- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Pet, Furbearer and Laboratory Animal Protection
Processes
Institutional animal programmes involve four major processes:
- receipt, quarantine and separation of animals
- separation of species or animals for individual projects when necessary
- housing, care and sanitation
- storage.
Husbandry tasks include feeding, watering, providing bedding, maintaining sanitation, disposing of waste including carcasses, controlling pests and veterinarian care. Materials handling is significant in most of these tasks, which include moving cages, feed, pharmaceuticals, biologics and other supplies. Handling and manipulating animals is also fundamental to this work. Sanitation involves changing bedding, cleaning and disinfecting, and cage washing is a significant sanitation task.
Institutional animal facilities include cages, hutches, pens or stalls within a room, barn or outdoor habitat. Adequate space, temperature, humidity, food and water, illumination, noise control and ventilation are provided in a modern facility. The facility is designed for the type of animal that is confined. Animals that are typically confined in institutional settings include group-housed rodents (mice, rats, hamsters and guinea pigs), rabbits, cats, dogs, mink, non-human primates (monkeys, baboons and apes), birds (pigeons, quail and chickens) and farm animals (sheep and goats, swine, cattle, horses and ponies).
Hazards and Precautions
Persons involved with the production, care and handling of pet, furbearer and laboratory animals are potentially exposed to a variety of biological, physical and chemical hazards that can be controlled effectively through available risk reduction practices. The biological hazards intrinsic to the various animal species of concern to personnel include: bites and scratches; highly sensitizing allergens in dander, serum, tissues, urine or salivary secretions; and a wide variety of zoonotic agents. Although the biological hazards are more diverse and potentially more devastating in the work environments supporting these types of animals, the physical and chemical hazards generally are more pervasive, as reflected by their contribution to illness and injury in the workplace.
Personnel involved in the care and production of pet, furbearer or laboratory animals should receive appropriate training in handling techniques and behaviour of the animal species in question, because incorrect handling of an intractable animal frequently is a precipitating cause of a bite or scratch. Such injuries can become contaminated with micro-organisms from the animal’s rich oral and skin microflora or the environment, necessitating immediate wound disinfection and prompt and aggressive antimicrobial therapy and tetanus prophylaxis to avert the serious complications of wound infection and disfigurement. Personnel should appreciate that some zoonotic bite infections can produce generalized disease and even death; examples of the former include cat scratch fever, rat bite fever and human orf infection; examples of the latter include rabies, B virus and hantavirus infection.
Due to these extraordinary risks, wire-mesh, bite-proof gloves can be beneficial in some circumstances, and the chemical restraint of animals to facilitate safe handling is sometimes warranted. Personnel also can contract zoonoses through the inhalation of infectious aerosols, contact of the organisms with the skin or mucous membranes, ingestion of infectious materials or transmission by specific fleas, ticks or mites associated with the animals.
All types of zoonotic agents occur within pet, furbearer and laboratory animals, including viruses, bacteria, fungi and internal and external parasites. Some examples of zoonoses include: giardiasis and campylobacterosis from pets; anthrax, tularaemia and ringworm from furbearers; and lymphocytic choriomeningitis, hantavirus and dwarf tapeworm infestation from the laboratory rodent. The distribution of zoonotic agents varies widely according to host animal species, location and isolation from other disease reservoirs, housing and husbandry methods, and history and intensity of veterinary care. For example, some of the commercially produced laboratory animal populations have undergone extensive disease eradication programmes and been maintained subsequently under strict quality control conditions precluding the reintroduction of diseases. However, comparable measures have not been applicable universally in the various settings for pet, furbearer and laboratory animal maintenance and production, enabling the persistence of zoonoses in some circumstances.
Allergic reactions, ranging from ocular and nasal irritation and drainage to asthma or manifesting on the skin as contact urticaria (“hives”), are common in individuals who work with laboratory rodents, rabbits, cats and other animal species. An estimated 10 to 30% of individuals working with these animal species eventually develop allergic reactions, and persons with pre-existing allergic disease from other agents are at higher risk and have an increased incidence of asthma. In rare circumstances, such as a massive exposure to the inciting allergen through an animal bite, susceptible persons can develop anaphylaxis, a potentially life-threatening generalized allergic reaction.
Good personal hygiene practices should be observed by personnel to reduce their likelihood of exposure to zoonoses and allergens during work with animals or animal by-products. These include the use of dedicated work clothing, the availability and use of hand washing and shower facilities and separation of personnel areas from animal housing areas. Work clothing or protective outer garments covering the skin should be worn to prevent exposure to bites, scratches and hazardous microbes and allergens. Personal protective equipment, such as impervious gloves, safety glasses, goggles or other eye protection, and respiratory protection devices (e.g., particle masks, respirators or positive air pressure respirators) appropriate to the potential hazards and the individual’s vulnerability, should be provided and worn to promote safe work conditions. Engineering controls and equipment design also can effectively reduce the exposure of personnel to hazardous allergens and zoonoses through directional air flow and the use of isolation caging systems that partition the workers’ and animals’ environments.
Personnel also encounter significant physical and chemical hazards during animal care. Routine husbandry tasks involve moving or lifting heavy equipment and supplies, and performing repetitive tasks, affording personnel the ubiquitous opportunity to develop cuts and crush injuries, muscular strains and repetitive motion injuries. Work practice redesign, specialized equipment and personnel training in safe work practices can be used to curb these untoward outcomes. Equipment and facility sanitation frequently relies on machinery operating on live steam or extremely hot water, placing personnel at risk of severe thermal injury. The correct design, maintenance and utilization of these devices should be assured to prevent personnel injury and facilitate heat dissipation to provide a comfortable work environment. Personnel who work around large equipment, as well as around rambunctious dog or non-human primate populations, may be exposed to extremely high noise levels, necessitating the use of hearing protection. The various chemicals used for cage and facility sanitation, pest control within the animal facility and external parasite control on animals should be reviewed carefully with personnel to ensure their strict adherence to practices instituted to minimize exposure to these potentially irritating, corrosive or toxic substances.
Bull Raising
While the term bull refers to the male of several species of livestock (elephant, water buffalo and cattle) this article will deal specifically with the cattle industry. The National Traumatic Occupational Fatalities (NTOF) surveillance system in the United States, based on death certificates and maintained by the National Institute for Occupational Safety and Health (NIOSH), identified 199 fatalities from 1980 to 1992 associated with the agricultural production industry and inflicted by livestock. Of these, about 46% (92) were directly attributed to beef and dairy bull handling.
Cattle raisers have for centuries used castration of male animals as a means of producing docile males. Castrated males are generally passive, indicating that hormones (largely testosterone) are related to aggressive behaviour. Some cultures place high value on the fighting character of bulls, which is utilized in sports and social events. In this case, certain bloodlines are bred to maintain and enhance these fighting characteristics. In the United States, demand has increased for bulls used in rodeos as these entertainment events have increased in popularity. In Spain, Portugal, parts of France, Mexico and parts of South America, bullfighting has been popular for centuries. (See the article “Bullfighting and rodeos” in the chapter Entertainment and the Arts.)
The cattle industry can be divided into two major categories—dairy and beef—with some dual-purpose breeds. Most commercial beef operations purchase bulls from pure-bred producers, while dairy operations have moved more toward artificial insemination (AI). Thus, the pure-bred producer generally raises the bulls and then sells them when they are of breeding age (2 to 3 years of age). There are three systems of mating currently used in the cattle industry. Pasture mating allows bull to run with the herd and breed cows as they come into oestrus (heat). This can be for the entire year (historically) or for a specific breeding season. If specific breeding seasons are utilized, this necessitates separating the bull from the herd for periods of time. Hand mating keeps the bull isolated from the cows, except when a cow in oestrus is brought to the bull for mating. Generally, only a single mating is allowed, with the cow being removed after service. Finally, AI is the process of using proven sires, through the use of frozen semen, to be bred to many cows by AI technicians or the producer. This has the advantage of not having a bull at the ranch, which is a reduction of risk for the producer. However, there is still potential for human-animal interaction at the point of semen collection.
When a bull is removed from the herd for hand mating or kept isolated from the herd to establish a breeding season, he may become aggressive when he detects a cow in oestrus. Since he cannot respond naturally through mating, this can lead to the “mean bull” complex, which is an example of abnormal behaviour in bulls. Typical antagonistic or combative behaviour of bulls includes pawing the ground and bellowing. Furthermore, disposition often deteriorates with age. Old breeding stock can be cantankerous, deceptive, unpredictable and large enough to be dangerous.
Facilities
To ensure movement of animals through facilities, chutes should be curved so that the end cannot be seen when first entering, and the corral should be designed with a gap to the left or right so that animals do not sense that they are trapped. Putting rubber bumpers on metal items which create a loud noise when they close can help lessen the noise and reduce stress to the animal. Ideally, facilities should maximize the reduction of hazards due to physical contact between the bull and humans through use of barriers, overhead walkways and gates that can be manipulated from outside the enclosure. Animals are less likely to balk in chutes built with solid walls instead of fencing materials, since they would not be distracted by movement outside the chutes. Alleyways and chutes should be large enough so the animals can move through them, but not so wide they can turn around.
Guidelines for Handling
Male animals should be considered potentially dangerous at all times. When bulls are kept for breeding, injuries can be avoided by having adequate bull-confinement and restraint facilities. Extreme caution should be practised when handling male animals. Bulls may not purposefully hurt people, but their size and bulk make them potentially dangerous. All pens, chutes, gates, fences and loading ramps should be strong and work properly. Proper equipment and facilities are necessary to assure safety. Ideally, when working with bulls, having the handler physically separated from contact with the bull (outside the area and protected by chutes, walls, barriers and so on) greatly reduces the risk of injury. When handlers are with the animal, escape passages should be provided to allow handlers to escape from animals in an emergency. Animals should not be prodded when they have no place to go. Handlers should stay clear of animals that are frightened or “spooked” and be extra careful around strange animals. Solid wall chutes, instead of fencing, will lower the number of animals that balk in the chute. Since bulls see colours as different shades of black and white, facilities should be painted all in the same colour. Properly designed treatment stalls and appropriate animal-restraint equipment and facilities can reduce injuries during animal examination, medication, hoof trimming, dehorning and hand mating.
People who work with animals recognize that animals can communicate despite being unable to speak. Handlers should be sensitive to warnings such as raised or pinned ears, raised tail, pawing the ground and bellowing. General information and guidelines for working with bulls are provided in the checklist and article on animal behaviour in this chapter.
Zoonoses
Handlers should also be concerned with zoonotic diseases. A livestock handler can contract zoonotic illnesses by handling an infected animal or animal products (hides), ingesting animal products (milk, undercooked meat) and disposing of infected tissues. Leptospirosis, rabies, brucellosis (undulant fever in humans), salmonellosis and ringworm are especially important. Tuberculosis, anthrax, Q fever and tularaemia are other illness that should be of concern. To reduce exposure to disease, basic hygiene and sanitation practices should be used, which include prompt treatment or proper disposal of infected animals, adequate disposal of infected tissues, proper cleaning of contaminated sites and proper use of personal protective equipment.
The most sanitary method of carcass disposal is burning it at the site of death, to avoid contamination of the surrounding ground. A hole of appropriate size should be dug, flammable materials of sufficient quantity placed inside and the carcass placed on top in order that it can be consumed in its entirety. However, the most common method of carcass disposal is burial. In this procedure, the carcass should be buried at least 4 feet deep and covered with quicklime in soil that is not susceptible to contamination by drainage and away from flowing streams.
Draught Animals in Asia
Livestock contributes significantly to the life of small farmers, nomads and foresters all over the world and increases their productivity, income, employment and nutrition. This contribution is expected to rise. The world population will rise from its present 4.8–5.4 billion people to at least 10 billion in the next 100 years. The population of Asia can be expected to double over that same period. The demand for food will rise even more as the standard of living also rises. Along with this will be a rise in the need for draught power to produce the increased food required. According to Ramaswami and Narasimhan (1982), 2 billion people in the developing countries depend on draught animal power for farming and rural transportation. Draught power is critically short at the time of crop planting and is insufficient for other purposes throughout the year. Draught power will remain a major source of energy in agriculture into the foreseeable future, and the lack of draught power in some places may be the primary constraint to increasing crop production.
Animal draught power was the first supplement to human energy inputs in agriculture. Mechanized power has been used in agriculture only in the last century or so. In Asia, a greater proportion of farmers depend on animals for draught power than in any other parts of the world. A large proportion of these animals belong to farmers who have limited resources and cultivate small areas of land. In most parts of Asia, animal power is supplied by bullocks, buffalo and camels. Bullocks will continue to be the common source of farm power, mainly because they are adequate and live on waste residues. Elephants are also used in some places.
Production
In Asian countries, there are three main sources of power used in agriculture: human, mechanical and animal. Human beings provide the main source of power in developing countries for hoeing, weeding, rice transplanting, seed broadcasting and harvesting of crops. Mechanical power with its versatility is used for practically all the field operations, and the intensity of usage varies considerably from one developing country to another (Khan 1983). Animal power is generally used for tillage operations, haulage and operation of some water-lifting devices. A draught cow is a multipurpose farm animal, providing power, milk, dung, calves and meat. Normal draught power of various animals is presented in table 1.
Table 1. Normal draught power of various animals
|
Animals |
Weight (kg) |
Approx. draught (kg) |
Average speed of work (m/sec) |
Power developed (h.p.) |
|
Light horses |
400–700 |
60–80 |
1.0 |
1.00 |
|
Bullocks |
500–900 |
60–80 |
0.6–0.85 |
0.75 |
|
Buffaloes |
400–900 |
50–80 |
0.8–0.90 |
0.75 |
|
Cows |
400–600 |
50–60 |
0.7 |
0.45 |
|
Mules |
350–500 |
50–60 |
0.9–1.0 |
0.70 |
|
Donkeys |
200–300 |
30–40 |
0.7 |
0.35 |
Source: FAO 1966.
To have better draught animal power the following aspects should be considered:
For landless people to repay a loan for purchase of bullocks, feed them, and earn sufficient income to meet everyday costs, they must be able to work their animals for six hours per day.
- Draught animal nutrition. Animal nutrition is a principal factor in increasing the productivity of draught animal power. This is possible only if the necessary feed is available. In some areas, more effort is made to ensure the best use of available resources, such as treating straw with alkali (molasses urea block (MUB)) to improve its nutrient availability. As draught power availability is presently limiting the production of staple crops (there is an estimated 37% deficiency in draught requirements at the time of harvest), a primary objective is to produce draught animals and improve the efficiency of draught power. The opportunity to use improved nutritional technology (e.g., MUB) may assist draught power development through improved animal work capacity and reproduction rates in the female herd as well as better growth of young animals, which will lead to larger body size.
- Breeding and selection. Culling of local unproductive breed bulls and selection of the best local bull is necessary. Draught animals are currently selected according to their conformation, temperament and health; however, farmers often must rely on what is available locally.
Some crossbreds show a significant increase not only in milk and meat producing capability, but also in draught power. In India, Pakistan and Australia there have been tremendous efforts made in cross-breeding buffalo, cattle, horses (to produce mules) and, in some places, camels. This has produced very encouraging results. In many other Asian countries, especially developing countries, this research work for improving draught power as well as milk and meat production is very much needed.
- Equipment. Most farm equipment is old and unproductive. Much of the equipment that is used in conjunction with draught animals (harnesses, cultivation tools and carts) is of traditional type, the design of which has not changed for hundreds of years. In addition, farm implements are often badly designed and achieve low work output.
- Health. The stress of working may upset the balance which often exists between healthy animals and parasites.
Management
The daily feeding of draught animals varies according to work season. Both draught cattle and buffalo are fed in confinement (year-round) through a cut and carry system, with little or no grazing. Rice straw is fed all year long, depending on farmer preference, at either a measured rate of 8 to 10 kg per day or as necessary. Other crop residues such as rice hulls, pulse straw and cane tops are fed when available. In addition to these crop residues, cut or grazed green grass from roadsides and embankments is fed during the rainy season (April into November) at the rate of 5 to 7 kg/day and may be increased during times of heavy work to 10 kg/day.
Draught animal feed is usually supplemented with small amounts of by-product concentrates such as brans, oil cakes, pulses, rice hulls and molasses. The predominant means of feeding concentrates to draught animals is in a liquid form with all of the ingredients mixed together. The types and amounts of ingredients vary according to the daily workload of the animal, the geographical area, farmer preference and capability. Increased amounts of concentrates are fed during the heavy work seasons, and they are reduced during the monsoon season, when the workload is light.
Animal feed ingredients are also chosen by farmers based on availability, price, and their perception and understanding of its feeding value. For example, during the work season from November to June, daily rations may be: 200 g of mustard seed oil cake along with 100 g (dry weight) of boiled rice; 3/4 g of mustard seed oil cake, 100 g boiled rice and 3/4 g of molasses; or 2 kg total of equal parts sesame oil cake, rice polish, wheat bran and boiled rice, along with salt. On actual workdays during this period (163 days), animals are fed an extra 50% of these same rations. If animals are fed any concentrates at all during the non-working season, the rate ranges from 1/4 to 1/2 kg.
Draught Power in Australia
The Australian continent was first colonized by Europeans in 1788. Cattle were introduced with the first ships, but escaped into the surrounding forest. During those days ploughing and other land preparation was done with the heavy bullock plough, and light cultivation either with bullocks or horses. The bullock cart became the standard means of land transport in Australia and remained so until road building and railway construction began and became more widespread following the gold rushes from 1851 onwards.
In Australia other draught animals include the camel and the donkey. Although mules were used, they never became popular in Australia (Auty 1983).
Draught Power in Bangladesh
In Bangladesh livestock play a vital role in the economy, providing both draught power and milk and contributing up to 6.5% of the gross domestic product (GDP) (Khan 1983). Out of the 22 million head of cattle, 90% are used for draught power and transportation. Of this total, 8.2 million are dual purpose, supplying both draught power and dairy products, such as milk and meat (although in minimal amounts) for household consumption and trade. Adding energy value from draught power and dung (fertilizer and fuel), livestock contribute an estimated 11.3% to the GDP.
It has been observed that some cows are used for draught purposes, despite problems with fertility and health complications, which result in lower milk production and fewer calvings per lifetime. While cows are not usually worked during lactation, they contribute significantly to the annual supply of draught power in Bangladesh: 2.14 million (31%) adult female cattle and 60,000 (47%) adult buffalo cows supply animal power (Robertson et al. 1994). When combined with the male workforce, 76% of all adult cattle (11.2 million) and 85 to 90% of all adult buffalo (0.41 million) are used for draught purposes (Khan 1983).
There is no aggregate shortage of draught animals. Rather, the shortfall is based on the quality of draught power available, since malnourished animals are largely unproductive (Orlic and Leng 1992).
There are various breeds of cattle used for draught purposes, including pure deshi cattle and deshi cattle crossed with Sahiwal, Haryana and Red Sindhi cattle and Manipuri, Nili-Ravi and Murrah breeds of buffalo. Deshi bullocks weigh an average of 225 kg, crossbreds are slightly heavier at 275 kg and buffalo weigh an average of 400 kg. Bulls, cows, heifers and bullocks all provide animal power, but bullocks constitute the main workforce.
In Bangladesh, land preparation employs the highest percentage of draught animals. Research workers recommend that land be ploughed six to seven times prior to sowing. However, due to the shortage of draught power, many producers plough only four to five times in preparation for each crop. All ploughs in Bangladesh require two animals. Two bullocks can plough 1 acre in 2.75 (at 6 hours each day) (Orlic and Leng 1992; Robertson et al. 1994).
Draught Power in China
China has a long history of buffalo raising. The animals were used for farming as early as 2,500 years ago. Buffalo have a larger body size than the native cattle. Farmers prefer to use buffalo for farm work because of their great draught power, long working life and docile temperament. One buffalo can provide draught power for the production of 7,500 to 12,500 kg of rice (Yang 1995). Most of them are kept by small-scale farmers for draught purpose. The imported dairy buffalo, Murrah and Nili/Ravi, and crossbreds with these two breeds, are mainly raised on state farms and in research institutes. For centuries, buffalo have been reared mainly for draught purposes. The animals were slaughtered for meat only when they become old or disabled. Milking of buffalo was rare. After generations of selection and breeding, the buffalo have become extremely suitable for working, with deep and strong chests, strong legs, large hoofs and a docile temperament.
In China, buffalo are mainly used for paddy land and for field haulage. They are also employed in raising water, pudding clay for bricks, milling and pressing the juice from sugarcane. The extent of such use is declining due to mechanization. Training of buffalo usually starts at the age of two years. They begin to work a year later. Their working life is longer than that of cattle, usually more than 17 years. It is possible to see buffalo more than 25 years old still working in the fields. They work 90 to 120 days per year in the rice-growing area, with intensive work in the spring and autumn, when they work as long as 7 to 8 hours per day. The working capability varies widely with size, age and sex of the animal. The draught power reaches its maximum between the age of five and 12 years, remains high from 13 to 15 and begins to decline from 16 years. Most of the buffalo bulls are castrated (Yang 1995).
The Shanghai buffalo, one of the largest in China, has an excellent working capability. Working for 8 hours a day, one animal can plough 0.27 to 0.4 hectare of paddy land or 0.4 to 0.53 hectare of non-irrigated land (maximum 0.67 hectare). A load of 800 to 1,000 kg on a wooden-wheeled, bearingless vehicle can be drawn by a buffalo over 24 km within a working day. A buffalo can raise enough water to irrigate 0.73 hectares of paddy land in 4 hours.
In some sugar-producing areas, buffalo are used to draw stone rollers for sugar cane pressing. Six buffalo working in shifts can press 7,500 to 9,000 kg of sugar cane, requiring 15 to 20 minutes for every 1,000 kg.
Draught Power in India
According to Ramaswami and Narasimhan (1982) 70 million bullocks and 8 million buffalo generate about 30,000 million watts of power, assuming the Indian Council of Agricultural Research (ICAR) average of 0.5 hp output per animal. To generate, transmit and distribute this power at the same multitudinous points of application would call for an investment of 3,000,000 million rupees. It has also been estimated that an investment of 30,000 million rupees has gone into the Indian bullock cart system as against 45,000 million rupees in railways.
The Ministry of Shipping and Transport estimated that 11,700 to 15,000 million tonnes of freight in the urban areas is carried by cart each year, as against the railway haulage of 200,000 million tonnes. In the rural areas, where railroad service is not available, animal-drawn vehicles carry approximately 3,000 million tonnes of freight (Gorhe 1983).
Draught Power in Nepal
In Nepal, bullocks and male buffalo are the main source of draught power for tilling the fields. They are also used for carting, crushing sugar cane and oil seeds and for tracting loads. Due to the topographic nature of the country as well as the high cost of fuel, there is little opportunity for farm mechanization. Therefore, the demand for draught animal power in the country is high (Joshi 1983).
In wheat production, the contribution of bullocks in terms of labour days is 42% in ploughing, 3% in transplanting and 55% in threshing. In paddy production, it is 63% in ploughing, 9% in transplanting and 28% in threshing (Joshi 1983; Stem, Joshi and Orlic 1995).
Depending on the task, draught animals are generally worked a consistent number of hours each day and for a predetermined number of consecutive days before being allowed to rest. For instance, a full day of ploughing averages 6 hours for a bullock, and the average workday for a cow ranges from 4 to 5 hours per day. Animals used for ploughing follow a pattern of 6 to 8 consecutive days of work, followed by 2 days of rest. In the case of threshing, cows or lighter-weight animals usually work for 6 to 8 hours each day. The length and pattern of use for threshing and transport varies according to need. A bullock in full-time ploughing (maximum heavy labour) typically works for 163 days per year.
Draught Power in Sri Lanka
The total cattle population in Sri Lanka is estimated at 1.3 million. Various breeds are used as draught animals. Cattle breeds are used for draught purposes such as transport and ploughing of both wet and dry fields, as well as in farm operations. Indigenous animals have been used popularly in road transport for several decades. Crosses of Indian breeds with the indigenous cattle have resulted in larger animals that are used extensively for road transport. Out of a total buffalo population of 562,000, the number available in the work age range of three to 12 years is estimated at 200,000 males and 92,000 females.
Potential Hazards and Their Control
Other articles in this chapter address hazards and preventive actions for the draught animals discussed in this article. General information on animal behaviour and a checklist for livestock rearing safety practices are found in articles on these subjects and in the article “Animal husbandry”. Horses are addressed in the article “Horses and other equines”. Cattle (and by close association, bullocks and buffalo) are addressed in the article “Cattle, sheep and goats”. “Bull raising” also offers pertinent information on potential hazards and their control.
Case Study: Elephants
The largest draught animal is the elephant, but its role is slowly becoming one of tradition rather than necessity. Two decades ago, 4,000 Asian elephants were used for logging in Thailand, but the forests there have been clear-cut and mechanization has displaced the elephant. However, they are still used in Myanmar, where elephant logging is prevalent. Logging companies frequently lease working elephants from their owners, who are typically urban businessmen.
The elephant handler (or trainer) is called an oozie in Myanmar and a mahout in India and Sri Lanka. The trainer mounts a saddle—a thick pad of leaves and bark—on the elephant’s back to protect its sensitive spine from the dragging gear, or tack, used in pulling logs. The trainer sits on the elephant’s neck as it uses its trunk, tusks, feet, mouth and forehead to accomplish its daily chores. A well-trained elephant in logging work will respond to more than 30 vocal commands and 90 pressure points on its body from a skilled handler. They work until 2:45 every afternoon, then the oozie scrubs the elephant in water with coconut halves for up to an hour. The oozie then feeds the elephant salted, cooked rice and hobbles and releases it to feed in the forest at night. At about 4:00 a.m., the oozie locates the elephant by unique tones of a bell that is attached to the elephant (Schmidt 1997).
Elephant bulls are rarely held in captivity, and cows are traditionally released to be bred in the wild. Artificial insemination is also used to breed elephants. Bull elephants donate semen to an elephant-sized artificial cow. It is impossible to observe visually the cow in oestrus (three times per year), so weekly samples of blood are taken for progesterone analysis. When a cow is in oestrus, she is bred by injecting semen into her vagina with a long, flexible pneumatic insemination tube.
Several hazards are associated with elephant handling; they arise from elephants’ size, the massive objects of their work and their behaviour. Mounting the tack on the elephant and manipulating logging gear exposes the handler to injury hazards. In addition, the handler is exposed to falls from the elephant’s neck. The potential for injury is aggravated by the logging operations, which include carrying, pushing, pulling and stacking; teak logs can weigh as much as 1,360 kg. The elephant’s behaviour may be unpredictable and cause injury to its handler. Captive bulls are very dangerous and are difficult to contain. Breeding bulls are particularly dangerous. A working bull elephant in Sri Lanka has been reported to have killed nine mahouts. He was retained after each death, however, because of his value to his owners (Schmidt 1997).
Some elephants will respond only to their trainer. The principal method for controlling unpredictable elephants is to allow only their oozie to handle them. Elephants are creatures of habit, so trainers should maintain a daily routine. The afternoon scrubbing by the trainer has been found to be critical in establishing a bond with the elephant. Maintaining the trainer’s dominance is another safeguard against unsafe elephant behaviour.
The swimmers who carry blood samples to a laboratory for progesterone analysis are exposed to a particularly dangerous task: they swim across rivers during the monsoon season. This drowning hazard can be corrected by providing laboratory services near the working elephants.
Hazards in Sewage (Waste) Treatment Plants
Without treatment of waste the current concentration of people and industry in many parts of the world would very quickly make portions of the environment incompatible with life. Although reduction of the amount of waste is important, the proper treatment of waste is essential. Two basic types of waste enter a treatment plant, human/animal waste and industrial waste. Humans excrete about 250 grams of solid waste per capita per day, including 2000 million coliform and 450 million streptococci bacteria per person per day (Mara 1974). Industrial solid waste production rates range from 0.12 tons per employee per year at professional and scientific institutions to 162.0 tons per employee per year at sawmills and planing mills (Salvato 1992). Although some waste treatment plants are exclusively dedicated to handling one or the other type of material, most plants handle both animal and industrial waste.
Hazards and Their Prevention
The goal of waste water treatment plants is to remove as much of the solid, liquid and gaseous contaminants as possible within technically feasible and financially achievable constraints. There are a variety of different processes that are used to remove contaminants from waste water including sedimentation, coagulation, flocculation, aeration, disinfection, filtration and sludge treatment. (See also the article “Sewage treatment” in this chapter.) The specific hazard associated with each process varies depending on the design of the treatment plant and the chemicals used in the different processes, but the types of hazard can be classified as physical, microbial and chemical. The key to preventing and/or minimizing the adverse effects associated with working in sewage treatment plants is to anticipate, recognize, evaluate and control the hazards.
Figure 1. Manhole with cover removed.
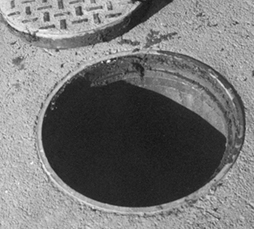
Mary O. Brophy
Physical hazards
Physical hazards include confined spaces, inadvertent energizing of machines or machine parts and trips and falls. The result of an encounter with a physical hazards can often be immediate, irreversible and serious, even fatal. Physical hazards vary with the design of the plant. Most sewage treatment plants, however, have confined spaces which include underground or below grade vaults with limited access, manholes (figure 1) and the sedimentation tanks when they have been emptied of liquid content during, for example, repairs (figure 2). Mixing equipment, sludge rakes, pumps and mechanical devices used for a variety of operations in sewage treatment plants can maim, and even kill, if they are inadvertently activated when a worker is servicing them. Wet surfaces, often encountered in sewage treatment plants, contribute to slipping and falling hazards.
Figure 2. Empty tank in a sewage treatment plant.

Mary O. Brophy
Confined-space entry is one of the most common and one of the most serious hazards faced by sewage treatment workers. A universal definition of a confined space is elusive. In general, however, a confined space is an area with limited means of entry and egress that was not designed for continuous human habitation and that does not have adequate ventilation. Hazards occur when the confined space is associated with a deficiency of oxygen, the presence of a toxic chemical or an engulfing material, such as water. Decreased oxygen levels can be the result of a variety of conditions including the replacement of oxygen with another gas, such as methane or hydrogen sulphide, the consumption of oxygen by the decay of organic material contained in the waste water or the scavenging of oxygen molecules in the rusting process of some structure within the confined space. Because low levels of oxygen in confined spaces cannot be detected by unaided human observation it is extremely important to use an instrument that can determine the level of oxygen before entering any confined space.
The earth’s atmosphere consists of 21% oxygen at sea level. When the percentage of oxygen in breathing air falls below about 16.5% a person’s breathing becomes more rapid and more shallow, the heart rate increases and the person begins to lose coordination. Below about 11% the person experiences nausea, vomiting, inability to move and unconsciousness. Emotional instability and impaired judgement may occur at oxygen levels somewhere between these two points. When individuals enter an atmosphere with oxygen levels below 16.5% they may immediately become too disoriented to get themselves out and eventually succumb to unconsciousness. If the oxygen depletion is great enough individuals can become unconscious after one breath. Without rescue they can die within minutes. Even if rescued and resuscitated, permanent damage can occur (Wilkenfeld et al. 1992).
Lack of oxygen is not the only hazard in a confined space. Toxic gases can be present in a confined space at a concentration level high enough to do serious harm, even kill, despite adequate oxygen levels. The effects of toxic chemicals encountered in confined spaces are discussed further below. One of the most effective ways to control the hazards associated with low oxygen levels (below 19.5%) and atmospheres contaminated with toxic chemicals is to thoroughly and adequately ventilate the confined space with mechanical ventilation prior to allowing anyone to enter it. This is usually done with a flexible duct through which outside air is blown into the confined space (see figure 3). Care must be taken to ensure that fumes from a generator or the fan motor are not also blown into the confined space (Brophy 1991).
Figure 3. Air moving unit for entering a confined space.
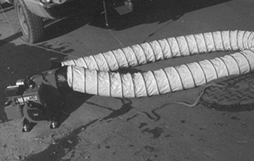
Mary O. Brophy
Sewage treatment plants often have large pieces of machinery to move sludge or raw sewage from one place in the plant to another. When repairs are made on this type of equipment the entire machine should be de-energized. Furthermore, the switch to re-energize the equipment should be under the control of the person performing the repairs. This prevents another worker in the plant from inadvertently energizing the equipment. Development and implementation of procedures to achieve these goals is called a lockout/tagout programme. Mutilation of body parts, such as fingers, arms and legs, dismemberment and even death can result from ineffective or inadequate lockout/tagout programmes.
Sewage treatment plants often contain large tanks and storage containers. People sometimes need to work on top of the containers, or walk by pits that have been emptied of water and may contain an 8 to 10 foot (2.5 to 3 m) drop (see figure 4). Sufficient protection against falls as well as adequate safety training should be provided for the workers.
Microbial hazards
Microbial hazards are primarily associated with the treatment of human and animal waste. Although bacteria are often added to alter the solids contained in waste water, the hazard to sewage treatment workers comes primarily from exposure to micro-organisms contained in human and other animal waste. When aeration is used during the sewage treatment process these micro-organisms can become airborne. The long term effect on the immune system of individuals exposed to these micro-organisms for extended periods of time has not been conclusively evaluated. In addition, workers who remove solid refuse from the influent stream before any treatment is begun are often exposed to micro-organisms contained in material splashing onto their skin and making contact with the mucous membranes. The results of encountering micro-organisms found in sewage treatment plants for extended periods of time are often more subtle than resulting from acute intense exposures. Nevertheless, these effects can also be irreversible and serious.
The three main categories of microbes relevant to this discussion are fungi, bacteria and viruses. All three of these can cause acute illness as well as chronic disease. Acute symptoms including respiratory distress, abdominal pains and diarrhoea have been reported in waste treatment workers (Crook, Bardos and Lacey 1988; Lundholm and Rylander 1980). Chronic diseases, such as asthma and allergic alveolitis, have been traditionally associated with exposure to high levels of airborne microbes and, recently, with microbial exposure during the treatment of domestic waste (Rosas et al. 1996; Johanning, Olmstead and Yang 1995). Reports of significantly elevated concentrations of fungi and bacteria in waste treatment, sludge dewatering and composting facilities are beginning to be published (Rosas et al. 1996; Bisesi and Kudlinski 1996; Johanning Olmstead and Yang 1995). Another source of airborne microbes is the aeration tanks which are used in many sewage treatment plants.
In addition to inhalation, microbes can be transmitted through ingestion and through contact with skin that is not intact. Personal hygiene, including washing hands before eating, smoking and going to the bathroom, is important. Food, drink, eating utensils, cigarettes and anything that would be put into the mouth should be kept away from areas of possible microbial contamination.
Chemical hazards
Chemical encounters at waste treatment plants can be both immediate and fatal, as well as protracted. A variety of chemicals are used in the process of coagulation, flocculation, disinfection and sludge treatment. The chemical of choice is determined by the contaminant or contaminants in the raw sewage; some industrial waste requires somewhat exotic chemical treatment. In general, however, the primary hazards from chemicals used in the coagulation and flocculation processes are skin irritation and eye injury due to direct contact. This is especially true of solutions which have a pH (acidity) less than 3 or greater than 9. The disinfection of effluent is often achieved by using either liquid or gaseous chlorine. Use of liquid chlorine can cause eye injury if splashed into the eyes. Ozone and ultraviolet light are also used to achieve disinfection of the effluent.
One way to monitor the effectiveness of sewage treatment is to measure the amount of organic material which remains in the effluent after treatment is complete. This can be done by determining the amount of oxygen that would be required to biodegrade the organic material contained in 1 litre of liquid over a period of 5 days. This is referred to as the 5-day biological oxygen demand (BOD5).
Chemical hazards in sewage treatment plants arise from the decomposition of organic material which results in the production of hydrogen sulphide and methane, from toxic waste dumped down the sewer lines and from the contaminants produced by operations performed by the workers themselves.
Hydrogen sulphide is almost always found in waste treatment plants. Hydrogen sulphide, also known as sewer gas, has a distinctive, unpleasant smell, often identified as rotten eggs. The human nose, however, quickly becomes accustomed to the smell. People who are exposed to hydrogen sulphide often lose their ability to detect its odour (i.e., olfactory fatigue). Furthermore, even if the olfactory system is able to detect hydrogen sulphide, it is not able to accurately judge its concentration in the atmosphere. Hydrogen sulphide biochemically interferes with the electron transport mechanism and blocks the utilization of oxygen at the molecular level. The result is asphyxiation and ultimately death due to the lack of oxygen in the brainstem cells that control the breathing rate. High levels of hydrogen sulphide (greater than 100 ppm) can, and often do, occur in the confined spaces found in sewage treatment plants. Exposure to very high levels of hydrogen sulphide can result in almost instantaneous suppression of the respiratory centre in the brainstem. The US National Institute for Occupational Safety and Health (NIOSH) has identified 100 ppm of hydrogen sulphide as immediately dangerous to life and health (IDLH). Lower levels of hydrogen sulphide (less than 10 ppm) are almost always present in some areas of sewage treatment plants. At these lower levels hydrogen sulphide can be irritating to the respiratory system, be associated with headaches and result in conjunctivitis (Smith 1986). Hydrogen sulphide is produced whenever organic matter decays and, industrially, during the production of paper (Kraft process), the tanning of leather (hair removal with sodium sulphide), and the production of heavy water for nuclear reactors.
Methane is another gas produced by the decomposition of organic matter. In addition to displacing oxygen, methane is explosive. Levels can be reached which result in an explosion when a spark or source of ignition is introduced.
Plants that handle industrial waste should have a thorough knowledge of the chemicals used in each of the industrial plants that utilize their services and a working relationship with the management of those plants so that they are promptly informed of any changes in processes and waste contents. Dumping of solvents, fuels and any other substance into sewer systems presents a hazard to treatment workers not only because of the toxicity of the material dumped but also because the dumping is unanticipated.
Whenever any industrial operation, such as welding or spray painting, is performed in a confined space special care must be taken to provide sufficient ventilation to prevent an explosion hazard as well as to remove toxic material produced by the operation. When an operation performed in a confined space produces a toxic atmosphere it is often necessary to equip the worker with a respirator because ventilation of the confined space may not ensure that the concentration of the toxic chemical can be maintained below the permissible exposure limit. Selection and fitting of a proper respirator falls within the purview of industrial hygiene practice.
Another serious chemical hazard in sewage treatment plants is the use of gaseous chlorine to decontaminate the effluent from the plant. The gaseous chlorine comes in a variety of containers weighing from 70 kg to roughly 1 tonne. Some of the very large sewage treatment plants use chlorine delivered in railroad cars. Gaseous chlorine is extremely irritating to the alveolar portion of the lungs, even in levels as low as a few ppm. Inhalation of higher concentrations of chlorine can cause inflammation of the alveoli of the lung and produce the adult respiratory distress syndrome, which has a 50% death rate. When a sewage treatment plant utilizes large amounts of chlorine (1 tonne and greater) the hazard exists not only for the plant workers but for the surrounding community as well. Unfortunately, the plants that use the largest amounts of chlorine are often located in large metropolitan centres with high density of people. Other methods of decontamination of sewage treatment plant effluent are available, including ozone treatment, the use of liquid hypochlorite solution and ultraviolet irradiation.
Horses and Other Equines
Horses belong to the equine family, which includes the domesticated African wild ass, also known as the donkey or burro. Historians believe that domestication of the horse began circa 6000 BC and the donkey at least as early as 2600 BC. The mule, bred for work, is a cross between a male donkey (jack or jackass) and a female horse (mare). A mule is unable to reproduce. When a male horse (stallion) is bred with a female donkey (jennet), the offspring, also sterile, is called a hinny. Horses and donkeys have also been crossed with another equine, the zebra, and the offspring are collectively called zebroids. Zebroids are also sterile and of little economic importance (Caras 1996).
Processes
Of the 10 million horses in the United States, about 75% are used for personal pleasure riding. Other uses include racing, ranching, breeding and commercial riding. The horse has become a performer in racing, jumping, rodeo and many more events.
The three main horse enterprises are breeding, training and boarding stables. Horse breeding farms breed mares and sell the offspring. Some farms specialize in training horses for show or racing. Boarding stables feed and care for horses for customers who have no facilities to house their horses. All three of these enterprises are labour intensive.
Horse breeding is an increasingly scientific process. Pasture breeding was typical, but now it is generally controlled within a breeding barn or corral. Although artificial insemination is used, it is more common that mares are brought to the stallion for breeding. The mare is checked by a veterinarian and, during breeding, trained workers handle the stallion and the mare.
After giving birth, the mare nurses the foal until it is from 4 to 7 months of age; after weaning, the foal is separated from the mare. Some colts not meant for breeding may be castrated (gelded) as early as 10 months of age.
When a racehorse becomes a two-year-old, professional trainers and riders start breaking it to ride. This involves a gradual process of getting the horse used to human touch, being saddled and bridled, and finally mounted. Horses that race with carts and heavy draught horses are broke to drive at about two years of age, and ranch horses are broke at closer to three years old, sometimes using the rougher method of bucking a horse out.
In horse racing, the groom leads the horse to the saddling paddock, a trainer and a valet saddle it, and a jockey mounts it. The horse is led by a pony horse and rider, warmed up and loaded into the starting gate. Racehorses can become excited, and the noise of a race can further excite and frighten the horse. The groom takes a winning horse to a drug test barn for blood and urine samples. The groom must then cool the horse down with a bath, walking and sipping water.
A groom cares for the performance horse and is responsible for brushing and bathing it, saddling it for the exercise rider, applying any protective bandages or boots to its legs, cleaning the stall and bedding down straw, shavings, peat moss, peanut skins, shredded newspaper or even rice hulls. The groom or a “hot” walker walks the horse; sometimes a mechanical walker is used. The groom feeds the horse hay, grain and water, rakes and sweeps, washes the horse’s laundry and carts manure away in a wheelbarrow. The groom holds the horse for others such as the veterinarian or farrier (farrier work is traditionally done by a blacksmith). All horses require parasite control, hoof care and teeth-filing.
Performance horses are typically stabled and given daily exercise. However, young stock and pleasure riding horses are generally stabled at night and released during the day, while others are kept outdoors in paddocks or pastures with sheds for shelter. Race horses in training are fed three or four times a day, while show horses, other performance horses, and breeding stock are fed twice a day. Range or ranch stock are fed once a day, depending on the forage present.
Horses travel for many reasons: shows, races, for breeding or to riding trails. Most are shipped by truck or trailer; however, some travel by rail or plane to major events.
Hazards and Precautions
Several hazards are associated with working around horses. A groom has a physically demanding job with a lot of forking of manure, moving 25 to 50 kg hay and straw bales and handling active horses. Startled or threatened horses may kick; thus, workers should avoid walking behind a horse. A frightened horse may jump and step on a worker’s foot; this can also occur accidentally. Various restraints are available to handle fractious horses, such as a chain over the nose or a lip chain. Stress on horses due to shipping may cause balking and injuries to the horses and handlers.
The groom is potentially exposed to hay and grain dust, dust from bedding, moulds, horse dander and ammonia from the urine. Wearing a respirator can provide protection. Grooms do a lot of leg work on the horses, sometimes using liniments containing hazardous chemicals. Gloves are recommended. Some leather-tack care products can contain hazardous solvents, requiring ventilation and skin protection. Cuts can lead to serious infections such as tetanus or septicaemia. Tetanus shots should be maintained current, especially because of exposure to manure.
A farrier is exposed to injury when shoeing a horse. The groom’s job is to hold the horse to keep it from kicking the farrier or pulling its foot in a way that could strain the farrier’s back or cut the farrier with the horseshoe and nails.
In the drug test barn, the test person is enclosed in a stall with a loose, excited and unfamiliar horse. He or she holds a stick (with a cup for urine) that may frighten the horse.
When riding horses, it is important to wear a good pair of boots and a helmet. Any mounted person needs a protective vest for racing, jumping, rodeo broncs, and ponying or exercising racehorses. There is always a danger of being bucked off or of a horse stumbling and falling.
Studs can be unpredictable, very strong and can bite or kick viciously. Brood mares are very defensive of their foals and can fight if threatened. Studs are kept individually in high-fenced paddocks, while other breeding stock are kept in groups with their own pecking order. Horses trying to move away from a boss horse or a group of yearlings at play can run over anyone who gets in the way. Foals, weanlings, yearlings and two-year-olds will bite and nip.
Some drugs (e.g., hormones) used in breeding are given orally and can be harmful to humans. Wearing gloves is recommended. Needle-stick injuries are another hazard. Good restraints, including stocks, can be used to control the animal during administration of medication. Topical sprays and automatic stable spray systems to control flies can easily be overused in horse rearing. These insecticides should be used in moderation, and warning labels should be read and recommendations followed.
There are a variety of zoonoses that can be passed from horses to humans, especially skin infections from contact with infected secretions. Horse bites can be a cause of some bacterial infections. See table 1 for a list of zoonoses associated with horses.
Table 1. Zoonoses associated with horses
Viral diseases
Rabies (very low occurrence)
Eastern, western and some subtypes of Venezuelan equine encephalomyelitis
Vesicular stomatitis
Equine influenza
Equine morbillvirus disease (first documented in Australia in 1994)
Fungus infections
Ringworm (dermatomycoses)
Parasitic zoonoses
Trichinosis (large outbreaks in France and Italy in the 1970s and 1980s)
Hydatid disease (echinoccosis) (very rare)
Bacterial diseases
Salmonellosis
Glanders (now very rare, restricted to Middle East and Asia)
Brucellosis (rare)
Anthrax
Leptospirosis (relatively rare, direct human contamination not definitively proven)
Melioidosis (outbreaks in France in the 1970s and 1980s; direct transmission not reported)
Tuberculosis (very rare)
Pasteurellosis
Actinobacillus lignieresii, A., A. suis (suspected in Lyme disease transmission, Belgium)
Case Study: Poultry Catching, Live Hauling and Processing
The potential for back injuries and respiratory disorders is high for poultry catchers. Many poultry companies in the United States contract out catching birds. Due to the transient nature of the catching crews there are no data indicating injuries or losses. Usually, catching crews are picked up and driven to the grower by company-owned truck. The crew members are either given or sold single use disposable respirators and disposable cotton gloves to protect their hands. Companies should make sure that respiratory protection is worn properly and that their crews have been properly medically evaluated and trained.
Each catch crew member must reach down and grab several struggling birds one after another and may be required to handle multiple birds at once. The birds are placed in a tray or drawer of a multi-bay module. The module holds several trays and is loaded by a company-owned fork-lift onto the bed of the company’s flat bed trailer. The fork-lift operator may either be the company’s truck driver or the contract crew leader. In either case, proper training and operation of the fork-lift must be assured. Speed and coordination are essential among the catching crew.
New methods of catching and loading have been experimented with in the US. One method being tried is a guided gatherer which has arms sweeping inwards guiding the chickens to a vacuum system. Attempts at automation to reduce the physical stresses and potential for respiratory exposure are a long way from success. Only the larger, more efficient poultry companies can afford the capital expenditures necessary to purchase and support such equipment.
A chicken’s normal body temperature is 42.2 °C. Consequently, the mortality rate increases in the winter and in locations where the summers are hot and humid. Both in the summer and winter, the flock must be transported as quickly as possible to be processed. In the summer, prior to processing, trailer loads of modules containing birds must be kept out of the sun and cooled with large fans. Dust, dried faecal matter and chicken feathers are often airborne as a result.
Throughout the entire processing of chicken, rigid sanitation requirements must be met. This means floors must be periodically and often washed down and debris, parts and fat removed. Conveyors and processing equipment must be accessible, washed down and sanitized also. Condensation must not be allowed to accumulate on ceilings and equipment over exposed chicken. It must be wiped down with long-handled sponge mops.
In the majority of the processing plant’s production areas, there is high noise exposure. Unguarded overhead radial blade fans circulate the air in the processing areas. Because of the sanitation requirements, guarded rotating equipment cannot be silenced for noise abatement purposes. An appropriate and well-run hearing conservation programme is necessary. Initial audiograms and annual audiograms should be given and periodic dosimetry should be performed to document exposure. Purchased processing equipment need to have as low an operating noise level as possible.
Particular care needs to be taken in educating and training the workforce. Workers must understand the full implications of exposure to noise and how to wear their hearing protection correctly.
Poultry and Egg Production
Farm production of birds weighing 18 kg or less includes not only domestic birds such as chickens, turkeys, ducks, geese and guineas, but also game birds produced for hunting, such as partridges, quail, grouse and pheasants. While some of these birds are raised outdoors, the majority of commercial poultry and egg production occurs in specially designed confinement houses or barns. Larger birds weighing between 40 and 140 kg, such as cassowaries, rheas, emus and ostriches, are also raised on farms for their meat, eggs, leather, feathers and fat. However, because of their larger size, most of these birds, which are known collectively as ratites, are usually raised outdoors in fenced-in areas containing shelters.
Chickens and turkeys comprise the majority of poultry produced in the world. US farmers annually produce one-third of the world’s chickens—more than the next six leading chicken-producing countries combined (Brazil, China, Japan, France, the United Kingdom and Spain). Similarly, more than half the world’s turkey production occurs in the United States, followed by France, Italy, the United Kingdom and Germany.
While commercial chicken production occurred in the United States as early as 1880, poultry and egg production was not recognized as a large-scale industry until about 1950. In 1900, a chicken weighed slightly less than a kilogram after 16 weeks. Before the emergence of poultry production as an industry, chickens purchased for eating were seasonal, being most abundant in early summer. Improvements in breeding, feed-to-weight conversion, processing and marketing practices, housing and disease control contributed to the poultry industry’s growth. The availability of artificial vitamin D also made a major contribution. All these improvements resulted in year-round poultry production, shorter production periods per flock and an increase in the number of birds housed together from only a few hundred to several thousand. The production of broilers (7-week-old chickens weighing approximately 2 kg) increased dramatically in the United States, from 143 million chickens in 1940, to 631 million in 1950, to 1.8 billion in 1960 (Nesheim, Austic and Card 1979). US farmers produced approximately 7.6 billion broilers in 1996 (USDA 1997).
Egg production has also seen dramatic growth similar to broiler production. At the beginning of the twentieth century, a laying hen annually produced about 30 eggs, mostly in the spring. Today, the annual average per layer is more than 250 eggs.
Ratite farming primarily consists of the ostrich from Africa, the emu and cassowary from Australia and the rhea from South America. (Figure 1 shows a farm flock of ostriches, and figure 2 shows a farm flock of emus.) Ratite farming first started in South Africa in the late 1800s in response to a fashion demand for the wing and tail feathers of ostriches. While ostrich plumes no longer decorate hats and clothing, commercial production still occurs not only in South Africa, but also in other African countries such as Namibia, Zimbabwe and Kenya. Ratite farming also occurs in Australia, Germany, Great Britain, Italy, China and the United States. The meat of these birds is gaining popularity because, while it is a red meat with a beefy taste and texture, it has total and saturated fat levels much lower than beef.
Figure 1. Part of a commercial flock of 3- to 6-week old ostriches

Roger Holbrook, Postime Ostrich, Guilford, Indiana
When processed at about 12 months of age, each bird will weigh approximately 100 kg, of which 35 kg is boneless meat. An adult ostrich can weigh as much as 140 kg.
Figure 2. Commercial flock of 12-month old emus
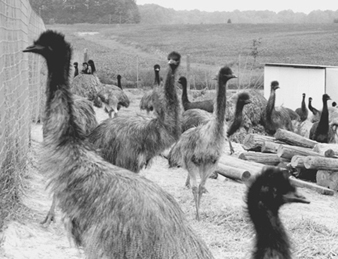
Volz Emu Farm, Batesville, Indiana
When processed at about 14 months of age, each bird will weigh between 50 and 65 kilograms, of which approximately 15 kilograms is meat and 15 kilograms is fat for oil and lotions.
Poultry Confinement Housing
A typical poultry confinement house in the United States is a long (60 to 150 m), narrow (9 to 15 m) single-storey barn with a dirt floor covered with litter (a layer of wood shavings, sphagnum peat or sawdust). Both ends of a confinement house have large doors, and both sides have half-side curtains running the length of the structure. Watering systems (called drinkers) and automatic feeding systems are located close to the floor and run the entire length of a house. Large, 1.2-m diameter propeller fans are also present in a poultry house to keep the birds comfortable. A poultry farmer’s daily tasks include maintaining acceptable environmental conditions for the birds, ensuring the continuous flow of feed and water and collecting and disposing of dead birds.
Watering and feeding systems are raised 2.5 to 3 metres above the floor when a flock reaches its processing age to accommodate catchers, workers who collect the birds for transport to a poultry processing plant. Collecting chickens is usually done by hand. Each member of a crew must bend over or stoop to gather several birds at a time and place them into coops, cages or crates. Each worker will repeat this process several hundred times during a work shift (see figure 3). For other types of poultry (e.g., ducks and turkeys), workers herd the birds to a collection area. Turkey catchers wave sticks with red bags tied to them in order to separate several birds at a time from a flock and drive them into a holding pen at the barn’s entrance (see figure 4).
Figure 3. Chicken catchers collecting broilers and placing them in crates for delivery to a poultry processing plant.

Steven W. Lenhart
Figure 4. Turkey catchers separating birds from a flock and driving them into a holding pen.
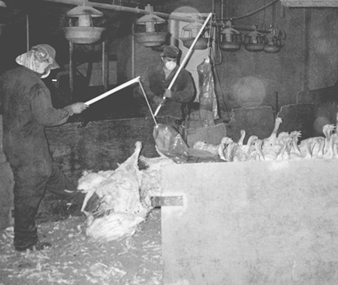
Steven W. Lenhart
Poultry confinement houses vary from this general description depending primarily on the type of birds being housed. For example, in commercial egg production, adult hens or layers have traditionally been kept in cages arranged in parallel banks. Caged laying-hen systems will be banned in Sweden in 1999 and replaced by loose laying-hen systems. (A loose laying system is shown in figure 5). Another difference between poultry confinement houses is that some do not have litter-covered floors but instead have either slotted or plastic-coated wire floors with manure pits or liquid manure catchment areas under them. In western Europe, poultry confinement houses tend to be smaller than US houses, and they utilize block construction with cement floors for easy litter removal. Western European poultry confinement houses are also decontaminated and floor litter removed after every flock.
Figure 5. A loose laying system
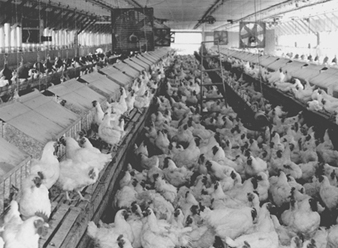
Steven W. Lenhart
Health Risks
The health and safety risks of poultry farmers, their family members (including children) and others who work in poultry confinement houses have increased as the poultry industry has grown. Raising a poultry flock requires a farmer to work 7 days a week. Consequently, unlike most occupations, exposures to contaminants occur over several consecutive days, with the period between flocks (as short as 2 days) being the only time of non-exposure to poultry house contaminants. The air of a poultry house can contain gaseous agents such as ammonia from litter, carbon monoxide from poorly ventilated gas-fired heaters and hydrogen sulphide from liquid manure. Also, particles of organic or agricultural dust are aerosolized from poultry house litter. Poultry house litter contains an assortment of contaminants including bird excreta, feathers and dander; feed dust; insects (beetles and flies), mites and their parts; micro-organisms (viral, bacterial and fungal); bacterial endotoxin; and histamine. The air of a poultry house can be very dusty, and for a first-time or occasional visitor, the smell of manure and the pungent odour of ammonia can at times be overwhelming. However, poultry farmers seemingly develop an adaptive tolerance to the smell and to ammonia’s odour.
Because of their inhalation exposures, unprotected poultry workers are at risk of developing respiratory diseases such as allergic rhinitis, bronchitis, asthma, hypersensitivity pneumonitis or allergic alveolitis and organic dust toxic syndrome. Acute and chronic respiratory symptoms experienced by poultry workers include cough, wheezing, excessive mucus secretion, shortness of breath and chest pain and tightness. Pulmonary function testing of poultry workers has provided evidence suggesting not only the risk for chronic obstructive diseases such as chronic bronchitis and asthma, but also restrictive diseases such as chronic hypersensitivity pneumonitis. Common non-respiratory symptoms among poultry workers include eye irritation, nausea, headache and fever. Of approximately 40 zoonotic diseases of agricultural importance, six (Mycobacterium avium infection, erysipeloid, listeriosis, conjunctival Newcastle infection, psittacosis and dermatophytosis) are of concern to poultry workers, although they occur only rarely. Non-zoonotic infectious diseases of concern include candidiasis, staphylococcosis, salmonellosis, aspergillosis, histoplasmosis and cryptococcosis.
There are also health issues affecting poultry workers that are as yet unstudied or poorly understood. For example, poultry farmers and especially chicken catchers develop a skin condition they refer to as galding. This condition has an appearance of a rash or dermatitis and primarily affects a person’s hands, forearms and inner thighs. The ergonomics of poultry catching are also unstudied. Bending to collect several thousand birds every work shift and carrying eight to fifteen chickens, each weighing from 1.8 to 2.3 kg, is physically demanding, but how this work affects a catcher’s back and upper extremities is unknown.
The extent to which the many psychosocial factors associated with farming have affected the lives of poultry farmers and their families is also unknown, but occupational stress is perceived by many poultry farmers as a problem. Another important but unstudied issue is the extent to which the health of farmers’ children is affected as a consequence of work in poultry houses.
Respiratory Health Protection Measures
The best way to protect any worker from exposure to airborne contaminants is with effective engineering controls that capture potential contaminants at their source before they can become airborne. In most industrial environments, airborne contaminants can be reduced to safe levels at their source by the installation of effective engineering control measures. Wearing respirators is the least desirable method for reducing workers’ exposures to airborne contaminants, and respirator use is recommended only when engineering controls are not feasible, or while they are being installed or repaired. Nevertheless, at present, wearing a respirator is still probably the most feasible method available for reducing poultry workers’ exposures to airborne contaminants. The general ventilation systems in poultry houses are not primarily intended to reduce the exposures of poultry workers. Research is going on to develop appropriate ventilation systems to reduce airborne contamination.
Not all respirators provide the same level of protection, and the type of respirator selected for use in a poultry confinement house can vary depending on the age of the birds being raised, age and condition of the litter, drinker type and position of the side curtains (open or closed). All of these are factors affecting airborne agricultural dust and ammonia concentrations. Airborne dust levels are highest during poultry-catching operations, at times to the point that one cannot see from one end of a poultry house to the other. A full-facepiece respirator with high-efficiency filters is recommended as the minimum protection for poultry workers based on bacterial endotoxin measurements made during chicken catching.
When ammonia levels are high, combination or “piggyback” cartridges are available that filter ammonia and particulates. A more expensive powered air-purifying respirator with a full-facepiece and high-efficiency filters may also be appropriate. These devices have the advantage that filtered air is constantly delivered to the wearer’s facepiece, resulting in less breathing resistance. Hooded, powered air-purifying respirators are also available and can be used by bearded workers. Respirators providing less protection than full-facepiece or powered air-purifying types may be adequate for some work situations. However, downgrading the level of protection, such as to a half-mask disposable respirator, is recommended only after environmental measurements and medical monitoring show that the use of a less protective respirator will reduce exposures to safe levels. Repeated exposures of the eyes to poultry dust increase the risk for eye injury and disease. Respirators with full-facepieces and those with hoods have a benefit of also providing eye protection. Poultry workers who choose to wear half-mask respirators should also wear eyecup goggles.
For any respirator to protect its wearer, it must be used in accordance with a complete respiratory-protection programme. However, while poultry farmers experience inhalation exposures for which respirator usage may be beneficial, most of them are not currently prepared to carry out a respiratory protection programme by themselves. This need may be addressed by the development of regional or local respiratory protection programmes in which poultry farmers can participate.
Manure pits should be considered confined spaces. A pit’s atmosphere should be tested if entry is unavoidable, and a pit should be ventilated if it is oxygen-deficient or contains toxic levels of gases or vapours. Safe entry may also require wearing a respirator. In addition, a standby person may be needed to stay in constant visual or speech contact with workers inside a manure pit.
Safety Risks
Safety risks associated with poultry and egg production include unguarded chains, sprockets, winches, belts and pulleys on fans, feeding equipment and other machinery. Scratches, pecks and even bites by the larger birds are also safety hazards. A male ostrich is especially protective of his nest during mating season, and when he feels threatened, he will attempt to kick any intruder. Long toes with sharp nails add to the danger of an ostrich’s powerful kick.
Electrical hazards created by improperly grounded or non-corrosion-resistant equipment or poorly insulated wires in a poultry house can result in electrocution, non-fatal electrical shock or fire. Poultry dust will burn, and poultry farmers tell anecdotes about accumulated dust exploding within gas-fired heaters when the dust was aerosolized during housekeeping chores. Researchers with the US Bureau of Mines have performed explosiveness testing of agricultural dusts. When aerosolized in a 20-litre test chamber and ignited, dust that was collected from the tops of heater cabinets and from window ledges in chicken houses was determined to have a minimum explosible concentration of 170 g/m3. Sieved samples of poultry house litter could not be ignited. By comparison, grain dust evaluated under the same laboratory conditions had a minimum explosible concentration of 100 g/m3.
Safety Measures
Measures can be taken to reduce safety risks associated with poultry and egg production. For protection from moving parts, all machinery should be guarded, and fans should be screened. For tasks involving hand contact with birds, gloves should be worn. High standards of personal hygiene should be maintained, and any injuries, no matter how minor, caused by machinery or birds should be treated immediately to avoid infection. When approaching a ratite, movement toward the bird should be from the side or behind to avoid being kicked. A lockout system should be used when servicing electrical equipment. Poultry farmers should frequently remove settled dust from surfaces, but they should be aware that, on rare occasions, an explosion can result when high concentrations of accumulated dust are aerosolized within an enclosure and ignited.
Telecommunications
Telecommunications is the act of communicating with others through the use of electronic equipment like telephones, computer modems, satellites and fibre optic cables. Telecommunications systems comprise telecommunications cables from the user to the local switching office (local loops), the switching facilities which provide the communications connection to the user, the trunks or channels that transmit calls between the switching offices and, of course, the user.
During the early to mid-twentieth century, telephone exchanges, electromechanical switching systems, cables, repeaters, carrier systems and microwave equipment were introduced. After this occurrence, telecommunications systems spread to the industrialized areas of the world.
From the 1950s to 1984, technological advances continued to appear. For example, satellite systems, improved cable systems, the use of digital technology, fibre optics, computerization and video telephony were introduced throughout the communications industry. These changes allowed for the expansion of telecommunications systems throughout more areas of the world.
In 1984 a court ruling in the United States led to the breakup of the telecommunications monopoly held by American Telegraph and Telephone (AT&T). This breakup coincided with many rapid, major changes in the technology of the telecommunications industry itself.
Until the 1980s telecommunications services were considered to be public services operating within a legislative framework that provided monopoly status in virtually all countries. Along with the development of economic activity, the advent of new technologies has led to the privatization of the telecommunications industry. This trend culminated in the divestiture of AT&T and the deregulation of the US telecommunications system. Similar privatization activities are underway in a number of other countries.
Since 1984, technological advances have produced and expanded telecommunications systems that can provide universal service to all people throughout the world. This occurs as telecommunications technology is now converging with other information technologies. Related fields such as electronics and data processing are involved.
The impact of the introduction of new technology on employment has been mixed. Without question, it has reduced levels of employment and produced the de-skilling of jobs, radically altering the tasks of telecommunications workers as well as the qualifications and experience required of them. However, it is anticipated by some that employment growth will occur in the future as a result of the new business activity stimulated by the deregulated telecommunications industry that will produce many highly skilled jobs.
Occupations within the telecommunications industry can be categorized as either skilled craft or clerical work. Craft jobs include cable splicers, installers, outside plant technicians, central office technicians and frame technicians. These jobs are highly skilled, particularly as a result of the new technological equipment. For example, employees must be very proficient in the electrical, electronics and/or mechanical fields as they relate to the installation, service and maintenance of telecommunications equipment. Training is acquired through classroom and on-the-job training.
Clerical occupations include directory assistance operators, customer service representatives, account representatives and sales clerks. In general these tasks involve the operation of communications equipment such as VDUs private branch exchange (PBX) and facsimile machines which are used to establish local and/or long distance connections, perform business office work inside or outside the workplace and handle sales contacts with customers.
Hazards and Controls
The occupational safety and health hazards within the telecommunications industry can be categorized by the type of tasks or services performed.
Building and construction operations
In general, the same risks occur as in construction and building operations. However, several noteworthy activities which are specific to telecommunications include working at heights on poles or pylons, installing telecommunications wiring systems and excavating for cable laying. The usual means of protection, such as climbing gaffs, safety harnesses, lines and raise platforms and proper shoring for excavations, are applicable in telecommunications. Often, this work is performed during emergency repairs made necessary by storms, landslides or floods.
Electricity
The safe use of electricity and electrical equipment is extremely important when performing telecommunications work. The normal preventive measures against electrocution, electric shock, short circuits and fires or explosions are fully applicable to telecommunications. Also, a serious source of danger may arise when telecommunications and electricity cables are within close proximity to one another.
Cable laying and maintenance
A significant safety and health concern is cable laying and maintenance. Work on underground cables, pipelines and jointing chambers involves handling heavy cable drums and pulling cables into pipelines with power-driven winches and cable equipment as well as cable splicing or jointing and insulation or waterproofing. During cable splicing and insulation jobs, workers suffer exposure to health hazards such as lead, solvents and isocyanates. Preventive measures include use of the least toxic chemicals, adequate ventilation and PPE. Often, maintenance and repair work is performed in confined spaces like manholes and vaults. Such work necessitates special ventilation equipment, harness and lifting equipment and the provision of a worker stationed above ground who is able to perform emergency cardiopulmonary resuscitation (CPR) and rescue activities.
Another health and safety concern is working with fibre optic telecommunications cables. Fibre optic cables are being installed as an alternative to lead and polyurethane-encased cables because they carry many more communications transmission and they are much smaller in size. Health and safety concerns involve potential burns to the eyes or skin from exposure to the laser beam when cables become disconnected or broken. When this occurs, protective engineering controls and equipment should be provided.
Also, cable installation and maintenance work performed in buildings involves potential exposure to asbestos products. Exposure occurs as a result of the deterioration or break-up of asbestos products like pipes, patching and taping compounds, floor and ceiling tiles and reinforcing fillers in paints and sealants. During the late 1970s, asbestos products were banned or their use was discouraged in many countries. Adherence to a worldwide prohibition will eliminate exposure and resultant health disorders for future generations of workers, but there are still large amounts of asbestos to contend with in older buildings.
Telegraph services
Telegraph workers use VDUs and, in some cases, telegraph equipment to perform their work. A frequent hazard associated with this type of work is upper extremity (particularly hand and wrist) musculoskeletal cumulative trauma. These health problems may be minimized and prevented with attention to ergonomic work stations, work environment and work organization factors.
Telecommunications service
Automatic switching and connecting circuits are the mechanical operations components of modern telecommunications systems. Connections are generally made by microwave and radio frequency waves in addition to cables and wires. Potential hazards are associated with microwave and radio frequency exposures. According to available scientific data, there is no indication that exposure to most types of radiation-emitting telecommunications equipment is directly linked to human health disorders. However, craft employees may be exposed to high levels of radio frequency radiation while working in close proximity to electrical power lines. Data have been collected that suggest a relationship between these emissions and cancer. Further scientific investigations are being conducted to more clearly determine the seriousness of this hazard as well as appropriate prevention equipment and methods. In addition, health concerns have been associated with emissions from cellular telephone equipment. Further research is being conducted to draw conclusions regarding potential health hazards.
The vast majority of telecommunications services are performed with the use of VDUs. Work with VDUs is associated with the occurrence of upper extremity (particularly hand and wrist) musculoskeletal cumulative trauma disorders. Many telecommunications unions, such as the Communications Workers of America (US), Seko (Sweden) and the Communication Workers Union (United Kingdom), have identified catastrophic rates of VDU workplace musculoskeletal cumulative trauma disorders among the workers they represent. Proper design of the VDU workplace with attention to work station, work environment and work organization variables will minimize and prevent these health problems.
Additional health concerns include stress, noise and electrical shock.
Pigs
Pigs were primarily domesticated from two wild stocks—the European wild boar and the East Indian pig. The Chinese domesticated the pig as early as 4900 BC, and today more than 400 million pigs are reared in China out of 840 million worldwide (Caras 1996).
Pigs are reared primarily for food and have many distinguishing attributes. They grow fast and large, and the sows have large litters and short gestation periods of about 100 to 110 days. Pigs are omnivores and eat berries, carrion, insects and garbage, as well as the corn, silage and pasture of high-production enterprises. They convert 35% of their feed into meat and lard, which is more efficient than ruminant species such as cattle (Gillespie 1997).
Production Processes
Some pig holdings are small—for example, one or two animals, which can represent much of a family’s wealth (Scherf 1995). Large pig operations include two major processes (Gillespie 1997).
One process is pure-bred production, in which pig breeding stock are improved. Within the pure-bred operation, artificial insemination is prevalent. Pure-bred boars are typically used to breed sows in the other major process, commercial production. The commercial production process rears pigs for the slaughter market and typically follows one of two different types of operations. One operation is a two-stage system. The first stage is feeder pig production, which uses a herd of sows to farrow litters of 14 to 16 piglets per sow. The pigs are weaned, then sold to the next stage of the system, the buying and finishing enterprise, which feeds them for the slaughter market. The most common feeds are corn and soybean oil meal. The feed grains are typically ground.
The other and most common operation is the complete sow and litter system. This production operation rears a herd of breeding sows and farrowing pigs, caring for and feeding the farrowed pigs for the slaughter market.
Some sows give birth to a litter that may outnumber her teats. To feed the excess piglets, a practice is to spread piglets from large litters into other sows’ smaller litters. Pigs are born with needle teeth, which are typically clipped at the gum-line before the pig is two days old. Ears are notched for identification. Tail docking occurs when the pig is about 3 days old. Male pigs raised for the slaughter market are castrated before they are 3 weeks old.
Maintaining a healthy herd is the single most important management practice in pig production. Sanitation and the selection of healthy breeding stock are important. Vaccination, sulpha drugs and antibiotics are used to prevent many infectious diseases. Insecticides are used to control lice and mites. The large roundworm and other parasites of pigs are controlled through sanitation and drugs.
Facilities used for pig production include pasture systems, a combination of pasture and low-investment housing and high-investment total-confinement systems. The trend is toward more confinement housing because it produces faster growth than does pasture rearing. However, pasture is valuable in feeding the pig-breeding herd to prevent fattening the breeding herd; it may be used for all or part of the production operation with the use of portable housing and equipment.
Confinement buildings require ventilation to control temperature and moisture. Heat may be added in farrowing houses. Slotted floors are used in confinement houses as a labour-saving approach for handling manure. Fencing and handling feeding and watering equipment are needed for the pig production enterprise. Facilities are cleaned by power washing and disinfecting after all bedding, manure and feed are removed (Gillespie 1997).
Hazards
Injuries from pigs usually occur within or close to farm buildings. Dangerous environments include slippery floors, manure pits, automatic feeding equipment and confinement buildings. Confinement buildings have a manure storage pit that emits gases that, if not ventilated, can kill not only pigs, but workers as well.
Pig behaviour can pose hazards to workers. A sow will attack if her piglets are threatened. Pigs can bite, step on or knock people down. They tend to stay in or return to familiar areas. A pig will try to return to the herd when attempts are made to separate it. Pigs are likely to balk when moved from a dark area into a light area, such as out of a pig house into the daylight. At night, they will resist moving into dark areas (Gillespie 1997).
In a Canadian study of pig farmers, 71% reported chronic back problems. Risk factors include intervertebral disc loading associated with driving and sitting for long periods while operating heavy equipment. This study also identified lifting, bending, twisting, pushing and pulling as risk factors. In addition, more than 35% of these farmers reported chronic knee problems (Holness and Nethercott 1994).
Three types of air exposures pose hazards on pig farms:
- dust from feed, animal hair and faecal matter
- pesticides used on pigs and other chemicals, such as disinfectants
- ammonia, hydrogen sulphide, methane and carbon monoxide from manure storage pits.
Fires in buildings are another potential hazard, as is electricity.
Some zoonotic infections and parasites can be transmitted from the pig to the worker. Common zoonoses associated with pigs include brucellosis and leptospirosis (swineherd’s disease).
Preventive Action
Several safety recommendations have evolved for the safe handling of pigs (Gillespie 1997):
- Working with small pigs in the same pen as the sow should be avoided.
- A hurdle or solid panel should be used when handling pigs to avoid bites and being knocked over.
- A pig can be moved backwards by placing a basket over its head.
- Children should be kept out of pig pens and not allowed to reach through fences to pet pigs.
- Because of their herding instincts, it is easier to separate a group of pigs from a herd than a single animal.
- Pigs can be moved from dark to light areas with the use of artificial light. When pigs are moved at night, such as through chutes or alleys, a light should be placed at the destination.
- Loading chutes should be level or at not more than a 25-degree angle.
Musculoskeletal injury risk can be decreased by reducing exposure to repetitive trauma (by taking frequent breaks or by varying the kinds of tasks), improving posture, reducing the weight lifted (use co-worker or mechanical assistance) and avoiding rapid, jerking movements.
Dust control techniques include lowering stock density to reduce dust concentration. In addition, automatic feed delivery systems should be enclosed to contain dust. Water misting can be used, but it is ineffective in freezing weather and can contribute to the survival of bioaerosols and increase endotoxin levels. Filters and scrubbers in the air handling system show promise in cleaning dust particles from recirculated air. Respirators are another way to control dust exposures (Feddes and Barber 1994).
Vent pipes should be installed in manure pits to prevent dangerous gases from recirculating into the farm buildings. Electrical power should be maintained to vent fans at the pits. Workers should be trained in the safe use of pesticides and other chemicals, such as disinfectants, used in pig production.
Cleanliness, vaccination, quarantine of sick animals and avoiding exposures are ways to control zoonoses. When treating sick pigs, wear rubber gloves. A person who becomes sick after working with sick pigs should contact a physician (Gillespie 1997).
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."