- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Case Study: Exposure Standards in Russia
Comparison of the Philosophical Bases of Maximum Allowable Concentrations (MACs) and Threshold Limit Values (TLVs)
Rapid development of chemistry and wide usage of chemical products require specific toxicological studies and hazards evaluation with regard to long-term and combined effects of chemical substances. The setting of standards for chemicals in the working environment is being conducted by occupational hygienists in many countries of the world. Experience on the matter has been accumulated in international and multilateral organizations such as the International Labour Organization, the World Health Organization, the United Nations Environment Programme, the Food and Agriculture Organization and the European Union.
Much has been done in this field by Russian and American scientists. In 1922 studies were launched in Russia to set up standards for chemicals in the air of indoor work areas, and the first maximum allowable concentration (MAC) value for sulphur-containing gas was adopted. By 1930 only 12 MAC values were established, whereas by 1960 their number reached 181.
The American Conference of Governmental Industrial Hygienists (ACGIH) started its work in 1938, and the first threshold limit values (TLVs) list was published in 1946 for 144 substances. The TLVs are to be interpreted and used only by the specialists in this field. If a TLV has been included in the safety standards (the so-called standards of national consensus) and the federal standards, it becomes legal.
At present more than 1,500 MAC values have been adopted for workplace air in Russia. More than 550 TLVs for chemical substances have been recommended in the United States.
Analysis of hygienic standards made in 1980–81 showed that 220 chemicals of the MAC list (Russia) and the TLV list (United States) had the following differences: from two- to fivefold differences were found in 48 substances (22%), 42 substances had five- to ten-fold differences, and 69% substances (31%) had more than ten-fold differences. Ten per cent of the recommended TLVs were 50 times higher than the MAC values for the same substances. The MAC values, in turn, were higher than the TLVs for 16 substances.
The largest divergence of standards occurs in the class of chlorinated hydrocarbons. Analysis of the TLV list adopted in 1989–90 showed a trend toward a reduction of the earlier recommended TLVs compared with the MAC values for chlorinated hydrocarbons and some solvents. Differences among the TLVs and the MACs for the majority of metal aerosols, metalloids, and their compounds were insignificant. The divergences for irritant gases were also slight. The TLVs for lead, manganese and tellurium compared with their MAC analogues disagreed 15, 16 and 10 times, respectively. The differences for acetic aldehyde and formaldehyde were the most extreme—36 and 6 times, respectively. In general, the MAC values adopted in Russia are lower than the TLVs recommended in the United States.
These divergences are explained by the principles used in the development of hygienic standards in the two countries and by the way of these standards are applied to protect workers’ health.
A MAC is a hygienic standard used in Russia to denote a concentration of a harmful substance in the air of the workplace which will not cause, in the course of work for eight hours daily or for any other period of time (but not more than 41 hours per week throughout the working life of an individual), any disease or deviation in the health status as detectable by the available methods of investigation, during the working life or during the subsequent life of the present and next generations. Thus, the concept used in defining the MAC does not allow for any adverse effect on a worker or his or her progeny. The MAC is a safe concentration.
A TLV is the concentration (in air) of a material to which most workers can be exposed daily without adverse effect. These values are established (and revised annually) by the ACGIH and are time-weighted concentrations for a seven- or eight-hour workday and 40-hour workweek. For most materials the value may be exceeded, to a certain extent, provided there are compensatory periods of exposure below the value during the workday (or in some cases the week). For a few materials (mainly those that produce a rapid response) the limit is given as ceiling concentration (i.e., a maximum allowable concentration) that should never be exceeded. The ACGIH states that TLVs should be used as guides in the control of health hazards, and are not fine lines between safe and dangerous concentrations, nor are they a relative index of toxicity.
The TLV definition also contains the principle of inadmissibility of harmful impact. However, it does not cover all of the working population, and it is admitted that a small percentage of workers may manifest health changes or even occupational pathologies. Thus TLVs are not safe for all workers.
According to ILO and WHO experts, these divergences are the result of different scientific approaches to a number of interrelated factors including the definition of an adverse health effect. Therefore, different initial approaches for the control of chemical hazards lead to different methodological principles, essential points of which are presented below.
The main principles of setting hygienic standards for dangerous substances in the air of workplaces in Russia compared with those in the United States are summarized in table 1. Of special importance is the theoretical concept of the threshold, the basic difference between the Russian and the American specialists that underlies their approaches to setting standards. Russia accepts the concept of a threshold for all types of dangerous effects of chemical substances.
Table 1. A comparison of some ideological bases for Russian and American standards
|
Russia (MACs) |
United States (TLVs) |
|
Threshold nature of all kinds of adverse effects. Changes of specific and non-specific factors regarding the criteria of harmful impact are evaluated. |
No recognition of threshold for mutagens and some carcinogens. Changes of specific and non-specific factors depending on “dose-effect ”and “dose-response” relationship are evaluated. |
|
Priority of medical and biological factors over technological and economic criteria. |
Technological and economic criteria prevail. |
|
Prospective toxicological assessment and interpretation of standards before the commercialization of chemical products. |
Retrospective setting of standards. |
However, the recognition of a threshold for some types of effects requires the distinction between injurious and non-injurious effects produced by chemical substances. Consequently, the threshold of unhealthy effects established in Russia is the minimal concentration (dose) of a chemical that causes changes beyond the limits of physiological adaptive responses or produces latent (temporarily compensated) pathologies. In addition, various statistical, metabolic, and toxico-kinetic criteria of adverse effects of chemicals are used to differentiate between the processes of physiological adaptation and pathological compensation. Pathomorphological changes and narcotic symptoms of earliest impairment have been suggested in the United States for the identification of injurious and non-injurious effects. It means that more sensitive methods have been chosen for the toxicity evaluation in Russia than those in the United States. This, therefore, explains the generally lower levels of MACs compared to TLVs. When the detection criteria for injurious and non-injurious effects of chemicals are close or practically coincide, as in the case of irritant gases, the differences in standards are not so significant.
The evolution of toxicology has put into practice new methods for the identification of minor changes in tissues. These are enzyme induction in the smooth endoplastic reticular hepatic tissue and reversible hypertrophy of the liver. These changes may appear after exposure to low concentrations of many chemical substances. Some researchers consider these to be adaptive reactions, while others interpret them as early impairments. Today, one of the most difficult tasks of toxicology is obtaining data that show whether enzyme disturbances, nervous system disorders and changes in behavioural responses are the result of deteriorated physiological functions. This would make it possible to predict more serious and/or irreversible impairments in case of long-term exposure to dangerous substances.
Special emphasis is placed on the differences in the sensitivity of methods used for the establishment of MACs and TLVs. Very sensitive methods of conditioned reflexes applied to studies of the nervous system in Russia have been found to be the main cause of divergences between the MACs and the TLVs. However, the use of this method in the process of hygienic standardization is not obligatory. Numerous methods of different sensitivities are normally used for the developing of a hygienic standard.
A great number of studies conducted in the United States in connection with the setting-up of exposure limits are aimed at examining the transformation of industrial compounds in the human body (routes of exposure, circulation, metabolism, removal, etc.). Methods of chemical analysis used to establish the values of TLVs and MACs also cause divergences due to their different selectivities, accuracies and sensitivities. An important element usually taken into consideration by OSHA in the standardization process in the United States is the “technical attainability” of a standard by industry. As a result, some standards are recommended on a basis of the lowest presently existing concentrations.
MAC values in Russia are established on a basis of the prevalence of medico-biological characteristics, whereas the technological attainability of a standard is practically ignored. This partly explains lower MAC values for some chemical substances.
In Russia MAC values are assessed in toxicological studies before a substance is authorized for industrial use. A tentative safe exposure level is established during the laboratory synthesis of a chemical. The MAC value is established after animal experiments, at the design stage of the industrial process. The correction of the MAC value is carried out after evaluation of working conditions and workers’ health when the substance is used in industry. Most of the safe levels of exposure in Russia have been recommended after experiments on animals.
In the United States a final standard is established after a chemical substance has been introduced in industry, because the values of permissible levels of exposure are based on the assessment of health. As long as the differences of principle between the MACs and the TLVs remain, it is unlikely to expect the convergence of these standards in the near future. However, there is a trend towards the reduction of some TLVs that makes this not so impossible as it may seem.
Legislation Guaranteeing Benefits for Workers in China
The occupational safety and health of workers has been an important aspect of legislation laid down in the form of the Labour Law promulgated in July 1994. To urge enterprises into the market system, and in the meantime to protect the rights of labourers, in-depth reforms in the system of labour contracts and wage distribution and in social security have been major priorities in the government agenda. Establishing a uniform welfare umbrella for all workers regardless of the ownership of the enterprises is one of the goals, which also include unemployment coverage, retirement pension systems, and occupational disease and injuries compensation insurance. The Labour Law requires that all employers pay a social security contribution for their workers. Part of the legislation, the draft of the Occupational Disease Prevention and Control Law, will be an area of the Labour Law to which major attention has been devoted in order to regulate the behaviour and define the responsibilities of employers in controlling occupational hazards, while at the same time giving more rights to workers in protecting their own health.
Cooperation Between Governmental Agencies and the All-China Federation of Trade Unions in Policy Making and Legislation Enforcement
The Ministry of Public Health (MOPH), the Ministry of Labour (MOL), and the All-China Federation of Trade Unions (ACFTU) have a long history of cooperation. Many important policies and activities have resulted from their joint efforts.
The current division of responsibility between the MOPH and the MOL in occupational safety and health is as follows:
- From the preventive medical point of view, the MOPH oversees industrial hygiene and occupational health, enforcing national health inspection.
- The focus of the MOL is on engineering the control of occupational hazards and on the organization of labour, as well as overseeing occupational safety and health and enforcing national labour inspection (figure 1) (MOPH and MOL 1986).
Figure 1. Governmental organization and division of responsibility for occupational health and safety
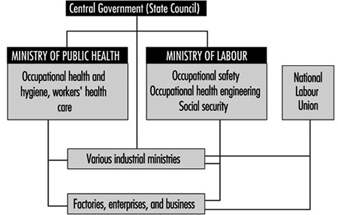
It is difficult to draw a line between the responsibilities of the MOPH and the MOL. It is expected that further cooperation will focus on enhancing enforcement of occupational safety and health regulations.
The ACFTU has been increasingly involved in safeguarding workers’ rights. One of the important tasks of the ACFTU is to promote the establishment of trade unions in foreign-funded enterprises. Only 12% of overseas-funded enterprises have established unions.
Occupational Health and Safety: The European Union
The European Union (EU) today exercises a major influence on worldwide health and safety law and policy. In 1995, the Union comprised the following Member States: Austria, Belgium, Denmark, Finland, France, Germany, Greece, Ireland, Italy, Luxembourg, Netherlands, Portugal, Spain, Sweden and the United Kingdom. It will probably expand in years to come.
The forerunner of the Union, the European Community, was created in the 1950s by three treaties: The European Coal and Steel Community Treaty (ECSC) signed in Paris in 1951, and the European Economic Community (EEC) and European Atomic Energy Community (EAEC) Treaties signed in Rome in 1957. The European Union was formed with the entry into force of the Maastricht Treaty (concluded in 1989) on 1 January 1992.
The Community has four institutions, namely, the Commission, the Council, the Parliament and the European Court of Justice. They derive their powers from the treaties.
The Structures
The Commission
The Commission is the Community’s executive body. It is responsible for initiating, proposing and implementing Community policy, and if a Member State fails to fulfil its obligations under the treaties, the Commission can take proceedings against that Member State in the European Court of Justice.
It is composed of seventeen members appointed by the governments of Member States for a renewable four-year period. Each Commissioner is responsible for a portfolio and has authority over one or more Directorates General. One such Directorate General, DG V, is concerned with Employment, Industrial Relations and Social Affairs, and it is from within this Directorate General (DG V/F) that health and safety and public health policies are both initiated and proposed. The Commission is assisted in its health and safety law and policy-making role by the Advisory Committee on Safety, Hygiene and Health Protection at Work and the European Foundation for the Improvement of Living and Working Conditions.
Advisory Committee on Safety, Hygiene and Health Protection at Work
The Advisory Committee was established in 1974 and is chaired by the Commissioner responsible for the Directorate-General for Employment, Industrial Relations and Social Affairs. It consists of 96 full members: two representatives each of government, trade unions, and employers’ organizations from each Member State.
The role of the Advisory Committee is to “assist the Commission in the preparation and implementation of activities in the fields of safety, hygiene and health protection at work”. Because of its constitution and membership, the Advisory Committee is much more important and pro-active than its title suggests, so that, over the years, it has had a significant influence on strategic policy development, acting alongside the European Parliament and the Economic and Social Committee. More specifically, the Committee is responsible for the following matters within its general frame of reference:
- conducting exchanges of views and experience regarding existing or planned regulations
- contributing towards the development of a common approach to problems existing in the fields of safety, hygiene and health protection at work and towards the choice of Community priorities as well as measures necessary for implementing them
- drawing the Commission’s attention to areas in which there is an apparent need for the acquisition of new knowledge and for the implementation of appropriate educational and research projects
- defining, within the framework of Community action programmes, and in cooperation with the Mines Safety and Health Commission, (i) the criteria and aims of the campaign against the risk of accidents at work and health hazards within the undertaking; and (ii) methods enabling undertakings and their employees to evaluate and to improve the level of protection
- contributing towards keeping national administrations, trade unions and employers’ organizations informed of Community measures in order to facilitate their cooperation and to encourage initiatives promoted by them aiming at exchanges of experience and at laying down codes of practice
- submitting opinions on proposals for directives and on all measures proposed by the Commission which are of relevance to health and safety at work.
In addition to these functions, the Committee prepares an annual report, which the Commission then forwards to the Council, the Parliament and the Economic and Social Committee.
The Dublin Foundation
The European Foundation for the Improvement of Living and Working Conditions, located in Dublin, was established in 1975 as a specialized, autonomous Community body. The Foundation is primarily engaged in applied research in the areas of social policy, the application of new technologies, and the improvement and protection of the environment, in an effort to identify, cope with and forestall problems in the working environment.
European Agency for Health and Safety at the Workplace
The European Council has recently established the European Agency for Health and Safety at the Workplace in Bilbao, Spain, which is responsible for collating and disseminating information in its sector of activities. It will also organize training courses, supply technical and scientific support to the Commission and forge close links with specialized national bodies. The agency will also organize a network system with a view to exchanging information and experiences between Member States.
The European Parliament
The European Parliament exercises an increasingly important consultative role during the Community’s legislative process, controls a part of the Community’s budget jointly with the Council, approves Community Association agreements with non-member countries and treaties for the accession of new Member States, and is the Community’s supervisory body.
The Economic and Social Committee
The Economic and Social Committee is an advisory and consultative body which is required to give its opinion on a range of social and vocational issues, including health and safety at work. The Committee draws its membership from three main groups: employers, workers and an independant group comprising members with a wide spectrum of interests including professional, business, farming, the cooperative movement and consumer affairs.
Legal Instruments
There are four main instruments available to the Community legislator. Article 189 of the EEC Treaty as amended provides that “In order to carry out their task and in accordance with the provisions of this Treaty, the European Parliament acting jointly with the Council and the Commission shall make regulations and issue directives, take decisions, make recommendations or deliver opinions.”
Regulations
It is stated that “A regulation shall have general application. It shall be binding in its entirety and directly applicable in all Member States.” Regulations are directly enforceable in Member States. There is no need for further implementation. Indeed, it is not permissible for legislatures to consider them with a view to that end. In the field of health and safety at work, regulations are rare and those that have been made are administrative in nature.
Directives and decisions
It is stated that “A directive shall be binding, as to the result to be achieved, upon each Member State to which it is addressed, but shall leave to the national authorities the choice of form and methods.” Directives are instructions to Member States to enact laws to achieve an end result. In practice, directives are used mainly to bring about the harmonization or approximation of national laws in accordance with Article 100. They are therefore the most appropriate and commonly used instruments for occupational health and safety matters. In relation to decisions, it is stated that “A decision shall be binding in its entirety upon those to whom it is addressed.”
Recommendations and opinions
Recommendations and opinions have no binding force but are indicative of policy stances.
Policy
The European Communities made a decision in the mid-1980s to press ahead strongly with harmonization measures in the field of health and safety. Various reasons have been put forward to explain the developing importance of this area, of which four may be considered to be significant.
First, it is said that common health and safety standards assist economic integration, since products cannot circulate freely within the Community if prices for similar items differ in various Member States because of variable health and safety costs imposed on business. Second, 10 million people a year are the victims of, and 8,000 people a year die from, workplace accidents (out of a workforce which numbered 138 million people in 1994). These grim statistics give rise to an estimated bill of ECU 26,000 million paid in compensation for occupational accidents and diseases annually, whilst in Britain alone the National Audit Office in their Report Enforcing Health and Safety in the Workplace estimated that the cost of accidents to industry and the taxpayer is £10 billion per year. It is argued that a reduction of the human, social and economic costs of accidents and ill-health borne by this workforce will not only bring about a huge financial saving but will also bring about a significant increase in the quality of life for the whole Community. Third, the introduction of more efficient work practices is said to bring with it increased productivity, lower operational costs and better industrial relations.
Finally, it is argued that the regulation of certain risks, such as those arising from massive explosions, should be harmonized at a supranational level because of the scale of resource costs and (an echo of the first reason canvassed above) because any disparity in the substance and application of such provisions produces distortions of competition and affects product prices.
Much impetus was given to this programme by the campaign organized by the Commission in collaboration with the twelve Member States in the European Year of Health and Safety, which took place during the 12-month period commencing 1 March 1992. This campaign sought to reach the whole of the Community’s working population, particularly targeting high-risk industries and small and medium-sized enterprises.
Each of the founding treaties laid the basis for new health and safety laws. The EEC Treaty, for example, contains two provisions which are, in part at least, devoted to the promotion of health and safety, namely articles 117 and 118.
Community Charter of the Fundamental Social Rights of Workers
To meet the challenge, a comprehensive programme of measures was proposed by the Commission in 1987 and adopted by the Council in the following year. This programme contained a series of health and safety measures grouped under the headings of safety and ergonomics, health and hygiene, information and training, initiatives concerning small and medium enterprises, and social dialogue. Added impetus to these policies was provided by the Community Charter of the Fundamental Social Rights of Workers, adopted in Strasbourg in December 1989 by 11 of the 12 Member States (the United Kingdom abstained).
The Social Charter, as agreed in December 1989, covers 12 categories of “fundamental social rights” among them are several of practical relevance here:
- Improvement of living and working conditions. There should be improvement in working conditions, particularly in terms of limits on working time. particular mention is made of the need for improved conditions for workers on part-time or seasonal contracts and so on.
- Social protection. Workers, including the unemployed, should receive adequate social protection and social security benefits.
- Information, consultation and participation for workers. This should apply especially in multinational companies and in particular at times of restructuring, redundancies or the introduction of new technology.
- Health protection and safety at the workplace.
- Protection of children and adolescents. The minimum employment age should be no lower than the minimum school-leaving age, and in any case not lower than 15 years. The hours which those aged under 18 can work should be limited, and they should not generally work at night.
- Elderly persons. Workers should be assured of resources providing a decent standard of living upon retirement. Others should have sufficient resources and appropriate medical and social assistance.
- Disabled people. All disabled people should have additional help towards social and professional integration.
Member States are given responsibility in accordance with national practices for guaranteeing the rights in the Charter and implementing the necessary measures, and the Commission is asked to submit proposals on areas within its competence.
Since 1989, it has become clear that within the Community as a whole there is much support for the Social Charter. Undoubtedly, Member States are anxious to show that workers, children and older workers should benefit from the Community as well as shareholders and managers.
The 1989 Framework Directive
The principles in the Commission’s health and safety programme were set out in another “Framework Directive” (89/391/EEC) on the introduction of measures to encourage improvements in the safety and health of workers at work. This makes a significant step forward from the approach witnessed in the earlier “Framework Directive” of 1980. In particular, the 1989 Directive, while endorsing and adopting the approach of “self-assessment”, also sought to establish a variety of basic duties, especially for the employer. Furthermore, the promotion of “social dialogue” in the field of health and safety at work was explicitly incorporated into detailed provisions in the 1989 Directive, introducing significant requirements for information, consultation and participation for workers and their representatives at the workplace. This 1989 Directive required compliance by 31 December 1992.
The Directive contains re-stated general principles concerning, in particular, the prevention of occupational risks, the protection of safety and health and the informing, consultation and training of workers and their representatives, as well as principles concerning the implementation of such measures. This measure constituted a first attempt to provide an overall complement to the technical harmonization directives designed to complete the internal market. The 1989 Directive also brought within its scope the provisions of the 1980 Framework Directive on risks arising from use at work of chemical, physical and biological agents. It parallels the ILO Convention concerning Occupational Safety and Health, 1981 (No. 155) and its accompanying Recommendation (No. 161).
The overall objectives of the 1989 Directive may be summarized as being:
- humanization of the working environment
- accident prevention and health protection at the workplace
- to encourage information, dialogue and balanced participation on safety and health by means of procedures and instruments
- to promote throughout the Community, the harmonious development of economic activities, a continuous and balanced expansion and an accelerated rise in the standard of living
- to encourage the increasing participation of management and labour in decisions and initiatives
- to establish the same level of health protection for workers in all undertakings, including small and medium-sized enterprises, and to fulfil the single market requirements of the Single European Act 1986; and
- the gradual replacement of national legislation by Community legislation.
General duties placed upon the employer include duties of awareness, duties to take direct action to ensure safety and health, duties of strategic planning to avoid risks to safety and health, duties to train and direct the workforce, duties to inform, consult and involve the workforce, and duties of recording and notification.
The Directive provided similar safeguards for small and medium-sized enterprises. It is stated, for example, that the size of the undertaking and/or establishment is a relevant matter in relation to determining the sufficiency of resources for dealing with the organization of protective and preventive measures. It is also a factor to be considered in relation to obligations concerning first aid, fire fighting and evacuation of workers. Furthermore, the Directive included a power for differential requirements to be imposed upon varying sizes of undertakings as regards documentation to be provided. Finally, in relation to the provision of information, it is stated that national measures “may take account, inter alia, of the size of the undertaking and/or establishment”.
Under the umbrella of the 1989 Directive, a number of individual directives have also been adopted. In particular, “daughter” directives have been adopted on minimum safety and health requirements for the workplace, for the use of work equipment, for the use of personal protective equipment, for the manual handling of loads, and for work with display screen equipment.
The following Directives have also been adopted:
- Council Directive of 20 December 1993 concerning the minimum safety and health requirements for work on board fishing vessels (93/103/EEC)
- Council Directive of 12 October 1993 amending Directive 90/679/EEC on the protection of workers from risks related to exposure to biological agents at work (93/88/EEC)
- Council Directive of 3 December 1992 on the minimum requirements for improving the safety and health protection of workers in surface and underground mineral-extracting industries (92/104/EEC)
- Council Directive of 3 November 1992 on the minimum requirements for improving the safety and health protection of workers in mineral-extracting industries that involve drilling (92/91/EEC)
- Council Directive of 19 October 1992 on the introduction of measures to encourage improvements in the safety and health at work of pregnant workers and workers who have recently given birth or who are breast-feeding (92/85/EEC)
- Council Directive of 24 June 1992 on the minimum requirements for the provision of safety and/or health signs at work (92/58/EEC)
- Council Directive of 24 June 1992 on the implementation of minimum safety and health requirements at temporary or mobile construction sites (92/57/EEC)
- Council Directive of 31 March 1992 on the minimum safety and health requirements for improved medical treatment on board vessels (92/29/EEC)
- Council Directive of 23 April 1990 on the contained use of genetically modified micro-organisms. (90/219/ EEC)
Since the passage of the Maastricht Treaty, further measures have been passed, namely: a Recommendation on a European schedule of industrial diseases; a directive on asbestos; a directive on safety and health signs at the workplace; a directive on medical assistance on board vessels; directives on health and safety protection in the extractive industries; and a directive introducing measures to promote improvements in the travel conditions of workers with motor disabilities.
The Single Market
The original Article 100 has been replaced by a new provision in the Treaty of European Union. The new Article 100 ensures that the European Parliament and the Economic and Social Committee must be consulted in all cases and not simply when the implementation of a directive would involve the amendment of legislation in one or more Member States.
The COSH Movement and Right to Know
Formed in the wake of the US Occupational Safety and Health Act of 1970, committees on occupational safety and health initially emerged as local coalitions of public health advocates, concerned professionals, and rank-and-file activists meeting to deal with problems resulting from toxics in the workplace. Early COSH groups started in Chicago, Boston, Philadelphia and New York. In the south, they evolved in conjunction with grass roots organizations such as Carolina Brown Lung, representing textile mill workers suffering from byssinosis. Currently there are 25 COSH groups around the country, at various stages of development and funded through a wide variety of methods. Many COSH groups have made a strategic decision to work with and through organized labor, recognizing that union-empowered workers are the best equipped to fight for safe working conditions.
COSH groups bring together a broad coalition of organizations and individuals from unions, the public health community and environmental interests, including rank-and-file safety and health activists, academics, lawyers, doctors, public health professionals, social workers and so on. They provide a forum in which interest groups that do not normally work together can communicate about workplace safety and health problems. In the COSH, workers have a chance to discuss the safety and health issues they confront on the shop floor with academics and medical experts. Through such discussions, academic and medical research can get translated for use by working people.
COSH groups have been highly active politically, both through traditional means (such as lobbying campaigns) and through more colorful methods (such as picketing and carrying coffins past the homes of anti-labor elected officials). COSH groups played a key role in the struggles for local and state right-to-know legislation, building broad-based coalitions of union, environmental and public interest organizations to support this cause. For example, the Philadelphia area COSH group (PHILAPOSH) ran a campaign which resulted in the first city right-to-know law passed in the country. The campaign climaxed when PHILAPOSH members dramatized the need for hazard information by opening an unmarked pressurized canister at a public hearing, sending members of the City Council literally diving under tables as the gas (oxygen) escaped.
Local right-to-know campaigns eventually yielded more than 23 local and state right-to-know laws. The diversity of requirements was so great that chemical corporations ultimately demanded a national standard, so they would not have to comply with so many differing local regulations. What happened with COSH groups and right to know is an excellent example of how the efforts of labor and community coalitions working at the local level can combine to have a powerful national impact on occupational safety and health policy.
Right to Know: The Role of Community-Based Organizations
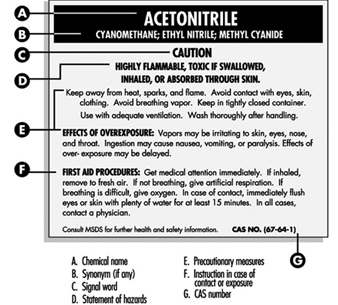
In the context of occupational health and safety, “right to know” refers generally to laws, rules and regulations requiring that workers be informed about health hazards related to their employment. Under right-to-know mandates, workers who handle a potentially harmful chemical substance in the course of their job duties cannot be left unaware of the risk. Their employer is legally obligated to tell them exactly what the substance is chemically, and what kind of health damage it can cause. In some cases, the warning must also include advice on how to avoid exposure and must state the recommended treatment in case exposure does occur. This policy contrasts sharply with the situation it was meant to replace, unfortunately still prevailing in many workplaces, in which workers knew the chemicals they used only by trade names or generic names such as “Cleaner Number Nine” and had no way to judge whether their health was being endangered.
Under right-to-know mandates, hazard information is usually conveyed through warning labels on workplace containers and equipment, supplemented by worker health and safety training. In the United States, the major vehicle for worker right to know is the Occupational Safety and Health Administration’s Hazard Communication Standard, finalized in 1986. This federal regulatory standard requires labelling of hazardous chemicals in all private-sector workplaces. Employers must also provide workers access to a detailed Materials Safety Data Sheet (MSDS) on each labelled chemical, and provide worker training in safe chemical handling. Figure 1 shows a typical US right-to-know warning label.
Figure 1. Right-to-know chemical warning label
It should be noted that as a policy direction, the provision of hazard information differs greatly from direct regulatory control of the hazard itself. The labelling strategy reflects a philosophical commitment to individual responsibility, informed choice and free market forces. Once armed with knowledge, workers are in theory supposed to act in their own best interests, demanding safe working conditions or finding different work if necessary. Direct regulatory control of occupational hazards, by contrast, assumes a need for more active state interventions to counter the power imbalances in society that prevent some workers from making meaningful use of hazard information on their own. Because labelling implies that the informed workers bear ultimate responsibility for their own occupational safety, right-to-know policies occupy a somewhat ambiguous status politically. On the one hand, they are cheered by labour advocates as a victory enabling workers to protect themselves more effectively. On the other hand, they can threaten workers’ interests if right to know is allowed to replace or weaken other occupational safety and health regulations. As activists are quick to point out, the “right to know” is a starting point that needs to be complemented with the “right to understand” and the “right to act”, as well as with continued effort to control work hazards directly.
Local organizations play a number of important roles in shaping the real-world significance of worker right-to-know laws and regulations. First and foremost, these rights often owe their very existence to public interest groups, many of them community based. For example, “COSH groups” (grass-roots Committees on Occupational Safety and Health) were central participants in the lengthy rule-making and litigation that went into establishing the Hazard Communication Standard in the United States. See box for a more detailed description of COSH groups and their activities.
Organizations in the local community also play a second critical role: assisting workers to make more effective use of their legal rights to hazard information. For example, COSH groups advise and assist workers who feel they may suffer retaliation for seeking hazard information; raise consciousness about reading and observing warning labels; and help bring to light employer violations of right-to-know requirements. This help is particularly important to workers who feel intimidated in using their rights due to low education levels, low job security, or lack of a supportive trade union. COSH groups also assist workers in interpreting the information contained on labels and in Material Safety Data Sheets. This kind of support is badly needed for workers with limited literacy. It can also help workers with good reading skills but insufficient technical background to understand the MSDSs, which are often written in scientific language confusing to an untrained reader.
Worker right to know is not only a matter of transmitting factual information; it also has an emotional side. Through right to know, workers may learn for the first time that their jobs are dangerous in ways they had not realized. This disclosure can stir up feelings of betrayal, outrage, dread and helplessness—sometimes with great intensity. Accordingly, a third important role that some community-based organizations play in worker right to know is to provide emotional support for workers struggling to deal with the personal implications of hazard information. Through self-help support groups, workers receive validation, a chance to express their feelings, a sense of collective support, and practical advice. In addition to COSH groups, examples of this kind of self-help organization in the United States include Injured Workers, a national network of support groups that provides a newsletter and locally available support meetings for individuals contemplating or involved in workers’ compensation claims; the National Center for Environmental Health Strategies, an advocacy organization located in New Jersey, serving those at risk of or suffering from multiple chemical sensitivity; and Asbestos Victims of America, a national network centred in San Francisco that offers information, counselling, and advocacy for workers exposed to asbestos.
A special case of right to know involves locating workers known to have been exposed to occupational hazards in the past, and informing them of their elevated health risk. In the United States, this kind of intervention is called “high-risk worker notification”. Numerous state and federal agencies in the United States have developed programmes of worker notification, as have some unions and a number of large corporations. The federal government agency most actively involved with worker notification at present is the National Institute for Occupational Safety and Health (NIOSH). This agency carried out several ambitious community-based pilot programmes of worker notification in the early 1980s, and now includes worker notification as a routine part of its epidemiological research studies.
NIOSH’s experience with this kind of information provision is instructive. In its pilot programmes, NIOSH undertook to develop accurate lists of workers with probable exposure to hazardous chemicals in a particular plant; to send personal letters to all workers on the list, informing them of the possibility of health risk; and, where indicated and feasible, to provide or encourage medical screening. It immediately became obvious, however, that the notification did not remain a private matter between the agency and each individual worker. On the contrary, at every step the agency found its work affected by community-based organizations and local institutions.
NIOSH’s most controversial notification took place in the early 1980s in Augusta, Georgia, with 1,385 chemical workers who had been exposed to a potent carcinogen (β-naphthylamine). The workers involved, predominantly African-American males, were unrepresented by a union and lacked resources and formal education. The community’s social climate was, in the words of programme staff, “highly polarized by racial discrimination, poverty, and substantial lack of understanding of toxic hazards”. NIOSH helped establish a local advisory group to encourage community involvement, which quickly took on a life of its own as more militant grass-roots organizations and individual worker advocates joined the effort. Some of the workers sued the company, adding to the controversies already surrounding the programme. Local organizations such as the Chamber of Commerce and the county Medical Society also became involved. Even many years later, echoes can still be heard of the conflicts among local organizations involved in the notification. In the end, the programme did succeed in informing the exposed workers of their life-long risk for bladder cancer, a highly treatable disease if caught early. Over 500 of them were medically screened through the programme, and a number of possibly life-saving medical interventions resulted.
A striking feature of the Augusta notification is the central role played by the news media. Local news coverage of the programme was extremely heavy, including over 50 newspaper articles and a documentary film about the chemical exposures (“Lethal Labour”) shown on local TV. This publicity reached a wide audience and had enormous impact on the notified workers and the community as a whole, leading the NIOSH project director to observe that “in actuality, the news media perform the real notification”. In some situations, it may be useful to regard local journalists as an intrinsic part of right to know and plan a formal role for them in the notification process to encourage more accurate and constructive reporting.
While the examples here are drawn from the United States, the same issues arise worldwide. Worker access to hazard information represents a step forward in basic human rights, and has properly become a focal point of political and service effort for pro-worker community-based organizations in many countries. In nations with weak legal protections for workers and/or weak labour movements, community-based organizations are all the more important in terms of the three roles discussed here—advocating for stronger right-to-know (and right-to-act) laws; assisting workers to use right-to-know information effectively; and providing social and emotional support for those who learn they are at risk from work hazards.
Community-Based Organizations
The role of community groups and the voluntary sector in occupational health and safety has grown rapidly during the past twenty years. Hundreds of groups spread across at least 30 nations act as advocates for workers and sufferers from occupational diseases, concentrating on those whose needs are not met within workplace, trade union or state structures. Health and safety at work forms part of the brief of many more organizations which fight for workers’ rights, or on broader health or gender-based issues.
Sometimes the life-span of these organizations is short because, in part as a result of their work, the needs to which they respond become recognized by more formal organizations. However, many community and voluntary sector organizations have now been in existence for 10 or 20 years, altering their priorities and methods in response to changes in the world of work and the needs of their constituency.
Such organizations are not new. An early example was the Health Care Association of the Berlin Workers Union, an organization of doctors and workers which provided medical care for 10,000 Berlin workers in the mid-nineteenth century. Before the rise of industrial trade unions in the nineteenth century, many informal organizations fought for a shorter working week and the rights of young workers. The lack of compensation for certain occupational diseases formed the basis for organizations of workers and their relatives in the United States in the mid-1960s.
However, the recent growth of community and voluntary sector groups can be traced to the political changes of the late 1960s and 1970s. Increasing conflict between workers and employers focused on working conditions as well as pay.
New legislation on health and safety in the industrialized countries arose from an increased concern with health and safety at work amongst workers and trade unions, and these laws in turn led to further increases in public awareness. While the opportunities offered by this legislation have seen health and safety become an area for direct negotiation between employers, trade unions and government in most countries, workers and others suffering from occupational disease and injury have frequently chosen to exert pressure from outside these tripartite discussions, believing that there should be no negotiation over fundamental human rights to health and safety at work.
Many of the voluntary sector groups formed since that time have also taken advantage of cultural changes in the role of science in society: an increasing awareness amongst scientists of the need for science to meet the needs of workers and communities, and an increase in the scientific skills of workers. Several organizations recognize this alliance of interest in their title: the Academics and Workers Action (AAA) in Denmark, or the Society for Participatory Research in Asia, based in India.
Strengths and Weaknesses
The voluntary sector identifies as its strengths an immediacy of response to emerging problems in occupational health and safety, open organizational structures, the inclusion of marginalized workers and sufferers from occupational disease and injury, and a freedom from institutional constraints on action and utterance. The problems of the voluntary sector are uncertain income, difficulties in marrying the styles of voluntary and paid staff, and difficulties in coping with the overwhelming unmet needs of workers and sufferers from occupational ill-health.
The transient character of many of these organizations has already been mentioned. Of 16 such organizations known in the UK in 1985, only seven were still in existence in 1995. In the meantime, 25 more had come into existence. This is characteristic of voluntary organizations of all kinds. Internally they are frequently non-hierarchically organized, with delegates or affiliates from trade unions and other organizations as well as others suffering from work-related health problems. While links with trade unions, political parties and governmental bodies are essential to their effectiveness in improving conditions at work, most have chosen to keep such relationships indirect, and to be funded from several sources—typically, a mixture of statutory, labour movement, commercial or charitable sources. Many more organizations are entirely voluntary or produce a publication from subscriptions which cover printing and distribution costs only.
Activities
The activities of these voluntary sector bodies can be broadly categorized as based on single hazards (illnesses, multinational companies, employment sectors, ethnic groups or gender); advice centres; occupational health services; newsletter and magazine production; research and educational bodies; and supranational networks.
Some of the longest-established bodies fight for the interests of sufferers from occupational diseases, as shown in the following list, which summarizes the principal concerns of community groups around the world: multiple chemical sensitivity, white lung, black lung, brown lung, Karoshi (sudden death through overwork), repetitive strain injury, accident victims, electrical sensitivity, women’s occupational health, Black and ethnic minority occupational health, white lung (asbestos), pesticides, artificial mineral fibres, microwaves, visual display units, art hazards, construction work, Bayer, Union Carbide, Rio Tinto Zinc.
Concentration of efforts in this way can be particularly effective; the publications of the Center for Art Hazards in New York City were models of their kind, and projects drawing attention to the special needs of migrant minority ethnic workers have had successes in the United Kingdom, the United States, Japan and elsewhere.
A dozen organizations around the world fight for the particular health problems of ethnic minority workers: Latino workers in the United States; Pakistani, Bengali and Yemeni workers in England; Moroccan and Algerian workers in France; and South-East Asian workers in Japan among others. Because of the severity of the injuries and illnesses suffered by these workers, adequate compensation, which often means recognition of their legal status, is a first demand. But an end to the practice of double standards in which ethnic minority workers are employed in conditions which majority groups will not tolerate is the main issue. A great deal has been achieved by these groups, in part through securing better provision of information in minority languages on health and safety and employment rights.
The work of the Pesticides Action Network and its sister organizations, especially the campaign to get certain pesticides banned (the Dirty Dozen Campaign) has been notably successful. Each of these problems and the systematic abuse of the working and external environments by certain multinational companies are intractable problems, and the organizations dedicated to resolving them have in many cases won partial victories but have set themselves new goals.
Advice Centres
The complexity of the world of work, the weakness of trade unions in some countries, and the inadequacy of statutory provision of health and safety advice at work, have resulted in the setting up of advice centres in many countries. The most highly developed networks in English-speaking countries deal with tens of thousands of enquiries each year. They are largely reactive, responding to needs as reflected by those who contact them. Recognized changes in the structure of advanced economies, towards a reduction in the size of workplaces, casualization, and an increase in informal and part-time work (each of which creates problems for the regulation of working conditions) have enabled advice centres to obtain funding from state or local government sources. The European Work Hazards Network, a network of workers and workers’ health and safety advisers, has recently received European Union funding. The South African advice centres network received EU development funding, and community-based COSH groups in the United States at one time received funds through the New Directions programme of the US Occupational Safety and Health Administration.
Occupational Health Services
Some of the clearest successes of the voluntary sector have been in improving the standard of occupational health service provision. Organizations of medically and technically trained staff and workers have demonstrated the need for such provision and pioneered novel methods of delivering occupational health care. The sectoral occupational health services which have been brought into existence progressively over the last 15 years in Denmark received powerful advocacy from the AAA particularly for the role of workers’ representatives in management of the services. The development of primary-care-based services in the UK and of specific services for sufferers from work-related upper limb disorders in response to the experience of workers’ health centres in Australia are further examples.
Research
Changes within science during the 1960s and 1970s have lead to experimentation with new methods of investigation described as action research, participatory research or lay epidemiology. The definition of research needs by workers and their trade unions has created an opportunity for a number of centres specializing in carrying out research for them; the network of Science Shops in the Netherlands, DIESAT, the Brazilian trade union health and safety resource centre, SPRIA (the Society for Participatory Research in Asia) in India, and the network of centres in the Republic of South Africa are amongst the longest established. Research carried out by these bodies acts as a route by which workers’ perceptions of hazards and their health become recognized by mainstream occupational medicine.
Publications
Many voluntary sector groups produce periodicals, the largest of which sell thousands of copies, appear up to 20 times a year and are read widely within statutory, regulatory and trade union bodies as well as by their target audience amongst workers. These are effective networking tools within countries (Hazards bulletin in the United Kingdom; Arbeit und Ökologie (Work and the Environment) in Germany). The priorities for action promoted by these periodicals may initially reflect cultural differences from other organizations, but frequently become the priorities of trades unions and political parties; the advocacy of stiffer penalties for breaking health and safety law and for causing injury to, or the death of, workers are recurrent themes.
International Networks
The rapid globalization of the economy has been reflected in trade unions through the increasing importance of the international trade secretariats, area-based trade union affiliations like the Organization of African Trade Union Unity (OATUU), and meetings of workers employed in particular sectors. These new bodies frequently take up health and safety concerns, the African Charter on Occupational Health and Safety produced by OATUU being a good example. In the voluntary sector international links have been formalized by groups which concentrate on the activities of particular multinational companies (contrasting the safety practices and health and safety record of constituent businesses in different parts of the world, or the health and safety record in particular industries, such as cocoa production or tyre manufacture), and by networks across the major free trade areas: NAFTA, EU, MERCOSUR and East Asia. All these international networks call for the harmonization of standards of worker protection, the recognition of, and compensation for, occupational disease and injury, and worker participation in health and safety structures at work. Upward harmonization, to the best extant standard, is a consistent demand.
Many of these international networks have grown up in a different political culture from the organizations of the 1970s, and see direct links between the working environment and the environment outside the workplace. They call for higher standards of environmental protection and make alliances between workers in companies and those who are affected by the companies’ activities; consumers, indigenous people in the vicinity of mining operations, and other residents. The international outcry following the Bhopal disaster has been channelled through the Permanent People’s Tribunal on Industrial Hazards and Human Rights, which has made a series of demands for the regulation of the activities of international business.
The effectiveness of voluntary sector organizations can be assessed in different ways: in terms of their services to individuals and groups of workers, or in terms of their effectiveness in bringing about changes in working practice and the law. Policy making is an inclusive process, and policy proposals rarely originate from one individual or organization. However, the voluntary sector has been able to reiterate demands which were at first unthinkable until they have become acceptable.
Some recurrent demands of voluntary and community groups include:
- a code of ethics for multinational companies
- higher penalties for corporate manslaughter
- workers’ participation in occupational health services
- recognition of additional industrial diseases (e.g., for the purpose of compensation awards)
- bans on the use of pesticides, asbestos, artificial mineral fibres, epoxy resins and solvents.
The voluntary sector in occupational health and safety exists because of the high cost of providing a healthy working environment and appropriate services and compensation for the victims of poor working conditions. Even the most extensive systems of provision, like those in Scandinavia, leave gaps which the voluntary sector attempts to fill. The increasing pressure for deregulation of health and safety in the long-industrialized countries in response to competitive pressures from transitional economies has created a new campaign theme: the maintenance of high standards and upward harmonization of standards in different nations’ legislation.
While they can be seen as performing an essential role in the process of initiating legislation and regulation, they are necessarily impatient about the speed with which their demands are accepted. They will continue to grow in importance wherever workers find that state provisions fall short of what is needed.
Occupational Health as a Human Right
* This article is based on a presentation to the Columbia University Seminars on Labour and Employment, sponsored by the Center for the Study of Human Rights, Columbia University, February 13, 1995.
“The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being .... The achievement of any State in the promotion and protection of health is of value to all.” Preamble to the Constitution of the World Health Organization (WHO).
The concept of universality is a fundamental tenet of international law. This concept is exemplified by the issues raised in occupational safety and health because no work is immune from the dangers of occupational hazards. (Examples of the literature describing occupational safety and health hazards from different types of work include: Corn 1992; Corn 1985; Faden 1985; Feitshans 1993; Nightingale 1990; Rothstein 1984; Stellman and Daum 1973; Weeks, Levy and Wagner 1991.)
The universal threat to the fundamental human rights of life and security of person posed by unhealthy working conditions has been characterized in international human rights instruments and ILO standards. According to the Universal Declaration of Human Rights, proclaimed in 1948 (United Nations General Assembly 1994) Article 3, “Everyone has the right to life, liberty and security of person”. The Preamble to the ILO Constitution considers “the protection of the worker against sickness, disease and injury arising out of his employment” as a precondition to “Universal and lasting peace”. Therefore, improvement of the conditions of living and work is a fundamental component of the ILO’s view of universal rights.
As described in a recent exhibit at the UN Secretariat in New York, United Nations staff have been tortured, imprisoned, kidnapped and even killed by terrorists. United Nations Commission on Human Rights, (UNCHR) Resolution 1990/31 pays attention to these hazards, underscoring the need to implement existing mechanisms for compliance with international human rights to occupational safety and health. For these professionals, their role as a conduit for life-saving communication about other people, and their commitment to their employer’s principled work, placed them at equal if not greater risk to other workers, without the benefit of recognizing occupational safety and health concerns when formulating their own work agenda.
All workers share the right to safe and healthful working conditions, as articulated in international human rights instruments, regardless of whether they be confronted in fieldwork, in traditional offices or workplace settings, or as “telecommuters”. This view is reflected in international human rights instruments regarding occupational safety and health, codified in the United Nations Charter in 1945 (United Nations 1994) and the Universal Declaration of Human Rights, amplified in major international covenants on human rights (e.g., the International Covenant on Economic, Social and Cultural Rights 1966), described in major human rights treaties, such as the International Convention on the Elimination of All Discrimination Against Women passed in 1979, and embodied in the work of the ILO and the WHO as well as in regional agreements (see below).
Defining occupational health for the purposes of understanding the magnitude of the governmental and employers’ responsibility under international law is complex; the best statement is found in the Preamble of the Constitution of the WHO: “Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.” The term “well-being” is extremely important, because it is consistently used in human rights instruments and international agreements pertaining to health. Equally important is the construction of the definition itself: by its very terms, this definition reveals the consensus that health is a composite of the interaction of several complex factors: physical, mental and social well-being, all of these together being measured by an adequate standard of well-being that is greater than “merely the absence of disease or infirmity”. This term, by its very nature, is not tied to specific standards of health, but is amenable to interpretation and application in a flexible framework for compliance.
Thus, the legal foundation for implementing international human rights to occupational health protections in the workplace from the perspective of security of the person as a facet of protecting the human right to health constitutes an important corpus of international labour standards. The question therefore remains whether the right of individuals to occupational safety and health falls under the rubric of international human rights, and if so, which mechanisms can be deployed to assure adequate occupational safety and health. Further, developing new methods for resolving compliance issues will be the major task for ensuring the application of human rights protection in the next century.
Overview of International Rights to Protectionfor Occupational Safety and Health
Law of human rights reflected in the United NationsCharter
Protection of the right to health is among the fundamental constitutional principles of many nations. In addition, an international consensus exists regarding the importance of providing safe and healthful employment, which is reflected in many international human rights instruments, echoing legal concepts from many nations, including national or local legislation or constitutionally guaranteed health protections. Laws requiring inspections to prevent occupational accidents were passed in Belgium in 1810, France in 1841 and Germany in 1839 (followed by medical examination requirements in 1845).The issue of “entitlements” to health care and health protections was raised in the analysis of the potential for US ratification of the International Covenant on Economic, Social and Cultural Rights (e.g., Grad and Feitshans 1992). Broader questions regarding the human right to health protections have been addressed, although not fully resolved, in the United Nations Charter; in the Universal Declaration of Human Rights; in Articles 7 and 12 of the International Covenant on Economic and Social Rights; and in subsequent standards by the ILO and the WHO, and other UN-based international organizations.
Under the United Nations Charter the contracting parties state their aspiration to “promote” economic and social advancement and “better standards of life”, including the promotion of human rights protections, in Article 13. Using language that recalls the ILO’s Constitutional mandate under the Treaty of Versailles, Article 55 specifically notes the linkage between the “creation of conditions of stability and well-being” for peace and “higher standards of living” and “universal respect for, and observance of, human rights and fundamental freedoms”. The debate regarding the interpretation of these terms, and whether they encompassed all or only a fraction of recognized constitutional rights of UN Member States, was unduly politicized throughout the Cold War Era.
This handful of basic documents share one weakness, however—they offer vague descriptions of protections for life, security of the person and economically-based rights to employment without explicitly mentioning occupational safety and health. Each of these documents employs human rights rhetoric ensuring “adequate” health and related basic human rights to health, but it is difficult to patch together a consensus regarding the quality of care or “better standards of life” for implementing protections.
Occupational safety and health protections underthe Universal Declaration of Human Rights (UDHR)
Security of the person, as discussed in UDHR Article 3
Although there is no case-law interpreting this term, Article 3 of the UDHR ensures each person’s right to life. This includes occupational health hazards and the effects of occupational accidents and work-related diseases.
The cluster of employment rights in UDHR Articles 23, 24 and 25
There is a small but significant cluster of rights relating to employment and “favourable conditions of work” listed in the Universal Declaration of Human Rights. The principles articulated in three consecutive articles of the UDHR are an outgrowth of history, reflected in older laws. One problem exists from the standpoint of occupational health analysis: the UDHR is a very important, widely-accepted document but it does not specifically address the issues of occupational safety and health. Rather, references to issues surrounding security of person, quality of conditions of work and quality of life allow for an inference that occupational safety and health protections fall under UDHR’s rubric. For example, while the right to work in “favourable conditions of work” is not actually defined, occupational health and safety hazards certainly impact upon the achievement of such social values. Also, the UDHR requires that human rights protections at the worksite ensure the preservation of “human dignity”, which has implications not only for the quality of life, but for the implementation of programmes and strategies that prevent degrading working conditions. The UDHR therefore provides a vague but valuable blueprint for international human rights activity surrounding issues of occupational safety and health.
International Covenant on Economic, Social and Cultural Rights (ICESCR)
The meaning and enforcement of these rights are amplified by the principles enumerated in the International Covenant on Economic, Social and Cultural Rights (ICESCR), Part III, Article 6 and 7b, which assures all workers the right to “Safe and healthy working conditions”. Article 7 provides greater insight to the meaning of the right to just and favourable conditions of work. “Favourable conditions of work” includes wages and hours of work (ICESCR Article 7.1 (a) (i)) as well as “Safe and healthy working conditions” (Summers 1992). The use of this phrase within the context of favourable conditions of work therefore lends greater meaning to the UDHR’s protections and demonstrates the clear nexus between other human rights principles and protection of occupational safety and health, as further amplified in ICESCR Article 12.
Promotion of industrial hygiene under Article 12of the International Covenant on Economic, Socialand Cultural Rights
Of all the UN-based international human rights documents, ICESCR Article 12 most clearly and deliberately addresses health, referring to the explicit right to health protection through “industrial hygiene” and protection against “occupational disease”. Further, Article 12’s discussion regarding improved industrial hygiene is consistent with Article 7(b) of the ICESCR regarding safe and healthful working conditions. Yet, even this express guarantee of occupational safety and health protection does not offer detailed exposition of the meaning of these rights, nor does it list the possible approaches that could be applied for achieving the ICESCR’s goals. Consistent with the principles articulated in many other international human rights documents, Article 12 employs deliberate language that recalls the WHO’s Constitutional notions of health. Without question, Article 12 embraces the notion that health concerns and attention to individual well-being include occupational safety and health. Article 12 reads:
The States Parties to the present Covenant recognize the right of everyone to the enjoyment of the highest attainable standard of physical and mental health.... The steps to be taken by the States Parties to the present Covenant to achieve the full realization of this right shall include those necessary for: ...
(b)The improvement of all aspects of environmental and industrial hygiene;
(c)The prevention, treatment and control of epidemic, endemic, occupational and other diseases.
Significantly, Article 12 also pays direct attention to the impact of occupational disease on health, thereby accepting and giving validity to a sometimes-controversial area of occupational medicine as worthy of human rights protection. Under Article 12 the States Parties recognize the right to physical and mental health proclaimed indirectly in Article 25 of the UDHR, in the American Declaration, the European Social Charter, and the revised Organization of American States (OAS) Charter (see below). Additionally, in Paragraph 2, they commit themselves to a minimum of four “steps” to be taken to achieve the “full realization” of this right.
It should be noted that Article 12 does not define “health”, but follows the definition stated in the WHO Constitution. According to Grad and Feitshans (1992), Paragraph 1 of the Draft Covenant prepared under the auspices of the Commission on Human Rights, however, did define the term by applying the definition in the WHO Constitution: “a state of complete physical, mental and social well-being, and not merely the absence of disease or infirmity.” Like the ILO with respect to Articles 6-11 of the ICESCR, WHO provided technical help in drafting Article 12. The Third Committee did not accept WHO’s efforts to include a definition, arguing that such detail would be out of place in a legal text, that no other definitions were included in other articles of the Covenant, and that the proposed definition was incomplete.
The words “environmental and industrial hygiene” appear without the benefit of interpretive information in the text of the preparatory records. Citing other resolutions of the 1979 World Health Assembly, the report also expresses concern for “the uncontrolled introduction of some industrial and agricultural process(es) with physical, chemical, biological and psychosocial hazards” and notes that the Assembly further urged Member States “to develop and strengthen occupational health institutions and to provide measures for preventing hazards in work places” (Grad and Feitshans 1992). Repeating a theme expressed in many prior international human rights documents, “The right of everyone to the enjoyment of the highest attainable standard of physical and mental health” is a goal clearly shared by employers, workers and governments of many nations—a goal that unfortunately remains as elusive as it is universal.
International Convention on the Eliminationof All Forms of Discrimination Against Women
The International Convention on the Elimination of All Forms of Discrimination Against Women (1979), Part III, Article 11(a), states that “The right to work is an inalienable right of all human beings”, and Article 11(f) lays down “The right of protection of health and to safety in working conditions, including the safeguarding of the function of reproduction”.
Article 11.2(a) prohibits “sanctions, dismissal on the grounds of maternity leave”, a subject of profound contemporary and historical conflict and violation of international human rights, under many legal systems of UN Member States. For pregnant women and other people who work, these important issues remain unresolved in the jurisprudence of pregnancy. Thus, Article 11.2 is unquestionably geared to overturning generations of ingrained institutional discrimination under law, which was an outgrowth of mistaken values regarding women’s ability during pregnancy or while raising a family. Issues from the perspective of the jurisprudence of pregnancy include the dichotomy between protectionism and paternalism which has been played out in litigation throughout the twentieth century. (US Supreme Court cases in this area range from a concern for limiting the hours of women’s work because of their need to be home raising families, upheld in Muller v. the State of Oregon, 208 U.S. 412 (1908), to the decision banning forced sterilizations of women who are exposed to reproductive health hazards in the workplace among other things in UAW v. Johnson Controls, 499 U.S. 187 (1991) (Feitshans 1994). The imprint of this dichotomy on the conceptual matrix of this Convention is reflected in Article 11.2(d), but is not clearly resolved since “special protections”, which are often necessary to prevent the disproportionately dangerous effects of working conditions, are often inappropriately viewed as beneficial.
Under the terms of this Convention, Article 11.2(d) endeavours “To provide special protection to women during pregnancy in types of work proved to be harmful to them”. Many facets of this provision are unclear, such as: what is meant by special protection; are effects limited to maternal harm during pregnancy; and if not, what are the implications for foetal protection? It is unclear from this Convention, however, what the standard of proof is to make a “special protection” necessary or acceptable, and also what is the scope of an acceptable protective mechanism.
Article 11.3 limits the reach of “special protections”, by clearly stating that implementation of occupational safety and health protections must be based on scientific evidence, rather than social values. Article 11.3 states: “Protective legislation relating to matters covered in this article shall be reviewed periodically in the light of scientific and technological knowledge and shall be revised, repealed or extended as necessary.” Methods for oversight and appropriate risk assessment also need to be spelled out, in order to ensure that improper exclusionary policies, such as forced sterilizations to retain or obtain employment, will be viewed as constituting gross violations of international human rights, and therefore will not be given credence under this Convention. These thorny issues have been litigated and will raise increasingly perplexing questions regarding implementation and compliance with the Convention’s principles as occupational epidemiology uncovers more reproductive health hazards and the need for effective preventive measures.
Additionally, the Convention’s drafters followed the pattern set by the ILO, describing a detailed reporting mechanism for oversight and compliance, in the form of mandatory regular reporting before the Convention’s Human Rights Commission. Under the Commission’s procedures, set forth in Article 18, State Parties to the Convention undertake to “report on the legislative, judicial, administrative or other measures which they have adopted to give effect to [these] provisions” within one year and at least once every four years, and may indicate impediments to implementation. The requisite development of standards that are needed to determine the necessary preventive strategies for reproductive health hazards in the workplace, may be addressed through this mechanism for the exchange of vital compliance information.
Regional Treaties and DeclarationsRegarding Human Rights
American Convention on Human Rights
The American Convention’s Preamble refers to economic and social rights including, in Article 3, the right to life. Yet the Convention does not specifically address health or working conditions as fundamental rights protected in other treaties. Significantly for the implementation of international human rights, however, this treaty provides a structure for a human rights commission and court by establishing the Inter-American Commission on Human Rights. The Commission’s powers include the procedures for requests for information by the Commission against governments who are believed to have violated human rights. It does not directly address occupational safety and health questions confronting people who work in the Inter-American system.
The African [Banjul] Charter on Human and Peoples’ Rights
The African [Banjul] Charter on Human and Peoples’ Rights, adopted June 27, 1981, provides an innovative perspective on established concepts of international human rights, as articulated in human rights instruments. As discussed by Alston (1984) from a theoretical standpoint without making specific reference to the African [Banjul] Charter itself, this instrument clearly represented a groundbreaking attempt to expand the realm of international human rights protections and make such protections available in a flexible framework for all people. Within its broad scope, the African [Banjul] Charter includes rights to a clean environment, political rights, and rights to sustainable aspects of development. Interestingly, and in stark contrast to the European Social Charter, the African [Banjul] Charter does not address protection of working conditions or occupational safety and health. In a manner that parallels the UDHR’s protection, the African [Banjul] Charter Article 4 prohibits human rights violations against “his life and integrity of his person”. Also consistent with UDHR Article 3, the African [Banjul] Charter Article 6 assures the security of person.
Following some of the language from the WHO Constitution which has become seminal to international human rights to health, Article 16 requires Parties to protect the “right to enjoy the best attainable state of physical and mental health”. Signatory Parties endeavour to “take the necessary measures to protect the health of their people and to ensure that they receive medical attention when they are sick”.
As in the case of many other international human rights instruments, the African [Banjul] Charter establishes a mechanism for oversight and compliance, in the form of a Human Rights Commission. States may request the examination of human rights violations by other States, assuming that exhaustion of remedies requirements have been met. These procedures are discussed in detail in Articles 30 through 59.
European Social Charter
In the European Social Charter promulgated in 1965, Part I(2) clearly states, “All workers have the right to just conditions of work”, and Part I(3) states, “All workers have the right to safe and healthy working conditions”. These rights are further described in Part II, Article 3, which offers a detailed discussion of “The Right to Safe and Healthy Working Conditions”, with a view to ensuring the effective exercise of the right to safe and healthy working conditions. Unlike other international human rights instruments, however, the European Social Charter also hints at the prospect of creating mechanisms for enforcement and other issues raised by implementation and compliance with international human rights norms within the plain meaning of the document itself. Article 3.2 requires Contracting Parties “to provide for the enforcement of such regulations by measures of supervisions”, and in Article 3.3 “to consult, as appropriate, employers’ and workers’ organizations on measures intended to improve upon industrial safety and health”. This impressive provision is amplified in its intensity by reporting mechanisms in Part IV, Articles 21 and 22, which allow for international scrutiny of implementation activities at regular intervals.
In addition to its remarkably comprehensive approach to international human rights protections, especially concerning occupational safety and health, it is also worth noting that the European Social Charter clearly and decisively sets forth the groundwork for future activities towards implementation and compliance with its provisions. For example, the reference to regulation and supervision in Article 3 is consistent with international monitoring and enforcement by Contracting Parties as well as NGOs, both in the European system and in their home jurisdictions. The concept of consultation between employers and workers, articulated in Article 3.3, goes beyond mirroring the tripartite structure of the ILO, foreshadowing as well the increasing acceptance of joint labour-management safety committees to achieve internal compliance with international human rights in employment.
ILO standards
As indicated in the Preamble to the ILO Constitution, “the protection of the worker against sickness, disease and injury arising out of his employment” is a precondition to “Universal and lasting peace”. Therefore, improvement of the conditions of living and work is a fundamental component of ILO Conventions and Recommendations. Johnston (1970) wrote, “The underlying principle is that certain basic human requirements should be removed from the sphere of international competition to secure certain minimum standards of strength and human dignity”. Although the ILO lacks the “universal authority ...to exclude a non-complying employer ...from the legitimate labour market”, Friedman (1969) envisions a stronger role for the ILO: “The day can be foreseen when the ILO laws and directives will attain such force, and the stigma of non-compliance will mean exclusion from an international labour market.”
The ILO has also fostered the creation of consistent standards for those safety problems which cannot be covered by Convention provisions without broaching ILO jurisdiction over sovereign nations. For example, ILO Codes of Practice regarding safety protections have served as the blueprint for occupational safety laws and regulations in such areas as dock work, transfer of technology to developing nations, civil engineering and heavy industries. These model codes, which are sometimes applied with minor modification as draft legislation, share the values expressed in several ILO Conventions pertaining to occupational safety and health (e.g., the Protection Against Accidents (Dockers) Convention (Revised), 1932 (No. 32); the Safety Provisions (Building) Convention, 1937 (No. 62); the Medical Examination of Young Persons (Industry) Convention, 1946 (No. 77) and the Medical Examination of Young Persons (Non-Industrial Occupations) Convention, 1946 (No. 78); the Guarding of Machinery Convention, 1963 (No. 119); the Hygiene (Commerce and Offices) Convention, 1964 (No. 120); the Occupational Safety and Health (Dock Work) Convention, 1979 (No. 152); and the Occupational Safety and Health Convention, 1981 (No. 155). The latter is considered in more detail below).
ILO Convention 155: Convention Concerning OccupationalSafety and Health and the Working Environment, 1981,and its antecedents
Since its inception, the ILO has encouraged promotion of better working conditions. Early efforts focused upon accidents in particular, and legal remedies for workers’ compensation. This is evinced in the ILO’s early Conventions, such as: Convention 32, the Protection Against Accidents (Dockers) Convention (Revised), 1932; Convention 62, the Safety Provisions (Building) Convention, 1937 and in Conventions concerning medical examinations for workers and machine guards. By setting forth specific requirements for accident prevention, these Conventions served as a precedent for performance standards found in occupational safety regulations in many nations today. These Conventions reflect the constant theme that protection against occupational accidents is a right shared by all workers.
Consistent also with this heritage, Convention 155, Article 3(e) offers the definition of health, “in relation to work, indicates not merely the absence of disease or infirmity; it also includes the physical and mental elements affecting health which are directly related to safety and hygiene at work.” This definition is deceptively simple and comprehensive at the same time: it bespeaks the complex interaction between dangerous workplace exposures; individual lifestyle and environmental factors that impact upon the effects of working conditions (Mausner and Kramer 1985). In addition, this approach is multidimensional, because its concern for both physical and mental elements of health and well-being implicitly takes into account the effects of occupational stress and other mental problems.
But the heart of Convention 155 concerns the creation of effective national, regional and workplace mechanisms for implementation and compliance with other ILO standards. As adopted by the 67th Session of the International Labour Conference in 1981, Convention 155 fosters the creation, implementation and periodic evaluation of occupational safety and health standards among Member States of the ILO. For example, Article 4.1 states Convention 155’s goal of fostering the development of a “coherent national policy” concerning occupational safety and health protections. To this end, Convention 155 obligates ratifying Member States to promote research, statistical monitoring of hazardous exposures (such as medical surveillance measures, not unlike technical standards in Member States) and worker education and training. Convention 155 uses broad terminology to provide a regulatory framework. Consultation with representative organizations and employers is required before exemptions will be granted, and any exclusions of categories of workers requires reporting on efforts to achieve “any progress towards wider application” pursuant to Article 2.3. Convention 155 also fosters education for “representative organizations” and worker participation in the development and enforcement of occupational safety and health regulations internally and on regional, national and international levels.
ILO Conventions instituting workers’ compensation
The ILO is responsible for the successful drafting and adoption of several ILO Conventions pertaining to workers’ compensation (ILO 1996a.)
These include the Workmen’s Compensation (Agriculture) Convention, 1921 (No. 12); the Workmen’s Compensation (Accidents) Convention, 1925 (No. 17); the Workmen’s Compensation (Occupational Diseases) Convention, 1925 (No. 18); the Sickness Insurance (Industry) Convention, 1927 (No. 24); the Sickness Insurance (Agriculture) Convention, 1927 (No. 25); the Medical Care and Sickness Benefits Convention, 1969 (No. 130). Generally speaking, workers’ compensation statutes are common among ILO Member States. Such statutes represent an economically-based (rather than human rights-oriented) compromise: providing care and assistance to injured workers and replacing the uncertainties of litigation with a scheduled system of payment that does not examine the issue of fault and places a monetary limit on the recovery afforded to people who have been injured by occupational accidents or occupational disease. (One example in the United States is found in the Virginia Workmens’ Compensation Act Annotated (1982): voluntary acts that are related to requirements of the employment contract are entitled to compensation.) Delay, underreporting, low payments and legal disputes when obtaining coverage for medical care under these separate systems are common. Despite such practical limits upon their effectiveness, the “universality” of these protections in the United States and under international law indicates a societal will to provide monetary disincentives for dangerous work practices, and financial support for injured workers.
Due process and reporting mechanisms within the ILO
Alston views the ILO as an international model for procedural requirements, which, in his opinion, “legitimize the declaration of new norms” (1984). Such features of ILO procedures include: preparation of a preliminary survey of relevant laws among Member States, followed by its Governing Body’s decision whether to place the item on the agenda of the annual International Labour Conference (ILC), followed by a questionnaire from the ILO Secretariat to participating Member States. After the draft has been referred to a technical committee, a draft instrument is circulated to Member States and the appropriate worker and employer representatives; a revised draft instrument is then prepared and submitted to the technical committee, discussed by plenary and drafting committee, and adopted after voting by the ILC. This approach allows for maximum discussion and communication between regulated entities and their governing parties. For a detailed examination of ILO reporting mechanisms see “International Labour Organization” later in this chapter.
These procedures, initiated in 1926 at the inception of the Committee of Experts on the Application of Conventions and Recommendations, have continued vibrancy in the international system. For example, the ILO’s model forms the blueprint in the contemporary Convention on the Elimination of All Forms of Discrimination Against Women: Article 18 sets forth a mandatory reporting mechanism before an international Committee also described within the provisions of the Convention. Mandatory reports regarding activities towards implementation and compliance should be heard by the Committee at the end of the first year following ratification, then at least every four years. Additional reporting procedures for monitoring the application of ILO standards and Conventions include but are not limited to: direct contact missions (for an excellent description of the ILO’s mediation and conciliation role on “direct contact” missions, see Samson 1984); Commissions of Inquiry to investigate particular cases of egregious violations of ILO Conventions and Constitutional provisions; and regularly scheduled periodic oversight through reporting to Conference meetings and reporting to the Governing Body and the Administrative Tribunal. Reporting mechanisms are slow but invaluable; these constitute an important component of a much larger process of mobilizing world opinion towards positive change regarding labour issues.
Ruda (1994) notes that ILO Conventions 87 (Freedom of Association and Protection of the Right to Organize, 1948) and 98 (Right to Organize and Collective Bargaining, 1949) were written into the Gdansk agreements between the Polish government and the union Solidarity. “Neither the Committee of Experts nor the Conference’s Committee on the Application of Standards may impose sanctions of any kind, though their conclusions are sometimes regarded as political or moral sanctions.” This has been a constant frustration throughout the history of the Committee, even though its ability to influence certain governments under the appropriate circumstances is a point of pride.
World Health Organization
WHO’s Alma-Ata Declaration on Primary Care
In the so-called Alma-Ata Declaration (World Health Organization 1978), coming out of the International Conference on Primary Health Care, held by WHO/UNICEF in Alma-Ata, USSR, from 6 to 12 September 1978. WHO launched an international campaign widely known as “Health For All 2000” which reflects a concerted international effort to improve the quality of health and the rendering of health services, especially primary care but also including occupational safety and health, throughout the world. Even though occupational safety and health does not appear within the plain language of the Declaration it has been included in strategic programming, such that realization of basic health protections has also been fostered by disseminating information and developing programme strategies with the goal of achieving “Health for All 2000” under the auspices of the Declaration.
Consistent with the letter and the spirit of the WHO Constitution discussed above, the Alma-Ata Declaration calls for “urgent action by all governments, all health and development workers, and the world community to protect and promote the health of all people of the world”. Notably, Article 1 clearly reaffirms that “health ...is a fundamental human right and that the attainment of the highest possible level of health is a most important worldwide social goal. ...” Article 3 says, “The promotion and protection of the health of the people is essential to sustained economic development and contributes to a better quality of life and to world peace.” In addition, the conference laid the groundwork for concrete programmatic strategies, to achieve these goals. Implications for occupational safety and health derived from the Alma-Ata implementation include the development of occupational health facilities as a part of both regional and international strategies. The Pan-American Health Organization (PAHO) provides one example of regional activities that follow WHO’s Plan of Action, “Health for All 2000: Strategies” (Pan-American Health Organization 1990) where occupational safety and health concerns are included in the development of training institutes and the development of health programmes.
WHO’s Beijing Declaration on Occupational Health For All, 1994
In October, 1994, the Second Meeting of the WHO Collaborating Centres in Occupational Health convened and signed the Declaration on Occupational Health For All. The Beijing Declaration is clearly rooted in the heritage of the WHO Alma-Ata Declaration on Primary Care, as well as many ILO instruments pertaining to occupational safety and health. Noting that 100 million workers are injured and 200,000 die each year in occupational accidents, and that 68 to 157 million new cases of occupational disease are attributed to hazardous exposures or workloads, the Beijing Declaration calls for “new strategies and programmes for occupational health throughout the world” and further asserts that occupational health programmes “are not a burden but have a positive and productive impact on the company and the national economy”, therefore linked to notions of sustainable development. The Declaration also calls for the development of infrastructure, including occupational health services with medical surveillance and health promotion, as well as for stronger linkage between occupational health programmes, other health activities, and the programmes and activities sponsored by the WHO.
ILO/WHO Joint Safety and Health Committee
WHO cooperates with the ILO under the auspices of the Joint ILO/WHO Committee on Occupational Health founded in 1946. One early project was the International Anti-Venereal Disease Commission of the Rhine, and in the 1950s, requests from Egypt and Iran were met by ILO and WHO expert consultants who provided technical assistance for comprehensive occupational health surveys.
The Committee has defined occupational safety and health as follows: “the promotion and maintenance of the highest degree of physical, mental and social well-being of all workers in all occupations; the prevention among workers of departures from health caused by their working conditions; the protection of workers in their employment from risks resulting from factors adverse to health; the placing and maintenance of the worker in an occupational environment adapted to his physiological and psychological equipment and, to summarize, the adaptation of work to man and of each man to his job”.
Summary of Law and Theory Regarding Human Rights to Health Protection in the Workplace
Since there are no expressly articulated mechanisms for enforcing occupational safety and health rights, it could be argued that there is no established jurisprudence of the right to protection for human life or health in the workplace except through unusual interpretations of leading human rights instruments, which are strained at best. For example, Article 3 of the United Nations’ UDHR expressly mentions the need to protect the right to life, liberty and security of the person without making reference to the environmental or workplace context in which such protections can or should prevail. Additionally, the absence of criminal sanctions or penalties for human rights violations in general (other than gross violations of human rights, such as slavery, genocide, war crimes, apartheid) or any standard requiring international penalties for violations of personal security caused by occupational safety and health hazards, calls for the exploration of alternatives to traditional law enforcement if occupational safety and health protections are to be realized.
As described above, many international human rights instruments express the concept that occupational safety and health is a fundamental human right, especially insofar as individual human rights to life, well-being and security of the person are concerned. The assurance of these rights is also codified in a cluster of international instruments that do not traditionally fall within the rubric of human rights. Taken together, one can conclude that the human right to healthy workplaces is therefore an accepted norm of international law. At the same time, however, domestic laws of Member States share the same dilemma as is found in the international system: fragile protections of overall working conditions in general, and protections of workplace health in particular, raise complex issues that arise from the tension between prevention strategies, which target broad segments of a given population to reduce the spread of disease or the effects of specific dangers on the one hand, balanced against the popular sentiment that resists the temporary abrogation of certain individual rights to travel, engage in certain activities, or engage in commerce in order to protect the individual right to occupational health protections. It therefore remains unclear to what extent that cluster of rights to occupational safety and health may be enforceable on an international or state-by-state basis to provide practical amelioration of working conditions experienced by individuals. Can the promise of protection for these human rights be met within the context of new workplaces and the codified rules of the international system?
Codification of the jurisprudential notion of occupational safety and health protections therefore is found within the rubric of human rights. Monitoring and implementing these articulated protections, therefore, constitutes the first phase of the next century’s human rights concerns. Mindful of these questions, new approaches that can be employed to solve these problems are discussed below.
Overview of Implementation and ComplianceIssues in the International System
Ever since the UN Charter was adopted, sceptics have questioned the viability of enforcing international public law, especially in areas concerning the prevention of gross violations of human rights. Preventing such harms under the international system is at least a two-part process, requiring (1) codification of principles, followed by (2) meaningful steps towards implementation and compliance. Typically, such theories assume a context of an organized society with traditional types of legal institutions and enforcement procedures to provide punishment, and deterrence for “bad actors” who refuse to comply with the system’s articulated goals and shared values. Achieving implementation and compliance for human rights in general, and for healthy workplaces in particular, is problematic and complex. Fifty years after the UN Charter was written, there exists a viable international system that works with some level of efficiency to codify norms into written standards; the development of compliance mechanisms for implementation, however, remains uncharted. Therefore the emerging vital questions must be explored: What are the alternative models which do not rely on coercion for enforcement in order to implement the maximum occupational safety and health protection? How can new, extra-legal incentives to compliance with international human rights protections for occupational safety and health be created?
Inherent limits upon the effectiveness of the international system impede the implementation of any set of principles or norms for occupational safety and health protection, so long as the international system remains without some underlying enforcement or positive incentive for compliance. The application of quantifiable measures is not the case in international occupational safety and health practice, however, using ILO Convention 162 Concerning Safety in the Use of Asbestos, 1986 as an example. Under Convention 162, Article 11.1 specifically bans the use of crocidolite. But Article 11.2 reverses this approach; there is no formalized enforcement mechanism for inspection leading to abatement of hazards or for imposing penalties, beyond the limited oversight provided by institutions for reporting. In addition, the actual standard for exposure limits to asbestos is not articulated in Convention 162. Instead, Convention 162 leaves the appropriate standards to the competent authority in a given nation. Consequently, the very nature of reporting without enforcement or positive incentives for compliance by nations or employer-entities generates practical constraints on the implementation of human rights principles and laws (Henkin 1990). As Henkin notes, “International law is constantly apologizing for itself...to justify its very existence” because it has no government and no institutions of governance.
Even though the international system has a recognized ability to limit aggression between states, as evinced by diplomatic relations and other areas of compliance, there are few instances where the international system can enforce sanctions or penalties against so-called bad actors, as are commonly enforced under domestic laws. For this reason, the sound of frustrated pleas for the implementation of international human rights protections have echoed through the corridors of the United Nations and at international conferences involving NGOs. Without a schedule of enforcement —sanctions or fines or penalties—to generate punishment and deterrence, there is an immediate need to develop effective mechanisms for implementation and compliance with international human rights protections of occupational safety and health. Such approaches to “interactive” compliance are therefore ideally suited to fill this void, when this approach is taken in tandem with practical strategies for applying such positive incentives to improve working conditions throughout the international system (Feitshans 1993). Therefore, there is a clear demand for compliance mechanisms that will take the weak and undervalued reporting system to, in the words of K.T. Samson (former Chief, Application of Standards Branch of the International Labour Office), “a dimension beyond dialogue”.
Now that the international system has outgrown the need for codification of universal human rights norms as the primary focus for international activity, many have suggested that the time has come to turn international attention towards implementation and compliance with those norms. Leading commentary (Sigler and Murphy 1988), for example, has an unclearly articulated but important working assumption that competition between entities—be they employer corporations or UN Member States—can be used as a tool to achieve effective occupational safety and health protections, if that competition is fuelled by positive incentives instead of the traditional punishment and deterrence model. “We are moving more toward getting organizations to control and police themselves,” says Joseph Murphy, a lawyer and co-editor of Corporate Conduct Quarterly, a newsletter on compliance and ethics.
Conclusions
The first half-century of UN activity brought codification of international human rights norms regarding the right to a healthy workplace in several key international human rights instruments. These international instruments have implicitly limited effectiveness, however, because other than administrative monitoring, they lack enforcement and deterrence mechanisms to ensure their implementation. There has been marked frustration with these limitations upon the effectiveness of the international system, despite an impressive accumulation of international documents and reports before many UN organs, because these efforts offer little oversight or monitoring beyond reporting. The treaties and conventions discussed in this paper enforcing or protecting health rights, share in this frustration, despite important strides that have been achieved through diligent use of reporting mechanisms.
The important concepts found in international human rights instruments are based upon the philosophy that work-related illnesses are an avoidable aspect of industrialization and also reflect a poorly articulated international consensus that people should not be killed or seriously injured for their work. Designed to protect the human right to safety in the workplace, such instruments and their underlying principles are not standards for perfection. These instruments express international human rights to occupational safety and health but should not, therefore, be viewed as the maximum level to ensure an improved quality of life for people who work; nor should they be viewed as the maximum achievable level from the perspective of improvements that can be fostered through competition for positive incentives. Rather, these standards are intended to serve as “minimum” levels of international human rights protection in the workplace, ameliorating the quality of life for all people who work.
Civil and Criminal Liability in Relation to Occupational Safety and Health
Felice Morgenstern*
* This article is adapted from Deterrence and Compensation by Felice Morgenstern (ILO 1982).
Duties in Respect of Safety and Health
Liability and responsibility in law have two aspects: one is the duty to do, or not to do, something; the other is the obligation to answer for what has been done, or not done. Any examination of the manner in which different categories of person may be made answerable at the national level for causes of occupational accidents or diseases should be preceded by a summary of the duties laid upon them with a view to the prevention of such accidents and diseases. These duties are often expressly laid down in international standards, or national laws or regulations but may also be defined by case-law. Questions have been raised as to the appropriateness of determining, in (civil) legal proceedings subsequent to injury, what the conduct of those concerned should have been beforehand. But it is also clear that some of the decisions in question, and the publicity surrounding them, have acted as a spur in the field of prevention.
Public bodies
Public bodies (whether government departments, special safety and health executives or other, autonomous bodies) play a large part in setting the framework within which liability and responsibility arise, by formulating rules, both general and particular, regarding the duties of various categories of persons, as well as by participating in their enforcement.
General rules regarding occupational safety and health, and rules regarding safety and health in particular industries or in respect of particular hazards, may be laid down by such means as laws or regulations, codes of practice and technical standards approved by public bodies. A number of international labour Conventions require this to be done as regards the entire subject-matter of the Convention; others call for specific prohibitions, criteria or exposure limits to be established. National legislation, whether in the form of labour codes or specific laws on occupational safety and health, often further provides for detailed standards or regulations to be laid down by public bodies in mandatory form or approved as guidelines; normally, the bodies concerned enjoy considerable discretion regarding the areas in which rules are to be established and their content. In the context of this article, it may be of importance for such rules to specify the persons or bodies on whom the obligation to ensure compliance with their terms rests. A number of international labour Conventions call for this to be done; for instance, the ILO Occupational Cancer Convention, 1974 (No. 139).
Failure to observe provisions of non-mandatory rules such as codes of practice does not in itself provide a ground for civil or criminal proceedings. At the same time, such failure may be taken into account in proceedings regarding non-compliance with a more general, mandatory requirement, as showing that not all necessary care for its fulfilment has been taken.
The absence of general rules, or the failure of such rules to reflect up-to-date knowledge, does not necessarily release employers, manufacturers and others concerned from all liability and responsibility: some courts have taken the view that employers cannot shelter behind the inaction of public bodies. Thus, in 1971, the English High Court of Justice found, in a claim for damages for a severe form of decompression sickness (bone necrosis), that at the time when the injury occurred it was common knowledge among those concerned with compressed air tunnelling that the statutory decompression table was inadequate; the court held that it was the employer’s duty to keep his own knowledge up to date (Ransom v. Sir Robert McAlpine and Sons Ltd. 1971). In some countries the labour inspectorate appears to be expressly empowered to serve notice on employers to remedy dangerous conditions in respect of which no mandatory standards exist.
Manufacturers, suppliers and so on
Most countries have passed legislation or guidelines regarding the duties of manufacturers, suppliers and so on, in respect of occupational safety and health. Generally these relate to machinery and equipment, on the one hand, and dangerous substances on the other. Safety and health requirements regarding machinery and equipment, prior to their use at the workplace, may be said to be threefold: they must be as safe in design and construction as practicable; they must be tested to ensure that they are indeed safe; and they must be made available on the market (through sale, hire, import or export) only when known to be safe. The primary obligation in this matter may lie with the vendor, the manufacturer or on all those concerned.
While general requirements regarding substances for use in work may be analogous to those regarding machinery, it is often a great deal more difficult to determine the effects of a particular substance on health. Consequently, while some national laws treat obligations regarding substances in the same way as those regarding machinery, others are also directly responsive to this difficulty. For example, the French Labour Code as amended in 1976 requires that, before any substance that may involve a danger to workers is marketed, “any person manufacturing, importing or selling it” shall provide approved institutions with the information necessary to the assessment of risks (section L. 231-7); any such person may further be required to assist in evaluating the risk. In many countries, duties in this matter also include factors such as the labelling of hazardous substances and information on safe handling procedures. These duties may not necessarily be confined to the period when the product was first marketed: in the United Kingdom, for example, there may be an obligation to do whatever might be reasonable in the circumstances to keep up to date with current knowledge and to act with whatever promptness fairly reflects the nature of that information. The action to be taken would depend on the gravity of likely consequences of the risk, as well as the gravity of the consequences arising from withdrawal of the product (Wright v. Dunlop Rubber Co. and another 1971). It should also be noted that there is increasing international interest and activity concerning the harmonization of labels for hazardous substances. For example, ILO Conventions 170 and 174 contain export notification requirements.
Enforcement of Duties in Respect of Safetyand Health
There are two ways of being made liable for failure to comply with a duty: one is to be called to account for the failure itself, irrespective of whether it has had any consequences. The other is to be made answerable for the consequences of that failure.
Public bodies
It is very difficult in most countries to enforce by legal action obligations of public bodies to exercise their regulatory power, such as the obligation deriving from certain labour Conventions and much national legislation to establish regulations on occupational safety and health. Some common law countries know procedures such as the order of mandamus, which can be claimed by a directly interested person to compel public officers to perform duties imposed upon them by common law or by statute (there is, however, little evidence that such procedures are currently used in the present context). In any case, their use is made more difficult where, as often, the legislation in question leaves public bodies a large discretion as to the areas, means and timing of action. The main methods for obtaining action by public authorities are extra-legal. For example, pressure may be brought to bear by unions, consumer groups or other forms of public opinion (these methods do not constitute enforcement in any proper sense of the term).
More widely, measures taken by public authorities can be set aside on the ground that they do not comply with the law, go beyond the powers conferred by the law (ultra vires) or, more generally, are inappropriate or unreasonable. This is not strictly enforcement of an obligation, but rather definition of its limits.
Manufacturers and suppliers
Where legislation in the area of occupational safety and health places express obligations on manufacturers and suppliers, it tends also to lay down penalties for failure to observe those obligations (e.g., France, United Kingdom, Denmark, Sweden). In some countries the penalty for infringement can be only a fine; this would appear to be the situation in the United Kingdom except where a prohibition notice has not been complied with. In some countries repeated infringements may involve liability to imprisonment, as in France and Venezuela. In yet other countries, the basic sanctions can be either fine or imprisonment; this is the case under Section 1, Chapter 8, of the Swedish Working Environment Act, 1978.
Preventing the distribution of machinery and substances not meeting safety and health requirements must be one of the main aims of enforcement in relation to manufacturers and suppliers. A number of legislative provisions directly reflect that concern (e.g., the French Labour Code provides for possible emergency procedures to suspend the marketing of dangerous substances or the use of unsafe machinery; it also provides for the possible cancellation of sales or leases under which unsafe equipment was provided).
Employers
All recent international labour Conventions in the field of occupational safety and health provide for the supervision of their implementation by appropriate inspection services. For an in-depth discussion on labour inspectorates, see “Labour inspection” in this chapter. Of particular relevance here, however, is the question whether labour inspectors may directly initiate prosecutions, whether they have to go through hierarchical superiors or whether they have to submit their recommendations to other authorities such as public prosecutors. Various statistics show that the number of prosecutions, in relation to the number of violations of safety provisions found, is very low.
Workers
Where an employer may delegate responsibility for occupational safety and health matters, or where relevant legislation places obligations directly on technical or supervisory staff, the duties of the persons concerned are usually enforced in a manner analogous to the enforcement of those of the employer. Some legislation expressly makes it clear that orders and prohibitions issued by the labour inspectorate may be addressed to such persons (e.g., Sweden and the United Kingdom). Similarly, the persons concerned are often expressly covered by the same penalty provisions of the relevant legislation as employers. Moreover, measures may be taken in relation to them which are not possible in relation to an employer.
Differing disciplinary powers exist in a number of jurisdictions in relation to the obligations regarding safety and health of workers. The range of disciplinary penalties for minor offences goes from verbal warning to withholding of one day’s wages; for serious offences, from public reprimand through transfer and suspension for a few days to debarment from promotion for up to one year; and for very serious offences, from the withholding of seven to 15 days’ wages through suspension for up to two months, and debarment from promotion for two years to dismissal.
Penal liability may also exist for violation of the duties of workers in respect of occupational safety and health. In some cases such liability is expressly limited to serious offences (e.g., Spain); in others, such liability is limited to specific duties. For instance, under Section L. 263-2 of the French Labour Code as amended in 1976, the ordinary worker appears to be penally liable only for the introduction or distribution of alcoholic beverages in the place of work. Elsewhere, the liability is more general (e.g., the United Kingdom, Denmark and Sweden) but the possible fine may nevertheless be limited (e.g., in Mexico to not more than one week’s wages). At the same time, there are countries in which there is no penal liability as an enforcement measure for a duty of workers who exercise no supervisory responsibility. This would appear to be the case, for example, under the labour codes of certain countries of Eastern Europe. Similarly, in the United States, under the Occupational Safety and Health Act, 1970, only the employer is liable to the civil penalties laid down for nonobservance of safety and health provisions.
Consequences of Occupational Accidents or Diseases
Social security
One of the main concerns, following an occupational accident or illness, is to ensure the continued livelihood of the victim and the victim’s family. The main means to that end is workers’ compensation. An examination of employment injury benefit schemes in general falls outside the scope of this chapter, but some aspects of the subject are relevant.
First, in quite a number of countries employment injury benefit is provided under schemes based on the principle of the individual employer’s liability. In some countries this liability is compulsorily insured, while in many others it is up to the employer to decide whether to insure or not, and he or she may remain jointly and severally liable with the insurer even if the employer does insure. In addition, there are a number of countries in which national social insurance schemes do not yet cover all workers and the remainder are protected under a scheme of employer’s liability. Individual employer’s liability is based on risk, not fault: in other words, the employer is required to meet the consequences of an accident or disease causally related to employment, within defined limits and on prescribed conditions. There may be provision for additional benefit in case of “serious fault” of the employer.
Secondly, account may be taken, in the financing of employment injury insurance, of the employment injury record of particular industries or of individual employers. (As a general principle of financing, this applies only where employment injuries are covered as a distinct branch of social security and, even in such cases, not universally.) Collective or individual rating as applied in many countries is designed to establish a contribution rate corresponding to likely expenditure, but there are also systems of individual rating that are designed to meet actual cost during the observation period (France, United States), or under which a collective rate is increased or decreased for individual undertakings in the light of expenditure on accidents in their employment or the effectiveness of preventive measures (Canada, Germany, Italy, Japan). Whatever the general principle of financing applied, there may be penalties added to the contribution rate of an employer who fails to carry out prescribed preventive measures, and many countries make special provision, under the social security scheme and, again, whatever the general principle of financing, for financial penalties where accidents occur owing to the serious misconduct or gross negligence of the employer; in some countries, the employer is liable in such a case for the reimbursement of the entire expenditure incurred by the insurance institution. There are divergences of view regarding the value of recourse to one or another of the various schemes. All of them, though in different ways, require an administrative infrastructure which makes them difficult to apply in developing countries and costly anywhere. In addition, individual rating based on recorded experience is difficult to apply to small undertakings.
Thirdly, in a number of countries social security institutions play an active role in the promotion of occupational safety and health. In some countries that role includes not only the setting of safety standards but also their enforcement, including the imposition of penalties. This has been the case, in particular, in Canada, Chile, France, Germany and Luxembourg.
Finally, the possibilities open to a worker or to his or her survivors to bring into play the civil liability of the employer or of fellow-employees are often limited by reference to the existence of social security. Three main approaches may be distinguished.
First, in some countries with employment injury schemes based on the principle of the individual employer’s liability, there is an option: the worker can claim the benefit of the statutory no-fault workers’ compensation legislation or he or she can sue under the general rules of tort, in principle on the ground of fault. The choice cannot be altered once made to the extent of lodging a claim or instituting proceedings. Accordingly, a worker who opts for the potentially higher benefits of the civil action also runs the risk of obtaining no benefit at all if the action does not succeed.
A second solution—applied in many Western European countries, in French-speaking Africa, in Canada, in Mexico, and in Pakistan—is that of giving the employer and fellow employees immunity from civil action in respect of normal cases covered by the employment injury scheme. Civil action remains possible—perhaps in theory rather than in practice—where the employer or a fellow employee can be shown to have acted with intent. In some countries it also remains possible where there has been penal sanction (Italy), gross negligence (Norway) or serious fault (Switzerland), while elsewhere the “inexcusable” or other serious fault of the employer leads to an increase of social security benefits at the employer’s expense (France, Spain, Mexico, many French-speaking African countries). The concepts of serious or inexcusable fault have been defined by case-law or legislation in the countries concerned; the gravity of the fault tends to be either in the degree of disregard for the likely consequences of an act or omission, or in the failure to deal with dangers which have been drawn expressly to the employer’s attention, as a result of previous accidents or otherwise. In some of the countries following this approach, civil action also remains possible to cover elements of compensation, such as damages for pain and suffering, which are not covered by the statutory scheme (Austria, Belgium, Switzerland).
The third approach is to allow unlimited recourse to civil liability actions, with a view to supplementing the employment injury benefit received under social security. That recourse applies in some countries—Greece, Japan, Sweden, and the United Kingdom—to liability both for fault and, in so far as it exists, to liability without fault; in others it applies only to liability for fault (Chile, Columbia, Peru). The approach is also followed in the Netherlands and some of the countries of Eastern Europe, where occupational accidents and diseases are not treated as a distinct branch of social security.
It should be added that, while social security schemes regarding employment injuries tend to cover all employment-related accidents, they are often far from covering all employment-related diseases. Causality may be more difficult to establish in cases of occupational disease, and the question of responsibility may be further complicated where a disease takes a long period of time to manifest itself and may not appear until some time after employment has ceased. As regards diseases not covered—for instance, because the scheme has an exhaustive list of compensable diseases—the ordinary rules of civil liability apply.
Civil liability
The possibility of recourse to civil action in respect of the consequences of occupational accidents and diseases is far from general. Where action against the employer and fellow employees is excluded or severely limited, it remains open against the manufacturer or supplier, but only in respect of the consequences of shortcomings in machinery, equipment or substances. Moreover, in some of the countries in which civil action is freely available both the number of claims made and the proportion of them which go to the courts are relatively small (this is true of both accident/illness and discrimination cases).
There are a number of bases on which a civil action can be brought. It may be based on the breach of a contractual obligation (under a contract of employment, a contract for services, or, conceivably, a supply contract). It is more likely to be brought in tort, on the ground of a civil wrong or breach of a duty established by law. Such actions may in turn relate to a breach of a duty at common law, under the general terms of a civil code or under a labour code, or they may relate to a breach of specific statutory obligations in the field of safety and health. Finally, a tort action may be available for fault or on the basis of “strict” or “objective” liability—that is, for risk without fault.
The plaintiff
Where a civil action is not excluded by the system of workers’ compensation, that action is available to those injured by the consequences of a breach of duty, whether by fault or by the creation of a risk. First and foremost, the action is available to the worker who suffered an employment injury due to such a breach. It is generally also available, in case of death of the worker, to his or her survivors, although these may be variously defined as persons actually dependent on the worker, or persons whose maintenance the worker was required by law to ensure. There have been some decisions recognizing that in certain circumstances trade unions may have an interest in bringing an independent civil action (for example, this has occurred in France and Italy). Elsewhere there is no evidence of a systematic attempt by unions to bring civil actions to defend their own interests in the matter; the more usual situation is that of unions supporting, financially or otherwise, the claims of those directly concerned. Proceedings under social security legislation for increases in benefit on the ground of inexcusable fault of the employer may, in some countries, be initiated by the competent social security institution as well as by those directly concerned. Moreover, social security institutions which have paid benefits may be able to sue to recover these from a person civilly liable for an employment injury.
The defendant
A civil action may lie against a wide range of persons or bodies with duties in the field of safety and health. In practice, where such action is not precluded by social security legislation, the great majority of civil claims are made against the employer. Nearly everywhere, the employer is also liable to make good injuries caused by the wrongful acts or omissions of his or her employees, whatever the level of their responsibilities, in the exercise of their duties, although the basis for that liability differs. Common law countries have the concept of “vicarious liability”; some civil law countries base liability on the fact that the employer is the commetant (the one having engaged in the act). Both of these have undertones of agency and the practical effects are analogous. Elsewhere, the liability of the employer is derived from his or her own fault in the choice of employees or their supervision. Usually, the liability of the employer does not prevent simultaneous or parallel action against the worker who caused the damage. In any case, the injured party usually prefers to sue the employer.
The extent to which the employer is liable to make good injuries caused by the wrongful acts or omissions of persons other than his or her employees is a more difficult question. In some jurisdictions, there is legislation or case-law the effect of which is to make an undertaking responsible in certain circumstances for compliance with duties in respect of safety and health of workplaces under its control, even if the risks at issue have been created by third parties such as sub-contractors, or with duties in respect of employees working outside the employing undertaking even where another undertaking has control of the workplace. Except to the extent that statutory provisions go further, liability in such a case appears to be based on the notion that the employer is at fault in that he or she is not ensuring the execution of duties laid upon him or her and of which one cannot rid oneself by contractual or other relations with third parties; if he or she has done all that a reasonable employer could have done, there is no liability.
There is also the question of recourse actions. More than one person may be concurrently responsible for the situation which led to an employment injury: manufacturer and employer, employer and contractor, and so forth. Or the employer may have been made liable for the acts of others. Where the worker chooses or is compelled to seek a remedy against only one of several joint “tortfeasors” or against the employer rather than against those for whose acts the employer is liable, the person sued is normally able to claim a contribution from the others responsible.
Burden of proof and causation
The burden of proof in a civil action rests with the plaintiff: it is up to the plaintiff to demonstrate the grounds for that action. The plaintiff has to show, first, that he or she has the correct defendant. This should not normally create any difficulty in relation to an action against the employer. On the other hand, there may be a real difficulty—particularly in cases of disease with slow manifestation—in showing who was the manufacturer or supplier of the machinery or substances alleged to be unsafe. It appears that in certain matters related to workplace injuries, such as the manufacture of asbestos, suits are now brought jointly against all major manufacturers if responsibility cannot initially be pinned on one company.
Secondly, the plaintiff has to make out the claim against the defendant. Where a claim is based on strict liability, whether in respect of employment injuries in general or in respect of injuries caused by particular categories of dangerous objects, it is necessary only to show that the injury was indeed caused by employment or by the risk in question. Where a claim is based on non-performance of a specific statutory duty and the statutory provision leaves no discretion as to the manner of its performance, it is necessary to make out a case that the duty was not performed as stated; since this is a question of fact, it should not normally create major problems of proof. But where a statutory duty leaves a discretion—for instance by the use of such terms as “reasonably practicable”—or where a claim is based on a duty of care (under common law, under the general provisions of civil codes or under labour codes) demonstrating that the duty has not been fulfilled is not always easy. Accordingly, courts have considered to what extent the burden of proving whether there has or has not been fault should be placed on the employer or other defendant rather than the worker.
While some national approaches such as these relieve the plaintiff of the need to demonstrate the manner in which a careful employer would have prevented the accident or illness, they do not at all imply that the case will necessarily be won. In a proportion of cases it will be possible for the defendant to demonstrate that he or she had been as careful as possible in the circumstances (i.e., that he or she was not at fault). This is particularly true if a special degree of fault is necessary for an action to succeed—as in actions for additional social security benefits by reference to an “inexcusable fault” of the employer.
Whether the civil action is based on fault or on risk, it is necessary to show that the injury suffered is the result of that fault or risk (i.e., a causal connection between them must be demonstrated). It is not usually required that the fault or risk be the sole or determining cause, but it must be one immediate cause of the injury. The problem of showing a causal connection is particularly acute in cases of illness the origin of which is not yet fully understood—although courts have sometimes interpreted the law so as to give the benefit of the doubt to the worker. This difficulty may be caused by factors such as the worker having been exposed to new technology or a new substance, the full implications of which are not yet known; the disease may have a long latency period, or the worker may have been subject to complex exposures. Even in cases of accidental injury it is not always possible to prove “on the balance of probabilities” (the required degree of proof in civil actions) that the injury was due to the demonstrated fault. There are also cases in which the causal connection between a demonstrated fault and an injury is broken by the intervening tortious act of a person for whose acts the person being sued is not liable, although an intervening act does not necessarily break the chain of causation.
Defences
Even where fault or risk and its causal connection to an injury has been demonstrated, a number of possible defences may permit the defendant to reduce or even avoid liability.
First and foremost is the fault of the injured worker. Such fault may take the forms of failure to comply with safety instructions, of a degree of carelessness going beyond inadvertence, of “frolics” (behaviour at the workplace unrelated to the normal performance of work), of violation of orders, or of drunkenness. Different systems of law have sought to balance the degree of such fault and the degree of fault of the defendant in compensating injury.
A second defence known in some countries is that of volenti non fit injuria (i.e., that the injured worker knowingly and voluntarily assumed the risk which led to the injury). Given the inequality in standing between employer and worker, courts have been reluctant to consider that this defence applied in ordinary cases in which a worker performed work, with or without protest, which he or she knew to involve a risk other than the normal risk inherent in the work. While in the past it was a recognized practice to give workers who enter inherently dangerous jobs “hazard pay” as a contractual counterpart for the assumption of the risk, there is doubt as to the validity of contracts under which the worker agrees, even for consideration, to bear the consequences of risks for which the employer would normally be liable, and such contracts may indeed be expressly prohibited. On the other hand, the law looks kindly on the worker who knowingly and deliberately courts danger in order to save other persons. The law also increasingly protects workers who remove themselves from situations involving imminent danger and who “whistle-blow” on violations of safety and health laws.
It is too early to say what effect, if any, this defence will have on statutory provisions permitting or requiring workers to stop work when they believe serious danger to be imminent. In any case, the protection of workers who choose to stop work (or to “blow the whistle”) from recriminations and victimization deserves further attention in all jurisdictions.
From time to time, defendants have tried to rely on the fact that the dangerous working practice which led to an accident was widely used in the industry. There is no evidence that this has led to a limitation of liability. Conversely, the fact that certain good practices are widely followed in an industry has been regarded as evidence that a particular defendant not applying these practices was at fault.
Time limits for the submission of claims
Most legal systems permit civil actions to be brought only within a relatively short period after the date when the cause accrued; the usual period is two or three years and may be as short as 12 months. Since longer delays increase the difficulties of establishing facts, these time bars are in the interests of all concerned.
However, with the emergence of occupational diseases which manifest themselves only many years after exposure to the substances or agents responsible for them—in particular, but not exclusively, various forms of occupational cancer—it became clear that in certain circumstances it was necessary to have, as the starting point of the time limits for the submission of claims, the moment at which the worker concerned knew that he or she had a cause of action. This is now widely provided for in relevant special legislation or as a special provision in general Limitation Acts. This does not necessarily resolve all difficulty: it is not always easy to determine the precise moment in time when a claimant had or should have had all the elements enabling the worker to sue. This is somewhat easier where the disease is included in a schedule or classification of diseases
Categories of damage
Damages which may be obtained through a civil action tend to fall into three main categories, although not all three are universally obtainable: (a) payment of all medical and rehabilitation expenses not covered by social security; (b) payment of earnings lost, in most countries to the extent that they are not covered by social security; and (c) damages for pain and suffering, disfigurement and loss of enjoyment and expectation of life. The principle of tort is restitution—that is, the plaintiff should be in a position no worse than he or she would have been had the tort not been committed.
Earnings lost are in some cases compensated by periodic payments supplementary to any relevant periodic payments from social security and to such earnings as the worker is able to obtain after the injury, so as to bring total income to the level of previous earnings. It is more usual for compensation to take the form of lump sums. Where there is continuing incapacity or death, the assessment of future losses which has to be made is necessarily speculative both as to the level of earnings and as to life expectancy. Where there is an award to survivors the speculation bears not only on likely future earnings but on likely future support. Although an attempt is made to take inflation and taxation into account, it is very difficult to do so to a realistic extent with lump sum payments. It is not surprising in these circumstances that lump sum awards for loss of earnings vary greatly, and that a periodic allocation will sometimes be preferable (period payments may more feasibly take taxation and inflation into account).
Compensation for non-pecuniary loss (such as pain and suffering) can necessarily be only an estimation of what is reasonable. Again, this leads to variations in the sums awarded. Some legal systems permit courts to award punitive damages, which may reach very large amounts.
Conflicts of law
Some reference must be made to the operation of civil liability where an employment injury arises in circumstances having potential links with several systems of law. Situations are now prevalent in which dangerous activities such as construction or rig drilling are carried out within the jurisdiction of one country by undertakings having the nationality of another country and employing workers from yet other countries. Should injury or disease accrue in such a situation, the rules of conflict of laws (which may also be called private international law) will come into play. These rules are not international in the sense of being universally or even generally recognized in all legal systems, but are a branch of and peculiar to each system of private law; with regard to many issues, however, there is little disagreement and certain areas of disagreement which remain are being diminished, in particular through the adoption of international conventions. When the rules of private international law are invoked in any legal system, they decide only three preliminary points. First, whether or not the courts of that legal system have jurisdiction over the issue at hand. If it is decided that the courts do indeed have jurisdiction, they must then go on to decide whether to apply their own internal rules or those of another legal system involved. Finally, they will decide whether they must recognize as decisive any foreign judgement already pronounced on the issue, or enforce any right vested in a party under a foreign judgement, or on the other hand treat such judgement or rights as nullities. The links between an injury and several countries may lead to “forum shopping” (i.e., the attempt to bring an action in the country where the highest damages are likely to be obtained).
Penal (criminal) liability
Penal or criminal liability following an employment injury, in the widest sense of liability to a penalty, may be incurred on four possible bases.
First, the occurrence of an accident or the apparent incidence of disease may bring into operation the provisions designed for the enforcement of laws and regulations regarding occupational safety and health. The inspectorate in most countries is too understaffed to keep a constant eye on all possible dangers. On the other hand, when accidents or diseases become known, in particular through their obligatory notification, this may lead to inspection visits and, as appropriate, criminal prosecution.
Secondly, some legislation concerning occupational safety and health contains special provisions regarding penalties applicable in the case of accidents or diseases, particularly where these are serious. The equivalent may be found in most systems of workers’ compensation in the form of increased contributions for poor health and safety performance.
Thirdly, employment injuries, particularly if serious or fatal, may bring into operation rules of criminal law not specifically related to occupational safety and health, such as those related to manslaughter, special rules on fires and explosions, and so on. There are some cases (examples may be found in Italy and the Netherlands) in which the normal penalties for the offences in question are increased where they were committed in a work setting.
Finally, there are cases in which penal codes contain specific provisions regarding injuries caused by violations of requirements on occupational safety and health.
It is sometimes expressly provided that action on one of these four bases does not exclude action on another. In some countries the reverse is true: in Sweden, for example, use by labour inspectors of their power to make compliance with remedial or prohibition orders subject to fines excludes recourse to action through the criminal courts. In some cases, but not always, the attitude to plurality of sanctions derives from the nature—civil, administrative or criminal—of those sanctions specifically designed for enforcement. There would seem to be little doubt, although there are no formal statistics to prove it, that most of the low number of prosecutions in relation to occupational safety and health infringements relate to infringements which have caused injury. There is similarly no statistical information on the use made of general rules of criminal law in relation to employment injuries. It would appear, however, that there are greater variations in this respect from country to country than with respect to other aspects of enforcement.
Elements of the offence
There is a wide acceptance of the maxim that there should be no penalty without previous legal authority. While, therefore, it is possible for courts in civil proceedings to affirm the existence of legal duties not previously defined, this is not normally possible in penal proceedings. On the other hand, it is possible in penal proceedings to determine the practical implications of a duty established by previous authority: in practice, this distinction between civil and penal liability may be one of degree. Different legal systems also appear to agree that an offence is committed only if there has been intent or, in many of them, culpable negligence, unless a legislative enactment expressly provides otherwise.
The enforcement provisions of some legislation on occupational safety and health make it an offence not to comply with statutory requirements in the field, irrespective of whether there was intent or culpable negligence, and so do some special provisions in penal codes. This has been confirmed by case-law. For instance, in a decision of 28 February 1979, the Supreme Court of Spain held that failure to comply with prescribed safety measures in the construction industry was sufficient in itself to give rise to sanctions under the corresponding enforcement measures. In some cases this strict liability carries only administrative or civil penalties. In many countries, the difference between strict liability, on the one hand, and the requirement of deliberate action, on the other, may not be as great in practice as appears at first sight. There are variations between different legal systems as regards the degree of negligence necessary for it to be “culpable” so as to warrant the imposition of penalties.
Initiation of penal proceedings
In principle, all prosecutions are a matter for the appropriate public authorities; criminal sanctions are intended for the protection of the interests of the community and not of the individual. There are, however, some possibilities for private prosecutions in certain circumstances (e.g., in Switzerland, Austria, England, Finland and France). Sometimes an inspector may institute proceedings, but it is more usual for action to be taken by public prosecutors, district attorneys, state solicitors and similar authorities. They act upon information from inspectors, social security bodies, the injured person, or members of the public, but the final decision regarding action is theirs. In principle, if they are satisfied that an offence appears to have been committed, they should act.
Two additional comments should be made. First, in respect of penal proceedings, the statutory periods of limitation do not so far appear to have given rise to difficulty (possibly because periods of limitation for penal purposes are often very long). Secondly, penal legislation is territorial, in the sense that it applies only to an offence which has effect in the territory over which the enacting legislation has jurisdiction. In transnational work situations, this limitation of jurisdiction can raise the problem of where the power to control health and safety lies.
Persons liable
Penal proceedings, like civil proceedings, are in principle possible in relation to any person with duties in the field of occupational safety and health. A problem which arises is that of the liability of legal persons (i.e., of corporations which have duties as manufacturers or employers). It is a widespread principle in criminal law that only natural persons can be liable: in many cases that principle is absolute, in others it applies only to some offences. In connection with occupational safety and health some countries expressly envisage the possible penal liability of corporations. Because of general principles of criminal law, certain of these do so only as regards penalties imposed by the labour inspectorate or other administrative and civil sanctions (e.g., some Scandinavian countries, Belgium, Spain), whereas others do not make that distinction (e.g., England, the United States). It is sometimes expressly specified that the liability of companies is to be enforced by means of fines. Contrary to the situation in many countries, proceedings in England are brought against the corporate employer in preference to any individual working within the undertaking, on the assumption that the company has a much greater degree of control.
Individuals—whether non-corporate employers, or directors or managers of companies—may be made liable for violation of the employer’s duties, directors or managers being liable in place of or in addition to corporations. For this purpose there must be a personal fault. Given the generality of the duties widely laid upon the employer, it is not difficult for courts to find that there is some omission. Nevertheless, there are cases of acquittal on the ground that there was no personal fault of the individual employer or director. In certain circumstances an employer may delegate duties as regards occupational safety and health (and the corresponding penal liability) to line management, or duties in this matter may be laid directly upon technical and supervisory staff. Case-law shows that the penal liability so laid on the staff in question is not simply theoretical. In France, the Criminal Court of Béthune, on 22 January 1981, held the chief engineer of a mine guilty of involuntary manslaughter in respect of a firedamp explosion in 1974 which cost 40 lives; he was found seriously negligent in not having installed a gas detector. In Italy, in the 1977 case concerning the use of benzene in a dye factory, the general manager, the technical manager and the works physician, as well as the owners and the managing director, were found guilty of involuntary homicide. A study made in Finland (1979) of penal responsibility in practice showed that 19% of charges and 15% of convictions concerned managers, 36% and 36% respectively concerned executives, and 35% and 38% respectively concerned supervisors. Penal proceedings against workers who do not have technical or supervisory responsibilities are possible in a number of countries, but not universally; they would appear to be used relatively sparingly and to require a high level of personal fault.
Defences
It is generally no defence in penal proceedings that the accused did not know the law. Conversely, it is often emphasized that it is the duty of the employer and of technical and supervisory staff to have all relevant knowledge.
In penal proceedings, contrary to the situation in civil cases, the fact that the negligence of the victim contributed to an accident is also generally not a defence. For instance, a Swiss court in 1972 convicted an employer following the electrocution of a worker who was loading metal onto a truck under a live electric main; it held that, while the worker himself could have taken the essential precaution of switching off the current, it was the responsibility of the supervisor (in this case the employer) to ensure the safety of the worker by so doing.
On the other hand, there may be a variety of extenuating circumstances which are taken into account by courts with respect to the penalty to be imposed (for example, an exemplary work record). In a Swiss case in which an accident resulted from the insufficient shoring of a drainage trench, the fact that the employer had tried to save working hours for the benefit of the employees working on piece rates, while not a defence, was taken into account in sentencing.
Penalties
Earlier (in the section on enforcement) some examples were given of the penalties possible under legislation on occupational safety and health. In many cases the financial penalties so laid down have higher ceilings than those available under more general penal codes and statutes.
On the other hand, the range of possible sentences of imprisonment is more likely to be greater under general penal codes and statutes.
In certain circumstances, other types of penalty are possible, such as being banned from the occupation in which a homicide occurred. Moreover, under Section L. 263-3-1 of the French Labour Code as amended in 1976, in the case of accident in an undertaking where serious or repeated infringements of safety and health rules have been observed, the court may require the undertaking to submit for its approval a plan to normalize conditions; if the undertaking fails to do so it may be required to implement some other plan approved by the court.
As in other areas of criminal law, it would appear that in practice the penalties imposed seldom encompass all possibilities or reach the possible maxima. Instances of imprisonment occur, but rarely. Fines are imposed, but rarely at maximum levels.
Largely as a result of the scarcity of specifically compiled statistical information, and the fact that it appears very few health and safety claims actually make it as far as a courtroom, it is extremely difficult to evaluate the deterrent effects of civil and criminal liability, either in absolute terms or in relation to each other. It is similarly difficult to determine the role which legal liability plays in prevention relative to social security or voluntary compliance measures. The criminal law none the less remains a deterrent, along with civil law remedies, of health and safety violations.
Labour Inspection
The ILO Labour Administration Convention, 1978 (No. 150) and its related Recommendation (No. 158) provide the basis for the development and operation of any modern system of labour administration. These two international instruments provide a most useful source of guidance and a standard against which any national labour administration can compare its orientation, role, scope, structures and functions, as well as actual performance.
Labour administration is concerned with the management of public affairs in the field of labour which, in its traditional sense, can be taken to mean all matters relating to the economically active human resource, in whatever sector. This is a broad concept, but supported by Convention No. 150, which defines labour administration as “public administration activities in the field of national labour policy”. Such activities would typically include the following:
- policy formulation involving the preparation of guidelines for new initiatives
- drafting of labour laws and regulations as a means of giving positive expression to labour policies
- planning of programmes, projects and activities in support of policy interventions
- policy shaping, involving drafting and inviting discussions on new initiatives
- policy implementation, involving the enforcement of labour laws, and the provision of advisory services as to how to comply with labour laws
- policy monitoring and evaluation
- providing information and raising awareness on matters of labour policy and labour laws.
From this comprehensive definition, it is apparent that labour administration may cover more than the responsibilities and activities of a typical ministry of labour (employment, social affairs and so on) in that the “field of labour policy may extend to various ministries, departments, parastatal agencies, or other public ministries outside labour”.
It is therefore necessary to think in terms of a labour administration system consisting of various components related to or interacting in the same way, to form a synergetic unity. The common unifying element is labour policy, and this includes all activities carried out under its purview. This will vary from one national system to another (for historical, political, economic, social or other reasons), but may typically include the following components: industrial relations, labour inspection, work safety, occupational hygiene, workers’ compensation, employment services, employment promotion, vocational training, guidance and counselling, trade testing and certification, personnel planning, employment and occupational information, foreign workers and work permits, social security, vulnerable and under-privileged groups, labour statistics, and indeed other elements.
From this it is apparent that a system of labour administration tends to be complex, that it requires coordination at all levels if it is to serve its purpose, and that it is dynamic in that, according to ILO Convention No. 150, it covers all “public administration bodies” and “any institutional framework” concerned with national labour policy. Finally, it becomes evident from this set of international standards that labour inspection should be an integral part of labour administration, and that in the field of labour protection (which includes but goes considerably beyond occupational safety and health) labour inspection is the operational instrument of any labour administration system to ensure compliance with national labour policy and legislation. To quote a former Director-General of the ILO: “Labour legislation without inspection is an essay in ethics rather than a binding social discipline.”
Two Levels of Labour Inspection
Labour inspection, as part of labour administration, as a rule is organized at two levels: field inspection offices devoted mainly to action, and the central authority devoted to policy development and monitoring, and to programme planning and management. The field services and the central authority must obviously work in close collaboration.
Field services
Labour inspection performs its functions of inspection and advice through the field services that constitute its foundation. These give it the advantage over other services of being in direct touch with the world of labour at the enterprise level—with the employers and workers, the active population of the country.
Conversely, carrying out inspections in enterprises puts the inspectorate in a position to provide the central administration with detailed information collected during visits or in meetings with the social partners and unobtainable otherwise, on the social climate, working conditions and the working environment or the difficulties of enforcing the legislation: the inadequacy of the deterrent action of the courts, problems with the regional authorities, pressure exerted by certain enterprises because of their economic role, and lack of coordination in the work of the various public services. The field services are also well placed to bring to light, as required by the international standards, defects or abuses not covered by the legal provisions.
Under ILO Convention No. 81 on Labour Inspection in Industry and Commerce (1947) (and, by virtue of Article 2, Mining and Transport), inspectors of local offices are required “to submit to the central ...authority periodical reports on the results of their inspection activities”. This provision, which is also contained in Convention No. 129 (Labour Inspection (Agriculture) Convention, 1969) leaves States a wide latitude to determine the form, content and frequency of the reports. The provision is essential, however, to ensuring continuous contact between the inspectors and the central body and to keeping the latter informed of the economic and social situation in the regions and allowing it to define and direct national inspection policy, as well as to compile an annual report on the activities of the inspection services for national distribution and in time with international obligations.
The central authority
The central authority directs the labour inspectorate (or, in the case of many federal countries, state inspectorates) and ensures its place in the administrative machinery of the ministry responsible for labour policy administration and of the state administration. Carrying out the tasks of inspection is not, in fact, dependent solely on the personal initiative of the inspectors, even though this remains of fundamental importance. Labour inspectors do not work in isolation; they are part of an administration and execute a set of national corporate objectives.
The first step in directing is to draw up a budget, have it adopted and administer it. The budget reflects the social choices of the government; its amount determines the scale of the means accorded the services. Consultation with the trade union organizations, which have an interest in the effectiveness of inspection, can be important from this point of view.
To direct is also to define a labour protection policy, to work out the principles for the work of inspection, to set an order or priority in accordance with the characteristics of the various branches of activity and the type of the enterprises and the results they obtain, to rationalize the activities (enforcement policy), to perfect the methods and programme, to encourage and coordinate the different services, to evaluate results and to make suggestions to improve the functioning of inspection.
It is the central authority that must give the external services sufficiently clear instructions to ensure the coherent and consistent interpretation of the legal provisions throughout the country. This is usually done by way of a comprehensive national enforcement policy, often (and preferably) designed in consultation with the most representative social partner organizations. Finally, it must manage the staff, see to training and refresher training (training policy), ensure independence and respect for professional ethics and periodically assess the work of the officials.
Under the terms of ILO Conventions Nos. 81 and 129, the central authority has to draw up an annual report, the essential elements of which are indicated in Articles 20 and 21, on the work of the inspection services. The publication of these reports within 12 months after the end of the year to which they relate allows the workers, the employers and the authorities concerned to become familiar with the work of inspection. The communication of these reports to the International Labour Office within three months of publication provides the material for an extremely useful study of the systems established and the results obtained in the member States and allows the competent services of the ILO to remind governments of their obligations, if need be. Unfortunately, this obligation, binding on all member States having ratified the Convention, in practice is all too often overlooked.
It remains for the central body to transmit the information received from the inspection services to the advisory bodies set up within the ministry (e.g., the national safety and health committee or the collective agreements board), to the ministries concerned and to the social partners. It also has to use this information itself and take the appropriate action, either in the work of inspection or in the drafting of laws and regulations. In all, this publication activity is a most useful means for the labour inspectorate to document its activities and achievements at the national and international levels.
Technical Collaboration
ILO Conventions Nos. 81 and 129 provide that appropriate arrangements shall be made to promote cooperation between the labour inspection services and other government services or public or private institutions engaged in similar activities.
Collaboration with other labour administration services
Collaboration must first be established with the other labour administration services, both central and local. The problems dealt with by labour administration—working conditions, health and safety, wages, employment, labour relations, social security and statistics—are often closely linked and must be seen as a whole.
The central authority must exchange information and assist in preparing a common policy and common guidelines for decisions by the competent minister or ministers or by a central planning body. On the local scale, labour inspection must maintain regular contact, in particular, with the employment services, those dealing with foreign workers and those dealing with labour relations (when these come under specialized services).
In countries where there are different labour inspection services under the same ministry (as in Belgium) or attached to different ministries, very close collaboration must be arranged for the exchange of information, the specification of methods or procedures for action and the drawing up of common programmes of action. The effectiveness of work carried out by several services is directly linked to the quality of the cooperation between them, but experience shows that in practice such cooperation is very difficult to organize and time- and resource-consuming even in the best of circumstances. It therefore almost always tends to be a second-best choice. It also tends to render the necessary holistic approach to prevention as the primary objective of labour inspection very difficult.
Collaboration with the social security administration
In many countries, parts of the social security services, notably those responsible for workers’ compensation and occupational accident and disease insurance, deal with the prevention of occupational risks. Other specialized officials carry out checks in enterprises to see what health and safety measures must be applied. In some countries (Australia (New South Wales), Zimbabwe), the labour inspectorate is actually operated by the social security system. In others (France, Germany), they run a separate, parallel inspection system. In still others (Switzerland), the state labour inspectorate is reimbursed on a pro-rata basis for inspection activities devoted to occupational safety and health prevention at enterprises. Though social security officials’ actions are not directly backed, like those of labour inspection, by the authority of the State, except where they are civil servants, such as in New South Wales or Zimbabwe, they are accompanied by financial penalties in the form of increased contributions for enterprises with a high accident rate that do not act on the advice given. On the other hand, enterprises that make a real effort in prevention can benefit from reduced contributions or have loans on special terms to continue their work. These inducements and deterrents (bonus-malus system) obviously constitute an effective way of bringing pressure to bear.
Collaboration between services of social security and labour inspection is essential, but not always easy to establish, even though both usually but not necessarily come under the same ministerial department. This is largely due to the attitude of more or less independent administrations firmly attached to their prerogatives. When the controlling authority is fully effective, however and coordination is achieved, the results, particularly in terms of preventive action and cost control, can be remarkable.
Collaboration with the central authority must be evident in the exchange of information, the utilization of data and the joint preparation of programmes of prevention. Locally, collaboration can take various forms: joint inquiries (in the event of accidents, for example), exchange of information and the possibility of using the equipment of the social security services (often much better endowed from a financial point of view) for labour inspection.
Collaboration with research bodies, technical bodiesand experts
Labour inspection cannot remain isolated; it must make close contact with research bodies or universities to keep up with technological change and with progress in the social and human sciences, to obtain specialized information and to follow new trends. Collaboration must not be one-sided. Labour inspection has an important role to play with regard to research bodies; it can point out to them certain subjects for study and help them to test results in the field. Labour inspectorates are sometimes invited to participate in seminars or colloquia on social questions, or to provide specialized teaching. In many countries (e.g., the Federal Republic of Germany, the Russian Federation, or the United Kingdom) such collaboration, sometimes on a regular basis, is found to be of great value.
In the field of occupational health and safety, labour inspection must either approve or collaborate with the bodies approved for carrying out the technical verification of certain types of plant and equipment, where they exist (appliances under pressure, lifting gear, electrical installations). In other countries, such as South Africa, this is still largely done by the labour inspectorate itself. By calling on such external bodies regularly, it can obtain technical opinions and observe the effects of the measures recommended.
The problems faced by labour inspection today, especially in the technical and legal fields, are so complex that inspectorates could not fully ensure the inspection of enterprises without specialist assistance. Convention No. 81 requires States to take the necessary measures “to ensure that ...technical experts and specialists, including specialists in medicine, engineering, electricity and chemistry, are associated in the work of inspection ...for the purpose of securing the enforcement of the legal provisions relating to the protection ...health and safety ...and of investigating the effects of processes, materials and methods of work”. Convention No. 129 has a similar provision.
It remains true that the many aspects of working conditions are closely linked—recent research only goes to confirm this—and that labour inspection services must be able to deal with them as a whole. For this reason, the multidisciplinary approach, which makes it possible to combine the advantages of specialization and versatility where financial resources are adequate, appears especially promising.
Regional or departmental authorities
In almost all countries, the national territory is divided into a number of districts called by different names (regions, provinces, cantons, departments), themselves sometimes subdivided into smaller districts, in which the central authority is represented by senior officials (e.g., governors or prefects). The staff of the external services of the various ministries often come under these senior officials as regards the civil service rules and information on policy, and it is often their senior officials who install labour inspectors in their posts when they are appointed. Inspectors (or, if they exist, departmental, provincial or regional directors of labour) subsequently should keep these senior officials informed of any events that they should know about. Similarly, inspectors must collaborate with these officials to provide them, either directly or through their immediate staff, with any information that they require. Inspectors, however, should always come under their minister, generally the minister of labour, through their superior in the hierarchy (the departmental, provincial or regional director), as regards the content of their work, their manner of carrying it out, and their reporting on its results.
This can put labour inspectors in a delicate situation, for the officials representing the central authority are seldom well informed of the functions of labour inspection and they may be tempted, especially in certain disputes, to base their decision on considerations of law and order and social peace. Labour inspectors must stress the importance of the general application of the labour laws, where this is in question, and, if difficulties arise, they must refer the matter to their superiors.
Judicial authorities
Labour inspectors normally have regular administrative relations with the judicial authorities, whose support is essential for preventing infringements. In most countries, inspectors do not institute proceedings themselves—this is the prerogative of the public prosecutor’s office in the ministry of justice. When they note an infringement and they think it their duty to take it up against the employer, they draft a report of irregularity for the public prosecutor’s office. This report is an important document that must clearly establish the infringement, indicating the provision violated and the facts as observed by the inspector. The public prosecutor’s office generally has discretion either to act on the report and prosecute or to shelve the matter.
It can be seen not only how important it is to draft the report of irregularity, but also how desirable it may be for inspectors and officials of the public prosecutor’s office to meet, if only once. The labour inspector who reports an infringement has generally tried, before resorting to this measure, to use persuasion as a means of having the legal provisions respected. Officials of the public prosecutor’s office and judges are not always adequately informed of this, and it is often lack of knowledge of the inspectors’ working methods that leads them to pronounce trifling penalties or to shelve the case. For this reason, discussions between ministries are also essential at the highest level.
There are other circumstances in which labour inspectors may be in touch with the judiciary—for example, if a piece of information is requested of them for the preliminary investigation of a case or if they are called as witnesses during proceedings. It is important for them to receive communication of the complete text of judgements (including the reasons adduced), as soon as the judgements are handed down. This allows them to report the repetition of the offence, if the infringement continues; if the case is dismissed or the penalty given appears inadequate, it allows the inspectorate to request the public prosecutor’s office to appeal. Finally, communication is all the more useful if the judgement sets a precedent.
Other authorities
Labour inspectors may have occasion to maintain regular or sporadic contact with various other public authorities. They may be invited, for example, to cooperate with development planning services. Their role will then be to draw their attention to certain social factors and to the possible consequences of certain economic decisions. With regard to political personalities (mayors, members of parliament, party members), if labour inspectors should receive requests for information from them, for example, it is important that they should maintain the impartiality that must be their rule of conduct and display increased prudence. Procedures for relations with the police must also be established, for instance to control working hours in public road transport (only the police have the right to halt vehicles) or in case of suspected illegal immigrant labour. There must also be procedures, often lacking, to ensure inspectors the right of entry into workplaces, if necessary with the help of the police.
Relations with Employers’ and Workers’ Organizations
The labour inspection services naturally maintain close and regular relations with employers, workers and their organizations. Conventions Nos. 81 and 129, moreover, call on the appropriate authority to make arrangements to promote this collaboration.
Inspectors have contact in the first place with employers and workers in the enterprise, either during visits, or at meetings of bodies such as safety and health committees or works councils, or during conciliation meetings to prevent or attempt to settle disputes. Inspectors also have frequent contact with workers and employers outside the enterprise. Very often, they provide advice, information and opinions in their offices. Sometimes they preside over joint committees, for example to negotiate collective agreements or to settle disputes. They can also give courses on labour topics for trade unionists or heads of enterprises.
Labour Inspection and the Workers
As it is the clear and daily responsibility of labour inspectors to ensure the protection of the workers, it is inevitable that inspectors and workers should have extremely close relations. First of all, the individual worker can make a direct approach to the inspectors to ask for advice or to consult them on some question. Relations are most frequently established, however, through trade union organizations, shop stewards or workers’ representatives. As the purpose of trade unions is to defend and represent workers, their role is generally essential.
This set of relations, varying in form with the country and with the problem at issue, is discussed in the chapter Labour Relations and Human Resources Management. It should be recalled that the international standards—Conventions Nos. 81 and 129 and the Protocol of 1995 to Convention No. 81—lay down the principle of collaboration, both with the employers and the workers: the competent authority must “make appropriate arrangements to promote ...collaboration between officials of the labour inspectorate and employers and workers or their organizations”. It should also be noted that relations between the labour inspectorate, the employers and the workers cannot be separated from labour relations as a whole and are necessarily marked by the fact that labour inspection forms part of a socio-economic system that differs from country to country.
Collaboration
Collaboration can be established in various ways, in particular through direct relations or through bodies set up within the enterprise for representation or participation. Other forms of collaboration are practised on a departmental or regional scale in certain countries, in accordance with various procedures.
Direct relations
One of the basic functions of labour inspection as described in Article 3 of ILO Convention No. 81 is to provide information and advice to employers and workers, who can ask the inspectors for their opinions on problems that come within their competence and also ask them to take action. The workers can address a complaint or a request for opinion or action (visiting a workplace, for example) to the inspectorate through the trade unions; although labour inspectors remain free to act or not and to choose the form of their action, workers and their organizations have a certain initiative in the matter of inspection.
Relations between labour inspection and representative or participative bodies within the enterprise
This is probably the most obvious and the most regular form of collaboration. Because of workers’ experience and familiarity with work, they are particularly well placed to detect problems arising in working conditions, especially regarding safety and health, and to suggest remedies. It is normal for them to be consulted and associated in the study and solution of problems and in decisions that concern them. These principles, which call for dialogue and participation within the enterprise, call no less naturally for an exchange of information and collaboration with the labour inspectorate.
One of the most usual bodies for participation within the enterprise is the safety and health committee. This committee, which includes the representatives of the employer and the workers, continues in its own sphere the work of the labour inspectorate. The workers’ representatives are normally the most numerous. Committee coordinators are generally the heads of the enterprises or their representatives, which helps to ensure that the decisions taken by the committee will be followed by action. Technical experts, including occupational physicians and safety officers, assist the committee if possible. For its more important meetings the committee can also call on the labour inspector and the engineer of the social security services. The safety and health committee can and indeed should make the rounds and pay very regular visits to workplaces to detect hazards, draw the attention of the management to safety and health problems or address complaints to it about such matters, suggest improvements, verify the action taken on earlier decisions, carry out inquiries in the event of occupational accidents and take the initiative in introducing the workers to the basic prevention of occupational hazards and in improving their knowledge and making the whole staff of the enterprise, from the top of the hierarchy to the bottom, participate in the fight against occupational accidents and diseases.
In many countries, the members of the safety and health committee have the right to accompany labour inspectors on their visits. Experience shows that, where safety and health committees work well, collaboration with the labour inspectorate is common practice. Other representative bodies, the works councils or committees, which have a wider competence, play the same role of extension. Many problems relating to the application of labour legislation can be solved in this way: appropriate solutions can be found that go further than enforcing the letter of the texts, and it is only in difficult cases that the labour inspector is called in.
In many countries, the legislation provides for the appointment in the enterprise of staff representatives or shop stewards, who deal with conditions of employment and working conditions, among other things, and can maintain a dialogue with the employer. All sorts of problems can be brought up in this way that would not otherwise come to light. These problems can often be solved without the help of the labour inspector, who intervenes only if difficulties arise. In certain countries, staff representatives are entrusted with presenting complaints and observations relating to the application of legislation to the inspectorate. The inspectors often have the right and sometimes the obligation to be accompanied by staff representatives during their visits. Elsewhere, workers’ representatives must be informed of the visits of the inspectors and sometimes also of their observations or findings.
A highly important task of labour inspection is to maintain conditions such that the representative or participative bodies can function normally. One is to ensure the observance of trade union rights, the protection of workers’ representatives and the smooth running of the work of these bodies, in conformity with the legal provisions. Labour inspectors have a very important role to play in ensuring that the representative and participative bodies have a genuine existence and carry on useful activities, and this is one of the main areas in which they can give advice.
Participation in Inspection Duties
In some countries, the legislation explicitly provides for the involvement of workers’ representatives—trade unions, shop stewards or elected representatives—in labour inspection duties in certain circumstances.
Compulsory consultation of trade unions
In Italy, in certain cases specified by law, the labour inspectorate is obliged to seek the opinion of the trade union organizations before adopting a provision. Frequently, too, when the ministry of labour provides explanations for labour inspectors on the interpretation and application of the laws, these explanations are also communicated to the trade union organizations by way of circulars, briefings or meetings. In accordance with ministerial instructions, the labour inspectors’ visits must be preceded and followed by meetings with the trade unions, which are entitled, moreover, to see the reports of the visits. This latter practice is followed in more and more countries, often required by law, and has proved a most effective tool against unethical behaviour or negligence on the part of certain inspectors.
In Norway, the Act of 4 February 1977 respecting Workers’ Protection and the Working Environment lays down in certain of its provisions that the inspection services shall allow workers’ representatives to express their opinion before the Inspectorate makes a decision.
Participation and direct intervention of workers’ representatives
The participation of the social partners in inspection has been strengthened in various countries, especially in the Nordic countries.
In Sweden, the Working Environment Act of 19 December 1977 provides for the establishment of a safety committee which shall plan and supervise safety activities, and for the appointment of one or more workers’ safety delegates with wide powers of inspection and access to information. They are authorized to order work to be suspended when they consider a situation to be dangerous, pending a ruling by the labour inspection service and despite opposition by the employer. No penalty can be imposed on a delegate whose decision to have the work suspended is not confirmed by the labour inspector, and the employer cannot claim any compensation for the suspension from the delegate or trade union organization.
Similar provisions on the appointment and duties of safety delegates appear in the 1977 Act of Norway. This Act also provides for the establishment, in all enterprises employing 50 or more persons, of a working environment committee, which participates in the planning and organization of safety and can make decisions; the coordinator of this joint committee changes annually, being elected alternately by the employers’ and the workers’ representatives, and casts a vote.
In Denmark, the organization of safety inspection, based on cooperation between workers and the employer in the enterprise, has been clarified and strengthened, a greater role being given to the trade union representatives. The basic principle underlying the Act of 23 December 1975 respecting the Working Environment is that the responsibility for ensuring occupational safety must be decentralized and, ultimately, assumed in full by the enterprise—and that most problems can and must be solved there, without external intervention.
Workers’ Role in the Inspection of Working Conditions and the Working Environment: International Trends
In general, it would seem that the participation of the workers in the inspection of working conditions and the working environment will continue to increase, particularly in countries that have introduced “self-inspection regimes” or internal control, such as some of the Nordic countries. Any such regimes depend on strong workers’ organizations and their active involvement in the underlying audit process at the enterprise level, which is the centrepiece of any such “self inspection”. It is in this direction that many trade union organizations are moving. The determination of these organizations, whatever their leaning, to participate in the examination and application of measures to make working conditions and the working environment more human has been documented in many recent international meetings.
In particular, the election of safety representatives to represent the workers in the enterprise in all matters of safety and health protection is essential. These officials should receive appropriate training at the expense of the enterprise. They should have the necessary time to carry out inspections and have the right to stop any work that seems to them dangerous, pending verification by the public authorities (in principle, the labour inspectorate).
Trade union participation in the determination of the criteria governing the use of dangerous substances and products is another essential criterion. The workers’ representatives should have a real influence on the management process regarding the use of dangerous substances, the choice of materials, the working out of production methods and the protection of the environment. In general, trade unions and workers’ representatives should have the right to participate, both on the national scale and at the workplace, in the protection of the health and safety of their members.
The ILO’s Occupational Safety and Health Convention, 1981 and Recommendation (Nos. 155 and 164 respectively) show a similar trend. The Convention states that occupational safety, occupational health and the working environment must be the subject of a “coherent national policy”, formulated, implemented and periodically reviewed “in consultation with the most representative organizations of employers and workers”. The two instruments, which lay down the principles of this policy and indicate the measures that must be taken on the national scale and in the enterprise, call on States to secure the enforcement of laws and regulations concerning occupational safety and health and the working environment by an appropriate system of inspection, to furnish guidance to employers and workers and to impose penalties in the event of infringements.
The provisions that are of the greatest interest to labour inspection and local trade union officials are those dealing with the enterprise. The Convention contains the following passages:
(1)workers ...cooperate in the fulfilment by their employer of the obligations placed upon him;
(2)representatives of workers in the undertaking cooperate with the employer in the field of occupational safety and health;
(3)representatives of workers in an undertaking are given adequate information on measures taken by the employer to secure occupational safety and health and may consult their representative organizations about such information provided they do not disclose commercial secrets;
(4)workers and their representatives in the undertaking are given appropriate training in occupational safety and health;
(5)workers or their representatives and, as the case may be, their representative organizations in an undertaking ...are enabled to enquire into, and are consulted by the employer on, all aspects of occupational safety and health associated with their work; for this purpose technical advisers may, by mutual agreement, be brought in from outside the undertaking;
(6)a worker reports forthwith ...any situation which he has reasonable justification to believe presents an imminent and serious danger to his life or health; until the employer has taken remedial action, if necessary, the employer cannot require workers to return to work. …
The Recommendation (No. 164) that accompanies the Convention naturally contains much fuller and more detailed provisions concerning the whole matter of working conditions and the working environment. It specifies, among other things, what should be provided for workers’ representatives to enable them to carry out their task: training, information, consultation, time during paid working hours, association in decisions and negotiations, access to all parts of the workplace, possibility of communicating with the workers and freedom to contact labour inspectors and to have recourse to specialists. The representatives should “be given protection from dismissal and other measures prejudicial to them while exercising their functions in the field of occupational safety and health”.
The provisions of the Convention and the Recommendation as a whole, on which governments and the social partners have reached general agreement on the international scale, are a pointer to the general direction not only of trade union action within the enterprise in respect of working conditions and the working environment but also of the work of labour inspection.
It is clear that cooperation between heads of enterprises and workers or their representatives will develop simultaneously with the strengthening of participation by the workers in the supervision of their working conditions. The role of labour inspection will then become essentially an advisory role in a system in which the social partners participate actively. Labour inspection will also have the task of supervising the smooth running of the machinery for cooperation within the enterprise, without ever abandoning its function of inspection in situations where violations call for inspection or in the workplaces—becoming fewer no doubt but remaining numerous for some time (in particular small and medium-sized enterprises) where such cooperation has not yet been firmly established. The external check of labour inspection will remain indispensable, even in countries where the social dialogue is the most advanced and the consciousness of occupational hazards the keenest. It will remain the principal tool in more effectively securing the protection of workers.
The Purposes of Inspection
Many different forms and systems of labour inspection exist throughout the world. Beyond their differences, however, they all have common basic purposes that determine the broad functions of inspection. What are these purposes? ILO Convention No. 81, which has acquired virtually universal status through its ratification by almost 120 member States, defines them in Article 3 as follows:
The functions of the system of labour inspection shall be:
(1)to secure the enforcement of the legal provisions relating to conditions of work and the protection of workers while engaged in their work, such as provisions relating to hours, wages, safety, health and welfare, the employment of children and young persons and other connected matters, in so far as such provisions are enforceable by labour inspectors;
(2)to supply technical information and advice to employers and workers concerning the most effective means of complying with the legal provisions;
(3)to bring to the notice of the competent authority defects or abuses not specifically covered by existing legal provisions.
The wording is both strong and flexible, and marks out a vast field for the activities of labour inspection. The obligation is placed on labour inspection “to secure the enforcement of the legal provisions”. These terms were chosen carefully by the authors of the Convention, who did not wish to speak simply of “supervising” or “promoting” the application of the legal provisions, and they clearly state it is the duty of labour inspection services to obtain effective application.
What are these provisions? According to the Convention, in addition to laws and regulations, they include arbitration awards and collective agreements upon which the force of law is conferred and which are enforceable by labour inspectors. These provisions form the common basis for the work of all the inspectors in a country and the guarantee for enterprises and workers against what is arbitrary, unfair and unjust. The role of labour inspectors is not to promote their own ideas, however noble these may be, but to make sure that the legislation in force is carried out (i.e., to be the faithful and active instrument of the competent authorities of their country—the law-makers—in the field of labour protection).
Reference to the legal provisions might appear to restrict the scope of the inspectors in so far as they are not empowered to enforce every improvement in working conditions that seems desirable to them. In fact, one of the functions of labour inspection is “to bring to the notice of the competent authority defects or abuses not specifically covered by existing legal provisions”. This function is given the same priority as the function of enforcing the legislation, and it makes labour inspection an instrument of social development by according it a right of initiative in labour protection.
The scope of labour inspection varies from country to country, with the extent and nature of the legislation in force, with the powers conferred on the inspectors by the State, and with the field covered by the system. The powers of the inspectors may be general and relate to all legislation dealing with working conditions and the working environment; they may on the other hand be restricted to certain matters—for example, safety and health or wages. The system can cover all sectors of the economy or only some of them; it can cover the whole of the national territory or only part of it. Convention No. 81 covers all these situations, so that the tasks of the national inspection services can be narrowly restricted or extremely wide, depending on the country, and still meet the international definition of the purposes of inspection.
Among international standards, those concerning labour inspection appear to be indispensable to the formulation, application and improvement of labour legislation. Labour inspection is one of the driving forces behind social progress, since it ensures the implementation of established social measures (provided of course that it has the means to do so) and brings to light the improvements that may be made to them.
The Functions of Inspection
It has been seen that the purposes of labour inspection, as defined above, are made up of three main tasks: the enforcement of legislation mainly through supervision, the supply of information and advice to employers and workers, and the supply of information to the competent authority.
Inspection
Inspection is based essentially on visits to workplaces liable to inspection, and it aims, by observation and discussion, first at establishing the situation and then at promoting (by methods to be discussed below) and actually ensuring the application of the legislation for purposes of prevention.
Inspection must not be directed towards the systematic repression of lapses: its aim is to have legislation applied, not to catch offenders. It is, however, essential for inspectors to be able, if need be, to resort to coercive measures by drawing up a report with a view to the infliction of penalties severe enough to be deterrent. If there are no penalties or if penalties do not produce the desired result within a reasonable period, labour inspectors lose all their credibility, and their work loses all its effectiveness This is especially the case when labour inspection has to refer to civil courts for improvement notices and sanctions.
It is obvious that the aim of inspection is the future protection of workers through the ending of dangerous or irregular situations. In the field of safety and health, inspection operates at three stages. Before the construction of a factory, the fitting out of a plant or the manufacture of a machine, for example, it ensures, from the planning stage, conformity with the relevant legislation. This preliminary check will be followed by the normal inspection carried out during visits to workplaces. Lastly, in the event of accident, supervision will take the form of an inquiry intended mainly to prevent repetition of the accident.
Inspection can take various forms depending on the inspection system adopted by the country and its precise purpose. In the field of occupational safety and health, inspection is based mainly on visits to workshops and other places of work. In that of hours of work, wages and child labour, inspectors must demand the records that the enterprise is obliged to keep, and check their accuracy. In the field of freedom of association, inspectors must verify, in accordance with the legal provisions, that the elections laid down are held correctly, that the trade union can carry out its legal activities and that there is no discrimination against its members.
In their work of inspection, inspectors can call on certain sources of assistance (see preceding section on collaboration), either to get a better understanding of the situation (supervisory bodies, appointed experts, the accident prevention departments of social security funds, bodies within the enterprise such as the safety and health committee), or to extend their own work (staff representatives, the above-mentioned prevention departments, employers’ and workers’ organizations). The action of inspectors is discontinuous, and something permanent must be found in the enterprise to carry it on.
Information and advice for employers and workers
The function of supplying information and advice to employers and workers has a clear aim, in the words of Convention No. 81: to indicate “the most effective means of complying with the legal provisions”. Like the function of inspection, it contributes to ensuring the application of the legislation. Information and advice complement inspection, since, as noted above, the labour inspector’s task is not solely coercive.
Accordingly, the effects of the necessarily brief acts of inspectors may endure at the workplace. The advice and information provided by inspectors are thus directed towards the future. Inspectors cannot restrict themselves to carrying out a sort of retrospective supervision to ensure that everything is in order: they have to give advice about the measures to be taken to ensure labour protection, to explain the legal requirements concerning the payment of wages, to indicate where and how medical examinations can be carried out, to demonstrate the importance of limiting work hours and to discuss existing or potential problems with the employer. Authoritative opinion holds that the inspectors who get the best results are those who devote most of their efforts to educational work at the workplace among management or its agent and the workers’ representation. This is current practice in countries such as the Federal Republic of Germany, the United Kingdom, the Scandinavian countries and many others.
Because of its educational nature, the function of supplying information and advice can exert an influence beyond the case in question and play a part in prevention: its effects can be felt on other, similar, or even different, cases and can entail improvements going further than the legal requirements.
Information and advice during visits to workplaces
It is almost inevitable, as has been noted more than once above, that the function of inspection, which is performed mainly during visits to workplaces, should involve the provision of information and advice. Labour inspectors have to answer any questions that employers, their assistants or the workers’ representatives may ask. It is just as natural for them to give opinions and explanations. In fact, the provision of information and advice is so much bound up with the function of inspection that it is difficult to distinguish one from the other. However, the proper balance between advisory and supervisory intervention is a matter of considerable national and international debate. Typically, it is the centrepoint of any comprehensive and coherent national enforcement policy statement.
Information and advice at labour inspection offices
Labour inspectors should be easily accessible, and the doors to their offices should be wide open to anyone wishing to consult them, lay a problem before them or address complaints to them about given situations. Their attitude should always be guided by the same concern: to promote an intelligent and fuller observance of the legal provisions.
A connection must be made between these activities and the handling of individual disputes. These concern as a rule the application of the laws or regulations and, in some countries, take up much of the time of the inspection staff, including that of the inspectors. The problem raised by activities of this type has been settled by Conventions Nos. 81 and 129, which tolerate them only if they do not interfere with the effective discharge of the primary duties of inspectors or prejudice their authority or impartiality. A number of countries consider that this is a question of adequate staffing and that the organization should be large enough to allow inspectors to carry out their other duties properly as well.
Educational activities
To inform and advise are tasks of an educational nature, in so far as the information and advice given are intended not only to be acted on to the letter in a given situation but also to be understood and absorbed, to be convincing and, in short, to have a wide and lasting effect. The provision of information and advice can also take the form of courses, lectures or talks, as suggested, moreover, in Recommendation No. 81. These activities clearly make it possible to reach a wide audience, to explain both the letter and the spirit of labour legislation and to ensure that it is better understood, better accepted and, therefore, better applied. For example, in Norway there is a national training committee made up of representatives of the labour inspection service and of the employers and workers.
Dissemination of information
Ignorance of the social legislation and failure to recognize its underlying purpose and its usefulness are among the greatest obstacles faced by labour inspection, particularly in developing countries. There is no need to stress the great utility of every measure that helps to promote the dissemination of information on labour legislation. Nothing should be neglected in this field, in which employers’ and workers’ organizations can also play an important role. Mention may be made here of the work of the information services of the United Kingdom Health and Safety Executive, which collect and disseminate a great deal of information (a library, documentation and translation service are available; radio and television programmes are prepared, exhibitions arranged, and so on).
Informing the competent authority
This function is often underestimated or neglected. It is nevertheless explicitly mentioned by ILO Conventions Nos. 81 and 129: labour inspection has an obligation “to bring to the notice of the competent authority defects or abuses not specifically covered by existing legal provisions”. This obligation imposed on labour inspection as a whole, from the most junior inspectors to their highest superiors, completes the terms of reference that make labour inspection an active agent for social progress. The inspectors’ knowledge of labour problems and of the workers’ situation, especially concerning the protection guaranteed to the workers by the social laws and regulations, puts them in a position to keep the authorities informed.
Other functions
In many countries, the labour inspection services are entrusted with other tasks. Conventions Nos. 81 and 129 admit this situation but specify that “any further duties which may be entrusted to labour inspectors shall not be such as to interfere with the effective discharge of their primary duties or to prejudice ...the authority and impartiality which are necessary to inspectors in their relations with employers and workers”.
The economic field
Economic and social questions are often closely linked. Owing to the contacts it maintains with the world of labour and the information it collects in the normal course of its work, the labour inspection service possesses a large amount of information of a social nature (occupational safety and health, the position of women workers and young workers, the state of labour relations, the conclusion and signature of collective agreements) or economic nature (number of enterprises, numerical strength of staff, hours of work carried out, average wages paid in different sectors of activity, requirements in skilled labour in the various economic sectors or geographic regions, and so on).
It is not surprising that the authorities in many countries have considered making use of so valuable a source of information, in particular in drawing up development plans. The labour inspectorate, by its nature objective and serious, can certainly supply such information and thus contribute to the administration and development of the country.
Labour relations: conciliation and arbitration
The international Conventions make no provision for either conciliation or arbitration to be entrusted to the labour inspection services. The Labour Inspection Recommendation, 1947 (No. 81), however, explicitly excludes them, for, by carrying them out, labour inspectors risk their independence and impartiality. Conciliation and arbitration are thus not dealt with here. In many countries, however, these functions, particularly conciliation, are in fact entrusted to the labour inspection services. Since the adoption of Recommendation No. 81 in 1947, this question has always given rise to discussion. The Labour Inspection (Agriculture) Recommendation, 1969 (No. 133), moreover, is less definite than Recommendation No. 81, for it accepts the participation of labour inspectors in the settlement of labour disputes, as a temporary measure, where no special bodies exist for the purpose of conciliation.
Protection of workers’ representatives
The Workers’ Representatives Convention, 1971 (No. 135), which is supplemented by Recommendation No. 143 of the same year, provides that
Workers’ representatives in the undertaking shall enjoy effective protection against any act prejudicial to them, including dismissal, based on their status or activities as a workers’ representative or on union membership or participation in union activities, in so far as they act in conformity with existing laws or collective agreements or other jointly agreed arrangements.
Some countries require employers to obtain union agreement or a court authorization before they can dismiss a workers’ representative. In other countries, including France and the countries in the French administrative tradition, the dismissal of shop stewards or elected staff representatives is subject to authorization by the labour inspection service (unless the works council is in agreement, needless to say an extremely rare occurrence). In making their decisions labour inspectors must try to establish whether faults imputed by employers to the workers’ representatives are or are not linked to their union activities, as defined by law and precedent. If so, they will reject the dismissal; if not, they will allow it (provided, of course, that the charges against the persons concerned are sufficiently serious).
Supervision in the field of employment
In many countries, especially those following the French administrative system, labour inspection services play an important role in the field of employment, particularly in checking terminations of employment. In France, in the event of a request for mass terminations, the labour inspection officials have the task of checking the way in which the consultation procedure has been followed, the validity of the reasons given to justify the terminations and the extent of the measures to be taken for resettlement and compensation. After examining the financial position of the enterprise or the employment market, the labour inspector can in theory refuse the terminations (in fact, this appears to happen in only about 5% of cases).
Still in the field of employment, labour inspectors are often mandated to ensure that the principle of non-discrimination is observed during recruitment or termination (prohibition of any discrimination based on such factors as race, sex, religion, political opinion, nationality and family situation). They supervise the activities of temporary employment agencies to prevent the negative effects that the development of precarious forms of employment, in particular temporary work, may have on wage earners. The economic problems and unemployment prevailing in many countries lead to increased supervision relating to the struggle against clandestine employment and the regulation of foreign labour or overtime, for example.
Miscellaneous functions
Labour inspection can be entrusted with tasks other than those mentioned above, such as keeping a watch on the protection of the environment against pollution from enterprises, or on fire prevention in premises open to the public. These functions, which sometimes only the labour inspection service is in a position to fulfil, do not come directly within its province and they must not interfere with its main functions of protecting workers in the enterprise.
The Different Systems of Inspection
Labour inspection services differ from country to country, but it is possible to distinguish two main systems: those that cover all sectors of activity and those that have specialized departments for each sector (mining, agriculture, manufacturing, transport and so on). The purpose of inspection may also vary with the inspection service: safety and health, working conditions, wages and labour relations. A distinction may similarly be made between systems whose officials enforce the statutory provisions in all the fields covered and those that have sections specialized in accordance with the purpose of inspection. In some countries, certain tasks of inspection are entrusted to local communities, and countries with a mining industry generally have a special system for this sector.
Structure of the systems
Competence as regards the sector of activity
In some countries, there is a single labour inspection system competent for all sectors of economic activity. If mining, which in almost all countries comes under the corresponding ministry (there are exceptions: Mexico, for example), is disregarded, this system is found in European countries such as Luxembourg, Spain or Switzerland. It is also found in many African and Asian countries. The French-speaking countries of Africa, for example, have inspection systems that come under the ministry of labour and cover all branches of activity.
The advantage of this system is that it gives the inspectorate and, above it, the ministry of labour a general view of the different sectors, the problems of protecting wage earners often being similar. Moreover, in countries with limited resources, this system makes it possible to reduce the number of visits needed to supervise different activities. In other countries, a specialized inspection service exists for each sector of activity, coming under the ministry concerned.
At the end of the nineteenth century, most European countries had a body to deal with questions of labour legislation, generally attached to a ministry, such as the ministry of the interior or the ministry of industry and commerce. In the years preceding the First World War, autonomous ministries of labour were established with the task of enforcing the labour legislation through a specialized public administration. This explains why, in certain branches of activity, supervising the observance of the laws protecting workers has remained among the functions of the ministerial department previously competent.
Between these two extremes—a single inspection system under one ministry competent to deal with all sectors of activity and many specialized sectoral services coming under several ministries—there are intermediate systems in which one inspection service deals with a few sectors only, or several inspection services come under one and the same ministry.
For several years a trend has been developing towards grouping the inspection services under the control of a single authority, generally the ministry of labour, both because the problems that arise in most of the sectors are very similar if not identical and because this makes for more efficient and more economical administration. A unified and integrated system increases the opportunities open to the government in the prevention of occupational hazards and the legal protection of the workers.
In 1975, France unified the main inspection services, the whole of the inter-ministerial body thus established being governed by identical conditions of service, coming under the Ministry of Labour. In 1975, the United Kingdom also decided to group its health and safety inspection services (there had been seven separate services under five different ministries) under the Health and Safety Executive. With the creation of this Executive, the Factory Inspectorate, the other inspection services (and successively even those for the exploitation of offshore oil and gas and public transport), the Employment Medical Advisory Service and other official bodies carrying out work in prevention all became part of a single institution responsible to a single ministry, the Department of Employment. (However, this Department was dissolved in 1995, and labour inspection now comes under the Department of Environment, a trend that can also be observed in other countries—e.g., Germany.) The concern to coordinate efforts in prevention and in the improvement of working conditions in the face of increasingly complicated legislation has also led other countries to entrust the supervision of the effect given to the laws on labour protection to a single inspection body, generally coming under the ministry of labour.
Competence as regards the purpose of inspection
The labour inspection services are responsible for ensuring that the legal provisions are observed in many fields: health and safety, working conditions, wages and labour relations.
In certain countries—for example, Belgium, Italy and the United Kingdom—the inspection system includes services specialized in accordance with the purpose of inspection. In Belgium, there are the following services: a technical inspectorate for prevention and safety in the enterprise; a medical inspectorate, dealing with health and hygiene; an inspectorate concerned with social legislation, dealing with conditions of employment (wages, hours of work and so on); an inspectorate to supervise the payment of social contributions; and officials dealing with questions of labour relations. In systems of this type, although the different services are specialized in particular fields, they are generally competent for all economic sectors.
The specialization of labour inspectors is an attempt to respond to the increasing complexity of the tasks of inspection. Advocates of specialization hold that an inspector cannot possess enough knowledge to deal with all the problems of workers’ protection. Specialization is such in certain countries that working conditions, in the broad sense of the term, can come under four or five types of inspection in the same enterprise.
Other countries, however, have a single system under which officials are competent for all questions relating to labour inspection. This is the situation in Austria, Germany and the French-speaking countries of Africa, for example; the latter, for obvious reasons, did not embark on the costly organization of several specialized bodies and thus have a single inspectorate under the ministry of labour. In such cases, the inspectorate is responsible for all the tasks that have to be carried out in the enterprise, the inspector or supervisor being the only representative of the ministry to deal with it.
This system has the advantage of giving inspectors a comprehensive view of labour problems, which are often interdependent, and avoids a proliferation of inspections and a lack of coordination; but it may be wondered how far inspectors can carry out so extensive a programme in view of the increasing complexity of the legal and technical problems.
There is an intermediate solution, consisting in a system under which labour inspectors are competent in many fields but have sufficient technical knowledge to recognize danger situations and call in specialists in medicine, engineering and chemistry, as provided by Convention No. 81. This is the situation in France. Another example is provided by the United Kingdom, where the general inspectors in the field of safety and health call upon inspectors who are specialists in the very technical branches (electricity, chemistry, atomic energy) when particular problems arise. Labour inspection then has a tendency to become multidisciplinary; in Denmark and other Nordic countries, as well as the Netherlands, it has actually become multidisciplinary, with district inspection teams made up of inspectors (who have received technical training), engineers, physicians, psychologists, lawyers and ergonomists. The introduction of multidisciplinary teams allows the coordinators to have a general view of the various aspects of working conditions and to base their decisions on a synthesis of the opinions expressed. The cost of such an organization is high, but it is very effective, provided that the work of the various specialists is satisfactorily coordinated.
The bringing together of established inspection services in a number of countries, or at least the closer coordination of their activities, may be explained by the close relations between the different aspects of working conditions. Such measures meet the wishes both of the officials responsible for supervision and of the workers and unions. Workers grappling with difficulties do not see why they should have to get in touch with several officials, each competent to deal with a different aspect of the problem, and to explain their situation repeatedly, perhaps with a great waste of their working time. The concern of the unions is to improve the effectiveness of labour inspection and to facilitate contacts between it and their members.
Functions of Local Communities
A few States still call upon local communities either to help the labour inspection services carry out their tasks or even to perform inspection functions in the place of the state services.
For instance, in Sweden, the Working Environment Act of 19 December 1977 entrusted the enforcement of its provisions and of the regulations issued under it to the Workers’ Protection Board and to the labour inspection service, under the supervision and direction of this Board. The Act calls on each commune, in consultation with the labour inspection service, to appoint one or more supervision officers to assist the inspection service in carrying out its task, generally by supervising enterprises employing fewer than ten persons and not using machinery. All communes have to submit an annual report to the inspection service on the way in which this supervision has been exercised.
Notably in Italy, the law of 23 December 1978 to reform the health system decentralized responsibility for public health, including occupational hygiene and safety, to the regional and local health authorities. The local health units, designated by the communal authorities, deal with everything concerning public health: hospital administration, organization of local health services, health and safety in enterprises and so on. This reform thus withdraws from the labour inspection service, a state service coming under the Ministry of Labour, the function for which it was originally established.
The transfer of the functions formerly carried out by the labour inspection service in safety and health to local health units has resulted in the creation of two labour inspection services: one coming under the Ministry of Labour, which continues to supervise the application of the social laws and regulations (wages, hours of work, paid leave and so on) and to carry out a few tasks related to safety and health (verification of ionizing radiations, supervision of the railways in collaboration with railway officials and so on) and another competent to deal with most safety and health questions, which is an integral part of the National Health Service and is based on municipal bodies, namely local health units.
In Uganda, a major decentralization drive has also brought the labour inspectorate, though not the factory inspectorate, under the direct responsibility of the local (district) authorities. These few examples are, however, exceptions and do not constitute the rule. They also raise serious doubt as to compatibility with important standards in the relevant ILO Conventions (notably Convention No. 81, Article 4), which stipulate that labour inspection should be placed under a central authority.
Labour Inspection in Mines
Almost all countries with a mining industry have an inspection system for this sector based on the system that has been operating for several generations in the old mining countries of Europe—Belgium, France, the Federal Republic of Germany and the United Kingdom.
The existing systems have two major characteristics in common. While the supervision of working conditions on the surface remains the province of the labour inspectorate, the inspection of safety and health underground, except in a few countries (for example, Mexico), is the responsibility of the mining engineers, who form a specialized body. Furthermore, all these systems associate miners’ delegates, more or less closely and with varying powers, in labour inspection at the worksite.
Powers and Duties of Labour Inspectors
Powers
Right of free entry and investigation
The first power of the inspector—without which there would obviously be little inspection—is that of visiting enterprises. The provisions of Convention No. 81 (repeated in Convention No. 129, which applies to agriculture) regarding this power are as follows:
Labour inspectors provided with proper credentials shall be empowered:
(1)to enter freely and without previous notice at any hour of the day or night any workplace liable to inspection;
(2)to enter by day any premises which they may have reasonable cause to believe to be liable to inspection.
During the drafting of the international standards, there was a great deal of opposition to the institution of the right to enter workplaces. Obstacles have not been lacking either to the incorporation of this right in national laws. In particular, it was argued that it was an unacceptable breach of the right of ownership. The possibility of entering establishments at any time was the subject of special resistance, but it is quite obvious that inspectors can establish the illegal employment of workers, where it exists, only by carrying out verifications at unusual hours. In practice, the right of entry is normal in all countries with inspection services.
This issue (and others related to powers of inspection) was again the subject of intense debate at the 1995 Session of the International Labour Conference, which dealt with the issue of labour inspection in the non-commercial services sector. The Conference adopted a “Protocol to extend Convention No. 81” to that sector, and essentially reaffirmed the fundamental powers of inspectors, while allowing for certain exceptions and restrictions, for instance for national security reasons or in the light of specific operational exigencies, for workplaces under the authority of the armed services, police services, prison services, fire and other rescue services, and so on (see Articles 2 to 4 of the 1995 Protocol in ILO 1996).
Under Conventions Nos. 81 and 129, inspectors must be authorized “to carry out any examination, test or enquiry which they may consider necessary in order to satisfy themselves that the legal provisions are being strictly observed”, which implies, in the words of the two instruments, the right to interrogate, alone or in the presence of witnesses, the employer or the staff, the right to require the production of any books, registers or other documents the keeping of which is prescribed by national laws or regulations, and the right to take samples for purposes of analysis. These rights are generally recognized, although in certain countries restrictions may be imposed on the consultation of financial documents.
It thus seems that, with rare exceptions, the supervising powers of inspectors are accepted and no longer meet with flat opposition. The possibility of calling in the police, which is provided for in most laws, is no doubt a sufficient deterrent, provided effective procedure to this end has been established between the different ministries concerned.
These powers, of course, are subject to the same limitations as any others. If exercised indiscriminately, they could ultimately produce a result opposite to that desired. These rights are accorded to inspectors so that they may exercise them intelligently and, as experience has shown, their ability to do so depends largely on the quality of their training.
Powers of injunction
Convention No. 81 states that “Labour inspectors shall be empowered to take steps with a view to remedying defects observed in plant, layout or working methods which they may have reasonable cause to believe constitute a threat to the health or safety of the workers”. This provision is repeated in almost the same words in Convention No. 129, which also covers the use of dangerous substances, because, no doubt, of the increasingly widespread use of chemicals in agriculture.
If labour inspection were devoid of the means to rectify irregular situations found in enterprises, its effectiveness would obviously be limited. It is largely by the real extent of these powers, the manner in which they are carried out and the consequences of the warnings and orders that the effectiveness of the inspection services can be gauged.
Though the two Conventions as well as the Protocol stress the importance in principle of the powers of injunction, they both leave governments a certain latitude. After providing that inspectors “shall be empowered to make or to have made orders” requiring the necessary measures to be taken, alterations to be carried out within a specified time limit, or measures with immediate executory force—they go on to provide that where this procedure is not compatible with the administrative or judicial practice of the State, inspectors can “apply to the competent authority for the issue of orders or for the initiation of measures with immediate executory force”. Account had to be taken of the impossibility, under the constitutions of certain States, of entrusting such powers to an administrative authority. The powers of the inspectors thus tend to vary from country to country even in those States that have ratified ILO Convention No. 81.
With a view to “remedying defects observed”, the inspector can either draft an order allowing the employer a specified period in which to rectify matters or require immediate measures to be taken in the event of imminent danger. The latter power is available to inspectors in more and more countries: mention may be made of Belgium, the Federal Republic of Germany, Japan, the United Kingdom, the Scandinavian countries, South Africa and many others that have reformed their occupational safety and health legislation in the 1980s and early 1990s. In other countries, such measures may still have to be ordered by the courts; but the time it takes for the court to give its decision and for that decision to be executed causes a delay during which an accident may happen. Furthermore, judges in civil courts are often not specially trained in labour protection matters, and are often found to be insensitive to violations; fines tend to be low; and these and many other factors which tend to undermine the authority of the inspectorates have reinforced the trend away from court proceedings for even minor violations including criminal proceedings to administrative proceedings over which the inspectorates have more effective control. To reduce this delay, certain countries have instituted an emergency procedure that allows the inspector to apply to the presiding judge at any time, even at home, for an order with immediate executory force.
Right of appeal
It is obvious that the mandatory decisions taken by the inspector are generally subject to a right of appeal by the employer, for provision should be made for the prevention or rectification of all possible abuses. Appeals, as a rule, are suspensory in respect of orders with a time limit, but non-suspensory in respect of orders with immediate executory force, in view of the imminent danger they are aimed at.
Action taken on infringements
“Persons who violate or neglect to observe legal provisions enforceable by labour inspectors shall be liable to prompt legal proceedings without previous warning.” This strict principle laid down in Convention No. 81 and repeated in Convention No. 129 is, nevertheless, tempered in two ways. Firstly, “exceptions may be made by national laws or regulations in respect of cases in which previous notice to carry out remedial or preventive measures is to be given”. Secondly, “it shall be left to the discretion of labour inspectors to give warning and advice instead of instituting or recommending proceedings”.
The second of these provisions gives inspectors complete freedom of choice. In each case, they must determine what means—advice, warning or legal proceedings—will best ensure that the law is observed. The choice must fit in with a plan that they have specially adapted to the nature of the enterprise and with a sequence of aims arranged in order of importance.
If inspectors decide on legal proceedings, they can either place the matter before the courts themselves (as in countries in the British administrative tradition) or recommend legal proceedings to the public prosecutor or the judiciary (this is the most common situation). Labour inspectors then draw up reports, which are treated as authentic, depending on the country, either until they are disproved or until their authenticity is challenged before the courts.
Conventions Nos. 81 and 129 state that “adequate penalties for violations of the legal provisions ...shall be provided for by national laws or regulations and effectively enforced”. While all national laws provide penalties for violations, all too often these are not “adequate”. Fines, the amount of which is often fixed when the corresponding legal provisions are adopted and remains unchanged for years, are so light as to have hardly any deterrent value. If the court pronounces imprisonment, it is generally through a suspended sentence, though the sentence may be enforced in the event of a repetition of the offence. The courts always have full discretion. Here it must be clearly recognized that the will of a government to enforce the laws and regulations protecting workers can be judged by the weight of the penalties prescribed and the way in which they are applied by the courts.
Opposition to the performance of the tasks of labour inspection or contestation of the authority of the State is generally severely punished by national laws and regulations, which in addition must provide for the possibility of calling in the police force. In fact, it is rare for heads of enterprise to practise obstructive tactics.
Obligations
Impartiality
In the words of Conventions Nos. 81 and 129, labour inspectors “shall be prohibited from having any direct or indirect interest in the undertakings under their supervision”. In most countries, this prohibition is set out in the conditions of service for civil servants and in special provisions.
Professional secrecy
Inspectors “shall be bound on pain of appropriate penalties or disciplinary measures not to reveal, even after leaving the service, any manufacturing or commercial secrets or working processes which may come to their knowledge in the course of their duties”. Inspectors are generally bound to secrecy because of their status as civil servants, in accordance with the legal provisions applicable to the civil service. This obligation is often included in the written undertaking that they have to sign or the oath that they have to swear on taking up their duties. They promise to observe secrecy, not only for the period of their employment, but for life.
Discretion regarding the source of complaints
Inspectors “shall treat as absolutely confidential the source of any complaint, and shall give no intimation to the employer or his representative that a visit of inspection was made in consequence of the receipt of such a complaint”. This obligation arises from the dual concern to protect workers who have made complaints and to render the inspector’s work more effective. It is binding. Like the preceding obligations, it is generally the object of a legal provision or a clause in the conditions of service of inspectors and normally appears in the undertakings that they give during their swearing in.
Independence of inspectors
This entails both an obligation placed on the inspectors and a guarantee accorded them. Conventions Nos. 81 and 129 provide that “the inspection staff shall be composed of public officials whose status and conditions of service are such that they are assured of stability of employment and are independent of changes of government and of improper external influences”, such as those that certain unscrupulous heads of enterprise or certain political elements might try to exert.
Preventive Labour Inspection
At the end of the twentieth century, many institutions in the field of labour and social policy which often originated, such as labour inspection, in the nineteenth, very much concerned with and interested in the function of prevention, are undergoing profound, rapid and dramatic changes. These changes are due to a combination of internal and external factors—political, social, economic, administrative and technological. They will have a profound impact on the respective role, scope and functions of these institutions, their relationships with each other and with their principal clients as they head into the twenty-first century. It is necessary to understand and analyse the nature of these changes, the way they affect the capacity, performance, impact and relationships of the principal actors, and the social reality in which they operate.
Prevention in the context of labour protection, and the role of labour inspection in this regard, is referred to in numerous international labour standards (e.g., ILO Conventions Nos. 81, 129, 155, 174 and others). However, the instruments on labour inspection (Conventions Nos. 81 and 129, and Recommendations Nos. 81, 82 and 133), while generally conducive to and promoting principles of prevention, specifically address the issue only at the pre-workplace stage (cf. paragraphs 1 to 3 of Recommendation No. 81 and paragraph 11 of Recommendation No. 133).
Since the adoption of these labour inspection standards (of which in particular Convention No. 81 on labour inspection in commerce and industry has acquired universal character through its ratification by almost 120 ILO member States), the concept of prevention has changed substantially. To speak of prevention implies first of all a determined effort to avoid incidents, accidents, disputes, conflicts and so on. However, what has occurred and has been the subject of intervention and sanctions is much more readily documented, measured and valorized than what has been avoided. How does one measure the number and effect of accidents that did not take place? And how does one show evidence of effectiveness and efficiency as a result, and as proof of achievement?
Today, preventive orientation as a social and labour policy paradigm aims at the broad goal of enabling individuals to lead a long, productive and healthy life, and thereby also to reduce the exponentially growing costs for the different elements of social security to individuals, to enterprises and to society. Furthermore, prevention in the world of work is identified more and more not only by short-term advantages but as supporting and sustaining working capacity, productivity and quality, security of employment and so on, and is therefore increasingly seen as a decisive prerequisite for an individual to lead a dignified life in society. Prevention is thus defined as a holistic “open” or pluralistic concept aimed at avoiding a multiplicity of social, technical, medical, psychological, economic and other hazards, and whose effectiveness depends increasingly on the recognition, analysis and consideration of early indicators.
The very considerable ILO experience in cooperation with its worldwide constituents over the last decade shows that the shift from a relatively rigid concept of reactive control to one of anticipatory prevention invariably leads to substantive progress in labour administration activities and in results obtained. But this body of experience has also shown the difficulties in achieving this indispensable evolution and in maintaining its orientation against a host of diverse impeding factors.
Furthermore, for any policy of prevention to be effective requires the participation of all the parties and individuals directly concerned. It must therefore often pass through the involvement of organized social partner representatives and their commitment to any such initiatives. The pursued prevention objectives must, additionally, be fully integrated into the system of objectives of the enterprises concerned. This in turn includes the active participation, indeed leadership, of management. Such conditions are far from being fulfilled worldwide or indeed even in the most industrially advanced market economies.
Added to that, the budgetary constraints now weighing on governments everywhere (in developing and developed countries alike), and therefore on the means available to labour administrations and their field services and labour inspection (indeed often disproportionately so), risk jeopardizing or weakening any such policy (re)orientations, as they are, at least initially, costly in time and resources and, as already mentioned, difficult to measure and therefore to justify.
However, in industrialized countries the economic and social costs of non-prevention are everywhere growing out of hand, to financially unaffordable and politically unacceptable levels. To this must be added the growing recognition of the general insufficiency of corrective ex post factum intervention. This has led to the conclusion that the preventative elements of any system of social and labour protection absolutely have to be reinforced. In consequence, a broad discussion at the national and international levels has begun with a view to developing valid, practical concepts for preventive labour inspection.
The increasingly rapid pace of change and innovation in all aspects of the world of work—social relations, work organization, production technology, conditions of employment, informatics, new hazards and so on—creates a mounting challenge for labour inspectorates. Inspectors must not only keep abreast of developments in more and more complex, divergent and increasingly specialized fields necessary for their competence, they must, in fact, anticipate trends and developments and be able to rapidly identify and understand their consequences in terms of labour protection, and thus to develop and implement new strategies for prevention.
In the world of work, labour inspection is one of the most (if not the most) important instruments of state presence and intervention to design, stimulate and contribute to the development of a culture of prevention in all aspects under its purview: industrial relations, general conditions of work, occupational safety and health, social security. For inspectorates to successfully accomplish this primary task they must reorient their policies, influence reform of legislation, of methods, relations and so on towards developing a preventative capacity, internally and externally. This concerns both the policies and methods which the inspection authority must pursue, as well as the methods of inspection at workplaces to be adopted by inspectors.
Major determining factors in this context are the challenges and pressures on labour inspection from the economic, political and administrative context. These are generally described by concepts such as deregulation, privatization, structural adjustment and market testing. These policies tend in practice to make the work of labour inspection more difficult and complex, although they may also provide a driving force for innovation. They regularly, however, tend to exacerbate the usually already chronic resource deficiencies. Labour protection, therefore, must also look for alternative resources for the development of its own contribution to prevention.
Ultimately, the aim is to develop a comprehensive, sustained “prevention culture” in workplaces (and society), taking into account the dynamics of change in social relations within the enterprise, the challenges to traditional notions of authority and legitimacy which arise from changes in attitudes, in work organization and so on, the generally higher (and still rising) levels of training and education among both employers and workers, new forms of participation which create an enabling environment and so on. All these require new forms of cooperation by the labour inspectorate with employers and workers and other institutions, not only as regards enforcement of labour protection standards and regulations, but in view of achieving comprehensive compliance with the preventive objectives of new protective social and labour policy and legislation.
Institutional, Structural and Legal Resources: Introduction
National and international structures concerned with workplace health and safety have developed rapidly during the last 25 years in response to growing concerns about workers’ health. Economic, social and political changes provide the context for this development.
Amongst the economic factors have been the relocation of power away from workers into multinational enterprises and supranational legislatures, rapid changes in the relative competitiveness of different states in the world economy, and technological change in the productive process. Amongst the social factors are advance of medical knowledge with consequent raised expectations of health, and the growth of scepticism about the effects of scientific and technological advances on the environment inside and outside the workplace. The political context includes the calls for greater participation in the political process in many countries since the 1960s, the crisis in social welfare in several long-industrialized nations, and a growing sensitivity to the practices of multinationals in developing countries. Organizational structures have reflected these developments.
Workers’ organizations have taken on health and safety specialists to provide guidance to their members and negotiate on their behalf at local and national levels. There has been a rapid growth in the number of organizations of the victims of occupational disease over the last ten years, which can be seen as a response to the special hardships which they face where social welfare provisions are inadequate. Both developments have been mirrored at an international level by the increased importance given to health and safety by international trade union federations, and by international conferences of workers in particular industrial sectors. The structural and legal issues related to workers’ organizations, employers’ associations, and labour relations are discussed in a separate chapter of the Encyclopaedia.
The changes in employers’ and state organizations in recent years can be seen as partly reactive and partly pre-emptive. Law introduced in the last 25 years is in part a response to concerns expressed by workers since the late 1960s, and in part regulation of the rapid development of new technologies of production in the post-war period. Constitutional structures set up in different legislatures are of course consonant with national legislation and culture, but there are common features. These include an increase in the importance attached to prevention services and training for workers, managers and health and safety specialists, the establishment of participatory or consultative organizations at the workplace and at the national level, and the reorganization of the labour inspectorates and other state bodies concerned with enforcement. Differing mechanisms have been set up in different States for the insurance coverage provided for a worker injured or made ill by work, and for the relationship of health and safety enforcement to other state bodies concerned with employment and the environment.
Organizational changes such as these create new training requirements in the professions concerned—inspectors, safety engineers, industrial hygienists, ergonomists, occupational psychologists, doctors and nurses. Training is discussed by professional and other bodies at national and international levels, with the major professions meeting in international congresses and developing common requirements and codes of practice.
Research is an essential part of planned and reactive prevention programmes. Governments are the single largest source of research funds, which are predominantly organized into national research programmes. At the international level, there are, in addition to sections of the International Labour Organization (ILO) and the World Health Organization (WHO), research institutions such as the European Joint Safety Institute and the International Agency for Research into Cancer which carry out international programmes of research in occupational safety and health.
While the ILO, WHO and other UN organizations have had a concern with occupational health written into their statutes since the Second World War or even earlier, many international bodies concerned with occupational health date back less than 25 years. Health and safety is now a significant concern of world trade bodies and regional free trade areas, with the social consequences of trade agreements often being discussed during negotiations. The Organization for Economic and Cultural Development (OECD) evaluates health and safety practices in different countries along with purely economic performance. Prolonged debate over the inclusion of a social clause in the GATT negotiations has re-emphasized this linkage.
Acceptance of the authority of national and international organizations is essential if they are to function effectively. For legislative and enforcement bodies, this legitimacy is conferred by law. For research organizations, their authority derives from their adherence to accepted scientific procedures. However, the shift of the formulation of law and the negotiation of agreements on health and safety at work to international bodies poses problems of authority and legitimacy for other organizations such as employers’ associations and workers’ organizations.
The authority of employers comes from the social value of the services or products which they provide, whereas workers’ organizations owe their position in negotiations to the democratic structures which enable them to reflect the views of their members. Each of these forms of legitimacy is more difficult to establish for international organizations. The increased integration of the world economy is likely to bring about an ever-increasing coordination of policy in all areas of occupational safety and health, with emphasis on commonly accepted standards of prevention, compensation, professional training and enforcement. The problem of the organizations which grow up in response to these needs will be to maintain their authority through responsive and interactive relations with workers and the workplace.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."