Over the last two decades the emphasis in disaster reduction has switched from mainly improvised relief measures in the post-impact phase to forward planning, or disaster preparedness. For natural disasters this approach has been embraced in the philosophy of the United Nations International Decade for Natural Disaster Reduction (IDNDR) programme. The following four phases are the components of a comprehensive hazard management plan which can be applied to all types of natural and technological disasters:
- pre-disaster planning
- emergency preparedness
- emergency response
- post-impact recovery and reconstruction.
The aim of disaster preparedness is to develop disaster prevention or risk reduction measures in parallel with emergency preparedness and response capabilities. In this process hazard and vulnerability analyses are the scientific activities which provide the basis for the applied tasks of risk reduction and emergency preparedness to be undertaken in collaboration with planners and the emergency services.
Most health professionals would see their role in disaster preparedness as one of planning for the emergency treatment of large numbers of casualties. However, if the impact of disasters is to be drastically reduced in the future, the health sector needs to be involved in the development of preventive measures and in all phases of disaster planning, with scientists, engineers, emergency planners and decision makers. This multidisciplinary approach poses a major challenge to the health sector at the end of the 20th century as natural and human-made calamities become increasingly destructive and costly in terms of lives and property with the expansion of human populations across the globe.
Natural sudden or rapid-onset disasters include extreme weather conditions (floods and high winds), earthquakes, landslides, volcanic eruptions, tsunamis and wild fires, and their impacts have much in common. Famines, drought and desertification, on the other hand, are subject to more long-term processes which at present are only very poorly understood, and their consequences are not so amenable to reduction measures. Presently the most common cause of famine is war or so-called complex disasters (e.g., in Sudan, Somalia or former Yugoslavia).
Large numbers of displaced persons are a common feature of natural and complex disasters, and their nutritional and other health needs require specialized management.
Modern civilization is also becoming accustomed to technological or human-made disasters such as acute air pollution episodes, fires and chemical and nuclear reactor accidents, the last two being the most important today. This article will focus on disaster planning for chemical disasters, as nuclear power accidents are dealt with elsewhere in the Encyclopaedia.
Natural Sudden-Onset Disasters
The most important of these in terms of destructiveness are floods, hurricanes, earthquakes and volcanic eruptions. There have already been some well-publicized successes in disaster reduction through early warning systems, hazard mapping and structural engineering measures in seismic zones.
Thus satellite monitoring using global weather forecasting, together with a regional system for timely delivery of warnings and effective evacuation planning, was responsible for the comparatively small loss of life (just 14 deaths) when Hurricane Hugo, the strongest hurricane so far recorded in the Caribbean, struck Jamaica and the Cayman Islands in 1988. In 1991 adequate warnings provided by Philippine scientists closely monitoring Mount Pinatubo saved many thousands of lives through timely evacuation in one of the largest eruptions of the century. But the “technological fix” is only one aspect of disaster mitigation. The large human and economic losses wrought by disasters in developing countries highlight the major importance of socio-economic factors, above all poverty, in increasing vulnerability, and the need for disaster preparedness measures to take these into account.
Natural disaster reduction has to compete in all countries with other priorities. Disaster reduction can also be promoted through legislation, education, building practices and so on, as part of a society’s general risk reduction programme or safety culture—as an integral part of sustainable development policies and as a quality assurance measure for investment strategies (e.g., in the planning of buildings and infrastructure in new land developments).
Technological Disasters
Clearly, with natural hazards it is impossible to prevent the actual geological or meteorological process from occurring.
However, with technological hazards, major inroads into disaster prevention can be made using risk reduction measures in the design of plants and governments can legislate to establish high standards of industrial safety. The Seveso Directive in EC countries is an example which also includes requirements for the development of onsite and offsite planning for emergency response.
Major chemical accidents comprise large vapour or flammable gas explosions, fires, and toxic releases from fixed hazardous installations or during the transport and distribution of chemicals. Special attention has been given to the storage in large quantities of toxic gases, the most common being chlorine (which, if suddenly released due to the disruption of a storage tank or from a leak in a pipe, can form large denser-than-air clouds which can be blown in toxic concentrations for large distances downwind). Computer models of dispersion of dense gases in sudden releases have been produced for chlorine and other common gases and these are used by planners to devise emergency response measures. These models can also be used to determine the numbers of casualties in a reasonably foreseeable accidental release, just as models are being pioneered for predicting the numbers and types of casualties in major earthquakes.
Disaster Prevention
A disaster is any disruption of the human ecology that exceeds the capacity of the community to function normally. It is a state which is not merely a quantitative difference in the functioning of the health or emergency services—for example, as caused by a large influx of casualties. It is a qualitative difference in that the demands cannot be adequately met by a society without help from unaffected areas of the same or another country. The word disaster is too often used loosely to describe major incidents of a highly publicized or political nature, but when a disaster has actually occurred there may be a total breakdown in normal functioning of a locality. The aim of disaster preparedness is to enable a community and its key services to function in such disorganized circumstances in order to reduce human morbidity and mortality as well as economic losses. Large numbers of acute casualties are not a prerequisite for a disaster, as was shown in the chemical disaster at Seveso in 1976 (when a massive evacuation was mounted because of fears of long-term health risks arising from ground contamination by dioxin).
“Near disasters” may be a better description of certain events, and outbreaks of psychological or stress reactions may also be the only manifestation in some events (e.g., at the reactor accident at Three Mile Island, USA, in 1979). Until the terminology becomes established we should recognize Lechat’s description of the health objectives of disaster management, which include:
- prevention or reduction of mortality due to the impact, to a delay in rescue and to lack of appropriate care
- provision of care for casualties such as immediate post-impact trauma, burns and psychological problems
- management of adverse climatic and environmental conditions (exposure, lack of food and drinking water)
- prevention of short-term and long-term disaster-related morbidity (e.g., outbreaks of communicable diseases due to disruption of sanitation, living in temporary shelters, overcrowding and communal feeding; epidemics such as malaria due to interruption of control measures; rise of morbidity and mortality due to disruption of the health care system; mental and emotional problems)
- ensuring restoration of normal health by preventing long-term malnutrition due to disruption of food supplies and agriculture.
Disaster prevention cannot take place in a vacuum, and it is essential that a structure exists at the national governmental level of every country (the actual organization of which will vary from country to country), as well as at the regional and community level. In countries with high natural risks, there may be few ministries which can avoid being involved. The responsibility for planning is given to existing bodies such as armed forces or civil defence services in some countries.
Where a national system exists for natural hazards it would be appropriate to build on to it a response system for technological disasters, rather than devise a whole new separate system. The Industry and Environment Programme Activity Centre of the United Nations Environment Programme has developed the Awareness and Preparedness for Emergencies at Local Level (APELL) Programme. Launched in cooperation with industry and government, the programme aims to prevent technological accidents and reduce their impacts in developing countries by raising community awareness of hazardous installations and providing assistance in developing emergency response plans.
Hazard Assessment
The different types of natural disaster and their impacts need to be assessed in terms of their likelihood in all countries. Some countries such as the UK are at low risk, with wind storms and floods being the main hazards, while in other countries (e.g., the Philippines) there is a wide range of natural phenomena which strike with relentless regularity and can have serious effects on the economy and even the political stability of the country. Each hazard requires a scientific evaluation which will include at least the following aspects:
- its cause or causes
- its geographical distribution, magnitude or severity and probable frequency of occurrence
- the physical mechanisms of destruction
- the elements and activities most vulnerable to destruction
- possible social and economic consequences of a disaster.
Areas at high risk of earthquakes, volcanoes and floods need to have hazard zone maps prepared by experts to predict the locations and nature of the impacts when a major event occurs. Such hazard assessments can then be used by land-use planners for long-term risk reduction, and by emergency planners who have to deal with the pre-disaster response. However, seismic zoning for earthquakes and hazard mapping for volcanoes are still in their infancy in most developing countries, and extending such risk mapping is seen as a crucial need in the IDNDR.
Hazard assessment for natural hazards requires a detailed study of the records of previous disasters in the preceding centuries and exacting geological field work to ascertain major events such as earthquakes and volcanic eruptions in historic or prehistoric times. Learning about the behaviour of major natural phenomena in the past is a good, but far from infallible, guide for hazard assessment for future events. There are standard hydrological methods for flood estimation, and many flood-prone areas can be easily recognized because they coincide with a well-defined natural flood plain. For tropical cyclones, records of impacts around coastlines can be used to determine the probability of a hurricane striking any one part of the coastline in a year, but each hurricane has to be urgently monitored as soon as it has formed in order to actually forecast its path and speed at least 72 hours ahead, before it makes landfall. Associated with earthquakes, volcanoes and heavy rains are landslides which may be triggered by these phenomena. In the last decade it has been increasingly appreciated that many large volcanoes are at risk from slope failure because of the instability of their mass, which has been built up during periods of activity, and devastating landslides may result.
With technological disasters, local communities need to make inventories of the hazardous industrial activities in their midst. There are now ample examples from past major accidents of what these hazards can lead to, should a failure in a process or containment occur. Quite detailed plans now exist for chemical accidents around hazardous installations in many developed countries.
Risk Assessment
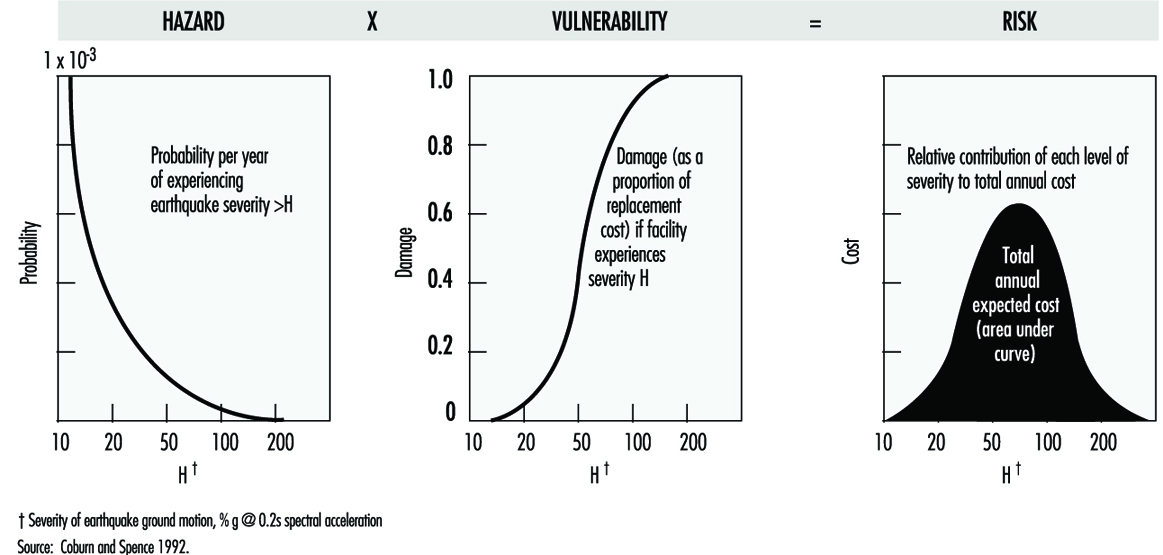
After evaluating a hazard and its likely impacts, the next step is to undertake a risk assessment. Hazard may be defined as the possibility of harm, and risk is the probability of lives being lost, persons injured or property damaged due to a given type and magnitude of natural hazard. Risk can be quantitatively defined as:
Risk = value x vulnerability x hazard
where value can represent a potential number of lives or capital value (of buildings, for example) which may be lost in the event. Ascertaining vulnerability is a key part of risk assessment: for buildings it is the measure of the intrinsic susceptibility of structures exposed to potentially damaging natural phenomena. For example, the likelihood of a building collapsing in an earthquake can be determined from its location relative to a fault line and the seismic resistance of its structure. In the above equation the degree of loss resulting from the occurrence of a natural phenomenon of a given magnitude can be expressed on a scale from 0 (no damage) to 1 (total loss), while hazard is the specific risk expressed as a probability of preventable loss per unit time. Vulnerability is therefore the fraction of value that is likely to be lost as a result of an event. The information needed for making a vulnerability analysis can come, for example, from surveys of homes in hazard areas by architects and engineers. Figure 1 provides some typical risk curves.
Figure 1. Risk is a product of hazard and vulnerability: typical curve shapes
Vulnerability assessments utilizing information on different causes of death and injury according to the different types of impact are much more difficult to undertake at the present time, as the data on which to base them are crude, even for earthquakes, since standardization of injury classifications and even the accurate recording of the number, let alone the causes of deaths, are not yet possible. These serious limitations show the need for much more effort to be put into epidemiological data-gathering in disasters if preventive measures are to develop on a scientific basis.
At present mathematical computation of risk of building collapse in earthquakes and from ash falls in volcanic eruptions can be digitalized onto maps in the form of risk scales, to graphically demonstrate those areas of high risk in a foreseeable event and predict where, therefore, civil defence preparedness measures should be concentrated. Thus risk assessment combined with economic analysis and cost effectiveness will be invaluable in deciding between different options for risk reduction.
In addition to building structures, the other important aspect of vulnerability is infrastructure (lifelines) such as:
- transport
- telecommunications
- water supplies
- sewer systems
- electricity supplies
- health care facilities.
In any natural disaster all of these are at risk of being destroyed or heavily damaged, but as the type of destructive force may differ according to the natural or technological hazard, appropriate protective measures need to be devised in conjunction with the risk assessment. Geographical information systems are modern computer techniques for mapping different data sets to assist in such tasks.
In planning for chemical disasters, quantified risk assessment (QRA) is used as a tool to determine the probability of plant failure and as a guide for decision makers, by providing numerical estimates of risk. Engineering techniques for making this type of analysis are well advanced, as are the means of developing hazard zone maps around hazardous installations. Methods exist for predicting pressure waves and concentrations of radiant heat at different distances from the sites of vapour or flammable gas explosions. Computer models exist for predicting the concentration of denser-than-air gases for kilometres downwind from an accidental release in specified amounts from a vessel or plant under different weather conditions. In these incidents vulnerability mainly has to do with the proximity of housing, schools, hospitals and other key installations. Individual and societal risks need to be computed for the different types of disaster and their significance should be communicated to the local population as part of overall disaster planning.
Risk Reduction
Once vulnerability has been assessed, the feasible measures to reduce vulnerability and overall risk need to be devised.
Thus new buildings should be made seismic resistant if built in a seismic zone, or old buildings can be retrofitted so that they are less likely to collapse. Hospitals may need resiting or “hardening” against hazards such as windstorms, for example. The need for good roads as evacuation routes must never be forgotten in land developments in areas at risk of windstorms or volcanic eruptions and a host of other civil engineering measures can be enacted depending upon the situation. In the longer term the most important measure is the regulation of land use to prevent the development of settlements in hazardous areas, such as flood plains, the slopes of active volcanoes or around major chemical plants. Over-reliance on engineering solutions can bring false reassurance in at-risk areas, or be counterproductive, increasing the risk of rare catastrophic events (e.g., building levees along major rivers prone to severe flooding).
Emergency Preparedness
The planning and organization of emergency preparedness should be a task for a multidisciplinary planning team involved at the community level, and one which should be integrated into hazard assessment, risk reduction and emergency response. In the management of casualties it is now well recognized that medical teams from outside may take at least three days to arrive at the scene in a developing country. As most preventable deaths occur within the first 24 to 48 hours, such assistance will arrive too late. Thus it is at the local level that emergency preparedness should be focused, so that the community itself has the means to begin rescue and relief actions immediately after an event.
Providing adequate information to the public in the planning phase should therefore be a key aspect of emergency preparation.
Information and communication needs
On the basis of the hazard and risk analyses, the means of providing early warning will be essential, together with a system for evacuating people from areas of high risk should an emergency arise. Pre-planning of communications systems between the different emergency services at the local and national levels is necessary and for the effective provision and dissemination of information in a disaster a formal chain of communication will have to be established. Other measures such as stockpiling emergency food and water supplies in households may be included.
A community near a hazardous installation needs to be aware of the warning it may receive in an emergency (e.g., a siren if there is a gas release) and the protective measures people should adopt (e.g., immediately go inside houses and close windows until advised to come out). An essential feature of a chemical disaster is the need to be able to rapidly define the health hazard posed by a toxic release, which means identifying the chemical or chemicals involved, having access to knowledge of their acute or long-term effects and determining who, if anyone, in the general population has been exposed. Establishing lines of communication with poison information and chemical emergency centres is an essential planning measure. Unfortunately it may be difficult or impossible to know the chemicals involved in the event of runaway reactions or chemical fires, and even if it is easy to identify a chemical, knowledge of its toxicology in humans, particularly chronic effects, may be sparse or non-existent, as was found after the release of methyl isocyanate at Bhopal. Yet without information on the hazard, the medical management of casualties and the exposed population, including decisions on the need for evacuation from the contaminated area, will be severely hampered.
A multidisciplinary team to gather information and to undertake rapid health risk assessments and environmental surveys to exclude contamination of ground, water and crops should be pre-planned, recognizing that all available toxicological databases may be inadequate for decision making in a major disaster, or even in small incidents in which a community believes it has suffered serious exposure. The team should have the expertise to confirm the nature of the chemical release and to investigate its likely health and environmental impacts.
In natural disasters, epidemiology is also important for making an assessment of the health needs in the post-impact phase and for infectious diseases surveillance. Information gathering on the effects of the disaster is a scientific exercise which should also be part of a response plan; a designated team should undertake this work to provide important information for the disaster coordinating team as well as for assisting in the modification and improvement of the disaster plan.
Command and control and emergency communications
The designation of the emergency service in charge, and the constitution of a disaster coordinating team, will vary from country to country and with the type of disaster, but it needs to be pre-planned. At the scene a specific vehicle may be designated as the command and control, or onsite coordinating centre. For example, emergency services cannot rely on telephone communications, as these may become overloaded, and so radio links will be needed.
The hospital major incident plan
The capability of hospitals in terms of staff, physical reserves (theatres, beds and so on) and treatment (medicines and equipment) for dealing with any major incident will need to be assessed. Hospitals should have specific plans for dealing with a sudden large influx of casualties, and there should be provision for a hospital flying squad to go to the scene to work with search and rescue teams in extricating trapped victims or to undertake field triage of large numbers of casualties. Major hospitals may be unable to function because of disaster damage, as happened in the earthquake in Mexico City in 1985. Restoring or supporting devastated health services may therefore be necessary. For chemical incidents, hospitals should have established links with poison information centres. As well as being able to draw on a large fund of health care professionals from inside or outside a disaster area to cope with the injured, planning should also include the means for the rapid sending of emergency medical equipment and drugs.
Emergency equipment
The types of search and rescue equipment needed for a specific disaster should be identified at the planning stage along with where it will be stored, as it will need to be rapidly deployed in the first 24 hours, when the most lives can be saved. Key medicines and medical equipment need to be available for rapid deployment, along with personal protective equipment for emergency crews, including health workers at the disaster scene. Engineers skilled in urgently restoring water, electricity, communications and roads can have a major role in alleviating the worst effects of disasters.
Emergency response plan
The separate emergency services and the health care sector, including public health, occupational health and environmental health practitioners, should each have plans for dealing with disasters, which can be incorporated together as one major disaster plan. In addition to the hospital plans, health planning should include detailed response plans for different types of disaster, and these need to be devised in the light of the hazard and risk assessments produced as part of disaster preparedness. Treatment protocols should be drawn up for the specific types of injury that each disaster may produce. Thus a range of traumas, including crush syndrome, should be anticipated from the collapse of buildings in earthquakes, whereas body burns and inhalational injuries are a feature of volcanic eruptions. In chemical disasters, triage, decontamination procedures, the administration of antidotes where applicable and emergency treatment of acute pulmonary injury from irritant toxic gases should all be planned for. Forward planning should be flexible enough to cope with transport emergencies involving toxic substances, especially in areas without fixed installations which would normally require the authorities to make intensive local emergency plans. The emergency management of physical and chemical trauma in disasters is a vital area of health care planning and one which requires training of hospital staff in disaster medicine.
The management of evacuees, the location of evacuation centres and the appropriate preventive health measures should be included. The need for emergency stress management to prevent stress disorders in victims and emergency workers should also be considered. Sometimes psychological disorders may be the predominant or even the only health impact, particularly if the response to an incident has been inadequate and engendered undue anxiety in the community. This is also a special problem of chemical and radiation incidents which can be minimized with adequate emergency planning.
Training and education
Medical staff and other health care professionals at the hospital and primary care level are likely to be unfamiliar with working in disasters. Training exercises involving the health sector and the emergency services are a necessary part of emergency preparedness. Table-top exercises are invaluable and should be made as realistic as possible, since large-scale physical exercises are likely to be held very infrequently because of their high cost.
Post-impact recovery
This phase is the returning of the affected area to its pre-disaster state. Pre-planning should include post-emergency social, economic and psychological care and rehabilitation of the environment. For chemical incidents the latter also includes environmental assessments for contaminants of water and crops, and remedial actions, if needed, such as decontamination of soils and buildings and restoration of potable water supplies.
Conclusion
Relatively little international effort has been put into disaster preparedness compared to relief measures in the past; however, although investment in disaster protection is costly, there is now a large body of scientific and technical knowledge available which if applied correctly would make a substantial difference to the health and economic impacts of disasters in all countries.