Shiftwork is work scheduled, either permanently or frequently, outside normal daytime working hours. Shiftwork can be e.g., permanent work at night, permanent work during the evening, or work hours can have changing assignment patterns. Each type of shift system has its advantages and disadvantages, and each is associated with differing effects on well-being, health, social life and work performance.
In the traditional slowly rotating shift systems, shifts change weekly; that is, a week of night shifts is followed by a week of evening shifts and then a week of morning shifts. In a quickly rotating shift system only one, two or a maximum of three consecutive days are spent on each shift. In some countries, like the United States, shifts longer than 8 hours, in particular 12 hours, are gaining in popularity (Rosa et al. 1990).
Human beings have evolved as essentially diurnal; that is, the body is mainly “programmed” towards daytime work performance and for night-time recreation and rest. Internal mechanisms (sometimes called the body or biological clock) control the physiology and biochemistry of the body to fit in with a 24-hour environment. These cycles are called circadian rhythms. The disruption of circadian variations in physiological function caused by having to be awake and at work at biologically unusual hours, as well as to sleep during the daytime, is one of the major stresses associated with shiftwork.
Despite the widespread assumption that disturbances of the circadian system may result, over the long run, in harmful effects, the actual cause-effect relation has been difficult to establish. Despite this lack of absolute proof, it is widely accepted that it is prudent to adopt shift systems at the workplace that minimize long-lasting disruption of circadian rhythms.
Combined Effects of Workplace Factors
Some shiftworkers are also exposed to other workplace hazards, such as toxic agents, or to jobs with high mental loads or physical demands. Only a few studies, however, have addressed the problems caused by the combination of shiftwork and unfavourable working, organizational and environmental conditions where the negative effects of shiftwork could be caused not only by the phase difference between circadian rhythms and living conditions, but also by the adverse negative working conditions that may be combined with shiftwork.
A variety of workplace hazards, such as noise, unfavourable climatic conditions, unfavourable lighting conditions, vibration and combinations of these, can sometimes occur more often in three-shift systems, irregular systems and night-shift systems than in two-shift systems or daywork.
Intervening Variables
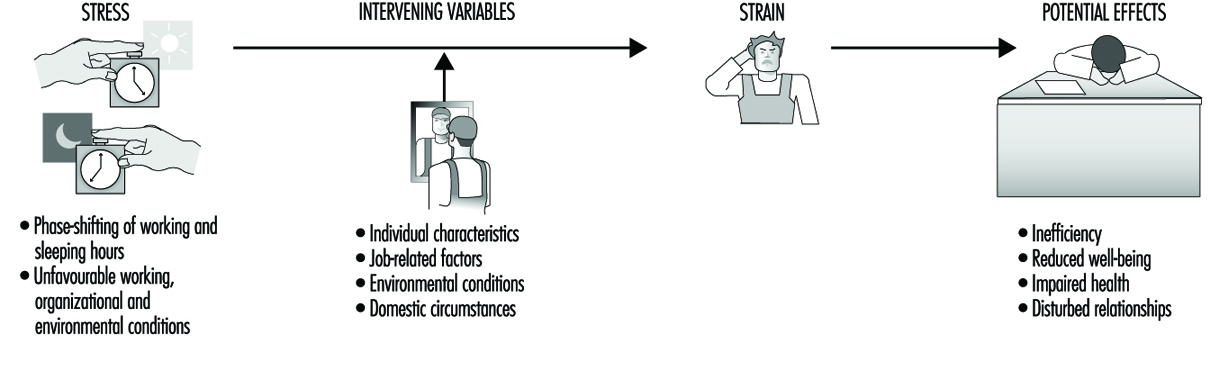
People vary widely in their tolerance of shiftwork, according to Härmä (1993), which may be explained by the influence of many intervening variables. Some individual differences which may modify the strain of shiftworkers are: differences in the phase and amplitude of the circadian cycle, age, gender, pregnancy, physical fitness and flexibility in sleeping habits, and the ability to overcome drowsiness, as illustrated by figure 1.
Figure 1. Model of stress and strain of shiftworkers.
Although some authors found a correlation between a larger amplitude of circadian rhythms and fewer medical complaints (Andlauer et al. 1979; Reinberg et al. 1988; Costa et al. 1989; Knauth and Härmä 1992), others have found that it does not predict adjustment to shiftwork (Costa et al. 1989; Minors and Waterhouse 1981) even after three years of work (Vidacek et al. 1987).
There appear to be two main dimensions of personality related to the circadian phase: “morningness”/“eveningness” and intro-version/extroversion (Kerkhof 1985). Morningness/eveningness can be assessed by questionnaire (Horne and Östberg 1976; Folkard et al. 1979; Torsval and Åkerstedt 1980; Moog 1981) or by measuring body temperature (Breithaupt et al. 1978). Morning types, “larks”, having an advanced phase position of the circadian body temperature, go to bed earlier and rise earlier than the average population, whereas evening types, “owls,” have a delayed circadian phase position and go to bed and rise later. To be a “lark” would appear to be an advantage for morning shifts and an “owl” for night shifts. However, some authors report that a disproportionally large number of those who give up shiftwork were morning types (Åkerstedt and Fröberg 1976; Hauke et al. 1979; Torsvall and Åkerstedt 1979). A relation between morningness and decreased tolerance to shiftwork has been found by Bohle and Tilley (1989) and Vidacek et al. (1987). Other researchers, however, have found opposite results (Costa et al. 1989), and it should be noted that most studies have involved only extreme “larks” and “owls”, where each represents only 5% of the population.
In many questionnaire studies, more adverse health effects of shiftwork have been found with increasing age, the critical age being 40 to 50 years on average (Foret et al. 1981; Koller 1983; Åkerstedt and Torsvall 1981). With increasing age, sleep during the day becomes progressively more difficult (Åkerstedt and Torsvall 1981). There are also some indications of slower circadian adjustment to shiftwork in middle-aged shiftworkers compared to younger ones (Härmä et al. 1990; Matsumoto and Morita 1987).
Gender and pregnancy are two intervening variables which have often been discussed but not yet adequately investigated in longitudinal studies. Based on a review of the literature, Rutenfranz et al. (1987) conclude that the circadian rhythms of men and women react in the same way to the phase shifting of work and sleep in connection with night work. However, two aspects—the menstrual cycle and the additional load of child care and household duties—have to be taken into consideration.
Although some authors have found more frequent menstrual problems in groups of women shiftworkers compared to women in day work (Tasto et al. 1978; Uehata and Sasakawa 1982), the comparability of these shift and day-work groups was question-able. Pokorski et al. (1990) studied perception of discomfort among female triple-shift workers during three phases of the menstrual cycle (praemenstruum, menstruation and postmen-struum). Phase-related differences were more pronounced than differences between morning, evening and night shifts.
Child care at home reduced the duration of sleep and of leisure time in female shiftworking nurses. Estryn-Behar questioned 120 women on permanent night shift and found that the average duration of sleep after night shifts was 6 h 31 min for women without children, 5 h 30 min for women with older children, and 4 h 55 min for women with very young children (Estryn-Behar et al. 1978). Nevertheless, a study of policewomen found that those with children were more favourable towards shiftwork than were women without children (Beermann et al. 1990).
Physical fitness appeared to be a factor in increasing tolerance to shiftwork in a study by Härmä et al. (1988a, b). In a follow-up study with matched pair design, the group of participants who exercised regularly on a four-month programme reported a significant decrease in general fatigue, particularly when on the night shift, as well as a decrease in musculoskeletal symptoms and an increase in sleep length.
The “flexibility of sleeping habits” and “ability to overcome drowsiness”, as assessed by a questionnaire developed by Folkard et al. (1979; 1982) were related, in some studies, to a better tolerance to shiftwork (Wynne et al. 1986; Costa et al. 1989; Vidacek et al. 1987). In other studies, however, this relationship was not confirmed (e.g., Bohle and Tilley 1989).
Other intervening variables that may be important for shiftwork tolerance are the “commitment to night work” as the way in which people schedule their lives (Folkard et al. 1979; Minors and Waterhouse 1981) or the coping style of shiftworkers (Olsson et al. 1987; Olsson and Kandolin 1990).
Besides individual characteristics, situational factors seem to be of importance for explaining the extent of problems reported by shiftworkers. Küpper et al. (1980) and Knauth (1983) found that shiftworkers who tried to sleep during the day and were often or always disturbed by noise, complained more frequently about nervous and gastrointestinal symptoms than did shiftworkers with undisturbed or rarely disturbed sleep.
Health Effects of Shiftwork
Most of the health complaints of shiftworkers can be related to the quality of the day sleep after night shifts and, to a lesser extent, to the sleep before morning shifts. As circadian rhythms generally function such that the body is programmed for daytime performance and for night-time sleep, after the night shift the body is, in general, not completely adjusted for going to sleep. Other factors may also intervene. Daylight may disturb sleep. Noise during the day is in general louder than during the night. Most nightworkers complain about the noise of children and of traffic. Some nightworkers interrupt their day sleep in order to partake of a joint meal with the family, and some reduce their sleep because of their household duties and child care responsibilities. In one study of shiftworkers, the duration of night sleep was found to be reduced to 6 hours (Knauth 1983). Although there are large interindividual differences in sleep needs, 6 or less hours of sleep per day is inadequate for many human beings (Williams et al. 1974). In particular, after many consecutive night shifts an accumulation of sleep deficits has to be expected, with its accompanying effects in both social life and productivity (Naitoh et al. 1990) as well as the possibility of an increased accident rate. Several electroencephalographic studies have also shown that the quality of day sleep is also lower (Knauth 1983).
Sleep deficits may occur in both a week of night shifts and in a week of morning shifts. The prolonged sleep duration at the weekend after a week of morning shifts seems to indicate that there is an increased need for sleep.
Hak and Kampmann (1981) studied sleep and fatigue in train drivers. The earlier the morning shift started, the shorter was the preceding night-shift sleep and the more fatigued the train drivers during the morning shift. The reduction of sleep in connection with an earlier start of the morning shift has also been confirmed by studies of Moors (1990) as well as Folkard and Barton (1993). Such findings may be partially explained by the social pressure of the family not to go to bed too early, or by the body clock, which according to Lavie (1986) causes a “forbidden zone” for sleep, during which sleep propensity is greatly reduced. The latter explanation means that even if the shiftworkers go to bed earlier—because of the early start of the following morning shift—they might find it difficult to fall asleep.
Gastrointestinal disturbances. Night work leads to a change in the sequence and timing of meals. During the night, the stomach cannot cope with the composition and the quantity of a typical daytime meal. It is then understandable that nightworkers often suffer more from disturbances of appetite than do dayworkers or shiftworkers not on night shift, as Rutenfranz et al. (1981) have concluded from a review of the literature.
In the long run, irregular food intake can lead to gastrointestinal complaints or even to disorders. However, the reasons for the complex gastrointestinal symptoms are surely manifold. An analysis of existing studies, such as that of Costa (1996), is difficult, because of methodological differences. Most results are based on cross-sectional studies—that is, on workers currently engaged in shiftwork. Thus, if individuals have left shiftwork because of problems or diseases, we are left with a more or less self-selected population (the “healthy worker” effect). Therefore the health status of a group of shiftworkers may be better than a group of dayworkers, simply because shiftworkers with poorer health or social problems have changed to day work and those that remain may be better able to cope.
In longitudinal studies, which have been almost exclusively retrospective, the problems with self-selection and loss to follow-up are well known. For example, for the sample in the study of Leuliet (1963), the study population was almost halved in size during the study period of 12 years. As with cross-sectional studies, it is often former shiftworkers, who have transferred to day work out of shifts because of medical problems, who show the most serious effects. Thiis-Evensen (1958) found that peptic ulcers were twice as frequent among former shiftworkers as among dayworkers. Aanonsen (1964) and Angersbach et al. (1980) observed, respectively, two and three-and-a-half times as many cases of peptic ulcers among former regular shiftworkers, with a subsequent significant decrease in gastrointestinal disease after the transfer out of the shiftwork pattern.
Costa et al. (1981) computed the time interval between beginning shiftwork and when illnesses were diagnosed (table 1). Comparing groups with different working time arrangements, Costa et al. found the shortest mean intervals (4.7 years) for the appearance of gastroduodenitis in permanent nightworkers. In groups with night work (i.e., three-shift workers and permanent nightworkers), within an interval of about 5 years peptic ulcers developed. In his review Costa (1996) concludes that “there is sufficient evidence to consider shiftwork as a risk factor for gastrointestinal disorders and diseases—in particular peptic ulcer” (table 1).
Table 1. Time intervals from the beginning of shiftwork to the moment when the three illnesses were diagnosed (mean and standard deviation in years).
|
Work schedule |
Gastroduodenitis |
Peptic ulcer |
Neurotic disorders |
|
Day work |
12.6 ± 10.9 |
12.2 ± 9.9 |
9.7 ± 6.8 |
|
Two shifts |
7.8 ± 6.6 |
14.4 ± 8.2 |
9.0 ± 7.5 |
|
Three shifts |
7.4 ± 6.5 |
5.0 ± 3.9 |
6.8 ± 5.2 |
|
Night work |
4.7 ± 4.3 |
5.6 ± 2.8 |
3.6 ± 3.3 |
Source: Costa et al. 1981
Cardiovascular disorders. Kristensen (1989) has analysed the relevant studies on the incidence of cardiovascular disorders in shiftworkers for methodological and analytical factors, as shown in Table 2. Papers published after 1978 were more likely to report an increase in cardiovascular disorders, particularly among those who transferred away from shiftwork. Waterhouse et al. (1992) conclude that it is not possible simply to dismiss the relationship as had been generally accepted (Harrington 1978).
Table 2. Relationship between shiftwork and incidence of cardiovascular disorders
|
Reference |
Publication years |
Conclusion |
Methodological comments/ratings |
|
Thiis-Evenson (1949); Aanonsen (1964) |
1949-1964 |
0 |
2 |
|
Taylor and Pocock (1972) |
1972 |
0 |
? correct choice for controls |
|
Rutenfranz et el. (1977); Carpentier et al. (1977) |
1977 |
0, review articles |
|
|
Angersbach et al. (1980); |
1980-1983 |
+, particularly dropouts; |
2-3 |
|
Michel-Briand et al. (1981) |
1981 |
+, in retired workers |
1 |
|
Alfredsson et al. (1982; 1983; 1985); |
1982-1986 |
+, in men and women; |
3-4 |
|
Åkerstedt et al. (1984) |
1984-1986 |
+, review article |
|
|
Orth-Gomer (1985) |
1985 |
+, review article |
|
|
Andersen (1985) |
1985 |
+, occupations involving shiftwork |
|
|
Frese and Semmer (1986) |
1986 |
+, in dropouts |
Source: Waterhouse et al. 1992. Based on Kristensen 1989. Ratings on conclusions used by Kristensen: +, increased incidence; 0, no difference.
Methodological ratings, 1-4 from lowest to highest quality methodology.
Neurological disorders. Although there is a lack of standardization of the symptoms and disorders in studies of neurological disorders of shiftworkers (Waterhouse et al. 1992; Costa 1996), according to Waterhouse (1992), however, “there is now evidence for a greater tendency towards general malaise—including anxiety and depression elements—in shiftworkers than in day-working colleagues”. Costa (1996) comes to a similar but more cautious conclusion: “there is sufficient evidence to suggest that morbidity for psychoneurotic disorders can be influenced by shiftwork to a greater or lesser extent in relation to other individual and social factors.”
Mortality. There is only one very careful epidemiological study on the mortality of shiftworkers. Taylor and Pocock (1972) compared mortality rates in shiftworkers and dayworkers over a 13-year period in a sample of over 8,000 persons. There were no differences in rates between current shiftworkers and dayworkers. However, the standardized mortality ratio for former shiftworkers was 118.9, compared to 101.5 for current shiftworkers, which “might imply a selecting-out of less fit men” (Harrington 1978).
Social Problems of Shiftworkers
Shiftwork may have negative effects on family life, participation in institutional life and social contacts. The extent of problems which may exist is dependent on many factors, such as the type of shift system, gender, age, marital status, composition of family of the shiftworker, as well as how common shiftwork is in a particular region.
During a week of evening shifts, regular contacts between a shiftworker and his or her school-age children, or partner who may work in morning or day shifts, are dramatically reduced. This is an important problem for shiftworkers who work so-called permanent afternoon shifts (Mott et al. 1965). In the traditional discontinuous two-shift system, a week of morning shifts and evening shifts alternates such that every second week the contacts are disturbed. The traditional weekly rotating three-shift system has evening shifts every third week. In quickly rotating shift systems, contacts within the family are never impaired during a whole week. Researchers have obtained contradicting results. Mott et al. (1965) found that many consecutive evening or night shifts could impair the marital happiness of shiftworkers, while Maasen (1981) did not observe this. Shiftwork—in particular when both parents are shiftworkers—may have negative effects on the school performance of children (Maasen 1981; Diekmann et al. 1981).
Studies concerning the subjective value of free time during different hours of the week showed that weekends were rated higher than weekdays, and evenings higher than time off during the day (Wedderburn 1981; Hornberger and Knauth 1993). The contacts with friends, relatives, clubs, political parties, churches and so on are mainly impoverished by weekend work, evening shifts and night shifts (Mott et al. 1965), as has been reviewed by Bunnage (1981); Walker (1985); and Colligan and Rosa (1990).
Only with respect to hobbies and activities of a solitary or near-solitary nature are shiftworkers at an advantage compared to dayworkers, since gardening, walking, fishing or “do it yourself” projects are comparatively flexible activities which are possible any time, not only in the evening or on weekends.
Some studies have dealt with the burden of shiftworkers’ spouses (Banks 1956; Ulich 1957; Downie 1963; Sergean 1971), who have to alter their lifestyle (for example mealtimes) in order to fit in with the shift system of their mates. They may be forced to postpone noisy household duties and to keep children quiet when the shiftworker is asleep after the night shift. Furthermore, they are alone during evening, night and weekend shifts and have to cope with an irritable spouse. After a change from a weekly to a quickly rotating continuous shift system, 87% of shiftworkers’ spouses voted in favour of the new shift system. They argued that in the old shift system the spouse was very tired after the end of the period of night shifts, needed several days to recover and was not in the mood for joint leisure activities. However, in the new shift system with only two or three consecutive night shifts, the worker was less tired and they enjoyed more joint leisure activities.
Women on shiftwork may have more problems with domestic duties and sleep since household responsibility is not equally shared by the marriage partners. Nevertheless some permanent night nurses have specifically chosen to work at night for domestic reasons (Barton et al. 1993). However, as Walker (1985) concludes in his review, “to say that fixed night shifts for mothers is compatible with their child-rearing responsibilities ignores the ‘costs’”. Constant tiredness because of reduced sleep may be the cost.
Worker Performance
In addition to possible effects of shiftwork on worker health, worker performance can also be affected. Harrington’s (1978) generalized conclusions about performance were reached through consideration of productivity and accidents. They are still valid and have been reformulated by Waterhouse et al. (1992):
- Errors and general performance often showed rhythmic changes, with the night shift being worst.
- The nocturnal decrement in performance could be lessened or prevented if breaks in the work were feasible, if the work were interesting, or if motivation could be maintained.
- The performance worsened (generally with the night shift being more adversely affected than others) if boring, repetitive tasks were involved, if sleep loss had occurred, or if the amount of time spent on duty were increased.
Differences between individuals were often the largest variable in performance.
One problem in comparing productivity and accidents in morning, afternoon and night shifts is methodological. Working, environmental and organizational conditions at night and in the daytime in general are not completely comparable (Colquhoun 1976; Carter and Corlett 1982; Waterhouse et al. 1992). Therefore it is difficult to control all the variables. It is not astonishing that in a review of 24 studies there were almost as many studies with a higher frequency of accidents at night as studies with a higher frequency of accidents in the daytime (Knauth 1983). In some studies the workload in the daytime and during night-time were comparable and measures were available for all 24 hours. In most of these studies the authors found a degraded night-shift performance (e.g., Browne 1949; Bjerner et al. 1955; Hildebrandt et al. 1974; Harris 1977; Hamelin 1981). However, as Monk (1990) has concluded, it is possible that circadian effects can “show through” only when workers are under pressure. In the absence of pressure, workers may be able to equate day-shift and night-shift performance, because both are considerably suboptimal.
The Design of Shift Systems
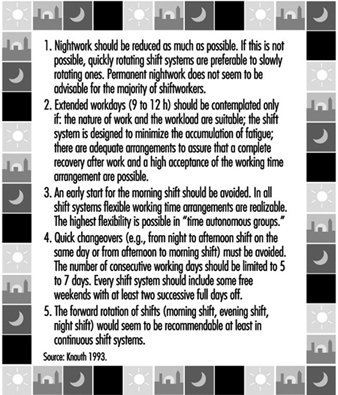
The most important recommendations for the design of shift systems are summarized in figure 2.
Figure 2. Recommendations for the design of shift systems.
Permanent night work
The night shift is the most disruptive of all shifts in terms of physiological adjustment, sleep and well-being. The circadian physiological rhythms of most shiftworkers may require more than one week for complete adjustment to night work. Any partial adjustment will be lost following days off from night shift. Thus, the body rhythms of permanent nightworkers are constantly in a state of disruption. In one study (Alfredsson et al. 1991) the permanent night security guards had a 2-to-3-times higher occurrence of sleep disturbances and fatigue than the national sample of the working population.
Some authors have suggested various ways in which to match employee tolerance for shiftwork and certain external stimuli for helping workers to adjust. According to Hildebrandt et al. (1987) persons with a late phase position (evening types) are able to adjust to night work. Moog (1988) posited that they should work in very long periods of night shifts—that is, much more than 10 nights in a row. To profit from an adjustment to night work, Folkard (1990) even suggested the creation of a “nocturnal subsociety”, which in addition to working permanently at night, would continue to be active at night and to sleep during the day, even when not at work. Although performance at night might in the long run be increased (Wilkinson 1992), such a proposal causes an accumulation of sleep deficits and social isolation, which seems to be unacceptable for most persons (Smith and Folkard 1993).
There are an increasing number of studies dealing with the influence of bright light on re-entrainment of circadian rhythms (some examples are Wever et al. 1983; special session at the IXth International Symposium on Night and Shift Work; Costa et al. 1990a; Rosa et al. 1990; Czeisler et al. 1990). However, “much work is necessary to determine the optimal light-work-sleep schedules for shift workers in terms of their ability to shift circadian rhythms, improve sleep, reduce fatigue, as well as in terms of their social feasibility”, according to Eastman (1990).
In comparison with other shift systems, fixed night shifts have more negative effects on families who must adapt their lifestyles to this schedule, on sexual relations and on workers’ ability to fulfil familial roles (Stein 1963; Mott et al. 1965; Tasto et al. 1978; Gadbois 1981). However, in some studies of permanent night shift, nurses reported fewer complaints than rotating nurses or dayshift nurses (Verhaegen et al. 1987; Barton et al. 1993). Barton et al. propose that one possible explanation for these results may be that the freedom to choose either day- or night-work may greatly influence the degree to which subsequent problems are experienced. The notion that this represents “freedom” is, however, questionable when many female nurses prefer permanent night work because this represents the only way of better arranging domestic responsibilities and employment outside the home (Gadbois 1981).
Permanent night work also has some advantages. Nightworkers report a greater feeling of independence and less supervision at night (Brown 1990; Hoff and Ebbing 1991). Furthermore, because it is less easy to obtain work relief for night-shift staff, apparently more “team spirit” (esprit de corps) develops. However, in most cases night work is chosen because of the increase in income due to the night-shift allowance (Hoff and Ebbing 1991).
Although we have insufficient knowledge about the long-term health effects of permanent night work and about optimal bright-light work-sleep schedules, it is known that the night shift is the most disruptive of all shifts in terms of physiological adjustment, sleep and well-being, and until results from further research are available, we will assume for the moment that permanent night work is not recommendable for the majority of shiftworkers.
Quickly rotating versus slowly rotating shift systems
More rapidly rotating schedules are more advantageous compared to weekly shift rotation. A fast rotation keeps the circadian rhythm in a daytime orientation and it is not in a constant state of disruption from partial adjustment to different day and night orientations. Consecutive night shifts may cause an accumulation of sleep deficits—that is, a chronic sleep deprivation (Tepas and Mahan 1989; Folkard et al. 1990). In the long run this could lead to long-term biological “costs” or even medical disorders. However, no well-controlled epidemiological study is available that compares the effects of permanent, slowly and quickly rotating shift systems. In most published studies the groups are not comparable with regard to the age structure, job content, degree of self-selection (e.g., Tasto et al. 1978; Costa et al. 1981) or because the employees working on fixed morning, afternoon and night shifts were combined to form a single category (Jamal and Jamal 1982). In several longitudinal field studies, the effects of a change from weekly to quicker rotating shift systems have been investigated (Williamson and Sanderson 1986; Knauth and Kiesswetter 1987; Knauth and Schönfelder 1990; Hornberger and Knauth 1995; Knauth 1996). In all 27 studied groups of shiftworkers, the majority of the shiftworkers voted in favour of the quicker rotating shifts after a trial period. Summing up, quickly rotating shift systems are preferable to slowly rotating ones. Åkerstedt (1988), however, does not agree, because the maximum sleepiness usually occurs on the first night shift because of extended prior waking. He recommends slow rotation.
Another argument for a quickly rotating shift system is that shiftworkers have free evenings in every week and thus more regular contact with friends and colleagues is possible than with weekly rotating shifts. Based on analyses of the periodic components of work and leisure time, Hedden et al. (1990) conclude that rotations that allow for a shorter but more frequent synchronization of work life with social life result in less impairment than rotations that lead to longer but infrequent synchronization.
Duration of shifts
There are many contradictory results of the effects of extended workdays, and thus a general recommendation for extended workdays cannot be made (Kelly and Schneider 1982; Tepas 1985). An extended workday of 9 to 12 hours should be contemplated only in the following cases (Knauth and Rutenfranz 1982; Wallace 1989; Tsaneva et al. 1990; Ong and Kogi 1990):
- The nature of work and the workload are suitable for extended working hours.
- The shift system is designed to minimize the accumulation of fatigue.
- There are adequate arrangements for cover of absentees.
- Overtime is not added.
- Toxic exposure is limited.
- It is likely that a complete recovery after work and a high acceptance of the working time arrangements are possible (e.g., housing, family problems, commuting, climate, no moonlighting).
Physiological requirements must be taken into account. According to Bonjer (1971), the acceptable oxygen rate consumption during an 8-hour shift should be about 30% or less of the maximum oxygen consumption. During a 12-hour shift it should be about 23% or less of the maximum oxygen consumption. Since the amount of oxygen consumption increases with the physical demands of the job, it would seem that 12-hour shifts are acceptable only for physically light work. However, even in this case, if the mental or emotional stress caused by the job is too high, extended working hours are not advisable. Before the introduction of extended working hours, the stress and strain at the specific workplace must be accurately evaluated by experts.
One of the potential disadvantages of 12-hour shifts, in particular 12-hour night shifts, is increased fatigue. Therefore the shift system should be designed to minimize the accumulation of fatigue—that is, there should not be many 12-hour shifts in a row and the day shift should not start too early. Koller et al. (1991) recommend single night shifts or a maximum of two night shifts. This recommendation is supported by favourable results of studies in shift systems with single 12-hour night shifts (Nachreiner et al. 1975; Nedeltcheva et al. 1990). In a Belgian study, the length of the shift was extended to 9 hours by starting one hour earlier in the morning (Moors 1990). The day shift started at 0630 instead of 0730 and the morning shift in a two-shift system started at 0500 instead of 0600. In a 5-day week these working time arrangements led to an accumulation of sleep deficits and complaints of tiredness. The author recommends that the shifts start as in the old working time arrangements and that the shift be extended by one hour in the evening.
Our knowledge is very limited concerning another problem: toxic exposure and toxic clearance during the time off work in connection with extended working hours (Bolt and Rutenfranz 1988). In general, exposure limits are based on 8 hours exposure, and one cannot simply extrapolate them to cover a 12-hour shift. Some authors have proposed mathematical procedures for adjusting these exposures for working times that deviate from the usual 8-hour shift, but no method has been uniformly adopted (e.g., Hickey and Reist 1977; OSHA 1978; Brief and Scala 1986; Koller et al. 1991).
Designers of shift systems must consider the workload, the working environment and the conditions outside the place of work. Ong and Kogi (1990) report that “the hot, tropical climate and noisy dwelling units of Singapore were not conducive to sound sleep for shiftworkers, who needed to sleep in the daytime”. Such circumstances increased fatigue and affected productivity on the 12-hour shift worked the next day. Another concern that relates to workers’ well-being is the way shiftworkers use their large blocks of leisure time. In some studies it appears that they may have second jobs (moonlighting), thus increasing their total workload (Angersbach et al. 1980; Wallace 1989; Ong and Kogi 1990). Many other social factors, like commuting, individual differences, social support or events in life must also be considered in the 12-hour shift systems (e.g., Tsaneva et al. 1990).
Timing of shifts
Although there is no optimal solution for the timing of shifts, there is much evidence in the literature that an early start for the morning shift should be avoided. An early start often reduces total sleep because the majority of shiftworkers go to bed at the usual time (Knauth et al. 1980; Åkerstedt et al. 1990; Costa et al. 1990b; Moors 1990; Folkard and Barton 1993). An increase in fatigue during the morning shift has also been observed (Reinberg et. al. 1975; Hak and Kampman 1981; Moors 1990), as well as an increase in the risk of errors and accidents in the morning shift (Wild and Theis 1967; Hildebrandt et al. 1974; Pokorny et al. 1981; Folkard and Totterdell 1991).
Assuming a constant shift length of 8 hours, a late start for the morning shift also means a late start for the night shift (e.g., shift change times at 0700/1500/2300 or 0800/1600/2400). A late start for the night shift means also a late end for the evening shift. In both cases there might be transport problems because buses, trams and trains run less frequently.
The decision in favour of a specific shift change time may also be dependent on the job content. In hospitals, in general, it is the night shift that wakes up, washes and prepares patients (Gadbois 1991).
Arguments in favour of an earlier start have also been made. Some studies have shown that the later the day sleep begins after a night shift, the shorter it will be (Foret and Lantin 1972; Åkerstedt and Gillberg 1981; Knauth and Rutenfranz 1981). Day sleep may be disturbed and a very early start of sleep after night shifts might avoid these problems. Debry et al. (1967) have proposed shift change times at 0400, 1200 and 2000 in order to facilitate workers having as many meals with the family as possible. According to Gadbois (1991) an early start for the night shift improves the contact between staff and patients in hospitals.
Flexible working time arrangements are also possible even in three-shift systems, where employees can choose their working hours (McEwan 1978; Knauth et al. 1981b; 1984; Knauth and Schönfelder 1988). However, in contrast to flexitime in dayworkers, shiftworkers must make pre-arrangements with co-workers.
Distribution of leisure time within the shift system
The distribution of leisure time between consecutive shifts has important implications for sleep, fatigue and well-being, as well as social and family life and the overall satisfaction of the shiftworker with the shift system. If there are only 8 hours between the end of one shift and the start of the next, there will be a reduction of sleep between the shifts and increased fatigue in the second shift (Knauth and Rutenfranz 1972; Saito and Kogi 1978; Knauth et al. 1983; Totterdell and Folkard 1990).
Too many working days in succession can lead to an accumulation of fatigue and sometimes overexposure to toxic substances (Bolt and Rutenfranz 1988). It is not easy to define a limit for the maximum number of consecutive working days, because the workload, the organization of breaks, and exposure to unfavourable environmental conditions vary. However, Koller et al. (1991) recommend limiting the number of consecutive working days to between 5 and 7.
Free weekends are of particular social importance. Pátkei and Dahlgren (1981) studied satisfaction with different types of rapidly rotating shift systems. The satisfaction with a 7-day shift system with 3 to 5 regular days free was significantly higher than in a system with only 2 free days. The authors concluded that “the length of the break might be an important factor in determining the attractivity of rapidly rotating shifts”. On the other hand, free days in the first shift system were counterbalanced by additional periods of holidays during the year.
Direction of rotation. The direction of rotation is another important consideration (Tsaneva et al. 1987; Totterdell and Folkard 1990). A shift system which first moves from morning shift to evening shift, and then to night shift, has a forward rotation (phase delay, clockwise rotation). An anticlockwise, or backward, rotation has a phase advance which moves from night to evening to morning shifts. The forward rotation appears to correspond more closely to the endogenous circadian rhythm, which has a period of more than 24 hours, but only two longitudinal field studies on the effects of different directions of rotation exist (Landen et al. 1981; Czeisler et al. 1982). The majority of the shiftworkers in these studies seem to prefer the forward rotation, but the studies are not definitive. Barton and Folkard (1993) found that an anticlockwise system led to higher levels of fatigue and more sleep disturbances between shifts. “Hybrid” systems were not better. Clockwise rotation was associated with the fewest problems. Turek (1986) proposes, however, that the sleep disturbance of both systems would be comparable.
Shiftworkers on a discontinuous shift system with backward rotation were found to like the long period off work between the end of the last morning shift and the start of the first night shift, in particular if this period includes a weekend.
Although the evidence is limited and further research is needed, forward rotation seems to be recommendable at least in continuous shift systems.
Optimizing shift systems
There is no “optimal” shift system. Each enterprise, its managers and shiftworkers should seek the best compromise between the demands of the enterprise and the needs of the workers. Furthermore, the decision should be founded on scientific recommendations for the design of shift systems. The implementation strategy is of particular importance for the acceptance of a new shift system. Many manuals and guidelines for the implementation of new working time arrangements have been published (ILO 1990). Too often shiftworkers are not sufficiently involved in the analysis, planning and design stage of the shifts.
A continuous shift system that has a rapid forward rotation pattern, with 8 hours of work per shift, some free weekends, at least two successive full days off and no quick changeovers, appears to be the system to be recommended. Such a basic shift system has an average of 33.6 hours per week, which may not be universally acceptable. If additional shifts are required, acceptance is higher when the additional shifts are planned on a long-term basis, such as at the beginning of the year so workers can plan holidays. Some employers do not require older shiftworkers to work additional shifts.
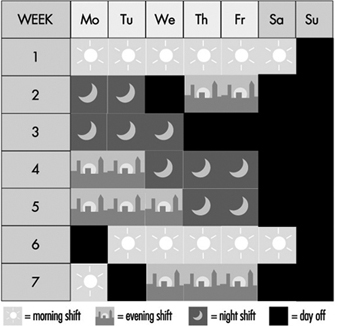
Figures 3 and 4 show schemes for continuous and discontinuous shift systems which accommodate these rules. Figure 5 shows a shift system for a less flexible workplace. It covers 128 operational hours per week, with an average individual workweek of 37 hours. This system has a maximum of three night shifts and two longer free weekends (third week: Thursday to Sunday; fifth/sixth week: Saturday to Monday). It is irregular and does not rotate in a forward direction, which is less optimizing. For shift systems with an operational time of 120 hours per week, gradually rotating shift systems cannot be used, such as from Monday 0600 to Saturday 0600, and an average working time of 40 hours per week.
Figure 3. Rotating continuous shift system.
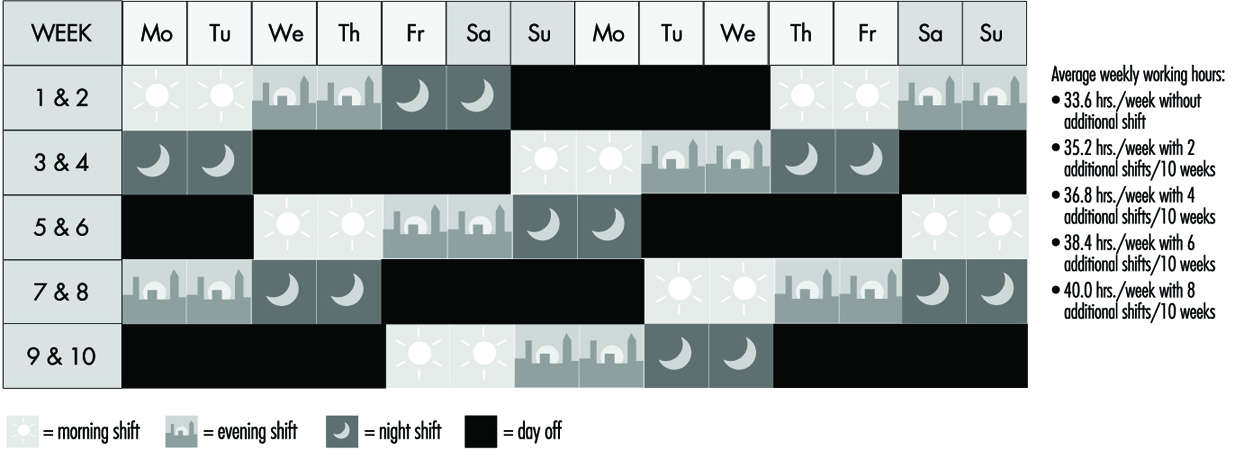
Figure 4. Rotating discontinuous shift system.
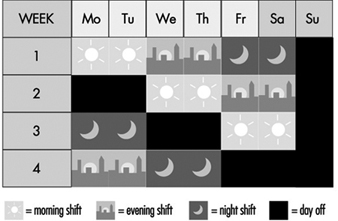
Figure 5. Rotating discontinuous shift system with seven teams.
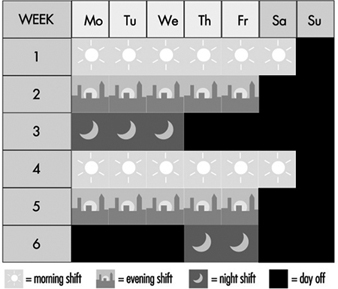
When the crew can be thinned out during the night, a shift system as shown in Figure 6 may be possible. From Monday to Friday, each day two subgroups work in morning shifts, two in evening shifts but only one subgroup works in night shifts. Therefore, the number of night shifts per person would be reduced, compared with the traditional three-shift system.
Figure 6. Discontinuous shift system with a 50% reduced staffing of night shifts.
Rest Periods
In connection with the arrangement of hours of work, adequate periods of rest, such as breaks during working hours, breaks for meals, daily or nightly rest and weekly rest are also important for the workers’ well-being, health and safety.
There are various reasons for the introduction of rest periods.
Recuperation
When a worker performs heavy physical work, fatigue develops and it is necessary for the worker to stop and rest at intervals. During the breaks the symptoms of reversible functional changes of the organism disappear. When, for instance, heart rate is increased by physical work, it will return to the initial value before work during an adequate rest period. The efficiency of a rest period decreases exponentially with the increasing length of the break. As short breaks have a high efficiency, the rule has been deduced that many short breaks are better than a few long breaks.
Prevention of fatigue
During heavy physical work, many rest periods may not only reduce, but under certain circumstances, also prevent fatigue. This is illustrated by the classic studies of Karrasch and Müller (1951). In the laboratory, subjects had to exercise on bicycle ergonometers (Figure 7). This heavy physical work (10 mkp/s) was organized in the following way: after each period of work (100%) a longer rest period (150%) followed. The three experiments each had a different arrangement of work and rest periods. In the first experiment the subject worked 5 min, rested for 7.5 min, then worked again for 5 min and broke off the experiment when exhausted. The heart rate reached about 140 beats/minute in the first work period and more than 160 beats/minute in the second work period. Even one hour after the end of the experiment the heart rate had not returned to the initial value before the experiment. The second experiment shown in the figure involved shorter work and shorter rest periods (2 min and 3 min). Although the workload was identical to the first experiment, the subject in the second experiment was able to work longer before complete exhaustion set in. An extreme arrangement of 0.5 min work and 0.75 min rest period was set up in the third experiment. The heart rate remained at the steady-state level. The experiment was stopped, not because the subject was exhausted but for technical reasons. This extreme organization of work and of rest periods of course cannot be implemented in industry, but it illustrates that extreme fatigue may be prevented if rest periods are split up.
This phenomenon has also been demonstrated in other studies with other indicators such as blood lactic acid (Åstrand and Rodahl 1970).
Figure 7. Heart rate during and after heavy physical work with different lengths of work and rest periods but a constant work/rest ratio of 2:3.

In a study on foundry workers, the comparison of an arrangement of 20 min of work followed always by a 10-min break with an arrangement of 10 min of work and a 5-min break showed the superiority of the second approach (Scholz 1963), because the average heart rate over 8 hours was lower in the second case.
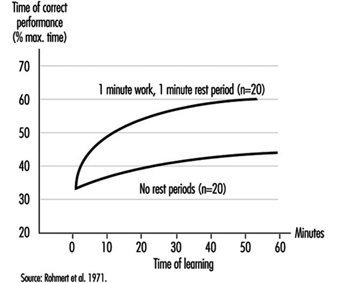
The prevention of fatigue has also been demonstrated with help of heart rate measurements in experiments with learning of sensorimotoric performances (Rutenfranz et al. 1971). Moreover, the progress in learning was clearly greater in experiments with regular rest periods compared with experiments without rest periods, as shown in figure 8.
Figure 8. Effect of rest periods on the learning of simple sensumotoric performance.
Increase in performance
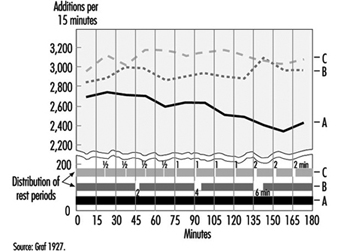
In general, rest periods are considered simply as unproductive interruptions of working time. However, Graf (1922; 1927) showed that rest periods may be, so-to-speak, “rewarding”. We know from sports that athletes running 100 metres start at a high speed, whereas athletes running 5,000 metres start at a “throttled down” speed. Analogue findings on mental work have been published by Graf (figure 9). Three experimental groups were asked to perform calculations. Wages were dependent on the performance. Without being aware of this fact, group A (having the first rest period after 3 hours) started with a reduced speed compared to group B (expecting the first rest period after 45 minutes of work). The highest initial speed and subsequent performance was found in the group C (with rest periods after each 15 minutes of work).
Figure 9. Effects of short rest periods on mental performance.
Maintaining an adequate level of vigilance
In some monotonous monitoring or watchkeeping tasks and in highly simplified tasks with short cycle times, it is difficult to remain alert over longer periods. The reduction of alertness may be overcome by rest periods (or work-structuring measures).
Food intake
The recuperative value of meal breaks is often limited, in particular when the worker has to go a long distance to the canteen, line up for food, eat quickly and hurry back to the working place.
Compensatory physical exercise
If workers, such as visual display unit operators, have to work in constrained postures, it is recommended that they do some compensatory physical exercises during rest periods. Of course the better solution would be to improve the design of the workplace according to ergonomic principles. Physical exercises at the workplace seem to be more accepted in Asian countries than in many other places.
Communication
The social aspect of rest periods, referring to private communication between the workers, should not be neglected. There is a contradiction between the physiologically based recommendation of very short breaks in connection with heavy physical work and the wish of the workers to come together in rest areas and talk with colleagues. Therefore a compromise has to be found.
Hettinger (1993) has published the following rules for the optimal design of rest periods:
- The initial parts of a rest period have the highest recuperative value, which is what results in the effectiveness of short breaks (i.e., many short breaks are more favourable than a few longer breaks with regard to the recuperative value).
- Exceptions to this rule: The cooling-down rest period after work in a hot climate should last at least 10 min in a room with a neutral climate. The warming-up rest period after work in a cold climate (–15 to –30°C) should last for at least 30 min in a room with a neutral climate. The rest period after working in a very loud working environment should be relatively long in a room with less than 70 dB(A). These rest periods are problematic, if one bears in mind that, if the time of exposure is halved, merely a reduction of about 3 dB(A) is achieved in the noise dose.
- The frequency and duration of the rest period is dependent on the degree of difficulty of the physical or mental work. Concerning physical work, it may be specified that physical work with an energy consumption above the acceptable endurance limit but less than 40 KJ/min permits the rest period to be arranged within the shiftworking time. Physical work with an energy consumption of greater than 40 KJ/min demands a rest period immediately after stopping the heavy work, because of the exponential increase of fatigue.
- The efficiency of a rest period should not be reduced by “pseudo-activities” (disguised breaks). Workers and superiors should be informed accordingly.
Rest periods for food intake should last at least 15 minutes.
For further information concerning rest periods after muscular work, see Laurig (1981); and for rest periods after mental work, see Luczak (1982).
Reduction of Sleep Problems
There are no magic formulae to help shiftworkers fall asleep quickly or sleep well. What works for one person may not work for another.
Some useful proposals, mainly for day sleep following night shifts, include:
- Use individual headphones for TV and radio for the other members of the family, and a silent telephone answering machine. Switch off the door-bell.
- Let one’s family know about the work schedule and avoid household noise during sleep times.
- Reduce outside light and noise by using heavy, dark curtains, soundproofed doors and windows, and an air conditioner.
- Ear plugs, a sleeping mask and not drinking any caffeinated drinks within 5 hours of your expected bedtime can also help.
- If the living quarters are noisy, workers should consider moving to quieter living quarters.
Workers should avoid using alcohol to assist in going to sleep and should give themselves time to slow down after work (Community Health Network 1984; Monk 1988; Wedderburn 1991).
For cases where safety is at stake, some authors recommend “maintenance naps” during the night shift as a bridge over the night-time low point in circadian alertness (Andlauer et al. 1982). Many Japanese 24-hour industries allow napping practices on night shifts (Kogi 1981).
Diet
Although there is no evidence that diet assists in coping with night work (Rosa et al. 1990), the following prudent recommendations have been made:
- During night shift, the main meal should be eaten at or before 0100 and should be rich in protein rather than carbohydrates, and have a low fat content.
- Have a snack of fresh fruit or milk products at about 0400–0415.
- Eating meals at the same time each day is recommended.
- A heavy meal just before bedtime should be avoided. Workers should learn to listen to their bodies, to judge stomach comfort and energy levels (Community Health Network 1984; Wedderburn 1991; Knauth et al. 1991).
Occupational Health Measures
Some authors recommend pre-employment screening and medical surveillance of shiftworkers (e.g., Rutenfranz et al. 1985; Scott and LaDou 1990). Workers should be counselled against night work if they have or are:
- a history of digestive tract disorders (e.g., recurrent peptic ulcer disease, irritable bowel syndrome, if symptoms are severe)
- insulin-dependent diabetes mellitus
- thyrotoxicosis
- coronary artery disease, especially if there is unstable angina or a history of myocardial infarction
- narcoleptics and others suffering from chronic sleep disturbances
- epileptics
- severe psychiatric disorders, in particular chronic depression
- asthma requiring medication, especially if the patient is steroid dependent
- active and extensive tuberculosis
- alcoholics and drug addicts
- marked visual impairment or hemeralopia (day blindness) that is too severe for effective correction.
In addition, Scott and LaDou (1990) also mention some “relative contra-indications” most appropriately used for counselling prospective employees, such as extreme “morningness”, sleep rigidity. They may wish to consider their age and the extent of their family responsibilities.
Hermann (1982) has proposed the following intervals for regular health checks: there should be a second health check not later than 12 months after starting night work, and regular health checks at least every 2 years for those under 25, every 5 years for those between 25 and 50, every 2 to 3 years for those between 50 and 60, and every 1 to 2 years for those above 60.
Individual Behavioural Techniques
There are only a few studies analysing shiftworkers’ ability to cope with stress (Olsson et al. 1987; Olsson and Kandolin 1990; Kandolin 1993, Spelten et al. 1993). An active coping strategy—for example, discussing the problems with others—appears to reduce stress better than passive strategies, such as the use of alcohol (Kandolin 1993). However, longitudinal studies are necessary to study the relationship between coping style or behavioural techniques and stress.
Money Payments
Although many compensation plans exist whereby a worker is compensated more for shiftwork (shift bonus), money payments are not an appropriate trade-off for possible negative health effects and disruption of social life.
The best way, of course, to solve problems is to eliminate or reduce the causes. However, since complete elimination of shiftwork is not possible, an alternative strategy worth considering is such as the following: a reduction of unusual working hours for the individual; reduction of night shifts; reduce the unnecessary part of the night work (sometimes activities may be shifted to the morning or evening shift by reorganization of work); implement mixed shift systems with, for example, at least one month per year without shiftwork; insertion of additional shift crews, such as by changing from a 3-shift system to a 4-shift system or from a 4-shift system to a 5-shift system, or by reduction of overtime. Reduction of working time for shiftworkers is another possibility, with shorter weekly working hours for shiftworkers than for dayworkers, with paid breaks and longer holiday periods. Extra days off and stepwise or early retirement are other possible remedies.
All these proposals have already been implemented in some companies in industry or the services sector (e.g., Knauth et al. 1990).
Other Measures
Many other measures such as physical exercise (Härmä et al. 1988a, b), pharmacological aids (Rosa et al. 1990), family counselling (Rosa et al. 1990), improvement of environmental conditions at work (Knauth et al. 1989), better communication between shiftworkers and unions or shiftworkers and their congressperson (Monk 1988; Knauth et al. 1989), or a “Shift Work Awareness Programme” within the company (Monk 1988) have been proposed to reduce the problems of shiftworkers. As there is not one best way to reduce the problems of shiftworkers many creative solutions should be tried (Colquhoun et al. 1996).