- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Ergonomic Aspects of Human-Computer Interaction
Introduction
The development of effective interfaces to computer systems is the fundamental objective of research on human-computer interactions.
An interface can be defined as the sum of the hardware and software components through which a system is operated and users informed of its status. The hardware components include data entry and pointing devices (e.g., keyboards, mice), information-presentation devices (e.g., screens, loudspeakers), and user manuals and documentation. The software components include menu commands, icons, windows, information feedback, navigation systems and messages and so on. An interface’s hardware and software components may be so closely linked as to be inseparable (e.g., function keys on keyboards). The interface includes everything the user perceives, understands and manipulates while interacting with the computer (Moran 1981). It is therefore a crucial determinant of the human-machine relation.
Research on interfaces aims at improving interface utility, accessibility, performance and safety, and usability. For these purposes, utility is defined with reference to the task to be performed. A useful system contains the necessary functions for the completion of tasks users are asked to perform (e.g., writing, drawing, calculations, programming). Accessibility is a measure of an interface’s ability to allow several categories of users—particularly individuals with handicaps, and those working in geographically isolated areas, in constant movement or having both hands occupied—to use the system to perform their activities. Performance, considered here from a human rather than a technical viewpoint, is a measure of the degree to which a system improves the efficiency with which users perform their work. This includes the effect of macros, menu short-cuts and intelligent software agents. The safety of a system is defined by the extent to which an interface allows users to perform their work free from the risk of human, equipment, data, or environmental accidents or losses. Finally, usability is defined as the ease with which a system is learned and used. By extension, it also includes system utility and performance, defined above.
Elements of Interface Design
Since the invention of shared-time operating systems in 1963, and especially since the arrival of the microcomputer in 1978, the development of human-computer interfaces has been explosive (see Gaines and Shaw 1986 for a history). The stimulus for this development has been essentially driven by three factors acting simultaneously:
First, the very rapid evolution of computer technology, a result of advances in electrical engineering, physics and computer science, has been a major determinant of user interface development. It has resulted in the appearance of computers of ever-increasing power and speed, with high memory capacities, high-resolution graphics screens, and more natural pointing devices allowing direct manipulation (e.g., mice, trackballs). These technologies were also responsible for the emergence of microcomputing. They were the basis for the character-based interfaces of the 1960s and 1970s, graphical interfaces of the late 1970s, and multi- and hyper-media interfaces appearing since the mid-1980s based on virtual environments or using a variety of alternate-input recognition technologies (e.g., voice-, handwriting-, and movement-detection). Considerable research and development has been conducted in recent years in these areas (Waterworth and Chignel 1989; Rheingold 1991). Concomitant with these advances was the development of more advanced software tools for interface design (e.g., windowing systems, graphical object libraries, prototyping systems) that greatly reduce the time required to develop interfaces.
Second, users of computer systems play a large role in the development of effective interfaces. There are three reasons for this. First, current users are not engineers or scientists, in contrast to users of the first computers. They therefore demand systems that can be easily learned and used. Second, the age, sex, language, culture, training, experience, skill, motivation and interest of individual users is quite varied. Interfaces must therefore be more flexible and better able to adapt to a range of needs and expectations. Finally, users are employed in a variety of economic sectors and perform a quite diverse spectrum of tasks. Interface developers must therefore constantly reassess the quality of their interfaces.
Lastly, intense market competition and increased safety expectations favour the development of better interfaces. These preoccupations are driven by two sets of partners: on the one hand, software producers who strive to reduce their costs while maintaining product distinctiveness that furthers their marketing goals, and on the other, users for whom the software is a means of offering competitive products and services to clients. For both groups, effective interfaces offer a number of advantages:
For software producers:
- better product image
- increased demand for products
- shorter training times
- lower after-sales service requirements
- solid base upon which to develop a product line
- reduction of the risk of errors and accidents
- reduction of documentation.
For users:
- shorter learning phase
- increased general applicability of skills
- improved use of the system
- increased autonomy using the system
- reduction of the time needed to execute a task
- reduction in the number of errors
- increased satisfaction.
Effective interfaces can significantly improve the health and productivity of users at the same time as they improve the quality and reduce the cost of their training. This, however, requires basing interface design and evaluation on ergonomic principles and practice standards, be they guidelines, corporate standards of major system manufacturers or international standards. Over the years, an impressive body of ergonomic principles and guidelines related to interface design has accumulated (Scapin 1986; Smith and Mosier 1986; Marshall, Nelson and Gardiner 1987; Brown 1988). This multidisciplinary corpus covers all aspects of character-mode and graphical interfaces, as well as interface evaluation criteria. Although its concrete application occasionally poses some problems—for example, imprecise terminology, inadequate information on usage conditions, inappropriate presentation—it remains a valuable resource for interface design and evaluation.
In addition, the major software manufacturers have developed their own guidelines and internal standards for interface design. These guidelines are available in the following documents:
- Apple Human Interface Guidelines (1987)
- Open Look (Sun 1990)
- OSF/Motif Style Guide (1990)
- IBM Common User Access guide to user interface design (1991)
- IBM Advanced Interface Design Reference (1991)
- The Windows interface: An application design guide (Microsoft 1992)
These guidelines attempt to simplify interface development by mandating a minimal level of uniformity and consistency between interfaces used on the same computer platform. They are precise, detailed, and quite comprehensive in several respects, and offer the additional advantages of being well-known, accessible and widely used. They are the de facto design standards used by developers, and are, for this reason, indispensable.
Furthermore, the International Organization for Standardization (ISO) standards are also very valuable sources of information about interface design and evaluation. These standards are primarily concerned with ensuring uniformity across interfaces, regardless of platforms and applications. They have been developed in collaboration with national standardization agencies, and after extensive discussion with researchers, developers and manufacturers. The main ISO interface design standard is ISO 9241, which describes ergonomic requirements for visual display units. It is comprised of 17 parts. For example, parts 14, 15, 16 and 17 discuss four types of human-computer dialogue—menus, command languages, direct manipulation, and forms. ISO standards should take priority over other design principles and guidelines. The following sections discuss the principles which should condition interface design.
A Design Philosophy Focused on the User
Gould and Lewis (1983) have proposed a design philosophy focused on the video display unit user. Its four principles are:
- Immediate and continuous attention to users. Direct contact with users is maintained, in order to better understand their characteristics and tasks.
- Integrated design. All aspects of usability (e.g., interface, manuals, help systems) are developed in parallel and placed under centralized control.
- Immediate and continuous evaluation by users. Users test the interfaces or prototypes early on in the design phase, under simulated work conditions. Performance and reactions are measured quantitatively and qualitatively.
- Iterative design. The system is modified on the basis of the results of the evaluation, and the evaluation cycle started again.
These principles are explained in further detail in Gould (1988). Very relevant when they were first published in 1985, fifteen years later they remain so, due to the inability to predict the effectiveness of interfaces in the absence of user testing. These principles constitute the heart of user-based development cycles proposed by several authors in recent years (Gould 1988; Mantei and Teorey 1989; Mayhew 1992; Nielsen 1992; Robert and Fiset 1992).
The rest of this article will analyse five stages in the development cycle that appear to determine the effectiveness of the final interface.
Task Analysis
Ergonomic task analysis is one of the pillars of interface design. Essentially, it is the process by which user responsibilities and activities are elucidated. This in turn allows interfaces compatible with the characteristics of users’ tasks to be designed. There are two facets to any given task:
- The nominal task, corresponding to the organization’s formal definition of the task. This includes objectives, procedures, quality control, standards and tools.
- The real task, corresponding to the users’ decisions and behaviours necessary for the execution of the nominal task.
The gap between nominal and real tasks is inevitable and results from the failure of nominal tasks to take into account variations and unforeseen circumstances in the work flow, and differences in users’ mental representations of their work. Analysis of the nominal task is insufficient for a full understanding of users’ activities.
Activity analysis examines elements such as work objectives, the type of operations performed, their temporal organization (sequential, parallel) and frequency, the operational modes relied upon, decisions, sources of difficulty, errors and recovery modes. This analysis reveals the different operations performed to accomplish the task (detection, searching, reading, comparing, evaluating, deciding, estimating, anticipating), the entities manipulated (e.g., in process control, temperature, pressure, flow-rate, volume) and the relation between operators and entities. The context in which the task is executed conditions these relations. These data are essential for the definition and organization of the future system’s features.
At its most basic, task analysis is composed of data collection, compilation and analysis. It may be performed before, during or after computerization of the task. In all cases, it provides essential guidelines for interface design and evaluation. Task analysis is always concerned with the real task, although it may also study future tasks through simulation or prototype testing. When performed prior to computerization, it studies “external tasks” (i.e., tasks external to the computer) performed with the existing work tools (Moran 1983). This type of analysis is useful even when computerization is expected to result in major modification of the task, since it elucidates the nature and logic of the task, work procedures, terminology, operators and tasks, work tools and sources of difficulty. In so doing, it provides the data necessary for task optimization and computerization.
Task analysis performed during task computerization focuses on “internal tasks”, as performed and represented by the computer system. System prototypes are used to collect data at this stage. The focus is on the same points examined in the previous stage, but from the point of view of the computerization process.
Following task computerization, task analysis also studies internal tasks, but analysis now focuses on the final computer system. This type of analysis is often performed to evaluate existing interfaces or as part of the design of new ones.
Hierarchical task analysis is a common method in cognitive ergonomics that has proven very useful in a wide variety of fields, including interface design (Shepherd 1989). It consists of the division of tasks (or main objectives) into sub-tasks, each of which can be further subdivided, until the required level of detail is attained. If data is collected directly from users (e.g., through interviews, vocalization), hierarchical division can provide a portrait of users’ mental mapping of a task. The results of the analysis can be represented by a tree diagram or table, each format having its advantages and disadvantages.
User Analysis
The other pillar of interface design is the analysis of user characteristics. The characteristics of interest may relate to user age, sex, language, culture, training, technical or computer-related knowledge, skills or motivation. Variations in these individual factors are responsible for differences within and between groups of users. One of the key tenets of interface design is therefore that there is no such thing as the average user. Instead, different groups of users should be identified and their characteristics understood. Representatives of each group should be encouraged to participate in the interface design and evaluation processes.
On the other hand, techniques from psychology, ergonomics and cognitive engineering can be used to reveal information on user characteristics related to perception, memory, cognitive mapping, decision-making and learning (Wickens 1992). It is clear that the only way to develop interfaces that are truly compatible with users is to take into account the effect of differences in these factors on user capacities, limits and ways of operating.
Ergonomic studies of interfaces have focused almost exclusively on users’ perceptual, cognitive and motor skills, rather than on affective, social or attitudinal factors, although work in the latter fields has become more popular in recent years. (For an integrated view of humans as information-processing systems see Rasmussen 1986; for a review of user-related factors to consider when designing interfaces see Thimbleby 1990 and Mayhew 1992). The following paragraphs review the four main user-related characteristics that should be taken into account during interface design.
Mental representation
The mental models users construct of the systems they use reflect the manner in which they receive and understand these systems. These models therefore vary as a function of users’ knowledge and experience (Hutchins 1989). In order to minimize the learning curve and facilitate system use, the conceptual model upon which a system is based should be similar to users’ mental representation of it. It should be recognized however that these two models are never identical. The mental model is characterized by the very fact that it is personal (Rich 1983), incomplete, variable from one part of the system to another, possibly in error on some points and in constant evolution. It plays a minor role in routine tasks but a major one in non-routine ones and during diagnosis of problems (Young 1981). In the latter cases, users will perform poorly in the absence of an adequate mental model. The challenge for interface designers is to design systems whose interaction with users will induce the latter to form mental models similar to the system’s conceptual model.
Learning
Analogy plays a large role in user learning (Rumelhart and Norman 1983). For this reason, the use of appropriate analogies or metaphors in the interface facilitates learning, by maximizing the transfer of knowledge from known situations or systems. Analogies and metaphors play a role in many parts of the interface, including the names of commands and menus, symbols, icons, codes (e.g., shape, colour) and messages. When pertinent, they greatly contribute to rendering interfaces natural and more transparent to users. On the other hand, when they are irrelevant, they can hinder users (Halasz and Moran 1982). To date, the two metaphors used in graphical interfaces are the desktop and, to a lesser extent, the room.
Users generally prefer to learn new software by using it immediately rather than by reading or taking a course—they prefer action-based learning in which they are cognitively active. This type of learning does, however, present a few problems for users (Carroll and Rosson 1988; Robert 1989). It demands an interface structure which is compatible, transparent, consistent, flexible, natural-appearing and fault tolerant, and a feature set which ensures usability, feedback, help systems, navigational aides and error handling (in this context, “errors” refer to actions that users wish to undo). Effective interfaces give users some autonomy during exploration.
Developing knowledge
User knowledge develops with increasing experience, but tends to plateau rapidly. This means that interfaces must be flexible and capable of responding simultaneously to the needs of users with different levels of knowledge. Ideally, they should also be context sensitive and provide personalized help. The EdCoach system, developed by Desmarais, Giroux and Larochelle (1993) is such an interface. Classification of users into beginner, intermediate and expert categories is inadequate for the purpose of interface design, since these definitions are too static and do not account for individual variations. Information technology capable of responding to the needs of different types of users is now available, albeit at the research, rather than commercial, level (Egan 1988). The current rage for performance-support systems suggests intense development of these systems in coming years.
Unavoidable errors
Finally, it should be recognized that users make mistakes when using systems, regardless of their skill level or the quality of the system. A recent German study by Broadbeck et al. (1993) revealed that at least 10% of the time spent by white-collar workers working on computers is related to error management. One of the causes of errors is users’ reliance on correction rather than prevention strategies (Reed 1982). Users prefer acting rapidly and incurring errors that they must subsequently correct, to working more slowly and avoiding errors. It is essential that these considerations be taken into account when designing human-computer interfaces. In addition, systems should be fault tolerant and should incorporate effective error management (Lewis and Norman 1986).
Needs Analysis
Needs analysis is an explicit part of Robert and Fiset’s development cycle (1992), it corresponds to Nielsen’s functional analysis and is integrated into other stages (task, user or needs analysis) described by other authors. It consists of the identification, analysis and organization of all the needs that the computer system can satisfy. Identification of features to be added to the system occurs during this process. Task and user analysis, presented above, should help define many of the needs, but may prove inadequate for the definition of new needs resulting from the introduction of new technologies or new regulations (e.g., safety). Needs analysis fills this void.
Needs analysis is performed in the same way as functional analysis of products. It requires the participation of a group of people interested by the product and possessing complementary training, occupations or work experience. This can include future users of the system, supervisors, domain experts and, as required, specialists in training, work organization and safety. Review of the scientific and technical literature in the relevant field of application may also be performed, in order to establish the current state of the art. Competitive systems used in similar or related fields can also be studied. The different needs identified by this analysis are then classified, weighted and presented in a format appropriate for use throughout the development cycle.
Prototyping
Prototyping is part of the development cycle of most interfaces and consists of the production of a preliminary paper or electronic model (or prototype) of the interface. Several books on the role of prototyping in human-computer interaction are available (Wilson and Rosenberg 1988; Hartson and Smith 1991; Preece et al. 1994).
Prototyping is almost indispensable because:
- Users have difficulty evaluating interfaces on the basis of functional specifications—the description of the interface is too distant from the real interface, and evaluation too abstract. Prototypes are useful because they allow users to see and use the interface and directly evaluate its usefulness and usability.
- It is practically impossible to construct an adequate interface on the first try. Interfaces must be tested by users and modified, often repeatedly. To overcome this problem, paper or interactive prototypes that can be tested, modified or rejected are produced and refined until a satisfactory version is obtained. This process is considerably less expensive than working on real interfaces.
From the point of view of the development team, prototyping has several advantages. Prototypes allow the integration and visualization of interface elements early on in the design cycle, rapid identification of detailed problems, production of a concrete and common object of discussion in the development team and during discussions with clients, and simple illustration of alternative solutions for the purposes of comparison and internal evaluation of the interface. The most important advantage is, however, the possibility of having users evaluate prototypes.
Inexpensive and very powerful software tools for the production of prototypes are commercially available for a variety of platforms, including microcomputers (e.g., Visual Basic and Visual C++ (™Microsoft Corp.), UIM/X (™Visual Edge Software), HyperCard (™Apple Computer), SVT (™SVT Soft Inc.)). Readily available and relatively easy to learn, they are becoming widespread among system developers and evaluators.
The integration of prototyping completely changed the interface development process. Given the rapidity and flexibility with which prototypes can be produced, developers now tend to reduce their initial analyses of task, users and needs, and compensate for these analytical deficiencies by adopting longer evaluation cycles. This assumes that usability testing will identify problems and that it is more economical to prolong evaluation than to spend time on preliminary analysis.
Evaluation of Interfaces
User evaluation of interfaces is an indispensable and effective way to improve interfaces’ usefulness and usability (Nielsen 1993). The interface is almost always evaluated in electronic form, although paper prototypes may also be tested. Evaluation is an iterative process and is part of the prototype evaluation-modification cycle which continues until the interface is judged acceptable. Several cycles of evaluation may be necessary. Evaluation may be performed in the workplace or in usability laboratories (see the special edition of Behaviour and Information Technology (1994) for a description of several usability laboratories).
Some interface evaluation methods do not involve users; they may be used as a complement to user evaluation (Karat 1988; Nielsen 1993; Nielsen and Mack 1994). A relatively common example of such methods consists of the use of criteria such as compatibility, consistency, visual clarity, explicit control, flexibility, mental workload, quality of feedback, quality of help and error handling systems. For a detailed definition of these criteria, see Bastien and Scapin (1993); they also form the basis of an ergonomic questionnaire on interfaces (Shneiderman 1987; Ravden and Johnson 1989).
Following evaluation, solutions must be found to problems that have been identified, modifications discussed and implemented, and decisions made concerning whether a new prototype is necessary.
Conclusion
This discussion of interface development has highlighted the major stakes and broad trends in the field of human-computer interaction. In summary, (a) task, user, and needs analysis play an essential role in understanding system requirements and, by extension, necessary interface features; and (b) prototyping and user evaluation are indispensable for the determination of interface usability. An impressive body of knowledge, composed of principles, guidelines and design standards, exists on human-computer interactions. Nevertheless, it is currently impossible to produce an adequate interface on the first try. This constitutes a major challenge for the coming years. More explicit, direct and formal links must be established between analysis (task, users, needs, context) and interface design. Means must also be developed to apply current ergonomic knowledge more directly and more simply to the design of interfaces.
Psychosocial Aspects of VDU Work
Introduction
Computers provide efficiency, competitive advantages and the ability to carry out work processes that would not be possible without their use. Areas such as manufacturing process control, inventory management, records management, complex systems control and office automation have all benefited from automation. Computerization requires substantial infrastructure support in order to function properly. In addition to architectural and electrical changes needed to accommodate the machines themselves, the introduction of computerization requires changes in employee knowledge and skills, and application of new methods of managing work. The demands placed on jobs which use computers can be very different from those of traditional jobs. Often computerized jobs are more sedentary and may require more thinking and mental attention to tasks, while at the same time require less physical energy expenditure. Production demands can be high, with constant work pressure and little room for decision-making.
The economic advantages of computers at work have overshadowed associated potential health, safety and social problems for workers, such as job loss, cumulative trauma disorders and increased mental stress. The transition from more traditional forms of work to computerization has been difficult in many workplaces, and has resulted in significant psychosocial and sociotechnical problems for the workforce.
Psychosocial Problems Specific to VDUs
Research studies (for example, Bradley 1983 and 1989; Bikson 1987; Westlander 1989; Westlander and Aberg 1992; Johansson and Aronsson 1984; Stellman et al. 1987b; Smith et al. 1981 and 1992a) have documented how the introduction of computers into the workplace has brought substantial changes in the process of work, in social relationships, in management style and in the nature and content of job tasks. In the 1980s, the implementation of the technological changeover to computerization was most often a “top-down” process in which employees had no input into the decisions regarding the new technology or the new work structures. As a result, many industrial relations, physical and mental health problems arose.
Experts disagree on the success of changes that are occurring in offices, with some arguing that computer technology improves the quality of work and enhances productivity (Strassmann 1985), while others compare computers to earlier forms of technology, such as assembly-line production that also make working conditions worse and increase job stress (Moshowitz 1986; Zuboff 1988). We believe that visual display unit (VDU) technology does affect work in various ways, but technology is only one element of a larger work system that includes the individual, tasks, environment and organizational factors.
Conceptualizing Computerized Job Design
Many working conditions jointly influence the VDU user. The authors have proposed a comprehensive job design model which illustrates the various facets of working conditions which can interact and accumulate to produce stress (Smith and Carayon-Sainfort 1989). Figure 1 illustrates this conceptual model for the various elements of a work system that can exert loads on workers and may result in stress. At the centre of this model is the individual with his/her unique physical characteristics, perceptions, personality and behaviour. The individual uses technologies to perform specific job tasks. The nature of the technologies, to a large extent, determines performance and the skills and knowledge needed by the worker to use the technology effectively. The requirements of the task also affect the required skill and knowledge levels needed. Both the tasks and technologies affect the job content and the mental and physical demands. The model also shows that the tasks and technologies are placed within the context of a work setting that comprises the physical and the social environment. The overall environment itself can affect comfort, psychological moods and attitudes. Finally, the organizational structure of work defines the nature and level of individual involvement, worker interactions, and levels of control. Supervision and standards of performance are all affected by the nature of the organization.
Figure 1. Model of working conditions and their impact on the individual
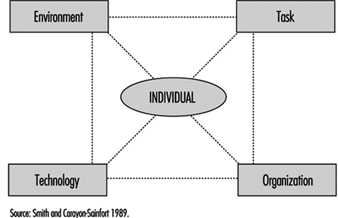
This model helps to explain relationships between job requirements, psychological and physical loads and resulting health strains. It represents a systems concept in which any one element can influence any other element, and in which all elements interact to determine the way in which work is accomplished and the effectiveness of the work in achieving individual and organizational needs and goals. The application of the model to the VDU workplace is described below.
Environment
Physical environmental factors have been implicated as job stressors in the office and elsewhere. General air quality and housekeeping contribute, for example, to sick building syndrome and other stress responses (Stellman et al. 1985; Hedge, Erickson and Rubin 1992.) Noise is a well-known environmental stressor which can cause increases in arousal, blood pressure, and negative psychological mood (Cohen and Weinstein 1981). Environmental conditions that produce sensory disruption and make it more difficult to carry out tasks increase the level of worker stress and emotional irritation are other examples (Smith et al. 1981; Sauter et al. 1983b).
Task
With the introduction of computer technology, expectations regarding performance increase. Additional pressure on workers is created because they are expected to perform at a higher level all the time. Excessive workload and work pressure are significant stressors for computer users (Smith et al. 1981; Piotrkowski, Cohen and Coray 1992; Sainfort 1990). New types of work demands are appearing with the increasing use of computers. For instance, cognitive demands are likely to be sources of increased stress for VDU users (Frese 1987). These are all facets of job demands.
Electronic Monitoring of Employee Performance
The use of electronic methods to monitor employee work performance has increased substantially with the widespread use of personal computers which make such monitoring quick and easy. Monitoring provides information which can be used by employers to better manage technological and human resources. With electronic monitoring it is possible to pinpoint bottlenecks, production delays and below average (or below standard) performance of employees in real time. New electronic communication technologies have the capability of tracking the performance of individual elements of a communication system and of pinpointing individual worker inputs. Such work elements as data entry into computer terminals, telephone conversations, and electronic mail messages can all be examined through the use of electronic surveillance.
Electronic monitoring increases management control over the workforce, and may lead to organisational management approaches that are stressful. This raises important issues about the accuracy of the monitoring system and how well it represents worker contributions to the employer’s success, the invasion of worker privacy, worker versus technology control over job tasks, and the implications of management styles that use monitored information to direct worker behaviour on the job (Smith and Amick 1989; Amick and Smith 1992; Carayon 1993b). Monitoring can bring about increased production, but it may also produce job stress, absences from work, turnover in the workforce and sabotage. When electronic monitoring is combined with incentive systems for increased production, work-related stress can also be increased (OTA 1987; Smith et al. 1992a). In addition, such electronic performance monitoring raises issues of worker privacy (ILO 1991) and several countries have banned the use of individual performance monitoring.
A basic requirement of electronic monitoring is that work tasks be broken up into activities that can easily be quantified and measured, which usually results in a job design approach that reduces the content of the tasks by removing complexity and thinking, which are replaced by repetitive action. The underlying philosophy is similar to a basic principle of “Scientific Management” (Taylor 1911) that calls for work “simplification.”
In one company, for example, a telephone monitoring capability was included with a new telephone system for customer service operators. The monitoring system distributed incoming telephone calls from customers, timed the calls and allowed for supervisor eavesdropping on employee telephone conversations. This system was instituted under the guise of a work flow scheduling tool for determining the peak periods for telephone calls to determine when extra operators would be needed. Instead of using the monitoring system solely for that purpose, management also used the data to establish work performance standards, (seconds per transaction) and to bring disciplinary action against employees with “below average performance.” This electronic monitoring system introduced a pressure to perform above average because of fear of reprimand. Research has shown that such work pressure is not conducive to good performance but rather can bring about adverse health consequences (Cooper and Marshall 1976; Smith 1987). In fact, the monitoring system described was found to have increased employee stress and lowered the quality of production (Smith et al. 1992a).
Electronic monitoring can influence worker self-image and feelings of self-worth. In some cases, monitoring could enhance feelings of self-worth if the worker gets positive feedback. The fact that management has taken an interest in the worker as a valuable resource is another possible positive outcome. However, both effects may be perceived differently by workers, particularly if poor performance leads to punishment or reprimand. Fear of negative evaluation can produce anxiety and may damage self-esteem and self-image. Indeed electronic monitoring can create known adverse working conditions, such as paced work, lack of worker involvement, reduced task variety and task clarity, reduced peer social support, reduced supervisory support, fear of job loss, or routine work activities, and lack of control over tasks (Amick and Smith 1992; Carayon 1993).
Michael J. Smith
Positive aspects also exist since computers are able to do many of the simple, repetitive tasks that were previously done manually, which can reduce the repetitiveness of the job, increase the content of the job and make it more meaningful. This is not universally true, however, since many new computer jobs, such as data entry, are still repetitive and boring. Computers can also provide performance feedback that is not available with other technologies (Kalimo and Leppanen 1985), which can reduce ambiguity.
Some aspects of computerized work have been linked to decreased control, which has been identified as a major source of stress for clerical computer users. Uncertainty regarding the duration of computer-related problems, such as breakdown and slowdown, can be a source of stress (Johansson and Aronsson 1984; Carayon-Sainfort 1992). Computer-related problems can be particularly stressful if workers, such as airline reservation clerks, are highly dependent on the technology to perform their job.
Technology
The technology being used by the worker often defines his or her ability to accomplish tasks and the extent of physiological and psychological load. If the technology produces either too much or too little workload, increased stress and adverse physical health outcomes can occur (Smith et al. 1981; Johansson and Aronsson 1984; Ostberg and Nilsson 1985). Technology is changing at a rapid pace, forcing workers to adjust their skills and knowledge continuously to keep up. In addition, today’s skills can quickly become obsolete. Technological obsolescence may be due to job de-skilling and impoverished job content or to inadequate skills and training. Workers who do not have the time or resources to keep up with the technology may feel threatened by the technology and may worry about losing their job. Thus, workers’ fears of having inadequate skills to use the new technology are one of the main adverse influences of technology, which training, of course, can help to offset. Another effect of the introduction of technology is the fear of job loss due to increased efficiency of technology (Ostberg and Nilsson 1985; Smith, Carayon and Miezio 1987).
Intensive, repetitive, long sessions at the VDU can also contribute to increased ergonomic stress and strain (Stammerjohn, Smith and Cohen 1981; Sauter et al. 1983b; Smith et al. 1992b) and can create visual or musculoskeletal discomfort and disorders, as described elsewhere in the chapter.
Organizational factors
The organizational context of work can influence worker stress and health. When technology requires new skills, the way in which workers are introduced to the new technology and the organizational support they receive, such as appropriate training and time to acclimatize, has been related to the levels of stress and emotional disturbances experienced (Smith, Carayon and Miezio 1987). The opportunity for growth and promotion in a job (career development) is also related to stress (Smith et al. 1981). Job future uncertainty is a major source of stress for computer users (Sauter et al. 1983b; Carayon 1993a) and the possibility of job loss also creates stress (Smith et al. 1981; Kasl 1978).
Work scheduling, such as shift work and overtime, have been shown to have negative mental and physical health consequences (Monk and Tepas 1985; Breslow and Buell 1960). Shift work is increasingly used by companies that want or need to keep computers running continuously. Overtime is often needed to ensure that workers keep up with the workload, especially when work remains incomplete as a result of delays due to computer breakdown or misfunction.
Computers provide management with the capability to continuously monitor employee performance electronically, which has the potential to create stressful working conditions, such as by increasing work pressure (see the box “Electronic Monitoring”). Negative employee-supervisor relationships and feelings of lack of control can increase in electronically supervised workplaces.
The introduction of VDU technology has affected social relationships at work. Social isolation has been identified as a major source of stress for computer users (Lindström 1991; Yang and Carayon 1993) since the increased time spent working on computers reduces the time that workers have to socialize and receive or give social support. The need for supportive supervisors and co-workers has been well documented (House 1981). Social support can moderate the impact of other stressors on worker stress. Thus, support from colleagues, supervisor or computer staff becomes important for the worker who is experiencing computer-related problems but the computer work environment may, ironically, reduce the level of such social support available.
The individual
A number of personal factors such as personality, physical health status, skills and abilities, physical conditioning, prior experiences and learning, motives, goals and needs determine the physical and psychological effects just described (Levi 1972).
Improving the Psychosocial Characteristics of VDU Work
The first step in making VDU work less stressful is to identify work organization and job design features that can promote psychosocial problems so that they can be modified, always bearing in mind that VDU problems which can lead to job stress are seldom the result of single aspects of the organization or of job design, but rather, are a combination of many aspects of improper work design. Thus, solutions for reducing or eliminating job stress must be comprehensive and deal with many improper work design factors simultaneously. Solutions that focus on only one or two factors will not succeed. (See figure 2.)
Figure 2. Keys to reducing isolation and stress
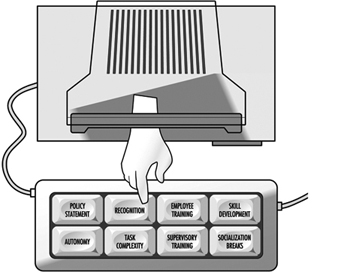
Improvements in job design should start with the work organization providing a supportive environment for employees. Such an environment enhances employee motivation to work and feelings of security, and it reduces feelings of stress (House 1981). A policy statement that defines the importance of employees within an organization and is explicit on how the organization will provide a supportive environment is a good first step. One very effective means for providing support to employees is to provide supervisors and managers with specific training in methods for being supportive. Supportive supervisors can serve as buffers that “protect” employees from unnecessary organizational or technological stresses.
The content of job tasks has long been recognized as important for employee motivation and productivity (Herzberg 1974; Hackman and Oldham 1976). More recently the relationship between job content and job stress reactions has been elucidated (Cooper and Marshall 1976; Smith 1987). Three main aspects of job content that are of specific relevance to VDU work are task complexity, employee skills and career opportunities. In some respects, these are all related to the concept of developing the motivational climate for employee job satisfaction and psychological growth, which deals with the improvement of employees’ intellectual capabilities and skills, increased ego enhancement or self-image and increased social group recognition of individual achievement.
The primary means for enhancing job content is to increase the skill level for performing job tasks, which typically means enlarging the scope of job tasks, as well as enriching the elements of each specific task (Herzberg 1974). Enlarging the number of tasks increases the repertoire of skills needed for successful task performance, and also increases the number of employee decisions made while defining task sequences and activities. An increase in the skill level of the job content promotes employee self-image of personal worth and of value to the organization. It also enhances the positive image of the individual in his or her social work group within the organization.
Increasing the complexity of the tasks, which means increasing the amount of thinking and decision-making involved, is a logical next step that can be achieved by combining simple tasks into sets of related activities that have to be coordinated, or by adding mental tasks that require additional knowledge and computational skills. Specifically, when computerized technology is introduced, new tasks in general will have requirements that exceed the current knowledge and skills of the employees who are to perform them. Thus there is a need to train employees in the new aspects of the tasks so that they will have the skills to perform the tasks adequately. Such training has more than one benefit, since it not only may improve employee knowledge and skills, and thus enhance performance, but may also enhance employee self-esteem and confidence. Providing training also shows the employee that the employer is willing to invest in his or her skill enhancement, and thus promotes confidence in employment stability and job future.
The amount of control that an employee has over the job has a powerful psychosocial influence (Karasek et al. 1981; Sauter, Cooper and Hurrell 1989). Important aspects of control can be defined by the answers to the questions, “What, how and when?” The nature of the tasks to be undertaken, the need for coordination among employees, the methods to be used to carry out the tasks and the scheduling of the tasks can all be defined by answers to these questions. Control can be designed into jobs at the levels of the task, the work unit and the organization (Sainfort 1991; Gardell 1971). At the task level, the employee can be given autonomy in the methods and procedures used in completing the task.
At the work-unit level, groups of employees can self-manage several interrelated tasks and the group itself can decide on who will perform particular tasks, the scheduling of tasks, coordination of tasks and production standards to meet organizational goals. At the organization level, employees can participate in structured activities that provide input to management about employee opinions or quality improvement suggestions. When the levels of control available are limited, it is better to introduce autonomy at the task level and then work up the organizational structure, insofar as possible (Gardell 1971).
One natural result of computer automation appears to be an increased workload, since the purpose of the automation is to enhance the quantity and quality of work output. Many organizations believe that such an increase is necessary in order to pay for the investment in the automation. However, establishing the appropriate workload is problematic. Scientific methods have been developed by industrial engineers for determining appropriate work methods and workloads (the performance requirements of jobs). Such methods have been used successfully in manufacturing industries for decades, but have had little application in office settings, even after office computerization. The use of scientific means, such as those described by Kanawaty (1979) and Salvendy (1992), to establish workloads for VDU operators, should be a high priority for every organization, since such methods set reasonable production standards or work output requirements, help to protect employees from excessive workloads, as well as help to ensure the quality of products.
The demand that is associated with the high levels of concentration required for computerized tasks can diminish the amount of social interaction during work, leading to social isolation of employees. To counter this effect, opportunities for socialization for employees not engaged in computerized tasks, and for employees who are on rest breaks, should be provided. Non-computerized tasks which do not require extensive concentration could be organized in such a way that employees can work in close proximity to one another and thus have the opportunity to talk among themselves. Such socialization provides social support, which is known to be an essential modifying factor in reducing adverse mental health effects and physical disorders such as cardiovascular diseases (House 1981). Socialization naturally also reduces social isolation and thus promotes improved mental health.
Since poor ergonomic conditions can also lead to psychosocial problems for VDU users, proper ergonomic conditions are an essential element of complete job design. This is covered in some detail in other articles in this chapter and elsewhere in the Encyclopaedia.
Finding Balance
Since there are no “perfect” jobs or “perfect” workplaces free from all psychosocial and ergonomic stressors, we must often compromise when making improvements at the workplace. Redesigning processes generally involves “trade-offs” between excellent working conditions and the need to have acceptable productivity. This requires us to think about how to achieve the best “balance” between positive benefits for employee health and productivity. Unfortunately, since so many factors can produce adverse psychosocial conditions that lead to stress, and since these factors are interrelated, modifications in one factor may not be beneficial if concomitant changes are not made in other related factors. In general, two aspects of balance should be addressed: the balance of the total system and compensatory balance.
System balance is based on the idea that a workplace or process or job is more than the sum of the individual components of the system. The interplay among the various components produces results that are greater (or less) than the sum of the individual parts and determines the potential for the system to produce positive results. Thus, job improvements must take account of and accommodate the entire work system. If an organization concentrates solely on the technological component of the system, there will be an imbalance because personal and psychosocial factors will have been neglected. The model given in figure 1 of the work system can be used to identify and understand the relationships between job demands, job design factors, and stress which must be balanced.
Since it is seldom possible to eliminate all psychosocial factors that cause stress, either because of financial considerations, or because it is impossible to change inherent aspects of job tasks, compensatory balance techniques are employed. Compensatory balance seeks to reduce psychological stress by changing aspects of work that can be altered in a positive direction to compensate for those aspects that cannot be changed. Five elements of the work system—physical loads, work cycles, job content, control, and socialization—function in concert to provide the resources for achieving individual and organizational goals through compensatory balance. While we have described some of the potential negative attributes of these elements in terms of job stress, each also has positive aspects that can counteract the negative influences. For instance, inadequate skill to use new technology can be offset by employee training. Low job content that creates repetition and boredom can be balanced by an organizational supervisory structure that promotes employee involvement and control over tasks, and job enlargement that introduces task variety. The social conditions of VDU work could be improved by balancing the loads that are potentially stressful and by considering all of the work elements and their potential for promoting or reducing stress. The organizational structure itself could be adapted to accommodate enriched jobs in order to provide support to the individual. Increased staffing levels, increasing the levels of shared responsibilities or increasing the financial resources put toward worker well-being are other possible solutions.
Skin Problems
The first reports of skin complaints among people working with or near VDUs came from Norway as early as 1981. A few cases have also been reported from the United Kingdom, the United States and Japan. Sweden, however, has provided many case reports and public discussion on the health effects of exposure to VDUs was intensified when one case of skin disease in a VDU worker was accepted as an occupational disease by the Swedish National Insurance Board in late 1985. The acceptance of this case for compensation coincided with a marked increase in the number of cases of skin disease that were suspected to be related to work with VDUs. At the Department of Occupational Dermatology at Karolinska Hospital, Stockholm, the caseload increased from seven cases referred between 1979 and 1985, to 100 new referrals from November 1985 to May 1986.
Despite the relatively large number of people who sought medical treatment for what they believed to be VDU-related skin problems, no conclusive evidence is available which shows that the VDUs themselves lead to the development of occupational skin disease. The occurrence of skin disease in VDU-exposed people appears to be coincidental or possibly related to other workplace factors. Evidence for this conclusion is strengthened by the observation that the increased incidence of skin complaints made by Swedish VDU workers has not been observed in other countries, where the mass media debate on the issue has not been as intense. Further, scientific data collected from provocation studies, in which patients have been purposely exposed to VDU-related electromagnetic fields to determine whether a skin effect could be induced, have not produced any meaningful data demonstrating a possible mechanism for development of skin problems which could be related to the fields surrounding a VDU.
Case Studies: Skin Problems and VDUs
Sweden: 450 patients were referred and examined for skin problems which they attributed to work at VDUs. Only common facial dermatoses were found and no patients had specific dermatoses that could be related to work with VDUs. While most patients felt that they had pronounced symptoms, their visible skin lesions were, in fact, mild according to standard medical definitions and most of the patients reported improvement without drug therapy even though they continued to work with VDUs . Many of the patients were suffering from identifiable contact allergies, which explained their skin symptoms . Epidemiological studies comparing the VDU-work patients to a non-exposed control population with a similar skin status showed no relationship between skin status and VDU work. Finally, a provocation study did not yield any relation between the patient symptoms and electrostatic or magnetic fields from the VDUs (Wahlberg and Lidén 1988; Berg 1988; Lidén 1990; Berg, Hedblad and Erhardt 1990; Swanbeck and Bleeker 1989).In contrast to a few early nonconclusive epidemiological studies (Murray et al. 1981; Frank 1983; Lidén and Wahlberg 1985), a large-scale epidemiological study (Berg, Lidén, and Axelson 1990; Berg 1989) of 3,745 randomly selected office employees, of whom 809 persons were medically examined, showed that while the VDU-exposed employees reported significantly more skin problems than a nonexposed control population of office employees, upon examination, they were not actually found to have no more visible signs or more skin disease.
Wales (UK): A questionnaire study found no difference between reports of skin problems in VDU workers and a control population (Carmichael and Roberts 1992).
Singapore: A control population of teachers reported significantly more skin complaints than did the VDU users (Koh et al. 1991).
It is, however, possible that work-related stress could be an important factor that can explain VDU-associated skin complaints. For example, follow-up studies in the office environment of a subgroup of the VDU-exposed office employees being studied for skin problems showed that significantly more people in the group with skin symptoms experienced extreme occupational stress than people without the skin symptoms. A correlation between levels of the stress-sensitive hormones testosterone, prolactin and thyroxin and skin symptoms were observed during work, but not during days off. Thus, one possible explanation for VDU-associated facial skin sensations could be the effects of thyroxin, which causes the blood vessels to dilate (Berg et al. 1992).
Musculoskeletal Disorders
Introduction
VDU operators commonly report musculoskeletal problems in the neck, shoulders and upper limbs. These problems are not unique to VDU operators and are also reported by other workers performing tasks which are repetitive or which involve holding the body in a fixed posture (static load). Tasks which involve force are also commonly associated with musculoskeletal problems, but such tasks are not generally an important health and safety consideration for VDU operators.
Among clerical workers, whose jobs are generally sedentary and not commonly associated with physical stress, the introduction into workplaces of VDUs caused work-related musculoskeletal problems to gain in recognition and prominence. Indeed, an epidemic-like increase in reporting of problems in Australia in the mid 1980s and, to a lesser extent, in the United States and the United Kingdom in the early 1990s, has led to a debate about whether or not the symptoms have a physiological basis and whether or not they are work-related.
Those who dispute that musculoskeletal problems associated with VDU (and other) work have a physiological basis generally put forward one of four alternative views: workers are malingering; workers are unconsciously motivated by various possible secondary gains, such as workers’ compensation payments or the psychological benefits of being sick, known as compensation neurosis; workers are converting unresolved psychological conflict or emotional disturbance into physical symptoms, that is, conversion disorders; and finally, that normal fatigue is being blown out of proportion by a social process which labels such fatigue as a problem, termed social iatrogenesis. Rigorous examination of the evidence for these alternative explanations shows that they are not as well supported as explanations which posit a physiological basis for these disorders (Bammer and Martin 1988). Despite the growing evidence that there is a physiological basis for musculoskeletal complaints, the exact nature of the complaints is not well understood (Quintner and Elvey 1990; Cohen et al. 1992; Fry 1992; Helme, LeVasseur and Gibson 1992).
Symptom Prevalence
A large number of studies have documented the prevalence of musculoskeletal problems among VDU operators and these have been predominantly conducted in western industrialized countries. There is also growing interest in these problems in the rapidly industrializing nations of Asia and Latin America. There is considerable inter-country variation in how musculoskeletal disorders are described and in the types of studies carried out. Most studies have relied on symptoms reported by workers, rather than on the results of medical examinations. The studies can be usefully divided into three groups: those which have examined what can be called composite problems, those which have looked at specific disorders and those which have concentrated on problems in a single area or small group of areas.
Composite problems
Composite problems are a mixture of problems, which can include pain, loss of strength and sensory disturbance, in various parts of the upper body. They are treated as a single entity, which in Australia and the United Kingdom is referred to as repetitive strain injuries (RSI), in the United States as cumulative trauma disorders (CTD) and in Japan as occupational cervicobrachial disorders (OCD). A 1990 review (Bammer 1990) of problems among office workers (75% of the studies were of office workers who used VDUs) found that 70 studies had examined composite problems and 25 had found them to occur in a frequency range of between 10 and 29% of the workers studied. At the extremes, three studies had found no problems, while three found that 80% of workers suffer from musculoskeletal complaints. Half of the studies also reported on severe or frequent problems, with 19 finding a prevalence between 10 and 19%. One study found no problems and one found problems in 59%. The highest prevalences were found in Australia and Japan.
Specific disorders
Specific disorders cover relatively well-defined problems such as epicondylitis and carpal tunnel syndrome. Specific disorders have been less frequently studied and found to occur less frequently. Of 43 studies, 20 found them to occur in between 0.2 and 4% of workers. Five studies found no evidence of specific disorders and one found them in between 40–49% of workers.
Particular body parts
Other studies focus on particular areas of the body, such as the neck or the wrists. Neck problems are the most common and have been examined in 72 studies, with 15 finding them to occur in between 40 and 49% of workers. Three studies found them to occur in between 5 and 9% of workers and one found them in more than 80% of workers. Just under half the studies examined severe problems and they were commonly found in frequencies that ranged between 5% and 39%. Such high levels of neck problems have been found internationally, including Australia, Finland, France, Germany, Japan, Norway, Singapore, Sweden, Switzerland, the United Kingdom and the United States. In contrast, only 18 studies examined wrist problems, and seven found them to occur in between 10% and 19% of workers. One found them to occur in between 0.5 and 4% of workers and one in between 40% and 49%.
Causes
It is generally agreed that the introduction of VDUs is often associated with increased repetitive movements and increased static load through increased keystroke rates and (compared with typewriting) reduction in non-keying tasks such as changing paper, waiting for the carriage return and use of correction tape or fluid. The need to watch a screen can also lead to increased static load, and poor placement of the screen, keyboard or function keys can lead to postures which may contribute to problems. There is also evidence that the introduction of VDUs can be associated with reductions in staff numbers and increased workloads. It can also lead to changes in the psychosocial aspects of work, including social and power relationships, workers’ responsibilities, career prospects and mental workload. In some workplaces such changes have been in directions which are beneficial to workers.
In other workplaces they have led to reduced worker control over the job, lack of social support on the job, “de-skilling”, lack of career opportunities, role ambiguity, mental stress and electronic monitoring (see review by Bammer 1987b and also WHO 1989 for a report on a World Health Organization meeting). The association between some of these psychosocial changes and musculoskeletal problems is outlined below. It also seems that the introduction of VDUs helped stimulate a social movement in Australia which led to the recognition and prominence of these problems (Bammer and Martin 1992).
Causes can therefore be examined at individual, workplace and social levels. At the individual level, the possible causes of these disorders can be divided into three categories: factors not related to work, biomechanical factors and work organization factors (see table 1). Various approaches have been used to study causes but the overall results are similar to those obtained in empirical field studies which have used multivariate analyses (Bammer 1990). The results of these studies are summarized in table 1 and table 2. More recent studies also support these general findings.
Table 1. Summary of empirical fieldwork studies which have used multivariate analyses to study the causes of musculoskeletal problems among office workers
|
Factors |
||||
|
|
|
|
|
Work organisation |
|
Blignault (1985) |
146/90% |
ο |
ο |
● |
|
South Australian Health Commission Epidemiology Branch (1984) |
456/81% |
●
|
●
|
●
|
|
Ryan, Mullerworth and Pimble (1984) |
52/100% |
● |
●
|
●
|
|
Ryan and |
143 |
|||
|
Ellinger et al. (1982) |
280 |
● |
●
|
● |
|
Pot, Padmos and |
222/100% |
not studied |
● |
● |
|
Sauter et al. (1983b) |
251/74% |
ο |
●
|
● |
|
Stellman et al. (1987a) |
1, 032/42% |
not studied |
●
|
● |
ο = non-factor ●= factor.
Source: Adapted from Bammer 1990.
Table 2. Summary of studies showing involvement of factors thought to cause musculoskeletal problems among office workers
|
Non-work |
Biomechanical |
Work organization |
|||||||||||||
|
Country |
No./% VDU |
Age |
Biol. |
Neuro ticism |
Joint |
Furn. |
Furn. |
Visual |
Visual |
Years |
Pressure |
Autonomy |
Peer |
Variety |
Key- |
|
Australia |
146/ |
Ø |
Ø |
Ø |
Ø |
Ο |
● |
● |
● |
Ø |
|||||
|
Australia |
456/ |
● |
Ο |
❚ |
Ø |
Ο |
● |
Ο |
|||||||
|
Australia |
52/143/ |
▲ |
❚ |
❚ |
Ο |
Ο |
● |
Ο |
|||||||
|
Germany |
280 |
Ο |
Ο |
❚ |
Ø |
❚ |
Ο |
Ο |
● |
● |
Ο |
||||
|
Netherlands |
222/ |
❚ |
❚ |
Ø |
Ø |
Ο |
● |
(Ø) |
Ο |
||||||
|
United States |
251/ |
Ø |
Ø |
❚ |
❚ |
Ο |
● |
(Ø) |
●
|
||||||
|
United States |
1,032/ |
Ø |
❚ |
❚ |
Ο |
● |
● |
||||||||
Ο = positive association, statistically significant. ● = negative association, statistically significant. ❚ = statistically significant association. Ø = no statistically significant association. (Ø) = no variability in the factor in this study. ▲ = the youngest and the oldest had more symptoms.
Empty box implies that the factor was not included in this study.
1 Matches references in table 52.7.
Source: adapted from Bammer 1990.
Factors not related to work
There is very little evidence that factors not related to work are important causes of these disorders, although there is some evidence that people with a previous injury to the relevant area or with problems in another part of the body may be more likely to develop problems. There is no clear evidence for involvement of age and the one study which examined neuroticism found that it was not related.
Biomechanical factors
There is some evidence that working with certain joints of the body at extreme angles is associated with musculoskeletal problems. The effects of other biomechanical factors are less clear-cut, with some studies finding them to be important and others not. These factors are: assessment of the adequacy of the furniture and/or equipment by the investigators; assessment of the adequacy of the furniture and/or equipment by the workers; visual factors in the workplace, such as glare; personal visual factors, such as the use of spectacles; and years on the job or as an office worker (table 2).
Organizational factors
A number of factors related to work organization are clearly associated with musculoskeletal problems and are discussed more fully elsewhere is this chapter. Factors include: high work pressure, low autonomy (i.e., low levels of control over work), low peer cohesion (i.e., low levels of support from other workers) which may mean that other workers cannot or do not help out in times of pressure, and low task variety.
The only factor which was studied for which results were mixed was hours using a keyboard (table 2). Overall it can be seen that the causes of musculoskeletal problems on the individual level are multifactorial. Work-related factors, particularly work organization, but also biomechanical factors, have a clear role. The specific factors of importance may vary from workplace to workplace and person to person, depending on individual circumstances. For example, the large-scale introduction of wrist rests into a workplace when high pressure and low task variety are hallmarks is unlikely to be a successful strategy. Alternatively, a worker with satisfactory delineation and variety of tasks may still develop problems if the VDU screen is placed at an awkward angle.
The Australian experience, where there was a decline in prevalence of reporting of musculoskeletal problems in the late 1980s, is instructive in indicating how the causes of these problems can be dealt with. Although this has not been documented or researched in detail, it is likely that a number of factors were associated with the decline in prevalence. One is the widespread introduction into workplaces of “ergonomically” designed furniture and equipment. There were also improved work practices including multiskilling and restructuring to reduce pressure and increase autonomy and variety. These often occurred in conjunction with the implementation of equal employment opportunity and industrial democracy strategies. There was also widespread implementation of prevention and early intervention strategies. Less positively, some workplaces seem to have increased their reliance on casual contract workers for repetitive keyboard work. This means that any problems would not be linked to the employer, but would be solely the worker’s responsibility.
In addition, the intensity of the controversy surrounding these problems led to their stigmatization, so that many workers have become more reluctant to report and claim compensation when they develop symptoms. This was further exacerbated when workers lost cases brought against employers in well-publicized legal proceedings. A decrease in research funding, cessation in publication of incidence and prevalence statistics and of research papers about these disorders, as well as greatly reduced media attention to the problem all helped shape a perception that the problem had gone away.
Conclusion
Work-related musculoskeletal problems are a significant problem throughout the world. They represent enormous costs at the individual and social levels. There are no internationally accepted criteria for these disorders and there is a need for an international system of classification. There needs to be an emphasis on prevention and early intervention and this needs to be multifactorial. Ergonomics should be taught at all levels from elementary school to university and there need to be guidelines and laws based on minimum requirements. Implementation requires commitment from employers and active participation from employees (Hagberg et al. 1993).
Despite the many recorded cases of people with severe and chronic problems, there is little available evidence of successful treatments. There is also little evidence of how rehabilitation back into the workforce of workers with these disorders can be most successfully undertaken. This highlights that prevention and early intervention strategies are paramount to the control of work-related musculoskeletal problems.
Reproductive Effects - Human Evidence
The safety of visual display units (VDUs) in terms of reproductive outcomes has been questioned since the widespread introduction of VDUs in the work environment during the 1970s. Concern for adverse pregnancy outcomes was first raised as a result of numerous reports of apparent clusters of spontaneous abortion or congenital malformations among pregnant VDU operators (Blackwell and Chang 1988). While these reported clusters were determined to be no more than what could be expected by chance, given the widespread use of VDUs in the modern workplace (Bergqvist 1986), epidemiologic studies were undertaken to explore this question further.
From the published studies reviewed here, a safe conclusion would be that, in general, working with VDUs does not appear to be associated with an excess risk of adverse pregnancy outcomes. However, this generalized conclusion applies to VDUs as they are typically found and used in offices by female workers. If, however, for some technical reason, there existed a small proportion of VDUs which did induce a strong magnetic field, then this general conclusion of safety could not be applied to that special situation since it is unlikely that the published studies would have had the statistical ability to detect such an effect. In order to be able to have generalizable statements of safety, it is essential that future studies be carried out on the risk of adverse pregnancy outcomes associated with VDUs using more refined exposure measures.
The most frequently studied reproductive outcomes have been:
- Spontaneous abortion (10 studies): usually defined as a hospitalized unintentional cessation of pregnancy occurring before 20 weeks of gestation.
- Congenital malformation (8 studies): many different types were assessed, but in general, they were diagnosed at birth.
- Other outcomes (8 studies) such as low birthweight (under 2,500 g), very low birthweight (under 1,500 g), and fecundability (time to pregnancy from cessation of birth control use) have also been assessed. See table 1.
Table 1. VDU use as a factor in adverse pregnancy outcomes
|
Objectives |
Methods |
Results |
|||||
|
Study |
Outcome |
Design |
Cases |
Controls |
Exposure |
OR/RR (95% CI) |
Conclusion |
|
Kurppa et al. |
Congenital malformation |
Case-control |
1, 475 |
1, 475 same age, same delivery date |
Job titles, |
235 cases, |
No evidence of increased risk among women who reported exposure to VDU or among women whose job titles indicated possible exposure |
|
Ericson and Källén (1986) |
Spontaneous abortion, |
Case-case |
412 |
1, 032 similar age and from same registry |
Job titles |
1.2 (0.6-2.3) |
The effect of VDU use was not statistically significant |
|
Westerholm and Ericson |
Stillbirth, |
Cohort |
7 |
4, 117 |
Job titles |
1.1 (0.8-1.4) |
No excesses were found for any of the studied outcomes. |
|
Bjerkedal and Egenaes (1986) |
Stillbirth, |
Cohort |
17 |
1, 820 |
Employment records |
NR(NS) |
The study concluded that there was no indication that introduction of VDUs in the centre has led to any increase in the rate of adverse pregnancy outcomes. |
|
Goldhaber, Polen and Hiatt |
Spontaneous abortion, |
Case-control |
460 |
1, 123 20% of all normal births, same region, same time |
Postal questionnaire |
1.8 (1.2-2.8) |
Statistically increased risk for spontaneous abortions for VDU exposure. No excess risk for congenital malformations associates with VDU exposure. |
|
McDonald et al. (1988) |
Spontaneous abortion, |
Cohort |
776 |
Face-to-face interviews |
1.19 (1.09-1.38) |
No increase in risk was found among women exposed to VDUs. |
|
|
Nurminen and Kurppa (1988) |
Threatened abortion, |
Cohort |
239 |
Face-to-face interviews |
0.9 |
The crude and adjusted rate ratios did not show statistically significant effects for working with VDUs. |
|
|
Bryant and Love (1989) |
Spontaneous abortion |
Case-control |
344 |
647 |
Face-to-face interviews |
1.14 (p = 0.47) prenatal |
VDU use was similar between the cases and both the prenatal controls and postnatal controls. |
|
Windham et al. (1990) |
Spontaneous abortion, |
Case-control |
626 |
1,308 same age, same last menstrual period |
Telephone interviews |
1.2 (0.88-1.6) |
Crude odds ratios for spontaneous abortion and VDU use less than 20 hours per week were 1.2; 95% CI 0.88-1.6, minimum of 20 hours per week were 1.3; 95% CI 0.87-1.5. Risks for low birthweight and intra-uterine growth retardation were not significantly elevated. |
|
Brandt and |
Congenital malformation |
Case-control |
421 |
1,365; 9.2% of all pregnancies, same registry |
Postal questionnaire |
0.96 (0.76-1.20) |
Use of VDUs during pregnancy was not associated with a risk of congenital malformations. |
|
Nielsen and |
Spontaneous abortion |
Case-control |
1,371 |
1,699 9.2% |
Postal questionnaire |
0.94 (0.77-1.14) |
No statistically significant risk for spontaneous abortion with VDU exposure. |
|
Tikkanen and Heinonen |
Cardiovascular malformations |
Case-control |
573 |
1,055 same time, hospital delivery |
Face-to-face interviews |
Cases 6.0%, controls 5.0% |
No statistically significant association between VDU use and cardiovascular malformation |
|
Schnorr et al. |
Spontaneous abortion |
Cohort |
136 |
746 |
Company records measurement of magnetic field |
0.93 (0.63-1.38) |
No excess risk for women who used VDUs during first trimester and no apparent |
|
Brandt and |
Time to pregnancy |
Cohort |
188 |
Postal questionnaire |
1.61 (1.09-2.38) |
For a time to pregnancy of greater than 13 months, there was an increased relative risk for the group with at least 21 hours of weekly VDU use. |
|
|
Nielsen and |
Low birthweight, |
Cohort |
434 |
Postal questionnaire |
0.88 (0.67-1.66) |
No increase in risk was found among women exposed to VDUs. |
|
|
Roman et al. |
Spontaneous abortion |
Case-control |
150 |
297 nulliparous hospital |
Face-to-face interviews |
0.9 (0.6-1.4) |
No relation to time spent using VDUs. |
|
Lindbohm |
Spontaneous abortion |
Case-control |
191 |
394 medical registers |
Employment records field measurement |
1.1 (0.7-1.6), |
Comparing workers with exposure to high magnetic field strengths to those with undetectable levels the ratio was 3.4 (95% CI 1.4-8.6) |
OR = Odds ratio. CI = Confidence Interval. RR = Relative risk. NR = Value not reported. NS = Not statistically significant.
Discussion
Evaluations of reported clusters of adverse pregnancy outcomes and VDU use have concluded that there was a high probability that these clusters occurred by chance (Bergqvist 1986). In addition, the results of the few epidemiologic studies which have assessed the relation between VDU use and adverse pregnancy outcomes have, on the whole, not shown a statistically significant increased risk.
In this review, out of ten studies of spontaneous abortion, only two found a statistically significant increased risk for VDU exposure (Goldhaber, Polen and Hiatt 1988; Lindbohm et al. 1992). None of the eight studies on congenital malformations showed an excess risk associated with VDU exposure. Of the eight studies which looked at other adverse pregnancy outcomes, one has found a statistically significant association between waiting time to pregnancy and VDU use (Brandt and Nielsen 1992).
Although there are no major differences between the three studies with positive findings and those with negative ones, improvements in exposure assessment may have increased the chances of finding a significant risk. Though not exclusive to the positive studies, these three studies attempted to divide the workers into different levels of exposure. If there is a factor inherent in VDU use which predisposes a woman to adverse pregnancy outcomes, the dose received by the worker may influence the outcome. In addition, the results of the studies by Lindbohm et al. (1992) and Schnorr et al. (1991) suggest that only a small proportion of the VDUs may be responsible for increasing the risk of spontaneous abortion among users. If this is the case, failure to identify these VDUs will introduce a bias that could lead to underestimating the risk of spontaneous abortion among VDU users.
Other factors associated with work on VDUs, such as stress and ergonomic constraints, have been suggested as possible risk factors for adverse pregnancy outcomes (McDonald et al. 1988; Brandt and Nielsen 1992). Failure of many studies to control for these possible confounders may have lead to unreliable results.
While it may be biologically plausible that exposure to high levels of extremely low frequency magnetic fields through some VDUs carries an increased risk for adverse pregnancy outcomes (Bergqvist 1986), only two studies have attempted to measure these (Schnorr et al. 1991; Lindbohm et al. 1992). Extremely low frequency magnetic fields are present in any environment where electricity is used. A contribution of these fields to adverse pregnancy outcomes could only be detected if there was a variation, in time or in space, of these fields. While VDUs contribute to the overall levels of magnetic fields in the workplace, only a small percentage of the VDUs are thought to have a strong influence on the magnetic fields measured in the working environment (Lindbohm et al. 1992). Only a fraction of the women working with VDUs are thought to be exposed to levels of magnetic radiation above that which is normally encountered in the working environment (Lindbohm et al. 1992). The lack of precision in exposure assessment encountered in counting all VDU users as “exposed” weakens the ability of a study to detect the influence of magnetic fields from VDUs on adverse pregnancy outcomes.
In some studies, women who are not gainfully employed represented a large proportion of the comparison groups for women exposed to VDUs. In this comparison, certain selective processes may have affected the results (Infante-Rivard et al. 1993); for instance, women with severe diseases are selected out of the workforce, leaving healthier women more likely to have favourable reproductive outcomes in the workforce. On the other hand, an “unhealthy pregnant worker effect” is also possible, since women who have children may stop work, whereas those without children and who experience pregnancy loss may continue working. A suggested strategy to estimate the magnitude of this bias is to do separate analyses with and without women not gainfully employed.
Reproductive Hazards - Experimental Data
The purpose of the experimental studies described here, using animal models is, in part, to answer the question as to whether extremely low frequency (ELF) magnetic field exposures at levels similar to those around VDU workstations can be shown to affect reproductive functions in animals in a manner that can be equated to a human health risk.
The studies considered here are limited to in vivo studies (those performed on live animals) of reproduction in mammals exposed to very low frequency (VLF) magnetic fields with appropriate frequencies, excluding, therefore, studies on the biological effects in general of VLF or ELF magnetic fields. These studies on experimental animals fail to demonstrate unequivocally that magnetic fields, such as are found around VDUs, affect reproduction. Moreover, as can be seen from considering the experimental studies described in some detail below, the animal data do not shed a clear light on possible mechanisms for human reproductive effects of VDU use. These data complement the relative absence of indications of a measurable effect of VDU use on reproductive outcomes from human population studies.
Studies of Reproductive Effects of VLF Magnetic Fields in Rodents
VLF magnetic fields similar to those around VDUs have been used in five teratological studies, three with mice and two with rats. The results of these studies are summarized in table 1. Only one study (Tribukait and Cekan 1987), found an increased number of foetuses with external malformations. Stuchly et al. (1988) and Huuskonen, Juutilainen and Komulainen (1993) both reported a significant increase in the number of foetuses with skeletal abnormalities, but only when the analysis was based on the foetus as a unit. The study by Wiley and Corey (1992) did not demonstrate any effect of magnetic field exposures on placental resorption, or other pregnancy outcomes. Placental resorptions roughly correspond to spontaneous abortions in humans. Finally, Frölén and Svedenstål (1993) performed a series of five experiments. In each experiment, the exposure occurred on a different day. Among the first four experimental subgroups (start day 1–start day 5), there were significant increases in the number of placental resorptions among exposed females. No such effects were seen in the experiment where exposure started on day 7 and which is illustrated in figure 1.
Table 1. Teratological studies with rats or mice exposed to 18-20 kHz saw-tooth formed magnetic fields
|
Magnetic field exposure |
|||||
|
Study |
Subject1 |
Frequency |
Amplitude2 |
Duration3 |
Results4 |
|
Tribukait and Cekan (1987) |
76 litters of mice |
20 kHz |
1 μT, 15 μT |
Exposed to day 14 of pregnancy |
Significant increase in external malformation; only if foetus is used as the unit of observation; and only in the first half of the experiment; no difference as to resorption or foetal death. |
|
Stuchly et al. |
20 litters of rats |
18 kHz |
5.7μT, 23μT, |
Exposed throughout |
Significant increase in minor skeletal malformations; only if foetus is used as the unit of observation; some decrease in blood cell concentrations no difference as to resorption, nor as to other types of malformations |
|
Wiley and Corey |
144 litters of |
20 kHz |
3.6 μT, 17μT, |
Exposed throughout |
No difference as to any observed outcome (malformation, |
|
Frölén and |
In total 707 |
20 kHz |
15 μT |
Beginning on various days of pregnancy in |
Significant increase in resorption; only if exposure starts on day 1 to day 5; no difference as to malformations |
|
Huuskonen, |
72 litters of rats |
20 kHz |
15 μT |
Exposed to day 12 of pregnancy |
Significant increase in minor skeletal malformations; only if foetus is used as the unit of observation; no difference as to |
1 Total number of litters in the maximum exposure category.
2 Peak-to-peak amplitude.
3 Exposure varied from 7 to 24 hours/day in different experiments.
4 “Difference” refers to statistical comparisons between exposed and unexposed animals, “increase” refers to a comparison of the highest exposed group vs. the unexposed group.
Figure 1. The percentage of female mice with placental resorptions in relation to exposure
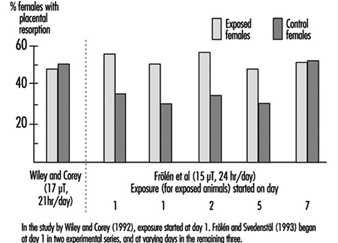
The interpretations given by the researchers to their findings include the following. Stuchly and co-workers reported that the abnormalities they observed were not unusual and ascribed the result to “common noise that appears in every teratological evaluation”. Huuskonen et al., whose findings were similar to Stuchly et al., were less negative in their appraisal and considered their result to be more indicative of a real effect, but they too remarked in their report that the abnormalities were “subtle and would probably not impair the later development of the foetuses”. In discussing their findings in which effects were observed in the early onset exposures but not the later ones, Frölén and Svedenstål suggest that the effects observed could be related to early effects on reproduction, before the fertilized egg is implanted in the uterus.
In addition to the reproductive outcomes, a decrease in white and red blood cells were noted in the highest exposure group in the study by Stuchly and co-workers. (Blood cell counts were not analysed in the other studies.) The authors, while suggesting that this could indicate a mild effect of the fields, also noted that the variations in blood cell counts were “within the normal range”. The absence of histological data and the absence of any effects on bone marrow cells made it difficult to evaluate these latter findings.
Interpretation and comparison of studies
Few of the results described here are consistent with one another. As stated by Frölén and Svedenstål, “qualitative conclusions with regard to corresponding effects in human beings and test animals may not be drawn”. Let us examine some of the reasoning that could lead to such a conclusion.
The Tribukait findings are generally not considered to be conclusive for two reasons. First, the experiment only yielded positive effects when the foetus was used as the unit of observation for statistical analysis, whereas the data themselves actually indicated a litter-specific effect. Second, there is a discrepancy in the study between the findings in the first and the second part, which implies that the positive findings may be the result of random variations and/or uncontrolled factors in the experiment.
Epidemiological studies investigating specific malformations have not observed an increase in skeletal malformations among children born of mothers working with VDUs—and thus exposed to VLF magnetic fields. For these reasons (foetus-based statistical analysis, abnormalities probably not health-related, and lack of concordance with epidemiological findings), the results—on minor skeletal malformations—are not such as to provide a firm indication of a health risk for humans.
Technical Background
Units of observation
When statistically evaluating studies on mammals, consideration must be given to at least one aspect of the (often unknown) mechanism. If the exposure affects the mother—which in turn affects the foetuses in the litter, it is the status of the litter as a whole which should be used as the unit of observation (the effect which is being observed and measured), since the individual outcomes among litter-mates are not independent. If, on the other hand, it is hypothesized that the exposure acts directly and independently on the individual foetuses within the litter, then one can appropriately use the foetus as a unit for statistical evaluation. The usual practice is to count the litter as the unit of observation, unless evidence is available that the effect of the exposure on one foetus is independent of the effect on the other foetuses in the litter.
Wiley and Corey (1992) did not observe a placental resorption effect similar to that seen by Frölén and Svedenstål. One reason put forward for this discrepancy is that different strains of mice were used, and the effect could be specific for the strain used by Frölén and Svedenstål. Apart from such a speculated species effect, it is also noteworthy that both females exposed to 17 μT fields and controls in the Wiley study had resorption frequencies similar to those in exposed females in the corresponding Frölén series, whereas most non-exposed groups in the Frölén study had much lower frequencies (see figure 1). One hypothetical explanation could be that a higher stress level among the mice in the Wiley study resulted from the handling of animals during the three hour period without exposure. If this is the case, an effect of the magnetic field could perhaps have been “drowned” by a stress effect. While it is difficult to definitely dismiss such a theory from the data provided, it does appear somewhat far-fetched. Furthermore, a “real” effect attributable to the magnetic field would be expected to be observable above such a constant stress effect as the magnetic field exposure increased. No such trend was observed in the Wiley study data.
The Wiley study reports on environmental monitoring and on rotation of cages to eliminate the effects of uncontrolled factors which might vary within the room environment itself, as magnetic fields can, while the Frölén study does not. Thus, control of “other factors” is at least better documented in the Wiley study. Hypothetically, uncontrolled factors that were not randomized could conceivably offer some explanations. It is also interesting to note that the lack of effect observed in the day 7 series of the Frölén study appears to be due not to a decrease in the exposed groups, but to an increase in the control group. Thus variations in the control group are probably important to consider while comparing the disparate results of the two studies.
Studies of Reproductive Effects of ELF Magnetic Fields in Rodents
Several studies have been performed, mostly on rodents, with 50–80 Hz fields. Details on six of these studies are shown in table 2. While other studies of ELF have been carried out, their results have not appeared in the published scientific literature and are generally available only as abstracts from conferences. In general the findings are of “random effects”, “no differences observed” and so on. One study, however, found a reduced number of external abnormalities in CD–1 mice exposed to a 20 mT, 50 Hz field but the authors suggested that this might reflect a selection problem. A few studies have been reported on species other than rodents (rhesus monkeys and cows), again apparently without observations of adverse exposure effects.
Table 2. Teratological studies with rats or mice exposed to 15-60 Hz sinusoidal or square pulsed magnetic fields
|
Magnetic field exposure |
||||||
|
Study |
Subject1 |
Frequency |
Amplitude |
Description |
Exposure duration |
Results |
|
Rivas and Rius |
25 Swiss mice |
50 Hz |
83 μT, 2.3 mT |
Pulsed, 5 ms pulse duration |
Before and during pregnancy and offspring growth; total 120 days |
No significant differences at birth in any measured parameter; decreased male body weight when adult |
|
Zecca et al. (1985) |
10 SD rats |
50 Hz |
5.8 mT |
Day 6-15 of pregnancy, |
No significant differences |
|
|
Tribukait and Cekan (1987) |
35 C3H mice |
50 Hz |
1 μT, 15 μT |
Square wave-forms, 0.5 ms duration |
Day 0-14 of pregnancy, |
No significant differences |
|
Salzinger and |
41 off-springs of SD rats. Only male pups used |
60 Hz |
100 μT (rms). Also electric |
Uniform circular polarized |
Day 0-22 of pregnancy and |
Lower increase in operand response during training commencing at 90 days of age |
|
McGivern and |
11 offsprings of SD rats. Only male pups used. |
15 Hz |
800 μT (peak) |
Square wave-forms, 0.3 ms duration |
Day 15-20 of pregnancy, |
Territorial scent marking behaviour reduced at 120 days of age. |
|
Huuskonen et al. |
72 Wistar rats |
50 Hz |
12.6μT (rms) |
Sinusoidal |
Day 0-12 of pregnancy, |
More foetuses/litter. Minor skeletal malformations |
1 Number of animals (mothers) in the highest exposure category given unless otherwise noted.
As can be seen from table 2, a wide range of results were obtained. These studies are more difficult to summarize because there are so many variations in exposure regimens, the endpoints under study as well as other factors. The foetus (or the surviving, “culled” pup) was the unit used in most studies. Overall, it is clear that these studies do not show any gross teratogenic effect of magnetic field exposure during pregnancy. As remarked above, “minor skeletal anomalies” do not appear to be of importance when evaluating human risks. The behavioural study results of Salzinger and Freimark (1990) and McGivern and Sokol (1990) are intriguing, but they do not form a basis for indications of human health risks at a VDU workstation, either from the standpoint of procedures (use of the foetus, and, for McGivern, a different frequency) or of effects.
Summary of specific studies
Behavioural retardation 3–4 months after birth was observed in the offspring of exposed females by Salzinger and McGivern. These studies appear to have used individual offspring as the statistical unit, which may be questionable if the stipulated effect is due to an effect on the mother. The Salzinger study also exposed the pups during the first 8 days after birth, so that this study involved more than reproductive hazards. A limited number of litters was used in both studies. Furthermore, these studies cannot be considered to confirm each other’s findings since the exposures varied greatly between them, as can be seen in table 2.
Apart from a behavioural change in the exposed animals, the McGivern study noted an increased weight of some male sex organs: the prostate, the seminal vesicles and the epididymis (all parts of the male reproductive system). The authors speculate as to whether this could be linked to stimulation of some enzyme levels in the prostate since magnetic field effects on some enzymes present in the prostate have been observed for 60 Hz.
Huuskonen and co-workers (1993) noted an increase in the number of foetuses per litter (10.4 foetuses/litter in the 50 Hz exposed group vs. 9 foetuses/litter in the control group). The authors, who had not observed similar trends in other studies, downplayed the importance of this finding by noting that it “may be incidental rather than an actual effect of the magnetic field”. In 1985 Rivas and Rius reported a different finding with a slightly lower number of live births per litter among exposed versus nonexposed groups. The difference was not statistically significant. They carried out the other aspects of their analyses on both a “per foetus” and “per litter” basis. The noted increase in minor skeletal malformations was only seen with the analysis using the foetus as the unit of observation.
Recommendations and Summary
Despite the relative lack of positive, consistent data demonstrating either human or animal reproductive effects, attempts at replications of the results of some studies are still warranted. These studies should attempt to reduce the variations in exposures, methods of analysis and strains of animals used.
In general, the experimental studies performed with 20 kHz magnetic fields have provided somewhat varied results. If adhering strictly to the litter analysis procedure and statistical hypothesis testing, no effects have been shown in rats (although similar nonsignificant findings were made in both studies). In mice, the results have been varied, and no single coherent interpretation of them appears possible at present. For 50 Hz magnetic fields, the situation is somewhat different. Epidemiological studies which are relevant to this frequency are scarce, and one study did indicate a possible risk of miscarriage. By contrast, the experimental animal studies have not produced results with similar outcomes. Overall, the results do not establish an effect of extremely low frequency magnetic fields from VDUs on the outcome of pregnancies. The totality of results fails thus to suggest an effect of VLF or ELF magnetic fields from VDUs on reproduction.
Ocular and Visual Problems
There have been a comparatively large number of studies devoted to visual discomfort in visual display unit (VDU) workers, many of which have yielded contradictory results. From one survey to another, there are discrepancies in reported prevalence of disorders ranging from practically 0 per cent to 80 per cent or more (Dainoff 1982). Such differences should not be considered too surprising because they reflect the large number of variables which can influence complaints of eye discomfort or disability.
Correct epidemiological studies of visual discomfort must take into account several population variables, such as sex, age, eye deficiencies, or use of lenses, as well as socio-economic status. The nature of the job being carried out with the VDU and the characteristics of the workstation layout and of the work organization are also important and many of these variables are interrelated.
Most often, questionnaires have been used to assess the eye discomfort of VDU operators. The prevalence of visual discomfort differs thus with the content of questionnaires and their statistical analysis. Appropriate questions for surveys concern the extent of symptoms of distress asthenopia suffered by VDU operators. Symptoms of this condition are well known and can include itching, redness, burning and tearing of the eyes. These symptoms are related to the fatigue of the accommodative function in the eye. Sometimes this eye symptoms are accompanied by a headache, with the pain located in the front portion of the head. There may also be disturbances in eye function, with symptoms such as double vision and reduced accommodative power. Visual acuity, itself, however, is rarely depressed, provided the conditions of measurement are carried out with a constant pupil size.
If a survey includes general questions, such as “Do you feel well at the end of the working day?” or “Have you ever had visual problems when working with VDUs?” the prevalence of positive responses may be higher than when single symptoms related to asthenopia are evaluated.
Other symptoms may also be strongly associated to asthenopia. Pains in the neck, shoulders and arms are frequently found. There are two main reasons that these symptoms may occur together with eye symptoms. The muscles of the neck participate in keeping a steady distance between eye and screen in VDU work and VDU work has two main components: screen and keyboard, which means that the shoulders and arms and the eyes are all working at the same time and thus may be subject to similar work-related strains.
User Variables Related to Visual Comfort
Sex and Age
In the majority of surveys, women report more eye discomfort than men. In one French study, for example, 35.6% of women complained of eye discomfort, against 21.8% of men (p J 05 significance level) (Dorard 1988). In another study (Sjödren and Elfstrom 1990) it was observed that while the difference in the degree of discomfort between women (41%) and men (24%) was great, it “was more pronounced for those working 5-8 hours a day than for those working 1-4 hours a day”. Such differences are not necessarily sex-related, however, since women and men seldom share similar tasks. For example, in one computer plant studied, when women and men were both occupied in a traditional “woman’s job”, both sexes displayed the same amount of visual discomfort. Furthermore when women worked in traditional “men’s jobs”, they did not report more discomfort than men. In general, regardless of sex, the number of visual complaints among skilled workers who use VDUs on their jobs is much lower than the number of complaints from workers in unskilled, hectic jobs, such as data entry or word processing (Rey and Bousquet 1989). Some of these data are given in table 1.
Table 1. Prevalence of ocular symptoms in 196 VDU operators according to 4 categories
|
Categories |
Percentage of symptoms (%) |
|
Females in "female" jobs |
81 |
|
Males in "female" jobs |
75 |
|
Males in "male" jobs |
68 |
|
Females in "male" jobs |
65 |
Source: From Dorard 1988 and Rey and Bousquet 1989.
The highest number of visual complaints usually arise in the 40–50-year-old group, probably because this is the time when changes in accommodation ability of the eye are occurring rapidly. However, although older operators are perceived as having more visual complaints than younger workers, and, as a consequence, presbyopia (vision impairment due to ageing) is often cited as the main visual defect associated with visual discomfort at VDU workstations, it is important to consider that there is also a strong association between having acquired advanced skills in VDU work and age. There is usually a higher proportion of older women among unskilled female VDU operators, and younger male workers tend to more often be employed in skilled jobs. Thus before broad generalizations about age and visual problems associated with VDU can be made, the figures should be adjusted to take into account the comparative nature and skill level of the work being done at the VDU.
Eye defects and corrective lenses
In general, about half of all VDU operators display some kind of eye deficiency and most of these people use prescriptive lenses of one type or another. Often VDU user populations do not differ from the working population as far as eye defects and eye correction are concerned. For example, one survey (Rubino 1990) conducted among Italian VDU operators revealed that roughly 46% had normal vision and 38% were nearsighted (myopic), which is consistent with figures observed among Swiss and French VDU operators (Meyer and Bousquet 1990). Estimates of the prevalence of eye defects will vary according to the assessment technique used (Çakir 1981).
Most experts believe that presbyopia itself does not appear to have a significant influence on the incidence of asthenopia (persistent tiredness of the eyes). Rather, the use of unsuitable lenses appears to be likely to induce eye fatigue and discomfort. There is some disagreement about the effects in shortsighted young persons. Rubino has observed no effect while, according to Meyer and Bousquet (1990), myopic operators readily complain of undercorrection for the distance between eye and screen (usually 70 cm). Rubino also has proposed that people who suffer from a deficiency in eye coordination may be more likely to suffer from visual complaints in VDU work.
One interesting observation that resulted from a French study involving a thorough eye examination by ophthalmologists of 275 VDU operators and 65 controls was that 32% of those examined could have their vision improved by good correction. In this study 68% had normal vision, 24% were shortsighted and 8% farsighted (Boissin et al., 1991). Thus, although industrialized countries are, in general, well equipped to provide excellent eye care, eye correction is probably either completely neglected or inappropriate for those working at a VDU. An interesting finding in this study was that more cases of conjunctivitis were found in the VDU operators (48%) than in the controls. Since conjunctivitis and poor eyesight are correlated, this implies that better eye correction is needed.
Physical and Organizational Factors Affecting Visual Comfort
It is clear that in order to assess, correct and prevent visual discomfort in VDU work an approach which takes into account the many different factors described here and elsewhere in this chapter is essential. Fatigue and eye discomfort can be the result of individual physiological difficulties in normal accommodation and convergence in the eye, from conjunctivitis, or from wearing glasses that are poorly corrected for distance. Visual discomfort can be related to the workstation itself and can also be linked to work organization factors such as monotony and time spent on the job with and without a break. Inadequate lighting, reflections on screen, flicker and too much luminance of characters can also increase the risk of eye discomfort. Figure 1 illustrates some of these points.
Figure 1. Factors that increase the risk of eye fatigue among VDU workers
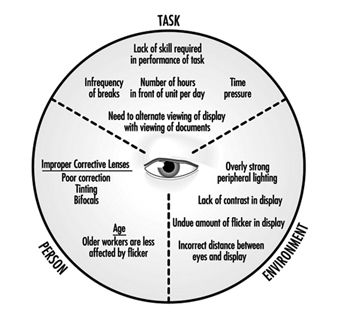
Many of the appropriate characteristics of workstation layout are described more fully earlier in the chapter.
The best viewing distance for visual comfort which still leaves enough space for the keyboard appears to be about 65 cm. However, according to many experts, such as Akabri and Konz (1991), ideally, “it would be best to determine an individual’s dark focus so workstations could be adjusted to specific individuals rather than population means”. As far as the characters themselves go, in general, a good rule of thumb is “bigger is better”. Usually, letter size increases with the size of the screen, and a compromise is always struck between the readability of letters and the number of words and sentences that can be displayed on the screen at one time. The VDU itself should be selected according to the task requirements and should try to maximize user comfort.
In addition to the design of the workstation and the VDU itself is the need to allow the eyes to rest. This is particularly important in unskilled jobs, in which the freedom of “moving around” is generally much lower than in skilled jobs. Data entry work or other activities of the same type are usually performed under time pressure, sometimes even accompanied by electronic supervision, which times operator output very precisely. In other interactive VDU jobs which involve using databases, operators are obliged to wait for a response from the computer and thus must remain at their posts.
Flicker and eye discomfort
Flicker is the change in brightness of the characters on the screen over time and is more fully described above. When characters do not refresh themselves frequently enough, some operators are able to perceive flicker. Younger workers may be more affected since their flicker fusion frequency is higher than that of older people (Grandjean 1987). The rate of flicker increases with increase in brightness, which is one reason why many VDU operators do not commonly make use of the whole range of brightness of the screen that are available. In general a VDU with a refresh rate of at least 70 Hz should “fit” the visual needs of a large proportion of VDU operators.
The sensitivity of the eyes to flicker is enhanced by increased brightness and contrast between the fluctuating area and the surrounding area. The size of the fluctuating area also affects sensitivity because the larger the area to be viewed, the larger the area of the retina that is stimulated. The angle at which the light from the fluctuating area strikes the eye and the amplitude of modulation of the fluctuating area are other important variables.
The older the VDU user, the less sensitive the eye because older eyes are less transparent and the retina is less excitable. This is also true in sick people. Laboratory findings such as these help to explain the observations made in the field. For example, it has been found that operators are disturbed by flicker from the screen when reading paper documents (Isensee and Bennett as quoted in Grandjean 1987), and the combination of fluctuation from the screen and fluctuation of fluorescent light has been found to be particularly disturbing.
Lighting
The eye functions best when the contrast between the visual target and its background is maximum, as for example, with a black letter on white paper. Efficiency is further enhanced when the outer edge of the visual field is exposed to slightly lower levels of brightness. Unfortunately, with a VDU the situation is just the reverse of this, which is one reason that so many VDU operators try to protect their eyes against excess light.
Inappropriate contrasts in brightness and unpleasant reflections produced by fluorescent light, for example, can lead to visual complaints among VDU operators. In one study, 40% of 409 VDU workers made such complaints (Läubli et al., 1989).
In order to minimize problems with lighting, just as with viewing distances, flexibility is important. One should be able to adapt light sources to the visual sensitivity of individuals. Workplaces should be provided to offer individuals the opportunity to adjust their lighting.
Job characteristics
Jobs which are carried out under time pressure, especially if they are unskilled and monotonous, are often accompanied by sensations of general fatigue, which, in turn, can give rise to complaints of visual discomfort. In the authors’ laboratory, it was found that visual discomfort increased with the number of accommodative changes the eyes needed to make to carry out the task. This occurred more often in data entry or word processing than in tasks which involved dialogues with the computer. Jobs which are sedentary and provide little opportunity for moving around also provide less opportunity for muscular recovery and hence enhance the likelihood of visual discomfort.
Job organization
Eye discomfort is just one aspect of the physical and mental problems that can be associated with many jobs, as described more fully elsewhere in this chapter. It is not surprising, therefore, to find a high correlation between the level of eye discomfort and job satisfaction. Although night work is still not widely practised in office work, its effects on eye discomfort in VDU work may well be unexpected. This is because, although there are few data as yet available to confirm this, on the one hand, eye capacity during the night shift may be somehow depressed and thus more vulnerable to VDU effects, while on the other hand, the lighting environment is easier to adjust without disturbance from natural lighting, provided that the reflections from fluorescent lamps on dark windows are eliminated.
Individuals who use VDUs to work at home should ensure that they provide themselves with the appropriate equipment and lighting conditions to avoid the adverse environmental factors found in many formal workplaces.
Medical Surveillance
No single, particular hazardous agent has been identified as a visual risk. Asthenopia among VDU operators appears rather to be an acute phenomenon, although there is some belief that sustained strain of accommodation may occur. Unlike many other chronic diseases, misadjustment to VDU work is usually noticed very soon by the “patient”, who may be more likely to seek medical care than will workers in other workplace situations. After such visits, spectacles are often prescribed, but unfortunately they are sometimes ill adapted to needs of the workplace which have been described here. It is essential that practitioners be specially trained to care for patients who work with VDUs. A special course, for example, has been created at the Swiss Federal Institute of Technology in Zurich just for this purpose.
The following factors must be taken into consideration in caring for VDU workers. In comparison to traditional office work, the distance between the eye and the visual target, the screen, is usually of 50 to 70 cm and cannot be changed. Therefore, lenses should be prescribed which take this steady viewing distance into account. Bifocal lenses are inappropriate because they will require a painful extension of the neck in order for the user to read the screen. Multifocal lenses are better, but as they limit rapid eye movements, their use can lead to more head movements, producing additional strain.
Eye correction should be as precise as possible, taking into account the slightest visual defects (e.g., astigmatism) and also the viewing distance of the VDU. Tinted glasses which reduce the illumination level in the centre of the visual field should not be prescribed. Partially tinted spectacles are not useful, since eyes at the workplace are always moving in all directions. Offering special spectacles to employees, however, should not mean that further complaints of visual discomfort from workers may be ignored since the complaints could be justified by poor ergonomic design of the workstation and equipment.
It should be said, finally, that the operators who suffer the most discomfort are those who need raised illumination levels for detail work and who, at the same time, have a higher glare sensitivity. Operators with undercorrected eyes will thus display a tendency to get closer to the screen for more light and will be in this way more exposed to flicker.
Screening and secondary prevention
The usual principles of secondary prevention in public health are applicable to the working environment. Screening therefore should be targeted towards known hazards and is most useful for diseases with long latency periods. Screening should take place prior to any evidence of preventable disease and only tests with high sensitivity, high specificity and high predictive power are useful. The results of screening examinations can be used to assess the extent of exposure both of individuals and of groups.
Since no severe adverse effects on the eye have ever been identified in VDU work, and since no hazardous level of radiations associated with visual problems have been detected, it has been agreed that there is no indication that work with VDUs “will cause disease or damage to the eye” (WHO 1987). The ocular fatigue and eye discomfort that have been reported to occur in VDU operators are not the kinds of health effect which generally form the basis for medical surveillance in a secondary prevention programme.
However, pre-employment visual medical examinations of VDU operators are widespread in most member countries of the International Labour Organization, a requirement supported by trade unions and employers (ILO 1986). In many European countries (including France, the Netherlands and the United Kingdom), medical surveillance for VDU operators, including ocular tests, has also been instituted subsequent to the issuing of Directive 90/270/EEC on work with display screen equipment.
If a programme for the medical surveillance of VDU operators is to be set up, the following issues must be addressed in addition to deciding on the contents of the screening programme and the appropriate testing procedures:
- What is the meaning of the surveillance and how should its results be interpreted?
- Are all VDU operators in need of the surveillance?
- Are any ocular effects which are observed appropriate for a secondary prevention programme?
Most routine visual screening tests available to the occupational physician have poor sensitivity and predictive power for eye discomfort associated with VDU work (Rey and Bousquet 1990). Snellen visual testing charts are particularly inappropriate for the measurement of visual acuity of VDU operators and for predicting their eye discomfort. In Snellen charts the visual targets are dark, precise letters on a clear, well illuminated background, not at all like typical VDU viewing conditions. Indeed, because of the inapplicability of other methods, a testing procedure has been developed by the authors (the C45 device) which simulates the reading and lighting conditions of a VDU workplace. Unfortunately, this remains for the time being a laboratory set-up. It is important to realise, however, that screening examinations are not a substitute for a well-designed workplace and good work organization.
Ergonomic Strategies to Reduce Visual Discomfort
Although systematic ocular screening and systematic visits to the eye specialist have not been shown to be effective in reducing visual symptomatology, they have been widely incorporated into occupational health programmes for VDU workers. A more cost-effective strategy could include an intensive ergonomic analysis of both the job and the workplace. Workers with known ocular diseases should try to avoid intensive VDU work as much as possible. Poorly corrected vision is another potential cause of operator complaints and should be investigated if such complaints occur. The improvement of the ergonomics of the workplace, which could include providing for a low reading angle to avoid a decreased blinking rate and neck extension, and providing the opportunity to rest and to move about on the job, are other effective strategies. New devices, with separate keyboards, allow distances to be adjusted. The VDU may also be made to be moveable, such as by placing it on a mobile arm. Eye strain will thus be reduced by permitting changes in viewing distance which match the corrections to the eye. Often the steps taken to reduce muscular pain in the arms, shoulders and back will at the same time also allow the ergonomist to reduce visual strain. In addition to the design of equipment, the quality of the air can affect the eye. Dry air leads to dry eyes, so that appropriate humidification is needed.
In general the following physical variables should be addressed:
- the distance between the screen and the eye
- the reading angle, which determines the position of the head and the neck
- the distance to walls and windows
- the quality of paper documents (often very poor)
- luminances of screen and surroundings (for artificial and natural lighting)
- flicker effects
- glare sources and reflections
- the humidity level.
Among the organizational variables that should be addressed in improving visual working conditions are:
- content of the task, responsibility level
- time schedules, night work, duration of work
- freedom to “move around”
- full time or part time jobs, etc.
Characteristics of Visual Display Workstations
Workstation Design
On workstations with visual display units
Visual displays with electronically generated images (visual display units or VDUs) represent the most characteristic element of computerized work equipment both in the workplace and in private life. A workstation may be designed to accommodate just a VDU and an input device (normally a keyboard), as a minimum; however, it can also provide room for diverse technical equipment including numerous screens, input and output devices, etc. As recently as the early 1980s, data entry was the most typical task for computer users. In many industrialized countries, however, this type of work is now performed by a relatively small number of users. More and more, journalists, managers and even executives have become “VDU users”.
Most VDU workstations are designed for sedentary work, but working in standing postures may offer some benefits for the users. Thus, there is some need for generic design guidelines applicable to simple and complex workstations used both while sitting and standing. Such guidelines will be formulated below and then applied to some typical workplaces.
Design guidelines
Workplace design and equipment selection should consider not only the needs of the actual user for a given task and the variability of users’ tasks during the relatively long life cycle of furniture (lasting 15 years or longer), but also factors related to maintenance or change of equipment. ISO Standard 9241, part 5, introduces four guiding principles to be applied to workstation design:
Guideline 1: Versatility and flexibility.
A workstation should enable its user to perform a range of tasks comfortably and efficiently. This guideline takes into account the fact that users’ tasks may vary often; thus, the chance of a universal adoption of guidelines for the workplace will be small.
Guideline 2: Fit.
The design of a workstation and its components should ensure a “fit” to be achieved for a variety of users and a range of task requirements. The concept of fit concerns the extent to which furniture and equipment can accommodate an individual user’s various needs, that is, to remain comfortable, free from visual discomfort and postural strain. If not designed for a specific user population, e.g., male European control room operators younger than 40 years of age, the workstation concept should ensure fit for the entire working population including users with special needs, e.g., handicapped persons. Most existing standards for furniture or the design of workplaces take only parts of the working population into consideration (e.g., “healthy” workers between the 5th and 95th percentile, aged between 16 and 60, as in German standard DIN 33 402), neglecting those who may need more attention.
Moreover, though some design practices are still based on the idea of an “average” user, an emphasis on individual fit is needed. With regard to workstation furniture, the fit required may be achieved by providing adjustability, designing a range of sizes, or even by custom-made equipment. Ensuring a good fit is crucial for the health and safety of the individual user, since musculoskeletal problems associated with the use of VDUs are common and significant.
Guideline 3: Postural change.
The design of the workstation should encourage movement, since static muscular load leads to fatigue and discomfort and may induce chronic musculoskeletal problems. A chair that allows easy movement of the upper half of the body, and provision of sufficient space to place and use paper documents as well as keyboards at varying positions during the day, are typical strategies for facilitating body movement while working with a VDU.
Guideline 4: Maintainability—adaptability.
The design of the workstation should take into consideration factors such as maintenance, accessibility, and the ability of the workplace to adapt to changing requirements, such as the ability to move the work equipment if a different task is to be performed. The objectives of this guideline have not received much attention in the ergonomics literature, because problems related to them are assumed to have been solved before users start to work at a workstation. In reality, however, a workstation is an ever-changing environment, and cluttered workspaces, partly or fully unsuitable for the tasks at hand, are very often not the result of their initial design process but are the outcome of later changes.
Applying the guidelines
Task analysis.
Workplace design should be preceded by a task analysis, which provides information about the primary tasks to be performed at the workstation and the equipment needed for them. In such an analysis, the priority given to information sources (e.g., paper-based documents, VDUs, input devices), the frequency of their use and possible restrictions (e.g., limited space) should be determined. The analysis should include major tasks and their relationships in space and time, visual attention areas (how many visual objects are to be used?) and the position and use of the hands (writing, typing, pointing?).
General design recommendations
Height of the work surfaces.
If fixed-height work surfaces are to be used, the minimum clearance between the floor and the surface should be greater than the sum of the popliteal height (the distance between the floor and the back of the knee) and thigh clearance height (sitting), plus allowance for footwear (25 mm for male users and 45 mm for female users). If the workstation is designed for general use, the popliteal height and thigh clearance height should be selected for the 95th percentile male population. The resulting height for the clearance under the desk surface is 690 mm for the population of Northern Europe and for North American users of European origin. For other populations, the minimum clearance needed is to be determined according to the anthropometric characteristics of the specific population.
If the legroom height is selected this way, the top of the work surfaces will be too high for a large proportion of intended users, and at least 30 per cent of them will need a footrest.
If work surfaces are adjustable in height, the required range for adjustment can be calculated from the anthropometric dimensions of female users (5th or 2.5th percentile for minimum height) and male users (95th or 97.5th percentile for maximum height). A workstation with these dimensions will in general be able to accommodate a large proportion of persons with little or no change. The result of such a calculation yields a range between 600 mm to 800 mm for countries with an ethnically varied user population. Since the technical realization of this range may cause some mechanical problems, best fit can also be achieved, for example, by combining adjustability with different size equipment.
The minimum acceptable thickness of the work surface depends on the mechanical properties of the material. From a technical point of view, a thickness between 14 mm (durable plastic or metal) and 30 mm (wood) is achievable.
Size and form of the work surface.
The size and the form of a work surface are mainly determined by the tasks to be performed and the equipment needed for those tasks.
For data entry tasks, a rectangular surface of 800 mm by 1200 mm provides sufficient space to place the equipment (VDU, keyboard, source documents and copy holder) properly and to rearrange the layout according to personal needs. More complex tasks may require additional space. Therefore, the size of the work surface should exceed 800 mm by 1,600 mm. The depth of the surface should allow placing the VDU within the surface, which means that VDUs with cathode ray tubes may require a depth of up to 1,000 mm.
In principle, the layout displayed in figure 1 gives maximum flexibility for organizing the workspace for various tasks. However, workstations with this layout are not easy to construct. Thus, the best approximation of the ideal layout is as displayed in figure 2. This layout allows arrangements with one or two VDUs, additional input devices and so on. The minimum area of the work surface should be larger than 1.3 m2.
Figure 1. Layout of a flexible workstation that can be adapted to fit the needs of users with different tasks
Arranging the workspace.
The spatial distribution of equipment in the workspace should be planned after a task analysis determining the importance and use frequency of each element has been conducted (table 1). The most frequently used visual display should be located within the central visual space, which is the shaded area of figure 3, while the most important and frequently used controls (such as the keyboard) should be located within optimum reach. In the workplace represented by the task analysis (table 1), the keyboard and the mouse are by far the most frequently handled pieces of equipment. Therefore, they should be given the highest priority within the reach area. Documents which are frequently consulted but do not need much handling should be assigned priority according to their importance (e.g., handwritten corrections). Placing them on the right-hand side of the keyboard would solve the problem, but this would create a conflict with the frequent use of the mouse which is also to be located to the right of the keyboard. Since the VDU may not need adjustment frequently, it can be placed to the right or left of the central field of vision, allowing the documents to be set on a flat document holder behind the keyboard. This is one possible, though not perfect, “optimized” solution.
Table 1. Frequency and importance of elements of equipment for a given task
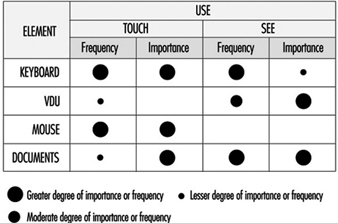
Figure 3. Visual workplace range
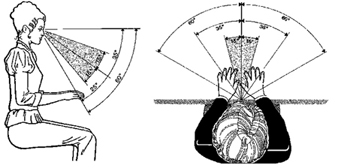
Since many elements of the equipment possess dimensions comparable to corresponding parts of the human body, using various elements within one task will always be associated with some problems. It also may require some movements between parts of the workstation; hence a layout like that shown in figure 1 is important for various tasks.
In the course of the last two decades, computer power that would have needed a ballroom at the beginning was successfully miniaturized and condensed into a simple box. However, contrary to the hopes of many practitioners that miniaturization of equipment would solve most problems associated with workplace layout, VDUs have continued to grow: in 1975, the most common screen size was 15"; in 1995 people bought 17" to 21”:monitors, and no keyboard has become much smaller than those designed in 1973. Carefully performed task analyses for designing complex workstations are still of growing importance. Moreover, although new input devices have emerged, they have not replaced the keyboard, and require even more space on the work surface, sometimes of substantial dimensions, e.g., graphic tablets in an A3-format.
Efficient space management within the limits of a workstation, as well as within work rooms, may help in developing acceptable workstations from an ergonomic point of view, thus preventing the emergence of various health and safety problems.
Efficient space management does not mean saving space at the expense of the usability of input devices and especially vision. Using extra furniture, such as a desk return, or a special monitor-holder clamped to the desk, may appear to be a good way to save desk space; however, it may be detrimental to posture (raised arms) and vision (raising the line of vision upwards from the relaxed position). Space-saving strategies should ensure that an adequate visual distance (approximately 600 mm to 800 mm) is maintained, as well as an optimum line-of-vision, obtained from an inclination of approximately 35º from the horizontal (20º head and 15º eyes).
New furniture concepts.
Traditionally, office furniture was adapted to the needs of businesses, supposedly reflecting the hierarchy of such organizations: large desks for executives working in “ceremonial” offices at one end of the scale, and small typists furniture for “functional” offices at the other. The basic design of office furniture did not change for decades. The situation changed substantially with the introduction of information technology, and a completely new furniture concept has emerged: that of systems furniture.
Systems furniture was developed when people realized that changes in working equipment and work organization could not be matched by the limited capabilities of existing furniture to adapt to new needs. Furniture today offers a tool-box that enables the user organizations to create workspace as needed, from a minimal space for just a VDU and a keyboard up to complex workstations that can accommodate various elements of equipment and possibly also groups of users. Such furniture is designed for change and incorporates efficient and flexible cable management facilities. While the first generation of systems furniture did not do much more than add an auxiliary desk for the VDU to an existing desk, the third generation has completely broken its ties to the traditional office. This new approach offers great flexibility in designing workspaces, limited only by the available space and the abilities of organizations to use this flexibility.
Radiation
Radiation in the context of VDU applications
Radiation is the emission or transfer of radiant energy. The emission of radiant energy in the form of light as the intended purpose for the use of VDUs may be accompanied by various unwanted by-products such as heat, sound, infrared and ultraviolet radiation, radio waves or x rays, to name a few. While some forms of radiation, like visible light, may affect humans in a positive way, some emissions of energy can have negative or even destructive biological effects, especially when the intensity is high and the duration of exposure is long. Some decades ago exposure limits for different forms of radiation were introduced to protect people. However, some of these exposure limits are questioned today, and, for low frequency alternating magnetic fields, no exposure limit can be given based on levels of natural background radiation.
Radiofrequency and microwave radiation from VDUs
Electromagnetic radiation with a frequency range from a few kHz to 109 Hertz (the so-called radiofrequency, or RF, band, with wavelengths ranging from some km to 30 cm) can be emitted by VDUs; however, the total energy emitted depends on the characteristics of the circuitry. In practice, however, the field strength of this type of radiation is likely to be small and confined to the immediate vicinity of the source. A comparison of the strength of alternating electric fields in the range of 20 Hz to 400 kHz indicates that VDUs using cathode ray tube (CRT) technology emit, in general, higher levels than other displays.
“Microwave” radiation covers the region between 3x108 Hz to 3x1011 Hz (wavelengths 100 cm to 1 mm). There are no sources of microwave radiation in VDUs that emit a detectable amount of energy within this band.
Magnetic fields
Magnetic fields from a VDU originate from the same sources as alternating electric fields. Although magnetic fields are not “radiation”, alternating electric and magnetic fields cannot be separated in practice, since one induces the other. One reason why magnetic fields are discussed separately is that they are suspected to have teratogenic effects (see discussion later in this chapter).
Although the fields induced by VDUs are weaker than those induced by some other sources, such as high-voltage power lines, power plants, electrical locomotives, steel ovens and welding equipment, the total exposure produced by VDUs may be similar since people may work eight or more hours in the vicinity of a VDU but seldom near power lines or electric motors. The question of the relationship between electromagnetic fields and cancer, however, is still a matter for debate.
Optical radiation
“Optical” radiation covers visible radiation (i.e., light) with wavelengths from 380 nm (blue) to 780 nm (red), and the neighbouring bands in the electromagnetic spectrum (infrared from 3x1011 Hz to 4x1014 Hz, wavelengths from 780 nm to 1 mm; ultraviolet from 8x1014 Hz to 3x1017 Hz). Visible radiation is emitted at moderate levels of intensity comparable with that emitted by room surfaces (»100 cd/m2). However, ultraviolet radiation is trapped by the glass of the tube face (CRTs) or not emitted at all (other display technologies). Levels of ultraviolet radiation, if detectable at all, stay well below occupational exposure standards, as do those of infrared radiation.
X rays
CRTs are well-known sources of x rays, while other technologies like liquid crystal displays (LCDs) do not emit any. The physical processes behind emissions of this type of radiation are well understood, and tubes and circuitry are designed to keep the emitted levels far below the occupational exposure limits, if not below detectable levels. Radiation emitted by a source can only be detected if its level exceeds the background level. In the case of x rays, as for other ionizing radiation, the background level is provided by cosmic radiation and by radiation from radioactive materials in the ground and in buildings. In normal operation, a VDU does not emit x rays exceeding the background level of radiation (50 nGy/h).
Radiation recommendations
In Sweden, the former MPR (Statens Mät och Provråd, the National Council for Metrology and Testing) organization, now SWEDAC, has worked out recommendations for evaluating VDUs. One of their main objectives was to limit any unwanted by-product to levels that can be achieved by reasonable technical means. This approach goes beyond the classical approach of limiting hazardous exposures to levels where the likelihood of an impairment of health and safety seems to be acceptably low.
At the beginning, some recommendations of MPR led to the unwanted effect of reducing the optical quality of CRT displays. However, at present, only very few products with extremely high resolution may suffer any degradation if the manufacturer attempts to comply with the MPR (now MPR-II). The recommendations include limits for static electricity, magnetic and electric alternating fields, visual parameters, etc.
Image Quality
Definitions for image quality
The term quality describes the fit of distinguishing attributes of an object for a defined purpose. Thus, the image quality of a display includes all properties of the optical representation regarding the perceptibility of symbols in general, and the legibility or readability of alphanumeric symbols. In this sense, optical terms used by tube manufacturers, like resolution or minimum spot size, describe basic quality criteria concerning the abilities of a given device for displaying thin lines or small characters. Such quality criteria are comparable with the thickness of a pencil or brush for a given task in writing or painting.
Some of the quality criteria used by ergonomists describe optical properties that are relevant for legibility, e.g., contrast, while others, like character size or stroke width, refer more to typographical features. In addition, some technology-dependent features like the flicker of images, the persistence of images, or the uniformity of contrast within a given display are also considered in ergonomics (see figure 4).
Figure 4. Criteria for image evaluation
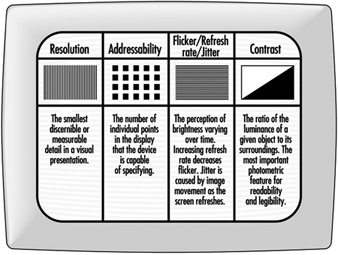
Typography is the art of composing “type”, which is not only shaping the fonts, but also selecting and setting of type. Here, the term typography is used in the first meaning.
Basic characteristics
Resolution.
Resolution is defined as the smallest discernible or measurable detail in a visual presentation. For example, the resolution of a CRT display can be expressed by the maximum number of lines that can be displayed in a given space, as usually done with the resolution of photographic films. One can also describe the minimum spot size that a device can display at a given luminance (brightness). The smaller the minimum spot, the better the device. Thus, the number of dots of minimum size (picture elements—also known as pixels) per inch (dpi) represents the quality of the device, e.g., a 72 dpi device is inferior to a 200 dpi display.
In general, the resolution of most computer displays is well below 100 dpi: some graphic displays may achieve 150 dpi, however, only with limited brightness. This means, if a high contrast is required, the resolution will be lower. Compared with the resolution of print, e.g., 300 dpi or 600 dpi for laser printers, the quality of VDUs is inferior. (An image with 300 dpi has 9 times more elements in the same space than a 100 dpi image.)
Addressability.
Addressability describes the number of individual points in the field that the device is capable of specifying. Addressability, which is very often confused with resolution (sometimes deliberately), is one specification given for devices: “800 x 600” means that the graphic board can address 800 points on every one of 600 horizontal lines. Since one needs at least 15 elements in the vertical direction to write numbers, letters and other characters with ascenders and descenders, such a screen can display a maximum of 40 lines of text. Today, the best available screens can address 1,600 x 1,200 points; however, most displays used in industry address 800 x 600 points or even less.
On displays of the so-called “character-oriented” devices, it is not dots (points) of the screen that are addressed but character boxes. In most such devices, there are 25 lines with 80 character positions each in the display. On these screens, each symbol occupies the same space regardless of its width. In industry the lowest number of pixels in a box is 5 wide by 7 high. This box allows both upper and lower case characters, although the descenders in “p”, “q” and “g”, and the ascenders above “Ä” or “Á” cannot be displayed. Considerably better quality is provided with the 7 x 9 box, which has been “standard” since the mid-1980s. To achieve good legibility and reasonably good character shapes, the character box size should be at least 12 x 16.
Flicker and refresh rate.
The images on CRTs and on some other types of VDU are not persistent images, as on paper. They only appear to be steady by taking advantage of an artefact of the eye. This, however, is not without penalty, since the screen tends to flicker if the image is not refreshed constantly. Flicker can influence both performance and comfort of the user and should always be avoided.
Flicker is the perception of brightness varying over time. The severity of flicker depends on various factors such as the characteristics of the phosphor, size and brightness of the flickering image, etc. Recent research shows that refresh rates up to 90 Hz may be needed to satisfy 99 per cent of users, while in earlier research, refresh rates well below 50 Hz were thought to be satisfactory. Depending on various features of the display, a flicker-free image may be achieved by refresh rates between 70 Hz and 90 Hz; displays with a light background (positive polarity) need a minimum of 80 Hz to be perceived as flicker-free.
Some modern devices offer an adjustable refresh rate; unfortunately, higher refresh rates are coupled with lower resolution or addressability. The ability of a device to display high “resolution” images with high refresh rates can be assessed by its video bandwidth. For displays with high quality, the maximum video bandwidth lies above 150 MHz, while some displays offer less than 40 MHz.
To achieve a flicker-free image and a high resolution with devices with lower video bandwidth, the manufacturers apply a trick that stems from commercial TV: the interlace mode. In this case, every second line on the display is refreshed with a given frequency. The result, however, is not satisfactory if static images, such as text and graphics, are displayed and the refresh rate is below 2 x 45 Hz. Unfortunately, the attempt to suppress the disturbing effect of flicker may induce some other negative effects.
Jitter.
Jitter is the result of spatial instability of the image; a given picture element is not displayed at the same location on the screen after each refresh process. The perception of jitter cannot be separated from the perception of flicker.
Jitter may have its cause in the VDU itself, but it can also be induced by interaction with other equipment at the workplace, such as a printer or other VDUs or devices that generate magnetic fields.
Contrast.
Brightness contrast, the ratio of the luminance of a given object to its surroundings, represents the most important photometric feature for readability and legibility. While most standards require a minimum ratio of 3:1 (bright characters on dark background) or 1:3 (dark characters on bright background), optimum contrast is actually about 10:1, and devices of good quality achieve higher values even in bright environments.
The contrast of “active” displays is impaired when the ambient light is increased, while “passive” displays (e.g., LCDs) lose contrast in dark environments. Passive displays with background lighting may offer good visibility in all environments under which people may work.
Sharpness.
Sharpness of an image is a well-known, but still ill-defined feature. Hence, there is no agreed-upon method to measure sharpness as a relevant feature for legibility and readability.
Typographical features
Legibility and readability.
Readability refers to whether a text is understandable as a series of connected images, while legibility refers to the perception of single or grouped characters. Thus, good legibility is, in general, a precondition for readability.
Legibility of text depends on several factors: some have been investigated thoroughly, while other relevant factors like character shapes are yet to be classified. One of the reasons for this is that the human eye represents a very powerful and robust instrument, and the measures used for performance and error rates often do not help to distinguish between different fonts. Thus, to some extent, typography still remains an art rather than a science.
Fonts and readability.
A font is a family of characters, designed to yield either optimum readability on a given medium, e.g., paper, electronic display or projection display, or some desired aesthetic quality, or both. While the number of available fonts exceeds ten thousand, only a few fonts, numbered in tens, are believed to be “readable”. Since legibility and readability of a font are also affected by the experience of the reader—some “legible” fonts are believed to have become so because of decades or even centuries of use without changing their shape—the same font may be less legible on a screen than on paper, merely because its characters look “new”. This, however, is not the main reason for the poor legibility of screens.
In general, the design of screen fonts is restricted by shortcomings in technology. Some technologies impose very narrow limits on the design of characters, e.g., LEDs or other rastered screens with limited numbers of dots per display. Even the best CRT displays can seldom compete with print (figure 5). In the last years, research has shown that speed and accuracy of reading on screens is about 30% lower than on paper, but whether this is due to features of the display or to other factors is not yet known.
Figure 5. Appearance of a letter at various screen resolutions and on paper (right)

Characteristics with measurable effects.
The effects of some characteristics of alphanumeric representations are measurable, e.g., apparent size of the characters, height/width ratio, stroke width/size ratio, line, word and character spacing.
The apparent size of the characters, measured in minutes of arc, shows an optimum by 20' to 22'; this corresponds to about 3 mm to 3.3 mm in height under normal viewing conditions in offices. Smaller characters may lead to increased errors, visual strain, and also to more postural strain due to restricted viewing distance. Thus, text should not be represented in an apparent size of less than 16'.
However, graphical representations may require text of smaller size to be displayed. To avoid errors, on the one hand, and a high visual load for the user on the other, parts of the text to be edited should be displayed in a separate window to assure good readability. Characters with an apparent size of less than 12' should not be displayed as readable text, but replaced by a rectangular grey block. Good programs allow the user to select the minimum actual size of characters that are to be displayed as alphanumerics.
The optimum height/width ratio of characters is about 1:0.8; legibility is impaired if the ratio is above 1:0.5. For good legible print and also for CRT screens, the ratio of character height to stroke width is about 10:1. However, this is only a rule of thumb; legible characters of high aesthetical value often show different stroke widths (see figure 5).
Optimal line spacing is very important for readability, but also for space saving, if a given amount of information is to be displayed in limited space. The best example for this is the daily newspaper, where an enormous amount of information is displayed within a page, but is still readable. The optimum line spacing is about 20% of character height between the descenders of a line and the ascenders of the next; this is a distance of about 100% of the character height between the baseline of a line of text and the ascenders of the next. If the length of the line is reduced, the space between the lines may be reduced, too, without losing readability.
Character spacing is invariable on character-oriented screens, making them inferior in readability and aesthetic quality to displays with variable space. Proportional spacing depending on the shape and width of the characters is preferable. However, a typographical quality comparable to well-designed printed fonts is achievable only on few displays and when using specific programs.
Ambient Lighting
The specific problems of VDU workstations
During the last 90 years of industrial history, the theories about the lighting of our workplaces have been governed by the notion that more light will improve vision, reduce stress and fatigue, as well as enhance performance. “More light”, correctly speaking “more sunlight”, was the slogan of people in Hamburg, Germany, more than 60 years ago when they took to the streets to fight for better and healthier homes. In some countries like Denmark or Germany, workers today are entitled to have some daylight at their workplaces.
The advent of information technology, with the emergence of the first VDUs in working areas, was presumably the first event ever when workers and scientists began to complain about too much light in working areas. The discussion was fuelled by the easily detectable fact that most VDUs were equipped with CRTs, which have curved glass surfaces prone to veiling reflections. Such devices, sometimes called “active displays”, lose contrast when the level of ambient lighting becomes higher. Redesigning lighting to reduce the visual impairments caused by these effects, however, is complicated by the fact that most users also use paper-based information sources, which generally require increased levels of ambient light for good visibility.
The role of ambient light
Ambient light found in the vicinity of VDU workstations serves two different purposes. First, it illuminates the workspace and working materials like paper, telephones, etc. (primary effect). Secondly, it illuminates the room, giving it its visible shape and giving the users the impression of a light surrounding (secondary effect). Since most lighting installations are planned according to the concept of general lighting, the same lighting sources serve both purposes. The primary effect, illuminating passive visual objects to make them visible or legible, became questionable when people started to use active screens that do not need ambient light to be visible. The remaining benefit of the room lighting was reduced to the secondary effect, if the VDU is the major source of information.
The function of VDUs, both of CRTs (active displays) and of LCDs (passive displays), is impaired by the ambient light in specific ways:
CRTs:
- The curved glass surface reflects bright objects in the environment, and forms a kind of visual “noise”.
- Depending on the intensity of ambient illumination, the contrast of displayed objects is reduced to a degree that readability or legibility of the objects is impaired.
- Images on colour CRTs suffer a twofold degradation: First, the brightness contrast of all displayed objects is reduced, as on monochrome CRTs. Secondly, the colours are changed so that colour contrast is also reduced. In addition, the number of distinguishable colours is reduced.
LCDs (and other passive displays):
- The reflections on LCDs cause less concern than those on CRT surfaces, since these displays have flat surfaces.
- In contrast to active displays, LCDs (without backlight) lose contrast under low levels of ambient illumination.
- Due to poor directional characteristics of some display technologies, visibility or legibility of displayed objects is substantially reduced if the main direction of light incidence is unfavourable.
The extent to which such impairments exert a stress on users or lead to a substantial reduction of visibility/readability/legibility of visual objects in real working environments varies greatly. For example, the contrast of alphanumeric characters on monochrome (CRT) displays is reduced in principle, but, if the illuminance on the screen is ten times higher than in normal working environments, many screens will still have a contrast sufficient to read alphanumeric characters. On the other hand, colour displays of computer-aided design (CAD) systems decrease substantially in visibility so that most users prefer to dim the artificial lighting or even to switch it off, and, in addition, to keep the daylight out of their working area.
Possible remedies
Changing illuminance levels.
Since 1974, numerous studies have been performed which led to recommendations for reducing illuminance at the workplace. However, these recommendations were mostly based on studies with unsatisfactory screens. The recommended levels were between 100 lux and 1,000 lx, and generally, levels well below the recommendations of the existing standards for office lighting (e.g., 200 lx or 300 to 500 lx) have been discussed.
When positive screens with a luminance of approximately 100 cd/m2 brightness and some kind of efficient anti-glare treatment are used, the utilization of a VDU does not limit the acceptable illuminance level, since users find illuminance levels up to 1,500 lx acceptable, a value which is very rare in working areas.
If the relevant characteristics of the VDUs do not allow comfortable working under normal office lighting, as can occur when working with storage tubes, microimage readers, colour screens etc., the visual conditions can be improved substantially by introducing two-component lighting. Two-component lighting is a combination of indirect room lighting (secondary effect) and direct task lighting. Both components should be controllable by the users.
Controlling glare on screens.
Controlling glare on screens is a difficult task since almost all remedies that improve the visual conditions are likely to impair some other important characteristic of the display. Some remedies, proposed for many years, such as mesh filters, remove reflections from the displays but they also impair the legibility of the display. Low luminance luminaires cause less reflected glare on screens, but the quality of such lighting generally is judged by users to be worse than that of any other type of lighting.
For this reason, any measures (see figure 6) should be applied cautiously, and only after analysing the real cause of the annoyance or disturbance. Three possible ways of controlling glare on screens are: selection of the correct location of the screen with respect to glare sources; selection of suitable equipment or addition of elements to it; and use of lighting. The costs of the measures to be taken are of the same order: it costs almost nothing to place screens in such a way as to eliminate reflected glare. However, this may not be possible in all cases; thus, equipment-related measures will be more expensive but may be necessary in various working environments. Glare control by lighting is often recommended by lighting specialists; however, this method is the most expensive but not the most successful way of controlling glare.
Figure 6. Strategies for controlling glare on screens
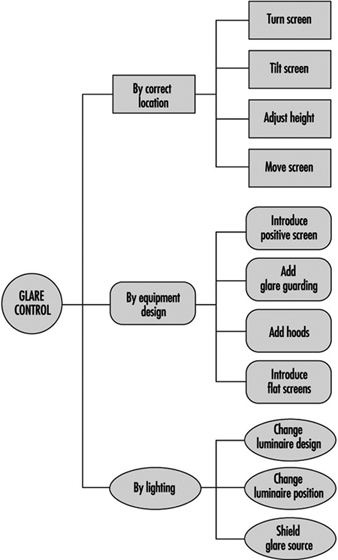
The most promising measure at present is the introduction of positive screens (displays with bright background) with an additional anti-glare treatment for the glass surface. Even more successful than this will be the introduction of flat screens with a nearly matt surface and bright background; such screens, however, are not available for general use today.
Adding hoods to displays is the ultima ratio of the ergonomists for difficult work environments like production areas, towers of airports or operator cabins of cranes, etc. If hoods are really needed, it is likely that there will be more severe problems with lighting than just reflected glare on visual displays.
Changing luminaire design is mainly accomplished in two ways: first, by reducing the luminance (corresponds to apparent brightness) of parts of the light fittings (so called “VDU lighting”), and secondly, by introducing indirect light instead of direct light. The results of current research show that introducing indirect light yields substantial improvements for users, reduces visual load, and is well accepted by users.
Overview
New information technologies are being introduced in all industrial sectors, albeit to varying extents. In some cases, the costs of computerizing production processes may constitute an impediment to innovation, particularly in small and medium-sized companies and in developing countries. Computers make possible the rapid collection, storage, processing and dissemination of large quantities of information. Their utility is further enhanced by their integration into computer networks, which allow resources to be shared (Young 1993).
Computerization exerts significant effects on the nature of employment and on working conditions. Beginning about the mid-1980s, it was recognized that workplace computerization may lead to changes in task structure and work organization, and by extension to work requirements, career planning and stress suffered by production and management personnel. Computerization may exert positive or negative effects on occupational health and safety. In some cases, the introduction of computers has rendered work more interesting and resulted in improvements in the work environment and reductions of workload. In others, however, the result of technological innovation has been an increase in the repetitive nature and intensity of tasks, a reduction of the margin for individual initiative and the isolation of the worker. Furthermore, several companies have been reported to increase the number of work shifts in an attempt to extract the largest possible economic benefit from their financial investment (ILO 1984).
As far as we have been able to determine, as of 1994 statistics on the worldwide use of computers are available from one source only—The Computer Industry Almanac (Juliussen and Petska-Juliussen 1994). In addition to statistics on the current international distribution of computer use, this publication also reports the results of retrospective and prospective analyses. The figures reported in the latest edition indicate that the number of computers is increasing exponentially, with the increase becoming particularly marked at the beginning of the 1980s, the point at which personal computers began to attain great popularity. Since 1987, total computer processing power, measured in terms of the number of million instructions per second executed (MIPS) has increased 14-fold, thanks to the development of new microprocessors (transistor components of microcomputers which perform arithmetical and logical calculations). By the end of 1993, total computing power attained 357 million MIPS.
Unfortunately, available statistics do not differentiate between computers used for work and personal purposes, and statistics are unavailable for some industrial sectors. These knowledge gaps are most likely due to methodological problems related to the collection of valid and reliable data. However, reports of the International Labour Organization’s tripartite sectoral committees contain relevant and comprehensive information on the nature and extent of the penetration of new technologies in various industrial sectors.
In 1986, 66 million computers were in use throughout the world. Three years later, there were more than 100 million, and by 1997, it is estimated that 275–300 million computers will be in use, with this number reaching 400 million by 2000. These predictions assume the widespread adoption of multimedia, information highway, voice recognition and virtual reality technologies. The Almanac’s authors consider that most televisions will be equipped with personal computers within ten years of publication, in order to simplify access to the information highway.
According to the Almanac, in 1993 the overall computer: population ratio in 43 countries in 5 continents was 3.1 per 100. It should however be noted that South Africa was the only African country reporting and that Mexico was the only Central American country reporting. As the statistics indicate, there is a very wide international variation in the extent of computerization, the computer:population ratio ranging from 0.07 per 100 to 28.7 per 100.
The computer:population ratio of less than 1 per 100 in developing countries reflects the generally low level of computerization prevailing there (table 1) (Juliussen and Petska-Juliussen 1994). Not only do these countries produce few computers and little software, but lack of financial resources may in some cases prevent them from importing these products. Moreover, their often rudimentary telephone and electrical utilities are often barriers to more widespread computer use. Finally, little linguistically and culturally appropriate software is available, and training in computer-related fields is often problematic (Young 1993).
Table 1. Distribution of computers in various regions of the world
|
REGION |
COMPUTERS PER 100 PEOPLE |
|
NORTH AMERICA |
|
|
United States |
28.7 |
|
Canada |
8.8 |
|
CENTRAL AMERICA |
|
|
Mexico |
1.7 |
|
SOUTH AMERICA |
|
|
Argentina |
1.3 |
|
Brazil |
0.6 |
|
Chile |
2.6 |
|
Venezuela |
1.9 |
|
WESTERN EUROPE |
|
|
Austria |
9.5 |
|
Belgium |
11.7 |
|
Denmark |
16.8 |
|
Finland |
16.7 |
|
France |
12.9 |
|
Germany |
12.8 |
|
Greece |
2.3 |
|
Ireland |
13.8 |
|
Italy |
7.4 |
|
Netherlands |
13.6 |
|
Norway |
17.3 |
|
Portugal |
4.4 |
|
Spain |
7.9 |
|
Sweden |
15 |
|
Switzerland |
14 |
|
United Kingdom |
16.2 |
|
EASTERN EUROPE |
|
|
Czech Republic |
2.2 |
|
Hungary |
2.7 |
|
Poland |
1.7 |
|
Russian Federation |
0.78 |
|
Ukraine |
0.2 |
|
OCEANIA |
|
|
Australia |
19.2 |
|
New Zealand |
14.7 |
|
AFRICA |
|
|
South Africa |
1 |
|
ASIA |
|
|
China |
0.09 |
|
India |
0.07 |
|
Indonesia |
0.17 |
|
Israel |
8.3 |
|
Japan |
9.7 |
|
Korea, Republic of |
3.7 |
|
Phillipines |
0.4 |
|
Saudi Arabia |
2.4 |
|
Singapore |
12.5 |
|
Taiwan |
7.4 |
|
Thailand |
0.9 |
|
Turkey |
0.8 |
|
Less than 1 |
1 - 5 6 - 10 11 - 15 16-20 21 - 30 |
Source: Juliussen and Petska-Juliussen 1994.
Computerization has significantly increased in the countries of the former Soviet Union since the end of the Cold War. The Russian Federation, for example, is estimated to have increased its stock of computers from 0.3 million in 1989 to 1.2 million in 1993.
The largest concentration of computers is found in the industrialized countries, especially in North America, Australia, Scandinavia and Great Britain (Juliussen and Petska-Juliussen 1994). It was principally in these countries that the first reports of visual display unit (VDU) operators’ fears regarding health risks appeared and the initial research aimed at determining the prevalence of health effects and identifying risk factors undertaken. The health problems studied fall into the following categories: visual and ocular problems, musculoskeletal problems, skin problems, reproductive problems, and stress.
It soon became evident that the health effects observed among VDU operators were dependent not only on screen characteristics and workstation layout, but also on the nature and structure of tasks, organization of work and manner in which the technology was introduced (ILO 1989). Several studies have reported a higher prevalence of symptoms among female VDU operators than among male operators. According to recent studies, this difference is more reflective of the fact that female operators typically have less control over their work than do their male counterparts than of true biological differences. This lack of control is thought to result in higher stress levels, which in turn result in increased symptom prevalence in female VDU operators.
VDUs were first introduced on a widespread basis in the tertiary sector, where they were used essentially for office work, more specifically data entry and word processing. We should not therefore be surprised that most studies of VDUs have focused on office workers. In industrialized countries, however, computerization has spread to the primary and secondary sectors. In addition, although VDUs were used almost exclusively by production workers, they have now penetrated to all organizational levels. In recent years, researchers have therefore begun to study a wider range of VDU users, in an attempt to overcome the lack of adequate scientific information on these situations.
Most computerized workstations are equipped with a VDU and a keyboard or mouse with which to transmit information and instructions to the computer. Software mediates information exchange between the operator and the computer and defines the format with which information is displayed on the screen. In order to establish the potential hazards associated with VDU use, it is first necessary to understand not only the characteristics of the VDU but also those of the other components of the work environment. In 1979, Çakir, Hart and Stewart published the first comprehensive analysis in this field.
It is useful to visualize the hardware used by VDU operators as nested components that interact with each other (IRSST 1984). These components include the terminal itself, the workstation (including work tools and furniture), the room in which the work is carried out, and the lighting. The second article in this chapter reviews the main characteristics of workstations and their lighting. Several recommendations aimed at optimizing working conditions while taking into account individual variations and variations in tasks and work organization are offered. Appropriate emphasis is placed on the importance of choosing equipment and furniture which allow flexible layouts. This flexibility is extremely important in light of international competition and rapidly evolving technological development that are constantly driving companies to introduce innovations and while simultaneously forcing them to adapt to the changes these innovations bring.
The next six articles discuss health problems studied in response to fears expressed by VDU operators. The relevant scientific literature is reviewed and the value and limitations of research results highlighted. Research in this field draws upon numerous disciplines, including epidemiology, ergonomics, medicine, engineering, psychology, physics and sociology. Given the complexity of the problems and more specifically their multifactorial nature, the necessary research has often been conducted by multidisciplinary research teams. Since the 1980s, these research efforts have been complemented by regularly organized international congresses such as Human-Computer Interaction and Work with Display Units, which provide an opportunity to disseminate research results and promote the exchange of information between researchers, VDU designers, VDU producers and VDU users.
The eighth article discusses human-computer interaction specifically. The principles and methods underlying the development and evaluation of interface tools are presented. This article will prove useful not only to production personnel but also those interested in the criteria used to select interface tools.
Finally, the ninth article reviews international ergonomic standards as of 1995, related to the design and layout of computerized workstations. These standards have been produced in order to eliminate the hazards to which VDU operators can be exposed in the course of their work. The standards provide guidelines to companies producing VDU components, employers responsible for the purchase and layout of workstations, and employees with decision-making responsibilities. They may also prove useful as tools with which to evaluate existing workstations and identify modifications required in order to optimize operators’ working conditions.
Organizing for Fire Protection
Private Emergency Organization
Profit is the main objective of any industry. To achieve this objective, an efficient and alert management and continuity of production are essential. Any interruption in production, for any reason, will adversely affect profits. If the interruption is the result of a fire or explosion, it may be long and may cripple the industry.
Very often, a plea is taken that the property is insured and loss due to fire, if any, will be indemnified by the insurance company. It must be appreciated that insurance is only a device to spread the effect of the destruction brought by fire or explosion on as many people as possible. It cannot make good the national loss. Besides, insurance is no guarantee of continuity of production and elimination or minimization of consequential losses.
What is indicated, therefore, is that the management must gather complete information on the fire and explosion hazard, evaluate the loss potential and implement suitable measures to control the hazard, with a view to eliminating or minimizing the incidence of fire and explosion. This involves the setting up of a private emergency organization.
Emergency Planning
Such an organization must, as far as possible, be considered from the planning stage itself, and implemented progressively from the time of selection of site until production has started, and then continued thereafter.
Success of any emergency organization depends to a large extent on the overall participation of all workers and various echelons of the management. This fact must be borne in mind while planning the emergency organization.
The various aspects of emergency planning are mentioned below. For more details, a reference may be made to the US National Fire Protection Association (NFPA) Fire Protection Handbook or any other standard work on the subject (Cote 1991).
Stage 1
Initiate the emergency plan by doing the following:
- Identify and evaluate fire and explosion hazards associated with the transportation, handling and storage of each raw material, intermediate and finished products and each industrial process, as well as work out detailed preventive measures to counteract the hazards with a view to eliminating or minimizing them.
- Work out the requirements of fire protection installations and equipment, and determine the stages at which each is to be provided.
- Prepare specifications for the fire protection installation and equipment.
Stage 2
Determine the following:
- availability of adequate water supply for fire protection in addition to the requirements for processing and domestic use
- susceptibility of site and natural hazards, such as floods, earthquakes, heavy rains, etc.
- environments, i.e., the nature and extent of surrounding property and the exposure hazard involved in the event of a fire or explosion
- existence of private (works) or public fire brigade(s), the distance at which such fire brigade(s) is (are) located and the suitability of the appliances available with them for the risk to be protected and whether they can be called upon to assist in an emergency
- response from the assisting fire brigade(s) with particular reference to impediments, such as railway crossings, ferries, inadequate strength and (or) width of bridges in relation to the fire appliances, difficult traffic, etc.
- socio-political environment , i.e., incidence of crime, and political activities leading to law-and-order problems.
Stage 3
Prepare the layout and building plans, and the specifications of construction material. Carry out the following tasks:
- Limit the floor area of each shop, workplace, etc. by providing fire walls, fire doors, etc.
- Specify the use of fire-resistant materials for construction of building or structure.
- Ensure that steel columns and other structural members are not exposed.
- Ensure adequate separation between building, structures and plant.
- Plan installation of fire hydrants, sprinklers, etc. where necessary.
- Ensure the provision of adequate access roads in the layout plan to enable fire appliances to reach all parts of the premises and all sources of water for fire-fighting.
Stage 4
During construction, do the following:
- Acquaint the contractor and his or her employees with the fire risk management policies, and enforce compliance.
- Thoroughly test all fire protection installations and equipment before acceptance.
Stage 5
If the size of the industry, its hazards or its out-of-the-way location is such that a full-time fire brigade must be available on the premises, then organize, equip and train the required full-time personnel. Also appoint a full-time fire officer.
Stage 6
To ensure full participation of all employees, do the following:
- Train all personnel in the observance of precautionary measures in their day-to-day work and the action required of them upon an outbreak of fire or explosion. The training must include operation of fire-fighting equipment.
- Ensure strict observance of fire precautions by all concerned personnel through periodic reviews.
- Ensure regular inspection and maintenance of all fire protection systems and equipment. All defects must be rectified promptly.
Managing the emergency
To avoid confusion at the time of an actual emergency, it is essential that everyone in the organization knows the precise part that he (she) and others are expected to play during the emergency. A well-thought-out emergency plan must be prepared and promulgated for this purpose, and all concerned personnel must be made fully familiar with it. The plan must clearly and unambiguously lay down the responsibilities of all concerned and also specify a chain of command. As a minimum, the emergency plan should include the following:
1. name of the industry
2. address of the premises, with telephone number and a site plan
3. purpose and objective of the emergency plan and effective date of its coming in force
4. area covered, including a site plan
5. emergency organization, indicating chain of command from the work manager on downwards
6. fire protection systems, mobile appliances and portable equipment, with details
7. details of assistance availability
8. fire alarm and communication facilities
9. action to be taken in an emergency. Include separately and unambiguously the action to be taken by:
- the person discovering the fire
- the private fire brigade on the premises
- head of the section involved in the emergency
- heads of other sections not actually involved in theemergency
- the security organization
- the fire officer, if any
- the works manager
- others
10. chain of command at the scene of incident. Consider all possible situations, and indicate clearly who is to assume command in each case, including the circumstances under which another organization is to be called in to assist.
11. action after a fire. Indicate responsibility for:
- recommissioning or replenishing of all fire protectionsystems, equipment and water sources
- investigating the cause of fire or explosion
- preparation and submission of reports
- initiating remedial measures to prevent re-occurrence of similar emergency.
When a mutual assistance plan is in operation, copies of emergency plan must be supplied to all participating units in return for similar plans of their respective premises.
Evacuation Protocols
A situation necessitating the execution of the emergency plan may develop as a result of either an explosion or a fire.
Explosion may or may not be followed by fire, but in almost all cases, it produces a shattering effect, which may injure or kill personnel present in the vicinity and/or cause physical damage to property, depending upon the circumstances of each case. It may also cause shock and confusion and may necessitate the immediate shut-down of the manufacturing processes or a portion thereof, along with the sudden movement of a large number of people. If the situation is not controlled and guided in an orderly manner immediately, it may lead to panic and further loss of life and property.
Smoke given out by the burning material in a fire may involve other parts of the property and/or trap persons, necessitating an intensive, large-scale rescue operation/evacuation. In certain cases, large-scale evacuation may have to be undertaken when people are likely to get trapped or affected by fire.
In all cases in which large-scale sudden movement of personnel is involved, traffic problems are also created—particularly if public roads, streets or areas have to be used for this movement. If such problems are not anticipated and suitable action is not preplanned, traffic bottlenecks result, which hamper and retard fire extinguishment and rescue efforts.
Evacuation of a large number of persons—particularly from high-rise buildings—may also present problems. For successful evacuation, it is not only necessary that adequate and suitable means of escape are available, but also that the evacuation be effected speedily. Special attention should be given to the evacuation needs of disabled individuals.
Detailed evacuation procedures must, therefore, be included in the emergency plan. These must be frequently tested in the conduct of fire and evacuation drills, which may also involve traffic problems. All participating and concerned organizations and agencies must also be involved in these drills, at least periodically. After each exercise, a debriefing session must be held, during which all mistakes are pointed out and explained. Action must also be taken to prevent repetition of the same mistakes in future exercises and actual incidents by removing all difficulties and reviewing the emergency plan as necessary.
Proper records must be maintained of all exercises and evacuation drills.
Emergency Medical Services
Casualties in a fire or explosion must receive immediate medical aid or be moved speedily to a hospital after being given first aid.
It is essential that management provide one or more first-aid post(s) and, where necessary because of the size and hazardous nature of the industry, one or more mobile paramedical appliances. All first-aid posts and paramedical appliances must be staffed at all times by fully trained paramedics.
Depending upon the size of the industry and the number of workers, one or more ambulance(s) must also be provided and staffed on the premises for removal of casualties to hospitals. In addition, arrangement must be made to ensure that additional ambulance facilities are available at short notice when needed.
Where the size of the industry or workplace so demands, a full-time medical officer should also be made available at all times for any emergency situation.
Prior arrangements must be made with a designated hospital or hospitals at which priority is given to casualties who are removed after a fire or explosion. Such hospitals must be listed in the emergency plan along with their telephone numbers, and the emergency plan must have suitable provisions to ensure that a responsible person shall alert them to receive casualties as soon as an emergency arises.
Facility Restoration
It is important that all fire protection and emergency facilities are restored to a “ready” mode soon after the emergency is over. For this purpose, responsibility must be assigned to a person or section of the industry, and this must be included in the emergency plan. A system of checks to ensure that this is being done must also be introduced.
Public Fire Department Relations
It is not practicable for any management to foresee and provide for all possible contingencies. It is also not economically feasible to do so. In spite of adopting the most up-to-date method of fire risk management, there are always occasions when the fire protection facilities provided on the premises fall short of actual needs. For such occasions, it is desirable to preplan a mutual assistance programme with the public fire department. Good liaison with that department is necessary so that the management knows what assistance that unit can provide during an emergency on its premises. Also, the public fire department must become familiar with the risk and what it could expect during an emergency. Frequent interaction with the public fire department is necessary for this purpose.
Handling of Hazardous Materials
Hazards of the materials used in industry may not be known to fire-fighters during a spill situation, and accidental discharge and improper use or storage of hazardous materials can lead to dangerous situations that can seriously imperil their health or lead to a serious fire or explosion. It is not possible to remember the hazards of all materials. Means of ready identification of hazards have, therefore, been developed whereby the various substances are identified by distinct labels or markings.
Hazardous materials identification
Each country follows its own rules concerning the labelling of hazardous materials for the purpose of storage, handling and transportation, and various departments may be involved. While compliance with local regulations is essential, it is desirable that an internationally recognized system of identification of hazardous materials be evolved for universal application. In the United States, the NFPA has developed a system for this purpose. In this system, distinct labels are conspicuously attached or affixed to containers of hazardous materials. These labels indicate the nature and degree of hazards in respect of health, flammability and the reactive nature of the material. In addition, special possible hazards to fire-fighters can also be indicated on these labels. For an explanation of the degree of hazard, refer to NFPA 704, Standard System for the Identification of the Fire Hazards of Materials (1990a). In this system, the hazards are categorized as health hazards, flammability hazards, and reactivity (instability) hazards.
Health hazards
These include all possibilities of a material causing personal injury from contact with or absorption into the human body. A health hazard may arise out of the inherent properties of the material or from the toxic products of combustion or decomposition of the material. The degree of hazard is assigned on the basis of the greater hazard that may result under fire or other emergency conditions. It indicates to fire-fighters whether they can work safely only with special protective clothing or with suitable respiratory protective equipment or with ordinary clothing.
Degree of health hazard is measured on a scale of 4 to 0, with 4 indicating the most severe hazard and 0 indicating low hazard or no hazard.
Flammability hazards
These indicate the susceptibility of the material to burning. It is recognized that materials behave differently in respect of this property under varying circumstances (e.g., materials that may burn under one set of conditions may not burn if the conditions are altered). The form and inherent properties of the materials influence the degree of hazard, which is assigned on the same basis as for the health hazard.
Reactivity (instability) hazards
Materials capable of releasing energy by itself, (i.e., by self-reaction or polymerization) and substances that can undergo violent eruption or explosive reactions on coming in contact with water, other extinguishing agents or certain other materials are said to possess a reactivity hazard.
The violence of reaction may increase when heat or pressure is applied or when the substance comes in contact with certain other materials to form a fuel-oxidizer combination, or when it comes in contact with incompatible substances, sensitizing contaminants or catalysts.
The degree of reactivity hazard is determined and expressed in terms of the ease, rate and quantity of energy release. Additional information, such as radioactivity hazard or prohibition of water or other extinguishing medium for fire-fighting, can also be given on the same level.
The label warning of a hazardous material is a diagonally placed square with four smaller squares (see figure 1).
Figure 1. The NFPA 704 diamond.
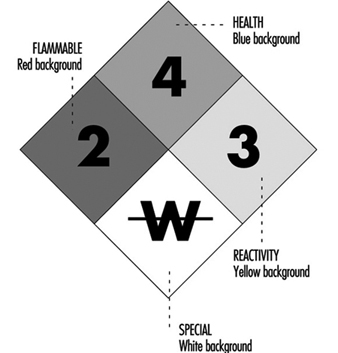
The top square indicates the health hazard, the one on the left indicates the flammability hazard, the one on the right indicates the reactivity hazard, and the bottom square indicates other special hazards, such as radioactivity or unusual reactivity with water.
To supplement the above mentioned arrangement, a colour code may also be used. The colour is used as background or the numeral indicating the hazard may be in coded colour. The codes are health hazard (blue), flammability hazard (red), reactivity hazard (yellow) and special hazard (white background).
Managing hazardous materials response
Depending on the nature of the hazardous material in the industry, it is necessary to provide protective equipment and special fire-extinguishing agents, including the protective equipment required to dispense the special extinguishing agents.
All workers must be trained in the precautions they must take and the procedures they must adopt to deal with each incident in the handling of the various types of hazardous materials. They must also know the meaning of the various identification signs.
All fire-fighters and other workers must be trained in the correct use of any protective clothing, protective respiratory equipment and special fire-fighting techniques. All concerned personnel must be kept alert and prepared to tackle any situation through frequent drills and exercises, of which proper records should be kept.
To deal with serious medical hazards and the effects of these hazards on fire-fighters, a competent medical officer should be available to take immediate precautions when any individual is exposed to unavoidable dangerous contamination. All affected persons must receive immediate medical attention.
Proper arrangements must also be made to set up a decontamination centre on the premises when necessary, and correct decontamination procedures must be laid down and followed.
Waste control
Considerable waste is generated by industry or because of accidents during handling, transportation and storage of goods. Such waste may be flammable, toxic, corrosive, pyrophoric, chemically reactive or radioactive, depending upon the industry in which it is generated or the nature of goods involved. In most cases unless proper care is taken in safe disposal of such waste, it may endanger animal and human life, pollute the environment or cause fire and explosions that may endanger property. A thorough knowledge of the physical and chemical properties of the waste materials and of the merits or limitations of the various methods of their disposal is, therefore, necessary to ensure economy and safety.
Properties of industrial waste are briefly summarized below:
- Most industrial waste is hazardous and can have unexpected significance during and after disposal. The nature and behavioural characteristics of all waste must therefore be carefully examined for their short- and long-term impact and the method of disposal determined accordingly.
- Mixing of two seemingly innocuous discarded substances may create an unexpected hazard because of their chemical or physical interaction.
- Where flammable liquids are involved, their hazards can be assessed by taking into consideration their respective flash points, ignition temperature, flammability limits and the ignition energy required to initiate combustion. In the case of solids, particle size is an additional factor that must be considered.
- Most flammable vapours are heavier than air. Such vapours and heavier-than-air flammable gases that may be accidentally released during collection or disposal or during handling and transportation can travel considerable distances with the wind or towards a lower gradient. On coming in contact with a source of ignition, they flash back to source. Major spills of flammable liquids are particularly hazardous in this respect and may require evacuation to save lives.
- Pyrophoric materials, such as aluminium alkyls, ignite spontaneously when exposed to air. Special care must therefore be taken in handling, transportation, storage and disposal of such materials, preferably carried out under a nitrogen atmosphere.
- Certain materials, such as potassium, sodium and aluminium alkyls, react violently with water or moisture and burn fiercely. Bronze powder generates considerable heat in the presence of moisture.
- The presence of potent oxidants with organic materials can cause rapid combustion or even an explosion. Rags and other materials soaked with vegetable oils or terpenes present a risk of spontaneous combustion due to the oxidation of oils and subsequent build-up of heat to the ignition temperature.
- Several substances are corrosive and may cause severe damage or burns to skin or other living tissues, or may corrode construction materials, especially metals, thereby weakening the structure in which such materials may have been used.
- Some substances are toxic and can poison humans or animals by contact with skin, inhalation or contamination of food or water. Their ability to do so may be short lived or may extend over a long period. Such substances, if disposed of by dumping or burning, can contaminate water sources or come into contact with animals or workers.
- Toxic substances that are spilled during industrial processing, transportation (including accidents), handling or storage, and toxic gases that are released into the atmosphere can affect emergency personnel and others, including the public. The hazard is all the more severe if the spilled substance(s) is vaporized at ambient temperature, because the vapours can be carried over long distances due to wind drift or run-off.
- Certain substances may emit a strong, pungent or unpleasant odour, either by themselves or when they are burnt in the open. In either case, such substances are a public nuisance, even though they may not be toxic, and they must be disposed of by proper incineration, unless it is possible to collect and recycle them. Just as odorous substances are not necessarily toxic, odourless substances and some substances with a pleasant odour may produce harmful physiological effects.
- Certain substances, such as explosives, fireworks, organic peroxides and some other chemicals, are sensitive to heat or shock and may explode with devastating effect if not handled carefully or mixed with other substances. Such substances must, therefore, be carefully segregated and destroyed under proper supervision.
- Waste materials that are contaminated with radioactivity can be as hazardous as the radioactive materials themselves. Their disposal requires specialized knowledge. Proper guidance for disposal of such waste may be obtained from a country’s nuclear energy organization.
Some of the methods that may be employed to dispose of industrial and emergency waste are biodegradation, burial, incineration, landfill, mulching, open burning, pyrolysis and disposal through a contractor. These are briefly explained below.
Biodegradation
Many chemicals are completely destroyed within six to 24 months when they are mixed with the top 15 cm of soil. This phenomenon is known as biodegradation and is due to the action of soil bacteria. Not all substances, however, behave in this way.
Burial
Waste, particularly chemical waste, is often disposed of by burial. This is a dangerous practice in so far as active chemicals are concerned, because, in time, the buried substance may get exposed or leached by rain into water resources. The exposed substance or the contaminated material can have adverse physiological effects when it comes in contact with water that is drunk by humans or animals. Cases are on record in which water was contaminated 40 years after burial of certain harmful chemicals.
Incineration
This is one of the safest and most satisfactory methods of waste disposal if the waste is burned in a properly designed incinerator under controlled conditions. Care must be taken, however, to ensure that the substances contained in the waste are amenable to safe incineration without posing any operating problem or special hazard. Almost all industrial incinerators require the installation of air pollution control equipment, which must be carefully selected and installed after taking into consideration the composition of the stock effluent given out by the incinerator during the burning of industrial waste.
Care must be taken in the operation of the incinerator to ensure that its operative temperature does not rise excessively either because a large amount of volatiles is fed or because of the nature of the waste burned. Structural failure can occur because of excessive temperature, or, over time, because of corrosion. The scrubber must also be periodically inspected for signs of corrosion which can occur because of contact with acids, and the scrubber system must be maintained regularly to ensure proper functioning.
Landfill
Low-lying land or a depression in land is often used as a dump for waste materials until it becomes level with the surrounding land. The waste is then levelled, covered with earth and rolled hard. The land is then used for buildings or other purposes.
For satisfactory landfill operation, the site must be selected with due regard to the proximity of pipelines, sewer lines, power lines, oil and gas wells, mines and other hazards. The waste must then be mixed with earth and evenly spread out in the depression or a wide trench. Each layer must be mechanically compacted before the next layer is added.
A 50 cm layer of earth is typically laid over the waste and compacted, leaving sufficient vents in the soil for the escape of gas that is produced by biological activity in the waste. Attention must also be paid to proper drainage of the landfill area.
Depending on the various constituents of waste material, it may at times ignite within the landfill. Each such area must, therefore, be properly fenced off and continued surveillance maintained until the chances of ignition appear to be remote. Arrangements must also be made for extinguishing any fire that may break out in the waste within the landfill.
Mulching
Some trials have been made for reusing polymers as mulch (loose material for protecting the roots of plants) by chopping the waste into small shreds or granules. When so used, it degrades very slowly. Its effect on the soil is, therefore, purely physical. This method has, however, not been used widely.
Open burning
Open burning of waste causes pollution of the atmosphere and is hazardous in as much as there is a chance of the fire getting out of control and spreading to the surrounding property or areas. Also, there is a chance of explosion from containers, and there is a possibility of harmful physiological effects of radioactive materials that may be contained in the waste. This method of disposal has been banned in some countries. It is not a desirable method and should be discouraged.
Pyrolysis
Recovery of certain compounds, by distillation of the products given out during pyrolysis (decomposition by heating) of polymers and organic substances, is possible, but not yet widely adopted.
Disposal through contractors
This is probably the most convenient method. It is important that only reliable contractors who are knowledgeable and experienced in the disposal of industrial waste and hazardous materials are selected for the job. Hazardous materials must be carefully segregated and disposed of separately.
Specific classes of materials
Specific examples of the types of hazardous materials that are often found in today’s industry include: (1) combustible and reactive metals, such as magnesium, potassium, lithium, sodium, titanium and zirconium; (2) combustible refuse; (3) drying oils; (4) flammable liquids and waste solvents; (5) oxidizing materials (liquids and solids); and (6) radioactive materials. These materials require special handling and precautions that must be carefully studied. For more details on identification of hazardous materials and hazards of industrial materials, the following publications may be consulted: Fire Protection Handbook (Cote 1991) and Sax’s Dangerous Properties of Industrial Materials (Lewis 1979).
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."