Nations maintain military forces to deter aggression, discourage conflict and, should the need arise, to be prepared to fight and win their wars. Military forces are also used in non-combat roles that are referred to as “peacetime engagements” or “operations other than war”. These include: humanitarian missions such as emergency disaster assistance; peacemaking and peacekeeping operations; counter-drug and counter-terrorism work; and security assistance.
Men and women of the armed forces work under the sea, on surface ships, above the earth, on all kinds of terrain, in extremes of temperature and at high elevations. Many military jobs relate to maintaining the skills needed to operate equipment unique to the military (like submarines, fighter aircraft and tanks) in action against an armed enemy. The military also has a large number of uniformed people who perform maintenance, repair, administrative, medical and other functions to support those who fight battles.
All military people maintain proficiency in basic military skills, such as marksmanship, and a high level of physical fitness so that they may react appropriately if they become involved in warfare. Exercise programmes are used extensively to develop and maintain strength and aerobic fitness. If used in excess or poorly managed, these programmes may cause excessive injuries.
In addition to their job exposures, uniformed people are often at enhanced risk of acquiring infectious diseases. Basic training camp environments and close living spaces, as found on ships, may contribute to outbreaks of acute respiratory and other infectious diseases. Noise is a universal problem. Also, service in many parts of the world brings with it exposure to contaminated food and water, and to disease vectors carrying protozoan, viral and bacterial agents.
The armed forces rely on many civilian employees to do research and development and provide maintenance, administrative and other support services. Some civilians are paid by the military; others work for companies under contract to the military. In the past, civilian workers did not routinely accompany members of the armed forces into hostile areas. Recently, civilians have been performing many support functions in close proximity to deployed military forces, and may face similar occupational and environmental exposures.
The Fixed Workplace
In many fixed military facilities (such as repair depots, administrative offices and hospitals) uniformed members and civilians perform operations that are similar to those found in non-military workplaces. These include painting; degreasing; welding; grinding; chipping; electroplating; handling hydraulic fluids, fuels and cleaning agents; using microcomputers; and managing patients with infectious diseases. However, performing industrial operations in confined spaces in ships and submarines, or inside armoured vehicles, increases the risk of overexposure to toxicants. Additionally, some work must be done by divers at various depths.
In some fixed facilities, militarily unique items are developed, manufactured, serviced or stored. These items may include: nerve and mustard agent munitions; military explosives, propellants and special fuels, such as hydroxylammonium nitrate; laser range finders and target designators; microwave radiation sources in radar and communications equipment; and ionizing radiation from munitions, armour and nuclear power plants. Composite materials are not militarily unique but are common in military equipment. Where older military equipment is used, workers may be exposed to polychlorinated biphenyls in electrical systems, asbestos in the lagging around steam pipes and lead-based paints.
The Militarily Unique Workplace
People in the armed forces are always on duty, but commanders try to maintain acceptable work-rest cycles. However, battles are not fought on prearranged schedules, and military forces train as they expect to fight. During intense training, fatigue and sleep deprivation are common. The situation is worsened by quickly transporting military forces across time zones and having them perform their jobs immediately upon arrival. In all military operations, and particularly large operations that cover wide areas and involve air, land and sea forces from different countries, there is considerable pressure to maintain effective coordination and communication among the various elements to reduce the risk of accidents, such as placing weapons fire upon a friendly target. Stress is increased if operations result in long family separations, or if the possibility of hostile action exists.
Naval Vessels
On naval vessels, the tight spaces, multiple doors and ladders and narrow passageways close to operating equipment are hazardous. The confined spaces also restrict movement during work and contribute to ergonomic injuries (see figure 1). In submarines, air quality is a major concern that requires constant monitoring and the restriction of unnecessary contaminants. In all military environments where exposure to nuclear power plants, nuclear weapons or other radioactive material may occur, exposures are assessed, controls are implemented and monitoring is conducted as appropriate.
Figure 1. On aircraft carriers, naval flight deck personnel must work in extremely close proximity to operating fixed-wing jets and helicopters, and their associated safety hazards, exhaust combustion products and noise.

US Army
Aircraft
Flight operations in the aerospace environment involve a variety of fixed-wing and rotary-wing (helicopter) aircraft. Military air crews experience exposures that are different from those in the civilian environment. Many military aircraft are unique in their design, flight characteristics and mission performance. Air crew members are frequently at risk of exposure to excessive accelerative forces (centrifugal and gravitational), decompression sickness, circadian desynchrony resulting from long missions or night operations and spatial disorientation. Vibration originating from the aircraft and/or atmospheric turbulence may affect vision, result in motion sickness, produce fatigue and contribute to the development of disorders of the lumbar spine, particularly in helicopter pilots. Exposure to products of combustion from engine exhaust, overheating or burning of aircraft components may pose a toxic hazard if the aircraft is damaged during combat operations. Fatigue is a major concern when flight operations occur over extended periods of time, or involve long distances. Spatial disorientation and illusionary sensations of aircraft attitude and motion can be causes of mishaps, particularly when flights occur at high speeds in close proximity to the ground. Ground crews may be under considerable time pressure to perform maintenance and resupply (often with aircraft engines running) under difficult working conditions.
Helicopters are used extensively in the military as low-altitude weapons systems and observation platforms, and as medical evacuation and utility vehicles. These rotary-wing aircraft are associated with unique physical hazards, mission profiles and physiological implications for air crews. Helicopters have the ability to fly forward, sideward and rearward, but are inherently unstable flight platforms. Consequently, helicopter air crews must maintain constant concentration and have exceptional vision and muscle coordination to operate flight control systems and avoid collisions with terrain and other obstructions during low-level flight.
Fatigue is a serious concern for crew members involved in extended flights, large numbers of short missions and/or low-level, nap-of-the-earth (NOE) flights in which pilots fly as close to terrain contours as the speed and performance contours will allow. Low-level flights at night are particularly challenging. Night vision goggles are commonly used by helicopter pilots in military aviation and law enforcement; however, their use may restrict depth perception, field of view and colour differentiation. Engines, transmissions and rotors of helicopters produce unique vibration spectra which can adversely affect visual acuity and contribute to muscle strain and fatigue. These aircraft components also produce intense noise levels which can disrupt cockpit communications and contribute to hearing loss. Shrouds enclosing noisy components, acoustic blankets as insulation in cockpit/cabin areas and hearing protective devices are used to reduce the risk of hearing loss. Heat stress may be a special problem for helicopter air crews given the lower altitudes at which helicopters operate. Helicopter crashes tend to involve vertical impacts with the ground, often at relatively low forward speeds (in contrast to the longitudinal pattern of fixed-wing aircraft). Compression fractures of the spine and basilar skull fractures are common injuries in crash victims. Design features employed to prevent and control injuries include protective helmets, crash-worthy fuel systems, strengthened cockpit areas to prevent intrusion of the rotor system or transmission, and special seats and restraint systems utilizing shock-absorbing devices.
Ground Forces
Ground troops fire rifles, large guns and rockets, and ride in vehicles over rough terrain. At times they work under the cover of smokes produced from fog oil, diesel fuel or other chemicals (see figure 2). Exposures to noise, blast overpressure from large guns, vibration and propellant combustion products are common. Ballistic eye injuries occur but can be prevented by protective eyewear. The possibility of adverse health effects is increased when rockets and large guns are fired in enclosed areas, as in buildings. Armoured vehicle crew compartments are closed spaces where carbon monoxide concentrations may reach thousands of parts per million after weapons firing, and require effective ventilation systems. Heat stress in some vehicles may necessitate the use of cooling vests. Troops may also experience heat stress from wearing special clothing, hoods and masks to protect against chemical and biological agent attacks. These personal protective measures may contribute to accidents because of interference with vision and mobility. In field medical facilities, infection control practices and containment of waste anaesthetic gases may present unique challenges.
Figure 2. This mechanized smoke generator produces a curtain of fog oil smoke through heat evaporation; fog oil may cause a slipping hazard.
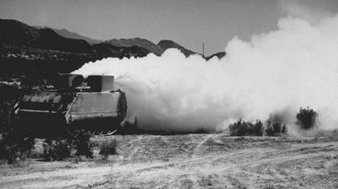
US Army
Military personnel face injury and illness from a variety of weapons. The more conventional weapons produce casualties using projectiles and fragments, blast effects (which may result in lung contusion trauma) and flame and incendiary devices, such as those containing napalm and phosphorus. Eye injuries from lasers may occur accidentally or when lasers are used as offensive weapons. Other weapons systems employ biological material, such as anthrax spores, or chemicals like anticholinesterase agents.
Extensive use of mines has caused concern because of the casualties that have occurred in civilian non-combatants. Narrowly defined, a mine is an explosive ordinance designed to be buried in the ground. In reality, a mine is any hidden explosive that lies in wait and may be detonated by enemy forces, friendly forces, non-combatants or animals. Mines may be employed against matériel or people. Anti-matériel mines are directed at military vehicles and may contain about 5 to 10 kg of explosive, but require 135 kg or more of compressive force to be activated. Antipersonnel mines are designed to maim rather than to kill. Less than 0.2 kg of explosive buried in the ground can blow off a foot. The dirt particles surrounding a mine become missiles that grossly contaminate wounds. The radius in which a mine can produce casualties was expanded with the development of the “pop-up mine”. In these mines a small explosive charge sends a canister about a metre into the air. The canister immediately detonates, spraying fragments to a distance of 35 m. Modern mine designs, like the “Claymore”, can be detonated electrically, by timed fuse or by a trip wire, and can send hundreds of steel spheres, each weighing 0.75 g, over a 60° arc for distances up to 250 m. Within 50 m, gross mutilation and lethal injuries are common.
A range of chemical agents have been employed in warfare. Herbicides (e.g., 2,4-D n-butyl ester mixed with 2,4,5-T n-butyl ester, also known as Agent Orange) were used in Vietnam to control terrain. Some chemicals (e.g., tear gas) have been used as incapacitating agents to produce transient physical or mental effects, or both. Other chemicals are extremely toxic and capable of producing serious injury or death. This category includes the anticholinesterase agents (e.g., Tabun and Sarin), the vesicants or blister agents (e.g., mustard and arsenicals), the lung-damaging or “choking” agents (e.g., phosgene and chlorine) and the blood agents that block the oxidative processes (e.g., hydrogen cyanide and cyanogen chloride).
In addition to armed conflict, other potential sources of exposure to chemical agents include: terrorist activities; storage sites for old military chemical stocks, where leaking containers may occur; sites where military chemical stocks are being destroyed through incineration or other means; and the accidental unearthing of old, forgotten chemical disposal sites.
The Medical Care System
Medical care for the armed forces and civilian workers is focused on prevention. Often, medical personnel study military vehicles and equipment during development to identify potential health hazards to users and maintainers so that these can be controlled. Training and user manuals and educational programmes address protection against hazards. Medical care includes initial medical screening, periodic medical assessment, health education and promotion, and disability evaluations, in addition to primary care and emergency services. Medical personnel also participate in accident investigations. When people deploy to areas presenting new health risks, medical risk assessments are used to identify threats and interventions like vaccines, prophylactic drugs, personnel protective measures and educational programmes.
Medical personnel who provide preventive and primary care to members of the armed forces must be knowledgeable about the characteristics of weapons used in training and on the battlefield to: predict and prepare for the casualties that may occur; take preventive actions that may reduce morbidity and/or mortality; and provide appropriate treatment when casualties do occur. Personal protective equipment is important in defending against chemical and biological agents and eye injuries from missiles and lasers. Other measures to be considered are vaccines and chemoprophylactic drugs for biological agents, and drug pre-treatment and antidotes for chemical agents. Training medical personnel in the early detection and management of illnesses and injuries caused by weapons is critical. Early recognition can result in rapid initiation of appropriate therapy and possibly a reduction in future morbidity and mortality. Also, military surgical staffs are better prepared to take care of their patients and themselves if they are knowledgeable about the wounds they are treating. For example: wounds made by high-velocity rifles often do not require extensive debridement for soft-tissue destruction; wounds made by fragmentation bullets may require extensive exploration; and wounds may contain unexploded munitions.