In some industries, air contaminated with potentially harmful dusts, fumes, mists, vapours or gases may cause harm to the workers. The control of exposure to these materials is important to decrease the risk of occupational diseases caused by breathing the contaminated air. The best method to control exposure is to minimize workplace contamination. This can be accomplished by using engineering control measures (e.g., by enclosure or confinement of the operation, by general and local ventilation and substitution of less toxic materials). When effective engineering controls are not feasible, or while they are being implemented or evaluated, respirators can be used to protect the health of the worker. For respirators to work as anticipated, an appropriate and well-planned respirator programme is necessary.
Respiratory Hazards
Hazards to the respiratory system can be in the form of air contaminants or due to a lack of sufficient oxygen. The particulates, gases or vapours that constitute air contaminants may be associated with different activities (see table 1).
Table 1. Material hazards associated with particular activities
|
Type of hazard |
Typical sources or activities |
Examples |
|
Dusts |
Sewing, grinding, sanding, chipping, sand blasting |
Wood dust, coal, silica dust |
|
Fumes |
Welding, brazing, smelting |
Lead, zinc, iron oxide fumes |
|
Mists |
Spray painting, metal plating, machining |
Paint mists, oil mists |
|
Fibers |
Insulation, friction products |
Asbestos, fiber glass |
|
Gases |
Welding, combustion engines, water treatment |
Ozone, carbon dioxide, carbon monoxide, chlorine |
|
Vapours |
Degreasing, painting, cleaning products |
Methylene chloride, toluene, mineral spirits |
Oxygen is a normal component of the environment that is necessary to sustain life. Physiologically speaking, oxygen deficiency is a reduction in the availability of oxygen to the body’s tissues. It may be caused by the reduction in the percentage of oxygen in the air or by the reduction in the partial pressure of oxygen. (The partial pressure of a gas equals the fractional concentration of the gas in question times the total atmospheric pressure.) The most common form of oxygen deficiency in working environments occurs when the percentage of oxygen is reduced because it is displaced by another gas in a confined space.
Types of Respirators
Respirators are categorized by the type of cover offered for the respiratory system (inlet covering) and by the mechanism used to protect the wearer from the contaminant or from oxygen deficiency. The mechanism is either air purification or supplied air.
Inlet coverings
The “inlets” to the respiratory system are the nose and the mouth. For a respirator to work, these must be sealed by a cover that will in some way isolate the person’s respiratory system from hazards in the respirable environment while simultaneously permitting the intake of sufficient oxygen. The types of coverings that are used may be either tight or loose.
Tight-fitting coverings may take the form of a quarter mask, a half mask, a full facepiece, or a mouth bit. A quarter mask covers both the nose and the mouth. The sealing surface extends from the bridge of the nose to below the lips (a quarter of the face). A half facepiece forms a seal from the bridge of the nose to underneath the chin (half the face). The seal of a full facepiece extends from above the eyes (but below the hair line) to underneath the chin (covering the full face).
With a respirator employing a mouth bit, the mechanism for covering the respiratory system inlets is slightly different. The person bites onto a rubber bit that is attached to the respirator and uses a nose clip to seal the nose. Thus both of the respiratory system inlets are sealed. Mouth bit type respirators are a special type that are used only in situations that call for escape from a hazardous atmosphere. They will not be discussed further in this chapter, since their use is so specialized.
The quarter, half or full-face types of coverings can be used with either an air-purifying or supplied-air type of respirator. The mouth bit type exists only as an air-purifying type.
Loose-fitting inlet coverings, as suggested by their name, do not rely on a sealing surface to protect the worker’s respiratory system. Rather they cover the face, head, or head and shoulders, providing a safe environment. Also included in this group are suits that cover the entire body. (Suits do not include garments that are worn solely to protect the skin, such as splash suits.) Since they do not seal to the face, loose-fitting inlet coverings operate only in systems that provide a flow of air. The flow of air must be greater than the air required for breathing to prevent the contaminant outside the respirator from leaking to the inside.
Air-purifying respirators
An air-purifying respirator causes ambient air to be passed through an air-purifying element that removes the contaminants. Air is passed through the air-purifying element by means of the breathing action (negative pressure respirators) or by a blower (powered air-purifying respirators, or PAPRs).
The type of air-purifying element will determine which contaminants are removed. Filters of varying efficiencies are used to remove aerosols. The choice of filter will depend on the properties of the aerosol; normally, particle size is the most important characteristic. Chemical cartridges are filled with a material that is specifically chosen to absorb or react with the vapour or gaseous contaminant.
Supplied-air respirators
Atmosphere-supplying respirators are a class of respirators that supply a respirable atmosphere independent of the workplace atmosphere. One type is commonly called an air-line respirator and operates in one of three modes: demand, continuous flow or pressure demand. Respirators operating in demand and pressure-demand modes can be equipped with either a half-face or a full facepiece inlet covering. The continuous-flow type can also be equipped with a helmet/hood or a loose-fitting facepiece.
A second type of atmosphere-supplying respirator, called a self-contained breathing apparatus (SCBA), is equipped with a self-contained air supply. It may be used for escape only or for entry into and escape from a hazardous atmosphere. The air is supplied from a compressed-air cylinder or by a chemical reaction.
Some supplied-air respirators are equipped with a small supplemental air bottle. The air bottle provides the person using the respirator with the ability to escape if the main air supply fails.
Combination units
Some specialized respirators may be made to operate both in a supplied-air mode and in an air-purifying mode. They are called combination units.
Respiratory Protection Programmes
For a respirator to function as intended, a minimal respirator programme needs to be developed. Regardless of the type of respirator used, the number of people involved and the complexity of the respirator use, there are basic considerations that need to be included in every programme. For simple programmes, adequate requirements may be minimal. For larger programmes, one may have to prepare for a complex undertaking.
By way of illustration, consider the need of keeping records of fit testing of equipment. For a one- or two-person programme, the date of last fit test, the respirator fit tested and the procedure could be kept on a simple card, while for a large programme with hundreds of users, a computerized database with a system to track those persons who are due for fit testing may be required.
The requirements for a successful programme are described in the following six sections.
1. Programme administration
The responsibility for the respirator programme should be assigned to a single person, called the programme administrator. A single person is assigned this task so that management clearly understands who is responsible. Just as important, this person is given the status necessary to make decisions and run the programme.
The programme administrator should have sufficient knowledge of respiratory protection to supervise the respirator programme in a safe and effective manner. The programme administrator’s responsibilities include the monitoring of respiratory hazards, maintaining records and conducting programme evaluations.
2. Written operating procedures
Written procedures are used to document the programme so that each participant knows what needs to be done, who is responsible for the activity and how it is to be carried out. The procedure document should include a statement of the goals of the programme. This statement would make it clear that the management of the company is responsible for the health of the workers and the implementation of the respirator programme. A written document setting forth the essential procedures of a respirator programme should cover the following functions:
- respirator selection
- maintenance, inspection and repair
- training of employees, supervisors and the person issuing the respirators
- fit testing
- administrative activities including purchasing, inventory control and record keeping
- monitoring of hazards
- monitoring of respirator use
- medical evaluation
- the provision of emergency-use respirators
- programme evaluation.
3. Training
Training is an important part of a respirator programme. The supervisor of the people using respirators, the users themselves and the people who issue respirators to the users all need to be trained. The supervisor needs to know enough about the respirator being used and why it is being used so that he or she will be able to monitor for proper usage: in effect, the person issuing the respirator to the user needs enough training to be sure that the correct respirator is handed out.
The workers who use respirators need to be given training and periodic retraining. The training should include explanations and discussions of the following:
- the nature of the respiratory hazard and possible health effects if the respirator is not used properly
- the reason a particular type of respirator was selected
- how the respirator works and its limitations
- how to put the respirator on and check that it is working and adjusted properly
- how to maintain, inspect and store the respirator
- a respirator fit test for negative pressure respirators.
4. Respirator maintenance
Respirator maintenance includes regular cleaning, inspection for damage, and replacement of worn parts. The manufacturer of the respirator is the best source of information on how to perform cleaning, inspection, repair and maintenance.
Respirators need to be cleaned and sanitized periodically. If a respirator is to be used by more than a single person, it should be cleaned and sanitized before being worn by others. Respirators intended for emergency use should be cleaned and sanitized after each use. This procedure should not be neglected, since there may be special needs to keep the respirator functioning properly. This may include controlled temperatures for cleaning solutions to prevent damage to the device’s elastomers. Furthermore, some parts may need to be cleaned carefully or in a special manner to avoid damage. The manufacturer of the respirator will provide a suggested procedure.
After cleaning and sanitizing, each respirator needs to be inspected to determine if it is in proper working condition, if it needs replacement of parts or repairs, or if it should be discarded. The user should be sufficiently trained and familiar with the respirator in order to be able to inspect the respirator immediately prior to each use in order to ensure that it is in proper working condition.
Respirators that are stored for emergency use need to be periodically inspected. A frequency of once each month is suggested. Once an emergency use respirator is used, it needs to be cleaned and inspected prior to re-use or storage.
In general, inspection will include a check for tightness of connections; for the condition of the respiratory inlet covering, head harness, valves, connecting tubes, harness assemblies, hoses, filters, cartridges, canisters, end of service life indicator, electrical components and shelf life date; and for the proper function of regulators, alarms and other warning systems.
Particular care needs to be given in the inspection of the elastomers and plastic parts commonly found on this equipment. Rubber or other elastomeric parts can be inspected for pliability and signs of deterioration by stretching and bending the material, looking for signs of cracking or wear. Inhalation and exhalation valves are generally thin and easily damaged. One should also look for the build-up of soaps or other cleaning materials on the sealing surfaces of valve seats. Damage or build-up can cause undue leakage through the valve. Plastic parts need to be inspected for damage, such as having stripped or broken threads on a cartridge, for example.
Air and oxygen cylinders should be inspected to determine that they are fully charged according to the manufacturer’s instructions. Some cylinders require periodic inspection to make sure the metal itself is not damaged or rusting. This might include periodic hydrostatic testing of the integrity of the cylinder.
Parts that are found to be defective need to be replaced by stock supplied by the manufacturer itself. Some parts may look very similar to another manufacturer’s, but may perform differently in the respirator itself. Anyone making repairs should to be trained in proper respirator maintenance and assembly.
For supplied-air and self-contained equipment, a higher level of training is required. Reducing or admission valves, regulators and alarms should be adjusted or repaired only by the respirator manufacturer or by a technician trained by the manufacturer.
Respirators that do not meet applicable inspection criteria should be immediately removed from service and repaired or replaced.
Respirators need to be properly stored. Damage can occur if they are not protected from physical and chemical agents such as vibration, sunlight, heat, extreme cold, excessive moisture or damaging chemicals. The elastomers used in the facepiece can be easily damaged if not protected. Respirators should not be stored in such places as lockers and tool boxes unless they are protected from contamination and damage.
5. Medical evaluations
Respirators may affect the health of the person using the equipment because of added stress on the pulmonary system. It is recommended that a physician evaluate each respirator user to determine that he or she can wear a respirator without difficulty. It is up to the physician to determine what will constitute a medical evaluation. A physician may or may not require a physical examination as part of the health assessment.
To perform this task the physician must be given information on the type of respirator being used and the type and length of work the worker will be performing while using the respirator. For most respirators, a normal healthy individual will not be affected by respirator wear, especially in the case of the lightweight air-purifying types.
Someone expected to use an SCBA under emergency conditions will need a more careful evaluation. The weight of the SCBA by itself adds considerably to the amount of work that must be performed.
6. Approved respirators
Many governments have systems to test and approve the performance of respirators for use in their jurisdictions. In such cases, an approved respirator should be used since the fact of its approval indicates that the respirator has met some minimum requirement for performance. If no formal approval is required by the government, any validly approved respirator is likely to provide better assurance that it will perform as intended when compared to a respirator that has gone through no special approval testing whatsoever.
Problems Affecting Respirator Programmes
There are several areas of respirator use that may lead to difficulties in managing a respirator programme. These are the wearing of facial hair and the compatibility of glasses and other protective equipment with the respirator being worn.
Facial hair
Facial hair can present a problem in managing a respirator programme. Some workers like to wear beards for cosmetic reasons. Others experience difficulty shaving, suffering from a medical condition where the facial hairs curl and grow into the skin after shaving. When a person inhales, negative pressure is built up inside the respirator, and if the seal to the face is not tight, contaminants can leak inside. This applies to both air-purifying and supplied-air respirators. The issue is how to be fair, to allow people to wear facial hair, yet to be protective of their health.
There are several research studies that demonstrate that facial hair in the sealing surface of a tight-fitting respirator leads to excessive leakage. Studies have also shown that in connection with facial hair the amount of leakage varies so widely that it is not possible to test whether workers may receive adequate protection even if their respirators were measured for fit. This means that a worker with facial hair wearing a tight-fitting respirator may not be sufficiently protected.
The first step in the solution of this problem is to determine if a loose-fitting respirator can be used. For each type of tight-fitting respirator—except for self contained breathing apparatus and combination escape/air-line respirators—a loose-fitting device is available that will provide comparable protection.
Another alternative is to find another job for the worker which does not require the use of a respirator. The final action that can be taken is to require the worker to shave. For most people who have difficulty shaving, a medical solution can be found that would allow them to shave and wear a respirator.
Eyeglasses and other protective equipment
Some workers need to wear eyeglasses in order to see adequately and in some industrial environments, safety glasses or goggles have to be worn to protect the eyes from flying objects. With a half-mask respirator, eyeglasses or goggles can interfere with the fit of the respirator at the point where it is seated on the bridge of the nose. With a full facepiece, the temple bars of a pair of eyeglasses would create an opening in the sealing surface of the respirator, causing leakage.
Solutions to these difficulties run as follows. For half-mask respirators, a fit test is first carried out, during which the worker should wear any glasses, goggles or other protective equipment that may interfere the respirator’s function. The fit test is used to demonstrate that eyeglasses or other equipment will not interfere with the function of the respirator.
For full-facepiece respirators, the options are to use contact lenses or special eyeglasses that mount inside the facepiece—most manufacturers supply a special spectacles kit for this purpose. At times, it has been thought that contact lenses should not be used with respirators, but research has shown that workers can use contact lenses with respirators without any difficulty.
Suggested Procedure for Respirator Selection
Selecting a respirator involves analysing how the respirator will be used and understanding the limitations of each specific type. General considerations include what the worker will be doing, how the respirator will be used, where the work is located and any limitations a respirator may have on work, as shown schematically in figure 1.
Figure 1. Guide to Respirator Selection
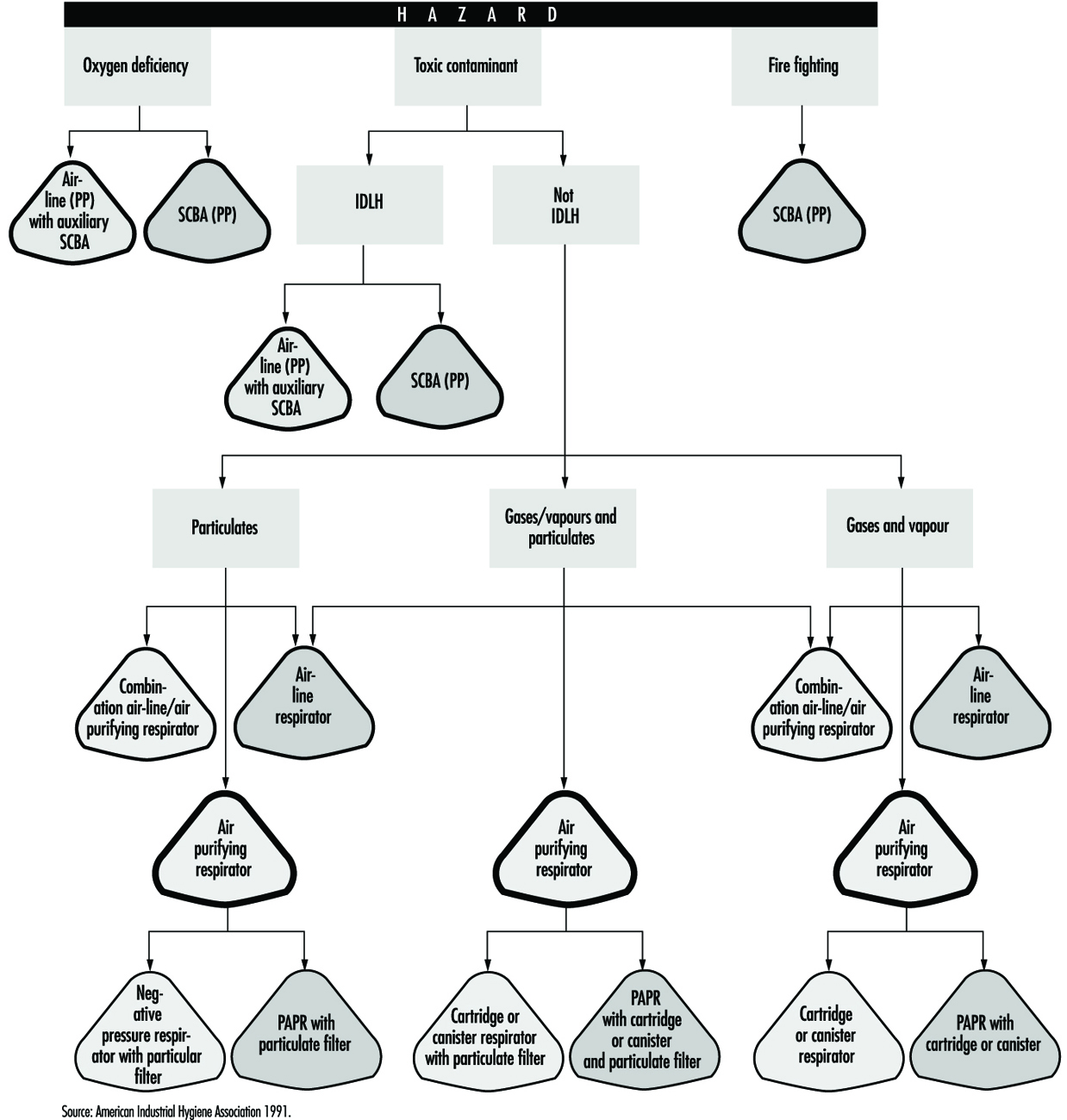
Worker activity and worker location in a hazardous area need to be considered in selecting the proper respirator (for example, whether the worker is in the hazardous area continuously or intermittently during the work shift and whether the work rate is light, medium or heavy). For continuous use and heavy work a lightweight respirator would be preferred.
Environmental conditions and level of effort required of the respirator wearer may affect respirator service life. For example, extreme physical exertion can cause the user to deplete the air supply in a SCBA such that its service life is reduced by half or more.
The period of time that a respirator must be worn is an important factor that has to be taken into account in selecting a respirator. Consideration should be given to the type of task—routine, nonroutine, emergency, or rescue work—that the respirator will be called upon to perform.
The location of the hazardous area with respect to a safe area having respirable air must be considered in selecting a respirator. Such knowledge will permit planning for the escape of workers if an emergency occurs, for the entry of workers to perform maintenance duties and for rescue operations. If there is a long distance to breathable air or if the worker needs to be able to walk around obstacles or climb steps or ladders, then a supplied-air respirator would not be a good choice.
If the potential for an oxygen-deficient environment exists, measure the oxygen content of the relevant work space. The class of respirator, air-purifying or supplied-air, that can be used will depend on the partial pressure of oxygen. Because air-purifying respirators only purify the air, sufficient oxygen must be present in the surrounding atmosphere to support life in the first place.
Respirator selection involves reviewing each operation to ascertain what dangers may be present (hazard determination) and to select the type or class of respirators that can offer adequate protection.
Hazard Determination Steps
In order to determine the properties of the contaminants that may be present in the workplace, one should consult the key source for this information, namely, the supplier of the material. Many suppliers provide their customers with a material safety data sheet (MSDS) which reports the identity of the materials in a product and supplies information on exposure limits and toxicity as well.
One should determine whether there is a published exposure limit such as a threshold limit value (TLV), permissible exposure limit (PEL), maximum acceptable concentration, (MAK), or any other available exposure limit or estimate of toxicity for the contaminants. It ought to be ascertained whether a value for the immediately dangerous to life or health (IDLH) concentration for the contaminant is available. Each respirator has some use limitation based on the level of exposure. A limit of some sort is needed to determine whether the respirator will provide sufficient protection.
Steps should be taken to discover if there is a legally mandated health standard for the given contaminant (as there is for lead or asbestos). If so, there may be specific respirators required that will help narrow the selection process.
The physical state of the contaminant is an important characteristic. If an aerosol, its particle size should be determined or estimated. The vapour pressure of an aerosol is also significant at the maximum expected temperature of the work environment.
One should determine whether the contaminant present can be absorbed through the skin, produce skin sensitization or be irritating or corrosive to the eyes or skin. It should also be found for a gaseous or vapour contaminant if a known odour, taste or irritation concentration exists.
Once the identity of the contaminant is known, its concentration needs to be determined. This is normally done by collecting the material on a sample medium with subsequent analysis by a laboratory. Sometimes the assessment can be accomplished by estimating exposures, as described below.
Estimating Exposure
Sampling is not always required in hazard determination. Exposures can be estimated by examining data relating to similar tasks or by calculation by means of a model. Models or judgment can be used to estimate the likely maximum exposure and this estimate can be used to select a respirator. (The most basic models suitable to such a purpose is the evaporation model, a given amount of material is either assumed or allowed to evaporate into an air space, its vapour concentration found, and an exposure estimated. Adjustments can be made for dilution effects or ventilation.)
Other possible sources of exposure information are articles in journals or trade publications which present exposure data for various industries. Trade associations and data collected in hygiene programmes for similar processes are also useful for this purpose.
Taking protective action based on estimated exposure involves making a judgement based on experience vis-à-vis the type of exposure. For example, air monitoring data of previous tasks will not be useful in the event of the first occurrence of a sudden break in a delivery line. The possibility of such accidental releases must be anticipated in the first place before the need of a respirator can be decided, and the specific type of respirator chosen can then be made on the basis of the estimated likely concentration and nature of the contaminant. For example, for a process involving toluene at room temperatures, a safety device that offers no more protection than a continuous-flow air line need be chosen, since the concentration of toluene would not be expected to exceed its IDLH level of 2,000 ppm. However, in the case of a break in a sulphur dioxide line, a more effective device—say, an air-supplied respirator with an escape bottle—would be called for, since a leak of this sort could quite readily result in an ambient concentration of contaminant above the IDLH level of 20 ppm. In the next section, respirator selection will be examined in further detail.
Specific Respirator Selection Steps
If one is unable to determine what potentially hazardous contaminant may be present, the atmosphere is considered immediately dangerous to life or health. An SCBA or air line with an escape bottle is then required. Similarly, if no exposure limit or guideline is available and estimates of the toxicity cannot be made, the atmosphere is considered IDLH and an SCBA is required. (See the discussion below on the subject of IDLH atmospheres.)
Some countries have very specific standards governing respirators that can be used in given situations for specific chemicals. If a specific standard exists for a contaminant, the legal requirements must be followed.
For an oxygen-deficient atmosphere, the type of respirator selected depends on the partial pressure and concentration of oxygen and the concentration of the other contaminants that may be present.
Hazard ratio and assigned protection factor
The measured or estimated concentration of a contaminant is divided by its exposure limit or guideline to obtain its hazard ratio. With respect to this contaminant, a respirator is selected that has an assigned protection factor (APF) greater than the value of the hazard ratio (the assigned protection factor is the estimated performance level of a respirator). In many countries, a half mask is assigned an APF of ten. It is assumed that the concentration inside the respirator will be reduced by a factor of ten, that is, the APF of the respirator.
The assigned protection factor can be found in any existent regulations on respirator use or in the American National Standard for Respiratory Protection (ANSI Z88.2 1992). ANSI APFs are listed in table 2.
Table 2. Assigned protection factors from ANSI Z88 2 (1992)
|
Type of respirator |
Respiratory inlet covering |
|||
|
Half mask1 |
Full facepiece |
Helmet/hood |
Loose-fitting facepiece |
|
|
Air-Purifying |
10 |
100 |
||
|
Atmosphere-supplying |
||||
|
SCBA (demand-type)2 |
10 |
100 |
||
|
Airline(demand-type) |
10 |
100 |
||
|
Powered air-purifying |
50 |
10003 |
10003 |
25 |
|
Atmosphere-supplying air-line type |
||||
|
Pressure-fed demand type |
50 |
1000 |
— |
— |
|
Continuous Flow |
50 |
1000 |
1000 |
25 |
|
Self-contained breathing apparatus |
||||
|
Positive pressure (demand open/closed circuit) |
— |
4 |
— |
— |
1 Includes one-quarter mask, disposable half masks and half masks with elastomeric facepieces.
2 Demand SCBA shall not be used for emergency situations such as fire fighting.
3 Protection factors listed are for high efficiency filters and sorbents (cartridges and canisters). With dust filters an assigned protection factor of 100 is to be used due to the limitations of the filter.
4 Although positive pressure respirators are currently regarded as providing the highest level of respiratory protection, a limited number of recent simulated workplace studies concluded that all users may not achieve protection factors of 10,000. Based on this limited data, a definitive assigned protection factor could not be listed for positive pressure SCBAs. For emergency planning purposes where hazardous concentrations can be estimated, an assigned protection factor of no higher than 10,000 should be used.
Note: Assigned protection factors are not applicable for escape respirators. For combination respirators, e.g., air-line respirators equipped with an air-purifying filter, the mode of operation in use will dictate the assigned protection factor to be applied.
Source: ANSI Z88.2 1992.
For example, for a styrene exposure (exposure limit of 50 ppm) with all of the measured data at the worksite less than 150 ppm, the hazard ratio is 3 (that is, 150 ¸ 50 = 3). Selection of a half-mask respirator with an assigned protection factor of 10 will assure that most unmeasured data will be well below the assigned limit.
In some cases where “worst-case” sampling is done or only a few data are collected, judgement must be used to decide if enough data have been collected for an acceptably reliable assessment of exposure levels. For example, if two samples were collected for a short-term task that represents the “worst-case” for that task and both samples were less than two times the exposure limit (a hazard ratio of 2), a half-mask respirator (with an APF of 10) would likely be an appropriate choice and certainly a continuous-flow full facepiece respirator (with an APF of 1,000) would be sufficiently protective. The contaminant’s concentration must also be less than the maximum-use concentration of the cartridge/canister: this latter information is available from the manufacturer of the respirator.
Aerosols, gases and vapours
If the contaminant is an aerosol, a filter will have to be used; the choice of filter will depend on the efficiency of the filter for the particle. The literature provided by the manufacturer will provide guidance on the appropriate filter to use. For example, if the contaminant is a paint, lacquer or enamel, a filter designed specifically for paint mists may be used. Other special filters are designed for fumes or dust particles that are larger than usual.
For gases and vapours, adequate notice of cartridge failure is necessary. Odour, taste or irritation are used as indicators that the contaminant has “broken through” the cartridge. Therefore, the concentration at which the odour, taste or irritation is noted must be less than the exposure limit. If the contaminant is a gas or vapour that has poor warning properties, the use of an atmosphere-supplying respirator is generally recommended.
However, atmosphere-supplying respirators sometimes cannot be used because of the lack of an air supply or because of the need for worker mobility. In this case, air-purifying devices may be used, but it is necessary that it be equipped with an indicator signalling the end of the device’s service life so that the user will be given adequate warning prior to contaminant breakthrough. Another alternative is to use a cartridge change schedule. The change schedule is based on cartridge service data, expected concentration, pattern of use and duration of exposure.
Respirator selection for emergency or IDLH conditions
As noted above, IDLH conditions are presumed to exist when the concentration of a contaminant is not known. Furthermore, it is prudent to consider any confined space containing less than 20.9% oxygen as an immediate danger to life or health. Confined spaces present unique hazards. Lack of oxygen in confined spaces is the cause of numerous deaths and serious injuries. Any reduction in the percentage of oxygen present is proof, at a minimum, that the confined space is not adequately ventilated.
Respirators for use under IDLH conditions at normal atmospheric pressure include either a positive-pressure SCBA alone or a combination of a supplied-air respirator with an escape bottle. When respirators are worn under IDLH conditions, at least one standby person must be present in a safe area. The standby person needs to have the proper equipment available to assist the wearer of the respirator in case of difficulty. Communications have to be maintained between the standby person and the wearer. While working in the IDLH atmosphere, the wearer needs to be equipped with a safety harness and safety lines to permit his or her removal to a safe area, if necessary.
Oxygen-deficient atmospheres
Strictly speaking, oxygen deficiency is a matter only of its partial pressure in a given atmosphere. Oxygen deficiency can be caused by a reduction in the percentage of oxygen in the atmosphere or by reduced pressure, or both reduced concentration and pressure. At high altitudes, reduced total atmospheric pressure can lead to very low oxygen pressure.
Humans need a partial oxygen pressure of approximately 95 mm Hg (torr) to survive. The exact pressure will vary among people depending on their health and acclimatization to reduced oxygen pressure. This pressure, 95 mm Hg, is equivalent to 12.5% oxygen at sea level or 21% oxygen at an altitude of 4,270 meters. Such an atmosphere may adversely affect either the person with reduced tolerance to reduced oxygen levels or the unacclimatized person performing work requiring a high degree of mental acuity or heavy stress.
To prevent adverse effects, supplied-air respirators should be provided at higher oxygen partial pressures, for example, about 120 mm Hg or 16% oxygen content at sea level. A physician should be involved in any decisions where people will be required to work in reduced-oxygen atmospheres. There may be legally mandated levels of oxygen percent or partial pressure that require supplied-air respirators at different levels than these broadly general guidelines suggest.
Suggested Procedures for Fit Testing
Each person assigned a tight-fitting negative-pressure respirator needs to be fit tested periodically. Each face is different, and a specific respirator may not fit a given person’s face. Poor fit would allow contaminated air to leak into the respirator, lowering the amount of protection the respirator provides. A fit test needs to be repeated periodically and must be carried out whenever a person has a condition that may interfere with facepiece sealing, e.g., significant scarring in the area of the face seal, dental changes, or reconstructive or cosmetic surgery. Fit testing has to be done while the subject is wearing protective equipment such as spectacles, goggles, a face shield or a welding helmet that will be worn during work activities and could interfere with respirator fit. The respirator should be configured as it will be used, that is, with a chin canister or cartridge.
Fit test procedures
Respirator fit testing is conducted to determine if a particular model and size of mask fits an individual’s face. Before the test is made, the subject should be oriented on the respirator’s proper use and donning, and the test’s purpose and procedures should be explained. The person being tested should understand that the he or she is being asked to select the respirator that provides the most comfortable fit. Each respirator represents a different size and shape and, if fit properly and used properly, will provide adequate protection.
No one size or model of respirator will fit all types of faces. Different sizes and models will accommodate a broader range of facial types. Therefore, an appropriate number of sizes and models should be available from which a satisfactory respirator can be selected.
The person being tested should be instructed to hold each facepiece up to the face and eliminate those which obviously do not give a comfortable fit. Normally, selection will begin with a half mask, and if a good fit cannot be found, the person will need to test a full facepiece respirator. (A small percentage of users will not be able to wear any half mask.)
The subject should conduct a negative- or positive-pressure fit check according to the instructions provided by the manufacturer before the test is begun. The subject is now ready for fit testing by one of the methods listed below. Other fit test methods are available, including quantitative fit test methods which use instruments to measure leakage into the respirator. The fit test methods, which are outlined in the boxes here, are qualitative and do not require expensive test equipment. These are (1) the isoamyl acetate (IAA) protocol and (2) the saccharin solution aerosol protocol.
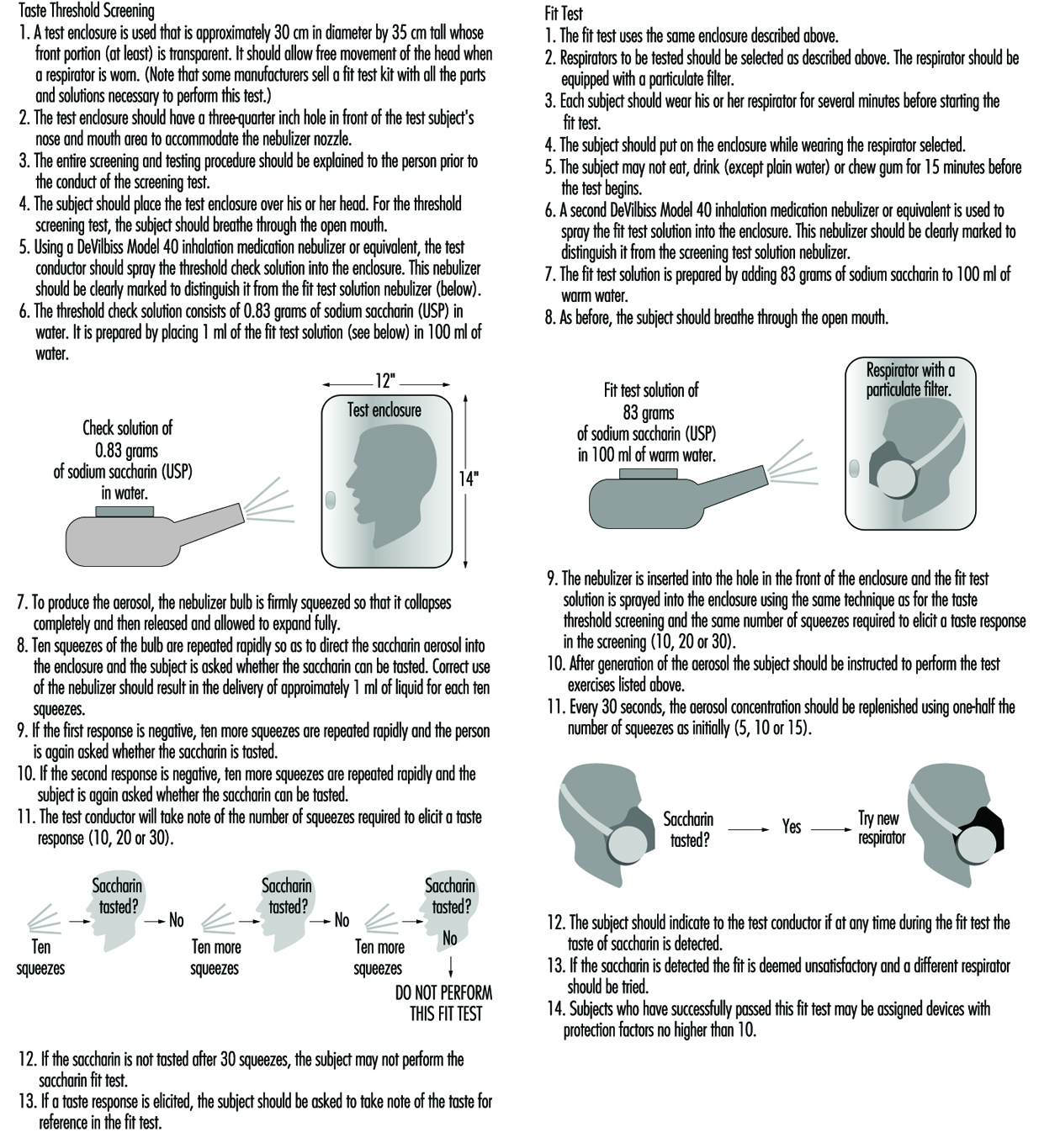
Test exercises. During the fit test, the wearer should carry out a number of exercises in order to verify that the respirator will allow him or her to perform a set of basic and necessary actions. The following six exercises are recommended: standing still, breathing normally, breathing deeply, moving the head from side to side, moving the head up and down, and speaking. (See figure 2 and figure 3).
Figure 2. Isoamly acetate quantitive fit-test method

Figure 3. Sacharin aerosol quantitive fit-test method