- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Work Organization
Design of Production Systems
Many companies invest millions in computer-supported production systems and at the same time do not make full use of their human resources, whose value can be significantly increased through investments in training. In fact, the use of qualified employee potential instead of highly complex automation can not only, in certain circumstances, significantly reduce investment costs, it can also greatly increase flexibility and system capability.
Causes of Inefficient Use of Technology
The improvements which investments in modern technology are intended to make are frequently not even approximately achieved (Strohm, Kuark and Schilling 1993; Ulich 1994). The most important reasons for this are due to problems in the areas of technology, organization and employee qualifications.
Three main causes can be identified for problems with technology:
- Insufficient technology. Because of the rapidity of technological changes, new technology reaching the market has sometimes undergone inadequate continuous usability tests, and unplanned downtime can result.
- Unsuitable technology. Technology developed for large companies is often not suitable for smaller companies. When a small firm introduces a production planning and control system developed for a large company, it may deprive itself of the flexibility necessary for its success or even survival.
- Excessively complex technology. When designers and developers use their entire planning knowledge to realize what is technically feasible without taking into account the experience of those involved in production, the result can be complex automated systems which are no longer easy to master.
Problems with organization are primarily attributable to continuous attempts at implementing the latest technology in unsuitable organizational structures. For instance, it makes little sense to introduce third, fourth and fifth generation computers into second generation organizations. But this is exactly what many companies do (Savage and Appleton 1988). In many companies, a radical restructuring of the organization is a precondition for the successful use of new technology. This particularly includes an examination of the concepts of production planning and control. Ultimately, local self-control by qualified operators can in certain circumstances be significantly more efficient and economical than a technically highly developed production planning and control system.
Problems with the qualifications of employees primarily arise because a large number of companies do not recognize the need for qualification measures in conjunction with the introduction of computer-supported production systems. In addition, training is too frequently regarded as a cost factor to be controlled and minimized, rather than as a strategic investment. In fact, system downtime and the resulting costs can often be effectively reduced by allowing faults to be diagnosed and remedied on the basis of operators’ competence and system-specific knowledge and experience. This is particularly the case in tightly coupled production facilities (Köhler et al. 1989). The same applies to introducing new products or product variants. Many examples of inefficient excessive technology use testify to such relationships.
The consequence of the analysis briefly presented here is that the introduction of computer-supported production systems only promises success if it is integrated into an overall concept which seeks to jointly optimize the use of technology, the structure of the organization and the enhancement of staff qualifications.
From the Task to the Design of Socio-Technical Systems
Work-related psychological concepts of production design are based on the primacy of
the task. On the one hand, the task forms the interface between individual and organization (Volpert 1987). On the other hand, the task links the social subsystem with the technical subsystem. “The task must be the point of articulation between the social and technical system—linking the job in the technical system with its correlated role behaviour, in the social system” (Blumberg 1988).
This means that a socio-technical system, for example, a production island, is primarily defined by the task which it has to perform. The distribution of work between human and machine plays a central role, because it decides whether the person “functions” as the long arm of the machine with a function leftover in an automation “gap” or whether the machine functions as the long arm of the person, with a tool function supporting human capabilities and competence. We refer to these opposing positions as “technology-oriented” and “work-oriented” (Ulich 1994).
The Concept of Complete Task
The principle of complete activity (Hacker 1986) or complete task plays a central role in work-related psychological concepts for defining work tasks and for dividing up tasks between human and machine. Complete tasks are those “over which the individual has considerable personal control” and that “induce strong forces within the individual to complete or to continue them”. Complete tasks contribute to the “development of what has been described ... as ‘task orientation’—that is, a state of affairs in which the individual’s interest is aroused, engaged and directed by the character of the task” (Emery 1959). Figure 1 summarizes characteristics of completeness which must be taken into account for measures geared towards work-oriented design of production systems.
Figure 1. Characteristics of complete tasks
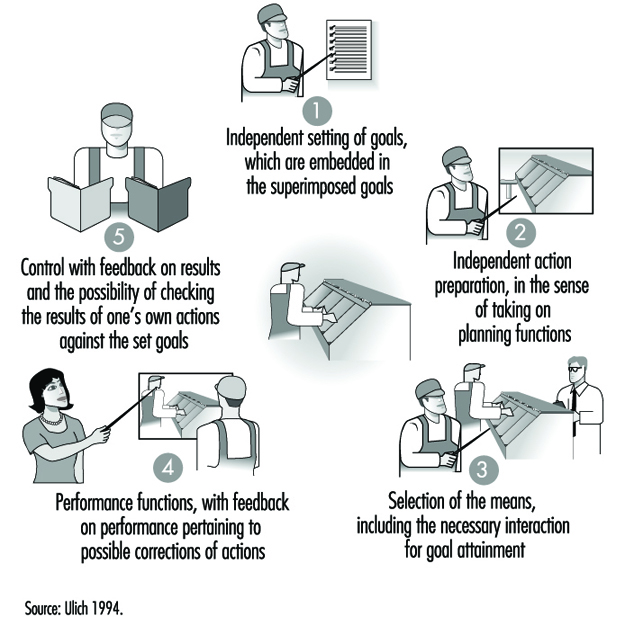
- The independent setting of objectives, which can be incorporated into higher-order goals, requires turning away from central planning and control in favour of decentralized shop-floor control, which provides the possibility of making self-determined decisions within defined periods of time.
- Self-determined preparation for action, in the sense of carrying out planning functions, requires the integration of work preparation tasks on the shop-floor.
- Selecting methods means, for example, allowing a designer to decide whether he or she wishes to use the drawing board instead of an automated system (such as a CAD application) to perform certain subtasks, provided that it is ensured that data required for other parts of the process are entered in the system.
- Performance functions with process feedback for correcting actions where appropriate require in the case of encapsulated work processes “windows to the process” which help to minimize process distance.
- Action control with feedback of results means that shop-floor workers take on the function of quality inspection and control.
These indications of the consequences arising from realizing the principle of the complete task make two things clear: (1) in many cases—probably even the majority of cases—complete tasks in the sense described in figure 1 can only be structured as group tasks on account of the resulting complexity and the associated scope; (2) restructuring of work tasks—particularly when it is linked to introducing group work—requires their integration into a comprehensive restructuring concept which covers all levels of the company.
The structural principles which apply to the various levels are summarized in table 1.
Table 1. Work-oriented principles for production structuring
|
Organizational level |
Structural principle |
|
Company |
Decentralization |
|
Organizational unit |
Functional integration |
|
Group |
Self-regulation1 |
|
Individual |
Skilled production work1 |
1 Taking into account the principle of differential work design.
Source: Ulich 1994.
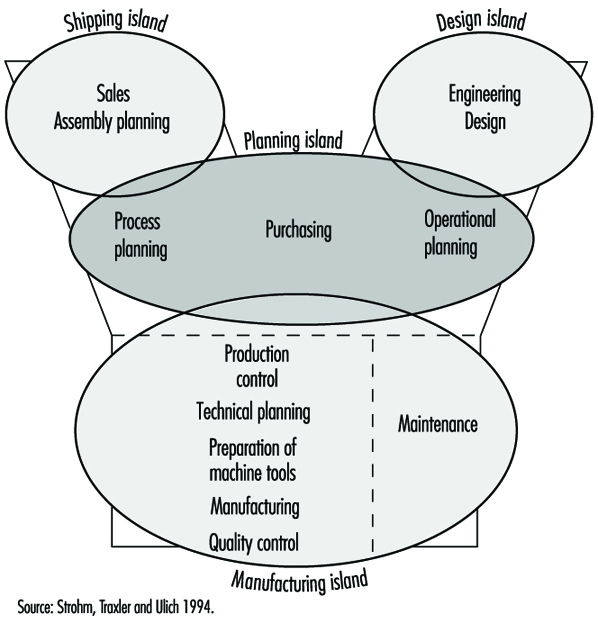
Possibilities for realizing the principles for production structuring outlined in table 1 are illustrated by the proposal for restructuring a production company shown in figure 2. This proposal, which was unanimously approved both by those responsible for production and by the project group formed for the purpose of restructuring, also demonstrates a fundamental turning away from Tayloristic concepts of labour and authority divisions. The examples of many companies show that the restructuring of work and organization structures on the basis of such models is able to meet both work psychological criteria of promoting health and personality development and the demand for long-term economic efficiency (see Ulich 1994).
Figure 2. Proposal for restructuring a production company
The line of argument favoured here—only very briefly outlined for reasons of space—seeks to make three things clear:
- Concepts like the ones mentioned here represent an alternative to “lean production” in the sense described by Womack, Jones and Roos (1990). While in the latter approach “every free space is removed” and extreme breaking down of work activities in the Tayloristic sense is maintained, in the approach being advanced in these pages, complete tasks in groups with wide-ranging self-regulation play a central role.
- Classical career paths for skilled workers are modified and in some cases precluded by the necessary realization of the functional integration principle, that is, with the reintegration on the shop-floor of what are known as indirectly productive functions, such as shop-floor work preparation, maintenance, quality control and so forth. This requires a fundamental reorientation in the sense of replacing the traditional career culture with a competence culture.
- Concepts such as those mentioned here mean a fundamental change to corporate power structures which must find their counterpart in the development of corresponding possibilities for participation.
Workers’ Participation
In the previous sections types of work organization were described that have as one basic characteristic the democratization at lower levels of an organization’s hierarchy through increased autonomy and decision latitude regarding work content as well as working conditions on the shop-floor. In this section, democratization is approached from a different angle by looking at participative decision-making in general. First, a definitional framework for participation is presented, followed by a discussion of research on the effects of participation. Finally, participative systems design is looked at in some detail.
Definitional framework for participation
Organizational development, leadership, systems design, and labour relations are examples of the variety of tasks and contexts where participation is considered relevant. A common denominator which can be regarded as the core of participation is the opportunity for individuals and groups to promote their interests through influencing the choice between alternative actions in a given situation (Wilpert 1989). In order to describe participation in more detail, a number of dimensions are necessary, however. Frequently suggested dimensions are (a) formal-informal, (b) direct-indirect, (c) degree of influence and (d) content of decision (e.g., Dachler and Wilpert 1978; Locke and Schweiger 1979). Formal participation refers to participation within legally or otherwise prescribed rules (e.g., bargaining procedures, guidelines for project management), while informal participation is based on non-prescribed exchanges, for example, between supervisor and subordinate. Direct participation allows for direct influence by the individuals concerned, whereas indirect participation functions through a system of representation. Degree of influence is usually described by means of a scale ranging from “no information to employees about a decision”, through “advance information to employees” and “consultation with employees” to “common decision of all parties involved”. As regards the giving of advance information without any consultation or common decision-making, some authors argue that this is not a low level of participation at all, but merely a form of “pseudo-participation” (Wall and Lischeron 1977). Finally, the content area for participative decision-making can be specified, for example, technological or organizational change, labour relations, or day-to-day operational decisions.
A classification scheme quite different from those derived from the dimensions presented so far was developed by Hornby and Clegg (1992). Based on work by Wall and Lischeron (1977), they distinguish three aspects of participative processes:
- the types and levels of interactions between the parties involved in a decision
- the flow of information between the participants
- the nature and degree of influence the parties exert on each other.
They then used these aspects to complement a framework suggested by Gowler and Legge (1978), which describes participation as a function of two organizational variables, namely, type of structure (mechanistic versus organic) and type of process (stable versus unstable). As this model includes a number of assumptions about participation and its relationship to organization, it cannot be used to classify general types of participation. It is presented here as one attempt to define participation in a broader context (see table 2). (In the last section of this article, Hornby and Clegg’s study (1992) will be discussed, which also aimed at testing the model’s assumptions.)
Table 2. Participation in organizational context
|
Organizational structure |
||
|
Mechanistic |
Organic |
|
|
Organizational processes |
||
|
Stable |
Regulated |
Open |
|
Unstable |
Arbitrary |
Regulated |
Source: Adapted from Hornby and Clegg 1992.
An important dimension usually not included in classifications for participation is the organizational goal behind choosing a participative strategy (Dachler and Wilpert 1978). Most fundamentally, participation can take place in order to comply with a democratic norm, irrespective of its influence on the effectiveness of the decision-making process and the quality of the decision outcome and implementation. On the other hand, a participative procedure can be chosen to benefit from the knowledge and experience of the individuals involved or to ensure acceptance of a decision. Often it is difficult to identify the objectives behind choosing a participative approach to a decision and often several objectives will be found at the same time, so that this dimension cannot be easily used to classify participation. However, for understanding participative processes it is an important dimension to keep in mind.
Research on the effects of participation
A widely shared assumption holds that satisfaction as well as productivity gains can be achieved by providing the opportunity for direct participation in decision-making. Overall, research has supported this assumption, but the evidence is not unequivocal and many of the studies have been criticized on theoretical and methodological grounds (Cotton et al. 1988; Locke and Schweiger 1979; Wall and Lischeron 1977). Cotton et al. (1988) argued that inconsistent findings are due to differences in the form of participation studied; for instance, informal participation and employee ownership are associated with high productivity and satisfaction whereas short-term participation is ineffective in both respects. Although their conclusions were strongly criticized (Leana, Locke and Schweiger 1990), there is agreement that participation research is generally characterized by a number of deficiencies, ranging from conceptual problems like those mentioned by Cotton et al. (1988) to methodological issues like variations in results based on different operationalizations of the dependent variables (e.g., Wagner and Gooding 1987).
To exemplify the difficulties of participation research, the classic study by Coch and French (1948) is briefly described, followed by the critique of Bartlem and Locke (1981). The focus of the former study was overcoming resistance to change by means of participation. Operators in a textile plant where frequent transfers between work tasks occurred were given the opportunity to participate in the design of their new jobs to varying degrees. One group of operators participated in the decisions (detailed working procedures for new jobs and piece rates) through chosen representatives, that is, several operators of their group. In two smaller groups, all operators participated in those decisions and a fourth group served as control with no participation allowed. Previously it had been found in the plant that most operators resented being transferred and were slower in relearning their new jobs as compared with learning their first job in the plant and that absenteeism and turnover among transferred operators was higher than among operators not recently transferred.
This occurred despite the fact that a transfer bonus was given to compensate for the initial loss in piece-rate earnings after a transfer to a new job. Comparing the three experimental conditions it was found that the group with no participation remained at a low level of production—which had been set as the group standard—for the first month after the transfer, while the groups with full participation recovered to their former productivity within a few days and even exceeded it at the end of the month. The third group that participated through chosen representatives did not recover as fast, but showed their old productivity after a month. (They also had insufficient material to work on for the first week, however.) No turnover occurred in the groups with participation and little aggression towards management was observed. The turnover in the participation group without participation was 17% and the attitude towards management was generally hostile. The group with no participation was broken up after one month and brought together again after another two and one-half months to work on a new job, and this time they were given the opportunity to participate in the design of their job. They then showed the same pattern of recovery and increased productivity as the groups with participation in the first experiment. The results were explained by Coch and French on the basis of a general model of resistance to change derived from work by Lewin (1951, see below).
Bartlem and Locke (1981) argued that these findings could not be interpreted as support for the positive effects of participation because there were important differences between the groups as regards the explanation of the need for changes in the introductory meetings with management, the amount of training received, the way the time studies were carried out to set the piece rate, the amount of work available and group size. They assumed that perceived fairness of pay rates and general trust in management contributed to the better performance of the participation groups, not participation per se.
In addition to the problems associated with research on the effects of participation, very little is known about the processes that lead to these effects (e.g., Wilpert 1989). In a longitudinal study on the effects of participative job design, Baitsch (1985) described in detail processes of competence development in a number of shop-floor employees. His study can be linked to Deci’s (1975) theory of intrinsic motivation based on the need for being competent and self-determining. A theoretical framework focusing on the effects of participation on the resistance to change was suggested by Lewin (1951) who argued that social systems gain a quasi-stationary equilibrium which is disturbed by any attempt at change. For the change to be successfully carried through, forces in favour of the change must be stronger than the resisting forces. Participation helps in reducing the resisting forces as well as in increasing the driving forces because reasons for resistance can be openly discussed and dealt with, and individual concerns and needs can be integrated into the proposed change. Additionally, Lewin assumed that common decisions resulting from participatory change processes provide the link between the motivation for change and the actual changes in behaviour.
Participation in systems design
Given the—albeit not completely consistent—empirical support for the effectiveness of participation, as well as its ethical underpinnings in industrial democracy, there is widespread agreement that for the purposes of systems design a participative strategy should be followed (Greenbaum and Kyng 1991; Majchrzak 1988; Scarbrough and Corbett 1992). Additionally, a number of case studies on participative design processes have demonstrated the specific advantages of participation in systems design, for example, regarding the quality of the resulting design, user satisfaction, and acceptance (i.e., actual use) of the new system (Mumford and Henshall 1979; Spinas 1989; Ulich et al. 1991).
The important question then is not the if, but the how of participation. Scarbrough and Corbett (1992) provided an overview of various types of participation in the various stages of the design process (see table 3). As they point out, user involvement in the actual design of technology is rather rare and often does not extend beyond information distribution. Participation mostly occurs in the latter stages of implementation and optimization of the technical system and during the development of socio-technical design options, that is, options of organizational and job design in combination with options for the use of the technical system.
Table 3. User participation in the technology process
|
Type of participation |
||
|
Phases of technology process |
Formal |
Informal |
|
Design |
Trade union consultation |
User redesign |
|
Implementation |
New technology agreements |
Skills bargaining |
|
Use |
Job design |
Informal job redesign |
Adapted from Scarbrough and Corbett 1992.
Besides resistance in managers and engineers to the involvement of users in the design of technical systems and potential restrictions embedded in the formal participation structure of a company, an important difficulty concerns the need for methods that allow the discussion and evaluation of systems that do not yet exist (Grote 1994). In software development, usability labs can help to overcome this difficulty as they provide an opportunity for early testing by future users.
In looking at the process of systems design, including participative processes, Hirschheim and Klein (1989) have stressed the effects of implicit and explicit assumptions of system developers and managers about basic topics such as the nature of social organization, the nature of technology and their own role in the development process. Whether system designers see themselves as experts, catalysts or emancipators will greatly influence the design and implementation process. Also, as mentioned before, the broader organizational context in which participative design takes place has to be taken into account. Hornby and Clegg (1992) provided some evidence for the relationship between general organizational characteristics and the form of participation chosen (or, more precisely, the form evolving in the course of system design and implementation). They studied the introduction of an information system which was carried out within a participative project structure and with explicit commitment to user participation. However, users reported that they had had little information about the changes supposed to take place and low levels of influence over system design and related questions like job design and job security. This finding was interpreted in terms of the mechanistic structure and unstable processes of the organization that fostered “arbitrary” participation instead of the desired open participation (see table 2).
In conclusion, there is sufficient evidence demonstrating the benefits of participative change strategies. However, much still needs to be learned about the underlying processes and influencing factors that bring about, moderate or prevent these positive effects.
Mental Fatigue
Mental strain is a normal consequence of the coping process with mental workload (MWL). Long-term load or a high intensity of job demands can result in short-term consequences of overload (fatigue) and underload (monotony, satiation) and in long-term consequences (e.g., stress symptoms and work-related diseases). The maintenance of the stable regulation of actions while under strain can be realized through changes in one’s action style (by variation of strategies of information-seeking and decision-making), in the lowering of the level of need for achievement (by redefinition of tasks and reduction of quality standards) and by means of a compensatory increase of psychophysiological effort and afterwards a decrease of effort during work time.
This understanding of the process of mental strain can be conceptualized as a transactional process of action regulation during the imposition of loading factors which include not only the negative components of the strain process but also the positive aspects of learning such as accretion, tuning and restructuring and motivation (see figure 2).
Figure 1. Components of the process of strain and its consequences
Mental fatigue can be defined as a process of time-reversible decrement of behavioural stability in performance, mood and activity after prolonged working time. This state is temporarily reversible by changing the work demands, the environmental influences or stimulation and is completely reversible by means of sleep.
Mental fatigue is a consequence of performing tasks with a high level of difficulty that involve predominantly information processing and/or are of protracted duration. In contrast with monotony, the recovery of the decrements is time-consuming and does not occur suddenly after changing task conditions. Symptoms of fatigue are identified on several levels of behavioural regulation: dis-regulation in the biological homeostasis between environment and organism, dis-regulation in the cognitive processes of goal-directed actions and loss of stability in goal-oriented motivation and achievement level.
Symptoms of mental fatigue can be identified in all subsystems of the human information processing system:
- perception: reduced eye movements, reduced discrimination of signals, threshold deterioration
- information processing: extension of decision time, action slips, decision uncertainty, blockings, “risky strategies” in action sequences, disturbances in sensorimotor coordination of movements
- memory functions: prolongation of information in ultrashort-term storages, disturbances in the rehearsal processes in short-term memory, delay in information transmission in long-term memory and in memory searching processes.
Differential Diagnostic of Mental Fatigue
Sufficient criteria exist to differentiate amongst menta fatigue, monotony, mental satiation and stress (in a narrow sense) (table 1).
Table 1. Differentiation among several negative consequences of mental strain
|
Criteria |
Mental fatigue |
Monotony |
Satiation |
Stress |
|
Key |
Poor fit in terms of overload |
Poor fit in terms |
Loss of perceived sense of tasks |
Goals perceived |
|
Mood |
Tiredness without |
Tiredness with |
Irritability |
Anxiety, threat |
|
Emotional |
Neutral |
Neutral |
Increased affective aversion |
Increased anxiety |
|
Activation |
Continuously |
Not continuously |
Increased |
Increased |
|
Recovery |
Time-consuming |
Suddenly after task alternation |
? |
Long-term |
|
Prevention |
Task design, |
Enrichment of job content |
Goal-setting |
Job redesign, |
Degrees of Mental Fatigue
The well-described phenomenology of mental fatigue (Schmidtke 1965), many valid methods of assessment and the great amount of experimental and field results offer the possibility of an ordinal scaling of degrees of mental fatigue (Hacker and Richter 1994). The scaling is based on the individual’s capacity to cope with behavioural decrements:
Level 1: Optimal and efficient performance: no symptoms of decrement in performance, mood and activation level.
Level 2: Complete compensation characterized by increased peripheral psycho-physiological activation (e.g., as measured by electromyogram of finger muscles), perceived increase of mental effort, increased variability in performance criteria.
Level 3: Labile compensation additional to that described in level 2: action slips, perceived fatigue, increasing (compensatory) psycho-physiological activity in central indicators, heart rate, blood pressure.
Level 4: Reduced efficiency additional to that described in level 3: decrease of performance criteria.
Level 5: Yet further functional disturbances: disturbances in social relationships and cooperation at workplace; symptoms of clinical fatigue like loss of sleep quality and vital exhaustion.
Prevention of Mental Fatigue
The design of task structures, environment, rest periods during working time and sufficient sleep are the ways to reduce symptoms of mental fatigue in order that no clinical consequences will occur:
1. Changes in the structure of tasks. Designing of preconditions for adequate learning and task structuring is not only a means of furthering the development of efficient job structures, but is also essential for the prevention of a misfit in terms of mental overload or underload:
- Information processing burdens can be relieved by developing efficient internal task representations and organization of information. The resulting enlargement of cognitive capacity will match information needs and resources more aptly.
- Human-centred technologies with high compatibility between the order of information as it is presented and the required task (Norman 1993) will reduce the mental effort necessary for information recoding and, in consequence, relieve symptoms of fatigue and stress.
- Well-balanced coordination of different levels of regulations (as they apply to skills, rules and knowledge) may reduce effort and, moreover, increase human reliability (Rasmussen 1983).
- Training workers in goal-directed action sequences in advance of actual problems will lighten their sense of mental effort by making their jobs clearer, more predictable and more evidently under their control. Their psychophysiological activation level will be effectively reduced.
2. Introduction of systems of short-term breaks during work. The positive effects of such breaks depend on the observance of some preconditions. More short breaks are more efficient than fewer long breaks; effects depend on a fixed and therefore anticipatable time schedule; and the content of the breaks should have a compensatory function to the physical and mental job demands.
3. Sufficient relaxation and sleep. Special employee-assistant programmes and stress-management techniques may support the ability of relaxation and the prevention of the development of chronicle fatigue (Sethi, Caro and Schuler 1987).
Vigilance
The concept of vigilance refers to a human observer’s state of alertness in tasks that demand efficient registration and processing of signals. The main characteristics of vigilance tasks are relatively long durations and the requirement to detect infrequent and unpredictable target stimuli (signals) against a background of other stimulus events.
Vigilance Tasks
The prototypical task for vigilance research was that of radar operators. Historically, their apparently unsatisfactory performance during the Second World War has been a major impetus for the extensive study of vigilance. Another major task requiring vigilance is an industrial inspection. More generally, all kinds of monitoring tasks which require the detection of relatively infrequent signals embody the risk of failures to detect and to respond to these critical events.
Vigilance tasks make up a heterogeneous set and vary on several dimensions, in spite of their common characteristics. An obviously important dimension is the overall stimulus rate as well as the rate of target stimuli. It is not always possible to define the stimulus rate unambiguously. This is the case in tasks that require the detection of target events against continuously presented background stimuli, as in detecting critical values on a set of dials in a monitoring task. A less obviously important distinction is that between successive-discrimination tasks and simultaneous-discrimination tasks. In simultaneous-discrimination tasks, both target stimuli and background stimuli are present at the same time, while in successive-discrimination tasks one is presented after the other so that some demands on memory are made. Although most vigilance tasks require the detection of visual stimuli, stimuli in other modalities have also been studied. Stimuli can be confined to a single spatial location, or there can be different sources for target stimuli. Target stimuli can differ from background stimuli by physical characteristics, but also by more conceptual ones (like a certain pattern of meter readings that can differ from other patterns). Of course, the conspicuousness of targets can vary: some can be detected easily, while others may be hard to discriminate from background stimuli. Target stimuli can be unique or there can be sets of target stimuli without well-defined boundaries to set them off from background stimuli, as is the case in many industrial inspection tasks. This list of dimensions on which vigilance tasks differ can be expanded, but even this length of the list suffices to emphasize the heterogeneity of vigilance tasks and thus the risks involved in generalizing certain observations across the full set.
Performance Variations and the Vigilance Decrement
The most frequently used performance measure in vigilance tasks is the proportion of target stimuli, for example, faulty products in industrial inspection, that have been detected; this is an estimate of the probability of so-called hits. Those target stimuli that remain unnoticed are called misses. Although the hit rate is a convenient measure, it is somewhat incomplete. There is a trivial strategy that allows one to achieve 100% hits: one only has to classify all stimuli as targets. However, the hit rate of 100% is then accompanied by a false-alarm rate of 100%, that is, not only the target stimuli are correctly detected, but the background stimuli are incorrectly “detected” as well. This line of reasoning makes it quite clear that whenever there are false alarms at all, it is important to know their proportion in addition to the hit rate. Another measure for performance in a vigilance task is the time needed to respond to target stimuli (response time).
Performance in vigilance tasks exhibits two typical attributes. The first one is the low overall level of vigilance performance. It is low in comparison with an ideal situation for the same stimuli (short observation periods, high readiness of the observer for each discrimination, etc.). The second attribute is the so-called vigilance decrement, the decline of performance in the course of the watch which can start within the first few minutes. Both these observations refer to the proportion of hits, but they have also been reported for response times. Although the vigilance decrement is typical of vigilance tasks, it is not universal.
In investigating the causes of poor overall performance and vigilance decrements, a distinction will be made among concepts that are related to the basic characteristics of the task and concepts that are related to organismic and task-unrelated situational factors. Among the task-related factors strategic and non-strategic ones can be distinguished.
Strategic processes in vigilance tasks
The detection of a signal like a faulty product is partly a matter of the observer’s strategy and partly a matter of the signal’s discriminability. This distinction is based on the theory of signal detection (TSD), and some basics of the theory need to be presented in order to highlight the distinction’s importance. Consider a hypothetical variable, defined as “evidence for the presence of a signal”. Whenever a signal is presented, this variable takes on some value, and whenever a background stimulus is presented, it takes on a value that is lower on the average. The value of the evidence variable is assumed to vary across repeated presentations of the signal. Thus it can be characterized by a so-called probability density function as is illustrated in figure 1. Another density function characterizes the values of the evidence variable upon presentation of a background stimulus. When the signals are similar to the background stimuli, the functions will overlap, so that a certain value of the evidence variable can originate either from a signal or from a background stimulus. The particular shape of the density functions of figure 1 is not essential for the argument.
Figure 1. Thresholds and discriminability
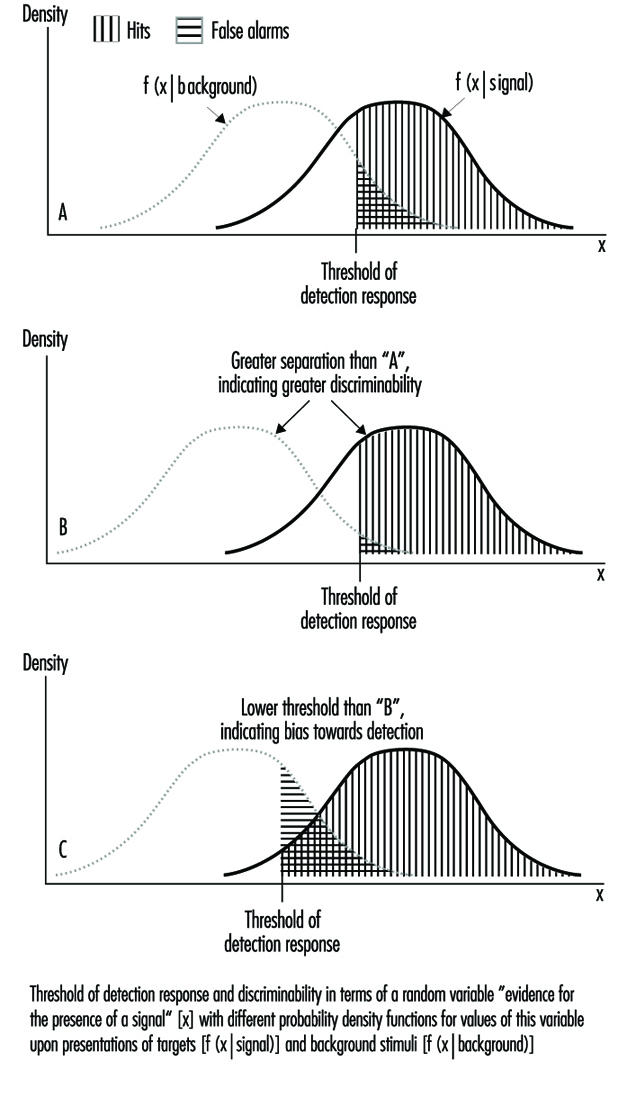
The detection response of the observer is based on the evidence variable. It is assumed that a threshold is set so that a detection response is given whenever the value of the evidence variable is above the threshold. As is illustrated in figure 1, the areas under the density functions to the right of the threshold correspond to the probabilities of hits and false alarms. In practice, estimates of the separation of the two functions and the location of the threshold can be derived. The separation of the two density functions characterizes the discriminability of the target stimuli from the background stimuli, while the location of the threshold characterizes the observer’s strategy. Variation of the threshold produces a joint variation of the proportions of hits and false alarms. With a high threshold, the proportions of hits and false alarms will be small, while with a low threshold the proportions will be large. Thus, the selection of a strategy (placement of the threshold) essentially is the selection of a certain combination of hit rate and false-alarm rate among the combinations that are possible for a certain discriminability.
Two major factors that influence the location of the threshold are payoffs and signal frequency. The threshold will be set to lower values when there is much to gain from a hit and little to lose from a false alarm, and it will be set to higher values when false alarms are costly and the benefits from hits are small. A low threshold setting can also be induced by a high proportion of signals, while a low proportion of signals tends to induce higher threshold settings. The effect of signal frequency on threshold settings is a major factor for the low overall performance in terms of the proportion of hits in vigilance tasks and for the vigilance decrement.
An account of the vigilance decrement in terms of strategic changes (threshold changes) requires that the reduction of the proportion of hits in the course of the watch is accompanied by a reduction of the proportion of false alarms. This is, in fact, the case in many studies, and it is likely that the overall poor performance in vigilance tasks (in comparison with the optimal situation) does also result, at least partly, from a threshold adjustment. In the course of a watch, the relative frequency of detection responses comes to match the relative frequency of targets, and this adjustment implies a high threshold with a relatively small proportion of hits and a relatively small proportion of false alarms as well. Nevertheless, there are vigilance decrements that result from changes in discriminability rather than from changes in threshold settings. These have been observed mainly in successive-discrimination tasks with a relatively high rate of stimulus events.
Nonstrategic processes in vigilance tasks
Although part of the overall poor performance in vigilance tasks and many instances of the vigilance decrement can be accounted for in terms of strategic adjustments of the detection threshold to low signal rates, such an account is not complete. There are changes in the observer during a watch that can reduce the discriminability of stimuli or result in apparent threshold shifts that cannot be considered as an adaptation to the task characteristics. In the more than 40 years of vigilance research, a number of nonstrategic factors that contribute to poor overall performance and to the vigilance decrement have been identified.
A correct response to a target in a vigilance task requires a sufficiently precise sensory registration, an appropriate threshold location, and a link between the perceptual processes and the associated response-related processes. During the watch the observers have to maintain a certain task set, a certain readiness to respond to target stimuli in a certain way. This is a nontrivial requirement because without a particular task set no observer would respond to target stimuli in the way required. Two major sources of failures are thus inaccurate sensory registration and lapses in the readiness to respond to target stimuli. Major hypotheses to account for such failures will be briefly reviewed.
Detection and identification of a stimulus are faster when there is no temporal or spatial uncertainty about its appearance. Temporal and/or spatial uncertainty is likely to reduce vigilance performance. This is the essential prediction of expectancy theory. Optimal preparedness of the observer requires temporal and spatial certainty; obviously vigilance tasks are less than optimal in this respect. Although the major focus of expectancy theory is on the overall low performance, it can also serve to account for parts of the vigilance decrement. With infrequent signals at random intervals, high levels of preparedness might initially exist at times when no signal is presented; in addition, signals will be presented at low levels of preparedness. This discourages occasional high levels of preparedness in general so that whatever benefits accrue from them will vanish in the course of a watch.
Expectancy theory has a close relation to attentional theories. Variants of attentional theories of vigilance, of course, are related to dominant theories of attention in general. Consider a view of attention as “selection for processing” or “selection for action”. According to this view, stimuli are selected from the environment and processed with high efficiency whenever they serve the currently dominant action plan or task set. As already said, the selection will benefit from precise expectations about when and where such stimuli will occur. But stimuli will only be selected if the action plan—the task set—is active. (Drivers of cars, for example, respond to traffic lights, other traffic, etc.; passengers don’t do so normally, although both are in almost the same situation. The critical difference is that between the task sets of the two: only the driver’s task set requires responses to traffic lights.)
The selection of stimuli for processing will suffer when the action plan is temporarily deactivated, that is when the task set is temporarily absent. Vigilance tasks embody a number of features that discourage continuous maintenance of the task set, like short cycle times for processing stimuli, lack of feedback and little motivational challenge by apparent task difficulty. So-called blockings can be observed in almost all simple cognitive tasks with short cycle times like simple mental arithmetic or rapid serial responses to simple signals. Similar blockings occur in the maintenance of the task set in a vigilance task as well. They are not immediately recognizable as delayed responses because responses are infrequent and targets that are presented during a period of absent task set may no longer be there when the absence is over so that a miss will be observed instead of a delayed response. Blockings become more frequent with time spent on the task. This can give rise to the vigilance decrement. There may be additional reasons for temporary lapses in the availability of the appropriate task set, for example, distraction.
Certain stimuli are not selected in the service of the current action plan, but by virtue of their own characteristics. These are stimuli that are intense, novel, moving toward the observer, have an abrupt onset or for any other reason might require immediate action no matter what the current action plan of the observer is. There is little risk of not detecting such stimuli. They attract attention automatically, as is indicated, for example, by the orienting response, which includes a shift of the direction of the gaze toward the stimulus source. However, answering an alarm bell is not normally considered a vigilance task. In addition to stimuli that attract attention by their own characteristics, there are stimuli that are processed automatically as a consequence of the practice. They seem to “pop out” from the environment. This kind of automatic processing requires extended practice with a so-called consistent mapping, that is, a consistent assignment of responses to stimuli. The vigilance decrement is likely to be small or even absent once automatic processing of stimuli has been developed.
Finally, vigilance performance suffers from a lack of arousal. This concept refers in a rather global manner to the intensity of neural activity, ranging from sleep through normal wakefulness to high excitement. One of the factors that is thought to affect arousal is external stimulation, and this is fairly low and uniform in most vigilance tasks. Thus, the intensity of central nervous system activity can decline overall over the course of a watch. An important aspect of arousal theory is that it links vigilance performance to various task-unrelated situational factors and factors related to the organism.
The Influence of Situational and Organismic Factors
Low arousal contributes to poor performance in vigilance tasks. Thus performance can be enhanced by situational factors that tend to enhance arousal, and it can be reduced by all measures that reduce the level of arousal. On balance, this generalization is mostly correct for the overall performance level in vigilance tasks, but the effects on the vigilance decrement are absent or less reliably observed across different kinds of manipulation of arousal.
One way to raise the level of arousal is the introduction of additional noise. However, the vigilance decrement is generally unaffected, and with respect to overall performance the results are inconsistent: enhanced, unchanged and reduced performance levels have all been observed. Perhaps the complex nature of noise is relevant. For example, it can be affectively neutral or annoying; it cannot only be arousing, but also be distracting. More consistent are the effects of sleep deprivation, which is “de-arousing”. It generally reduces vigilance performance and has sometimes been seen to enhance the vigilance decrement. Appropriate changes of vigilance performance have also been observed with depressant drugs like benzodiazepines or alcohol and stimulant drugs like amphetamine, caffeine or nicotine.
Individual differences are a conspicuous feature of performance in vigilance tasks. Although individual differences are not consistent across all sorts of vigilance tasks, they are fairly consistent across similar ones. There is only little or no effect of sex and general intelligence. With respect to age, vigilance performance increases during childhood and tends to decline beyond the age of sixty. In addition there is a good chance that introverts will show better performance than extroverts.
The Enhancement of Vigilance Performance
The existing theories and data suggest some means to enhance vigilance performance. Depending on the amount of specificity of the suggestions, it is not difficult to compile lists of various lengths. Some rather broad suggestions are given below that have to be fitted to specific task requirements. They are related to the ease of perceptual discriminations, the appropriate strategic adjustments, the reduction of uncertainty, the avoidance of the effects of attentional lapses and the maintenance of arousal.
Vigilance tasks require discriminations under non-optimal conditions. Thus one is well advised in making the discriminations as easy as possible, or the signals as conspicuous as possible. Measures related to this general goal can be straightforward (like appropriate lighting or longer inspection times per product) or more sophisticated, including special devices to enhance the conspicuousness of targets. Simultaneous comparisons are easier than successive ones, so the availability of a reference standard can be helpful. By means of technical devices, it is sometimes possible to present the standard and the object to be examined in rapid alternation, so that differences will appear as motions in the display or other changes for which the visual system is particularly sensitive.
To counteract the strategic changes of the threshold that lead to a relatively low proportion of correct detections of targets (and for making the task less boring in terms of the frequency of actions to be taken) the suggestion has been made to introduce fake targets. However, this seems not to be a good recommendation. Fake targets will increase the proportion of hits overall but at the cost of more frequent false alarms. In addition, the proportion of undetected targets among all stimuli that are not responded to (the outgoing faulty material in an industrial inspection task) will not necessarily be reduced. Better suited seems to be explicit knowledge about the relative importance of hits and false alarms and perhaps other measures to obtain an appropriate placement of the threshold for deciding between “good” and “bad”.
Temporal and spatial uncertainty are important determinants of poor vigilance performance. For some tasks, spatial uncertainty can be reduced by way of defining a certain position of the object to be inspected. However, little can be done about temporal uncertainty: the observer would be unnecessary in a vigilance task if the occurrence of a target could be signaled in advance of its presentation. One thing that can be done in principle, however, is to mix objects to be inspected if faults tend to occur in bunches; this serves to avoid very long intervals without targets as well as very short intervals.
There are some obvious suggestions for the reduction of attentional lapses or at least their impact on performance. By proper training, some kind of automatic processing of targets can perhaps be obtained provided that the background and target stimuli are not too variable. The requirement for sustained maintenance of the task set can be avoided by means of frequent short breaks, job rotation, job enlargement or job enrichment. Introduction of variety can be as simple as having the inspector himself or herself getting the material to be inspected from a box or other location. This also introduces self-pacing, which may help in avoiding signal presentations during temporary deactivations of the task set. Sustained maintenance of task set can be supported by means of feedback, indicated interest by supervisors and operator’s awareness of the importance of the task. Of course, accurate feedback of performance level is not possible in typical vigilance tasks; however, even inaccurate or incomplete feedback can be helpful as far as the observer’s motivation is concerned.
There are some measures that can be taken to maintain a sufficient level of arousal. Continuous use of drugs may exist in practice but is never found among recommendations. Some background music can be useful, but can also have an opposite effect. Social isolation during vigilance tasks should mostly be avoided, and during times of day with low levels of arousal like the late hours of the night, supportive measures such as short watches are particularly important.
Mental Workload
Mental Versus Physical Workload
The concept of mental workload (MWL) has become increasingly important since modern semi-automated and computerized technologies may impose severe requirements on human mental or information-processing capabilities within both manufacturing and administrative tasks. Thus, especially for the domains of job analysis, evaluation of job requirements and job design, the conceptualization of mental workload has become even more important than that of traditional physical workload.
Definitions of Mental Workload
There is no agreed-upon definition of mental workload. The main reason is that there are at least two theoretically well-based approaches and definitions: (1) MWL as viewed in terms of the task requirements as an independent, external variable with which the working subjects have to cope more or less efficiently, and (2) MWL as defined in terms of an interaction between task requirements and human capabilities or resources (Hancock and Chignell 1986; Welford 1986; Wieland-Eckelmann 1992).
Although arising from different contexts, both approaches offer necessary and well-founded contributions to different problems.
The requirements resources interaction approach was developed within the context of personality-environment fit/misfit theories which try to explain interindividually differing responses to identical physical and psychosocial conditions and requirements. Thus, this approach may explain individual differences in the patterns of subjective responses to loading requirements and conditions, for example, in terms of fatigue, monotony, affective aversion, burnout or diseases (Gopher and Donchin 1986; Hancock and Meshkati 1988).
The task requirements approach was developed within those parts of occupational psychology and ergonomics which are predominantly engaged in task design, especially in the design of new and untried future tasks, or so-called prospective task design. The background here is the stress-strain concept. Task requirements constitute the stress and the working subjects try to adapt to or to cope with the demands much as they would to other forms of stress (Hancock and Chignell 1986). This task requirements approach tries to answer the question of how to design tasks in advance in order to optimize their later impact on the—often still unknown—employees who will accomplish these future tasks.
There are at least a few common characteristics of both conceptualizations of MWL.
- MWL mainly describes the input aspects of tasks, that is to say, the requirements and demands made by the tasks on the employees, which might be used in forecasting the task outcome.
- The mental aspects of MWL are conceptualized in terms of information processing. Information processing includes cognitive as well as motivational/volitional and emotional aspects, since the persons always will evaluate the demands which they have to cope with and, thus, will self-regulate their effort for processing.
- Information-processing integrates mental processes, representations (for example, knowledge, or mental models of a machine) and states (for example, states of consciousness, degrees of activation and, less formally, mood).
- MWL is a multidimensional characteristic of task requirements, since every task varies in a couple of interrelated but nevertheless distinct dimensions which separately must be dealt with in task design.
- MWL will have a multidimensional impact which at least will determine (a) behaviour, for example, the strategies and the resulting performance, (b) perceived, subjective short-term well-being with consequences for health in the long run, and (c) psycho-physiological processes, for example, alterations of blood pressure at work, which may become long-term effects of a positive kind (promoting, say, fitness improvement) or of a negative kind (involving impairments or ill-health).
- From the point of view of task design, MWL should not be minimized—as would be necessary in the case of carcinogenic air pollution—but optimized. The reason is that demanding mental task requirements are inevitable for well-being, health promotion and qualification since they offer the necessary activating impulses, fitness prerequisites and learning/training options. Missing demands on the contrary may result in deactivation, loss of physical fitness, de-qualification and deterioration of so-called intrinsic (task content-dependent) motivation. Findings in this area led to the technique of health and personality promoting task design (Hacker 1986).
- MWL therefore, in any case, must be dealt with in task analysis, task requirement evaluation as well as in corrective and prospective task design.
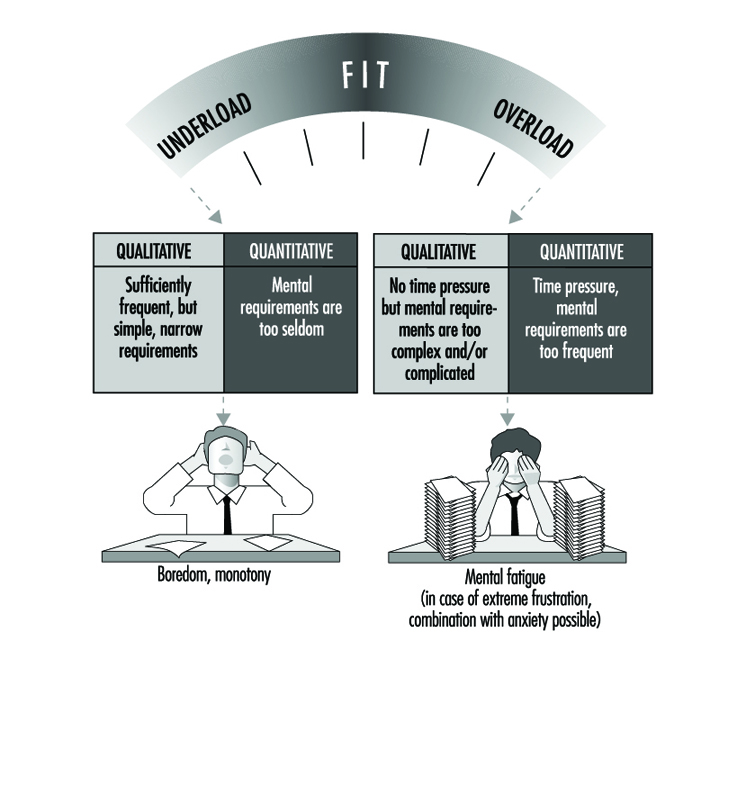
Theoretical Approaches: Requirement-Resources Approaches
From the person-environment fit point of view, MWL and its consequences may be roughly categorized—as is shown in figure 1—into underload, properly fitting load, and overload. This categorization results from the relationships between task requirements and mental capabilities or resources. Task requirements may exceed, fit with or fail to be satisfied by the resources. Both types of misfit may result from quantitative or qualitative modes of misfit and will have qualitatively differing, but in any case negative, consequences (see figure 1).
Figure 1. Types and consequences of requirements-resources relationships
Some theories attempt to define MWL starting from the resource or capacity side of the requirements, namely, resources relationships. These resource theories might be subdivided into resource volume and resource allocation theories (Wieland-Eckelmann 1992). The amount of available capacity may come from a single source (single resource theories) which determines processing. The availability of this resource varies with arousal (Kahneman 1973). Modern multiple resource theories suppose a set of relatively independent processing resources. Thus, performance will depend on the condition whether the same resource or different resources are required simultaneously and concurrently. Different resources are, for example, encoding, processing or responding resources (Gopher and Donchin 1986; Welford 1986). The most critical problem for these types of theories is the reliable identification of one or more well-defined capacities for qualitatively different processing operations.
Resource allocation theories suppose qualitatively changing processing as a function of varying strategies. Depending on the strategies, differing mental processes and representations may be applied for task accomplishment. Thus, not the volume of stable resources but flexible allocation strategies become the key point of interest. Again, however, essential questions—especially concerning the methods of diagnosis of the strategies—remain to be answered.
Assessment of MWL: using requirement-resource approaches
A strict measurement of MWL at present would be impossible since well-defined units of measurement are lacking. But, to be sure, the conceptualization and the instruments for an assessment should meet the general quality criteria of diagnostic approaches, which have objectivity, reliability, validity and usefulness. However, as of now, only a little is known about the overall quality of proposed techniques or instruments.
There are a sizeable number of reasons for the remaining difficulties with assessing MWL according to the requirement-resource approaches (O’Donnell and Eggemeier 1986). An attempt at MWL assessment has to cope with questions like the following: is the task self-intended, following self-set goals, or is it directed with reference to an externally defined order? Which type of capacities (conscious intellectual processing, application of tacit knowledge, etc.) are required, and are they called upon simultaneously or sequentially? Are there different strategies available and, if so, which ones? Which coping mechanisms of a working person might be required?
The most often discussed approaches try to assess MWL in terms of:
- required effort (effort assessment) approaches applying—in some versions psychophysiologically validated—scaling procedures such as those offered by Bartenwerfer (1970) or Eilers, Nachreiner and Hänicke (1986), or
- occupied or, vice versa, residual mental capacity (mental capacity assessment) approaches applying the traditional dual task techniques as, for example, discussed by O’Donnell and Eggemeier (1986).
Both approaches are heavily dependent on the assumptions of single resource theories and consequently have to struggle with the above-mentioned questions.
Effort assessment. Such effort assessment techniques as, for example, the scaling procedure applied to a perceived correlate of the general central activation, developed and validated by Bartenwerfer (1970), offer verbal scales which may be completed by graphic ones and which grade the unidimensionally varying part of the perceived required effort during task accomplishment. The subjects are requested to describe their perceived effort by means of one of the steps of the scale provided.
The quality criteria mentioned above are met by this technique. Its limitations include the unidimensionality of the scale, covering an essential but questionable part of perceived effort; the limited or absent possibility of forecasting perceived personal task outcomes, for example, in terms of fatigue, boredom or anxiety; and especially the highly abstract or formal character of effort which will identify and explain nearly nothing of the content-dependent aspects of MWL as, for example, any possible useful applications of the qualification or the learning options.
Mental capacity assessment. The mental capacity assessment consists of the dual task techniques and a related data interpretation procedure, called the performance operating characteristic (POC). Dual task techniques cover several procedures. Their common feature is that subjects are requested to perform two tasks simultaneously. The crucial hypothesis is: the less an additional or secondary task in the dual task situation will deteriorate in comparison with the base-line single task situation, the lower the mental capacity requirements of the primary task, and vice versa. The approach is now broadened and various versions of task interference under dual task conditions are investigated. For example, the subjects are instructed to perform two tasks concurrently with graded variations of the priorities of the tasks. The POC curve graphically illustrates the effects of possible dual-task combinations arising from sharing limited resources among the concurrently performed tasks.
The critical assumptions of the approach mainly consist in the suggestions that every task will require a certain share of a stable, limited conscious (versus unconscious, automated, implicit or tacit) processing capacity, in the hypothetical additive relationship of the two capacity requirements, and in the restriction of the approach to performance data only. The latter might be misleading for several reasons. First of all there are substantial differences in the sensitivity of performance data and subjectively perceived data. Perceived load seems to be determined mainly by the amount of required resources, often operationalized in terms of working memory, whereas performance measures seem to be determined predominantly by the efficiency of the sharing of resources, depending on allocation strategies (this is dissociation theory; see Wickens and Yeh 1983). Moreover, individual differences in information processing abilities and personality traits strongly influence the indicators of MWL within the subjective (perceived), performance and psychophysiological areas.
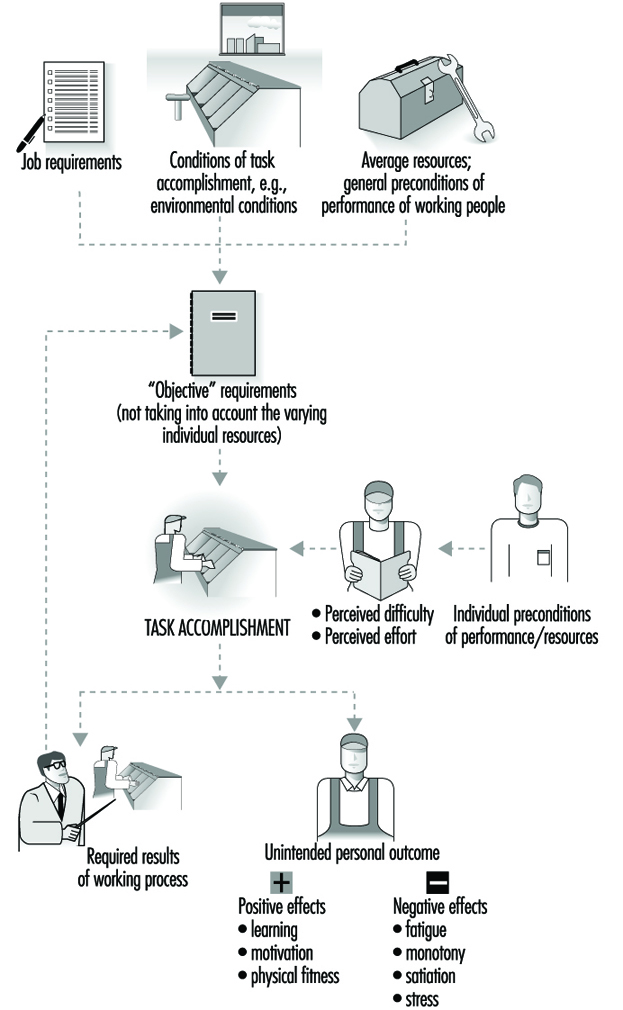
Theoretical Approaches: Task Requirement Approaches
As has been shown, task requirements are multidimensional and, thus, may not be described sufficiently by means of only one dimension, whether it be the perceived effort or the residual conscious mental capacity. A more profound description might be a profile-like one, applying a theoretically selected pattern of graded dimensions of task characteristics. The central issue is thus the conceptualization of “task”, especially in terms of task content, and of “task accomplishment”, especially in terms of the structure and phases of goal-oriented actions. The role of the task is stressed by the fact that even the impact of contextual conditions (like temperature, noise or working hours) on the persons are task-dependent, since they are mediated by the task acting as a gate device (Fisher 1986). Various theoretical approaches sufficiently agree regarding those critical task dimensions, which offer a valid prediction of the task outcome. In any case, task outcome is twofold, since (1) the intended result must be achieved, meeting the performance-outcome criteria, and (2) a number of unintended personal short-term and cumulative long-term side effects will emerge, for example fatigue, boredom (monotony), occupational diseases or improved intrinsic motivation, knowledge or skills.
Assessment of MWL. With task requirement approaches, action-oriented approaches like those of complete versus partialized actions or the motivation potential score (for an elaboration of both see Hacker 1986), propose as indispensable task characteristics for analysis and evaluation at least the following:
- temporal and procedural autonomy regarding decisions on self-set goals and, consequently, transparency, predictability and control of the work situation
- number and variety of subtasks (especially concerning preparation, organization and checking of the results of implementation) and of actions accomplishing these subtasks (i.e., whether such actions involve cyclical completeness versus fragmentation)
- variety (“level”) of action-regulating mental processes and representations. These may be mentally automated or routinized ones, knowledge-based “if-then” ones or intellectual and problem-solving ones. (They may also be characterized by hierarchical completeness as opposed to fragmentation)
- required cooperation
- long-term learning requirements or options.
The identification of these task characteristics requires the joint procedures of job/task analysis, including document analyses, observations, interviews and group discussions, which must be integrated in a quasi-experimental design (Rudolph, Schönfelder and Hacker 1987). Task analysis instruments which may guide and assist the analysis are available. Some of them assist only the analysis (for example, NASA-TLX Task Load Index, Hart and Staveland, 1988) while others are useful for evaluation and design or redesign. An example here is the TBS-GA (Tätigkeitsbewertungs System für geistige Arbeit [Task Diagnosis Survey—Mental Work]); see Rudolph, Schönfelder and Hacker (1987).
Environmental Health Issues
Forestry operations invariably affect the environment in one way or another. Some of these effects can be beneficial to the environment while others can be adverse. Obviously, it is the latter that is regarded with concern by both regulatory authorities and the public.
The Environment
When we speak of the environment, we often think of the physical and biological components of the environment: that is, the soil, the existing vegetation and wildlife and the waterways. Increasingly, the cultural, historic and amenity values associated with these more fundamental components are being considered part of the environment. Considering the impact of forest operations and management at the landscape level, not only on physical and biological objectives but also on the social values, has resulted in the evolution of concepts such as ecosystem management and forest stewardship. Therefore, this discussion of environmental health also draws on some of the social impacts.
Not All Bad News
Understandably, regulation and public concern regarding forestry throughout the world have focused on, and will continue to focus on, the negative impacts on environmental health. Despite this focus, forestry has the potential to benefit the environment. Table 1 highlights some of the potential benefits of both planting commercial tree species, and harvesting both natural and plantation forests. These benefits can be used to help establish the net effect (sum of positive and negative impacts) of forest management on environmental health. Whether such benefits accrue, and to what extent, often depends on the practices adopted (e.g., biodiversity depends on species mix, extent of tree mono-cultures and treatment of remnants of natural vegetation).
Table 1. Potential benefits to environmental health.
|
Forest operations |
Potential benefits |
|
Planting (afforestation) |
Increased carbon absorption (sequestration) Increased slope stability Increased recreational opportunity (amenity forests) Increased landscape biodiversity Flood control management |
|
Harvesting |
Increased public access Reduced wildfire and disease risk Promotion of secessional development of natural forests |
Environmental Health Issues
Despite there being major differences in forest resources, environmental regulations and concerns, as well as in forest practices throughout the world, many of the existing environmental health issues are generic across the forest industry. This overview focuses on the following issues:
- decline in soil quality
- soil erosion
- changes in water quality and quantity (including sedimentation)
- impacts on biodiversity
- adverse public perception of forestry
- discharge of chemicals (oil and pesticides) into the environment.
The degrees to which these general issues are a concern in a particular area will be largely dependent on the sensitivity of the forested area, and the nature of the water resources and water users downstream or offsite from the forest.
Activities within forested areas can affect other areas. These impacts can be direct, such as visual impacts, or they may be indirect, such as the effects of increased suspended sediment on marine farming activities. Therefore, it is important to recognize the pathways linking different parts of the environment. For example: skidder logging --- streamside soils --- stream water quality --- downstream recreational water users.
Decline in soil quality
Forest management can affect soil quality (Powers et al. 1990; FAO/ECE/ILO 1989, 1994). Where forests have been planted to rehabilitate degraded soils, such as eroded soils or mining overburden, this net impact may be an increase in quality by improving soil fertility and structural development. Conversely, forest activities on high-quality soil have the potential to reduce soil quality. Activities causing nutrient depletion, organic matter loss and structural loss through compaction are particularly important.
Soil nutrients are used by vegetation during the growing cycle. Some of these nutrients may be recycled back to the soil through litter fall, death or by residual logging waste. Where all the vegetative material is removed during harvest (i.e., whole tree harvest) these nutrients are removed from the onsite nutrient cycle. With successive growing and harvesting cycles, the store of available nutrients within the soil may decline to levels where growth rates and tree nutrient status cannot be sustained.
Burning of logging wastes has in the past been a preferred means of promoting regeneration or preparing a site for planting. However, research has shown that intensely hot burns can result in the loss of soil nutrients (carbon, nitrogen, sulphur and some phosphorus, potassium and calcium). The consequences of depleting the store of soil nutrients can be reduced tree growth and changes in species composition. The practice of replacing lost nutrients through inorganic fertilizers may address some of the nutrient depletion. However, this will not mitigate the effects of the loss of organic matter which is an important medium for soil fauna.
The use of heavy machinery for harvesting and preparation for planting can result in soil compaction. Compaction can cause reduced air and water movement in a soil and increase the strength of the soil to the extent that tree roots can no longer penetrate. Consequently, compaction of forest soils can reduce tree survival and growth and increase rainfall runoff and soil erosion. Importantly, without cultivation, compaction of subsoils may persist for 20 to 30 years after logging. Increasingly, logging methods that reduce the areas and degree of compaction are being used to reduce decline in soil quality. The codes of forest practices adopted in a growing number of countries and discussed in the article “Rules, legislation, regulations and codes of forest practices” in this chapter provide guidance on such methods.
Soil erosion
Soil erosion is a major concern to all land users, as it can result in irreversible loss of productive soils, adversely impact visual and amenity values, and may impact water quality (Brown 1985). Forests can protect soils from erosion by:
- intercepting rainfall
- regulating ground water levels
- increasing slope stability because of root growth
- protecting soil from wind and frost action.
However, when an area of forest is harvested, the level of soil protection is significantly reduced, increasing the potential for soil erosion.
It is recognized worldwide that forest operations associated with the following activities are major contributors to increased soil erosion during the forest management cycle:
- road work
- earthworks
- harvesting
- burning
- cultivation.
Road work activities, particularly in steep terrain where cut and fill construction is used, produce significant areas of loose unconsolidated soil material that are exposed to rainfall and runoff. If drainage control on roads and tracks is not maintained, they can channel rainfall runoff, increasing the potential for soil erosion on lower slopes and on the road edges.
Harvesting of forest trees can increase soil erosion in four main ways:
- exposing surface soils to rainfall
- reducing stand water usage, thereby increasing soil water contents and groundwater levels
- causing gradual decline in slope stability as the root system decomposes
- disturbance of soils during wood extraction.
Burning and cultivation are two techniques often used to prepare a site for regeneration or planting. These practices can increase the potential for surface erosion by exposing surface soil to the erosive effects of rainfall.
The degree of increased soil erosion, by either surface erosion or mass wasting, will depend on many factors including the size of the area logged, the slope angles, the strength of slope materials and the time since the harvesting occurred. Large clear cuts (i.e., total removal of almost all trees) can be a cause of severe erosion.
The potential for soil erosion can be very high during the first year after harvest relative to before road construction and harvesting. As the re-established or regenerating crop begins to grow, the risk of increased soil erosion decreases as water interception (protection of surface soils) and transpiration increase. Usually, the potential for increased erosion declines to pre-harvest levels once the forest canopy masks the ground surface (canopy closure).
Forest managers aim to reduce the period of vulnerability or the area of a catchment vulnerable at any one time. Staging the harvesting to spread harvesting over several catchments and reducing the size of individual harvest areas are two alternatives.
Changes in water quality and quantity
The quality of water discharged from undisturbed forest catchments is often very high, relative to agricultural and horticultural catchments. Certain forest activities can reduce the quality of water discharged by increasing nutrient and sediment contents, increasing water temperatures and decreasing dissolved oxygen levels.
Increased nutrient concentrations and exports from forest areas that have been burnt, undergone soil disturbance (scarification) or had fertilizer applied, can adversely effect water weed growth and cause pollution of downstream waters. In particular, nitrogen and phosphorus are important because of their association with toxic algae growth. Similarly, increased sediment input into waterways can adversely affect freshwater and marine life, flooding potential and water utilization for drinking or industrial uses.
The removal of streamside vegetation and the introduction of green and woody material into waterways during thinning or harvesting operations can adversely affect the aquatic ecosystem by increasing water temperatures and levels of dissolved oxygen in the water, respectively.
Forestry can also have an impact on the seasonal volume of water leaving a forest catchment (water yield) and peak discharges during storm events. Planting of trees (afforestation) in catchments previously under a pastoral farming regime can reduce water yields. This issue can be of particular importance where the water resource below an afforested area is utilized for irrigation.
Conversely harvesting within an existing forest can increase water yields because of the loss of water transpiration and interception, increasing the potential for flooding and erosion in the waterways. The size of a catchment and the proportion harvested at any one time will influence the extent of any water yield increase. Where only small proportions of a catchment are harvested, such as patch cuts, the effects on yield may be minimal.
Impacts on biodiversity
Biodiversity of plants and animals within forest areas has become an important issue for the forest industry worldwide. Diversity is a complex concept, not being confined to different plant and animal species alone. Biodiversity also refers to functional diversity (the role of a particular species in the ecosystem), structural diversity (layering within the forest canopy) and genetic diversity (Kimmins 1992). Forest operations have the potential to impact species diversity as well as the structural and functional diversity.
Identifying what is the optimum mix of species, ages, structures and functions is subjective. There is a general belief that a low level of species and structural diversity predisposes a forest to increased risk of disturbance with a pathogen or pest attack. To some extent this may be true; however, individual species in a mixed natural forest may suffer exclusively from a particular pest. A low level of biodiversity does not imply that a low level of diversity is an unnatural and unwanted outcome of forest management. For instance, many mixed species natural forests which are naturally subject to wildfire and pest attack go through stages of low species and structural diversity.
Adverse public perception of forestry
The public perception and acceptance of forest practice are two increasingly important issues for the forest industry. Many forest areas provide considerable recreational and amenity value to the resident and travelling public. The public often associates pleasurable outdoors experiences with mature managed and natural forested landscapes. Through insensitive harvesting, particularly large clearcuts, the forest industry has the potential to dramatically modify the landscape, the effects of which are often evident for many years. This contrasts with other land uses such as agriculture or horticulture, where the cycles of change are less evident.
Part of the negative public response to such activities stems from a poor understanding of forest management regimes, practices and outcomes. This clearly puts the onus on the forest industry to educate the public while at the same time modifying their own practices to increase public acceptance. Large clearcuts and the retention of logging residues (branch materials and standing dead wood) are two issues often causing public reaction because of the association of these practices with a perceived decline in ecosystem sustainability. However, this association may not be based in fact, as what is valued in terms of visual quality does not imply benefit for the environment. Retention of residues, although looking ugly, does provide habitat and food for animal life, and provides for some cycling of nutrients and organic matter.
Oil in the environment
Oil can be discharged in the forest environment through the dumping of machine oil and filters, the use of oil to control dust on unpaved roads and from chain-saws. Because of concerns about contamination of soil and water by mineral oil, oil dumping and its application on roads are becoming unacceptable practices.
However, the use of mineral oil to lubricate chain-saw bars is still common practice in much of the world. About 2 litres of oil are used by a single chain-saw per day, which adds up to considerable volumes of oil over a year. For example, it has been estimated that chain-saw oil usage was approximately 8 to 11.5 million litres/year in Germany, approximately 4 million litres/year in Sweden and approximately 2 million litres/year in New Zealand.
Mineral oil has been linked with skin disorders (Lejhancova 1968) and respiratory problems (Skyberg et al. 1992) in workers in contact with the oil. Furthermore, the discharge of mineral oil into the environment can result in soil and water contamination. Skoupy and Ulrich (1994) quantified the fate of chain-saw bar lubricant and found that between 50 and 85% was incorporated in the sawdust, 3 to 15% remained on trees, less than 33% was discharged onto the forest floor and 0.5% sprayed onto the operator.
Concerns primarily for the environment have led to biodegradable oils being compulsory in Swedish and German forests. Based on rapeseed or synthetic-based oils, these oils are more friendly to the environmentally and worker, and can also out-perform mineral-based lubricants by offering better chain life and reduced oil and fuel consumption.
Use of herbicides and insecticides
Herbicides (chemicals that kill plants) are employed by the forest industry to reduce weed competition for water, light and nutrients with young planted or regenerating trees. Often herbicides offer a cost-effective alternative to mechanical or manual weed control.
Despite there being a general mistrust of herbicides, possibly as a result of the use of Agent Orange during the Vietnam war, there have been no real documented adverse impacts on soils, wildlife and humans from herbicide use in forestry (Kimmins 1992). Some studies have found decreases in mammal numbers following herbicide treatment. However, by also studying the effects of manual or mechanical weed control, it has been shown that these decreases are coincidental with the loss of vegetation rather than the herbicide itself. Herbicides sprayed near waterways can potentially enter and be transported in the water, although herbicide concentrations are usually low and short term as dilution takes effect (Brown 1985).
Prior to the 1960s, the use of insecticides (chemicals that kill insects) by the agricultural, horticultural and public health sectors was widespread, with lesser amounts being used in forestry. Perhaps one of the more commonly used insecticides used during this time was DDT. Public reaction to health issues has largely curbed the indiscriminate use of insecticides, leading to the development of alternative practices. Since the 1970s, there have been moves towards the use of insect disease organisms, the introduction of insect pests and predators and modification of silvicultural regimes to reduce the risk of insect attack.
Living Conditions
Forestry operations, especially in developing countries, tend to be temporary and seasonal. In general, this work takes place far from urban centres, and workers must travel long distances every day or remain for several days or weeks in camps near the worksites. When workers commute from their homes every day, working conditions depend in large measure on their wages, the size of their family, their level of education and the access they have to health services. These variables, which are related to the level of development a nation has achieved and to the organization of the family group, are key to guaranteeing that basic necessities will be covered. These basic necessities include adequate nourishment, which is especially important given the intensity of the effort required of forestry workers. In many regions even commuting workers will still need protection against adverse weather conditions during breaks, particularly against rain and cold. Mobile shelters are available that are specially designed and equipped for forestry. If such forestry shelters are not provided, those used on construction sites can serve the purpose too. The situation in the camps is different, since their quality depends on the facilities provided by the company in terms of infrastructure and maintenance. The discussion which follows therefore refers to living conditions in forestry camps in so far as housing, leisure and nourishment are concerned.
Camp Infrastructure
Camps can be defined as temporary homes for forestry workers when they operate in remote or hard-to-reach locations. To fulfil their purpose, the camps should provide at least minimal levels of sanitation and comfort. It is therefore important to ask: How do different people interpret what these minimal levels should be? The concept is subjective, but it is possible to assert that, in the case of a camp, the minimal conditions required are that the infrastructure provide facilities and basic services that are consistent with human dignity, where each worker can partake with others on the crew without having to significantly alter his or her personal habits or beliefs.
One question that needs to be addressed when planning a forestry camp is the time that the camp will remain in a particular location. Since normally tasks must be shifted from one place to the other, fixed camps, while easier to set up and maintain, are not the solution that is usually required. In general, mobile structures are the most practical, and they should be easy to take down and move from one location to the next. This presents a complex problem, because even well-built modules deteriorate easily as they are moved. Conditions at mobile camps, therefore, tend to be very primitive.
In terms of facilities, a camp should offer an adequate supply of water, enough dormitories, a kitchen, bathrooms and recreation facilities. The size of each site will depend on the number of people who will be using it. In addition there should be separate stores for food, fuel, tools and materials.
Dormitories should allow workers to maintain their privacy. Since this is generally not possible in a camp, the number of people should not exceed six in each dormitory. This number has been arrived at through experience, since it has been found that a collapsible structure can accommodate six workers comfortably, allowing enough room for lockers where they can keep their personal belongings. In sharp contrast to this example, a dormitory that is crowded and dirty is absolutely inadequate for human use. An adequate dormitory is sanitary, with a clean floor, good ventilation and a minimal effort to create a comfortable atmosphere (e.g., with curtains and bedspreads of the same colour).
The kitchen, for its part, constitutes one of the most critical facilities in a camp. The first requirement is that the individuals in charge of the kitchen be skilled in sanitation and food handling. They should be licensed by an authorized authority and be supervised regularly. The kitchen should be easy to clean and should have adequate space for food storage. If food is stocked weekly or biweekly the kitchen should have a refrigerator to keep perishable food. It may be inconvenient and time-consuming for workers to return to camp for lunch: sanitary arrangements should be provided for packing lunches for workers to carry with them or to be delivered to them.
With regards to recreation facilities, mess halls are commonly used for this purpose. If workers are at their tasks all day and the only place to unwind is the eating quarters, these rooms should have enough of an infrastructure to allow workers to feel comfortable and recuperate physically and mentally from their workday. There should be adequate ventilation and, if the season requires, heating. Eating tables should not be for more than six people and should be lined with an easy to clean surface. If the dining-room is also used for recreation it should have, when possible, a television or a radio that can let workers stay in touch with the rest of the world. It is also advisable to provide some table games like checkers, cards and dominoes. Since among forestry workers there is an important contingent of young workers, it is not a bad idea to set up an area where they can play sports.
One aspect that is extremely important is the quality of sanitary facilities, showers and facilities for workers to wash and dry their belongings. It is important to keep in mind that faeces and waste in general are one of the most common avenues for the transmission of disease. It is therefore better to obtain water from a deep well than from a shallow one. If electric pumps can be installed, well-water may be raised into tanks that can then supply the camp. If for any reason it is not possible to erect sanitary services of this kind, chemical latrines should be installed. In any case, the elimination of human and other waste should be done carefully, making especially sure that they are not discharged in areas close to where food is kept or where drinking water is obtained.
Nutrition
Nutrition is a basic necessity for the maintenance of life and for the health of all human beings. Food provides not only nutrients but the energy required to carry out all activities in daily life. In the case of forestry workers, the caloric content of foods consumed is especially important because most of the harvesting, handling and forest protection activities demand great physical exertion (see the article “Physical load” in this chapter for data on energy consumption in forest work). Forestry workers need, therefore, more nourishment than people who do less demanding work. When a worker does not consume enough energy to offset daily energy expenditures, at first he or she will burn the reserves accumulated in body fat, losing weight. However, this can be done for only a limited time. It has been observed that, in the medium term, those workers who do not obtain in their diet the energy equivalent to their daily expenditures will limit their activity and lower their output. As a consequence, if they are paid by piece rate, their income also decreases.
Before analysing just how much energy a worker must consume as part of his or her diet, it bears mentioning that modern forestry work relies on increasingly sophisticated technology, where human energy is replaced by that of machinery. In those situations, operators run the risk of consuming more energy than they require, accumulating the excess as fat and risking obesity. In modern society, obesity is a malady that affects many people, but it is unusual in forestry workers where traditional methods are employed. According to studies carried out in Chile, it is becoming more common among machine operators. Obesity diminishes the quality of life because it is associated with a lower physical aptitude, predisposing those who suffer from it to accidents and to illnesses such as cardiovascular disease and more joint and muscle lesions.
For this reason all forestry workers, whether their daily activity is heavy or sedentary, should have access to a well-balanced diet that provides them with adequate amounts of energy. The key is to educate them so that they can regulate their food needs themselves. Unfortunately, this is a fairly difficult problem to solve; the tendency observed in studies carried out in Chile is for workers to consume all the food provided by the company and, in general, to still find their diet insufficient even though their weight variations indicate the opposite. The solution therefore is to educate the workers so that they learn to eat according to their energy requirements.
If workers are well informed about the problems created by eating too much, camps should offer diets keeping in mind the workers with the highest energy expenditures. The intake and expenditure of human energy is commonly expressed in kilojoules. However, the more widely known unit is the kilocalorie. The amount of energy required by a forestry worker when the job demands intense physical exertion, as in the case of a chain-saw operator or a worker using an axe, can reach 5,000 calories a day or even more. However, to expend those high amounts of energy, a worker must have a very good physical aptitude and reach the end of the workday without undue fatigue. Studies carried out in Chile have resulted in recommendations of an average of 4,000 calories provided daily, in the form of three basic meals at breakfast, lunch and dinnertime. This allows for the possibility of snacking at mid-morning and mid-afternoon so that additional amounts of energy can be provided. Studies over periods of more than a year have shown that, with a system like the one described, workers tend to maintain their body weight and increase their output and their incomes when pay is tied to their output.
A good diet must be balanced and provide, in addition to energy, essential nutrients for the maintenance of life and good health. Among other elements a diet should provide adequate amounts of carbohydrates, proteins, fats, minerals and vitamins. The tendency in developing countries is for groups that have low incomes to consume fewer proteins and fats and higher amounts of carbohydrates. The lack of the first two elements is due to a low consumption of foods of animal origin. In addition, a lack of certain vitamins and minerals has been observed due to a low consumption of foods of animal origin, fruits and vegetables. To summarize, the diet should be varied to balance the intake of essential nutrients. The most convenient option is to seek the help of specialized dieticians who know about the demands of heavy work. These professionals can develop diets that are reasonably cost efficient and that take into account the tastes, the traditions and the beliefs of the consumers and provide the amounts of energy required by forestry workers for their daily labour.
A very important element is a supply of liquid of good quality—not contaminated and in sufficient quantity. In manual and chain-saw work with high temperatures, a worker needs approximately 1 litre of liquid per hour. Dehydration drastically reduces working capacity and ability to concentrate, thereby increasing the risk of accidents. Therefore water, tea or other suitable drinks need to be available at the worksite as well as in the camp.
Consumption of alcohol and drugs should be strictly forbidden. Cigarette smoking, which is a fire hazard as well as a health hazard, should only be allowed in restricted areas and never in dormitories, recreation areas, dining halls and worksites.
Comments
This article has dealt with some of the general measures that can improve the living conditions and the diet of forestry camps. But while these two aspects are fundamental, they are not the only ones. It is also important to design the work in an ergonomically appropriate way because accidents, occupational injuries and the general fatigue that result from these activities have an impact on output and consequently on incomes. This last aspect of forestry work is of vital importance if workers and their families are to enjoy a better quality of life.
Skills and Training
Skills, Training and Exposure
In many industries, attention to safety in the design of equipment, workplaces and work methods can go a long way toward reducing occupational safety and health hazards. In the forestry industry, exposure to risks is largely determined by the technical knowledge, skill and experience of the individual worker and the supervisor, and their commitment to a joint effort in planning and performing the work. Training, therefore, is a crucial determinant of health and safety in forestry.
Studies in different countries and for different jobs in forestry all concur that three groups of workers have a disproportionately high accident frequency: the unskilled, often seasonal, workers; the young; and new entrants. In Switzerland, fully 73% of the accidents affect workers with less than one year in forestry; likewise, three-quarters of the accident victims had no or only rudimentary training (Wettman 1992).
Untrained workers also tend to have a much higher workload and higher risk of back injuries because of poor technique (see “Tree planting” in this chapter for an example). If training is critically important both from a safety and a productivity point of view in normal operations, it is absolutely indispensable in high-risk tasks like salvaging windblown timber or firefighting. No personnel should be allowed to participate in such activities unless they have been especially trained.
Training Forest Workers
On-the-job training is still very common in forestry. It is usually very ineffective, because it is a euphemism for imitation or simply trial and error. Any training needs to be based on clearly established objectives and on well-prepared instructors. For new chain-saw operators, for example, a two-week course followed by systematic coaching at the workplace is the bare minimum.
Fortunately, there has been a trend towards longer and well-structured training in industrialized countries, at least for directly employed workers and most new entrants. Various European countries have 2-to-3-year apprenticeships for forest workers. The structure of training systems is described and contacts to schools are listed in FAO/ECE/ILO 1996b. Even in these countries there is, however, a widening gap between the above and problem groups such as self-employed, contractors and their workers, and farmers working in their own forest. Pilot schemes to provide training for these groups have demonstrated that they can be profitable investments, as their cost is more than offset by savings resulting from reductions in accident frequency and severity. In spite of its demonstrated benefits and of some encouraging examples, like the Fiji Logging School, forest worker training is still virtually non-existent in most tropical and subtropical countries.
Forest worker training has to be based on the practical needs of the industry and the trainee. It has to be hands-on, imparting practical skill rather than merely theoretical knowledge. It can be provided through a variety of mechanisms. Schools or training centres have been used widely in Europe with excellent results. They do, however, carry a high fixed cost, need a fairly high annual enrolment to be cost-effective, and are often far from the workplace. In many countries mobile training has, therefore, been preferred. In its simplest form, specially prepared instructors travel to workplaces and offer courses according to programmes that may be standard or modular and adaptable to local needs. Skilled workers with some further training have been used very effectively as part-time instructors. Where demand for training is higher, specially equipped trucks or trailers are used as mobile classrooms and workshops. Designs and sample equipment lists for such units are available (Moos and Kvitzau 1988). For some target groups, such as contractors or farmers, mobile training may be the only way to reach them.
Minimum Competence Standards and Certification
In all countries, minimum standards of skill should be defined for all major jobs, at least in forest harvesting, the most hazardous operation. A very suitable approach to make sure minimum standards are defined and actually met in the industry is skill certification based on testing workers in short theoretical and practical exams. Most schemes place emphasis on standardized tests of workers’ skill and knowledge, rather than on whether these have been acquired through training or long experience. Various certification schemes have been introduced since the mid-1980s. In many cases certification has been promoted by workers’ compensation funds or safety and health directorates, but there have also been initiatives by large forest owners and industry. Standard tests are available for chain-saw and skidder operators (NPTC and SSTS 1992, 1993; Ministry of Skills Development 1989). Experience shows that the tests are transferable without or with only minor amendment. In 1995 for example the ILO and the Zimbabwe Forestry Commission successfully introduced the chain-saw test developed in an ILO logging training project in Fiji.
Working Conditions and Safety in Forestry Work
Safety in the forestry sector depends on matching individuals’ work capacities to the conditions under which they perform their tasks. The closer the mental and physical requirements of the work approach the workers’ capacities (which, in turn, vary with age, experience and health status), the less likely safety is to be sacrificed in an attempt to satisfy production goals. When individual capacities and working conditions are in a precarious balance, decreased individual and collective safety is inevitable.
As figure 1 illustrates, there are three sources of safety hazards related to working conditions: the physical environment (climate, lighting, terrain, types of trees), deficient safety laws and standards (inadequate content or application) and inappropriate work organization (technical and human).
Figure 1. Determinants of safety hazards in forestry work.
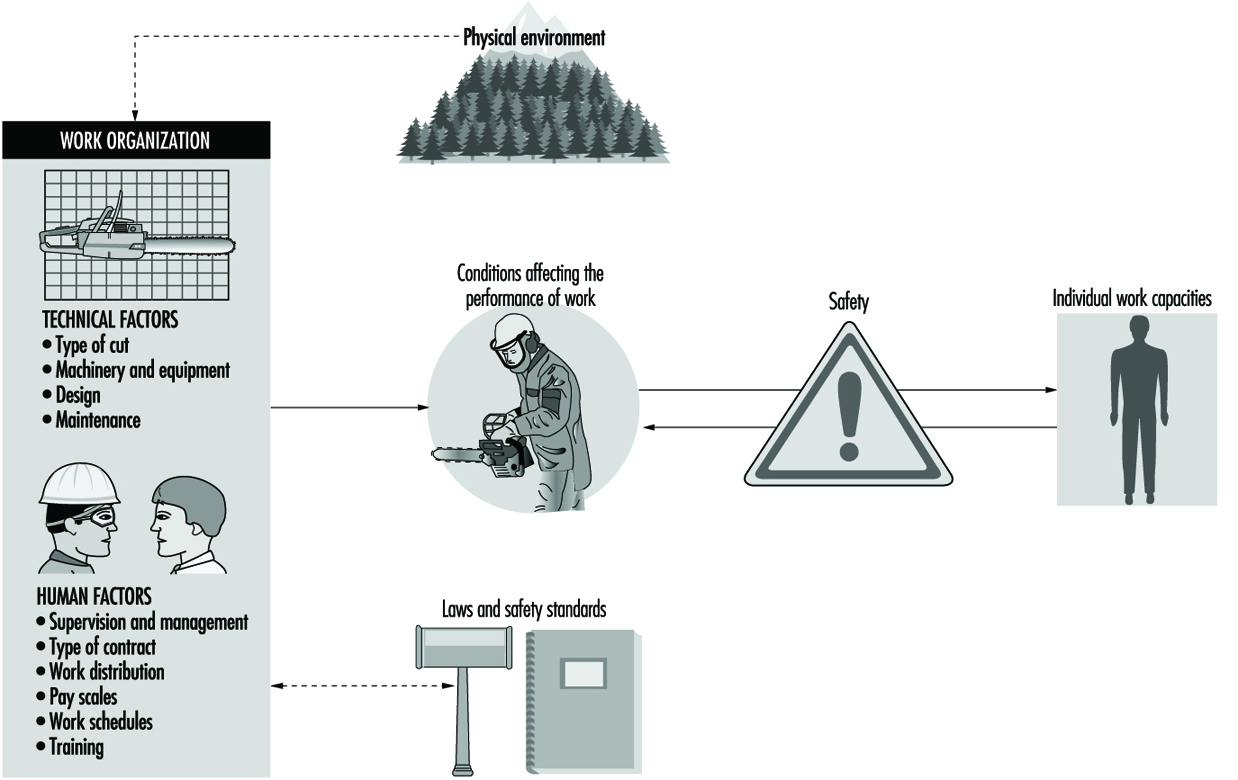
The technical and human organization of work encompasses potentially hazardous factors that are both distinct and tightly linked: distinct, because they refer to two intrinsically different resources (i.e., humans and machines); linked, because they interact and complement each other during the execution of work activities, and because their interaction allows production goals to be reached safely.
This article details how flaws in the components of work organization listed in figure 1 can compromise safety. It should be noted that measures to protect safety and health cannot be retro-fitted onto an existing work method, machine or organization. They need to be part of the design and planning.
Technical Work Organization
The term technical work organization refers to operational considerations of forestry work, including the type of cut, the choice of machinery and production equipment, equipment design, maintenance practices, size and composition of the work crew(s) and the time allotted in the production schedule.
Type of cut
There are two main types of cut used in forestry operations, distinguished by the technology used to fell and debranch trees: conventional cutting, which relies on mechanical saws, and mechanical cutting, which relies on machines operated from control cabins and equipped with articulated booms. In both cases, skidders, especially chain- or claw-propelled ones, are the usual means of transporting felled trees along the side of the road or waterways. Conventional cutting is the more widespread and the more dangerous of the two.
Mechanization of cutting is known to considerably reduce the frequency of accidents. This is most apparent for accidents occurring during production operations, and is due to the replacement of mechanical saws by machines operated from remote control cabins which isolate operators from hazards. At the same time, however, mechanization appears to increase the risk of accidents during machine maintenance and repair. This effect is due to both technological and human factors. Technological factors include machine deficiencies (see below) and the often improvised, if not frankly ludicrous, conditions under which maintenance and repair operations are performed. Human factors include the existence of production bonuses, which often result in low priority being given to maintenance and repair operations and the tendency to perform them hastily.
Machine design
There are no design codes for forestry machinery, and comprehensive maintenance manuals are rare. Machines such as fellers, debranchers and skidders are often a mixture of disparate components (e.g., booms, cabins, base machines), some of which are designed for use in other sectors. For these reasons, machinery used in forestry operations may be poorly suited to some environmental conditions, especially those related to the state of the forest and the terrain, and to continuous operation. Finally, machine repair is frequently necessary but very difficult to perform.
Machine and equipment maintenance
Maintenance practices in the forest are usually corrective rather than preventive. Various working conditions—such as production pressures, the absence of strict maintenance guidelines and schedules, the lack of appropriate maintenance and repair sites (garages, shelters), the harsh conditions under which these operations are performed, and the lack of adequate tools—may explain this situation. In addition, financial constraints may operate on one-person operations or sites operated by subcontractors.
Human Work Organization
The term human work organization refers to the way in which collective or individual human efforts are administered and organized, and to training policies designed to satisfy production requirements.
Supervision
Supervision of forestry work is not easy, due to the constant relocation of worksites and the geographic dispersion of workers over multiple worksites. Production is controlled through indirect strategies, of which production bonuses and the maintenance of precarious employment status are probably the most insidious. This type of work organization does not favour good safety management, since it is easier to transmit information concerning safety guidelines and regulations than it is to ensure their application and evaluate their practical value and the extent to which they are understood. Managers and supervisors need to be clear that they have primary responsibility for safety. As can be seen in figure 2 the worker controls very few of the elements that determine safety performance.
Figure 2. Human factors have an impact on safety in forest work.

Type of contract
Regardless of the type of cut, work contracts are almost always negotiated individually, and are often of fixed or seasonal duration. This precarious work situation is likely to lead to a low priority being accorded to personal safety, since it is difficult to promote occupational safety in the absence of minimal guarantees of employment. In concrete terms, fellers or operators may find it difficult to work safely if this compromises the production goals upon which their employment depends. Longer-term contracts of guaranteed minimum volumes per year stabilize the workforce and increase safety.
Subcontracting
Subcontracting the responsibility (and costs) for selected production activities to owner-operators is becoming more widespread in the forestry sector, as a result of mechanization and its corollary, work specialization (i.e., using a specific machine for tasks such as felling, pruning, felling-pruning and skidding).
Subcontracting may affect safety in several ways. In the first place, it should be recognized that subcontracting does not reduce safety hazards as such, but merely transfers them from the entrepreneur to the subcontractor. Secondly, subcontracting may also exacerbate certain hazards, since it stimulates production rather than safety-oriented behaviour. Subcontractors have in fact been observed to neglect some safety precautions, especially those related to preventive maintenance, training of new hires, the provision of personal protective equipment (PPE) and the promotion of its use, and the observance of safety rules. Finally, the responsibility for safety maintenance and management at worksites where subcontracting is practised is a judicial grey zone. It may even be difficult to determine the responsibility for declaring accidents to be work related. Work contracts should make compliance with safety regulations binding, include sanctions against offences, and assign responsibility for supervision.
Division of labour
The division of labour on forestry sites is often rigid and encourages specialization rather than flexibility. Task rotation is possible with conventional cutting, but is fundamentally dependent on team dynamics. Mechanized cutting, on the other hand, encourages specialization, although the technology itself (i.e., machine specialization) is not the sole cause of this phenomenon. Specialization is also encouraged by organizational factors (one operator per machine, shift work), geographic dispersion (remoteness of machines and cutting zones) and the fact that operators commonly own their machines.
Isolation and communication problems resulting from this division of labour may have serious consequences for safety, especially when they hamper the efficient circulation of information concerning imminent dangers or the occurrence of an incident or accident.
Work capacities of machines and workers need to be carefully matched and crews composed accordingly, to avoid overloading elements in the production chain. Shift schedules can be designed that maximize the use of expensive machines but give enough rest and variety of tasks to the operators.
Production-based pay scales
Forestry workers are frequently paid on a piece-work basis, which is to say that their salary is determined by their output (number of felled, pruned or transported trees, or some other index of productivity), not by its duration. For example, the rate which machine owners are paid for the use of their machines is proportional to their productivity. This type of pay scale, while not directly controlling workers, is notorious for stimulating production.
Production-based pay scales may encourage high work rates and the recourse to unsafe work practices during production and short-cuts in maintenance and repair operations. Practices like these persist because they save time, even though they ignore established safety guidelines and the risks involved. The greater the production incentive, the more safety is compromised. Workers paid on the basis of production have been observed to suffer more accidents, as well as different types of accidents, than hourly-paid workers performing the same type of work. Piece rates and prices for contracts need to be adequate for safe execution and acceptable working hours. (For a recent empirical study in Germany, see Kastenholz 1996.)
Work schedules
In the forest, long daily and weekly work schedules are the norm, since worksites and cutting zones are remote, work is seasonal, and the often difficult climatic and environmental factors encourage workers to work as long as possible. Other factors encouraging longer work schedules include production incentives (pay scales, subcontracting) and the possibility of using certain machines on a continuous basis (i.e., without stopping at night).
Long work schedules often result in decreased vigilance and a loss of sensory acuity, both of which may have effects on individual and collective safety. These problems are aggravated by the rarity and brevity of rest periods. Planned breaks and maximum working hours should be observed. Ergonomic research demonstrates that output can actually be increased that way.
Training
There can be no doubt that forestry work is physically and mentally demanding. The skill level required is continually increasing, as a result of technological advances and the growing complexity of machines. Prior and onsite training of forestry workers are therefore very important. Training programmes should be based on clearly defined objectives and reflect the actual work to be performed. The more the training programmes’ content corresponds to actual working conditions and the greater the integration of safety and production concerns, the more useful the programmes will be, both individually and collectively. Effective training programmes not only reduce material losses and production delays but also avoid additional safety hazards. For guidance on training, see “Skills and training” in this chapter.
Conclusion
The safety of forestry work is determined by factors related to work organization, and technical and human aspects of work organization may disrupt the equilibrium between production goals and safety. The influence of each individual factor on occupational safety will of course vary from setting to setting, but their combined effect will always be significant. Furthermore, their interaction will be the prime determinant of the degree to which prevention is possible.
It should also be noted that technological developments do not, in and of themselves, eliminate all hazards. Design criteria for machines should take into account their safe operation, maintenance and repair. Finally, it appears that some increasingly widespread management practices, especially subcontracting, may exacerbate rather than reduce safety hazards.
Personal Protective Equipment
Forestry work is one of those occupations where personal protective equipment (PPE) is always needed. Mechanization has decreased the number of workers using hand-held chain-saws, but the remaining tasks are often in difficult places where the big machines cannot reach.
The efficiency and chain speed of the hand-held chain-saws have increased, while the protection given by protective clothing and footwear has decreased. The higher requirement for the protection has made the equipment heavy. Especially in summertime in Nordic countries, and all around the year in other countries, the protective devices add an extra load to the heavy work of forest workers. This article focuses on chain-saw operators, but protection is needed in most forestry work. Table 1 provides an overview of what should normally be required.
Table 1. Personal protective equipment appropriate for forestry operations.
| Operations | PPE1 |
| Planting Manual Mechanized | Safety boots or shoes Safety boots or shoes, close-fit clothing, ear muffs2 |
| Weeding/cleaning Smooth-edged tools Hand-saw Chain-saw | Safety boots or shoes, gloves, goggles Safety boots or shoes, gloves Safety boots or shoes,3 safety trousers, close-fit clothing, gloves,4 safety helmet, goggles, visor (mesh), ear muffs |
| Brush saw: with metal blade with nylon filament | Safety boots or shoes,3 safety trousers, close-fit clothing, gloves,4 safety helmet, goggles, visor (mesh), ear muffs Safety boots or shoes, safety trousers, gloves, goggles, ear muffs |
| Rotating knife/flail | Safety boots or shoes, close-fit clothing, gloves, ear muffs2 |
| Pesticide application | To comply with the specifications for the particular substance and application technique |
| Pruning5 Hand tools | Safety boots or shoes, gloves, safety helmet, 6 goggles, ear muffs |
| Felling7 Hand tools Chain-saw | Safety boots or shoes, close-fit clothing, gloves,8 safety helmet Safety boots or shoes, safety trousers, close-fit clothing, gloves,4 safety helment, visor (mesh), ear muffs |
| Mechanized | Safety boots or shoes, close-fit clothing, safety helmet, ear muffs |
| Debarking Manual Mechanized | Safety boots or shoes, gloves Safety boots or shoes, close-fit clothing, gloves, goggles, ear muffs2 |
| Splitting Manual Mechanized | Safety boots or shoes, gloves, goggles Safety boots or shoes, close-fit clothing, gloves, goggles, ear muffs |
| Extraction Manual, chute and animal Mechanized -skidder -forewarder -cable crane -heliocopter | Safety boots or shoes, gloves, safety helmet9 Safety boots or shoes, close-fit clothing, gloves,10 safety helmet, ear muffs2 Safety boots or shoes, close-fit clothing, safety helmet, ear muffs2 Safety boots or shoes, close-fit clothing, gloves,10 safety helmet, ear muffs2 Safety boots or shoes, close-fit clothing,11 gloves,10 safety helmet, goggles, ear muffs |
| Stacking/loading | Safety boots or shoes, close-fit clothing, gloves, safety helmet, ear muffs2 |
| Chipping | Safety boots or shoes, close-fit clothing, gloves, safety helmet, visor (mesh), ear muffs2 |
| Tree climbing: using a chain-saw not using a chain-saw | Safety boots or shoes,3 safety trousers, close-fit clothing, gloves,4 safety helmet,13 goggles, ear muffs Safety boots or shoes, safety helmet |
1 Safety boots or shoes should include integrated steel toes for medium or heavy loads. Safety trousers should incorporate clogging material; in hot climates/weather chain-saw leggings or chaps may be used. Safety trousers and chaps contain fibres that are inflammable and can melt; they should not be worn during firefighting. Ear plugs and ear valves are generally not suitable for forestry because of risk of infection.
2 When noise level at work position exceeds 85 dBA.
3 Chain-saw boots must have protective guarding at front vamp and instep.
4 Cut-resistant material must be incorporated.
5 If pruning involves tree climbing above 3 m, a fall-restricting device should be used. PPE must be used when falling branches are likely to cause injury.
6 When pruning to a height exceeding 2.5 m.
7 Felling includes debranching and crosscutting.
8 When using a hand-saw.
9 When extracting near unstable trees or branchwood.
10 Only if manipulating logs; gloves with heavy-duty palm if handling wire choker rope or tether line.
11 Highly visible colours should be used.
12 Helmet must have a chin strap.
13 Climbing helmets are preferable; if they are not available, safety helmets with chin straps may be used.
Source: ILO 1997.
Protection Mechanism and Efficiency of Personal Protective Devices
Protective clothing
Protective clothing against cuts protects by three different main mechanisms. In most cases the trousers and gloves contain a safety padding made of multilayer cloth having fibres with high tensile strength. When the moving chain touches the fibres, they are pulled out and will resist the movement of the chain. Second, these padding materials can go around the drive sprocket and the groove of the blade and increase the friction of the chain against the blade so much that the chain will stop. Third, the material can also be made such that the chain glides on the surface and cannot easily penetrate it.
Different work tasks require different protective coverage. For normal forest work the protective padding covers only the front part of the trousers and the back of safety gloves. Special tasks (e.g., gardening or tree surgery) often require a larger area of protective coverage. The protective paddings cover the legs totally, including the back side. If the saw is held above the head, protection of the upper body may be needed.
It must always be remembered that all PPE gives only limited protection, and correct and careful working methods must be used. The new hand-held chain-saws are so effective that the chain can easily go through the best protective material when the chain speed is high or the force of the chain against the protective material is great. Cut-proof protective paddings made of the best materials known at present would be so thick that they could not be used in heavy forest work. The compromise between protection efficiency and comfort is based on field experiments. It has been unavoidable that the protection level has been reduced to be able to increase the comfort of the clothing.
Protective footwear
Protective footwear made of rubber resists against cuts by the chain-saw quite well. The most frequent type of cut comes from contact of the chain with the toe area of the footwear. The safety footwear must have a cut-resistant lining on the front and metallic toe cups; this protects against these cuts very well. In higher temperatures the use of rubber boots is uncomfortable, and leather boots or ankle-high shoes should be used. These shoes too must be equipped with metallic toe cups. The protection is normally considerably lower than that of the rubber boots, and extra care should be taken when using leather boots or shoes. The working methods must be so planned that the possibility of chain contact with the feet is minimized.
Good fit and construction of the outer sole is essential to avoid slipping and falling accidents, which are very common. In areas where the ground may be covered by ice and snow or where workers walk on slippery logs, boots which can be equipped with spikes are preferred.
Protective helmet
Protective helmets provide protection against falling branches and trees. They also give protection against the chain-saw if a kick-back occurs. The helmet should be as light as possible to minimize neck strain. The headband must be correctly adjusted to make the helmet sit firmly on the head. The headbands of most helmets are so designed that vertical adjustment is possible as well. It is important to have the helmet sitting low on the brow so its weight does not cause too much discomfort when working in face-down posture. In cold weather it is necessary to use a textile or fur cap under the helmet. Special caps designed to be used with the helmet should be used. The cap can lower the protection efficiency of the helmet by wrong positioning of the helmet. The protection efficiency of hearing protectors can go to near zero when the cups of the hearing protectors are placed outside the cap. Forestry helmets have built-in devices to attach a visor and earmuffs for hearing protection. The cups of the hearing protectors should be placed directly against the head by insertion of the cups through slits in the cap.
In hot weather, helmets should have ventilation holes. The holes have to be part of the design of the helmet. Under no circumstances should holes be drilled into the helmet, as this may greatly reduce its strength.
Face and eye protection
The face protector or shield is normally attached to the helmet and is most commonly made of a mesh material. The plastic sheets easily get dirty after a relatively short working time. Cleaning is also difficult because the plastics resist solvents poorly. The mesh reduces the light coming to the eyes of the worker, and reflections on the surface of the threads can make seeing difficult. Sealed goggles worn under face protectors mist easily, and distortion of vision is often too high. Metal masks with a black coating and rectangular rather than round openings are preferable.
Hearing protectors
Hearing protectors are efficient only if the cups are placed firmly and tightly against the head. Therefore hearing protectors must be used carefully. Any space between the head and the sealing rings of the cups will decrease the efficiency markedly. For example, the side-arms of spectacles can cause this. The sealing ring shall be inspected often and must be changed when damaged.
Selection of Personal Protective Equipment
Before starting work in a new area, the possible risks should be evaluated. The working tools, methods, environment, the skills of the workers and so on should be evaluated, and all technical and organizational measures should be planned. If the risks cannot be eliminated by those methods, PPE can be used to improve the protection. PPE can never be used as the only preventive method. It must be seen as a complementary means only. The saw must have a chain brake, the worker must be trained and so on.
On the basis of this risk analysis, the requirements for personal protective devices must be defined. Environmental factors should be taken into account in order to minimize the load cased by the equipment. The hazard caused by the saw must be evaluated and the protection area and efficiency of clothing defined. If the workers are not professionals, the protection area and level should be higher, but this extra loading must be taken into account when the work periods are planned. After the requirements for PPE are defined according to the risks and tasks, the proper equipment is selected from among devices that have been approved. The workers should have the privilege of trying different models and sizes to select the one that best suits them. Improperly selected clothing can cause abnormal postures and movements, and thus can increase accident and health hazard risks. Figure 1 illustrates the selection of equipment.
Figure 1. Bodily location of injuries and personal protective equipment recommended for forest work, the Netherlands, 1989.

Determination of the Conditions of Use
All workers should be efficiently instructed and trained in the use of PPE. The protection mechanism must be described so that the workers themselves can inspect and evaluate the condition of the equipment daily. The consequences of non-use must be made clear. Proper cleaning and repair instructions must be given.
The protective equipment used in forestry work may constitute a relatively great extra burden to the worker. This must be taken into account when planning the working times and rest periods.
Often the use of PPE gives a false sense of safety. The supervisors must make sure that risk taking is not increasing and that the workers know well the limits of the protection efficiency.
Care and Maintenance
Improper methods used for maintenance and repair can destroy the protection efficiency of the equipment.
The shell of the helmet must be cleaned by weak detergent solutions. Resins cannot be removed efficiently without the use of solvents, but the use of solvents should be avoided because the shell can be damaged. The instructions of the manufacturer must be followed and the helmet discarded if it cannot be cleaned. Some materials are more resistant against the effects of solvents, and those should be selected for forest work use.
Also other environmental factors affect the materials used in a helmet. Plastic materials are sensitive to ultraviolet (UV) radiation of the sun, which makes the shell more rigid, especially at low temperatures; this ageing weakens the helmet, and it will not protect against impacts as planned. The ageing is difficult to see, but small hairline cracks and the loss of gloss can be signs of ageing. Also, when gently twisted, the shell may make cracking noises. The helmets should be carefully visually inspected at least every six months.
If the chain has been in contact with the trousers, the protection efficiency can be much reduced or disappear totally. If the safety padding fibres are drawn out, the trousers should be discarded and new ones should be used. If only the outer material is damaged it can be repaired carefully without making any stitches through the safety padding. The protection efficiency of safety trousers is commonly based on the strong fibres, and if those are fixed tightly during repair they will not provide protection as planned.
Washing must be done according to the instructions given by the manufacturer. It has been shown that wrong washing methods can destroy protection efficiency. The clothing of the forest worker is difficult to clean, and products should be selected which withstand the hard washing methods needed.
How the Approved Protective Equipment is Marked
The design and quality of manufacture of PPE must meet high standards. In the European Economic area, personal protective devices must be tested before they are placed on the market. The basic health and safety requirements for PPE are described in a directive. To clarify those requirements European harmonized standards have been drafted. The standards are voluntary, but devices designed to meet the requirements in the appropriate standards are deemed to meet the requirements of the directive. The International Standards Organization (ISO) and the European Committee for Standardization (CEN) are working on these standards together according to the Vienna Agreement. So there will be technically identical EN and ISO standards.
Accredited test stations are testing the devices and issuing a certificate if they meet the requirements. After that the manufacturer can mark the product with CE-marking, which shows that the conformity assessment has been carried out. In other countries the procedure is similar and the products are marked with the national approval mark.
An essential part of the product is the leaflet giving the user information about its proper use, the degree of protection it can provide and instructions for its cleaning, washing and repair.
Rules, Legislation, Regulations and Codes of Forest Practices
In a high-risk occupation like forestry, relevant and job-specific safety regulations are a critical element of any strategy to reduce the high frequencies of accidents and health problems. To develop such regulation and to obtain compliance is unfortunately much more difficult in forestry than in many other occupations. Occupational safety legislation and existing general regulations are often not specific for forestry. Moreover, they are often difficult to apply in the highly variable outdoor context of forestry, because they were typically conceived with factory-type workplaces in mind.
This article outlines the route from general legislation to forestry-specific regulations and makes some suggestions for contributions that the various actors in the forestry sector may make to the improvement of compliance with regulations. It concludes with a brief presentation of the concept of codes of forest practices, which holds considerable promise as a form of regulation or self-regulation.
The Law Outlines the Principles
Safety legislation usually merely lays out some basic principles, such as:
- The employer is primarily responsible for the safety of employees and must take the necessary protective measures.
- Employees must be involved in this.
- Employees, in turn, are obliged to support the employer’s efforts.
- Laws are enforced through the labour inspectorate, the health service or an analogous body.
What the General Regulations Specify
Regulations on prevention of accidents and occupational diseases often specify a number of points, such as:
- the duties of employers and employees
- the consultation of doctors and other occupational safety specialists
- the safety regulations for buildings and other construction, for technical equipment and devices, and on the working environment and the work organization.
The regulations also contain instructions on:
- organization of workplace safety
- implementing the provisions on workplace safety
- occupational medical care
- financing workplace safety.
As the legislation has evolved over time, there are often laws for other areas and sectors that also contain regulations applicable to workplace safety in forestry. In Switzerland, for example, these include the labour code, the law on explosives, the law on poisons and traffic legislation. It would be advantageous to users if all these provisions and related regulations were collected into a single law.
Safety Regulations for Forestry: As Concrete as Possible and Nevertheless Flexible
In most cases, these laws and regulations are too abstract for daily, on-the-job use. They do not correspond to the hazards and risks involved in using machines, vehicles and work materials in the various industries and plants. This is particularly true for a sector with such varied and atypical working conditions as forestry. For this reason, specific safety regulations are worked out by sectoral commissions for the individual industries, their specific jobs, or equipment and devices. In general, this proceeds consciously or unconsciously as follows:
First, the dangers that can arise in an activity or a system are analysed. For example, cuts into the leg are a frequent injury among chain-saw operators.
Second, protection goals that are based on the dangers identified and which describe “what should not happen” are enunciated. For example: “Appropriate measures should be taken to prevent the chain-saw operator from injuring his or her leg”.
Only in the third step are solutions or measures sought that, in accordance with the state of technology, reduce or eliminate the dangers. In the above-mentioned example, cut-protected trousers are one of the appropriate measures. The state of technology for this item can be defined by requiring that trousers correspond to European Norms (EN) 381-5, Protective clothing for users of hand-operated chain-saws, Part 5: Regulations for leg protection.
This procedure offers the following advantages:
- Protective goals are based on concrete hazards. The safety requirements are therefore practice-oriented.
- Safety regulations in the form of protective goals allow for greater flexibility in the choice and development of solutions than the prescription of concrete measures. Specific measures can also be adapted continuously to advances in the state of technology.
- When new hazards appear, safety regulations can be supplemented in a targeted manner.
Establishing bi- or tripartite sectoral commissions that involve the interested employer and employee organizations has proven an effective way of improving the acceptance and application of safety regulations in practice.
Content of Safety Rules
When certain jobs or types of equipment have been analysed for their hazards and protective goals derived, measures in the areas of technology, organization and personnel (TOP) can be formulated.
Technical questions
The state of technology for part of the forestry equipment and devices, such as power saws, brush cutters, leg protection for power saw operators and so on, is set in international norms, as discussed elsewhere in this chapter. Over the long term, the EN and the norms of the International Organization for Standardization (ISO) should be unified. Adoption of these norms by the individual countries will contribute to the uniform protection of the employee in the industry. Proof from the seller or manufacturer that a piece of equipment complies with these standards guarantees to the buyer that the equipment corresponds to the state of technology. In the numerous cases where no international standards exist, national minimum requirements need to be defined by groups of experts.
In addition to the state of technology, the following issues, among other things, are important:
- availability of the necessary equipment and materials on the job
- reliable condition of the equipment and materials
- maintenance and repair.
Forestry operations often leave much to be desired in these respects.
Organizational questions
Conditions must be established in the enterprise and at the workplace so that the individual jobs can be carried out safely. In order for this to happen, the following issues must be addressed:
- tasks, authority and responsibilities of all participants clearly defined
- a wage system that promotes safety
- working hours and breaks adapted to the difficulty of the work
- work procedures
- work planning and organization
- first aid and alarms
- where workers have to live in camps, minimum requirements defined for dormitories, sanitation, nutrition, transport and recreation.
Personnel questions
Personnel questions can be divided into:
Training and continuing education. In some countries this includes employees of forestry companies, for example, those who work with power saws are obliged to attend appropriate training and continuing education courses.
Guidance, welfare and support of the employee. Examples include showing new employees how the job is done and supervising the employees. Practice shows that the state of workplace safety in an enterprise depends in large measure on whether and how the management maintains discipline and carries out its supervisory responsibilities.
Doing the job
Most safety regulations contain rules of behaviour that the employee is supposed to abide by in doing the job. In forestry work these rules relate primarily to critical operations such as:
- felling and working with trees
- extraction, storing and transporting wood
- working with wind-felled trees
- climbing trees and working in treetops.
In addition to international standards and national regulations that have proved effective in several countries, the International Labour Organization (ILO) Code of Practice Safety and Health in Forestry Work provides examples and guidance for the design and formulation of national or company-level regulations (ILO 1969, 1997, 1998).
Safety regulations have to be reviewed and constantly adapted to changing circumstances or supplemented to cover new technology or work methods. A suitable accident reporting and investigation system can be of great help toward this end. Unfortunately, few countries are making use of this possibility. The ILO (1991) provides some successful examples. Even rather simple systems can provide good pointers. (For further information see Strehlke 1989.) The causes of accidents in forestry are often complex. Without a correct and full understanding, preventive measures and safety regulations often miss the point. A good example is the frequent but often erroneous identification of “unsafe behaviour” as the apparent cause. In accident investigation, the emphasis should as much as possible be on understanding the causes of accidents, rather than on establishing the responsibility of individuals. The “tree of causes” method is too onerous to be used routinely, but has given good results in complicated cases and as a means of raising safety awareness and of improving communication in enterprises. (For a report on the Swiss experience see Pellet 1995.)
Promoting Compliance
Safety regulations remain a dead letter unless all stakeholders in the forestry sector play their part in implementation. Jokulioma and Tapola (1993) give a description of such cooperation in Finland, which has produced excellent results. For information, education and training on safety, including for groups that are difficult to reach like contractors and forest farmers, the contractor and forest owner associations play a critical role.
Safety regulations need to be made available to users in accessible form. A good practice is the publishing in a pocket-size format of illustrated concise extracts relevant to particular jobs such as chain-saw operation or cable cranes. In many countries migrant workers account for a significant percentage of the forestry workforce. Regulations and guides need to be available in their respective languages. Forestry equipment manufacturers should also be required to include in the owner’s manual comprehensive information and directions on all aspects of the maintenance and safe use of the equipment.
The cooperation of workers and employers is of course particularly important. This is true at the sectoral level, but even more so at the enterprise level. Examples for successful and very cost effective cooperation are given by the ILO (1991). The generally unsatisfactory safety situation in forestry is often aggravated further where the work is carried out by contractors. In such cases, the contracts offered by the commissioning party, forest owner or industry should always include a clause requiring compliance with safety requirements as well as sanctions in cases of breach of regulations. The regulations themselves should be an annex to the contract.
In some countries, general legislation provides for a joint or subsidiary responsibility and liability of the commissioning party—in this case a forest owner or company—with the contractor. Such a provision can be very helpful in keeping irresponsible contractors out and favouring the development of a qualified service sector.
A more specific measure in the same direction is the accreditation of contractors through government authorities or workers’ compensation administrators. In some countries contractors have to demonstrate that they are sufficiently equipped, economically independent and technically competent to carry out forestry work. Contractor associations could conceivably play a similar role, but voluntary schemes have not been very successful.
Labour inspection in forestry is a very difficult task, because of the dispersed, temporary worksites, often in faraway, inaccessible places. A strategy motivating the actors to adopt safe practices is more promising than isolated policing. In countries where large forestry companies or forest owners predominate, self-inspection of contractors by such companies, monitored by the labour inspectorate or workers’ compensation administration, is one way of increasing coverage. Direct labour inspection should be focused both in terms of issues and geography, to make optimum use of staff and transport. As labour inspectors are often non-foresters, inspection should best be based on thematic checklists (“chain-saws”, “camps” and so on), which inspectors can use after a 1- or 2-day training. A video on labour inspection in forestry is available from the ILO.
One of the biggest challenges is to integrate safety regulations into routine procedures. Where forestry-specific regulations exist as a separate body of rules, they are often perceived by supervisors and operators as an additional constraint on top of technical, logistic and other factors. As a result, safety considerations tend to be ignored. The remainder of this article describes one possibility of overcoming this obstacle.
Codes of Forest Practice
In contrast to general occupational safety and health regulations, codes of practice are sets of rules, prescriptions or recommendations that are forestry-specific and practice-oriented and ideally cover all aspects of an operation. They include safety and health considerations. Codes vary greatly in scope and coverage. Some are very concise while others are elaborate and go into considerable detail. They may cover all types of forest operations or be limited to the ones considered most critical, such as forest harvesting.
Codes of practice can be a very interesting complement to general or forestry-specific safety regulations. Over the last decade, codes have been adopted or are being developed in a growing number of countries. Examples include Australia, Fiji, New Zealand, South Africa and numerous states in the United States. At the time of writing, work was in progress or planned in various other countries, including Chile, Indonesia, Malaysia and Zimbabwe.
There are also two international codes of practice that are designed as guidelines. The FAO Model Code of Forest Harvesting Practice (1996) covers all aspects of general forest harvesting practices. The ILO Code of Practice Safety and Health in Forestry Work, first published in 1969 and to be published in a completely revised form in 1998 (available in 1997 as a working paper (ILO 1997)), deals exclusively with occupational safety and health.
The driving force behind new codes has been environmental rather than safety concerns. There is, however, a growing recognition that in forestry, operational efficiency, environmental protection and safety are inseparable. They result from the same planning, work methods and practices. Directional felling to reduce impact on the remaining stand or regeneration, and rules for extraction in steep terrain, are good examples. Some codes, like the FAO and the Fiji Codes, make this link explicit and simultaneously address productivity, environmental protection and work safety. Ideally, codes should not have separate chapters on safety, but should have occupational safety and health built into their provisions.
Codes should be based on the safest work methods and technology available, require safety to be considered in planning, establish required safety features for equipment, list required personal protective equipment and contain rules on safe work practices. Where applicable, regulations about camps, nutrition and worker transport should also be included. Safety considerations should also be reflected in rules about supervision and training.
Codes can be voluntary and be adopted as mandatory by groups of companies or the forestry sector of a country as a whole. They can also be legally binding. In all cases they may be enforceable through legal or other complaints procedures.
Many codes are drawn up by the forestry sector itself, which ensures practicability and relevance, and enhances commitment to comply. In the case of Chile, a tripartite committee has been established to develop the code. In Fiji the code was originally designed with strong industry involvement and then made binding by the Ministry of Forests.
The characteristics described above and the experience with existing codes make them a most interesting tool to promote safety in forestry, and offer the possibility of very effective cooperation between safety officers, worker’s compensation administrators, labour inspectors and forestry practitioners.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."