- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Health and Safety Regulations: The Netherlands Experience
Implementation of the EC directive Minimum Regulations for Health and Safety on Temporary and Mobile Building Sites typifies the legal regulations emanating from the Netherlands and from the European Union. Their aim is to improve working conditions, to combat disability and to reduce sickness absenteeism. In the Netherlands, these regulations for the construction industry are expressed in the Arbouw Resolution, Chapter 2, Section 5.
As is often the case, the legislation seems to be following the social changes that began in 1986, when organizations of employers and employees joined to establish the Arbouw Foundation to provide services for construction companies in civil engineering and utility construction, earth works, roadbuilding and water construction and the completion sectors of the industry. Thus, the new regulations are scarcely a problem for the responsible companies already committed to implement health and safety considerations. The fact that these principles are often very difficult to put into practice, however, has led to non-observance and unfair competition and, consequently, the need for legal regulations.
Legal Regulations
The legal regulations focus on preventive measures before the construction project is started and while it is in progress. This will yield the greatest long-term benefit.
The Health and Safety Act stipulates that evaluations of risks must address not only those arising from materials, preparations, tools, equipment and so on, but also those involving special groups of workers (e.g., pregnant women, young and elderly workers and those with disabilities).
Employers are obliged to have written risk evaluations and inventories produced by certified experts, who may be employees or external contractors. The document must include recommendations for eliminating or limiting the risks and must also stipulate phases of the work when qualified specialists will be required. Some construction companies have developed their own approach to the evaluation, the General Business Investigation and Risk Inventory and Evaluation (ABRIE), which has become the prototype for the industry.
The Health and Safety Act obliges employers to offer a periodic health examination to their employees. The purpose is to identify health problems that may make certain jobs especially hazardous for some workers unless certain precautions are taken. This requirement echoes the various collective labour agreements in the construction industry which for years have required employers to provide employees with comprehensive occupational health care, including periodic medical examinations. The Arbouw Foundation has contracted with the Federation of Occupational Health and Safety Care Centres for the provision of these services. Over the years, a wealth of valuable information has been accumulated which has contributed to enhancement of the quality of the risk inventories and evaluations.
Absenteeism Policy
The Health and Safety Act also requires employers to have an absenteeism policy which includes a stipulation that experts in this field be retained to monitor and counsel disabled employees.
Joint Responsibility
Many health and safety risks can be traced to inadequacies in the building and organization choices or to poor planning of the work when setting up a project. To obviate this, the employers, employees and the government agreed in 1989 on a working conditions covenant. Among other things, it specified cooperation between clients and contractors and between contractors and subcontractors. This has resulted in a code of conduct which serves as a model for the implementation of the European directive on temporary and mobile building sites.
As part of the covenant, Arbouw formulated limits for exposure to hazardous substances and materials, along with guidelines for the application in various construction operations.
Under the leadership of Arbouw, the FNV Building Workers and Wood Workers Union, the FNV Industry Union and the Mineral Wool Association, Benelux, agreed to a contract that called for the development of glass wool and mineral wool products with less dust emission, development of the safest possible production methods for glass wool and mineral wool, formulation and promotion of working methods for the safest use of these products and performance of the research necessary to establish safe exposure limits to them. The exposure limit for respirable fibres was set at 2/cm3 although a limit of 1/cm3 was regarded as feasible. They also agreed to eliminate the use of raw and secondary materials that are health risks, using as criteria the exposure limits formulated by Arbouw. Performance under this agreement will be monitored until it expires on 1 January 1999.
Construction Process Quality
The implementation of the EC directive does not stand in isolation but is an integral part of company health and safety policies, along with quality and environmental policies. Health and safety policy is critical part of the quality policy of the companies. The laws and regulations will be enforceable only if the employers and employees of the construction industry have played a role in their development. The government has dictated the development of a model health and safety plan that is practicable and can be enforced to prevent unfair competition from companies that ignore or subvert it.
Preventive Health Services in Construction
The construction industry forms 5 to 15% of the national economy of most countries and is usually one of the three industries having the highest rate of work-related injury risks. The following chronic occupational health risks are pervasive (Commission of the European Communities 1993):
- Musculoskeletal disorders, occupational hearing loss, dermatitis and lung disorders are the most common occupational diseases.
- An increased risk of respiratory tract carcinomas and mesothelioma caused by asbestos exposure has been observed in all countries where occupational mortality and morbidity statistics are available.
- Disorders resulting from improper nutrition, smoking or use of alcohol and drugs are associated especially with migrant workers, a substantial portion of construction employment in many countries.
Preventive health services for construction workers should be planned with these risks as priorities.
Types of Occupational Health Services
Occupational health services for construction workers consist of three main models:
- specialized services for construction workers
- occupational health care for construction workers rendered by providers of broad-based occupational health services
- health services provided voluntarily by the employer.
Specialized services are the most effective but also the most expensive in terms of direct costs. Experiences from Sweden indicate that the lowest injury rates on construction sites worldwide and a very low risk for occupational diseases among construction workers are associated with extensive preventive work through specialized service systems. In the Swedish model, called Bygghälsan, technical and medical prevention have been combined. Bygghälsan operates through regional centres and mobile units. During the severe economic recession of the late 1980s, however, Bygghälsan severely cut back its health service activities.
In countries that have occupational health legislation, construction companies usually buy the needed health services from companies serving general industries. In such cases, the training of occupational health personnel is important. Without special knowledge of the circumstances surrounding construction, medical personnel cannot provide effective preventive occupational health programmes for construction companies.
Some large multinational companies have well-developed occupational safety and health programmes that are part of the culture of the enterprise. The cost-benefit calculations have proved these activities economically profitable. Nowadays, occupational safety programmes are included in quality management of most international companies.
Mobile health clinics
Because construction sites are often situated far from any established providers of health services, mobile health service units may be necessary. Practically all countries that have specialized occupational health services for construction workers use mobile units for delivering the services. The mobile unit’s advantage is the saving of work time by bringing the services to worksites. Mobile health centres are contained in a specially equipped bus or trailer and are especially suitable for all types of screening procedures, such as periodic health examinations. Mobile services should be careful to arrange in advance for collaboration with local providers of health services in order to secure follow-up evaluation and treatment for workers whose test results suggest a health problem.
Standard equipment for a mobile unit includes a basic laboratory with a spirometer and an audiometer, an interview room and x-ray equipment, when needed. It is best to design module units as multipurpose spaces so they can be used for different types of projects. The Finnish experience indicates that mobile units are also suitable for epidemiological studies, which can be incorporated into occupational health programmes, if properly planned in advance.
Contents of preventive occupational health services
Identification of risk at construction sites should guide medical activity, although this is secondary to prevention through proper design, engineering and work organization. Risk identification requires a multidisciplinary approach; this requires close collaboration between the occupational health personnel and the enterprise. A systematic workplace survey of risks using standardized checklists is one option.
Preplacement and periodic health examinations are usually conducted according to requirements set by legislation or guidance provided by authorities. The examination’s content depends on the exposure history of each worker. Short work contracts and frequent turnover of the construction workforce can result in “missed” or “inappropriate” health examinations, a failure to follow up on findings or unwarranted duplication of health examinations. Therefore, regular standard periodic examinations are recommended for all workers. A standard health examination should contain: an exposure history; symptom and illness histories with special emphasis on musculoskeletal and allergic diseases; a basic physical examination; and audiometry, vision, spirometry and blood pressure tests. The examinations should also provide health education and information on how to avoid occupational risks known to be common.
Surveillance and Prevention of Key Construction-related Problems
Musculoskeletal disorders and their prevention
Musculoskeletal disorders have multiple origins. Lifestyle, hereditary susceptibility and ageing, combined with improper physical strain and minor injuries, are commonly accepted risk factors for musculoskeletal disorders. The types of musculoskeletal problems have different exposure patterns in different construction professions.
There is no reliable test to predict an individual’s risk for acquiring a musculoskeletal disorder. Medical prevention of musculoskeletal disorders is based on guidance in ergonomic matters and lifestyles. Preplacement and periodic examinations can be used for this purpose. Non-specific strength testing and routine x rays of the skeletal system have no specific value for prevention. Instead, early detection of symptoms and a detailed work history of musculoskeletal symptoms can be used as a basis for medical counselling. A programme that performs periodic symptom surveys to identify work factors that can be changed has been shown to be effective.
Often, workers who have been exposed to heavy physical loads or strain think the work keeps them fit. Several studies have proved that this is not the case. Therefore, it is important that, in the context of health examinations, the examinees be informed about proper ways to maintain their physical fitness. Smoking has also been associated with lumbar disk degeneration and low-back pain. Therefore, anti-smoking information and therapy should be included in the periodic health examinations, too (Workplace Hazard and Tobacco Education Project 1993).
Occupational noise-induced hearing loss
The prevalence of noise-induced hearing loss varies among construction occupations, depending on levels and duration of exposure. In 1974, less than 20% of Swedish construction workers at age 41 had normal hearing in both ears. Implementation of a comprehensive hearing conservation programme increased the proportion in that age group having normal hearing to almost 40% by the late 1980s. Statistics from British Columbia, Canada, show that construction workers generally suffer significant loss of hearing after working more than 15 years in the trades (Schneider et al. 1995). Some factors are thought to increase susceptibility to occupational hearing loss (e.g., diabetic neuropathy, hypercholesterolemia and exposure to certain ototoxic solvents). Whole-body vibration and smoking may have an additive effect.
A large-scale programme for hearing conservation is advisable for the construction industry. This type of programme requires not only collaboration at the worksite level, but also supportive legislation. Hearing conservation programmes should be specific in work contracts.
Occupational hearing loss is reversible in the first 3 or 4 years after initial exposure. Early detection of hearing loss will provide opportunities for prevention. Regular testing is recommended to detect the earliest possible changes and to motivate workers to protect themselves. At the time of testing, the exposed workers should be educated in the principles of personal protection, as well as the maintenance and proper use of protection devices.
Occupational dermatitis
Occupational dermatitis is prevented mainly by hygienic measures. The proper handling of wet cement and skin protection are effective in promoting hygiene. During health examinations, it is important to stress the importance of avoiding skin contact with wet cement.
Occupational lung diseases
Asbestosis, silicosis, occupational asthma and occupational bronchitis can be found among construction workers, depending on their past work exposures (Finnish Institute of Occupational Health 1987).
There is no medical method to prevent the development of carcinomas after someone has been sufficiently exposed to asbestos. Regular chest x rays, every third year, are the most common recommendation for medical surveillance; there is some evidence that x-ray screening improves the outcome in lung cancer (Strauss, Gleanson and Sugarbaker 1995). Spirometry and anti-smoking information are usually included in the periodic health examination. Diagnostic tests for the early diagnosis of asbestos-related malignant tumours are not available.
Malignant tumours and other lung diseases related to asbestos exposure are widely underdiagnosed. Therefore, many construction workers eligible for compensation remain without benefits. In the late 1980s and early 1990s, Finland conducted a nationwide screening of workers exposed to asbestos. The screening revealed that only one-third of the workers with asbestos-related diseases and who had access to occupational health services had been diagnosed earlier (Finnish Institute of Occupational Health 1994).
Special needs of migrant workers
Depending on the construction site, the social context, sanitary conditions and climate may present important risks to construction workers. Migrant workers often suffer from psychosocial problems. They have a higher risk of work-related injuries than native workers. Their risk of carrying infectious diseases, such as HIV/AIDS, tuberculosis, and parasitic diseases must be taken into account. Malaria and other tropical diseases are problems for workers in areas where they are endemic.
In many large construction projects, a foreign workforce is used. A preplacement medical examination should be conducted in the home country. Also, the spreading of contagious diseases must be prevented through proper vaccination programmes. In the host countries, proper vocational training, health and safety education, and housing should be organized. Migrant workers should be provided the same access to health care and social security as native workers (El Batawi 1992).
In addition to preventing construction-related ailments, the health practitioner should work to promote positive changes in lifestyle, which can improve a worker’s health overall. Avoiding alcohol and smoking are the most important and fruitful themes for health promotion for construction workers. It has been estimated that a smoker costs the employer 20 to 30% more than a non-smoking worker. Investments in anti-smoking campaigns pay not only in the short term, with lower accident risks and shorter sick leaves, but also in the long term, with lower risks of cardiovascular pulmonary diseases and cancer. In addition, tobacco smoke has harmful multiplier effects with most dusts, especially with asbestos.
Economic benefits
It is difficult to prove any direct economic benefit of occupational health services to an individual construction company, especially if the company is small. Indirect cost-benefit calculations show, however, that accident prevention and health promotion are economically beneficial. Cost-benefit calculations of investments in preventive programmes are available for companies to use internally. (For a model used extensively in Scandinavia, see Oxenburg 1991.)
Health Risks of Underground Construction Work
Hazards
Underground construction work includes tunnelling for roads, highways and railroads and laying pipelines for sewers, hot water, steam, electrical conduits, telephone lines. Hazards in this work include hard physical labour, crystalline silica dust, cement dust, noise, vibration, diesel engine exhaust, chemical vapours, radon and oxygen-deficient atmospheres. Occasionally this work must be done in a pressurized environment. Underground workers are at risk for serious and often fatal injuries. Some hazards are the same as those of construction on the surface, but they are amplified by working in a confined environment. Other hazards are unique to underground work. These include being struck by specialized machinery or being electrocuted, being buried by roof falls or cave-ins and being asphyxiated or injured by fires or explosions. Tunnelling operations may encounter unexpected impoundments of water, resulting in floods and drowning.
The construction of tunnels requires a great deal of physical effort. Energy expenditure during manual work is usually from 200 to 350 W, with a great part of static load of the muscles. Heart rate during work with compressed-air drills and pneumatic hammers reaches 150 to 160 per minute. Work is often done in unfavourable cold and humid microclimatic conditions, sometimes in cumbersome work postures. It is usually combined with exposure to other risk factors which depend on the local geological conditions and on the type of technology used. This heavy workload can be an important contribution to heat stress.
The need for heavy manual labour can be reduced by mechanization. But mechanization brings its own hazards. Large and powerful mobile machines in a confined environment introduce risks of serious injury to persons working nearby, who may be struck or crushed. Underground machinery also may generate dust, noise, vibration and diesel exhaust. Mechanization also results in fewer jobs, which reduces the number of persons exposed but at the expense of unemployment and all of its attendant problems.
Crystalline silica (also known as free silica and quartz) occurs naturally in many different types of rock. Sandstone is practically pure silica; granite may contain 75%; shale, 30%; and slate, 10%. Limestone, marble and salt are, for practical purposes, completely free of silica. Considering that silica is ubiquitous in the earth’s crust, dust samples should be taken and analysed at least at the start of an underground job and whenever the type of rock changes as work progresses through it.
Respirable silica dust is generated whenever silica-bearing rock is crushed, drilled, ground or otherwise pulverized. The main sources of airborne silica dust are compressed-air drills and pneumatic hammers. Work with these tools most often occurs in the fore part of the tunnel and, therefore, workers in these areas are the most heavily exposed. Dust suppression technology should be applied in all instances.
Blasting generates not only flying debris, but also dust and nitrogen oxides. To prevent excessive exposure, the customary procedure is to prevent re-entry to the affected area until the dust and gases have cleared. A common procedure is to blast at the end of the last work shift of the day and to clear out debris during the next shift.
Cement dust is generated when cement is mixed. This dust is a respiratory and mucous membrane irritant in high concentrations, but chronic effects have not been observed. When it settles on skin and mixes with sweat, however, cement dust can cause dermatoses. When wet concrete is sprayed in place, it too can cause dermatoses.
Noise can be significant in underground construction work. Principal sources include pneumatic drills and hammers, diesel engines and fans. Since the underground work environment is confined, there is also considerable reverberant noise. Peak noise levels can exceed 115 dBA, with time-weighted average noise exposure equivalent to 105 dBA. Noise-reducing technology is available for most equipment and should be applied.
Underground construction workers can also be exposed to whole-body vibration from mobile machinery and to hand-arm vibration from pneumatic drills and hammers. The levels of acceleration transmitted to the hands from pneumatic tools can reach about 150 dB (comparable to 10 m/s2). Harmful effects of hand-arm vibration can be aggravated by a cold and damp working environment.
If soil is highly saturated with water or if construction is conducted under water, the work environment may have to be pressurized to keep water out. For underwater work, caissons are used. When workers in such a hyperbaric environment make too rapid a transition to normal air pressure, they risk decompression sickness and related disorders. Since the absorption of most toxic gases and vapours depends on their partial pressure, more may be absorbed at higher pressure. Ten ppm of carbon monoxide (CO) at 2 atmospheres of pressure, for example, will have the effect of 20 ppm CO at 1 atmosphere.
Chemicals are used in underground construction in a variety of ways. For example, insufficiently coherent layers of rock may be stabilized with an infusion of urea formaldehyde resin, polyurethane foam or mixtures of sodium water glass with formamide or with ethyl and butyl acetate. Consequently, vapours of formaldehyde, ammonia, ethyl or butyl alcohol or di-isocyanates may be found in the tunnel atmosphere during application. Following application, these contaminants may escape into the tunnel from the surrounding walls, and it may therefore be difficult to fully control their concentrations, even with intensive mechanical ventilation.
Radon occurs naturally in some rock and may leak into the work environment, where it will decay into other radioactive isotopes. Some of these are alpha emitters that may be inhaled and increase the risk of lung cancer.
Tunnels constructed in inhabited areas can also be contaminated with substances from surrounding pipes. Water, heating and cooking gas, fuel oil, petrol and so on may leak into a tunnel or, if pipes carrying these substances are broken during excavation, they may escape into the work environment.
The construction of vertical shafts using mining technology poses similar health problems to those of tunnelling. In terrain where organic substances are present, products of microbiological decomposition may be expected.
Maintenance work in tunnels used for traffic differs from similar work on the surface mainly in the difficulty of installing safety and control equipment, for example, ventilation for electric arc welding; this may influence the quality of safety measures. Work in tunnels in which pipelines for hot water or steam are present is associated with great heat load, demanding a special regime of work and breaks.
Oxygen deficiency may occur in tunnels either because oxygen is displaced by other gases or because it is consumed by microbes or by the oxidation of pyrites. Microbes may also release methane or ethane, which not only displace oxygen but, in sufficient concentration, may create the risk of explosion. Carbon dioxide (commonly called blackdamp in Europe) is also generated by microbial contamination. The atmospheres in spaces which have been closed for a long time may contain mostly nitrogen, practically no oxygen and 5 to 15% carbon dioxide.
Blackdamp penetrates into the shaft from the surrounding terrain due to changes in the atmospheric pressure. The composition of the air in the shaft may change very quickly—it may be normal in the morning, but be deficient in oxygen by the afternoon.
Prevention
Prevention of exposure to dust should in the first place be implemented by technical means, such as wet drilling (and/or drilling with LEV), wetting of the material before it is pulled down and loaded to the transport, LEV of mining machines and mechanical ventilation of tunnels. Technical control measures may not be sufficient to lower the concentration of respirable dust to an acceptable level in some technological operations (e.g., during drilling and sometimes also in the case of wet drilling), and therefore it may be necessary to supplement the protection of the workers engaged in such operations by the use of respirators.
The efficiency of technical control measures must be checked by monitoring the concentration of airborne dust. In the case of fibrogenic dust, it is necessary to arrange the programme of monitoring in such a way that it allows the registration of the exposure of individual workers. The individual exposure data, in connection with data about each worker’s health, are necessary for the assessment of the risk of pneumoconiosis in particular work conditions, as well as for the assessment of the efficiency of control measures in the long-run. Last but not least, the individual registration of exposure is necessary for evaluating the ability of individual workers to continue in their jobs.
Due to the nature of underground work, protection against noise depends mostly on the personal protection of hearing. Effective protection against vibrations, on the other hand, can be achieved only by eliminating or decreasing the vibration by mechanization of risky operations. PPE is not effective. Similarly, the risk of diseases due to physical overload of the upper extremities can be lowered only by mechanization.
Exposure to chemical substances can be influenced by the selection of appropriate technology (e.g., the use of formaldehyde resins and formamide should be eliminated), by good maintenance (e.g., of diesel engines) and by adequate ventilation. Organization and work regime precautions are sometimes very effective, especially in the case of the prevention of dermatoses.
Work in underground spaces in which the composition of the air is not known demands strict adherence to safety rules. Entering such spaces without isolating breathing apparatuses must not be allowed. The work should be done only by a group of at least three people—one worker in the underground space, with breathing apparatus and safety harness, the others outside with a rope to secure the inside worker. In case of accident it is necessary to act quickly. Many lives have been lost in efforts to save the victim of an accident when the safety of the rescuer was disregarded.
Pre-placement, periodic and post-employment preventive medical examinations are a necessary part of the health and safety precautions for workers in tunnels. The frequency of periodic examinations and the type and scope of special examinations (x ray, lung functions, audiometry and so on) should be individually determined for each workplace and for each job according to the working conditions.
Prior to groundbreaking for underground work, the site should be inspected and soil samples should be taken in order to plan the excavation. Once work is underway, the work site should be inspected daily to prevent roof falls or cave-ins. The workplace of solitary workers should be inspected at least twice each shift. Fire suppression equipment should be strategically placed throughout the underground work site.
Health and Safety Hazards in the Construction Industry
Construction workers build, repair, maintain, renovate, modify and demolish houses, office buildings, temples, factories, hospitals, roads, bridges, tunnels, stadiums, docks, airports and more. The International Labour Organization (ILO) classifies the construction industry as government and private-sector firms erecting buildings for habitation or for commercial purposes and public works such as roads, bridges, tunnels, dams or airports. In the United States and some other countries, construction workers also clean hazardous waste sites.
Construction as a proportion of gross domestic product varies widely in industrialized countries. It is about 4% of GDP in the United States, 6.5% in Germany and 17% in Japan. In most countries, employers have relatively few full-time employees. Many companies specialize in skilled trades—electricity, plumbing or tile setting, for instance—and work as subcontractors.
The Construction Labour Force
A large portion of construction workers are unskilled labourers; others are classified in any of several skilled trades (see table 1). Construction workers include about 5 to 10% of the workforce in industrialized countries. Throughout the world, over 90% of construction workers are male. In some developing countries, the proportion of women is higher and they tend to be concentrated in unskilled occupations. In some countries, the work is left to migrant workers, and in others, the industry provides relatively well-paid employment and an avenue to financial security. For many, unskilled construction work is the entry into the paid labour force in construction or other industries.
Work Organization and Labour Instability
Construction projects, especially large ones, are complex and dynamic. Several employers may work on one site simultaneously, with the mix of contractors changing with the phases of the project; for example, the general contractor is present at all times, excavating contractors early, then carpenters, electricians and plumbers, followed by floor finishers, painters and landscapers. And as the work develops—for instance, as a building’s walls are erected, as the weather changes or as a tunnel advances—the ambient conditions such as ventilation and temperature change too.
Construction workers typically are hired from project to project and may spend only a few weeks or months at any one project. There are consequences for both workers and work projects. Workers must make and remake productive and safe working relationships with other workers whom they may not know, and this may affect safety at the work site. And in the course of the year, construction workers may have several employers and less than full employment. They might work an average of only 1,500 hours in a year while workers in manufacturing, for example, are more likely to work regular 40 hour weeks and 2,000 hours per year. In order to make up for slack time, many construction workers have other jobs—and exposure to other health or safety hazards—outside of construction.
For a particular project, there is frequent change in the number of workers and the composition of the labour force at any one site. This change results both from the need for different skilled trades at different phases of a work project and from the high turnover of construction workers, particularly unskilled workers. At any one time, a project may include a large proportion of inexperienced, temporary and transient workers who may not be fluent in the common language. Although construction work often must be done in teams, it is difficult to develop effective, safe teamwork under such conditions.
Like the workforce, the universe of construction contractors is marked by high turnover and consists mainly of small operations. Of the 1.9 million construction contractors in the United States identified by the 1990 Census, only 28% had any full-time employees. Just 136,000 (7%) had 10 or more employees. The degree of contractor participation in trade organizations varies by country. In the United States, only about 10 to 15% of contractors participate; in some European countries, this proportion is higher but still involves less than half of contractors. This makes it difficult to identify contractors and inform them of their rights and responsibilities under pertinent health and safety or any other legislation or regulations.
As in some other industries, an increasing proportion of contractors in the United States and Europe consists of individual workers hired as independent contractors by prime- or sub-contractors who employ workers. Ordinarily, an employing contractor does not provide subcontractors with health benefits, workers’ compensation coverage, unemployment insurance, pension benefits or other benefits. Nor do prime contractors have any obligation to subcontractors under health and safety regulations; these regulations govern rights and responsibilities as they apply to their own employees. This arrangement gives some independence to individuals who contract for their services, but at the cost of removing a wide range of benefits. It also relieves employing contractors of the obligation to provide mandated benefits to individuals who are contractors. This private arrangement subverts public policy and has been successfully challenged in court, yet it persists and may become more of a problem for the health and safety of workers on the job, regardless of their employment relationship. The US Bureau of Labor Statistics (BLS) estimates that 9% of the US workforce is self-employed, but in construction as many as 25% of workers are self-employed independent contractors.
Health Hazards on Construction Sites
Construction workers are exposed to a wide variety of health hazards on the job. Exposure differs from trade to trade, from job to job, by the day, even by the hour. Exposure to any one hazard is typically intermittent and of short duration, but is likely to reoccur. A worker may not only encounter the primary hazards of his or her own job, but may also be exposed as a bystander to hazards produced by those who work nearby or upwind. This pattern of exposure is a consequence of having many employers with jobs of relatively short duration and working alongside workers in other trades that generate other hazards. The severity of each hazard depends on the concentration and duration of exposure for that particular job. Bystander exposures can be approximated if one knows the trade of workers nearby. Hazards present for workers in particular trades are listed in table 2.
Table 2. Primary hazards encountered in skilled construction trades.
Each trade is listed below with an indication of the primary hazards to which a worker in that trade might be exposed. Exposure may occur to either supervisors or to wage earners. Hazards that are common to nearly all construction-heat, risk factors for musculoskeletal disorders and stress-are not listed.
The classifications of construction trades used here are those used in the United States. It includes the construction trades as classified in the Standard Occupational Classification system developed by the US Department of Commerce. This system classifies the trades by the principal skills inherent in the trade.
|
Occupations |
Hazards |
|
Brickmasons |
Cement dermatitis, awkward postures, heavy loads |
|
Stonemasons |
Cement dermatitis, awkward postures, heavy loads |
|
Hard tile setters |
Vapour from bonding agents, dermatitis, awkward postures |
|
Carpenters |
Wood dust, heavy loads, repetitive motion |
|
Drywall installers |
Plaster dust, walking on stilts, heavy loads, awkward postures |
|
Electricians |
Heavy metals in solder fumes, awkward posture, heavy loads, asbestos dust |
|
Electrical power installers and repairers |
Heavy metals in solder fumes, heavy loads, asbestos dust |
|
Painters |
Solvent vapours, toxic metals in pigments, paint additives |
|
Paperhangers |
Vapours from glue, awkward postures |
|
Plasterers |
Dermatitis, awkward postures |
|
Plumbers |
Lead fumes and particles, welding fumes |
|
Pipefitters |
Lead fumes and particles, welding fumes, asbestos dust |
|
Steamfitters |
Welding fumes, asbestos dust |
|
Carpet layers |
Knee trauma, awkward postures, glue and glue vapour |
|
Soft tile installers |
Bonding agents |
|
Concrete and terrazzo finishers |
Awkward postures |
|
Glaziers |
Awkward postures |
|
Insulation workers |
Asbestos, synthetic fibres, awkward postures |
|
Paving, surfacing and tamping equipment operators |
Asphalt emissions, gasoline and diesel engine exhaust, heat |
|
Rail- and track-laying equipment operators |
Silica dust, heat |
|
Roofers |
Roofing tar, heat, working at heights |
|
Sheetmetal duct installers |
Awkward postures, heavy loads, noise |
|
Structural metal installers |
Awkward postures, heavy loads, working at heights |
|
Welders |
Welding emissions |
|
Solderers |
Metal fumes, lead, cadmium |
|
Drillers, earth, rock |
Silica dust, whole-body vibration, noise |
|
Air hammer operators |
Noise, whole-body vibration, silica dust |
|
Pile driving operators |
Noise, whole-body vibration |
|
Hoist and winch operators |
Noise, lubricating oil |
|
Crane and tower operators |
Stress, isolation |
|
Excavating and loading machine operators |
Silica dust, histoplasmosis, whole-body vibration, heat stress, noise |
|
Grader, dozer and scraper operators |
Silica dust, whole-body vibration, heat noise |
|
Highway and street construction workers |
Asphalt emissions, heat, diesel engine exhaust |
|
Truck and tractor equipment operators |
Whole-body vibration, diesel engine exhaust |
|
Demolition workers |
Asbestos, lead, dust, noise |
|
Hazardous waste workers |
Heat, stress |
Construction Hazards
As in other jobs, hazards for construction workers are typically of four classes: chemical, physical, biological and social.
Chemical hazards
Chemical hazards are often airborne and can appear as dusts, fumes, mists, vapours or gases; thus, exposure usually occurs by inhalation, although some airborne hazards may settle on and be absorbed through the intact skin (e.g., pesticides and some organic solvents). Chemical hazards also occur in liquid or semi-liquid state (e.g., glues or adhesives, tar) or as powders (e.g., dry cement). Skin contact with chemicals in this state can occur in addition to possible inhalation of the vapour resulting in systemic poisoning or contact dermatitis. Chemicals might also be ingested with food or water, or might be inhaled by smoking.
Several illnesses have been linked to the construction trades, among them:
- silicosis among sand blasters, tunnel builders and rock drill operators
- asbestosis (and other diseases caused by asbestos) among asbestos insulation workers, steam pipe fitters, building demolition workers and others
- bronchitis among welders
- skin allergies among masons and others who work with cement
- neurologic disorders among painters and others exposed to organic solvents and lead.
Elevated death rates from cancer of the lung and respiratory tree have been found among asbestos insulation workers, roofers, welders and some woodworkers. Lead poisoning occurs among bridge rehabilitation workers and painters, and heat stress (from wearing full-body protective suits) among hazardous-waste clean-up workers and roofers. White finger (Raynaud’s syndrome) appears among some jackhammer operators and other workers who use vibrating drills (e.g., stoper drills among tunnellers).
Alcoholism and other alcohol-related disease is more frequent than expected among construction workers. Specific occupational causes have not been identified, but it is possible that it is related to stress resulting from lack of control over employment prospects, heavy work demands or social isolation due to unstable working relationships.
Physical hazards
Physical hazards are present in every construction project. These hazards include noise, heat and cold, radiation, vibration and barometric pressure. Construction work often must be done in extreme heat or cold, in windy, rainy, snowy, or foggy weather or at night. Ionizing and non-ionizing radiation is encountered, as are extremes of barometric pressure.
The machines that have transformed construction into an increasingly mechanized activity have also made it increasingly noisy. The sources of noise are engines of all kinds (e.g., on vehicles, air compressors and cranes), winches, rivet guns, nail guns, paint guns, pneumatic hammers, power saws, sanders, routers, planers, explosives and many more. Noise is present on demolition projects by the very activity of demolition. It affects not only the person operating a noise-making machine, but all those close-by and not only causes noise-induced hearing loss, but also masks other sounds that are important for communication and for safety.
Pneumatic hammers, many hand tools and earth-moving and other large mobile machines also subject workers to segmental and whole-body vibration.
Heat and cold hazards arise primarily because a large portion of construction work is conducted while exposed to the weather, the principal source of heat and cold hazards. Roofers are exposed to the sun, often with no protection, and often must heat pots of tar, thus receiving both heavy radiant and convective heat loads in addition to metabolic heat from physical labour. Heavy equipment operators may sit beside a hot engine and work in an enclosed cab with windows and without ventilation. Those that work in an open cab with no roof have no protection from the sun. Workers in protective gear, such as that needed for removal of hazardous waste, may generate metabolic heat from hard physical labour and get little relief since they may be in an air-tight suit. A shortage of potable water or shade contributes to heat stress as well. Construction workers also work in especially cold conditions during the winter, with danger of frostbite and hypothermia and risk of slipping on ice.
The principal sources of non-ionizing ultraviolet (UV) radiation are the sun and electric arc welding. Exposure to ionizing radiation is less common, but can occur with x-ray inspection of welds, for example, or it may occur with instruments such as flow meters that use radioactive isotopes. Lasers are becoming more common and may cause injury, especially to the eyes, if the beam is intercepted.
Those who work under water or in pressurized tunnels, in caissons or as divers are exposed to high barometric pressure. Such workers are at risk of developing a variety of conditions associated with high pressure: decompression sickness, inert gas narcosis, aseptic bone necrosis and other disorders.
Strains and sprains are among the most common injuries among construction workers. These, and many chronically disabling musculoskeletal disorders (such as tendinitis, carpal tunnel syndrome and low-back pain) occur as a result of either traumatic injury, repetitive forceful movements, awkward postures or overexertion (see figure 1). Falls due to unstable footing, unguarded holes and slips off scaffolding (see figure 2) and ladders are very common.
Figure 1. Carrying without appropriate work clothing and protective equipment.
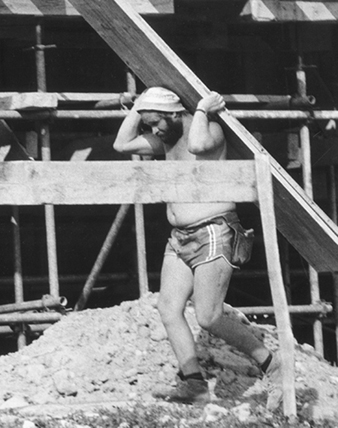
Figure 2. Unsafe scaffolding in Kathmandu, Nepal, 1974

Jane Seegal
Biological hazards
Biological hazards are presented by exposure to infectious micro-organisms, to toxic substances of biological origin or animal attacks. Excavation workers, for example, can develop histoplasmosis, an infection of the lung caused by a common soil fungus. Since there is constant change in the composition of the labour force on any one project, individual workers come in contact with other workers and, as a consequence, may become infected with contagious diseases—influenza or tuberculosis, for example. Workers may also be at risk of malaria, yellow fever or Lyme disease if work is conducted in areas where these organisms and their insect vectors are prevalent.
Toxic substances of plant origin come from poison ivy, poison oak, poison sumac and nettles, all of which can cause skin eruptions. Some wood dusts are carcinogenic, and some (e.g., western red cedar) are allergenic.
Attacks by animals are rare but may occur whenever a construction project disturbs them or encroaches on their habitat. This could include wasps, hornets, fire ants, snakes and many others. Underwater workers may be at risk from attack by sharks or other fish.
Social hazards
Social hazards stem from the social organization of the industry. Employment is intermittent and constantly changing, and control over many aspects of employment is limited because construction activity is dependent on many factors over which construction workers have no control, such as the state of an economy or the weather. Because of the same factors, there can be intense pressure to become more productive. Since the workforce is constantly changing, and with it the hours and location of work, and many projects require living in work camps away from home and family, construction workers may lack stable and dependable networks of social support. Features of construction work such as heavy workload, limited control and limited social support are the very factors associated with increased stress in other industries. These hazards are not unique to any trade, but are common to all construction workers in one way or another.
Evaluating Exposure
Evaluating either primary or bystander exposure requires knowing the tasks being done and the composition of ingredients and by-products associated with each job or task. This knowledge usually exists somewhere (e.g., material safety data sheets, MSDSs) but may not be available at the job site. With continually evolving computer and communications technology, it is relatively easy to obtain such information and make it available.
Controlling Occupational Hazards
Measuring and evaluating exposure to occupational hazards requires consideration of the novel manner in which construction workers are exposed. Conventional industrial hygiene measurements and exposure limits are based on 8-hour time-weighted averages. But since exposures in construction are usually brief, intermittent, varied but likely to be repeated, such measures and exposure limits are not as useful as in other jobs. Exposure measurement can be based on tasks rather than shifts. With this approach, separate tasks can be identified and hazards characterized for each. A task is a limited activity such as welding, soldering, sanding drywall, painting, installing plumbing and so on. As exposures are characterized for tasks, it should be possible to develop an exposure profile for an individual worker with knowledge of the tasks he or she performed or was near enough to be exposed to. As knowledge of task-based exposure increases, one may develop task-based controls.
Exposure varies with the concentration of the hazard and the frequency and duration of the task. As a general approach to hazard control, it is possible to reduce exposure by reducing the concentration or the duration or frequency of the task. Since exposure in construction is already intermittent, administrative controls that rely on reducing the frequency or duration of exposure are less practical than in other industries. Consequently, the most effective way to reduce exposure is to reduce the concentration of hazards. Other important aspects of controlling exposure include provisions for eating and sanitary facilities and education and training.
Decreasing exposure concentration
For reducing exposure concentration, it is useful to consider the source, the environment in which a hazard occurs and the workers who are exposed. As a general rule, the closer controls are to a source, the more efficient and effective they are. Three general types of controls can be used to reduce the concentration of occupational hazards. These are, from most to least effective:
- engineering controls at the source
- environmental controls that remove the hazard from the environment
- personal protection provided to the worker.
Engineering controls
Hazards originate at a source. The most efficient way to protect workers from hazards is to change the primary source with some sort of engineering change. For example, a less hazardous substance can be substituted for one that is more hazardous. Non-respirable synthetic vitreous fibres can be substituted for asbestos, and water can be substituted for organic solvents in paints. Similarly, non-silica abrasives can replace sand in abrasive blasting (also known as sand blasting). Or a process can be fundamentally changed, such as by replacing pneumatic hammers with impact hammers that generate less noise and vibration. If sawing or drilling generates harmful dusts, particulate matter or noise, these processes could be done by shear cutting or punching. Technological improvements are reducing the risks of some musculoskeletal and other health problems. Many of the changes are straightforward—for example, a two-handed screwdriver with a longer handle increases torque on the object and reduces stress on the wrists.
Environmental controls
Environmental controls are used to remove a hazardous substance from the environment, if the substance is airborne, or to shield the source, if it is a physical hazard. Local exhaust ventilation (LEV) can be used at a particular job with a ventilation duct and a hood to capture the fumes, vapours or dust. However, since the location of tasks that emit toxic materials changes, and because the structure itself changes, any LEV would have to be mobile and flexible in order to accommodate these changes. Mobile truck-mounted dust collectors with fans and filters, independent power sources, flexible ducts and mobile water supplies have been used on many job sites to provide LEV for a variety of hazard-producing processes.
The simple and effective method for controlling exposure to radiant physical hazards (noise, ultraviolet (UV) radiation from arc welding, infrared radiant (IR) heat from hot objects) is to shield them with some appropriate material. Plywood sheets shield IR and UV radiation, and material that absorbs and reflects sound will provide some protection from noise sources.
Major sources of heat stress are weather and hard physical labour. Adverse effects from heat stress can be avoided through reductions in the workload, provision of water and adequate breaks in the shade and, possibly, night work.
Personal protection
When engineering controls or changes in work practices do not adequately protect workers, workers may need to use personal protective equipment (PPE) (see figure 3). In order for such equipment to be effective, workers must be trained in its use, and the equipment must fit properly and be inspected and maintained. Furthermore, if others who are in the vicinity may be exposed to the hazard, they should either be protected or prevented from entering the area.
Figure 3. Construction worker in Nairobi, Kenya, without foot protection or hard hat

The use of some personal controls can create problems. For instance, construction workers often perform as teams and thus have to communicate with each other, but respirators interfere with communication. And full-body protective gear can contribute to heat stress because it is heavy and because body heat is not allowed to dissipate.
Having protective gear without knowing its limitations can also give workers or employers the illusion that the workers are protected when, with certain exposure conditions, they are not protected. For instance, there are no gloves currently available that protect for more than 2 hours against methylene chloride, a common ingredient in paint strippers. And there are few data on whether gloves protect against solvent mixtures such as those containing both acetone and toluene or both methanol and xylene. The level of protection depends on how a glove is used. In addition, gloves are generally tested on one chemical at a time and rarely for more than 8 hours.
Eating and sanitary facilities
A lack of eating and sanitary facilities may also lead to increased exposures. Often, workers cannot wash before meals and must eat in the work zone, which means they may inadvertently swallow toxic substances transferred from their hands to food or cigarettes. A lack of changing facilities at a worksite may result in transport of contaminants from the workplace to a worker’s home.
Injuries and Illnesses in Construction
Fatal injuries
Because construction involves a large proportion of the workforce, construction fatalities also affect a large population. For instance, in the United States, construction represents 5 to 6% of the workforce but accounts for 15% of work-related fatalities—more than any other sector. The construction sector in Japan is 10% of the workforce but has 42% of the work-related deaths; in Sweden, the numbers are 6% and 13%, respectively.
The most common fatal injuries among construction workers in the United States are falls (30%), transportation accidents (26%), contact with objects or equipment (e.g., struck by an object or caught in machinery or materials) (19%) and exposure to harmful substances (18%), most of which (75%) are electrocutions from contact with electrical wiring, overhead power lines or electrically powered machinery or hand tools. These four types of events account for nearly all (93%) fatal injuries among construction workers in the United States (Pollack et al. 1996).
Among trades in the US, the rate of fatal injuries is highest among structural steel workers (118 fatalities per 100,000 full-time equivalent workers for 1992–1993 compared to a rate of 17 per 100,000 for other trades combined) and 70% of structural steel worker fatalities were from falls. Labourers experienced the greatest number of fatalities, with an annual average number of about 200. Overall, the rate of fatalities was highest for workers 55 years and older.
The proportion of fatalities by event differed for each trade. For supervisors, falls and transportation accidents accounted for about 60% of all fatalities. For carpenters, painters, roofers and structural steel workers, falls were most common, accounting for 50, 55, 70 and 69% of all fatalities for those trades, respectively. For operating engineers and excavating machine operators, transportation accidents were the most common causes, accounting for 48 and 65% of fatalities for those trades, respectively. Most of these were associated with dump trucks. Fatalities from improperly sloped or shored trenches continue to be a major cause of fatalities (McVittie 1995). The primary hazards in the skilled trades are listed in table 2.
A study of Swedish construction workers did not find a high overall work-related mortality rate, but did find high death rates for particular conditions (see table 3).
Table 3. Construction occupations with excess standardized mortality rates (SMRs)and standardized incidence rates (SIRs) for selected causes.
|
Occupation |
Significantly higher SMRs |
Significantly higher SIRs |
|
Bricklayers |
- |
Peritoneal tumour |
|
Concrete workers |
All causes,* all cancers,* stomach cancer, violent death,* accidental falls |
Lip cancer, stomach and larynx cancer,*a lung cancerb |
|
Crane drivers |
Violent death* |
- |
|
Drivers |
All causes,* cardiovascular* |
Lip cancer |
|
Insulators |
All causes,* lung cancer, pneumoconiosis, violent death* |
Peritoneal tumour, lung cancer |
|
Machine operators |
Cardiovascular,* other accidents |
- |
|
Plumbers |
All cancers,* lung cancer, pneumoconiosis |
All cancers, pleural tumour, lung cancer |
|
Rock workers |
All causes,* cardiovascular,* |
- |
|
Sheet metal workers |
All cancers,* lung cancer, accidental falls |
All cancers, lung cancer |
|
Woodworkers/carpenters |
- |
Nose and nasal sinus cancer |
* Cancers or causes of death are significantly higher in comparison to all other occupational groups combined. “Other accidents” includes typical work-related injuries.
a The relative risk for larynx cancer among concrete workers, compared to carpenters, is 3 times higher.
b The relative risk for lung cancer among concrete workers, compared to carpenters, is almost double.
Source: Engholm and Englund 1995.
Disabling or lost time injuries
In the United States and Canada, the most common causes of lost time injuries are overexertion; being struck by an object; falls to a lower level; and slips, trips and falls on the same level. The most common category of injury is strains and sprains, some of which become sources of chronic pain and impairment. The activities most often associated with lost time injuries are manual materials handling and installation (e.g., installing dry-wall, piping or ventilation duct-work). Injuries occurring in transit (e.g., walking, climbing, descending) are also common. Underlying many of these injuries is the problem of housekeeping. Many slips, trips and falls are caused by walking through construction debris.
Costs of Injuries and Illness
Occupational injuries and illnesses in construction are very costly. Estimates for the cost of injuries in construction in the US range from $10 billion to $40 billion annually (Meridian Research 1994); at $20 billion, the cost per construction worker would be US$3,500 yearly. Workers’ compensation premiums for three trades—carpenters, masons and structural iron workers— averaged 28.6% of payroll nationally in mid-1994 (Powers 1994). Premium rates vary enormously, depending on trade and jurisdiction. The average premium cost is several times higher than in most industrialized countries, where workers’ compensation insurance premiums range from 3 to 6% of payroll. In addition to workers’ compensation, there are liability insurance premiums and other indirect costs, including reduced work crew efficiency, clean-up (from a cave-in or collapse, for instance) or overtime necessitated by an injury. Such indirect costs can be several times the workers’ compensation award.
Management for Safe Construction Work
Effective safety programmes have several features in common. They are manifest throughout organizations, from the highest offices of a general contractor to project managers, supervisors, union officials and workers on the job. Codes of practice are conscientiously implemented and evaluated. Costs of injury and illness are calculated and performance is measured; those that do well are rewarded, those that do not are penalized. Safety is an integral part of contracts and subcontracts. Everybody—managers, supervisors and workers—receives general, site-specific and site-relevant training and re-training. Inexperienced workers receive on-the-job training from experienced workers. In projects where such measures are implemented, injury rates are significantly lower than on otherwise comparable sites.
Preventing Accidents and Injuries
Entities in the industry with lower injury rates share several common characteristics: they have a clearly defined policy statement that applies throughout the organization, from top management to the project site. This policy statement refers to a specific code of practice that describes, in detail, the hazards and their control for the pertinent occupations and tasks at a site. Responsibilities are clearly assigned and standards of performance are stated. Failures to meet these standards are investigated and penalties imposed as appropriate. Meeting or exceeding standards is rewarded. An accounting system is used that shows the costs of each injury or accident and the benefits of injury prevention. Employees or their representatives are involved in establishing and administering a programme of injury prevention. Involvement often occurs in the formation of a joint labour or worker management committee. Physical examinations are performed to determine workers’ fitness for duty and job assignment. These exams are provided when first employed and when returning from a disability or other layoff.
Hazards are identified, analysed and controlled following the classes of hazards discussed in other articles in this chapter. The entire work site is inspected on a regular basis and results are recorded. Equipment is inspected to ensure its safe operation (e.g., brakes on vehicles, alarms, guards and so on). Injury hazards include those associated with the most common types of lost-time injuries: falls from heights or at the same level, lifting or other forms of manual materials handling, risk of electrocution, risk of injury associated with either highway or off-road vehicles, trench cave-ins and others. Health hazards would include airborne particles (such as silica, asbestos, synthetic vitreous fibres, diesel particulates), gases and vapours (such as carbon monoxide, solvent vapour, engine exhaust), physical hazards (such as noise, heat, hyperbaric pressure) and others, such as stress.
Preparations are made for emergency situations and emergency drills are conducted as needed. Preparations would include assignment of responsibilities, provision of first aid and immediate medical attention at the site, communication at the site and with others off the site (such as ambulances, family members, home offices and labour unions), transportation, designation of health care facilities, securing and stabilizing the environment where the emergency occurred, identifying witnesses and documenting events. As needed, emergency preparedness would also cover means of escape from an uncontrolled hazard such as fire or flood.
Accidents and injuries are investigated and recorded. The purpose of reports is to identify causes that could have been controlled so that, in the future, similar occurrences can be prevented. Reports should be organized with a standardized record-keeping system to better facilitate analysis and prevention. To facilitate comparison of injury rates from one situation to another, it is useful to identify the pertinent population of workers within which an injury occurred, and their hours worked, in order to calculate an injury rate (i.e., the number of injuries per hour worked or the number of hours worked between injuries).
Workers and supervisors receive training and education in safety. This education consists of teaching general principles of safety and health, is integrated into task training, is specific for each work site and covers procedures to follow in the event of an accident or injury. Education and training for workers and supervisors is an essential part of any effort to prevent injuries and disease. Training about safe work practices and procedures have been provided in many countries by some companies and trade unions. These procedures, include lockout and tagout of electrical power sources during maintenance procedures, use of lanyards while working at heights, shoring trenches, providing safe walking surfaces and so on. It is also important to provide site-specific training, covering unique features about the job site such as means of entry and exit. Training should include instruction about dangerous substances. Performance or hands-on training, demonstrating that one knows safe practices, is much better for instilling safe behaviour than classroom instruction and written examination.
In the United States, training about certain hazardous substances is mandated by federal law. The same concern in Germany led to development of the Gefahrstoff-Informationssystem der Berufsgenossenschaften der Bauwirtschaft, or GISBAU, programme. GISBAU works with manufacturers to determine the content of all substances used on construction sites. Equally important, the programme provides the information in a form to suit the differing needs of health staff, managers and workers. The information is available through training programmes, in print and on computer terminals at work sites. GISBAU gives advice about how to substitute for some hazardous substances and tells how to safely handle others. (See the chapter Using, storing and transporting chemicals.)
Information about chemical, physical and other health hazards is available at the work site in the languages that workers use. If workers are to work intelligently on the job, they should have the information necessary to decide what to do in specific situations.
And finally, contracts between contractors and subcontractors should include safety features. Provisions could include establishing a unified safety organization at multi-employer work sites, performance requirements and rewards and penalties.
Indoor Air Quality: Introduction
The connection between the use of a building either as a workplace or as a dwelling and the appearance, in certain cases, of discomfort and symptoms that may be the very definition of an illness is a fact that can no longer be disputed. The main culprit is contamination of various kinds within the building, and this contamination is usually referred to as “poor quality of indoor air”. The adverse effects due to poor air quality in closed spaces affect a considerable number of people, since it has been shown that urban dwellers spend between 58 and 78% of their time in an indoor environment which is contaminated to a greater or lesser degree. These problems have increased with the construction of buildings that are designed to be more airtight and that recycle air with a smaller proportion of new air from the outside in order to be more energy efficient. The fact that buildings that do not offer natural ventilation present risks of exposure to contaminants is now generally accepted.
The term indoor air is usually applied to nonindustrial indoor environments: office buildings, public buildings (schools, hospitals, theatres, restaurants, etc.) and private dwellings. Concentrations of contaminants in the indoor air of these structures are usually of the same order as those commonly found in outdoor air, and are much lower than those found in air in industrial premises, where relatively well-known standards are applied in order to assess air quality. Even so, many building occupants complain of the quality of the air they breathe and there is therefore a need to investigate the situation. Indoor air quality began to be referred to as a problem at the end of the 1960s, although the first studies did not appear until some ten years later.
Although it would seem logical to think that good air quality is based on the presence in the air of the necessary components in suitable proportions, in reality it is the user, through respiration, who is the best judge of its quality. This is because inhaled air is perceived perfectly through the senses, as human beings are sensitive to the olfactory and irritant effects of about half a million chemical compounds. Consequently, if the occupants of a building are as a whole satisfied with the air, it is said to be of high quality; if they are unsatisfied, it is of poor quality. Does this mean that it is possible to predict on the basis of its composition how the air will be perceived? Yes, but only in part. This method works well in industrial environments, where specific chemical compounds related to production are known, and their concentrations in the air are measured and compared with threshold limit values. But in nonindustrial buildings where there may be thousands of chemical substances in the air but in such low concentrations that they are, perhaps, thousands of times less than the limits set for industrial environments, the situation is different. In most of these cases information about the chemical composition of indoor air does not allow us to predict how the air will be perceived, since the combined effect of thousands of these contaminants, together with temperature and humidity, can produce air that is perceived as irritating, foul, or stale—that is, of poor quality. The situation is comparable to what happens with the detailed composition of an item of food and its taste: chemical analysis is inadequate to predict whether the food will taste good or bad. For this reason, when a ventilation system and its regular maintenance are being planned, an exhaustive chemical analysis of indoor air is rarely called for.
Another point of view is that people are considered the only sources of contamination in indoor air. This would certainly be true if we were dealing with building materials, furniture and ventilation systems as they were used 50 years ago, when bricks, wood and steel predominated. But with modern materials the situation has changed. All materials contaminate, some a little and others much, and together they contribute to a deterioration in the quality of indoor air.
The changes in a person’s health due to poor indoor air quality can show up as a wide array of acute and chronic symptoms and in the form of a number of specific illnesses. These are illustrated in figure 1. Although poor indoor air quality results in fully developed illness in only a few cases, it can give rise to malaise, stress, absenteeism and loss of productivity (with concomitant increases in production costs); and allegations about problems related to the building can develop rapidly into conflict between the occupants, their employers and the owners of the buildings.
Figure 1. Symptoms and illnesses related to the quality of indoor air.

Normally it is difficult to establish precisely to what extent poor indoor air quality can harm health, since not enough information is available concerning the relationship between exposure and effect at the concentrations in which the contaminants are usually found. Hence, there is a need to take information obtained at high doses—as with exposures in industrial settings—and extrapolate to much lower doses with a corresponding margin of error. In addition, for many contaminants present in the air, the effects of acute exposure are well known, whereas there are considerable gaps in the data regarding both long-term exposures at low concentrations and mixtures of different contaminants. The concepts of no-effect-level (NOEL), harmful effect and tolerable effect, already confusing even in the sphere of industrial toxicology, are here even more difficult to define. There are few conclusive studies on the subject, whether relating to public buildings and offices or private dwellings.
Series of standards for outdoor air quality exist and are relied on to protect the general population. They have been obtained by measuring adverse effects on health resulting from exposure to contaminants in the environment. These standards are therefore useful as general guidelines for an acceptable quality of indoor air, as is the case with those proposed by the World Health Organization. Technical criteria such as the threshold limit value of the American Conference of Governmental Industrial Hygienists (ACGIH) in the United States and the limit values legally established for industrial environments in different countries have been set for the working, adult population and for specific lengths of exposure, and cannot therefore be applied directly to the general population. The American Society of Heating, Refrigeration and Air Conditioning Engineers (ASHRAE) in the United States has developed a series of standards and recommendations that are widely used in assessing indoor air quality.
Another aspect that should be considered as part of the quality of indoor air is its smell, because smell is often the parameter that ends up being the defining factor. The combination of a certain smell with the slight irritating effect of a compound in indoor air can lead us to define its quality as “fresh” and “clean” or as “stale” and “polluted”. Smell is therefore very important when defining the quality of indoor air. While odours objectively depend on the presence of compounds in quantities above their olfactory thresholds, they are very often evaluated from a strictly subjective point of view. It should also be kept in mind that the perception of an odour may result from the smells of many different compounds and that temperature and humidity may also affect its characteristics. From the standpoint of perception there are four characteristics that allow us to define and measure odours: intensity, quality, tolerability and threshold. When considering indoor air, however, it is very difficult to “measure” odours from a chemical standpoint. For that reason the tendency is to eliminate odours that are “bad” and to use, in their place, those considered good in order to give air a pleasant quality. The attempt to mask bad odours with good ones usually ends in failure, because odours of very different qualities can be recognized separately and lead to unforeseeable results.
A phenomenon known as sick building syndrome occurs when more than 20% of the occupants of a building complain about air quality or have definite symptoms. It is evidenced by a variety of physical and environmental problems associated with non-industrial indoor environments. The most common features seen in cases of sick building syndrome are the following: those affected complain of non-specific symptoms similar to the common cold or respiratory illnesses; the buildings are efficient as regards energy conservation and are of modern design and construction or recently remodelled with new materials; and the occupants cannot control the temperature, humidity and illumination of the workplace. The estimated percentage distribution of the most common causes of sick building syndrome are inadequate ventilation due to lack of maintenance; poor distribution and insufficient intake of fresh air (50 to 52%); contamination generated indoors, including from office machines, tobacco smoke and cleaning products (17 to 19%); contamination from the outside of the building due to inadequate placement of air intake and exhaust vents (11%); microbiological contamination from stagnant water in the ducts of the ventilation system, humidifiers and refrigeration towers (5%); and formaldehyde and other organic compounds emitted by building and decoration materials (3 to 4%). Thus, ventilation is cited as an important contributory factor in the majority of cases.
Another question of a different nature is that of building-related illnesses, which are less frequent, but often more serious, and are accompanied by very definite clinical signs and clear laboratory findings. Examples of building-related illnesses are hypersensitivity pneumonitis, humidifier fever, legionellosis and Pontiac fever. A fairly general opinion among investigators is that these conditions should be considered separately from sick building syndrome.
Studies have been done to ascertain both the causes of air quality problems and their possible solutions. In recent years, knowledge of the contaminants present in indoor air and the factors contributing to a decline in indoor air quality has increased considerably, although there is a long way to go. Studies carried out in the last 20 years have shown that the presence of contaminants in many indoor environments is higher than anticipated, and moreover, different contaminants have been identified from those that exist in outside air. This contradicts the assumption that indoor environments without industrial activity are relatively free of contaminants and that in the worst of cases they may reflect the composition of outside air. Contaminants such as radon and formaldehyde are identified almost exclusively in the indoor environment.
Indoor air quality, including that of dwellings, has become a question of environmental health in the same way as has happened with control of outdoor air quality and exposure at work. Although, as already mentioned, an urban person spends 58 to 78% of his or her time indoors, it should be remembered that the most susceptible persons, namely the elderly, small children and the sick, are the ones who spend most of their time indoors. This subject began to be particularly topical from around 1973 onwards, when, because of the energy crisis, efforts directed at energy conservation concentrated on reducing the entry of outside air into indoor spaces as much as possible in order to minimize the cost of heating and cooling buildings. Although not all the problems relating to indoor air quality are the result of actions aimed at saving energy, it is a fact that as this policy spread, complaints about indoor air quality began to increase, and all the problems appeared.
Another item requiring attention is the presence of micro-organisms in indoor air which can cause problems of both an infectious and an allergic nature. It should not be forgotten that micro-organisms are a normal and essential component of ecosystems. For example, saprophytic bacteria and fungi, which obtain their nutrition from dead organic material in the environment, are found normally in the soil and atmosphere, and their presence can also be detected indoors. In recent years problems of biological contamination in indoor environments have received considerable attention.
The outbreak of Legionnaire’s disease in 1976 is the most discussed case of an illness caused by a micro-organism in the indoor environment. Other infectious agents, such as viruses that can cause acute respiratory illness, are detectable in indoor environments, especially if the occupation density is high and much recirculation of air is taking place. In fact, the extent to which micro-organisms or their components are implicated in the outbreak of building-associated conditions is not known. Protocols for demonstrating and analysing many types of microbial agents have been developed only to a limited degree, and in those cases where they are available, the interpretation of the results is sometimes inconsistent.
Aspects of the Ventilation System
Indoor air quality in a building is a function of a series of variables which include the quality of the outdoor air, the design of the ventilation and air-conditioning system, the conditions in which this system operates and is serviced, the compartmentalization of the building and the presence of indoor sources of contaminants and their magnitude. (See figure 2) By way of summary it may be noted that the most common defects are the result of inadequate ventilation, contamination generated indoors and contamination coming from outside.
Figure 2. Diagram of building showing sources of indoor and outdoor pollutants.
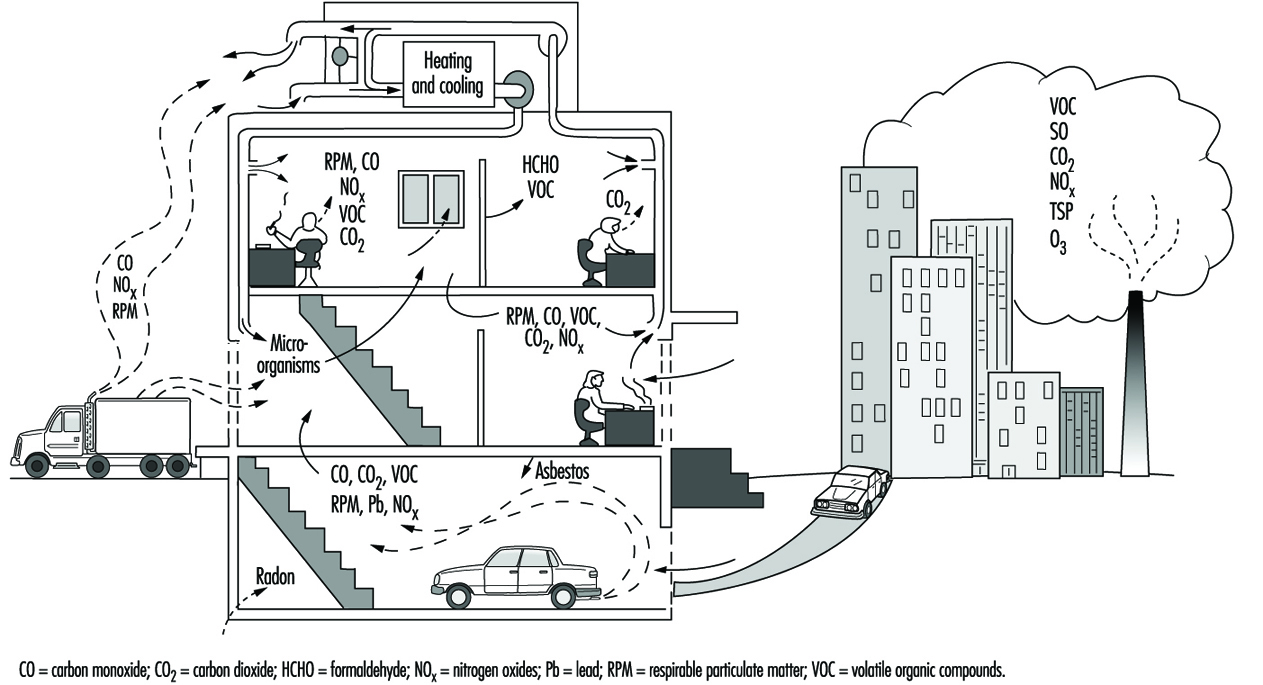
Regarding the first of these problems, causes of inadequate ventilation can include: an insufficient supply of fresh air due to a high level of recirculation of the air or a low volume of intake; incorrect placement and orientation in the building of intake points for outside air; poor distribution and consequently incomplete mixing with the air of the premises, which can produce stratification, unventilated zones, unforeseen pressure differences giving rise to unwanted air currents and continuous changes in the thermohygrometric characteristics noticeable as one moves about the building—and incorrect filtration of the air because of lack of maintenance or inadequate design of the filtering system—a deficiency which is particularly serious where the outdoor air is of poor quality or where there is a high level of recirculation.
Origins of Contaminants
Indoor contamination has different origins: the occupants themselves; inadequate materials or materials with technical defects used in the construction of the building; the work performed within; excessive or improper use of normal products (pesticides, disinfectants, products used for cleaning and polishing); combustion gases (from smoking, kitchens, cafeterias and laboratories); and cross-contamination coming from other poorly ventilated zones which then diffuses towards neighbouring areas and affects them. It should be borne in mind that substances emitted in indoor air have much less opportunity of being diluted than those emitted in outdoor air, given the difference in the volumes of air available. As regards biological contamination, its origin is most frequently due to the presence of stagnant water, materials impregnated with water, exhausts and so on, and to defective maintenance of humidifiers and refrigeration towers.
Finally, contamination coming from outside must also be considered. As regards human activity, three main sources may be mentioned: combustion in stationary sources (power stations); combustion in moving sources (vehicles); and industrial processes. The five main contaminants emitted by these sources are carbon monoxide, oxides of sulphur, oxides of nitrogen, volatile organic compounds (including hydrocarbons), polycyclic aromatic hydrocarbons and particles. Internal combustion in vehicles is the principal source of carbon monoxide and hydrocarbons and is an important source of oxides of nitrogen. Combustion in stationary sources is the main origin of oxides of sulphur. Industrial processes and stationary sources of combustion generate more than half of the particles emitted into the air by human activity, and industrial processes can be a source of volatile organic compounds. There are also contaminants generated naturally that are propelled through the air, such as particles of volcanic dust, soil and sea salt, and spores and micro-organisms. The composition of outdoor air varies from place to place, depending both on the presence and the nature of the sources of contamination in the vicinity and on the direction of the prevailing wind. If there are no sources generating contaminants, the concentration of certain contaminants that will typically be found in “clean” outdoor air are as follows: carbon dioxide, 320 ppm; ozone, 0.02 ppm: carbon monoxide, 0.12 ppm; nitric oxide, 0.003 ppm; and nitrogen dioxide, 0.001 ppm. However, urban air always contains much higher concentrations of these contaminants.
Apart from the presence of the contaminants originating from outside, it sometimes happens that contaminated air from the building itself is expelled to the exterior and then returns inside again through the intakes of the air-conditioning system. Another possible way by which contaminants may enter from the exterior is by infiltration through the foundations of the building (e.g., radon, fuel vapors, sewer effluvia, fertilizers, insecticides and disinfectants). It has been shown that when the concentration of a contaminant in the outdoor air increases, its concentration in the air inside the building also increases, although more slowly (a corresponding relationship obtains when the concentration decreases); it is therefore said that buildings exert a shielding effect against external contaminants. However, the indoor environment is not, of course, an exact reflection of the conditions outside.
Contaminants present in indoor air are diluted in the outdoor air that enters the building and they accompany it when it leaves. When the concentration of a contaminant is less in the outdoor air than the indoor air, the interchange of indoor and outdoor air will result in a reduction in the concentration of the contaminant in the air inside the building. If a contaminant originates from outside and not inside, this interchange will result in a rise in its indoor concentration, as mentioned above.
Models for the balance of amounts of contaminants in indoor air are based on the calculation of their accumulation, in units of mass versus time, from the difference between the quantity that enters plus what is generated indoors, and what leaves with the air plus what is eliminated by other means. If appropriate values are available for each of the factors in the equation, the indoor concentration can be estimated for a wide range of conditions. Use of this technique makes possible the comparison of different alternatives for controlling an indoor contamination problem.
Buildings with low interchange rates with outdoor air are classified as sealed or energy-efficient. They are energy-efficient because less cold air enters in winter, reducing the energy required to heat the air to the ambient temperature, thus cutting the cost of heating. When the weather is hot, less energy is also used to cool the air. If the building does not have this property, it is ventilated through open doors and windows by a process of natural ventilation. Although they may be closed, differences of pressure, resulting both from the wind and from the thermal gradient existing between the interior and the exterior, force the air to enter through crevices and cracks, window and door joints, chimneys and other apertures, giving rise to what is called ventilation by infiltration.
The ventilation of a building is measured in renewals per hour. One renewal per hour means that a volume of air equal to the volume of the building enters from outside every hour; in the same way, an equal volume of indoor air is expelled to the exterior every hour. If there is no forced ventilation (with a ventilator) this value is difficult to determine, although it is considered to vary between 0.2 and 2.0 renewals per hour. If the other parameters are assumed to be unchanged, the concentration of contaminants generated indoors will be less in buildings with high renewal values, although a high renewal value is not a complete guarantee of indoor air quality. Except in areas with marked atmospheric pollution, buildings that are more open will have a lower concentration of contaminants in the indoor air than those constructed in a more closed manner. However, buildings that are more open are less energy-efficient. The conflict between energy efficiency and air quality is of great importance.
Much action undertaken to reduce energy costs affects indoor air quality to a greater or lesser extent. In addition to reducing the speed with which the air circulates within the building, efforts to increase the insulation and waterproofing of the building involve the installation of materials that may be sources of indoor contamination. Other action, such as supplementing old and frequently inefficient central heating systems with secondary sources that heat or consume the indoor air can also raise contaminant levels in indoor air.
Contaminants whose presence in indoor air is most frequently mentioned, apart from those coming from outside, include metals, asbestos and other fibrous materials, formaldehyde, ozone, pesticides and organic compounds in general, radon, house dust and biological aerosols. Together with these, a wide variety of types of micro-organisms can be found, such as fungi, bacteria, viruses and protozoa. Of these, the saprophytic fungi and bacteria are relatively well known, probably because a technology is available for measuring them in air. The same is not true of agents such as viruses, rickettsiae, chlamydias, protozoa and many pathogenic fungi and bacteria, for the demonstration and counting of which no methodology is as yet available. Among the infectious agents, special mention should be made of: Legionella pneumophila, Mycobacterium avium, viruses, Coxiella burnetii and Histoplasma capsulatum; and among the allergens: Cladosporium, Penicillium and Cytophaga.
Investigating Indoor Air Quality
Experience so far suggests that the traditional techniques used in industrial hygiene and heating, ventilation and air-conditioning do not always provide satisfactory results at present for solving the ever more common problems of indoor air quality, although basic knowledge of these techniques permits good approximations for dealing with or reducing problems rapidly and inexpensively. The solution to problems of indoor air quality often requires, in addition to one or more experts in heating, ventilation and air-conditioning and industrial hygiene, specialists in indoor air quality control, analytical chemistry, toxicology, environmental medicine, microbiology, and also epidemiology and psychology.
When a study is carried out on indoor air quality, the objectives set for it will profoundly affect its design and the activities directed at sampling and evaluation, since in some cases procedures giving a rapid response will be required, while in others overall values will be of interest. The duration of the programme will be dictated by the time required to obtain representative samples, and will also depend on the season and on meteorological conditions. If the aim is to carry out an exposure-effect study, in addition to long-term and short-term samples for evaluating peaks, personal samples will be required for ascertaining the direct exposure of individuals.
For some contaminants, well-validated and widely used methods are available, but for the majority this is not the case. Techniques for measuring levels of many contaminants found indoors are normally derived from applications in industrial hygiene but, given that the concentrations of interest in indoor air are usually much lower than those occurring in industrial environments, these methods are frequently inappropriate. As for the measurement methods used in atmospheric contamination, they operate with margins of similar concentrations, but are available for relatively few contaminants and present difficulties in indoor use, such as would arise, for example, with a high-volume sampler for determining particulate matter, which on the one hand would be too noisy and on the other could modify the quality of the indoor air itself.
The determination of contaminants in indoor air is usually carried out by using different procedures: with continuous monitors, whole-time active samplers, whole-time passive samplers, direct sampling and personal samplers. Adequate procedures exist at present for measuring levels of formaldehyde, oxides of carbon and nitrogen, volatile organic compounds and radon, among others. Biological contaminants are measured using techniques of sedimentation on open culture plates or, more frequently nowadays, by using active systems that cause the air to impact on plates containing nutrient, which are subsequently cultured, the quantity of micro-organisms present being expressed in colony-forming units per cubic meter.
When a problem of indoor air quality is being investigated, it is usual to design beforehand a practical strategy consisting of an approximation in phases. This approximation begins with a first phase, the initial investigation, which can be carried out using industrial hygiene techniques. It must be structured so that the investigator does not need to be a specialist in the field of indoor air quality in order to carry out his work. A general inspection of the building is undertaken and its installations are checked, particularly as regards the regulation and adequate functioning of the heating, ventilation and air-conditioning system, according to the standards set at the time of its installation. It is important in this respect to consider whether the persons affected are able to modify the conditions of their surroundings. If the building does not have systems of forced ventilation, the degree of effectiveness of the existing natural ventilation must be studied. If after revision—and adjustment if necessary—the operational conditions of the ventilation systems are adequate for the standards, and if despite this the complaints continue, a technical investigation of a general kind will have to ensue to determine the degree and nature of the problem. This initial investigation should also allow an assessment to be made as to whether the problems can be considered solely from the functional point of view of the building, or whether the intervention of specialists in hygiene, psychology or other disciplines will be necessary.
If the problem is not identified and resolved in this first phase, other phases can follow involving more specialized investigations concentrating on potential problems identified in the first phase. The subsequent investigations may include a more detailed analysis of the heating, ventilation and air-conditioning system of the building, a more extensive evaluation of the presence of materials suspected of emitting gases and particles, a detailed chemical analysis of the ambient air in the building and medical or epidemiological assessments to detect signs of disease.
As regards the heating, ventilation and air-conditioning system, the refrigeration equipment should be checked in order to ensure that there is no microbial growth in them or accumulation of water in their drip trays, the ventilation units must be checked to see that they are functioning correctly, the air intake and return systems must be examined at various points to see that they are watertight, and the interior of a representative number of ducts must be checked to confirm the absence of micro-organisms. This last consideration is particularly important when humidifiers are used. These units require particularly careful programmes of maintenance, operation and inspection in order to prevent the growth of micro-organisms, which can propagate themselves throughout the air-conditioning system.
The options generally considered for improving indoor air quality in a building are the elimination of the source; its insulation or independent ventilation; separating the source from those who may be affected; general cleaning of the building; and increased checking and improvement of the heating, ventilation and air-conditioning system. This may require anything from modifications at particular points to a new design. The process is frequently of a repetitive nature, so that the study has to be started again several times, using more sophisticated techniques on each occasion. A more detailed description of control techniques will be found elsewhere in this Encyclopaedia.
Finally, it should be emphasized that, even with the most complete investigations of indoor air quality, it may be impossible to establish a clear relationship between the characteristics and composition of the indoor air and the health and comfort of the occupants of the building under study. Only the accumulation of experience on the one hand, and the rational design of ventilation, occupation and compartmentalization of buildings on the other, are possible guarantees from the outset of obtaining indoor air quality that is adequate for the majority of the occupants of a building.
Cleaner Production Technologies
Prevention, Control and Remediation
Conventionally, there are three ways of addressing pollution: prevention, control and remediation. These form a hierarchy, in which the first priority or option is prevention, followed by control measures, with remediation as a poor third. Pollution abatement can refer to any means that lessens pollution, or a mitigation of pollution; in practice, it usually means control. Though the hierarchy of the three ideas is in terms of preference or priority, this is not always so in practice: there may be regulatory pressures to choose one path rather than another; one strategy may be less expensive than another, or remediation may be the most urgent - for example, in the event of a major spill or the hazardous dissemination of pollutants from a contaminated site.
Pollution prevention
Pollution prevention can be defined as a strategy or strategies which avoid the creation of pollutants in the first place. In Barry Commoner’s phrase, “If it’s not there, it can’t pollute.” Thus, if a chemical whose use results in pollution is eliminated, there will be “zero discharge” (or “zero emission”) of the pollutant. Zero discharge is more convincing if the chemical is not replaced by another chemical - an alternative or substitute - which results in a different pollutant.
One central strategy of pollution prevention is the banning, elimination or the phasing out (“sunsetting”) of specified chemicals or classes of chemical. (Alternatively, use-restrictions may be specified.) Such strategies are laid down in the form of laws or regulations by national governments, less often by international instruments (conventions or treaties) or by sub-national governments.
A second strategy is pollution reduction, again in the context of prevention rather than control. If the use of a chemical which results in pollution is reduced, then the result will almost always be less pollution. Pollution reduction strategies are exemplified in North America by toxics use reduction (TUR) programmes and in Europe by “clean technology programmes”.
Unlike bans and phase-outs, which usually apply to all (relevant) workplaces within a political jurisdiction, pollution reduction programmes apply to specific workplaces or classes of workplace. These are usually industrial manufacturing (including chemical manufacturing) workplaces over a certain size, in the first instance, though the principles of pollution reduction can be applied generally - for example, to mines, power plants, construction sites, offices, agriculture (in regard to chemical fertilizers and pesticides) and municipalities. At least two US states (Michigan and Vermont) have legislated TUR programmes for individual households which are also workplaces.
Pollution reduction can result in the elimination of specific chemicals, thus achieving the same aims as bans and phase-outs. Again, this would result in zero discharge of the pollutant concerned, but requirements to eliminate specific chemicals are not part of pollution reduction programmes; what is prescribed is a general programme with a flexible range of specified methods. A requirement to eliminate a specific chemical is an example of a “specification standard”. A requirement to institute a general programme is a “performance standard” because it allows flexibility in the mode of implementation, though a specific mandatory target (outcome) for a general programme would (confusingly) count as a specification standard. When they have to choose, businesses usually prefer performance to specification standards.
Pollution control
Pollution control measures cannot eliminate pollution; all they can do is to mitigate its effects on the environment. Control measures are instituted “at the end of the (waste) pipe”. The usefulness of control measures will depend on the pollutant and the industrial circumstance. The main methods of pollution control, in no particular order, are:
- the capture and subsequent storage of pollutants
- filtration, whereby airborne or waterborne pollutants are removed from the waste stream by physical methods such as meshes, filters and other permeable barriers (such as coke)
- precipitation, whereby the pollutant is chemically precipitated and then captured in its transformed state or captured by physical methods such as an electrostatic charge
- destruction - for example, incineration, or neutralization, whereby pollutants are transformed chemically or biologically into substances which are less harmful
- dilution, whereby the pollutant is diluted or flushed in order to lessen its effects on any one organism or on an ecosystem; or concentration to lessen the effect of disposal
- evaporation or dissolution - for example, dissolving a gas in water
- utilization - for example, transforming a pollutant into a potentially useful (though not necessarily less toxic) product (such as sulphur dioxide into sulphuric acid or using solid waste as hard core or road bed)
- out-of-process recycling (where the recycling is not an integral part of the production process)
- media-shift, whereby a waste-stream is diverted from one medium, such as air, soil or water, to another, on the rationale that the medium-shift makes the pollutant less harmful
- state-changes—a change to the solid, liquid or gaseous state on the rationale that the new state is less harmful.
Pollution remediation
Remediation is needed to the extent that pollution prevention and control fail. It is also very expensive, with the costs not always accruing to the polluter. The modes of remediation are:
The clean-up of contaminated sites
Clean-up has a common sense meaning, as when an employer is required to “clean up his act”, which can mean a large number of different things. Within environmental protection, clean-up is a technical term meaning a branch or a mode of remediation. Even within this restricted use of the term, clean-up can mean (1) the removal of pollutants from a contaminated site or (2) the rehabilitation of a site so that it is restored to its full use-potential. Again, clean-up sometimes refers to nothing more than the containment of pollutants within a site, area or body of water—for example, by capping, sealing or the construction of an impermeable floor.
To be successful, clean-up has to be 100% effective, with full protection for workers, bystanders and the general public. A further consideration is whether the clean-up materials, methods and technology do not create further hazards. Though it is desirable to use engineering controls to protect clean-up workers, there will almost always be a need for appropriate personal protective equipment. Normally, workers engaged in remediation are classified as hazardous-waste workers, though aspects of such work are undertaken by fire fighters and municipal workers, among others.
A large number of physical, chemical, biological and biotechnological agents and methods are used in the clean-up of contaminated sites.
Hazardous-waste treatment
Most treatment of hazardous (or toxic) waste now takes place in purpose-built facilities by hazardous-waste workers. From an environmental point of view, the test of effectiveness of a hazardous-waste facility is that it produces no outputs which are not inert or virtually inert, such as silica, insoluble inorganic compounds, insoluble and non-corrosive slags, gaseous nitrogen or carbon dioxide - though carbon dioxide is a “greenhouse gas” which causes climate change and is, thus, a further environmental detriment.
A further test is that the facility be energy efficient - that is, energy is not wasted - and as energy non-intensive as possible (i.e., the ratio of energy use to the volume of waste treated be as low as possible). A general rule of thumb (it is fortunately not a universal law) is that the more effective the pollution (or waste) abatement strategy, the more energy is consumed, which by sustainable development criteria is another detriment.
Even when the workers are properly protected, it is easy to see the drawbacks of hazardous-waste treatment as a mode of addressing pollution. Pollution prevention methods can be applied to the operation of the treatment process but they cannot be applied to the principal “input” - the waste to be treated. Hazardous-waste treatment facilities will usually require at least as much energy to treat the waste as was expended in its creation, and there will always be further waste as an output, however inert or non-toxic.
Spills and leaks
The same considerations will apply to chemical spills and leaks as to the clean-up of contaminated sites, with the further hazards caused by the urgency of the clean-up. Workers cleaning up spills and leaks are almost always emergency workers. Depending on the scale and the nature of the pollutant, leaks and spills can become major industrial accidents.
The Modes of Pollution Prevention
Definition and philosophy
The definition of pollution prevention may seem to be a trivial matter, but it is important because advocates of pollution prevention want, as a principle of policy, to see a single-minded and aggressive prevention strategy at the expense of control methods, and to avoid remediation. The more strictly pollution prevention is defined, they say, the more likely it is to succeed as a practical strategy. Conversely, the more widely employers are allowed to define the term, the more likely their activities are to result in a mix of the same old (failed) strategies. Employers sometimes reply that even toxic waste can have a market value, and control methods have their place, so pollution is really only potential pollution. Besides, zero discharge is impossible and leads only to false expectations and misguided strategies. Proponents of pollution prevention respond that unless we have zero discharge as an aim or practical ideal, pollution prevention will not succeed and environmental protection will not improve.
Most of the strict definitions of pollution prevention have, as a sole or central element, the avoidance of the use of chemicals which result in pollutants so that pollution is not created in the first place. Some of the most important definitional controversies concern recycling, which is dealt with in the context of pollution prevention below.
Objectives
One possible objective of pollution prevention is zero discharge of pollutants. This is sometimes referred to as “virtual elimination”, since even zero discharge cannot solve the problem of contaminants already in the environment. Zero discharge of pollutants is possible using pollution prevention methods (while control methods cannot achieve zero in theory and are even less effective in practice, usually owing to lax enforcement). For instance, we can envisage automobile production in which there is zero discharge of pollutants from the plant; other waste is recycled and the product (the car) consists of parts which are reusable or recyclable. Certainly, zero discharge of specific pollutants has been achieved - for example, by modifying the production process in wood pulp mills so that no dioxins or furans are discharged in the effluent. The aim of zero discharge has also been written into environmental laws and into the policies of bodies commissioned to abate pollution.
In practice, zero discharge often gives way to target reductions - for example, a 50% reduction in pollution emissions by such-and-such a year. These targets or interim targets are usually in the form of “challenges” or aims by which to measure the success of the pollution prevention programme. They are rarely the product of a feasibility analysis or calculation, and there are invariably no penalties attached to failure to attain the target. Nor are they measured with any precision.
Reductions would have to be measured (as opposed to estimated) by variations on the formula:
Pollution (P) = Toxicity of the pollutant (T) × Volume (V) of the discharges
or:
P = T x V x E (exposure potential).
This is very difficult in theory and expensive in practice, though it could be done in principle by utilizing hazard assessment techniques (see below). The whole issue suggests that resources would be better allocated elsewhere - for example, in ensuring that proper pollution prevention plans are produced.
In regard to chemical pesticides, the objective of use-reduction can be achieved by the methods of integrated pest management (IPM), though this term, too, is capable of a wide or a strict definition.
Methods
The main methods of pollution prevention are:
- The elimination or phasing out of specific hazardous chemicals
- Input substitution - replacing a toxic or hazardous substance with a non-toxic or less hazardous substance or with a non-toxic process. Examples are the substitution of water-based for synthetic organic dyes in the printing industry; water - or citrus-based solvents for organic solvents; and, in some applications, the substitution of vegetable for mineral oils. Examples of non-chemical substitution include the substitution of pellet blasting technology for the use of fluid chemical paint strippers; the use of high-pressure hot water systems instead of caustic cleaning; and the substitution of kiln-drying for the use of pentachlophenols (PCPs) in the lumber industry.
In all cases, it is necessary to perform a substitution analysis to ensure that substitutes are genuinely less hazardous than what they replace. This is at least a matter of organized common sense, and at best the application of hazard assessment techniques (see below) to the chemical and its proposed substitute.
- Product reformulation - substituting for an existing end-product an end-product which is non-toxic or less toxic upon use, release or disposal
Whereas input substitution refers to the raw materials and adjuncts at the “front end” of the production process, product reformulation approaches the issue from the final product end of the production cycle.
General programmes to produce products which are more environmentally benign are examples of “economic conversion”. Examples of particular measures in the area of product reformulation include the production of rechargeable batteries instead of throw-away types and the use of water-based product coatings instead of those based on organic solvents and the like.
Again, substitution analysis will be necessary to ensure that the net environmental benefit is greater for the reformulated products that it is for the originals.
- Production unit redesign modernization or modification, which results in less chemical use or in the use of less toxic substances.
- Improved operation and maintenance of the production unit and production methods, including better housekeeping, more efficient production quality control, and process inspections.
Examples are spill prevention measures; the use of spill-proof containers; leak prevention; and floating lids for solvent tanks.
- Using less and reusing more. For instance, some degreasing operations take place too frequently on a single item. In other cases, chemicals can be used more sparingly in each operation. De-icing fluids can sometimes be reused, a case of “extended use”.
- Closed-loop methods and in-process recycling. Strictly speaking, a closed-loop process is one in which there are no emissions into the workplace or into the outside environment, not even waste water into surface water or carbon dioxide into the atmosphere. There are only inputs, finished products, and inert or non-toxic wastes. In practice, closed-loop methods eliminate some, but not all, hazardous releases. To the extent that this is achieved, it will count as a case of in-process recycling (see below).
Recycling
Any definition of pollution prevention is likely to result in a number of “grey areas” in which it is not easy to distinguish prevention measures from emission controls. For instance, to qualify as a prevention method, a phase of a production process may have to be “an integral part of the production unit”, but how far away the phase has to be from the periphery of the production process in order to qualify as a prevention measure is not always clear. Some processes may be so remote from the heart of an operation that they look more like an “add on” process and, thus, more like an “end of pipe” control measure than a prevention method. Again, there are unclear cases like a waste pipe that provides the feedstock for a neighbouring plant: taken together, the two plants provide a kind of closed loop; but the “upstream” plant still produces effluent and, thus, fails the prevention test.
Similarly with recycling. Conventionally, there are three types of recycling:
- in-process recycling - for example, when dry-cleaning solvent is filtered, cleaned and dried, then reused within a single process
- out-of-process but on-site, as when pesticide production waste is cleaned and then reused as the so-called inert base in a new production run
- out-of-process and off-site.
Of these, the third is usually ruled out as not qualifying as pollution prevention: the more remote the recycling site, the less of a guarantee that the recycled product is actually reused. There are also hazards in the transporting of waste to be recycled, and the financial uncertainty that the waste will have a continuous market value. Similar, though less acute, considerations apply to out-of-process but on-site recycling: there is always a possibility that the waste will not actually be recycled or, if recycled, not actually reused.
In the initial pollution prevention strategies of the 1980s, on-site but out-of-process recycling was ruled out as not being a genuine pollution prevention measure. There was a fear that an effective pollution prevention programme would be compromised or diluted by too great an emphasis on recycling. In the mid-1990s, some policy-makers are prepared to entertain on-site, out-of-process recycling as a legitimate pollution prevention method. One reason is that there are genuine “grey areas” between prevention and control. Another reason is that some on-site recycling really does do what it is supposed to do, even though it may not technically qualify as pollution prevention. A third reason is business pressure: employers see no reason why techniques should be ruled out it they serve the purposes of a pollution prevention programme.
Pollution prevention planning
Planning is an essential part of pollution prevention methodology, not least because the gains in both industrial efficiency and environmental protection are likely to be in the longer term (not immediate), reflecting the sort of planning that goes into product design and marketing. The production of periodic pollution prevention plans is the most usual way of realizing pollution prevention planning. There is no single model for such plans. One proposal envisages:
- aims and objectives
- chemical inventories and estimates of discharges into the environment
- pollution prevention methods used and methods proposed
- responsibilities and action in the event of the plan not being fulfilled or realized.
Another proposal envisages:
- a review of production processes
- identification of pollution prevention opportunities
- a ranking of the opportunities and a schedule for the implementation of the selected options
- measures of the success of the plan after the implementation period.
The status of such plans varies widely. Some are voluntary, though they can be spelled out in law as a (voluntary) code of practice. Others are mandatory in that they are required (1) to be kept on-site for inspection or (2) submitted to a regulatory authority on completion or (3) submitted to a regulatory authority for some form of scrutiny or approval. There are also variations, such as requiring a plan in the event that a “voluntary” plan is, in some way, inadequate or ineffective.
The degree to which mandatory plans are prescriptive also varies - for example, in regard to penalties and sanctions. Few authorities have the power to require specific changes in the content of pollution prevention plans; almost all have the power to require changes in the plan in the event that the formal requirements have not been met - for example, if some plan headings have not been addressed. There are virtually no examples of penalties or sanctions in the event that the substantive requirements of a plan have not been met. In other words, legal requirements for pollution prevention planning are far from traditional.
Issues surrounding the production of pollution prevention plans concern the degree of confidentiality of the plans: in some cases, only a summary becomes public, while in other cases, plans are released only when the producer fails in some way to comply with the law. In almost no cases do the requirements for pollution prevention planning override existing provisions regarding the trade secrecy or the business confidentiality of inputs, processes or the ingredients of products. In a few cases, community environmental groups have access to the planning process, but there are virtually no cases of this being required by law, nor are the legal rights of workers to participate in the production of plans widespread.
Legislation
In the Canadian provinces of British Columbia and Ontario, pollution prevention measures are “voluntary”; their effectiveness depends on “moral suasion” on the part of governments and environmentalists. In the United States, about half (26) of the states have some form of legislation, while in Europe, several northern countries have legislated clean technology programmes. There is quite a wide variety in both the content and the effectiveness of such legislation. Some laws define pollution prevention strictly; others define it widely or loosely and cover a wide variety of environmental protection activities concerning pollution and waste, not just pollution prevention. The New Jersey law is highly prescriptive; those of the Commonwealth of Massachusetts and the States of Minnesota and Oregon involve a high degree of government scrutiny and assistance; that of Alaska is little more than a statement of the government’s intentions.
Health, safety and employment
Pollution prevention is of central concern to occupational health: if the use of toxic substances decreases, there will almost always be a corresponding decrease in worker exposure to toxic substances and, thus, in industrial diseases. This is a prime case of prevention “at the source” of the hazard and, in many cases, the elimination of hazards by “engineering controls”
(i.e., methods), the first and best line of defence against chemical hazards. However, such preventive measures are different from one traditional strategy, which is the “total isolation” or the “total enclosure” of a chemical process. While total enclosure is highly useful and highly desirable, it does not count as a pollution prevention method since it controls, rather that reduces intrinsically, an existing hazard.
The pollutants which pose hazards to workers, communities and the physical environment alike, have usually been addressed primarily because of their impact on human communities (environmental health). Though the greatest exposures are often received by workers within a workplace (workplace pollution), this has not, so far, been the prime focus of pollution prevention measures. The Massachusetts legislation, for instance, aims to reduce the risks to the health of workers, consumers and the environment without shifting the risks between workers, consumers and parts of the environment (New Jersey is similar). But there was no attempt to focus on workplace pollution as a major detriment, nor was there a requirement to accord a primacy to the chief human exposures to hazards - often the workers. Nor is there any requirement to train workers in the discipline of pollution prevention.
There are several reasons for this. The first is that pollution prevention is a new discipline in the context of a general, traditional failure to see environmental protection as a function of processes utilized and adopted within workplaces. A second reason is that worker-management co-determination in the area of environmental protection is not well advanced. Workers in many countries have legal rights, for instance, to joint workplace health and safety committees; to refuse unsafe or unhealthy work; to health and safety information; and to training in health and safety issues and procedures. But there are few legal rights in the parallel and often overlapping area of environmental protection, such as the right to joint union-management environment committees; the right of employees to “blow the whistle” (go public) on an employer’s anti-environmental practices; the right to refuse to pollute or to degrade the outside environment; the right to environmental information; and the right to participate in workplace environmental audits (see below).
The impacts of pollution prevention planning on employment are hard to gauge. The explicit aim of pollution prevention initiatives is often to increase industrial efficiency and environmental protection at the same time and by the same set of measures. When this happens, the usual effect is to decrease overall employment within any given workplace (because of technological innovation) but to increase the skills required and then to increase job security (because there is planning for a longer-term future). To the extent that the use of raw materials and adjuncts is reduced, there will be decreased chemical manufacturing employment, though this is likely to be offset by the implied transition of feedstock to speciality chemicals and by the development of alternatives and substitutes.
There is one aspect of employment which pollution prevention planning cannot address. Pollution emissions from a single facility may decrease but to the extent that there is an industrial strategy to create wealth and value-added employment, an increase in the number of production facilities (however “clean”) will tend to nullify the environmental protection gains already achieved. The most notorious failing in environmental protection measures - that pollution emission reductions and controls are nullified by an increase in the number of sources - applies, unfortunately, to pollution prevention as well as to any other form of intervention. Ecosystems, according to one respected theory, have a “carrying capacity”, and that limit can be reached equally by a small number of highly polluting or “dirty” sources or by a correspondingly large number of clean ones.
Workplace environmental audits
Pollution prevention planning can form part of or be accommodated in a workplace environmental audit. Though there are many versions of such audits, they are likely to be in the form of a “site audit” or “production audit”, in which the whole production cycle is subjected to both an environmental and a financial analysis.
There are roughly three areas of sustainable development and environmental protection which can be covered in a workplace audit:
- the conservation of natural resource inputs - for example, minerals, water and wood products
- energy use, which may also include consideration of energy sources, energy efficiency, energy intensiveness and energy conservation
- pollution prevention, control and remediation.
To the extent that pollution prevention is successful, there will be a corresponding decrease in the importance of control and remediation measures; pollution prevention measures can form a major part of a workplace environmental audit.
Traditionally, businesses were able to “externalize” environmental detriments through such means as the profligate use of water or unloading their wastes onto the outside community and the environment. This has led to demands for taxes on the “front end” such as water use or on “outputs” such as environmentally unfriendly products or on wastes (“pollution taxes”).
In this way, costs to business are “internalized”. However, it has proved difficult to put the right price on the inputs and on the detriments - for example, the cost to communities and the environment of wastes. Nor is it clear that pollution taxes reduce pollution in proportion to the amounts levied; taxes may well “internalize” costs, but they otherwise only add to the cost of doing business.
The advantage of environmental auditing is that the audit can make economic sense without having to “cost” externalities. For instance, the “value” of waste can be calculated in terms of resource input loss and energy “non-utilization” (inefficiency) - in other words, of the difference in value between resources and energy on one side and the value of the product on the other. Unfortunately, the financial side of pollution prevention planning and its part in workplace environmental audits is not well advanced.
Hazard assessment
Some pollution prevention schemes work without any hazard evaluation - that is, without criteria to decide whether a plant or facility is more or less environmentally benign as a result of pollution prevention measures. Such schemes may rely on a list of chemicals which are objects of concern or which define the scope of the pollution prevention programme. But the list does not grade chemicals as to their relative hazardousness, nor is there a guarantee that a chemical substitute not on the list is, in fact, less hazardous than a listed chemical. Common sense, not scientific analysis, tells us how to go about implementing a pollution prevention programme.
Other schemes rest on criteria for assessing hazardousness, that is, on hazard assessment systems. They work, essentially, by laying down a number of environmental parameters, such as persistence and bioaccumulation in the environment, and a number of human health parameters which serve as measures of toxicity - for example, acute toxicity, carcinogenicity, mutagenicity, reproductive toxicity and so on.
There is then a weighted scoring system and a decision procedure for scoring those parameters on which there is inadequate information on the chemicals to be scored. Relevant chemicals are then scored and ranked, then (often) assembled in groups in descending order of hazardousness.
Though such schemes are sometimes devised with a specific purpose in mind - for example, for assessing priorities for control measures or for elimination (banning) - their essential use is as an abstract scheme which can be used for a large variety of environmental protection measures, including pollution prevention. For instance, the top group of scored chemicals could be the prime candidates for a mandatory pollution prevention programme, or they could be candidates for phasing-out or substitution. In other words, such schemes do not tell us how much we should reduce environmental health hazards; they tell us only that any measures we take should be informed by the hazard assessment scheme.
For instance, if we have to make decisions about substituting a less hazardous chemical for a more dangerous one, we can use the scheme to tell us whether, prima facie, the substitution decision is a good one: we run both chemicals through the scheme to determine whether there is a wide or merely a narrow gap between them regarding their hazardousness.
There are two sorts of considerations which rarely fall within the scope of hazard assessment schemes. The first is exposure data, or the potential for human exposure to the chemical. The latter is difficult to calculate, and, arguably, it distorts the “intrinsic hazard” of the chemicals concerned. For instance, a chemical could be accorded an artificially low priority on the grounds that its exposure potential is low; though it may, in fact, be highly toxic and relatively easy to deal with.
The second sort of consideration is the socioeconomic impact of eliminating or reducing the use of the chemical concerned. While we can start to make substitution decisions on the basis of the hazard analysis, we would have to make a further and distinct socioeconomic analysis and consider, for example, the social utility of the product associated with the chemical use (which may, e.g., be a useful drug), and we would also have to consider the impact on workers and their communities. The reason for keeping such analysis separate is that it is impossible to score the results of a socioeconomic analysis in the same way that the intrinsic hazards of chemicals are scored. There are two entirely distinct sets of values with different rationales.
However, hazard assessment schemes are crucial in assessing the success of pollution prevention programmes. (They are also relatively new, both in their impact and their utility.) For instance, it is possible to apply them without reference to risk assessments, risk analysis and (with reservations) without reference to cost-benefit analysis. An earlier approach to pollution was to first do a risk assessment and only then decide what sort of action, and how much, was necessary to reduce the risk to an “acceptable” level. The results were rarely dramatic. Hazard assessment, on the other hand, can be utilized very quickly and in such a way that it does not delay or compromise the effectiveness of a pollution prevention programme. Pollution prevention is, above all, a pragmatic programme capable of constantly and speedily addressing pollution issues as they arise and before they arise. It is arguable that traditional control measures have reached their limit and only the implementation of comprehensive pollution prevention programmes will be capable of addressing the next phase of environmental protection in a practical and effective way.
Case Study: Canadian Multimedia Pollution Control and Prevention on the Great Lakes
The Challenge
The Great Lakes are a shared resource between Canada and the United States (see figure 1). The five large lakes contain over 18% of the world’s surface water. The basin is home to one in every three Canadians (approximately 8.5 million ) and one in every nine Americans (27.5 million). The basin is the industrial heartland of both countries - one-fifth of the US industrial base and one-half of Canada’s. Economic activities around the Great Lakes basin generate an estimated 1 trillion dollars of wealth each year. Over time, increasing population and industrial activities created a variety of stresses on the lakes until the need for concerted action to protect the Great Lakes by the two countries was recognized in mid-century.
Figure 1. Great Lakes drainage basin: St. Lawrence River

The Response
Since the 1950s, both countries have put in place domestic and bilateral programmes to address gross pollution problems and also to respond to more subtle water quality concerns. As a result of these actions, Great Lakes waters are visibly cleaner than they were at mid-century, loadings of heavy metals and organic chemicals have decreased and contaminant levels in fish and aquatic birds have gone down significantly. The successes of Canada–United States actions to restore and protect the Great Lakes provide a model for bilateral cooperation on resource management, but challenges remain.
The Case Study in Perspective
The threats posed by persistent toxic substances, however, are long term in nature and their management requires a multimedia, comprehensive at-source approach. To achieve a long-term goal of virtual elimination of persistent toxic substances from the Great Lakes, environmental authorities, industries and other stakeholders in the basin were challenged to develop new approaches and programmes. The purpose of this case study report is to provide a brief summary of Canadian pollution control programmes and the progress achieved by 1995, and to outline initiatives for managing persistent toxics in the Great Lakes. Similar US initiatives and programmes are not discussed herein. Interested readers should contact the Great Lakes National Program Office of the US Environmental Protection Agency in Chicago for information on federal and state programmes for protecting the Great Lakes.
1970s–1980s
A significant problem acknowledged to be affecting Lake Erie in the 1960s was nutrient enrichment or eutrophication. The identified need for bilateral actions prompted Canada and the United States to sign the first Great Lakes Water Quality Agreement (GLWQA) in 1972. The Agreement outlined abatement goals for reducing phosphorus loadings primarily from laundry detergents and municipal sewage effluent. In response to this commitment Canada and Ontario enacted legislation and programmes for controlling point sources. Between 1972 and 1987, Canada and Ontario invested more than 2 billion dollars in sewage treatment plant construction and upgrading in the Great Lakes basin.
Figure 2. Progress on industrial abatement
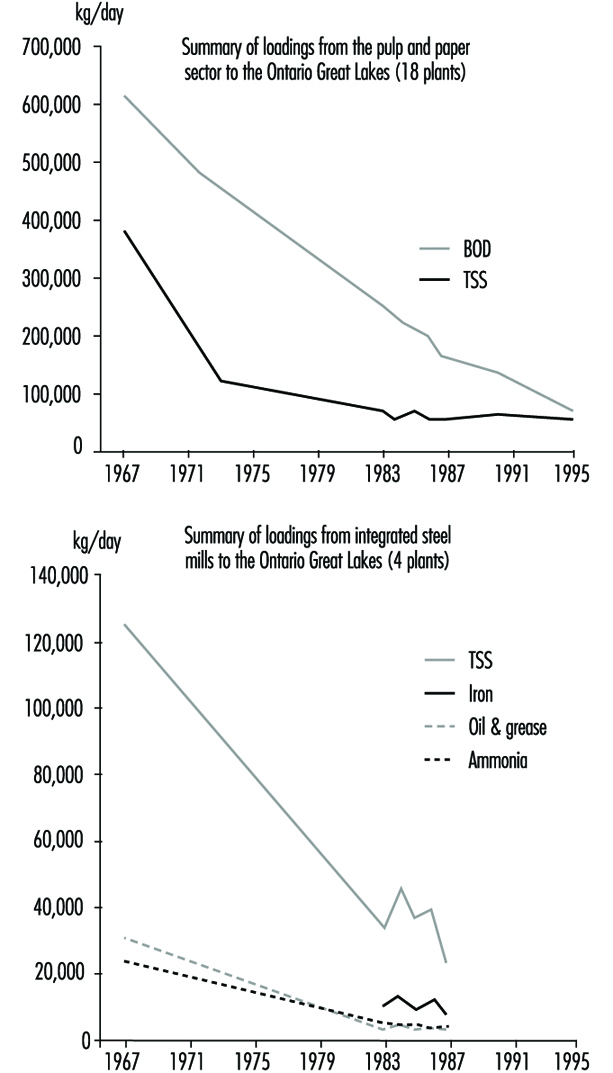
The 1972 GLWQA also identified the need to reduce releases of toxic chemicals into the lakes from industries and other sources such as spills. In Canada, the promulgation of federal effluent (end of pipe) regulations in the 1970s for conventional pollutants from major industrial sectors (pulp and paper, metal mining, petroleum refining and so on) provided a national baseline standard, while Ontario established similar effluent guidelines tailored for local needs including the Great Lakes. Actions by industries and municipalities to meet these federal and Ontario effluent requirements produced impressive results; for example, phosphorus loadings from point sources to Lake Erie were reduced by 70% between 1975 and 1989, and discharges of conventional pollutants from the seven Ontario petroleum refineries were cut by 90% since the early 1970s. Figure 2 shows similar loading reduction trends for the pulp and paper and the iron and steel sectors.
By the mid-1970s evidence of elevated concentrations of toxic chemicals in Great Lakes fish and wildlife, reproductive abnormalities in some fish-eating birds and population decline in a number of species implicated persistent bioaccumulative toxic substances, which became the new focus for the binational protection effort. Canada and the United States signed a second Great Lakes Water Quality Agreement in 1978, in which the two countries pledged to “restore and maintain the chemical, physical and biological integrity of the waters of the Great Lakes Ecosystem”. A key challenge was the policy “that the discharge of toxic substances in toxic amounts be prohibited and the discharge of any or all persistent toxic substances be virtually eliminated”. The call for virtual elimination was necessary, as persistent toxic chemicals may concentrate and accumulate in the food chain, causing severe and irreversible damages to the ecosystem, whereas chemicals which are not persistent needed to be kept below levels which cause immediate harm.
In addition to tighter controls on point sources, Canada and Ontario developed and/or strengthened controls on pesticides, commercial chemicals, hazardous wastes and non-point sources of pollution such as dump sites and incinerators. Government initiatives became more multimedia oriented, and the concept of “cradle to grave” or “responsible care” for chemicals became the new environmental management philosophy for government and industries alike. A number of persistent toxic pesticides were banned under the federal Pest Control Products Act (DDT, Aldrin, Mirex, Toxaphene, Chlordane) and the Environmental Contaminants Act was used to (1) prohibit commercial, manufacturing and processing uses of persistent toxics (CFC, PPB, PCB, PPT, Mirex, lead) and (2) to limit chemical releases from specific industrial operations (mercury, vinyl chloride, asbestos).
By the early 1980s, results from these programmes and measures and similar American efforts started producing evidence of a rebound. Contaminant levels in Great Lakes sediments, fish and wildlife were on the decline, and noted environmental improvements included the return of bald eagles to the Canadian shore of Lake Erie, a 200-fold increase in cormorant population, a resurgence in osprey on Georgian Bay and the re-establishment in the Toronto Harbour area of common terns - all have been affected by levels of persistent toxic substances in the past, and their recovery illustrates the success of this approach to date.
Figure 3. Mirex in herring gull eggs

The trend toward reduced concentrations for some of the persistent toxic substances in fish, wildlife and sediments levelled off by the mid-1980s (see Mirex in herring gull eggs in figure 3). It was concluded by scientists that:
- While the water pollution and contaminants control programmes in place were helpful, they were not enough to bring about further reductions in contaminant concentrations.
- Additional measures were required for non-point sources of persistent toxics including contaminated sediments, long range atmospheric input of pollutants, abandoned dump sites and so on.
- Some pollutants can persist in the ecosystem at minute concentrations and can bioaccumulate in the food chain for a long time.
- The most efficient and effective approach for dealing with persistent toxics is to prevent or eliminate their generation at source rather than virtually eliminate their release.
It was generally agreed that achieving virtual elimination in the environment through the application of zero-discharge philosophy to sources and the ecosystem approach to Great Lakes water quality management needed to be further strengthened and promoted.
To reaffirm their commitment to the virtual elimination goal for persistent toxic substances, Canada and the United States amended the 1978 Agreement through a protocol in November 1987 (United States and Canada 1987). The protocol designated areas of concern where beneficial uses have been impaired around the Great Lakes, and required the development and implementation of remedial action plans (RAPs) for both point and non-point sources in the designated areas. The protocol also stipulated lakewide management plans (LAMPs) to be used as the main framework for resolving whole-lake impairment of beneficial uses and for coordinating control of persistent toxic substances impacting each of the Great Lakes. Furthermore, the protocol included new annexes for establishing programmes and measures for airborne sources, contaminated sediments and dump sites, spills and control of exotic species.
1990s
Following the signing of the 1987 protocol, the goal of virtual elimination was strongly promoted by environmental interest groups on both sides of the Great Lakes as concerns about the threat of persistent toxics increased. The International Joint Commission (IJC), the binational advisory body created under the 1909 Boundary Waters Treaty, also strongly advocated the virtual elimination approach. An IJC binational task force recommended a strategy for Virtual Elimination in 1993 (see figure 4). By the mid-1990s, the IJC and the parties are attempting to define a process for implementing this strategy, including considerations for socioeconomic impacts.
Figure 4. Decision-making process for virtual elimination of persistent toxic substances from the Great Lakes
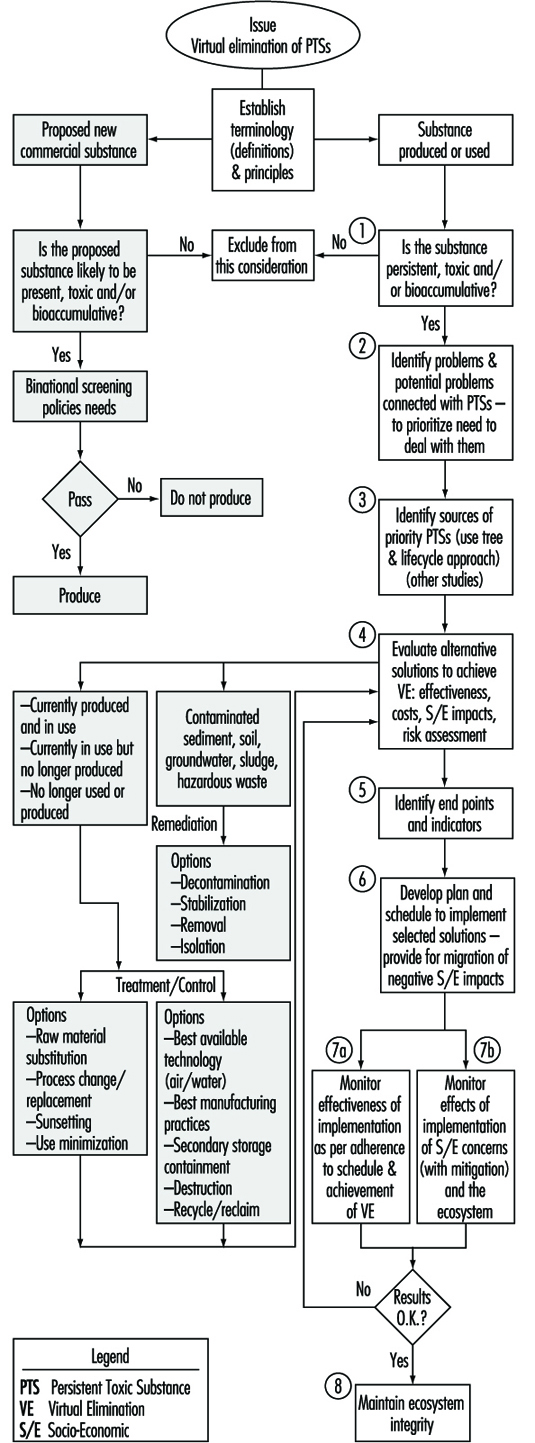
The governments of Canada and Ontario responded in a number of ways to control or reduce the release of persistent toxics. The important programmes and initiatives are briefly summarized below.
Canadian Environmental Protection Act (CEPA)
In 1989, Environment Canada consolidated and streamlined its legal mandates into a single statute. CEPA provides the federal government with comprehensive powers (e.g., information gathering, regulations making, enforcement) over the entire life cycle of chemicals. Under CEPA, the New Substances Notification Regulations establish screening procedures for new chemicals so that persistent toxics that cannot be adequately controlled will be prohibited from being imported, manufactured or used in Canada. The first phase of the Priority Substances List (PSL I) assessment programme was completed in 1994; 25 of the 44 substances assessed were found to be toxic under the definition of CEPA, and the development of management strategies for these toxic chemicals was initiated under a Strategic Options Process (SOP); an additional 56 priority substances will be nominated and assessed in phase II of the PSL programme by the year 2000. The National Pollutant Release Inventory (NPRI) was implemented in 1994 to mandate industrial and other facilities that meet the reporting criteria to annually report their releases to air, water and land, and their transfers in waste, of 178 specified substances. The inventory, modelled on the Toxic Release Inventory (TRI) in the United States, provides an important database for prioritizing pollution prevention and abatement programmes.
Canada-Ontario Agreement (COA)
In 1994, Canada and Ontario set out a strategic framework for coordinated action to restore, protect and conserve the Great Lakes ecosystem with a key focus on reducing the use, generation or release of 13 Tier I persistent toxic substances by the year 2000 (Canada and Ontario 1994). COA also targets an additional list of 26 priority toxics (Tier II) for significant reductions. Specifically for Tier I substances, COA will: (1) confirm zero discharge of five banned pesticides (Aldrin, DDT, Chlordane, Mirex, Toxaphene); (2) seek to decommission 90% of high-level PCBs, destroy 50% now in storage and accelerate destruction of low-level PCBs in storage; and (3) seek 90% reduction in the release of the remaining seven Tier I substances (benzo(a)pyrene, hexachlorobenzene, alkyl-lead, octachlorostyrene, PCDD (dioxins) PCDF (furans) and mercury).
The COA approach is to seek quantitative reductions wherever feasible, and sources are challenged to apply pollution prevention and other means to meet the COA targets. Fourteen projects have already been launched by federal Ontario staff to achieve reduction/elimination of Tiers I and II substances.
Toxic Substances Management Policy
In recognition of the need for a preventive and precautionary approach, Environment Canada announced in June 1995 a national Toxic Substances Management Policy as the framework for efficient management of toxic substances in Canada (Environment Canada 1995a). The policy adopts a two-track approach (see figure 5) that recognizes management actions must be tailored to the characteristics of chemicals; that is:
- to virtually eliminate from the environment substances that are predominantly anthropogenic, persistent, bioaccumulative and toxic (Track I)
- to implement full life cycle (cradle-to-grave) management of all other substances of concern (Track II).
Figure 5. Selection of management objectives under the Toxic Substances Management Policy
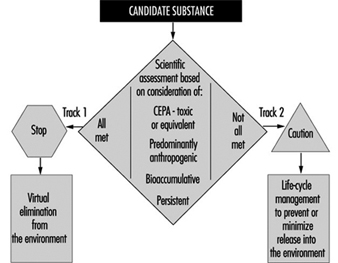
A set of scientifically based criteria (Environment Canada 1995b) (see table 1) will be used to categorize substances of concern into the two tracks. If a substance identified for either track is not adequately controlled under existing programmes, additional measures will be identified under the multi-stakeholder Strategic Options Process. The policy is consistent with the Great Lakes Water Quality Agreement and will direct and frame a number of domestic programmes by defining their ultimate environmental objective, but the means and pace of achieving the ultimate objective will vary by chemical and source. Further, Canada’s position on persistent toxics will also be framed by this policy in international discussions.
Table 1. Criteria for the selection of substances for Track 1 toxic substances management policy
|
Persistence |
Bioaccumulation |
Toxicity |
Predominantly Anthropogenic |
|
|
Medium |
Half-life |
|||
|
Air |
≥2 days |
BAF≥5,000 |
CEPA-toxic |
Concentration |
Chlorine Action Plan
A comprehensive approach to managing chlorinated substances within the context of the Toxic Substances Management Policy was announced in October 1994 by Environment Canada (Environment Canada 1994). The approach will be to prune the chlorine-use tree with a five-part action plan that will (1) target action on critical uses and products, (2) improve scientific understanding of chlorine and its impact on health and the environment, (3) detail socioeconomic implications, (4) improve public access to information and (5) promote international actions on chlorinated substances. Chlorine use has already decreased in Canada in recent years, for example by 45% in the pulp and paper sector since 1988. Implementation of the Chlorine Action Plan will accelerate this reduction trend.
Great Lakes Pollution Prevention Initiative
A strong pollution prevention programme has been put in place for the Great Lakes basin. Since March 1991, Environment Canada and the Ontario Ministry of the Environment and Energy have been working together with industries and other stakeholders to develop and implement pollution prevention projects, in contrast to waste treatment or reducing pollution after its generation. In 1995/96, more than 50 projects will cover commercial chemicals, hazardous waste management, federal facilities, industries, municipalities and the Lake Superior basin. Figure 6 provides an overview of these projects, which fall into two main categories: programme integration or voluntary agreements. The figure also shows programme linkages with other programmes discussed earlier (NPRI, RAP, LAMP) and a number of institutions that work with Environment Canada closely on green technologies and clean processes, as well as on training, information and communications. Pollution prevention projects can produce impressive results, as evidenced by the Automotive Manufacturers, who have undertaken 15 pilot projects recently, thereby reducing or eliminating 2.24 million kilograms of targeted substances from the manufacture of automobiles at the Ontario facilities of Chrysler, Ford and General Motors.
Figure 6. Great Lakes pollution prevention
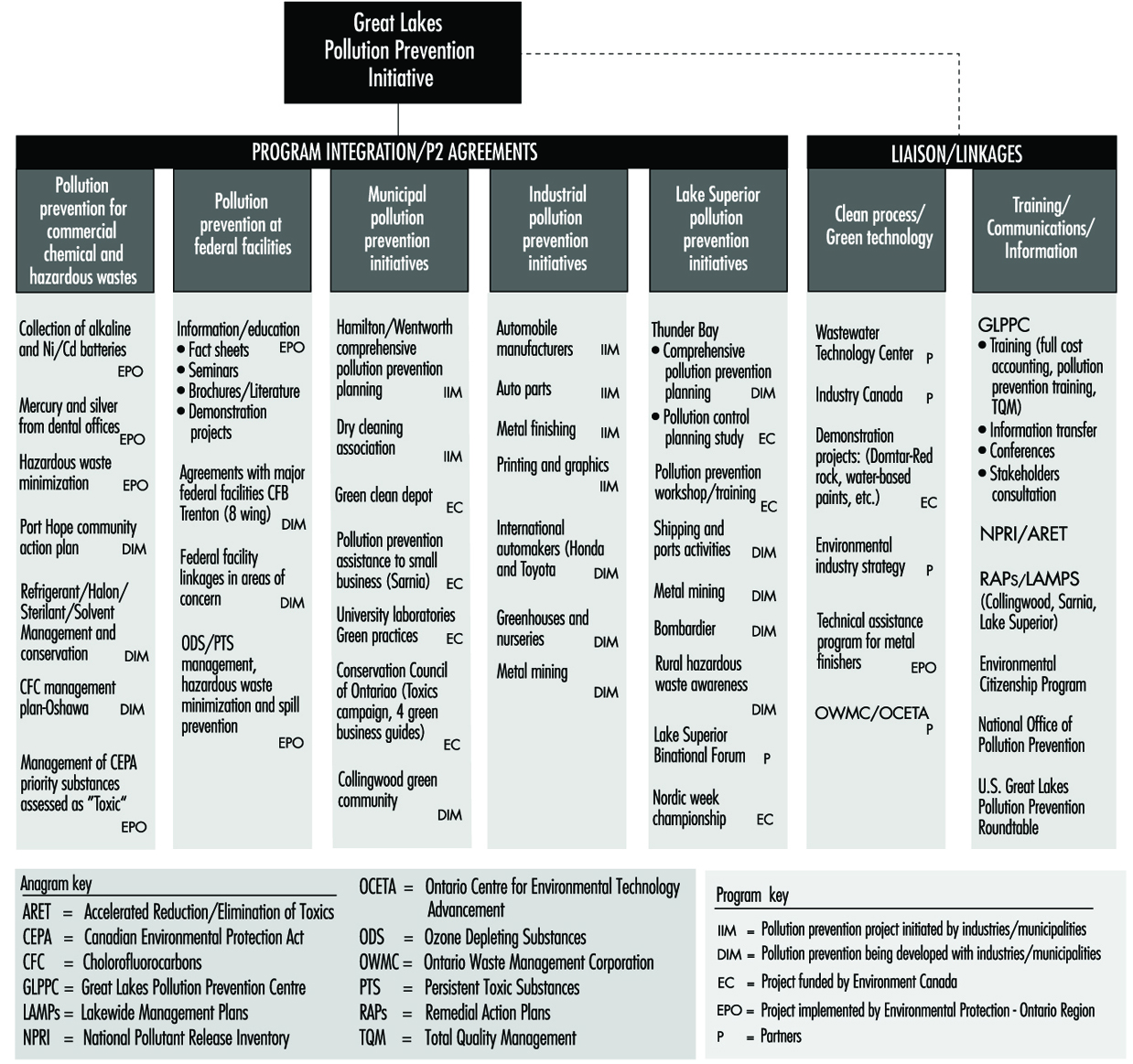
Accelerated Reduction/Elimination of Toxics (ARET)
ARET is a cooperative multi-stakeholder initiative launched in 1994 that seeks the eventual elimination of 14 priority toxics with an interim target (by the year 2000) of a 90% reduction/elimination and reduced emission (50%) of 87 less harmful toxic substances (ARET Secretariat 1995). As of 1995, more than 200 companies and government agencies are participating in this voluntary initiative. Together, they reduced emissions by 10,300 tonnes in comparison with the 1988 base year and are committed to an additional 8,500 tonnes reduction by the year 2000.
Binational and international strategies
In addition to the above domestic initiatives, Canada and the United States are currently developing a binational strategy to coordinate agency action and to establish shared goals for persistent toxics in the Great Lakes basin. Goals and objectives similar to the Canada-Ontario Agreement for the Tiers I and II substances and a similar US list will be adopted. Joint projects will be developed and implemented to facilitate information exchange and agency action on priority chemicals such as PCBs and mercury. By taking an aggressive approach to virtual elimination as outlined above, Canada will be able to assume a leadership role in promoting international action on persistent toxics. Canada hosted a United Nations conference in June 1995 in Vancouver to focus global dialogue on persistent organic pollutants (POP) and to explore pollution prevention approaches to reducing their emissions around the world. Canada also co-chairs the United Nations Economic Commission for Europe (UNECE) workgroup to develop a protocol for persistent organic pollutants under the Convention on Long Range Transboundary Air Pollution.
An Example—Dioxins and Furans
For more than a decade, polychlorinated dibenzo-dioxins and furans have been recognized as a group of persistent toxics of concern to the Canadian environment and the Great Lakes. Table 2 summarizes federal actions and the reductions in releases achieved to date, illustrating the mix of programmes and initiatives which has resulted in significant reductions of these toxics. In spite of these impressive results, dioxins and furans will remain priorities under the Toxic Substances Management Policy, the Chlorine Action Plan, the Canada Ontario Agreement and the binational strategy outlined above, because virtual elimination requires further reductions.
Table 2. Summary of reductions in releases of dioxin and furan in Canada
|
Sources of Emissions |
Reductions |
Reporting Period |
Canadian Government Initiatives |
|
Bleached kraft pulpmill effluents |
82% |
1989-94 |
CEPA defoamer, wood chip and |
|
2,4,5-T—pesticide |
100% |
1985 |
Banned from use under PCPA |
|
2,4-D—pesticide |
100% |
1987-90 |
Dioxin content and use heavily |
|
Pentachlorophenol |
|
|
|
|
PCBs |
23% |
1984-93 |
CCME PCB Action Plan |
|
Incineration |
|
|
|
CCME: Canadian Council of Environmental Ministers; CEPA: Canadian Environmental Protection Act; PCPA: Pest Control Products Act.
Summary
There has been a significant improvement in the water quality of the Great Lakes as a result of pollution control actions taken by governments and stakeholders in Canada and the United States since the early 1970s. This case study report provides a summary of the Canadian effort and successes in dealing with gross pollution and conventional pollutants. It also outlines the evolution of a new approach (the Toxic Substances Management Policy, the Chlorine Action Plan, pollution prevention, voluntary action, stakeholder consultations and so on) for dealing with the much more difficult problems with persistent toxic substances in the Great Lakes. Comprehensive programmes (COA, NPRI, SOP, PSL and so on) that are being put in place with the aim of achieving the virtual elimination goal are briefly described. Details of the Canadian approach are contained in the listed references.
Solid Waste Management and Recycling
Solid wastes are traditionally described as residual products, which represent a cost when one has to resort to disposal.
Management of waste encompasses a complex set of potential impacts on human health and safety, and the environment. The impacts, although the type of hazards may be similar, should be distinguished for three distinct types of operation:
- handling and storage at the waste producer
- collection and transportation
- sorting, processing and disposal.
One should bear in mind that health and safety hazards will arise where the waste is produced in the first place - in the factory or with the consumer. Hence, waste storage at the waste generator - and especially when waste is separated at source - may cause harmful impact on the nearby surroundings. This article will focus on a framework for understanding solid waste management practices and situating the occupational health and safety risks associated with the waste collection, transportation, processing and disposal industries.
Why Solid Waste Management?
Solid waste management becomes necessary and relevant when the structure of the society changes from agricultural with low-density and widespread population to urban, high-density population. Furthermore, industrialization has introduced a large number of products which nature cannot, or can only very slowly, decompose or digest. Hence, certain industrial products contain substances which, due to low degradability or even toxic characteristics, may build up in nature to levels representing a threat to humanity’s future use of the natural resources - that is, drinking water, agricultural soil, air and so on.
The objective of solid waste management is to prevent pollution of the natural environment.
A solid waste management system should be based on technical studies and overall planning procedures including:
- studies and estimates on waste composition and amounts
- studies on collection techniques
- studies on processing and disposal facilities
- studies on prevention of pollution of the natural environment
- studies on occupational health and safety standards
- feasibility studies.
The studies must include protection of the natural environment and occupational health and safety aspects, taking the possibilities of sustainable development into consideration. As it seldom is possible to solve all problems at one time, it is important at the planning stage to note that it is helpful to set up a list of priorities. The first step in solving environmental and occupational hazards is to recognize the existence of the hazards.
Principles of Waste Management
Waste management involves a complex and wide range of occupational health and safety relations. Waste management represents a “reverse” production process; the “product” is removal of surplus materials. The original aim was simply to collect the materials, reuse the valuable part of the materials and dispose of what remained at the nearest sites not used for agriculture purposes, buildings and so on. This is still the case in many countries.
Sources of waste can be described by the different functions in a modern society (see table 1).
Table 1. Sources of waste
|
Activity |
Waste description |
|
Industry |
Product residues |
|
Wholesale |
Default products |
|
Retail |
Transport packaging |
|
Consumer |
Transport packaging |
|
Construction and demolition |
Concrete, bricks, iron, soil, etc. |
|
Infrastructure activities |
Park waste |
|
Waste processing |
Rejects from sorting facilities |
Each type of waste is characterized by its origin or what type of product it was before it became waste. Hence, basically its health and safety hazards should be laid down upon the restriction of handling the product by the waste producer. In any case, storage of the waste may create new and stronger elements of hazards (chemical and/or biological activity in the storage period).
Solid waste management can be distinguished by the following stages:
- separation at source into specific waste fraction depending on material characteristics
- temporary storage at the waste producer in bins, sacks, containers or in bulk
- collection and transportation by vehicle:
- manual, horse team, motorized and so on
- open platform, closed truck body, compacting unit and so on
- transfer station: compaction and reloading to larger transport units
- recycling and/or waste processing facilities
- waste processing:
- manual or mechanical sorting out into different material fractions for recycling
- processing of presorted waste fractions to secondary raw materials
- processing for new (raw) materials
- incineration for volume reduction and/or energy recovery
- anaerobic digestion of organics for production of soil conditioner, fertilizer and energy (biogas)
- composting of organics for production of soil conditioner and fertilizer
- waste disposal:
- landfill, which should be designed and located to prevent migration of polluted water (landfill leachate), especially into drinking water resources (groundwater resources, wells and rivers).
Recycling of waste can take place at any stage of the waste system, and at each stage of the waste system, special occupational health and safety hazards may arise.
In low-income societies and non-industrial countries, recycling of solid waste is a basic income for the waste collectors. Typically, no questions are put on the health and safety hazards in these areas.
In the intensely industrialized countries, there is a clear trend for putting increased focus on recycling of the huge amounts of waste produced. Important reasons go beyond the direct market value of the waste, and include the lack of proper disposal facilities and the growing public awareness of the imbalance between consumption and protection of the natural environment. Thus, waste collection and scavenging have been renamed recycling to upgrade the activity in the mind of the public, resulting in a steeply growing awareness of the working conditions in the waste business.
Today, the occupational health and safety authorities in the industrialized countries are focusing on working conditions which, a few years ago, passed off unnoticed with unspoken acceptance, such as:
- improper heavy lifting and excessive amount of materials handled per working day
- inappropriate exposure to dust of unknown composition
- unnoticed impact by micro-organisms (bacteria, fungi) and endotoxins
- unnoticed exposure to toxic chemicals.
Recycling
Recycling or salvaging is the word covering both reuse (use for the same purpose) and reclamation/recovery of materials or energy.
The reasons for implementing recycling may change depending on national and local conditions, and the key ideas in the arguments for recycling may be:
- detoxification of hazardous waste when high environmental standards are set by the authorities
- resource recovery in low income areas
- reduction of volume in areas where landfilling is predominant
- energy recovery in areas where conversion of waste to energy can replace fossil fuel (coal, natural gas, crude oil and so on) for energy production.
As previously mentioned, recycling can occur at any stage in the waste system, but recycling can be designed to prevent waste from being “born”. That is the case when products are designed for recycling and a system for repurchasing after end-use, for instance by putting a deposit on beverage containers (glass bottles and so on).
Hence, recycling may go further than mere implementation of reclamation or recovery of materials from the waste stream.
Recycling of materials implies, in most situations, separation or sorting of the waste materials into fractions with a minimum degree of fineness as a prerequisite to the use of the waste as a substitute for virgin or primary raw materials.
The sorting may be performed by waste producers (source separation), or after collection, meaning separation at a central sorting plant.
Source Separation
Source separation will, by today’s technology, result in fractions of waste which are “designed” for processing. A certain degree of source separation is inevitable, as some mixtures of waste fractions can be separated into usable material fractions again only by great (economic) effort. The design of source separation must always take the final type of recycling into consideration.
The goal of the source sorting system should be to avoid a mixing or pollution of the different waste fractions, which could be an obstacle to easy recycling.
The collection of source-sorted waste fractions will often result in more distinct occupational health and safety hazards than does collection in bulk. This is due to concentration of specific waste fractions - for instance, toxic substances. Sorting out of easily degradable organics may result in producing high levels of exposure to hazardous fungi, bacteria, endotoxins and so on, when the materials are handled or reloaded.
Central Sorting
Central sorting may be done by mechanical or manual methods.
It is the general opinion that mechanical sorting without prior source separation by today’s known technology should be used only for production of refuse derived fuel (RDF). Prerequisites for acceptable working conditions are total casing of the mechanical equipment and use of personal “space suits” when service and maintenance have to be carried out.
Mechanical central sorting with prior source separation has, with today’s technology, not been successful due to difficulties in reaching proper sorting efficiency. When the characteristics of the sorted out waste fractions become more clearly defined, and when these characteristics become valid on a national or international basis, then it can be expected that new proper and efficient techniques will be developed. The success of these new techniques will be closely linked to prudent consideration to obtaining acceptable working conditions.
Manual central sorting should imply prior source separation to avoid occupational health and safety hazards (dust, bacteria, toxic substances and so on). The manual sorting should be limited to only a limited number of waste fraction “qualities” to avoid foreseeable sorting mistakes at the source, and to facilitate easy control facilities at the plant’s reception area. As the waste fractions become more clearly defined, it will be possible to develop more and more devices for automatic sorting procedures to minimize direct human exposure to noxious substances.
Why Recycling?
It is important to note that recycling is not a waste processing method that should be seen independently of other waste management practices. In order to supplement recycling, it is necessary to have access to a properly managed landfill and perhaps to more traditional waste processing facilities such as incineration plants and composting facilities.
Recycling should be evaluated in connection with
- local supply of raw materials and energy
- what is substituted - renewable (i.e., paper/tree) resources or non-renewable (i.e., oil) resources.
As long as oil and coal are used as energy resources, for example, incineration of waste and refuse-derived fuel with energy recovery will constitute a viable waste management option based on energy recovery. Minimization of waste quantities by this method, however, must end in final deposits subject to extremely strict environmental standards, which may be very expensive.
Principles of Waste Management
Environmental awareness is leading to a rapid transformation of waste management practices. Interpretation of this change is necessary before examining in more detail the methods that are applied to waste management and to the handling of residues.
Modern principles of waste management are based on the paradigm of a geared connection between the biosphere and the anthroposphere. A global model (figure 1) relating these two spheres is based on the assumption that all materials drawn out of the environment end up as waste either directly (from the production sector) or indirectly (from the recycling sector), bearing in mind that all consumption waste flows back to this recycling sector either for recycling and/or for disposal.
Figure 1. A global model of the principles of waste management
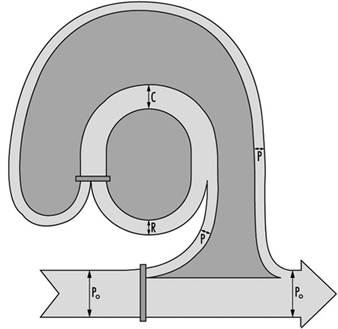
From this perspective, recycling must be defined broadly: from the recycling of whole objects (returnables), to the recycling of objects for some of their spare parts (e.g., cars, computers), to the production of new materials (e.g., paper and cardboard, tin cans) or the production of similar objects (recycling, downcycling and so on). Over the long term, this model can be visualized as a steady-state system wherein goods end up as waste after a few days or often a few years.
Deductions from the Model
Some major deductions can be made from this model, provided the various flows are clearly defined. For purposes of this model:
- Po=the annual input of materials drawn from the environment (bio-, hydro- or lithospheres). In a steady state, this input is equal to the annual final disposal of waste.
- P=the annual production of goods from Po.
- C=the annual flow of goods in the anthroposphere.
- R=the annual flow of waste converted to goods through recycling. (In a steady state: C=R+ P)
- p=the effectiveness of production, measured as the ratio of P/Po.
- If r=the effectiveness of recycling, measured as the ratio of R/C, then the relationship is: C/Po=p(1-r).
- If C/Po=C*; then C* is the ratio of goods to the materials drawn out of nature.
In other words, C* is a measure of the meshing of the connection between environment and anthroposphere. It is related to the efficiency of the production and of the recycling sectors. The relationship between C*, p and r, which is a utility function, can be charted as in figure 2, which shows the explicit trade-off between p and r, for a selected value of C*.
Figure 2. A utility function illustrating production recycling trade-offs
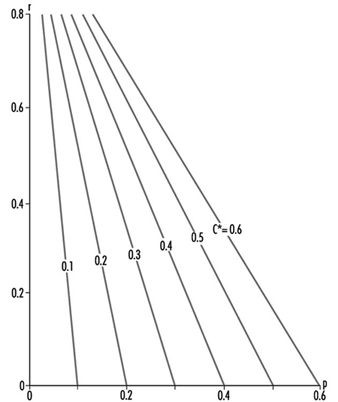
In the past, industry has developed along the line of an increase of the efficiency of production, p. Currently, in the late 1990s, the price of waste disposal through dispersion into the atmosphere, into bodies of water or into soils (uncontrolled tipping), or the burial of waste in confined deposit sites has increased very rapidly, as a result of increasingly stringent environmental protection standards. Under these conditions, it has become economically attractive to increase the effectiveness of recycling (in other words, to increase r). This trend will persist through the coming decades.
One important condition has to be met in order to improve the effectiveness of recycling: the waste to be recycled (in other words the raw materials of the second generation) must be as “pure” as possible (i.e., free of unwanted elements which would preclude the recycling). This will be achieved only through the implementation of a generalized policy of “non-mixing” of domestic, commercial and industrial waste at the source. This is often incorrectly termed sorting at the source. To sort is to separate; but the idea is precisely not to have to separate by storing the various categories of waste in separate containers or places until they are collected. The paradigm of modern waste management is non-mixing of waste at the source so as to enable an increase in the efficiency of recycling and thus to achieve a better ratio of goods per material drawn out of the environment.
Waste Management Practices
Waste may be grouped into three major categories, depending on its production:
- from the primary sector of production (mining, forestry, agriculture, animal breeding, fishery)
- from the production and transformation industry (foods, equipment, products of all types)
- from the consumption sector (households, enterprises, transportation, trade, construction, services, etc.).
Waste can be also classified by legislative decree:
- municipal waste and mixed waste from enterprises which may be aggregated as municipal waste, since both consist of the same categories of waste and are of small size (vegetables, paper, metals, glass, plastics and so on), although in differing proportions.
- bulky urban waste (furniture, equipment, vehicles, construction and demolition waste other than inert material)
- waste subject to special legislation (e.g., hazardous, infectious, radioactive).
Management of municipal and ordinary commercial waste:
Collected by trucks, these wastes can be transported (directly or by road-to-road, road-to-rail or road-to-waterway transfer stations and long-distance transportation means) to a landfill, or to a treatment plant for material recovery (mechanical sorting, composting, biomethanization), or for energy recovery (grid or kiln incinerator, pyrolysis).
Treatment plants produce proportionally small quantities of residues which may be more hazardous for the environment than the original waste. For example, incinerators produce fly ashes with very high heavy metal and complex chemical content. These residues are often classified by legislation as hazardous waste and require appropriate management. Treatment plants differ from landfills because they are “open systems” with inputs and outputs, whereas landfills are essentially “sinks” (if one neglects the small quantity of leachate which deserves further treatment and the production of biogas, which may be an exploited source of energy on very large landfills).
Industrial and domestic equipment:
The present trend, which also has commercial contributions, is for the producers of the waste sectors (e.g., cars, computers, machines) to be responsible for the recycling. Residues are then either hazardous waste or are similar to ordinary waste from enterprises.
Construction and demolition waste:
The increasing prices of landfills is an incentive for a better sorting of such waste. Separation of the hazardous and burnable waste from the large quantity of inert materials allows the latter to be disposed of at a far lower rate than mixed waste.
Special waste:
Chemically hazardous waste must be treated through neutralization, mineralization, insolubilization or be made inert before it can be deposited in special landfills. Infectious waste is best burnt in special incinerators. Radioactive waste is subject to very strict legislation.
Management of Residues
Production and consumption waste which cannot be recycled, down-cycled, reused or incinerated to produce energy must eventually be disposed of. The toxicity for the environment of these residues should be reduced according to the principle of “best available technology at an acceptable price.” After this treatment, the residues should be deposited in sites where they will not contaminate the water and the ecosystem and spread into the atmosphere, into the sea or into lakes and streams.
Deposits of waste are usually dated by the combination of multilayer isolation (using clay, geotextiles, plastic foils and so on), the diversion of all exogenous water, and waterproof cover layers. Permanent deposits need to be monitored for decades. Restrictions on land use of a deposit site must also be controlled for long periods of time. Controlled drainage systems for leachates or gases are necessary in most cases.
More biochemically stable and chemically inert residues from waste treatment require less stringent conditions for their final disposal, making it less difficult to find a deposit site for them within the region of production of the waste. Export of wastes or their residues, which always awakens NIMBY (Not In My Back Yard) reactions, might thus be avoided.
Dan Region Sewage Reclamation Project: A Case Study
Conception and Design
The Dan Region Reclamation Project of municipal wastewater is the biggest project of its kind in the world. It consists of facilities for treatment and groundwater recharge of municipal wastewater from the Dan Region Metropolitan Area - an eight-city conglomerate centred around Tel Aviv, Israel, with a combined population of about 1.5 million inhabitants. The project was created for the purpose of collection, treatment and disposal of municipal wastewater. The reclaimed effluent, after a relatively long detention period in the underground aquifer, is pumped for unrestricted agricultural use, irrigating the arid Negev (the southern part of Israel). A general scheme of the project is given in figure 1. The project was established in the 1960s, and has been growing continuously. At present, the system collects and treats about 110 x 106 m3 per year. Within a few years, at its final stage, the system will handle 150 to 170 x 106 m3 per year.
Figure 1. Dan Region Sewage Reclamation Plant: layout
Sewage treatment plants are known to create a multitude of environmental and occupational health problems. The Dan Region project is a unique system of national importance that combines national benefit together with considerable saving of water resources, high treatment efficiency and production of inexpensive water, without creating excessive occupational hazards.
Throughout the design, installation and routine operation of the system, careful consideration has been given to water sanitation and occupational hygiene concerns. All necessary precautions have been taken to ensure that the reclaimed wastewater will be practically as safe as regular drinking water, in the event that people accidentally drink or swallow it. Similarly, appropriate attention has been given to the issue of reducing to the minimum any potential exposure to accidents or other biological, chemical or physical hazards that may affect either the workers at the wastewater treatment plant proper or other workers engaged in the disposal and agricultural use of the reclaimed water.
At Stage One of the project, the wastewater was biologically treated by a system of facultative oxidation ponds with recirculation and additional chemical treatment by a lime-magnesium process, followed by detention of the high-pH effluent in “polishing ponds”. The partially treated effluent was recharged to the regional groundwater aquifer by means of the Soreq spreading basins.
At Stage Two, the wastewater conveyed to the treatment plant undergoes mechanical-biological treatment by means of an activated-sludge process with nitrification-denitrification. The secondary effluent is recharged to the groundwater by means of the spreading basins Yavneh 1 and Yavneh 2.
The complete system consists of a number of different elements complementing each other:
- a wastewater treatment plant system, comprised of an activated-sludge plant (the biomechanical plant), which treats most of the wastes, and of a system of oxidation and polishing ponds used mostly for treatment of excess sewage flows
- a groundwater recharge system for the treated effluent, which consists of spreading basins, at two different sites (Yavneh and Soreq), that are intermittently flooded; the absorbed effluent passes through the soil’s unsaturated zone and through a portion of the aquifer, and creates a special zone that is dedicated to complementary effluent treatment and seasonal storage, which is called SAT (soil-aquifer-treatment)
- networks of observation wells (53 wells all together) which surround the recharge basins and allow the monitoring of the efficiency of the treatment process
- networks of recovery wells (a total of 74 active wells in 1993) which surround the recharge sites
- a special and separate reclaimed water conveyance main for unrestricted irrigation of agricultural areas in the Negev; this main is called “The Third Negev Line”, and it complements the water supply system to the Negev, which includes another two major fresh water supply main lines
- a setup for chlorination of the effluent, which consists, at present, of three chlorination sites (two more to be added in the future)
- six operational reservoirs along the conveyance system, which regulate the amounts of water pumped and consumed along the system
- an effluent distribution system, composed of 13 major pressure zones, along the effluent main, that supply the treated water to the consumers
- a comprehensive monitoring system which supervises and controls the complete operation of the project.
Description of the Reclamation System
The general scheme of the reclamation system is presented in figure 1 and the flow diagram in figure 2. The system consists of the following segments: wastewater treatment plant, water recharge fields, recovery wells, conveyance and distribution system, chlorination setup and a comprehensive monitoring system.
Figure 2. Flow diagram of Dan Region Project

The wastewater treatment plant
The wastewater treatment plant of the Dan Region Metropolitan Area receives the domestic wastes of the eight cities in the region, and also handles part of their industrial wastes. The plant is located within the Rishon-Lezion sand dunes and is based mostly on secondary treatment of the wastes by the activated-sludge method. Some of the wastes, mostly during peak-flow discharges, are treated in another, older system of oxidation ponds occupying an area of 300 acres. The two systems together can handle, at present, about 110 x 106 m3 per year.
The recharge fields
The treatment plant effluents are pumped into three different sites located within the regional sand dunes, where they are spread on the sand and percolate downward into the underground aquifer for temporary storage and for additional time-dependent treatment. Two of the spreading basins are used for recharge of the mechanical-biological treatment-plant effluent. These are Yavneh 1 (60 acres, located 7 km to the south of the plant) and Yavneh 2 (45 acres, 10 km south of the plant); the third basin is used for recharge of a mixture of the oxidation ponds effluent and a certain fraction from the biomechanical treatment plant that is required in order to improve the quality of the effluent to the necessary level. This is the Soreq site, which has an area of about 60 acres and is located to the east of the ponds.
The recovery wells
Around the recharge sites there are networks of observation wells through which the recharged water is re-pumped. Not all of the 74 wells in operation in 1993 were active during the whole project. In 1993 a total of about 95 million cubic metres of water were recovered from the system’s wells and pumped into the Third Negev Line.
The conveyance and distribution systems
The water pumped from the various recovery wells is collected into the conveyance and distribution system of the Third Line. The conveyance system is composed of three sections, having a combined length of 87 km and a diameter ranging from 48 to 70 inches. Along the conveyance system six different operational reservoirs, “floating” on the main line, were constructed, in order to regulate the water flow of the system. The operational volume of these reservoirs ranges from 10,000 m3 to 100,000 m3.
The water flowing in the Third Line system was supplied to the customers in 1993 through a system of 13 major pressure zones. Numerous water consumers, mostly farms, are connected to these pressure zones.
The chlorination system
The purpose of the chlorination that is carried out in the Third Line is “breakage of the human connection”, which means elimination of any possibility for existence of micro-organisms of human origin in Third Line water. Throughout the course of monitoring it was found that there is a considerable increase of fecal micro-organisms during the stay of the reclaimed water in the water reservoirs. Therefore it was decided to add more chlorination points along the line, and by 1993 three separate chlorination points were routinely operating. Two more chlorination points are to be added to the system in the near future. The residual chlorine ranges between 0.4 and 1.0 mg/l of free chlorine. This method, whereby low concentrations of free chlorine are maintained at various points along the system rather than a single massive dose at the beginning of the line, secures the breakage of the human connection, and at the same time enables fish to live in the reservoirs. In addition, this chlorination method will disinfect the water in the downstream sections of the conveyance and distribution system, in the event that pollutants entered the system at a point downstream from the initial chlorination point.
The monitoring system
Operation of the reclamation system of the Third Negev Line is dependent upon routine functioning of a monitoring setup which is supervised and controlled by a professional and independent scientific entity. This body is the Research and Development Institute of the Technion - Israel Institute of Technology, in Haifa, Israel.
The establishment of an independent monitoring system has been a mandatory requirement of the Israeli Ministry of Health, the local legal authority according to the Israeli Public Health Ordinance. The need for establishing this monitoring setup stems from the facts that:
- This wastewater reclamation project is the biggest one in the world.
- It comprises some non-routine elements that have not as yet been experimented with.
- The reclaimed water is to be used for unlimited irrigation of agricultural crops.
The major role of the monitoring system is therefore to secure the chemical and sanitary quality of the water supplied by the system and to issue warnings regarding any change in the water quality. In addition, the monitoring setup is conducting a follow-up of the complete Dan Region reclamation project, also investigating certain aspects, such as the routine operation of the plant and the chemico-biological quality of its water. This is necessary in order to determine the adaptability of the Third Line water for unlimited irrigation, not only from the sanitary aspect but also from the agricultural viewpoint.
The preliminary monitoring layout was designed and prepared by the Mekoroth Water Co., the major Israeli water supplier and the operator of the Dan Region project. A specially appointed steering committee has been reviewing the monitoring programme on a periodic basis, and has been modifying it according to the accumulated experience gained through the routine operation. The monitoring programme dealt with the various sampling points along the Third Line system, the various investigated parameters and the sampling frequency. The preliminary programme referred to various segments of the system, namely the recovery wells, conveyance line, reservoirs, a limited number of consumer connections, as well as the presence of potable water wells in the vicinity of the plant. The list of parameters included within the monitoring schedule of the Third Line is given in table 1.
Table 1. List of investigated parameters
|
Ag |
Silver |
μg/l |
|
Al |
Aluminium |
μg/l |
|
ALG |
Algae |
No./100 ml |
|
ALKM |
Alkalinity as CaCO3 |
mg/l |
|
As |
Arsenic |
μg/l |
|
B |
Boron |
mg/l |
|
Ba |
Barium |
μg/l |
|
BOD |
Biochemical oxygen demand |
mg/l |
|
Br |
Bromide |
mg/l |
|
Ca |
Calcium |
mg/l |
|
Cd |
Cadmium |
μg/l |
|
Cl |
Chloride |
mg/l |
|
CLDE |
Chlorine demand |
mg/l |
|
CLRL |
Chlorophile |
μg/l |
|
CN |
Cyanides |
μg/l |
|
Co |
Cobalt |
μg/l |
|
COLR |
Colour (platinum cobalt) |
|
|
COD |
Chemical oxygen demand |
mg/l |
|
Cr |
Chromium |
μg/l |
|
Cu |
Copper |
μg/l |
|
DO |
Dissolved oxygen as O2 |
mg/l |
|
DOC |
Dissolved organic carbon |
mg/l |
|
DS10 |
Dissolved solids at 105 ºC |
mg/l |
|
DS55 |
Dissolved solids at 550 ºC |
mg/l |
|
EC |
Electrical conductivity |
μmhos/cm |
|
ENTR |
Enterococcus |
No./100 ml |
|
F– |
Fluoride |
mg/l |
|
FCOL |
Faecal coliforms |
No./100 ml |
|
Fe |
Iron |
μg/l |
|
HARD |
Hardness as CaCO3 |
mg/l |
|
HCO3 – |
Bicarbonate as HCO3 – |
mg/l |
|
Hg |
Mercury |
μg/l |
|
K |
Potassium |
mg/l |
|
Li |
Lithium |
μg/l |
|
MBAS |
Detergents |
μg/l |
|
Mg |
Magnesium |
mg/l |
|
Mn |
Manganese |
μg/l |
|
Mo |
Molybdenum |
μg/l |
|
Na |
Sodium |
mg/l |
|
NH4 + |
Ammonia as NH4 + |
mg/l |
|
Ni |
Nickel |
μg/l |
|
NKJT |
Kjeldahl nitrogen total |
mg/l |
|
NO2 |
Nitrite as NO2 – |
mg/l |
|
NO3 |
Nitrate as NO3 – |
mg/l |
|
ODOR |
Odour-threshold odour number |
|
|
OG |
Oil and grease |
μg/l |
|
Pb |
Lead |
μg/l |
|
PHEN |
Phenols |
μg/l |
|
PHFD |
pH measured at field |
|
|
PO4 |
Phosphate as PO4 –2 |
mg/l |
|
PTOT |
Total phosphorus as P |
mg/l |
|
RSCL |
Residual free chlorine |
mg/l |
|
SAR |
Sodium adsorption ratio |
|
|
Se |
Selenium |
μg/l |
|
Si |
Silica as H2SiO3 |
mg/l |
|
Sn |
Tin |
μg/l |
|
SO4 |
Sulphate |
mg/l |
|
Sr |
Strontium |
μg/l |
|
SS10 |
Suspended solids at 100 ºC |
mg/l |
|
SS55 |
Suspended solids at 550 ºC |
mg/l |
|
STRP |
Streptococcus |
No./100 ml |
|
T |
Temperature |
ºC |
|
TCOL |
Total coliforms |
No./100 ml |
|
TOTB |
Total bacteria |
No./100 ml |
|
TS10 |
Total solids at 105 ºC |
mg/l |
|
TS55 |
Total solids at 550 ºC |
mg/l |
|
TURB |
Turbidity |
NTU |
|
UV |
UV (absorb. at 254 nm)(/cm x 10) |
|
|
Zn |
Zinc |
μg/l |
Recovery wells monitoring
The sampling programme of the recovery wells is based upon a bi-monthly or tri-monthly measurement of a few “indicator-parameters” (table 2). When the chlorides concentration at the sampled well exceeds by more than 15% the initial chlorides level of the well, it is interpreted as a “significant” increase of the share of the recovered effluent within the underground aquifer water, and the well is transferred into the next category of sampling. Here, 23 “characteristic-parameters” are determined, once every three months. In some of the wells, once a year, a complete water investigation, including 54 various parameters, is carried out.
Table 2. The various parameters investigated at the recovery wells
|
Group A |
Group B |
Group C |
|
Indicator parameters |
Characteristic Parameters |
Complete-Test Parameters |
|
1. Chlorides |
Group A and: |
Groups A+B and: |
Conveyance system monitoring
The conveyance system, the length of which is 87 km, is monitored at seven central points along the wastewater line. At these points 16 different parameters are sampled once per month. These are: PHFD, DO, T, EC, SS10, SS55, UV, TURB, NO3 +, PTOT, ALKM, DOC, TOTB, TCOL, FCOL and ENTR. Parameters which are not expected to change along the system are measured at two sampling points only - at the beginning and at the end of the conveyance line. These are: Cl, K, Na, Ca, Mg, HARD, B, DS, SO4 –2, NH4 +, NO2 – and MBAS. At those two sampling points, once a year, various heavy metals are sampled (Zn, Sr, Sn, Se, Pb, Ni, Mo, Mn, Li, Hg, Fe, Cu, Cr, Co, Cd, Ba, As, Al, Ag).
Reservoirs monitoring
The monitoring setup of the Third Line reservoirs is based mostly on examination of a limited number of parameters which serve as indicators of biological development in the reservoirs, and for pinpointing the entry of external pollutants. Five reservoirs are sampled, once per month, for: PHFD, T, DO, Total SS, Volatile SS, DOC, CLRL, RSCL, TCOL, FCOL, STRP and ALG. At these five reservoirs Si is also sampled, once per two months. All these parameters are also sampled at another reservoir, Zohar B, at a frequency of six times per year.
Summary
The Dan Region Reclamation Project supplies high-quality reclaimed water for unrestricted irrigation of the Israeli Negev.
Stage One of this project is in partial operation since 1970 and in full operation since 1977. From 1970 to 1993, a total raw sewage amount of 373 million cubic metres (MCM) was conveyed to the facultative oxidation ponds, and a total water amount of 243 MCM was pumped from the aquifer in the period 1974–1993 and supplied to the South of the country. Part of the water was lost, mostly due to evaporation and seepage from the ponds. In 1993 these losses amounted to about 6.9% of the raw sewage conveyed to the Stage One plant (Kanarek 1994).
The mechanical-biological treatment plant, Stage Two of the project, has been in operation since 1987. During the 1987-1993 period of operation a total raw sewage amount of 478 MCM was conveyed to the mechanical-biological treatment plant. In 1993 about 103 MCM of water (95 MCM reclaimed water plus 8 MCM potable water) were conveyed through the system, and used for unlimited irrigation of the Negev.
The recovery-wells water represents the underground aquifer water quality. The aquifer water quality is changing all the time as a result of the percolation of effluent into it. The aquifer water quality approaches that of the effluent for those parameters that are not influenced by the Soil-Aquifer Treatment (SAT) processes, while parameters that are affected by the passage through the soil layers (e.g., turbidity, suspended solids, ammonia, dissolved organic carbon and so on) show considerably lower values. Noteworthy is the chloride content of the aquifer water, which increased within a recent four-year period by 15 to 26%, as evidenced by the changing water quality in the recovery wells. This change indicates the continuous replacement of aquifer water by effluent having a considerably higher chloride content.
The quality of the water in the six reservoirs of the Third Line system is influenced by biological and chemical changes that occur within the open reservoirs. The oxygen content is increased, as a result of photosynthesis of algae and due to dissolution of atmospheric oxygen. Concentrations of various types of bacteria are also increased as a result of random pollution by various water fauna residing near the reservoirs.
The quality of the water supplied to the customers along the system is dependent upon the quality of water from the recovery wells and the reservoirs. Mandatory chlorination of the system’s water constitutes an additional safeguard against erroneous use of the water as potable water. Comparison of the Third Line water data with the requirements of the Israeli Ministry of Health regarding quality of wastewater to be used for unlimited agricultural use shows that most of the time the water quality fully satisfies the requirements.
In conclusion it might be said that the Third Line wastewater recovery and utilization system has been a successful environmental and national Israeli project. It has solved the problem of sanitary disposal of the Dan Region sewage and at the same time it has increased the national water balance by a factor of about 5%. In an arid country such as Israel, where water supply, especially for agricultural use, is quite limited, this is a real contribution.
The costs of the recharge operation and maintenance of the reclaimed water, in 1993, was about 3 US cents per m3 (0.093 NIS/m3).
The system has been operating since the late 1960s under strict surveillance of the Israeli Ministry of Health and of Mekoroth’s occupational safety and hygiene department. There have been no reports of any occupational disease resulting from the operation of this intricate and comprehensive system.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."