from compensation are those who would give it greater emphasis as part of workers’ compensation. This is particularly true for Germany. This is also seen in Switzerland since the new law on accidents and occupational diseases (LAA) went into effect in 1984 covering the entire field of work safety. The federal commission of coordination (CFST) was then created with representatives of the confederation and cantons and representatives of the CNA and of other insurance carriers, public and private.
The CFST is responsible, among other things, for formulating technical regulations in the form of directives for the prevention of accidents and occupational diseases. It is also responsible for financing the workplace safety enforcement authorities (e.g., by reimbursements to the cantons) for the costs of workplace inspection.
The CNA is the major insurance carrier for occupational injuries and diseases and, in the field of workplace safety, monitors the application of rules of prevention for occupational accidents in approximately 60,000 enterprises—those that, in principle, expose the workers to the most serious dangers (e.g., those that produce or use explosives, use the greatest quantities of solvents, chemical companies). The CNA also issues directives on concentration limits for toxic substances on the job, limits that are supposed to be respected by the employers.
As the agency that applies the LAA and its regulations, the CNA must inform the employers and the workers of their respective responsibilities. The employer is required to take all steps and measures required by the regulation on accident and occupational disease prevention (OPA). The worker is required to follow the instructions of the employer on the question of workplace safety.
During factory visits to verify compliance with regulations carried out by the CNA (or by other, especially cantonal, monitoring bodies) the employer is required to permit inspectors access to all premises and job sites. If a violation is found, the CNA draws the employer’s attention to it and sets a deadline by which the situation must be corrected. If a warning is not heeded, the CNA orders the necessary measures by way of executory decision. In case of non-compliance, the company can be placed in a higher risk category, warranting an increased premium. The insurer (CNA or other insurer) must make the decision to increase the premium immediately. Furthermore, the executory body (in particular, the CNA) takes coercive measures, with the assistance of the cantonal authorities, if needed.
The CNA’s technical services participate in the factory visits, but are also available to the employers to offer advice on safety matters.
In the field of occupational diseases, the employer has to see that the workers to whom the regulations apply undergo preventative medical examinations, performed by the nearest doctor, or by the CNA’s own medical service. The CNA determines the content of the preventative medical examination and ultimately decides on a worker’s aptitude to fill the job.
All the technical and medical measures that the employer must take to fulfil his legal obligations are at his expense. Financing the inspection and administrative activity of the CFST and its executory bodies is ensured by the supplementary premium.
The CNA and the other insurers are required to furnish to the CFST the information that allows it to form the basis necessary for its action, especially establishing the accident and occupational disease statistics. When a new regulation was promulgated on company doctors and other safety specialists, the federal social insurance office (OFAS) issued report number 92.023, 1992. This report says that risk analysis cannot rest solely on accident and occupational disease statistics available to authorities (known case), but equally on epidemiological research, carried out in Switzerland or abroad.
Finally, the CFST is responsible for promoting information and instruction on job safety at every level. In Geneva, workplace inspection is organized with the CFST and the CNA, and with the support of the university scientists, conferences, practical safety courses for businesses in Geneva or other groups of interested persons. A tripartite commission with representatives from government, the employers and the workers is behind this initiative, which is largely subsidized by the canton.
Abandoning the one-dimensional causal relationship in favour of a multifactorial view of the links connecting workplace risk and disease
In most cases of occupational accidents causing injury or death, there is a clear-cut and direct causal relationship between the incident and the trauma. Such an “iron rule” is hard to impose when confronted by occupational diseases, which are generally multicausal in origin. Causality is further complicated by the long latency period from the initial exposure to the first recognizable manifestations of the disease. For many occupational diseases, such as work-related cancer, it is difficult if not impossible to identify a specific cause and then link it to a particular workplace exposure or set of exposures. Accordingly, rather than pursuing the workers’ compensation route, many workers with these diseases turn to the general health-care system (in the United States, for example, private health insurance—or Medicare if they are old enough, Medicaid if they are poor enough) and to the public welfare system when financial support is needed.
As a result, “employers for all practical purposes are paying little or nothing for occupational disease and, in fact, are being subsidized by the public welfare system and workers themselves” (Mallino 1989).
The results of a study conducted in francophone Switzerland (Rey and Bousquet 1995; Von Allmen and Ramaciotti 1993) came to the same conclusion. The medical insurance carriers are thus required to assume the costs, at the expense of the insured and of the taxpayer, for health hazards clearly linked to workplace activity, such as certain back pains among workers who carry heavy loads.
As the employers do not feel constrained to correct the problems of jobs that are nevertheless responsible for these health hazards, this anomaly is also unhealthy from the perspective of prevention, which should be based on the existence of cases registered by the workers’ compensation system.
To resolve this type of problem, Mallino proposes an approach that requires only a demonstration that the occupational exposure was a contributing factor to the disease rather than the immediate, direct and only cause. Such an approach is much more consistent with modern medical science, which has established the multicausality of many diseases.
Using a set of presumptions based on the entire worker population, Mallino evokes what has been labelled the “30% rule”. If the incidence of a particular disease in an exposed population of workers is 30% higher than in a comparable non-exposed population, that disease would be deemed to be work-related. To be eligible for workers’ compensation, a worker with that disease would simply have to prove that he or she was a member of an exposed group and that his or her level of exposure was sufficient to have been a factor in causing the disease (Mallino 1989).
We should note that this notion of probability has found its way into some legislation, such as, for example, Swiss legislation, which identifies two categories of disease. The second allows for recognizing cases that are not on the lists of occupational diseases or of chemical or physical agents recognized as noxious at the workplace. In the CNA’s actual practice, admissibility on the individual level also rests on the notion of probability, particularly for traumas to the musculoskeletal system.
Promoting rehabilitation and return to work—proposals by therapists
A major approach to minimizing the human and economic costs of workers’ compensation injuries and diseases involves promoting rehabilitation and early return to work. This is particularly applicable in cases of back injuries and other musculoskeletal disorders, which place a very heavy burden on WCS budgets in the United States and the countries of Northern Europe (Mikaelsson and Lister 1991; Aronoff et al. 1987).
According to Walsh and Dumitru (1988), the workers who have the most trouble returning to work after a lost-time illness are those with the best insurance. This fact should lead to a reform in the relations between the different actors. “Although progress in treatment is being made, modification of our present scheme of benefit disbursement seems necessary to optimize recovery after injury. Systems that reduce adversarial interactions between claimant, employer and insurer should be investigated.”
Aronoff et al. (1987) after evoking the costs of back pain in the United States, boosts methods of re-education that should permit insured persons to return to their jobs and to avoid falling into the trap of “chronic disability”.
“Impairment is a medical term, referring to reduction of body or organ function. Disability, a legal determination, refers to a task-specific limitation of performance. The chronic disability syndrome refers to a state in which individuals who are capable of working choose to remain disabled. The disability is often the result of a minor injury but actually represents an inability to cope with other life problems. The features of the syndrome are: out of work at least six months; disability claim and claim for financial compensation; subjective complaints disproportionate to objective findings; lack of motivation to recover and negative attitude toward return to work” (Aronoff et al. 1987).
Von Allmen and Ramaciotti (1993) analysed the process leading to chronic LBP among affected workers in different jobs. The complexity of the problem is even more manifest during a recession, when assignment changes and the possibility of returning to a less strenuous workplace are being more and more restricted.
The chronic disability syndrome is often associated with chronic pain. According to 1983 data from the United States, it is estimated that 75 to 80 million Americans suffer from chronic pain, generating annual costs between $65 and $60 billion. As many as 31 million of these individuals have lower back pain—almost two-thirds of whom report limitation of social and work functions. With chronic pain, the pain no longer serves an adaptive purpose but often becomes the disease itself (Aronoff et al. 1987).
Not all individuals with chronic pain are disabled, and many can be restored to productivity by referral to a chronic pain centre where the approach to such patients is multidisciplinary and features attention to the psychosocial aspects of the case. Success in such treatment is related to level of education, age (the older workers naturally having more trouble than younger ones in overcoming their mechanical problem) and duration of absence from the job prior to the referral (Aronoff et al. 1987).
Workers most likely to forego workers’ compensation benefits and return to work include those who have benefited from early intervention and referral for rehabilitation services as promptly as possible; those who effectively master the pain and are successful with stress reduction strategies; those with a positive work history; and those whose work offers a sense of purpose and job satisfaction. (Aronoff et al. 1987).
In some WCSs, benefits are cut off abruptly and the case closed as soon as a disabled worker returns to work. Then, if his or her disability recurs or new problems arise, the worker must face bureaucratic procedures and a more or less long wait for resumption of benefit payments. This is often a formidable obstacle to persuading workers that they are well enough to try returning to work. To overcome this, some WCSs allow a trial period when benefits are continued for a time during which the worker attempts to return to his or her old job or see if retraining has made him or her capable of performing a new job. Under these circumstances, the worker loses nothing if the trial turns out to be unsuccessful.
Ergonomic approaches: From the perspective of risk prevention
French-speaking ergonomists (members of SELF: an international society of French-speaking ergonomists) have shown the complex web of relations that link the job and accidents. Faverge (1977), based on studies conducted in coal mines by his collaborators, created a system of analysing accidents that today is applied in practice by the INRS in France.
It is not necessary for the effects on health to be serious and lead to grave injuries for the method to be useful. This is how very complicated links have been made between work with VDUs and visual fatigue (Rey, Meyer and Bousquet 1991).
In establishing these connections, the ergonomist has in his or her possession a precious tool for proposing preventive actions at different levels of the workflow.
Ergonomic analysis of the job has become a common technique that today goes beyond SELF, and the authors who are cited below include Americans and Canadians, as well as Europeans.
Ergonomic analysis of the job is original in that it cannot forego the worker’s participation. This is because, in addition to the knowledge that the worker has of the level of constraint that his or her job imposes, his or her perception of risk, as we explained above, depends on many factors that are foreign to the technical analysis of the situation conducted by the engineers and safety specialists.
In performing work tasks, the worker does not always follow exactly the advice of the safety specialist but relies also on his or her attitudes toward the job and perceptions of risks. As noted by Walters and Haines (1988):
Workers’ perceptions of hazards are formed and expressed in ways different from the dominant medical-technical paradigm in occupational health and safety. The main sources of information about chemicals, for example, are not supervisors, health representatives, or training courses, but their own experience, the observations of co-workers, or just their feelings. Workers employ a different complex of experience-based knowledge than is embodied in technical expertise.
In Quebec, Mergler (cited by Walters and Haines) has suggested (1987), that workers’ experience should be more fully recognised, since it does represent expressions of impairment. Having conducted numerous field studies, Mergler also knows that the workers’ testimony is difficult to obtain if they fear that by explaining their working conditions, they might lose their jobs.
With Durrafourg and Pélegrin (1993), we take even more distance from the cause-effect schemas of the insurers and safety officials. In order for prevention to be effective, according to these writers, the workers’ health and the work situation must be considered as a global system.
Although the major risks may have a preponderant cause (e.g., the level of noise to be heard or the presence of a noxious chemical substance for a poisoning), this is not the case for the majority of problems affecting working conditions, hygiene and safety. According to Durrafourg and Pélegrin, the risk in this case “is made up of the intersection of work demands, the condition of the workers, and the constraints of the situation on the job”.
If, for example, older workers have fewer accidents than workers with less seniority, this is because they have “acquired a knowledge of carefulness and of effective guidelines for avoiding danger”.
Ergonomic analysis should allow for identifying “the factors upon which it is possible to act to give a value to the knowledge of carefulness of men at work and to give them all the means they need to direct their health and safety”.
In brief, according to the ergonomists and labour doctors with modern training, risk is not expressed solely by a knowledge of the physical, chemical and bacteriological milieu, but also by a knowledge of the social milieu and the characteristics of workplace populations. A deeper study of the job, in the ergonomic sense of the word, should necessarily be conducted for every registered case. This effort at analysis is only very partially made by the existing authorities (workplace inspections, company health and safety services, medical services), but moving in this direction is necessary for effective prevention.
Equalization of social protection
Faced with rising costs due only in part to the costs of workers’ compensation and preventive programmes, employers are moving jobs from industrialized countries to less developed areas where wages and benefits are generally lower and health and safety regulations and administration are less burdensome. Faced with the need to install often costly preventive measures, some employers are simply closing down their enterprises and moving them to areas with lower wage costs. With this increase in unemployment, workers may have no jobs to return to when they are rehabilitated and, therefore, elect to continue to collect disability benefits for as long as possible (Euzéby 1993).
To meet the competition from low-wage areas, employers are reducing their workforce and demanding greater productivity from the workers they retain. With a simultaneous tendency to overlook or defer considerations of workplace safety, there may be more accidents and injuries putting additional pressure on the WCSs.
At the same time as workers’ compensation payments/premiums by employers—which are usually based on numbers of employees and a percentage of payroll—decline with workforce reductions, the resources of the WCSs may also be reduced. This has occurred in Switzerland, for example, where the CNA has had to reduce its own staff.
In the United States, a congressional movement to reduce the federal role in regulating and enforcing occupational and environmental health and safety laws and shifting it to the states and localities has not been accompanied by budgetary allocations and grants large enough to do this job properly.
Tchopp (1995) has called for an international equalization of social protection that will maintain the WCSs along with preventive programmes in developed countries and improve the working conditions and well-being in developing countries. The aim in these countries, he emphasizes, should be to improve the lives of their workers.
Conclusion
Although improvements are still possible, WCSs in general are doing a fair job of providing health care and rehabilitation services and disability benefits to workers with job-related injuries, but there are significant deficiencies in their handling of occupational diseases. The latter would be improved considerably by broadening the relevant legislation to include more bona fide occupational illnesses, improvements in the statistical systems and epidemiological studies that track their impact on the workforce, and appropriate recognition of medical and scientific developments demonstrating the multicausality of many of these diseases.
The role of WCSs in preventing occupational injuries and diseases, beyond providing data about their epidemiology, is problematic. The theory that effective approaches to prevention will lower employers’ costs for mandatory workers’ compensation taxes or insurance premiums does not always prove to be true in practice. In fact, some have argued for the separation of the prevention imperative from workers’ compensation administration and assigning it elsewhere, where occupational health and safety specialists may play a greater role. At the least, it requires appropriate governmental regulation and stronger enforcement, ideally internationalized to equalize conditions in developing countries with those in industrialized areas.
The ILO should encourage member countries to develop solid policies in the area of accident prevention and occupational diseases in the broadest sense.
Work-related Diseases and Occupational Diseases: The ILO International List
In 1919, the year of its creation, the International Labour Organization (ILO) declared that anthrax was an occupational disease. In 1925, the first ILO List of Occupational Diseases was established by the Workmen’s Compensation (Occupational Diseases) Convention (No. 18). There were three occupational diseases listed. Convention No. 42 (1934) revised Convention No. 18 with a list of ten occupational diseases. In 1964, the International Labour Conference adopted the Employment Injury Benefits Convention (No. 121), this time with a separate schedule (List of Occupational Diseases) appended to the Convention, which allows for amending the schedule without having to adopt a new Convention (ILO 1964).
Definition of Work-Related Diseases and Occupational Diseases
In the third edition of the ILO’s Encyclopaedia of Occupational Health and Safety, a distinction was made among the pathological conditions that could affect workers in which diseases due to occupation (occupational diseases) and diseases aggravated by work or having a higher incidence owing to conditions of work (work-related diseases) were separated from conditions having no connection with work. However, in some countries work-related diseases are treated the same as work-caused diseases, which are in fact occupational diseases. The concepts of work-related diseases and occupational diseases have always been a matter of discussion.
In 1987, a joint ILO/WHO expert committee on occupational health offered the suggestion that the term work-related diseases may be appropriate to describe not only recognized occupational diseases, but other disorders to which the work environment and performance of work contribute significantly as one of the several causative factors (Joint ILO/WHO Committee on Occupational Health 1989). When it is clear that a causal relationship exists between an occupational exposure and a specific disease, that disease is usually considered both medically and legally as occupational and may be defined as such. However, not all work-related diseases can be defined so specifically. The ILO Employment Injury Benefits Recommendation, 1964 (No. 121), paragraph 6(1), defines occupational disease as follows: “Each Member should, under prescribed conditions, regard diseases known to arise out of the exposure to substances and dangerous conditions in processes, trades or occupations as occupational diseases.”
Nevertheless, it is not always that easy to designate a disease as being work-related. In fact, there is a wide range of diseases that could be related in one way or another to occupation or working conditions. On the one hand, there are the classical diseases that are occupational in nature, generally related to one causal agent and relatively easy to identify. On the other hand, there are all sorts of disorders without strong or specific connections to occupation and with numerous possible causal agents.
Many of these diseases with a multifactorial aetiology may be work-related only under certain conditions. The subject was discussed at an international symposium on work-related diseases organized by the ILO in Linz, Austria, in October 1992 (ILO 1993). The relationship between work and disease could be identified in the following categories:
- occupational diseases, having a specific or a strong relation to occupation, generally with only one causal agent, and recognized as such
- work-related diseases, with multiple causal agents, where factors in the work environment may play a role, together with other risk factors, in the development of such diseases, which have a complex aetiology
- diseases affecting working populations, without causal relationship with work but which may be aggravated by occupational hazards to health.
Criteria for Identification of Occupational Diseases in General
Two main elements are present in the definition of occupational diseases:
- the exposure-effect relationship between a specific working environment and/or activity and a specific disease effect
- the fact that these diseases occur among the group of persons concerned with a frequency above the average morbidity of the rest of the population.
It is apparent that the exposure-effect relationship must be clearly established: (a) clinical and pathological data and (b) occupational background and job analysis are indispensable, while (c) epidemiological data are useful, for determining the exposure-effect relationship of a specific occupational disease and its corresponding activity in specific occupations.
As a general rule, the symptoms of such disorders are not sufficiently characteristic to enable occupational diseases to be diagnosed other than on the basis of the knowledge of the pathological changes engendered by the physical, chemical, biological or other factors encountered in the exercise of an occupation. It is therefore normal that, as a result of the improvement of knowledge regarding the action processes of the factors in question, the steady increase in the number of substances employed, and the quality used or the variety of agents suspected, it should be more and more possible to make an accurate diagnosis while at the same time broadening the range of these diseases. Parallel with the boom in the research in this field, the development and refinement of epidemiological surveys have made a substantial contribution towards furthering the knowledge of exposure/effect relationships, making it easier, inter alia, to define and identify the various occupational diseases. The identification of a disease as being of occupational origin is, in reality, a specific example of clinical decision-making or applied clinical epidemiology. Deciding on the cause of a disease is not an exact science but rather a question of judgement based on a critical review of all the available evidence, which should include a consideration of:
- Strength of association. An occupational disease is one where there is an obvious and real increase in disease in association with exposure to the risk.
- Consistency. The various research reports have generally similar results and conclusions.
- Specificity. The risk exposure results in a clearly defined pattern of disease or of diseases and not simply in an increasing number of causes of morbidity or mortality.
- Appropriate time relationship. The disease follows after the exposure and with an appropriate time interval.
- Biological gradient. The greater the level of exposure, the greater the prevalence of severity of diseases.
- Biological plausibility. From what is known of toxicology, chemistry, physical properties or other attributes of the studied risk, it does really make biological sense to suggest that the exposure leads to a certain disorder.
- Coherence. A general synthesis of all the evidence (human epidemiology, animal studies and so on) leads to the conclusion that there is a causative effect in its broad sense and in terms of general common sense.
The magnitude of the risk is another basic element generally used for determining whether a disease is to be considered occupational in origin. Quantitative and qualitative criteria play an important role in evaluating the risk of contracting an occupational disease. Such a risk may be expressed either in terms of its magnitude—for instance, the quantities in which the substance is employed, the number of workers exposed, the prevalence rates for the disease in different countries—or in terms of the seriousness of the risk, which may be assessed on the basis of its effects upon workers’ health (e.g., the likelihood of its causing cancer or mutations or having highly toxic effects or leading in due course to disablement). It should be noted that the figures available as to prevalence rates and the degree of seriousness of occupational diseases should be viewed with some circumspection due to the differences in procedures for reporting cases and compiling and evaluating data. The same is true for the number of workers exposed, as figures can only be approximate.
Finally, at the international level, another very important factor must be taken into account: the fact that the disease is recognized as being occupational by the law of a certain number of countries constitutes an important criterion on which to base a decision to include it in the international list. It may indeed be considered that its incorporation in the list of diseases carrying entitlement to benefit in a large number of countries shows that it is of considerable social and economic importance and that the risk factors involved are recognized and widely encountered.
To summarize, criteria for determining a new occupational disease to be added on an international list are: the strength of the exposure-effect relationship, the occurrence of the disease with specific activity or specific work environment (which includes the occurrence of the event and a specific nature of this relationship), the magnitude of the risk on the basis of the number of workers exposed or the seriousness of the risk, and the fact that a disease is recognized on many national lists.
Criteria for Identification of an Individual Disease
The exposure-effect relationship (relation between exposure and the severity of the impairment in the subject) and the exposure-response relationship (connection between exposure and the relative number of subjects affected) are important elements for the determination of occupational diseases, which research and epidemiological studies have greatly contributed to developing in the last decade. This information pertaining to the causal relationship between diseases and exposure in the workplace has allowed us to achieve a better medical definition of occupational diseases. Therefore it follows that the legal definition of occupational diseases, which was a rather complex problem before, is becoming more and more linked to the medical definitions. The legal system entitling the victim to compensation varies from country to country. Article 8 of the Employment Injury Benefits Convention (No. 121), which indicates the various possibilities regarding the form of the schedule of occupational diseases entitling workers to a compensation benefit, states:
Each Member shall:
- prescribe a list of diseases, comprising at least the diseases enumerated in Schedule I to this Convention, which shall be regarded as occupational diseases under prescribed conditions; or
- include in its legislation a general definition of occupational diseases broad enough to cover at least the diseases enumerated in Schedule I to this Convention; or
- prescribe a list of diseases in conformity with clause (a), complemented by a general definition of occupational diseases or by other provisions for establishing the occupational origin of diseases not so listed or manifesting themselves under conditions different from those prescribed.
Point (a) is called the list system, point (b) is the general definition system or overall coverage system while point (c) is generally referred to as the mixed system.
While the list system has the disadvantage of covering only a certain number of occupational diseases, it has the advantage of listing diseases for which there is a presumption that they are of occupational origin. Frequently it is very difficult if not impossible to prove that a disease is directly attributable to the victim’s occupation. Paragraph 6(2) of Recommendation No. 121 indicates that “Unless proof to the contrary is brought, there should be a presumption of the occupational origin of such diseases” (under prescribed conditions). It also has the important advantage of indicating clearly where prevention should take place.
The general definition system covers theoretically all occupational diseases; it affords the widest and most flexible protection, but leaves it to the victim to prove the occupational origin of the disease, and no emphasis is placed on specific prevention.
Because of this marked difference between a general definition and a list of specific diseases, the mixed system has been favoured by many ILO Member States because it combines the advantages of the two others without their disadvantages.
List of Occupational Diseases
Convention No. 121 and Recommendation No. 121
The ILO list plays a key role in harmonizing the development of policy on occupational diseases and in promoting their prevention. It has in fact achieved considerable status in the field of occupational health and safety. It presents a clear statement of diseases or disorders that can and should be prevented. As it is, it does not include all occupational diseases. It should represent those that are most common in the industries of many countries and where prevention can have the greatest impact on the health of workers.
Because the patterns of employment and risks are changing greatly and continuously in many countries, and because of the evolution of knowledge on occupational diseases through epidemiological studies and research, the list must be modified and added to, reflecting an updated state of knowledge, to be fair to the victims of these diseases.
In developed countries, heavy industries such as steel fabrication and underground mining have greatly diminished, and environmental conditions have improved. Service industries and automated offices have risen in relative importance. A far greater proportion of the workforce is made up of women who still, for the most part, manage the home and care for children in addition to working on the outside. The need for day care for children is increasing while these developments place added stress on women. Night work and rotating shift work have become a normal pattern. Stress, in all aspects, is now an important problem.
In developing countries, heavy industries are rising rapidly to supply local and export needs, and providing employment to these burgeoning populations. Rural populations are moving to cities in search of employment and to escape poverty.
The human health risks of some new chemicals are known, and special emphasis is given to short-term biological tests or to long-term animal exposures for the purpose of toxicological and carcinogenic incidence. Exposures of working populations in most developed countries are probably controlled at low levels, but no such assurance can be assumed for the use of chemicals in many other nations. A particularly important example is provided by the use of pesticides and herbicides in agriculture. Although there can be no serious doubt that they increase crop yields in the short term as well as increasing the control of vector-borne diseases such as malaria, we do not know clearly in which controlled conditions they can be used without major impact on the health of agricultural workers or those who eat the foods so produced. It seems that in certain countries, very large numbers of agricultural workers have been poisoned by their use. Even in well industrialized countries the health of farm workers is a serious problem. The isolation and lack of supervision place them at real risk. A prominent issue is provided by the continued manufacture of some chemicals in countries where their use is banned, in order to export these chemicals to countries where no such ban exists.
The design and function of enclosed modern buildings in industrialized countries and of the electronic office equipment within them have received close attention. Continuous repetitive movements are widely considered to be the cause of debilitating symptoms.
Tobacco smoke in the workplace, although not seen as a cause of occupational disease by itself, seems likely to be an issue in the future. Non-smokers are increasingly intolerant of the perceived health hazard from the smoke emitted by smokers in the vicinity. The pressure to sell tobacco products in developing countries is likely to produce an unprecedented epidemic of diseases in the near future. Exposure of non-smokers to tobacco smoke pollution will have to be taken as a matter of increasing consideration. Relevant legislation is already in place in some countries. A most important hazard is associated with health care workers who are exposed to a wide variety of chemicals, sensitizers and infections. Hepatitis and AIDS provide special examples.
The entry of women into the workforce in all countries underlies the problem of reproductive disorders associated with workplace factors. These include infertility, sexual dysfunction and effects on foetus and pregnancy when the women are exposed to chemical agents and workplace factors, including ergonomic strain. There is increasing evidence that the same problems may affect male workers.
Within this framework of changing populations and changing patterns of risk, it is necessary to review the list and add those diseases identified as being occupational. The list appended to Convention No. 121 should accordingly be brought up to date so as to include the disorders most widely recognized as being of occupational origin and those involved in most dangers to health. In this regard, an informal consultation on the revision of the list of occupational diseases appended to Convention No. 121 was held by the ILO in Geneva in December 1991. In their report, the experts proposed a new list, which is shown in table 1.
Table 1. Proposed ILO list of occupational diseases
|
1. |
Diseases caused by agents |
||
|
|
1.1 |
Diseases caused by chemical agents |
|
|
|
|
1.1.1 |
Diseases caused by beryllium or its toxic compounds |
|
|
|
1.1.2 |
Diseases caused by cadmium or its toxic compounds |
|
|
|
1.1.3 |
Diseases caused by phosphorus or its toxic compounds |
|
|
|
1.1.4 |
Diseases caused by chromium or its toxic compounds |
|
|
|
1.1.5 |
Diseases caused by manganese or its toxic compounds |
|
|
|
1.1.6 |
Diseases caused by arsenic or its toxic compounds |
|
|
|
1.1.7 |
Diseases caused by mercury or its toxic compounds |
|
|
|
1.1.8 |
Diseases caused by lead or its toxic compounds |
|
|
|
1.1.9 |
Diseases caused by fluorine or its toxic compounds |
|
|
|
1.1.10 |
Diseases caused by carbon disulphide |
|
|
|
1.1.11 |
Diseases caused by the toxic halogen derivatives of aliphatic or aromatic hydrocarbons |
|
|
|
1.1.12 |
Diseases caused by benzene or its toxic homologues |
|
|
|
1.1.13 |
Diseases caused by toxic nitro- and amino-derivatives of benzene or its homologues |
|
|
|
1.1.14 |
Diseases caused by nitroglycerin or other nitric acid esters |
|
|
|
1.1.15 |
Diseases caused by alcohols glycols or ketones |
|
|
|
1.1.16 |
Diseases caused by asphyxiants: carbon monoxide hydrogen cyanide or its toxic derivatives hydrogen sulphide |
|
|
|
1.1.17 |
Diseases caused by acrylonitrite |
|
|
|
1.1.18 |
Diseases caused by oxides of nitrogen |
|
|
|
1.1.19 |
Diseases caused by vanadium or its toxic compounds |
|
|
|
1.1.20 |
Diseases caused by antimony or its toxic compounds |
|
|
|
1.1.21 |
Diseases caused by hexane |
|
|
|
1.1.22 |
Diseases of teeth due to mineral acids |
|
|
|
1.1.23 |
Diseases due to pharmaceutical agents |
|
|
|
1.1.24 |
Diseases due to thallium or its compounds |
|
|
|
1.1.25 |
Diseases due to osmium or its compounds |
|
|
|
1.1.26 |
Diseases due to selenium or its toxic compounds |
|
|
|
1.1.27 |
Diseases due to copper or its compounds |
|
|
|
1.1.28 |
Diseases due to tin or its compounds |
|
|
|
1.1.29 |
Diseases due to zinc or its toxic compounds |
|
|
|
1.1.30 |
Diseases due to ozone, phosgene |
|
|
|
1.1.31 |
Diseases due to irritants: benzoquinone and other corneal irritants |
|
|
|
1.1.32 |
Diseases caused by any other chemical agents not mentioned in the preceding items 1.1.1 to 1.1.31 where a link between the exposure of a worker to this chemical agent and the disease suffered is established. |
|
|
1.2 |
Diseases caused by physical agents |
|
|
|
|
1.2.1 |
Hearing impairment caused by noise |
|
|
|
1.2.2 |
Diseases caused by vibration (disorders of muscles, tendons, bones, joints, peripheral blood vessels or peripheral nerves) |
|
|
|
1.2.3 |
Diseases caused by work in compressed air |
|
|
|
1.2.4 |
Diseases caused by ionizing radiation |
|
|
|
1.2.5 |
Diseases caused by heat radiation |
|
|
|
1.2.6 |
Diseases caused by ultra violet radiation |
|
|
|
1.2.7 |
Diseases due to extreme temperature (e.g., sunstroke, frostbite) |
|
|
|
1.2.8 |
Diseases caused by any other physical agents not mentioned in the preceding items 1.2.1 to 1.2.7 where a direct link between the exposure of a worker to this physical agent and the disease suffered is established. |
|
|
1.3 |
Biological agents |
|
|
|
|
1.3.1 |
Infections or parasitic diseases contracted in an occupation where there is a particular risk of contamination |
|
2. |
Diseases by target organ systems |
||
|
|
2.1 |
Occupational respiratory diseases |
|
|
|
|
2.1.1 |
Pneumoconioses caused by sclerogenic mineral dust (silicosis, anthraco-silicosis, asbestosis) and silicotubercolosis, provided that silicosis is an essential factor in causing the resultant incapacity or death |
|
|
|
2.1.2 |
Bronchopulmonary diseases caused by hard-metal dust |
|
|
|
2.1.3 |
Bronchopulmonary diseases caused by cotton, flax, hemp or sisal dust (byssinosis) |
|
|
|
2.1.4 |
Occupational asthma caused by recognized sensitizing agents or irritants inherent to the work process |
|
|
|
2.1.5 |
Extrinsic allergic alveolitis caused by the inhalation of organic dusts as prescribed by national legislation |
|
|
|
2.1.6 |
Siderosis |
|
|
|
2.1.7 |
Chronic obstructive pulmonary diseases |
|
|
|
2.1.8 |
Diseases of lung due to aluminium |
|
|
|
2.1.9 |
Upper airways disorders caused by recognized sensitizing agents or irritants inherent to the work process |
|
|
|
2.1.10 |
Any other respiratory disease not mentioned in the preceding items 2.1.1 to 2.1.9 caused by an agent where a direct link between the exposure of a worker to this agent and the disease suffered is established |
|
|
2.2 |
Occupational skin diseases |
|
|
|
|
2.2.1 |
Skin diseases caused by physical, chemical, or biological agents not included under other items |
|
|
|
2.2.2 |
Occupational vitiligo |
|
|
2.3 |
Occupational musculo-skeletal disorders |
|
|
|
|
2.3.1 |
Musculo-skeletal diseases caused by specific work activities or work environment where particular risk factors are present. Examples of such activities or environment include: (a) Rapid or repetitive motion (b) Forceful exertions (c) Excessive mechanical force concentrations (d) Awkward or non-neutral postures (e) Vibration Local or environmental cold may potentiate risk. |
|
|
|
2.3.2 |
Miner’s nystagmus |
|
3. |
Occupational cancer |
||
|
|
3.1 |
Cancer caused by the following agents: |
|
|
|
|
3.1.1 |
Asbestos |
|
|
|
3.1.2 |
Benzidine and salts |
|
|
|
3.1.3 |
Bichloromethyl ether (BCME) |
|
|
|
3.1.4 |
Chromium and chromium compounds |
|
|
|
3.1.5 |
Coal tars and coal tar pitches; soot |
|
|
|
3.1.6 |
Beta-naphthylamine |
|
|
|
3.1.7 |
Vinyl chloride |
|
|
|
3.1.8 |
Benzene or its toxic homologues |
|
|
|
3.1.9 |
Toxic nitro- and amino-derivatives of benzene or its homologues |
|
|
|
3.1.10 |
Ionizing radiation |
|
|
|
3.1.11 |
Tar, pitch, bitumen, mineral oil, anthracene, or the compounds, products or residues of these substances |
|
|
|
3.1.12 |
Coke oven emissions |
|
|
|
3.1.13 |
Compounds of nickel |
|
|
|
3.1.14 |
Dust from wood |
|
|
|
3.1.15 |
Cancer caused by any other agents not men- tioned in the preceding items 3.1.1 to 3.1.14 where a direct link between the exposure of a worker to this agent and the cancer suffered is established. |
In their report, the experts indicated that the list should be brought up to date regularly to contribute to harmonizing social security benefits at the international level. It was clearly indicated that there is no moral or ethical reason to recommend standards in one country that are lower than those in another. Additional reasons to revise this list frequently include (1) stimulating the prevention of occupational diseases by facilitating a greater awareness of the risks involved in work, (2) encouraging combating the use of harmful substances, and (3) keeping workers under medical surveillance. The prevention of occupational diseases remains an essential objective of any system of social security concerned with the protection of workers’ health.
A new format has been proposed, breaking down the list into the three following categories:
- diseases caused by agents (chemical, physical, biological)
- diseases of target organ systems (respiratory, skin, musculoskeletal)
- occupational cancer.
Workers' Compensation Systems, Overview
This chapter deals with compensation systems for disability (by injury or disease) or premature death resulting from employment. Its purpose is to explain the provisions and the diversity that are commonly found, but not to describe or itemize the systems of each nation.
Compensation may be provided by:
- a workers’ compensation system
- a broad-based social insurance or social security system
- an accident compensation system
- sick pay
- disability insurance
- employers’ liability.
Most industrial nations use some combination of these regimes. Part One of this chapter deals with Workers’ Compensation. Part Two deals with Other Systems.
PART ONE: WORKERS’ COMPENSATION
[Note on “jurisdiction”. This word is used to refer to a country or a unit within a country (such as a state or province) that operates a workers’ compensation system.]
Although traces of workers’ compensation can be found in earlier civilizations, particularly in Maritime Law, the systems that we now have were created in the latter half of the nineteenth century, or in the present century. The subject was known as workmen’s compensation, but the trend for the last twenty years has been to change this title to workers’ compensation, and that term is now in common use.
Coverage
Industries covered
The coverage of a workers’ compensation system is usually compulsory in relation to a specified list of industries, or in relation to all industries subject to some exceptions. Mining, manufacturing, forestry, fishing, transport, construction, distribution, health care institutions and other public services are typically covered. Examples of industries that are excluded in some jurisdictions are agriculture, service industries (such as travel agencies), and domestic service. Employers’ liability (described in Part Two) may apply to industries that are excluded. Where an industry is outside the compulsory coverage, some jurisdictions allow for the coverage to apply upon application by an employer. In some jurisdictions, employers with less than a minimum number of employees (usually in the range of 3 to 20) are excluded.
People covered
Where an industry is covered, all workers in that industry are commonly included, whether regular or casual, full-time or part-time, and whether production workers or office staff. Migrant workers usually come within the defined category of people who are covered, but the coverage may be excluded on another ground. For example, they may be employed in an industry that is not covered. There is no waiting period for the coverage to apply. Officers of corporations and other management personnel are included in some jurisdictions and excluded in others. Classifications used in the laws relating to corporations or labour relations are commonly irrelevant in workers’ compensation. Some jurisdictions exclude members of an employer’s family, and some exclude workers whose earnings are above a certain level. It is also common to exclude people whose employment is of a casual nature and who are employed otherwise than for the purpose of the employer’s trade or business. Where a worker has reached the age of eligibility for a retirement pension, that does not exclude the coverage of workers’ compensation in most jurisdictions, but it is common for the benefits to be more limited.
The nationality of a worker is generally irrelevant. All people who are lawfully employed in a covered industry are generally included, and some jurisdictions also cover those who are unlawfully employed. In some others, compensation benefits are discretionary if the worker was employed under an unlawful contract. A child born with a disability arising out of the employment of one of the parents is covered in a few jurisdictions, and in some others, the law is unsettled.
Territorial connection
The coverage generally applies to workers whose usual place of employment is within the jurisdiction. In mobile industries, such as fishing, trucking and airlines, there is usually a home port or base of the worker that is considered to be the usual place of employment of that worker. The location of the employer’s head office is generally irrelevant. It is also generally irrelevant where the payroll is administered, except that in mobile occupations, this may be part of the evidence from which to determine the home port or base of particular workers. The place of residence of a worker or dependant is generally irrelevant, though it is relevant in some jurisdictions for some purposes.
Opting-in
Unincorporated employers and the officers of corporations (where they are not within the compulsory coverage) may elect in some jurisdictions to be covered as workers. They then have the benefits and obligations of being a worker under the legislation as well as the benefits and obligations of being an employer.
Self-employed people (independent operators)
This term is used here to refer to people who earn a living by work, and who are neither employers nor employees.
Self-employed people are either:
- included in the compulsory coverage
- excluded from the compulsory coverage but may be covered upon application, or
- excluded entirely.
In some jurisdictions, people considered to be self-employed for other purposes are treated as employees for workers’ compensation. For example, in some jurisdictions, commercial fishermen may be treated as employees and within the compulsory coverage regardless of whether they are considered employees, for other purposes.
The distinction between an employee and an independent operator (self-employed person) is often controversial because of the incentive that an employer or employee may have to treat their relationship as an arrangement between independent contractors rather than as one of employment. Portraying the relationship in this way may avoid obligations to contribute to various public funds, and other obligations of an employer. Thus it is common to find that a relationship that is obviously one of employment in substance has been documented to appear as a relationship between independent contractors. To recognize such documentation as valid for workers’ compensation purposes would usually be incompatible with statutory requirements if the coverage is compulsory. Where one person is working exclusively, or almost exclusively, for another, that is cogent evidence that the relationship is one of employment. Similarly, where a contract has been signed to the effect that the relationship is not one of employment, that is usually cogent evidence that the relationship is one of employment.
Miscellaneous extensions
Some jurisdictions use the workers’ compensation system to cover people who are not employees, or to cover disabilities that did not result from employment. Usually these extensions of the coverage apply to people for whom governments have some responsibility. Examples are volunteer fire-fighters and other categories of people doing voluntary work of a charitable nature. Less common examples are prisoners, students and school-children. In some jurisdictions, the coverage applies to someone who is injured while acting in the public interest by seeking to save the life of someone in danger, or to prevent a crime. The coverage of all these groups, where it applies, is usually financed out of public funds.
Specialized systems
Some jurisdictions have a separate system for a particular industry, such as merchant seamen, the military or the public service. In federal countries, there is sometimes a system created by the federal government and limited to particular industries, while the state or provincial governments provide for the general systems.
Organization, Administration and Adjudication
Basic structures
Most systems of workers’ compensation fall into one of three basic organizational categories.
- The obligation to provide the benefits is placed upon employers. Insurance coverage is available, and in some jurisdictions it is compulsory. The insurance companies are usually subject to regulation and supervision by an agency of government. Some jurisdictions limit the number of insurance companies that may be involved. Adjudication is on an adversarial model in the ordinary courts, or in a specialized court or other tribunal.
- The system is one of social insurance operated by a government department, often a ministry of labour. Decisions are made within the department. Usually there is a system of review or appeal to resolve disputes, and there may be appeals to an outside body.
- The system is one of social insurance administered by a government agency, sometimes called a “workers’ compensation board”. Such an agency is (at least in theory) independent of ministerial control. The agency is responsible for adjudication and administration, as well as being the insurer. In some jurisdictions, the agency provides medical care and rehabilitation services, and in a few jurisdictions, it also exercises the regulatory functions of government in relation to occupational health and safety. Procedures may be adversarial or inquisitorial, or may have features of both. It can fairly be described as a social insurance system because it is a system of compulsory insurance administered by government, but it must be distinguished from the broad-based social insurance systems described elsewhere in this article.
A few jurisdictions use a mixture of insurance companies and a state fund. Large employers in some jurisdictions are allowed to carry their own risks, so that the insurance company plays the role only of claims administrator, or the government agency plays the roles of administrator and adjudicator, but has only a back-up role as insurer.
Under all three models, a worker is required to notify an injury or disease to the employer where this is possible. There are usually detailed requirements relating to such notices and to subsequent reporting. The insurer usually receives reports from the employer, the claimant and attending physicians. In some social insurance systems, an employer who fails to file a report on time is subject to a penalty or surcharge. Otherwise, such an employer is subject to prosecution. The reporting requirements of claimants are usually enforceable by the denial or suspension of benefits, but non-compliance by a claimant can often be waived, so that disqualification from benefits is not automatic. The reporting requirements of attending physicians may be enforced by suspending the payment of fees.
Traditionally, reports have been received as paper documents and the files of administering agencies have been paper files, but recently, electronic methods of communication and of information storage have been introduced.
Most jurisdictions require a claim to be filed within a specified time, though a few allow payments to commence without a claim form having been received. There is commonly a power to extend the time for filing a claim, but even so, statutory time limits can be a cause of serious injustice in some disease cases.
Primary decisions
The initial decisions made in response to a claim are sometimes made by employers, but more commonly by insurers. Where a system is administered by insurance companies, the initial decision may be the acceptance or rejection of a claim or offer made by the claimant, or it may be an offer by the insurer that can be accepted or rejected by the claimant. Commonly, a settlement is reached by negotiation. In some jurisdictions, there are provisions to prevent an insurance company from coercing a low settlement by the withholding of periodic payments. Where there is no agreement, the case may go to a court or other adjudicating body for primary adjudication.
Where the system is one of social insurance, the adjudicating body is usually also the insurer, so that the primary decision is adjudicative. It is part of the rationale for a social insurance system that disabled workers should not have to bargain from a position of weakness. They should be entitled to a prompt adjudication of their statutory rights. If a claim is allowed but the benefits are determined to be less than the claimant feels they should be, the benefits as determined are payable while the claimant pursues any appeal.
Primary decisions are commonly based on the documents on file. Administration and adjudication are heavily centralized in insurance company systems and in some social insurance systems. Local administration and adjudication enable an adjudicator to receive evidence and argument firsthand, and to test the credibility of the evidence. For these and other reasons, some social insurance systems have decentralized.
In social insurance systems, hearings are not generally held in primary adjudication, even when expressly provided for by law, though they are held in some cases in some jurisdictions. Where a system is administered by insurance companies and is officially operating on an adversary model, a hearing in primary adjudication by a court or tribunal is normal unless the employer, or the employer’s insurer, concurs in the worker’s claim, or any dispute is settled. A few jurisdictions provide for mediation. However, to require or permit mediation when one of the parties has impaired bargaining power and needs income diminishes the right to adjudication. If a system is intended to provide for continuity of income without the need for professional advocacy, the need is for prompt adjudication. This is even more important where a delay in adjudication may delay rehabilitation.
A widespread problem in primary decision-making is the use of referral systems. Under these systems, the person who receives communications from the claimant has only limited decision-making authority, so that decisions of any complexity have to be referred to someone else who has not received the evidence and arguments first hand. Commonly, different decisions on the same claim have to be referred to different people, with consequential risks of misunderstanding, mistake, and inconsistency. Such referral systems are a major cause of delay, waste, therapeutic harm, error, injustice and damage to rehabilitation prospects.
Investigation, evidence and proof
In jurisdictions using an adversarial model, the responsibility for providing evidence about the facts, and for providing medical opinions, generally lies with the parties. In some social insurance systems, the parties are expected to produce the evidence that they have and that which it lies within their power to obtain, but the adjudicating agency commonly has a responsibility for making the inquiries necessary to produce any further evidence. Similarly, investigation to test the credibility of the evidence, or for other purposes, may be a function of the parties, the insurer or the adjudicating body. In social insurance systems, investigation may be a normal function of an adjudicator, or there may be a separate investigation unit (though that is a less efficient structure for normal investigations).
In adversarial systems, and in some social insurance systems that are not adversarial, there is a burden of proof on the worker to establish a claim, though there is sometimes a burden of proof on the employer with regard to particular issues. In other social insurance systems, there is no burden of proof on anyone except the adjudicating body. Sometimes there are legislated presumptions. There is usually no general presumption in favour of or against the worker, but there are commonly presumptions that apply in particular situations. The broadest example is that where an injury resulted from an accident that occurred in the course of employment, it is presumed to have arisen out of the employment, and conversely, where it arose out of the employment it is presumed to have arisen in the course of employment, unless the contrary is shown. Some jurisdictions provide that where a worker is found dead at a place of employment, the death is presumed to have resulted from the employment unless the contrary is shown.
The standard of proof is generally the balance of probabilities. This might also be described as the best available hypothesis. With regard to the etiology of disease and some other medical issues, however, the input of the medical profession is not always controlled by the relevant legal criteria, with the result that a higher and unlawful standard of proof is often required for a claim to be allowed. One aspect of this is that when physicians are asked for advice on etiology, there is commonly a reluctance to write a report concluding that “I do not know” even when that is clearly stated earlier in the report. Thus a negative conclusion in a medical report may reflect nothing more than an assumption of the negative applied by the advising physician in the absence of positive data. It is, therefore, a conclusion of law (sometimes erroneous), not a conclusion of medicine. Some jurisdictions include a provision that where the disputed possibilities are evenly balanced, an issue must be decided in favour of the worker or dependants. Where those provisions apply, the issue must be decided in favour of the worker or dependants unless there is contrary evidence to tip the balance against that conclusion.
In some jurisdictions, the prescribed standard of proof is not the balance of probabilities on an issue of employment causation. A claim must be denied unless the affirmative is proved to a higher degree of probability than the negative. Such provisions sometimes apply only to disease cases. Even in these jurisdictions, the balance of probabilities may still be a standard of proof for other issues, such as the existence of a disability.
Some systems include a unit to investigate abuse. This may be confined to abuse by claimants, or it may include abuse by system administrators, claimants, employers, insurance companies and the providers of health care and rehabilitation services.
Advocacy
The preparation and filing of claims is usually a simple matter that does not require legal talent, and some jurisdictions prohibit the charging of legal fees for these functions. Advocacy is common in disputed claims, the more so as cases reach the higher levels of decision-making. Where experience rating applies or an employer is self-insured, there may be an advocate for the worker and another for the employer. Otherwise advocacy is normal only for the worker.
In systems administered by insurance companies, the advocates in adjudicative processes are normally lawyers. In social insurance systems, an advocate may be a lawyer, a trade union official or some other lay advocate specializing in workers’ compensation cases. In some jurisdictions, the government or the compensation authority provides a group of advocates to assist workers, and in some jurisdictions, a similar group is provided to assist employers. Sometimes, a worker may also be eligible for legal assistance under a government plan of Legal Aid.
Access to files
Where a system is administered by insurance companies, the file of the insurer is not usually accessible to the claimant, though if the case is litigated, certain documents may be obtainable from the insurer’s file, and the file of the court is usually accessible to both parties. Where a system is one of social insurance, the same body is commonly the insurer and the adjudicating tribunal, and in many jurisdictions, the file of that body is accessible to the claimant. In some jurisdictions, access to the file is allowed as a matter of procedural fairness, and it is then sometimes accessible also to the employer, at least to some extent in some circumstances, and this may result in a loss of confidentiality of medical information. Alternatively, access to the file by the claimant may be available under human rights legislation, or freedom of information legislation. An employer is generally not allowed access to a claim file on those grounds, but may be entitled on those grounds to access to the employer’s file relating to classification and assessments.
Employers sometimes need medical information for health and safety purposes, or for rehabilitation, but there are usually more efficient ways of meeting those needs than by access to a claim file.
Finality
Workers’ compensation differs from ordinary litigation in the courts with regard to finality. When a personal injury claim is made in the courts under the general law, the decision of the court is normally final. In workers’ compensation, there are usually provisions for decisions to be reopened in the event of some change in circumstances. The most common example is where a pension has been awarded for a permanent partial disability, and some years later, the disability has worsened (or rarely, the disability has been cured).
Where workers’ compensation is a system of social insurance, it is also normal to permit the reopening of decisions, even when there has been no change in circumstances. These provisions for reopening (or reconsideration) serve a useful purpose, but they are also vulnerable to misuse by system administrators. A common practice is to divert every complaint or appeal into a process of reconsideration. This has several negative consequences. One is delay in appellate adjudication, sometimes with consequential delay in rehabilitation. Another is that when, in primary adjudication, a claim seems doubtful or the evidence is incomplete, the claim can be denied, and then the decision can be reconsidered if the claimant complains or appeals. An inquiry to complete the evidence can then be made in the reconsideration process which ought to have been made in the first instance. The use of “reconsideration” in this way is a negative influence on the quality of primary adjudication and a cause of injustice to those who acquiesce in initial negative decisions.
Medical issues
Some jurisdictions require a claimant or attending physician to file a medical “certificate”. Others require the attending physician to file a “report”. A “certificate” is sometimes considered to be decisive on certain points, whereas a medical “report” is usually considered to be evidence that may be weighed in the balance with any other evidence.
Medical questions are commonly decided in the same way as other questions of fact, but some jurisdictions include special provisions for the decision of medical questions. Adjudicating agencies often have staff doctors who advise on or decide medical questions. In many jurisdictions, a claimant must submit to any medical examination arranged by the compensation authority or other insurer. In some jurisdictions, the claimant must submit to a medical examination by a physician appointed by the employer, but such provisions are controversial because of the risk of therapeutic damage and the loss of confidentiality of medical information. In fatal cases, autopsy reports are commonly used as part of the evidence relating to the causes of death. Death certificates are sometimes referred to, but they are often unreliable on the causes of death.
Medico-legal interaction involves some of the most widespread and intractable problems in the adjudication of workers’ compensation claims. Probably the most common example is the provision of medical reports by physicians who have not been informed of the legally relevant questions on which medical evidence is needed. When this happens, a “medical report” often includes, explicitly or implicitly, assumptions of background facts (which are sometimes erroneous), an opinion on law (which is commonly erroneous), as well as any medical opinion. Unravelling these components of a “medical report” requires a level of legal talent which is commonly not available in primary decisionmaking. To avoid this problem, some jurisdictions have a process whereby the legally relevant medical question is formulated before a medical opinion is sought.
In systems administered by insurance companies, it is normal for the insurer or the employer to participate in the decision of medical issues, and to have access to medical information for that purpose. Where a system is one of social insurance, one rationale for that choice is to preserve the confidentiality of medical information. Employers may be prohibited from participation in the decision of medical issues, or they may be left with no incentive to participate because the rate of assessment is one that does not vary by reference to claims cost experience. Where experience rating is used, a system becomes adversarial and medical information about a worker is commonly disclosed to the employer.
Sometimes there is also provision for an external medical referee or a medical panel to be used in some cases. In some jurisdictions, the conclusions of a medical panel or referee are final and binding. In others, the conclusions may be subject to challenge by further medical evidence or argument in the ordinary appellate process.
Where a separate structure or procedure is available for the resolution of a medical question, this requires a process to decide which questions are “medical”. The responsibility for deciding this would normally lie with those responsible for deciding the general issue. There is a broad consensus about what is a “medical” question, but there is also some diversity. For example, in cases of permanent disability in jurisdictions where the physical impairment method is used to arrive at a pension, establishing the degree (percentage) of impairment is classified as a medical question in some jurisdictions. In others, it is classified as a general question that requires an input of medical opinion.
Appeals
It is normal to have a structure for appeals. Where the system is one of social insurance, the appellate structure may be completely internal, or there may be an external tribunal. Usually this is at the final level of appeal, though in some jurisdictions, it is at an intermediate level. In some other jurisdictions, appeals lie to an ordinary court, and in others to a specialized court or tribunal. In some jurisdictions, hearings are automatic in appellate adjudication. In others, hearings are held if one is requested, or if the appellate body perceives a need for a hearing. In social insurance systems, it is normal for the appellate body, and in some jurisdictions also the parties, to have access to the file that was used in primary adjudication. This avoids wasteful duplication of effort and it may also enable the appellate tribunal to see what, if anything, went wrong in primary adjudication. The information on that file may be supplemented or contradicted by fresh evidence or argument on the appeal.
Rights of appeal are commonly unrestricted in relation to monetary benefits, but may be more limited in relation to rehabilitation assistance. Appeals on questions of medical aid are usually permitted, though in many jurisdictions they are rare.
Where an appeal lies to an ordinary court, the grounds upon which an appeal may be brought are commonly narrower than when an appeal lies to a specialized court or tribunal. Also an ordinary appellate court is less likely to review the evidence, or to receive new evidence, than a specialized court or tribunal.
Complaints to an ombudsman are available in some jurisdictions, sometimes with regard to the substance of conclusions that have been reached, but sometimes limited to matters of procedure.
Adjudicative manuals
Where a system is one of social insurance, it is normal to have an adjudicative manual comprising the law of the system, which is used as the guidance material for adjudicators. It is commonly a synthesis of the statute law, regulations, case law, and decisions made by the adjudicating or administering body in the exercise of delegated powers. Commonly it has the title of “Policy Manual”, but that is misleading. Only portions of the manual relating to the exercise of discretionary powers can fairly be called policy. For the most part, the manual is a rule book, and a part of public law.
For decades, these manuals were treated as secret documents. Use of the word “policy” in the overall title of a manual tended to disguise the fact that it was, in substance, a body of secret law. In recent years, this has commonly been recognized, and publication of the manuals has been required by statute, or by the decisions of adjudicating or administering bodies.
Eligibility for Benefits
Causation in injury cases
The general principle is that compensation is payable for injuries and deaths that result from some event or circumstance of the employment. In many jurisdictions, the legislation refers to an injury “arising out of and in the course of the employment”. There is usually no requirement that an injury or accident must have occurred in the course of the employment. The essential test is employment causation. For example, suppose that during an afternoon, A places a rat in the lunch box of B (a fellow worker), perhaps maliciously, or perhaps as a practical joke. When B opens the lunch box later at home, the rat bites B, causing a significant disability. The injury did not occur in the course of employment, but there is no requirement that it should. It arose in the course of the employment (though there may still be scope for debate about whether it arose out of the employment). Some jurisdictions, however, require that an “accident” must have occurred in the course of employment.
Some other jurisdictions refer to an injury “arising out of or in the course of employment”, but there appear to be few cases in which this difference in language would make any difference to the result. Some jurisdictions do not define a compensable disability in any general words. Instead, they have a list of circumstances that will constitute a sufficient employment connection for a disability to be compensable.
In most cases in most jurisdictions, the place of occurrence of an injury is not determinative. It is merely part of the evidence on the question of employment causation. Similarly, there is usually no requirement that an injury must have occurred during stipulated working hours. Whether it did so occur is, again, part of the evidence for deciding whether it resulted from the employment. Some other jurisdictions place greater emphasis on geographical or chronological connections with the employment, and in some jurisdictions, the injury must have occurred at a place of employment, though that may include any place where the worker was supposed to be for carrying out the work.
Some jurisdictions have a requirement that the disability must have occurred within the jurisdiction, but such requirements are incompatible with the general principle that disabilities resulting from employment should be covered. Generally, it is sufficient that the usual place of employment of the worker was within the jurisdiction in which the claim is made. Thus where the employment involves international travel, a workers’ compensation claim for a disability sustained when abroad would normally be paid by the system in the home base of the worker’s employment.
The term “work-related” is commonly found in compensation literature, but it is generally inappropriate and misleading. In most jurisdictions, there is no requirement that for an injury to be compensable, it must have resulted from work (productive activity). A few jurisdictions require that for an injury to be compensable, it must have resulted from work, but in most jurisdictions, it is sufficient that it resulted from employment. For example, an injury sustained in the course of entering or leaving the employer’s premises, or during a break period, or when receiving pay, would be compensable in most jurisdictions.
Some jurisdictions specify that an injury sustained while retraining or preparing equipment for work is covered. In many others, such an injury is covered as one arising out of and in the course of the employment.
Accident
One of the eligibility requirements for compensation used to be that an injury should have been caused by an “accident”. In some jurisdictions, that word has been repealed. In others, it is generally superfluous and misleading. Regardless of whether the word “accident” is used, compensation is not generally confined to injuries that occur on a particular occasion, or by a “specific incident”. The coverage applies also to disabilities that result from strain over time, or other causes that have a gradual or cumulative impact, and the coverage includes disabilities that result from the normal routine of work. Where the word “accident” appears in the legislation, its only significance may be to cause confusion and wasteful adjudicative costs in marginal cases. Sometimes, however, an unusual event may be crucial evidence on etiology. For example, in heart attack cases, some jurisdictions look for some unusual strain or stress to determine whether the employment was a contributing cause of the heart attack, or whether it resulted solely from natural degeneration so that its occurrence in the course of employment was purely coincidental.
Commuting
Many jurisdictions cover injuries that result from commuting to and from work, at least when the worker is travelling by the most direct route, and without any significant interruption for personal business that is unrelated to the needs of the journey. These jurisdictions usually have detailed rules about whether the coverage still applies in all the circumstances, such as where a worker travels by a longer route for reasons of personal pleasure, or where the worker stops for personal shopping in the course of the journey. Some of these jurisdictions also specifically include an injury that results from travel between work and a place of medical treatment if the treatment was required during working hours.
In other jurisdictions, injuries that result from commuting are not covered when a worker is travelling between home and a fixed place of employment. The theory is that since the worker has selected where to live and where to work, the worker has selected the journey to be undertaken and the risks of that journey are not, therefore, considered to be risks of the employment. If the worker does not have a fixed place of employment, but travels between home and different places designated by the employer, such journeys are in the course of the employment and injuries resulting from them are compensable. This is common in the transport and construction industries. Similarly, where a worker normally works at a fixed place of employment but is temporarily assigned to work at a different place, an injury resulting from a journey between home and the temporarily assigned place of work is compensable. Even journeys between home and a fixed place of employment are covered in some circumstances; for example, where a worker who is not on shift is called out by the employer to deal with an emergency, or where the worker is using transport provided by the employer.
Commencement and termination of the coverage
The coverage of any particular worker may apply for slightly longer than the contract of employment. For example, if a worker is injured upon entering an employer’s premises for the intended first day of work, that injury would be compensable in many jurisdictions notwithstanding that the formalities of a contract of employment have not yet been completed. Similarly, if a worker who has been dismissed from the employment is injured before leaving the employer’s premises, or sometimes before arriving home, that injury would be compensable in many jurisdictions notwithstanding that the contract of employment had terminated.
Fault
Workers’ compensation systems were designed to provide automatic compensation for industrial disabilities, and to avoid the cost and therapeutic damage of evidentiary inquiries about who, if anyone, was to blame. Hence it is usually irrelevant whether there was any fault on the part of the employer, the worker, or anyone else. Some exceptions to that principle are mentioned below.
Natural phenomena
Different views are taken about eligibility for compensation when a disability or death has resulted from a natural phenomenon. For example, if a worker is killed by a lightning strike, the death would be compensable in some jurisdictions but not in others. The test applied in some jurisdictions is whether the employment exposed the worker to a risk of that type of occurrence greater than the risk to which the public are normally exposed. The natural phenomena covered by this test include injuries caused by plants and animals.
Disease cases
There is more diversity among the jurisdictions in eligibility criteria for disease cases. The terms “industrial disease” or “occupational disease” are commonly used, but they are misleading and a cause of great confusion. They tend to imply that compensation is payable for and is limited to a certain category of diseases known as “industrial” or “occupational”. That is commonly not so.
In some jurisdictions, the coverage is narrowly confined. It may apply only to diseases that are specified on a closed list; but that list will not include all of the diseases commonly known as “industrial” or “occupational”. In other jurisdictions, the coverage is broadly defined so that diseases are covered to the same extent as injuries, including diseases that affect the general population and that are not known as “industrial” or “occupational”. As in injury cases, the test in these jurisdictions is whether the disease resulted from employment in the particular case, not whether the disease is of a type that usually results from employment. For example, a claim by a health care worker for tuberculosis may succeed if it is shown to have resulted from employment in the particular case, notwithstanding that the disease is prevalent in the general community.
Other jurisdictions adopt an intermediate position. The coverage is not confined to a closed list of diseases, but it falls short of the coverage in injury cases. For example, some jurisdictions require that a disease must be “peculiar to or characteristic of the employment”, or that it must be “due to the nature of” the employment. Some jurisdictions provide that no compensation (other than medical aid) is payable in a disease case unless there is both a physical impairment and a loss of earnings, even though the jurisdiction is one in which a pension would be paid for a permanent physical impairment in an injury case regardless of any loss of earnings. Some jurisdictions also have notice requirements or time limits that apply only to disease cases. Some of these time limits are unrealistic having regard to the latency periods that are common for some of the most serious diseases.
Where a disease is alleged to have resulted from exposure to contamination, evidence that the exposure of the worker to the contaminant has exceeded the maximum levels established for regulatory purposes is evidence of causation, but it is not conclusive. Evidence that the exposure of the worker was always below the prescribed limit is usually much weaker. The general principle that it is more difficult to prove a negative applies here. Exposure records of earlier years may be of unknown credibility, and they may relate to the work environment rather than to the exposure of the claimant, which could have been higher than the environmental average. Also because of variations in individual susceptibility and the scientific uncertainty behind most of the exposure limits, the disease may have resulted from the exposure of the claimant even if it always was below the prescribed limit. For these reasons, any evidence that the exposure of the worker was always below the prescribed limit is not very persuasive, and it is not a bar to a claim.
Traditionally, the lung diseases among miners and other workers in heavy industry have been prominent among the serious and fatal claims for disease. In recent years, there has been greater recognition of diseases among workers in light industry, and in office occupations, many of which are more subtle in their effects on body function. For example, it is now recognized in some jurisdictions that a claim may succeed for sealed building syndrome.
The legislation of many jurisdictions includes a schedule of diseases. It is in two columns. The first is a list of diagnoses. Opposite to each diagnosis in the second column is a type of industry, work or process that is known to cause that disease. The significance of the schedule varies in different jurisdictions. It may be:
- Exclusive and Conclusive. Only the diseases listed in the schedule are compensable. If the conditions indicated in the second column apply in a particular case, the claim is allowed. Otherwise it is denied. Evidence of etiology in the particular case is irrelevant and inadmissible.
- Exclusive and Presumptive. Only the diseases listed in the schedule are compensable. When the conditions indicated in the second column apply, the disease is presumed to have resulted from the employment. However, evidence that the disease did not result from the employment in the particular case is admissible, and so is evidence to support the presumption that it did result from the employment. Where the evidence, on balance, is sufficient to outweigh the presumption, the claim is denied. Otherwise the presumption holds and the claim is allowed.
- Presumptive, but Not Exclusive. For scheduled diseases, the position is the same as under (2) above. For an unscheduled disease, there is no presumption, but it may still be compensable. In many jurisdictions, unscheduled diseases are compensable if the evidence indicates employment causation in the particular case and the eligibility requirements relating to disease claims have been met. In some other jurisdictions, an unscheduled disease must be recognized by the adjudicating or administrating body as an industrial disease, or an occupational disease, before it is compensable, though there is no restriction on the range of diseases that may be so recognized. Recognition may be general or for the particular case. It is not a recognition that the disease fits within a preconceived category of industrial or occupational diseases. It is simply a recognition that there is no overriding policy reason why the disease should not be compensable. In some jurisdictions, unscheduled diseases are only compensable if the disability reaches a prescribed degree of impairment.
- Conclusive, but Not Exclusive. Where a disease is scheduled and the conditions in the second column apply, the claim must be allowed. Evidence of etiology in the particular cases is irrelevant and inadmissible. For unscheduled diseases, the position is the same as under (3).
In earlier years, positions 1 and 2 were commonly found, but position 3 has become more common over the last forty years. Position 4 is rare. In many jurisdictions the schedules are too limited and out of date to be of broad-scale use in relation to contemporary disabilities.
A danger of schedules that are not intended to be exclusive is that there may be a tendency, in practice, for them to become exclusive. The theory is that when a claim is made for an unscheduled disease, the evidence will be investigated to determine whether the disease resulted from employment. The danger is that this will not be done, so that in practice, the coverage tends to become confined to the scheduled diseases. Some jurisdictions seek to avoid this danger by not using a schedule at all.
It is sometimes assumed that a diagnosis is required for a disease claim, but that is usually true only in jurisdictions where compensation is confined to the diseases shown on an exclusive schedule or other closed list. In most other jurisdictions, a diagnosis is necessary for the application of any presumptive schedule, but otherwise a diagnosis is not necessary if employment etiology can be shown without one. The eligibility requirements usually relate to etiology, and if that can be shown, usually to the balance of probabilities, without a diagnosis, a disease may be compensable.
Distinction between injury and disease
Because many jurisdictions have different eligibility criteria for disease from those applicable in injury cases, it is sometimes necessary to determine whether a disability should be classified as one resulting from injury or disease. The distinction has been made pragmatically, not by reference to any principle. Hence there is no fixed rule for distinguishing between the two, but the following are common practices.
Disabilities resulting from trauma are generally classified as injuries, and any disease resulting from an injury (such as by the infection of a wound) is classified as part of the injury. Where a disease is listed, scheduled or otherwise specifically mentioned in the legislation, any such case is classified as a disease. Otherwise, disabilities that result from a specific incident are more commonly classified as injuries, while those that result from exposure over time are more commonly classified as diseases, but that is not consistently so, and there is no fixed rule to that effect. For example, sprains and strains are generally classified as injuries, whether they result from a specific incident or from exposure over time. Similarly, dermatitis is commonly classified as a disease, whether it results from a specific incident or from exposure over time, though burns caused by a single incident of chemical exposure may be classified as an injury. Hearing loss due to noise exposure is classified as an injury if it resulted from an explosion, but as a disease if it resulted from exposure over time. Disabilities caused by the gradual absorption of chemical or biological agents are classified as diseases. Allergic reactions are generally classified as diseases, whether they result from a single incident or from exposure over time.
Mental disorders—stress
Compensation for a physical disability generally includes all mental dimensions and consequences of the disability. Similarly, where a mental disorder that resulted from employment causes a physical disability, that disability is generally recognized as compensable. The language of the statutes is not generally confined to physical disabilities, so that there is no reason in principle why compensation should not also be payable where a mental disorder has resulted from employment with no physical disability being involved. In many jurisdictions, such cases are covered by the legislation, but there is often a reluctance to recognize the coverage in subsequent adjudication. In recent years, there has been an increase in claims for occupational stress, and in many jurisdictions, it falls within the meaning of injury or disease. Of stress claims that have been allowed, the stress has been caused sometimes by environmental conditions, such as temperature, sometimes by the behaviour of fellow workers or supervisors, such as sexual harassment, and sometimes by the systems of work, including claims for karoshi (death from overwork). In jurisdictions in which disabilities that result from commuting are compensable, the combined effects of commuting and what happened in the course of work are relevant in deciding whether the worker was disabled or killed by occupational stress.
Contemporary political developments, which emphasize “competitiveness” and “deregulation”, including the deregulation of overtime, have led to apprehensions about the rising incidence of occupational stress. The response in some jurisdictions has been to create a statutory bar against claims for mental stress.
Bad backs
In many jurisdictions, the largest volume of controversial claims in workers’ compensation are bad-back cases. Typically, the worker suffers a severe acute pain following lifting or twisting at work. Sometimes this is followed by chronic pain.
Bad-back claims are generally treated in one of three ways:
- The claim is accepted and paid in the ordinary way for the duration of the disability. This is very common because most bad backs resolve within a month.
- The claim is denied.
- The claim is accepted for an initial period, and then benefits are terminated on the ground that any continuing disability beyond that point is a result of an underlying disease condition rather than the employment. Typically, the medical reports indicate a degenerative disease in the spine, which is common in the general population.
The overriding dilemma in bad-back cases is that typically, there is no scientific way of establishing the long-term causative significance of any particular event at work, or of the ordinary pattern of work, compared with natural degeneration or other causative factors. The bad-back cases illustrate very graphically the difficulties of compensating or not by reference to the cause of a disability.
Death
In fatal cases, there is generally no requirement that the death must occur within any particular time of the accident, injury or disease, and a death may be compensable notwithstanding that it occurs many years after termination of the employment in which it was caused. A death resulting from a self-inflicted injury is not generally compensable, but a suicide is compensable in some circumstances; for example, if a compensable injury that was not self-inflicted caused a serious depression that led to the suicide. A few claims have also been allowed for suicide resulting from the process of dealing with the compensation authority.
Multiple Causes of Disability
Controversies commonly arise when a disability has resulted from the combined effects of an event or circumstance of the employment and another event or circumstance that is unrelated to the employment. An example would be lung cancer that appears to have resulted from the combined effects of industrial contamination and smoking. In many jurisdictions, a claimant is entitled to compensation if the employment was a significant contributing cause of the disability, notwithstanding that non-employment factors were also causative. Some jurisdictions require the adjudicator to select the predominant or primary cause, but that makes the result a matter of arbitrary choice if the reality is that the disability would not have occurred in the absence of either cause, or if it is unknown whether the disability would have occurred in the absence of either cause.
In some jurisdictions, there are provisions for apportionment, so that a claimant is entitled to compensation, but only at a reduced level of benefits. Such provisions are difficult in adjudication, mainly because there is commonly no scientific way of deciding in what proportion the disability should be attributed to the different causes. Another difficulty with such provisions is that the resulting benefits may be below the level of social security (welfare) to which the claimant would be entitled if there were no workers’ compensation claim. To avoid the hassle of a disputed compensation claim, therefore, the claimant may apply for and receive social security (welfare) benefits. To the extent that this happens, the cost of occupational disability is shifted from the workers’ compensation system onto general revenue.
Where a contributing cause of a disability was a susceptibility or a pre-existing condition of the claimant, that is usually just as irrelevant to the level of compensation as it is to eligibility. This would seem fair if the wage rate on the claim is the rate that the claimant was able to earn with the pre-existing condition. However, susceptibility or a pre-existing condition may be relevant to the duration of benefits. Where a pre-existing condition is aggravated by an event or exposure of the employment, the aggravation may produce a compensable disability, but if the aggravation is temporary, eligibility for compensation will terminate on the expiry of the aggravation.
Where some circumstance of an employment had causative significance in producing a disability, it is generally compensable notwithstanding that the claimant was already allergic to that type of disability. Where some circumstance of an employment caused an allergy that the worker did not previously have, any subsequent periods of disability caused by subsequent allergic reactions are usually compensable regardless of whether a subsequent allergic reaction was triggered by anything relating to employment. Thus in allergy cases in jurisdictions in which the critical etiological requirement is that the employment should have been a significant contributing cause, it is sufficient for compensation if the employment either caused the allergy or triggered the reaction.
Subsequent Consequential Disabilities
Where a disability is compensable, any other disability that is subsequent and consequential is also compensable. For example, where a compensable injury becomes infected, any consequential disease is compensable. Where a worker sustains a compensable disability for which medical treatment is undertaken, and that treatment causes another disability, that is also compensable. For example, if a claimant falls down the stairs at a clinical rehabilitation facility when attending for treatment, any injury resulting from that fall would generally be considered compensable. However, where the connection between the original and subsequent disabilities is indirect, diverse views are taken. For example, if the second injury resulted from a motor vehicle accident when driving to a rehabilitation facility, that would be compensable in some jurisdictions, but not in others.
Where a subsequent disability is more distant in time, place, or causal connection, it may be considered too remote to be compensable. Suppose, for example, that a claimant sustained a compensable leg amputation. Ten years later, the claimant is run down by a motor vehicle when on a vacation. An argument might be made that the claimant could have avoided the second accident if it were not for the prosthesis, so that the second disability is a consequence of the first. Even if the causal connection is established as a matter of fact, it would probably be concluded that any disability resulting from the motor vehicle accident is “too remote” to be considered a compensable consequence of the amputation. Also if the leg amputation resulted in a pension measured by the degree of physical impairment, one of the factors taken into account in establishing a percentage rate is the limitation on body movement. Where that is so, if that same limitation of body movement were to produce further compensation when it has resulted in a known monetary loss, it would be arguable that the claimant is receiving compensation for the same factor twice over.
Compensable Losses
The most common types of compensable loss are economic. Thus the most common benefits are medical care and compensation for loss of income or earning capacity, but many jurisdictions also pay benefits for physical or mental impairment, and for disfigurement, regardless of the economic consequences. Property damage is generally excluded, though compensation is commonly payable for damage to eyeglasses, dentures or a prosthesis. A few jurisdictions also provide compensation for damage to clothing.
Multiple Disabilities
Where a claimant has two or more compensable disabilities with the same date of commencement, they are generally aggregated for the calculation of compensation, but the total payable cannot exceed what would be paid for a total disability. Where two or more compensable disabilities occurred on different occasions, they are usually treated as separate claims. Benefits are calculated separately in respect of each, and different wage rates may apply. A worker may, therefore, be eligible for benefits concurrently under two or more claims. This is normal, for example, when a worker is receiving a pension calculated by reference to the degree of physical impairment in respect of a permanent partial disability, has returned to work, and then sustains a further injury causing a temporary total disability. In some jurisdictions, there is a maximum applicable to the combined total of benefits that may be received at any one time under all claims, but not in others.
Where a claimant has two or more disabilities, not all of which are compensable, problems can arise in deciding which losses are attributable to each. This is not usually a problem where the compensable disability is the most recent. General principles normally require that compensation must be paid for loss of earnings if, prior to the compensable disability, the claimant was working with the non-compensable disability. Where compensation is supposed to be payable by reference to actual loss of earnings and the non-compensable disability is the most recent, there may be adjudicative difficulties in deciding whether the compensable disability is currently causative in relation to any absence from work.
Objections to Claims
The objections most commonly raised are that a claimant has not met one or more of the eligibility requirements. Even when those requirements have been met, there may still be a few grounds on which an objection can be raised. Because workers’ compensation systems were generally established to avoid evidentiary inquiries on questions of fault, any allegation that a disability resulted from the negligence of the claimant is generally irrelevant, and so is any allegation that the cause of the disability was outside the control of the employer.
A self-inflicted injury is not compensable. It is usually excluded in the definition of a compensable injury or accident, but sometimes there is an express bar. To be excluded, the injury must have been deliberately inflicted by the claimant. It is no bar to a claim that the claimant deliberately undertook the risk of injury.
Some jurisdictions provide that misconduct of a claimant is or can be a bar to a claim, but in most jurisdictions this bar can only be raised in exceptional cases. To avoid having evidentiary inquiries on questions of fault as a normal routine, this bar is confined in various ways. In some jurisdictions the bar only applies if the misconduct is criminal or gross, and in others, if it is serious and wilful. Some jurisdictions provide that the bar does not apply in fatal cases, or where a disability is serious or permanent. In some jurisdictions, it is a requirement for the bar to apply that the misconduct must have been the “sole cause” of the disability, and very few injuries are caused solely by anything.
Where misconduct bars a claim, it is usually a bar to all benefits, though some jurisdictions permit a reduction of benefits for misconduct.
One explanation for the reluctance to allow allegations of misconduct is that in serious and fatal cases, innocent dependants could suffer. In minor injury cases, allowing issues of misconduct to be raised would defeat the goal of economy in adjudicative costs. Related to this, most systems are not organized to conduct an evidentiary inquiry in primary decisions, and it would be unfortunate to allow allegations of misconduct to be raised if the system is not designed to make a fair judgement upon them.
It has sometimes happened that a claim has been barred on the ground that misconduct took the worker outside the course of the employment, but that is a very difficult ground on which to bar a claim. Unless great care is taken, it can have the effect of barring a claim for misconduct in circumstances in which the statutory limitations on that bar do not apply. The point can be illustrated by cases of injuries resulting from horseplay. A worker injured by horseplay is not outside the course of employment if the worker was an unwilling participant, or had not made any substantial deviation from productive activity, or if the horseplay was an ordinary part of human nature in the ordinary course of employment, or if it was simply a more entertaining way of doing the work. However, if the worker was completely removed from any productive activity and was an initiator or a willing participant in the horseplay, it may be legitimate to decide that the injury did not arise in the course of the employment. In other circumstances, a claim may only be barred for horseplay if the statutory criteria relating to misconduct have been met.
In some jurisdictions, a claim is barred if the disability was caused by the intoxication of the worker from alcohol or drugs. This bar may not apply to all claims. For example, it may not apply to fatal cases. In other jurisdictions, intoxication is generally irrelevant except that it may be a species of misconduct, in which case, the objection is subject to the limitations that apply to an allegation of misconduct.
In some jurisdictions, a claim may be barred if the disability resulted from non-compliance by the worker with occupational health and safety regulations, or with safety rules issued by the employer. However, this bar can tend to undermine the incentive for employers to engage in proper health and safety planning. If an employer can issue rules, or seek the issuance of regulations, requiring workers to protect themselves from hazardous conditions by appropriate behaviour, this could reduce the incentive to avoid or minimize the creation of hazardous conditions by proper planning. A related problem is that the behaviour of workers is to some extent self-initiated and to some extent conditioned by the decisions of employers. Thus it would be difficult to legislate this bar without getting into evidentiary inquiries on fault. It may be for these reasons that this bar is not widespread.
In some jurisdictions, a claim for disease may be barred because of fraudulent misstatements previously made by the worker. There are practical problems with these provisions. In particular, it would be hard to prove that a statement was made fraudulently if the worker merely signed a printed form on an occasion that was not conducive to reading and contemplation.
It is sometimes alleged that a worker was susceptible to the disability that occurred, but that is generally irrelevant.
In some jurisdictions, the parents of a child who was killed are not eligible for compensation if the child was employed contrary to the laws relating to child labour.
The availability of benefits from another source is usually irrelevant. Workers’ compensation systems are generally in the position of first payer, so that eligibility for benefits from another source is not a bar to a workers’ compensation claim. In some jurisdictions, however, there are some provisions for a reduction in workers’ compensation benefits if there is eligibility for benefits from another source.
The non-payment of assessments by an employer is not usually a bar to a claim in social insurance systems. In systems administered by insurance companies, non-payment of the premium by an employer may extinguish the liability of the insurer, leaving the claimant only with a claim against the employer.
Where an objection to a claim is valid, it is usually a total bar. However, some jurisdictions provide that certain objections may have the effect of reducing benefits. For example, a few jurisdictions provide that misconduct by a worker may have the effect of disentitling the worker from monetary benefits for an initial period of a week or two weeks.
Employer Misconduct
In most jurisdictions, misconduct by the employer is irrelevant to the validity of a claim, except that it may be part of the evidence on the general question of whether a disability resulted from employment. In some jurisdictions, however, additional benefits, or higher levels of benefits, are payable where a disability resulted from misconduct of the employer. Some of these provisions are narrow, referring only to criminal misconduct, to “gross” negligence, or to serious and wilful misconduct. Others are broader, referring to negligence or a breach of occupational health and safety regulations. These provisions are part of the workers’ compensation system, and are unrelated to “employers’ liability” (discussed in Part Two). These provisions are open to the same objection as provisions relating to misconduct by workers; that is, they may require an evidentiary inquiry in the context of a system that was designed to operate, as far as possible, without evidentiary inquiries. For this reason, some jurisdictions confine the provision to cases in which the employer has been convicted in a criminal court.
In jurisdictions in which a claim may be barred because of intoxication by the worker, or a wilful failure of the worker to comply with safety rules, it is sometimes provided that the bar will not apply if fault can be shown on the part of the employer.
Medical Aid
In some jurisdictions, disabilities resulting from employment are treated in the same way as other disabilities under a government system of medical care. In other jurisdictions, the workers’ compensation system provides the medical aid for compensable disabilities. This may be extensive, including the attendances of medical practitioners and other health care professionals, hospital care, surgery, prostheses, appliances, drugs, dental care, orthopaedic footwear and therapies required for rehabilitation. Where a claimant is entitled to a prosthesis or other appliance for a permanent disability, subsequent servicing and replacements are also provided. Medical aid is commonly provided on a full indemnity basis for all necessary services, even though monetary compensation benefits for economic losses are less than a full indemnity. Thus in some jurisdictions, the medical aid coverage in workers’ compensation is more extensive than the coverage under the general government system. In countries that have no government system of medical care, the medical aid provided in workers’ compensation cases can be a striking contrast to the medical care that is otherwise available, and to the medical insurance coverage that is otherwise available to workers. However, in some jurisdictions, there are restrictions on the medical aid that may be provided. For example, treatments that may be considered “experimental” are sometimes excluded.
Travel costs and other expenses incurred by a claimant to receive medical aid are usually covered, but many systems restrict the level of reimbursement to the cost of using public transport unless that is unavailable or inappropriate.
Some jurisdictions have separate workers’ compensation hospitals, rehabilitation clinics, or other health care facilities. Otherwise, workers’ compensation cases are treated at the same hospitals and other places of medical treatment, and by the same personnel, as other cases. The only difference between the workers’ compensation cases and the others may relate to the sources of payment. Sometimes, however, there are also other differences. For example, a workers’ compensation authority may contract with a general hospital for additional services in workers’ compensation cases.
It is not usually a condition of eligibility for medical aid that the claimant should be impeded from work, or otherwise entitled to money payments. Thus a large proportion of workers’ compensation claims are for medical aid only. In jurisdictions that use experience rating, the pressures not to report employment injuries to the workers’ compensation authority or insurer sometimes result in medical care being provided under the general health care system rather than under the medical aid provisions of workers’ compensation.
Usually the obligation to provide medical aid is placed upon the insurer (whether a government agency or an insurance company), but there is commonly an obligation upon the employer to provide medical aid for the initial phase of an injury, such as first aid and ambulance transportation to a hospital. Usually payments for medical aid are made directly by the insurer to the provider of the treatment or service. In most jurisdictions, it is considered inappropriate to require the claimant to pay and then claim reimbursement. That could create a cash-flow problem for people whose incomes have been reduced by their disabilities. It could also facilitate overcharging by service providers, leaving claimants caught in the middle and having to bear the excess cost.
In systems administered by insurance companies and where medical care is otherwise a matter for the market, and where there are no other controls on overservicing, workers’ compensation claimants may be required to receive their care at a limited range of hospitals and other health care facilities, and their choice of attending physicians may be limited.
Some jurisdictions provide that compensation benefits may or must be suspended or terminated if a claimant unreasonably declines to accept medical treatment that is offered; but these provisions are usually relevant only in very exceptional cases where the refusal is equivalent to a self-inflicted injury. Workers’ compensation legislation was not usually intended to stifle patient choice in medical care, or to negate the basic human right to be selective in the acceptance of treatment. Also in at least some jurisdictions, compensation authorities are more concerned to prevent the overuse of drugs and surgery than to prevent their underuse.
In some jurisdictions, there are temporal or territorial limits on the provision of medical aid. In others, medical aid for a compensable disability is provided as it is needed for the lifetime of the worker and regardless of any change in the worker’s country of residence. In these jurisdictions, this feature distinguishes medical aid under workers’ compensation from the coverage under general government systems of medical care.
Money Payments
Wage rate
The calculation of monetary compensation usually begins by establishing an earnings level or wage rate for the claim. This is usually the gross level of earnings of the worker (including overtime pay) at the time of disability, or the average earnings during some preceding period, usually in the range of four weeks to three years. The rate of compensation is then set by reference to this wage rate. There are sometimes provisions for a wage rate to be established by reference to the average wage in an industry, or a national average, but such provisions only apply in exceptional situations.
Unlike the process of assessing of damages on employers’ liability claims, establishing the wage rate does not usually include any speculation about what changes to the earnings of the worker would have occurred in the future but for the disability. In relation to cases of long-term and permanent disability, however, there are commonly provisions to the effect that where a worker became disabled when a learner, apprentice or student at the early stages of a career, the wage rate will be subject to upward adjustment to the basic earnings level of that career.
Each jurisdiction usually has detailed rules relating to the calculation of previous earnings; for example, whether notional earnings should be attributed to free board and lodging provided by the employer, whether concurrent earnings from other employment or self-employment should be excluded or modified, or whether earnings from seasonal employment should be adjusted to an annual average.
Some diseases sometimes result in a gradual erosion of earning capacity as the worker moves to lighter and less rewarding employment. If a claim is not filed until a total cessation of work, it would not compensate for the loss if the immediately preceding level of earnings was used as the wage rate on the claim. To meet this problem, some jurisdictions provide for the wage rate to be set by reference to the contemporary earnings of other workers in the occupation in which the disease was contracted.
Where the coverage applies to a self-employed worker, the wage rate is usually set at the time when the coverage is arranged. In jurisdictions in which the self-employed are covered only upon application, an applicant may be allowed to nominate the wage rate, subject to a minimum and maximum, and subject to rejection of the application if the nominated rate appears to be out of line with potential earnings. The rate established at the time of coverage is then used for calculating the assessment (premium) as well as for the subsequent calculation of benefits in the event of a compensable disability.
In some jurisdictions, the wage rate remains fixed for the duration of the claim. In others, it is subject to change after a specified period. Usually the rationale for the change is that the wage rate for long-term and permanent disabilities should be changed to reflect a longer period of average earnings prior to the disability. Switching to a longer period of average earnings makes it easier to include earnings from all sources, to take account of variations in overtime, and to take account of seasonal or other variations in the continuity of employment.
Usually, the rate reflects the average gross earnings of the worker (excluding the employer’s contributions to employee benefits), but in some jurisdictions where compensation benefits are not taxable income, the wage rate is adjusted to a notional “net” earnings before the compensation rate is derived. The notional “net” is the gross amount less amounts for income tax and other payments to government funds that are deductible from earnings.
The compensation rate
Usually there is a formula for moving from the wage rate to a rate of compensation that is payable for total disability. This rate is usually a percentage of the wage rate, or of the notional “net” earnings that have been derived from the wage rate. It is usually less than a full indemnity for lost earnings. One rationale for this is the theory that the difference between the wage rate and the compensation rate represents the worker’s contribution to the cost of occupational disability. This rationale is dubious, bearing in mind that the assessment (premium) is, to some extent, an opportunity cost of labour. A more realistic rationale is that the difference between the wage rate and the compensation rate provides an incentive for an injured worker to return to work. A difference of 10% is usually considered sufficient for this purpose. This rationale has no significance in relation to disabilities that are severe and permanent.
The ceiling—maximum
Usually a ceiling (maximum) is prescribed, either for the wage rate or for the compensation rate. A historical rationale for a ceiling was that workers with earnings above the ceiling could, if they wished, insure those earnings by taking out their own policies of accident and sickness insurance. However, this rationale was never in accord with reality. There were no policies on the market that were available to industrial workers and that would pay benefits to compensate for the higher levels of earnings loss for the duration of a disability.
Where a ceiling applies to the wage rate, and a worker suffers a compensable disability with a loss of earnings, but still has residual earnings above the ceiling, it may be thought an injustice that the worker has suffered a loss of earnings from an occupational disability and is not receiving compensation. This problem can be avoided by applying the ceiling to the compensation rate, or by compensating by reference to the degree of physical impairment regardless of actual earnings loss, or by having no ceiling at all.
Another problem with a ceiling on the wage rate is that the same ceiling is then generally used on the level of earnings on which the assessments (premiums) must be paid. For example, if the ceiling is 50,000 monetary units per year, this means that the maximum level of compensation will be a percentage of 50,000 units per year. The assessment paid by an employer will be a percentage of the payroll, but subject to a ceiling of 50,000 units per year per worker. This ceiling on the assessment can be one of the factors making it cheaper for an employer to require regular overtime rather than increasing the size of the workforce. It may, therefore, be considered counter-productive in terms of social policy, occupational stress and the rehabilitation of disabled workers.
Classification of disabilities
Some jurisdictions classify compensable disabilities as temporary total, temporary partial, permanent total or permanent partial. The same disability will often move from one of these classifications to another. Some jurisdictions do not use all of these categories. Some use a variation of them, or may apply similar principles without classifying disabilities in these terms. In recent years, some jurisdictions that are supposed to compensate by reference to actual loss of earnings have abandoned the use of these classifications altogether.
Temporary total disability
Most jurisdictions pay benefits for temporary total disabilities. As well as transitory disabilities, this category includes the initial stage of most permanent disabilities. In some jurisdictions, there is a time limit for these benefits, but usually there is not. The benefit continues until the claimant makes a total or partial recovery, the disability is classified as permanent, or the claimant dies. In some exceptional cases, the benefit may be terminated by disqualification, such as where a claimant has left the jurisdiction during the period in which medical attention was required.
Since the vast majority of occupational disabilities are minor and temporary, this benefit is paid for only a few days in most cases—too short a time in many situations to make it worth the cost of considering whether the case should be processed as temporary partial. In some jurisdictions, the level of this benefit is reduced after a specified period, or reduced in stages after two or more specified periods, such as three months and six months. Such reductions are not usual in advanced industrial nations.
This benefit usually commences on the day following the incapacity for work, but in some jurisdictions there is a waiting period of three days. In some systems, the employer has an obligation to pay this benefit for a brief initial period, with the obligation of the insurer commencing after that. Such provisions can cause problems in the context of a workers’ compensation system. For example, they may delay the collection by the insurer of evidence about the cause of the disability.
Apart from compensation, some jurisdictions require an employer to continue the earnings of a disabled worker for a very brief initial period, commonly for the day of injury.
Temporary partial disability
Some jurisdictions do not use this classification at all. Others use it where a claimant has made a sufficient recovery from the disability to engage in some work, but is not yet able to return to the regular occupation. In most cases in many situations, it is not worth the administrative and adjudicative cost of using this classification because the claimant will be fit to return to the regular occupation in any event within a few days.
In jurisdictions that use experience rating, or in which employers otherwise have a financial incentive to invoke this classification, there are substantial administrative and adjudicative difficulties in deciding what type of work is suitable to the current condition of the claimant. The fear of abuse of the system by claimants creates a reluctance to let the worker decide, and there would be comparable difficulties in allowing the employer to decide. To have the matter decided adjudicatively creates the problem that disputes about what is suitable work for a particular medical condition cannot be resolved fairly and efficiently without an evidentiary inquiry. Most systems are not designed to conduct one promptly, and some do not provide for one at all, except on appeals. Decisions made on such issues in more peremptory ways are a cause of therapeutic damage, as well as injustice and waste. They can also create a strain in the employment relationship that becomes an impediment to rehabilitation. It is partly for these reasons that some jurisdictions prefer to avoid or minimize the use of this category.
For cases that are classified as temporary partial, the rate of benefit is commonly a percentage of the difference between the previous earnings of the claimant and the current earnings, or the amount which it is thought that the claimant could be earning (“deemed” earnings). In a few jurisdictions, the rate of benefit is required to be calculated by reference to the degree of physical impairment, but that is unrealistic. The period during which this classification may be applied is usually too short, and the gravity of the disability may be changing too fast, for the rate of benefit to be calculated in this way. Some jurisdictions exclude compensation for a temporary partial disability if the impact on earning capacity, or on earnings, is minor.
Some jurisdictions require the presence of a claimant within the jurisdiction as a condition of continuing eligibility for temporary benefits. Others require presence only during the period in which medical treatment is needed.
Permanent total disability
In many jurisdictions, severe disabilities are classified as total regardless of the impact on earnings or earning capacity. For example, total blindness, paraplegia or the loss of two limbs are commonly classified as permanent total disabilities. One rationale is that compensation should be paid for the disability itself, regardless of its economic significance. Another is that disabilities commonly involve costs, and therefore economic losses, regardless of the impact on earnings. Perhaps the most important rationale is that the payment of a fixed pension without inquiry into economic loss preserves the freedom of the individual, alleviates anxiety and maximizes the incentive to rehabilitation. A few jurisdictions provide for a lump sum in addition to the pension.
In some other jurisdictions, benefits for permanent disability are payable by reference to loss of earnings, so that benefits for permanent total disability are only payable where it is estimated that the loss of earnings will be permanent and total. In some cases, particularly among older workers, this may be the economic significance of a disability even when the degree of physical impairment is low. In such cases, however, there is commonly a reluctance to recognize that the loss of earnings resulting in the disability is likely to be permanent and total.
Where a case has been classified as one of permanent total disability, a pension may be payable for life or until a standard retirement age, but in some jurisdictions, it is for a more limited duration. The formula for calculating the pension may be the same as for temporary total disability benefits, but in some jurisdictions, a different formula is used. In particular, the wage rate on the claim may be adjusted as mentioned under Wage rate (above).
In systems administered by insurance companies, the right to periodic payments for a permanent disability is often settled for a lump sum, but some jurisdictions provide for annuities.
Permanent partial disability
This classification refers to permanent disabilities that are not classified as total. The methods (described below) that are used for estimating the degree of partial disability are also commonly used for distinguishing total from partial. Compensation for a permanent partial disability is commonly paid in a lump sum for minor and less serious disabilities, and in periodic payments for those that are more serious. A pension may be payable for life or until a standard retirement age, but in some jurisdictions, it is for a more limited duration.
Except for minor disabilities, a fixed pension has great advantages compared with a lump sum. Where the compensation is intended primarily for any future loss of earnings and some of the future costs of the disability, a pension has the great advantage that it can be paid for exactly the duration of the loss. A lump sum would require estimating an expectation of life, and in almost every case, that estimate would be wrong. Also lump sums tend to be spent in a relatively short time, and a claimant may then be supported out of general revenue. A fixed pension offers the best protection for the social security (welfare) budget.
How to calculate the benefits for permanent partial disability has been the most intractable problem in the history of workers’ compensation. Basically, three methods are used.
Physical impairment method
This method of calculating a fixed pension has been traditional and widespread in workers’ compensation, as well as for military pensions. Compensation is calculated by reference to the estimated degree of physical and mental impairment resulting from the disability. Rating schedules are commonly used that attribute percentage rates to a list of disabilities. In some jurisdictions, the rating schedule is rigidly followed. In others, the schedule is used as a guide. Variations are sometimes permitted or prescribed. One example is where there is some aggravating factor.
The content of these schedules is often criticized as too orthopaedic. For example, amputations commonly have a percentage rate that seems high, having regard to modern prostheses. More subtle disturbances of body function are commonly rated low, compared with their impacts on the lives of the claimants. A more comprehensive schedule is produced by the American Medical Association. This is used in some jurisdictions, either exclusively, or as a reference source when the primary scheduled used in the jurisdiction does not cover a particular disability.
Regardless of how a percentage rate is established, a pension is then calculated by applying that percentage to what would have been paid if the claimant had been classified as totally disabled. In jurisdictions that use this method, the schedule is also commonly used to distinguish total from partial disability. For disabilities that are rated below a certain percentage (commonly 10%) a lump sum is generally paid instead of a pension. This may be calculated by using the same calculations as for a pension, and then commuting the resulting pension to a lump sum, or some other method may be used for arriving at the lump sum. Since the vast majority of permanent disabilities are minor, the majority of awards for permanent partial disability take the form of a lump sum. A few jurisdictions provide that minor disabilities are not compensable.
Lump sums for minor disabilities, rather than pensions, have the advantage of avoiding ongoing administrative costs, but they can create a problem in some situations, such as where a worker suffers successive minor disabilities that become cumulative in their impact. There is the risk that the worker will become substantially disabled but without eligibility for a pension. A similar problem can arise when a lump sum has been awarded for a minor disability which deteriorates later to become more serious. If the deterioration is gradual, successive lump sums might be awarded for the same disability, and again, the end result may be a substantial disability without eligibility for a pension. In anticipation of this problem, some jurisdictions insist on a pension, rather than a lump sum, even for a minor disability, if the condition is unstable, or if it is considered prone to deterioration.
For unscheduled disabilities, most jurisdictions adopt one of four positions.
- A percentage rate is established by extrapolation from the schedule, using the schedule figures as benchmarks.
- Unscheduled permanent disabilities are compensated by using one of the other methods of calculation (described below).
- Unscheduled permanent disabilities do not receive benefits beyond those provided for a temporary disability, though temporary benefits may continue.
- Periodic payments terminate after a specified period notwithstanding that the disability, and any consequential losses, continues.
A major advantage of the physical impairment method is that it maximizes the incentive to rehabilitation while preserving its voluntariness and the civil liberties of the claimant. In jurisdictions that have a ceiling on the wage rate for the claim, this method also has the advantage that a pension is payable notwithstanding that there may be no loss of earnings below the ceiling.
Since evidence of actual loss of earnings is irrelevant under this method, a pension is paid notwithstanding that there may be no loss of earnings. That is considered a price worth paying to maximize the incentive to rehabilitation and to avoid the other disadvantages (mentioned below) of attempting to calculate compensation by reference to actual loss of earnings. Also the cases in which there is no apparent loss of earnings are commonly cases in which the claimant is continuing to work for the same employer. The economic impact of the disability may be more severe if the claimant is later in search of employment on the open labour market. Also the pension awarded by this method is usually the only compensation for non-monetary losses, and that rationale for the pension is independent of any actual loss of earnings.
Pensions awarded under this method are subject to reopening upon application by the claimant in the event of a deterioration in the condition. In some jurisdictions, the pension can also be reopened at the initiative of the compensation authority, insurer or employer, in the event of the disability being cured. This is rare, because disabilities are not generally classified as permanent until there is no realistic prospect of further cure. However, it can happen occasionally when medical research produces a cure that was not previously known.
The use of this method is sometimes abandoned in favour of the actual loss of earnings method (mentioned below), but the physical impairment method is sometimes reinstated when the difficulties and injustices of the actual loss of earning method have been rediscovered.
The projected loss of earnings method
This is an alternative method of arriving at a fixed pension and is used in a few jurisdictions. A pension is calculated by estimating the extent to which the earnings of the claimant are likely to be reduced by the compensable disability in the long run. In most cases, the claimant will have resumed employment by the time that the calculation is made, so that current earnings can be used as a starting point. It then has to be considered whether those earnings are more or less than the long-term earnings potential. Where a claimant has not resumed employment, the calculation can be more difficult; but since it only has to be made once in those cases, it is feasible to do it by an evidentiary inquiry where that is requested or otherwise seems appropriate. Statistical data are generally not of much use for this purpose. They cannot be used exclusively, or as the primary evidence, and if they are used at all, there is a danger that they will become a diversion from the facts of the particular case.
Like the physical impairment method, this method preserves the incentive to rehabilitation, its voluntariness and the civil liberties of the claimant. Also, like the physical impairment method, a pension awarded under this method is subject to re-opening in the event of a deterioration in the condition. The pension is, however, not subject to re-opening in the event of any change in the actual loss of earnings. This method avoids, therefore, most of the problems (mentioned below) of the actual loss of earnings method. Since this method takes no account of the expenses of the disability, or of non-monetary losses, it may be used in conjunction with other benefits.
Actual loss of earnings method
This method of compensating for permanent disability, which is used in some jurisdictions, does not provide any fixed pension. Periodic payments are supposed to be made according to the estimated actual loss of earnings resulting from the disability. These periodic payments are subject to variation according to changes in the estimated actual loss of earnings. In some jurisdictions, the payments are reconsidered from time to time when there is any change in actual earnings. In others, the payments are reconsidered at fixed intervals, sometimes yearly.
One problem with this method is the difficulty of estimating, as time goes by, the impact of the compensable disability on the earnings of the claimant compared with the impact of other factors, such as subsequent disabilities, natural ageing, technological change or political or economic changes that affect the labour market.
Another major problem with this method is the response to the risk of a claimant earning less than could be earned. The usual response is to “deem” each claimant to be earning what he or she is considered to be capable of earning. The use of such “deeming” provisions has been one of the greater causes of injustice and resentment in the history of workers’ compensation. While the initial intention was often that deeming should only be done by way of exception, it becomes the normal routine when the actual loss of earnings method is used. Claimants are “deemed” to be capable of earning in a “phantom job”; that is, a job that is unavailable to them. “Deeming” is also applied when a claimant declines to undertake a job because of health or moral objections. Compensation benefits are then commonly terminated while the disability and its consequential economic losses continue. In the jurisdictions in which this method is used, the periodic payments are usually the only compensation that a claimant receives for the economic losses resulting from a permanent disability. It is not part of the legislative prescription that these periodic payments should be temporary, but that is commonly the practical result of “deeming”.
Another injustice results from the way in which this method deals with career progression. Under a fixed pension system, a claimant loses the benefit of career progression in the pre-morbid occupation, but retains the benefit of any career progression in any subsequent occupation. Under the actual loss of earnings method, the claimant loses the benefit of any career progression in the pre-morbid occupation and also loses the benefit of any career progression in any subsequent occupation.
“Deeming” provisions also create a pressure to undertake any rehabilitation measures that the compensation authority may recommend (or require) regardless of whether they accord with the rehabilitation aspirations of the claimant, so that the voluntariness of rehabilitation is lost, and the ordinary civil liberties of the claimant may be impaired. For example, even the basic human right to move to another country may be lost or impaired when this method is used. For this reason alone, the use of this method can cause serious injustice when a migrant worker is disabled.
Another concern is that this method creates apprehensions about rehabilitation, as well as disincentives. If ongoing success is uncertain in relation to any employment opportunity, claimants are sometimes fearful of trying the employment in case it does not work out. The risk is that termination of the employment may then be attributed to reasons other than the disability, and the periodic payments may not be resumed.
Another serious problem with this method is the impossibility, in many cases, of making the relevant decisions fairly and accurately without an evidentiary inquiry. Yet such an inquiry is generally considered not to be feasible with the volume of decisions that have to be made when periodic payments are subject to change from time to time.
Variations and hybrids
Many variations of these methods are found, and some jurisdictions use a combination of them. Some use a hybrid method that draws features from among the three methods described above. One such hybrid is to award a pension by the projected loss of earnings method, but make it subject to review on two occasions, perhaps two years after the initial assessment and again at five years. This has the advantage of permitting the correction of any projection that turns out to be erroneous, but it has serious disadvantages. It prolongs insecurity, and if a claimant has any propensity to compensation neurosis or any other form of anxiety, this could become more entrenched. This method also prolongs any disincentive to succeed in vocational rehabilitation. It is also open to some of the other objections to the actual loss of earnings method, such as impairment of the basic right to move.
Dependants
Since compensation benefits in non-fatal cases are usually earnings related, it is not usual to have variations for dependants, but supplementary benefits for dependants are provided in some jurisdictions.
In jurisdictions in which the benefits are taxable income, the existence of dependants may influence the net amount received in the same way it would influence the net amount of wages received. In jurisdictions in which the benefits are not taxable income, but where the compensation rate is a percentage of estimated “net” earnings, dependants are sometimes counted in estimating the level of income tax that would have been paid on wages, and in this way the existence of dependants can influence the compensation rate.
Disfigurement
Many jurisdictions provide compensation for disfigurement, particularly facial disfigurement. In some jurisdictions, this is a lump sum, and it is separate from compensation for loss of earnings. In others, disfigurement is a factor to be considered in calculating the lump sum or pension for permanent partial disability.
Pain and suffering
Unlike employers’ liability, workers’ compensation systems do not usually provide compensation specifically for pain, suffering, loss of expectation of life, loss of enjoyment of life or loss of social functioning. However, such losses are compensated to some extent. Where the physical impairment method is used to calculate a pension for permanent disability, the pension is normally payable regardless of any loss of earnings. It might be seen, therefore, as compensation for non-monetary as well as monetary losses. In jurisdictions in which compensation for permanent disability is supposed to be paid by reference to actual loss of earnings, there is sometimes a separate benefit for the disability itself; that is, for the non-monetary losses. This benefit is usually a lump sum, but in some jurisdictions, it may be a pension in very severe cases.
Indirect economic losses
Compensation is not generally payable for economic losses that are indirect consequences of the disability or the accident. For example, if a worker had paid in advance for a vacation and then sustained a compensable injury that prevented the vacation from being taken, the loss of payment for the vacation would not be compensable.
Expenses and allowances
It is normal for the system to meet the expenses resulting from a compensable disability, or at least some of them. For example, claimants are commonly reimbursed for the cost of attending medical examinations or the processes for deciding claims. Irregular expenses are usually reimbursed by reference to actual cost, and ongoing expenses are sometimes met in the same way. Otherwise, an expense allowance may be paid for ongoing expenses. An allowance for attendant care is probably the most common and significant. Other examples that are broad in their application are an allowance for the extra wear on clothing that is caused by the use of a prosthesis, a pension supplement to those who are not ambulatory and “inconvenience allowances” for a broad range of disabilities. A more specific example of local application is a smokeless fuel allowance.
Off-sets
Where benefits are payable to a claimant under two or more sections of a workers’ compensation statute, whether on the same claim or different claims, the general rule is that the entitlement is cumulative. There are no off-sets unless the legislation so provides. Sometimes, however, the cumulative benefits may be subject to an overall maximum. There is also sometimes an implied exception when alternative benefits are payable in respect of the same loss. A common example is where a claimant has been awarded a pension for a permanent partial disability, and subsequently suffers a recurrence, causing a temporary total disability from the same injury. If a new wage rate is not being used for the temporary benefits, it would be normal to suspend the pension while the wage loss benefits are being paid for temporary total disability, or to continue the pension and reduce the temporary wage loss benefits by the amount of the pension.
The same person may be eligible for benefits for a compensable disability and for benefits as a surviving dependent spouse of a deceased worker. Each is a separate claim. There is usually no provision for any off-set, and commonly no maximum applicable to the aggregate.
With regard to benefits from other systems, usually other systems of insurance, workers’ compensation is usually in the position of first-payer, so there is no off-set or reduction of benefits because of money received from another system. Sometimes the other system may deny or reduce benefits when the claimant is receiving workers’ compensation. In some jurisdictions, however, workers’ compensation benefits are reduced by any amounts received by a claimant from certain other systems, usually social security or social insurance systems, or payments arranged by the employer.
Property damage
The general rule is that no compensation is payable for damage to a worker’s property, but there are exceptions. Many jurisdictions compensate for damage to dentures, eyeglasses, a hearing aid or a prosthesis. A few jurisdictions also compensate for damage to a worker’s clothing. Where compensation is payable for property damage, the eligibility criteria are generally the same as for an injury, though some jurisdictions require an “accident” for a property damage claim when that is not a requirement for an injury claim.
The provisions mentioned above relate to property damage that occurs in the course of employment. There are also some provisions relating to property damage that subsequently results from a compensable disability. The most common example is the clothing allowance (see Expenses and allowances, above) that is paid to compensate for the extra wear on clothing that is caused by using a prosthesis.
Recurrences
Where a claimant who has been receiving benefits for a temporary disability returns to regular employment, the temporary benefits are usually terminated, though a pension and other benefits may continue in any respect of any residual disability. In the event of a recurrence of temporary total disability, the claimant may be entitled to a resumption of temporary benefits, but by this time the claimant may have established a new level of earnings. Some jurisdictions provide that this new level of earnings must or may be used for estimating the compensation benefits following the recurrence if this would be more favourable to the claimant. These provisions are particularly important in jurisdictions in which the wage rate on the claim is not indexed for inflation. Commonly, these provisions only apply after a specified number of years from the initial disability.
Non-compensable death of a disability claimant
This sub-heading refers to cases in which a person who is receiving or eligible for a pension for a permanent disability dies, and the death is not compensable because it did not result from the disability, or otherwise from employment. The general rule is that benefits terminate upon the death (or at the end of the month in which the death occurs). The following exceptions are sometimes found.
- Where the deceased claimant was receiving benefits for a total or very severe disability, some jurisdictions provide for the same death benefits to be payable as if the disability had been the cause of death. (These benefits are mentioned under the next sub-heading.)
- Some jurisdictions provide for the disability pension to continue in favour of a surviving dependent spouse for a short period, such as three months, or for a lump sum to be paid to the surviving spouse equivalent to the pension benefits for such a period.
- Where a pension is being awarded for a permanent disability, some jurisdictions provide that, in certain conditions, the entitlement may be converted into a pension for the joint lives of the claimant and spouse, and if that is done, the level of pension will be lower.
- A few jurisdictions provide for a survivor’s benefit, in the form of a pension or lump sum, to be paid regardless of the cause of death.
Fatal cases
This sub-heading relates to cases in which the death itself is compensable. It may have been an instantaneous death that was caused by the employment, or death may have resulted later from a compensable disability. In most jurisdictions, the death need not have occurred within any particular time from the date of disability. However, the length of time between the disability and the death may sometimes be part of the evidence on whether the death resulted from the disability.
It is normal to provide a funeral benefit. In some jurisdictions, a standard amount is payable regardless of the actual cost. In others, the actual cost is reimbursed, subject to a maximum. Commonly the legislation does not specify to whom this benefit should be paid, so that it can be claimed by anyone who has paid for the funeral.
The most substantial benefits in fatal cases are the payments to surviving dependants. These may be by lump sums, periodic payments, or both. Some jurisdictions provide for standard amounts to be paid per dependant; for example, so much per month for a surviving dependent spouse and so much per month for each child. In other jurisdictions, the amounts vary by reference to the previous earnings of the deceased worker. This is usually done by establishing pensions for dependants at a percentage of what would have been paid to the deceased worker for a total disability. Some jurisdictions use a blended formula that refers to standard amounts and a variation by reference to the previous earnings of the deceased worker.
Where the benefits are a standard amount for each dependant, there is usually no maximum, so that the total might exceed what would have been payable to the deceased worker for a total disability. Where the benefits are earnings related, a maximum is sometimes established at the amount that would have been paid to the deceased for a total disability, or a percentage of that amount, and sometimes there is a lower maximum when there is no surviving spouse. In jurisdictions that use a blended formula, there may or may not be an applicable maximum.
Historically, death benefits have been payable to a surviving widow or disabled widower, and that is still the position in many jurisdictions. In others, recent moves to sex equality have eliminated the distinction, usually by reducing the benefits payable to surviving widows, and sometimes by abolishing pensions. Also, pensions for surviving widows used to be subject to termination upon a remarriage, often with a lump sum then being payable. In some jurisdictions, those provisions have been repealed. Even where they still apply, the children’s allowances continue. Also in some jurisdictions in which a widow’s pension is terminated upon a remarriage, that only applies if there are no children. When a widow’s pension has been terminated because of a remarriage, it is subject to revival in the event of divorce in some jurisdictions, but not in others. In some jurisdictions, the pension of a surviving spouse is also subject to termination if that spouse abandons the children.
Sometimes benefits are payable simply by reference to a family relationship. Otherwise it may be necessary to show a family relationship plus dependency. It is usually sufficient evidence of dependency that the claimant lived in a common household with the deceased worker, or that the claimant was receiving support payments from the deceased worker. It is not usually a disqualification from benefits that the claimant was earning, though if there was no common household and no significant support payments, that might be evidence that the claimant was not a dependant of the deceased worker.
Some jurisdictions recognize partial dependency, usually for cases in which the claimant and the deceased worker were not living in a common household. It may be decided that the claimant was partially dependent upon the deceased worker and benefits may be awarded based on a proportion of what would have been awarded if the claimant had been considered totally dependent. Other jurisdictions do not recognize partial dependency, so that a simple decision must be made that the claimant was or was not a dependant of the deceased worker.
Benefits for dependants are payable directly to those dependants (or to the person having care of a dependent child), not to the estate of the deceased worker. In some jurisdictions, dependants’ (survivors’) benefits are confined to a spouse (or widow) and children. In others, the range of eligible dependants can include siblings, parents, grandparents, grandchildren and other family members. In these jurisdictions, it is usual for a spouse (or widow) and children of the deceased, if any, to have priority. Subject to that, benefits may be payable to other family members who were, or who would in the future have probably been, dependent on the deceased.
Pensions to a surviving spouse are commonly payable for life. In some jurisdictions, they are payable for a fixed term of years, or until a standard retirement age. Periodic payments for a child usually terminate when the child reaches a specified age. There are commonly provisions extending the payments for a few years beyond that age when a child is undertaking full-time education, or for life if the child is disabled.
Where there are surviving children and no surviving spouse, an allowance is commonly payable to a foster parent. The amount is often equivalent to the amount that would have been paid to a surviving dependent spouse, but the duration is different. A foster parent’s allowance usually terminates when the last child reaches a certain age, or sooner if the foster care terminates.
A legal marriage is not usually required to qualify for spousal benefits. A couple who were cohabiting at the time of death and for a specified period prior to the death are considered spouses. The period is commonly less, or there is no minimum period, if there is a child of the union.
A legally married spouse who was separated from the worker at the time of death may be disqualified from benefits in some jurisdictions, or entitled only to reduced amounts. Where the deceased worker was supporting a separated legal spouse and there was a cohabiting spouse, some jurisdictions provide for the spousal benefits to be divisible between them, but the total payable is not increased. In deciding on the apportionment, it used to be normal for a legally married spouse to have priority, but the contemporary trend in some jurisdictions is for the cohabiting spouse to have priority.
In most jurisdictions, it is not a disqualification that a marriage took place or cohabitation began after the disability that caused the death.
Inflation adjustments
In some jurisdictions, monetary benefits are not adjusted automatically for inflation, so that their values deteriorate over time, subject to such episodic adjustments as may be legislated. In other jurisdictions, benefits have a stable value by being indexed for inflation. This may take two forms. First, indexing of the payments that apply to new claims, including indexing of the ceiling. Second, indexing of the ongoing periodic payments that are being made in respect of earlier claims. The indexing factor may be applied directly to the benefits, or it may be applied to the wage rate on the claim, with consequential adjustments being made to the benefits.
Taxation of benefits
In some jurisdictions, the benefits, or some of them, are subject to income tax, and the tax is then commonly deducted at source. In other jurisdictions, the benefits are not taxable income. Where this is so, the ceiling on the wage rate, or on the level of benefits, is usually designed to ensure that a worker will not be better off on compensation than when earning. As an alternative to a ceiling, this result could be achieved by establishing the compensation rate as a percentage of the wage rate according to a scale of percentages that descends at higher levels of income.
Protection of benefits
To ensure that the benefits are available for the maintenance of the disabled worker and dependants, some jurisdictions prohibit any assignment of the benefits to creditors or others, and the benefits cannot be attached to satisfy any judgement. In recognition of this statutory principle, some compensation authorities also decline to accept any direction from a claimant to send compensation benefits to the address of a lawyer.
There are several common exceptions. Where an employer has continued to pay wages or has paid other benefits to a worker who has a compensable disability, some jurisdictions provide for the compensation authority to reimburse the employer for the lesser of the compensation benefits to which the worker was entitled and the amounts paid to the worker by the employer. Where a claimant has been receiving benefits from social security (welfare) pending the outcome of the workers’ compensation claim, some jurisdictions provide for the social security department (welfare office) to be reimbursed by the workers’ compensation insurer. Where a claimant with a compensable disability is failing to support dependants, some jurisdictions provide for a portion of the compensation benefits to be paid directly to those dependants.
Suspension of benefits
There are various provisions for the suspension of periodic payments. Common examples are the absence of a disability claimant from the jurisdiction during a period in which medical care is required, the unreasonable refusal of medical care, the cohabitation of a surviving dependent spouse with another person, and imprisonment of the recipient of the benefit. The significance of the suspension is not always clear in the legislation. Where words are used to indicate suspension, without any words being used to indicate disqualification, it may mean simply that the payments are postponed, with the entitlement remaining intact, so that the arrears are payable at the end of the suspension period. Sometimes words of disqualification are used, or it is otherwise apparent from the context that no benefits are payable at any time in respect of the suspension period.
Overpayments
The term “overpayments” refers to payments to which the recipient was not entitled, or payments in an amount that exceeds the entitlement. An overpayment might result from a mistake by the insurer, the recipient or a third party, or it may be the result of fraud by the recipient or a third party. The obligation of the recipient to repay the overpayment may sometimes depend upon the circumstances; in particular, on the recipient’s culpability. The recipient may:
- have induced the overpayment by fraud, negligence, or failure to comply with obligations to report information
- have been innocent of the cause of the overpayment, but aware that it was received, and may have deliberately or negligibly failed to inform the insurer
- have been innocent of any contribution to the cause of the overpayment and unaware of any overpayment.
Some workers’ compensation statutes provide that the insurer may recover overpayments, though not necessarily in all circumstances. Where the legislation is silent on the question, overpayments may be recovered under general legal principles, though not in all circumstances. For example, in some jurisdictions, an overpayment is not recoverable if it resulted from a mistake of law by the insurer and the recipient had not induced the mistake.
Where an overpayment is legally recoverable, the methods of recovery are generally the methods available in the particular jurisdiction to any other creditor. For example, the available method might be a court proceeding for debt, with the judgement being enforced by a seizure of the goods of the recipient. There may be no right, or only a limited right, to recover an overpayment by deductions from future benefits. Bearing in mind that compensation payments are commonly spent by the recipient as they are received, and that future benefits are intended to provide for future needs, there is sometimes an obligation under compensation legislation to make all future payments as they fall due without any set-off for past overpayments. Where that is so, any overpayment is only recoverable by other methods of enforcement.
The actual practice varies. If it is discovered that an overpayment was obtained by fraud, it is normal to seek recovery by all available legal methods of enforcement, and there may also be a criminal prosecution. Where an overpayment occurred by mistake, it may be written off, particularly if it was received in innocence. Otherwise the overpayment may be enforced by ordinary legal processes, and in jurisdictions where it is legitimate to recover overpayments by deductions from future benefits, this may be done in instalments. However, compensation authorities sometimes strive to avoid deductions from future benefits, even where such deductions are legally permissible.
Where an overpayment has been made to a physician or other service provider, the legal position is generally the same as for an overpayment to a disabled worker, except that a right of set-off is more widespread, so that recovery can be made by deductions from future bills, and that is a common practice.
Where an overpayment has been made to a disabled worker who has subsequently died, recovery may be sought from the estate of the deceased worker, but deductions are not generally permitted from any benefits that are payable to dependants.
Commutations (redemptions)
Some jurisdictions permit the commutation (redemption) of all or a part of a pension into a lump sum. This may take the form of:
- a total commutation of the whole pension
- a commutation of full pension benefits for a term of years, so that the pension resumes after that period
- a partial commutation that reduces the level of pension benefits for the duration of the pension
- a partial commutation for term of years, so that pension benefits are reduced during that period, after which the pension resumes in full.
Among the jurisdictions that permit commutations, many do not permit all types, and the first is the most common.
Commutation provisions are vulnerable to abuse by system administrators, particularly by using a formula to calculate a lump sum that is much less than the real capital value of the pension. The availability of a commutation may also make a claimant vulnerable to predatory practices by service providers. It may also mean that taxpayers lose the protection that the system was intended to create by preventing a claimant from spending a lump sum and subsequently becoming a burden on public funds.
To avoid these problems, some jurisdictions prohibit commutations (or have no provision to allow them). Others provide that a commutation is only available at the discretion of the compensation authority, and this discretionary power may be defined (by the statute or by the compensation authority) to permit commutations only for certain purposes. Notwithstanding that a commutation is discretionary, some jurisdictions allow the denial of a commutation to be the subject of an appeal, and where that is so, the administrative and adjudicative cost of such discretionary powers can be unduly high in relation to the amounts involved.
In jurisdictions where the system is administered by insurance companies, the insurer (or the employer) or the worker, or both, may have a right, after some initial period, such as 12 months, to require the redemption of all future periodic payments by a lump sum. Failing an agreement, the amount may be determined by the court. Such provisions are open to the objections that, in practice, the worker receives substantially less than the full capital value of the future periodic payments, and that the future income needs of the claimant become a burden on public funds.
Rehabilitation and Care
Clinical facilities for rehabilitation, and the services of physicians and various types of therapists, are generally provided under the heading of medical aid. The rehabilitation provisions of workers’ compensation statutes usually relate to other types of rehabilitation assistance. Some items, such as prostheses, are provided under the heading of rehabilitation in some jurisdictions and under the heading of medical aid (or health care) in others.
Rehabilitation assistance is part of the coverage under many workers’ compensation systems, and so is chronic care. Alternatively, workers’ compensation claimants may be eligible for such assistance under a general social security system that covers all disabled people. In some jurisdictions, the social security system may exclude workers’ compensation cases, but in others, it does not, so that there is a measure of overlap, and assistance may be provided by either.
The goals to be sought in the provision of rehabilitation assistance are commonly not prescribed. Goal definitions produced at international conferences are found in the literature of workers’ compensation, but they are seldom treated as the guides for daily practice. In particular, there is an ambiguity in many jurisdictions about whether the goal of a vocational rehabilitation programme should be to maximize or improve employment opportunities for claimants, or whether the goal should be to coerce them back to work.
To some extent, however, the goals of vocational rehabilitation are implicit in the way benefits are provided for permanent disability. A pension by the physical impairment method is most consistent with the notion that rehabilitation is voluntary, and that therefore the overall goal of any programme of rehabilitation assistance should be to expand the opportunities of claimants, so that the goals in any particular case are the goals of the claimant. Use of the actual loss of earnings method implies that rehabilitation is compulsory, that it is indistinguishable from benefit control, that the goal of the programme in each case is to restore the claimant to employment, or alternatively, to provide the evidence that will justify a termination of benefits.
Where rehabilitation assistance is provided under a workers’ compensation system, the services are commonly discretionary, particularly where a broad range of services is offered. There has been a trend in recent years to legislate an ostensible “right” to rehabilitation, but it is hard to define an enforceable “right” in this context. The attempt to do so has commonly been accompanied by the reduction of monetary benefits and new limits on the rehabilitation assistance that may be provided.
For vocational rehabilitation, the assistance offered may include counselling, training for job interviews, a placement service, support during a period of job search, retraining, further education and sometimes relocation expenses. As well as vocational rehabilitation, some jurisdictions offer social rehabilitation assistance, such as equipment for hobbies or sports, courses on makeup, assistance with social adjustment or assistance in the resolution of marital problems. Social rehabilitation may be provided as a goal in itself, or in aid of vocational rehabilitation. Chronic care may consist of electronic, pneumatic or mechanical aids, or home help. Such assistance is usually provided under the heading of “rehabilitation”, though in many cases it is really chronic care.
In some jurisdictions, rehabilitation services reached a peak during the 1970s and have declined in recent years. In particular, the provision of placement services has declined, and delays have developed in the provision of other services. Where placement services are still provided, there has been some erosion of the traditional principle that disabled workers should be placed in productive employment. For example, they are now sometimes coerced or required to work in telemarketing (making unsolicited advertising calls to people’s homes) notwithstanding objections that this is a form of public nuisance and electronic trespass. One aspect of the deterioration is that the provision of rehabilitation assistance is now commonly perceived as a role for unqualified office workers rather than professionally qualified and trained field workers.
Rehabilitation is commonly perceived as something that follows the occurrence of a disability, but some jurisdictions recognize the value of preventive rehabilitation; that is, rehabilitation assistance for the prevention of a disability, even in cases in which none has yet occurred. For example, bad backs and certain diseases from industrial contamination are often predictable, and assisting a worker to obtain another job may sometimes be appropriate as a preventive measure. Rehabilitation assistance for this purpose is not usually provided, but it is done in some jurisdictions in some circumstances. Rehabilitation assistance may then be one of the remedies available in a health and safety programme. A few jurisdictions also have rehabilitation measures for the protection of a foetus, or a newborn baby who is being breast-fed by the worker, where exposure of the worker to contamination, or to some other condition of the employment, would otherwise endanger the health of the foetus or baby.
The decision-making process for rehabilitation matters is the same as for compensation matters in some jurisdictions. In others, it is different, with a greater emphasis on discussion and consensus, and a reduced role for adjudication and appeals.
In some jurisdictions, the costs of rehabilitation assistance are charged in the same way as monetary benefits. In others, the costs of rehabilitation assistance are charged to the general fund and spread over the classes, even though experience rating may be in effect for the cost of monetary benefits. Since the cases in which vocational rehabilitation assistance is needed are usually those in which the accident employer is not offering continuing employment, this method of charging the cost enables the rehabilitation decisions to be made without the accident employer being involved as a party. In that way, this method avoids the therapeutic damage of adversarial processes. Where the costs of rehabilitation assistance are charged to the general fund, the costs of compensation for injuries sustained during rehabilitation may be charged in the same way.
Obligations to Continue the Employment
In recent years, some jurisdictions have purported to create an obligation upon an employer in whose service a worker became disabled by a compensable injury or disease (the accident employer) to continue the employment of that worker. Typically, the obligation commences when the worker has made a sufficient recovery to return to some type of work that the employer can make available, and continues for a period of one or two years. The enactment of such provisions is usually accompanied or followed by a reduction in compensation benefits for permanent disabilities.
In jurisdictions with a largely unregulated market economy, and where most employment is not covered by collective bargaining, such provisions are counter-productive. They detract from and tend to undermine the provision of any genuine rehabilitation service. A worker with a permanent disability is not usually assisted by a temporary “right” to employment. Moreover, these provisions change the image of a disabled worker from that of a person whose continuing employment with the same employer could be expected in the ordinary course of things to that of a burden that the employer should bear. This change of image is not confined to the cases that would have been a rehabilitation problem in any event, and for this reason alone, these provisions can create rehabilitation problems.
Given that the ostensible “right” is only relevant in cases in which the employer would like to terminate the employment relationship, the “right” is inevitably fragile. In most jurisdictions, an employment relationship can be terminated on a variety of grounds, and these grounds for termination are not usually extinguished by the worker’s “right” to continuing employment. Even if employment is unlawfully terminated, the remedies may be difficult to enforce. The “right” is, therefore, a fragile one, and notwithstanding its fragility, its exercise, or the refusal of the worker to exercise it, are both grounds for the termination of compensation benefits.
Disputes about what is suitable employment, having regard to the residual disability, are commonplace, and they can be hard to resolve without an evidentiary inquiry. Even when such an inquiry is conducted and a well-reasoned decision is made, it may still have limited significance, particularly if the circumstances are changing or the period of the obligation is expiring. When a dispute about the obligation is resolved in favour of the worker, this may still not produce a continuation of the employment. It generally produces a cash settlement instead. Thus even when the outcome is “successful” for the worker, the result is the delivery of a monetary benefit through a process that is highly inefficient, and a cause of therapeutic damage.
The enactment of such a “right” also detracts from the provision of a genuine rehabilitation service. Since the worker has an ostensible “right” to return to the same employer, that tends to be perceived as what ought to happen, so that assistance for alternative forms of rehabilitation are less likely to be considered. For all of these reasons, legislation which was intended to create an obligation on the employer and a choice for the worker turns out, in practice, to create an obligation on the worker and a choice for the employer.
Some jurisdictions require the continuing employment of a worker who has sustained a disability, regardless of the cause. Such provisions are probably workable only in the context of collective bargaining or a highly regulated labour market.
A few other jurisdictions prohibit the dismissal of a worker who is off work by reason of a compensable disability, but do not prohibit the dismissal of such a worker upon recovery from the disability.
Finance
Cost distribution
The cost of workers’ compensation is generally raised by premiums or assessments that are paid by employers. Because of this, it is commonly asserted or assumed that employers bear the cost of the system, but that is manifestly incorrect. The burden of any tax may move from the party with the initial obligation to pay, and there is a wealth of economic literature explaining that a payroll tax is commonly an opportunity cost of labour. Part of the cost of workers’ compensation assessments (premiums) may rest with employers, but part of it is passed onto labour in the form of lower wage rates or other benefits, and part of it may be passed onto consumers. Also workers’ compensation benefits do not provide a complete indemnity for the economic losses of disabled workers. To the extent that these losses exceed any compensation received, these are costs of occupational disabilities that are not shown as costs of the workers’ compensation system. These costs are borne for the most part by disabled workers, though to some extent they may be passed on to others, such as family members or creditors.
Balancing of accounts
The first step in the financial design of a system is a criterion for balancing accounts, so that aggregate revenues and aggregate expenditures will be approximately equal over time. In systems operated by insurance companies, this is supposed to be done by adjusting premiums, so that the revenue will reflect the claims cost experience. In social insurance systems, the legislation usually requires accounts to be balanced in the same way, but there are often political pressures to reduce the level of assessments, and then bring the expenditures into line with the assessment decisions. Unless a government maintains the integrity to block these pressures, ongoing conflict between the legislation and the political pressures causes ongoing friction in the administration of the system, and in adjudication. It can also cause unfunded liabilities to accrue.
Revenue and classification
Most workers’ compensation systems use industrial classifications and establish a rate of premium or assessment for each class or sub-class of industrial activity. The classification may be by reference to the end product, or by reference to the job functions of employees. Classification by end product is easier from the standpoint of administration and adjudication. Classification by reference to the job functions of employees can increase the complexities of auditing, particularly where some employees perform multiple functions.
Once a rate of assessment has been established for an employer, that rate is usually applied as a percentage of the payroll. In jurisdictions in which there is a ceiling on the wage rate for a claim, the same ceiling is commonly applied as a maximum on the amount of pay per worker to which the percentage rate is applied for assessment purposes. For example, an employer might be required to pay 2 currency units per 100 units of payroll to a maximum of 50,000 units of payroll in respect of any one worker per year. Usually the rates are revised annually. While assessment as a percentage of payroll is normal, alternative methods are sometimes found, such as assessment on the estimated value of assets, or on the price of goods sold. Some systems also have a partial subsidy from government.
Experience rating
In many systems, the premium or assessment payable by an employer will vary from the standard rate for the class or sub-class to which the employer belongs by reference to the claims experience of that employer, compared with others. This is called “experience rating”. It is sometimes called “merit rating”, but that is a misnomer, because the rate variations have no known connection with any type of merit. Usually the formula for calculating the variations uses predominantly claims cost experience, but it may include a variation by reference to other factors such as the frequency of claims. Sometimes there is also a minimum deemed cost for fatal cases. Small employers are commonly excluded from experience-rating plans, or where they are included, the rate variations applied to small employers may be more limited.
Experience rating is standard in systems administered by insurance companies. It is sometimes used also in social insurance systems of workers’ compensation, and its use in these systems has been expanding in recent years, but to a large extent, it is incompatible with the rationale for their creation. A major advantage of a social insurance system is that in the adjudication of claims, it can avoid adversarial processes. The use of experience rating deprives the system of that advantage.
In systems administered by insurance companies, experience rating usually applies to all expenditures made on a claim. Sometimes that is also the case in social insurance systems, but in some such systems, experience rating is confined to the monetary benefits. It does not apply to medical aid or rehabilitation expenditures. This is to minimize the use of adversarial processes for decisions on those expenditures.
The rationale most commonly heard for experience rating is that it will create an incentive for an employer to reduce the frequency and gravity of occupational disabilities, but there is no credible evidence that it has that effect. The only “studies” that purport to show experience rating having any beneficial effect on health and safety use claims data as the measure of the effect. For several reasons, claims data cannot properly be used in that way. Experience rating creates an economic incentive for employers to prevent or discourage the filing of claims, to withhold positive information, to oppose claims, to appeal decisions that are favourable to claimants, to press claimants to return to work prematurely, to seek personal medical information relating to claimants and to require further medical examinations of claimants. Although some of these practices are commonly legitimate, their extensive use makes it impossible to use claims data as a measure of the “success” of experience rating in relation to health and safety. These practices also increase the administrative and adjudicative costs of the system; and because of the delays and therapeutic damage that they create, they probably increase also the compensation costs.
Experience rating can create an incentive for an employer to facilitate the rehabilitation of a disabled worker in some circumstances, but on the whole, experience rating is probably negative in its influence on rehabilitation. It commonly results in all soft tissue injuries being treated with suspicion. Such attitudes can be a cause of anxiety and an impediment to rehabilitation. Experience rating can also discourage an employer from hiring disabled people and from continuing the employment of workers who become disabled. This is primarily because the compensation cost of any subsequent disability can be greater when its impact is compounded by the previous disability. To counteract this negative influence of experience rating, some jurisdictions use a “Second Injury Fund”. Part of the compensation cost of the subsequent disability can be charged to that fund, rather than to the employer’s experience account. The costs of this fund are spread over all assessment classes and all employers. Rules for the use of the Fund vary, but the general principle is that where some pre-existing disability or condition has contributed to the cause of a compensable disability, has enhanced its gravity or otherwise increased its compensation consequences, a portion of the compensation cost of the disability should be charged to the Second Injury Fund.
These funds do not achieve their objective. This is partly because of other reasons (real or perceived) why many employers avoid the employment of disabled people, and partly because the transfer of costs to a Second Injury Fund depends upon a judgement being made in claims adjudication after the subsequent disability has occurred. Also the cost of processing applications for a transfer of costs to a Second Injury Fund is another reason why experience rating increases the overall costs of the system.
Experience rating would seem, at first impression, to improve equity in cost distribution among employers. To some extent it does, but it also creates new inequities. For example, applications for the transfer of costs to a Second Injury Fund, or to other general funds, are more commonly made by large employers who have staff or outside consultants engaged for that purpose. The result of these transfers is to elevate the standard rate for the class or sub-class, with the end result being a subsidy from smaller to larger employers.
Funding
In terms of a time dimension, the financing of workers’ compensation is arranged in one of two basic ways.
- Funding. The total revenues required in any year are determined by estimating the total present and future costs of all compensable disabilities that occur during that year (or of all claims received during the year).
- Current Cost Financing (sometimes called pay-as-you-go). The total revenues required in any year are determined by estimating the total costs that will be paid during that year in respect of all current and past claims.
Variations on one of these positions are found, and so is some middle ground between them. Funding requires substantial reserves to be established, and their adequacy is commonly re-estimated each year. With current cost financing, some reserve is required as a cushion, but it does not require repeated actuarial calculations.
Where a system is administered by insurance companies, the general principles of insurance law require that it must be funded. A social insurance system is in a different position because a government can, by law, compel future contributions. In practice, some social insurance systems have a statutory requirement of full funding, and some use current cost financing. Others adopt a different position, such as partial funding, or funding for some items of future cost and not for others.
Current cost financing is marginally cheaper in the long run, but funding is essential in many jurisdictions, such as smaller ones, and those that are heavily dependent upon primary producing industries.
Non-payment of assessments or premiums
In systems administered by insurance companies, an insurer may be allowed to terminate the insurance coverage if the premium is not paid. The employer is then responsible for the compensation payments on future claims, and future claimants are dependent on the continuing solvency of the employer. Where there is a legal requirement to carry workers’ compensation insurance, and an employer has failed to pay a premium, there is commonly a provision for criminal sanctions, usually a fine or imprisonment, and this is in addition to the employer’s liability for claims. The continuation of the business may also be stopped in some jurisdictions.
Where a workers’ compensation system is one of social insurance, some jurisdictions require or permit the coverage to be terminated when assessments have not been paid by an employer. More commonly, the payment of compensation is not dependent upon the assessments having been paid, and termination of the coverage is not permitted as a response to any non-payment. Each claim is a charge on the relevant class fund, and in some jurisdictions, it is a charge on the whole fund.
In the event of non-payment of an assessment, various enforcement mechanisms are used. Commonly they are similar to the enforcement mechanisms that are available in the jurisdiction in relation to other forms of taxation. These methods may include seizure of the employer’s property (including land and goods), attachment of the employer’s bank account, and orders for the cessation of business. In some jurisdictions, non-payment of the assessments is also a criminal offence. Penalties may be payable in addition to the overdue assessments, and the employer may also be required to reimburse the administering agency for the costs of claims arising during the period of non-payment. Where an employer is incorporated, there may also be some personal liabilities on the directors of the company.
Vicarious Liability
This term refers to situations in which one person may be liable for the obligations of another. Where the employees of one person (the “contractor”) are used to doing work for another person (the “principal”) some jurisdictions provide that in some circumstances, the principal is, in effect, a guarantor of the obligations of the contractor in relation to workers’ compensation. Such provisions commonly apply to work being done on construction sites, though they also sometimes apply to other situations.
Health and Safety
In systems operated by insurance companies, the practice varies among jurisdictions and among companies with regard to what role, if any, the insurer will play in relation to occupational health and safety. Sometimes the insurer plays little or no role. Sometimes the insurer undertakes a survey of risk, but limited to a standard range of items. Sometimes the insurer may undertake a more professional and sophisticated survey of risk. This is more common in particular industries where the insurer may be undertaking other types of coverage as well as workers’ compensation. Where surveys are undertaken, they may be repeated later, or they may be used only for initial premium setting, with the insurer using claims cost experience for subsequent premium adjustments.
Where workers’ compensation is a system of social insurance, the most common position is that the workers’ compensation system supports the government agency that has the regulatory jurisdiction in relation to occupational health and safety. This support commonly consists of statistical information, and the distribution of health and safety messages to employers, unions and workers. The workers’ compensation system may also provide some other health and safety services directly to employers, such as technical advice, or it may finance the provision of services by industry associations (though the value of this is controversial).
In some jurisdictions, the workers’ compensation agency also has the regulatory jurisdiction of the government in relation to occupational health and safety. In these jurisdictions, the workers’ compensation system can be, and sometimes is, used extensively in aid of occupational health and safety. This use may include the provision of health and safety information from claims records to programme inspections and for other purposes, the sharing of some technical and professional resources, and some sharing of support services. By far the most valuable connection is the use of compensation assessment adjustments as a sanction for the enforcement of occupational health and safety regulations and orders. The assessment payable by an employer may be increased by reference to hazardous conditions observed upon an inspection (not by reference to any paper records). This is the only suitable and available sanction for the enforcement of health and safety requirements that can be used in the broad range of situations for which criminal sanctions are inappropriate or inadequate (including, continuing high levels of toxic contamination).
The compensation system can also be used in other ways to provide a sanction for the enforcement of occupational health and safety regulations. For example, where a disability resulted from a serious neglect of regulations or orders by the employer, or other serious negligence, the employer may be ordered to pay the whole or part of the cost of the claim. Thus while fault on the part of an employer is irrelevant as a general rule in workers’ compensation, it can be invoked in a few jurisdictions by way of exception in extreme cases as a sanction for the violation of health and safety requirements. Assessment variations by the use of health and safety audits has no potential on a broad scale, but it can be done in limited circumstances.
Claims against Third Parties
This heading refers to any civil claims that a disabled worker may have against anyone who is alleged to have caused the disability, other than the employer. In some jurisdictions, some of these claims are barred by the workers’ compensation legislation. Where they are not so barred, some jurisdictions provide that the worker may pursue the claim, but the defendant is entitled to have the damages reduced by the amount that the claimant has received, or will receive, in workers’ compensation benefits.
Other jurisdictions provide that the insurer (the compensation authority, the insurance company, or the employer, as the case may be) may take over the right to pursue the claim against the third party. This is called “subrogation”. In some jurisdictions, this right of subrogation is total. The insurer takes over the whole claim; but if any amount is recovered above the compensation that has been or will be paid, the insurer must account to the worker for the excess. In other jurisdictions, the subrogation is partial. For example, the legislation might provide that the insurer can pursue the claim to the extent of the compensation paid and payable, while the worker can pursue the claim for the excess. Or it might provide that the insurer can pursue the claim for monetary losses while the worker can pursue the claim for non-monetary losses.
PART TWO: OTHER SYSTEMS
Social Insurance and Social Security
The term “social insurance” usually refers to a system of insurance administered by government with the coverage being compulsory, and with contributions being required from employers, employees or both, though there may also be a contribution from general revenue. Such a system usually covers employees, though the self-employed may be included, at least to some extent. A system may be specific; for example, a workers’ compensation system may be one of social insurance; or it may be broad, with benefits payable in the event of unemployment, sickness, disability, pregnancy, retirement and death. It is the broad social insurance systems that are discussed under this heading. The benefits may be flat-rate or earnings related. There may be exclusions from the coverage for particular industries or particular categories of employees, but the exclusions are commonly less extensive than the exclusions under a system of workers’ compensation.
The term “social security” is used with several meanings. In its narrowest meaning, it commonly refers to a system of benefits paid by government out of general revenue to people who qualify by reason of disability, old age, unemployment or some other qualifying cause. Commonly there is a means test. The system usually covers all people who are usual residents of the jurisdiction. The benefits are usually flat-rate, though there may be a variation by reference to dependants. The term “social security” is also commonly used in a much broader sense to include these benefits, plus social insurance, medical care and social services. In this chapter, the term “social security” is used in the narrower sense, so that it refers to money benefits that are distinct from social insurance benefits.
Many countries do not have a separate system of workers’ compensation. Disabilities and deaths that result from employment are covered under a broad social security or social insurance system that includes disabilities and deaths from other causes. Medical aid for disabilities resulting from employment is usually provided in these countries under the same government system of medical care that applies to disabilities caused in other ways. In some jurisdictions, additional types or levels of medical care are sometimes provided when a disability has resulted from employment, or certain services or treatments may be free which involve a cost for disabilities that did not result from employment.
For money benefits, disabilities and deaths that result from employment may be treated in the same way as those that result from other causes, and this is common with regard to short-term benefits, but in many jurisdictions, there is an additional benefit, or a higher rate of benefit, when a disability resulted from employment. This is common for permanent disabilities and it is sometimes found also in fatal cases. The historical explanation is often that the broad social insurance system replaced an earlier workers’ compensation system. This structure may also be a way of complying with ILO conventions. Some systems also include special benefits, or special levels of benefit, for those in particular occupations.
The coverage of broad social insurance systems is generally universal, applying to all those who live or who work in the country, though there are commonly some exceptions for foreign nationals.
Contributions for the cost of the system are commonly required from employees, and from employers in respect of their employees. The contributions may be at a standard rate (which is usual if benefits are flat-rate), or they may be earnings-related (which is usual if benefits are earnings-related). A certain personal contribution record may be a prerequisite for benefits, and the contribution record of a worker or the employer of the worker may also be relevant to the level of benefits. Where additional or higher benefits are payable for disabilities or deaths that result from employment, the costs of these provisions is commonly a charge on the employers’ contributions.
Where contributions and benefits are earnings-related, there is commonly a ceiling applicable to both. Thus the insurance coverage commonly applies only to income at lower levels, and the costs of the system are commonly borne wholly or predominantly from income at the lower levels. The benefits under a general social insurance system are commonly at lower levels than under workers’ compensation systems. However, various supplements are commonly found, such as supplements for dependants.
Administration and primary adjudication are usually in a government department. If there is any dispute, it is usually between a claimant and the department. Experience rating is not generally used in social insurance systems. Hence an employer is not usually seen as having an interest in the result of any particular claim and is not considered a party to the claim, though employers may sometimes be required to supply information. Appeals may lie within the department or to a separate tribunal. Appeals to the ordinary courts are sometimes possible, but the courts are not readily available to deal with social insurance cases in any significant volume.
Under a broad social insurance system, there is often a waiting period of three days. For temporary disabilities and during the initial phase of permanent disabilities, periodic payments are made. They are commonly called a “sickness benefit”, though they are paid also in injury cases. The cause of a disability is generally irrelevant, but the benefit is usually payable only if the disability causes an absence from work.
Pensions are normally paid for permanent total disabilities. In many jurisdictions, pensions are also paid for permanent partial disabilities, though in some jurisdictions, this benefit is limited to disabilities that have resulted from employment. Partial disabilities that are classified as minor may be compensated by a lump sum or not at all. The distinction between total and partial, and the rate of pension for partial disability, depends in some jurisdictions on the estimated impact of the disability on the earning capacity of the claimant. In others, it may be measured by the degree of physical and mental impairment. Sometimes there is a blended formula in which both factors are considered. In some jurisdictions, a partial disability is classified as total during any period of hospitalization for the treatment of that disability. Commonly there are additional benefits for special needs, such as attendant care.
Death benefits commonly include a lump sum for funeral costs, a pension for any surviving spouse, or in some jurisdictions for any surviving widow, and periodic payments for surviving children.
Many features that are commonly found in workers’ compensation systems are uncommon, or not found at all, in broad social insurance systems. These include optional coverage, commutations, industrial classifications, experience rating, funding and a role in occupational health and safety.
In some jurisdictions that have a separate workers’ compensation system, the claimants on that system are disqualified from receiving disability benefits under a general social insurance or social security plan. In other jurisdictions that have a separate workers’ compensation system, the total or partial stacking of benefits is permitted. In some of these jurisdictions, the general social insurance system is in the position of first-payer, both with regard to medical care and monetary benefits, with the workers’ compensation system topping up the benefits, sometimes to the extent of a full indemnity for all losses.
Rehabilitation assistance is commonly provided under social insurance and social security programmes. The range of assistance varies, as it does under workers’ compensation systems. There is a contemporary trend in some countries to reduce the scope of disability pensions in favour of vocational rehabilitation assistance. The problem with this development is that the curtailment of monetary benefits may be real while the substitution of rehabilitation assistance may be illusory in view of the economic and political developments that are making vocational rehabilitation more difficult. The viability of social insurance systems is also currently threatened in some countries by the weakening of the State, the weakening of organized employment, the expansion of the “informal economy”, of self-employment, and of very small businesses.
These systems are discussed more fully in works on social security and social insurance.
Accident Compensation
A few jurisdictions have a scheme of accident compensation or accident insurance administered by government. These schemes differ from workers’ compensation in that they cover all injuries by accident, regardless of the cause, plus a category of occupational diseases, or all diseases resulting from employment. These schemes are in lieu of workers’ compensation and the personal injury component of motor vehicle insurance, but they also cover injuries that occur at home, during sports, or in other ways. The benefits are typical of the benefits that are commonly found in workers’ compensation, including medical aid, monetary compensation and rehabilitation assistance. These schemes differ from broad social insurance systems in that they do not cover most disabilities and deaths from diseases that are not shown to have resulted from employment. For this reason, they do not cover the majority of disabilities and deaths.
Sick Pay
In some jurisdictions, the law of employment requires employers, or some employers, to continue the payment of salary or wages, at least to some extent, when an employee is unable to work because of sickness or injury. Also, regardless of any legal obligation, it is common for many employers to continue the payment of salary or wages for some period when an employee is unfit for work. Although this is often called “sick pay”, these provisions usually apply to absences from work that are caused by injury as well as sickness or disease. These arrangements are commonly informal, particularly among small employers. Larger employers commonly have contractual sick pay schemes, sometimes the result of collective bargaining. Some jurisdictions have a statutory scheme of sick pay.
A workers’ compensation system, where applicable, is usually in a first-payer position, so that sick pay is inapplicable to cases that are covered by workers’ compensation, or it provides a supplementary amount of income. Alternatively, the employer may continue to pay the wages and receive a total or partial reimbursement from the workers’ compensation agency. In a few jurisdictions, sick pay covers an initial period for all disabilities, with workers’ compensation providing the benefits after that period for those disabilities that qualify.
In jurisdictions that do not have a workers’ compensation system, sick pay generally applies to disabilities that result from employment as well as those that result from other causes. The sick pay may then provide the total income of the worker, or it may supplement a social insurance benefit.
Disability Insurance
As an alternative to sick pay, short-term disability insurance (sometimes called “weekly indemnity insurance”) is organized by some employers in some jurisdictions. It is similar to sick pay except that it is administered by insurance companies.
Long-term disability insurance is organized by many employers in many jurisdictions by arranging a group policy with an insurance company. In the organized sector, these policies are often the result of collective bargaining. In the unorganized sector, such a group policy is sometimes arranged at the initiative of the employer. The premiums are commonly paid by the employer, though sometimes by the employees or with a contribution from the employees.
In jurisdictions that have a workers’ compensation system, these policies generally exclude disabilities that are covered by workers’ compensation. In other jurisdictions, the coverage of these policies may include disabilities that result from employment. The benefits usually take the form of periodic payments, though they may be commuted to a lump sum.
These policies are commonly limited to cases of total disability, or they include certain cases of partial disability but only for a limited period. In other ways too, the coverage of these policies is more restricted than workers’ compensation. For example, the benefits may be subject to termination after two years if the claimant is capable of any type of work, even though it may be at a much lower rate of pay, and even though the claimant may only be able to do that work for a few hours each week. It is also normal to terminate the benefits after an initial period on the ground that the claimant is capable of some type of work, even though that type of work is unavailable to the claimant.
Employers’ Liability
Most jurisdictions have, or have had, a law that makes employers liable in some circumstances for disabilities caused to their employees. Commonly, the criteria of liability are negligence by the employer, by management personnel, or by a fellow worker, or some breach of statute law or of a health or safety regulation. This liability may be the creation of the courts through case-law, the creation of statute, or it may be part of a civil code.
The compensation takes the form of a lump sum, known as “damages”. The amount may include an estimate of economic losses (usually loss of earnings) and an intuitive award for non-economic losses (such as pain and suffering, disfigurement, sexual dysfunction, impairment of social activities and loss of expectation of life). The lump sum will cover estimates of future and past loss. In fatal cases, the damages recoverable by dependants may include the loss of their participation in what would have been the future earnings of the worker, and in some jurisdictions, an award may also be made to dependants for non-economic losses. If negligence by the worker was a contributing cause, that would bar the claim in some jurisdictions. In others it would reduce the damages.
In jurisdictions that do not have a workers’ compensation system, the law of employers’ liability usually remains in full effect, though eligibility for benefits under a broad-based social insurance or social security system may reduce the damages. In some jurisdictions, employers’ liability remains in effect, but its scope is more confined. Where a disabled worker in some jurisdictions receives benefits under a broad social insurance system, that system is subrogated to the claim against the employer.
In jurisdictions that have a workers’ compensation system, but one that does not cover all industries or all occupations, the law of employers’ liability usually remains in full effect for those who are not covered by workers’ compensation.
Where a disability or death is covered by a workers’ compensation system, this usually has one of the following consequences for employers’ liability.
- Employers’ liability remains in effect, but a claimant must elect whether to claim workers’ compensation benefits or pursue the liability claim against the employer. Where the worker elects to pursue the employers’ liability claim, that extinguishes the workers’ compensation claim in some jurisdictions. In others, the workers’ compensation claim may be pursued if the employers’ liability claim fails.
- Employers’ liability remains in effect, but there is a set-off so that damages can only be recovered for any losses in excess of workers’ compensation benefits.
- Employers’ liability remains in effect, but it is confined to damages for non-monetary losses.
- Employers’ liability claims are excluded for workers who are covered by workers’ compensation, but with some limited exceptions, such as injuries that were caused “intentionally” by the employer, or that occurred on a highway. Subparagraphs 1, 2 or 3 may then apply.
- Employers’ liability claims are excluded for workers who are covered by workers’ compensation. In some jurisdictions, this exclusion also covers claims for damages for personal injury against fellow employees, against any other employer who is covered by the workers’ compensation system, and against any worker of such other employer, as long as the claim is based on conduct of the defendant that occurred in the course of employment or business.
In jurisdictions in which employers’ liability remains in effect for cases that are covered by workers’ compensation, the workers’ compensation benefits seem to be more restricted, and that is to be expected.
Where employers’ liability claims are prohibited, the prohibition often applies only to claims for damages for the injury or disease. Thus in some jurisdictions, a claim may still lie on other grounds. For example, a claim for damages may still lie against an employer for impeding the processing of a workers’ compensation claim, such as by failing to comply with statutory obligations to maintain or supply data relating to the exposure of a worker to contamination. Also the prohibition of employers’ liability claims usually applies only to disabilities that are compensable under the workers’ compensation system. Thus if a worker becomes disabled because of negligence by an employer, but is not eligible for workers’ compensation, an action for damages against the employer would not be barred. For example, in some jurisdictions, compensation is not payable for occupational stress; nor is workers’ compensation payable for a disability to a child resulting from a pre-natal exposure or injury to a parent during the course of employment. In these situations, an action for damages against the employer would not usually be precluded by workers’ compensation legislation.
Globalizing Technologies and the Decimation/Transformation of Work
The new technologies of computer-communications are no longer a set of tools and production methods within an industrial landscape. They have become the landscape, and they surround us, as Canadian communications scholar Marshall McLuhan predicted in the 1960s. The communications systems of the new economy constitute not only the new tools of production; they are also the new and fully programmed environment for work and economic activity, which changes everything, both quantitatively (in terms of jobs and skill sets) and qualitatively (in terms of control and domination). With the magnitude of the transformation, it is fitting to think of the changes as a paradigm shift from the industrial to the post-industrial era.
The paradigm shift began with computerization and its related automation of work in the 1970s and early 1980s. The shift continued with the integration of computers and communications, which created back-office production sub-systems and front-office management information systems in the white-collar environment. As the convergence improved, the integration was extended from small, local sub-systems to large national and multinational units, with “back-office” and “front-office” operations fully integrated. Gradually, the communications aspect became more central, and the “netware” for networking became as important as stand-alone hardware and software. By the early 1990s, perceptions about the systems also started to shift. Corporate and other networks were seen to be a means to achieving other ends, and the networks were regarded as ends in themselves. The global information superhighway, or autobahn, has emerged to become a new post-industrial networking infrastructure, and the paradigm has shifted completely. Networks have become the context of the new economy. Increasingly, they are the site where business deals are made, and the medium through which not only money but also goods and services, and work itself, are distributed. Networks are also the key to the re-engineering and restructuring of the industrial economy into a post-industrial economy—at least in that sector of the international economy which is dominated by monopoly-scale transnational corporations. The global information and production networks provide these companies with a distinct advantage over newly developed and developing countries on every measure of corporate performance from productivity to scale to speed. Networking can position these companies to launch a new wave of global “colonization” if they so desired.
Three technologies in particular highlight the scope of the transformation taking place:
- the information superhighway
- a planning tool called “quick response”
- a production-organizing strategy called “agility”.
The superhighway represents the convergence of many technologies, including television, video games, interactive shopping and electronic publishing, with the core technologies of computers and communications. Computers and communications remain the bedrock technologies, enabling and extending the scope of all the others. That scope has been boosted significantly since the early 1990s through major public investment in the highway infrastructures in many industrialized countries. Furthermore, while media coverage boosting the highway among the general public has emphasized its potential in education and entertainment, its core use from the beginning has been for business. The forerunner to the US National Information Infrastructure Program launched in 1994 was the then Senator Al Gore’s High Performance Computing Act of 1988, which was directed exclusively at big business. In Canada, the first federal government publication on the information highway, in 1994, referred to it as a tool for business competitiveness.
Quick response (QR) might have remained simply an interesting marketing ploy by the Italian clothing chain Benetton, but for the new centrality of networks. The original idea was simply to create an on-line feedback link between stores selling Benetton clothing and the company head office where the work of actually making the clothes in different styles, colours and sizes was contracted out to local knitters. Since the early 1990s, QR has come to set a new standard for performance in every sector of the economy.
In the military, quick response was used to produce innovative weapons systems during the Persian Gulf War. In industry, it has been used in the production of semi-customized jeans and other retail products. In the service sector, it has been used to provide health care to the community, where cutbacks in public-service spending have closed hospitals and reduced or eliminated institutional services. Through QR techniques, what had proceeded as a series of stages or separate activities occurring within one or two institutional sites has become a fluid interplay of concurrent stages and disaggregated actions occurring within a host of disparate sites. Yet they are all coordinated through electronic networks and centralized management information systems. Where people and work groups had provided the necessary coordination and integration within different worksites, now systems software knits and manages the links.
Agility is the term used to describe that which delivers the necessary fluidity to actual sites on the ground. Agility is considered to be the final stage of re-engineering the production process through the use of computer communications. The restructuring began with the integration of automated sub-systems to create larger, semi-cybernetic operating systems. This was called computer-integrated manufacturing. As the systems involved in this stage were steadily expanded to include subcontractors and suppliers within corporations’ operating networks, computer-integrated manufacturing gave way to just-in-time manufacturing, which represents the “hinge” of the paradigm shift, wherein the re-engineered production system was transformed (or “morphed”) into a new time-sensitive conception of the production process. With lean production, as it is also described, the focus shifted from integrating the machines in this new process to integrating the people who were left operating the systems. Quality circles, total quality management and other “cultural training” programmes schooled workers to identify with the productivity and competitive goals of management and to assist in constantly fine-tuning the production process to achieve these goals. Increasingly in the early 1990s, that fine-tuning shifted towards the harmonization of operations around standardized norms and sub-systems. Increasingly, too, the focus shifted from flexibility and interchangeability within local production facilities to interchangeability across globally- networked facilities. The goal of agility, which had yet to be realized in the mid-1990s, was the flexible dispatch of work among a distributed array of worksites plugged into (and plug-compatible with) the information highway. The related goal was to create and tap a global pool of labour located everywhere, from automated factories, workshops, clinics and offices to private homes, basements, garages and trucks.
Such restructuring has had a profound impact on the extent and nature of employment, the dimensions of which include:
- rising levels of structural unemployment as machines and machine intelligence take over what people and human intelligence used to do
- increasing polarization in the labour force, characterized on the one hand by those who work too hard, with chronic overtime and full-time jobs, and, on the other hand, by those constituting a growing “contingent” labour force on the periphery, employed on a part-time, temporary or short-term contract basis only
- a transformation of the labour process, particularly for many in the second group of workers as they become totally enclosed in a programmed work environment, with computers both defining the work to be done and monitoring and measuring its performance.
In essence, the working relationship is increasingly being transformed from an open system featuring labour, capital equipment and management to a closed cybernetic system of which the worker is a functioning part or, in the service sector, a personable human extension. Instead of people working with machines and tools, more and more people work for the machines, and even inside them in the sense of functioning as the human voice-boxes, fingers and arms of fully programmed production or information-processing systems. It could represent what Donna Haraway calls a new cybernetics of labour, with labour relations defined and negotiated entirely in systems operating terms (Haraway 1991).
There is little consensus on these trends. In fact, there is considerable controversy, sustained in part by lack of research in important areas, and by rigidities in the discourse. As one example the annual OECD Jobs Study for 1994 refused to draw a link between technological restructuring and the wretchedly high rates of unemployment which have prevailed through the industrialized and industrializing world since the 1980s. The report acknowledged that the new technologies have had some “labour-displacing” effects; however, it also assumed that firms “may be able to create compensating employment whenever they are successful in combining such processes of technological change with product innovation and sound marketing policies” (OECD 1994).
The discourse on technological change has been rigid in at least two ways, the results of which could now be to misinform and even disinform the debate on restructuring as much as they have intended to inform it. In the first instance, it pursues a narrowly abstract economic or “economistic” model of restructuring, and ignores not only the social but also the psychological and cultural dimensions involved. Secondly, this economistic model is seriously flawed. It assumes that as technology increases productivity through automation, innovative new economic activity and new employment will emerge to compensate (though perhaps not with the same skill requirements) for what was lost in the automation phase. Not only is new economic activity (and what new employment it does generate) emerging in globally remote sites, but much of the new economic growth since the late 1980s has been “jobless economic growth”. Sometimes it is fully automated production and processing facilities churning out double and triple what they put through previously, with no increase in staff. Or it is fully automated new services such as call-forwarding in telecommunications or multi-branch banking in finance, “produced” and “delivered” by software alone. Increasingly too, semi-automated work has been transferred from the paid hands of workers to the unpaid hands of consumers. Consumers using digital phones now “work” their way through a string of computerized voice clips to order goods and services, register for courses, negotiate for government services, and obtain customer service.
It is important to confront the rigidities permeating the discourse because, here, the separation of economistic “supply-side” issues from “labour market”, “demand-side” issues in the social and cultural context blocks the gathering of information essential for developing a consensus on what’s happening with the new technologies. For example, Statistics Canada has conducted some excellent macro-level studies exploring the increased polarization of the Canadian labour force. These emerged following a 1988 study on changing youth wages and the declining middle wage (Myles, Picot and Wannell 1988). The study documented a massive hollowing out of middle-ranking jobs (according to pay scale) in virtually every industrial sector and in every major occupation between 1981 and 1986. Furthermore, job growth was severely polarized between the lowest wage levels and the high end of the wage scale (see figure 1).
Figure 1. Net change in full-time equivalent jobs, 1981-1986, by occupation and wage level (in thousand US$).
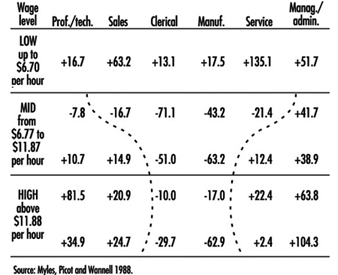
The study seemed to provide a macro-level confirmation of the computerization, and related simplification and de-skilling, of work which the case studies of technological restructuring during that period had identified everywhere from resource industries through manufacturing to services (Menzies 1989). A follow-up study began by referring to literature arguing a link between widening wage differentials and technological change (Morissette, Myles and Picot 1993). However, it then confined itself to examining strictly “labour market” factors such as hours of work, gender, age and educational attainment. It concluded that a “growing polarization in both weekly and annual hours worked accounted for much of the rise in earnings inequality in the 1980s”. It sidestepped the possible link between the computer simplification of work and the rise of a contingent labour force of part-time, temporary workers employed at well below a standard week’s worth of hours and income. Instead, it ended lamely, saying that “If changing technologies and the associated changing skill mix required are a major part of the story, existing data sources are not up to the task.”
The existing data sources are case studies, many undertaken by unions or women’s groups. Their methodologies might not be of a uniform standard. Nevertheless, their findings suggest a decided pattern. In case after case through the late 1980s and early 1990s, computer systems were implemented not to enhance what people were doing but to replace them or diminish and control what they were doing (Menzies 1989). Not only did layoffs accompany large-scale computerization, but full-time staff were replaced by part-time or other temporary staff, in a wide array of industries and occupations. From the evidence, particularly of interview-based studies, it seems clear that it was the computer-simplification of work—particularly the takeover of administration, planning and management by software—which made it possible to replace full-time staff with part-time staff or to transfer it outside the labour force into the unpaid hands of consumers.
Often, the technological change was accompanied by organizational restructuring. This included a collapsing of job-classification levels and an integration of computer-simplified tasks. This has often resulted in a streamlining of jobs around computer systems so that the work can be entirely defined by the computer system, and its performance can be monitored and measured by it as well. Sometimes this has resulted in some re-skilling or skills upgrading. For instance, in the automobile, aerospace and electronics industries in Canada, reports repeatedly point to the creation of a fairly senior new multi-task, multi-skilled position. Sometimes it is called electronics technician, or ET. Here, the work often involves overseeing the operations of several automated machines or sub-systems, troubleshooting and even some planning and analysis. The people involved not only have to be familiar with a number of operating systems, but sometimes also have to do some simple programming to knit different sub-systems together. Often, too, however, these positions represent a trickling down of what had been highly skilled tools and trades jobs as computerization has turned the creative work over to engineers and salaried programmers. Nevertheless, for the people involved, it often represents a large and welcome step up in terms of job challenge and responsibility.
While there is evidence of re-skilling, this is the minority trend, generally affecting a more privileged core of full-time and fully unionized industrial-sector workers—most of them men. The larger trend is toward de-skilling and even the degradation of work as people become enclosed in computer-operating environments which rigorously programme, and monitor, everything they do. Essentially, the person works as the human extension of the computer operating system, while the system does all the essential thinking and decision making. This new form of work is becoming more and more prevalent in more and more lines of work, particularly where women are concentrated: in clerical, sales and service work.
The term McJob has become a popular epithet for this new form of work where the computer defines and controls the work to be done. By the 1990s, the term applied in a host of settings from fast-food restaurants to grocery check-out lines to accounting, insurance claims-processing and other types of offices, and even in the health-care field. By the mid-1990s, however, another trend had emerged from the computerization of work—at least of information-processing work. This trend has been called “telework”. Once work had come to be fully defined and controlled by computer systems, it could also be de-institutionalized and redeployed through electronic networks to remote call-processing centres or to teleworkers employed in their homes via computers and modem attachments. Telework was starting to emerge as a major labour issue in the mid-1990s, with the proliferation of call centres for handling airline and hotel reservations, remote banking and insurance service work, courier and other services. As well, the 1991 Canadian Census recorded a 40% rise in the “at-home” workforce, compared to a 16% rise in the labour force as a whole. It also found a high concentration of women in this growing at-home labour force. They were concentrated in clerical, sales and service work. They were working for incomes of less than Can$20,000 and often less than Can$10,000—not enough to support a life, let alone a family.
Depending on the trends, and on how the technological landscape for work and economic activity is structured and governed, telework could emerge as the post-Fordist work model—that is the successor to a high-wage full employment pattern—in place of the high-value-added model associated with Toyota and Suzuki and Japanese “lean production”. However, both models might prevail, with the precarious low wage telework model identified more with women, young workers and other less privileged groups, and the latter identified more with men holding the additional advantage of strong unions, seniority and full-time jobs in capital-intensive industries such as autos, aerospace and electronics.
The rise of telework surfaces a number of labour issues: the danger of sweatshop-like exploitation, highlighted by the rise in performance-related compensation as an adjunct to or replacement for a regular hourly wage; poor and debilitating working conditions as people rig up modems and computers in their basements or in the bedroom of one-bedroom apartments, often bearing overhead and maintenance costs themselves; stagnation, boredom and loneliness as people work in isolated silicon cells, without the camaraderie of others, and without the protection of collective organization. One of the most pressing labour issues, however, involves the new cybernetics of labour, and what happens as people’s work lives become totally controlled by computer systems. There has been little research into these more qualitative aspects of work. Perhaps, they require a more qualitative story-telling approach, rather than the more objectifying methods of social-science research. In Canada, two documentary films have shed valuable light on the personal experience of computer-defined, computer-controlled work. One film, “Quel Numéro/ What Number?” directed by Sophie Bissonette, features telephone operators talking about working in isolated work cubicles at long-distance call-processing centres. Not only does the computer control every aspect of their work but it also provides them with their only feedback on how well they’re performing at it. This is the computer’s feedback on the average time (AWT) they take processing each customer call. The women talk about becoming so well adjusted to “operating” as part of the computer-defined system that they get “hooked” on trying to beat their own AWT work-time score. It is a psychosocial process of adjustment when the only context and meaning for one’s activity is being dictated, here by the computer system.
Another film, “Working Lean”, directed by Laura Sky, documents a similar effect achieved through the cultural training programmes of Total Quality Management. In this film the workers are not totally enclosed and isolated inside a wholly computer-programmed work cell but are auto workers involved in TQM teams. Here the rhethoric of co-management and empowerment closed the horizon on workers’ perceptions. Training urges them to identify with management’s productivity goals built into the production systems, by finding ways to fine-tune them. (The Japanese prototype of this management programme defines quality in strictly systems terms, as “performance to requirements” (Davidow and Malone 1992).) Union officials refer to the programme as “management by stress”. Meanwhile, in many workplaces, repetitive-strain injury and other stress-related disease is on the rise as workers find themselves driven by fast-paced technology and its accompanying rhetoric.
A survey of Canadian workplace training found that at least half of the “training” companies are providing is in areas associated with TQM: corporate communications, leadership and other “cultural training”. “Training more closely linked to developing human capital was far less frequently reported.” On the other hand, within the category of computer-skills training, the study found a decided shift in who gets this training—a shift dramatically favouring managerial, professional and technical employees after 1985 (Betcherman 1994).
There are many contradictory trends. For example, there are some workplaces—some hotels, for instance—where co-management seems to be living up to its rhetoric. There are some worksites where workers are doing more with the new technologies than they were able or allowed to do with the old. But overall, the trends associated with restructuring in the new economy are towards the replacement of smart people with smart machines, and the use of machines to diminish and control what other people are doing, particularly at work. The central issue is not job creation or training in new computer skills. The issue is control: people are coming to be controlled by cybernetic computer systems. This needs to be turned around before both democratic rights and basic human rights are destroyed.
Transformations in Markets and Labour
The massive and dramatic restructuring that is evident at the local, national and international levels has profound implications for the health of workers.
At the international level, a new global economy has emerged as both capital and labour have become increasingly mobile within and among countries. This new economy has been marked by the negotiation of trade agreements which simultaneously remove barriers among countries and provide protection from those outside their common markets. These agreements, such as the North American Free Trade Agreement (NAFTA) and the European Union, cover much more than trade issues; indeed they encompass the entire role of the state. Along with these agreements have come a commitment to freer markets, deregulation of the private sector and the privatization of many state enterprises.
In some cases, the agreements have led to common standards that raise the level of protection provided to workers in countries where previously such protection was minimal or absent. In other cases, the condition of membership or aid has been de-unionization and movement away from social services, rural agriculture and local enterprise. And in still other cases, unionized workers have successfully resisted efforts to change their conditions. In all cases, however, national boundaries, national economies and national governments have become less important in structuring work relations and in determining the location of work.
Although the new global economy is characterized by the continuing expansion of transnational corporations, it has not been accompanied by the creation of larger and larger establishments. Indeed, the opposite is the case. The prototype enterprise is no longer the giant car plant with thousands of employees producing a standard product by following a fixed production line. Instead, more and more corporations use niche production to provide customized goods and, increasingly, services. Rather than employ economies of scale they employ economies of scope, shifting from one product to another with the help of sub-contracting and equipment that can easily be reprogrammed.
In fact, at least part of the massive shift to the service industries and the rapid growth in small businesses can be explained by transnational corporations contracting out their work. In the work that continues to be done directly by the corporation, large inventories and buffer stocks are frequently replaced by “just-in-time” production, and firms see themselves as increasingly customer driven. More employers are demanding a flexible workforce, one that has a range of skills and a variety of work times. In this way, employees too can work “just-in-time” and at a number of work stations. This increase in contracting out and in multi-tasking, along with the move to “non-standard” forms of employment such as part-time and part-year work, make it difficult for unions to follow the traditional means of organizing workplaces.
Both the development of a global economy and the restructuring of work have been made possible by the new microelectronics technology. This technology makes niche production possible, because new equipment can be altered quickly and cheaply to accommodate new lines. Moreover, this technology not only creates inexpensive and instant communication throughout the world, independent of time zones or other barriers , but also allows the corporation to maintain control over remote enterprises of workers, because it can monitor output in other locations. It thus creates the possibility for production in the home with workers employed anywhere in the world at any time of the day or night.
At the same time, this technology helps to transform the kinds of skill required and the organization of work within enterprises. Increasingly, employers are talking about multi-skilling for workers who control and monitor a variety of machines and who must move between work stations. More and more workers analyse and apply the information generated, processed, stored and retrieved by the new technologies. Both kinds of worker may be organized in teams so that they can work together to continuously improve quality.
This continuous quality improvement is intended to put the focus on the work process as a means of eliminating error and waste. Much of this quality improvement is measured by the new technologies that allow employers and employees to monitor continually the time taken by each worker, the resources used and the amount and quality of the product or service. Managers, especially at the intermediate level, become less necessary because there are fewer supervisory tasks. As a result, hierarchies are flattened and there are fewer promotion routes to the top. Those managers who remain are more involved with strategic considerations than with direct supervision.
The technologies also make it possible for employers to demand a flexible labour force, not just in terms of skills, but also in terms of time. The technology allows employers to use formulas to calculate the precise amount of work time required for the job, and the hours when the work must be done. It therefore allows employers to hire precisely for the number of work hours required. Moreover, the technology can eliminate the traditional costs associated with hiring a variety of workers for short periods of time, because it can determine how many workers are necessary, call them to come to work, calculate their pay and write their cheques. Although the technologies make it possible to monitor and count in incredible detail, they also make transnational corporations more vulnerable, because one power failure, or a computer “glitch”, could delay or shut down the entire process.
All this restructuring has been accompanied by rising unemployment and increasing disparities between the rich and the poor. As companies become leaner and meaner, the demand for employees declines. Even among those who still have jobs, there is little employment security in the new global economy. Many of those with jobs are working very long work weeks, although some do so for only short periods of time as more and more work is done on a contract or piece-work basis. Shift work and irregular work hours have increased significantly as employers rely on a flexible workforce. With only irregular employment, fewer workers have employment-linked protection from unemployment and fewer are represented by strong unions.
This is particularly the case for women, who already form the majority of the casual labour force and of the non-unionized workforce. Governments are also reducing the provision of social services for those without work. Moreover, the combination of new technologies and new organizations of work often results in jobless growth, with both profit and unemployment increasing simultaneously. Economic development no longer means more paid work.
The implication of these developments for workers’ health are enormous, although often more difficult to see than those found in traditional industrial work organizations. Non-standard employment, like unemployment, can increase the health risks for workers. While workers can be quite productive in short work periods, irregular employment may have the opposite effect over the long term, especially if workers are unable to make plans for the future. It can lead to increased levels of anxiety and nervousness, to irritability and lack of confidence and an inability to concentrate. It also can have physical consequences such as high blood pressure and an increased incidence of illnesses such as diabetes and bronchitis. Moreover, irregular employment and non-standard work times can make it very difficult for the women who bear the major responsibility for child care, elder care and domestic chores to organize their work, and thus can significantly increase their stress levels. Furthermore, irregular employment usually means irregular income and often loss of work-related benefits such as dental care, pensions, sick leave and health care. These, too, contribute to the stress workers face and limit their ability to remain healthy or productive.
New methods of organizing work also may be increasing the health hazards for those with more regular employment. A number of studies indicate that unhealthy or inappropriate job design and work organization can increase the risk of heart disease and stroke, as well as other work-related health concerns such as repetitive strain injury. The greatest stress is produced by jobs that offer workers little control over their work or work time, those which require few recognized skills and those that do not allow workers to determine which skills they use. These stress levels may be increased even more for the majority of women, who also have a second job at home.
Although the new work organizations based on teams and multi-skilling promise to increase both the range of skills workers employ and their control over work, in the context of continuous quality improvement they can have the opposite effect. The focus is usually on short-term, easily quantifiable increases in productivity rather than on the long-term results or overall health of the workers. Especially when team members are not replaced during sickness, when team quotas are set by management alone or when output is measured by detailed formulas, team structures may mean less individual control and little collective collaboration to establish individual contributions. In addition, multi-skilling may mean that workers are required to do a wide variety of tasks in rapid succession. Their range of skills is intended to ensure that every second is used, that there are no breaks created by the nature of the work or the transfer of tasks from one worker to another. Particularly in the context of less individual control, the pace set by such work can result in repetitive strain injury or a variety of stress-related symptoms.
Similarly, the new technologies that increase output and make flexible work schedules more possible also can mean loss of control for workers, increased work speed and more repetitious work. In allowing the precise calculation of both work time and output, the new technologies make possible continuous quality improvement and the elimination of waste time. But slack time also can be physical and psychological recovery time, and without such time, workers often experience higher blood pressure levels, increased nervous system activity and generally greater strain. In allowing the electronic measurement of workers’ activities, the new technologies also limit workers’ control, and less control means higher risk of illness. In eliminating many of the mental and manual aspects of the work previously done by a range of workers, the new technologies can also reduce the variety in jobs and thus make work more stultifying and less skilled.
At the same time that work is being reorganized, it is also being relocated both within and among countries. What may be called outwork or home work is increasing. New organizations of work make it possible for more and more production to be done in small workplaces. And new technologies make it possible for more workers to buy their own equipment and work at home. Today, many service jobs such as accounting and filing can be done at home, and even auto parts can be produced within households. Although work at home can reduce commuting time, can increase choices about work time, can make it possible for the disabled to take on paid employment and can allow women to care for their children or the elderly, it also can be dangerous to health. Health hazards in the home are even less visible to others than those in the new workplaces.
Any health hazards created directly by the equipment or the materials involved in the workplace can place the entire household at risk twenty-four hours a day. Without the separation of home and work, workers often feel pressured to work all the time at work that is never done. Conflicts can develop between the demands of children, the elderly and household chores that raise the levels of stress for the entire household. The isolation from other workers doing a similar job can make the work both less satisfying and less likely to be protected through union membership. Physical and mental assault problems remain hidden in the household. This may be the case particularly for the disabled, who then have less choice about working with others because the pressure on employers to make jobs in the market accessible for the disabled is reduced.
Although people in many countries throughout the world have long worked from their homes, the new global economy often involves a new kind of home work. This home work includes new work relations with a remote employer who can have a great deal of control over the home work. Thus, in spite of allowing workers to remain within their households far away from their employers, the new home work may decrease workers’ control over the nature and pace of their work without improving their work environment.
Those who live in many of the southern countries are drawn into the global economy as homeworkers for international corporations. These homeworkers are even more vulnerable to health risks than those in the north and even more likely to have less control over their work. Many are located in free trade zones where protection for workers is eliminated, often as a means of encouraging investment.
At the same time, in both the north and south, cutbacks in state services frequently mean a relocation and redistribution of work for women. With fewer services provided in the public sector, there are fewer paid jobs for women in the labour force. More services are expected to be provided by women, without pay, in the home. Although women bear most of the burden, this transfer of work to the home increases the strain on all household members and lowers their immunity. The increased responsibility at home also may increase the pressure on women and their children to do home work.
In some countries, the growth of both home work and small business means that many employers are no longer subject to state regulations that provide standards for pay, promotion, work hours, conditions and relations, standards such as those forbidding sexual harassment and arbitrary firing. In any case, the expansion of small businesses and home work makes it more difficult to enforce health and safety standards in these many and varied workplaces. Similarly, the growth in contract work often means that the worker is defined as self-employed and thus ineligible for protection from the person who pays for the work. What might be called a legal underground economy is emerging: an economy in which standards related to health and safety no longer apply and unions are more difficult to organize.
There certainly are still significant differences in economies throughout the world. And there are certainly large differences among workers both within and between countries regarding the kinds of work and pay they receive, as well as the protection they have and the hazards they face. However, the emerging global economy is threatening the protection many workers have gained, and there is a growing pressure for states to “harmonize down” in terms of less emphasis on protection and services as free trade increasingly becomes the goal.
Precarious Employment and Child Labour
The section of this article devoted to child labour is based largely on the report of the ILO Committee on Employment and Social Policy: Child Labour, GB.264/ESP/1, 264th Session, Geneva, November 1995
Throughout the world, not only in the developing but also in the industrialized countries, there are many millions of workers whose employment may be termed precarious from the standpoint of its potential effect on their health and well-being. They may be divided into a number of non-exclusive categories based on the kinds of work they perform and the types of relationship to their jobs and to their employers, such as the following:
- child labourers
- contract labourers
- enslaved and bonded workers
- informal sector workers
- migrant workers
- piece-workers
- unemployed and underemployed workers.
Their common denominators include: poverty; lack of education and training; exposure to exploitation and abuse; ill health and lack of adequate medical care; exposure to health and safety hazards; lack of protection by governmental agencies even where laws and regulations have been articulated; lack of social welfare benefits (e.g., minimum wages, unemployment insurance, health insurance and pensions); and lack of an effective voice in movements to improve their lot. In large part, their victimization stems from the poverty and the lack of education/training that force them to take whatever kind of work may be available. In some areas and in some industries, the existence of these classes of workers is fostered by explicit economic and social policies of the government or, even where they have been prohibited by local laws and/or endorsement of international Conventions, by the deliberate inattention of governmental regulatory agencies. The costs to these workers and their families in terms of ill-health, shortened life-expectancy and impact on well-being are imponderable; they often extend from one generation to the next. By any sort of measure, they may be considered disadvantaged.
The exploitation of labour is also one deleterious aspect of the global economy wherein the most dangerous and precarious work is transferred from the richer countries to the poorer ones. Thus, precarious employment can and should be viewed in macro-economic terms as well. This is discussed more fully elsewhere in this Encyclopaedia.
This article briefly summarizes the characteristics of the more important of these employment categories and their effects on workers’ health and well-being.
Migrant Workers
Migrant workers often represent a critically important segment of a country’s labour force. Some bring developed skills and professional competencies that are in short supply, particularly in areas of rapid industrial growth. Typically, however, they perform the unskilled and semi-skilled, low-paying jobs that are scorned by workers native to the area. These include “stooped labour” such as cultivating and harvesting crops, manual labour in the construction industry, menial services such as cleaning and refuse removal, and poorly remunerative repetitive jobs such as those in “sweatshops” in the apparel industry or on assembly-line work in light industries.
Some migrant workers find jobs in their own countries, but, more recently, they are for the most part “external” workers in that they come from another, usually less-developed country. Thus, they make unique contributions to the economy of two nations: by doing necessary work in the country in which they are working, and by their remittances of “hard” money to the families they leave behind in the country from which they came.
During the nineteenth century, large numbers of Chinese labourers were imported into the United States and Canada, for example, to work on the construction of the western portions of the transcontinental railroads. Later, during the Second World War, while American workers were serving in the armed forces or in the war industries, the United States reached a formal agreement with Mexico known as the Bracero Program (1942–1964) that provided millions of temporary Mexican workers for the vitally important agricultural industry. During the postwar period, “guest” workers from southern Europe, Turkey and North Africa helped to rebuild the war-ravaged countries of western Europe and, during the 1970s and 1980s, Saudi Arabia, Kuwait and the other newly rich oil-producing countries of the Near East imported Asians to build their new cities. During the early 1980s, external migrant workers accounted for approximately two-thirds of the workforces in the Arab Gulf states (citizen workers outnumbered the expatriates only in Bahrain).
Except for teachers and health workers, most of the migrants have been male. However, in most countries throughout these periods as families became wealthier, there has been an increasing demand for the importation of domestic workers, mostly women, to perform housework and provide care for infants and children (Anderson 1993). This has also been true in industrialized countries where increasing numbers of women were entering the workforce and needed household help to take up their traditional home-making activities.
Another example can be found in Africa. After the Republic of Transkei was created in 1976 as the first of the ten independent homelands called for in South Africa’s 1959 Promotion of Self-Government Act, migrant labour was its major export. Located on the Indian Ocean on the east coast of South Africa, it sent about 370,000 Xhosa males, its dominant ethnic group, as migrant workers to neighbouring South Africa, a number representing approximately 17% of its total population.
Some migrant workers have visas and temporary work permits, but these are often controlled by their employers. This means that they cannot change jobs or complain about mistreatment for fear that this will lead to revocation of their work permits and forced repatriation. Often, they evade the official immigration procedures of the host country and become “illegal” or “undocumented" workers. In some instances, migrant workers are recruited by labour “contractors” who charge exorbitant fees to smuggle them into the country to meet the needs of local employers. Fear of arrest and deportation, compounded by their unfamiliarity with the language, laws and customs of the host country, makes such workers particularly vulnerable to exploitation and abuse.
Migrant workers are frequently overworked, deprived of the benefit of proper tools and equipment, and often knowingly exposed to preventable health and safety hazards. Crowded, sub-standard housing (often lacking potable drinking water and basic sanitary facilities), malnutrition and the absence of access to medical care make them particularly subject to contagious diseases such as parasitic infections, hepatitis, tuberculosis and, more recently, AIDS. They are often underpaid or actually cheated of much of what they earn, especially when they are living illegally in a country and hence are denied basic legal rights. If apprehended by authorities, it is usually the “undocumented” migrant workers who are penalized rather than the employers and contractors who exploit them. Further, particularly during periods of economic downturn and rising unemployment, even documented migrant workers may be subject to deportation.
The International Labour Organization has for long been concerned with the problems of migrant workers. It first addressed them in its Migration for Employment Convention, 1949 (No. 97), and the related Recommendation No. 86, and revisited them in its Migrant Workers (Supplementary Provisions) Convention, 1975 (No. 143), and the related Recommendation No. 151. These Conventions, which have the force of treaties when ratified by countries, contain provisions aimed at eliminating abusive conditions and ensuring basic human rights and equal treatment for migrants. The recommendations provide non-binding guidelines to orient national policy and practice; Recommendation No. 86, for example, includes a model bilateral agreement that can be used by two countries as the basis for an operational agreement on the management of migrant labour.
In 1990, the United Nations adopted the International Convention on the Protection of the Rights of All Migrant Workers and Members of Their Families, which formulates basic human rights for migrant workers and their families, including: the right not to be subjected to torture or to cruel, inhuman or degrading treatment or punishment; the right to be treated no less favourably than national workers in respect to conditions of work and terms of employment; and the right to join unions and seek their assistance. This UN Convention will enter into force when it has been ratified by 20 nations; as of July 1995, it had been ratified by only five (Egypt, Colombia, Morocco, the Philippines and Seychelles) and it had been signed but not yet formally ratified by Chile and Mexico. It should be noted that neither the ILO nor the UN has any power to compel compliance with the Conventions other than collective political pressures, and must rely on the Member States to enforce them.
It has been observed that, at least in Asia, international dialogue on the matter of migrant workers has been hindered by its political sensitivity. Lim and Oishi (1996) note that countries exporting workers are fearful of losing their market share to others, especially since the recent global economic downturn has prompted more countries to enter the international market for migrant labour and to export their ‘‘cheap and docile’’ labour to a limited number of increasingly choosy host countries.
Piece-Workers
Piece-work is a compensation system that pays workers per unit of production accomplished. The unit of payment may be based on completion of the entire item or article or just one stage in its production. This system is generally applied in industries where the method of production consists of distinct, repetitive tasks whose performance can be credited to an individual worker. Thus, earnings are directly linked to the individual worker’s productivity (in some workplaces producing larger or more complicated items, such as automobiles, the workers are organized into teams which divide the per piece payment). Some employers share the rewards of greater productivity by supplementing the per piece payments with bonuses based on the profitability of the enterprise.
Piece-work is concentrated, by and large, in low-paying, light industries such as apparel and small assembly shops. It is also characteristic for sales people, independent contractors, repair personnel and others who are usually seen as different from shop workers.
The system can work well when employers are enlightened and concerned about workers’ health and welfare, and particularly where the workers are organized into a trade union in order to bargain collectively for rates of payment per unit, for appropriate and well-maintained tools and equipment, for a working environment where hazards are eliminated or controlled and personal protective equipment is provided when needed, and for pensions, health insurance and other such benefits. It is helped by the ready accessibility of managers or supervisors who are themselves skilled in the production process and can train or assist workers who may be having difficulty with it and who can help to maintain a high level of morale in the workplace by paying attention to workers’ concerns.
The piece-work system, however, readily lends itself to the exploitation of the workers, with adverse effects on their health and well-being, as in the following considerations:
- Piece-work is characteristic of the notorious sweatshops, unfortunately still common in the garment and electronic industries, where workers must toil at repetitive tasks, often for 12-hour days and 7-day weeks in sub-standard and hazardous workplaces.
- Even where the employer may manifest concern about potential occupational hazards—and this does not always occur—the pressure for productivity may leave little inclination for workers to devote what amounts to unpaid time to health and safety education. It may lead them to ignore or by-pass measures designed to control potential hazards, such as removing safety guards and shields. At the same time, employers have found that there may be a drop in the quality of the work, which dictates enhancement of product inspections to prevent defective merchandise from being passed along to the customers.
- The rate of pay may be so low that earning a living wage becomes difficult or nigh impossible.
- Piece-workers may be considered “temporary” workers and as such can be declared ineligible for benefits that may be mandatory for most workers.
- Less-skilled, slower workers may be denied training that would enable them to keep pace with those who can work faster, while employers may establish quotas based on what the best workers can produce and fire those unable to meet them. (In some workplaces, workers agree among themselves on production quotas that require the faster workers to slow down or stop working, thereby spreading the available work and the earnings more evenly among the work group.)
Contract Labour
Contract labour is a system in which a third party or organization contracts with employers to provide the services of workers when and where they are needed. They fall into three categories:
- Temporary workers are hired for a short period to fill in for employees who are absent because of illness or who are on leave, to augment the workforce when peaks in workload are not likely to be sustained, and when particular skills are needed only for a limited period.
- Leased workers are supplied on a more or less permanent basis to employers who, for a variety of reasons, do not wish to increase their workforces. These reasons include saving the effort and costs of personnel management and avoiding commitments such as rate of pay and the benefits won by the “regular” employees. In some instances, jobs have been eliminated in the course of a “downsizing” and the same people rehired as leased workers.
- Contract workers are groups of workers recruited by contractors and transported, sometimes for great distances and to other countries, to perform jobs that cannot be filled locally. These are usually low-paying, less desirable jobs involving hard physical labour or repetitive work. Some contractors recruit workers striving to improve their lots by emigrating to a new country and make them sign agreements committing them to work at the behest of the particular contractor until the often exorbitant transportation costs, fees and living expenses have been repaid.
One fundamental issue among the many possible problems with such arrangements, is whether the owner of the enterprise or the contractor supplying the workers is responsible for the safety, health and welfare of the workers. There is often “buck-passing”, in which each claims that the other is responsible for substandard working conditions (and, when the workers are migrants, living conditions) while the workers, who may be unfamiliar with the local language, laws and customs and too poor to obtain legal assistance, remain powerless to correct them. Contract workers are often exposed to physical and chemical hazards and are denied the education and training required to recognize and cope with them.
Informal Workers
The informal or “ undocumented” work sector includes workers who agree to work “off the books”—that is, without any formal registration or employer/employee arrangement. Payment may be in cash or in “in kind” goods or services and, since earnings are not reported to the authorities, they are not subject either to regulation or taxation for the worker and the employer. As a rule, there are no fringe benefits.
In many instances, informal work is done on an ad hoc, part-time basis, often while “moonlighting” during or after working hours on another job. It is also common among housekeepers and nannies who may be imported (sometimes illegally) from other countries where paid work is difficult to find. Many of these are required to “live in” and work long hours with very little time off. Since room and board may be considered part of their pay, their cash earnings may be very small. Finally, physical abuse and sexual harassment are not infrequent problems for these household workers (Anderson 1993).
The employer’s responsibility for the informal worker’s health and safety is only implicit, at best, and is often denied. Also, the worker is generally not eligible for workers’ compensation benefits in the event of a work-related accident or illness, and may be forced to take legal action when needed health services are not provided by the employer, a major undertaking for most of these individuals and not possible in all jurisdictions.
Slavery
Slavery is an arrangement in which one individual is regarded as an item of property, owned, exploited and dominated by another who can deny freedom of activity and movement, and who is obliged to provide only minimal food, shelter and clothing. Slaves may not marry and raise families without the owner’s permission, and may be sold or given away at will. Slaves may be required to perform any and all kinds of work without compensation and, short of the threat of impairing a valuable possession, with no concern for their health and safety.
Slavery has existed in every culture from the beginnings of human civilization as we know it down to the present. It was mentioned in the Sumerian legal codes recorded around 4,000 BC and in the Code of Hammurabi that was spelled out in ancient Babylon in the eighteenth century BC, and it exists today in parts of the world despite being prohibited by the UN’s 1945 Declaration of Human Rights and attacked and condemned by virtually every international organization including the UN Economic and Social Council, the Food and Agriculture Organization (FAO), the World Health Organization (WHO), and the ILO (Pinney 1993). Slaves have been employed in every kind of economy and, in some agricultural and manufacturing societies, have been the mainstay of production. In the slave-owning societies in the Middle East, Africa and China, slaves were employed primarily for personal and domestic services.
Slaves have traditionally been members of a different racial, ethnic, political or religious group from their owners. They were usually captured in wars or raids but, ever since the time of ancient Egypt, it has been possible for impoverished workers to sell themselves, or their wives and children, into bondage in order to pay off debts (ILO 1993b).
Unemployment and Employment Opportunity
In every country and in every type of economy there are workers who are unemployed (defined as those who are able and willing to work and who are seeking a job). Periods of unemployment are a regular feature of some industries in which the labour force expands and contracts in accord with the seasons (e.g., agriculture, construction and the apparel industry) and in cyclical industries in which workers are laid off when business declines and are rehired when it improves. Also, a certain level of turnover is characteristic of the labour market as employees leave one job to seek a better one and as young people enter the workforce replacing those who are retiring. This has been labelled frictional unemployment.
Structural unemployment occurs when whole industries decline as a result of technological advances (e.g., mining and the manufacture of steel) or in response to gross changes in the local economy. An example of the latter is the moving of manufacturing plants from an area where wages have become high to less developed areas where cheaper labour is available.
Structural unemployment, during recent decades, has also resulted from the spate of mergers, takeovers and restructurings of large enterprises that have been a common phenomenon, particularly in the United States which has far fewer mandated safeguards for worker and community well-being than do other industrialized countries. These have led to “downsizing” and shrinkage of their workforces as duplicative plants and offices have been eliminated and many jobs declared unnecessary. This has been damaging not only to those who lost their jobs but also to those who remained and were left with a loss of job security and a fear of being declared redundant.
Structural unemployment is often intractable as many workers lack the skill and flexibility to qualify for other jobs at a comparable level that may be available locally, and they often lack the resources to migrate to other areas where such jobs may be available.
When sizeable layoffs occur, there is often a “domino” effect on the community. The loss of earnings has a dampening effect on the local economy, causing the closing of shops and service enterprises frequented by the unemployed and, thereby, increasing their number.
The economic and mental stress resulting from unemployment often has significant adverse effects on the health of the workers and their families. Loss of job and, particularly, threats of job loss, have been found to be the most potent work-related stressors and have been shown to have precipitated emotional illnesses (this is discussed elsewhere in this Encyclopaedia). To prevent such adverse effects, some employers offer retraining and assistance in finding new jobs, and many countries have laws that place specific economic and social requirements on employers to provide financial and social benefits to the affected employees.
The underemployed comprise workers whose productive capacities are not fully utilized. They include part-time workers who are seeking full-time jobs, and those with higher levels of skill who can find only relatively unskilled work. In addition to lower earnings, they suffer the adverse effects of the stress of dissatisfaction with the job.
Child Labour
In most families, as soon as they are old enough to contribute, children are expected to work. This may involve helping with housekeeping chores, running errands or caring for younger siblings—in general, helping with the traditional homemaking responsibilities. In farming families or those engaged in some form of home industry, children are usually expected to help with tasks suited to their size and capabilities. These activities are almost invariably part-time, and often seasonal. Except in families where the children may be abused or exploited, this work is defined by the size and “values” of the particular family; it is unpaid and it usually does not interfere with nurturing, education and training. This article does not address such work. Rather, it focuses on children under the age of 14 who work outside the family framework in one industry or another, usually in defiance of laws and regulations governing the employment of children.
Although only sparse data are available, the ILO Bureau of Statistics has estimated that “in the developing countries alone, there are at least 120 million children between the ages of 5 and 14 who are fully at work, and more than twice as many (or about 250 million) if those for whom work is a secondary activity are included” (ILO 1996).
Earlier figures are thought to be grossly understated, as demonstrated by the much higher numbers yielded by independent surveys carried out in several countries in 1993–1994. For example, in Ghana, India, Indonesia and Senegal, approximately 25% of all children were engaged in some form of economic activity. For one-third of these children, work was their principal activity.
Child labour is found everywhere, although it is much more prevalent in poor and developing areas. It disproportionately involves girls who are not only likely to work for longer hours but, like older women, are also required to perform homemaking and housekeeping tasks to a much greater extent than their male counterparts. Children in rural areas are, on average, twice as likely to be economically active; among migrant farmworker families, it is almost the rule that all of the children work alongside their parents. However, the proportion of urban children who work is increasing steadily, mainly in the informal sector of the economy. Most urban children work in domestic services, although many are employed in manufacturing. While public attention has been focused on a few export industries such as textiles, clothing, footwear and carpets, the great majority work in jobs geared towards domestic consumption. On the whole, however, child labour remains more common on plantations than in manufacturing.
Child slavery
Many child workers are slaves. That is, the employer exercises the right of either temporary or permanent ownership in which the children have become “commodities” that can be rented out or exchanged. Traditional in South Asia, the sub-Saharan strip of East Africa and, more recently, in several South American countries, it appears to be evolving all over the world. Despite the facts that it is illegal in most countries where it exists and that the international Conventions banning it have been widely ratified, the ILO estimated (accurate data are not available) that there are tens of millions of child slaves around the world (ILO 1995). Large numbers of child slaves are to be found in agriculture, domestic service, the sex industry, the carpet and textile industries, quarrying and brick-making.
According to the report of an ILO Committee of Experts (ILO 1990), more than 30 million children are thought to be in slavery or bondage in several countries. The report cited, among others, India, Ghana, Gaza, Pakistan, Philippines, Dominican Republic, Haiti, Brazil, Peru, Mauritania, South Africa and Thailand. More than 10 million of them are concentrated in India and Pakistan. Common sites of employment for enslaved children are small workshops and as forced labour on plantations. In the informal sector they can be found in carpet weaving, match factories, glass factories, brick making, fish cleaning, mines and quarries. Children are also used as enslaved domestic labourers, as slave-prostitutes and drug carriers.
Child slavery predominates mainly where there are social systems that are based on the exploitation of poverty. Families sell the children outright or bond them into slavery in order to pay off debts or simply provide the wherewithal to survive, or to supply the means to meet social or religious obligations. In many instances, the payment is considered an advance against the wages the child slaves are expected to earn during their indenture. Wars and the forced migrations of large populations which disrupt the normal family structure force many children and adolescents into slavery.
Causes of child labour
Poverty is the greatest single factor responsible for the movement of children into the workplace. The survival of the family as well as the children themselves often dictates it; this is particularly the case when poor families have many children. The necessity of having them work full-time makes it impossible for families to invest in the children’s education.
Even where tuition is free, many poor families are unable to meet the ancillary costs of education (e.g., books and other school supplies, clothing and footwear, transportation and so on). In some places, these costs for one child attending a primary school may represent as much as one-third of the cash income of a typical poor family. This leaves going to work as the only alternative. In some large families, the older children will work to provide the means for educating their younger siblings.
In some areas, it is not so much the cost but the lack of schools providing an acceptable quality of education. In some communities, schools may just be unavailable. In others, children drop out because the schools serving the poor are of such abysmal quality that attendance does not seem to be worth the cost and effort involved. Thus, while many children drop out of school because they have to work, many become so discouraged that they prefer to work. As a result, they may remain totally or functionally illiterate and unable to develop the skills required for their advancement in the world of work and in society.
Finally, many large urban centres have developed an indigenous population of street children who have been orphaned or separated from their families. These scratch out a precarious existence by doing odd jobs, begging, stealing, and participating in the traffic of illegal drugs.
The demand for child labour
In most instances, children are employed because their labour is less expensive and they are less troublesome than adult workers. In Ghana, for example, an ILO-supported study showed that three-fourths of children engaged in paid work were paid less than one-sixth of the statutory minimum wage (ILO 1995). In other areas, although the differentials between the wages of children and adults were much less impressive, they were large enough to represent a very significant burden to the employers, who were usually poor, small contractors who enjoyed a very slim profit margin.
In some instances, as in the hand-woven carpet and glass bracelet (bangles) industries in India, child workers are preferred to adults because of their smaller size or the perception that their “nimble fingers” make for greater manual dexterity. An ILO study demonstrated that adults were no less competent in performing these tasks and that the child workers were not irreplaceable (Levison et al. 1995).
Parents are a major source of demand for the work of children in their own families. Huge numbers of children are unpaid workers in family farms, shops and stores that depend on family labour for their economic viability. It is conventionally assumed that these children are much less likely to be exploited than those working outside the family, but there is ample evidence that this is not always the case.
Finally, in urban areas in developed countries where the labour market is very tight, adolescents may be the only workers available and willing to take the minimum wage, mostly part-time jobs in retail establishments such as fast-food shops, retail trade and messenger services. Recently, where even these have not been available in sufficient numbers, employers have been recruiting elderly retirees for these positions.
Working conditions
In many establishments employing child labour, working conditions range from bad to abysmal. Since many of these enterprises are poor and marginal to start with, and are often operating illegally, little or no attention is paid to amenities that would be required to retain all but slave labourers. Lack of elementary sanitation, air quality, potable water and food are often compounded by crowding, harsh discipline, obsolete equipment, poor quality tools and the absence of protective measures to control exposure to occupational hazards. Even where some protective equipment may be available, it is rarely sized to fit the smaller frames of children and is often poorly maintained.
Too many children work too many hours. Dawn to dusk is not an unusual working day, and the need for rest periods and holidays is generally ignored. In addition to chronic fatigue, which is a major cause of accidents, the most damaging effect of the long hours is the inability to benefit from education. This may occur even where the children work only part-time; studies have shown that working more than 20 hours per week can negatively affect education (ILO 1995). Functional illiteracy and lack of training, in turn, lead to greatly diminished opportunities for advancing to improved employment.
Girls are particularly at risk. Because they are often also responsible for household tasks, they work longer hours than boys, who usually engage only in economic activities. As a result, they generally have lower rates of school attendance and completion.
Children are emotionally immature and need a nurturing psychological and social environment that will socialize them into their cultural environment and enable them to take their places as adults in their particular society. For many labouring children, the work environment is oppressive; in essence, they do not have a childhood.
Prevention of Injuries to Children
Child labour is not restricted to developing countries. The following set of precautions is adapted from advice put forth by the United States Centers for Disease Control and Prevention.
The risks for work-related injuries and illnesses in children, as in workers of all ages, can be reduced through adherence to routine precautions such as: prescribed housekeeping practices; training and safe work procedures; use of proper shoes, gloves and protective clothing; and maintenance and use of equipment with safety features. In addition, workers under the age of 18 should not be required to lift objects weighing more than 15 pounds (approximately 7kg) more than once per minute, or ever to lift objects weighing more than 30 pounds (14kg); tasks involving continuous lifting should never last more than 2 hours. Children under the age of 18 should not participate in work requiring the routine use of respirators as a means of preventing the inhalation of hazardous substances.
Employers should be knowledgeable about and comply with child labour laws. School counsellors and physicians who sign permits allowing children to work should be familiar with child labour laws and ensure that the work they approve does not involve prohibited activities.
Most children who begin working under the age of 18 enter the workplace with minimal prior experience for a job. Advanced industrial countries are not exempt from these hazards. For example, during the summer of 1992 in the United States, more than half (54%) of persons aged 14 to 16 years treated in emergency departments for work injuries reported that they had received no training in prevention of the injury they had sustained, and that a supervisor was present at the time of injury in only approximately 20% of the cases. Differences in maturity and developmental level regarding learning styles, judgement and behaviour should be considered when providing training for youth in occupational safety and health.
Centers for Disease Control and Prevention, 1996
Exposure to occupational hazards
In general, the risks that children face in the workplace are the same that adult workers encounter. However, their effects may be greater because of the kinds of tasks to which children are assigned and the biological differences between children and adults.
Children tend to be given more menial tasks, often without instruction and training in minimizing exposure to the hazards that may be encountered, and without proper supervision. They may be assigned to cleaning-up duties, often using solvents or strong alkalis, or they may be required to clean up hazardous wastes that have accumulated in the workplace without awareness of potential toxicity.
Because of their smaller size, children are more likely to be given tasks that require working in odd, confined places or long periods of stooping or kneeling. Often, they are required to handle objects that even adults would consider too bulky or too heavy.
Because of their continuing growth and development, children differ biologically from adults. These differences have not been quantified, but it is reasonable to assume that the more rapid cell division involved in the growth process may make them more vulnerable to many toxic agents. Exposure earlier in life to toxic agents with long latency periods may result in the onset of disabling chronic occupational diseases such as asbestosis and cancer in young adulthood rather than at older ages, and there is evidence that childhood exposure to toxic chemicals may alter the response to future toxic exposures (Weisburger et al. 1966).
Table 1 summarizes information on some of the hazardous agents to which working children may be exposed, according to the sources of exposure and the types of health consequences. It should be noted that these consequences may be aggravated when the exposed children are undernourished, anaemic or suffer from chronic diseases. Finally, the lack of primary medical care, much less the services of health professionals with some sophistication in occupational health, means that these health consequences are not likely to be recognized promptly or treated effectively.
Table 1. Some occupations and industries, and their associated hazards, where children are employed.
|
Occupation/industry |
Hazards |
|
Abattoirs and meat rendering |
Injuries from cuts, burns, falls, dangerous equipment; exposure to infectious disease; heat stress |
|
Agriculture |
Unsafe machinery; hazardous substances; accidents; chemical poisoning; arduous work; dangerous animals, insects and reptiles |
|
Alcohol production and/or sale |
Intoxication, addiction; environment may be prejudicial to morals; risk of violence |
|
Carpet-weaving |
Dust inhalation, poor lighting, poor posture (squatting); respiratory and musculoskeletal diseases; eye strain; chemical poisoning |
|
Cement |
Harmful chemicals, exposure to harmful dust; arduous work; respiratory and musculoskeletal disease |
|
Construction and/or demolition |
Exposure to heat, cold, dust; falling objects; sharp objects; accidents; musculoskeletal diseases |
|
Cranes/hoists/lifting machinery Tar, asphalt, bitumen |
Accidents; falling objects; musculoskeletal diseases; risk of injury to others Exposure to heat, burns; chemical poisoning; respiratory diseases |
|
Crystal and/or glass manufacture |
Molten glass; extreme heat; poor ventilation; cuts from broken glass; carrying hot glass; burns; respiratory disease; heat stress; toxic dust |
|
Domestic service |
Long hours; physical, emotional, sexual abuse; malnutrition; insufficient rest; isolation |
|
Electricity |
Dangerous work with high voltage; risk of falling; high level of responsibility for safety of others |
|
Entertainment (night clubs, bars, casinos, circuses, gambling halls) |
Long, late hours; sexual abuse; exploitation; prejudicial to morals |
|
Explosives (manufacture and handling) |
Risk of explosion, fire, burns, mortal danger |
|
Hospitals and work with risk of infection |
Infectious diseases; responsibility for well-being of others |
|
Lead/zinc metallurgy |
Cumulative poisoning; neurological damage |
|
Machinery in motion (operation, cleaning, repairs, etc.) |
Danger from moving engine parts; accidents; cuts, burns, exposure to heat and noise; noise stress; eye and ear injuries |
|
Maritime work (trimmers and stokers, stevedores) |
Accidents; heat, burns; falls from heights; heavy lifting, arduous work, musculoskeletal diseases; respiratory diseases |
|
Mining, quarries, underground work |
Exposure to dusts, gases, fumes, dirty conditions; respiratory and musculoskeletal diseases; accidents; falling objects; arduous work; heavy loads |
|
Rubber |
Heat, burns, chemical poisoning |
|
Street trades |
Exposure to drugs, violence, criminal activities; heavy loads; musculoskeletal diseases; venereal diseases; accidents |
|
Tanneries |
Chemical poisoning; sharp instruments; respiratory diseases |
|
Transportation, operating vehicles |
Accidents; danger to self and passengers |
|
Underwater (e.g., pearl diving) |
Decompression illness; dangerous fish; death or injury |
|
Welding and smelting of metals, metalworking |
Exposure to extreme heat; flying sparks and hot metal objects; accidents; eye injuries; heat stress |
Source: Sinclair and Trah 1991.
Social and economic consequences of child labour
Child labour is largely generated by poverty, as noted above, and child labour tends to perpetuate poverty. When child labour precludes or seriously handicaps education, lifetime earnings are reduced and upward social mobility is retarded. Work that hampers the physical, mental and social development ultimately taxes the health and welfare resources of the community and perpetuates poverty by degrading the stock of human capital needed for the economic and social development of the society. Since the societal costs of child labour are visited primarily on the population groups that already are poor and less privileged, access to democracy and social justice is eroded and social unrest is fomented.
Future trends
Although much is being done to eliminate child labour, it is clearly not enough nor is it effective enough. What is needed first is more and better information about the extent, dynamics and effects of child labour. The next step is to increase, amplify and improve educational and training opportunities for children from pre-school through universities and technical institutes, and then to provide the means for children of the poor to take advantage of them (e.g., adequate housing, nutrition and preventive health care).
Well-drafted legislation and regulations, reinforced by such international efforts as the ILO Conventions, need constantly to be revised and strengthened in the light of current developments in child labour, while the effectiveness of their enforcement should be enhanced.
The ultimate weapon may be the nurturing of greater awareness and abhorrence of child labour among the general public, which we are beginning to see in several industrialized countries (motivated in part by adult unemployment and the price competition that drives producers of consumer goods to migrate to areas where labour may be cheaper). The resultant publicity is leading to damage to the image of organizations marketing products produced by child labour, protests by their stockholders and, most important, refusal to purchase these products even though they may cost a bit less.
Conclusions
There are many forms of employment in which workers are vulnerable to impoverishment, exploitation and abuse, and where their safety, health and well-being are at great risk. Despite attempts at legislation and regulation, and notwithstanding their condemnation in international agreements, Conventions, and resolutions, such conditions are likely to persist as long as people are poor, ill-housed, malnourished and oppressed, and are denied the information, education and training and the curative and preventive health services required to enable them to extricate themselves from the social quicksand in which they exist. Wealthy people and nations often respond magnanimously to such natural disasters as storms, floods, fires, volcanic eruptions and earthquakes but, important as they are, the benefits of such help are short-lived. What is needed is a long-term application of human effort fortified by the needed resources that will overcome the political, racial and religious barriers that would thwart its thrust.
Finally, while it is entirely appropriate and healthy for children to work as part of normal development and family life, child labour as described in this article is a scourge that not only damages the health and well-being of the child workers but, in the long run, also impairs the social and economic security of communities and nations. It must be attacked with vigour and persistence until it is eradicated.
Health, Safety and Equity in the Workplace
Occupational health policies often co-exist with policies to ensure equity in the workplace. Laws, regulations, and standards adopted or endorsed in many countries prohibit various forms of workplace discrimination and require safety and health goals to be achieved in ways that do not infringe workers’ other rights and interests. Legal obligations compel employers in some jurisdictions to implement practices that ensure workplace equity; policy considerations may encourage similar practices even when they are not legally mandated, for the reasons set forth by Freda Paltiel at the beginning of this chapter.
As a practical matter, workers’ acceptance of health and safety programmes may be affected by the extent to which they incorporate and reflect equitable principles. Workers are more likely to reject occupational safety and health programmes if they are implemented at the expense of other important interests, such as the interest in self-determination and economic security. There are additional reasons to implement health and safety programmes with attention to workplace equity. Rational and fair workplace rules improve workers’ job satisfaction, productivity and emotional well-being, and reduce work-related stress. An individualized approach to workers’ needs and abilities, which is at the core of both occupational safety and health and workplace equity, expands the pool of qualified workers and maximizes their skills and abilities.
There are certain areas in which equitable principles and occupational safety and health seem to conflict, and these tend to be situations in which certain workers appear to have unique or special needs. Pregnant workers, older workers, and disabled workers fall into these categories. Closer inspection often reveals that the needs of these workers are not so dissimilar to those of workers generally, and that well-accepted workplace policies and practices can ordinarily be adapted to create programmes that implement health and safety and equity in tandem. The guiding principle is the flexibility to make individual assessments and adjustments, which is a familiar reality in most work settings, since illness, temporary disability, and work restrictions often require flexibility and adaptation. At some point in their working lives, almost all workers have occupational health needs related to “age, physiological condition, social aspects, communication barriers or similar factors (which) should be met on an individual basis” (ILO 1992).
General Principles
Workplace equity connotes fairness in the allocation of jobs, duties, promotion, benefits, and other terms and conditions of employment. Employment-related distinctions on the basis of race, sex, national origin and religion, in particular, have been recognized as perpetuating invidious forms of social bias and discrimination, and have been almost universally condemned. More recently, distinctions drawn on the basis of age and disability have come to be recognized as similarly inequitable. These characteristics are generally irrelevant to an individual’s desire to work, financial need for employment, and are often irrelevant to the ability to perform a job. Failure to integrate all able and willing individuals into productive activity not only stymies human potential but also defeats social needs by reducing the population of self-sufficient individuals.
Principles of equity rely on the premise that workers should be judged on the basis of an objective assessment of their own skills, abilities and characteristics, not on assumptions about any group to which they belong. Thus, at the core of workplace equity is the repudiation of stereotypes and generalizations to judge individuals, since even accurate generalizations often inaccurately describe many individuals. For example, even if it is true on average that men are stronger than women, some women are stronger than some men. In hiring workers to perform a job requiring strength, it would be inequitable to exclude all women, including those who are strong enough to do the job, on the basis of a generalization about the sexes. Instead, a fair assessment of individual abilities will reveal which women and men have the requisite strength and ability to perform the job adequately.
Some kinds of screening tests disproportionately exclude members of certain groups. Written tests may disadvantage individuals whose native language is different or who have had less access to educational opportunities. Such tests are justifiable if they actually measure the abilities that are needed to perform the job in question. Otherwise, they operate to bar qualified individuals and reduce the pool of eligible workers. Reliance on certain kinds of screening devices also reflects stereotypes about who should do particular types of work. For example, height requirements imposed for law enforcement jobs assumed that greater height correlated with successful job performance. Elimination of these requirements has demonstrated that height per se is not a necessary element of the ability to function effectively in law enforcement, and it has opened this field to more women and members of certain ethnic groups.
The classic barriers to workplace equity include physical requirements such as height and weight, written tests, and education or diploma requirements. Seniority systems sometimes exclude members of groups that have been disfavoured, and veterans’ preferences often disadvantage women workers, who are often neither required nor permitted to do military service. Stereotypes, traditions and assumptions about skills and characteristics associated with race, sex and ethnicity also operate, often subconsciously, to perpetuate a traditional allocation of employment opportunities, as do other factors, such as preferences for friends or relatives. The presence of such barriers is often signified by a work environment that does not accurately reflect the composition of the pool of qualified workers, but shows members of certain groups holding a greater share of desired positions than would be expected based on their representation in the field or labour pool. In such cases, careful evaluation of the practices by which workers are chosen usually reveals either reliance on screening practices that unfairly eliminate certain qualified applicants, or unconscious bias, stereotyping or favouritism.
Notwithstanding almost universal adherence to workplace equity principles and the desire to implement equitable practices, these goals are sometimes confounded, ironically, by the view that they conflict with occupational safety and health goals. The area in which this issue is most prominent relates to women of childbearing capacity, pregnant women and new mothers. Unlike other workers who ordinarily enjoy the right to undertake any work for which they are qualified, women workers are often subject to involuntary restrictions in the name of health protection either for themselves or their children. Sometimes these provisions secure much-needed benefits, and sometimes they exact a high price in terms of access to economic independence and personal autonomy.
Many of the principles relevant to the consideration of women workers’ rights and needs apply to workers who are disabled or ageing. Most important is the notion that workers should be judged on the basis of their own skills and abilities, not on the basis of generalizations or stereotypes. This principle has resulted in recognition of the fact that disabled individuals can be highly productive and valuable workers. Some investment may be necessary to accommodate a disabled worker’s needs, but there is growing appreciation that such investment is well worth the cost, especially in light of the consequences of the alternative course.
Sex Discrimination, Pregnancy and Childbirth
Many international conventions and recommendations advocate the elimination of sex discrimination in employment, for example, the International Convention on the Elimination of All Forms of Discrimination Against Women (1979), the International Covenant on Civil and Political Rights (1976), and the Equal Treatment Directive (76/207/EEC). The concept of equal pay for male and female workers doing work of equal value was adopted by the ILO in the Convention Concerning Equal Remuneration for Men and Women Workers for Work of Equal Value, 1951 (No. 100). The Recommendation Concerning Equal Remuneration for Men and Women Workers for Work of Equal Value, 1951 (No. 90), which supplemented that Convention, also urged “promoting equality of men and women workers as regards access to occupations and posts”. A more comprehensive statement of the non-discrimination principle was adopted in June 1958 in the Convention Concerning Discrimination in Respect of Employment and Occupation (No. 111) and the Recommendation Concerning Discrimination in Respect of Employment and Occupation (No. 111).
The European Community Directive 76/207/EEC on equal treatment of women and men with respect to access to employment is consistent with these provisions. There is thus widespread agreement with the principle that women and men should enjoy equal access to employment opportunities and equality in the terms and conditions of employment. For example, Austria has amended its Equal Opportunities Act to place Austrian law in line with European Community Law. The Austrian amendments stipulate that there may be no discrimination in connection with an employment relationship on grounds of gender. This extends the prohibition of discrimination to all aspects of the employment relationship.
Long before international bodies and national laws condemned sex discrimination, many recognized a need for maternity protection. The Maternity Protection Convention which was first adopted in 1919, gave pregnant women with a medical certificate the right to a leave six weeks before the expected date of delivery, and prohibited a woman from working “during the six weeks following her confinement”. Pregnant women were required to receive breaks during work hours. (ILO 1994). The Convention also entitled women workers to free medical care and cash benefits. The dismissal of a woman during maternity leave or during an illness arising out of pregnancy or confinement was “unlawful”. The revised Maternity Protection Convention, 1952 (No. 103), provided that maternity leave be extended to 14 weeks where necessary for the health of the mother, expanded the provisions for nursing mothers, and prohibited night work and overtime for pregnant and nursing mothers. It also stated that work that could be harmful to a pregnant or nursing mother’s health, such as any hard labour or work requiring special equilibrium, should be prohibited. Notably, Member States were allowed to make exceptions for women who fell into certain occupational categories, such as non-industrial occupations, domestic work in private households, and labour involving the transport of goods or passengers by sea.
Consistent with ILO Conventions on maternity protection, the European Community adopted Council Directive 92/85/EEC of 19 October 1992, to encourage improvements in the safety and health of pregnant workers and workers who have recently given birth or are breast-feeding. This calls for the evaluation and communication of types of activityies which may pose specific risks to pregnant and nursing women, prohibition of the requirement of night work when necessary for the health and safety of pregnant and nursing workers, the right to maternity leave, and the maintenance of the rights of the employment contract during pregnancy and confinement. While these Conventions and Directives contain provisions that enhance the ability of women to work and bear children safely, they have been criticized for failing to guarantee that result. For example, studies done by the Indian Government found that few women received maternity benefits as a result of poor enforcement and the exclusion from coverage of temporary and seasonal workers, women working in small industries, and homebased workers (Vaidya 1993). In addition to maternity benefits, some countries require that women receive rest breaks, seats, sanitary facilities and other benefits.
In contrast, other measures adopted to protect women workers’ health include limitations on women’s work. These take the form of exclusion from dangerous jobs or heavy work, restriction from jobs thought to pose a moral danger, restrictions during menstruation, maximum hours and overtime prohibitions and so on (ILO 1989). Unlike maternity benefits provisions, these actions are restrictive: that is, they limit women’s access to certain kinds of jobs. One example is the prohibition of night work by women, which was one of the first items addressed at the International Labour Conference in 1919. Four ILO documents provide further discussion of these issues (ILO 1919a; 1921; 1934; 1948). (It is interesting to note that there is no standard definition of the word night.) The history of attitudes towards night-work restrictions provides an instructive study in the relationship between health and safety goals and workplace equity.
The prohibition of night work was meant to protect family life and to protect workers against the particularly arduous physical burden of night work. In practice, the ILO Conventions are meant to prohibit night work by women doing manual work in industry, but not to prohibit white-collar or managerial work or work in service sectors. But night-work restrictions also denied women job opportunities. In the name of health and morality, women were restricted from some jobs altogether and limited in their ability to progress in other jobs. The impulse to legislate restrictions on night-work was in response to the exploitation of workers of both sexes, who were required to work exceedingly long hours. However, in the United States, for example, night- work restrictions prevented women from obtaining lucrative jobs as streetcar conductors. Restrictions did not, however, bar women from working as nightclub dancers (Kessler-Harris 1982).
Inconsistencies of this sort, along with the economic disadvantage experienced by women workers, fuelled criticism of night-work restrictions for women, which were ultimately replaced in the United States by legal protections against exploitation for workers of both sexes. The US Fair Labor Standards Act provided for the establishment of regulations regarding hours of work.
Other countries have likewise rejected the sex-specific approach to protecting working women, responding to increasing awareness of the economic penalties on women workers and other aspects of sex discrimination. In 1991, the Court of Justice of the EEC held that under European Community Directive 76/207/EEC, Member States may not statutorily ban night work for women. The European Commission requested that ILO Member States bound to the ILO Convention banning night work for women renounce it, and many have done so. In 1992, the German Constitutional Court declared the prohibition of night work for women to be unconstitutional. Within the last ten years, laws prohibiting night work by women have been repealed in Barbados, Canada, Guyana, Ireland, Israel, New Zealand, Spain and Surinam. Currently, the law in 20 countries contains no prohibition on night work by women. A summary of the actions repealing protective laws prior to 1989 has been published by the ILO (1989b).
This trend is most pronounced in developed countries where women have enforceable rights protecting their legal status and where occupational health and safety concerns are recognized. In countries where conditions for women are “deplorable” and are much worse than they are for men, however, it is sometimes argued that “more protection is needed, not less” (ILO 1989b). For example, the average number of hours women in Kenya work per week, 50.9, greatly exceeds the average number of hours worked per week by men, 33.2 (Waga 1992). Notwithstanding this caveat, in general protecting women workers by restricting their ability to work has clear disadvantages. In June 1990, the ILO passed the Night Work Convention (No. 171) stating that all night workers, not just those who are female, need protection (ILO 1990). This approach is consistent with the ILO’s general position that all “work should take place in a safe and healthy working environment” (ILO 1989) and is an approach which accords health protection and workplace equity equivalent respect.
The evolution of efforts to protect women from the effects of hazardous workplaces and toxic substances at work demonstrates some of the same concerns and trends that appear in the discussion of night work. Early in the twentieth century, the ILO and many countries barred women from dangerous workplaces, as illustrated by Conventions prohibiting women and children from exposure to lead (ILO 1919b). By custom and by law, women were barred from many kinds of work, ranging from bar tending to mining. These restrictions undermined women’s employment options and economic status, and were implemented inconsistently—barring women from lucrative jobs held exclusively by men, while permitting work in equally hazardous, but low-paid, jobs frequented by women. Critics charged that all workers need protection from toxic chemicals.
In the United States, the effort to exclude women from hazardous work took the form of “foetal protection” policies. Proponents claimed that the foetus is more sensitive to certain workplace hazards and that it is therefore rational to exclude women who are or might be pregnant from such environments. The United States Supreme Court rejected that claim and held that occupational safety and health practices must account for the health needs of both women and men. The Court’s decision vigorously enforces women’s right to employment, while recognizing the equally important right to health protection. On a theoretical level, this solution accords equal weight and respect to equity and safety and health goals and obligations. As a practical matter, some have expressed concern whether the absence of adequate mechanisms to enforce occupational safety and health laws leaves both sexes vulnerable to reproductive and other injuries (International Union 1991).
Other countries have sought a different solution. For example, Finland’s Act on the Special Maternity Leave, which came into force in July 1991, allows women who are exposed to agents considered to be harmful to the pregnancy or to the offspring, to request a transfer to a different job which does not involve such exposure from the beginning of their pregnancy. If such a job is not available to them, they may be entitled to special maternity leave and benefits (Taskinen 1993). Similarly, the Pregnant Workers Directive (92/85/EEC) contemplates a series of accommodations to women who require additional protection for pregnancy or breast-feeding, including modifications of the work environment or conditions of work, temporary transfer, and leave of absence.
This approach, like the one discussed above, solves some, but not all, problems: the different level of benefits accorded to women may make them less desirable and more expensive employees and may encourage sex discrimination; and the failure to accord male workers protection against reproductive risks may result in future illness and injury.
Provisions that accord women the right to request transfers, modification of work conditions, and other accommodations point up the importance of how rights and obligations are allocated between workers and employers: the workers’ right to request certain benefits, which the employer is required to provide on request, accords with principles of equity, while rules which permit employers to impose unwanted restrictions on workers, even if “for their own good”, do not. Allowing employers to control the conditions of women’s work, as opposed to men’s work, would deprive women, as a class, of decision-making power and personal autonomy, and would also violate basic concepts of equity. The notion that workers retain control over health-related decisions, even though employers are required to observe certain standards and provide benefits, is already recognized in the context of biological monitoring (ILO 1985) and is equally applicable to address the health needs of women and other identifiable sub-groups of workers.
As the foregoing discussion indicates, efforts to protect women workers as a separate group, through benefits not available to other workers, have had mixed success. Some women have undoubtedly benefited, but not all. Poor enforcement, especially in the case of maternity benefit laws, has limited their intended beneficial effect. Limits on the employability of women workers themselves, as in the case of night-work restrictions, impose economic and other penalties on women workers themselves by restricting their options, opportunities and contributions.
At the same time, other factors have forced re-evaluation of the best ways to meet workers’ needs for health protection. Entry of more women into all parts of the workforce has exposed more women to the full range of occupational risks previously experienced only by men, while increasing knowledge of male susceptibility to reproductive and other injury from occupational exposures reveals the need for comprehensive health policies. Other trends also influence the direction of all employment-related policies. These include not just the demand for equality between the sexes, but also the fact that more women work, work longer, and in more kinds of jobs. As a result, the recent trend is to allow men and women more choices concerning all aspects of family and employment: more men have elected to participate in the care of young children, more women are principal wage-earners, and more workers of both sexes seek greater flexibility in managing their work and family lives. These factors contribute to a trend to provide benefits to both men and women to accommodate a range of predictable needs associated with family welfare, including reproductive health concerns, pregnancy, temporary disability, childbirth and child care and elder care. For example, the Workers With Family Responsibilities Convention, 1981 (No. 156), applies equally to both men and women. In addition, France, Germany, Belgium, Denmark and Greece permit some form of parental leave to address a range of family needs. The benefits for men still do not equal the maternity benefits received by women, however (Dumon 1990). Instead of excluding workers thought to be susceptible to the effects of toxins, some reproductive toxins have been banned altogether and others have been strictly regulated to prevent reproductive harm by reducing exposures to both sexes. Transfer options for men and women exposed to reproductive hazards at work have been adopted in several countries, such as in the United States for workers exposed to lead. A number of countries have adopted parental leave benefits that allow parents greater freedom in caring for young children.
Conclusion
The examples drawn from the historical and current experiences of women workers demonstrate principles that apply with equal force to the situation of many disabled and older workers. Like women, these workers have sometimes been protected from employment-related risks in ways that have deprived them of economic self-sufficiency and the other rewards of work. Restricting the choices of these workers suggests that they are incapable of making appropriate decisions about the risks and benefits of work. All three groups have been burdened with negative assumptions about their abilities, and often denied the opportunity to demonstrate their skills. And there has been a tendency to view accommodation of these workers as especially burdensome, even though it may be routine to accommodate a worker injured in a traffic accident or an executive who has had a heart attack.
Equity is served when workplace policies are established to meet the needs of all workers. This principle is essential to address situations in which members of identifiable ethnic or racial groups are thought to be especially susceptible to certain work-related risks. Such claims must be carefully scrutinized to ensure their validity; they have sometimes been advanced without foundation and used to justify exclusion of affected workers, even though individual variation in susceptibility is usually more important than group-based differences (Bingham 1986). Even if true, however, equitable principles suggest that the risk should be reduced or avoided through engineering controls, product substitution, or other means, rather than by depriving an entire class of individuals of employment opportunities or subjecting them to conditions that are known to pose a hazard.
Ideally, workers’ abilities and needs should be assessed individually, and individual needs accommodated to the extent possible. Risk-benefit calculations are ordinarily best performed by the individuals most directly affected. The possibility that workers will sacrifice their health for their economic well-being can be reduced if government standards are established with the expectation that the workplace will contain a representative sample of the population, including pregnant women, older workers, those who are disabled, and members of different racial and ethnic groups. Certain events in life are highly predictable: procreation and ageing affect a large proportion of the working population, disability affects significant numbers, and everyone belongs to some racial or ethnic sub-group. Work-related policies that treat these circumstances as normal, and that anticipate them, create workplace environments in which equity, and health and safety, can co-exist comfortably.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."