The liver acts as a vast chemical factory with diverse vital functions. It plays an essential role in the metabolism of protein, carbohydrate and fat, and is concerned with the absorption and storage of vitamins and with the synthesis of prothrombin and other factors concerned with blood clotting. The liver is responsible for the inactivation of hormones and the detoxification of many drugs and exogenous toxic chemical substances. It also excretes the breakdown products of haemoglobin, which are the principal constituents of the bile. These widely varying functions are performed by parenchymal cells of uniform structure which contain many complex enzyme systems.
Pathophysiology
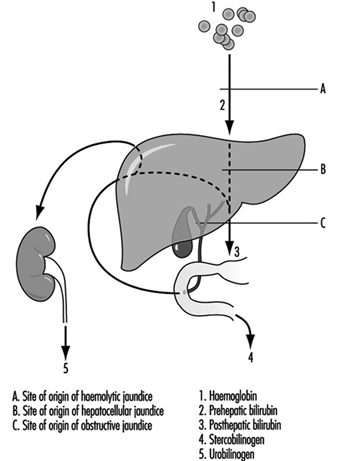
An important feature of liver disease is a rise in the level of bilirubin in the blood; if of sufficient magnitude, this stains the tissues to give rise to jaundice. The mechanism of this process is shown in figure 1. Haemoglobin released from worn out red blood cells is broken down to haem and then, by removal of iron, to bilirubin before it reaches the liver (prehepatic bilirubin). In its passage through the liver cell, bilirubin is conjugated by enzymatic activity into water-soluble glucuronides (posthepatic bilirubin) and then secreted as bile into the intestine. The bulk of this pigment is eventually excreted in the stool, but some is reabsorbed through the intestinal mucosa and secreted a second time by the liver cell into the bile (enterohepatic circulation). However, a small proportion of this reabsorbed pigment is finally excreted in the urine as urobilinogen. With normal liver function there is no bilirubin in the urine, as prehepatic bilirubin is protein bound, but a small amount of urobilinogen is present.
Figure 1. The excretion of bilirubinthrough thte liver, showing the enterohepatic circulation.
Obstruction to the biliary system can occur in the bile ducts, or at cellular level by swelling of the hepatic cells due to injury, with resulting obstruction to the fine bile canaliculi. Posthepatic bilirubin then accumulates in the bloodstream to produce jaundice, and overflows into the urine. The secretion of bile pigment into the intestine is hindered, and urobilinogen is no longer excreted in the urine. The stools are therefore pale due to lack of pigment, the urine dark with bile, and the serum conjugated bilirubin raised above its normal value to give rise to obstructive jaundice.
Damage to the liver cell, which may follow injection of or exposure to toxic agents, also gives rise to an accumulation of posthepatic, conjugated bilirubin (hepatocellular jaundice). This may be sufficiently severe and prolonged to give rise to a transient obstructive picture, with bilirubin but no urobilinogen in the urine. However, in the early stages of hepatocellular damage, without obstruction present, the liver is unable to re-excrete reabsorbed bilirubin, and an excessive amount of urobilinogen is excreted in the urine.
When blood cells are broken down at an excessive rate, as in the haemolytic anaemias, the liver becomes overloaded and the unconjugated prehepatic bilirubin is raised. This again gives rise to jaundice. However, prehepatic bilirubin cannot be excreted in the urine. Excessive amounts of bilirubin are secreted into the intestine, rendering the faeces dark. More is reabsorbed via the enterohepatic circulation and an increased amount of urobilinogen excreted in the urine (haemolytic jaundice).
Diagnosis
Liver function tests are used to confirm suspected liver disease, to estimate progress and to assist in the differential diagnosis of jaundice. A series of tests is usually applied to screen the various functions of the liver, those of established value being:
- Examination of the urine for the presence of bilirubin and urobilinogen: The former is indicative of hepatocellular damage or of biliary obstruction. The presence of excessive urobilinogen can precede the onset of jaundice and forms a simple and sensitive test of minimal hepatocellular damage or of the presence of haemolysis.
- Estimation of total serum bilirubin: Normal value 5-17 mmol/l.
- Estimation of serum enzyme concentration: Hepatocellular damage is accompanied by a raised level of a number of enzymes, in particular of g-glutamyl transpeptidase, alanine amino-transferase (glutamic pyruvic transaminase) and aspartate amino-transferase (glutamic oxalo-acetic transaminase), and by a moderately raised level of alkaline phosphatase. An increasing level of alkaline phosphatase is indicative of an obstructive lesion.
- Determination of plasma protein concentration and electrophoretic pattern: Hepatocellular damage is accompanied by a fall in plasma albumin and a differential rise in the globulin fractions, in particular in g-globulin. These changes form the basis for the flocculation tests of liver function.
- Bromsulphthalein excretion test: This is a sensitive test of early cellular damage, and is of value in detecting its presence in the absence of jaundice.
- Immunological tests: Estimation of the levels of immunoglobulins and detection of autoantibodies is of value in the diagnosis of certain forms of chronic liver disease. The presence of hepatitis B surface antigen is indicative of serum hepatitis and the presence of alpha-fetoprotein suggests a hepatoma.
- Haemoglobin estimation, red cell indices and report on blood film.
Other tests used in the diagnosis of liver disease include scanning by means of ultrasound or radio-isotope uptake, needle biopsy for histological examination and peritoneoscopy. Ultrasound examination provides a simple, safe, non-invasive diagnostic technique but which requires skill in application.
Occupational disorders
Infections. Schistosomiasis is a widespread and serious parasitic infection which may give rise to chronic hepatic disease. The ova produce inflammation in the portal zones of the liver, followed by fibrosis. The infection is occupational where workers have to be in contact with water infested with the free-swimming cercariae.
Hydatid disease of the liver is common in sheep-raising communities with poor hygienic standards where people are in close contact with the dog, the definitive host, and sheep, the intermediate host for the parasite, Echinococcus granulosus. When a person becomes the intermediate host, a hydatid cyst may form in the liver giving rise to pain and swelling, which may be followed by infection or rupture of the cyst.
Weil’s disease may follow contact with water or damp earth contaminated by rats harbouring the causative organism, Leptospira icterohaemorrhagiae. It is an occupational disease of sewer workers, miners, workers in rice-fields, fishmongers and butchers. The development of jaundice some days after the onset of fever forms only one stage of a disease which also involves the kidney.
A number of viruses give rise to hepatitis, the most common being virus type A (HAV) causing acute infective hepatitis and virus type B (HBV) or serum hepatitis. The former, which is responsible for world-wide epidemics, is spread by the faecal-oral route, is characterized by febrile jaundice with liver cell injury and is usually followed by recovery. Type B hepatitis is a disease with a more serious prognosis. The virus is readily transmitted following skin or venipuncture, or transfusion with infected blood products and has been transmitted by drug addicts using the parenteral route, by sexual, especially homosexual contact or by any close personal contact, and also by blood-sucking arthropods. Epidemics have occurred in dialysis and organ transplant units, laboratories and hospital wards. Patients on haemodialysis and those in oncology units are particularly liable to become chronic carriers and hence provide a reservoir of infection. The diagnosis can be confirmed by the identification of an antigen in the serum originally called Australia antigen but now termed hepatitis B surface antigen HBsAg. Serum containing the antigen is highly infectious. Type B hepatitis is an important occupational hazard for health care personnel, especially for those working in clinical laboratories and on dialysis units. High levels of serum positivity have been found in pathologists and surgeons, but low in doctors without patient contact. There is also a hepatitis virus non-A, non-B, identified as hepatitis virus C (HCV). Other hepatitis virus types are likely to be still unidentified. The delta virus cannot cause hepatitis independently but it acts in conjunction with the hepatitis B virus. Chronic virus hepatitis is an important aetiology of liver cirrhosis and cancer (malignant hepatoma).
Yellow fever is an acute febrile illness resulting from infection with a Group B arbovirus transmitted by culicine mosquitoes, in particular Aedes aegypti. It is endemic in many parts of West and Central Africa, in tropical South America and some parts of the West Indies. When jaundice is prominent, the clinical picture resembles infective hepatitis. Falciparum malaria and relapsing fever may also give rise to high fever and jaundice and require careful differentiation.
Toxic conditions. Excessive red blood cell destruction giving rise to haemolytic jaundice may result from exposure to arsine gas, or the ingestion of haemolytic agents such as phenylhydrazine. In industry, arsine may be formed whenever nascent hydrogen is formed in the presence of arsenic, which may be an unsuspected contaminant in many metallurgical processes.
Many exogenous poisons interfere with liver-cell metabolism by inhibiting enzyme systems, or may damage or even destroy the parenchymal cells, interfering with the excretion of conjugated bilirubin and giving rise to jaundice. The injury caused by carbon tetrachloride may be taken as a model for direct hepatotoxicity. In mild cases of poisoning, dyspeptic symptoms may be present without jaundice, but liver damage is indicated by the presence of excess urobilinogen in the urine, raised serum amino-transferase (transaminase) levels and impaired bromsulphthalein excretion. In more severe cases the clinical features resemble those of acute infective hepatitis. Loss of appetite, nausea, vomiting and abdominal pain are followed by a tender, enlarged liver and jaundice, with pale stools and dark urine. An important biochemical feature is the high level of serum amino-transferase (transaminase) found in these cases. Carbon tetrachloride has been widely used in dry cleaning, as a constituent of fire extinguishers and as an industrial solvent.
Many other halogenated hydrocarbons have similar hepatotoxic properties. Those of the aliphatic series which damage the liver are methyl chloride, tetrachloroethane, and chloroform. In the aromatic series the nitrobenzenes, dinitrophenol, trinitrotoluene and rarely toluene, the chlorinated naphthalenes and chlorinated diphenyl may be hepatotoxic. These compounds are used variously as solvents, degreasers and refrigerants, and in polishes, dyes and explosives. While exposure may produce parenchymal cell damage with an illness not dissimilar to infectious hepatitis, in some cases (e.g., following exposure to trinitrotoluene or tetrachlorethane) the symptoms may become severe with high fever, rapidly increasing jaundice, mental confusion and coma with a fatal termination from massive necrosis of the liver.
Yellow phosphorus is a highly poisonous metalloid whose ingestion gives rise to jaundice which may have a fatal termination. Arsenic, antimony and ferrous iron compounds may also give rise to liver damage.
Exposure to vinyl chloride in the polymerization process for the production of polyvinyl chloride has been associated with the development of hepatic fibrosis of a non-cirrhotic type together with splenomegaly and portal hypertension. Angiosarcoma of the liver, a rare and highly malignant tumour developed in a small number of exposed workers. Exposure to vinyl chloride monomer, in the 40-odd years preceding the recognition of angiosarcoma in 1974, had been high, especially in men engaged in the cleaning of the reaction vessels, in whom most of the cases occurred. During that period the TLV for vinyl chloride was 500 ppm, subsequently reduced to 5 ppm (10 mg/m3). While liver damage was first reported in Russian workers in 1949, attention was not paid to the harmful effects of vinyl chloride exposure until the discovery of Raynaud’s syndrome with sclerodermatous changes and acro-osteolysis in the 1960s.
Hepatic fibrosis in vinyl chloride workers can be occult, for as parenchymal liver function can be preserved, conventional liver function tests may show no abnormality. Cases have come to light following haematemesis from the associated portal hypertension, the discovery of thrombocytopoenia associated with splenomegaly or the development of angiosarcoma. In surveys of vinyl chloride workers, a full occupational history including information on alcohol and drug consumption should be taken, and the presence of hepatitis B surface antigen and antibody determined. Hepatosplenomegaly may be detected clinically, by radiography or more precisely by grey scale ultrasonography. The fibrosis in these cases is of a periportal type, with a mainly presinusoidal obstruction to portal flow, attributed to an abnormality of the portal vein radicles or the hepatic sinusoids and giving rise to portal hypertension. The favourable progress of workers who have undergone portocaval shunt operations following haematemesis is likely to be attributed to the sparing of the liver parenchymal cells in this condition.
Fewer than 200 cases of angiosarcoma of the liver which fulfil current diagnostic criteria have been reported. Less than half of these have occurred in vinyl chloride workers, with an average duration of exposure of 18 years, range 4-32 years. In Britain, a register set up in 1974 has collected 34 cases with acceptable diagnostic criteria. Two of these occurred in vinyl chloride workers, with possible exposure in four others, eight were attributable to past exposure to thorotrast and one to arsenical medication. Thorium dioxide, used in the past as a diagnostic aid, is now responsible for new cases of angiosarcoma and hepatoma. Chronic arsenic intoxication, following medication or as an occupational disease among vintners in the Moselle has also been followed by angiosarcoma. Non-cirrhotic perisinusoidal fibrosis has been observed in chronic arsenic intoxication, as in vinyl chloride workers.
Aflatoxin, derived from a group of moulds, in particular Aspergillus flavus, gives rise to liver cell damage, cirrhosis and liver cancer in experimental animals. The frequent contamination of cereal crops, particularly on storage in warm, humid conditions, with A. flavus, may explain the high incidence of hepatoma in certain parts of the world, especially in tropical Africa. In industrialized countries hepatoma is uncommon, more often developing in cirrhotic livers. In a proportion of cases HBsAg antigen has been present in the serum and some cases have followed treatment with androgens. Hepatic adenoma has been observed in women taking certain oral contraceptive formulations.
Alcohol and cirrhosis. Chronic parenchymal liver disease may take the form of chronic hepatitis or of cirrhosis. The latter condition is characterized by cellular damage, fibrosis and nodular regeneration. While in many cases the aetiology is unknown, cirrhosis may follow viral hepatitis, or acute massive necrosis of the liver, which itself may result from drug ingestion or industrial chemical exposure. Portal cirrhosis is frequently associated with excessive alcohol consumption in industrialized countries such as France, Britain and the United States, although multiple risk factors may be involved to explain variation in susceptibility. While its mode of action is unknown, liver damage is primarily dependent on the amount and duration of drinking. Workers who have easy access to alcohol are at greatest risk of developing cirrhosis. Among the occupations with the highest mortality from cirrhosis are bartenders and publicans, restaurateurs, seafarers, company directors and medical practitioners.
Fungi. Mushrooms of the amanita species (e.g., Amanita phalloides) are highly toxic. Ingestion is followed by gastro-intestinal symptoms with watery diarrhoea and after an interval by acute liver failure due to centrizonal necrosis of the parenchyma.
Drugs. A careful drug history should always be taken before attributing liver damage to an industrial exposure, for a variety of drugs are not only hepatotoxic, but are capable of enzyme induction which may alter the liver’s response to other exogenous agents. Barbiturates are potent inducers of liver microsomal enzymes, as are some food additives and DDT.
The popular analgesic acetaminophen (paracetamol) gives rise to hepatic necrosis when taken in overdose. Other drugs with a predictable dose-related direct toxic action on the liver cell are hycanthone, cytotoxic agents and tetracyclines (though much less potent). Several antituberculous drugs, in particular isoniazid and para-aminosalicylic acid, certain monoamine oxidase inhibitors and the anaesthetic gas halothane may also be hepatotoxic in some hypersensitive individuals.
Phenacetin, sulphonamides and quinine are examples of drugs which may give rise to a mild haemolytic jaundice, but again in hypersensitive subjects. Some drugs may give rise to jaundice, not by damaging the liver cell, but by damaging the fine biliary ducts between the cells to give rise to biliary obstruction (cholestatic jaundice). The steroid hormones methyltestosterone and other C-17 alkyl-substituted compounds of testosterone are hepatotoxic in this way. It is important to determine, therefore, whether a female worker is taking an oral contraceptive in the evaluation of a case of jaundice. The epoxy resin hardener 4,4´-diamino-diphenylmethane led to an epidemic of cholestatic jaundice in England following ingestion of contaminated bread.
Several drugs have given rise to what appears to be a hypersensitive type of intrahepatic cholestasis, as it is not dose related. The phenothiazine group, and in particular chlorpromazine are associated with this reaction.
Preventive Measures
Workers who have any disorder of the liver or gall bladder, or a past history of jaundice, should not handle or be exposed to potentially hepatotoxic agents. Similarly, those who are receiving any drug which is potentially injurious to the liver should not be exposed to other hepatic poisons, and those who have received chloroform or trichlorethylene as an anaesthetic should avoid exposure for a subsequent interval. The liver is particularly sensitive to injury during pregnancy, and exposure to potentially hepatotoxic agents should be avoided at this time. Workers who are exposed to potentially hepatotoxic chemicals should avoid alcohol. The general principle to be observed is the avoidance of a second potentially hepatotoxic agent where there has to be exposure to one. A balanced diet with an adequate intake of first class protein and essential food factors affords protection against the high incidence of cirrhosis seen in some tropical countries. Health education should stress the importance of moderation in the consumption of alcohol in protecting the liver from fatty infiltration and cirrhosis. The maintenance of good general hygiene is invaluable in protecting against infections of the liver like hepatitis, hydatid disease and schistosomiasis.
Control measures for type B hepatitis in hospitals include precautions in the handling of blood samples in the ward; adequate labelling and safe transmission to the laboratory; precautions in the laboratory, with the prohibition of mouth pipetting; the wearing of protective clothing and disposable gloves; prohibition of eating, drinking or smoking in areas where infectious patients or blood samples might be handled; extreme care in the servicing of non-disposable dialysis equipment; surveillance of patients and staff for hepatitis and mandatory screening at intervals for the presence of HBsAg antigen. Vaccination against hepatitis A and B viruses is an efficient method to prevent infection in high risk occupations.