Categories of Occupational Safety and Health Professionals Requiring Training and Education
The delivery of occupational safety and health services requires a highly-trained and multidisciplinary team. In a few less-developed countries, such a team may not exist, but in the vast majority of countries in the world, experts in different aspects of OSH are usually at least available though not necessarily in sufficient numbers.
The question of who belong to the categories of OSH professionals is fraught with controversy. Usually there is no dispute that occupational physicians, occupational nurses, occupational hygienists and safety professionals (sometimes referred to as safety practitioners) are OSH professionals. However, there are also members of many other disciplines who can make a plausible claim to belonging to the OSH professions. They include those ergonomists, toxicologists, psychologists and others who specialize in the occupational aspects of their subjects. For the purpose of this article, nevertheless, the training of these latter types of personnel will not be discussed, as the main focus of their training is often not on OSH.
Historical Perspective
In most countries, specific OSH training is of fairly recent origin. Until the Second World War, most OSH professionals received little or no formal training in their chosen calling. Few schools of public health or universities provided formal OSH courses, though some such institutions offered OSH as a subject in the context of a wider degree course, usually in public health. Segments of OSH were taught at the postgraduate level for physicians training in disciplines such as dermatology or respiratory medicine. Some engineering aspects of safety, such as machine guarding, were taught in technological and engineering schools. In most countries, even training in individual components of occupational hygiene courses were hard to find before the Second World War. The development of occupational nursing training is even more recent.
In the developed countries, OSH training received a boost during the Second World War, just as OSH services did. The mass mobilization of whole nations for the war effort led to greater emphasis on protecting the health of workers (and therefore their fighting capability or productivity with respect to the manufacturing of more munitions, warplanes, tanks and warships). At the same time, however, wartime conditions and the drafting of both university teachers and students into the armed forces made it extremely difficult to set up formal courses of OSH training. After the Second World War, however, many such courses were established, some with the help of the generous study grants for demobilized servicemen awarded by grateful governments.
After the Second World War, most colonies of European empires achieved independence and embarked upon the path of industrialization to a greater or lesser extent as a means to national development. Before long, such developing countries found themselves confronting the ills of the industrial revolution of nineteenth-century Europe, but within a much telescoped time span and on an unprecedented scale. Occupational accidents and diseases and environmental pollution became rampant. This led to the development of OSH training, although even today there are large variations in the availability of such training in these countries.
Review of Current International Initiatives
International Labour Organization (ILO)
There have been several initiatives of the ILO in recent years which relate to OSH training. Many of them relate to practical training for interventive measures at the worksite. Some other initiatives are carried out in collaboration with national governments (Rantanen and Lehtinen 1991).
Other ILO activities since the 1970s have been carried on largely in developing countries throughout the world. Several such activities relate to the upgrading of training of factory inspectors in countries such as Indonesia, Kenya, the Philippines, Tanzania, Thailand, and Zimbabwe.
The ILO, together with other United Nations agencies such as the United Nations Development Programme, has also assisted in the establishment or upgrading of national institutes of OSH, the training functions of which are usually among their top priorities.
The ILO has also produced several practical monographs which are very useful as training materials for OSH courses (Kogi, Phoon and Thurman 1989).
World Health Organization (WHO)
The WHO has held in recent years a number of important international and regional conferences and workshops on OSH training. In 1981, a conference entitled “Training of Occupational Health Personnel” was held under the auspices of the Regional Office for Europe of the WHO. In the same year, the WHO convoked with the ILO a Joint ILO/WHO Committee on Occupational Health which focused on “educational and training in occupational health, safety and ergonomics” (WHO 1981). That meeting assessed the needs for education and training at different levels, developed policies in education and training and advised on methodology and programmes for education and training (WHO 1988).
In 1988 a WHO Study Group published a report entitled Training and Education in Occupational Health to address particularly the new policies on primary health care strategies adopted by the WHO member states, new needs resulting from technological developments and new approaches to health promotion at work (WHO 1988).
International Commission on Occupational Health (ICOH)
In 1985, the ICOH established a Scientific Committee on Education and Training in Occupational Health. This Committee has organized four international conferences as well as mini-symposia on the subject in the International Congresses on Occupational Health (ICOH 1987). Among the conclusions of the second conference, the need to develop training strategies and training methodologies received prominent mention in the list of priority issues (ICOH 1989).
A main feature of the third conference was the methodology of OSH training, including such functions as learning by participation, problem-based learning and evaluation of courses, teaching and students (ICOH 1991).
Regional initiatives
In different parts of the world, regional bodies have organized training activities in OSH. For example, the Asian Association of Occupational Health, established in 1954, has a Technical Committee in Occupational Health Education which conducts surveys on training of medical students and related subjects.
Types of Professional Programmes
Degree-granting and similar programmes
Probably the prototype of degree-granting and similar programmes is the sort which was developed in schools of public health or equivalent establishments. Higher education for public health is a relatively recent development. In the United States, the first school dedicated to this purpose was established in 1916 as the Institute of Hygiene at Johns Hopkins University. At that time, the overriding public health concerns centred around the communicable diseases. As time went on, education about the prevention and control of man-made hazards and about occupational health drew increasing emphasis in the training programmes of schools of public health (Sheps 1976).
Schools of public health offer OSH courses for a postgraduate diploma or for the degree of Master of Public Health, allowing students to concentrate in occupational health. Usually entry requirements include the possession of a tertiary educational qualification. Some schools insist upon relevant prior experience in OSH as well. The duration of training on a full-time basis is usually one year for the diploma and two years for the Master’s course.
Some of the schools train the different OSH personnel together in core courses, with training in the specific OSH disciplines (e.g., occupational medicine, hygiene or nursing) being offered to students specializing in these areas. This common training is probably a great advantage, as trainees of the different OSH disciplines could develop a greater understanding of each other’s functions and a better experience of team work.
Especially in recent years, schools of medicine, nursing and engineering have offered courses similar to those in schools of public health.
A few universities are offering OSH courses at the basic or undergraduate level. Unlike the traditional OSH tertiary courses, admission to which is usually dependent upon the acquisition of a previous degree, these newer courses admit students who have just graduated from high school. Much controversy still surrounds the merits of this development. Proponents of such courses argue that they produce more OSH professionals in less time and at lower cost. Their opponents argue that OSH practitioners are more effective if they build their OSH training on a basic discipline into which they integrate their special OSH practice, such as occupational medicine or nursing. Knowledge of basic sciences may be acquired at the specialization level if they have not been taught as part of undergraduate training.
Training courses in OSH for physicians vary in their clinical component. The conference, mentioned above, on the training of occupational health personnel organized by the WHO/Regional Office for Europe emphasized that “occupational medicine is fundamentally a clinical skill and its practitioners must be fully competent in clinical medicine”. It must also be stressed that the diagnosis of chemical intoxication among workers is largely clinical, as is the differentiation between “occupational disease” and other diseases and their management (Phoon 1986). It has become, therefore, a worldwide trend to insist upon postings to different clinics as part of the training of the occupational physician. In the United States and Canada, for example, trainees undergo a four-year residency programme which includes a substantial clinical component in such subjects as dermatology and respiratory medicine in addition to the curriculum required for the degree of Master of Public Health or its equivalent.
Formal training for occupational nurses probably varies even more in different parts of the world than that for occupational physicians. These differences hinge on the variations of responsibilities and functions of occupational nurses. Some countries define occupational health nursing as “the application of nursing principles in conserving the health of workers in all occupations. It involves prevention, recognition, and treatment of illness and injury and requires special skills and knowledge in the fields of health education and counselling, environmental health, rehabilitation and human relations” (Kono and Nishida 1991).On the other hand, other countries understand occupational nursing as the role of the nurse in an interdisciplinary occupational health team, who is expected to participate in all the fields of general health management, delivery of health services, environmental control, healthy and safe working procedures and OSH education. A survey in Japan showed, however, that not all the graduates from an occupational nursing staff took part in all these activities. This was probably due to a lack of understanding of the nurse’s role in OSH and to inadequate training in some of the fields (Kono and Nishida 1991).
The discipline of occupational hygiene has been defined by the American Industrial Hygiene Association as the science and art devoted to the recognition, evaluation and control of those environmental factors and stresses, arising in or from the workplace, which may cause sickness, impaired health and well-being, or significant discomfort and inefficiency among workers or among the citizens of the community. Speciality training has also emerged within the general field of occupational hygiene, including that in chemistry, engineering, noise, radiation, air pollution and toxicology.
Curricula for Occupational Safety and Health Personnel
The detailed contents of the curricula for the training of occupational physicians, nurses, hygienists and safety personnel, as recommended by the 1981 Joint ILO/WHO Committee an Occupational Health mentioned above will be represented in the pages to follow. As regards the main subject areas to be taught, the Committee recommends:
- organization of occupational safety and health services, their activities, legislation and regulations
- occupational medicine
- occupational hygiene
- occupational safety
- work physiology and ergonomics, dealing particularly with the adaptation of work to man, but also with the readjustment of the handicapped to work
- occupational psychology, sociology and health education.
According to the profile of the personnel, the educational programmes will go more or less deeply into different subjects to meet the demands of the respective professions, as discussed below for several categories.
It is difficult to comment in detail what should go into the curricula of OSH courses. It is generally agreed that such courses should have a greater input of behavioural sciences than is now the case, but such input should be relevant to the sociocultural milieu of a particular country or region for which a course is designed. Moreover, OSH should not be taught in isolation from the general health services and the community health situation in a given country or region. The fundamentals of management science should be included in OSH curricula to improve the understanding of organizational structures and practices in enterprises as well as to enhance administrative skills of OSH professionals. The art of communication and the ability to conduct an investigation of OSH problems scientifically and to formulate solutions were also recommended for inclusion in all OSH curricula (Phoon 1985b).
Physicians and nurses
All medical students should be taught some occupational health. In some countries, there are separate courses; in others, occupational health is dealt with in such courses as physiology, pharmacology and toxicology, public health, social medicine and internal medicine. Nevertheless, medical students do not, as a rule, acquire sufficient knowledge and skill to allow them to practice occupational health independently, and some postgraduate training in occupational health and safety is necessary. For further specialization in occupational health (e.g., occupational diseases, or even more narrow fields, like occupational neurology or dermatology), postgraduate training programmes should be available. For nurses active in occupational health services, both long-term and short-term courses need to be organized, depending on their range of activities.
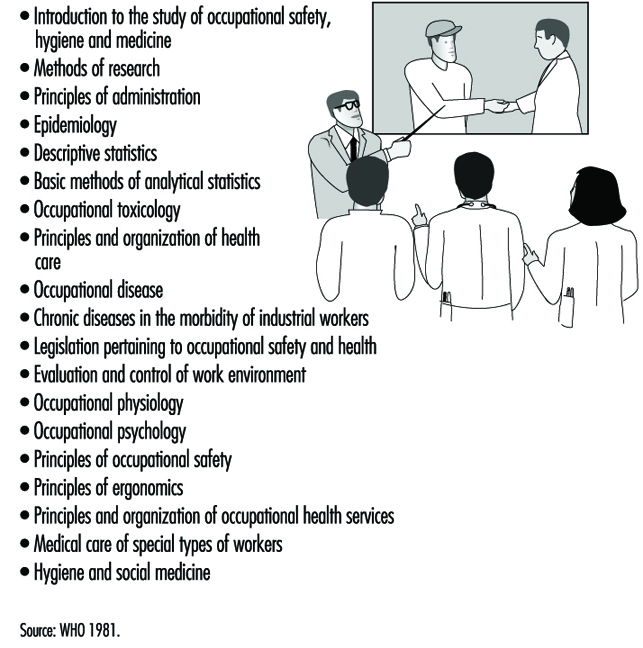
Figure 1 lists subjects to be included in specialized postgraduate training for physicians and nurses.
Figure 1. Postgraduate training syllabus for physicians and nurses.
Safety and health engineers and safety officers
The practice of occupational safety is concerned with such failures of materials, machines, processes and structures as may give rise to dangerous situations, including the release of harmful agents. The aim of education in this field is to enable students to foresee danger, both at the planning stage of projects and in existing situations, to quantify the danger and to design measures to combat it. Training in occupational safety involves the student in a substantial study of selected topics from engineering and materials science, particularly those related to mechanical, civil, chemical, electrical and structural engineering.
Separate curricular units would be concerned, for example, with the structure and strength of materials, in mechanical engineering; with forces in structures, in civil engineering; with handling and transportation of chemicals, in chemical engineering; with design standards, protective equipment and the theory of preventive maintenance, in electrical engineering; and with the behaviour of strata, in mining engineering.
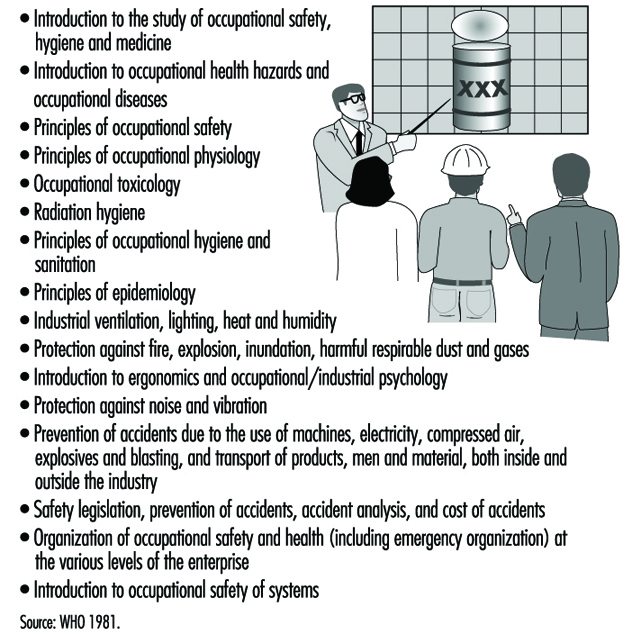
Safety engineers, in addition to acquiring a basic knowledge, should also undergo a course of specialization. The 1981 Joint ILO/WHO Committee recommendations for a specialized safety engineering course of study are listed in figure 2.
Figure 2. A syllabus for specialization in safety engineering.
Courses can be either full-time, part-time or “sandwich courses”—in the lattermost case, periods of studying are interspersed with periods of practice. The selection of which courses to take is very much a matter of individual circumstances or preference. This is especially true since many safety practitioners have extensive knowledge gained through on-the-job experience in particular industries. However, within a large community or a country, there should preferably be a large range of choices to cater for all these different needs.
The recent enormous advances in communications technology should enable the greater usage of distance-learning courses which can be delivered both to remote areas of a country or even across national frontiers. Unfortunately, such technology is still quite expensive, and countries or areas which need such distance-learning capabilities most may be the very ones least able to afford them.
Primary health care practitioners
There is a severe shortage of OSH professionals in developing countries. In addition, among primary health care practitioners and health professionals as a whole, there is a tendency to direct their main activities to curative services. This should be counterbalanced with the help of appropriate training to emphasize the great value of instituting preventive measures at the workplace in collaboration with other responsible parties such as workers and managers. This would help, to a certain extent, to alleviate the problems caused by the present shortage of OSH personnel in developing countries (Pupo-Nogueira and Radford 1989).
A number of developing countries have recently embarked on short courses of OSH training for primary health care and public health personnel. There is a wide spectrum of organizations which have undertaken such training. They include national productivity boards (Phoon 1985a), farmers’ associations, national safety councils, national institutes of health, and professional bodies such as medical and nurses’ associations (Cordes and Rea 1989).
A scarcity of OSH professionals affects not only developing countries, but many developed ones as well. In the United States, one response to this problem took the form of a joint report by a preventive medicine and internal medicine study group that recommended that training programmes in internal medicine emphasize controls of hazards in the workplace and in the environment, since most patients seen by internists are members of the workforce. Furthermore, the American Academy of Family Physicians and the American Medical Association have published several monographs on occupational health for the family physician. A study by the American Institute of Medicine reaffirmed the role of the primary care physician in occupational health, outlined the basic skills required and emphasized the need to enhance occupational health activity in basic training and continuing education (Ellington and Lowis 1991). In both developed and developing countries, however, there is still an inadequate number of OSH training programmes for primary health care personnel and an insufficient number of trained personnel.
Multidisciplinary training
Training in the multidisciplinary nature of OSH can be enhanced by making sure that everyone who trains is fully familiar with the roles, activities and areas of concern of the other OSH personnel. In an OSH course in Scotland, for example, members of the different OSH professions participate in the teaching programme. The students are also provided with self-instruction packages designed to give them detailed knowledge of and insight into the different OSH professional areas. Extensive use is also made of experiential learning techniques such as role-playing simulations and participative case studies. For example, students are asked to complete personal checklists on how each particular area of occupational health activity is likely to affect them in their own work situations, and on how they can cooperate effectively with other occupational health professionals.
In the running of a multidisciplinary OSH course, a key element is the mix of learners of different professional backgrounds in the same class. The course material, such as group exercises and essays, must be carefully selected without any bias to a particular discipline. Lecturers must also receive training in the setting of multidisciplinary questions and problems (D’Auria, Hawkins and Kenny 1991).
Continuing Education
In professional education as a whole, there is an increasing awareness of the need for continuing education. In the field of OSH, new knowledge concerning old hazards and new problems arising from changes in technology are developing so rapidly that no OSH practitioner could hope to keep up to date without making a systematic and constant effort to do so.
Continuing education in OSH can be formal or informal, voluntary or obligatory in order to maintain certification. It is essential for every OSH practitioner to keep up with reading the key professional journals, at least in his or her own disciplines. When a new hazard is encountered, it would be very useful to mount a literature search on that subject through a library. If such a library is unavailable, the CIS service of the ILO could be asked to undertake that service instead. Moreover, having continual and direct access to at least a few up-to-date texts on OSH is essential to any kind of OSH practice.
More formal kinds of continuing education could take the form of conferences, workshops, lectures, journal clubs or seminars. Usually tertiary institutions of learning or professional organizations can provide the means of delivery of such programmes. Whenever possible, there should be annual events in which a broader range of views or expertise could be canvassed than is usually available within the framework of a small community or town. Regional or international conferences or seminars can provide extremely useful opportunities for participants, not only to take advantage of the formal programme but also to exchange information with other practitioners or researchers outside the formal sessions.
Nowadays, more and more OSH professional organizations require members to attend a minimum number of continuing education activities as a condition for extension of certification or membership. Usually only the fact of attendance at approved functions is required. Attendance by itself is, of course, no guarantee that the participant has benefited from being present. Alternatives such as subjecting OSH professionals to regular examinations are also fraught with problems. Within a single OSH discipline, there is such a wide diversity of practice even within the same country that it is extremely difficult to devise an examination equitable to all the OSH practitioners concerned.
Self-learning
In every OSH training course there should be emphasis on the need for self-learning and its continuing practice. To this end, training in information retrieval and critical analysis of published literature is imperative. Training on the use of computers to facilitate obtaining of information from the many excellent OSH resources around the world would be also beneficial. Several courses have been developed in recent years to promote self-learning and information management through microcomputers (Koh, Aw and Lun 1992).
Curriculum Development
There is an increasing demand on the part of trainees and the community to ensure that curricula are constantly evaluated and improved. Many modern curricula are competency-based. A series of professional competencies required is first compiled. Since competence may be defined by different groups in different ways, extensive consultations on this matter should be held with faculty members and OSH practitioners (Pochyly 1973). In addition, there is a need for consultations with “consumers” (e.g., students, workers and employers), an inbuilt evaluation programme and well-defined but flexible educational objectives (Phoon 1988). Sometimes the establishment of advisory committees on curriculum or teaching programmes, which normally include faculty and student representatives, but sometimes also involve members of the general community, can provide a useful forum for such consultations.
Infrastructure Development
Infrastructure is often ignored in discussions on OSH training and education. Yet supporting facilities and human resources such as computers, libraries, efficient administrative staff and procedures and safe and convenient access are among the host of infrastructure considerations which could be crucial to the success of training courses. Proper monitoring of students’ progress, counselling and assistance of students with problems, health care of students and their families (where indicated), minding of students’ children, canteen and recreational facilities and provision of lockers or cupboards for the storage of personal possessions of trainees are all important details which should receive careful attention.
Faculty Recruitment and Development
The quality and popularity of a training programme are often vital factors in determining the quality of staff applying for a vacant position. Obviously, other factors such as satisfactory service conditions and opportunities for career and intellectual development are also important.
Careful consideration should be given to job specifications and job requirements. Faculty should have the necessary OSH qualifications, though flexibility should be exercised to allow the recruitment of staff from non-OSH disciplines who may be able to make special contributions to teaching or especially promising applicants who may have the capability but not all the qualifications or experience normally required for the job. Whenever possible, faculty should have practical OSH experience.
After recruitment, it is the responsibility of the leadership and senior members of the school or department to make sure that new staff are given as much encouragement and opportunity to develop as possible. New staff should be inducted into the culture of the organization but also encouraged to express themselves and to participate in decision-making processes related to teaching and research programmes. Feedback should be given to them concerning their teaching performance in a sensitive and constructive manner. Whenever necessary, offers of help to remedy identified limitations should be given. Many departments have found the regular holding of teaching or evaluation workshops for staff to be extremely useful. Cross-postings to industries and sabbatical leave are other important measures for staff development. Some extent of consultancy work, which could be either clinical, worksite or laboratory (depending on the discipline and areas of activity of the faculty member) helps to make academic teaching more practical.
Teaching Venues
Classrooms should be designed and furnished according to appropriate ergonomic principles and equipped with audio-visual aid equipment and video projection facilities. The lighting and acoustics should be satisfactory. Access to an exit should be located in such a way as to minimize the disturbance of an ongoing class.
Proper principles of OSH should be applied to the design and construction of laboratories. Such safety equipment as showers, eye washing facilities, first aid supplies and resuscitation equipment and fume cupboards should be installed or made available where indicated, and laboratories should be bright, airy and odourless.
Venues for field visits should be chosen to provide a wide range of OSH experiences for the trainees. If possible, worksites with different levels of OSH standards should be chosen. However, on no account should the safety or health of trainees be compromised.
Locations for clinical work would very much depend on the nature and level of the training course. In some circumstances, bedside teaching may be indicated to demonstrate the appropriate clinical approach to skills in history taking. In some other circumstances, presentation of cases with or without patients could serve the same purpose.
Examinations and Assessment
The recent trend has been to seek alternatives to administering an all-important and single final examination at the end of a course. Some courses have abolished formal examinations altogether and replaced them with assignments or periodic assessments. Some other courses have a combination of such assignments and assessments, open book examinations and closed book examinations as well. It is nowadays increasingly understood that examinations or assessments are as much measures of the quality of courses and teachers as of the trainees.
A feedback of trainees’ opinions concerning the entire course or components thereof through questionnaires or discussions is invaluable in the evaluation or revision of a course. As far as possible, all courses should be constantly evaluated, at least on an annual basis, and revised if necessary.
Insofar as modes of examination are concerned, essay questions can test organization, integrating ability and writing skills. The precision and validity of essay examinations, however, have been found to be weak. Multiple-choice questions (MCQs) are less subjective, but good ones are difficult to formulate and do not allow a display of practical knowledge. Modified essay questions (MEQs) differ from essays or MCQs in that the candidate is presented with a progressive amount of information about a problem. It avoids cueing by requesting short-answer responses rather than presenting candidates with alternatives from which to choose the appropriate answer. Oral examinations can measure problem-solving skills, professional judgement, communication skills and ability to retain composure under stress. The main difficulty with the oral examination is the potential for so-called “lack of objectivity”. The oral examination can be made more reliable by imposing some structure on it (Verma, Sass-Kortsak and Gaylor 1991). Perhaps the best alternative is to use a battery of these different types of examination rather than to rely on one or two of them only.
Certification and Accreditation
The word certification usually refers to the conferment upon a professional of authorization to practise. Such certification could be conferred by a national board or a college or an institution of practitioners of an OSH discipline. Usually, the OSH professional is given certification only after fulfilling a stipulated period of training in connection with an approved course or positions and also upon passing an examination. In general, such “global certification” is valid for life, unless there is proven professional negligence or misconduct. However, there are other forms of accreditation which require periodic renewal. They include such accreditation as that required in some countries to either conduct special statutory medical examinations or to report on radiographs of asbestos-exposed persons.
Accreditation, on the other hand, refers to the recognition of OSH courses by a national board or professional organization or a scholarship-granting body. Such accreditation should be subject to periodic reappraisal to ensure that courses keep to an appropriate level of currency and effectiveness.