- You are here:
-
Home

-
Part XVI. Construction
-
Construction
- Major Sectors and Their Hazards
Evaluating Health and Safety Training: A Case Study in Chemical Workers Hazardous Waste Worker Education
Until very recently the effectiveness of training and education in controlling occupational health and safety hazards was largely a matter of faith rather than systematic evaluation (Vojtecky and Berkanovic 1984-85; Wallerstein and Weinger 1992). With the rapid expansion of intensive federally-funded training and education programmes in the past decade in the United States, this has begun to change. Educators and researchers are applying more rigorous approaches to evaluating the actual impact of worker training and education on outcome variables such as accident, illness and injury rates and on intermediate variables such as the ability of workers to identify, handle and resolve hazards in their workplaces. The programme that combines chemical emergency training as well as hazardous waste training of the International Chemical Workers Union Center for Worker Health and Safety Education provides a useful example of a well-designed programme which has incorporated effective evaluation into its mission.
The Center was established in Cincinnati, Ohio, in 1988 under a grant which the International Chemical Workers Union (ICWU) received from the National Institute for Environmental Health Sciences to provide training for hazardous waste and emergency response workers. The Center is a cooperative venture of six industrial unions, a local occupational health centre and a university environmental health department. It adopted an empowerment education approach to training and defines its mission broadly as:
… promoting worker abilities to solve problems and to develop union-based strategies for improving health and safety conditions at the worksite (McQuiston et al. 1994).
To evaluate the programme’s effectiveness in this mission the Center conducted long-term follow-up studies with the workers who went through the programme. This comprehensive evaluation went considerably beyond the typical assessment which is conducted immediately following training, and measures trainees’ short-term retention of information and satisfaction with (or reaction to) the education.
Programme and Audience
The course that was the subject of evaluation is a four or five-day chemical emergency/hazardous waste training programme. Those attending the courses are members of six industrial unions and a smaller number of management personnel from some of the plants represented by the unions. Workers who are exposed to substantial releases of hazardous substances or who work with hazardous waste less proximately are eligible to attend. Each class is limited to 24 students so as to promote discussion. The Center encourages local unions to send three or four workers from each site to the course, believing that a core group of workers is more likely than an individual to work effectively to reduce hazards when they return to the workplace.
The programme has established interrelated long-term and short-term goals:
Long-term goal: for workers to become and remain active participants in determining and improving the health and safety conditions under which they work.
Immediate educational goal: to provide students with relevant tools, problem-solving skills, and the confidence needed to use those tools (McQuiston et al. 1994).
In keeping with these goals, instead of focusing on information recall, the programme takes a “process oriented” training approach which seeks “to build self-reliance that stresses knowing when additional information is needed, where to find it, and how to interpret and use it.” (McQuiston et al. 1994.)
The curriculum includes both classroom and hands-on training. Instructional methods emphasize small group problem-solving activities with the active participation of the workers in the training. The development of the course also employed a participatory process involving rank-and-file safety and health leaders, programme staff and consultants. This group evaluated initial pilot courses and recommended revisions of the curriculum, materials and methods based on extensive discussions with trainees. This formative evaluation is an important step in the evaluation process that takes place during programme development, not at the end of the programme.
The course introduces the participants to a range of reference documents on hazardous materials. Students also develop a “risk chart” for their own facility during the course, which they use to evaluate their plant’s hazards and safety and health programmes. These charts form the basis for action plans which create a bridge between what the students learn at the course and what they decide needs to be implemented back in the workplace.
Evaluation Methodology
The Center conducts anonymous pre-training and post-training knowledge tests of participants to document increased levels of knowledge. However, to determine the long-term effectiveness of the programme the Center uses telephone follow-up interviews of students 12 months after training. One attendee from each local union is interviewed while every manager attendee is interviewed. The survey measures outcomes in five major areas:
- students’ ongoing use of resource and reference materials introduced during training
- the amount of secondary training, that is, training conducted by participants for co-workers back at the worksite following attendance at the Center course
- trainee attempts and successes in obtaining changes in worksite emergency response or hazardous waste programmes, procedures or equipment
- post-training improvements in the way spills are handled at the worksite
- students' perceptions of training programme effectiveness.
The most recent published results of this evaluation are based on 481 union respondents, each representing a distinct worksite, and 50 management respondents. The response rates to the interviews were 91.9% for union respondents and 61.7% for management.
Results and Implications
Use of resource materials
Of the six major resource materials introduced in the course, all except the risk chart were used by at least 60% of the union and management trainees. The NIOSH Pocket Guide to Chemical Hazards and the Center’s training manual were the most widely used.
Training of co-workers
Almost 80% of the union trainees and 72% of management provided training to co-workers back at the worksite. The average number of co-workers taught (70) and the average length of training (9.7 hours) were substantial. Of special significance was that more than half of the union trainees taught managers at their worksites. Secondary training covered a wide range of topics, including chemical identification, selection and use of personal protective equipment, health effects, emergency response and use of reference materials.
Obtaining worksite improvements
The interviews asked a series of questions related to attempts to improve company programmes, practices and equipment in 11 different areas, including the following seven especially important ones:
- health effects training
- availability of material safety data sheets
- chemical labelling
- respirator availability, testing and training
- gloves and protective clothing
- emergency response
- decontamination procedures.
The questions determined whether respondents felt changes were needed and, if so, whether improvements had been made.
In general, union respondents felt greater need for and attempted more improvements than management, although the degree of difference varied with specific areas. Still fairly high percentages of both unions and management reported attempted improvements in most areas. Success rates over the eleven areas ranged from 44 to 90% for unionists and from 76 to 100% for managers.
Spill response
Questions concerning spills and releases were intended to ascertain whether attendance at the course had changed the way spills were handled. Workers and managers reported a total of 342 serious spills in the year following their training. Around 60% of those reporting spills indicated that the spills were handled differently because of the training. More detailed questions were subsequently added to the survey to collect additional qualitative and quantitative data. The evaluation study provides workers’ comments on specific spills and the role the training played in responding to them. Two examples are quoted below:
Following training the proper equipment was issued. Everything was done by the books. We have come a long way since we formed a team. The training was worthwhile. We don’t have to worry about the company, now we can judge for ourselves what we need.
The training helped by informing the safety committee about the chain of command. We are better prepared and coordination through all departments has improved.
Preparedness
The great majority of union and management respondents felt that they are “much better” or “somewhat better” prepared to handle hazardous chemicals and emergencies as a result of the training.
Conclusion
This case illustrates many of the fundamentals of training and education programme design and evaluation. The goals and objectives of the educational programme are explicitly stated. Social action objectives regarding workers’ ability to think and act for themselves and advocate for systemic changes are prominent along with the more immediate knowledge and behaviour objectives. The training methods are chosen with these objectives in mind. The evaluation methods measure the achievement of these objectives by discovering how the trainees applied the material from the course in their own work environments over the long term. They measure training impact on specific outcomes such as spill response and on intermediate variables such as the extent to which training is passed on to other workers and how course participants use resource materials.
Worker Education and Training
Worker training in occupational safety and health may serve many different purposes. Too often, worker training is viewed only as a way to comply with governmental regulations or to reduce insurance costs by encouraging individual workers to follow narrowly defined safe work behaviours. Worker education serves a far broader purpose when it seeks to empower workers to take an active part in making the workplace safe, rather than simply to encourage worker compliance with management safety rules.
Over the past two decades, there has been a move in many countries toward the concept of broad worker involvement in safety and health. New regulatory approaches rely less on government inspectors alone to enforce safety and health on the job. Labour unions and management are increasingly encouraged to collaborate in promoting safety and health, through joint committees or other mechanisms. This approach requires a skilled and well-informed workforce that can interact directly with management on issues of safety and health.
Fortunately, there are many international models for training workers in the full range of skills necessary to participate broadly in workplace health and safety efforts. These models have been developed by a combination of labour unions, university-based labour education programmes and community-based non-governmental organizations. Many innovative worker training programmes were developed originally with financing from special government grant programmes, union funds or employer contributions to collectively bargained safety and health funds.
These participatory worker training programmes, designed in a variety of national settings for diverse worker populations, share a general approach to training. The educational philosophy is based on sound adult education principles and draws upon the empowerment philosophy of “popular education”. This article describes the educational approach and its implications for designing effective worker training.
Educational Approach
Two disciplines have influenced the development of labour-oriented safety and health education programmes: the field of labour education and, more recently, the field of “popular” or empowerment education.
Labour education began simultaneously with the trade union movement in the 1800s. Its early goals were directed towards social change, that is, to promote union strength and the integration of working people into political and union organizing. Labour education has been defined as a “specialized branch of adult education that attempts to meet the educational needs and interests arising out of workers’ participation in the union movement”. Labour education has proceeded according to well-recognized principles of adult learning theory, including the following:
- Adults are self-motivated, especially with information that has immediate application to their lives and work. They expect, for example, practical tools to help them solve problems in the workplace.
- Adults learn best by building on what they already know so that they can incorporate new ideas into their existing, vast reservoir of learning. Adults wish to be respected for their experience in life. Therefore, effective methods draw on participants' own knowledge and encourage reflection on their knowledge base.
- Adults learn in different ways. Each person has a particular learning style. An educational session will work best if participants have the opportunity to engage in multiple learning modalities: to listen, look at visuals, ask questions, simulate situations, read, write, practice with equipment and discuss critical issues. Variety not only ensures that each cognitive style is addressed but also provides repetition to reinforce learning and, of course, combats boredom.
- Adults learn best when they are actively engaged, when they “learn by doing”. They are more responsive to active, participatory methods than to passive measures. Lectures and written materials have their place in a full repertoire of methods. But case studies, role plays, hands-on simulations and other small-group activities that allow each individual to be involved are more likely to result in the retention and application of new learning. Ideally, each session involves interaction between participants and includes occasions for learning new information, for applying new skills and for discussing causes of problems and barriers to solving them. Participatory methods require more time, smaller groups and perhaps different instructional skills than those that many trainers currently possess. But to increase the impact of education, active participation is essential.
Since the beginning of the 1980s, worker safety and health training has also been influenced by the perspective of “popular” or “empowerment” education. Popular education since the 1960s has developed largely from the philosophy of Brazilian educator Paulo Freire. It is an approach to learning that is participatory and is based on the reality of student/worker experiences in their worksites. It fosters dialogue between educators and workers; critically analyses the barriers to change, such as organizational or structural causes of problems; and has worker action and empowerment as its goals. These tenets of popular education incorporate the basic principles of adult education, yet stress the role of worker action in the educational process, both as a goal to improve worksite conditions and as a mechanism for learning.
Participatory education in an empowerment context is more than small group activities that involve students/workers in active learning within the classroom. Participatory popular education means students/workers have the opportunity to acquire analytic and critical thinking skills, practice social action skills and develop the confidence to develop strategies for the improvement of the work environment long after the education sessions end.
Design of Education Programmes
It is important to realize that education is a continuing process, not a one-time event. It is a process that requires careful and skilful planning though each major stage. To implement a participatory education process that is based on sound adult education principles and that empowers workers, certain steps must be taken for planning and implementing participatory worker education which are similar to those used in other training programmes (see “Principles of Training”), but require special attention to meeting the goal of worker empowerment:
Step one: Assess needs
Needs assessment forms the foundation for the entire planning process. A thorough needs assessment for worker training includes three components: a hazards assessment, a profile of the target population and background on the social context of training. The hazards assessment is aimed at identifying high-priority problems to be addressed. The target population profile attempts to answer a broad set of questions about the workforce: Who can most benefit from training? What training has the target population already received? What knowledge and experience will the trainees bring to the process? What is the ethnic and gender makeup of the workforce? What is the literacy level of the workers and what languages do they speak? Whom do they respect and whom do they mistrust? Finally, gathering information on the social context of training allows the trainer to maximize the impact of training by looking at the forces that may support improved safety and health conditions (such as strong union protection that allow workers to speak out freely about hazards) and those that may pose barriers (such as productivity pressures or lack of job security).
Needs assessment can be based on questionnaires, review of documents, observations made in the workplace and interviews with workers, their union representatives and others. The popular education approach utilizes an ongoing “listening” process to gather information about the social context of training, including people's concerns and the obstacles that might inhibit change.
Step two: Gain support
Successful worker education programmes rely on identifying and involving key actors. The target population must be involved in the planning process; it is difficult to gain their trust without having sought their input. In a popular education model, the educator attempts to develop a participatory planning team from the union or shop floor who can provide ongoing advice, support, networking and a check on the validity of the needs assessment findings.
Labour unions, management and community-based groups are all potential providers of worker safety and health education. Even if not sponsoring the training directly, each of these groups may have a key role to play in supporting the educational effort. The union can provide access to the workforce and back up the efforts for change that hopefully will emerge from the training. Union activists who are respected for their knowledge or commitment can assist in outreach and help ensure a successful training outcome. Management is able to provide paid released time for training and may more readily support efforts to improve safety and health that grow out of a training process they have “bought into”. Some employers understand the importance and cost-effectiveness of comprehensive worker training in safety and health, while others will not participate without government-mandated training requirements or a collectively bargained right to paid educational leave for safety and health training.
Community-based non-governmental organizations can provide training resources, support or follow-up activities. For non-union workers, who may be especially vulnerable to retaliation for safety and health advocacy on the job, it is particularly important to identify community support resources (such as religious groups, environmentalist organizations, disabled worker support groups or minority workers’ rights projects). Whoever has a significant role to play must be involved in the process through co-sponsorship, participation on an advisory committee, personal contact or other means.
Step three: Establish education objectives and content
Using information from the needs assessment, the planning team can identify specific learning objectives. A common mistake is to assume that the objective of workshops is simply to present information. What is presented matters less than what the target population receives. Objectives should be stated in terms of what workers will know, believe, be able to do or accomplish as a result of the training. The majority of traditional training programmes focus on objectives to change the individuals' knowledge or behaviours. The goal of popular worker education is to create an activist workforce that will advocate effectively for a healthier work environment. Popular education objectives may include learning new information and skills, changing attitudes and adopting safe behaviours. However, the ultimate goal is not individual change, but collective empowerment and workplace change. The objectives leading to this goal include the following:
- Information objectives are geared towards the specific knowledge the learner will receive, for example, information about the health hazards of solvents.
- Skill objectives are intended to ensure that participants can do specific tasks that they will need to be able to perform back on the job. These can range from individual, technical skills (such as how to lift properly) to group action skills (such as how to advocate for ergonomic redesign of the workplace). Empowerment-oriented education emphasizes social action skills over mastery of individual tasks.
- Attitude objectives aim to have an impact on what the worker believes. They are important for ensuring that people move beyond their own barriers to change so that they are able to actually put their new-found knowledge and skills to use. Examples of attitudes that may be addressed include beliefs that accidents are caused by the careless worker, that workers are apathetic and do not care about safety and health or that things never change and nothing one can do will make a difference.
- Individual behavioural objectives aim to affect not just what a worker can do, but what a worker actually does back on the job as a result of training. For example, a training programme with behavioural objectives would aim to have a positive impact on respirator use on the job, not just to convey information in the classroom as to how to use a respirator properly. The problem with individual behaviour change as an objective is that workplace safety and health improvements rarely take place on an individual level. One can use a respirator properly only if the right respirator is provided and if there is time allowed for taking all necessary precautions, regardless of production pressures.
- Social action objectives also aim to have an effect on what the worker will do back on the job but address the goal of collective action for change in the work environment, rather than individual behaviour change. Actions that result from such training can range from small steps, such as investigating one specific hazard, to large undertakings, such as starting an active safety and health committee or campaigning to redesign a dangerous work process.
There is a hierarchy of these objectives (figure 1). Compared with the other training objectives, knowledge objectives are the easiest to achieve (but they are by no means easy to attain in an absolute sense); skill objectives require more hands-on training to ensure mastery; attitude objectives are more difficult because they may involve challenging deeply held beliefs; individual behaviour objectives are achievable only if attitude barriers are addressed and if performance, practice and on-the-job follow-up are built into the training; and social action objectives are most challenging of all, because training must also prepare participants for collective action in order to achieve more than they can on an individual basis.
Figure 1. Hierarchy of training objectives.
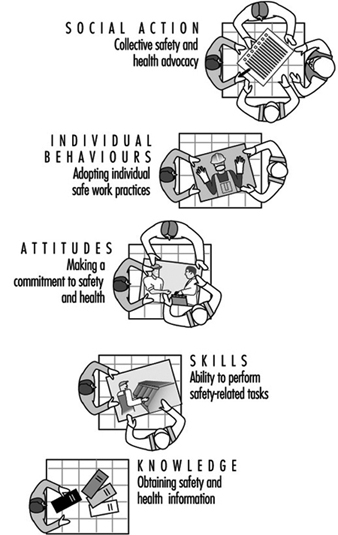
For example, it is a reasonably straightforward task to communicate the risks that asbestos poses to workers. The next step is to ensure that they have the technical skills to follow all safety procedures on the job. It is more difficult still to change what workers believe (e.g., to convince them that they and their fellow workers are at risk and that something can and should be done about it). Even armed with the right skills and attitudes, it may be difficult for workers to actually follow safe work practices on the job, especially since they may lack the proper equipment or management support. The ultimate challenge is to promote social action, so that workers may gain the skills, confidence and willingness to insist on using less hazardous substitute materials or to demand that all necessary environmental controls be used when they are working with asbestos.
Empowerment-oriented labour education always aims to have an impact on the highest level—social action. This requires that workers develop critical thinking and strategic planning skills that will allow them to set achievable goals, constantly respond to barriers and reshape their plans as they go. These are complex skills that require the most intensive, hands-on approach to training, as well as strong on-going support that the workers will need in order to sustain their efforts.
The specific content of educational programmes will depend on the needs assessment, regulatory mandates and time considerations. Subject areas that are commonly addressed in worker training include the following:
- health hazards of relevant exposures (such as noise, chemicals, vibration, heat, stress, infectious diseases and safety hazards)
- hazard identification methods, including means of obtaining and interpreting data regarding workplace conditions
- control technologies, including engineering and work organization changes, as well as safe work practices and personal protective equipment
- legal rights, including those relating to regulatory structures, the worker’s right to know about job hazards, the right to file a complaint and the right to compensation for injured workers
- union safety and health provisions, including collectively bargained agreements giving members the right to a safe environment, the right to information and the right to refuse to perform under hazardous conditions
- union, management, government and community resources
- the roles and responsibilities of safety and health committee members
- prioritizing hazards and developing strategies to improve the worksite, including analysis of possible structural or organizational barriers and design of action plans
Step four: Select education methods
It is important to select the right methods for the chosen objectives and content areas. In general, the more ambitious the objectives, the more intensive the methods must be. Whatever methods are selected, the profile of the workforce must be considered. For example, educators need to respond to workers’ language and literacy levels. If literacy is low, the trainer should use oral methods and highly graphic visuals. If a variety of languages is in use among the target population the trainer should use a multilingual approach.
Because of time limitations, it may not be possible to present all of the relevant information. It is more important to provide a good mix of methods to enable workers to acquire research skills and to develop social action strategies so that they can pursue their own knowledge, rather than attempt to condense too much information into a short period of time.
The teaching methods chart (see table 1) provides a summary of different methods and the objectives which each might fulfil. Some methods, such as lectures or informational films, primarily fulfil knowledge objectives. Worksheets or brainstorming exercises can fulfil information or attitude objectives. Other more comprehensive methods, such as case studies, role-plays or short videotapes that trigger discussion may be aimed at social action objectives, but may also contain new information and may present opportunities to explore attitudes.
Table 1. Teaching methods chart
| Teaching methods | Strengths | Limitations | Objectives achieved |
| Lecture | Presents factual material in direct and logical manner. Contains experiences which inspire. Stimulates thinking to open a discussion. For large audiences. |
Experts may not always be good teachers. Audience is passive. Learning difficult to gauge. Needs clear introduction and summary. |
Knowledge |
| Worksheets and questionnaires | Allow people to think for themselves without being influenced by others in discussion. Individual thoughts can then be shared in small or large groups. |
Can be used only for short period of time. Handout requires preparation time. Requires literacy. | Knowledge Attitudes/emotions |
| Brainstorming | Listening exercise that allows creative thinking for new ideas. Encourages full participation because all ideas equally recorded. | Can become unfocused. Needs to be limited to 10 to 15 minutes. |
Knowledge Attitudes/emotions |
| Planning deck | Can be used to quickly catalogue information. Allows students to learn a procedure by ordering its component parts. Group planning experience. |
Requires planning and creation of multiple planning decks. | Knowledge |
| Risk mapping | Group can create visual map of hazards, controls, and plans for action. Useful as follow-up tool. |
Requires workers from same or similar workplace. May require outside research. |
Knowledge Skills/social action |
| Audiovisual materials (films, slide shows, etc.) | Entertaining way of teaching content and raising issues. Keeps audience’s attention. Effective for large groups. |
Too many issues often presented at one time. Too passive if not combined with discussion. |
Knowledge/skills |
| Audiovisuals as triggers | Develops analytic skills. Allows for exploration of solutions. |
Discussion may not have full participation. | Social action Attitudes/emotions |
| Case studies as triggers | Develops analytic and problem-solving skills. Allows for exploration of solutions. Allows students to apply new knowledge and skills. |
People may not see relevance to own situation. Cases and tasks for small groups must be clearlydefined to be effective. |
Social action Attitudes/emotions Skills |
| Role playing session (trigger) | Introduces problem-situation dramatically. Develops analytic skills. Provides opportunity for people to assume roles of others. Allows for exploration of solutions. |
People may be too self-conscious. Not appropriate for large groups. |
Social action Attitudes/emotions Skills |
| Report back session | Allows for large group discussion of role plays, case studies, and small group exercise. Gives people a chance to reflect on experience. | Can be repetitive if each small group says the same thing. Instructors need to prepare focused questions to avoid repetitiveness. | Social action skills Information |
| Prioritizing and planning activity | Ensures participation by students. Provides experience in analysing and prioritizing problems. Allows for active discussion and debate. | Requires a large wall or blackboard for posting. Posting activity should proceed at a lively pace to be effective. | Social action Skills |
| Hands-on practice | Provides classroom practise of learned behaviour. | Requires sufficient time, appropriate physical space, and equipment. | Behaviours Skills |
Adapted from: Wallerstein and Rubenstein 1993. By permission.
Step five: Implementing an education session
Actually conducting a well-designed education session becomes the easiest part of the process; the educator simply carries out the plan. The educator is a facilitator who takes the learners through a series of activities designed to (a) learn and explore new ideas or skills, (b) share their own thoughts and abilities and (c) combine the two.
For popular education programmes, based on active participation and sharing of worker’s own experiences, it is critical that workshops establish a tone of trust, safety in discussion and ease of communication. Both physical and social environments need to be well planned to allow for maximum interaction, small group movement and confidence that there is a shared group norm of listening and willingness to participate. For some educators, this role of learning facilitator may require some “retooling”. It is a role that relies less on a talent for effective public speaking, the traditional centrepiece of training skills, and more on an ability to foster cooperative learning.
The use of peer trainers is gaining in popularity. Training workers to train their peers has two major advantages: (1) worker trainers have the practical knowledge of the workplace to make training relevant and (2) peer trainers remain in the workplace to provide on-going safety and health consultation. The success of peer trainer programmes is dependent on providing a solid foundation for worker trainers through comprehensive “training of trainer” programmes and access to technical experts when needed.
Step six: Evaluate and follow up
Though often overlooked in worker education, evaluation is essential and serves several purposes. It allows the learner to judge his or her progress toward new knowledge, skills, attitudes or actions; it allows the educator to judge the effectiveness of the training and to decide what has been accomplished; and it can document the success of training to justify future expenditures of resources. Evaluation protocols should be set up in concert with the education objectives. An evaluation effort should tell you whether or not you have achieved your training objectives.
The majority of evaluations to date have assessed immediate impact, such as knowledge learned or degree of satisfaction with the workshop. Behaviour-specific evaluations have used observations at the worksite to assess performance.
Evaluations that look at workplace outcomes, particularly injury and illness incidence rates, can be deceptive. For example, management safety promotion efforts often include incentives for keeping accident rates low (e.g., by offering a prize to the crew with the least accidents in a year). These promotional efforts result in under-reporting of accidents and often do not represent actual safety and health conditions on the job. Conversely, empowerment-oriented training encourages workers to recognize and report safety and health problems and may result, at first, in an increase in reported injuries and illnesses, even when safety and health conditions are actually improving.
Recently, as safety and health training programmes have begun to adopt empowerment and popular education goals and methods, evaluation protocols have been broadened to include assessment of worker actions back at the worksite as well as actual worksite changes. Social action objectives require long-term evaluation that assesses changes on both the individual level and on the environmental and organization level, and the interaction between individual and environmental change. Follow-up is critical for this long-term evaluation. Follow-up phone calls, surveys or even new sessions may be used not only to assess change, but also to support the students/workers in applying their new knowledge, skills, inspiration or social action resulting from training.
Several programmatic components have been identified as important for promoting actual behavioural and worksite changes: union support structures; equal union participation with management; full access to training, information and expert resources for workers and their unions; conducting training within the context of a structure for comprehensive changes; programme development based on worker and workplace needs assessments; use of worker-produced materials; and integration of small group interactive methods with worker empowerment and social action goals.
Conclusion
In this article, the growing need for preparing workers for broad participation in workplace injury and illness prevention efforts has been depicted as well as the critical role of workers as advocates for safety and health. The distinct role of labour empowerment training in responding to these needs and the educational principles and traditions that contribute to a labour empowerment approach to education were addressed. Finally, a step-by-step educational process that is required to achieve the goals of worker involvement and empowerment was described.
This learner-centred approach to education implies a new relationship between occupational safety and health professionals and workers. Learning can no longer be a one-way street with an “expert” imparting knowledge to the “students”. The educational process, instead, is a partnership. It is a dynamic process of communication that taps the skills and knowledge of workers. Learning occurs in all directions: workers learn from the instructors; instructors learn from workers; and workers learn from one another (see figure 2).
Figure 2. Learning is a three-way process.
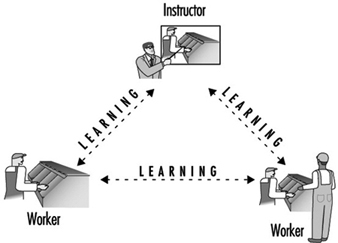
For a successful partnership, workers must be involved in every stage of the educational process, not just in the classroom. Workers must participate in the who, what, where, when and how of training: Who will design and deliver the training? What will be taught? Who will pay for it? Who will have access to it? Where and when will training take place? Whose needs will be met and how will success be measured?
Principles of Training
Training can and will produce positive results if it is based on clearly defined needs specific to the workplace and if it is delivered with a view to those needs and the ways in which adults learn. This is, of course, true for safety and health training as well. The principles of safety and health training are no different from those which apply to any form of industrial training. Indeed, a good case can be made for the integration of skill training along with safety training wherever possible. Safety and health training which fails to produce positive results because it is not based on sound analysis is, at best, a waste of time and money. At worst, such training may result in false confidence, thus increasing the risk of accidents.
Needs Assessment
The first step in safety and health training design is to identify the problems which need to be addressed. This may be done for the entire organization, for a particular location or for a particular job. Alternatively, the analysis of training needs may have a specific focus, for example, compliance with safety and health legislation or the performance of the joint safety and health committee. However, not all problems can be solved by training; in some cases, other action is needed to supplement it. A simple example of this is the case where the problem identified is a low level of compliance with the rule obliging workers to wear personal protective equipment. While part of the problem may be due to the fact that employees do not understand why the equipment is needed or how to use it correctly, it is equally possible that some or all of the problem may be caused by the fact that there is consistent failure to replace broken or missing equipment.
The existence of problems may surface in the form of a high rate of accidents, refusal-to-work situations or government inspectors' orders or citations. However, it is the problems which underlie such outward signs of trouble that need to be clearly identified. A training needs assessment may be defined as the process of identifying problems that are signalled by deficiencies in compliance with standards or external requirements and that can be resolved wholly or partly by training. A systems approach to training needs analysis involves a number of logical steps: problem identification, analysis, identification of training needs, the ranking of needs in order of urgency and the setting of training goals or objectives.
Problem identification
The sorts of problems that lend themselves to solution by means of training include the following:
Those that are identified after accidents have already happened. In this case, problems may be identified through review of accident statistics, accident investigation reports or, more broadly, through the failure to meet organizational goals for safety and health.
Problems that can be anticipated. Dangers can be identified before actual harm is done—for example, hazards can be foreseen when new machinery, substances or processes are introduced into the workplace, where there exist processes that have never been thoroughly analysed or where existing practice conflicts with known safe procedures .
The existence of external requirements. New legal requirements which either impose specific safety and health training duties or other requirements suggesting the need for training are examples of external requirements. The development of new industry codes of practice or national or international standards affecting safety and health are other examples.
Problem analysis
The next step is to analyse the problems so that necessary training may be identified. Problem analysis involves collecting information about the problem so that its causes can be determined. It also requires determining an appropriate standard which should be met. If, for example, the problem identified relates to a lack of effectiveness of the joint safety and health committee, analysis seeks to answer several questions. First, what is the committee supposed to be doing? Second, how well is the committee performing each of its required tasks? (This question requires the analyst to determine appropriate performance standards which should apply.) Third, why is the committee not performing particular tasks effectively?
Determining solutions
Once the problem has been analysed, the next step is to determine suitable solutions. If training is the solution or part of the solution, the particular training needs must be identified. What combination of skills and knowledge is required and by whom?
A critical part of the investigation of training needs is the assessment of the people involved. The purpose of this is threefold: first, people are likely to be more committed to training (and thus more likely to learn) if they have played a part in identifying the needs themselves; second, it is often necessary to assess the current level of required skill and knowledge among the target group of employees (for example, one might investigate whether joint safety and health committee members actually know what it is they are supposed to be doing); third, basic educational levels and literacy and language skills must be known so that appropriate instructional methods are applied. Surveys can be used to assess a number of these variables. If they are used, however, care should be taken to ensure individual confidentiality.
Setting priorities and goals
Once training needs have been clearly identified, the next step is to set priorities and objectives. Consideration must be given to the relative urgency of various training needs, taking into account factors such as the relative severity of consequences should accidents occur, the frequency with which problems are likely to occur, the number of people affected and legal compliance.
Training objectives must be specific because, if they are not, evaluating whether the training has been successful will prove difficult. Specifically defined objectives also help determine appropriate training content and delivery method. Training objectives or goals establish the results that training should achieve. Examples of specific training objectives might include (a) to ensure that every manager and supervisor knows and understands legal safety and health duties and rights applying to themselves and to all workers, (b) to ensure that all welders know and understand the hazards of welding and the required control procedures or (c) to provide fork-lift truck operators with the skill to operate their vehicles safely according to required procedures
Needs Assessment Methods
Methods for analysing training needs depend on the scope of the assessment and on available resources. All or some of the following methods may be used:
- Documentation review. For example, written statements of safe working practices, legal requirements, company policies and procedures, accident statistics and workplace inspection reports can be examined to determine their bearing on training needs.
- Specific analysis. Accident statistics, joint committee minutes, accident investigation reports and job and task hazard analyses may be examined for their specific relevance to the problem in question.
- Interviews and observation. Interviews with representative samples of supervisors, workers and others may be used to assess attitudes and perceived problem areas; observations can be made of representative jobs to assess compliance with safe working practices.
- Surveys. A survey can be used for relatively large groups to gain information about current skills and knowledge levels and about perceived training needs and problem areas as well.
Choosing Appropriate Instructional Methods
Instructional methods include a number of techniques such as lectures, problem-solving exercises, small group discussion and role-playing.The methods chosen must be appropriate to what is being learned (whether knowledge, skills or concepts) and the training objectives. If, for example, the training objective is to impart knowledge about basic safety rules in the workplace, then a short lecture may be appropriate. However, there are different levels of learning in adults. The lowest level of learning is listening to information; the next level is acquiring knowledge; then, developing understanding; and finally, at the highest level, the ability to apply what is learned to different situations. In most training situations, participants will need to learn at more than one level and so a variety of instructional techniques will be required. Instructional methods must also be based upon sound principles of how adults learn best.
Principles of Adult Learning
The way in which adults learn differs from the way children learn in several important respects. Adults approach the task of learning in possession of life experiences and a developed concept of self. The process of learning is an individual experience which takes place within the learner and depends on the learner's willingness to learn, the ability to relate his or her own experiences to what is being learned and the perceived value of what is being learned to the learner. In many cases, adults make a free choice to learn and so, unlike school children, they are voluntary participants. However, when safety and health training is provided in the workplace, workers and managers may be required to attend training sessions, with little room for individual choice. Where this is so, particular attention needs to be paid to involving learners both in the process of identifying training needs and in the design of the programme itself. Addressing the perceived training needs of workers may be as important as the identification of needs in other areas. Above all, adult training involves change. As with any change, acceptance is dependent on the learners’ belief that they have some control over the change and that the change is not perceived as threatening.
Research has identified a number of factors which facilitate learning in adults:
- Motivation. Since learning is an individual experience, adults must want to learn and must perceive the relevance of what they learn to their personal interest.
- Seeing and hearing. Adults tend to learn best when they can see as well as hear what is being taught. This means that lectures should include accompanying visual material such as overhead transparencies or slides.
- Practice. The opportunity to practise what is being taught facilitates learning. When a skill is being taught (for example, the correct fitting of self-contained breathing apparatus) learners should be allowed to exercise it for themselves. Where the objective is applied knowledge, problem-solving exercises can be used. “Experiential” exercises whereby learners actually experience the application of abstract concepts such as teamwork are valuable instructional tools.
- Relationship to practical experience. Learning is facilitated when the training material can easily be related to the practical experience of the learners. This suggests that examples used should, as far as possible, relate to the industry processes familiar to the learners.
- Participation in the learning process. Adults should know from the start what the learning objectives are and be given the opportunity to test the lesson content against these objectives.
- Feedback. Adults need feedback on their own results (how well they are doing) and positive reinforcement.
- Trying out ideas. The opportunity to try out and develop ideas is part of the individual process of internalizing new information and its application. This can be achieved through small peer group discussions.
- Physical environment. The training facility and equipment should be sympathetic to the learners, allowing them, for example, to see visual material and to work effectively in small groups.
Training Implementation
Careful consideration should be given to the selection of trainers, the scheduling of training and pilot testing. In selecting trainers, two equally important abilities must be sought: knowledge of the subject and teaching ability. Not everyone who has the required safety and health knowledge will necessarily have teaching ability. On the whole, it is easier for people to acquire knowledge than it is to acquire teaching ability. In most workplaces, including the shop floor, there will be a number of people who have a natural teaching ability, and they will have the advantage of knowing the workplace and being able to understand practical examples. In small group learning, a “group learning facilitator” may be used in place of a trainer. In this case, the facilitator is learning along with the group but has responsibilities for the process of learning.
The scheduling of training involves several important considerations. For example, it should be arranged at a time convenient for the learners and when interruptions can be minimized. Training can also be packaged in self-contained modules so that it can be spread out over time—perhaps a three hour module once a week could be scheduled. Not only does this approach sometimes cause less interference with production, it also allows time between sessions for learners to try to apply what has been learned.
Every training programme should be pilot tested before initial use. This allows the programme to be tested against training objectives. Pilot testing should involve not only the trainers but a representative sample of the prospective learners as well.
Training Evaluation
The purpose of evaluating training is quite simply to establish whether the training objectives have been met and, if so, whether this has resulted in solving the problem addressed by those objectives. Preparation for training evaluation should begin at the training design stage. In other words, the problem to be addressed by training must be clear, the training objectives must be specific and the status quo prior to training must be known. For example, if the problem to be addressed is poor observance of safe working practices in material handling operations, and training has been designed to address part of this problem by providing information and skills to, say, fork-lift operators, then a successful outcome in this case would be high observance of correct safe working practices.
Evaluation of training can be done at various levels. At the first level, the aim is simply to assess student reactions to the training programme. Did they like the programme, the instructor and the course material, were they bored, did they feel that they had learned something? This approach may be useful in assessing whether or not the programme was perceived to be of value by the students. Such evaluations are most usefully conducted through an attitude survey and should not generally be administered by the course instructor. Participants are unlikely to provide candid answers at this point even if the questionnaires are anonymous. As an aid to this type of evaluation, students can be allowed to test themselves on the training content.
The next level of evaluation is the assessment of whether or not the learning objectives have been met. Learning objectives are related to the content of the training and they define what the student should be able to do or know when training is completed. Learning objectives are usually developed for each part of the course content and are shared with students so that they know what they should expect to learn. Evaluation at this level is designed to assess whether or not students have learned what is defined in the learning objectives. This can be done by testing participants at the end of the course. Knowledge, concepts and abstract skills can be assessed in written tests whereas practical skills can be assessed by direct observation of students demonstrating the skill. Where this level of evaluation is used, it is absolutely necessary to have prior knowledge of the knowledge or skill baseline of the students before training begins.
The third level of evaluation is the assessment of whether or not the knowledge and skills learned in the training are actually being applied on the job. Such assessment can be made through direct observation at specified intervals of time following training. Evaluation of application on the day following training may produce a result quite different from that based on an evaluation some three months later. It is important to note, however, that if the evaluation shows a lack of application after three months, it may not be the training itself which is defective; it may be due to a lack of reinforcement in the workplace itself.
Finally, the highest level of evaluation is the determination of whether or not the problem addressed by the training has been resolved. If the problem identified was a high rate of musculoskeletal injuries in the shipping and receiving area, is there evidence of the desired drop in the injury rate? Here again, timing is important. In this case, it may take time for the training to become effective. The rate may not drop for a number of months because such injuries are often cumulative; and so the rate for some time may reflect conditions prior to training. Furthermore, the training may result in greater awareness of the problem leading to increased reporting soon after training.
Ideally, all four levels of training evaluation should be built into the training design and implementation. However, if only one level is used, its limitations should be clearly understood by all concerned.
Where training is designed and provided by an external agency, the organization can and should nevertheless evaluate its potential usefulness by applying criteria based on the principles outlined in this article.
Training Reinforcement
No matter how successful training is in meeting objectives, its effect will decline with time if reinforcement is not provided in the workplace on a regular and consistent basis. Such reinforcement should be the routine responsibility of supervisors, managers and joint safety and health committees. It can be provided through regular monitoring of performance on the job, recognition of proper performance and routine reminders through the use of short meetings, notices and posters.
Labor Relations And Human Resources Management: An Overview
Labour or Industrial Relations
The term labour relations, also known as industrial relations, refers to the system in which employers, workers and their representatives and, directly or indirectly, the government interact to set the ground rules for the governance of work relationships. It also describes a field of study dedicated to examining such relationships. The field is an outgrowth of the industrial revolution, whose excesses led to the emergence of trade unions to represent workers and to the development of collective labour relations. A labour or industrial relations system reflects the interaction between the main actors in it: the state, the employer (or employers or an employers’ association), trade unions and employees (who may participate or not in unions and other bodies affording workers’ representation). The phrases “labour relations” and “industrial relations” are also used in connection with various forms of workers’ participation; they can also encompass individual employment relationships between an employer and a worker under a written or implied contract of employment, although these are usually referred to as “employment relations”. There is considerable variation in the use of the terms, partly reflecting the evolving nature of the field over time and place. There is general agreement, however, that the field embraces collective bargaining, various forms of workers’ participation (such as works councils and joint health and safety committees) and mechanisms for resolving collective and individual disputes. The wide variety of labour relations systems throughout the world has meant that comparative studies and identification of types are accompanied by caveats about the limitations of over-generalization and false analogies. Traditionally, four distinct types of workplace governance have been described: dictatorial, paternalistic, institutional and worker-participative; this chapter examines primarily the latter two types.
Both private and public interests are at stake in any labour relations system. The state is an actor in the system as well, although its role varies from active to passive in different countries. The nature of the relationships among organized labour, employers and the government with respect to health and safety are indicative of the overall status of industrial relations in a country or an industry and the obverse is equally the case. An underdeveloped labour relations system tends to be authoritarian, with rules dictated by an employer without direct or indirect employee involvement except at the point of accepting employment on the terms offered.
A labour relations system incorporates both societal values (e.g., freedom of association, a sense of group solidarity, search for maximized profits) and techniques (e.g., methods of negotiation, work organization, consultation and dispute resolution). Traditionally, labour relations systems have been categorized along national lines, but the validity of this is waning in the face of increasingly varied practices within countries and the rise of a more global economy driven by international competition. Some countries have been characterized as having cooperative labour relations models (e.g., Belgium, Germany), whereas others are known as being conflictual (e.g., Bangladesh, Canada, United States). Different systems have also been distinguished on the basis of having centralized collective bargaining (e.g., those in Nordic countries, although there is a move away from this, as illustrated by Sweden), bargaining at the sectoral or industrial level (e.g., Germany), or bargaining at the enterprise or plant level (e.g., Japan, the United States). In countries having moved from planned to free-market economies, labour relations systems are in transition. There is also increasing analytical work being done on the typologies of individual employment relationships as indic- ators of types of labour relations systems.
Even the more classic portrayals of labour relations systems are not by any means static characterizations, since any such system changes to meet new circumstances, whether economic or political. The globalization of the market economy, the weakening of the state as an effective force and the ebbing of trade union power in many industrialized countries pose serious challenges to traditional labour relations systems. Technological development has brought changes in the content and organization of work that also have a crucial impact on the extent to which collective labour relations can develop and the direction they take. Employees’ traditionally shared work schedule and common workplace have increasingly given way to more varied working hours and to the performance of work at varied locations, including home, with less direct employer supervision. What have been termed “atypical” employment relationships are becoming less so, as the contingent workforce continues to expand. This in turn places pressure on established labour relations systems.
Newer forms of employee representation and participation are adding an additional dimension to the labour relations picture in a number of countries. A labour relations system sets the formal or informal ground rules for determining the nature of collective industrial relations as well as the framework for individual employment relationships between a worker and his or her employer. Complicating the scene at the management end are additional players such as temporary employment agencies, labour contractors and job contractors who may have responsibilities towards workers without having control over the physical environment in which the work is carried out or the opportunity to provide safety training. In addition, public sector and private sector employers are governed by separate legislation in most countries, with the rights and protections of employees in these two sectors often differing significantly. Moreover, the private sector is influenced by forces of international competition that do not directly touch public-sector labour relations.
Finally, neoliberal ideology favouring the conclusion of indi-vidualized employment contracts to the detriment of collectively bargained arrangements poses another threat to traditional labour relations systems. Those systems have developed as a result of the emergence of collective representation for workers, based on past experience that an individual worker’s power is weak when compared to that of the employer. Abandoning all collective representation would risk returning to a nineteenth century concept in which acceptance of hazardous work was largely regarded as a matter of individual free choice. The increasingly globalized economy, the accelerated pace of technological change and the resultant call for greater flexibility on the part of industrial relations institutions, however, pose new challenges for their survival and prosperity. Depending upon their existing traditions and institutions, the parties involved in a labour relations system may react quite differently to the same pressures, just as management may choose a cost-based or a value-added strategy for confronting increased competition (Locke, Kochan and Piore, 1995). The extent to which workers’ participation and/or collective bargaining are regular features of a labour relations system will most certainly have an impact on how management confronts health and safety problems.
Moreover, there is another constant: the economic dependence of an individual worker on an employer remains the underlying fact of their relationship–one that has serious potential consequences when it comes to safety and health. The employer is seen as having a general duty to provide a safe and healthful workplace and to train and equip workers to do their jobs safely. The worker has a reciprocal duty to follow safety and health instructions and to refrain from harming himself/herself or others while at work. Failure to live up to these or other duties can lead to disputes, which depend on the labour relations system for their resolution. Dispute resolution mechanisms include rules governing not only work stoppages (strikes, slowdowns or go-slows, work to rule, etc.) and lockouts, but the discipline and dismissal of employees as well. Additionally, in many countries employers are required to participate in various institutions dealing with safety and health, perform safety and health monitoring, report on-the-job accidents and diseases and, indirectly, to compensate workers who are found to be suffering from an occupational injury or disease.
Human Resources Management
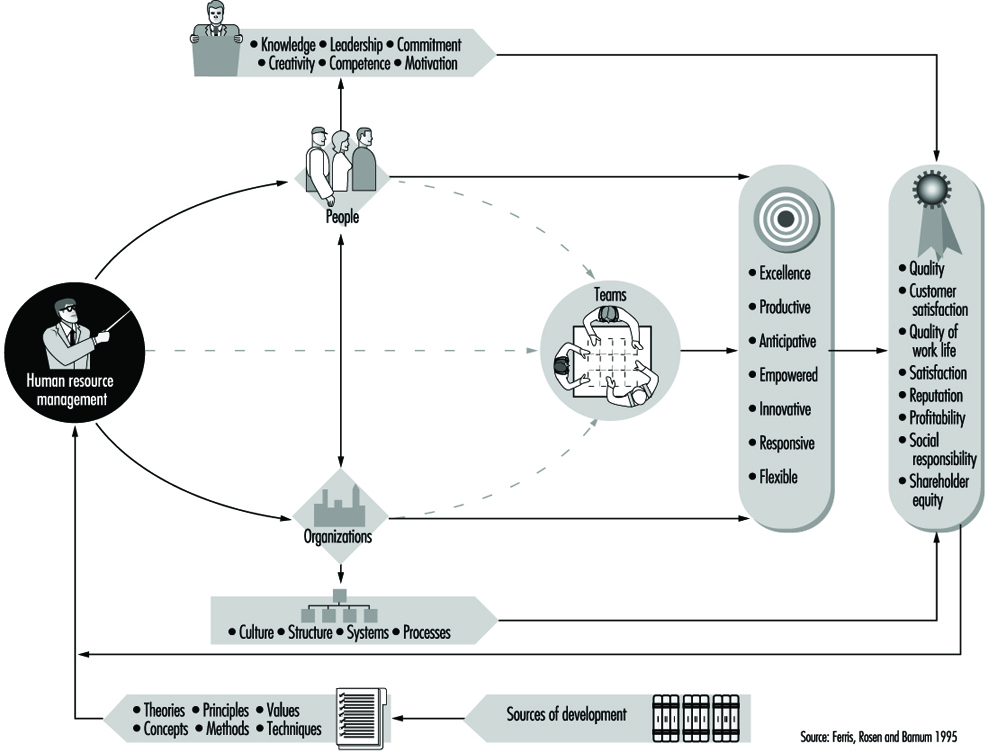
Human resources management has been defined as “the science and the practice that deals with the nature of the employment relationship and all of the decisions, actions and issues that relate to that relationship” (Ferris, Rosen and Barnum 1995; see figure 1). It encapsulates employer-formulated policies and practices that see the utilization and management of employees as a business resource in the context of a firm’s overall strategy to enhance productivity and competitiveness. It is a term most often used to describe an employer’s approach to personnel administration that emphasizes employee involvement, normally but not always in a union-free setting, with the goal of motivating workers to enhance their productivity. The field was formed from a merger of scientific management theories, welfare work and industrial psychology around the time of the First World War and has undergone considerable evolution since. Today, it stresses work organization techniques, recruitment and selection, performance appraisal, training, upgrading of skills and career development, along with direct employee participation and communication. Human resources management has been put forth as an alternative to “Fordism”, the traditional assembly-line type of production in which engineers are responsible for work organization and workers’ assigned tasks are divided up and narrowly circumscribed. Common forms of employee involvement include suggestion schemes, attitude surveys, job enrichment schemes, teamworking and similar forms of empowerment schemes, quality of working-life programmes, quality circles and task forces. Another feature of human resources management may be linking pay, individually or collectively, to performance. It is noteworthy that one of the three objectives of occupational health has been identified by the Joint ILO/WHO Committee on Occupational Health as “development of work organizations and working cultures in a direction which supports health and safety at work and in doing so also promotes a positive social climate and smooth operation and may enhance productivity of the undertakings...” (ILO 1995b). This is known as developing a “safety culture.”
Figure 1. The role of human resources management in adding value to people and to organizations
The example of a safety performance management programme illustrates some human resource management theories in the context of occupational safety and health. As described by Reber, Wallin and Duhon (1993), this approach has had considerable success in reducing lost time on account of accidents. It relies on specifying safe and unsafe behaviours, teaching employees how to recognize safe behaviour and motivating them to follow the safety rules with goal setting and feedback. The programme relies heavily on a training technique whereby employees are shown safe, correct methods via videotapes or live models. They then have a chance to practice new behaviours and are provided with frequent performance feedback. In addition, some companies offer tangible prizes and rewards for engaging in safe behaviour (rather than simply for having fewer accidents). Employee consultation is an important feature of the programme as well.
The implications of human resources management for industrial relations practices remain a source of some controversy. This is particularly the case for types of workers’ participation schemes that are perceived by trade unions as a threat. In some instances human resources management strategies are pursued alongside collective bargaining; in other cases the human resources management approach seeks to supplant or prevent the activities of independent organizations of workers in defence of their interests. Proponents of human resources management maintain that since the 1970s, the personnel management side of human resources management has evolved from being a maintenance function, secondary to the industrial relations function, to being one of critical importance to the effectiveness of an organization (Ferris, Rosen and Barnum 1995). Since human resources management is a tool for management to employ as part of its personnel policy rather than a relationship between an employer and workers’ chosen representatives, it is not the focus of this chapter.
The articles which follow describe the main parties in a labour relations system and the basic principles underpinning their interaction: rights to freedom of association and representation. A natural corollary to freedom of association is the right to engage in collective bargaining, a phenomenon which must be distinguished from consultative and non-union worker participation arrangements. Collective bargaining takes place as negotiations between representatives chosen by the workers and those acting on behalf of the employer; it leads to a mutually accepted, binding agreement that can cover a wide range of subjects. Other forms of workers’ participation, national-level consultative bodies, works councils and enterprise-level health and safety representatives are also important features of some labour relations systems and are thus examined in this chapter. Consultation can take various forms and occur at different levels, with national-, regional- and/or industrial- and enterprise-level arrangements. Worker representatives in consultative bodies may or may not have been selected by the workers and there is no obligation for the state or the employer to follow the wishes of those representatives or to abide by the results of the consultative process. In some countries, collective bargaining and consultative arrangements exist side by side and, to work properly, must be carefully intermeshed. For both, rights to information about health and safety and training are crucial. Finally, this chapter takes into account that in any labour relations system, disputes may arise, whether they are individual or collective. Safety and health issues can lead to labour relations strife, producing work stoppages. The chapter thus concludes with descriptions of how labour relations disputes are resolved, including by arbitration, mediation or resort to the regular or labour courts, preceded by a discussion of the role of the labour inspectorate in the context of labour relations.
The Actors in the Labour Relations System
Classically, three actors have been identified as parties to the labour relations system: the state, employers and workers’ representatives. To this picture must now be added the forces that transcend these categories: regional and other multilateral economic integration arrangements among states and multinational corporations as employers which do not have a national identity but which also can be seen as labour market institutions. Since the impact of these phenomena on labour relations remains unclear in many respects, however, discussion will focus on the more classic actors despite this caveat of the limitation of such an analysis in an increasingly global community. In addition, greater emphasis is needed on analysing the role of the individual employment relationship in labour relations systems and on the impact of the emerging alternative forms of work.
The State
The state always has at least an indirect effect on all labour relations. As the source of legislation, the state exerts an inevitable influence on the emergence and development of a labour relations system. Laws can hinder or foster, directly or indirectly, the establishment of organizations representing workers and employers. Legislation also sets a minimum level of worker protection and lays down “the rules of the game”. To take an example, it can provide lesser or greater protection for a worker who refuses to perform work he or she reasonably considers to be too hazardous, or for one who acts as a health and safety representative.
Through the development of its labour administration, the state also has an impact on how a labour relations system may function. If effective enforcement of the law is afforded through a labour inspectorate, collective bargaining can pick up where the law leaves off. If, however, the state infrastructure for having rights vindicated or for assisting in the resolution of disputes that emerge between employers and workers is weak, they will be left more to their own devices to develop alternative institutions or arrangements.
The extent to which the state has built up a well-functioning court or other dispute resolution system may also have an influence on the course of labour relations. The ease with which workers, employers and their respective organizations may enforce their legal rights can be as important as the rights themselves. Thus the decision by a government to set up special tribunals or administrative bodies to deal with labour disputes and/or disagreements over individual employment problems can be an expression of the priority given to such issues in that society.
In many countries, the state has a direct role to play in labour relations. In countries that do not respect freedom of association principles, this may involve outright control of employers’ and workers’ organizations or interference with their activities. The state may attempt to invalidate collective bargaining agreements that it perceives as interfering with its economic policy goals. Generally speaking, however, the role of the state in industrialized countries has tended to promote orderly industrial relations by providing the necessary legislative framework, including minimum levels of worker protection and offering parties information, advice and dispute settlement services. This could take the form of mere toleration of labour relations institutions and the actors in them; it could move beyond to actively encourage such institutions. In a few countries, the state is a more active participant in the industrial relations system, which includes national level tripartite negotiations. For decades in Belgium and more recently in Ireland, for instance, government representatives have been sitting down alongside those from employer and trade union circles to hammer out a national level agreement or pact on a wide range of labour and social issues. Tripartite machinery to fix minimum wages has long been a feature of labour relations in Argentina and Mexico, for example. The interest of the state in doing so derives from its desires to move the national economy in a certain direction and to maintain social peace for the duration of the pact; such bipartite or tripartite arrangements create what has been called a “social dialogue”, as it has developed in Australia (until 1994), Austria, Belgium, Ireland and the Netherlands, for instance. The pros and cons of what have been termed “corporatist” or “neocorporatist” approaches to labour relations have been extensively debated over the years. With its tripartite structure, the International Labour Organization has long been a proponent of strong tripartite cooperation in which the “social partners” play a significant role in shaping government policy on a wide range of issues.
In some countries, the very idea of the state becoming involved as a negotiator in private sector bargaining is unthinkable, as in Germany or the United States. In such systems, the role of the state is, aside from its legislative function, generally restricted to providing assistance to the parties in reaching an agreement, such as in offering voluntary mediation services. Whether active or passive, however, the state is a constant partner in any labour relations system. In addition, where the state is itself the employer, or an enterprise is publicly owned, it is of course directly involved in labour relations with the employees and their representatives. In this context, the state is motivated by its role as provider of public services and/or as an economic actor.
Finally, the impact of regional economic integration arrangements on state policy is also felt in the labour relations field. Within the European Union, practice in member countries has changed to reflect directives dealing with consultation of workers and their representatives, including those on health and safety matters in particular. Multilateral trade agreements, such as the labour side agreement to the North American Free Trade Agreement (Canada, Mexico, United States) or the agreements implementing the Mercosur Common Market (Argentina, Brazil, Chile, Paraguay, thought soon to be joined by Bolivia and Chile) also sometimes contain workers’ rights provisions or mechanisms that over time may have an indirect impact on labour relations systems of the participating states.
Employers
Employers–that is, providers of work–are usually differentiated in industrial relations systems depending upon whether they are in the private or the public sector. Historically, trade unionism and collective bargaining developed first in the private sector, but in recent years these phenomena have spread to many public sector settings as well. The position of state-owned enterprises—which in any event are dwindling in number around the world—as employers, varies depending upon the country. (They still play a key role in China, India, Viet Nam and in many African countries.) In Eastern and Central Europe, one of the major challenges of the post-Communist era has been the establishment of independent organizations of employers.
International Employers’ Organizations
Based in Geneva, Switzerland, the International Organization of Employers (IOE) in 1996 grouped 118 central national organizations of employers in 116 countries. The exact form of each member organization may differ from country to country, but in order to qualify for membership in the IOE an employers’ organization must meet certain conditions: it must be the most representative organization of employers - exclusively of employers - in the country; it must be voluntary and independent, free from outside interference; and it must stand for and defend the principles of free enterprise. Members include employer federations and confederations, chambers of commerce and industry, councils and associations. Regional or sectoral organizations cannot become members; nor can enterprises, regardless of their size or importance, affiliate themselves directly with the IOE - a factor that has served to ensure that its voice is representative of the employer community at large, and not of the particular interests of individual enterprises or sectors.
The IOE’s main activity, however, is to organize employers whenever they have to deal with social and labour matters at the global level. In practice, most of this takes place in the ILO, which has responsibility for these questions in the United Nations system. The IOE also has Category I consultative status with the Economic and Social Council of the United Nations, where it intervenes whenever matters of interest or consequence to employers arise.
The IOE is one of only two organizations that the employer community has set up to represent the interests of enterprise globally. The other is the International Chamber of Commerce, with its headquarters in Paris, which concerns itself principally with economic matters. While structurally quite different, the two organizations complement each other. They cooperate on the basis of an agreement which defines their areas of responsibility as well as through good personal relations between their representatives and, to a degree, on a common membership base. Many subjects cut across their mandates, of course, but are dealt with pragmatically without friction. On certain issues, such as multinational enterprises, the two organizations even act in unison.
by Chapter Editor (excerpted from: ILO 1994)
In the private sector, the situation has been summed up as follows:
Employers have common interests to defend and precise causes to advance. In organizing themselves, they pursue several aims which in turn determine the character of their organizations. These can be chambers of commerce, economic federations and employers’ organizations (for social and labour matters) ... Where issues centre essentially on social matters and industrial relations, including collective bargaining, occupational health and safety, human resource development, labour law and wages, the desire for co-ordinated action has led to the creation of employers’ organizations, which are always voluntary in nature ... (ILO 1994a).
Some employers’ organizations were initially established in response to pressure from the trade unions to negotiate, but others may be traced to medieval guilds or other groups founded to defend particular market interests. Employers’ organizations have been described as formal groups of employers set up to defend, represent and advise affiliated employers and to strengthen their position in society at large with respect to labour matters as distinct from economic matters ... Unlike trade unions, which are composed of individual persons, employers’ organizations are composed of enterprises (Oechslin 1995).
As identified by Oechslin, there tend to be three main functions (to some extent overlapping) common to all employers’ organizations: defence and promotion of their members’ interests, representation in the political structure and provision of services to their members. The first function is reflected largely in lobbying government to adopt policies that are friendly to employers’ interests and in influencing public opinion, chiefly through media campaigns. The representative function may occur in the political structure or in industrial relations institutions. Political representation is found in systems where consultation of interested economic groups is foreseen by law (e.g., Switzerland), where economic and social councils provide for employer representation (e.g., France, French-speaking African countries and the Netherlands) and where there is participation in tripartite forums such as the International Labour Conference and other aspects of ILO activity. In addition, employers’ organizations can exercise considerable influence at the regional level (especially within the European Union).
The way in which the representative function in the industrial relations system occurs depends very much on the level at which collective bargaining takes place in a particular country. This factor also largely determines the structure of an employers’ organization. If bargaining is centralized at the national level, the employers’ organization will reflect that in its internal structure and operations (central economic and statistical data bank, creation of a mutual strike insurance system, strong sense of member discipline, etc.). Even in countries where bargaining takes place at the enterprise level (such as Japan or the United States), the employers’ organization can offer its members information, guidelines and advice. Bargaining that takes place at the industrial level (as in Germany, where, however, some employers have recently broken ranks with their associations) or at multiple levels (as in France or Italy) of course also influences the structure of employers’ organizations.
As for the third function, Oechslin notes, “it is not always easy to draw a line between activities supporting the functions described above and those undertaken for the members in their interest” (p. 42). Research is the prime example, since it can be used for multiple purposes. Safety and health is an area in which data and information can be usefully shared by employers across sectors. Often, new concepts or reactions to novel developments in the world of work have been the product of broad reflection within employers’ organizations. These groups also provide training to members on a wide range of management issues and have undertaken social affairs action, such as in the development of workers’ housing or support for community activities. In some countries, employers’ organizations provide assistance to their members in labour court cases.
The structure of employers’ organizations will depend not only on the level at which bargaining is done, but also on the country’s size, political system and sometimes religious traditions. In developing countries, the main challenge has been the integration of a very heterogeneous membership that may include small and medium-sized businesses, state enterprises and subsidiaries of multinational corporations. The strength of an employers’ organi-zation is reflected in the resources its members are willing to devote to it, whether in the form of dues and contributions or in terms of their expertise and time.
The size of an enterprise is a major determinant in its approach to labour relations, with the employer of a small workforce being more likely to rely on informal means for dealing with its workers. Small and medium-sized enterprises, which are variously defined, sometimes fall under the threshold for legally mandated workers’ participation schemes. Where collective bargaining occurs at the enterprise level, it is much more likely to exist in large firms; where it takes place at the industry or national level, it is more likely to have an effect in areas where large firms have historically dominated the private sector market.
As interest organizations, employers’ organizations—like trade unions—have their own problems in the areas of leadership, internal decision-making and member participation. Since employers tend to be individualists, however, the challenge of marshalling discipline among the membership is even greater for employers’ organizations. As van Waarden notes (1995), “employers’ associations generally have high density ratios ... However, employers find it a much greater sacrifice to comply with the decisions and regulations of their associations, as these reduce their much cherished freedom of enterprise.” Trends in the structure of employers’ organizations very much reflect those of the labour market– towards or against centralization, in favour of or opposed to regulation of competition. Van Waarden continues: “even if the pressure to become more flexible in the ‘post-Fordist’ era continues, it does not necessarily make employers’ associations redundant or less influential ... [They] would still play an important role, namely as a forum for the coordination of labour market policies behind the scenes and as an advisor for firms or branch associations engaged in collective bargaining” (ibid., p. 104). They can also perform a solidarity function; through employers’ associations, small employers may have access to legal or advisory services they otherwise could not afford.
Public employers have come to see themselves as such only relatively recently. Initially, the government took the position that a worker’s involvement in trade union activity was incompatible with service to the sovereign state. They later resisted calls to engage in collective bargaining with the argument that the legislature, not the public administration, was the paymaster and that it was thus impossible for the administration to enter into an agreement. These arguments, however, did not prevent (often unlawful) public sector strikes in many countries and they have fallen by the wayside. In 1978, the International Labour Conference adopted the Labour Relations (Public Service) Convention (No. 151) and Recommendation (No. 159) on public employees’ right to organize and on procedures for determining their terms and conditions of employment. Collective bargaining in the public sector is now a way of life in many developed countries (e.g., Australia, France, United Kingdom) as well as in some developing countries (e.g., many francophone African countries and many countries in Latin America).
The level of employer representation in the public sector depends largely upon the political system of the country. In some this is a centralized function (as in France) whereas in others it reflects the various divisions of government (as in the United States, where bargaining can take place at the federal, state and municipal levels). Germany presents an interesting case in which the thousands of local communities have banded together to have a single bargaining agent deal with the unions in the public sector throughout the country.
Because public sector employers are already part of the state, they do not fall under laws requiring registration of employers’ organizations. The designation of the bargaining agent in the public sector varies considerably by country; it may be the Public Service Commission, the Ministry of Labour, the Ministry of Finance or another entity altogether. The positions taken by a public employer in dealing with employees in this sector tend to follow the political orientation of the ruling political party. This may range from taking a particular stance in bargaining to a flat-out denial of the right of public employees to organize into trade unions. However, while as an employer the public service is shrinking in many countries, there is an increasing readiness on its part to engage in bargaining and consultations with employee representatives.
International Labour Federations
The international labour movement on a global, as opposed to a regional or national level, consists of international associations of national federations of labour unions. There are currently three such internationals, reflecting different ideological tendencies: the International Confederation of Free Trade Unions (ICFTU), the World Federation of Trade Unions (WFTU) and the relatively small, originally Christian, World Congress of Labour (WCL). The ICFTU is the largest, with 174 affiliated unions from 124 countries in 1995, representing 116 million trade union members. These groups lobby intergovernmental organizations on overall economic and social policy and press for worldwide protection of basic trade union rights. They can be thought of as the political force behind the international labour movement.
The industrial force of the international labour movement lies in the international associations of specific labour unions, usually drawn from one trade, industry or economic sector. Known as International Trade Secretariats (ITSs) or Trade Union Internationals (TUIs), they may be independent, affiliated to, or controlled by the internationals. Coverage has traditionally been by sector, but also in some cases is by employee category (such as white-collar workers), or by employer (public or private). For example, in 1995 there were 13 operative ITSs aligned with the ICFTU, distributed as follows: building and woodworking; chemical and mining, energy; commercial, clerical, professional and technical; education; entertainment; food, agriculture, restaurant and catering; graphic arts; journalism; metalworking; postal and telecommunications; public service; textile, garment and leather work; transport. The ITSs concentrate mainly on industry-specific issues, such as industrial disputes and pay rates, but also the application of health and safety provisions in a specific sector. They provide information, education, training and other services to affiliated unions. They also help coordinate international solidarity between unions in different countries, and represent the interests of workers in various international and regional forums.
Such action is illustrated by the international trade union response to the incident at Bhopal, India, involving the leak of methyl isocyanate, which claimed thousands of victims on 3 December 1984. At the request of their Indian national trade union affiliates, the ICFTU and the International Federation of Chemical, Energy, Mine and General Workers’ Unions (ICEM) sent a mission to Bhopal to study the causes and effects of the gas leak. The report contained recommendations for preventing similar disasters and endorsed a list of safety principles; this report has been used by trade unionists in both industrialized and developing countries as a basis of programmes for improving health and safety at work.
Source: Rice 1995.
Trade Unions
The classic definition of a trade union is “a continuous association of wage earners for the purpose of maintaining or improving the conditions of their employment” (Webb and Webb 1920). The origins of trade unions go back as far as the first attempts to organize collective action at the beginning of the industrial revolution. In the modern sense, however, trade unions arose in the later part of the nineteenth century, when governments first began to concede the unions’ legal right to exist (previously, they had been seen as illegal combinations interfering with freedom of commerce, or as outlawed political groups). Trade unions reflect the conviction that only by banding together can workers improve their situation. Trade union rights were born out of economic and political struggle which saw short-term individual sacrifice in the cause of longer-term collective gain. They have often played an important role in national politics and have influenced developments in the world of work at the regional and international levels. Having suffered membership losses, however, in recent years in a number of countries (in North America and some parts of Europe), their role is under challenge in many quarters (see figure 2). The pattern is mixed with areas of membership growth in the public service in many countries around the world and with a new lease on life in places where trade unions were previously non-existent or active only under severe restrictions (e.g., Korea, the Philippines, some countries of Central and Eastern Europe). The flourishing of democratic institutions goes hand in hand with the exercise of trade union freedoms, as the cases of Chile and Poland in the 1980s and 1990s best illustrate. A process of internal reform and reorientation to attract greater and more diverse membership, particularly more women, can also be seen within trade union circles in a number of countries. Only time will tell if these and other factors will be sufficient to deflect the counterweighing tendencies towards the “de-collectivization”, also referred to as “atomization”, of labour relations that has accompanied increased economic globalization and ideological individualism.
Figure 2. Membership rates in trade unions, 1980-1990

In contemporary industrial relations systems, the functions fulfilled by trade unions are, like employers’ organizations, basically the following: defence and promotion of the members’ interests; political representation; and provision of services to members. The flip side of trade unions’ representative function is their control function: their legitimacy depends in part upon the ability to exert discipline over the membership, as for example in calling or ending a strike. The trade unions’ constant challenge is to increase their density, that is, the number of members as a percentage of the formal sector workforce. The members of trade unions are individuals; their dues, called contributions in some systems, support the union’s activities. (Trade unions financed by employers, called “company unions”, or by governments as in formerly Communist countries, are not considered here, since only independent organizations of workers are true trade unions.) Affiliation is generally a matter of an individual’s voluntary decision, although some unions that have been able to win closed shop or union security arrangements are considered to be the representatives of all workers covered by a particular collective bargaining agreement (i.e., in countries where trade unions are recognized as representatives of workers in a circumscribed bargaining unit). Trade unions may be affiliated to umbrella organizations at the industrial, national, regional and international levels.
Trade unions are structured along various lines: by craft or occupation, by branch of industry, by whether they group white- or blue-collar workers and sometimes even by enterprise. There are also general unions, which include workers from various occupations and industries. Even in countries where mergers of industrial unions and general unions are the trend, the situation of agricultural or rural workers has often favoured the development of special structures for that sector. On top of this breakdown there is often a territorial division, with regional and sometimes local subunits, within a union. In some countries there have been splits in the labour movement around ideological (party politics) and even religious lines which then come to be reflected in trade union structure and membership. Public sector employees tend to be represented by unions separate from those representing employees in the private sector, although there are exceptions to this as well.
The legal status of a trade union may be that of any other association, or it may be subject to special rules. A great number of countries require trade unions to register and to divulge certain basic information to the authorities (name, address, identity of officials, etc.). In some countries this goes beyond mere record-keeping to interference; in extreme cases of disregard for freedom of association principles, trade unions will need government authorization to operate. As representatives of workers, trade unions are empowered to enter into engagements on their behalf. Some countries (such as the United States) require employer recognition of trade unions as an initial prerequisite to engaging in collective bargaining.
Trade union density varies widely between and within countries. In some countries in Western Europe, for instance, it is very high in the public sector but tends to be low in the private sector and especially in its white-collar employment. The figures for blue-collar employment in that region are mixed, from a high in Austria and Sweden to a low in France, where, however, trade union political power far exceeds what membership figures would suggest. There is some positive correlation between centralization of bargaining and trade union density, but exceptions to this also exist.
As voluntary associations, trade unions draw up their own rules, usually in the form of a constitution and by-laws. In democratic trade union structures, members select trade union officers either by direct vote or through delegates to a general conference. Internal union government in a small, highly decentralized union of workers in a particular occupational group is likely to differ significantly from that found in a large, centralized general or industrial union. There are tasks to allocate among union officers, between paid and unpaid union representatives and coordination work to be done. The financial resources available to a union will also vary depending upon its size and the ease with which it can collect dues. Institution of a dues check-off system (whereby dues are deducted from a worker’s wages and paid directly to the union) alleviates this task greatly. In most of Central and Eastern Europe, trade unions that were dominated and funded by the state are being transformed and/or joined by new independent organizations; all are struggling to find a place and operate successfully in the new economic structure. Extremely low wages (and thus dues) there and in developing countries with government-supported unions make it difficult to build a strong independent union movement.
In addition to the important function of collective bargaining, one of the main activities of trade unions in many countries is their political work. This may take the form of direct representation, with trade unions being given reserved seats in some parliaments (e.g., Senegal) and on tripartite bodies that have a role in determining national economic and social policy (e.g., Austria, France, the Netherlands), or on tripartite advisory bodies in the fields of labour and social affairs (e.g., in many Latin American and some African and Asian countries). In the European Union, trade union federations have had an important impact on the development of social policy. More typically, trade unions have an influence through the exercise of power (backed up by a threat of industrial action) and lobbying political decision makers at the national level. It is certainly true that trade unions have successfully fought for greater legislative protection for all workers around the world; some believe that this has been a bittersweet victory, in the long run undermining their own justification to exist. The objectives and issues of union political action have often extended well beyond narrower interests; a prime example of this was the struggle against apartheid within South Africa and the international solidarity expressed by unions around the world in words and in deeds (e.g., organizing dockworker boycotts of imported South African coal). Whether trade union political activity is on the offence or the defence will of course depend largely on whether the government in power tends to be pro- or anti-labour. It will also depend upon the union’s relationship to political parties; some unions, particularly in Africa, were part of their countries’ struggles for independence and maintain very close ties with ruling political parties. In other countries there is a traditional interdependence between the labour movement and a political party (e.g., Australia, United Kingdom), whereas in others alliances may shift over time. In any event, the power of trade unions often exceeds what would be expected from their numerical strength, particularly where they represent workers in a key economic or public service sector, such as transport or mining.
Aside from trade unions, many other types of workers’ participation have sprung up to provide indirect or direct representation of employees. In some instances they exist alongside trade unions; in others they are the only type of participation available to workers. The functions and powers of workers’ representatives that exist under such arrangements are described in the article “Forms of workers’ participation’’.
The third type of function of trade unions, providing services to members, focuses first and foremost on the workplace. A shop steward at the enterprise level is there to ensure that workers’ rights under the collective bargaining agreement and the law are being respected–and, if not, to take action. The union officer’s job is to defend the interests of workers vis-à-vis management, thereby legitimizing his or her own representative role. This may involve taking up an individual grievance over discipline or dismissal, or cooperating with management on a joint health and safety committee. Outside the workplace, many unions provide other types of benefit, such as preferential access to credit and participation in welfare schemes. The union hall can also serve as a centre for cultural events or even large family ceremonies. The range of services a union can offer to its members is vast and reflects the creativity and resources of the union itself as well as the cultural milieu in which it operates.
As Visser observes:
The power of trade unions depends on various internal and external factors. We can distinguish between organizational power (how many internal sources of power can unions mobilize?), institutional power (which external sources of support can unions depend on?) and economic power (which market forces play into the hands of unions?) (Visser in van Ruysseveldt et al. 1995).
Among the factors he identifies for a strong trade union structure are the mobilization of a large, stable, dues-paying and well-trained membership (to this could be added a membership that reflects the composition of the labour market), avoidance of organizational fragmentation and political or ideological rifts and development of an organizational structure that provides a presence at the company level while having central control of funds and decision making. Whether such a model for success, which to date has been national in character, can evolve in the face of an increasingly internationalized economy, is the great challenge facing trade unions at this juncture.
Introduction and Overview
A 1981 study of worker safety and health training in the industrial nations begins by quoting the French writer Victor Hugo: “No cause can succeed without first making education its ally” (Heath 1981). This observation surely still applies to occupational safety and health in the late twentieth century, and is relevant to organization personnel at all levels.
As the workplace becomes increasingly complex, new demands have arisen for greater understanding of the causes and means of prevention of accidents, injuries and illnesses. Government officials, academics, management and labour all have important roles to play in conducting the research that furthers this understanding. The critical next step is the effective transmission of this information to workers, supervisors, managers, government inspectors and safety and health professionals. Although education for occupational physicians and hygienists differs in many respects from the training of workers on the shop floor, there are also common principles that apply to all.
National education and training policies and practices will of course vary according to the economic, political, social, cultural and technological background of the country. In general, industrially advanced nations have proportionally more specialized occupational safety and health practitioners at their disposal than do the developing nations, and more sophisticated education and training programmes are available to these trained workers. More rural and less industrialized nations tend to rely more on “primary health care workers”, who may be worker representatives in factories or fields or health personnel in district health centres. Clearly, training needs and available resources will vary greatly in these situations. However, they all have in common the need for trained practitioners.
This article provides an overview of the most significant issues concerning education and training, including target audiences and their needs, the format and content of effective training and important current trends in the field.
Target Audiences
In 1981, the Joint ILO/WHO Committee on Occupational Health identified the three levels of education required in occupational health, safety and ergonomics as (1) awareness, (2) training for specific needs and (3) specialization. These components are not separate, but rather are part of a continuum; any person may require information on all three levels. The main target groups for basic awareness are legislators, policy makers, managers and workers. Within these categories, many people require additional training in more specific tasks. For example, while all managers should have a basic understanding of the safety and health problems within their areas of responsibility and should know where to go for expert assistance, managers with specific responsibility for safety and health and compliance with regulations may need more intensive training. Similarly, workers who serve as safety delegates or members of safety and health committees need more than awareness training alone, as do government administrators involved in factory inspection and public health functions related to the workplace.
Those doctors, nurses and (especially in rural and developing areas) nonphysician primary health care workers whose primary training or practice does not include occupational medicine will need occupational health education in some depth in order to serve workers, for example by being able to recognize work-related illnesses. Finally, certain professions (for example, engineers, chemists, architects and designers) whose work has considerable impact on workers’ safety and health need much more specific education and training in these areas than they traditionally receive.
Specialists require the most intensive education and training, most often of the kind received in undergraduate and postgraduate programmes of study. Physicians, nurses, occupational hygienists, safety engineers and, more recently, ergonomists come under this category. With the rapid ongoing developments in all of these fields, continuing education and on-the-job experience are important components of the education of these professionals.
It is important to emphasize that increasing specialization in the fields of occupational hygiene and safety has taken place without a commensurate emphasis on the interdisciplinary aspects of these endeavours. A nurse or physician who suspects that a patient’s disease is work-related may well need the assistance of an occupational hygienist to identify the toxic exposure (for example) in the workplace that is causing the health problem. Given limited resources, many companies and governments often employ a safety specialist but not a hygienist, requiring that the safety specialist address health as well as safety concerns. The interdependence of safety and health issues should be addressed by offering interdisciplinary training and education to safety and health professionals.
Why Training and Education?
The primary tools needed to achieve the goals of reducing occupational injuries and illnesses and promoting occupational safety and health have been characterized as the “three E’s”—engineering, enforcement and education. The three are interdependent and receive varying levels of emphasis within different national systems. The overall rationale for training and education is to improve awareness of safety and health hazards, to expand knowledge of the causes of occupational illness and injury and to promote the implementation of effective preventive measures. The specific purpose and impetus for training will, however, vary for different target audiences.
Middle and upper level managers
The need for managers who are knowledgeable about the safety and health aspects of the operations for which they are responsible is more widely acknowledged today than heretofore. Employers increasingly recognize the considerable direct and indirect costs of serious accidents and the civil, and in some jurisdictions, criminal liability to which companies and individuals may be exposed. Although belief in the “careless worker” explanation for accidents and injuries remains prevalent, there is increasing recognition that “careless management” can be cited for conditions under its control that contribute to accidents and disease. Finally, firms also realize that poor safety performance is poor public relations; major disasters like the one in the Union Carbide plant in Bhopal (India) can offset years of effort to build a good name for a company.
Most managers are trained in economics, business or engineering and receive little or no instruction during their formal education in occupational health or safety matters. Yet daily management decisions have a critical impact on employee safety and health, both directly and indirectly. To remedy this state of affairs, safety and health concerns have begun to be introduced into management and engineering curricula and into continuing education programmes in many countries. Further efforts to make safety and health information more widespread is clearly necessary.
First-line supervisors
Research has demonstrated the central role played by first-line supervisors in the accident experience of construction employers (Samelson 1977). Supervisors who are knowledgeable about the safety and health hazards of their operations, who effectively train their crew members (especially new employees) and who are held accountable for their crew’s performance hold the key to improving conditions. They are the critical link between workers and the firm’s safety and health policies.
Employees
Law, custom and current workplace trends all contribute to the spread of employee education and training. Increasingly, employee safety and health training is being required by government regulations. Some apply to general practice, while in others the training requirements are related to specific industries, occupations or hazards. Although valid evaluation data on the effectiveness of such training as a countermeasure to work-related injuries and illnesses are surprisingly sparse (Vojtecky and Berkanovic 1984-85); nevertheless the acceptance of training and education for improving safety and health performance in many areas of work is becoming widespread in many countries and companies.
The growth of employee participation programmes, self-directed work teams and shop floor responsibility for decision-making has affected the way in which safety and health approaches are taken as well. Education and training are widely used to enhance knowledge and skills at the level of the line worker, who is now recognized as essential for the effectiveness of these new trends in work organization. A beneficial action employers can take is to involve employees early on (for example, in the planning and design stages when new technologies are introduced into a worksite) to minimize and to anticipate adverse effects on the work environment.
Trade unions have been a moving force both in advocating more and better training for employees and in developing and delivering curricula and materials to their members. In many countries, safety committee members, safety delegates and works council representatives have assumed a growing role in the resolution of hazard problems at the worksite and in inspection and advocacy as well. Persons holding these positions all require training that is more complete and sophisticated than that given to an employee performing a particular job.
Safety and health professionals
The duties of safety and health personnel comprise a broad range of activities that differ widely from one country to another and even within a single profession. Included in this group are physicians, nurses, hygienists and safety engineers either engaged in independent practice or employed by individual worksites, large corporations, government health or labour inspectorates and academic institutions. The demand for trained professionals in the area of occupational safety and health has grown rapidly since the 1970s with the proliferation of government laws and regulations paralleling the growth of corporate safety and health departments and academic research in this field.
Scope and Objectives of Training and Education
This ILO Encyclopaedia itself presents the multitude of issues and hazards that must be addressed and the range of personnel required in a comprehensive safety and health programme. Taking the large view, we can consider the objectives of training and education for safety and health in a number of ways. In 1981, the Joint ILO/WHO Committee on Occupational Health offered the following categories of educational objectives which apply in some degree to all of the groups discussed thus far: (1) cognitive (knowledge), (2) psychomotor (professional skills) and (3) affective (attitude and values). Another framework describes the “information–education–training” continuum, roughly corresponding to the “what”, the “why” and the “how” of hazards and their control. And the “empowerment education” model, to be discussed below, puts great emphasis on the distinction between training—the teaching of competency-based skills with predictable behavioural outcomes—and education—the development of independent critical thinking and decision-making skills leading to effective group action (Wallerstein and Weinger 1992).
Workers need to understand and apply the safety procedures, proper tools and protective equipment for performing specific tasks as part of their job skills training. They also require training in how to rectify hazards that they observe and to be familiar with internal company procedures, in accordance with the safety and health laws and regulations which apply to their area of work. Similarly, supervisors and managers must be aware of the physical, chemical and psychosocial hazards present in their workplaces as well as the social, organizational and industrial relations factors that may be involved in the creation of these hazards and in their correction. Thus, gaining knowledge and skills of a technical nature as well as organizational, communication and problem-solving skills are all necessary objectives in education and training.
In recent years, safety and health education has been influenced by developments in education theory, particularly theories of adult learning. There are different aspects of these developments, such as empowerment education, cooperative learning and participative learning. All share the principle that adults learn best when they are actively involved in problem-solving exercises. Beyond the transmission of specific bits of knowledge or skills, effective education requires the development of critical thinking and an understanding of the context of behaviours and ways of linking what is learned in the classroom to action in the workplace. These principles seem especially appropriate to workplace safety and health, where the causes of hazardous conditions and illnesses and injuries are often a combination of environmental and physical factors, human behaviour and the social context.
In translating these principles into an education programme four categories of objectives must be included:
Information objectives: the specific knowledge that trainees will acquire. For example, knowledge of the effects of organic solvents on the skin and on the central nervous system.
Behavioural objectives: the competencies and skills that workers will learn. For example, the ability to interpret chemical data sheets or to lift a heavy object safely.
Attitude objectives: the beliefs that interfere with safe performance or with response to training that must be addressed. The belief that accidents are not preventable or that “solvents can’t hurt me because I’ve worked with them for years and I’m fine” are examples.
Social action objectives: the ability to analyse a specific problem, identify its causes, propose solutions and plan and take action steps to resolve it. For example, the task of analysing a particular job where several people have sustained back injuries, and of proposing ergonomic modifications, requires the social action of changing the organization of work through labour-management cooperation.
Technological and Demographic Change
Training for awareness and management of specific safety and health hazards obviously depends on the nature of the workplace. While some hazards remain relatively constant, the changes that take place in the nature of jobs and technologies require continuous updating of training needs. Falls from heights, falling objects and noise, for example, have always been and will continue to be prominent hazards in the construction industry, but the introduction of many kinds of new synthetic building materials necessitates additional knowledge and awareness concerning their potential for adverse health effects. Similarly, unguarded belts, blades and other danger points on machinery remain common safety hazards but the introduction of industrial robots and other computer-controlled devices requires training in new types of machinery hazards.
With rapid global economic integration and the mobility of multinational corporations, old and new occupational hazards frequently exist side-by-side in both highly industrialized and developing countries. In an industrializing country sophisticated electronics manufacturing operations may be located next door to a metal foundry that still relies on low technology and the heavy use of manual labour. Meanwhile, in industrialized countries, garment sweatshops with miserable safety and health conditions, or lead battery recycling operations (with its threat of lead toxicity) continue to exist alongside highly automated state-of-the-art industries.
The need for continual updating of information applies as much to workers and managers as it does to occupational health professionals. Inadequacies in the training even of the latter is evidenced by the fact that most occupational hygienists educated in the 1970s received scant training in ergonomics; and even though they received extensive training in air monitoring, it was applied almost exclusively to industrial worksites. But the single largest technological innovation affecting millions of workers since that time is the widespread introduction of computer terminals with visual display units (VDUs). Ergonomic evaluation and intervention to prevent musculoskeletal and vision problems among VDU users was unheard of in the 1970s; by the mid-nineties, VDU hazards have become a major concern of occupational hygiene. Similarly, the application of occupational hygiene principles to indoor air quality problems (to remedy “tight/sick building syndrome”, for example) has required a great deal of continuing education for hygienists accustomed only to evaluating factories. Psychosocial factors, also largely unrecognized as occupational health hazards before the 1980s, play an important role in the treatment of VDU and indoor air hazards, and of many others as well. All parties investigating such health problems need education and training in order to understand the complex interactions among environment, the individual and social organization in these settings.
The changing demographics of the workforce must also be considered in safety and health training. Women make up an increasing proportion of the workforce in both developed and developing nations; their health needs in and out of the workplace must be addressed. The concerns of immigrant workers raise numerous new training questions, including those to do with language, although language and literacy issues are certainly not limited to immigrant workers: varying literacy levels among native-born workers must also be considered in the design and delivery of training. Older workers are another group whose needs must be studied and incorporated into education programmes as their numbers increase in the working population of many nations.
Training Venues and Providers
The location of training and education programmes is determined by the audience, the purpose, the content, the duration of the programme and, to be realistic, the resources available in the country or region. The audience for safety and health education starts with schoolchildren, trainees and apprentices, and extends to workers, supervisors, managers and safety and health professionals.
Training in schools
Incorporation of safety and health education into elementary and secondary education, and especially in vocational and technical training schools, is a growing and very positive trend. The teaching of hazard recognition and control as a regular part of skills training for particular occupations or trades is far more effective than trying to impart such knowledge later, when the worker has been in the trade for a period of years, and has already developed set practices and behaviours. Such programmes, of course, necessitate that the teachers in these schools also be trained to recognize hazards and apply preventive measures.
On-the-job training
On-the-job training at the worksite is appropriate for workers and supervisors facing specific hazards found onsite. If the training is of significant length, a comfortable classroom facility within the worksite is strongly recommended. In cases where locating the training at the workplace may intimidate workers or otherwise discourage their full participation in the class, an offsite venue is preferable. Workers may feel more comfortable in a union setting where the union plays a major role in designing and delivering the programme. However, field visits to actual work locations which illustrate the hazards in question are always a positive addition to the course.
Training of safety delegates and committee members
The longer and more sophisticated training recommended for safety delegates and committee representatives is often delivered at specialized training centres, universities or commercial facilities. More and more efforts are being made to implement regulatory requirements for training and certification of workers who are to perform in certain hazardous fields such as asbestos abatement and hazardous waste handling. These courses usually include both classroom and hands-on sessions, where actual performance is simulated and specialized equipment and facilities are required.
Providers of onsite and offsite programmes for workers and safety representatives include government agencies, tripartite organizations like the ILO or analogous national or sub-national bodies, business associations and labour unions, universities, professional associations and private training consultants. Many governments provide funds for the development of safety and health training and education programmes targeted at specific industries or hazards.
Academic and professional training
The training of safety and health professionals varies widely among countries, depending on the needs of the working population and the country’s resources and structures. Professional training is centred in undergraduate and postgraduate university programmes, but these vary in availability in different parts of the world. Degree programmes may be offered for specialists in occupational medicine and nursing and occupational health may be incorporated into the training of general practitioners and of primary care and public health nurses. The number of degree-granting programmes for occupational hygienists has increased dramatically. However, there remains a strong demand for short courses and less comprehensive training for hygiene technicians, many of whom have received their basic training on the job in particular industries.
There is an acute need for more trained safety and health personnel in the developing world. While more university-trained and credentialed physicians, nurses and hygienists will undoubtedly be welcomed in these countries, it is nonetheless realistic to expect that many health services will continue to be delivered by primary health care workers. These people need training in the relationship between work and health, in the recognition of the major safety and health risks associated with the type of work carried on in their region, in basic survey and sampling techniques, in the use of the referral network available in their region for suspected cases of occupational illness and in health education and risk communication techniques (WHO1988).
Alternatives to university-based degree programmes are critically important to professional training in both developing and industrialized nations, and would include continuing education, distance education, on-the-job training and self-training, among others.
Conclusion
Education and training cannot solve all occupational safety and health problems, and care must be taken that the techniques learned in such programmes are in fact applied appropriately to the identified needs. They are, however, critical components of an effective safety and health programme when employed in conjunction with engineering and technical solutions. Cumulative, interactive and continuous learning is essential to prepare our rapidly changing work environments to meet the needs of workers, especially as regards the prevention of debilitating injuries and illnesses. Those who labour in the workplace as well as those who provide support from the outside need the most up-to-date information available and the skills to put this information to use in order to protect and promote worker health and safety.
Carcinogen Risk Assessment
Whereas the principles and methods of risk assessment for non-carcinogenic chemicals are similar in different parts of the world, it is striking that approaches for risk assessment of carcinogenic chemicals vary greatly. There are not only marked differences between countries, but even within a country different approaches are applied or advocated by various regulatory agencies, committees and scientists in the field of risk assessment. Risk assessment for non-carcinogens is rather consistent and pretty well established partly because of the long history and better understanding of the nature of toxic effects in comparison with carcinogens and a high degree of consensus and confidence by both scientists and the general public on methods used and their outcome.
For non-carcinogenic chemicals, safety factors were introduced to compensate for uncertainties in the toxicology data (which are derived mostly from animal experiments) and in their applicability to large, heterogeneous human populations. In doing so, recommended or required limits on safe human exposures were usually set at a fraction (the safety or uncertainty factor approach) of the exposure levels in animals that could be clearly documented as the no observed adverse effects level (NOAEL) or the lowest observed adverse effects level (LOAEL). It was then assumed that as long as human exposure did not exceed the recommended limits, the hazardous properties of chemical substances would not be manifest. For many types of chemicals, this practice, in somewhat refined form, continues to this day in toxicological risk assessment.
During the late 1960s and early 1970s regulatory bodies, starting in the United States, were confronted with an increasingly important problem for which many scientists considered the safety factor approach to be inappropriate, and even dangerous. This was the problem with chemicals that under certain conditions had been shown to increase the risk of cancers in humans or experimental animals. These substances were operationally referred to as carcinogens. There is still debate and controversy on the definition of a carcinogen, and there is a wide range of opinion about techniques to identify and classify carcinogens and the process of cancer induction by chemicals as well.
The initial discussion started much earlier, when scientists in the 1940s discovered that chemical carcinogens caused damage by a biological mechanism that was of a totally different kind from those that produced other forms of toxicity. These scientists, using principles from the biology of radiation-induced cancers, put forth what is referred to as the “non-threshold” hypothesis, which was considered applicable to both radiation and carcinogenic chemicals. It was hypothesized that any exposure to a carcinogen that reaches its critical biological target, especially the genetic material, and interacts with it, can increase the probability (the risk) of cancer development.
Parallel to the ongoing scientific discussion on thresholds, there was a growing public concern on the adverse role of chemical carcinogens and the urgent need to protect the people from a set of diseases collectively called cancer. Cancer, with its insidious character and long latency period together with data showing that cancer incidences in the general population were increasing, was regarded by the general public and politicians as a matter of concern that warranted optimal protection. Regulators were faced with the problem of situations in which large numbers of people, sometimes nearly the entire population, were or could be exposed to relatively low levels of chemical substances (in consumer products and medicines, at the workplace as well as in air, water, food and soils) that had been identified as carcinogenic in humans or experimental animals under conditions of relatively intense exposures.
Those regulatory officials were confronted with two fundamental questions which, in most cases, could not be fully answered using available scientific methods:
- What risk to human health exists in the range of exposure to chemicals below the relatively intense and narrow exposure range under which a cancer risk could be directly measured?
- What could be said about risks to human health when experimental animals were the only subjects in which risks for the development of cancer had been established?
Regulators recognized the need for assumptions, sometimes scientifically based but often also unsupported by experimental evidence. In order to achieve consistency, definitions and specific sets of assumptions were adapted that would be generically applied to all carcinogens.
Carcinogenesis Is a Multistage Process
Several lines of evidence support the conclusion that chemical carcinogenesis is a multistage process driven by genetic damage and epigenetic changes, and this theory is widely accepted in the scientific community all over the world (Barrett 1993). Although the process of chemical carcinogenesis is often separated into three stages—initiation, promotion and progression—the number of relevant genetic changes is not known.
Initiation involves the induction of an irreversibly altered cell and is for genotoxic carcinogens always equated with a mutational event. Mutagenesis as a mechanism of carcinogenesis was already hypothesized by Theodor Boveri in 1914, and many of his assumptions and predictions have subsequently been proven to be true. Because irreversible and self-replicating mutagenic effects can be caused by the smallest amount of a DNA-modifying carcinogen, no threshold is assumed. Promotion is the process by which the initiated cell expands (clonally) by a series of divisions, and forms (pre)neoplastic lesions. There is considerable debate as to whether during this promotion phase initiated cells undergo additional genetic changes.
Finally in the progression stage “immortality” is obtained and full malignant tumours can develop by influencing angiogenesis, escaping the reaction of the host control systems. It is characterized by invasive growth and frequently metastatic spread of the tumour. Progression is accompanied by additional genetic changes due to the instability of proliferating cells and selection.
Therefore, there are three general mechanisms by which a substance can influence the multistep carcinogenic process. A chemical can induce a relevant genetic alteration, promote or facilitate clonal expansion of an initiated cell or stimulate progression to malignancy by somatic and/or genetic changes.
Risk Assessment Process
Risk can be defined as the predicted or actual frequency of occurrence of an adverse effect on humans or the environment, from a given exposure to a hazard. Risk assessment is a method of systematically organizing the scientific information and its attached uncertainties for description and qualification of the health risks associated with hazardous substances, processes, actions or events. It requires evaluation of relevant information and selection of the models to be used in drawing inferences from that information. Further, it requires explicit recognition of uncertainties and appropriate acknowledgement that alternative interpretation of the available data may be scientifically plausible. The current terminology used in risk assessment was proposed in 1984 by the US National Academy of Sciences. Qualitative risk assessment changed into hazard characterization/identification and quantitative risk assessment was divided into the components dose-response, exposure assessment and risk characterization.
In the following section these components will be briefly discussed in view of our current knowledge of the process of (chemical) carcinogenesis. It will become clear that the dominant uncertainty in the risk assessment of carcinogens is the dose-response pattern at low dose levels characteristic for environmental exposure.
Hazard identification
This process identifies which compounds have the potential to cause cancer in humans—in other words it identifies their intrinsic genotoxic properties. Combining information from various sources and on different properties serves as a basis for classification of carcinogenic compounds. In general the following information will be used:
- epidemiological data (e.g., vinylchloride, arsenic, asbestos)
- animal carcinogenicity data
- genotoxic activity/DNA adduct formation
- mechanisms of action
- pharmacokinetic activity
- structure-activity relationships.
Classification of chemicals into groups based on the assessment of the adequacy of the evidence of carcinogenesis in animals or in man, if epidemiological data are available, is a key process in hazard identification. The best known schemes for categorizing carcinogenic chemicals are those of IARC (1987), EU (1991) and the EPA (1986). An overview of their criteria for classification (e.g., low-dose extrapolation methods) is given in table 1.
Table 1. Comparison of low-dose extrapolations procedures
| Current US EPA | Denmark | EEC | UK | Netherlands | Norway | |
| Genotoxic carcinogen | Linearized multistage procedure using most appropriate low-dose model | MLE from 1- and 2-hit models plus judgement of best outcome | No procedure specified | No model, scientific expertise and judgement from all available data | Linear model using TD50 (Peto method) or “Simple Dutch Method” if no TD50 | No procedure specified |
| Non-genotoxic carcinogen | Same as above | Biologically-based model of Thorslund or multistage or Mantel-Bryan model, based on tumour origin and dose-response | Use NOAEL and safety factors | Use NOEL and safety factors to set ADI | Use NOEL and safety factors to set ADI |
One important issue in classifying carcinogens, with sometimes far-reaching consequences for their regulation, is the distinction between genotoxic and non-genotoxic mechanisms of action. The US Environmental Protection Agency (EPA) default assumption for all substances showing carcinogenic activity in animal experiments is that no threshold exists (or at least none can be demonstrated), so there is some risk with any exposure. This is com- monly referred to as the non-threshold assumption for genotoxic (DNA-damaging) compounds. The EU and many of its members, such as the United Kingdom, the Netherlands and Denmark, make a distinction between carcinogens that are genotoxic and those believed to produce tumours by non-genotoxic mechanisms. For genotoxic carcinogens quantitative dose-response estimation procedures are followed that assume no threshold, although the procedures might differ from those used by the EPA. For non-genotoxic substances it is assumed that a threshold exists, and dose-response procedures are used that assume a threshold. In the latter case, the risk assessment is generally based on a safety factor approach, similar to the approach for non-carcinogens.
It is important to keep in mind that these different schemes were developed to deal with risk assessments in different contexts and settings. The IARC scheme was not produced for regulatory purposes, although it has been used as a basis for developing regulatory guidelines. The EPA scheme was designed to serve as a decision point for entering quantitative risk assessment, whereas the EU scheme is currently used to assign a hazard (classification) symbol and risk phrases to the chemical's label. A more extended discussion on this subject is presented in a recent review (Moolenaar 1994) covering procedures used by eight governmental agencies and two often-cited independent organizations, the Inter- national Agency for Research on Cancer (IARC) and the American Conference of Governmental Industrial Hygienists (ACGIH).
The classification schemes generally do not take into account the extensive negative evidence that may be available. Also, in recent years a greater understanding of the mechanism of action of carcinogens has emerged. Evidence has accumulated that some mechanisms of carcinogenicity are species-specific and are not relevant for man. The following examples will illustrate this important phenomenon. First, it has been recently demonstrated in studies on the carcinogenicity of diesel particles, that rats respond with lung tumours to a heavy loading of the lung with particles. However, lung cancer is not seen in coal miners with very heavy lung burdens of particles. Secondly, there is the assertion of the nonrelevance of renal tumours in the male rat on the basis that the key element in the tumourgenic response is the accumulation in the kidney of α-2 microglobulin, a protein that does not exist in humans (Borghoff, Short and Swenberg 1990). Disturbances of rodent thyroid function and peroxisome proliferation or mitogenesis in the mouse liver have also to be mentioned in this respect.
This knowledge allows a more sophisticated interpretation of the results of a carcinogenicity bioassay. Research towards a better understanding of the mechanisms of action of carcinogenicity is encouraged because it may lead to an altered classification and to the addition of a category in which chemicals are classified as not carcinogenic to humans.
Exposure assessment
Exposure assessment is often thought to be the component of risk assessment with the least inherent uncertainty because of the ability to monitor exposures in some cases and the availability of relatively well-validated exposure models. This is only partially true, however, because most exposure assessments are not conducted in ways that take full advantage of the range of available information. For that reason there is a great deal of room for improving exposure distribution estimates. This holds for both external as well as for internal exposure assessments. Especially for carcinogens, the use of target tissue doses rather than external exposure levels in modelling dose-response relationships would lead to more relevant predictions of risk, although many assumptions on default values are involved. Physiologically based pharmacokinetic (PBPK) models to determine the amount of reactive metabolites that reaches the target tissue are potentially of great value to estimate these tissue doses.
Risk Characterization
Current approaches
The dose level or exposure level that causes an effect in an animal study and the likely dose causing a similar effect in humans is a key consideration in risk characterization. This includes both dose-response assessment from high to low dose and interspecies extrapolation. The extrapolation presents a logical problem, namely that data are being extrapolated many orders of magnitude below the experimental exposure levels by empirical models that do not reflect the underlying mechanisms for carcinogenicity. This violates a basic principle in fitting of empirical models, namely not to extrapolate outside the range of the observable data. Therefore, this empirical extrapolation results in large uncertainties, both from a statistical and from a biological point of view. At present no single mathematical procedure is recognized as the most appropriate one for low-dose extrapolation in carcinogenesis. The mathematical models that have been used to describe the relation between the administered external dose, the time and the tumour incidence are based on either tolerance-distribution or mechanistic assumptions, and sometimes based on both. A summary of the most frequently cited models (Kramer et al. 1995) is listed in table 2.
Table 2. Frequently cited models in carcinogen risk characterization
| Tolerance distribution models | Mechanistic models | |
| Hit-models | Biologically based models | |
| Logit | One-hit | Moolgavkar (MVK)1 |
| Probit | Multihit | Cohen and Ellwein |
| Mantel-Bryan | Weibull (Pike)1 | |
| Weibull | Multistage (Armitage-Doll)1 | |
| Gamma Multihit | Linearized Multistage, |
1 Time-to-tumour models.
These dose-response models are usually applied to tumour-incidence data corresponding to only a limited number of experimental doses. This is due to the standard design of the applied bioassay. Instead of determining the complete dose-response curve, a carcinogenicity study is in general limited to three (or two) relatively high doses, using the maximum tolerated dose (MTD) as highest dose. These high doses are used to overcome the inherent low statistical sensitivity (10 to 15% over background) of such bioassays, which is due to the fact that (for practical and other reasons) a relatively small number of animals is used. Because data for the low-dose region are not available (i.e., cannot be determined experimentally), extrapolation outside the range of observation is required. For almost all data sets, most of the above-listed models fit equally well in the observed dose range, due to the limited number of doses and animals. However, in the low-dose region these models diverge several orders of magnitude, thereby introducing large uncertainties to the risk estimated for these low exposure levels.
Because the actual form of the dose-response curve in the low-dose range cannot be generated experimentally, mechanistic insight into the process of carcinogenicity is crucial to be able to discriminate on this aspect between the various models. Comprehensive reviews discussing the various aspects of the different mathematical extrapolation models are presented in Kramer et al. (1995) and Park and Hawkins (1993).
Other approaches
Besides the current practice of mathematical modelling several alternative approaches have been proposed recently.
Biologically motivated models
Currently, the biologically based models such as the Moolgavkar-Venzon-Knudson (MVK) models are very promising, but at present these are not sufficiently well advanced for routine use and require much more specific information than currently is obtained in bioassays. Large studies (4,000 rats) such as those carried out on N-nitrosoalkylamines indicate the size of the study which is required for the collection of such data, although it is still not possible to extrapolate to low doses. Until these models are further developed they can be used only on a case-by-case basis.
Assessment factor approach
The use of mathematical models for extrapolation below the experimental dose range is in effect equivalent to a safety factor approach with a large and ill-defined uncertainty factor. The simplest alternative would be to apply an assessment factor to the apparent “no effect level”, or the “lowest level tested”. The level used for this assessment factor should be determined on a case-by-case basis considering the nature of the chemical and the population being exposed.
Benchmark dose (BMD)
The basis of this approach is a mathematical model fitted to the experimental data within the observable range to estimate or interpolate a dose corresponding to a defined level of effect, such as one, five or ten per cent increase in tumour incidence (ED01, ED05, ED10). As a ten per cent increase is about the smallest change that statistically can be determined in a standard bioassay, the ED10 is appropriate for cancer data. Using a BMD that is within the observable range of the experiment avoids the problems associated with dose extrapolation. Estimates of the BMD or its lower confidence limit reflect the doses at which changes in tumour incidence occurred, but are quite insensitive to the mathematical model used. A benchmark dose can be used in risk assessment as a measure of tumour potency and combined with appropriate assessment factors to set acceptable levels for human exposure.
Threshold of regulation
Krewski et al. (1990) have reviewed the concept of a “threshold of regulation” for chemical carcinogens. Based on data obtained from the carcinogen potency database (CPDB) for 585 experiments, the dose corresponding to 10-6 risk was roughly log-normally distributed around a median of 70 to 90 ng/kg/d. Exposure to dose levels greater than this range would be considered unacceptable. The dose was estimated by linear extrapolation from the TD50 (the dose inducing toxicity is 50% of the animals tested) and was within a factor of five to ten of the figure obtained from the linearized multistage model. Unfortunately, the TD50 values will be related to the MTD, which again casts doubt on the validity of the measurement. However the TD50 will often be within or very close to the experimental data range.
Such an approach as using a threshold of regulation would require much more consideration of biological, analytical and mathematical issues and a much wider database before it could be considered. Further investigation into the potencies of various carcinogens may throw further light onto this area.
Objectives and Future of CarcinogenRisk Assessment
Looking back to the original expectations on the regulation of (environmental) carcinogens, namely to achieve a major reduction in cancer, it appears that the results at present are disappointing. Over the years it became apparent that the number of cancer cases estimated to be produced by regulatable carcinogens was disconcertingly small. Considering the high expectations that launched the regulatory efforts in the 1970s, a major anticipated reduction in the cancer death rate has not been achieved in terms of the estimated effects of environmental carcinogens, not even with ultraconservative quantitative assessment procedures. The main characteristic of the EPA procedures is that low-dose extrapolations are made in the same way for each chemical regardless of the mechanism of tumour formation in experimental studies. It should be noted, however, that this approach stands in sharp contrast to approaches taken by other governmental agencies. As indicated above, the EU and several European governments—Denmark, France, Germany, Italy, the Netherlands, Sweden, Switzerland, UK—distinguish between genotoxic and non-genotoxic carcinogens, and approach risk estimation differently for the two categories. In general, non-genotoxic carcinogens are treated as threshold toxicants. No effect levels are determined, and uncertainty factors are used to provide an ample margin of safety. To determine whether or not a chemical should be regarded as non-genotoxic is a matter of scientific debate and requires clear expert judgement.
The fundamental issue is: What is the cause of cancer in humans and what is the role of environmental carcinogens in that causation? The hereditary aspects of cancer in humans are much more important than previously anticipated. The key to signifi- cant advancement in the risk assessment of carcinogens is a better understanding of the causes and mechanisms of cancer. The field of cancer research is entering a very exciting area. Molecular research may radically alter the way we view the impact of environmental carcinogens and the approaches to control and prevent cancer, both for the general public and the workplace. Risk assessment of carcinogens needs to be based on concepts of the mechanisms of action that are, in fact, just emerging. One of the important aspects is the mechanism of heritable cancer and the interaction of carcinogens with this process. This knowledge will have to be incorporated into the systematic and consistent methodology that already exists for the risk assessment of carcinogens.
Appendix: Overall Evaluations of Carcinogenicity to Humans: IARC Monographs Volumes 1-69 (836)
Group 1—Carcinogenic to Humans (74)
Agents and groups of agents
Aflatoxins [1402-68-2] (1993)
4-Aminobiphenyl [92-67-1]
Arsenic [7440-38-2] and arsenic compounds2
Asbestos [1332-21-4]
Azathioprine [446-86-6]
Benzene [71-43-2]
Benzidine [92-87-5]
Beryllium [7440-41-7] and beryllium compounds (1993)3
Bis(2-chloroethyl)-2-naphthylamine (Chlornaphazine)[494-03-1]
Bis(chloromethyl)ether [542-88-1] and chloromethyl methyl ether [107-30-2] (technical-grade)
1,4-Butanediol dimethanesulphonate (Myleran) [55-98-1]
Cadmium [7440-43-9] and cadmium compounds (1993)3
Chlorambucil [305-03-3]
1-(2-Chloroethyl)-3-(4-methylcyclohexyl)-1-nitrosourea (Methyl-CCNU; Semustine) [13909-09-6]
Chromium[VI] compounds (1990)3
Ciclosporin [79217-60-0] (1990)
Cyclophosphamide [50-18-0] [6055-19-2]
Diethylstilboestrol [56-53-1]
Erionite [66733-21-9]
Ethylene oxide4 [75-21-8] (1994)
Helicobacter pylori (infection with) (1994)
Hepatitis B virus (chronic infection with) (1993)
Hepatitis C virus (chronic infection with) (1993)
Human papillomavirus type 16 (1995)
Human papillomavirus type 18 (1995)
Human T-cell lymphotropic virus type I (1996)
Melphalan [148-82-3]
8-Methoxypsoralen (Methoxsalen) [298-81-7] plus ultraviolet A radiation
MOPP and other combined chemotherapy including alkylating agents
Mustard gas (Sulphur mustard) [505-60-2]
2-Naphthylamine [91-59-8]
Nickel compounds (1990)3
Oestrogen replacement therapy
Oestrogens, nonsteroidal2
Oestrogens, steroidal2
Opisthorchis viverrini (infection with) (1994)
Oral contraceptives, combined5
Oral contraceptives, sequential
Radon [10043-92-2] and its decay products (1988)
Schistosoma haematobium (infection with) (1994)
Silica [14808-60-7] crystalline (inhaled in the form of quartz or cristobalite from occupational sources)
Solar radiation (1992)
Talc containing asbestiform fibres
Tamoxifen [10540-29-1]6
Thiotepa [52-24-4] (1990)
Treosulphan [299-75-2]
Vinyl chloride [75-01-4]
Mixtures
Alcoholic beverages (1988)
Analgesic mixtures containing phenacetin
Betel quid with tobacco
Coal-tar pitches [65996-93-2]
Coal-tars [8007-45-2]
Mineral oils, untreated and mildly treated
Salted fish (Chinese-style) (1993)
Shale oils [68308-34-9]
Soots
Tobacco products, smokeless
Tobacco smoke
Wood dust
Exposure circumstances
Aluminium production
Auramine, manufacture of
Boot and shoe manufacture and repair
Coal gasification
Coke production
Furniture and cabinet making
Haematite mining (underground) with exposure to radon
Iron and steel founding
Isopropanol manufacture (strong-acid process)
Magenta, manufacture of (1993)
Painter (occupational exposure as a) (1989)
Rubber industry
Strong-inorganic-acid mists containing sulphuric acid (occupational exposure to) (1992)
Group 2A—Probably carcinogenic to humans (56)
Agents and groups of agents
Acrylamide [79-06-1] (1994)8
Acrylonitrile [107-13-1]
Adriamycin8 [23214-92-8]
Androgenic (anabolic) steroids
Azacitidine8 [320-67-2] (1990)
Benz[a]anthracene8 [56-55-3]
Benzidine-based dyes8
Benzo[a]pyrene8 [50-32-8]
Bischloroethyl nitrosourea (BCNU) [154-93-8]
1,3-Butadiene [106-99-0] (1992)
Captafol [2425-06-1] (1991)
Chloramphenicol [56-75-7] (1990)
1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea8 (CCNU)[13010-47-4]
p-Chloro-o-toluidine [95-69-2] and its strong acid salts (1990)3
Chlorozotocin8 [54749-90-5] (1990)
Cisplatin8 [15663-27-1]
Clonorchis sinensis (infection with)8 (1994)
Dibenz[a,h]anthracene8 [53-70-3]
Diethyl sulphate [64-67-5] (1992)
Dimethylcarbamoyl chloride8 [79-44-7]
Dimethyl sulphate8 [77-78-1]
Epichlorohydrin8 [106-89-8]
Ethylene dibromide8 [106-93-4]
N-Ethyl-N-nitrosourea8 [759-73-9]
Formaldehyde [50-00-0])
IQ8 (2-Amino-3-methylimidazo[4,5-f]quinoline) [76180-96-6] (1993)
5-Methoxypsoralen8 [484-20-8]
4,4´-Methylene bis(2-chloroaniline) (MOCA)8 [101-14-4] (1993)
N-Methyl-N´-nitro-N-nitrosoguanidine8 (MNNG) [70-25-7]
N-Methyl-N-nitrosourea8 [684-93-5]
Nitrogen mustard [51-75-2]
N-Nitrosodiethylamine8 [55-18-5]
N-Nitrosodimethylamine 8 [62-75-9]
Phenacetin [62-44-2]
Procarbazine hydrochloride8 [366-70-1]
Tetrachloroethylene [127-18-4]
Trichloroethylene [79-01-6]
Styrene-7,8-oxide8 [96-09-3] (1994)
Tris(2,3-dibromopropyl)phosphate8 [126-72-7]
Ultraviolet radiation A8 (1992)
Ultraviolet radiation B8 (1992)
Ultraviolet radiation C8 (1992)
Vinyl bromide6 [593-60-2]
Vinyl fluoride [75-02-5]
Mixtures
Creosotes [8001-58-9]
Diesel engine exhaust (1989)
Hot mate (1991)
Non-arsenical insecticides (occupational exposures in spraying and application of) (1991)
Polychlorinated biphenyls [1336-36-3]
Exposure circumstances
Art glass, glass containers and pressed ware (manufacture of) (1993)
Hairdresser or barber (occupational exposure as a) (1993)
Petroleum refining (occupational exposures in) (1989)
Sunlamps and sunbeds (use of) (1992)
Group 2B—Possibly carcinogenic to humans (225)
Agents and groups of agents
A–α–C (2-Amino-9H-pyrido[2,3-b]indole) [26148-68-5]
Acetaldehyde [75-07-0]
Acetamide [60-35-5]
AF-2 [2-(2-Furyl)-3-(5-nitro-2-furyl)acrylamide] [3688-53-7]
Aflatoxin M1 [6795-23-9] (1993)
p-Aminoazobenzene [60-09-3]
o-Aminoazotoluene [97-56-3]
2-Amino-5-(5-nitro-2-furyl)-1,3,4-thiadiazole [712-68-5]
Amitrole [61-82-5]
o-Anisidine [90-04-0]
Antimony trioxide [1309-64-4] (1989)
Aramite [140-57-8]
Atrazine9 [1912-24-9] (1991)
Auramine [492-80-8] (technical-grade)
Azaserine [115-02-6]
Benzo[b]fluoranthene [205-99-2]
Benzo[j]fluoranthene [205-82-3]
Benzo[k]fluoranthene [207-08-9]
Benzyl violet 4B [1694-09-3]
Bleomycins [11056-06-7]
Bracken fern
Bromodichloromethane [75-27-4] (1991)
Butylated hydroxyanisole (BHA) [25013-16-5]
β-Butyrolactone [3068-88-0]
Caffeic acid [331-39-5] (1993)
Carbon-black extracts
Carbon tetrachloride [56-23-5]
Ceramic fibres
Chlordane [57-74-9] (1991)
Chlordecone (Kepone) [143-50-0]
Chlorendic acid [115-28-6] (1990)
α-Chlorinated toluenes (benzyl chloride, benzal chloride,benzotrichloride)
p-Chloroaniline [106-47-8] (1993)
Chloroform [67-66-3]
1-Chloro-2-methylpropene [513-37-1]
Chlorophenols
Chlorophenoxy herbicides
4-Chloro-o-phenylenediamine [95-83-0]
CI Acid Red 114 [6459-94-5] (1993)
CI Basic Red 9 [569-61-9] (1993)
CI Direct Blue 15 [2429-74-5] (1993)
Citrus Red No. 2 [6358-53-8]
Cobalt [7440-48-4] and cobalt compounds3 (1991)
p-Cresidine [120-71-8]
Cycasin [14901-08-7]
Dacarbazine [4342-03-4]
Dantron (Chrysazin; 1,8-Dihydroxyanthraquinone) [117-10-2] (1990)
Daunomycin [20830-81-3]
DDT´-DDT, 50-29-3] (1991)
N,N´-Diacetylbenzidine [613-35-4]
2,4-Diaminoanisole [615-05-4]
4,4´-Diaminodiphenyl ether [101-80-4]
2,4-Diaminotoluene [95-80-7]
Dibenz[a,h]acridine [226-36-8]
Dibenz[a,j]acridine [224-42-0]
7H-Dibenzo[c,g]carbazole [194-59-2]
Dibenzo[a,e]pyrene [192-65-4]
Dibenzo[a,h]pyrene [189-64-0]
Dibenzo[a,i]pyrene [189-55-9]
Dibenzo[a,l]pyrene [191-30-0]
1,2-Dibromo-3-chloropropane [96-12-8]
p-Dichlorobenzene [106-46-7]
3,3´-Dichlorobenzidine [91-94-1]
3,3´-Dichloro-4,4´-diaminodiphenyl ether [28434-86-8]
1,2-Dichloroethane [107-06-2]
Dichloromethane (methylene chloride) [75-09-2]
1,3-Dichloropropene [542-75-6] (technical grade)
Dichlorvos [62-73-7] (1991)
Diepoxybutane [1464-53-5]
Di(2-ethylhexyl)phthalate [117-81-7]
1,2-Diethylhydrazine [1615-80-1]
Diglycidyl resorcinol ether [101-90-6]
Dihydrosafrole [94-58-6]
Diisopropyl sulphate [2973-10-6] (1992)
3,3´-Dimethoxybenzidine (o-Dianisidine) [119-90-4]
p-Dimethylaminoazobenzene [60-11-7]
trans-2-[(Dimethylamino)methylimino]-5-[2-(5-nitro-2-furyl)-vinyl]-1,3,4-oxadiazole [25962-77-0]
2,6-Dimethylaniline (2,6-xylidine) [87-62-7] (1993)
3,3´-Dimethylbenzidine (o-tolidine) [119-93-7]
Dimethylformamide [68-12-2] (1989)
1,1-Dimethylhydrazine [57-14-7]
1,2-Dimethylhydrazine [540-73-8]
3,7-Dinitrofluoranthene [105735-71-5]
3,9-Dinitrofluoranthene [22506-53-2]
1,6-Dinitropyrene [42397-64-8] (1989)
1,8-Dinitropyrene [42397-65-9] (1989)
2,4-Dinitrotoluene [121-14-2]
2,6-Dinitrotoluene [606-20-2]
1,4-Dioxane [123-91-1]
Disperse Blue 1 [2475-45-8] (1990)
Ethyl acrylate [140-88-5]
Ethylene thiourea [96-45-7]
Ethyl methanesulphonate [62-50-0]
2-(2-Formylhydrazino)-4-(5-nitro-2-furyl)thiazole [3570-75-0]
Glass wool (1988)
Glu-P-1 (2-amino-6-methyldipyrido[1,2-a:3´,2´-d]imidazole)[67730-11-4]
Glu-P-2 (2-aminodipyrido[1,2-a:3´,2´-d]imidazole) [67730-10-3]
Glycidaldehyde [765-34-4]
Griseofulvin [126-07-8]
HC Blue No. 1 [2784-94-3] (1993)
Heptachlor [76-44-8] (1991)
Hexachlorobenzene [118-74-1]
Hexachlorocyclohexanes
Hexamethylphosphoramide [680-31-9]
Human immunodeficiency virus type 2 (infection with) (1996)
Human papillomaviruses: some types other than 16, 18, 31 and 33 (1995)
Hydrazine [302-01-2]
Indeno[1,2,3-cd]pyrene [193-39-5]
Iron-dextran complex [9004-66-4]
Isoprene [78-79-5] (1994)
Lasiocarpine [303-34-4]
Lead [7439-92-1] and lead compounds, inorganic3
Magenta [632-99-5] (containing CI Basic Red 9) (1993)
MeA-α-C (2-Amino-3-methyl-9H-pyrido[2,3-b]indole)[68006-83-7]
Medroxyprogesterone acetate [71-58-9]
MeIQ (2-Amino-3,4-dimethylimidazo[4,5-f]quinoline)[77094-11-2] (1993)
MeIQx (2-Amino-3,8-dimethylimidazo[4,5-f]quinoxaline) [77500-04-0] (1993)
Merphalan [531-76-0]
2-Methylaziridine (propyleneimine) [75-55-8]
Methylazoxymethanol acetate [592-62-1]
5-Methylchrysene [3697-24-3]
4,4´-Methylene bis(2-methylaniline) [838-88-0]
4,4´-Methylenedianiline [101-77-9]
Methylmercury compounds (1993)3
Methyl methanesulphonate [66-27-3]
2-Methyl-1-nitroanthraquinone [129-15-7] (uncertain purity)
N-Methyl-N-nitrosourethane [615-53-2]
Methylthiouracil [56-04-2]
Metronidazole [443-48-1]
Mirex [2385-85-5]
Mitomycin C [50-07-7]
Monocrotaline [315-22-0]
5-(Morpholinomethyl)-3-[(5-nitrofurfurylidene)amino]-2-oxazolidinone [3795-88-8]
Nafenopin [3771-19-5]
Nickel, metallic [7440-02-0] (1990)
Niridazole [61-57-4]
Nitrilotriacetic acid [139-13-9] and its salts (1990)3
5-Nitroacenaphthene [602-87-9]
2-Nitroanisole [91-23-6] (1996)
Nitrobenzene [98-95-3] (1996)
6-Nitrochrysene [7496-02-8] (1989)
Nitrofen [1836-75-5], technical-grade
2-Nitrofluorene [607-57-8] (1989)
1-[(5-Nitrofurfurylidene)amino]-2-imidazolidinone [555-84-0]
N-[4-(5-Nitro-2-furyl)-2-thiazolyl]acetamide [531-82-8]
Nitrogen mustard N-oxide [126-85-2]
2-Nitropropane [79-46-9]
1-Nitropyrene [5522-43-0] (1989)
4-Nitropyrene [57835-92-4] (1989)
N-Nitrosodi-n-butylamine [924-16-3]
N-Nitrosodiethanolamine [1116-54-7]
N-Nitrosodi-n-propylamine [621-64-7]
3-(N-Nitrosomethylamino)propionitrile [60153-49-3]
4-(N-Nitrosomethylamino)-1-(3-pyridyl)-1-butanone (NNK) [64091-91-4]
N-Nitrosomethylethylamine [10595-95-6]
N-Nitrosomethylvinylamine [4549-40-0]
N-Nitrosomorpholine [59-89-2]
N‘-Nitrosonornicotine [16543-55-8]
N-Nitrosopiperidine [100-75-4]
N-Nitrosopyrrolidine [930-55-2]
N-Nitrososarcosine [13256-22-9]
Ochratoxin A [303-47-9] (1993)
Oil Orange SS [2646-17-5]
Oxazepam [604-75-1] (1996)
Palygorskite (attapulgite) [12174-11-7] (long fibres, >>5 micro-meters) (1997)
Panfuran S (containing dihydroxymethylfuratrizine [794-93-4])
Pentachlorophenol [87-86-5] (1991)
Phenazopyridine hydrochloride [136-40-3]
Phenobarbital [50-06-6]
Phenoxybenzamine hydrochloride [63-92-3]
Phenyl glycidyl ether [122-60-1] (1989)
Phenytoin [57-41-0]
PhIP (2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine) [105650-23-5] (1993)
Ponceau MX [3761-53-3]
Ponceau 3R [3564-09-8]
Potassium bromate [7758-01-2]
Progestins
1,3-Propane sultone [1120-71-4]
β-Propiolactone [57-57-8]
Propylene oxide [75-56-9] (1994)
Propylthiouracil [51-52-5]
Rockwool (1988)
Saccharin [81-07-2]
Safrole [94-59-7]
Schistosoma japonicum (infection with) (1994)
Slagwool (1988)
Sodium o-phenylphenate [132-27-4]
Sterigmatocystin [10048-13-2]
Streptozotocin [18883-66-4]
Styrene [100-42-5] (1994)
Sulfallate [95-06-7]
Tetranitromethane [509-14-8] (1996)
Thioacetamide [62-55-5]
4,4´-Thiodianiline [139-65-1]
Thiourea [62-56-6]
Toluene diisocyanates [26471-62-5]
o-Toluidine [95-53-4]
Trichlormethine (Trimustine hydrochloride) [817-09-4] (1990)
Trp-P-1 (3-Amino-1,4-dimethyl-5H-pyrido[4,3-b]indole) [62450-06-0]
Trp-P-2 (3-Amino-1-methyl-5H-pyrido[4,3-b]indole) [62450-07-1]
Trypan blue [72-57-1]
Uracil mustard [66-75-1]
Urethane [51-79-6]
Vinyl acetate [108-05-4] (1995)
4-Vinylcyclohexene [100-40-3] (1994)
4-Vinylcyclohexene diepoxide [107-87-6] (1994)
Mixtures
Bitumens [8052-42-4], extracts of steam-refined and air-refined
Carrageenan [9000-07-1], degraded
Chlorinated paraffins of average carbon chain length C12 and average degree of chlorination approximately 60% (1990)
Coffee (urinary bladder)9 (1991)
Diesel fuel, marine (1989)
Engine exhaust, gasoline (1989)
Fuel oils, residual (heavy) (1989)
Gasoline (1989)
Pickled vegetables (traditional in Asia) (1993)
Polybrominated biphenyls [Firemaster BP-6, 59536-65-1]
Toxaphene (Polychlorinated camphenes) [8001-35-2]
Toxins derived from Fusarium moniliforme (1993)
Welding fumes (1990)
Exposure circumstances
Carpentry and joinery
Dry cleaning (occupational exposures in) (1995)
Printing processes (occupational exposures in) (1996)
Textile manufacturing industry (work in) (1990)
Group 3—Unclassifiable as to carcinogenicity to humans (480)
Agents and groups of agents
Acridine orange [494-38-2]
Acriflavinium chloride [8018-07-3]
Acrolein [107-02-8]
Acrylic acid [79-10-7]
Acrylic fibres
Acrylonitrile-butadiene-styrene copolymers
Actinomycin D [50-76-0]
Aldicarb [116-06-3] (1991)
Aldrin [309-00-2]
Allyl chloride [107-05-1]
Allyl isothiocyanate [57-06-7]
Allyl isovalerate [2835-39-4]
Amaranth [915-67-3]
5-Aminoacenaphthene [4657-93-6]
2-Aminoanthraquinone [117-79-3]
p-Aminobenzoic acid [150-13-0]
1-Amino-2-methylanthraquinone [82-28-0]
2-Amino-4-nitrophenol [99-57-0] (1993)
2-Amino-5-nitrophenol [121-88-0] (1993)
4-Amino-2-nitrophenol [119-34-6]
2-Amino-5-nitrothiazole [121-66-4]
11-Aminoundecanoic acid [2432-99-7]
Ampicillin [69-53-4] (1990)
Anaesthetics, volatile
Angelicin [523-50-2] plus ultraviolet A radiation
Aniline [62-53-3]
p-Anisidine [104-94-9]
Anthanthrene [191-26-4]
Anthracene [120-12-7]
Anthranilic acid [118-92-3]
Antimony trisulphide [1345-04-6] (1989)
Apholate [52-46-0]
p-Aramid fibrils [24938-64-5] (1997)
Aurothioglucose [12192-57-3]
Aziridine [151-56-4]
2-(1-Aziridinyl)ethanol [1072-52-2]
Aziridyl benzoquinone [800-24-8]
Azobenzene [103-33-3]
Benz[a]acridine [225-11-6]
Benz[c]acridine [225-51-4]
Benzo[ghi]fluoranthene [203-12-3]
Benzo[a]fluorene [238-84-6]
Benzo[b]fluorene [243-17-4]
Benzo[c]fluorene [205-12-9]
Benzo[ghi]perylene [191-24-2]
Benzo[c]phenanthrene [195-19-7]
Benzo[e]pyrene [192-97-2]
p-Benzoquinone dioxime [105-11-3]
Benzoyl chloride [98-88-4]
Benzoyl peroxide [94-36-0]
Benzyl acetate [140-11-4]
Bis(1-aziridinyl)morpholinophosphine sulphide [2168-68-5]
Bis(2-chloroethyl)ether [111-44-4]
1,2-Bis(chloromethoxy)ethane [13483-18-6]
1,4-Bis(chloromethoxymethyl)benzene [56894-91-8]
Bis(2-chloro-1-methylethyl)ether [108-60-1]
Bis(2,3-epoxycyclopentyl)ether [2386-90-5] (1989)
Bisphenol A diglycidyl ether [1675-54-3] (1989)
Bisulphites (1992)
Blue VRS [129-17-9]
Brilliant Blue FCF, disodium salt [3844-45-9]
Bromochloroacetonitrile [83463-62-1] (1991)
Bromoethane [74-96-4] (1991)
Bromoform [75-25-2] (1991)
n-Butyl acrylate [141-32-2]
Butylated hydroxytoluene (BHT) [128-37-0]
Butyl benzyl phthalate [85-68-7]
γ-Butyrolactone [96-48-0]
Caffeine [58-08-2] (1991)
Cantharidin [56-25-7]
Captan [133-06-2]
Carbaryl [63-25-2]
Carbazole [86-74-8]
3-Carbethoxypsoralen [20073-24-9]
Carmoisine [3567-69-9]
Carrageenan [9000-07-1], native
Catechol [120-80-9]
Chloral [75-87-6] (1995)
Chloral hydrate [302-17-0] (1995)
Chlordimeform [6164-98-3]
Chlorinated dibenzodioxins (other than TCDD)
Chlorinated drinking-water (1991)
Chloroacetonitrile [107-14-2] (1991)
Chlorobenzilate [510-15-6]
Chlorodibromomethane [124-48-1] (1991)
Chlorodifluoromethane [75-45-6]
Chloroethane [75-00-3] (1991)
Chlorofluoromethane [593-70-4]
3-Chloro-2-methylpropene [563-47-3] (1995)
4-Chloro-m-phenylenediamine [5131-60-2]
Chloronitrobenzenes [88-73-3; 121-73-3; 100-00-5] (1996)
Chloroprene [126-99-8]
Chloropropham [101-21-3]
Chloroquine [54-05-7]
Chlorothalonil [1897-45-6]
2-Chloro-1,1,1-trifluoroethane [75-88-7]
Cholesterol [57-88-5]
Chromium[III] compounds (1990)
Chromium [7440-47-3], metallic (1990)
Chrysene [218-01-9]
Chrysoidine [532-82-1]
CI Acid Orange 3 [6373-74-6] (1993)
Cimetidine [51481-61-9] (1990)
Cinnamyl anthranilate [87-29-6]
CI Pigment Red 3 [2425-85-6] (1993)
Citrinin [518-75-2]
Clofibrate [637-07-0]
Clomiphene citrate [50-41-9]
Coal dust (1997)
Copper 8-hydroxyquinoline [10380-28-6]
Coronene [191-07-1]
Coumarin [91-64-5]
m-Cresidine [102-50-1]
Crotonaldehyde [4170-30-3] (1995)
Cyclamates [sodium cyclamate, 139-05-9]
Cyclochlorotine [12663-46-6]
Cyclohexanone [108-94-1] (1989)
Cyclopenta[cd]pyrene [27208-37-3]
D & C Red No. 9 [5160-02-1] (1993)
Dapsone [80-08-0]
Decabromodiphenyl oxide [1163-19-5] (1990)
Deltamethrin [52918-63-5] (1991)
Diacetylaminoazotoluene [83-63-6]
Diallate [2303-16-4]
1,2-Diamino-4-nitrobenzene [99-56-9]
1,4-Diamino-2-nitrobenzene [5307-14-2] (1993)
2,5-Diaminotoluene [95-70-5]
Diazepam [439-14-5]
Diazomethane [334-88-3]
Dibenz[a,c]anthracene [215-58-7]
Dibenz[a,j]anthracene [224-41-9]
Dibenzo-p-dioxin (1997)
Dibenzo[a,e]fluoranthene [5385-75-1]
Dibenzo[h,rst]pentaphene [192-47-2]
Dibromoacetonitrile [3252-43-5] (1991)
Dichloroacetic acid [79-43-6] (1995)
Dichloroacetonitrile [3018-12-0] (1991)
Dichloroacetylene [7572-29-4]
o-Dichlorobenzene [95-50-1]
trans-1,4-Dichlorobutene [110-57-6]
2,6-Dichloro-para-phenylenediamine [609-20-1]
1,2-Dichloropropane [78-87-5]
Dicofol [115-32-2]
Dieldrin [60-57-1]
Di(2-ethylhexyl)adipate [103-23-1]
Dihydroxymethylfuratrizine [794-93-4]
Dimethoxane [828-00-2]
3,3´-Dimethoxybenzidine-4,4´-diisocyanate [91-93-0]
p-Dimethylaminoazobenzenediazo sodium sulphonate[140-56-7]
4,4´-Dimethylangelicin [22975-76-4] plus ultraviolet Aradiation
4,5´-Dimethylangelicin [4063-41-6] plus ultraviolet A
N,N-Dimethylaniline [121-69-7] (1993)
Dimethyl hydrogen phosphite [868-85-9] (1990)
1,4-Dimethylphenanthrene [22349-59-3]
1,3-Dinitropyrene [75321-20-9] (1989)
Dinitrosopentamethylenetetramine [101-25-7]
2,4´-Diphenyldiamine [492-17-1]
Disperse Yellow 3 [2832-40-8] (1990)
Disulfiram [97-77-8]
Dithranol [1143-38-0]
Doxefazepam [40762-15-0] (1996)
Droloxifene [82413-20-5] (1996)
Dulcin [150-69-6]
Endrin [72-20-8]
Eosin [15086-94-9]
1,2-Epoxybutane [106-88-7] (1989)
3,4-Epoxy-6-methylcyclohexylmethyl-3,4-epoxy-6-methylcyclohexane carboxylate [141-37-7]
cis-9,10-Epoxystearic acid [2443-39-2]
Estazolam [29975-16-4] (1996)
Ethionamide [536-33-4]
Ethylene [74-85-1] (1994)
Ethylene sulphide [420-12-2]
2-Ethylhexyl acrylate [103-11-7] (1994)
Ethyl selenac [5456-28-0]
Ethyl tellurac [20941-65-5]
Eugenol [97-53-0]
Evans blue [314-13-6]
Fast Green FCF [2353-45-9]
Fenvalerate [51630-58-1] (1991)
Ferbam [14484-64-1]
Ferric oxide [1309-37-1]
Fluometuron [2164-17-2]
Fluoranthene [206-44-0]
Fluorene [86-73-7]
Fluorescent lighting (1992)
Fluorides (inorganic, used in drinking-water)
5-Fluorouracil [51-21-8]
Furazolidone [67-45-8]
Furfural [98-01-1] (1995)
Furosemide (Frusemide) [54-31-9] (1990)
Gemfibrozil [25812-30-0] (1996)
Glass filaments (1988)
Glycidyl oleate [5431-33-4]
Glycidyl stearate [7460-84-6]
Guinea Green B [4680-78-8]
Gyromitrin [16568-02-8]
Haematite [1317-60-8]
HC Blue No. 2 [33229-34-4] (1993)
HC Red No. 3 [2871-01-4] (1993)
HC Yellow No. 4 [59820-43-8] (1993)
Hepatitis D virus (1993)
Hexachlorobutadiene [87-68-3]
Hexachloroethane [67-72-1]
Hexachlorophene [70-30-4]
Human T-cell lymphotropic virus type II (1996)
Hycanthone mesylate [23255-93-8]
Hydralazine [86-54-4]
Hydrochloric acid [7647-01-0] (1992)
Hydrochlorothiazide [58-93-5] (1990)
Hydrogen peroxide [7722-84-1]
Hydroquinone [123-31-9]
4-Hydroxyazobenzene [1689-82-3]
8-Hydroxyquinoline [148-24-3]
Hydroxysenkirkine [26782-43-4]
Hypochlorite salts (1991)
Iron-dextrin complex [9004-51-7]
Iron sorbitol-citric acid complex [1338-16-5]
Isatidine [15503-86-3]
Isonicotinic acid hydrazide (Isoniazid) [54-85-3]
Isophosphamide [3778-73-2]
Isopropanol [67-63-0]
Isopropyl oils
Isosafrole [120-58-1]
Jacobine [6870-67-3]
Kaempferol [520-18-3]
Lauroyl peroxide [105-74-8]
Lead, organo [75-74-1], [78-00-2]
Light Green SF [5141-20-8]
d-Limonene [5989-27-5] (1993)
Luteoskyrin [21884-44-6]
Malathion [121-75-5]
Maleic hydrazide [123-33-1]
Malonaldehyde [542-78-9]
Maneb [12427-38-2]
Mannomustine dihydrochloride [551-74-6]
Medphalan [13045-94-8]
Melamine [108-78-1]
6-Mercaptopurine [50-44-2]
Mercury [7439-97-6] and inorganic mercury compounds (1993)
Metabisulphites (1992)
Methotrexate [59-05-2]
Methoxychlor [72-43-5]
Methyl acrylate [96-33-3]
5-Methylangelicin [73459-03-7] plus ultraviolet A radiation
Methyl bromide [74-83-9]
Methyl carbamate [598-55-0]
Methyl chloride [74-87-3]
1-Methylchrysene [3351-28-8]
2-Methylchrysene [3351-32-4]
3-Methylchrysene [3351-31-3]
4-Methylchrysene [3351-30-2]
6-Methylchrysene [1705-85-7]
N-Methyl-N,4-dinitrosoaniline [99-80-9]
4,4´-Methylenebis(N,N-dimethyl)benzenamine [101-61-1]
4,4´-Methylenediphenyl diisocyanate [101-68-8]
2-Methylfluoranthene [33543-31-6]
3-Methylfluoranthene [1706-01-0]
Methylglyoxal [78-98-8] (1991)
Methyl iodide [74-88-4]
Methyl methacrylate [80-62-6] (1994)
N-Methylolacrylamide [90456-67-0] (1994)
Methyl parathion [298-00-0]
1-Methylphenanthrene [832-69-9]
7-Methylpyrido[3,4-c]psoralen [85878-62-2]
Methyl red [493-52-7]
Methyl selenac [144-34-3]
Modacrylic fibres
Monuron [150-68-5] (1991)
Morpholine [110-91-8] (1989)
Musk ambrette [83-66-9] (1996)
Musk xylene [81-15-2] (1996)
1,5-Naphthalenediamine [2243-62-1]
1,5-Naphthalene diisocyanate [3173-72-6]
1-Naphthylamine [134-32-7]
1-Naphthylthiourea (ANTU) [86-88-4]
Nithiazide [139-94-6]
5-Nitro-o-anisidine [99-59-2]
9-Nitroanthracene [602-60-8]
7-Nitrobenz[a]anthracene [20268-51-3] (1989
6-Nitrobenzo[a]pyrene [63041-90-7] (1989)
4-Nitrobiphenyl [92-93-3]
3-Nitrofluoranthene [892-21-7]
Nitrofural (Nitrofurazone) [59-87-0] (1990)
Nitrofurantoin [67-20-9] (1990)
1-Nitronaphthalene [86-57-7] (1989)
2-Nitronaphthalene [581-89-5] (1989)
3-Nitroperylene [20589-63-3] (1989)
2-Nitropyrene [789-07-1] (1989)
N´-Nitrosoanabasine [37620-20-5]
N-Nitrosoanatabine [71267-22-6]
N-Nitrosodiphenylamine [86-30-6]
p-Nitrosodiphenylamine [156-10-5]
N-Nitrosofolic acid [29291-35-8]
N-Nitrosoguvacine [55557-01-2]
N-Nitrosoguvacoline [55557-02-3]
N-Nitrosohydroxyproline [30310-80-6]
3-(N-Nitrosomethylamino)propionaldehyde [85502-23-4]
4-(N-Nitrosomethylamino)-4-(3-pyridyl)-1-butanal (NNA) [64091-90-3]
N-Nitrosoproline [7519-36-0]
5-Nitro-o-toluidine [99-55-8] (1990)
Nitrovin [804-36-4]
Nylon 6 [25038-54-4]
Oestradiol mustard [22966-79-6]
Oestrogen-progestin replacement therapy
Opisthorchis felineus (infection with) (1994)
Orange I [523-44-4]
Orange G [1936-15-8]
Oxyphenbutazone [129-20-4]
Palygorskite (attapulgite) [12174-11-7] (short fibres, <<5 micro-meters) (1997)
Paracetamol (Acetaminophen) [103-90-2] (1990)
Parasorbic acid [10048-32-5]
Parathion [56-38-2]
Patulin [149-29-1]
Penicillic acid [90-65-3]
Pentachloroethane [76-01-7]
Permethrin [52645-53-1] (1991)
Perylene [198-55-0]
Petasitenine [60102-37-6]
Phenanthrene [85-01-8]
Phenelzine sulphate [156-51-4]
Phenicarbazide [103-03-7]
Phenol [108-95-2] (1989)
Phenylbutazone [50-33-9]
m-Phenylenediamine [108-45-2]
p-Phenylenediamine [106-50-3]
N-Phenyl-2-naphthylamine [135-88-6]
o-Phenylphenol [90-43-7]
Picloram [1918-02-1] (1991)
Piperonyl butoxide [51-03-6]
Polyacrylic acid [9003-01-4]
Polychlorinated dibenzo-p-dioxins (other than 2,3,7,8-tetra-chlorodibenzo-p-dioxin) (1997)
Polychlorinated dibenzofurans (1997)
Polychloroprene [9010-98-4]
Polyethylene [9002-88-4]
Polymethylene polyphenyl isocyanate [9016-87-9]
Polymethyl methacrylate [9011-14-7]
Polypropylene [9003-07-0]
Polystyrene [9003-53-6]
Polytetrafluoroethylene [9002-84-0]
Polyurethane foams [9009-54-5]
Polyvinyl acetate [9003-20-7]
Polyvinyl alcohol [9002-89-5]
Polyvinyl chloride [9002-86-2]
Polyvinyl pyrrolidone [9003-39-8]
Ponceau SX [4548-53-2]
Potassium bis(2-hydroxyethyl)dithiocarbamate[23746-34-1]
Prazepam [2955-38-6] (1996)
Prednimustine [29069-24-7] (1990)
Prednisone [53-03-2]
Proflavine salts
Pronetalol hydrochloride [51-02-5]
Propham [122-42-9]
n-Propyl carbamate [627-12-3]
Propylene [115-07-1] (1994)
Ptaquiloside [87625-62-5]
Pyrene [129-00-0]
Pyrido[3,4-c]psoralen [85878-62-2]
Pyrimethamine [58-14-0]
Quercetin [117-39-5]
p-Quinone [106-51-4]
Quintozene (Pentachloronitrobenzene) [82-68-8]
Reserpine [50-55-5]
Resorcinol [108-46-3]
Retrorsine [480-54-6]
Rhodamine B [81-88-9]
Rhodamine 6G [989-38-8]
Riddelliine [23246-96-0]
Rifampicin [13292-46-1]
Ripazepam [26308-28-1] (1996)
Rugulosin [23537-16-8]
Saccharated iron oxide [8047-67-4]
Scarlet Red [85-83-6]
Schistosoma mansoni (infection with) (1994)
Selenium [7782-49-2] and selenium compounds
Semicarbazide hydrochloride [563-41-7]
Seneciphylline [480-81-9]
Senkirkine [2318-18-5]
Sepiolite [15501-74-3]
Shikimic acid [138-59-0]
Silica [7631-86-9], amorphous
Simazine [122-34-9] (1991)
Sodium chlorite [7758-19-2] (1991)
Sodium diethyldithiocarbamate [148-18-5]
Spironolactone [52-01-7]
Styrene-acrylonitrile copolymers [9003-54-7]
Styrene-butadiene copolymers [9003-55-8]
Succinic anhydride [108-30-5]
Sudan I [842-07-9]
Sudan II [3118-97-6]
Sudan III [85-86-9]
Sudan Brown RR [6416-57-5]
Sudan Red 7B [6368-72-5]
Sulphafurazole (Sulphisoxazole) [127-69-5]
Sulphamethoxazole [723-46-6]
Sulphites (1992)
Sulphur dioxide [7446-09-5] (1992)
Sunset Yellow FCF [2783-94-0]
Symphytine [22571-95-5]
Talc [14807-96-6], not containing asbestiform fibres
Tannic acid [1401-55-4] and tannins
Temazepam [846-50-4] (1996)
2,2´,5,5´-Tetrachlorobenzidine [15721-02-5]
1,1,1,2-Tetrachloroethane [630-20-6]
1,1,2,2-Tetrachloroethane [79-34-5]
Tetrachlorvinphos [22248-79-9]
Tetrafluoroethylene [116-14-3]
Tetrakis(hydroxymethyl)phosphonium salts (1990)
Theobromine [83-67-0] (1991)
Theophylline [58-55-9] (1991)
Thiouracil [141-90-2]
Thiram [137-26-8] (1991)
Titanium dioxide [13463-67-7] (1989)
Toluene [108-88-3] (1989)
Toremifene [89778-26-7] (1996)
Toxins derived from Fusarium graminearum, F. culmorum andF. crookwellense (1993)
Toxins derived from Fusarium sporotrichioides (1993)
Trichlorfon [52-68-6]
Trichloroacetic acid [76-03-9] (1995)
Trichloroacetonitrile [545-06-2] (1991)
1,1,1-Trichloroethane [71-55-6]
1,1,2-Trichloroethane [79-00-5] (1991)
Triethylene glycol diglydicyl ether [1954-28-5]
Trifluralin [1582-09-8] (1991)
4,4´,6-Trimethylangelicin [90370-29-9] plus ultravioletradiation
2,4,5-Trimethylaniline [137-17-7]
2,4,6-Trimethylaniline [88-05-1]
4,5´,8-Trimethylpsoralen [3902-71-4]
2,4,6-Trinitrotoluene [118-96-7] (1996)
Triphenylene [217-59-4]
Tris(aziridinyl)-p-benzoquinone (Triaziquone) [68-76-8]
Tris(1-aziridinyl)phosphine oxide [545-55-1]
2,4,6-Tris(1-aziridinyl)-s-triazine [51-18-3]
Tris(2-chloroethyl)phosphate [115-96-8] (1990)
1,2,3-Tris(chloromethoxy)propane [38571-73-2]
Tris(2-methyl-1-aziridinyl)phosphine oxide [57-39-6]
Vat Yellow 4 [128-66-5] (1990)
Vinblastine sulphate [143-67-9]
Vincristine sulphate [2068-78-2]
Vinyl acetate [108-05-4]
Vinyl chloride-vinyl acetate copolymers [9003-22-9]
Vinylidene chloride [75-35-4]
Vinylidene chloride-vinyl chloride copolymers [9011-06-7]
Vinylidene fluoride [75-38-7]
N-Vinyl-2-pyrrolidone [88-12-0]
Vinyl toluene [25013-15-4] (1994)
Wollastonite [13983-17-0]
Xylene [1330-20-7] (1989)
2,4-Xylidine [95-68-1]
2,5-Xylidine [95-78-3]
Yellow AB [85-84-7]
Yellow OB [131-79-3]
Zectran [315-18-4]
Zeolites [1318-02-1] other than erionite (clinoptilolite,phillipsite, mordenite, non-fibrous Japanese zeolite,synthetic zeolites) (1997)
Zineb [12122-67-7]
Ziram [137-30-4] (1991)
Mixtures
Betel quid, without tobacco
Bitumens [8052-42-4], steam-refined, cracking-residue and air-refined
Crude oil [8002-05-9] (1989)
Diesel fuels, distillate (light) (1989)
Fuel oils, distillate (light) (1989)
Jet fuel (1989)
Mate (1990)
Mineral oils, highly refined
Petroleum solvents (1989)
Printing inks (1996)
Tea (1991)
Terpene polychlorinates (StrobaneR) [8001-50-1]
Exposure circumstances
Flat-glass and specialty glass (manufacture of) (1993)
Hair colouring products (personal use of) (1993)
Leather goods manufacture
Leather tanning and processing
Lumber and sawmill industries (including logging)
Paint manufacture (occupational exposure in) (1989)
Pulp and paper manufacture
Group 4—Probably not carcinogenic to humans (1)
Caprolactam [105-60-2]
The United States Approach to Risk Assessment of Reproductive Toxicants and Neurotoxic Agents
Neurotoxicity and reproductive toxicity are important areas for risk assessment, since the nervous and reproductive systems are highly sensitive to xenobiotic effects. Many agents have been identified as toxic to these systems in humans (Barlow and Sullivan 1982; OTA 1990). Many pesticides are deliberately designed to disrupt reproduction and neurological function in target organisms, such as insects, through interference with hormonal biochemistry and neurotransmission.
It is difficult to identify substances potentially toxic to these systems for three interrelated reasons: first, these are among the most complex biological systems in humans, and animal models of reproductive and neurological function are generally acknowledged to be inadequate for representing such critical events as cognition or early embryofoetal development; second, there are no simple tests for identifying potential reproductive or neurological toxicants; and third, these systems contain multiple cell types and organs, such that no single set of mechanisms of toxicity can be used to infer dose-response relationships or predict structure-activity relationships (SAR). Moreover, it is known that the sensitivity of both the nervous and reproductive systems varies with age, and that exposures at critical periods may have much more severe effects than at other times.
Neurotoxicity Risk Assessment
Neurotoxicity is an important public health problem. As shown in table 1, there have been several episodes of human neurotoxicity involving thousands of workers and other populations exposed through industrial releases, contaminated food, water and other vectors. Occupational exposures to neurotoxins such as lead, mercury, organophosphate insecticides and chlorinated solvents are widespread throughout the world (OTA 1990; Johnson 1978).
Table 1. Selected major neurotoxicity incidents
| Year(s) | Location | Substance | Comments |
| 400 BC | Rome | Lead | Hippocrates recognizes lead toxicity in the mining industry. |
| 1930s | United States (Southeast) | TOCP | Compound often added to lubricating oils contaminates “Ginger Jake,” an alcoholic beverage; more than 5,000 paralyzed, 20,000 to 100,000 affected. |
| 1930s | Europe | Apiol (with TOCP) | Abortion-inducing drug containing TOCP causes 60 cases of neuropathy. |
| 1932 | United States (California) | Thallium | Barley laced with thallium sulphate, used as rodenticide, is stolen and used to make tortillas; 13 family members hospitalized with neurological symptoms; 6 deaths. |
| 1937 | South Africa | TOCP | 60 South Africans develop paralysis after using contaminated cooking oil. |
| 1946 | — | Tetraethyl lead | More than 25 individuals suffer neurological effects after cleaning gasoline tanks. |
| 1950s | Japan (Minimata) | Mercury | Hundreds ingest fish and shellfish contaminated with mercury from chemical plant; 121 poisoned, 46 deaths, many infants with serious nervous system damage. |
| 1950s | France | Organotin | Contamination of Stallinon with triethyltin results in more than 100 deaths. |
| 1950s | Morocco | Manganese | 150 ore miners suffer chronic manganese intoxication involving severe neurobehavioural problems. |
| 1950s-1970s | United States | AETT | Component of fragrances found to be neurotoxic; withdrawn from market in 1978; human health effects unknown. |
| 1956 | — | Endrin | 49 persons become ill after eating bakery foods prepared from flour contaminated with the insecticide endrin; convulsions result in some instances. |
| 1956 | Turkey | HCB | Hexachlorobenzene, a seed grain fungicide, leads to poisoning of 3,000 to 4,000; 10 per cent mortality rate. |
| 1956-1977 | Japan | Clioquinol | Drug used to treat travellers’ diarrhoea found to cause neuropathy; as many as 10,000 affected over two decades. |
| 1959 | Morocco | TOCP | Cooking oil contaminated with lubricating oil affects some 10,000 individuals. |
| 1960 | Iraq | Mercury | Mercury used as fungicide to treat seed grain used in bread; more than 1,000 people affected. |
| 1964 | Japan | Mercury | Methylmercury affects 646 people. |
| 1968 | Japan | PCBs | Polychlorinated biphenyls leaked into rice oil; 1,665 people affected. |
| 1969 | Japan | n-Hexane | 93 cases of neuropathy occur following exposure to n-hexane, used to make vinyl sandals. |
| 1971 | United States | Hexachlorophene | After years of bathing infants in 3 per cent hexachlorophene, the disinfectant is found to be toxic to the nervous system and other systems. |
| 1971 | Iraq | Mercury | Mercury used as fungicide to treat seed grain is used in bread; more than 5,000 severe poisonings, 450 hospital deaths, effects on many infants exposedprenatally not documented. |
| 1973 | United States (Ohio) | MIBK | Fabric production plant employees exposed to solvent; more than 80 workers suffer neuropathy, 180 have less severe effects. |
| 1974-1975 | United States (Hopewell, VA) | Chlordecone (Kepone) | Chemical plant employees exposed to insecticide; more than 20 suffer severe neurologicalproblems, more than 40 have less severe problems. |
| 1976 | United States (Texas) | Leptophos (Phosvel) | At least 9 employees suffer severe neurological problems following exposure to insecticide during manufacturing process. |
| 1977 | United States (California) | Dichloropropene (Telone II) | 24 individuals hospitalized after exposure to pesticide Telone following traffic accident. |
| 1979-1980 | United States (Lancaster, TX) | BHMH (Lucel-7) | Seven employees at plastic bathtub manufacturing plant experience serious neurologicalproblems following exposure to BHMH. |
| 1980s | United States | MPTP | Impurity in synthesis of illicit drug found to cause symptoms identical to those of Parkinson’s disease. |
| 1981 | Spain | Contaminated toxic oil | 20,000 persons poisoned by toxic substance in oil, resulting in more than 500 deaths; many suffer severe neuropathy. |
| 1985 | United States and Canada | Aldicarb | More than 1,000 individuals in California and other Western States and British Columbia experience neuromuscular and cardiac problems following ingestion of melons contaminated with the pesticide aldicarb. |
| 1987 | Canada | Domoic acid | Ingestion of mussels contaminated with domoic acid causes 129 illnesses and 2 deaths; symptoms include memory loss, disorientation and seizures. |
Source: OTA 1990.
Chemicals may affect the nervous system through actions at any of several cellular targets or biochemical processes within the central or peripheral nervous system. Toxic effects on other organs may also affect the nervous system, as in the example of hepatic encephalopathy. The manifestations of neurotoxicity include effects on learning (including memory, cognition and intellectual performance), somatosensory processes (including sensation and proprioreception), motor function (including balance, gait and fine movement control), affect (including personality status and emotionality) and autonomic function (nervous control of endocrine function and internal organ systems). The toxic effects of chemicals upon the nervous system often vary in sensitivity and expression with age: during development, the central nervous system may be especially susceptible to toxic insult because of the extended process of cellular differentiation, migration, and cell-to-cell contact that takes place in humans (OTA 1990). Moreover, cytotoxic damage to the nervous system may be irreversible because neurons are not replaced after embryogenesis. While the central nervous system (CNS) is somewhat protected from contact with absorbed compounds through a system of tightly joined cells (the blood-brain barrier, composed of capillary endothelial cells that line the vasculature of the brain), toxic chemicals can gain access to the CNS by three mechanisms: solvents and lipophilic compounds can pass through cell membranes; some compounds can attach to endogenous transporter proteins that serve to supply nutrients and biomolecules to the CNS; small proteins if inhaled can be directly taken up by the olfactory nerve and transported to the brain.
US regulatory authorities
Statutory authority for regulating substances for neurotoxicity is assigned to four agencies in the United States: the Food and Drug Administration (FDA), the Environmental Protection Agency (EPA), the Occupational Safety and Health Administration (OSHA), and the Consumer Product Safety Commission (CPSC). While OSHA generally regulates occupational exposures to neurotoxic (and other) chemicals, the EPA has authority to regulate occupational and nonoccupational exposures to pesticides under the Federal Insecticide, Fungicide and Rodenticide Act (FIFRA). EPA also regulates new chemicals prior to manufacture and marketing, which obligates the agency to consider both occupational and nonoccupational risks.
Hazard identification
Agents that adversely affect the physiology, biochemistry, or structural integrity of the nervous system or nervous system function expressed behaviourally are defined as neurotoxic hazards (EPA 1993). The determination of inherent neurotoxicity is a difficult process, owing to the complexity of the nervous system and the multiple expressions of neurotoxicity. Some effects may be delayed in appearance, such as the delayed neurotoxicity of certain organophosphate insecticides. Caution and judgement are required in determining neurotoxic hazard, including consideration of the conditions of exposure, dose, duration and timing.
Hazard identification is usually based upon toxicological studies of intact organisms, in which behavioural, cognitive, motor and somatosensory function is assessed with a range of investigative tools including biochemistry, electrophysiology and morphology (Tilson and Cabe 1978; Spencer and Schaumberg 1980). The importance of careful observation of whole organism behaviour cannot be overemphasized. Hazard identification also requires evaluation of toxicity at different developmental stages, including early life (intrauterine and early neonatal) and senescence. In humans, the identification of neurotoxicity involves clinical evaluation using methods of neurological assessment of motor function, speech fluency, reflexes, sensory function, electrophysiology, neuropsychological testing, and in some cases advanced techniques of brain imaging and quantitative electroencephalography. WHO has developed and validated a neurobehavioural core test battery (NCTB), which contains probes of motor function, hand-eye coordination, reaction time, immediate memory, attention and mood. This battery has been validated internationally by a coordinated process (Johnson 1978).
Hazard identification using animals also depends upon careful observational methods. The US EPA has developed a functional observational battery as a first-tier test designed to detect and quantify major overt neurotoxic effects (Moser 1990). This approach is also incorporated in the OECD subchronic and chronic toxicity testing methods. A typical battery includes the following measures: posture; gait; mobility; general arousal and reactivity; presence or absence of tremor, convulsions, lacrimation, piloerection, salivation, excess urination or defecation, stereotypy, circling, or other bizarre behaviours. Elicited behaviours include response to handling, tail pinch, or clicks; balance, righting reflex, and hind limb grip strength. Some representative tests and agents identified with these tests are shown in table 2.
Table 2. Examples of specialized tests to measure neurotoxicity
| Function | Procedure | Representative agents |
| Neuromuscular | ||
| Weakness | Grip strength; swimming endurance; suspension from rod; discriminative motor function; hind limb splay | n-Hexane, Methylbutylketone, Carbaryl |
| Incoordination | Rotorod, gait measurements | 3-Acetylpyridine, Ethanol |
| Tremor | Rating scale, spectral analysis | Chlordecone, Type I Pyrethroids, DDT |
| Myoclonia, spasms | Rating scale, spectral analysis | DDT, Type II Pyrethroids |
| Sensory | ||
| Auditory | Discriminant conditioning, reflex modification | Toluene, Trimethyltin |
| Visual toxicity | Discriminant conditioning | Methyl mercury |
| Somatosensory toxicity | Discriminant conditioning | Acrylamide |
| Pain sensitivity | Discriminant conditioning (btration); functional observational battery | Parathion |
| Olfactory toxicity | Discriminant conditioning | 3-Methylindole methylbromide |
| Learning, memory | ||
| Habituation | Startle reflex | Diisopropylfluorophosphate (DFP) |
| Classical conditioning | Nictitating membrane, conditioned flavour aversion, passive avoidance, olfactory conditioning | Aluminium, Carbaryl, Trimethyltin, IDPN, Trimethyltin (neonatal) |
| Operant or instrumental conditioning | One-way avoidance, Two-way avoidance, Y-maze avoidance, Biol watermaze, Morris water maze, Radial arm maze, Delayed matching to sample, Repeated acquisition, Visual discrimination learning | Chlordecone, Lead (neonatal), Hypervitaminosis A, Styrene, DFP, Trimethyltin, DFP. Carbaryl, Lead |
Source: EPA 1993.
These tests may be followed by more complex assessments usually reserved for mechanistic studies rather than hazard identification. In vitro methods for neurotoxicity hazard identification are limited since they do not provide indications of effects on complex function, such as learning, but they may be very useful in defining target sites of toxicity and improving the precision of target site dose-response studies (see WHO 1986 and EPA 1993 for comprehensive discussions of principles and methods for identifying potential neurotoxicants).
Dose-response assessment
The relationship between toxicity and dose may be based upon human data when available or upon animal tests, as described above. In the United States, an uncertainty or safety factor approach is generally used for neurotoxicants. This process involves determining a “no observed adverse effect level” (NOAEL) or “lowest observed adverse effect level” (LOAEL) and then dividing this number by uncertainty or safety factors (usually multiples of 10) to allow for such considerations as incompleteness of data, potentially higher sensitivity of humans and variability of human response due to age or other host factors. The resultant number is termed the reference dose (RfD) or reference concentration (RfC). The effect occurring at the lowest dose in the most sensitive animal species and gender is generally used to determine the LOAEL or NOAEL. Conversion of animal dose to human exposure is done by standard methods of cross-species dosimetry, taking into account differences in lifespan and exposure duration.
The use of the uncertainty factor approach assumes that there is a threshold, or dose below which no adverse effect is induced. Thresholds for specific neurotoxicants may be difficult to determine experimentally; they are based upon assumptions as to mechanism of action which may or may not hold for all neurotoxicants (Silbergeld 1990).
Exposure assessment
At this stage, information is evaluated on sources, routes, doses and durations of exposure to the neurotoxicant for human populations, subpopulations or even individuals. This information may be derived from monitoring of environmental media or human sampling, or from estimates based upon standard scenarios (such as workplace conditions and job descriptions) or models of environmental fate and dispersion (see EPA 1992 for general guidelines on exposure assessment methods). In some limited cases, biological markers may be used to validate exposure inferences and estimates; however, there are relatively few usable biomarkers of neurotoxicants.
Risk characterization
The combination of hazard identification, dose-response and exposure assessment is used to develop the risk characterization. This process involves assumptions as to the extrapolation of high to low doses, extrapolation from animals to humans, and the appropriateness of threshold assumptions and use of uncertainty factors.
Reproductive Toxicology—Risk Assessment Methods
Reproductive hazards may affect multiple functional endpoints and cellular targets within humans, with consequences for the health of the affected individual and future generations. Reproductive hazards may affect the development of the reproductive system in males or females, reproductive behaviours, hormonal function, the hypothalamus and pituitary, gonads and germ cells, fertility, pregnancy and the duration of reproductive function (OTA 1985). In addition, mutagenic chemicals may also affect reproductive function by damaging the integrity of germ cells (Dixon 1985).
The nature and extent of adverse effects of chemical exposures upon reproductive function in human populations is largely unknown. Relatively little surveillance information is available on such endpoints as fertility of men or women, age of menopause in women, or sperm counts in men. However, both men and women are employed in industries where exposures to reproductive hazards may occur (OTA 1985).
This section does not recapitulate those elements common to both neurotoxicant and reproductive toxicant risk assessment, but focuses upon issues specific to reproductive toxicant risk assessment. As with neurotoxicants, authority to regulate chemicals for reproductive toxicity is placed by statute in the EPA, OSHA, the FDA and the CPSC. Of these agencies, only the EPA has a stated set of guidelines for reproductive toxicity risk assessment. In addition, the state of California has developed methods for reproductive toxicity risk assessment in response to a state law, Proposition 65 (Pease et al. 1991).
Reproductive toxicants, like neurotoxicants, may act by affecting any of a number of target organs or molecular sites of action. Their assessment has additional complexity because of the need to evaluate three distinct organisms separately and together—the male, the female and the offspring (Mattison and Thomford 1989). While an important endpoint of reproductive function is the generation of a healthy child, reproductive biology also plays a role in the health of developing and mature organisms regardless of their involvement in procreation. For instance, loss of ovulatory function through natural depletion or surgical removal of oocytes has substantial effects upon the health of women, involving changes in blood pressure, lipid metabolism and bone physiology. Changes in hormone biochemistry may affect susceptibility to cancer.
Hazard identification
The identification of a reproductive hazard may be made on the basis of human or animal data. In general, data from humans are relatively sparse, owing to the need for careful surveillance to detect alterations in reproductive function, such as sperm count or quality, ovulatory frequency and cycle length, or age at puberty. Detecting reproductive hazards through collection of information on fertility rates or data on pregnancy outcome may be confounded by the intentional suppression of fertility exercised by many couples through family-planning measures. Careful monitoring of selected populations indicates that rates of reproductive failure (miscarriage) may be very high, when biomarkers of early pregnancy are assessed (Sweeney et al. 1988).
Testing protocols using experimental animals are widely used to identify reproductive toxicants. In most of these designs, as developed in the United States by the FDA and the EPA and internationally by the OECD test guidelines program, the effects of suspect agents are detected in terms of fertility after male and/or female exposure; observation of sexual behaviours related to mating; and histopathological examination of gonads and accessory sex glands, such as mammary glands (EPA 1994). Often reproductive toxicity studies involve continuous dosing of animals for one or more generations in order to detect effects on the integrated reproductive process as well as to study effects on specific organs of reproduction. Multigenerational studies are recommended because they permit detection of effects that may be induced by exposure during the development of the reproductive system in utero. A special test protocol, the Reproductive Assessment by Continuous Breeding (RACB), has been developed in the United States by the National Toxicology Program. This test provides data on changes in the temporal spacing of pregnancies (reflecting ovulatory function), as well as number and size of litters over the entire test period. When extended to the lifetime of the female, it can yield information on early reproductive failure. Sperm measures can be added to the RACB to detect changes in male reproductive function. A special test to detect pre- or postimplantation loss is the dominant lethal test, designed to detect mutagenic effects in male spermatogenesis.
In vitro tests have also been developed as screens for reproductive (and developmental) toxicity (Heindel and Chapin 1993). These tests are generally used to supplement in vivo test results by providing more information on target site and mechanism of observed effects.
Table 3 shows the three types of endpoints in reproductive toxicity assessment—couple-mediated, female-specific and male-specific. Couple-mediated endpoints include those detectable in multigenerational and single-organism studies. They generally include assessment of offspring as well. It should be noted that fertility measurement in rodents is generally insensitive, as compared to such measurement in humans, and that adverse effects on reproductive function may well occur at lower doses than those that significantly affect fertility (EPA 1994). Male-specific endpoints can include dominant lethality tests as well as histopathological evaluation of organs and sperm, measurement of hormones, and markers of sexual development. Sperm function can also be assessed by in vitro fertilization methods to detect germ cell properties of penetration and capacitation; these tests are valuable because they are directly comparable to in vitro assessments conducted in human fertility clinics, but they do not by themselves provide dose-response information. Female-specific endpoints include, in addition to organ histopathology and hormone measurements, assessment of the sequelae of reproduction, including lactation and offspring growth.
Table 3. Endpoints in reproductive toxicology
| Couple-mediated endpoints | |
| Multigenerational studies | Other reproductive endpoints |
| Mating rate, time to mating (time to pregnancy1) Pregnancy rate1 Delivery rate1 Gestation length1 Litter size (total and live) Number of live and dead offspring (foetal death rate1) Offspring gender1 Birth weight1 Postnatal weights1 Offspring survival1 External malformations and variations1 Offspring reproduction1 |
Ovulation rate Fertilization rate Preimplantation loss Implantation number Postimplantation loss1 Internal malformations and variations1 Postnatal structural and functional development1 |
| Male-specific endpoints | |
| Organ weights Visual examination and histopathology Sperm evaluation1 Hormone levels1 Developmental |
Testes, epididymides, seminal vesicles, prostate, pituitary Testes, epididymides, seminal vesicles, prostate, pituitary Sperm number (count) and quality (morphology, motility) Luteinizing hormone, follicle stimulating hormone, testosterone, oestrogen, prolactin Testis descent1, preputial separation, sperm production1, ano-genital distance, normality of external genitalia1 |
| Female-specific endpoints | |
| Body weight Organ weights Visual examination and histopathology Oestrous (menstrual1) cycle normality Hormone levels1 Lactation1 Development Senescence (menopause1) |
Ovary, uterus, vagina, pituitary Ovary, uterus, vagina, pituitary, oviduct, mammary gland Vaginal smear cytology LH, FSH, oestrogen, progesterone, prolactin Offspring growth Normality of external genitalia1, vaginal opening, vaginal smear cytology, onset of oestrus behaviour (menstruation1) Vaginal smear cytology, ovarian histology |
1 Endpoints that can be obtained relatively noninvasively with humans.
Source: EPA 1994.
In the United States, the hazard identification concludes with a qualitative evaluation of toxicity data by which chemicals are judged to have either sufficient or insufficient evidence of hazard (EPA 1994). “Sufficient” evidence includes epidemiological data providing convincing evidence of a causal relationship (or lack thereof), based upon case-control or cohort studies, or well-supported case series. Sufficient animal data may be coupled with limited human data to support a finding of a reproductive hazard: to be sufficient, the experimental studies are generally required to utilize EPA’s two-generation test guidelines, and must include a minimum of data demonstrating an adverse reproductive effect in an appropriate, well-conducted study in one test species. Limited human data may or may not be available; it is not necessary for the purposes of hazard identification. To rule out a potential reproductive hazard, the animal data must include an adequate array of endpoints from more than one study showing no adverse reproductive effect at doses minimally toxic to the animal (EPA 1994).
Dose-response assessment
As with the evaluation of neurotoxicants, the demonstration of dose-related effects is an important part of risk assessment for reproductive toxicants. Two particular difficulties in dose-response analyses arise due to complicated toxicokinetics during pregnancy, and the importance of distinguishing specific reproductive toxicity from general toxicity to the organism. Debilitated animals, or animals with substantial nonspecific toxicity (such as weight loss) may fail to ovulate or mate. Maternal toxicity can affect the viability of pregnancy or support for lactation. These effects, while evidence of toxicity, are not specific to reproduction (Kimmel et al. 1986). Assessing dose response for a specific endpoint, such as fertility, must be done in the context of an overall assessment of reproduction and development. Dose-response relationships for different effects may differ significantly, but interfere with detection. For instance, agents that reduce litter size may result in no effects upon litter weight because of reduced competition for intrauterine nutrition.
Exposure assessment
An important component of exposure assessment for reproductive risk assessment relates to information on the timing and duration of exposures. Cumulative exposure measures may be insufficiently precise, depending upon the biological process that is affected. It is known that exposures at different developmental stages in males and females can result in different outcomes in both humans and experimental animals (Gray et al. 1988). The temporal nature of spermatogenesis and ovulation also affects outcome. Effects on spermatogenesis may be reversible if exposures cease; however, oocyte toxicity is not reversible since females have a fixed set of germ cells to draw upon for ovulation (Mattison and Thomford 1989).
Risk characterization
As with neurotoxicants, the existence of a threshold is usually assumed for reproductive toxicants. However, the actions of mutagenic compounds on germ cells may be considered an exception to this general assumption. For other endpoints, an RfD or RfC is calculated as with neurotoxicants by determination of the NOAEL or LOAEL and application of appropriate uncertainty factors. The effect used for determining the NOAEL or LOAEL is the most sensitive adverse reproductive endpoint from the most appropriate or most sensitive mammalian species (EPA 1994). Uncertainty factors include consideration of interspecies and intraspecies variation, ability to define a true NOAEL, and sensitivity of the endpoint detected.
Risk characterizations should also be focused upon specific subpopulations at risk, possibly specifying males and females, pregnancy status, and age. Especially sensitive individuals, such as lactating women, women with reduced oocyte numbers or men with reduced sperm counts, and prepubertal adolescents may also be considered.
Approaches to Hazard Identification: IARC
The identification of carcinogenic risks to humans has been the objective of the IARC Monographs on the Evaluation of Carcinogenic Risks to Humans since 1971. To date, 69 volumes of monographs have been published or are in press, with evaluations of carcinogenicity of 836 agents or exposure circumstances (see Appendix).
These qualitative evaluations of carcinogenic risk to humans are equivalent to the hazard identification phase in the now generally accepted scheme of risk assessment, which involves identification of hazard, dose-response assessment (including extrapolation outside the limits of observations), exposure assessment and risk characterization.
The aim of the IARC Monographs programme has been to publish critical qualitative evaluations on the carcinogenicity to humans of agents (chemicals, groups of chemicals, complex mixtures, physical or biological factors) or exposure circumstances (occupational exposures, cultural habits) through international cooperation in the form of expert working groups. The working groups prepare monographs on a series of individual agents or exposures and each volume is published and widely distributed. Each monograph consists of a brief description of the physical and chemical properties of the agent; methods for its analysis; a description of how it is produced, how much is produced, and how it is used; data on occurrence and human exposure; summaries of case reports and epidemiological studies of cancer in humans; summaries of experimental carcinogenicity tests; a brief description of other relevant biological data, such as toxicity and genetic effects, that may indicate its possible mechanism of action; and an evaluation of its carcinogenicity. The first part of this general scheme is adjusted appropriately when dealing with agents other than chemicals or chemical mixtures.
The guiding principles for evaluating carcinogens have been drawn up by various ad-hoc groups of experts and are laid down in the Preamble to the Monographs (IARC 1994a).
Tools for Qualitative Carcinogenic Risk (Hazard) Identification
Associations are established by examining the available data from studies of exposed humans, the results of bioassays in experimental animals and studies of exposure, metabolism, toxicity and genetic effects in both humans and animals.
Studies of cancer in humans
Three types of epidemiological studies contribute to an assessment of carcinogenicity: cohort studies, case-control studies and correlation (or ecological) studies. Case reports of cancer may also be reviewed.
Cohort and case-control studies relate individual exposures under study to the occurrence of cancer in individuals and provide an estimate of relative risk (ratio of the incidence in those exposed to the incidence in those not exposed) as the main measure of association.
In correlation studies, the unit of investigation is usually whole populations (e.g., particular geographical areas) and cancer frequency is related to a summary measure of the exposure of the population to the agent. Because individual exposure is not documented, a causal relationship is less easy to infer from such studies than from cohort and case-control studies. Case reports generally arise from a suspicion, based on clinical experience, that the concurrence of two events—that is, a particular exposure and occurrence of a cancer—has happened rather more frequently than would be expected by chance. The uncertainties surrounding interpretation of case reports and correlation studies make them inadequate, except in rare cases, to form the sole basis for inferring a causal relationship.
In the interpretation of epidemiological studies, it is necessary to take into account the possible roles of bias and confounding. By bias is meant the operation of factors in study design or execution that lead erroneously to a stronger or weaker association than in fact exists between disease and an agent. By confounding is meant a situation in which the relationship with disease is made to appear stronger or weaker than it truly is as a result of an association between the apparent causal factor and another factor that is associated with either an increase or decrease in the incidence of the disease.
In the assessment of the epidemiological studies, a strong association (i.e., a large relative risk) is more likely to indicate causality than a weak association, although it is recognized that relative risks of small magnitude do not imply lack of causality and may be important if the disease is common. Associations that are replicated in several studies of the same design or using different epidemiological approaches or under different circumstances of exposure are more likely to represent a causal relationship than isolated observations from single studies. An increase in risk of cancer with increasing amounts of exposure is considered to be a strong indication of causality, although the absence of a graded response is not necessarily evidence against a causal relationship. Demonstration of a decline in risk after cessation of or reduction in exposure in individuals or in whole populations also supports a causal interpretation of the findings.
When several epidemiological studies show little or no indication of an association between an exposure and cancer, the judgement may be made that, in the aggregate, they show evidence suggesting lack of carcinogenicity. The possibility that bias, confounding or misclassification of exposure or outcome could explain the observed results must be considered and excluded with reasonable certainty. Evidence suggesting lack of carcinogenicity obtained from several epidemiological studies can apply only to those type(s) of cancer, dose levels and intervals between first exposure and observation of disease that were studied. For some human cancers, the period between first exposure and the development of clinical disease is seldom less than 20 years; latent periods substantially shorter than 30 years cannot provide evidence suggesting lack of carcinogenicity.
The evidence relevant to carcinogenicity from studies in humans is classified into one of the following categories:
Sufficient evidence of carcinogenicity. A causal relationship has been established between exposure to the agent, mixture or exposure circumstance and human cancer. That is, a positive relationship has been observed between the exposure and cancer in studies in which chance, bias and confounding could be ruled out with reasonable confidence.
Limited evidence of carcinogenicity. A positive association has been observed between exposure to the agent, mixture or exposure circumstance and cancer for which a causal interpretation is considered to be credible, but chance, bias or confounding cannot be ruled out with reasonable confidence.
Inadequate evidence of carcinogenicity. The available studies are of insufficient quality, consistency or statistical power to permit a conclusion regarding the presence or absence of a causal association, or no data on cancer in humans are available.
Evidence suggesting lack of carcinogenicity. There are several adequate studies covering the full range of levels of exposure that human beings are known to encounter, which are mutually consistent in not showing a positive association between exposure to the agent and the studied cancer at any observed level of exposure. A conclusion of “evidence suggesting lack of carcinogenicity” is inevitably limited to the cancer sites, conditions and levels of exposure and length of observation covered by the available studies.
The applicability of an evaluation of the carcinogenicity of a mixture, process, occupation or industry on the basis of evidence from epidemiological studies depends on time and place. The specific exposure, process or activity considered most likely to be responsible for any excess risk should be sought and the evaluation focused as narrowly as possible. The long latent period of human cancer complicates the interpretation of epidemiological studies. A further complication is the fact that humans are exposed simultaneously to a variety of chemicals, which can interact either to increase or decrease the risk for neoplasia.
Studies on carcinogenicity in experimental animals
Studies in which experimental animals (usually mice and rats) are exposed to potential carcinogens and examined for evidence of cancer were introduced about 50 years ago with the aim of introducing a scientific approach to the study of chemical carcinogenesis and to avoid some of the disadvantages of using only epidemiological data in humans. In the IARC Monographs all available, published studies of carcinogenicity in animals are summarized, and the degree of evidence of carcinogenicity is then classified into one of the following categories:
Sufficient evidence of carcinogenicity. A causal relationship has been established between the agent or mixture and an increased incidence of malignant neoplasms or of an appropriate combination of benign and malignant neoplasms in two or more species of animals or in two or more independent studies in one species carried out at different times or in different laboratories or under different protocols. Exceptionally, a single study in one species might be considered to provide sufficient evidence of carcinogenicity when malignant neoplasms occur to an unusual degree with regard to incidence, site, type of tumour or age at onset.
Limited evidence of carcinogenicity. The data suggest a carcinogenic effect but are limited for making a definitive evaluation because, for example, (a) the evidence of carcinogenicity is restricted to a single experiment; or (b) there are some unresolved questions regarding the adequacy of the design, conduct or interpretation of the study; or (c) the agent or mixture increases the incidence only of benign neoplasms or lesions of uncertain neoplastic potential, or of certain neoplasms which may occur spontaneously in high incidences in certain strains.
Inadequate evidence of carcinogenicity. The studies cannot be interpreted as showing either the presence or absence of a carcinogenic effect because of major qualitative or quantitative limitations, or no data on cancer in experimental animals are available.
Evidence suggesting lack of carcinogenicity. Adequate studies involving at least two species are available which show that, within the limits of the tests used, the agent or mixture is not carcinogenic. A conclusion of evidence suggesting lack of carcinogenicity is inevitably limited to the species, tumour sites and levels of exposure studied.
Other data relevant to an evaluationof carcinogenicity
Data on biological effects in humans that are of particular relevance include toxicological, kinetic and metabolic considerations and evidence of DNA binding, persistence of DNA lesions or genetic damage in exposed humans. Toxicological information, such as that on cytotoxicity and regeneration, receptor binding and hormonal and immunological effects, and data on kinetics and metabolism in experimental animals are summarized when considered relevant to the possible mechanism of the carcinogenic action of the agent. The results of tests for genetic and related effects are summarized for whole mammals including man, cultured mammalian cells and nonmammalian systems. Structure-activity relationships are mentioned when relevant.
For the agent, mixture or exposure circumstance being evaluated, the available data on end-points or other phenomena relevant to mechanisms of carcinogenesis from studies in humans, experimental animals and tissue and cell test systems are summarized within one or more of the following descriptive dimensions:
- evidence of genotoxicity (i.e., structural changes at the level of the gene): for example, structure-activity considerations, adduct formation, mutagenicity (effect on specific genes), chromosomal mutation or aneuploidy
- evidence of effects on the expression of relevant genes (i.e., functional changes at the intracellular level): for example, alterations to the structure or quantity of the product of a proto-oncogene or tumour suppressor gene, alterations to metabolic activation, inactivation or DNA repair
- evidence of relevant effects on cell behaviour (i.e., morphological or behavioural changes at the cellular or tissue level): for example, induction of mitogenesis, compensatory cell proliferation, preneoplasia and hyperplasia, survival of premalignant or malignant cells (immortalization, immunosuppression), effects on metastatic potential
- evidence from dose and time relationships of carcinogenic effects and interactions between agents: for example, early versus late stage, as inferred from epidemiological studies; initiation, promotion, progression or malignant conversion, as defined in animal carcinogenicity experiments; toxicokinetics.
These dimensions are not mutually exclusive, and an agent may fall within more than one. Thus, for example, the action of an agent on the expression of relevant genes could be summarized under both the first and second dimension, even if it were known with reasonable certainty that those effects resulted from genotoxicity.
Overall evaluations
Finally, the body of evidence is considered as a whole, in order to reach an overall evaluation of the carcinogenicity to humans of an agent, mixture or circumstance of exposure. An evaluation may be made for a group of chemicals when supporting data indicate that other, related compounds for which there is no direct evidence of capacity to induce cancer in humans or in animals may also be carcinogenic, a statement describing the rationale for this conclusion is added to the evaluation narrative.
The agent, mixture or exposure circumstance is described according to the wording of one of the following categories, and the designated group is given. The categorization of an agent, mixture or exposure circumstance is a matter of scientific judgement, reflecting the strength of the evidence derived from studies in humans and in experimental animals and from other relevant data.
Group 1
The agent (mixture) is carcinogenic to humans. The exposure circumstance entails exposures that are carcinogenic to humans.
This category is used when there is sufficient evidence of carcinogenicity in humans. Exceptionally, an agent (mixture) may be placed in this category when evidence in humans is less than sufficient but there is sufficient evidence of carcinogenicity in experimental animals and strong evidence in exposed humans that the agent (mixture) acts through a relevant mechanism of carcinogenicity.
Group 2
This category includes agents, mixtures and exposure circumstances for which, at one extreme, the degree of evidence of carcinogenicity in humans is almost sufficient, as well as those for which, at the other extreme, there are no human data but for which there is evidence of carcinogenicity in experimental animals. Agents, mixtures and exposure circumstances are assigned to either group 2A (probably carcinogenic to humans) or group 2B (possibly carcinogenic to humans) on the basis of epidemiological and experimental evidence of carcinogenicity and other relevant data.
Group 2A. The agent (mixture) is probably carcinogenic to humans. The exposure circumstance entails exposures that are probably carcinogenic to humans. This category is used when there is limited evidence of carcinogenicity in humans and sufficient evidence of carcinogenicity in experimental animals. In some cases, an agent (mixture) may be classified in this category when there is inadequate evidence of carcinogenicity in humans and sufficient evidence of carcinogenicity in experimental animals and strong evidence that the carcinogenesis is mediated by a mechanism that also operates in humans. Exceptionally, an agent, mixture or exposure circumstance may be classified in this category solely on the basis of limited evidence of carcinogenicity in humans.
Group 2B. The agent (mixture) is possibly carcinogenic to humans. The exposure circumstance entails exposures that are possibly carcinogenic to humans. This category is used for agents, mixtures and exposure circumstances for which there is limited evidence of carcinogenicity in humans and less than sufficient evidence of carcinogenicity in experimental animals. It may also be used when there is inadequate evidence of carcinogenicity in humans but there is sufficient evidence of carcinogenicity in experimental animals. In some instances, an agent, mixture or exposure circumstance for which there is inadequate evidence of carcinogenicity in humans but limited evidence of carcinogenicity in experimental animals together with supporting evidence from other relevant data may be placed in this group.
Group 3
The agent (mixture or exposure circumstance) is not classifiable as to its carcinogenicity to humans. This category is used most commonly for agents, mixtures and exposure circumstances for which the evidence of carcinogenicity is inadequate in humans and inadequate or limited in experimental animals.
Exceptionally, agents (mixtures) for which the evidence of carcinogenicity is inadequate in humans but sufficient in experimental animals may be placed in this category when there is strong evidence that the mechanism of carcinogenicity in experimental animals does not operate in humans.
Group 4
The agent (mixture) is probably not carcinogenic to humans. This category is used for agents or mixtures for which there is evidence suggesting lack of carcinogenicity in humans and in experimental animals. In some instances, agents or mixtures for which there is inadequate evidence of carcinogenicity in humans but evidence suggesting lack of carcinogenicity experimental animals, consistently and strongly supported by a broad range of other relevant data, may be classified in this group.
Classification systems made by humans are not sufficiently perfect to encompass all the complex entities of biology. They are, however, useful as guiding principles and may be modified as new knowledge of carcinogenesis becomes more firmly established. In the categorization of an agent, mixture or exposure circumstance, it is essential to rely on scientific judgements formulated by the group of experts.
Results to Date
To date, 69 volumes of IARC Monographs have been published or are in press, in which evaluations of carcinogenicity to humans have been made for 836 agents or exposure circumstances. Seventy-four agents or exposures have been evaluated as carcinogenic to humans (Group 1), 56 as probably carcinogenic to humans (Group 2A), 225 as possibly carcinogenic to humans (Group 2B) and one as probably not carcinogenic to humans (Group 4). For 480 agents or exposures, the available epidemiological and experimental data did not allow an evaluation of their carcinogenicity to humans (Group 3).
Importance of Mechanistic Data
The revised Preamble, which first appeared in volume 54 of the IARC Monographs, allows for the possibility that an agent for which epidemiological evidence of cancer is less than sufficient can be placed in Group 1 when there is sufficient evidence of carcinogenicity in experimental animals and strong evidence in exposed humans that the agent acts through a relevant mechanism of carcinogenicity. Conversely, an agent for which there is inadequate evidence of carcinogenicity in humans together with sufficient evidence in experimental animals and strong evidence that the mechanism of carcinogenesis does not operate in humans may be placed in Group 3 instead of the normally assigned Group 2B—possibly carcinogenic to humans—category.
The use of such data on mechanisms has been discussed on three recent occasions:
While it is generally accepted that solar radiation is carcinogenic to humans (Group 1), epidemiological studies on cancer in humans for UVA and UVB radiation from sun lamps provide only limited evidence of carcinogenicity. Special tandem base substitutions (GCTTT) have been observed in p53 tumour suppression genes in squamous-cell tumours at sun-exposed sites in humans. Although UVR can induce similar transitions in some experimental systems and UVB, UVA and UVC are carcinogenic in experimental animals, the available mechanistic data were not considered strong enough to allow the working group to classify UVB, UVA and UVC higher than Group 2A (IARC 1992). In a study published after the meeting (Kress et al. 1992), CCTTT transitions in p53 have been demonstrated in UVB-induced skin tumours in mice, which might suggest that UVB should also be classified as carcinogenic to humans (Group 1).
The second case in which the possibility of placing an agent in Group 1 in the absence of sufficient epidemiological evidence was considered was 4,4´-methylene-bis(2-chloroaniline) (MOCA). MOCA is carcinogenic in dogs and rodents and is comprehensively genotoxic. It binds to DNA through reaction with N-hydroxy MOCA and the same adducts that are formed in target tissues for carcinogenicity in animals have been found in urothelial cells from a small number of exposed humans. After lengthy discussions on the possibility of an upgrading, the working group finally made an overall evaluation of Group 2A, probably carcinogenic to humans (IARC 1993).
During a recent evaluation of ethylene oxide (IARC 1994b), the available epidemiological studies provided limited evidence of carcinogenicity in humans, and studies in experimental animals provided sufficient evidence of carcinogenicity. Taking into account the other relevant data that (1) ethylene oxide induces a sensitive, persistent, dose-related increase in the frequency of chromosomal aberrations and sister chromatid exchanges in peripheral lymphocytes and micronuclei in bone-marrow cells from exposed workers; (2) it has been associated with malignancies of the lymphatic and haematopoietic system in both humans and experimental animals; (3) it induces a dose-related increase in the frequency of haemoglobin adducts in exposed humans and dose-related increases in the numbers of adducts in both DNA and haemoglobin in exposed rodents; (4) it induces gene mutations and heritable translocations in germ cells of exposed rodents; and (5) it is a powerful mutagen and clastogen at all phylogenetic levels; ethylene oxide was classified as carcinogenic to humans (Group 1).
In the case where the Preamble allows for the possibility that an agent for which there is sufficient evidence of carcinogenicity in animals can be placed in Group 3 (instead of Group 2B, in which it would normally be categorized) when there is strong evidence that the mechanism of carcinogenicity in animals does not operate in humans, this possibility has not yet been used by any working group. Such a possibility could have been envisaged in the case of d-limonene had there been sufficient evidence of its carcinogenicity in animals, since there are data suggesting that α2-microglobulin production in male rat kidney is linked to the renal tumours observed.
Among the many chemicals nominated as priorities by an ad-hoc working group in December 1993, some common postulated intrinsic mechanisms of action appeared or certain classes of agents based upon their biological properties were identified. The working group recommended that before evaluations are made on such agents as peroxisome proliferators, fibres, dusts and thyrostatic agents within the Monographs programme, special ad-hoc groups should be convened to discuss the latest state of the art on their particular mechanisms of action.
Principles of Hazard Identification: The Japanese Approach
As in many other countries, risk due to exposure to chemicals is regulated in Japan according to the category of chemicals concerned, as listed in table 1. The governmental ministry or agency in charge varies. In the case of industrial chemicals in general, the major law that applies is the Law Concerning Examination and Regulation of Manufacture, Etc. of Chemical Substances, or Chemical Substances Control Law (CSCL) for short. The agencies in charge are the Ministry of International Trade and Industry and the Ministry of Health and Welfare. In addition, the Labour Safety and Hygiene Law (by the Ministry of Labour) provides that industrial chemicals should be examined for possible mutagenicity and, if the chemical in concern is found to be mutagenic, the exposure of workers to the chemical should be minimized by enclosure of production facilities, installation of local exhaust systems, use of protective equipment, and so on.
Table 1. Regulation of chemical substances by laws, Japan
| Category | Law | Ministry |
| Food and food additives | Foodstuff Hygiene Law | MHW |
| Pharmaceuticals | Pharmaceuticals Law | MHW |
| Narcotics | Narcotics Control Law | MHW |
| Agricultural chemicals | Agricultural Chemicals Control Law | MAFF |
| Industrial chemicals | Chemical Substances Control Law | MHW & MITI |
| All chemicals except for radioactive substances | Law concerning Regulation of House-Hold Products Containing Hazardous Substances Poisonous and Deleterious Substances Control Law Labour Safety and Hygiene Law |
MHW MHW MOL |
| Radioactive substances | Law concerning Radioactive Substances | STA |
Abbreviations: MHW—Ministry of Health and Welfare; MAFF—Ministry of Agriculture, Forestry and Fishery; MITI—Ministry of International Trade and Industry; MOL—Ministry of Labour; STA—Science and Technology Agency.
Because hazardous industrial chemicals will be identified primarily by the CSCL, the framework of tests for hazard identification under CSCL will be described in this section.
The Concept of the Chemical SubstanceControl Law
The original CSCL was passed by the Diet (the parliament of Japan) in 1973 and took effect on 16 April 1974. The basic motivation for the Law was the prevention of environmental pollution and resulting human health effects by PCBs and PCB-like substances. PCBs are characterized by (1) persistency in the environment (poorly biodegradable), (2) increasing concentration as one goes up the food chain (or food web) (bioaccumulation) and (3) chronic toxicity in humans. Accordingly, the Law mandated that each industrial chemical be examined for such characteristics prior to marketing in Japan. In parallel with the passage of the Law, the Diet decided that the Environment Agency should monitor the general environment for possible chemical pollution. The Law was then amended by the Diet in 1986 (the amendment taking effect in 1987) in order to harmonize with actions of the OECD regarding health and the environment, the lowering of non-tariff barriers in international trade and especially the setting of a minimum premarketing set of data (MPD) and related test guidelines. The amendment was also a reflection of observation at the time, through monitoring of the environment, that chemicals such as trichloroethylene and tetrachloroethylene, which are not highly bioaccumulating although poorly biodegradable and chronically toxic, can pollute the environment; these chemical substances were detected in groundwater nationwide.
The Law classifies industrial chemicals into two categories: existing chemicals and new chemicals. The existing chemicals are those listed in the “Existing Chemicals Inventory” (established with the passage of the original Law) and number about 20,000, the number depending on the way some chemicals are named in the inventory. Chemicals not in the inventory are called new chemicals. The government is responsible for hazard identification of the existing chemicals, whereas the company or other entity that wishes to introduce a new chemical into the market in Japan is responsible for hazard identification of the new chemical. Two governmental ministries, the Ministry of Health and Welfare (MHW) and the Ministry of International Trade and Industry (MITI), are in charge of the Law, and the Environment Agency can express its opinion when necessary. Radioactive substances, specified poisons, stimulants and narcotics are excluded because they are regulated by other laws.
Test System Under CSCL
The flow scheme of examination is depicted in figure 1, which is a stepwise system in principle. All chemicals (for exceptions, see below) should be examined for biodegradability in vitro. In case the chemical is readily biodegradable, it is considered “safe”. Otherwise, the chemical is then examined for bioaccumulation. If it is found to be “highly accumulating,” full toxicity data are requested, based on which the chemical will be classified as a “Class 1 specified chemical substance” when toxicity is confirmed, or a “safe” one otherwise. The chemical with no or low accumulation will be subject to toxicity screening tests, which consist of mutagenicity tests and 28-day repeated dosing to experimental animals (for details, see table 2). After comprehensive evaluation of the toxicity data, the chemical will be classified as a “Designated chemical substance” if the data indicate toxicity. Otherwise, it is considered “safe”. When other data suggest that there is a great possibility of environmental pollution with the chemical in concern, full toxicity data are requested, from which the designated chemical will be reclassified as “Class 2 specified chemical substance” when positive. Otherwise, it is considered “safe”. Toxicological and ecotoxicological characteristics of “Class 1 specific chemical substance,” “Class 2 specific chemical substance” and “Designated chemical substance” are listed in table 3 together with outlines of regulatory actions.
Figure 1. Scheme of examination

Table 2. Test items under the Chemical Substance Control Law, Japan
| Item | Test design |
| Biodegradation | For 2 weeks in principle, in vitro, with activated sludge |
| Bioaccumulation | For 8 weeks in principle, with carp |
| Toxicity screening Mutagenicity tests Bacterial system Chromosome aberration |
Ames’ test and test with E. coli, ± S9 mix CHL cells, etc., ±S9 mix |
| 28-day repeated dosing | Rats, 3 dose levels plus control for NOEL, 2 weeks recovery test at the highest dose level in addition |
Table 3. Characteristics of classified chemical substances and regulations under the Japanese Chemical Substances Control Law
| Chemical substance | Characteristics | Regulation |
| Class 1 specified chemical substances |
Nonbiodegradability High bioaccumulation Chronic toxicity |
Authorization to manufacture or import necessary1 Restriction in use |
| Class 2 specified chemical substances |
Nonbiodegradability Non- or low bioaccumulation Chronic toxicity Suspected environmental pollution |
Notification on scheduled manu-facturing or import quantity Technical guideline to prevent pollution/heath effects |
| Designated chemical substances | Nonbiodegradability Non- or low bioaccumulation Suspected chronic toxicity |
Report on manufacturing or import quantity Study and literature survey |
1 No authorization in practice.
Testing is not required for a new chemical with a limited use amount (i.e., less than 1,000 kg/company/year and less than 1,000 kg/year for all of Japan). Polymers are examined following the high molecular-weight compound flow scheme, which is developed with an assumption that chances are remote for absorption into the body when the chemical has a molecular weight of greater than 1,000 and is stable in the environment.
Results of Classification of Industrial Chemicals,as of 1996
In the 26 years from the time CSCL went into effect in 1973 to the end of 1996, 1,087 existing chemical items were examined under the original and amended CSCL. Among the 1,087, nine items (some are identified by generic names) were classified as “Class 1 specified chemical substance”. Among those remaining, 36 were classified as “designated”, of which 23 were reclassified as “Class 2 specified chemical substance” and another 13 remained as “designated”. The names of Class 1 and 2 specified chemical substances are listed in figure 2. It is clear from the table that most of the Class 1 chemicals are organochlorine pesticides in addition to PCB and its substitute, except for one seaweed killer. A majority of the Class 2 chemicals are seaweed killers, with the exceptions of three once widely used chlorinated hydrocarbon solvents.
Figure 2. Specified and designated chemical substances under the Japanese Chemical Substances Control Law
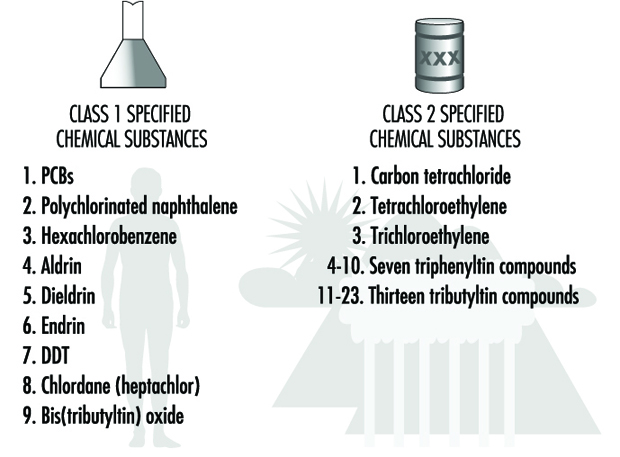
In the same period from 1973 to the end of 1996, about 2,335 new chemicals were submitted for approval, of which 221 (about 9.5%) were identified as “designated”, but none as Class 1 or 2 chemicals. Other chemicals were considered “safe” and approved for manufacturing or import.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."