- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Working Under Increased Barometric Pressure
The atmosphere normally consists of 20.93% oxygen. The human body is naturally adapted to breathe atmospheric oxygen at a pressure of approximately 160 torr at sea level. At this pressure, haemoglobin, the molecule which carries oxygen to the tissue, is approximately 98% saturated. Higher pressures of oxygen cause little important increase in oxyhaemoglobin, since its concentration is virtually 100% to begin with. However, significant amounts of unburnt oxygen may pass into physical solution in the blood plasma as the pressure rises. Fortunately, the body can tolerate a fairly wide range of oxygen pressures without appreciable harm, at least in the short term. Longer term exposures may lead to oxygen toxicity problems.
When a job requires breathing compressed air, as in diving or caisson work, oxygen deficiency (hypoxia) is rarely a problem, as the body will be exposed to an increasing amount of oxygen as the absolute pressure rises. Doubling the pressure will double the number of molecules inhaled per breath while breathing compressed air. Thus the amount of oxygen breathed is effectively equal to 42%. In other words, a worker breathing air at a pressure of 2 atmospheres absolute (ATA), or 10 m beneath the sea, will breathe an amount of oxygen equal to breathing 42% oxygen by mask on the surface.
Oxygen toxicity
On the earth’s surface, human beings can safely continuously breathe 100% oxygen for between 24 and 36 hours. After that, pulmonary oxygen toxicity ensues (the Lorrain-Smith effect). The symptoms of lung toxicity consist of substernal chest pain; dry, non-productive cough; a drop in the vital capacity; loss of surfactant production. A condition known as patchy atelectasis is seen on x-ray examination, and with continued exposure microhaemorrhages and ultimately production of permanent fibrosis in the lung will develop. All stages of oxygen toxicity through the microhaemorrhage state are reversible, but once fibrosis sets in, the scarring process becomes irreversible. When 100% oxygen is breathed at 2 ATA, (a pressure of 10 m of sea water), the early symptoms of oxygen toxicity become manifest after about six hours. It should be noted that interspersing short, five-minute periods of air breathing every 20 to 25 minutes can double the length of time required for symptoms of oxygen toxicity to appear.
Oxygen can be breathed at pressures below 0.6 ATA without ill effect. For example, a worker can tolerate 0.6 atmosphere oxygen breathed continuously for two weeks without any loss of vital capacity. The measurement of vital capacity appears to be the most sensitive indicator of early oxygen toxicity. Divers working at great depths may breathe gas mixtures containing up to 0.6 atmospheres oxygen with the rest of the breathing medium consisting of helium and/or nitrogen. Six tenths of an atmosphere corresponds to breathing 60% oxygen at 1 ATA or at sea level.
At pressures greater than 2 ATA, pulmonary oxygen toxicity no longer becomes the primary concern, as oxygen can cause seizures secondary to cerebral oxygen toxicity. Neurotoxicity was first described by Paul Bert in 1878 and is known as the Paul Bert effect. If a person were to breathe 100% oxygen at a pressure of 3 ATA for much longer than three continuous hours, he or she will very likely suffer a grand mal seizure. Despite over 50 years of active research as to the mechanism of oxygen toxicity of the brain and lung, this response is still not completely understood. Certain factors are known, however, to enhance toxicity and to lower the seizure threshold. Exercise, CO2 retention, use of steroids, presence of fever, chilling, ingestion of amphetamines, hyperthyroidism and fear can have an oxygen tolerance effect. An experimental subject lying quietly in a dry chamber at pressure has much greater tolerance than a diver who is working actively in cold water underneath an enemy ship, for example. A military diver may experience cold, hard exercise, probable CO2 build-up using a closed-circuit oxygen rig, and fear, and may experience a seizure within 10-15 minutes working at a depth of only 12 m, whereas a patient lying quietly in a dry chamber may easily tolerate 90 minutes at a pressure of 20 m without great danger of seizure. Exercising divers may be exposed to partial pressure of oxygen up to 1.6 ATA for short periods up to 30 minutes, which corresponds to breathing 100% oxygen at a depth of 6 m. It is important to note that one should never expose anyone to 100% oxygen at a pressure greater than 3 ATA, nor for a time longer than 90 minutes at that pressure, even with a subject quietly recumbent.
There is considerable individual variation in susceptibility to seizure between individuals and, surprisingly, within the same individual, from day to day. For this reason, “oxygen tolerance” tests are essentially meaningless. Giving seizure-suppressing drugs, such as phenobarbital or phenytoin, will prevent oxygen seizures but do nothing to mitigate permanent brain or spinal cord damage if pressure or time limits are exceeded.
Carbon monoxide
Carbon monoxide can be a serious contaminant of the diver’s or caisson worker’s breathing air. The most common sources are internal combustion engines, used to power compressors, or other operating machinery in the vicinity of the compressors. Care should be taken to be sure that compressor air intakes are well clear of any sources of engine exhaust. Diesel engines usually produce little carbon monoxide but do produce large quantities of oxides of nitrogen, which can produce serious toxicity to the lung. In the United States, the current federal standard for carbon monoxide levels in inspired air is 35 parts per million (ppm) for an 8-hour working day. For example, at the surface even 50 ppm would not produce detectable harm, but at a depth of 50 m it would be compressed and produce the effect of 300 ppm. This concentration can produce a level of up to 40% carboxyhaemoglobin over a period of time. The actual analysed parts per million must be multiplied by the number of atmospheres at which it is delivered to the worker.
Divers and compressed-air workers should become aware of the early symptoms of carbon monoxide poisoning, which include headache, nausea, dizziness and weakness. It is important to ensure that the compressor intake be always located upwind from the compressor engine exhaust pipe. This relationship must be continually checked as the wind changes or the vessels position shifts.
For many years it was widely assumed that carbon monoxide would combine with the body’s haemoglobin to produce carboxyhaemoglobin, causing its lethal effect by blocking transport of oxygen to the tissues. More recent work shows that although this effect does cause tissue hypoxia, it is not in itself fatal. The most serious damage occurs at the cellular level due to direct toxicity of the carbon monoxide molecule. Lipid peroxidation of cell membranes, which can only be terminated by hyperbaric oxygen treatment, appears to be the main cause of death and long-term sequelae.
Carbon dioxide
Carbon dioxide is a normal product of metabolism and is eliminated from the lungs through the normal process of respiration. Various types of breathing apparatus, however, can impair its elimination or cause high levels to build up in the diver’s inspired air.
From a practical point of view, carbon dioxide can exert deleterious effects on the body in three ways. First, in very high concentrations (above 3%), it can cause judgmental errors, which at first may amount to inappropriate euphoria, followed by depression if the exposure is prolonged. This, of course, can have serious consequences for a diver under water who wants to maintain good judgement to remain safe. As the concentration climbs, CO2 will eventually produce unconsciousness when levels rise much above 8%. A second effect of carbon dioxide is to exacerbate or worsen nitrogen narcosis (see below). At partial pressures of above 40 mm Hg, carbon dioxide begins to have this effect (Bennett and Elliot 1993). At high PO2‘s, such as one is exposed to in diving, the respiratory drive due to high CO2 is attenuated and it is possible under certain conditions for divers who tend to retain CO2 to increase their levels of carbon dioxide sufficient to render them unconscious. The final problem with carbon dioxide under pressure is that, if the subject is breathing 100% oxygen at pressures greater than 2 ATA, the risk for seizures is greatly enhanced as carbon dioxide levels rise. Submarine crews have easily tolerated breathing 1.5% CO2 for two months at a time with no functional ill effect, a concentration that is thirty times the normal concentration found in atmospheric air. Five thousand ppm, or ten times the level found in normal fresh air, is considered safe for the purposes of industrial limits. However, even 0.5% CO2 added to 100% oxygen mix will predispose a person to seizures when breathed at increased pressure.
Nitrogen
Nitrogen is an inert gas with regard to normal human metabolism. It does not enter into any form of chemical combination with compounds or chemicals within the body. However, it is responsible for severe impairment in a diver’s mental functioning when breathed under high pressure.
Nitrogen behaves as an aliphatic anaesthetic as atmospheric pressure increases, which results in the concentration of nitrogen also increasing. Nitrogen fits well into the Meyer-Overton hypothesis which states that any aliphatic anaesthetic will exhibit anaesthetic potency in direct proportion to its oil-water solubility ratio. Nitrogen, which is five times more soluble in fat than in water, produces an anaesthetic effect precisely at the predicted ratio.
In actual practice, diving to depths of 50 m can be accomplished with compressed-air, although the effects of nitrogen narcosis first become evident between 30 and 50 m. Most divers, however, can function adequately within these parameters. Deeper than 50 m, helium/oxygen mixtures are commonly used to avoid the effects of nitrogen narcosis. Air diving has been done to depths of slightly over 90 m, but at these extreme pressures, the divers were barely able to function and could hardly remember what tasks they had been sent down to accomplish. As noted earlier, any excess CO2 build-up further worsens the effect of nitrogen. Because ventilatory mechanics are affected by the density of gas at great pressures, there is an automatic CO2 build-up in the lung because of changes in laminar flow within the bronchioles and the diminution of the respiratory drive. Thus, air diving deeper than 50 m can be extremely dangerous.
Nitrogen exerts its effect by its simple physical presence dissolved in neural tissue. It causes a slight swelling of the neuronal cell membrane, which makes it more permeable to sodium and potassium ions. It is felt that interference with the normal depolarization/repolarization process is responsible for clinical symptoms of nitrogen narcosis.
Decompression
Decompression tables
A decompression table sets out the schedule, based on depth and time of exposure, for decompressing a person who has been exposed to hyperbaric conditions. Some general statements can be made about decompression procedures. No decompression table can be guaranteed to avoid decompression illness (DCI) for everyone, and indeed as described below, many problems have been noted with some tables currently in use. It must be remembered that bubbles are produced during every normal decompression, no matter how slow. For this reason, although it can be stated that the longer the decompression the less the likelihood of DCI, at the extreme of least likelihood, DCI becomes an essentially random event.
Habituation
Habituation, or acclimatization, occurs in divers and compressed-air workers, and renders them less susceptible to DCI after repeated exposures. Acclimatization can be produced after about a week of daily exposure, but it is lost after an absence from work of between 5 days to a week or by a sudden increase in pressure. Unfortunately construction companies have relied on acclimatization to make work possible with what are viewed as grossly inadequate decompression tables. To maximize the utility of acclimatization, new workers are often started at midshift to allow them to habituate without getting DCI. For example, the present Japanese Table 1 for compressed-air workers utilizes the split shift, with a morning and afternoon exposure to compressed air with a surface interval of one hour between exposures. Decompression from the first exposure is about 30% of that required by the US Navy and the decompression from the second exposure is only 4% of that required by the Navy. Nevertheless, habituation makes this departure from physiologic decompression possible. Workers with even ordinary susceptibility to decompression illness self-select themselves out of compressed-air work.
The mechanism of habituation or acclimatization is not understood. However, even if the worker is not experiencing pain, damage to brain, bone, or tissue may be taking place. Up to four times as many changes are visible on MRIs taken of the brains of compressed-air workers compared to age-matched controls that have been studied (Fueredi, Czarnecki and Kindwall 1991). These probably reflect lacunar infarcts.
Diving decompression
Most modern decompression schedules for divers and caisson workers are based on mathematical models akin to those developed originally by J.S. Haldane in 1908 when he made some empirical observations on permissible decompression parameters. Haldane observed that a pressure reduction of one half could be tolerated in goats without producing symptoms. Using this as a starting point, he then, for mathematical convenience, conceived of five different tissues in the body loading and unloading nitrogen at varying rates based on the classical half time equation. His staged decompression tables were then designed to avoid exceeding a 2:1 ratio in any of the tissues. Over the years, Haldane’s model has been modified empirically in attempts to make it fit what divers were observed to tolerate. However, all mathematical models for the loading and elimination of gases are flawed, since there are no decompression tables which remain as safe or become safer as time and depth are increased.
Probably the most reliable decompression tables currently available for air diving are those of the Canadian Navy, known as the DCIEM tables (Defence and Civil Institute of Environmental Medicine). These tables were tested thoroughly by non-habituated divers over a wide range of conditions and produce a very low rate of decompression illness. Other decompression schedules which have been well tested in the field are the French National Standards, originally developed by Comex, the French diving company.
The US Navy Air Decompression tables are unreliable, especially when pushed to their limits. In actual use, US Navy Master Divers routinely decompress for a depth 3 m (10 ft) deeper and/or one exposure time segment longer than required for the actual dive to avoid problems. The Exceptional Exposure Air Decompression Tables are particularly unreliable, having produced decompression illness on 17% to 33% of all the test dives. In general, the US Navy’s decompression stops are probably too shallow.
Tunnelling and caisson decompression
None of the air decompression tables which call for air breathing during decompression, currently in wide use, appear to be safe for tunnel workers. In the United States, the current federal decompression schedules (US Bureau of Labor Statuties 1971), enforced by the Occupational Safety and Health Administration (OSHA), have been shown to produce DCI in one or more workers on 42% of the working days while being used at pressures between 1.29 and 2.11 bar. At pressures over 2.45 bar, they have been shown to produce a 33% incidence of aseptic necrosis of the bone (dysbaric osteonecrosis). The British Blackpool Tables are also flawed. During the building of the Hong Kong subway, 83% of the workers using these tables complained of symptoms of DCI. They have also been shown to produce an incidence of dysbaric osteonecrosis of up to 8% at relatively modest pressures.
The new German oxygen decompression tables devised by Faesecke in 1992 have been used with good success in a tunnel under the Kiel Canal. The new French oxygen tables also appear to be excellent by inspection but have not yet been used on a large project.
Using a computer which examined 15 years of data from successful and unsuccessful commercial dives, Kindwall and Edel devised compressed-air caisson decompression tables for the US National Institute for Occupational Safety and Health in 1983 (Kindwall, Edel and Melton 1983) using an empirical approach which avoided most of the pitfalls of mathematical modelling. Modelling was used only to interpolate between real data points. The research upon which these tables was based found that when air was breathed during decompression, the schedule in the tables did not produce DCI. However, the times used were prohibitively long and therefore impractical for the construction industry. When an oxygen variant of the table was computed, however, it was found that decompression time could be shortened to times similar to, or even shorter than, the current OSHA-enforced air decompression tables cited above. These new tables were subsequently tested by non-habituated subjects of varying ages at pressures ranging from 0.95 bar to 3.13 bar in 0.13 bar increments. Average work levels were simulated by weight lifting and treadmill walking during exposure. Exposure times were as long as possible, in keeping with the combined work time and decompression time fitting into an eight-hour work day. These are the only schedules which will be used in actual practice for shift work. No DCI was reported during these tests and bone scan and x ray failed to reveal any dysbaric osteonecrosis. To date, these are the only laboratory-tested decompression schedules in existence for compressed-air workers.
Decompression of hyperbaric chamber personnel
US Navy air decompression schedules were designed to produce a DCI incidence of less than 5%. This is satisfactory for operational diving, but much too high to be acceptable for hyperbaric workers who work in clinical settings. Decompression schedules for hyperbaric chamber attendants can be based on naval air decompression schedules, but since exposures are so frequent and thus are usually at the limits of the table, they must be liberally lengthened and oxygen should be substituted for compressed-air breathing during decompression. As a prudent measure, it is recommended that a two-minute stop be made while breathing oxygen, at least three metres deeper than called for by the decompression schedule chosen. For example, while the US Navy requires a three-minute decompression stop at three metres, breathing air, after a 101 minute exposure at 2.5 ATA, an acceptable decompression schedule for a hyperbaric chamber attendant undergoing the same exposure would be a two-minute stop at 6 m breathing oxygen, followed by ten minutes at 3 m breathing oxygen. When these schedules, modified as above, are used in practice, DCI in an inside attendant is an extreme rarity (Kindwall 1994a).
In addition to providing a fivefold larger “oxygen window” for nitrogen elimination, oxygen breathing offers other advantages. Raising the PO2 in venous blood has been demonstrated to lessen blood sludging, reduce the stickiness of white cells, reduce the no-reflow phenomenon, render red cells more flexible in passing through capillaries and counteract the vast decrease in deformability and filterability of white cells which have been exposed to compressed air.
Needless to say, all workers using oxygen decompression must be thoroughly trained and apprised of the fire danger. The environment of the decompression chamber must be kept free of combustibles and ignition sources, an overboard dump system must be used to convey exhaled oxygen out of the chamber and redundant oxygen monitors with a high oxygen alarm must be provided. The alarm should sound if oxygen in the chamber atmosphere exceeds 23%.
Working with compressed air or treating clinical patients under hyperbaric conditions sometimes can accomplish work or effect remission in disease that would otherwise be impossible. When rules for the safe use of these modalities are observed, workers need not be at significant risk for dysbaric injury.
Caisson Work and Tunnelling
From time to time in the construction industry it is necessary to excavate or tunnel through ground which is either fully saturated with water, lying below the local water table, or following a course completely under water, such as a river or lake bottom. A time-tested method for managing this situation has been to apply compressed air to the working area to force water out of the ground, drying it sufficiently so that it can be mined. This principle has been applied to both caissons used for bridge pier construction and soft ground tunnelling (Kindwall 1994b).
Caissons
A caisson is simply a large, inverted box, made to the dimensions of the bridge foundation, which typically is built in a dry dock and then floated into place, where it is carefully positioned. It is then flooded and lowered until it touches bottom, after which it is driven down further by adding weight as the bridge pier itself is constructed. The purpose of the caisson is to provide a method for cutting through soft ground to land the bridge pier on solid rock or a good geologic weight-bearing stratum. When all sides of the caisson have been embedded in the mud, compressed air is applied to the interior of the caisson and water is forced out, leaving a muck floor which can be excavated by men working within the caisson. The edges of the caisson consist of a wedge-shaped cutting shoe, made of steel, which continues to descend as earth is removed beneath the descending caisson and weight is applied from above as the bridge tower is constructed. When bed rock is reached, the working chamber is filled with concrete, becoming the permanent base for the bridge foundation.
Caissons have been used for nearly 150 years and have been successful in the construction of foundations as deep as 31.4 m below mean high water, as on Bridge Pier No. 3 of the Auckland, New Zealand, Harbour Bridge in 1958.
Design of the caisson usually provides for an access shaft for workers, who can descend either by ladder or by a mechanical lift and a separate shaft for buckets to remove the spoil. The shafts are provided with hermetically sealed hatches at either end which enable the caisson pressure to remain the same while workers or materials exit or enter. The top hatch of the muck shaft is provided with a pressure sealed gland through which the hoist cable for the muck bucket can slide. Before the top hatch is opened, the lower hatch is shut. Hatch interlocks may be necessary for safety, depending on design. Pressure must be equal on both sides of any hatch before it can be opened. Since the walls of the caisson are generally made of steel or concrete, there is little or no leakage from the chamber while under pressure except under the edges. The pressure is raised incrementally to a pressure just slightly greater than is necessary to balance off sea pressure at the edge of the cutting shoe.
People working in the pressurized caisson are exposed to compressed air and may experience many of the same physiologic problems that face deep-sea divers. These include decompression illness, barotrauma of the ears, sinus cavities and lungs and if decompression schedules are inadequate, the long-term risk of aseptic necrosis of the bone (dysbaric osteonecrosis).
It is important that a ventilation rate be established to carry away CO2 and gases emanating from the muck floor (especially methane) and whatever fumes may be produced from welding or cutting operations in the working chamber. A rule of thumb is that six cubic metres of free air per minute must be provided for each worker in the caisson. Allowance must also be made for air which is lost when the muck lock and man lock are used for the passage of personnel and materials. As the water is forced down to a level exactly even with the cutting shoe, ventilation air is required as the excess bubbles out under the edges. A second air supply, equal in capacity to the first, with an independent power source, should be available for emergency use in case of compressor or power failure. In many areas this is required by law.
Sometimes if the ground being mined is homogeneous and consists of sand, blow pipes can be erected to the surface. The pressure in the caisson will then extract the sand from the working chamber when the end of the blow pipe is located in a sump and the excavated sand is shovelled into the sump. If coarse gravel, rock, or boulders are encountered, these have to be broken up and removed in conventional muck buckets.
If the caisson should fail to sink despite the added weight on top, it may sometimes be necessary to withdraw the workers from the caisson and reduce the air pressure in the working chamber to allow the caisson to fall. Concrete must be placed or water admitted to the wells within the pier structure surrounding the air shafts above the caisson to reduce the stress on the diaphragm at the top of the working chamber. When just beginning a caisson operation, safety cribs or supports should be kept in the working chamber to prevent the caisson from suddenly dropping and crushing the workers. Practical considerations limit the depth to which air-filled caissons can be driven when men are used to hand mine the muck. A pressure of 3.4 kg/cm2 gauge (3.4 bar or 35 m of fresh water) is about the maximum tolerable limit because of decompression considerations for the workers.
An automated caisson excavating system has been developed by the Japanese wherein a remotely operated hydraulically powered backhoe shovel, which can reach all corners of the caisson, is used for excavation. The backhoe, under television control from the surface, drops the excavated muck into buckets which are hoisted remotely from the caisson. Using this system, the caisson can proceed down to almost unlimited pressures. The only time that workers need enter the working chamber is to repair the excavating machinery or to remove or demolish large obstacles which appear below the cutting shoe of the caisson and which cannot be removed by the remote-controlled backhoe. In such cases, workers enter for short periods much as divers and can breathe either air or mixed gas at higher pressures to avoid nitrogen narcosis.
When people have worked long shifts under compressed-air at pressures greater than 0.8 kg/cm2 (0.8 bar), they must decompress in stages. This can be accomplished either by attaching a large decompression chamber to the top of the man shaft into the caisson or, if space requirements are such at the top that this is impossible, by attaching “blister locks” to the man shaft. These are small chambers which can accommodate only a few workers at a time in a standing position. Preliminary decompression is taken in these blister locks, where the time spent is relatively short. Then, with considerable excess gas remaining in their bodies, the workers rapidly decompress to the surface and quickly move to a standard decompression chamber, sometimes located on an adjacent barge, where they are repressurized for subsequent slow decompression. In compressed-air work, this process is known as “decanting” and was fairly common in England and elsewhere, but is prohibited in the United States. The object is to return workers to pressure within five minutes, before bubbles can grow sufficiently in size to cause symptoms. However, this is inherently dangerous because of the difficulties of moving a large gang of workers from one chamber to another. If one worker has trouble clearing his ears during repressurization, the whole shift is placed in jeopardy. There is a much safer procedure, called “surface decompression”, for divers, where only one or two are decompressed at the same time. Despite every precaution on the Auckland Harbour Bridge project, as many as eight minutes occasionally elapsed before bridge workers could be put back under pressure.
Compressed air tunnelling
Tunnels are becoming increasingly important as the population grows, both for the purposes of sewage disposal and for unobstructed traffic arteries and rail service beneath large urban centres. Often, these tunnels must be driven through soft ground considerably below the local water table. Under rivers and lakes, there may be no other way to ensure the safety of the workers than to put compressed air on the tunnel. This technique, using a hydraulically driven shield at the face with compressed air to hold back the water, is known as the plenum process. Under large buildings in a crowded city, compressed air may be necessary to prevent surface subsidence. When this occurs, large buildings can develop cracks in their foundations, sidewalks and streets may drop and pipes and other utilities can be damaged.
To apply pressure to a tunnel, bulkheads are erected across the tunnel to provide the pressure boundary. On smaller tunnels, less than three metres in diameter, a single or combination lock is used to provide access for workers and materials and removal of the excavated ground. Removable track sections are provided by the doors so that they may be operated without interference from the muck-train rails. Numerous penetrations are provided in these bulkheads for the passage of high-pressure air for the tools, low-pressure air for pressurizing the tunnel, fire mains, pressure gauge lines, communications lines, electrical power lines for lighting and machinery and suction lines for ventilation and removal of water in the invert. These are often termed blow lines or “mop lines”. The low-pressure air supply pipe, which is 15-35 cm in diameter, depending on the size of the tunnel, should extend to the working face in order to ensure good ventilation for the workers. A second low-pressure air pipe of equal size should also extend through both bulkheads, terminating just inside the inner bulkhead, to provide air in the event of rupture or break in the primary air supply. These pipes should be fitted with flapper valves which will close automatically to prevent depressurization of the tunnel if the supply pipe is broken. The volume of air required to efficiently ventilate the tunnel and keep CO2 levels low will vary greatly depending on the porosity of the ground and how close the finished concrete lining has been brought to the shield. Sometimes micro-organisms in the soil produce large amounts of CO2. Obviously, under such conditions, more air will be required. Another useful property of compressed air is that it tends to force explosive gases such as methane away from the walls and out of the tunnel. This holds true when mining areas where spilled solvents such as petrol or degreasers have saturated the ground.
A rule of thumb developed by Richardson and Mayo (1960) is that the volume of air required usually can be calculated by multiplying the area of the working face in square metres by six and adding six cubic metres per man. This gives the number of cubic metres of free air required per minute. If this figure is used, it will cover most practical contingencies.
The fire main must also extend through to the face and be provided with hose connections every sixty metres for use in case of fire. Thirty metres of rotproof hose should be attached to the water-filled fire main outlets.
In very large tunnels, over about four metres in diameter, two locks should be provided, one termed the muck lock, for passing muck trains, and the man lock, usually positioned above the muck lock, for the workers. On large projects, the man lock is often made of three compartments so that engineers, electricians and others can lock in and out past a work shift undergoing decompression. These large man locks are usually built external to the main concrete bulkhead so they do not have to resist the external compressive force of the tunnel pressure when open to the outside air.
On very large subaqueous tunnels a safety screen is erected, spanning the upper half of the tunnel, to afford some protection should the tunnel suddenly flood secondary to a blow-out while tunnelling under a river or lake. The safety screen is usually placed as close as practicable to the face, avoiding the excavating machinery. A flying gangway or hanging walkway is used between the screen and the locks, the gangway dropping down to pass at least a metre below the lower edge of the screen. This will allow the workers egress to the man lock in the event of sudden flooding. The safety screen can also be used to trap light gases which may be explosive and a mop line can be attached through the screen and coupled to a suction or blow line. With the valve cracked, this will help to purge any light gases from the working environment. Because the safety screen extends nearly down to the centre of the tunnel, the smallest tunnel it can be employed on is about 3.6 m. It should be noted that workers must be warned to keep clear of the open end of the mop line, as serious accidents can be caused if clothing is sucked into the pipe.
Table 1 is a list of instructions which should be given to compressed-air workers before they first enter the compressed-air environment.
It is the responsibility of the retained physician or occupational health professional for the tunnel project to ensure that air purity standards are maintained and that all safety measures are in effect. Adherence to established decompression schedules by periodically examining the pressure recording graphs from the tunnel and man locks must also be carefully monitored.
Table 1. Instructions for compressed-air workers
- Never “short” yourself on the decompression times prescribed by your employer and the official decompression code in use. The time saved is not worth the risk of decompression illness (DCI), a potentially fatal or crippling disease.
- Do not sit in a cramped position during decompression. To do so allows nitrogen bubbles to gather and concentrate in the joints, thereby contributing to the risk of DCI. Because you are still eliminating nitrogen from your body after you go home, you should refrain from sleeping or resting in a cramped position after work, as well.
- Warm water should be used for showers and baths up to six hours after decompressing; very hot water can actually bring on or aggravate a case of decompression illness.
- Severe fatigue, lack of sleep and heavy drinking the night before can also help bring on decompression illness. Drinking alcohol and taking aspirin should never be used as a “treatment” for pains of decompression illness.
- Fever and illness, such as bad colds, increase the risk of decompression illness. Strains and sprains in muscles and joints are also “favourite” places for DCI to begin.
- When stricken by decompression illness away from the job site, immediately contact the company’s physician or one knowledgeable in treating this disease. Wear your identifying bracelet or badge at all times.
- Leave smoking materials in the changing shack. Hydraulic oil is flammable and should a fire start in the closed environment of the tunnel, it could cause extensive damage and a shutdown of the job, which would lay you off work. Also, because the air is thicker in the tunnel due to compression, heat is conducted down cigarettes so that they become too hot to hold as they get shorter.
- Do not bring thermos bottles in your lunch box unless you loosen the stopper during compression; if you do not do this, the stopper will be forced deep into the thermos bottle. During decompression, the stopper must also be loosened so that the bottle does not explode. Very fragile glass thermos bottles might implode when pressure is applied, even if the stopper is loose.
- When the air lock door has been closed and pressure is applied, you will notice that the air in the air lock gets warm. This is called the “heat of compression” and is normal. Once the pressure stops changing, the heat will dissipate and the temperature will return to normal. During compression, the first thing you will notice is a fullness of your ears. Unless you “clear your ears” by swallowing, yawning, or holding your nose and trying to “blow the air out through your ears”, you will experience ear pain during compression. If you cannot clear your ears, notify the shift foreman immediately so that compression can be halted. Otherwise you may break your eardrums or develop a severe ear squeeze. Once you have reached maximum pressure, there will be no further problems with your ears for the remainder of the shift.
- Should you experience buzzing in your ears, ringing in your ears, or deafness following compression which persists for more than a few hours, you must report to the compressed-air physician for evaluation. Under extremely severe but rare conditions, a portion of the middle ear structure other than the eardrum may be affected if you have had a great deal of difficulty clearing your ears and in that case this must be surgically corrected within two or three days to avoid permanent difficulty.
- If you have a cold or an attack of hay fever, it is best not to try compressing in the air lock until you are over it. Colds tend to make it difficult or impossible for you to equalize your ears or sinuses.
Hyperbaric chamber workers
Hyperbaric oxygen therapy is becoming more common in all areas of the world, with some 2,100 hyperbaric chamber facilities now functioning. Many of these chambers are multiplace units, which are compressed with compressed air to pressures ranging from 1 to 5 kg/cm2 gauge. Patients are given 100% oxygen to breathe, at pressures up to 2 kg/cm2 gauge. At pressures greater than that they may breathe mixed gas for treatment of decompression illness. The chamber attendants, however, typically breathe compressed air and so their exposure in the chamber is similar to that experienced by a diver or compressed-air worker.
Typically the chamber attendant working inside a multiplace chamber is a nurse, respiratory therapist, former diver, or hyperbaric technician. The physical requirements for such workers are similar to those for caisson workers. It is important to remember, however, that a number of chamber attendants working in the hyperbaric field are female. Women are no more likely to suffer ill effects from compressed-air work than men, with the exception of the question of pregnancy. Nitrogen is carried across the placenta when a pregnant woman is exposed to compressed air and this is transferred to the foetus. Whenever decompression takes place, nitrogen bubbles form in the venous system. These are silent bubbles and, when small, do no harm, as they are removed efficiently by the pulmonary filter. The wisdom, however, of having these bubbles appear in a developing foetus is doubtful. What studies have been done indicate that foetal damage may occur under such circumstances. One survey suggested that birth defects are more common in the children of women who have engaged in scuba diving while pregnant. Exposure of pregnant women to hyperbaric chamber conditions should be avoided and appropriate policies consistent with both medical and legal considerations must be developed. For this reason, female workers should be precautioned about the risks during pregnancy and appropriate personnel job assignment and health education programmes should be instituted in order that pregnant women not be exposed to hyperbaric chamber conditions.
It should be pointed out, however, that patients who are pregnant may be treated in the hyperbaric chamber, as they breathe 100% oxygen and are therefore not subject to nitrogen embolization. Previous concerns that the foetus would be at increased risk for retrolental fibroplasia or retinopathy of the newborn have proven to be unfounded in large clinical trials. Another condition, premature closure of the patent ductus arteriosus, has also not been found to be related to the exposure.
Other Hazards
Physical injuries
Divers
In general, divers are prone to the same types of physical injury that any worker is liable to sustain when working in heavy construction. Breaking cables, failing loads, crush injuries from machines, turning cranes and so on, can be commonplace. However, in the underwater environment, the diver is prone to certain types of unique injury that are not found elsewhere.
Suction/entrapment injury is something especially to be guarded against. Working in or near an opening in a ship’s hull, a caisson which has a lower water level on the side opposite the diver, or a dam can be causative of this type of mishap. Divers often refer to this type of situation as being trapped by “heavy water”.
To avoid dangerous situations where the diver’s arm, leg, or whole body may be sucked into an opening such as a tunnel or pipe, strict precautions must be taken to tag out pipe valves and flood gates on dams so that they cannot be opened while the diver is in the water near them. The same is true of pumps and piping within ships that the diver is working on.
Injury can include oedema and hypoxia of an entrapped limb sufficient to cause muscle necrosis, permanent nerve damage, or even loss of the entire limb, or it may occasion gross crushing of a portion of the body or the whole body so as to cause death from simple massive trauma. Entrapment in cold water for a long period of time may cause the diver to die of exposure. If the diver is using scuba gear, he may run out of air and drown before his release can be effected, unless additional scuba tanks can be provided.
Propeller injuries are straightforward and must be guarded against by tagging out a ship’s main propulsion machinery while the diver is in the water. It must be remembered, however, that steam turbine-powered ships, when in port, are continuously turning over their screws very slowly, using their jacking gear to avoid cooling and distortion of the turbine blades. Thus the diver, when working on such a blade (trying to clear it from entangled cables, for example), must be aware that the turning blade must be avoided as it approaches a narrow spot close to the hull.
Whole-body squeeze is a unique injury which can occur to deep sea divers using the classical copper helmet mated to the flexible rubberized suit. If there is no check valve or non-return valve where the air pipe connects to the helmet, cutting the air line at the surface will cause an immediate relative vacuum within the helmet, which can draw the entire body into the helmet. The effects of this can be instant and devastating. For example, at a depth of 10 m, about 12 tons of force is exerted on the soft part of the diver’s dress. This force will drive his body into the helmet if pressurization of the helmet is lost. A similar effect may be produced if the diver fails unexpectedly and fails to turn on compensating air. This can produce severe injury or death if it occurs near the surface, as a 10-metre fall from the surface will halve the volume of the dress. A similar fall occurring between 40 and 50 m will change the suit volume only about 17%. These volume changes are in accordance with Boyle’s Law.
Caisson and tunnel workers
Tunnel workers are subject to the usual types of accidents seen in heavy construction, with the additional problem of a higher incidence of falls and injuries from cave-ins. It must be stressed that an injured compressed-air worker who may have broken ribs should be suspected of having a pneumothorax until proven otherwise and therefore great care must be taken in decompressing such a patient. If a pneumothorax is present, it must be relieved at pressure in the working chamber before decompression is attempted.
Noise
Noise damage to compressed-air workers may be severe, as air motors, pneumatic hammers and drills are never properly equipped with silencers. Noise levels in caissons and tunnels have been measured at over 125 dB. These levels are physically painful, as well as causative of permanent damage to the inner ear. Echo within the confines of a tunnel or caisson exacerbates the problem.
Many compressed-air workers balk at wearing ear protection, saying that blocking the sound of an approaching muck train would be dangerous. There is little foundation for this belief, as hearing protection at best only attenuates sound but does not eliminate it. Furthermore, not only is a moving muck train not “silent” to a protected worker, but it also gives other cues such as moving shadows and vibration in the ground. A real concern is complete hermetic occlusion of the auditory meatus provided by a tightly fitting ear muff or protector. If air is not admitted to the external auditory canal during compression, external ear squeeze may result as the ear drum is forced outward by air entering the middle ear via the Eustachian tube. The usual sound protective ear muff is usually not completely air tight, however. During compression, which lasts only a tiny fraction of the total shift time, the muff can be slightly loosened should pressure equalization prove a problem. Formed fibre ear plugs which can be moulded to fit in the external canal provide some protection and are not air tight.
The goal is to avoid a time weighted average noise level of higher than 85 dBA. All compressed-air workers should have pre-employment base line audiograms so that auditory losses which may result from the high-noise environment can be monitored.
Hyperbaric chambers and decompression locks can be equipped with efficient silencers on the air supply pipe entering the chamber. It is important that this be insisted on, as otherwise the workers will be considerably bothered by the ventilation noise and may neglect to ventilate the chamber adequately. A continuous vent can be maintained with a silenced air supply producing no more than 75dB, about the noise level in an average office.
Fire
Fire is always of great concern in compressed-air tunnel work and in clinical hyperbaric chamber operations. One can be lulled into a false sense of security when working in a steel-walled caisson which has a steel roof and a floor consisting only of unburnable wet muck. However, even in these circumstances, an electrical fire can burn insulation, which will prove highly toxic and can kill or incapacitate a work crew very quickly. In tunnels which are driven using wooden lagging before the concrete is poured, the danger is even greater. In some tunnels, hydraulic oil and straw used for caulking can furnish additional fuel.
Fire under hyperbaric conditions is always more intense because there is more oxygen available to support combustion. A rise from 21% to 28% in the oxygen percentage will double the burning rate. As the pressure is increased, the amount of oxygen available to burn increases The increase is equal to the percentage of oxygen available multiplied by the number of atmospheres in absolute terms. For example, at a pressure of 4 ATA (equal to 30 m of sea water), the effective oxygen percentage would be 84% in compressed-air. However, it must be remembered that even though burning is very much accelerated under such conditions, it is not the same as the speed of burning in 84% oxygen at one atmosphere. The reason for this is that the nitrogen present in the atmosphere has a certain quenching effect. Acetylene cannot be used at pressures over one bar because of its explosive properties. However, other torch gases and oxygen can be used for cutting steel. This has been done safely at pressures up to 3 bar. Under such circumstances, however, scrupulous care must be exercised and someone must stand by with a fire hose to immediately quench any fire which might start, should an errant spark come in contact with something combustible.
Fire requires three components to be present: fuel, oxygen and an ignition source. If any one of these three factors is absent, fire will not occur. Under hyperbaric conditions, it is almost impossible to remove oxygen unless the piece of equipment in question can be inserted into the environment by filling it or surrounding it with nitrogen. If fuel cannot be removed, an ignition source must be avoided. In clinical hyperbaric work, meticulous care is taken to prevent the oxygen percentage in the multiplace chamber from rising above 23%. In addition, all electrical equipment within the chamber must be intrinsically safe, with no possibility of producing an arc. Personnel in the chamber should wear cotton clothing which has been treated with flame retardant. A water-deluge system must be in place, as well as a hand-held fire hose independently actuated. If a fire occurs in a multiplace clinical hyperbaric chamber, there is no immediate escape and so the fire must be fought with a hand-held hose and with the deluge system.
In monoplace chambers pressurized with 100% oxygen, a fire will be instantly fatal to any occupant. The human body itself supports combustion in 100% oxygen, especially at pressure. For this reason, plain cotton clothing is worn by the patient in the monoplace chamber to avoid static sparks which could be produced by synthetic materials. There is no need to fireproof this clothing, however, as if a fire should occur, the clothing would afford no protection. The only method for avoiding fires in the monoplace oxygen-filled chamber is to completely avoid any source of ignition.
When dealing with high pressure oxygen, at pressures over 10 kg/cm2 gauge, adiabatic heating must be recognized as a possible source of ignition. If oxygen at a pressure of 150 kg/cm2 is suddenly admitted to a manifold via a quick-opening ball valve, the oxygen may “diesel” if even a tiny amount of dirt is present. This can produce a violent explosion. Such accidents have occurred and for this reason, quick-opening ball valves should never be used in high pressure oxygen systems.
Psychosocial Factors and Organizational Management
The term organization is often used in a broad sense, which is not so strange because the phenomenon of an “organization” has many aspects. It can be said that studying organizations makes up an entire problem area of its own, with no natural location within any specific academic discipline. Certainly the concept of organization has obtained a central position within what is called management science—which, in some countries, is a subject in its own right within the field of business studies. But in a number of other subject areas, among them occupational safety and health, there has also been reason to ponder why one is considering organizational theory and to determine which aspects of organization to embrace in research analyses.
The organization is not just of importance to company management, but is also of great significance for each person’s work situation, both in health terms and in relation to his or her short- and long-term opportunities for making an effective contribution to work. Thus, it is of key importance for specialists in the field of occupational safety and health to be acquainted with the theorizing, conceptualization and forms of thinking about social reality to which the terms organization and organizational development or change refer.
Organizational arrangements have consequences for social relationships that exist amongst the people who work in the organization. Organizational arrangements are conceived of and intended to achieve certain social relations at work. A multiplicity of studies on psychosocial aspects of working life have affirmed that the form of an organization “breeds” social relations. The choice between alternative organizational structures is governed by a variety of considerations, some of which have their origins in a particular approach to management and organizational coordination. One form can be based on the view that effective organizational management is achieved when specific social interactions between the organization’s members are enabled. The choice of the structural form in an organization is made on the basis of the way in which people are intended to be linked together to establish organizationally effective interdependent relations; or, as theorists of business administration tend to express the idea: “how the growth of critical combinations is facilitated”.
One of the prominent members of the “human relations school”, Rensis Likert (1961, 1967) has provided an enduring idea on how hierarchical “subsystems” in a complex organizational structure ideally should be linked together. Likert pointed to the importance of unity and solidarity among members of an organization. Here, the job supervisor/manager has a dual task:
- to maintain unity and create a sense of belonging within a work group, and
- to represent his or her work group in meetings with superior and parallel managerial staff. In this way the bonds between the hierarchical levels are reinforced.
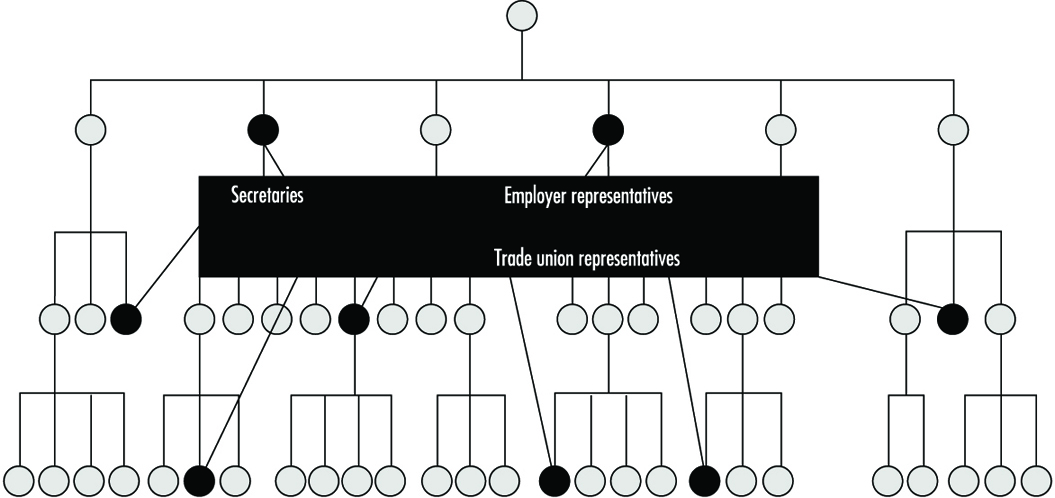
Likert’s “linking pin model” is shown in figure 1. Likert employed the analogy of the family to characterize desirable social interaction between different work units, which he conceived as functioning as “organizational families”. He was convinced that the provision by management of scope and encouragement for the strengthening of personal relations between workers at different levels was a powerful means for increasing organizational effectiveness and uniting personnel behind the goals of the company. Likert’s model is an attempt to achieve “a regularity of practice” of some kind, which would further reinforce the organizational structure laid down by management. From around the beginning of the 1990s his model has acquired increasing relevance. Likert’s model may be regarded as an example of a recommended structure.
Figure 1. Likert’s linking pin model
One way of using the term organization is with the focus on the human beings’ competence; the organization in that sense is the total combination of competences and, if one wants to go a bit further, their synergetic effects. Another and opposite perspective places its focus on the coordination of people’s activities needed to fulfil a set of goals of a business. We can call that the “organizational arrangement” which is decided upon on an agreed basis. In this chapter on organizational theory the presentation has its point of departure in organizational arrangement, and the members or workers participating in this arrangement are looked at from an occupational health perspective.
Structure as a Basic Concept in Organizational Theory
Structure is a common term within organization theory, referring to the form of organizational arrangement intended to bring a goal effectiveness. Business activities in working life can be analysed from a structural perspective. The structural approach has for long been the most popular, and has contributed most—quantitatively speaking—to the knowledge we have on organizations. (At the same time, members of a younger generation of organization researchers have expressed a series of misgivings concerning the value of this approach (Alvesson 1989; Morgan 1986)).
When adopting a structural perspective it is taken more or less for granted that there exists an agreed order (structure) to the form in which a set of activities is carried out. On the basis of this fundamental assumption, the organizational issue posed becomes one of the specific appearance of this form. In how much detail and in which ways have the tasks of persons in different job positions been described in formally issued, official documents? What rules apply to people in managerial positions? Information on the organizational pattern, the body of regulations and specified relations is available in documents such as instructions for management and job descriptions.
A second issue raised is how activities are organized and patterned in practice: what regularities actually exist, and what is the nature of relations between people? Raising this question in itself implies that a complete correspondence between formally decreed and practised forms of activities should not be expected. There are several reasons for this. Naturally, not all phases of work can be covered by a prescribed body of rules. Also, defining operations as they should be carried out will often not be adequate to describe the actual activities of workers and their interaction with each other because:
- The official structure will not necessarily be completely detailed, thus providing different degrees of scope for coordination/cooperation in practice.
- The normative (specified) nature of organizational structure will not match exactly the forms that members of the organization consider to be effective for activities.
- An organization’s stated norms or rules provide a greater or lesser degree of motivation.
- The normative structure itself will have varying degrees of visibility within the organization, depending on the access of members of the organization to relevant information.
In practical terms, it is probably impossible for the scope of any norms which are developed to describe adequately the normal routines that occur. Defined norms simply cannot encompass the full range of practice and relations between human beings. The adequacy of the norms will be dependent on the level of detail in which the official structure is expressed. It is interesting and important in the assessment of organizations and for any preventive programmes to establish the extent of the correspondence between the norms and the practices of organizational activities.
The extent of the contrast between norms and practices (objective and subjective definitions of organizational structure) is important as is the difference between the organizational structure that is perceived by an “investigator” and the individual organizational member’s image or perception of it. Not only is a lack of correspondence between the two of great intellectual interest, it can also constitute a handicap for the individual in the organization in that he or she may have far too inadequate a picture of the organization to be able to protect and/or promote his or her own interests.
Some Basic Structural Dimensions
There has been a long succession of ideas and principles concerning the management of organizations, each in turn striving for something new. Despite this, however, it remains the case that the official organizational structure generally stipulates a form of hierarchical order and a division of responsibilities.Thus, it specifies major aspects of vertical integration and functional responsibility or authorization.
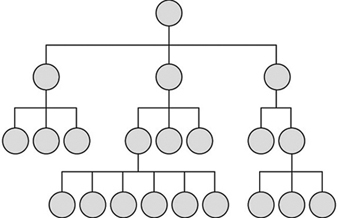
Figure 2. The classical original organizational form

We encounter the idea of vertical influence most readily in its simplest, classical original form (see Figure 2). The organization comprises one superior and a number of subordinates, a number small enough for the superior to exercise direct control. The developed classical form (see figure 3) demonstrates how a complex organizational structure can be built up from small hierarchical systems (see figure 1). This common, extended form of the classical organization, however, does not necessarily specify the nature of horizontal interaction between people in non-management positions.
Figure 3. The extended classical form
An organizational structure mostly consists of managerial layers (i.e., a “triangular” structure, with a few or several layers descending from the apex), and there is almost always a more or less accentuated hierarchically ordered form of organization desired. The basic principle is that of “unity of command” (Alvesson 1989): a “scalar” chain of authority is created, and applied more or less strictly according to the nature of the organizational structure selected. There may be long vertical channels of influence, forcing personnel to cope with the inconveniences of lengthy chains of command and indirect paths of communication when they wish to reach a decision-maker. Or, when there are only a few management layers (i.e., the organizational structure is flat—see Figure 4), this indicates a preference on the part of top management to de-emphasize the supervisor-subordinate relationship. The distance between top management and employees is shorter, and lines of contact are more direct. At the same time, however, each manager will have a relatively large number of subordinates—in fact, sometimes so many that he or she cannot usually exercise direct control over personnel. Greater scope is thereby given for horizontal interaction, which becomes a necessity for operational effectiveness.
Figure 4. The flat organization
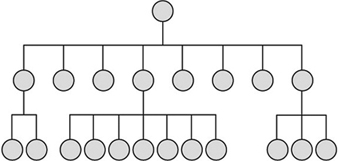
In a flat organizational structure, the norms for vertical influence are only crudely specified in a simple organizational chart. The chart thus has to be supplemented by instructions for managers and by detailed job instructions.
Hierarchical structures may be viewed as a normative means of control, which in turn may be characterized as offering minimum liability to members of the organization. Within this framework there is a more or less generously allocated amount of scope for individual influence and action, depending on what has been decided in relation to the decentralization of decision-making, delegation of tasks, temporary coordinating groups, and the structure of budgetary responsibilities. Where there is less generous scope for influence and action, there will be correspondingly smaller margin for error on the part of the individual. The degree of latitude can usually only be guessed at from the content of the official documents referred to.
In addition to the hierarchical order (vertical influence), the official organizational structure specifies some (normative) form of division of responsibility and thereby functional authority. It might be said that the art of leading an organization as a whole is largely a matter of structuring all its activities in such a way that the combination of different functions arrived at has the greatest conceivable external impact. The names of the different parts (the functions) of the structure specify, albeit only as an outline, how management has conceived the breakdown into various sections of activities and how these shall then be combined and accounted for. From this we can also trace the demands placed on managers’ functional authority.
Modifying the Organizational Structures
There are many variants on how an organization as a whole can be built up. One of the basic issues is how core activities (the production of goods or services) are to be combined with other necessary operational elements, including personnel management, information, administration, maintenance, marketing and so on. One alternative is to place major departments for administration, personnel, company finances and so on alongside production units (a functional or “staff” organization). Behind such an arrangement lies management’s interest in personnel, within their specialized areas, developing a broad range of skills so that they can provide production units with assistance and support, reduce the burden upon them and promote their development.
An alternative to “administration parallel” is to staff production units with people possessing the required specialized administrative skills. In this way cooperation across specialized administrative boundaries can be brought about, thus benefiting the production unit in question. Additional alternative structures are possible, based on ideas concerning functional combinations which would promote cooperative working within organizations. Often organizations are required to respond to change in the operating environment, and hence a change in structure occurs. The transition from one organizational structure to another can involve drastic changes in desired forms of interaction and cooperation. These need not affect everyone in the organization; often they are imperceptible to the occupiers of certain job positions. It is important to take the changes into account in any analysis of organizational structures.
Identifying types of existing structures has become a major research task for many organization theorists in the business administration field (see, for example, Mintzberg 1983; Miller and Mintzberg 1983), the idea being that it would be of benefit if researchers could recognize the nature of organizations and place them in easily identifiable categories. By contrast, other researchers have used empirical data (data based on observations of organizational structures) to demonstrate that limiting description to such strict typologies obscures the nuances of reality (Alvesson 1989). In their view, it is relevant to learn from the individual case rather than simply to generalize immediately to an existing typology. A researcher of occupational health should prefer the latter reality-based approach as it contributes to a better, more adequate understanding of the situational conditions in which the individual workers are involved.
Parallel Structures
Alongside its basic organizational structure (which specifies vertical influence and the functional distribution for core activities), an organization may also possess certain ad hoc structures, which may be set up for either a definite or indefinite time period. These are often called “parallel structures”. They can be instituted for a variety of reasons, such as to further reinforce the competitiveness of the company (primarily serve the company’s interests), as is the case with networking, or to strengthen the rights of employees (primarily serve the interests of employees), such as mechanisms for surveillance (e.g., health and safety committees).
As surveillance of the work environment has as its primary function to promote the safety interests of employees, it is frequently organized in a rather more permanent parallel structure. Such structures exist in many countries, often with operational procedures that are laid down by national legislation (see the chapter Labour Relations and Human Resources Management).
Networking
In modern corporate management, network is a term that has acquired a specialized usage. Creating a network means organizing circles of intermediate-level managers and key personnel from diverse parts of an organization for a specific purpose. The task of the network may be to promote development (e.g., that of secretarial positions throughout the company), provide training (e.g., personnel at all retail outlets), or effect rationalization (e.g., all the company’s internal order routines). Typically, a networking task involves improving corporate operations in some concrete respect, such that the entire company is permeated by the improvement.
Compared with Likert’s linking pin model, which aims to promote vertical as well as horizontal interaction within and between layers in the hierarchical structure, the point of a network is to tie people together in different constellations than those offered by the base structure (but, note, for no other reason than that of serving the interests of the company).
Networking is initiated by management to counter—but not dismantle—the established hierarchical structure (with its functional divisions) which has emerged as being far too sluggish in response to new demands from the environment. Creating a network can be a better option than embarking on an arduous process of changing or restructuring the entire organization. According to Charan (1991), the key to effective networking is that top management gets the network working and selects its members (who should be highly motivated, energetic and committed, quick and effective, and with an ability to easily disseminate information to other employees). Top management should also keep a watchful eye on continued activities within the network. In this sense, networking is a “top-down” approach. With the sanction of management and funds at its disposal, a network can become a powerful structure which cuts across the base organization.
Networking
One example of networking is the recent effort aimed at improving the general level of competence of operators which took place in a Volvo firm. Management initiated a network whose members could work out a system of tasks ordered according to the level of difficulty. A corresponding training programme guaranteed the workers a possibility of following a "career ladder" including a corresponding wage system. The members of the network were selected from among experienced employees from different parts of the plant and at different levels. Because the proposed system was perceived as an innovation, the collaboration in the network became highly motivating and the plan was realized in the shortest possible time.
Implications for Health and Safety
The occupational health specialist has much to gain by asking how much of the interaction between people in the organization rests on the basic organizational structure and how much on the parallel structures that have been set up. In which does the individual actively take part? What is demanded from the individual in terms of effort and loyalty? How does this affect encounters with and cooperation between colleagues, work mates, managers and other active participants in formal contexts?
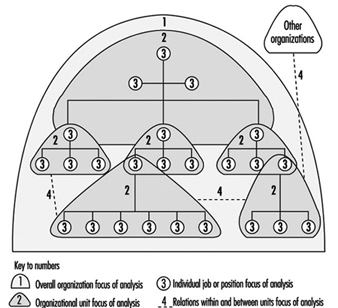
To the occupational health specialist concerned with psychosocial issues it is important to be aware that there is always some person(s) (from outside or inside the organization) who has taken on or been allocated the task of designing the set of normative prescriptions for activities. These “organizational creators” do not act alone but are assisted within the organization by loyal supporters of the structure they create. Some of the supporters are active participants in the creative process who use and further develop the principles. Others are the representatives or “mouthpieces” of personnel, either collectively or of specific groups (see figure 5). Moreover, there is also a large group of personnel who can be characterized as administrators of the prescribed form of activities but who have no say in its design or the method of its implementation.
Figure 5. The organization of occupational safety - a parallel structure
Organizational Change
By studying organizational change we adopt a process perspective. The concept organizational change covers everything from a change in the total macrostructure of a company to alterations in work allocation—coordination of activity in precisely defined smaller units; it may involve changes in administration or in production. In one or another way the issue is to rearrange the work-based relations between employees.
Organizational changes will have implications for the health and well-being of those in the organization. The most easily observed dimensions of health are in the psychosocial domain. We can state that organizational change is very demanding for many employees. It will be a positive challenge to many individuals, and periods of lassitude, tiredness and irritation are unavoidable. The important thing for those responsible for occupational health is to prevent such feelings of lassitude from becoming permanent and to turn them into something positive. Attention must be paid to the more enduring attitudes to job quality and the feedback one gets in the form of one’s own competence and personal development; the social satisfactions (of contacts, collaboration, “belongingness”, team spirit, cohesiveness) and finally the emotions (security, anxiety, stress and strain) deriving from these conditions. The success of an organizational change should be assessed by taking into consideration these aspects of job satisfaction.
A common misconception which may hinder the ability to respond positively to organizational change is that normative structures are just formalities which have no relevance to how people really act or how they perceive the state of affairs they encounter. People who are labouring under this misconception believe that what is important is “the order in practice”. They concentrate on how people actually act in “reality”. Sometimes this point of view may seem convincing, especially in the case of those organizations where structural change has not been implemented for a considerable period of time and where people have got used to the existing organizational system. Employees have become accustomed to an accepted, tried and tested order. In these situations, they do not reflect upon whether it is normative or just operates in practice, and do not care very much whether their own “image” of the organization corresponds with the official one.
On the other hand, it should also be noted that the normative descriptions may seem to provide a more accurate picture of an organization’s reality than is the case. Simply because such descriptions are documented in writing and have received an official stamp does not mean that they are an accurate representation of the organization in practice. Reality can differ greatly, as for example when normative organizational descriptions are so out of date as to have lost current relevance.
To optimize effectiveness in responding to change, one has to sort out carefully the norms and the practices of the organization undergoing change. That formally laid down norms for operations affect and intervene in interactions between people, first becomes apparent to many when they have personally witnessed or been drawn into structural change. Studying such changes requires a process perspective on the organization.
A process perspective includes questions of the type:
- How in reality do people interact within an organization that has been structured according to a certain principle or model?
- How do people react to a prescribed formal order for activities and how do they handle this?
- How do people react to a new order, proposed or already decided upon, and how do they handle this?
The point is to obtain an overall picture of how it is envisaged that workers shall relate to each other, the ways in which this happens in practice, and the nature of the state of tension between the official order and the order in practice.
The incompatibility between the description of organizations and their reality is one of the indications that there is no organizational model which is always “the best” for describing a reality. The structure selected as a model is an attempt (made with a greater or lesser degree of success) to adapt activities of the problems which management finds it most urgent to solve at a particular point in time when it is clear that an organization must undergo change.
The reason for effecting a transition from one structure to another may be the result of a variety of causes, such as changes in the skills of personnel available, the need for new systems of remuneration, or the requirement that the influence of a particular section of functions of the organization should be expanded—or contracted. One or several strategic motives can lie behind changes in the structure of an organization. Often the driving force behind change is simply that the need is so great, the goal has become one of organizational survival. Sometimes the issue is ease of survival and sometimes of survival itself. In some cases of structural change, employees are involved to only a limited extent, sometimes not at all. The consequences of change can be favourable for some, unfavourable for others. One occasionally encounters instances where organizational structures are changed primarily for the purpose of promoting employees’ occupational health and safety (Westlander 1991).
The Concept of Work Organization
Until now we have focused on the organization as a whole. We can also restrict our unit of analysis to the job content of the individual worker and the nature of his or her collaboration with colleagues. The most common term we find used for this is work organization. This too is a term which is employed in several disciplines and within various research approaches.
First, for example, the concept of work organization is to be found in the pure ergonomic occupational research tradition which considers the way in which equipment and people are adapted to each other at work. With respect to human beings, what is central is how they react to and cope with the equipment. In terms of strain and effectiveness, the amount of time spent at work is also important. Such time aspects include how long the work should go on, during which periods of the day or night, with what degree of regularity, and which time-related opportunities for recovery are offered in the form of the scheduling of breaks and the availability of lengthier periods of rest or time off. These time conditions must be organized by management. Thus, such conditions should be regarded as organizational factors within the field of ergonomic research—and as very important ones. It may be said that the time devoted to the work task can moderate the relationship between equipment and worker with respect to health effects.
But there are also wider ergonomic approaches: analyses are extended to take into account the work situation in which the equipment is employed. Here it is a question of the work situation and the worker being well adapted to each other. In such cases, it is the equipment plus a series of work organizational factors (such as job content, kinds and composition of tasks, responsibilities, forms of cooperation, forms of supervision, time devoted in all its aspects) which make up the complex situation which the worker reacts to, copes with and acts within.
Such work organizational factors are taken account of in broader ergonomic analyses; ergonomics has often included consideration of the type of work psychology which focuses on the job content of the individual (kinds and composition of tasks) plus other related demands. These are regarded as operating in parallel with physical conditions. In this way, it becomes the task of the researcher to adopt a position on whether and how the physical and work organizational conditions with which the individual is regularly confronted contribute to aspects of ill-health (e.g., to stress and strain). To isolate cause and effect is a considerably more difficult undertaking than is the case when a narrow ergonomic approach is adopted.
In addition to the work organizational conditions to which the individual is regularly exposed there are a number of work organizational phenomena (such as recruitment policies, training programmes, salary systems) which may be more peripheral, but still have decisive importance in terms of what is offered to the worker by his or her immediate work situation. This broader spectrum (and one might still wonder whether it has been treated broadly enough) is of interest to the researcher who wishes to understand the relationship between the individual worker and activities as a whole.
Organizational Psychology
Whereas work psychology has its focus on the individual’s occupational tasks and connected job demands in relation to the individual’s capacity, the subject of organizational psychology refers to individuals as defined by the place they occupy within an organization, as organizational members more or less outwardly visible, more or less active. The point of departure for the organizational approach is the operation of a company or organization and those various parts of it in which individuals are themselves involved.
Carrying out activities requires various organizational arrangements. A unifying organizational structure is required; activities as a whole need to be broken down into identifiable job tasks. A task structure has to be created in accordance with selected job distribution principles. Thus, management systems, technical systems and maintenance routines are all required; and, in many cases, there is a need for special safety systems and occupational health promotion systems in addition to the legally required safety organization.
In addition to the structural requirements for accomplishing tasks, systems for remuneration and control must be implemented. Co-determination systems and systems for skills development and training (not least so that the technical systems can be mastered) must all be in operation. All of these systems can be described as organizational factors. They have the character of formalized activities designed to achieve a specific purpose, and have a parallel existence within the company. As mentioned above, they may be either permanent or instigated for a shorter or longer temporary period, but they all have some sort of influence on the terms on which the individual works. They can be examined from various psychosocial perspectives: as support resources for the worker, as control instruments employed by management, or as success factors for management or employees. The interaction between these various organizational systems is of the greatest interest: their aims are not always compatible; rather, they can be on a collision course. The “bearers” of the systems are human beings.
Organizational Change and its Psychosocial Aspects
To survive as an organization, management must constantly pay attention to what is going on in the world outside, and must be constantly ready for change. Sudden changes forced by outside influences—such as a loss of interest by a major customer, changes in demand, sudden appearance of new competitors, demands for information from government authorities or governmental acts which restructure the public sector—must produce immediate but rational reactions from management. The reaction is often to reorganize part or all of the business activity. Most of the time, the situation is hardly one that puts the needs of health of the individual in the foreground, or provides the time required for long-drawn-out participation of employees in negotiations over change. Even if, in the long run, such negotiations would have been constructive, the fact is that management usually places its hope in the obedience and trust of the employees. Those who want to remain employed must accept the situation.
Karasek (1992) in a survey of papers written for the ILO distinguishes between planned organizational changes with regard to the extent to which they are “expert-directed” or “participation-directed”. The projects did not display any national differences with regard to the relative weight placed on expert and participation direction. However, it is maintained (Ivancevich et al. 1990) that the role of top management is important in organizational-change projects designed to reduce the presence of occupational stress and improve workers’ well-being and health. Such interventions require the collaborative efforts of management/staff and employees, and possibly also of experts.
When structural changes occur, it is inevitable that feelings of uncertainty will arise in all members of the organization. Despite the fact that all will experience uncertainty, the degree and types of uncertainty will vary according to position in the organization. The prerequisites for gaining a true picture of how well or badly the company is proceeding in the changes are completely different at the management and employee levels. At the risk of oversimplifying the situation somewhat, we can speak of two types of feelings of uncertainty:
1. Knowing about the uncertainty of the organization’s continued existence or success. This type of uncertainty feeling will be found in decisionmakers. “Knowing about the uncertainty” means that the person in question can make an evaluation of the relative advantages and disadvantages in coping with the uncertain situation. He or she has the opportunity to deal with the situation actively (e.g., by obtaining more information, trying to influence people and so on). Alternatively, a person can react to the change negatively by trying to avoid the situation in various ways, such as seeking other employment.
2. Not knowing about the uncertainty of the organization’s continued existence or success. This type of uncertainty will be found in employees in non-decision-making posts. “Not knowing about the uncertainty” means that the individual has difficulty in making a judgement and generally has only the opportunity to react passively (taking a wait-and-see approach, remaining in an unsettled and diffuse state, letting others take action).
Psychologically, especially when trying to prevent environmental effects of work, these differing feelings of uncertainty are very important. One side will feel alienated toward the subjective reality of the other side. The initiative for a change in organization usually comes from high up in the hierarchy, and the primary aim is increased efficiency. Work on organizational change revitalizes a manager’s work content since change brings about new conditions which must be dealt with. This can become a positive challenge, often a stimulation. Among non-management employees, a reorganization has a more conditional function: it is a good thing only to the extent that it improves, or leaves unaltered, the employees’ current and future work situation.
From a more detached perspective, people in specialist administrative positions or organizational experts may show a third reaction pattern: the reorganization is interesting, whatever the result. It can be looked on as an experiment showing how the employees and the business are affected—knowledge that will be of value in the future to an administrator or organizational expert in the same or another company.
Changes in organization are complicated actions not only because of the practical changes that must be introduced, but also because they often have psychological and psychosocial consequences. The result is that the atmosphere at work reflects differing interests in the proposed changes and various types of psychic stress. Also this complex social reality is difficult to study in a systematic way.
Business economists, sociologists, and psychologists differ in their approach to interpreting the links between organizational change and individual working conditions. The psychology of work and organization directs attention to the employees and to the conditions under which they labour. An effort is made to obtain systematized knowledge about the effects of organizational change on individual health and work opportunities. It is this approach that gives us information on the occupational mental health consequences.
In organizational sociology the individual conditions upon which organizational change has an impact are mostly analysed in order to understand/describe/discover the consequences for the content of intergroup and interorganizational relationships and dependencies. In the business and administrative sciences there may be an interest in psychological aspects, with the aim of understanding certain attitudes and behaviours of the members of the organization (sometimes only those of the key persons in some sense) crucial for the progress of business activities.
Measurement of Organizational Factors
Organizational factors, division of work, decentralization, reward systems are not physical objects! They are intangible. It is not possible to take hold of them, and most of them express themselves in activities and interactions which disappear with greater or lesser rapidity, only to be replaced by new ones. Those work organization dimensions which it is possible to “measure” (in roughly the same way as is the case with physical factors) are, not surprisingly, also the ones that a researcher with a background in the natural sciences finds most manageable and acceptable. Time, for example, can be measured objectively, with a measuring instrument that is independent of the human being. How work is organized in terms of time (the time spent at work and time for breaks and lengthier periods of rest) can scarcely cause major measurement problems for ergonomists. On the other hand, the individual’s own perception of aspects of time is psychological, and this is considerably more difficult to measure.
It is also relatively easier for the investigator to come to terms with work organizational factors that are given material form. This is what happens when instructions for managers, job descriptions and work procedures are put in writing, and also applies when control systems and forms of personnel coordination are documented. The systematic analysis of the contents of these texts can provide useful information. However, it should be remembered that actual practice can deviate—sometimes significantly—from what is prescribed in writing. In such cases, it is not so easy to obtain a systematic picture of people’s activities and attitudes.
Taking the Step from Conceptualization toEmpirical Study
Measurement of organizational phenomena is based on a variety of information sources:
- written prescriptions of operational and coordinative procedures
- investigators’ systematic observation of work behaviour and social interaction
- employees’ self-reports on behaviour, interactions, activities, attitudes, intentions and thoughts
- policy documents, agreements, minutes of conferences, long-term prospects
- views of key persons.
Which kind of information should be given priority has to do partly with the kind of organizational factor to be assessed and with method preferences, and partly with the organization’s generosity to let the investigator explore the field in the way he or she prefers.
Measurement in organizational research is seldom an either/or issue, and is most often a “multisource” enterprise.
In measuring organizational change it is even more necessary to give attention to the characteristic features. A great deal happens in interpersonal relationships before and at a very early stage after change is initiated. In contrast to laboratory experiments or in meetings where group questionnaires can be taken, the situation (i.e., the process of change) is not under control. Researchers who study organizational change should find this unpredictable process fascinating and not be irritated by it or be impatient. Industrial sociologists ought to have the same feeling. The idea of evaluating final effects should be abandoned. We must realize that preventive work consists of being at hand the whole time and providing adequate support. One should be especially careful with formal superior-subordinate (employee) situations.
Evaluating the research on organizational change from an occupational health perspective leads to the conclusion that there has been a great variation of interest shown in the health of employees, especially their psychosocial health, when organizational changes are taking place. In some cases the matter has been left totally to chance, with a complete lack of interest or consideration by top management and even among members of safety and health committees. In other cases there may be an interest, but no experience to base it on. In some cases, however, one can glimpse a combination of efficiency and health reasons as the motivation for organizational change. The case in which the main objective is to preserve or improve employee psychosocial health is a rarity. However, there is a growing awareness of the importance of considering employee health during all stages of organizational change (Porras and Robertson 1992).
During organizational change, relationships should ideally be marked by a feeling of cooperation, at least at the informal level. Resources for all these activities are available in many present-day companies with their personnel functions, their department charged with organization, company-run occupational health departments and interested union representatives. In some of these companies there is also a more explicit philosophy of prevention directing management on different levels towards an effective use of all these resources and moving the professionals of these various functions towards fruitful cooperation. This visible trend to consider occupational health aspects in the implementation of organizational change may hopefully expand—something which, however, requires more consciousness among occupational health-experts of the importance of being well acquainted with the thinking and theorizing on organizational conditions.
International Association of Labour Inspection (IALI)
Historical Perspective and Raison d’être
The International Association of Labour Inspection (IALI) was founded in 1972 in order to provide a professional forum for the exchange of information and experience between inspectors about their work. It promotes closer cooperation and greater understanding between inspectorates, authorities and other institutions of the role, the realities and challenges of labour inspection. The statutes exclude any political, trade union or religious activity and any judgement in respect of the labour law or inspection systems of individual states. The Association is a non-governmental organization (NGO) recognized by the ILO.
Structure and Membership
In 1996, the General Assembly (which meets every three years at the same time as the Triennial Congress) elected a seven-person Executive Committee (EC). The EC elected the President (Germany) and appointed the Honorary Secretary (United Kingdom) as well as the Honorary Treasurer (Switzerland). The four Vice-Presidents came from Spain, Denmark, Tunisia and Hungary. The EC meets as necessary to manage the affairs of the Association, whose registered office is at 23 rue Ferdinand-Hodler, CP3974/1211, Geneva 3, Switzerland. The Secretariat is located at: Hessisches Ministerium fur Frauen, Arbeit und Sozialordnung, Dostojewskistrasse 4, 65187 Wiesbaden, Germany. Tel: +49-611-8173316; Fax: +49-611-86837.
Membership of IALI is open to:
- national and regional labour departments (directorates of labour inspection, safety and hygiene directorates and so on)
- national groups of labour inspectors (associations, unions and so on).
There is an annual membership fee which is dependent upon the size of the organization making the application. This covers the expenses of organizing the programme of activities. In September 1995 the Association comprised 65 member organizations from 50 countries. The majority of members are now labour departments or labour inspectorates.
Activities
By gathering and summarizing information and documentation on particular aspects of labour inspectorate work and by undertaking comparative studies among its members, the Association promotes professional understanding of all aspects of labour inspection and provides opportunities for the exchange of views between practitioners. The technical symposia (organized jointly with member countries) and the triennial congress let inspectors get to know their colleagues personally, to exchange information on problems, solutions and new developments, and to develop their own thinking. These meetings also serve to focus attention in a practical way on a wide range of specific, but carefully chosen, aspects of labour inspection, thus promoting greater consistency of practice between inspectorates in different countries. The proceedings are published and a regular newsletter is also sent to members.
The programmes of IALI are devoted exclusively to the distribution of information collected through international enquiries based on questionnaires and reports from international or regional symposia. There is an international congress every three years in Geneva, undertaken with the generous technical assistance of the ILO at the time of its annual international conference. The ILO also collaborates in the organization of many of the symposia. Since 1974 programmes have been devoted to the study of a wide range of practices in the field of safety, health and the working environment. Topics have included recording systems for premises and accidents, methods of inspecting smaller enterprises, the problems of large construction sites and the use of computers by inspectors. The Association has considered causes of accidents and other problems in relation to the use of robots and other programmable electronic systems. More recently its symposia and congresses have included topics as diverse as human factors, training of inspectors, inspection of public services, child labour, agriculture, risk assessment and occupational health.
The Changing World of Work
The need for a more effective exchange of information and experience has been stimulated by a number of significant developments in the field of labour inspection, including:
- the increasing complexity and breadth of coverage of labour law
- the introduction of new concepts of oversight such as risk assessment and risk management
- the scale and breadth of technological innovation (seen, for instance, in the introduction of new chemicals and compounds, the increasing reliance on programmable electronic systems, genetic manipulation, new applications for ionizing radiation or generally the growth in the use of information technology)
- the changing structure of industry in established market economies, in countries in transition to a market economy and in developing countries
- the growth, in part as a result of the previous development, in the number of small and medium-sized enterprises
- the decline in membership and influence of trade unions, particularly in many industrial market economies
- the pressure on labour inspectorates themselves through budgetary constraints and demands by government that they justify their existence and demonstrate (and where possible improve) their efficiency and effectiveness.
Challenges to Inspection
Affecting all these issues is the increased emphasis on the human factor. Labour inspectors need to analyse, understand and constructively use their skills to help employers and employees to take this central element into account in developing preventive strategies for health and safety. In many countries too there is increasing public awareness of and concern about the consequences of work and work processes. In much forward-looking legislation this is expressed as the aim that no one should be harmed in any way by the need to work. But it is also evident in concerns about the impact of industry and commerce on the environment and the quality of life.
Labour inspectors cannot simply ignore these trends; they have to take the initiative and explain through the media their role, the advice they give and the effect of their compliance work, in order to promote confidence in the constructive work they do. Inspectorates throughout the world have had to review how they work, set their priorities and carry out their inspections so they can devote more time and more of their limited resources to productive activities.
The exchange of information and experience about all these matters is of enormous interest to inspectors. For whilst inspectorates operate in very different political, economic, legal and social climates, experience shows that they have many practical concerns in common and can benefit in a very instructive way from the experience, the different viewpoints, the ideas and the successes and failures of their colleagues in other countries.
The International Commission on Occupational Health (ICOH)
Historical Perspective and Raison d’être
The International Commission on Occupational Health (ICOH) is an international non-governmental professional society whose aims are to foster the scientific progress, knowledge and development of occupational health and safety in all its aspects. It was founded in 1906 in Milan as the Permanent Commission on Occupational Health. Today, ICOH is the world’s leading international scientific society in the field of occupational health, with a membership of 2,000 professionals from 91 countries. The ICOH is recognized by the United Nations and has close working relationships with ILO, WHO, UNEP, CEC and ISSA. Its official languages are English and French.
At its founding the Commission had 18 members representing 12 countries. One of its primary tasks was to organize international congresses every three years to exchange ideas and experience among leading scientists in occupational health, a tradition which has continued to this day, with the 25th Congress held in 1996 in Stockholm.
After the London Congress in 1948 the international interest was evident and the Commission was internationalized with changes in its constitution, and the name was changed to Permanent Commission and International Association on Occupation Health, a change finalized in 1957. The internationalization and democratization of the commission grew with time and in 1984 the present name was established.
ICOH provides a forum for scientific and professional communication. To achieve this purpose, the ICOH:
- sponsors international congresses and meetings on occupational health
- establishes scientific committees in various fields of occupational health and related subjects
- disseminates information on occupational health activities
- issues guidelines and reports on occupational health and related subjects
- collaborates with appropriate international and national bodies on matters concerning occupational and environmental health
- takes any other appropriate action related to the field of occupational health
- solicits and administers such funds as may be required in furtherance of its objectives.
Structure and Membership
The ICOH is governed by its officers and board on behalf of its membership. The officers of the ICOH are the President, two Vice-Presidents and the Secretary-General, while the board comprises the past president and 16 members elected from among the general membership. Further, if necessary the President may co-opt two members to the board to represent underrepresented geographical areas or disciplines.
ICOH has both individual and collective members. An organization, society, industry or enterprise may become a sustaining member of the ICOH. A professional organization or a scientific society may become an affiliate member.
Sustaining members may nominate a representative who fulfils the criteria for full membership and enjoys all the benefits of an individual member. An affiliate member may nominate one representative who fulfils the criteria for full membership and enjoys the same rights as a full member. ICOH’s individual members have a wide professional distribution and include medical doctors, occupational hygienists, occupational health nurses, safety engineers, psychologists, chemists, physicists, ergonomics, statisticians, epidemiologists, social scientists and physiotherapists. These professionals work either for universities, institutes of occupational health, governments or industries. At the end of 1993, the largest national groups were those of France, the United States, Finland, Japan, United Kingdom and Sweden, each with more than 100 members. Sustaining and affiliate members can be represented in the General Assembly, and can participate in the activities of scientific committees; they can also submit materials for publication in the newsletter, which also keeps them informed of ongoing and planned activities.
Activities
The most visible activities of ICOH are the triennial World Congresses on Occupational Health, which are usually attended by some 3,000 participants. The 1990 Congress was held in Montreal, Canada, and in 1993 in Nice and the 1996 Congress in Stockholm. The Congress in the year 2000 is scheduled to be held in Singapore. The venues of the triennial congresses since 1906 are listed in table 1.
Table 1. Venues of triennial congresses since 1906
|
Venue |
Year |
Venue |
Year |
|
Milan |
1906 |
Madrid |
1963 |
|
Brussels |
1910 |
Vienna |
1966 |
|
Vienna (cancelled) |
1924 |
Tokyo |
1969 |
|
Amsterdam |
1925 |
Buenos Aires |
1972 |
|
Budapest |
1928 |
Brighton |
1975 |
|
Geneva |
1931 |
Dubrovnik |
1978 |
|
Brussels |
1935 |
Cairo |
1981 |
|
Frankfurt |
1938 |
Dublin |
1984 |
|
London |
1948 |
Sydney |
1987 |
|
Lisbon |
1951 |
Montreal |
1990 |
|
Naples |
1954 |
Nice |
1993 |
|
Helsinki |
1957 |
Stockholm |
1996 |
|
New York |
1960 |
Singapore |
2000 |
At present the ICOH has 26 scientific committees and four working groups, listed in table 2. Most of the committees have regular symposia, publish monographs and preview the abstracts submitted to the international congresses. ICOH issues a quarterly newsletter, which is circulated to all members free of charge. The bilingual newsletter contains congress reports, reviews of publications, a list of coming events and information on research and education, and other announcements relevant to members. Several of the scientific committees also publish monographs and proceedings from their meetings. ICOH keeps a computerized membership file, which is printed at regular intervals and circulated to the membership. The ICOH sponsors its scientific journal, the International Journal of Occupational and Environmental Health (IJOEH). The journal is available for members at a very affordable subscription rate.
Table 2. List of ICOH scientific committees and working groups, 1996
Scientific committees
1. Accident prevention
2. Ageing and work
3. Agriculture
4. Cardiology
5. Chemical industry (Medichem)
6. Computing in occupational and environmental health
7. Construction industry
8. Developing countries
9. Education and training
10. Epidemiology in occupational health
11. Fibres
12. Health-care workers
13. Health services research and evaluation
14. Industrial hygiene
15. Musculoskeletal disorders
16. Neurotoxicology and psychophysiology
17. Occupational health nursing
18. Occupational toxicology
19. Organic dusts
20. Pesticides
21. Radiation and work
22. Occupational health services in small industries
23. Shiftwork
24. Toxicology of metals
25. Work-related respiratory disorders
26. Vibration and noise
Scientific working groups
1. Occupational and environmental dermatoses
2. Handicap and work
3. Reproductive hazards in the workplace
4. Thermal factors
International Social Security Association (ISSA)
Raison d’être and Historical Perspective
The aim of the ISSA is to cooperate, at the international level, in the defence, promotion and development of social security throughout the world, basically through its technical and administrative improvement. The prevention of social risks is today considered to form an integral part of social security.
The ISSA had an early forerunner, the Permanent International Committee on Social Insurance (CPIAS), which at first was concerned with the risk of accidents and in 1891 extended its scope to social insurance in general. In 1927, the Tenth Session of the International Labour Conference adopted Convention No. 24, known as the Sickness Insurance (Industry) Convention, and Convention No. 25, known as the Sickness Insurance (Agriculture) Convention. The ISSA was founded at this time, upon the initiative of the International Labour Office, with the aim of gaining support from experts in a number of European countries for the ratification of these instruments. Until 1947 the organization was known as the International Conference of Sickness Insurance Funds and Mutual Benefit Societies (CIMAS).
The concept of prevention already existed in the minds of the CIMAS pioneers when they included this notion in the fundamental policy principles adopted by their Constituent Assembly. It was not until 1954, however, that the Association became actively involved in occupational safety and health activities, through the establishment of its Permanent Committee on Prevention of Occupational Risks. It should be noted that, in this respect, the role of the ISSA is complementary to that of the ILO. The ISSA’s experts may not only be instrumental in bringing about ILO Conventions and Recommendations, but are also called upon to implement them.
Although prevention programmes are obviously most prevalent in the field of occupational safety and health, over the last two decades prevention has gained increasing importance in other branches of social security as well, particularly as regards sickness insurance and, more recently, unemployment insurance, as may be seen from the activities of ISSA Permanent Committees. Over the last decade, activities aimed at preventing employment accidents and occupational diseases have undergone considerable changes in modern industrialized societies, as elaborated below concerning the “Prevention Concept” of the Association.
Structure and Membership
The ISSA is an international organization of services, institutions or bodies administering one or more branches of social security or mutual benefit societies. It has its offices at the headquarters of the ILO in Geneva.
The Association has two categories of membership—affiliate membership, for government departments, central institutions and national federations of institutions administering social security or one of its branches at the national level, and associate membership, open to national non-profit institutions, such as research and safety and health institutions, the aims of which are compatible with those of the Association, but which are not qualified to become affiliate members.
In 1995 the ISSA had over 240 affiliate member organizations in 117 countries, and 95 associate member institutions in 35 countries, for a total membership of some 338 organizations in 127 countries around the world. More than 200 member institutions are directly involved in insurance against employment accidents and occupational diseases and/or in the prevention of accidents and the promotion of safety and health.
Figure 1. Structure of the International Social Security Association (ISSA)

As can be seen from the organigramme (figure 1), all ISSA activities are directed by the General Assembly, which is comprised of delegates appointed by member institutions and is sometimes described as the world parliament of social security. The Council, which consists of one delegate from each country having affiliate member institutions, meets regularly on the occasion of the Association’s triennial General Assemblies. The Bureau, which together with the Council gives effect to the decisions taken by the General Assembly, meets twice a year and is composed of 30 elected members and the Chairpersons of the Permanent Committees.
Activities
The Association has three main programmes:
- Regional activities. These are aimed at serving the special needs of member institutions in the various parts of the world. For this purpose the ISSA has regional offices for Africa, the Americas, Asia and the Pacific and Europe situated in Abidjan, Buenos Aires, Manila and Paris respectively.
- Research and documentation. Worldwide developments and trends in social security are monitored and analysed from the perspective of national and cross-national research through a network of correspondents. The Association maintains the largest social security library in the world and collaborates with the ILO’s Social Security Department in providing timely social security information.
- Technical activities. Ten Permanent Committees and a Study Group each deal with a specific branch or aspect of social security. They investigate sector-specific problems such as those relating to health insurance, pension insurance, unemployment insurance, family protection, rehabilitation, organization and methods, actuarial and statistical issues.
The Permanent Committee on Insurance against Employment Accidents and Occupational Diseases and the Permanent Committee on Prevention of Occupational Risks with its 11 International Sections on Accident Prevention are of particular importance in fostering safety and health.
The Permanent Committee on Prevention of Occupational Risks
Two different and complementary aspects (i.e., promotional activities related to prevention, and technical activities) fall within the scope of competence of this Committee, which together with its Advisory Council monitors worldwide developments and undertakes surveys and studies on overall problem areas.
The Committee is charged with undertaking at the international level the following types of activities for the prevention of occupational risks:
- exchange of information and experience
- organization of international meetings and World Congresses
- implementation of surveys and promotion of research in the field of prevention of occupational risks
- coordination of the activities of the ISSA International Sections for the Prevention of Occupational Risks
- cooperation with the ILO and other agencies active in the prevention of occupational risks
- other measures appropriate to the purposes of the Committee.
World Congresses
Since 1955 the ILO and the ISSA have organized triennial World Congresses on Occupational Safety and Health in cooperation with the ISSA member institutions and ILO constituents concerned in the host country. It is not easy to quantify the extent to which the World Congresses have kept pace with the different stages of development in the prevention of occupational risks coinciding with the social, economic and industrial progress of the past 25 years, or the extent to which they have given a lead to or encouraged this development. There is no doubt however that the resultant exchange of ideas and information relating to recent research and to its practical application in different countries, both at the national level and within industry, has enabled a large number of participants in these Congresses to be cognizant of the many changes being introduced. This, in turn, has enabled them to make a greater contribution to their particular field of activity.
The last four World Congresses took place in Ottawa-Hull (1983), Stockholm (1987), Hamburg (1990), New Delhi (1993) and Madrid (1996). In 1999, the site is Brazil.
ISSA International Sections for Prevention
Since the end of the 1960s, on the advice of the Permanent Committee on Prevention of Occupational Risks and its Advisory Council, the Bureau of the ISSA has set up 11 International Sections for the Prevention of Occupational Risks. Eight of them deal with accident prevention in various sectors of industry and agriculture and three deal respectively with information techniques, research in the area of occupational safety and health, and education and training for prevention of accidents.
Each ISSA International Section is represented by its Chairman and Secretary General on the Advisory Council of the Permanent Committee, which advises the Bureau of the Committee on fundamental questions relating to the activities of the Committee and its International Sections. A concrete example is the prevention concept (discussed separately below).
The International Sections are financially autonomous, having a decentralized structure and their own membership consisting of full members, associate members and corresponding members. Full membership is open to ISSA member institutions and other non-profit organizations; profit-making entities with activities compatible with the area of competence of a Section may be admitted as associate members, and individual experts may apply for corresponding membership. The Secretariats of the Sections are provided in various countries by member institutions of the ISSA specialized in the respective fields.
Each Section is a clearing house for information in its own area of competence. All Sections organize international symposia, round tables and expert meetings, the proceedings and reports of which are published in the ISSA Prevention Series 1000. The Sections currently have some 45 internationally composed working groups working on specific topical subjects, which range, for example, from safety advice for migrant workers in the construction industry or a checklist for the classification of machines on the basis of ergonomic principles, to safe working with biological agents. The findings of these working groups are published as technical brochures in the ISSA Prevention Series 2000. Most titles exist in English, French and German, some also in Spanish and other languages. Such publications may be ordered directly from the Secretariat of the Section concerned.
Of special interest are the International Film and Video Festivals, which are held during World Congresses and for which a Working Group of the Electricity Section forms a clearing house. All productions submitted to these festivals are listed in a catalogue in four languages which is available free from this Section.
A brief description of each of the ISSA International Sections follows.
ISSA International Section for Research.
The Section offers the latest information on both current and planned research projects worldwide. Two data banks allow quick and efficient access to this information. The Working Group “Research Concepts” promotes the necessary theoretical bases to effectively ensure that more than in the past research further serves both the field and the more practical implementation of research results.
ISSA International Section on Information.
The Information Section provides information on efficient information techniques. The Working Group “Safety and Health Periodicals” informs safety experts on the most effective way to reach their audience. The Section offers expert advice on “advertising for safety”.
ISSA International Section for the Mining Industry.
The Section deals with the classical risks of underground work in coal mines (darkness, dust, heat, gases, explosions, cave-ins) and concerns itself with the training of mine rescue teams.
ISSA International Section for the Chemical Industry.
Although new substances result in new risks, the chemical industry has developed high safety standards that have proven to be exemplary. The Chemical Section strives to ensure that these safety standards transcend borders just as much as—if not even more than—risks do.
ISSA International Section for the Iron and Metal Industry.
The high accident rate in this important branch of activity must be reduced. Safety strategies are developed against the most frequent hazards and causes of accident. The Section’s Working Groups are primarily concerned with new technologies and substitutes for dangerous working substances.
ISSA International Section for Electricity.
“Invisible” energy generates many invisible risks. The Section evolves recommendations for practical accident prevention, principles for a regulatory control of electrical appliances and systems, backed up by effective first aid measures in the event of electrical accidents. The Section maintains a clearinghouse for films and videos in the field of safety, health and the environment.
ISSA International Section for the Construction Industry.
The extremely high accident risks in the construction industry call for a safety strategy that can deal with the continuous changes of the working environment on construction sites. The Section’s aim is not only to solve individual problems, but to increase safety and accident prevention in construction industry operations overall, especially by intensified cooperation between the various trades working on the same site.
ISSA International Section for Agriculture.
The mechanization of agriculture and the use of chemical substances in agriculture are worldwide problems. The Section advocates a rapid socio-technical evolution in the light of the technical revolution, while endeavouring to ensure that the production of food does not put life at risk.
ISSA International Section for Machine Safety.
The Section deals with system safety and accident prevention relating to machines, appliances, apparatus and systems. Standardization of safety appliances, ergonomic questions, noise reduction, safety switches and the prevention of dust explosions are focal points of the Section’s Working Groups.
ISSA International Section for Education and Training.
Technical progress is expanding in all areas of life; but at the same time it brings along new risks. The major factor in accidents is the lack of education and training in the field of safety. Safety must be an integrated part of human behaviour in all areas of life. The Section deals with pedagogical aspects of education and training for prevention and aims at a global approach of prevention, making use of the experiences gained in prevention at the workplace for safety in all areas of life.
ISSA International Section for Health Services.
The Section endeavours through international cooperation to overcome the safety deficits in the health sector. The health sector has typical professional risks which in part differ greatly from those in other fields of activity—for instance, direct exposure to diseases, risks from medications, particularly gas anaesthetics, disinfectants and infectious waste.
The ISSA Prevention Concept “Safety Worldwide”
The ISSA Bureau adopted this concept in October 1994 under the title “ISSA Prevention Concept ‘Safety Worldwide’—The Golden Path to Social Policy”.
Because only seven out of every 100 fatal accidents are work accidents, with all others occurring in traffic, in the home, during sports or at school, the concept seeks to make meaningful use, in other areas, of the experience gained in prevention in the world of work.
Starting from the viewpoint that the preservation of health is a fundamental mission of humanity and thus a central aim of social security, the concept calls for the interlinking of prevention, rehabilitation and compensation and for the preservation of an intact environment. Emphasis will be laid on the human factor at the planning, organization and implementation stages and the need to begin education in prevention during early childhood. Efforts will be made to address all those who, through their own activities, can provide better protection against hazards for individuals. These include legislators and standard-setters, social partners, persons responsible for developing, planning, designing and manufacturing products and services, and school curriculum planners and teachers, as well as information specialists in public information work, occupational health physicians, supervisory and consultative bodies, responsible officials in social and private insurance, decision-makers and programme managers in international organizations, professional and other organizations and so on—and, last but not least, parents and children.
The thorough promotion of safety and health at work and elsewhere requires measures of three types—technical measures, behavioural change measures and organizational measures. To this end, the ISSA’s prevention concept defines three levels of intervention:
- informing the general public and developing awareness relating to safety and health matters through the mass media, newspapers, brochures, posters and so on
- achieving both broad and in-depth impact by seeking to change attitudes and behaviour through agents with a multiplier effect and using target-group-specific media and techniques such as educational films and other educational materials
- aiming at an in-depth impact on groups directly at risk through specific measures such as counselling or subject-specific brochures.
The first step in the implementation of the concept will be a stock-taking of prevention activities to determine regional needs and deficiencies. An inventory of existing support facilities and materials will also be drawn up. In addition, the ISSA will step up its information and research activities and its programme of meetings, strengthen cooperation with international organizations active in the prevention field, and take their projects into account in its own activities.
In summary, the only sure way to success lies in cooperation between prevention, rehabilitation and compensation services; the positive experiences of prevention within enterprises must be carried over into non-occupational fields; and greater account must be taken of the human factor.
Publications
The ISSA issues a whole range of periodical and non-periodical publications, studies, surveys, newsletters and bulletins; further information concerning them is contained in the ISSA Catalogue of Publications, which may be ordered free of charge at the following address: ISSA, Case postale 1, CH-1211 Geneva 22, Switzerland.
In addition to the proceedings of World Congresses on Occupational Safety and Health, which are published by the National Organizing Committee of the host country, the publications issued by the International Sections are listed in the ISSA Prevention Series 1000 and 2000, and are also available at the above address.
International Organization for Standardization (ISO)
The International Organization for Standardization (ISO) is a worldwide federation of national standards bodies at present comprising the national standards bodies of 120 countries as of 1996. The object of ISO is to promote the development of standards in the world with a view to facilitating international exchange of goods and services and to developing mutual cooperation in the sphere of intellectual, scientific, technological and economic activity. The results of ISO technical work are published as International Standards.
The scope of ISO is not limited to any particular branch; it covers all standardization fields except standards for electrical and electronic engineering, which are the responsibility of the International Electrotechnical Commission (IEC).
ISO brings together the interests of producers, users (including consumers), governments and the scientific community in the preparation of International Standards.
ISO work is carried out through some 2,800 technical bodies. More than 100,000 experts from all parts of the world are engaged in this work which, to date, has resulted in the publication of over 10,000 International Standards, representing some 188,000 pages of concise reference data in English and French.
Origin and Membership
International standardization started in the electrotechnical field some 90 years ago. While some attempts were made in the 1930s to develop International Standards in other technical fields, it was not until ISO was created that an international organization devoted to standardization as a whole came into existence.
Following a meeting in London in 1946, delegates from 25 countries decided to create a new international organization “whose object shall be to facilitate the international coordination and unification of industrial standards”. The new organization, ISO, began to function officially on 23 February 1947.
A member body of ISO is the national body “most representative of standardization in its country”. It follows that only one such body for each country is accepted for membership in ISO. Member bodies are entitled to participate and exercise full voting rights on any technical committee of ISO, are eligible for membership in the Council and have a seat in the General Assembly. By September 1995 the number of member bodies was 83. More than 70% of ISO member bodies are governmental institutions or organizations incorporated by public law. The remainder have close links with the public administration in their respective countries.
A correspondent member is normally an organization in a developing country which does not yet have its own national standards body. Correspondent members do not take an active part in the technical work, but are kept fully informed of it. Normally, a correspondent member becomes a member body after a few years. Nearly all the present correspondent members are governmental institutions. By September 1995 the number of correspondent members was 24.
A third category, subscriber membership, has been established for countries with smaller-scale economies. These subscriber members pay reduced membership fees that nevertheless allow them to maintain contact with international standardization. By September 1995, the number of subscriber members was eight.
Basic data on each ISO member body are given in the publication ISO Membership.
Technical Work
The technical work of ISO is carried out through technical committees (TC). The decision to set up a technical committee is taken by the Technical Management Board, which also approves the scope of the committee. Within this scope, the committee determines its own programme of work.
The technical committees may, in turn, create subcommittees (SC) and working groups (WG) to cover different aspects of the work. Each technical committee or subcommittee has a secretariat assigned to an ISO member body. At the end of 1995 there were in existence 185 technical committees, 611 subcommittees and 2,022 working groups.
A proposal to introduce a new field of technical activity into the ISO working programme normally comes from a member body, but it may also originate from some other international organization. Since resources are limited, priorities must be established. Therefore, all new proposals are submitted for consideration by the ISO member bodies. If accepted, either the new work will be referred to the appropriate existing technical committee or a new committee will be created.
Each member body interested in a subject for which a technical committee has been authorized has the right to be represented on that committee. Detailed rules of procedure are given in the ISO/IEC Directives.
International Standards
An International Standard is the result of an agreement between the member bodies of ISO. It may be used as such or implemented through incorporation into national standards of different countries.
An important first step towards an International Standard takes the form of a committee draft (CD), a document circulated for study within the technical committee. This document must pass through a number of stages before it can be accepted as an International Standard. This procedure is designed to ensure that the final result is acceptable to as many countries as possible. When agreement is finally reached within the technical committee, the draft proposal is sent to the central secretariat for registration as a draft International Standard (DIS); the DIS is then circulated to all member bodies for voting. In many countries, the DIS is made available for public enquiry, thereby ensuring the widest possible consultations. If 75% of the votes cast are in favour of the DIS, it is accepted for further processing as a Final Draft International Standard (FDIS) which is circulated to all member bodies for formal adoption by ISO. Again, 75% of the votes cast must be in favour of the FDIS in order for the International Standard to be published. Normally the fundamental technical issues are resolved at the technical committee level. However, the member body voting procedure provides assurance that no important objections have been overlooked.
The greater part of the work is done by correspondence, and meetings are convened only when thoroughly justified. Each year some 10,000 working documents are circulated. Most standards require periodic revision. Several factors combine to render a standard out of date: technological evolution, new methods and materials, and new quality and safety requirements. To take account of these factors, ISO has established the general rule that all ISO standards should be reviewed every five years. On occasion it is necessary to revise a standard earlier.
A full list of all published ISO standards is given in the ISO Catalogue.
ISO Work in the Field of Occupational Safety
Every ISO International Standard is prepared with concern for safety; the safety factor is an integral part of the work of ISO.
The more than 10,000 International Standards already published by ISO cover a wide spectrum, from aerospace, aircraft and agriculture to building, fire tests, containers, medical equipment, mining equipment, computer languages, the environment, personal safety, ergonomics, pesticides, nuclear energy and so on.
Many International Standards are easily recognized as important in preventing occupational risks: examples are the basic symbol for signifying ionizing radiation or radioactive materials (ISO 361), safety colours and signs (ISO 3864) and the industrial safety helmet (ISO 3873) specified for medium protection in mining, quarrying, shipbuilding, structural engineering and forestry, and so on. Other International Standards are not so easily identified as being directly relevant, but have an equal impact on the prevention of occupational accidents and diseases; one example is ISO 2631, Evaluation of human exposure to whole body vibration, published in three parts, which grades the “reduced comfort boundary”, the “fatigue-decreased proficiency boundary” and the “exposure limit” according to varying levels of vibration frequency, acceleration magnitude and exposure time, and according to the direction of vibration relative to recognized axes of the human body. This Standard, like all others, is continuously updated in the light of research and experience, and relates to such forms of transport as dumpers, tractors, excavators and many other vehicles and worksites.
The ISO technical committees listed in table 1 are among the most prominent in the work for safety and accidents and disease prevention.
Table 1. ISO technical committees most concerned with prevention of occupational accidents and diseases
|
No. |
Title |
Typical example of ISO standard |
|
|
10 |
Technical drawings, product definition and related documentation |
ISO/DIS 11604 |
Technical product documentation—Data sheets for drawing materials and equipment and related documentation |
|
21 |
Equipment for fire protection and fire-fighting |
ISO 3941 |
Classification of fires |
|
23 |
Tractors and machinery for agriculture and forestry |
ISO 3776 |
Tractors for agriculture—Seat belt anchorages |
|
35 |
Paints and varnishes |
ISO 3679 |
Paints, varnishes, petroleum and related products—Determination of flashpoint—Rapid equilibrium method |
|
43 |
Acoustics |
ISO 4872 |
Acoustics—Measurement of airborne noise emitted by construction equipment intended for outdoor use—Method for determining compliance with noise limits |
|
44 |
Welding and allied processes |
ISO/DIS 10882-2 |
Health and safety in welding and allied processes—Sampling of airborne particles and gases in the operator’s breathing zone—Part 2: Sampling of gases |
|
59 |
Building construction |
ISO/TR 9527 |
Building construction —Needs of disabled people in buildings —Design guidelines |
|
67 |
Materials, equipment and offshore structures for petroleum and natural gas industries |
ISO 10418 |
Petroleum and natural gas industries—Offshore production platforms—Analysis, design, installation and testing of basic surface safety systems |
|
82 |
Mining |
ISO 3155 |
Stranded wire ropes for mine hoisting—Fibre components—Characteristics and tests |
|
85 |
Nuclear energy |
ISO 1709 |
Nuclear energy—Fissile materials—Principles of criticality, safety in storing, handling and processing |
|
86 |
Refrigeration |
ISO 5149 |
Mechanical refrigerating systems used for cooling and heating—Safety requirements |
|
92 |
Fire safety |
ISO 1716 |
Building materials—Determination of calorific potential |
|
94 |
Personal safety—Protective clothing and equipment |
ISO 2801 |
Clothing for protection against heat and fire—General recommendations for users and for those in charge of such users |
|
96 |
Cranes |
ISO 10245-1 |
Cranes—Limiting and indicating devices—Part 1: General |
|
98 |
Bases for design of structures |
ISO 2394 |
General principles on reliability for structures |
|
101 |
Continuous mechanical handling equipment |
ISO 1819 |
Continuous mechanical handling equipment—Safety code—General rules |
|
108 |
Mechanical vibration and shock |
ISO 2631-1 |
Evaluation of human exposure to whole-body vibration—Part 1: General requirements |
|
110 |
Industrial trucks |
ISO 1074 |
Counterbalanced fork-lift trucks—Stability tests |
|
118 |
Compressors, pneumatic tools and pneumatic machines |
ISO 5388 |
Stationary air compressors—Safety rules and code of practice |
|
146 |
Air quality |
ISO 8518 |
Workplace air—Determination of particulate lead and lead compounds—Flame atomic absorption spectrometric method |
|
159 |
Ergonomics |
ISO 7243 |
Hot environments—Estimation of the heat stress on worker, based on the WBGT index (wet bulb globe temperature) |
|
199 |
Safety of machinery |
ISO/TR 12100-1 |
Safety of machinery—Basic concepts, general principles for design—Part 1: Basic terminology, methodology |
These technical committees and others have prepared or are preparing International Standards concerned with occupational risks in such areas as building construction sites, factories, docks, agriculture and forestry, nuclear installations, handling of materials and personal protective clothing and equipment.
The field of building provides a very clear example of the intensive concern for accident and disease prevention in the work of ISO. Of the more than 50 ISO technical committees dealing with some aspect of building or building materials, ten deal with the problems of the working environment. The physical factors in the building field cover aspects such as personal safety, vibration and shock, noise, plant and equipment, earth-moving machinery, cranes and lifting devices, and ergonomics. The chemical factors cover air quality, paints and varnishes, protection of welding workers, and protective clothing and equipment.
ISO TC 127 (Earth-moving machinery) has set up a subcommittee to deal specifically with safety requirements and human factors in respect of all the current basic types of earth-moving machinery such as tractors, loaders, dumpers, tractor scrapers, excavators and graders. Standards are already in existence for safe access to driving cabs via steps, ladders, walkways and platforms, and the dimensions of cabs have been established for both large and small operators, sitting or standing and in arctic clothing or not, as appropriate.
Sitting positions and the sizes and shapes of seats for different operators are also the subject of International Standards. Sitting positions are now being related to areas of comfort and to reach for both hand and foot controls, and Standards have been prepared to determine the field of view available to operators of earth-moving machines, based upon determination of the shape, size and position of areas of invisibility caused by obstructing parts of the machines.
To prevent machines from crushing their operators in the event of accidental overturning, roll-over protective structures (ROPS) have been developed and standardized. Falling rocks, trees and parts of buildings in the process of demolition can prove hazardous, so falling-object protective structures (FOPS) have been standardized so as to minimize the possibility of injury to the operator.
ISO 7000, Graphical symbols for use on equipment—Index and synopsis, provides a synopsis of several hundred internationally agreed graphic symbols to be placed on equipment or parts of equipment of any kind in order to instruct the persons handling the equipment as to its use and operation.
ISO work in the building field is both intensive and extensive, just as it is in other fields covered by ISO. (The scope of ISO includes most industrial, agricultural and maritime activities except the electrotechnical field, which is handled by the International Electrotechnical Commission, and pharmaceutical products, handled by the World Health Organization.)
On the factory floor, International Standards take on a special meaning as persons seeking work migrate from one country to another and often to jobs where they cannot speak or read the local language. Easily recognized graphic symbols for controls on machinery that conform to International Standards are vital here as in the building industry; so are standardized locations for foot and hand controls and International Standards for guards to moving parts.
An ISO safety code for compressors covers a wide range of safety and environmental factors, such as the prevention of oil inhalation and the control of toxic oil inhibitors, the prevention of oil coke ignition and of crankcase explosion, and the use of relief and safety valves.
The safety of continuous mechanical handling equipment is the subject of nearly 40 International Standards. They cover such aspects as safety and safety codes for the different kinds of equipment, such as belt conveyors, vibrating feeders, overhead chain conveyors, hydraulic conveyors, pneumatic handling equipment, and roller and screw conveyors.
In the field of agriculture and forestry, ISO has developed important International Standards that protect the worker. Anchorages for seat belts for farm tractors are the subject of a well known standard that is making the import-export trade easier for manufacturers as it is implemented, replacing a plethora of national standards and regulations on the subject. ISO standards even provide rules for presenting operators’ manuals and technical publications for agricultural tractors and machines, making them easy to read and understand.
On the docks the worker is protected by International Standards that determine the stability of cranes and mobile cranes in action and determine the effect of wind loads on crane structures. Other Standards cover indicators and safety devices that will operate in the event of an operator’s misjudgement. Still others cover indicators such as wind gauges, overvoltage annunciators and mass, slope and slew indicators and “automatic cut-off”, such as derricking limiters, load-lifting capacity limiters and slack rope stops. The Standards produced and in preparation should not only assist operators in their work, but enhance the working environment by inspiring confidence in all works personnel moving under and around cranage. A related International Standard provides discard criteria in relation to wear, corrosion, deformation and wire strand breaks, and is intended to guide competent persons involved in the maintenance and examination of cranes and lifting appliances. New Standards under development include out-of-service anchoring devices, maintenance, condition monitoring, safe use and safety signs.
Safety for the worker and others at or near nuclear installations is covered by a number of International Standards, and the work continues in this area. Subjects covered are methods for testing exposure meters and dosimeters, a test for contents leakage and radiation leakage, and the general principles for sampling airborne radioactive materials.
International Standards for protective clothing and equipment are the responsibility of ISO TC 94. In addition to the Standard for industrial safety helmets, it has developed a standardized vocabulary for personal eye-protectors, established utilization and transmittance requirements for infrared filters for eye protectors, and general recommendations for users and those in charge of users of clothing for protection against heat and fire.
The production and use of ISO International Standards such as these, produced through worldwide cooperation, have unquestionably improved the quality of the workplace.
ILO Conventions-Enforcement Procedures
A country ratifying an ILO Convention pledges to “take such action as may be necessary to make effective” its provisions (ILO Constitution, article 19(5)). There are several ways that other countries and workers’ and employers’ organizations (but not individuals) can take action to encourage a government to respect the obligations it has undertaken. An organization need only send a letter containing sufficient information to the Director-General, International Labour Office, 4 route des Morillons, 1211 Geneva 22, Switzerland (fax number 41-22-798-8685). The procedures described here are complemented by the ILO’s work to promote international labor standards, such as seminars and workshops carried out by regional advisers.
Article 22 procedures. A government must submit reports on the application of Conventions it has ratified to the International Labour Office (Article 22). The government is also bound to provide copies of those reports to the most representative organizations of employers and workers in the country (Article 23). These organizations can make comments on the reports and provide additional information on the application of an instrument. An independent Committee of Experts on the Application of Conventions and Recommendations (CEARC) examines the reports and any comments made, and it may then address comments to governments to recommend changes in law or practice or to note cases of progress. The CEARC in turn submits its report each year to the tripartite International Labour Conference. The Conference sets up an Applications Committee, which addresses selected cases before reporting to the plenary. The Conference report appeals to governments to respect the obligations they have undertaken by ratifying ILO Conventions and sometimes urges them to accept “direct contacts” missions, during which solutions can be sought in consultation with the government and workers’ and employers’ organizations in the country.
Article 24 procedures. Under this article of the ILO Constitution, any “industrial association of employers or of workers” may make a representation alleging that an ILO Member State has failed to observe any ILO Convention to which it is a party. To be receivable, a representation must come from such an organization, be in writing, refer to Article 24 of the ILO Constitution and indicate in which respect the Member State concerned has failed to secure the effective observance within its jurisdiction of a Convention (identified by name and/or number) it has ratified. The ILO Governing Body may then set up a committee to examine the representation, communicate it to the government for comment and prepare a report, which the Governing Body can order to be published. It may also lead to a direct contacts mission. Where a government has not acted on the report of an Article 24 representation, the Governing Body may initiate the complaint procedure provided by Article 26 of the ILO Constitution.
Article 26 procedures. This article of the ILO Constitution permits complaints to be filed with the International Labour Office against a Member State which has allegedly failed to secure the observance of a Convention it has ratified. A complaint may be lodged by another Member State having also ratified the same Convention, by a delegate (government, employer or worker) to the International Labour Conference or by the Governing Body of the ILO. The Governing Body may appoint a Commission of Inquiry to consider the complaint and report back to it. The Commission of Inquiry’s findings of fact and recommendations are then published. The recommendations may include a direct contacts mission. In case of disagreement as regards the recommendations of the Commission of Inquiry, a complaint may be referred to the International Court of Justice, whose decision is final.
Freedom of association procedures. With freedom of association and the right to engage in collective bargaining at the heart of membership of the ILO, it has established special procedures to deal with complaints alleging infringements of these rights. A Governing Body Committee on Freedom of Association examines complaints made by national or international organizations of employers or workers against any ILO Member State, even when it has not ratified the two main ILO Conventions on freedom of association and collective bargaining. This Committee can also recommend that a government accept a direct contacts mission to assist it in ensuring respect for these basic principles.
Effect. While the ILO has no police force or labor inspectorate empowered to order a workplace to be made safer, governments are sensitive to pleas that they fulfill the obligations they have undertaken in ratifying ILO Conventions. The public pressure brought to bear by use of the ILO procedures has in a number of cases led to changes in law and practice, and thus through them to an improvement of working conditions.
International Labour Organization
The ILO is one of 18 specialized agencies of the United Nations. It is the oldest international organization within the UN family, and was founded by the Versailles Peace Conference in 1919 after the First World War.
Foundation of the ILO
Historically, the ILO is the outgrowth of the social thought of the 19th century. Conditions of workers in the wake of the industrial revolution were increasingly seen to be intolerable by economists and sociologists. Social reformers believed that any country or industry introducing measures to improve working conditions would raise the cost of labour, putting it at an economic disadvantage compared to other countries or industries. That is why they laboured with such persistence to persuade the powers of Europe to make better working conditions and shorter hours of work the subject of international agreements. After 1890 three international conferences were held on the subject: the first was convened jointly by the German emperor and the Pope in Berlin in 1890; another conference held in 1897 in Brussels was stimulated by the Belgian authorities; and a third, held in 1906 in Bern, Switzerland, adopted for the first time two international agreements on the use of white phosphorus (manufacturing of matches) and on the ban of night work in industry by women. As the First World War had prevented any further activities on the internationalization of labour conditions, the Peace Conference of Versailles, in its intention to eradicate the causes of future war, took up the goals of the pre-war activities and established a Commission on International Labour Legislation. The elaborated proposal of the Commission on the establishment of an international body for the protection of workers became Part XIII of the Treaty of Versailles; to this day, it remains the charter under which the ILO operates.
The first International Labour Conference was held in Washington DC, in October 1919; the Permanent Secretariat of the Organization—the International Labour Office—was installed in Geneva, Switzerland.
The Constitution of the International Labour Organization
Permanent peace worldwide, justice and humanity were and are the motivations for the International Labour Organization, best expressed in the Preamble to the Constitution. It reads:
Whereas universal and lasting peace can be established only if it is based upon social justice;
And whereas conditions of labour exist involving such injustice, hardship and privation to large numbers of people as to produce unrest so great that the peace and harmony of the world are imperilled; and an improvement of those conditions is urgently required, as for example, by
- the regulation of the hours of work, including establishment of a maximum working day and week,
- the regulation of the labour supply,
- the prevention of unemployment,
- the provision of an adequate living wage,
- the protection of the worker against sickness, disease and injury arising out of his employment,
- the protection of children, young persons and women,
- the provision for old age and injury,
- the protection of the interests of workers when employed in countries other than their own,
- the recognition of the principle of equal remuneration for work of equal value,
- the recognition of the principle of freedom of association,
- the organization of vocational and technical education and other measures;
Whereas also the failure of any nation to adopt humane conditions of labour is an obstacle in the way of other nations which desire to improve the conditions in their own countries;
The High Contracting Parties, moved by sentiments of justice and humanity as well as by the desire to secure the permanent peace of the world, and with a view to attaining the objectives set forth in this Preamble, agree to the following Constitution of the International Labour Organisation. …”
The aims and purposes of the International Labour Organization in a modernized form are embodied in the Philadelphia Declaration, adopted in 1944 at the International Labour Conference in Philadelphia, USA. The Declaration is now an Annex to the Constitution of the ILO. It proclaims the right of all human beings “to pursue both their material well being and their spiritual development in conditions of freedom and dignity, of economic security and equal opportunity”. It further states that “poverty anywhere constitutes a danger to prosperity everywhere”.
The task of the ILO as determined in Article 1 of the Constitution is the promotion of the objects set forth in the Preamble and in the Philadelphia Declaration.
The International Labour Organization and its Structure
The International Labour Organization (ILO) is composed of 173 States. Any member of the United Nations may become a member of the ILO by communicating to the Director-General of the ILO its formal acceptance of the obligations of the Constitution. Non-Member States of the UN may be admitted by a vote of the International Labour Conference (Switzerland is a member of the ILO but not, however, of the UN) (Constitution, Article 1). Representation of Member States at the ILO has a structure which is unique within the UN family. In the UN and in all other specialized UN agencies, representation is only by government personnel: ministers, their deputies, or authorized representatives. However, at the ILO the concerned groups of society are part of the Member States’ representation. Representatives consist of government delegates, generally from the ministry of labour, and delegates representing the employers and the workers of each of the members (Constitution, Article 3). This is the ILO’s fundamental concept of tripartism.
The International Labour Organization consists of:
- the International Labour Conference, an annual Conference of representatives of all members
- the Governing Body, composed of 28 government representatives, 14 employers’ representatives, and 14 workers’ representatives
- the International Labour Office—the permanent secretariat of the organization—which is controlled by the Governing Body.
The International Labour Conference—also called the World Parliament of Labour—meets regularly in June each year with about 2,000 participants, delegates and advisers. The agenda of the Conference includes the discussion and adoption of international agreements (the ILO’s Conventions and Recommendations), the deliberation of special labour themes in order to frame future policies, the adoption of Resolutions directed towards action in Member States and instructions to the Director-General of the Organization on action by the Office, a general discussion and exchange of information and, every second year, the adoption of a biennial programme and budget for the International Labour Office.
The Governing Body is the link between the International Labour Conference of all Member States and the International Labour Office. In three meetings per year, the Governing Body executes its control over the Office by screening work progress, formulating instructions to the Director-General of the Office, adopting the output of Office activity such as Codes of Practice, monitoring and guiding financial affairs, and preparing the agendas for future International Labour Conferences. Membership of the Governing Body is subject to election for a three-year term by the three groups of Conference Representatives—governments, employers and workers. Ten government members of the Governing Body are permanent members as representatives of States of major industrial importance.
Tripartism
All the decision-making mechanisms of the ILO follow a unique structure. All decisions of Member representation are taken by the three groups of representatives, namely by the government representatives, the employers’ representatives and the workers’ representatives of each Member State. Decisions on the substance of work in the Conference Committees on International Conventions and Recommendations, in the Meeting of Experts on Codes of Practice, and in the Advisory Committees on conclusions regarding future labour conditions, are taken by members of the Committees, of which one-third represent governments, one-third represent employers and one-third represent workers. All political, financial and structural decisions are taken by the International Labour Conference (ILC) or the Governing Body, in which 50% of the voting power lies with government representatives (two per Member State in the Conference), 25% with employers’ representatives, and 25% with workers’ representatives (one for each group of a Member State in the Conference). Financial contributions to the Organization are paid solely by the governments, not by the two non-governmental groups; for this reason only governments comprise the Finance Committee.
The Conventions
The International Labour Conference has from 1919 to 1995 adopted 176 Conventions and 183 Recommendations.
Some 74 of the Conventions deal with working conditions, of which 47 are on general conditions of work and 27 are on safety and health in a narrow sense.
The subjects of the Conventions on general conditions of work are: hours of work; minimum age for admission to employment (child labour); night work; medical examination of workers; maternity protection; family responsibilities and work; and part time work. In addition, also relevant to health and safety are ILO Conventions aimed at eliminating discrimination against workers on various grounds (e.g., race, sex, disability), protecting them from unfair dismissal, and compensating them in case of occupational injury or disease.
Of the 27 Conventions on safety and health, 18 were adopted after 1960 (when decolonization led to a large increase in ILO membership) and only nine from 1919 to 1959. The most ratified Convention in this group is the Labour Inspection Convention, 1947 (No. 81), which has been ratified by more than 100 Member States of the ILO (its corollary for agriculture has been ratified by 33 countries).
High numbers of ratification can be one indicator of commitment to improving working conditions. For instance Finland, Norway and Sweden, which are famous for their safety and health record and which are the world’s showcase of safety and health practice, have ratified almost all Conventions in this field adopted after 1960.
The Labour Inspection Conventions are complemented by two further basic standards, the Occupational Safety and Health Convention, 1981 (No. 155) and the Occupational Health Services Convention, 1985 (No. 161).
The Occupational Safety and Health Convention establishes the framework for a national conception of safety and health constituting a model of what the safety and health law of a country should contain. The framework directive of the EU on safety and health follows the structure and contents of the ILO Convention. The EU directive has to be transposed into national legislation by all 15 members of the EU.
The Occupational Health Services Convention deals with the operational structure within enterprises for the implementation of safety and health legislation in companies.
Several Conventions have been adopted regarding branches of economic activity or hazardous substances. These include the Safety and Health in Mines Convention, 1995 (No. 176); the Safety and Health in Construction Convention, 1988 (No. 167); the Occupational Safety and Health (Dock Work) Convention, 1979 (No. 152); the White Lead (Painting) Convention, 1921 (No. 13); the Benzene Convention, 1971 (No. 136); the Asbestos Convention, 1986 (No. 162); the Chemicals Convention, 1990 (No. 170); and the Prevention of Major Industrial Accidents Convention, 1993 (No. 174).
Associated with these norms are: the Working Environment Convention, 1977 (No. 148) (Protection of Workers against occupational Hazards in the Working Environment due to Air Pollution, Noise and Vibration); the Occupational Cancer Convention, 1974 (No. 139); and the list of occupational diseases that is part of the Employment Injury Benefits Convention, 1964 (No. 121). The last revision of the list was adopted by the Conference in 1980 and is discussed in the Chapter Workers’ Compensation, Topics in.
Other safety and health Conventions are: the Marking of Weight Convention, 1929 (No. 27); the Maximum Weight Convention, 1967 (No. 127); the Radiation Protection Convention, 1960 (No. 115); the Guarding of Machinery Convention, 1963 (No. 119); and the Hygiene (Commerce and Offices) Convention, 1964 (No. 120).
During the early period of the ILO, Recommendations were adopted instead of Conventions, such as on anthrax prevention, white phosphorus and lead poisoning. However in recent times Recommendations have tended to complement a Convention by specifying details on implementing its provisions.
Contents of Conventions on Safety and Health
Structure and content of safety and health Conventions follow a general pattern:
- scope and definitions
- obligations of governments
- consultation with organizations of workers and employers
- obligations of employers
- duties of workers
- rights of workers
- inspections
- penalties
- final provisions (on conditions for entry into force, registrations of ratifications and denunciation).
A Convention prescribes the task of government or government authorities in regulating the subject matter, highlights obligations of owners of enterprises, specifies the role of workers and their organizations through duties and rights, and closes with provisions for inspection and action against violation of the law. The Convention must of course determine its scope of application, including possible exemptions and exclusions.
Design of Conventions concerning safetyand health at work
The Preamble
Each Convention is headed by a preamble referring to the dates and the item on the agenda of the International Labour Conference; other Conventions and documents related to the topic, concerns about the subject justifying the action; underlying causes; cooperation with other international organizations such as WHO and UNEP; the form of the international instrument as a Convention or Recommendation, and the date of the adoption and citation of the Convention.
Scope
Wording of the scope is governed by flexibility towards implementation of a Convention. The guiding principle is that the Convention applies to all workers and branches of economic activity. However, in order to facilitate ratification of the Convention by all Member States, the guiding principle is often supplemented by the possibility of partial or total non-application in various fields of activity. A Member State may exclude particular branches of economic activity or particular undertakings in respect of which special problems of a substantial nature arise from the application of certain provisions or of the Convention as a whole. The scope may also foresee step by step implementation of provisions to take into account existing conditions in a country. These exclusions reflect also the availability of national resources for the implementation of new national legislation on safety and health. General conditions of exclusion are that a safe and healthy working environment is otherwise attached by alternative means and that any decision on exclusion is subject to consultation with employers and workers. The scope also includes definitions of terms used in the wording of the international instrument such as branches of economic activity, workers, workplace, employer, regulation, workers’ representative, health, hazardous chemical, major hazard installation, safety report and so forth.
Obligations of governments
Conventions on safety and health establish as a first module the task for a government to elaborate, implement and review a national policy relating to the contents of the Convention. Organizations of employers and workers must be involved in the establishment of the policy and the specification of aims and objectives. The second module concerns the enactment of laws or regulations giving effect to the provisions of the Convention and the enforcement of the law, including the employment of qualified personnel and the provision of support for the staff for inspection and advisory services. Under Articles 19 and 22 of the ILO Constitution, governments are also obliged to report regularly or on request to the International Labour Office on the practice of implementation of the Convention and Recommendation. These obligations are the basis for ILO supervisory procedures.
Consultations with organizations of employers and workers
The importance of involvement of those who are directly associated with the implementation of regulations and the consequences of accidents is undoubted. Successful safety and health practice is based on collaboration and on incorporation of opinion and good will of the persons concerned. A Convention therefore provides that the government authorities must consult employers and workers when considering the exclusion of installations from legislation for step-by-step implementation of provisions and in the development of a national policy on the subject matter of the Convention.
Obligations of employers
The responsibility for the execution of legal requirements within an enterprise lies on the owner of an enterprise or his or her representative. Legal rights on workers’ participation in the decision-making process do not alter the primary responsibility of the employer. The obligations of employers as stated in Conventions include provision of safe and healthy working procedures; the purchase of safe machinery and equipment; the use of non-hazardous substances in work processes; the monitoring and assessment of airborne chemicals at the workplace; the provision of health surveillance of workers and of first aid; the reporting of accidents and diseases to the competent authority; the training of workers; the provision of information regarding hazards related to work and their prevention; cooperation in discharging their responsibilities with workers and their representatives.
Duties of workers
Since the 1980s, Conventions have stated that workers have a duty to cooperate with their employers in the application of safety and health measures and to comply with all procedures and practices relating to safety and health at work. The duty of workers may include the reporting to supervisors of any situation which could present a special risk, or the fact that a worker has removed himself/herself from the workplace in case of imminent and serious danger to his or her life or health.
Rights of workers
A variety of special rights of workers has been stated in ILO Conventions on safety and health. In general a worker is afforded the right to information on hazardous working conditions, on the identity of chemicals used at work and on chemical safety data sheets; the right to be trained in safe working practices; the right to consultation by the employer on all aspects of safety and health associated with the work; and the right to undergo medical surveillance free of charge and with no loss of earnings. Some of these Conventions also recognize the rights of workers’ representatives, particularly regarding consultation and information. These rights are reinforced by other ILO Conventions on freedom of association, collective bargaining, workers’ representatives and protection against dismissal.
Specific articles in Conventions adopted in 1981 and later deal with the worker’s right to remove himself/herself from danger at his or her workplace. A 1993 Convention (Prevention of Major Industrial Accidents, 1993 (No. 174)) recognized the worker’s right to notify the competent authority of potential hazards which may be capable of generating a major accident.
Inspection
Conventions on safety and health express the needs for the government to provide appropriate inspection services to supervise the application of the measures taken to implement the Convention. The inspection requirement is supplemented by the obligation to provide the inspection services with the resources necessary for the accomplishment of their task.
Penalties
Conventions on safety and health often call for national regulation regarding the imposition of penalties in case of non-compliance with legal obligations. Article 9 (2) of the framework Occupational Safety and Health Convention, 1981 (No 155) states: “The enforcement system shall provide for adequate penalties for violations of the laws and regulations.” These penalties may be administrative, civil or criminal in nature.
The Labour Inspection Convention, 1947 (No. 81)
The Labour Inspection Convention of 1947 (No. 81) calls on States to maintain a system of labour inspection in industrial workplaces. It fixes government obligations in regard to inspection and sets out rights, duties and powers of inspectors. This instrument is complemented by two Recommendations (Nos. 81 and 82) and by the Protocol of 1995, which extends its scope of application to the non-commercial services sector (such as the public service and state-run enterprises). The Labour Inspection (Agriculture) Convention, 1969 (No. 129), contains provisions very similar to Convention No. 81 for the agricultural sector. ILO Maritime Conventions and Recommendations also address inspection of seafarers’ working and living conditions.
The government has to establish an independent qualified corps of inspectors in sufficient number. The inspectorate must be fully equipped to provide good services. Legal provision of penalties for violation of safety and health regulations are an obligation of the government. Inspectors have the duty to enforce legal requirements, and to provide technical information and advice to employers and workers regarding effective means of complying with legal provisions.
Inspectors are to report gaps in regulations to authorities and submit annual reports on their work. Governments are called on to compile annual reports giving statistics on inspections done.
Rights and powers of inspectors are laid down, such as the right to enter workplaces and premises, to carry out examinations and tests, to initiate remedial measures, to issue orders on alteration of the installation and immediate execution. They have also the right to issue citations and institute legal proceedings in case of a violation of an employer’s duties.
The Convention contains provisions on the conduct of inspectors, such as having no financial interest in undertakings under supervision, no disclosure of trade secrets and, of particular importance, confidentiality in case of complaints by workers, which means giving no hint to the employer about the identity of complainant.
Promotion of progressive development by Conventions
Work on Conventions tries to mirror law and practice in Member States of the Organization. However, there are cases where new elements are introduced which have so far not been the subject of widespread national regulation. The initiative may come from delegates, during the discussion of a norm in a Conference Committee; where justified, it may be proposed by the Office in the first draft of a new instrument. Here are two examples:
(1)The right of a worker to remove himself or herself from work that poses an imminent and serious danger to his or her life or health.
Normally people consider that it is a natural right to leave a workplace in case of danger to life. However this action may cause damage to materials, machinery or products—and can sometimes be very costly. As installations get more sophisticated and expensive, the worker might be blamed for having unnecessarily removed himself or herself, with attempts to make him or her liable for the damage. During discussion in a Conference Committee on the Safety and Health Convention a proposal was made to protect the worker against recourse in such cases. The Conference Committee considered the proposal for hours and finally found wording to protect the worker which was acceptable to the majority of the Committee.
Article 13 of Convention No. 155 thus reads: “A worker who has removed himself from a work situation which he has reasonable justification to believe presents an imminent and serious danger to his life or health shall be protected from undue consequences in accordance with national conditions and practice”. The “undue consequences” include, of course, dismissal and disciplinary action as well as liability. Several years later, the situation was reconsidered in a new context. During the discussions at the Conference of the Construction Convention in 1987-88, the workers’ group tabled an amendment to introduce the right of a worker to remove himself or herself in case of imminent and serious danger. The proposal was finally accepted by the majority of Committee members under the condition that it was combined with a worker’s duty to immediately inform his or her supervisor about the action.
The same provision has been introduced in the Chemicals Convention, 1990 (No. 170); a similar text is included in the Safety and Health in Mines Convention, 1995 (No. 176). This means that countries which have ratified the Safety and Health Convention or the Convention on Construction, Chemical Safety or Safety and Health in Mines must provide in national law for the right of a worker to remove himself or herself and to be protected against “undue consequences”. This will probably sooner or later lead to application of this right for workers in all sectors of economic activity. This newly recognized right for workers has in the meantime been incorporated in the basic EU Directive on Safety and Health Organization of 1989; all Member States of the EU were to have incorporated the right in their legislation by the end of 1992.
(2)The right for a worker to have a medical examination instead of mandatory medical examinations.
For many years national legislation had required medical examinations for workers in special occupations as a prerequisite for assignment to or continuation of work. Over time, a long list of mandatory medical examinations before assignment and at periodic intervals had been prescribed. This well-meaning intention is increasingly turning into a burden, however, as there may be too many medical examinations administered to one person. Should the examinations be recorded in a health passport of a worker for lifelong testimony to ill-health, as practised in some countries, the medical examination in the end could become a tool for selection into unemployment. A young worker having recorded a long list of medical examinations in his or her life due to exposure to hazardous substances may not find an employer ready to give him or her a job. The doubt may be too strong that this worker may sooner or later be absent too often because of illness.
A second consideration has been that any medical examination is an intrusion into a person’s private life and therefore a worker should be the one to decide on medical procedures.
The International Labour Office proposed, therefore, to introduce in the Night Work Convention, 1990 (No. 171) the right of a worker to have a medical examination instead of calling for mandatory surveillance. This idea won broad support and was finally reflected in Article 4 of the Night Work Convention by the International Labour Conference in 1990, which reads:
1.At their request, workers shall have the right to undergo a health assessment without charge and to receive advice on how to reduce or avoid health problems associated with their work: (a) before taking up an assignment as a night worker; (b) at regular intervals during such an assignment; (c) if they experience health problems during such an assignment which are not caused by factors other than the performance of the night work.
2.With the exception of a finding of unfitness for night work, the findings of such assessments shall not be transmitted to others without the worker’s consent and shall not be used to their detriment.
It is difficult for many health professionals to follow this new conception. However, they should realize that a person’s right to determine whether to undergo a medical examination is an expression of contemporary notions of human rights. The provision has been already taken up by national legislation, for example in the 1994 Act on Working Time in Germany, which makes reference to the Convention. And more importantly, the EU Framework Directive on Safety and Health follows this model in its provisions on health surveillance.
Functions of the International Labour Office
The functions of the International Labour Office as laid down in Article 10 of the Constitution include the collection and distribution of information on all subjects related to the international adjustment of conditions of industrial life and labour with special emphasis on future international labour standards, the preparation of documents on the various items of the agenda for the meeting of the ILC (especially the preparatory work on contents and wording of Conventions and Recommendations), the provision of advisory services to governments, employers’ organizations and workers’ organizations of member states related to labour legislation and administrative practice, including systems of inspection, and the edition and dissemination of publications of international interest dealing with problems of industry and employment.
Like any ministry of labour, the International Labour Office is made up of bureaus, departments and branches concerned with the various fields of labour policy. Two special institutes were established to support the Office and Member States: the International Institute for Labour Studies at ILO headquarters, and the International Training Centre of the ILO in Turin, Italy.
A Director-General, elected by the Governing Body for a five-year term, and three Deputy Director-Generals, appointed by the Director-General, govern (as of 1996) 13 departments; 11 bureaus at headquarters in Geneva, Switzerland; two liaison offices with international organizations; five regional departments, in Africa, the Americas, Asia and the Pacific, the Arab States, and Europe, with 35 area and branch offices and 13 multi-disciplinary teams (a group of professionals of various disciplines who provide advisory services in Member States of a subregion).
The Working Conditions and Environment Department is the Department in which the bulk of safety and health work is carried out. It comprises a staff of about 70 professionals and general service personnel of 25 nationalities, including professional experts in the multi-disciplinary teams. As of 1996, it has two branches: the Conditions of Work and Welfare Facilities Branch (CONDI/T) and the Occupational Safety and Health Branch (SEC/HYG).
The Safety and Health Information Services Section of SEC/HYG maintains the International Occupational Safety and Health Information Centre (CIS) and the Occupational Safety and Health Information Support Systems Section. The work on this edition of the Encyclopaedia is housed in the Support Systems Section.
A special unit of the Department was established in 1991: the International Programme on the Elimination of Child Labour (IPEC). The new programme executes, jointly with Member States in all regions of the world, national programmes of activity against child labour. The programme is financed by special contributions of several Member States, such as Germany, Spain, Australia, Belgium, the United States, France and Norway.
In addition, in the course of the review of the ILO’s major safety and health programme established in the 1970s, the International Programme for the Improvement of Working Conditions and the Environment—known under its French acronym PIACT—the International Labour Conference adopted in 1984 the PIACT Resolution. In principle, the Resolution constitutes a framework of operation for all action by the ILO and by Member States of the Organization in the field of safety and health:
- Work should take place in a safe and healthy working environment.
- Conditions of work should be consistent with workers’ well-being and human dignity.
- Work should offer real possibilities for personal achievement, self-fulfilment, and service to society.
Publications concerning workers’ health are published in the Occupational Safety and Health Series, such as Occupational Exposure Limits for Airborne Toxic Substances, a listing of national exposure limits of 15 Member States; or the International Directory of Occupational Safety and Health Services and Institutions, which compiles information on the safety and health administrations of Member States; or Protection of Workers from Power Frequency Electric and Magnetic Fields, a practical guide to provide information on the possible effects of electric and magnetic fields on human health and on procedures for higher standards of safety.
Typical products of the safety and health work of the ILO are the codes of practice, which constitute a kind of model set of regulations on safety and health in many fields of industrial work. These codes are often elaborated in order to facilitate the ratification and application of ILO Conventions. For example, the Code of Practice on Prevention of Major Industrial Accidents, whose objective is to provide guidance in the setting up of an administrative, legal and technical system for the control of major hazard installations in order to avoid major disasters. The Code of Practice on Recording and Notification of Occupational Accidents and Diseases aims at a harmonized practice in the collection of data and the establishment of statistics on accidents and diseases and associated events and circumstances in order to stimulate preventive action and to facilitate comparative work between Member States (these are just two examples from a long list). Within the field of information exchange two major events are organized by the Safety and Health Branch of the ILO: the World Congress on Occupational Safety and Health, and the ILO International Pneumoconiosis Conference (which is now called The International Conference on Occupational Respiratory Diseases).
The World Congress is organized every three or four years jointly with the International Social Security Association (ISSA) and a national safety and health organization in one of the ILO Member States. World Congresses have been held since the 1950s. Some 2,000 to 3,000 experts from more than 100 countries meet at these congresses in order to exchange information on good practices in safety and health and on modern trend setting, and to establish relations with colleagues from other countries and other parts of the world.
The Pneumoconiosis Conference has been organized by the ILO since the 1930s; the next is planned for 1997 in Kyoto, Japan. One of the outstanding outputs of these conferences is the ILO International Classification of Radiographs of Pneumoconiosis.
The ILO’s technical cooperation in the field of safety and health has many facets. Several projects assisted Member States in preparing new legislation on safety and health and in strengthening their inspection services. In other countries, support has been provided for the creation of safety and health institutes in order to promote research work and develop training programmes and activities. Special projects were designed and executed on mine safety and chemical safety, including the establishment of major hazard control systems. These projects may be targeted towards one Member State, or to a regional group of countries. The tasks at ILO headquarters include the assessment of needs, project development and design, identification of financial support from international funds and national aid programmes, selection and provision of technical expertise, procurement of equipment and planning, and the organization and implementation of study tours and fellowship programmes.
Standard setting, research, collection and dissemination of information and technical cooperation reflect the operational arms of the ILO. In active partnership with the Organization’s tripartite membership these activities reinforce the struggle for the goal of social justice and peace in the world.
This is why in 1969, at the 50th anniversary of the Organization, the work and achievements of the International Labour Organization were awarded the Nobel Peace Prize.
The United Nations and Specialized Agencies
* This article is adapted from Basic Facts About the United Nations (United Nations 1992).
Origin of the United Nations
The United Nations was, in 1992, an organization of 179 nations legally committed to cooperate in supporting the principles and purposes set out in its Charter. These include commitments to eradicate war, promote human rights, maintain respect for justice and international law, promote social progress and friendly relations among nations, and use the Organization as a centre to harmonize their actions in order to attain these ends.
The United Nations Charter was written in the closing days of the Second World War by the representatives of 50 governments meeting at the United Nations Conference on International Organization in 1945. The Charter was drafted on the basis of proposals worked out by the representatives of China, France, the Soviet Union, the United Kingdom and the United States. It was adopted and signed on 26 June 1945.
To millions of refugees from war and persecution, the United Nations has provided shelter and relief. It has acted as a major catalyst in the evolution of 100 million people from colonial rule to independence and sovereignty. It has established peace-keeping operations many times to contain hostilities and to help resolve conflicts. It has expanded and codified international law. It has wiped smallpox from the face of the planet. In the five decades of its existence, the Organization has adopted some 70 legal instruments promoting or obligating respect for human rights, thus facilitating an historic change in the popular expectation of freedom throughout the world.
Membership
The Charter declares that membership of the UN is open to all peace-loving nations which accept its obligations and which, in the judgement of the Organization, are willing and able to carry out these obligations. States are admitted to membership by the General Assembly on the recommendation of the Security Council. The Charter also provides for the suspension or expulsion of Members for violation of the principles of the Charter, but no such action has ever been taken.
Official Languages
Under the Charter the official languages of the United Nations are Chinese, English, French, Russian and Spanish. Arabic has been added as an official language of the General Assembly, the Security Council and the Economic and Social Council.
Structure
The United Nations is a complex network consisting of six main organs with a large number of related programmes, agencies, commissions and other bodies. These related bodies have different legal status (some are autonomous, some are under the direct authority of the UN and so on), objectives and areas of responsibility, but the system displays a very high level of cooperation and collaboration. Figure 1 provides a schematic illustration of the structure of the system and some of the links between the different bodies. For further information, reference should be made to: Basic Facts About the United Nations (1992).
Figure 1. The Charter established six principal organs of the United Nations
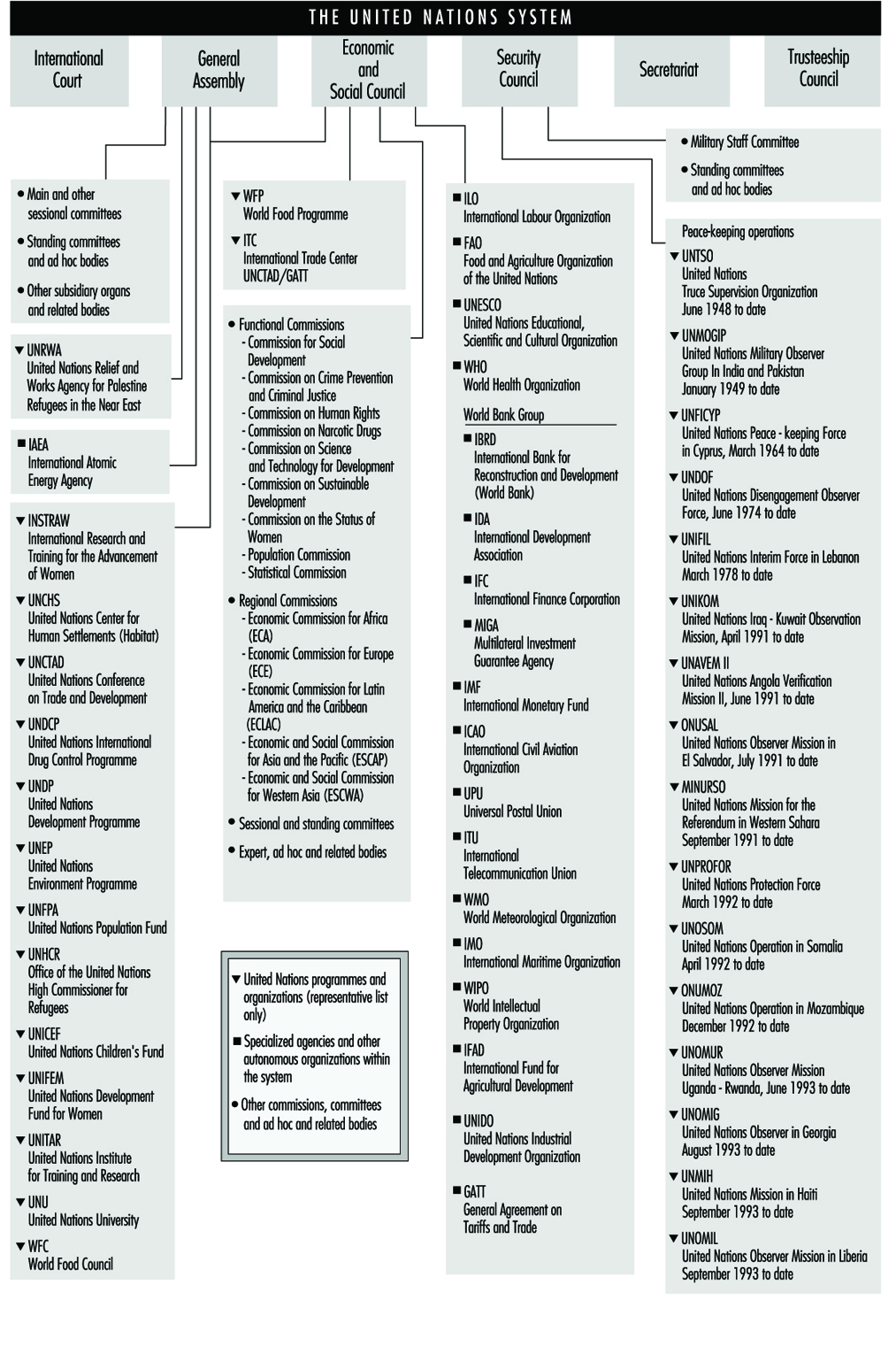
International Court of Justice
The International Court of Justice is the principal judicial organ of the UN. The Court is open to the parties to its Statute, which automatically includes all Members of the UN. Other States can refer cases to the Court under conditions laid down by the Security Council. In addition, the Security Council may recommend that a legal dispute be referred to the Court. Only States may be party to cases before the Court (i.e., the Court is not open to individuals). Both the General Assembly and the Security Council can ask the Court for an advisory opinion on any legal question; other organs of the UN and the specialized agencies, when authorized by the General Assembly, can ask for advisory opinions on legal questions within the scope of their activities (for example, the International Labour Organization could request an advisory opinion relating to an international labour standard).
The jurisdiction of the Court covers all matters provided for in the UN Charter or in treaties or conventions in force, and all other questions which States refer to it. In deciding cases, the Court is not restricted to principles of law contained in treaties or conventions, but may employ the entire sphere of international law (including customary law).
The General Assembly
The General Assembly is the main deliberative organ. It is composed of representatives of all Member States, each of which has one vote. Decisions on important questions, such as those on peace and security, admission of new Members and budgetary matters, require a two-thirds majority. Decisions on other questions are reached by a simple majority.
The functions and powers of the General Assembly include the consideration of and formulation of recommendations on the principles of cooperation in the maintenance of international peace and security, including disarmament and the regulation of armaments. The General Assembly also initiates studies and makes recommendations to promote international political cooperation, the development and codification of international law, the realization of human rights and fundamental freedoms for all, and international collaboration in the economic, social, cultural, educational and health fields. It receives and deliberates on reports from the Security Council and other UN organs; considers and approves the UN budget and apportions the contributions among Members; and elects the non-permanent members of the Security Council, the members of the Economic and Social Council and those members of the Trusteeship Council that are elected. The General Assembly also elects jointly with the Security Council the Judges of the International Court of Justice and, on the recommendation of the Security Council, appoints the Secretary-General.
At the beginning of each regular session, the General Assembly holds a general debate, in which Member States express their views on a wide range of matters of international concern. Because of the great number of questions which the General Assembly is called upon to consider (over 150 agenda items at the 1992 session, for example), the Assembly allocates most questions to its seven main committees:
- First Committee (disarmament and related international security matters)
- Special Political Committee
- Second Committee (economic and financial matters)
- Third Committee (social, humanitarian and cultural matters)
- Fourth Committee (decolonization matters)
- Fifth Committee (administrative and budgetary matters)
- Sixth Committee (legal matters).
Economic and Social Council (ECOSOC)
ECOSOC was established by the Charter as the principal organ to coordinate the economic and social work of the UN and the specialized agencies and institutions. The Economic and Social Council serves as the central forum for the discussion of international economic and social issues of a global or inter-disciplinary nature and the formulation of policy recommendations on those issues, and works to promote respect for, and observance of, human rights and fundamental freedoms for all. ECOSOC may make or initiate studies and reports and recommendations on international economic, social, cultural, educational, health and related matters, and call international conferences and prepare draft conventions for submission to the General Assembly. Other powers and functions include the negotiation of agreements with the specialized agencies defining their relationship with the UN and the coordination of their activities, and consultation with NGOs concerned with matters with which the Council deals.
Subsidiary bodies
The subsidiary machinery of the Council includes functional and regional commissions, six standing committees (for example, the Committee on Non-Governmental Organizations and on Transnational Corporations) and a number of standing expert bodies on such subjects as crime prevention and control, development planning, and the transport of dangerous goods.
Relations with non-governmental organizations
Over 900 NGOs have consultative status with the Council, with varying levels of involvement. These NGOs may send observers to public meetings of the Council and its subsidiary bodies and may submit written statements relevant to the Council’s work. They may also consult with the UN Secretariat on matters of mutual concern.
Security Council
The Security Council has primary responsibility, under the Charter, for the maintenance of international peace and security. While other organs of the UN make recommendations to governments, the Council alone has the power to take decisions which Member States are obligated under the Charter to carry out.
Secretariat
The Secretariat, an international staff working at UN Headquarters in New York and in the field, carries out the diverse day-to-day work of the Organization. It services the other organs of the UN and administers the programmes and policies laid down by them. At its head is the Secretary-General, who is appointed by the General Assembly on the recommendation of the Security Council for a term of five years.
Trusteeship Council
In setting up an International Trusteeship System, the Charter established the Trusteeship Council as one of the main organs of the UN and assigned to it the task of supervising the administration of Trust Territories placed under the Trusteeship System. Major goals of the System are to promote the advancement of the inhabitants of Trust Territories and their progressive development towards self-government or independence.
The Role of the United Nations System in Occupational Health and Safety
While the improvement of working conditions and environment will normally be part of national policy to further economic development and social progress in accordance with national objectives and priorities, a measure of international harmonization is necessary to ensure that the quality of the working environment everywhere is compatible with workers’ health and welfare, and to assist Member States to this effect. This is, essentially, the role of the UN system in this field.
Within the UN system, many organizations and bodies play a role in the improvement of the working conditions and the working environment. The International Labour Organization (ILO) has a constitutional mandate to improve working conditions and environment to humanize work; its tripartite structure can ensure that its international standards have a direct impact on national legislation, policies and practices and is discussed in a separate article in this chapter.
The World Health Organization (WHO) has a mandate in occupational health derived from its Constitution, which identified WHO as “the directing and coordinating authority on international health work”, and stated WHO’s functions which include the “promotion of ...economic and working conditions and other aspects of environmental hygiene”. Additional mandates are derived from various resolutions of the World Health Assembly and Executive Board. WHO’s occupational health programme aims to promote the knowledge and control of workers’ health problems, including occupational and work-related diseases, and to cooperate with countries in the development of health care programmes for workers, particularly those who are generally underserviced. The WHO, in collaboration with the ILO, UNEP and other organizations, undertakes technical cooperation with Member States, produces guidelines, and carries out field studies and occupational health training and personnel development. The WHO has set up the GEENET—the Global Environmental Epidemiology Network—which includes institutions and individuals from all over the world who are actively involved in research and training on environmental and occupational epidemiology. The International Agency for Research on Cancer (IARC) has been established as an independent research institute, but within the framework of the WHO. The statutes of the Agency set out its mission as “planning, promoting and developing research in all phases of the causation, treatment and prevention of cancer”. Since the start of its research activity, the Agency has devoted itself to studying the causes of cancer present in the human environment, in the belief that identification of a carcinogenic agent was the first and necessary step towards reducing or removing the causal agent from the environment, with the aim of preventing cancer that it might have caused. The Agency’s research activities fall into two main groups—epidemiological and laboratory-based experimental but there is considerable interaction between these groups in the actual research projects undertaken.
Besides these two organizations with a central focus on work and health, respectively, several UN bodies include health and safety matters within their specific sectoral or geographical functions:
The United Nations Environment Programme (UNEP) has the mandate to safeguard and enhance the environment for the benefit of present and future generations, including the working environment. It has a basic coordinating and catalytic function for environment in general within the UN system. It discharges this function through programme coordination and the support of activities by the Environment Fund. In addition to its general mandate, UNEP’s specific mandate with regard to the working environment stems from Recommendations 81 and 83 of the UN Conference on the Human Environment, and UNEP Governing Council Decisions requesting the Executive Director to integrate the principles and objectives related to the improvement of the working environment fully into the framework of the environment programme. UNEP is also required to collaborate with the appropriate organizations of workers and employers, in the development of a coordinated system-wide action programme on the working and living environment of workers, and with the UN bodies concerned (for example, UNEP cooperates with the WHO and the ILO in the International Programme on Chemical Safety).
UNEP maintains the International Register of Potentially Toxic Chemicals (IRPTC), which strives to bridge the gap between the world’s chemical knowledge and those who need to use it. UNEP’s network of environmental agreements is also having an ever-increasing international effect, and gathering momentum (for example, the historic Vienna Convention and the Montreal Protocol on the protection of the ozone layer).
The International Atomic Energy Agency (IAEA) is concerned with hazards resulting from ionizing radiation associated with the nuclear fuel cycle. The IAEA encourages and guides the development of peaceful uses of atomic energy, establishes standards for nuclear safety and environmental protection, aids member countries through technical cooperation, and fosters the exchange of scientific and technical information on nuclear energy. The activities of the Agency in the area of radiological protection of workers involve the development of these standards; preparation of safety guides, codes of practice and manuals; holding of scientific meetings for exchange of information or preparation of manuals or technical guidebooks; organizing training courses, visiting seminars and study tours; development of technical expertise in developing Member States through the awards of research contracts and fellowships; and helping the developing Member States in the organization of radiation protection programmes through the provision of technical assistance, experts’ services, advisory missions, and advisory services on nuclear law regulatory matters.
The United Nations Development Programme (UNDP) and the World Bank have included provisions on occupational safeguards in development assistance agreements. The UNDP is engaged in a large number of projects designed to assist developing countries to build up their nascent economies and raise their living standards. Several thousand internationally recruited experts are kept steadily at work in the field. Several amongst these projects are devoted to the improvement of occupational safety and health standards in industry and other walks of economic life, the implementation of which is entrusted to the ILO and WHO. Such field projects may range from the provision of short-term consultancy to more massive assistance over a period of several years for the establishment of fully fledged occupational safety and health institutes designed to provide training, applied field research and direct service to places of employment.
The International Maritime Organization (IMO) deals with the safety of workers on board ships. IMO provides a forum for member governments and interested organizations to exchange information and endeavour to solve problems connected with technical, legal and other questions concerning shipping and the prevention of marine pollution by ships. IMO has drafted a number of conventions and recommendations which governments have adopted and which have entered into force. Among them are international conventions for the safety of life at sea, the prevention of marine pollution by ships, the training and certification of seafarers, the prevention of collisions at sea, several instruments dealing with liability and compensation, and many others. IMO has also adopted several hundred recommendations dealing with subjects such as the maritime transport of dangerous goods, maritime signals, safety for fishermen and fishing vessels, and the safety of nuclear merchant ships.
The Food and Agriculture Organization of the United Nations (FAO) has a role in protecting agricultural workers against hazards resulting from the use of pesticides, farm tools and machinery. A number of activities of FAO are directly or indirectly concerned with occupational safety and health and ergonomics in agricultural, forestry and fishery work. In fishery activities, FAO collaborates at the secretariat level with the ILO and the IMO on the IMO Sub-Committee on Safety of Fishing Vessels and participates actively in the work of the IMO Sub-Committee on Standards of Training and Watchkeeping. FAO collaborates with ILO in regard to conditions of work in the fishing industry. In forestry activities, the FAO/ECE/ILO Committee on Forest Working Techniques and Training of Forest Workers deals at the interagency level with health and safety matters. Field projects and publications in this area cover such aspects as safety in logging and industry and heat stress in forest work.
In the agricultural field some of the diseases of economic importance in livestock also present hazards to persons handling livestock and animal products (e.g., brucellosis, tuberculosis, leptospirosis, anthrax, rabies, Rift Valley fever). For these disease-related activities, close liaison is maintained with WHO through joint committees. FAO is also concerned with the harmonization of registration requirements for pesticides and the assessment of pesticide residues in food and in the environment. As regards atomic energy in food and agriculture, programmes are coordinated with the IAEA in order to assist scientists of developing countries to make safe and effective use of relevant isotope techniques (e.g., the use of radio-labelled enzyme substrates for detecting occupational exposure to insecticides).
The UN Industrial Development Organization (UNIDO) aims to accelerate the industrial development of developing countries. It is concerned with occupational safety and health hazards, environment and hazardous waste management in relation to the industrialization process.
Regional UN Economic Commissions play a role in promoting more effective and harmonized action within their regions.
The UN Conference on Trade and Development (UNCTAD) is concerned with the occupational aspects of the international transfer of goods, services and technology.
International Cooperation in Occupational Health: The Role of International Organizations
The role of international organizations is essentially to offer an organized framework for international cooperation. Over the centuries people have exchanged information and experiences in many ways. Cooperation between countries, scientists and professional groups developed progressively over time, but by the beginning of the 20th century it had become obvious that some issues could be faced only collectively.
In general, a distinction is made between “intergovernmental” and “non-governmental” international organizations. Intergovernmental organizations (IGOs) include the United Nations and its specialized agencies. There are also many other intergovernmental organizations, such as the Organization for Economic Cooperation and Development (OECD), the Organization of African Unity (OAU), the Organization of American States (OAS), and regional or subregional entities, such as the European Union (formerly the European Communities), MERCOSUR (Southern Market—Mercado Comun del Sur), the Caribbean Community (CARICOM), the European Free Trade Association (EFTA) and the North American Free Trade Agreement (NAFTA) between Canada, the United States and Mexico.
Some international non-governmental organizations, such as the International Commission on Occupational Health (ICOH) and the International Social Security Association (ISSA), cover all aspects of occupational health and safety. Many international non-governmental organizations are interested in occupational health and safety within the frameworks of their broader activities, such as the employers’ and workers’ organizations and the international associations of various professional groups. Some non-governmental organizations, such as the International Organization for Standardization (ISO), deal with standardization, and many other non-governmental organizations deal with specific subject areas or with specific sectors of economic activities.
Many intergovernmental and non-governmental organizations have interests in occupational health and safety, which involves technical, medical, social and legal aspects as well as a variety of disciplines, professions and social groups. There is a comprehensive network of organizations whose knowledge and capabilities can be used to promote exchange of information and experience among countries.
Aims and Purposes of Intergovernmental Organizations
One of the important roles of international organizations is to translate agreed-upon values into rights and obligations. The Charter of the United Nations (United Nations 1994) provides a good example of what the role of an international organization in the UN system should be—that is, “to achieve international cooperation in solving international problems of an economic, social, cultural, or humanitarian character, and in improving and encouraging respect for human rights and for fundamental freedom for all without distinction as to race, sex, language or religion.” The International Covenant on Economic, Social and Cultural Rights refers to the principles proclaimed in the Charter of the United Nations and recognizes the right of everyone to safe and healthy working conditions.
The aims and purposes of international organizations are set out in their Charters, Constitutions, Statutes or Basic Texts. For example, the Constitution of the World Health Organization (WHO) (1978) states that its aim is “the attainment by all people of the highest possible level of health”. Protection of the worker against sickness, disease and injury arising from employment is one of the tasks assigned to the International Labour Organization (ILO) in the words of the Preamble of its Constitution (see below and ILO 1992). The Declaration on the Aims and Purposes of the International Labour Organization, adopted by the International Labour Conference at its 26th Session in Philadelphia in 1944, recognizes the obligation of the ILO to further, among the nations of the world, the implementation of programmes that will achieve “adequate protection for the life and health of workers in all occupations”.
The international community recognizes that there are issues where countries are interdependent. One of the main roles of the intergovernmental organizations is to address such issues. The Preamble of the ILO Constitution adopted in 1919 recognizes that “the failure of any nation to adopt humane conditions of labour is an obstacle in the way of other nations which desire to improve the conditions in their own countries” and considers that “a universal and lasting peace can only be established if it is based on social justice”. The ILO Declaration of Philadelphia states that “poverty anywhere constitutes a danger to prosperity everywhere”. The WHO Constitution states that an “unequal development in different countries in the promotion of health and control of diseases, especially communicable diseases, is a common danger” and that “the achievement of any State in the promotion and protection of health is valuable to all”. The role of international organizations is to ensure a continuity and create a stability over time towards such long-term policy objectives, while short- and medium-term planning often prevails at the national level because of local social and economic conditions and political circumstances.
Each international organization has a mandate assigned by its constituents. It is within their mandates that international organizations address specific issues such as occupational health and safety. Common features of intergovernmental organizations are that they provide guidance, formulate recommendations and develop standards. International instruments created within the United Nations system that can be applicable at the national level may be divided into two categories. Nonbinding instruments usually take the form of recommendations or resolutions and can serve as a basis for national legislation. Binding instruments entail the obligation that national laws and practices will be brought into line with the decisions agreed upon at the international level. Most binding instruments take the form of international Conventions that require an additional international act of ratification, approval or accession whereby a State establishes its consent to be bound by the obligations of the Convention.
International organizations represent a forum where their constituents elaborate and establish their common policies and strategies in a great variety of fields, including occupational safety and health. This is where countries confront their values and their opinions; exchange information and experience; discuss and propose solutions; and determine the ways to work together towards objectives in order to achieve consensus, agreement, or international conventions that define a common understanding of what is right to do and what should not be done.
One of the advantages of an international organization is to provide for international debates a controlled environment that is governed by rules and procedures agreed upon by its constituents, allowing, at the same time, for a multitude of informal and diplomatic contacts much wider than those that can be made at the level of a single country. Various groups and countries having similar problems in common may compare their approaches and improve their strategies. From an international perspective, it is easier to achieve objectivity about difficult but specific problems linked to national institutional arrangements or to particular historical conditions. Social partners who can hardly meet at the national level sit at the same table. The dialogue is renewed, and hope for a consensus may come to light where it might have been impossible at the national level. Pressure groups can play a catalytic role in the process of consensus building without a need for aggressive strategies. Not only can exchanges of information and experience take place at international conferences, but various groups can measure the worldwide acceptability of their ideas, values and policies at these conferences.
In practice, intergovernmental organizations are involved in a wide variety of activities covering exchange of information, transfer of knowledge, harmonization of terminology and concepts, consensus building, codes of conduct and of good practice, and promotion and coordination of research. Most international organizations also have numerous programmes and activities aimed at assisting their member States to achieve objectives relevant to their mandate, including technical cooperation. International organizations have at their disposal a variety of means of action, such as reports and studies, meetings of experts, seminars, workshops, symposia, conferences, technical advisory services, information exchanges, and a clearinghouse role. In the course of time, basic mandates of international organizations have been enlarged and made more specific by resolutions and programmes that have been approved by their constituents on the occasion of their general assemblies, such as the International Labour Conference of the ILO or the World Health Assembly of the WHO.
The United Nations and Its Specialized Agencies
In the United Nations system, two specialized agencies are directly concerned with occupational health and safety taken as a whole: the International Labour Organization (ILO) and the World Health Organization (WHO). Among the specialized agencies of the United Nations, the International Labour Organization has a unique character since it is tripartite (i.e., its constituents are governments, employers and workers). Another characteristic of the ILO is its standard-setting activities (i.e., the International Labour Conference adopts international Conventions and Recommendations). Since the working environment is considered an integral part of the human environment (International Labour Organization/United Nations Environment Programme/World Health Organization 1978) the United Nations Environment Programme (UNEP) also deals with the matter, in particular as regards chemicals. Its International Register of Potentially Toxic Chemicals (IRPTC) cooperates closely with the ILO and the WHO within the framework of the International Program on Chemical Safety (IPCS).
Apart from their headquarters, international organizations have field structures and specialized institutions or bodies, such as the WHO’s International Agency for Research on Cancer (IARC), and the Pan-American Centre for Human Ecology and Health (ECO), which contributes to the implementation of the Regional Workers’ Health Program of the Pan-American Health Organization (PAHO). The ILO International Training Centre in Turin (Italy) carries out training activities in occupational health and safety and develops training materials for various professional groups, and the International Institute for Labour Studies (IILS) addresses from time to time occupational safety and health issues. The WHO and the ILO have regional offices, area offices and national correspondents. Regional ILO and WHO conferences are convened periodically. The PAHO was founded in 1902 and is also the WHO Regional Office for the Americas. In 1990, the Pan-American Sanitary Conference adopted a resolution on workers’ health (PAHO 1990) which established guidelines for PAHO’s programme and designated 1992 the “Year of Workers’ Health in the Americas”.
The ILO headquarters and field structures support the commitment and the activities of its member States in occupational health and safety within the framework of its International Programme for the Improvement of Working Conditions and Environment (PIACT) (ILO 1984). This programme includes a large variety of advisory services and technical cooperation activities all over the world. The ILO has recently adopted an active partnership policy (APP) that brings the organization closer to its tripartite constituents in member States by strengthening its field structures, most notably through the establishment of multidisciplinary teams (MDTs).
Several other UN specialized agencies have an important role concerning specific aspects of occupational health and safety, such as the International Atomic Energy Agency (IAEA), which is concerned with nuclear safety, the protection of workers from radiation, and the safety of radiation sources. The United Nations Industrial Development Organization (UNIDO) is concerned with occupational safety and health in specific sectors of industry, and is engaged together with the UNEP and the World Bank in preparing guidelines for industrial pollution prevention and control that cover occupational health and safety issues as well. The Food and Agriculture Organization of the United Nations (FAO) promotes safety in the use of pesticides (FAO 1985) and occupational health and safety in forestry, including cooperative arrangements with the ILO and the United Nations Economic Commission for Europe.
The Committee of Experts on Transport of Dangerous Goods of the Economic and Social Council of the United Nations prepared the Recommendations on the Transport of Dangerous Goods, which provide guidance in drafting national legislation and achieving some uniformity throughout the world for various modes of transport. The International Civil Aviation Organization (ICAO) has established international standards for the operation of aircraft and has published a manual of civil aviation medicine that covers aspects relating to occupational health for flying personnel. The International Maritime Organization (IMO) has adopted an International Convention on Safety of Life at Sea (SOLAS). The WHO, the ILO, and the IMO have prepared an International Medical Guide for ships that includes distinct parts containing a schedule for the contents of a ship’s medicine chest and a medical section of the International Code of Signals. A medical first aid guide for use in accidents involving dangerous substances was jointly prepared by the IMO, the WHO and the ILO.
Funding organizations such as the United Nations Development Programme (UNDP) have been financially supporting over the last 25 years a large number of occupational health and safety projects in many countries, including the establishment of national occupational safety and health institutes. The executing agencies for these projects have been the ILO, the WHO, and both organizations jointly. In its economic development projects, the World Bank takes into account environmental, health and human ecological considerations (World Bank 1974), including occupational health and safety. In 1987, the World Bank embarked on a major effort to incorporate environmental concerns into all aspects of its activities. This includes a stronger focus on the development of institutional capacity for environmental management at the country level, a greater recognition of the need to embed environmental concerns into sectoral work, and increased emphasis on the social aspects of environmentally sustainable development (World Bank 1993a). Furthermore, the Report Investing in Health, examines the interplay between human health, health policy and economic development (World Bank 1993b).
Other Intergovernmental Organizations
The activities of the Organization for Economic Cooperation and Development (OECD) are particularly important as regards environmental health issues, safety in the use of chemicals, methods for the evaluation of chemical risks, and protection from radiation. The Council of Europe has adopted a number of resolutions relating to occupational safety and health concerning, for example, safety services within enterprises. The European Social Charter, adopted by the Council of Europe in 1961, recognizes the right of workers to safe and healthy working conditions. The Nordic Council is concerned with occupational safety and health and environmental problems and makes recommendations regarding toxic and dangerous substances, nuclear safety, and protection from radiation, as well as programmes of action on the occupational environment. The Arab Labour Organization, chartered in 1965, is a specialized agency within the framework of the Arab League; it undertakes studies and conducts research in industrial safety and occupational health. The countries from MERCOSUR have a special commission for the harmonization of legislation in occupational health and safety.
The European Union adopts directives that are compulsory for its member States and should be translated into national laws. The European directives cover the whole field of occupational health and safety with the aim of harmonizing national legislation, taking into account the principle of subsidiarity. Three levels of directives can be identified (TUTB 1991): the framework directives, such as the Directive on the Introduction of Measures to Encourage Improvement in Safety and Health of Workers at Work (89/391); those that cover the risks to which workers are exposed (lead, asbestos, noise, ionizing radiation and so on); and those that establish the rules governing the design of work equipment. Technical standards are developed by European Commissions for Standardization (CEN, CENELEC). The Commission of the European Union (formerly the Commission of the European Communities) prepares the directives and has an important occupational safety and health programme (Commission of the European Communities 1990). The European Foundation for the Improvement of Living and Working Conditions, in Dublin, has activities in occupational safety and health, including a working group on occupational health strategies in Europe. The year 1992 was designated the “European Year of Safety, Hygiene and Health Protection at Work”, and a large number of occupational safety and health activities have been supported in countries of the European Union. A European Agency for Safety and Health at Work was established in Bilbao (Spain) as a specialized body of the European Union.
International Non-governmental Organizations
Scientific, professional and other groups also felt the need to develop international cooperation and join in international non-governmental organizations. They may be formed of individual specialists, national associations of specialists, or institutions. The International Commission on Occupational Health (ICOH) was founded in 1906 as the Permanent Commission on Occupational Diseases. It is discussed in a separate article in this chapter.
The International Social Security Association (ISSA) is an international organization of official agencies responsible for the administration of social security and has had a programme concerning the prevention of occupational risks since 1954 and is also discussed separately in this chapter.
While the ICOH and the ISSA are concerned with the whole field of occupational health and safety, there are a number of non-governmental organizations that deal with specific sectors of economic activity, such as agriculture, or with specific subject areas as varied as technology, toxicology, psychology, work organization, process safety, human engineering, epidemiology, social medicine, lifting appliances, cargo handling, pressured vessels, transport of containers and of dangerous materials, safety signals, road safety and nuclear safety. Numerous international non-governmental organizations are concerned with the environment and the protection of consumers, including the International Union for Conservation of Nature and Natural Resources—World Conservation Union (IUCN) and the International Organization of Consumers Unions (IOCU). They are interested in environmental health and, to some extent, in occupational health, particularly in chemical safety and pesticides.
In the field of the protection of workers, patients and the public from adverse effects of ionizing radiation, the work of the International Commission on Radiological Protection (ICRP) is authoritative worldwide and serves as a basis for international recommendations by intergovernmental organizations. The International Radiation Protection Association (IRPA) has established an International Commission on Non-Ionizing Radiation Protection (ICNIRP), which issues guidelines on exposure limits and contributes to the ILO and WHO publications on non-ionizing radiation. Many other international non-governmental organizations or associations could be mentioned since they deal with occupational health and safety or are interested in specific aspects of occupational health and safety, including the International Ergonomic Association (IEA), the Ergonomics Society of French-Speaking Countries (SELF), the International Council of Nurses (ICN), the Inter-American Safety Council (IASC), the International Association of Labour Inspection (IALA), the International Occupational Hygiene Association (IOHA), the International Association on Agricultural Medicine and Rural Health (IAAMRH), the International Association of Public and Rural Health, the Latino-American Association of Occupational Safety and Hygiene (ALASEHT), the International Federation of Associations of Specialists in Occupational Safety and Industrial Hygiene, the European Association of Schools of Occupational Medicine, the World Federation of Associations of Clinical Toxicology and Poison Control Centres, and the International Safety Council, a global subsidiary of the US National Safety Council.
Another group of non-governmental organizations consists of those having standardization as their objective, such as the International Organization for Standardization (ISO) and the International Electrotechnical Commission (IEC). ISO is discussed in a separate article in this chapter.
International employers’ and workers’ organizations play a significant role in defining occupational health and safety policies and priorities at the international level. Their involvement is important because national labour laws and regulations make employers responsible for protection against occupational hazards, and the most concerned are the workers themselves, since it is their health and safety that are at risk. A number of employers’ and workers’ international organizations are concerned with occupational safety and health taken as a whole, including the International Employers Organization (IOE), the Union of Industrial and Employers Confederations of Europe (UNICE), the International Confederation of Free Trade Unions (ICFTU), the World Confederation of Labour (WCL), and the World Federation of Trade Unions (WFTU). There are many sectoral international trade union organizations that deal with specific aspects, such as the International Confederation of Chemical, Energy, Mine and General Workers’ Union (ICEM), the International Metal Workers Federation (IMF), the International Federation of Building and Wood Workers (IFBWW), the International Federation of Plantation, Agricultural and Allied Workers, and the International Federation of Commercial, Clerical and Technical Employees (FIET). There also exist regional organizations, such as the Organization of African Trade Union Unity (OATUU) and the European Confederation of Trade Unions (ECTU), which has established a European Trade Union Technical Bureau for Occupational Safety and Health (TUTB). These organizations have a wide variety of activities, in particular concerning the dissemination of information, technical advice, and training in occupational health and safety.
Producers, manufacturers, and operators are also active in the field of occupational safety and health, either through their associations or through institutes and bodies that they have established, such as the International Council of Chemical Associations (ICCA), the European Council of Chemical Manufacturers Federations (CEFIC), the International Group of National Associations of Agrochemical Manufacturers (GIFAP), the International Air Transport Association (IATA), the World Association of Nuclear Power Plant Operators (WANO), the Illuminating Engineering Society (IES), the Asbestos International Association (AIA), the International Fiber Safety Group (IFSG), and the Viral Hepatitis Prevention Board (action on hepatitis B as an occupational hazard). In addition, a number of institutions and international bodies established by producers, manufacturers and their organizations develop activities relating to the protection of the environment and environmental health, which may include occupational health to some extent, such as the International Centre for Industry and the Environment (ICIE), the International Council on Metals and the Environment (ICME), the International Primary Aluminum Institute (IPAI), and the Oil Companies International Study Group for Conservation of Clean Air and Water (CONCAWE).
Finally, there are many international non-governmental organizations established by scientists, professional associations or groups having similar scientific, humanitarian or economic interests that do not have direct interests in occupational health but are dealing with scientific, technical, medical or social issues that are relevant to occupational health and safety, such as the World Medical Association (WMA), the Council for International Organizations of Medical Sciences (CIOMS), the International Union of Pure and Applied Chemistry (IUPAC), the International Council for Building Research Studies and Documentation, the International Epidemiological Association, the International Society for Labour Law and Social Security, and the International Bureau for Epilepsy (IBE), which prepared a Code of Principles of Good Practice for Employing People with Epilepsy.
Joint Programmes in International Cooperation
It is interesting to examine how international organizations complement each other and mobilize their various means of action to combat specific occupational hazards. As regards noise and vibration, for example, the IEC provides standards for measuring equipment, the ISO defines methods of measurement, the WHO provides health criteria, the ILO recommends exposure limits in its Code of Practice on Noise and Vibration and defines a general approach and strategy in its Working Environment (Air Pollution, Noise and Vibration) Convention, 1977 (No. 148) and Recommendation (No. 156).
The role of international organizations is increasingly characterized by cooperation within the framework of international programmes or joint ventures on specific subjects involving the countries themselves and inter-governmental and non-governmental organizations. International cooperation in protection against ionizing radiation and in promotion of chemical safety are two examples of such activities.
In the field of protection against ionizing radiation, the International Commission on Radiological Protection (ICRP) and the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) provide the scientific input. The ILO adopted in 1960 the Radiation Protection Convention (No. 115) and Recommendation (No. 114), which make specific reference to the guidance issued by the ICRP. More guidance is given in a number of codes of practice prepared by the IAEA, cosponsored by the ILO and the WHO, where appropriate, and in the ILO Code of Practice on Radiation Protection (ionizing radiation), 1987. These are supplemented by guides, manuals, training materials and technical documents published essentially by the IAEA and by the Nuclear Energy Agency of the OECD. Technical cooperation activities in this field are mainly carried out by the IAEA; other organizations are involved when needed.
In 1990, an important step towards international harmonization of radiation safety took place: the Inter-Agency Committee on Radiation Safety (IACRS) was established as a forum for consultation on and collaboration in radiation safety matters between international organizations. A joint secretariat was set up to revise the 1982 edition of the IAEA/ILO/WHO/NEA-OECD Basic Safety Standards for Radiation Protection. Six international organizations—the FAO, the IAEA, the ILO, the Nuclear Energy Agency of the OECD, the PAHO, and the WHO—joined to prepare international standards with the aim of helping their member States in drafting their own laws. Under the leadership of the IAEA, a major process of consultations with countries and among intergovernmental and non-governmental organizations, including employers’ and workers’ organizations, led to the elaboration of the International Standards for Protection against Ionizing Radiation and the Safety of Radiation Sources (IAEA 1994). These international standards can be regarded as unified standards for the UN system.
International cooperation in promoting chemical safety illustrates how international organizations interact in order to respond to concerns of people in the world expressed by the international community, and how general declarations of principles adopted by intergovernmental conferences are translated into programmes of action and practical activities based on scientific knowledge. There is a consensus that the evaluation of chemicals should address concerns about occupational exposures, public exposures, and the environment. To carry out risk assessments in an international framework is an asset for mobilizing limited expertise and resources. This led to the establishment in 1980 of the International Programme on Chemical Safety (IPCS) by the WHO, the United Nations Environment Programme (UNEP) and the ILO. The commitment of the three cooperating organizations to collaborate in the IPCS was expressed through a memorandum of understanding in 1988 that establishes the objectives of the IPCS. The technical work of the IPCS relies on a network of national and international institutions that participate in its activities and are responsible for particular tasks. The programme maintains close and efficient working relations with several other intergovernmental and non-governmental organizations, associations, and professional bodies that have important activities in the field of chemical safety.
The United Nations Conference on Environment and Development (UNCED), held in Rio de Janeiro in 1992, recognized the need to ensure the environmentally sound management of toxic chemicals and identified six programme areas for international cooperation:
- expanding and accelerating the international assessment of chemical risks
- harmonization of classification and labelling of chemicals
- information exchange on toxic chemicals and chemical risks
- establishment of risk reduction programmes
- strengthening of national capabilities and capacities for management of chemicals
- prevention of illegal international traffic of toxic and dangerous products.
This was followed in 1994 by an International Conference on Chemical Safety (Stockholm Conference 1994), which established the Intergovernmental Forum on Chemical Safety, identified a number of priorities for action, and invited intergovernmental organizations to participate in an expanded collaborative programme on chemical safety. An Inter-Organization Programme for the Sound Management of Chemicals (IOMC) was established in which the WHO, ILO, UNEP, FAO, UNIDO and OECD participate. It includes an Inter-Organization Coordinating Committee (IOCC), which ensures the coordination of activities on chemical safety carried out by the participating organizations, individually or jointly, and follows up the implementation of the recommendations of UNCED.
There are signs of an increasing trend to mobilize expertise and resources within the framework of joint activities. Such is the case, for example, in the field of training and information exchange in occupational health and safety. As regards biological safety, cooperation was developed between the UNIDO, the UNEP, the WHO and the FAO, and some activities were carried out within the framework of the IPCS. The UNIDO has been designated to follow up Chapter 16 of Agenda 21 (environmentally sound management of biotechnology) of the Rio Conference, to catalyze joint activities and programmes, and to develop common UN system strategies on biotechnology. The OECD has a programme on environmental aspects of biotechnology. The European Directive concerning the protection of workers against biological agents at work (90/679 and 93/88) was adopted in 1990 and modified in 1993. In 1993, the International Labour Conference of the International Labour Organization adopted a resolution concerning exposure to and safety in the use of biological agents at work that indicates that the issue should be studied, including the need for new international instruments (convention, recommendation, or both) to minimize the risks to workers, the public and the environment.
Two additional examples concern the protection of workers against non-ionizing radiation and the harmonization of chemical classification and labelling systems. Environmental health criteria documents on non-ionizing radiation were prepared by the WHO, the UNEP and the International Commission on Non-Ionizing Radiation Protection (ICNIRP). A broader cooperation on protection against non-ionizing radiation, including occupational exposure, is now developing, which includes the ILO, the Commission of the European Union, the International Electrotechnical Commission (IEC), the International Agency for Research on Cancer (IARC) and the Scientific Committee on Radiation and Work of the ICOH. The harmonization of chemical classification and labelling systems is a field where extensive cooperation is promoted, under the leadership of the ILO, among countries, intergovernmental organizations (e.g., OECD; the European Union), non-governmental organizations (employers’ and workers’ organizations; international consumer and environmental protection associations), the UN Committee of Experts on Transport of Dangerous Goods, the FAO, the UNEP, the WHO, the IMO and the ICAO.
There are many other fields where new, flexible forms of international cooperation among countries and international organizations are emerging or could be developed, such as occupational stress and combating occupational lung diseases, in particular silicosis. International networking for occupational health and safety is developing increasingly with objectives such as coordinating research. It would be an advantage if an international network for occupational health and safety could be developed on the basis of existing structures in international organizations that could be interconnected, such as the Collaborating Centres of WHO, the Scientific Committees of ICOH, the International Sections of ISSA, the National Correspondents of IRPTC, the contact points of the OECD Complementary Information Procedure, the Participating Institutions of IPCS, the National and Collaborating Centres of the ILO International Occupational Safety and Health Information Centre (CIS), and the designated bodies of the ILO International Occupational Safety and Health Hazard Alert System.
Common Goals and Complementary Approaches in Occupational Health
In the field of occupational health, the ultimate goals of the WHO and the ILO are the same: to protect and promote the health of the workers in all occupations. Policy guidance is given by the ILO on the basis of its international Conventions and Recommendations on occupational health and safety and by the WHO through the resolutions adopted by the World Health Assembly concerning workers’ health and the primary health care approach that it advocates.
Since the Primary Health Care Conference in Alma-Ata in 1978, the WHO workers’ health programme has attempted to extend its health protection and health promotion activities to cover all people at work, paying special attention to the underserved and the vulnerable working populations. The 40th World Health Assembly requested the Director-General of the WHO:
- to promote the implementation of the workers’ health programme, as part of the national health system based on primary health care, in close cooperation with other relevant programmes, non-governmental organizations, and all United Nations agencies
- to elaborate guidelines on primary health care in the workplace, addressed particularly to the underserved working populations and including the educational materials needed at various levels
- to develop guidelines on health promotion in the workplace in cooperation with the WHO collaborating centres
- to promote regional activities in workers’ health where appropriate.
In October 1994, the Second Meeting of the Network of Collaborating Centres in Occupational Health (52 research and expert institutions from 35 countries) adopted a “Global Strategy on Occupational Health for All” and recommended that this document be submitted for consideration by the WHO to be converted into the WHO “Global Strategy on Occupational Health for All”. This was done in May 1996, with the support of the ILO.
The ILO Conventions and Recommendations on occupational safety and health define the rights of the workers and allocate duties and responsibilities to the competent authority, the employers and the workers in the field of occupational safety and health. The ILO Conventions and Recommendations adopted by the International Labour Conference, taken as a whole, constitute the International Labour Code, which defines minimum standards in the labour field. The ILO policy on occupational health and safety is essentially contained in two international Conventions and their accompanying Recommendations. The ILO Occupational Safety and Health Convention 1981 (No. 155) and Recommendation (No. 164), provide for the adoption of a national occupational safety and health policy and describe the actions needed at the national level and at the enterprise level to promote occupational safety and health and to improve the working environment. The ILO Occupational Health Services Convention 1985 (No. 161) and Recommendation (No. 171), provide for the establishment of occupational health services which will contribute to the implementation of the occupational safety and health policy and will perform their functions at the enterprise level.
In 1984, the International Labour Conference adopted a Resolution concerning the improvement of working conditions and environment, which recalled that the improvement of the working conditions and environment was an essential element in the promotion of social justice. It stressed that improved working conditions and improved environment are a positive contribution to national development and represent a measure of success of any economic and social policy. It spelled out the three fundamental principles that:
- Work should take place in a safe and healthy working environment.
- Conditions of work should be consistent with workers’ well-being and human dignity.
- Work should offer real possibilities for personal achievement, self-fulfilment, and service to society.
There are many similar features between the ILO strategy for the improvement of the working conditions and environment and the WHO primary health care approach. They rest on similar basic principles and they both:
- aim at all concerned, workers or the public
- define policies, strategies and means of action
- insist on the responsibility of each employer for the health and safety of the workers in his or her employment
- emphasize primary prevention, control of risk at the source, and health education
- give special importance to information and training
- indicate the need to develop an occupational health practice that is easily accessible to all and available at the workplace
- recognize the central place of participation—community participation in health programmes and workers’ participation in the improvement of the working conditions and the working environment.
- highlight the interactions between health environment and development, as well as between occupational safety and health and productive employment.
The current trend of globalization for the world economy, and regional integration, has increased interdependence and the need for cooperation between countries. This overview shows that there are common goals, approaches and policies in occupational health and safety. There is also a structure on which a global cooperation can be built. This is the objective of the Global Programme on Safety, Health and the Environment, to be launched by the ILO in 1998.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."