A tragic industrial fire in Thailand has focused worldwide attention on the need to adopt and enforce state-of-the-art codes and standards in industrial occupancies.
On May 10, 1993, a major fire at the Kader Industrial (Thailand) Co. Ltd. factory located in the Nakhon Pathom Province of Thailand killed 188 workers (Grant and Klem 1994). This disaster stands as the world’s worst accidental loss-of-life fire in an industrial building in recent history, a distinction held for 82 years by the Triangle Shirtwaist factory fire that killed 146 workers in New York City (Grant 1993). Despite the years between these two disasters, they share striking similarities.
Various domestic and international agencies have focused on this incident following its occurrence. With respect to fire protection concerns, the National Fire Protection Association (NFPA) cooperated with the International Labour Organization (ILO) and with the Bangkok Police Fire Brigade in documenting this fire.
Questions for a Global Economy
In Thailand, the Kader fire has created a great deal of interest about the country’s fire safety measures, particularly its building code design requirements and enforcement policies. Thai Prime Minister Chuan Leekpai, who travelled to the scene on the evening of the fire, has pledged that the government will address fire safety issues. According to the Wall Street Journal (1993), Leekpai has called for tough action against those who violate the safety laws. Thai Industry Minister Sanan Kachornprasart is quoted as saying that “Those factories without fire prevention systems will be ordered to install one, or we will shut them down”.
The Wall Street Journal goes on to state that labour leaders, safety experts and officials say that the Kader fire may help tighten building codes and safety regulations, but they fear that lasting progress is still far off as employers flout rules and governments allow economic growth to take priority over worker safety.
Because the majority of the shares of Kader Industrial (Thailand) Co. Ltd. are owned by foreign interests, the fire has also fuelled international debate about foreign investors’ responsibilities for ensuring the safety of the workers in their sponsoring country. Twenty per cent of the Kader shareholders are from Taiwan, and 79.96% are from Hong Kong. A mere 0.04% of Kader is owned by Thai nationals.
Moving into a global economy implies that products are manufactured at one location and used at other locations throughout the world. Desire for competitiveness in this new market should not lead to compromise in fundamental industrial fire safety provisions. There is a moral obligation to provide workers with an adequate level of fire protection, no matter where they are located.
The Facility
The Kader facility, which manufactured stuffed toys and plastic dolls primarily intended for export to the United States and other developed countries, is located in the Sam Phran District of Nakhon Pathom Province. This is not quite halfway between Bangkok and the nearby city of Kanchanaburi, the site of the infamous Second World War railroad bridge over the River Kwai.
The structures that were destroyed in the blaze were all owned and operated directly by Kader, which owns the site. Kader has two sister companies that also operate at the location on a lease arrangement.
The Kader Industrial (Thailand) Co. Ltd. was first registered on 27 January 1989, but the company’s licence was suspended on 21 November 1989, after a fire on 16 August 1989 destroyed the new plant. This fire was attributed to the ignition of polyester fabric used in the manufacture of dolls in a spinning machine. After the plant was rebuilt, the Ministry of Industry allowed it to reopen on 4 July 1990.
Between the time the factory reopened and the May 1993 fire, the facility experienced several other, smaller fires. One of them, which occurred in February 1993, did considerable damage to Building Three, which was still being repaired at the time of the fire in May 1993. The February fire occurred late at night in a storage area and involved polyester and cotton materials. Several days after this blaze a labour inspector visited the site and issued a warning that pointed out the plant’s need for safety officers, safety equipment and an emergency plan.
Initial reports following the May 1993 fire noted that there were four buildings on the Kader site, three of which were destroyed by the fire. In a sense this is true, but the three buildings were actually a single E-shaped structure (see figure 1), the three primary portions of which were designated Buildings One, Two and Three. Nearby was a one-storey workshop and another four-storey structure referred to as Building Four.
Figure 1. Site plan of the Kader toy factory
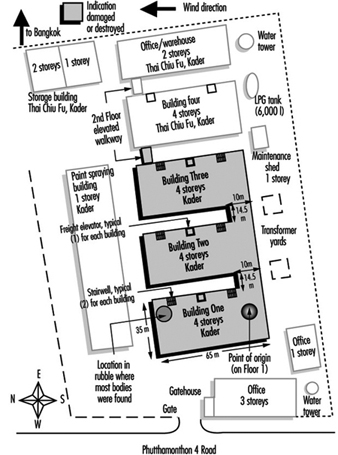
The E-shaped building was a four-storey structure composed of concrete slabs supported by a structural steel frame. There were windows around the perimeter of each floor and the roof was a gently sloped, peaked arrangement. Each portion of the building had a freight elevator and two stairwells that were each 1.5 metres (3.3 feet) wide. The freight elevators were caged assemblies.
Each building at the plant was equipped with a fire alarm system. None of the buildings had automatic sprinklers, but portable extinguishers and hose stations were installed on outside walls and in the stairwells of each building. None of the structural steel in the building was fireproofed.
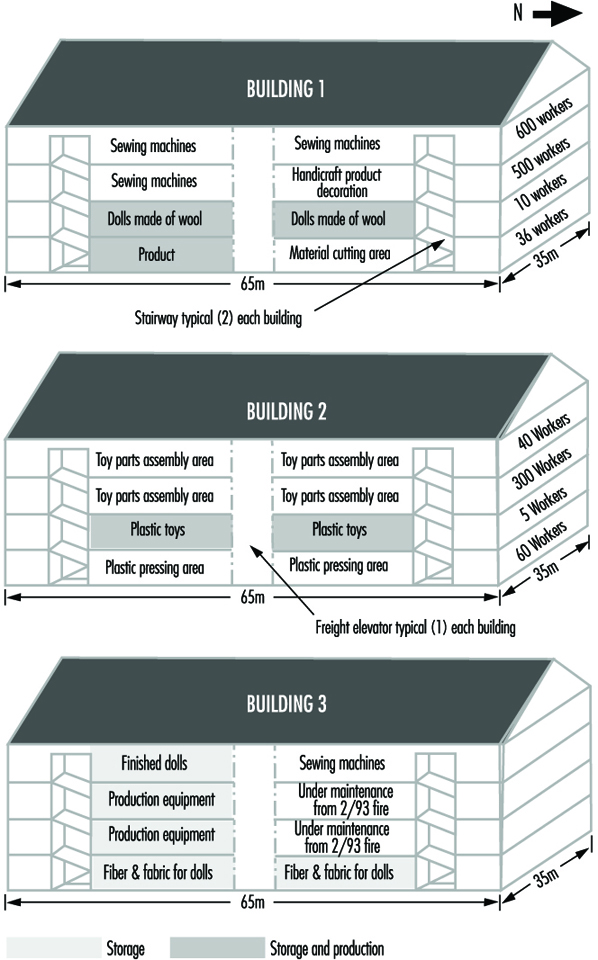
There is conflicting information about the total number of workers at the site. The Federation of Thai Industries had pledged to help 2,500 plant employees displaced by the fire, but it is unclear how many employees were at the site at any one time. When the fire occurred, it was reported that there were 1,146 workers in Building One. Thirty-six were on the first floor, 10 were on the second, 500 were on the third, and 600 were on the fourth. There were 405 workers in Building Two. Sixty of them were on the first floor, 5 were on the second, 300 were on the third and 40 were on the fourth. It is not clear how many workers were in Building Three since a portion of it was still being refurbished. Most of the workers at the plant were women.
The Fire
Monday, May 10, was a normal workday at the Kader facility. At approximately 4:00 p.m., as the end of the day shift approached, someone discovered a small fire on the first floor near the south end of Building One. This portion of the building was used to package and store the finished products, so it contained a considerable fuel load (see figure 2). Each building at the facility had a fuel load composed of fabric, plastics and materials used for stuffing, as well as other normal workplace materials.
Figure 2. Internal layout of buildings one, two and three
Security guards in the vicinity of the fire tried unsuccessfully to extinguish the flames before they called the local police fire brigade at 4:21 p.m. Authorities received two more calls, at 4:30 p.m. and 4:31 p.m. The Kader facility is just beyond the jurisdictional boundaries of Bangkok, but fire apparatus from Bangkok, as well as apparatus from Nakhon Pathom Province, responded.
As the workers and security guards tried in vain to extinguish the fire, the building began filling with smoke and other products of combustion. Survivors reported that the fire alarm never sounded in Building One, but many workers grew concerned when they saw smoke on the upper floors. Despite the smoke, security guards reportedly told some workers to stay at their stations because it was a small fire that would soon be under control.
The fire spread rapidly throughout Building One, and the upper floors soon became untenable. The blaze blocked the stairwell at the south end of the building, so most of the workers rushed to the north stairwell. This meant that approximately 1,100 people were trying to leave the third and fourth floors through a single stairwell.
The first fire apparatus arrived at 4:40 p.m., their response time having been extended because of the relatively remote location of the facility and the gridlock conditions typical of Bangkok traffic. Arriving fire-fighters found Building One heavily involved in flames and already beginning to collapse, with people jumping from the third and fourth floors.
Despite the fire-fighters’ efforts, Building One collapsed completely at approximately 5:14 p.m. Fanned by strong winds blowing toward the north, the blaze spread quickly into Buildings Two and Three before the fire brigade could effectively defend them. Building Two reportedly collapsed at 5:30 p.m., and Building Three at 6:05 p.m. The fire brigade successfully kept the fire from entering Building Four and the smaller, one-storey workshop nearby, and the fire-fighters had the blaze under control by 7:45 p.m. Approximately 50 pieces of fire apparatus were involved in the battle.
The fire alarms in Buildings Two and Three reportedly functioned properly, and all the workers in those two buildings escaped. The workers in Building One were not so fortunate. A large number of them jumped from the upper floors. In all, 469 workers were taken to the hospital, where 20 died. The other dead were found during the post-fire search of what had been the north stairwell of the building. Many of them apparently succumbed to lethal products of combustion before or during the building’s collapse. According to the latest information available, 188 people, most of them female, have died as a result of this fire.
Even with the help of six large hydraulic cranes that were moved to the site to facilitate the search for victims, it was several days before all the bodies could be removed from the rubble. There were no fatalities among the fire-fighters, although there was one injury.
Traffic in the vicinity, which is normally congested, made transporting the victims to hospitals difficult. Nearly 300 injured workers were taken to the nearby Sriwichai II Hospital, although many of them were transferred to alternate medical facilities when the number of victims exceeded the hospital’s capacity to treat them.
The day after the fire, Sriwichai II Hospital reported that it had kept 111 fire victims. The Kasemrat Hospital received 120; Sriwichai Pattanana received 60; Sriwichai I received 50; Ratanathibet I received 36; Siriraj received 22; and Bang Phai received 17. The remaining 53 injured workers were sent to various other medical facilities in the area. In all, 22 hospitals throughout Bangkok and Nakhon Pathom Province participated in treating victims of the disaster.
Sriwichai II Hospital reported that 80% of their 111 victims suffered serious injuries and that 30% required surgery. Half of the patients suffered only from smoke inhalation, while the remainder also suffered burns and fractures that ranged from broken ankles to fractured skulls. At least 10% of the injured Kader workers admitted to Sriwichai II Hospital risk permanent paralysis.
Determining the cause of this fire became a challenge because the portion of the facility in which it began was totally destroyed and the survivors have provided conflicting information. Since the fire started near a large electrical control panel, investigators first thought that problems with the electrical system might have been the cause. They also considered arson. At this time, however, Thai authorities feel that a carelessly discarded cigarette may have been the source of ignition.
Analysing the Fire
For 82 years, the world has recognized the 1911 Triangle Shirtwaist factory fire in New York City as the worst accidental loss-of-life industrial fire in which the fatalities were limited to the building of fire origin. With 188 fatalities, however, the Kader factory fire now replaces the Triangle fire in the record books.
When analysing the Kader fire, a direct comparison with the Triangle fire provides a useful benchmark. The two buildings were similar in a number of ways. The arrangement of the exits was poor, the fixed fire protection systems were insufficient or ineffective, the initial fuel package was readily combustible, and the horizontal and vertical fire separations were inadequate. In addition, neither company had provided its workers with adequate fire safety training. However, there is one distinct difference between these two fires: the Triangle Shirtwaist factory building did not collapse and the Kader buildings did.
Inadequate exit arrangements were perhaps the most significant factor in the high loss of life at both the Kader and the Triangle fires. Had the exiting provisions of NFPA 101, the Life Safety Code, which was established as a direct result of the Triangle fire, been applied at the Kader facility, substantially fewer lives would have been lost (NFPA 101, 1994).
Several fundamental requirements of the Life Safety Code pertain directly to the Kader fire. For example, the Code requires that every building or structure be constructed, arranged and operated in such a way that its occupants are not placed in any undue danger by fire, smoke, fumes or the panic that may occur during an evacuation or during the time it takes to defend the occupants in place.
The Code also requires that every building have enough exits and other safeguards of the proper size and at the proper locations to provide an escape route for every occupant of a building. These exits should be appropriate to the individual building or structure, taking into account the character of the occupancy, the capabilities of the occupants, the number of occupants, the fire protection available, the height and type of building construction and any other factor necessary to provide all the occupants with a reasonable degree of safety. This was obviously not the case in the Kader facility, where the blaze blocked one of Building One’s two stairwells, forcing approximately 1,100 people to flee the third and fourth floors through a single stairwell.
In addition, the exits should be arranged and maintained so that they provide free and unobstructed egress from all parts of a building whenever it is occupied. Each of these exits should be clearly visible, or the route to every exit should be marked in such a way that every occupant of the building who is physically and mentally able readily knows the direction of escape from any point.
Every vertical exit or opening between the floors of a building should be enclosed or protected as necessary to keep the occupants reasonably safe while they exit and to prevent fire, smoke and fumes from spreading from floor to floor before the occupants have had a chance to use the exits.
The outcomes of both the Triangle and the Kader fires were significantly affected by the lack of adequate horizontal and vertical fire separations. The two facilities were arranged and built in such a way that a fire on a lower floor could spread rapidly to the upper floors, thus trapping a large number of workers.
Large, open work spaces are typical of industrial facilities, and fire-rated floors and walls must be installed and maintained to slow the spread of fire from one area to another. Fire also must be kept from spreading externally from the windows on one floor to those on another floor, as it did during the Triangle fire.
The most effective way to limit vertical fire spread is to enclose stairwells, elevators, and other vertical openings between floors. Reports of features such as caged freight elevators at the Kader factory raise significant questions about the ability of the buildings’ passive fire protection features to prevent vertical spread of fire and smoke.
Fire Safety Training and Other Factors
Another factor that contributed to the large loss of life in both the Triangle and Kader fires was the lack of adequate fire safety training, and the rigid security procedures of both companies.
After the fire at the Kader facility, survivors reported that fire drills and fire safety training were minimal, although the security guards had apparently had some incipient fire training. The Triangle Shirtwaist factory had no evacuation plan, and fire drills were not implemented. Furthermore, post-fire reports from Triangle survivors indicate that they were routinely stopped as they left the building at the end of the work day for security purposes. Various post-fire accusations by Kader survivors also imply that security arrangements slowed their exit, although these accusations are still being investigated. In any case, the lack of a well-understood evacuation plan seems to have been an important factor in the high loss of life sustained in the Kader fire. Chapter 31 of the Life Safety Code addresses fire drills and evacuation training.
The absence of fixed automatic fire protection systems also affected the outcome of both the Triangle and the Kader fires. Neither facility was equipped with automatic sprinklers, although the Kader buildings did have a fire alarm system. According to the Life Safety Code, fire alarms should be provided in buildings whose size, arrangement or occupancy make it unlikely that the occupants themselves will notice a fire immediately. Unfortunately, the alarms reportedly never operated in Building One, which resulted in a significant delay in evacuation. There were no fatalities in Buildings Two and Three, where the fire alarm system functioned as intended.
Fire alarm systems should be designed, installed and maintained in accordance with documents like NFPA 72, the National Fire Alarm Code (NFPA 72, 1993). Sprinkler systems should be designed and installed in accordance with documents like NFPA 13, Installation of Sprinkler Systems, and maintained in accordance with NFPA 25, Inspection, Testing, and Maintenance of Water-Based Fire Protection Systems (NFPA 13, 1994; NFPA 25, 1995).
The initial fuel packages in both the Triangle and Kader fires were similar. The Triangle fire started in rag bins and quickly spread to combustible clothing and garments before involving wood furnishings, some of which were impregnated with machine oil. The initial fuel package at the Kader plant consisted of polyester and cotton fabrics, various plastics, and other materials used to manufacture stuffed toys, plastic dolls, and other related products. These are materials that can typically be ignited easily, can contribute to rapid fire growth and spread, and have a high heat release rate.
Industry will probably always handle materials that have challenging fire protection characteristics, but manufacturers should recognize these characteristics and take the necessary precautions to minimize associated hazards.
The Building’s Structural Integrity
Probably the most notable difference between the Triangle and Kader fires is the effect they had on the structural integrity of the buildings involved. Even though the Triangle fire gutted the top three floors of the ten-storey factory building, the building remained structurally intact. The Kader buildings, on the other hand, collapsed relatively early in the fire because their structural steel supports lacked the fireproofing that would have allowed them to maintain their strength when exposed to high temperatures. A post-fire review of the debris at the Kader site showed no indication that any of the steel members had been fireproofed.
Obviously, building collapse during a fire presents a great threat to both the building’s occupants and to the fire-fighters involved in controlling the blaze. However, it is unclear whether the collapse of the Kader building had any direct effect on the number of fatalities, since the victims may have already succumbed to the effects of heat and products of combustion by the time the building collapsed. If the workers on the upper floors of Building One had been shielded from the products of combustion and heat while they were trying to escape, the building’s collapse would have been a more direct factor in the loss of life.
Fire Focused Attention on Fire Protection Principles
Among the fire protection principles on which the Kader fire has focused attention are exit design, occupant fire safety training, automatic detection and suppression systems, fire separations and structural integrity. These lessons are not new. They were first taught more than 80 years ago at the Triangle Shirtwaist fire and again, more recently, in a number of other fatal workplace fires, including those at the chicken-processing plant in Hamlet, North Carolina, USA, that killed 25 workers; at a doll factory in Kuiyong, China, that killed 81 workers; and at the electrical power plant in Newark, New Jersey, USA, that killed all 3 workers in the plant (Grant and Klem 1994; Klem 1992; Klem and Grant 1993).
The fires in North Carolina and New Jersey, in particular, demonstrate that the mere availability of state-of-the-art codes and standards, such as NFPA’s Life Safety Code, cannot prevent tragic losses. These codes and standards must also be adopted and rigorously enforced if they are to have any effect.
National, state and local public authorities should examine the way they enforce their building and fire codes to determine whether new codes are needed or existing codes need to be updated. This review should also determine whether a building plan review and inspection process is in place to ensure that the appropriate codes are followed. Finally, provisions must be made for periodic follow-up inspections of existing buildings to ensure that the highest levels of fire protection are maintained throughout the life of the building.
Building owners and operators must also be aware that they are responsible for ensuring that their employees’ working environment is safe. At the very least, the state-of-the-art fire protection design reflected in fire codes and standards must be in place to minimize the possibility of a catastrophic fire.
Had the Kader buildings been equipped with sprinklers and working fire alarms, the loss of life might not have been so high. Had Building One’s exits been better designed, hundreds of people might not have been injured jumping from the third and fourth floors. Had vertical and horizontal separations been in place, the fire might not have spread so quickly throughout the building. Had the buildings’ structural steel members been fireproofed, the buildings might not have collapsed.
Philosopher George Santayana has written: “Those who forget the past are condemned to repeat it.” The Kader Fire of 1993 was unfortunately, in many ways, a repeat of the Triangle Shirtwaist Fire of 1911. As we look to the future, we need to recognize all that we need to do, as a global society, to prevent history from repeating itself.