- You are here:
-
Home

-
Contents
-
Part X. Industries Based on Biological Resources
-
Agriculture and Natural Resources Based Industries
- Farming Systems
Molybdenum
Gunnar Nordberg
Occurrence and Uses
Molybdenum (Mo) is widely distributed throughout the earth’s crust, but it is mined in only a limited number of countries due to the rarity of bodies of sufficiently high quality molybdenite ore (MoSO2). A certain amount of molybdenum is obtained as a by-product in the processing of copper ore. Coal-electrical power plants can be significant sources of molybdenum. Molybdenum is an essential trace element.
Molybdenum forms a large variety of commercially useful compounds in which it displays the valence numbers 0, +2, +3, +4, +5 and +6. It readily changes valence states (disproportionates) with only minor changes in external conditions. It has a strong tendency to form complexes; with the exception of the sulphides and halides, very few other simple compounds of molybdenum exist. The +6 molybdenum forms isopoly- and heteropoly- acids.
Over 90% of the molybdenum produced is used as an alloying element for iron, steel and non-ferrous metals, mainly because of its heat-resisting properties; the rest is used in chemicals and lubricants. As a steel alloy, molybdenum is utilized in the electric, electronics, military and automobile industries and in aeronautical engineering. Another important use of molybdenum is in the production of inorganic molybdenum pigments, dyes and lakes. Small but increasing amounts of molybdenum are used as trace elements in fertilizers.
The most important molybdenum chemical is molybdenum trioxide (MoO3), made from roasting the sulphide ore. Pure molybdenum trioxide is used in chemical and catalyst manufacture. The technical product is added to steel as an alloying agent. Molybdenum trioxide also serves as a catalyst in the petroleum industry and as a component of ceramics, enamels and pigments. Molybdenum disulphide (MoS2) is employed as a heat-resistant lubricant or a lubricant additive. Molybdenum hexacarbonyl (Mo(CO)6) is the starting product for the manufacture of organomolybdenum dyes. It is increasingly used for molybdenum plating by thermal decomposition.
Molybdenum compounds are widely used as catalysts or catalyst activators or promoters, especially for hydrogenation-cracking, alkylation and reforming in the petroleum industry. They are employed as laboratory reagents (phosphomolybdates). In addition, molybdenum compounds are used in electroplating and in tanning.
Hazards
In the processing and industrial utilization of molybdenum and its compounds there may be exposure to dusts and fumes of molybdenum and its oxides and sulphides. This exposure may occur, especially where high-temperature treatment is being carried out as, for example, in an electric furnace. Exposure to molybdenum disulphide lubricant spray, molybdenum hexacarbonyl and its breakdown products during molybdenum plating, molybdenum hydroxide (Mo(OH)3) mist during electroplating, and molybdenum trioxide fumes which sublime above 800 °C may all prove hazardous to health.
Molybdenum compounds are highly toxic based on animal experiments. Acute poisoning causes severe gastrointestinal irritation with diarrhoea, coma and deaths from heart failure. Pneumoconiosis-like effects in the lungs have been reported in animal studies. Workers exposed to pure molybdenum or to molybdenum oxide (MoO3) (concentration of 1 to 19 mg Mo/m3) over a period of 3 to 7 years have suffered from pneumoconiosis. Inhalation of molybdenum dust from alloys or carbides can cause “hard metal lung disease”.
There is a wide degree of variation in the hazard resulting from exposure. Insoluble molybdenum compounds (e.g., molybdenum disulphide and many of the oxides and halides) are characterized by low toxicity; however, the soluble compounds (i.e., those in which molybdenum is an anion, such as sodium molybdenate—Na2MoO4·2H2O) are considerably more toxic and should be handled with care. Likewise, precautions should be taken to prevent over-exposure to freshly generated molybdenum fumes as in the thermal decomposition of molybdenum hexacarbonyl.
Exposure to molybdenum trioxide produces irritation of the eyes and the mucous membranes of the nose and throat. Anaemia is a characteristic feature of molybdenum toxicity, with low haemoglobin concentrations and reduced red-cell counts.
High dietary levels of molybdenum in cattle were found to produce deformities in the joints of the extremities. Among chemists handling molybdenum and tungsten solutions, an abnormally high frequency of cases of gout have been reported, and a correlation has been found between the content of molybdenum in food, the incidence of gout, uricaemia and xanthine oxidase activity.
Safety Measures
While working with molybdenum in industry, proper local exhaust ventilation should be employed to collect fumes at their source. Respirators may be worn when engineering and work practices have failed, when such controls are in the process of being installed, for operations requiring entry into tanks or closed vessels, or in emergencies. In the paint, printing and coatings industries, local and general exhaust ventilation as well as safety glasses, protective clothing, face shields and acceptable respirators should be used to reduce exposure for workers handling molybdenum-based dry ingredients for inorganic and organic colours.
Case Study: Legal Classification of Disabled People in France
The heterogeneity of disability is mirrored in the diversity of legal provisions and benefits that most countries have introduced and codified over the last hundred years. The example of France is chosen because it has perhaps one of the most elaborate regulatory frameworks regarding the classification of disability. While the French system may not be typical compared with those of many other countries, it has—with respect to the topic of this chapter—all the typical elements of an historically grown classification system. Therefore, this case study reveals the fundamental issues that have to be tackled in any system that grants to disabled persons rights and entitlements which are subject to legal recourse.
The twentieth anniversary of the law of 30 June 1975 regarding disabled persons has triggered a renewed interest in the lot of the disabled in France. Estimates of the number of disabled French nationals range from 1.5 to 6 million (equivalent to 10% of the population), although these estimates suffer from a lack of precision in the definition of disability. This population is all too often relegated to the margins of society, and despite progress over the last two decades, their condition remains a serious societal problem with painful human, moral and emotional ramifications that transcend collective considerations of national solidarity.
Under French law, disabled persons enjoy the same rights and freedoms as other citizens, and are guaranteed equality of opportunity and treatment. Unless specific support mechanisms are implemented, this equality is, however, purely theoretical: disabled individuals may, for example, require specialized transportation and city planning to allow them to come and go as freely as other citizens. Measures such as these, which allow disabled persons to enjoy equal treatment in fact, are designed not to confer privilege, but to remove disadvantages associated with disability. These include legislation and other state-initiated measures that guarantee equitable treatment in education, training, employment and housing. Equality of treatment and palliation of the disability constitute the prime objectives of social policy concerning disabled persons.
In most cases, however, the various measures (usually termed political discriminatory measures) prescribed by French law are not available to all persons suffering from a given disability, but rather to selected subgroups: for example, a specific allowance or programme designed to favour occupational reintegration is available only to a specific category of disabled persons. The variety of disabilities and the multiple contexts in which disability may occur have necessitated the development of classification systems that take into account an individual’s official status as well as his or her level of disability.
Variety of Disabilities and Determination of Official Status
In France, the context in which disabilities arise constitutes the fundamental basis for classification. Classifications based on the nature (physical, mental or sensory) and degree of disability are also relevant to the treatment of disabled persons, of course, and are taken into account. These other classification systems are particularly important in determining whether health care or occupational therapy is the best approach, and whether guardianship is appropriate (persons suffering from mental disabilities may become wards of the state). Nevertheless, classification on the basis of the nature of the disability is the primary determinant of a disabled person’s official status, rights and eligibility for benefits.
A review of the body of French law applicable to disabled persons reveals the multiplicity and complexity of support systems. This organizational redundancy has historical origins, but persists to this day and remains problematic.
Development of “official status”
Until the end of the nineteenth century, care of the disabled was essentially a form of “good works” and usually took place in hospices. It was not until the beginning of the twentieth century that the ideas of rehabilitation and income replacement developed against the backdrop of a new cultural and social view of disability. In this view, the disabled were seen as damaged persons who needed to be rehabilitated—if not to the status quo ante, at least to an equivalent situation. This change in mentality was an outgrowth of the development of mechanization and its corollary, occupational accidents, and of the impressive number of First World War veterans suffering permanent disability.
The law of 8 April 1898 improved the occupational-accident compensation system by no longer requiring proof of employer liability and establishing a flat-fee compensation payment system. In 1946, management of the risk associated with occupational accidents and diseases was transferred to the social security system.
Several laws were passed in an attempt to correct prejudices suffered by injured or disabled First World War veterans. These include:
- a 1915 law establishing an occupational retraining system
- a 1916 law (complemented by a 1923 law) giving war invalids first call on public-sector jobs
- the law of 31 March 1918 instituting the right to a fixed pension based on the degree of disability
- the law of 26 April 1924 requiring private-sector companies to employ a specific percentage of war invalids
The interwar period saw the development of the first large-scale associations of civilian disabled persons. The most noteworthy of these are: the Fédération des mutilés du travail (1921), the Ligue pour l’adaptation des diminués physiques au travail (LADAPT) (1929) and the Association des Paralysés de France (APF) (1933). Under pressure from these associations and from unions, victims of work accidents, and eventually all the civilian disabled, progressively benefited from support systems based on those established for war invalids.
A disability insurance system was established for workers in 1930 and reinforced by the 1945 Decree creating the social security system. Under this system, workers receive a pension if their ability to work or earn a livelihood is significantly reduced by disease or accident. The right of victims of occupational accidents to retraining was recognized by a 1930 law. A training and retraining system for the blind was established in 1945 and extended to all seriously disabled persons in 1949. In 1955, the obligation to hire a minimum percentage of war invalids was extended to other disabled persons.
The development of the concept of occupational integration led to the promulgation of three laws which improved and reinforced existing support systems: the law of 27 November 1957 concerning occupational reclassification of disabled workers, the law of 30 June 1975 concerning disabled persons (the first to adopt a global approach to the problems faced by disabled persons, especially that of social reintegration), and the law of 10July 1987 favouring the employment of disabled workers. However, these laws in no way eliminated the specific dispositions of the systems responsible for war invalids and the victims of occupational accidents.
Multiplicity and diversity of regimes supporting disabled persons
Today, there are three quite distinct regimes providing support to disabled persons: one for war invalids, one for victims of occupational accidents, and the common-law system, which deals with all other disabled persons.
A priori, the coexistence of multiple regimes that select their clientele on the basis of the origin of disability does not appear to be a satisfactory arrangement, especially since each regime provides the same type of support, namely integration-support programmes, particularly those aimed at occupational reintegration, and one or more allowances. Accordingly, there has been a concerted effort to harmonize employment-support systems. For example, the vocational training and medical rehabilitation programmes of all the systems aim as much at distributing costs through society as at providing financial compensation for disability; the specialized training and medical rehabilitation centres, including the centres operated by the Office des anciens combattants (ONAC), are open to all disabled persons, and the reservation of positions in the public sector for war invalids was extended to disabled civilians by the Decree of 16 December 1965.
Finally, the law of 10 July 1987 united the private- and public-sector minimum-employment programmes. Not only were the conditions of these programmes extremely complex to apply, but they also differed depending on whether the individual was a disabled civilian (in which case the common law system applied) or a war invalid. With the coming into force of this law, however, the following groups are entitled to consideration for minimum-employment programmes: disabled workers recognized by the Commission technique d’orientation et de réinsertion professionnelle (COTOREP), victims of occupational accidents and diseases receiving a pension and suffering from a permanent disability of at least 10%, recipients of civilian disability allowances, former members of the armed forces and other recipients of military disability allowances. COTOREP is responsible, under the common law system, for the recognition of disabled status.
On the other hand, the actual allowances provided by the three regimes differ widely. Disabled persons benefiting from the common-law system receive what is essentially a disability pension from the social security system and a complementary allowance to bring their total benefit up to the adult disabled pension level (as of 1July 1995) of FF 3,322 per month. The amount of the state pension received by war invalids depends on the degree of disability. Finally, the monthly amount (or a lump-sum payment if the permanent disability is below 10%) received by victims of occupational accidents and diseases from the social security system depends on the recipient’s degree of disability and previous salary.
The eligibility criteria and amounts of these allowances are entirely different in each system. This leads to significant differences in the way individuals with disabilities of different organs are treated, and to anxiety that may interfere with rehabilitation and social integration (Bing and Levy 1978).
Following numerous calls for the harmonization, if not unification, of the various disability allowances (Bing and Levy 1978), the Government established a task force in 1985 to study solutions to this problem. To date, however, no solution has been forthcoming, in part because the different goals of the allowances constitute a serious obstacle to their unification. Common-law allowances are subsistence allowances—they are intended to allow recipients to maintain a decent standard of living. In contrast, the war disability pensions are intended to compensate for disabilities acquired while in national service, and allowances paid to victims of occupational accidents and diseases are intended to compensate for disabilities acquired while earning a living. These last two allowances are therefore generally significantly higher, for a given level of disability, than those received by individuals with disabilities that are either congenital or resulting from non-military, non-occupational accidents or illnesses.
Effect of Official Status on Assessments of the Degree of Disability
Different disability-compensation regimes have evolved over time. This diversity is reflected not only in the different allowances each pays to disabled persons but also in each system’s eligibility criteria and system for evaluating the degree of disability.
In all cases, eligibility for compensation and evaluation of the extent of disability is established by an ad hoc committee. Recognition of disability requires more than a simple declaration by the applicant—applicants are required to testify before the commission if they desire to be granted official status as a disabled person and receive eligible benefits. Some people may find this procedure dehumanizing and counter to the goal of integration, since individuals who do not wish to have their differences “officialized” and refuse, for example, to appear before the COTOREP, will not be granted official disabled-person status and will thus be ineligible for occupational reintegration programmes.
Disability eligibility criteria
Each of the three regimes relies on a different set of criteria to determine whether an individual is entitled to receive disability benefits.
Common-law regime
The common-law regime pays disabled persons subsistence allowances (including the adult disability allowance, a compensatory allowance, and the educational allowance for disabled children), to allow them to remain independent. Applicants must suffer from a serious permanent disability—an 80% disability is required in the majority of cases—to receive these allowances, although a lower level of disability (of the order of 50 to 80%) is required in the case of a child attending a specialized institute or receiving special education or home care. In all cases, the degree of disability is evaluated by reference to an official disability scale contained in Appendix 4 of the Decree of 4 November 1993 concerning the payment of various allowances to disabled persons.
Different eligibility criteria apply to applicants for disability insurance, which, like the common-law allowances, includes a subsistence component. To qualify for this pension, applicants must be receiving social security and must suffer from a disability that reduces their earning capacity by at least two thirds, that is, that prevents them from earning, in any occupation, a salary greater than one third of their pre-disability salary. The pre-disability salary is calculated on the basis of the salary of comparable workers in the same region.
There are no official criteria for the determination of eligibility, which instead is based on the individual’s overall situation. “The degree of disability is evaluated on the basis of residual fitness for work, overall condition, age, physical and mental faculties, aptitudes, and occupational training”, according to the social security law.
As this definition makes clear, disability is considered to include the inability to earn a living in general, rather than being limited to physical disability or the inability to exercise a given occupation, and is evaluated on the basis of factors likely to affect the occupational reclassification of the individual. These factors include:
- the nature and severity of the disability, and the applicant’s age, physical and mental faculties, aptitudes, occupational training and previous occupation
- the applicant’s residual fitness for work relative to the workforce in his or her region of residence.
To be eligible for specific occupational reintegration programmes, disabled adults must satisfy the following legal criterion: “a disabled worker is any person whose ability to obtain or maintain a job is reduced in fact as a result of inadequate or reduced physical or mental capacities”.
This definition was greatly influenced by the Vocational Rehabilitation of the Disabled Recommendation, 1955 (No. 99) (ILO 1955), which defines a disabled person as “an individual whose prospects of securing and retaining suitable employment are substantially reduced as a result of physical or mental impairment”.
This pragmatic approach nevertheless leaves room for interpretation: what does “in fact” mean? What is the standard to be used in determining whether fitness for work is “inadequate” or “reduced”? The absence of clear guidelines in these matters has resulted in widely divergent evaluations of occupational disability by different commissions.
Specific regimes
To accomplish their primary goal of reparation and compensation, these regimes pay the following allowances and pensions:
- War disability pensions are based on the degree of purely physical disability, as evaluated by experts. Permanent disabilities of at least 10 and 30% are generally required for injuries and diseases, respectively. The degree of disability is evaluated using the official disability scale (Decree of 29 May 1919).
- In the occupational accident system, victims of occupational accidents and diseases suffering from a permanent disability receive either a lump-sum payment or an allowance.
The degree of permanent disability is established using an official disability scale that takes into account the nature of the disability, and the applicant’s general condition, physical and mental faculties, aptitudes and occupational qualifications.
Disability evaluation scales
While eligibility for each regime’s benefits depends on administrative decisions, the medical evaluation of disability, established through examination or consultation, remains critically important.
There are two approaches to the medical evaluation of the degree of disability, one involving the calculation of compensation on the basis of the degree of permanent partial disability, the other based on the reduction in fitness for work.
The first system is used by the war disability system, while the occupational accident and common-law systems require the examination of the applicant by the COTOREP.
The degree of permanent partial disability in war invalids is established using standards contained in the official disability scale applicable to cases covered by the Code des pensions militaires d’invalidité et victimes de guerre (updated 1 August 1977 and including the scales of 1915 and 1919). For the victims of occupational accidents, a scale of occupational accidents and diseases established in 1939 and revised in 1995 is used.
The classification systems used in these two regimes are organ- and function-specific (such as blindness, renal failure, cardiac failure) and establish a level of permanent partial disability for each type of disability. Several possible classification systems for mental disability are suggested, but all of them are imprecise for these purposes. It should be noted that these systems, apart from their other weaknesses, may assess different levels of permanent partial disability for a given disability. Thus, a 30% reduction of bilateral visual acuity is equivalent to a permanent partial disability rating of 3% in the occupational-accident system and 19.5% in the war- disability system, while a 50% loss is equivalent to permanent partial disabilities of 10 and 32.5%, respectively.
Until recently, the COTOREP used the disability scale established in the Code des pensions militaires d’invalidité et victimes de guerre to determine compensation and benefits such as disability cards, adult disability allowances, and third-party compensatory allowances. This scale, developed to ensure fair compensation for war injuries, is not well suited to other uses, especially to birth rate. The absence of a common reference has meant that different sittings of the COTOREP have arrived at significantly different conclusions concerning the degree of disability, which has created serious inequities in the treatment of disabled persons.
To remedy this situation, a new scale of deficiencies and disabilities, which reflects a new approach to disability, came into force on 1 December 1993 (Appendix to Decree No.93-1216 of 4 November 1993, Journal Officiel of 6 November 1993). The methodological guide is based on concepts proposed by the WHO, namely impairment, disability and handicap, and is used primarily to measure disability in family, school and occupational life, regardless of the specific medical diagnosis. While the medical diagnosis is a critical predictor of the condition’s evolution and the most effective case management strategy, it nevertheless is of limited usefulness for the purposes of establishing the degree of disability.
With one exception, these scales are meant to be only indicative: their use is mandatory for the evaluation of permanent partial disability in recipients of military pensions who have suffered amputation or organ resection. Several other factors affect the evaluation of the degree of disability. In occupational accident victims; for example, the establishment of the degree of permanent partial disability must also take into account medical factors (general condition, nature of the disability, age, mental and physical faculties) and social factors (aptitudes and occupational qualifications). The inclusion of other factors allows physicians to fine-tune their evaluation of the degree of permanent partial disability to take into account therapeutic advances and the potential for rehabilitation, and to counteract the rigidity of the scales, which are rarely updated or revised.
The second system, based on the loss of working capacity, raises other questions. The reduction in working capacity may need to be evaluated for different purposes: evaluation of the reduction in working capacity for the purposes of disability insurance, recognition of the loss of working capacity by COTOREP, evaluation of an occupational deficit for the purposes of recognizing a worker as disabled or placing such a worker in a special workshop.
No standards can exist for the evaluation of the loss of working capacity, since the “average worker” is a theoretical construct. In fact, the whole field of working capacity is poorly defined, as it relies not only on an individual’s inherent aptitudes but also on the needs and adequacy of the occupational environment. This dichotomy illustrates the distinction between the capacity at work and the capacity for work. Schematically, two situations are possible.
In the first case, the degree of the loss of working capacity relative to the applicant’s recent and specific occupational situation must be objectively established.
In the second case, the loss of working capacity must be evaluated in disabled persons who are either not currently in the workforce (e.g., individuals with chronic illnesses who have not worked for a long time) or who have never been in the workforce. This last case is frequently encountered when establishing adult disability pensions, and eloquently illustrates the difficulties that physicians responsible for quantifying the loss of working capacity are faced with. Under these circumstances, physicians often refer, either consciously or unconsciously, to degrees of permanent partial disability for establishing working capacity.
Despite the obvious imperfections of this disability-evaluation system and the occasional medico-administrative contortions it imposes, it nevertheless allows the level of disability compensation to be established in most cases.
It is clear that the French system, involving official classification of disabled persons on the basis of the origin of their disability, is problematic on several levels under the best of circumstances. The case of individuals suffering from disabilities of different origins and who are therefore ascribed multiple official statuses is even more complex. Consider for example the case of a person suffering from a congenital motor disability who suffers an occupational accident: the problems associated with the resolution of this situation can easily be imagined.
Because of the historical origins of the various official statuses, it is unlikely that the regimes can ever be made completely uniform. On the other hand, continued harmonization of the regimes, especially their systems for the evaluation of disability for the purpose of the awarding of financial compensation, is highly desirable.
Disability: Concepts and Definitions
Preliminary Considerations
Most people seem to know what a disabled person is and are certain that they would be able to identify an individual as disabled, either because the disability is visible or because they are aware of a specific medical condition that lends itself to be called disability. However, what precisely the term disability means is less easy to determine. A common view is that having a disability makes an individual less capable of performing a variety of activities. In fact, the term disability is as a rule used to indicate a reduction or deviation from the norm, a shortcoming of an individual that society has to reckon with. In most languages, terms equivalent to that of disability contain the notions of less value, less ability, a state of being restricted, deprived, deviant. It is in line with such concepts that disability is exclusively viewed as a problem of the affected individual and that the problems indicated by the presence of a disability are considered to be more or less common to all situations.
It is true that a disabling condition may affect to varying degrees the personal life of an individual and his or her relations with family and community. The individual who has a disability may, in fact, experience the disability as something that sets him or her apart from others and that has a negative impact on the way life is organized.
However, meaning and impact of disability change substantially depending on whether the environment and the attitudes of the public accommodate a disability or whether they do not. For example, in one context, the person who uses a wheelchair is in a state of complete dependency, in another he or she is as independent and working as any other person.
Consequently, the impact of an alleged dysfunction is relative to the environment, and disability is thus a social concept and not solely the attribute of an individual. It is also a highly heterogeneous concept, making the search for a homogeneous definition a virtually impossible task.
Despite many attempts to define disability in general terms, the problem remains concerning what renders an individual disabled and who should belong to this group. For example, if disability is defined as dysfunction of an individual, how to classify a person who despite a serious impairment is fully functional? Is the blind computer specialist who is gainfully employed and has managed to solve his or her transport problems, secure adequate housing and have a family still a disabled person? Is the baker who can no longer exercise his profession because of a flour allergy to be counted among disabled job-seekers? If so, what is the real meaning of disability?
To understand this term better, one has first to distinguish it from other related concepts that are often confused with disability. The most common misunderstanding is to equate disability with disease. Disabled people are often described as the opposite of healthy people and, consequently, as needing the help of the health profession. However, disabled people, as anyone else, need medical help only in situations of acute sickness or illness. Even in cases where the disability results from a protracted or chronic illness, such as diabetes or a cardiac disease, it is not the sickness as such, but its social consequences that are involved here.
The other most common confusion is to equate disability with the medical condition that is one of its causes. For example, lists have been drawn up that classify disabled people by types of “disability”, such as blindness, physical malformations, deafness, paraplegia. Such lists are important for determining who should be counted as a disabled person, except that the use of the term disability is inaccurate, because it is confounded with impairment.
More recently, efforts have been made to describe disability as difficulty in performing certain types of function. Accordingly, a disabled person would be someone whose ability to perform in one or several key areas—such as communication, mobility, dexterity and speed—is affected. Again, the problem is that a direct link is made between the impairment and the resulting loss of function without taking into account the environment, including the availability of technology that could compensate for the loss of function and thus render it insignificant. To look at disability as the functional impact of impairment without acknowledging the environmental dimension means to put the blame for the problem entirely on the disabled individual. This definition of disability still stays within the tradition of regarding disability as a deviation from the norm and ignores all other individual and societal factors that together constitute the phenomenon of disability.
Can disabled people be counted? This may be possible within a system that applies precise criteria as to who is sufficiently impaired to be counted as disabled. The difficulty is to make comparisons between systems or countries that apply different criteria. However, who will be counted? Strictly speaking, censuses and surveys that undertake to produce disability data can count only people who themselves indicate that they have an impairment or a functional restriction on account of an impairment, or who believe that they are in a situation of disadvantage because of an impairment. Unlike gender and age, disability is not a clearly definable statistical variable, but a contextual term that is open to interpretation. Therefore, disability data can offer only approximations and should be treated with utmost care.
For the reasons outlined above, this article does not constitute yet another attempt to present a universal definition of disability, or to treat disability as an attribute of an individual or a group. Its intention is to create an awareness about the relativity and heterogeneity of the term and an understanding about the historical and cultural forces that have shaped legislation as well as positive action in favour of people identified as disabled. Such an awareness is the prerequisite for the successful integration of disabled people in the workplace. It will permit a better understanding of the circumstances that need to be in place to make the disabled worker a valuable member of the workforce instead of being barred employment or pensioned off. Disability is presented here as being manageable. This requires that individual needs such as skill upgrading or the provision with technical aids, be addressed, and accommodated by adjusting the workplace.
There is currently a vivid international debate, spearheaded by disability organizations, regarding a non-discriminatory definition of disability. Here, the view is gaining ground that disability should be identified where a particular social or functional disadvantage occurs or is anticipated, linked to an impairment. The issue is how to prove that the disadvantage is not the natural, but rather the preventable result of the impairment, caused by a failure of society to make adequate provision for the removal of physical barriers. Leaving aside that this debate reflects primarily the view of disabled people with a mobility impairment, the possible unwelcome consequence of this position is that the state may shift expenditures, such as for disability benefits or special measures, based on disability, to those that improve the environment.
Nevertheless, this debate, which is continuing, has highlighted the need to find a definition of disability that reflects the social dimension without sacrificing the specificity of the disadvantage based on an impairment, and without losing its quality as an operational definition. The following definition tries to reflect this need. Accordingly, disability can be described as the environmentally determined effect of an impairment that, in interaction with other factors and within a specific social context, is likely to cause an individual to experience an undue disadvantage in his or her personal, social or professional life. Environmentally determined means that the impact of the impairment is influenced by a variety of factors, including preventive, corrective and compensatory measures as well as technological and accommodative solutions.
This definition recognizes that in a different environment that erects fewer barriers, the same impairment could be without any significant consequences, hence without leading to a disability. It stresses the corrective dimension over a concept that takes disability as an unavoidable fact and that simply seeks to ameliorate the living conditions of the afflicted persons. At the same time, it maintains the grounds for compensatory measures, such as cash benefits, because the disadvantage is, despite the recognition of other factors, still specifically linked to the impairment, irrespective of whether this is the result of a dysfunction of the individual or of negative attitudes of the community.
However, many disabled people would experience substantial limitations even in an ideal and understanding environment. In such cases the disability is primarily based in the impairment and not in the environment. Improvements in environmental conditions can substantially reduce dependency and restrictions, but they will not alter the fundamental truth that for many of these severely disabled people (which is different from severely impaired) participation in social and professional life will continue to be restricted. It is for these groups, in particular, that social protection and ameliorative provisions will continue to play a more significant role than the aim of full integration into the workplace which, if it takes place, is often done for social rather than for economic reasons.
But this is not to suggest that persons thus defined as severely disabled should live a life apart and that their limitations should be grounds for segregation and exclusion from the life of the community. One of the major reasons for exercising utmost caution as regards the use of disability definitions is the widespread practice of making a person thus identified and labelled the object of discriminatory administrative measures.
Nevertheless, this points to an ambiguity in the concept of disability that gives rise to so much confusion and that could be a main reason for the social exclusion of disabled people. For, on the one hand, many campaign with the slogan that disability does not mean inability; on the other, all existing protective systems are based on the grounds that disability means inability to make a living on one’s own. The reluctance of many employers to hire disabled people may be founded in this basic contradiction. The answer to this is a reminder that disabled people are not a homogeneous group, and that each case should be judged individually and without bias. But it is true that disability may mean both: an inability to perform according to the norm or an ability to perform as well as or even better than others, if given the opportunity and the right kind of support.
It is obvious that a concept of disability as outlined above calls for a new foundation for disability policies: sources of inspiration for how to modernize policies and programmes in favour of disabled persons can be found among others in the Vocational Rehabilitation and Employment (Disabled Persons) Convention, 1983 (No. 159) (ILO 1983) and the United Nations Standard Rules on the Equalization of Opportunities for Persons with Disabilities (United Nations 1993).
In the following paragraphs, the various dimensions of the disability concept as it affects present law and practice will be explored and described in an empirical manner. Evidence will be provided that various disability definitions are in use, mirroring the world’s different cultural and political legacies rather than giving cause for the hope that a single universal definition can be found which is understood by everyone in the same manner.
Disability and normality
As mentioned above, most past regulatory attempts at defining disability have fallen prey, in one form or another, to the temptation of describing disability as primarily negative or deviatory. The human being afflicted with disability is seen as a problem and becomes a “social case”. A disabled person is assumed to be unable to pursue normal activities. He or she is a person with whom all is not quite in order. There is an abundance of scientific literature that depicts disabled people as having a behavioural problem, and in many countries “defectology” was and still is a recognized science that sets out to measure the degree of deviation.
Individuals who have a disability generally defend themselves against such a characterization. Others resign themselves to the role of a disabled person. Classifying persons as disabled disregards the fact that what disabled individuals have in common with the non-disabled usually far outweighs that which makes them different. Further, the underlying concept that disability is a deviation from the norm is a questionable value statement. These considerations have incited many people to prefer the term persons with disabilities to that of disabled persons, as the latter term could be understood as making disability the primary characteristic of an individual.
It is thoroughly conceivable that human and social reality be defined in such a way that disability be regarded as consistent with normalcy and not as a deviation from it. In fact, the Declaration that was adopted in 1995 by the heads of state and government at the UN World Summit for Social Development in Copenhagen describes disability as a form of social diversity. This definition demands a conception of society which is a society “for all”. Thereby previous attempts at defining disability negatively, as deviation from the norm or as deficiency, are no longer valid. A society which adapts itself to disability in an inclusive manner could substantially overcome those effects of disability which were previously experienced as overly restrictive.
Disability as identity
Despite the danger that the label will invite segregation and discrimination, there are valid reasons to adhere to the usage of the term disability and to group individuals in this category. It cannot be denied, from an empirical standpoint, that many individuals with disability share similar, mostly negative, experiences of discrimination, exclusion and economic or social dependency. There exists a factual categorization of human beings as disabled, because specific negative or censorious social behaviour patterns appear to be based upon disability. Conversely, where there are efforts made to fight discrimination on the basis of disability, it also becomes necessary to stipulate who should have the right to enjoy protection under such measures.
It is in reaction to the way society treats people with disabilities that many individuals who have experienced discrimination in one form or another because of their disability join together in groups. They do so partly because they feel more at ease among individuals who share their experience, partly because they wish to advocate common interests. They accordingly accept the disabled role, if indeed for very different motives: some, because they want to induce society to view disability, not as an attribute of isolated individuals, but rather as the result of action and neglect on the part of the community which unduly curtails their rights and opportunities; the others, because they acknowledge their disability and demand their right to be accepted and respected in their difference, which includes their right to struggle for equality of treatment.
However, most individuals who, on account of an impairment, have a functional limitation of one form or another appear not to see themselves as disabled. This creates a problem not to be underestimated for those engaged with the politics of disability. For example, should those who do not self-identify as disabled be counted among the numbers of disabled persons, or only those who register as disabled?
Legal recognition as disabled
In many constituencies definitions of disability are identical with an administrative act of recognizing a disability. This recognition as disabled becomes a prerequisite for the claiming of support on the basis of a physical or mental limitation or for litigation under an anti-discrimination law. Such support can comprise provisions for rehabilitation, special education, retraining, privileges in the securing and preserving of a place of employment, guarantee of subsistence through income, compensation payments and assistance with mobility, etc.
In all cases in which legal regulations are in force in order to compensate for or to prevent disadvantages, there arises the need to clarify who has a claim on such legal provisions, be these benefits, services or protective measures. It follows thereupon, that the definition of disability is conditioned by the type of service or regulation which is offered. Virtually every existing definition of disability thus mirrors a legal system and draws its meaning from this system. Being recognized as disabled means to fulfil the conditions for benefiting from the possibilities presented by this system. These conditions, however, may vary among constituencies and programmes and, consequently, many different definitions may coexist side by side within a country.
Further evidence that the legal realities of the respective nations determine the definition of disability is offered by those countries, such as Germany and France, which have introduced a regulation including quotas or the levying of fines in order to assure disabled people access to employment opportunities. It can be demonstrated that with the introduction of such legislation, the number of “disabled” workers has risen drastically. This rise is to be explained only by the fact that employees—often on the recommendation of employers—who in the absence of such a law would never have designated themselves as disabled, register themselves as such. These same individuals were also never previously registered statistically as disabled.
Another legal difference among countries is the treatment of a disability as a temporary or permanent condition. In some countries, which offer disabled persons specific advantages or privileges, these privileges are limited to the duration of a recognized disadvantage. If this state of disadvantage is overcome through corrective actions, the disabled person loses his or her privileges—independently of whether medical facts (e.g., the loss of an eye or a limb) remain. For example, an individual who has successfully completed rehabilitation that has re-established lost functional abilities may lose entitlements to disability benefits or may not even enter a benefit scheme.
In other countries, lasting privileges are offered to offset real or hypothetical handicaps. This practice has resulted in the development of a legally recognized disability status bearing elements of “positive discrimination”. These privileges often apply even to those who are no longer actually in need of them because they are socially and economically well integrated.
The problem with statistical registration
A definition of disability that can be applied universally is impossible, since every country, and practically every administrative body, works with different concepts of disability. Every attempt to measure disability statistically must take into account the fact that disability is a system-dependent, and therefore a relative, concept.
Consequently, most regular statistics contain information only about the beneficiaries of specific state or public provisions who have accepted disability status in accordance with the operative definitions of the law. People who do not view themselves as disabled and manage alone with a disability usually do not come within the purview of official statistics. In fact, in many countries, such as the United Kingdom, many disabled people avoid statistical registration. The right not to be registered as disabled is in keeping with the principles of human dignity.
Therefore, occasionally, efforts are made to determine the total number of disabled persons through surveys and censuses. As already argued above, these come up against objective conceptual limits which render the comparability of such data between countries practically impossible. Above all, it is controversial what precisely such surveys are meant to prove, in particular as the notion of disability, as an objective set of findings that is equally applied and understood in all countries, cannot be sustained. Thus, a low number of statistically registered persons with disability in some countries does not necessarily reflect an objective reality, but most likely the fact that the countries in question offer fewer services and legal regulations in favour of disabled persons. Conversely, those countries which have an extensive social protection and rehabilitation system are likely to show a high percentage of disabled individuals.
Contradictions in the use of the concept of disabled persons
Objective results are, therefore, not to be expected on the level of quantitative comparison. But there is also no uniformity of interpretation from a qualitative point of view. Here again, the respective context and the intention of lawmakers determine the definition of disability. For example, the effort to guarantee disabled persons social protection requires disability to be defined as the inability to earn one’s own living. In contrast, a social policy whose goal is vocational integration endeavours to describe disability as a condition that, with the help of appropriate measures, need not have any detrimental effects on the level of performance.
International Definitions of Disability
The concept of disability in Convention No. 159 of the International Labour Organization
The above considerations also underlie the framework definition used in the Vocational Rehabilitation and Employment (Disabled Persons) Convention, 1983 (No. 159) (ILO 1983). Article 1.1 contains the following formulation: “For the purposes of this Convention, the term ‘disabled person’ means an individual whose prospects of securing, retaining and advancing in suitable employment are substantially reduced as a result of a duly recognized physical or mental impairment”.
This definition contains the following constituent elements: the reference to mental or physical impairment as the original cause of the disability; the necessity of a state recognition procedure that—in accordance with the respective national realities—determines who should be considered disabled; the determination that disability is not constituted by the impairment itself but by the possible and real social consequences of an impairment (in this case a more difficult situation on the labour market); and the established entitlement to measures which help to secure equality of treatment on the labour market (see Article 1.2). This definition consciously avoids an association with concepts such as inability and leaves room for an interpretation which holds that disability can also be conditioned by misconceived opinions held by an employer which may result in conscious or unconscious discrimination. On the other hand, this definition does not rule out the possibility that, in the case of a disability, objective limitations with respect to performance can occur, and leaves open whether or not the equal treatment principle of the Convention would apply in this case.
The definition in the ILO Convention does not make a claim to be a comprehensive, universally applicable definition of disability. Its sole intention is to provide for a clarification of what disability could mean in the context of employment and labour measures.
The concept of disability in light of the definition of the World Health Organization
The International Classification of Impairments, Disabilities and Handicaps (ICIDH) of the World Health Organization (WHO 1980) offers a definition of disability, in the area of health policy, which differentiates between impairment, disability and handicaps:
- “In the context of health experience, an impairment is any loss or abnormality of psychological, physiological, or anatomical structure or function.”
- “In the context of health experience, a disability is any restriction or lack (resulting from an impairment) of ability to perform an activity in the manner or within the range considered normal for a human being.”
- “In the context of health experience, a handicap is a disadvantage for a given individual, resulting from an impairment or a disability, that limits or prevents the fulfilment of a role that is normal (depending on age, sex, and social and cultural factors) for that individual.”
The new and distinctive aspects of this conceptual differentiation do not lie in its traditional epidemiological approach and its classificatory apparatus, but rather in its introduction of the concept of handicap, which calls on those concerned with public health policy to reflect on the social consequences of specific impairments on a person affected and to regard the treatment process as part of a holistic concept of life.
The WHO clarification was especially necessary because the words impairment and disability were previously often equated with concepts such as crippled, mentally retarded and the like, which convey an exclusively negative image of disability to the public. A categorization of this kind is, in fact, not suited to a precise definition of the concrete situation of a disabled individual within society. The WHO terminology has since become a reference for the discussion on the concept of disability at the national and international levels. It will, therefore, be necessary to dwell on these concepts a little more.
Impairment. With this concept, health professionals customarily designate an existing or developing injury to bodily functions or to vital life processes in a particular person that affects one or more parts of the organism or that indicates a defect in the psychic, mental or emotional functioning as the result of an illness, accident or congenital or hereditary condition. An impairment can be temporary or permanent. The influences of professional or social contexts or of the environment as a whole are not taken into consideration in this category. Here, the physician’s assessment of a person’s medical condition or an impairment is exclusively at issue, without consideration of the consequences that this impairment may have upon that person.
Disability. Such impairment or loss can result in substantial limitation to the active lives of persons afflicted. This consequence of impairment is termed disability. Functional disorders of the organism, such as, for example, psychic disorders and mental breakdowns, can lead to more or less severe disabilities and/or negative effects in the execution of specific activities and duties of daily living. These effects can be temporary or permanent, reversible or irreversible, constant, progressive or subject to successful treatment. The medical concept of disability designates, therefore, functional limitations which arise in the lives of specific individuals as the direct or indirect result of a physical, psychosocial or mental impairment. Above all, disability reflects the personal situation of the individual who has an impairment. However, as the personal consequences of a disability depend upon age, sex, social position and profession, and so on, the same or similar functional disorders can have thoroughly different personal consequences for different individuals.
Handicap. As soon as persons with physical or mental impairments enter their social, professional or private context, difficulties may arise which bring them into a situation of disadvantage, or handicap, in relation to others.
In the original version of the ICIDH, the definition of handicap signifies a disadvantage which emerges as the result of an impairment or a disability, and which limits an individual in the performance of what is regarded as a “normal” role. This definition of handicap, which bases the problem exclusively upon the personal situation of the person afflicted, has since come under criticism, for the reason that it does not sufficiently take into account the role of the environment and the attitude of society in bringing about the situation of disadvantage. A definition which takes these objections into account should reflect upon the relationship between the disabled individual and the manifold environmental, cultural, physical or social barriers that a society reflecting the attitudes of non-disabled members tends to erect. In light of this, every disadvantage in the life of a specific person that is not so much the result of an impairment or a disability, but of negative or unaccommodating attitudes in the largest sense, should be termed “handicap”. Further, any measures taken towards the improvement of the situation of disabled individuals, including those that help them to fully participate in life and in society, would contribute to preventing the “handicap”. A handicap thus is not the direct result of an existing impairment or disability, but the result of the interaction between an individual with a disability, the social context and the immediate surroundings.
It may not be assumed at the outset, therefore, that a person with an impairment or disability must automatically also have a handicap. Many disabled individuals succeed, despite the limitations caused by their disability, in the full pursuit of a profession. On the other hand, not every handicap can be attributed to a disability. It can also be caused by a lack of education that may or may not be linked with disability.
This hierarchical system of classification—impairment, disability, handicap—can be compared with the various phases of rehabilitation; for example, when the purely curative treatment is followed by rehabilitation of functional and psycho-social limitations and is completed with vocational rehabilitation or training for an independent pursuit of life.
The objective assessment of the degree of a disability in the sense of its social consequences (handicap) cannot, for this reason, rely solely upon medical criteria, but must take into account the vocational, social and personal contexts—especially the attitude of the non-disabled population. This state of affairs makes it quite difficult to measure and unequivocally establish a “state of disability”.
Definitions in Use in Various Countries
Disability as a legal category for the establishment of claims
Disability status is determined, as a rule, by a competent national authority on the basis of findings after an examination of individual cases. Therefore, the purpose for which disability status should be recognized plays an essential role—for example, where the determination of the presence of a disability serves the purpose of laying claim to specific personal rights and legal benefits. The primary interest in having a legally sound definition of disability is thus motivated not by medical, rehabilitative or statistical reasons, but rather by juridical reasons.
In many countries, persons whose disability is recognized can lay claim to the right to various services and regulatory measures in specific areas of health and social policies. As a rule, such regulations or benefits are designed to improve their personal situation and to support them in overcoming difficulties. The basis for the guarantee of such benefits thus is an act of official recognition of an individual’s disability on the strength of the respective statutory provisions.
Examples of definition from legislative practice
These definitions vary widely between different states. Only a few examples that are currently in use can be cited here. They serve to illustrate the variety as well as the questionable character of many definitions. As it cannot be the purpose here to discuss specific legal models, the sources of the quotations are not given, nor is an evaluation of which definitions appear more adequate than others. Examples of national definitions of disabled persons:
- Those who are afflicted with a not only temporary functional impairment which is due to an irregular physical, mental or psychological condition or any who are threatened with such a disability. If the degree of disability amounts to at least 50%, it is considered a severe disability.
- All those whose working capacity is diminished by at least 30% (for physical disability) or at least 20% (for mental disability).
- All those whose opportunities to obtain and hold (secure and retain) employment are restricted by either a lack or limitation in their physical or mental capabilities.
- All those who because of an impairment or invalidity are hindered or prevented from the accomplishment of normal activities. The impairment may concern both mental and bodily functions.
- All those whose ability to work is permanently restricted because of a physical, psychical or sensory defect.
- All those who need care or special treatment to assure the support, development and restoration of their vocational capabilities. This includes physical, mental, psychical and social disabilities.
- All those who because of a permanent limitation to their physical, mental or sensory capabilities—independent of whether hereditary or acquired—enjoy only restricted opportunities to pursue an education and participate in vocational and social life.
- Victims of industrial accidents, war disabled and individuals who suffer from a physical, mental or psychical impairment. The reduction of working capacity must amount to at least 30%.
- All those who because of an impairment, illness or hereditary disease experience substantially reduced opportunities in securing and retaining employment appropriate to their age, experience and qualifications.
- Persons with a physical or mental impairment which, to a significant extent, restricts an important part of their life activity or those who are assumed to suffer from such an impairment or for whom earlier records about such impairments exist.
- Persons who are afflicted with a functional disorder or disease that leads to: (a) a total or partial loss of physical or mental functions; (b) illnesses caused or which will forseeably be caused by the presence of organisms in the body; (c) a loss of normal function due to deformation of body parts; (d) the appearance of learning difficulties not present in individuals without functional disorders or restrictions; (e) an impairment to behaviour, thought process, judgement and emotional life.
- Persons who, due to physical or mental impairment as a result of a birth defect, illness or accident, are presumed incapable of earning their living, either permanently or for an extended period of time.
- Persons who, as a result of an illness, injury, a mental or physical weakness, are not in the position for a period of at least six months to earn, from work that corresponds to their potential abilities and cultural level, a specific fraction (1/3, 1/2, 2/3) of that income, which an individual in good condition in the same profession and at the same cultural level would receive.
- The term disability means, with respect to an individual: (a) a physical or mental impairment that substantially limits one or more of the major life activities of such individual; (b) a record of such an impairment; or (c) being regarded as having such impairment.
The multitude of legal definitions which partially supplement and partially exclude one another suggest that definitions serve, above all, bureaucratic and administrative goals. Among all the listed definitions not one can be considered satisfactory, and all raise more questions than they answer. Beyond a few exceptions, most definitions are oriented towards the representation of an individual deficiency and do not address the correlation between an individual and his or her environment. What in reality is the reflection of a complex relativity is reduced in an administrative context to an apparently clear-cut and stable quantity. Such oversimplified definitions then tend to take on a life of their own and frequently force individuals into accepting a status that is commensurate with the law, but not necessarily with their own potential and aspirations.
Disability as an issue for sociopolitical action
Individuals who are recognized as disabled are, as a rule, entitled to measures such as medical and/or vocational rehabilitation or to draw on specific financial benefits. In some countries, the range of sociopolitical measures also includes the granting of certain privileges and support as well as special protective measures. Examples include: a legally embodied principle of equality of opportunity in vocational and social integration; a legally established right to needed assistance in the realization of equal opportunity, a constitutional right to education and vocational integration; the furtherance of vocational training and placement in employment; and a constitutional assurance of increased support in case of need of special help from the state. Several states proceed from the absolute equality of all citizens in all areas of life and have set the realization of this equality as their goal, without seeing a reason for treating the special problems of disabled persons in laws enacted expressly for that purpose. These states usually refrain from defining disability altogether.
Disability in the context of vocational rehabilitation
In contrast to the establishment of pension claims or privileges, the definition of disability in the area of vocational integration emphasizes the avoidable and correctable effects of disability. It is the purpose of such definitions to eliminate, through rehabilitative provisions and active labour market policies, the vocational disadvantages connected with disability. The vocational integration of disabled persons is supported by the allocation of financial assistance, by accompanying provisions in the area of vocational training and by the accommodation of the workplace to the special needs of the disabled worker. Here again, the practices vary greatly between different countries. The range of benefits runs from relatively slight and short-term financial allocations to large-scale, longer-term vocational rehabilitation measures.
Most states set a relatively high value on the furtherance of vocational training for disabled individuals. This can be provided in ordinary or special centres run by public or private agencies, as well as in an ordinary enterprise. Preference given to each differs from country to country. Sometimes the vocational training is conducted in a sheltered workshop or provided as on-the-job training that is reserved for a disabled worker.
As the financial implications of these measures can be considerable for the taxpayer, the act of recognizing a disability is a far-reaching measure. Often, however, the registration is done by a different authority than that which administers the vocational rehabilitation programme and which meets its costs.
Disability as a permanent disadvantage
While the goal of vocational rehabilitation is to overcome the possible negative effects of disability, there exists wide agreement in disability legislation that further protective social measures are sometimes necessary to assure the vocational and social integration of rehabilitated individuals. It is also generally recognized that disability presents the continuing risk of social exclusion independent of the existence of an actual functional disorder. In recognition of this permanent threat, legislators provide a series of protective and supportive measures.
In many countries, for example, employers who are prepared to employ disabled persons in their companies can expect subsidies towards the wages and social security contributions of the disabled workers, the amount and duration of which will vary. Generally, an effort is made to assure that disabled employees receive the same income as non-disabled employees. This can result in situations wherein disabled individuals who receive a lower wage from their employers are refunded up to the full difference through arrangements made by the social protection system.
Even the establishment of small businesses by disabled individuals may be supported through various measures such as loans and loan guarantees, interest subsidies and rent allowances.
In many countries, the protection of disabled individuals from dismissal and the protection of their right to re-employment is handled in different ways. Many states have no special legal regulation for the dismissal of disabled persons; in some, a special commission or institution decides on the justification and legitimacy of a dismissal; in others, special regulations for victims of industrial accidents, for severely disabled workers and for workers on extended periods of sick-leave are still in effect. The legal situation with regard to the re-employment of disabled individuals is similar. Here too, there are countries which recognize a general obligation of the enterprise to keep a worker employed after injury or to re-employ him or her after completion of rehabilitation measures. In other countries, businesses are not under any obligation to re-employ disabled employees. Furthermore, there exist in some countries recommendations and conventions as to how to proceed in such cases, as well as countries in which the employee who has suffered a specific occupational disability is guaranteed either redeployment or return to the previous job after his or her medical recovery is complete.
Differences in treatment by cause of disability
The above overview helps to illustrate that laws provide different types of legal claim which bear clear consequences for the respective national concept of disability. Also the reverse is true: in those countries which provide no such legal entitlements, there exists no need to define disability in legally clear and binding terms. In such cases, the predominant inclination is to recognize as disabled only those who are visibly and markedly disabled in a medical sense—that is, persons with physical impairments, blindness, deafness or mental handicap.
In modern disability legislation—though less in the realm of social security provision—the principle of finality is becoming more grounded. This principle means that not the cause of a disability, but exclusively the needs associated with the disability and the final outcome of measures should be the concern of legislators. Nevertheless, the social status and the legal claims of disabled individuals are often dependent on the cause of their disability.
In consideration of the cause of disability, definitions differ not only in meaning but also in the implications they have in terms of potential benefits and assistance. The most important distinctions are made between disabilities that result from hereditary or birth-related physical, mental or psychological deficiencies or impairments; disabilities brought on by diseases; disabilities caused by home, work, sport or traffic accidents; disabilities brought on by occupational or environmental influences; and disabilities as a result of civil strife and armed conflict.
The relative preference shown to some disabled groups is often the consequence of their respectively better coverage under the social security system. Preference can also reflect the attitude of a community—for instance in the case of war veterans or accident victims—that feels a co-responsibility for the incident that led to the disability, while hereditary disability is often regarded as a problem of the family only. Such societal attitudes towards disability often have more significant consequences than official policy and can sometimes exert a decisive influence—negative or positive—on the process of social reintegration.
Summary and outlook
The diversity of historical, legal and cultural situations renders the discovery of a unitary concept of disability, equally applicable to all countries and situations, virtually impossible. For lack of a common and objective definition of disability, statistics are frequently provided by authorities as a means of keeping client records and interpreting the outcome of measures—a fact that makes an international comparison very difficult, as systems and conditions vary greatly among countries. Even where reliable statistics exist, the problem remains that individuals may be included in statistics who are no longer disabled or who, after successful rehabilitation, are no longer inclined to consider themselves disabled.
In most industrialized countries, the definition of disability is, above all, connected with legal entitlements to medical, social and vocational measures, to protection against discrimination or to cash benefits. As such, most definitions in use reflect legal practice and requirements that differ from country to country. In many cases, the definition is linked to an act of official recognition of disability status.
Owing to developments as different as the emergence of human rights legislation and technological advancements, traditional concepts of disability that led to situations of protected exclusion and segregation are losing ground. A modern concept of disability puts the issue at the intersection between social and employment policies. Disability is thus a term of social and vocational, rather than of medical, relevance. It demands corrective and positive measures to ensure equal access and participation, rather than passive measures of income support.
A certain paradox arises out of the understanding of disability as, on the one hand, something which can be overcome through positive measures, and, on the other, as something lasting which necessitates permanent protective or ameliorative measures. A similar frequently encountered contradiction is that between the idea of disability as fundamentally an issue of individual performance or function restriction, and the idea of disability as the unjustified cause for social exclusion and discrimination.
Opting for one all-encompassing definition can have grave social consequences for particular individuals. Were it declared that all disabled persons are able to work, many would be deprived of their pension claims and social protection. Were all disabled persons judged to show a reduced productivity/performance, hardly a disabled individual would obtain employment. This means that a pragmatic approach must be sought that accepts the heterogeneity of the reality that an ambiguous term such as disability tends to conceal. The new view of disability takes into account the specific situation and needs of disabled individuals as well as the economic and social feasibility of removing barriers to integration.
The goal of preventing undue disadvantage that may be linked with a disability will best be achieved where a flexible definition of disability is applied that takes into account the specific personal and social circumstances of an individual and that avoids stereotyped assumptions. This calls for a case-by-case approach to recognizing disability, which still is needed where different statutory rights and entitlements, notably those to achieve equal training and employment opportunities, are granted under various national laws and regulations.
Nonetheless, definitions of disability are still in use that evoke negative connotations and that contradict integrative concepts by overemphasizing the limiting effects of an impairment. A new view of the matter is called for. The focus should be on recognizing disabled individuals as citizens endowed with rights and abilities, and on empowering them to take charge of their destiny as adults who want to take part in the mainstream of social and economic life.
Likewise, efforts must continue to instill in the community a sense of solidarity that no longer uses a flawed concept of disability as grounds for the careless exclusion of fellow citizens. Between excessive care and neglect there should exist a sober conception of disability which neither mystifies nor underestimates its consequences. Disability can, but need not always, provide the grounds for specific measures. It should in no case provide a justification for discrimination and social exclusion.
Practising Occupational Health in India
Workers’ health has been of interest to physicians in India for almost half a century. The Indian Association of Occupational Health was founded in the 1940s in the city of Jamshedpur, which has the country’s best known and oldest steel plant. However, multidisciplinary occupational health practice evolved in the 1970s and 1980s when the ILO sent a team which helped create a model occupational health centre in India. The industry and workplaces traditionally provided health care under the banner of First Aid Stations/Plant Medical Services. These outfits managed minor health problems and injuries at the worksite. Some companies have recently set up occupational health services, and, hopefully more should follow suit. However, the university hospitals have so far ignored the specialty.
Occupational safety and health practice started off with injuries and accident reporting and prevention. There is a belief, not without reason, that injuries and accidents remain under-reported. The 1990–91 incidence rates of injuries are higher in electricity (0.47 per 1,000 workers employed), basic metal (0.45), chemical (0.32) and non-metallic industries (0.27), and somewhat lower in wood and wood pulp industries (0.08) and machinery and equipment (0.09). The textile industry, employing more workers (1.2 million in 1991) had an incidence rate of 0.11 per 1,000 workers. With regard to fatal injuries, the incidence rates in 1989 were 0.32 per 1,000 workers in coal mines and 0.23 in non-coal mines. In 1992, a total of 20 fatal and 753 non-fatal accidents occurred in ports.
Figures are unavailable for occupational hazards as well as for the number of workers exposed to specific hazards. The statistics published by the Labour Bureau do not show these. The system of occupational health surveillance is yet to develop. The number of occupational diseases reported is abysmal. The number of diseases reported in 1978 was just 19, which climbed to 84 in 1982. There is no pattern or trend visible in the reported diseases. Benzene poisoning, halogen poisoning, silicosis and pneumoconiosis, byssinosis, chrome ulceration, lead poisoning, hearing loss and toxic jaundice are the conditions reported most frequently.
There is no comprehensive occupational health and safety legislation. The three principal acts are: the Factories Act, 1948; the Mines Act, 1952; and the Dock Workers Safety, Health and Welfare Act, 1986. A bill for construction workers’ safety is planned. The Factories Act, first adopted in 1881, even today covers workers only in the registered factories. Thus a large number of blue- as well as white-collar workers do not qualify for occupational safety and health benefits under any law. The inadequacy of law and poor enforcement are responsible for a not very satisfactory state of occupational health in the country.
Most occupational health services in industry are managed by either doctors or nurses, and there are few with multidisciplinary disposition. The latter are confined to large industry. The private industry and large public sector plants located in remote areas have their own townships and hospitals. Occupational medicine and occasionally industrial hygiene are the two common disciplines in most occupational health services. Some services have also started hiring an ergonomist. Exposure monitoring and biological monitoring have not received the desired attention. The academic base of occupational medicine and industrial hygiene is not yet well developed. Advanced courses in industrial hygiene and postgraduate degree courses in occupational health practice in the country are not widely available.
When Delhi became a state in 1993, the Health Ministry came to be headed by a health professional who reaffirmed his commitment to improving public and preventive health care. A committee set up to study the issue of occupational and environmental health recommended setting up an occupational and environmental medicine clinic in a prestigious teaching hospital in the city.
Dealing with the complex health problems arising out of environmental pollution and occupational hazards requires more aggressive involvement of the medical community. The teaching university hospital receives hundreds of patients a day, many of whom have exposure to hazardous materials at work and to the unhealthy urban environment. Detection of occupationally and environmentally induced health disorders requires inputs from many clinical specialists, imaging services, laboratories and so on. Owing to the advanced nature of disease, some supportive treatment and medical care becomes essential. Such a clinic enjoys the sophistication of a teaching hospital, and following detection of the health disorder, treatment or rehabilitation of the victim as well as the suggested intervention to protect others can be more effective as teaching hospitals enjoy more authority and command more respect.
The clinic has expertise in the area of occupational medicine. It intends to collaborate with the labour department, which has an industrial hygiene laboratory developed with liberal assistance under an ILO scheme to strengthen occupational safety and health in India. This will make the task of hazard identification and hazard evaluation easier. Medical practitioners will be advised about health assessment of the exposed groups at the point of entry and periodically, and regarding record keeping. The clinic will help sort out the complicated cases and ascertain work-relatedness. The clinic will offer expertise to industry and workers on health education and safe practices with regard to the use and handling of hazardous materials in the workplace. This should make primary prevention more easily achievable and will strengthen occupational health surveillance as envisaged under the ILO Convention on Occupational Health Services (No. 161) (ILO 1985a).
The clinic is being developed in two phases. The first phase is focusing on identifying hazards and creating a database. This phase will also emphasize the creation of awareness and developing outreach strategies with regard to hazardous working environments. The second phase will focus on strengthening exposure monitoring, medical toxicological evaluation and ergonomic inputs. The clinic plans to popularize occupational health teaching for undergraduate medical students. The postgraduate students working on dissertations are being encouraged to choose topics from the field of occupational and environmental medicine. A postgraduate student has recently completed a successful project on acquired blood-borne infections among health care workers in the hospitals.
The clinic also intends to take up environmental concerns, namely the adverse effects of noise and rising pollution, as well as the adverse effects of environmental lead exposure on children. In the long run education of primary health care providers and community groups is also planned through the clinic. The other goal is to create registers of prevalent occupational diseases. The involvement of several clinical specialists in occupational and environmental medicine is also going to create an academic nucleus for the future, when a higher postgraduate qualification hitherto unavailable in the country can be undertaken.
The clinic was able to draw the attention of enforcement and regulatory agencies towards the serious health risks to fire fighters when they fought a major polyvinyl chloride fire in the city. The media and environmentalists were only talking of risks to the community. It is hoped that such clinics will in the future be set up in all major city hospitals; they are the only way to involve senior medical specialists in occupational and environmental medicine practice.
Conclusion
There is an urgent need in India to introduce a Comprehensive Occupational Health and Safety Act in line with many indus-trialized countries. This should be associated with the creation of an appropriate authority to supervise its implementation and enforcement. This will enormously help ensure a uniform standard of occupational health care in all states. At present there is no linkage between the various occupational health care centres. Providing quality training in industrial hygiene, medical toxico-logy and occupational epidemiology are other priorities. Good analytical laboratories are required, which should be certified to ensure quality. India is a very rapidly industrializing country, and this pace will continue into the next century. Failing to address these issues will lead to incalculable morbidity and absenteeism as a consequence of work-related health problems. This will undermine the productivity and competitiveness of industry, and gravely affect the country’s resolve to eliminate poverty.
Occupational Safety and Health in the Czech Republic
Geopolitical Background
The predominant development of heavy industry (the iron and steel industry, smelting and refinery plants), metalworking and machinery industries, and the emphasis on the production of energy in Central and Eastern Europe, have significantly predetermined the structure of the economies in the region for the last four decades. This state of affairs has resulted in the relatively high exposures to certain types of occupational hazards in the workplace. Current efforts to transform the existing economies along the lines of the market economy model and to improve occupational safety and health have been considerably successful so far, given the short period of time for such an endeavour.
Until recently, ensuring the prevention of adverse health effects of chemicals present in occupational settings and in the environment, the drinking water and the food basket of the population was provided for by the compulsory observance of hygienic and sanitary standards and occupational exposure limits such as Maximum Allowable Concentrations (MACs), Threshold Limit Values (TLVs) and Acceptable Daily Intake (ADI). The principles of toxicity testing and exposure evaluation recommended by various international organizations, including standards applied in the countries of the European Union, will become more and more compatible with those used in the Central and Eastern European countries as the latter gradually integrate with other European economies.
During the 1980s the need was increasingly recognized to harmonize the methodologies and scientific approaches in the field of toxicology and hygienic standardization applied in the OECD countries with those used in the member countries of the Council of Mutual Economic Assistance (CMEA). This was mainly due to growing levels of production and trade, including industrial and agricultural chemicals. A contributing factor favouring the urgency with which these considerations were viewed was a growing problem of air and river pollution across national boundaries in Europe (Bencko and Ungváry 1994).
The Eastern and Central European economic model was based on a centrally planned economic policy oriented to the development of basic metal industries and the energy sector. As of 1994, except for minor changes, the economies of the Russian Federation, Ukraine, Belarus, Poland, and the Czech and the Slovak Republics had preserved their old structures (Pokrovsky 1993).
Coal mining is a widely developed industry in the Czech Republic. At the same time, black coal mining (e.g., in the northern Moravian region of the Czech Republic) is a cause of 67% of all new cases of pneumoconioses in the country. Brown coal is extracted in opencast mines in northern Bohemia, southern Silesia and neighbouring parts of Germany. Thermal power stations, chemical plants and brown coal mining heavily contributed to the environmental pollution of this region, forming the so-called “black” or “dirty triangle” of Europe. Uncontrolled use of pesticides and fertilizers in agriculture was not exceptional (Czech and Slovak Federal Republic 1991b).
The labour force of the Czech Republic numbers some 5 million employees. About 405,500 workers (that is, 8.1% of the working population) are involved in hazardous operations (Ministry of Health of the Czech Republic 1992). Figure 1 presents data on the number of workers exposed to different occupational hazards and the proportion of women among them.
Figure 1. Number of workers in the Czech Republic exposed to the most serious occupational risks

Changing Needs
The occupational health system of the Czech Republic underwent three consecutive stages in its development and was influenced by the political and economic changes in the country (Pelclová, Weinstein and Vejlupková 1994).
Stage 1: 1932-48. This period was marked by the foundation of the first Department of Occupational Medicine by Professor J. Teisinger at the oldest university in Central Europe—Charles University (founded in 1348). Later, in 1953, this department became the Clinic of Occupational Medicine, with 27 beds. Professor Teisinger also founded the Research Institute of Occupational Health and in 1962 the Poison Information Centre at the Clinic. He was granted several international awards, including an award from the American Association of Industrial Hygienists in 1972 for his personal contribution to occupational health development.
Stage 2: 1949-88. This period exhibited numerous inconsistencies, in some respects being marked by notable deficiencies and in others showing distinct advantages. It was recognized that the existing system of occupational health, in many ways reliable and well developed, nevertheless had to be reorganized. Health care was considered as a basic civil right guaranteed by the Constitution. The six basic principles of the health system (Czech and Slovak Federal Republic 1991a) were:
- planned integration of health care into the society
- promotion of a healthy lifestyle
- scientific and technical development
- prevention of physical and mental illnesses
- free and universal access to health care services
- concern on the part of the state for a healthy environment.
Despite certain progress none of these goals had been fully achieved. Life expectancy (67 years for men and 76 years for women) is the shortest among the industrialized countries. There is a high mortality rate from cardiovascular diseases and cancer. About 26% of adult Czechs are obese and 44% of them have cholesterol levels above 250 mg/dl. The diet contains much animal fat and is low in fresh vegetables and fruits. Alcohol consumption is relatively high, and around 45% of adults smoke; smoking kills about 23,000 persons a year.
Medical care, dental care and medicines were provided free of charge. The numbers of physicians (36.6 per 10,000 inhabitants) and nurses (68.2 per 10,000) were among the highest in the world. But in the course of time the government became unable to cover the continually increasing and abundant expenses needed for public health. There had been temporary shortages of some drugs and equipment as well as difficulties in providing health care services and rehabilitation. The existing structure, which did not allow a patient to choose his primary health care physician, created many problems. Medical staff working in the state-run hospitals received low fixed salaries and had no incentives to provide more health care services. A private health care system did not exist. In hospitals, the main criterion of acceptable functioning was the “percentage of occupied beds” and not the quality of the health care provided.
However, there were positive features of the state-run centralized system of occupational health. One of them was an almost complete registration of hazardous workplaces and a well-organized system of hygienic control provided by the Hygienic Service. In-plant occupational health services established in large industrial enterprises facilitated the provision of comprehensive health care services, including periodic medical examinations and treatment of workers. Small private enterprises, which usually pose many problems to occupational health programmes, did not exist.
The situation was similar in agriculture, where there were no small private farms, but large-scale cooperative ones: an occupational physician working in a health centre of a factory or a cooperative farm provided occupational health services for the workers.
Enforcement of occupational safety and health legislation was sometimes contradictory. After an inspection of a hazardous workplace was carried out by an industrial hygienist or factory inspector, who had required the reduction of the level of occupational exposure and the enforcement of prescribed health and safety standards, rather than correct the hazards the workers would receive monetary compensation instead. Besides the fact that enterprises often took no action at all to improve working conditions, the workers themselves were not interested in improving their working conditions but opted to continue receiving bonuses in lieu of changes in the working environment. Furthermore, a worker who contracted an occupational disease received a substantial monetary recompense according to the severity of the disease and to the level of his or her previous salary. Such a situation produced conflicts of interests among industrial hygienists, occupational physicians, trade unions and enterprises. As many of the benefits were paid by the state and not by the enterprise, the latter often found it cheaper not to improve safety and health in the workplace.
Strange as it may seem, some hygienic standards, including permissible levels and occupational exposure limits, were more rigorous than those in the United States and in the western European countries. Thus, it was sometimes impossible not to exceed them with outdated machinery and equipment. Workplaces exceeding the limits were classified under “category 4”, or most hazardous, but for economic reasons manufacturing was not stopped and workers were offered compensatory benefits instead.
Stage 3: 1989–the present. The “velvet revolution” of 1989 enabled an inevitable change of the public health care system. The reorganization has been rather complex and sometimes difficult to accomplish: consider, for example, that the health care system has more beds in hospitals and doctors per 10,000 inhabitants than any industrialized country while it uses disproportionately less financial resources.
The Current Status of Occupational Safety and Health
The most frequent occupational hazard at the workplace in the Czech Republic is noise—about 65.8% of all workers at risk are exposed to this occupational hazard (Figure 8). The second major work-related hazard is fibrogenic dust, which represents an occupational hazard to about 21.3% of all workers at risk. Approximately 14.3% of workers are exposed to toxic chemicals. More than one thousand of these are exposed to toluene, carbon monoxide, lead, gasoline, benzene, xylene, organophosphorus compounds, cadmium, mercury, manganese, trichlorethylene, styrene, tetrachloroethylene, aniline and nitrobenzene. Another physical hazard—local hand-arm vibration—is a danger for 10.5% of all workers at risk. Other workers are exposed to chemical carcinogens, ionizing radiation and dangerous substances causing skin lesions.
The number of acknowledged cases of occupational disease in the Czech Republic in 1981-92 is presented in figure 2.
Figure 2. Occupational diseases in the Czech Republic in the period 1981-1992
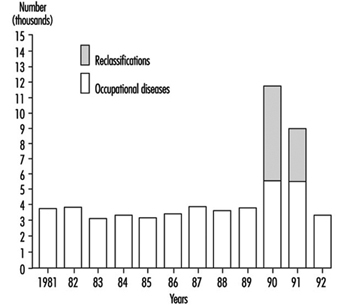
The increase of morbidity from occupational diseases in 1990–91 had been due to the process of reclassification of occupational illnesses requested by miners and workers in other occupations and by their trade unions. They asked to change the status of “being endangered with an occupational disease”, used for less obvious forms of occupational impairment with low compensation, to fully compensated disease. The status of “endangerment” was reconsidered by the Ministry of Health in 1990 for the following kinds of occupational pathology:
- mild forms of pneumoconioses
- mild forms of chronic musculoskeletal disorders due to overload and vibration
- mild forms of occupational hearing loss.
Reclassification was done for all cases before 1990 and concerned 6,272 cases in 1990 and 3,222 cases in 1991 (figure 2). After that the status of “endangerment” was abolished. Figure 3 presents data on 3,406 new cases of occupational diseases by category diagnosed in the Czech Republic in 1992; 1,022 cases of these occupational diseases were diagnosed in women (Urban, Hamsova and Neecek 1993).
Figure 3. Occupational diseases in the Czech Republic in 1992
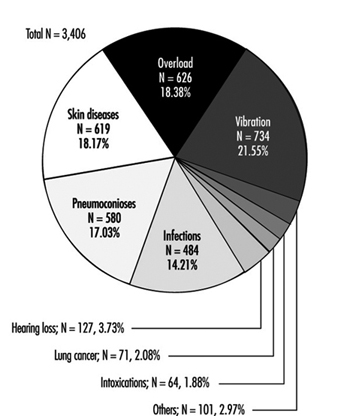
Some shortages in the supply of measuring equipment for sampling and analysis of toxic substances make it difficult to conduct occupational hygiene evaluations in the workplace. On the other hand, the use of biomarkers in exposure tests for the monitoring of workers in hazardous occupations is practised for a variety of dangerous substances according to the regulations of the Czech Republic. Similar tests have already been legally codified in Hungary, Slovakia, Slovenia, Croatia, Poland, and in some other countries of Central and Eastern Europe. The use of exposure tests for periodic medical examinations has proved to be a very efficient tool for personnel exposure monitoring. This practice has enabled early detection of some occupational diseases and permitted their prevention, thus decreasing compensation costs.
The transition to the market economy and the rising costs of health care services in the Czech Republic have had their influence on occupational health services. In the past, the in-plant based occupational health service or centre provided both health surveillance and treatment for workers. Nowadays, these activities are subjected to some restrictions. This has resulted in reduced activities in health surveillance and hazard control and in an increased number of occupational accidents and diseases. Workers in rapidly emerging small-scale enterprises, which often operate with unreliable machinery and equipment, are practically out of the reach of occupational health professionals.
Projects for the Future
A new system of public health in the Czech Republic is expected to incorporate the following principles:
- prevention and health promotion
- overall access to “standard” health care
- decentralized policy determining delivery of services
- integration of health services in a territorial network
- increased autonomy of health care professionals
- emphasis on outpatient care
- compulsory health insurance
- community participation
- more options for patients
- new public/private sector partnership to provide an “above standard” health care no longer offered by the public sector.
The introduction of the compulsory health insurance system and the creation of the General Health Insurance Office, which began operating in January 1993, as well as minor health insurance companies in the Czech Republic have marked the beginning of reform in the public health sector. These changes have brought some problems to the occupational health services, given their preventive character and the high cost of treatment in hospitals. Thus, the role of outpatient medical settings in treating patients with conventional as well as work-related diseases is steadily increasing.
The Potential Impact of Continuing Changes on Occupational Safety and Health
The growth of reform in the public health sector has created a need for change for occupational physicians, industrial hygienists and in-patient medical settings, and has also led to a focus on prevention. The ability to focus on prevention and milder forms of disease is partly explained by earlier positive results and by the relatively good functioning of the previous occupational health system, which had worked effectively towards eliminating major serious occupational diseases. The changes have involved a shift of attention from severe forms of occupational pathology that needed urgent treatment (such as industrial poisoning and pneumoconioses with respiratory and right-heart failure) to mild forms of disease. The change in the activities of the occupational health services from a curative orientation to early diagnosis now concerns such conditions as mild forms of pneumoconioses, farmer’s lung, chronic liver illnesses and chronic musculoskeletal disorders due to overload or vibration. Preventive measures at the earlier stages of occupational diseases also should be undertaken.
Industrial hygiene activities are not covered by the health insurance system, and the industrial hygienists in the hygienic stations are still paid by the government. Lowering their number and the reorganization of hygienic stations are also expected.
Another change in the health care system is the privatization of some health services. The privatization of small out-patient medical centres has already started. Hospitals—including university hospitals—are not involved in this process at present and details of their privatization still need to be clarified. New legislation concerning the duties of the enterprises, workers and occupational health services is being gradually created.
Occupational Health at the Crossroads
Thanks to the advanced system of occupational health founded by Professor Teisinger in 1932, the Czech Republic does not face a serious problem of education in occupational health for university students, even though in some countries of Central and Eastern Europe the rate of recognized occupational diseases is about five times less than that of the Czech Republic. The Czech List of Occupational Diseases does not differ notably from that appended to the ILO Employment Injury Benefits Convention, (No. 121), (ILO 1964). The proportion of unrecognized principal occupational diseases is low.
The occupational health system in the Czech Republic is now at the crossroads and there is an obvious need for its reorganization. But it is necessary at the same time to preserve whatever positive features have been acquired from experience with the previous occupational health system, namely:
- registration of working conditions at the workplaces
- maintaining in operation a broad system of periodic medical examinations of employees
- provision of curative health care services at large-scale enterprises
- offering a system of vaccination and communicable disease control
- preserving the system whereby occupational health services admit patients with various occupational illnesses, a system that would involve the university hospitals in providing treatment to patients as well as education and training to medical students and graduates.
The Practice of Occupational Health Service in the People's Republic of China
China, the world’s largest developing country, is striving to accomplish unprecedented modernization. The “opening-up” policy to outside interests and the economic reform in effect since 1979 have brought profound changes to China’s economy and to every aspect of its society. The GNP increased from 358.8 billion yuan RMB in 1978 to 2,403.6 billion in 1992, an increase of more than three times in terms of constant money value. The average annual growth rate of GNP was 9.0%. The gross industrial output value was 3,706.6 billion in 1992, an average annual growth of 13.2% from 1979 to 1992 (National Statistics Bureau 1993). China is being increasingly regarded as a “potential centre of economic activity” and has attracted 40% of all of the direct foreign investment in the developing world. By the end of 1993, 174,000 foreign-funded projects had been approved, bringing US$63.9 billion into the country, and the total cumulatively pledged foreign input was $224 billion (China Daily 1994a, 1994b).
In order to advance current reforms in a comprehensive manner ensuring harmonious progress in all economic sectors, an in-depth reform decision has been made. The objective of this reform of the economic structure is to establish a socialist market economy that will further liberate and expand China’s productive forces. The centrally planned economy which has been favoured for 40 years is being transformed into a market system. Whatever the market can manage itself should be left to be controlled by the market. The government should guide the growth of the market by economic policies, regulations, planning and necessary administrative means.
During the period of rapid social change and industrialization, especially the transition from a centrally planned economic system to a market-oriented economy, great challenges had to be faced by China’s traditional occupational health service. At the same time, many new occupational health problems are continually emerging while older ones have not yet been solved.
Reviewing the history of over 40 years of development of occupational health in China, one can observe that great achievements have been made and many efforts have proved to be successful. However, there is still a big gap between the growing need for occupational health capabilities and the currently limited service capacity. Like many other aspects of Chinese life, occupational health service is undergoing a tremendous reform.
Historical Review
Occupational health service, as a subsystem of China’s public health services, was established in the early 1950s. In 1949, when the People’s Republic of China was founded, the health status of the Chinese people was poor. Life expectancy at birth was 35 years. The occupational safety and health status of workers presented an even worse picture. The prevalence of occupational diseases, communicable diseases and injuries among workers was high. Workers were generally prematurely withdrawn from their jobs. To counter the hazardous working conditions and poor sanitation left over in the factories of the “old China”, the new government took three measures (Zhu 1990): (1) the establishment of health service institutions in large-scale industrial enterprises; (2) an extensive investigation of sanitation and safety in the factories; and (3) the improvement of sanitary conditions at the workplace and of worker’s living facilities.
The statistical data relating to China’s oldest industrial bases showed that, by 1952, 28 factory hospitals, 795 clinics and 30 sanatoria had been established in eastern China; in the northeastern region, the level of medical and health services in industrial enterprises had increased 27.6%, the number of health workers increased 53.2% and the number of hospital beds increased 12%—all these improvements took place in the three-year period from 1950 through 1952. Most of the seriously unsafe working conditions found in state-run enterprises by governmental checkups were improved through the joint endeavours of government and workers’ participation. The government also gave financial support to the construction of housing and sanitary facilities. By 1952, workers’ housing had increased ten times compared to 1950, the number of bathroom facilities increased 216%, restrooms increased 844% and workers’ clubs increased 207% (from the northeastern region statistics). Nutrition subsidies have been given to workers exposed to occupational hazards since 1950. These developments greatly promoted the resumption of industrial production at the time.
Since 1954, following Chairman Mao Ze-dong’s call for “approaching a socialist industrialized nation step by step”, China speeded up its industrial development. The government’s priorities for workers’ health started to be transferred from sanitation to occupational and environmental health and concentrated on the prevention and control of serious occupational diseases and injuries. The first Constitution of the People’s Republic of China stipulated that labourers should enjoy the right of protection by government and that the health and welfare of all labourers must be improved.
The central government—State Council—has paid great attention to the serious situation of occupational health problems. The First National Conference on Silica Dust Control in Working Environments was jointly convened by the Ministries of Public Health (MOPH) and Labour (MOL), and the All-China Federation of Trade Unions (ACFTU) in Beijing in 1954, just four years after the founding of the People’s Republic of China. The Second Conference on Silica Dust Control was convened five years later by the above-mentioned three agencies in conjunction with such industrial administration sectors as the Ministry of the Coal Industry and the Ministry of Constructive Material Manufacture, among others.
At the same time, heat stress, occupational poisoning, industrial noise injuries and other illnesses induced by physical factors as well as pesticide poisoning in agriculture were put on the agenda of occupational health. Through the active recommendations to the State Council expressed through the joint efforts of MOPH, MOL, ACFTU and the Ministry of Industrial Administration (MOIA), a series of decisions, policies and strategies to strengthen the occupational health programme have been made by the State Council, including those relating to labour insurance, health and safety requirements for working environments, medical care for occupational illnesses, health examinations for workers engaged in hazardous work, establishing “health inspection” systems, and also the large amount of financial support needed to improve working conditions.
Organizational Structure of Occupational Health Delivery
The occupational health service network in China was initially established in the 1950s and has gradually taken shape over forty years. It can be seen at different levels:
In-plant service
As early as 1957, MOPH (1957) published a Recommendation on Establishing and Staffing Medical and Health Institutions in Industrial Enterprises. The principles of the document were adopted as national standards in the Hygienic Standards for Design of Industrial Premises (MOPH 1979) (see table 1). There should be a health department or a health and safety department at the management level of the enterprise, which should also be under the supervision of the local public health authority of the government. A workers’ hospital affiliated with the department functions as a medical/health centre, which provides preventive and curative services, including health surveillance of workers for occupational safety and health purposes, evaluation of working capacity from the medical point of view and approval of sick leaves of workers. There are health care stations near the workshops, which, under the management of and with the technical support of the workers’ hospital, play an important role in first aid, occupational health education for workers, collection of health information of workers at the workplaces and supervision of occupational safety and health jointly with trade unions and safety engineering departments.
Table 1. Minimum requirements of an in-plant health facility
|
Size of enterprise (employees) |
In-plant health facility |
Floor space ( m2 ) |
Minimum requirement |
|
>5,000 |
Hospital* |
To meet the construction standard for Comprehensive Hospitals |
|
|
3,501–5,000 |
Clinic |
140–190 |
Waiting room, consulting room, therapy room, clinic and IH laboratory x-ray room and pharmacy |
|
2,001–3,500 |
Clinic |
110–150 |
(same as above) |
|
1,001–2,000 |
Clinic |
70–110 |
X-ray is not required |
|
300–1,000 |
Clinic |
30–0 |
X-ray and laboratory are not required |
* Industrial enterprises with more than 3,000 employees can establish an in-plant hospital if they have high-risk productive processes, are located at far distances from a city or are situated in mountain areas with poor transportation.
Administrative division-based occupational health delivery
Providing health service is one of the responsibilities of governments. In the early 1950s, to prevent and control serious communicable diseases and to improve environment health, Health and Epidemic Prevention Stations (HEPSs) were established in every administrative division from provinces down to counties. The functions of the HEPSs were expanded with the growing needs of society and economic development to include preventive medical services, which covered occupational health, environmental health, food hygiene, school health, radiation protection as well as control of communicable and some non-communicable diseases. With health legislation being emphasized, the HEPSs are authorized to enforce the public health regulations and standards promulgated by the state or local governments and to implement inspection. The HEPSs, especially those at the provincial level, also provide public health technical assistance and services to the community and are involved in in-service training and scientific research.
The industrialization drive in China in the 1950s and early 1960s greatly accelerated the development of the occupational health service programme, which became one of the biggest departments in the HEPS system. Most medium and small industrial enterprises which were not able to maintain in-plant occupational health and industrial hygiene services could be covered by the HEPSs occupational health services, most of which were free of charge.
During the “Cultural Revolution” from 1966 to 1976, the occupational health service network and its activities were seriously damaged. This is one of the important reasons why some occupational diseases are still seriously prevalent in China. The reconstruction of the occupational health programme started in the late 1970s, when China began to realize once again the importance of economic development. Since the beginning of the 1980s, hospitals for occupational disease prevention and treatment and institutes of occupational health, called occupational health institutions (OHIs) have rapidly been established in most provinces and some industrial administrative sectors under the favourable policy of the government. OHIs were formed mainly on the basis of utilizing occupational health personnel in HEPS integrated with occupational physicians from hospitals. During the period 1983 to 1991, the central and local governments invested 33.8 million yuan RMB in total to support building OHIs. At provincial and prefecture levels, 138 OHIs were set up, with appropriate laboratory or clinical equipment. At present, the number of OHIs has reached 204, of which there are 60 established by the industrial sector. Another 110 million yuan RMB have been invested to equip 1,789 health and epidemic prevention stations at the county level (He 1993). The occupational health programmes in county HEPSs were one of the important parts of the project to be first equipped. To strengthen the national capacity of research, training and coordination of occupational health service, a National Centre for Occupational Disease Prevention and Treatment (NCODPT) was set up in the Institute of Occupational Medicine, Chinese Academy of Preventive Medicine (IOM/CAPM), and seven regional centres of occupational health, located in Beijing, Shanghai, Shenyang, Lanzhou, Chengdu, Changsa and Guangzhou, were also established. The current national network of occupational health services is illustrated in figure 1.
Figure 1. National network of occupational health services
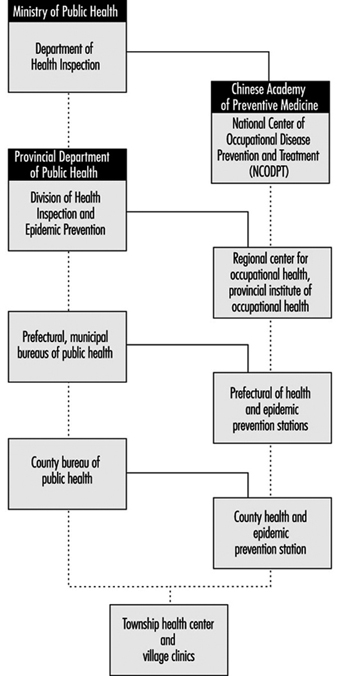
So far, 34 schools or departments of public health have been established in the medical colleges or medical universities. These are the main resources of occupational health personnel. Six national occupational health in-service training centres were established in 1983. The total professional occupational health personnel, including physicians, industrial hygienists, technicians in laboratories and other health workers involved in occupational health programmes, reached about 30,000 in 1992.
Occupational Health Standards and Legislation.
To encourage research in hygienic standards and in their establishment, a National Technical Committee of Hygienic Standards (NTCHS) was set up in 1981 as a consultative and technical reviewing agency of MOPH in hygienic standard setting. At present, NTCHS has eight subcommittees, which are responsible for occupational health, environmental health, school hygiene, food hygiene, radiation protection, occupational disease diagnosis, communicable disease and endemic disease prevention (figure 2). The members of NTCHS are experts from universities, research institutes, governmental agencies and the trade unions. The Hygienic Standards for Design of Industrial Premises (HSDIP) was first formulated in the 1950s and revised and promulgated again in 1979, so that it now contains a list of occupational exposure limits in terms of maximum allowable concentrations (MACs) for 120 toxic agents and dusts, and other requirements for hazards control measures in workplaces, sanitary and health facilities in plants and so forth. Also, there were 50 occupational hygienic standards for hazardous chemical and physical agents in the workplace promulgated by the Ministry of Public Health. Another 127 occupational hygienic standards are being reviewed. Diagnostic criteria for 50 compensable occupational diseases were issued by the Ministry of Public Health.
Figure 2. The management of health standard setting
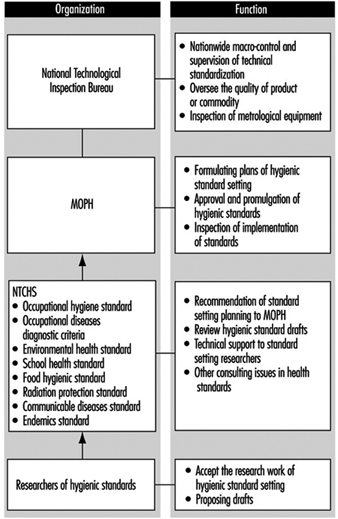
As is known to all, China has had a centrally planned economic system and has been a country controlled by a unified central government for more than 40 years. So, most regulatory requirements in occupational safety and health at the national level were stipulated in the form of “Red Title” documents of the central government. These documents had, indeed, the highest legal effect and have constituted the basic regulatory framework of China’s occupational health. There are more than 20 documents of this kind promulgated by the State Council or its ministries. The major differences between these documents and legislation are that there are no stipulations for penalties in the documents, the compulsory effect is not as high as it is with laws and enforcement is weak.
Since economic reform has favoured the market-oriented system following the opening-up policy, national legislation has been greatly emphasized. Occupational health management is also being transformed from traditional administration to regulation-based approaches. One of the most important legal documents is the Regulation on Pneumoconioses Prevention and Control, issued by the State Council in 1987. Another milestone in protecting workers’ rights is the promulgation of the Labour Law by the National People’s Congress, with an anticipated effect date of 1 January 1995. The occupational safety and health of workers, as one of the major aims of this measure, is stipulated in the Law. To implement the Labour Law for occupational disease control, a draft law for occupational disease prevention and control was submitted to the Bureau of Legislation of the State Council by the Ministry of Public Health, in which most of the successful occupational health policies basic to occupational institutions, and experiences both in China and abroad. The draft must undergo further review and be submitted to the Standing Committee of the National People’s Congress.
Health Inspection System
“Putting prevention first” has been emphasized by the government and has become an important national basic public health principle. As early as 1954, when industrialization had just begun, the central government made the decision to establish a health inspection system to enforce the national health regulations and policies of industrial hygiene. HEPSs were authorized to implement health inspection on behalf of the public health authorities of the government. The main tasks of health inspection of enterprises include the following:
- to inspect the enterprise for hazard control in workplaces so that the concentrations/intensities of occupational hazards meet national industrial hygienic standards
- to check whether or not the pre-placement and periodic health examinations of exposed workers have been conducted in compliance with related national regulations or local governmental requirements
- to ensure that workers who are suffering from occupational diseases be properly treated, allowed to recuperate, transferred to other jobs or offered some other suitable option in line with related regulations
- to conduct hygienic evaluation and to supervise hazard control measures in workplaces
- to supervise occupational health record keeping, occupational disease reporting and working environmental monitoring in enterprises.
- The above activities are part of “regular health inspection” and are considered routine inspecting tasks that should be carried out periodically. To continue, the remaining chief tasks of health inspection are:
- preventive health inspection on industrial construction projects (prior to a new industrial construction or reconstruc-ting/expanding of old industrial enterprises, all engineering designs, hazard control facilities, medical/health and workers’ living facilities must pass an initial inspection for occupational health purposes)
- toxicological assessment of new industrial chemical substances.
Health inspection, especially preventive health inspection as a fundamental principle of public health intervention measures, has been stipulated in a number of laws and public health regulations. Since the 1970s, as great attention has been paid to the control of environmental pollution, preventive occupational health inspection has further been expanded to whole process inspection. The principle that “hazard control installations must be simultaneously designed, constructed and put into use/operation with the principal part of the project” was one of the important requirements in the Regulation on Pneumoconiosis Prevention and Control and the Environmental Protection Law.
Comprehensive Prevention Strategy for Occupational Diseases
Along the way to controlling pneumoconioses and serious dust contamination in the working environment, comprehensive prevention was emphasized, which was summed up in eight Chinese characters, and so called the “Eight Characters” strategy. The meanings are translated in English as follows:
- innovation: technological improvement, such as using safe or low-risk materials and more productive processes, and replacing outmoded productive methods by appropriate advanced techniques
- keep it wet: keeping a dusty worksite wet to decrease the concentration of dust, especially for drilling and grinding in mining industries
- enclosure: segregating workers, equipment and environmental areas to prevent the escape of dust and operators’ subsequent contamination
- ventilation: improving natural and mechanical ventilation
- protection: providing personal protection for exposed workers
- supervision: setting up regulations and safe operating rules, and supervising workers to ensure that they follow them strictly
- education: implementing health and safety education programmes to promote workers’ participation and enhance their awareness and skills with regard to personal protection
- checking up: inspecting the working environments to meet national standards and regularly examining the workers’ health in line with national requirements.
It has been proved by the practices of many enterprises that the “Eight Characters” strategy is important and effective in improving working conditions.
Environmental Monitoring in Workplaces
Enterprises with hazardous working environments should periodically monitor the concentrations or intensities of the hazards at worksites and take measures to control risks to meet national industrial hygienic standards (for example, with reference to values of MACs). If the enterprises are not able to conduct environmental monitoring by themselves, local OHIs or HEPSs can provide services.
To control the quality of workplace monitoring conducted by enterprises, OHIs or HEPSs must conduct inspection regularly or whenever necessary. NCODPT is responsible for the nationwide quality control of workplace hazard monitoring. A number of technical regulations for air monitoring in the workplace have been promulgated by MOPH or been published as national recommendations by NCODPT—for example, Methods for Airborne Dust Measurement in the Workplace (GB 5748–85) (MOPH 1985) and Methods for Monitoring and Analysis of Chemical Hazards in Air of Workplace (Institute of Occupational Medicine 1987).
To control further the quality of environmental monitoring in workplaces a set of quality assurance norms for measurement of hazardous substances in the working environment has been submitted to MOPH for further review and approval. The qualifications of institutions which undertake workplace monitoring would be reviewed and licensed, requiring:
- professional ability on the part of the person who takes the samples or engages in analytical work
- necessary equipment for sampling and analysis and their proper calibration
- reagents and standard solutions
- quality assurances for air and biological material sampling
- inter-laboratory quality assurances and similar checks.
At present, a pilot study on assessment of the laboratories is being conducting in 200 laboratories or institutions. This is the first step to implement the Quality Assurance Norm.
Health Examinations of Workers
Workers exposed to occupational hazards in workplaces should have occupational health examinations. This was first required for workers exposed to dust in the 1950s. It quickly expanded to cover workers exposed to toxic chemicals and physical hazards.
The health examinations include a pre-employment or fitness-to-work examination and periodic examinations. These medical examinations must be carried out by OHIs or competent medical/health institutions licensed by government public health administrations.
Pre-employment examination
A pre-employment examination is required for new workers or workers newly transferred to hazardous workplaces. The medical examinations focus on assessment of the health of workers in relation to the workplace conditions to ensure that the specific job they intend to hold will be of no damage to their health, and those who are not fit for a given job are excluded. Health criteria to determine job contraindications for different hazardous work conditions have been stipulated in detail in the National Diagnostic Criteria and Principles of Management of Occupational Diseases (Health Standards Office 1993) and Guideline of Occupational Health Service and Inspection promulgated by MOPH (1991b).
Periodic examination
Workers exposed to different hazards have different intervals of medical examinations. The period of examination for workers exposed to dust, for example, is illustrated in table 2. Workers suffering from pneumoconioses should have annual physical examinations.
Table 2. Periodic examination requirement for workers exposed to dust
|
Nature of dust |
Examination intervals (years) |
|
|
Workers in service |
Workers withdrawn |
|
|
Free silica content (%) |
||
|
80 |
0.5–1 |
1 |
|
40 |
1–2 |
2 |
|
10 |
2–3 |
3 |
|
10 |
3–5 |
5 |
|
Asbestos |
0.5–1 |
1 |
|
Other dust |
3–5 |
5 |
All medical records should be well secured both in enterprises and in local OHIs, and should be reported annually to the local government public health authority, and then to the NCODPT and the MOPH.
When anyone transfers to an enterprise from a plant involving risks of hazardous exposure, a health examination must be given by a local OHI to clarify whether his or her health has been damaged by exposure, and the health records must be sent to the new enterprise with the worker (MOPH 1987).
Table 3 shows the statistics of workers’ health examinations in the period 1988-1993. A total of 64 million workers were covered by the network of the occupational health service, which included state-owned and city collective-owned enterprises, and a part of rural industries at the township level. The workers exposed to occupational hazards account for 30% of the total workers. Nearly 4 million exposed workers, about 20% of the total, had medical examinations every year. In 1993, for example, the total number of the industrial population was 64,345,193, according to the report from the National Centre of Occupational Health Reporting (NCOHR 1994) (there was, however, a lack of data from Neimeng, Tibet and Taiwan). The proportion of workers exposed to occupational hazards accounted for 31.28% (20,126,929), of which 3,982,940 were examined, accounting for 19.79%. The total rate of detected compensable occupational diseases was 0.46% in 1993 (MOPH 1994).
Table 3. Physical examinations for workers exposed to occupational hazards
|
Year |
Number of |
Proportion of |
Examination rate |
Detected rate of |
|
1988 |
62,680 |
29.36 |
18.60 |
0.90 |
|
1989 |
62,791 |
29.92 |
20.67 |
0.57 |
|
1990 |
65,414 |
29.55 |
20.47 |
0.50 |
|
1991 |
66,039 |
30.30 |
21.03 |
0.57 |
|
1992 |
64,222 |
30.63 |
20.96 |
0.40 |
|
1993 |
64,345 |
31.28 |
17.97 |
0.46 |
The Management of Occupational Diseases
Compensable occupational diseases
Generally speaking, any illnesses caused by exposure to hazardous factors present in the workplace or resulting from processes of production is considered an occupational disease. However, for compensation purposes, a list of occupational diseases has been issued by the MOPH, the MOL, the Ministry of Finance and the ACFTU (MOPH 1987). The list covers nine categories, including pneumoconioses; acute and chronic occupational poisonings; diseases induced by physical factors; occupational communicable diseases; occupational dermatoses; occupational eye impairments; occupational ear, nose and throat diseases; and occupational tumours. The total is 99 diseases. If any other disease is proposed by local governments or governmental sectors to supplement the list, it should be submitted to the MOPH for approval.
Diagnosis of compensable occupational diseases
According to stipulations of the Administrative Rule of Occupational Disease Diagnosis issued by the MOPH, at the provincial and prefecture levels, compensable occupational diseases must be diagnosed by OHIs or by medical/health institutions licensed by the public health departments of local governments. In order to control the quality of diagnosis and to provide technical assistance for confirmation of complicated cases and adjudications of diagnostic disputes, expert committees on occupational disease diagnosis have been established at the national, provincial and prefecture/municipal levels (figure 3) (MOPH 1984).
Figure 3. The management of occupational disease diagnosis in China

The National Committee on Occupational Disease Diagnosis (NCODD) consists of five subcommittees concerned with occupational poisoning, pneumoconiosis, physical factor-induced occupational disease, radiation sickness and pneumoconiosis pathology, respectively. The headquarters of the Committee is in the Department of Inspection of the MOPH. The executive office of the NCODD is in the IOM/CAPM. All members of the Committee were appointed by the MOPH.
Diagnostic Criteria of occupational illnesses are promulgated by the MOPH. There are such criteria for 66 occupational diseases in effect right now. For other compensable occupational diseases without national diagnostic criteria, the provincial public health departments could formulate temporary diagnostic criteria to be put into effect in their own provinces after being submitted to the MOPH for the records.
According to the Diagnostic Criteria, the diagnosis of occupational disease must be based on the following sorts of evidence: a history of exposure, clinical symptoms and signs, laboratory findings and results of working environmental monitoring, and reasonable exclusion of other diseases. Once the diagnosis is made, an Occupational Disease Certification (ODC) must be issued by the OHI. Three copies of the ODC should be sent: one to the worker, one to the enterprise for proper compensation arrangements and one should be kept in the OHI for further medical treatment and working capacity evaluation.
Management of occupational disease patients
Compensation and other welfare for patients suffering from occupational diseases must be provided by the enterprises according to the Labour Insurance Regulations (LIR). The management, labour union and committee of working capacity evaluation in the enterprise must jointly take part in the discussion and decision on proper treatment and compensation for the patients based on the ODC and the degree of working capacity loss. For those who are proved to be not suitable for doing their original jobs after the completion of proper medical treatment, the enterprise should transfer them to other worksites or make proper employment arrangements according to their health conditions within two months, and for special cases, at the latest in six months. When a worker suffering from occupational disease moves to another enterprise, his or her occupational disease benefits should be borne by the original enterprise where the occupational disease was caused, or shared by both enterprises after they have come to an agreement. All the health records, the ODC and other information relating to the health care of the worker must be transferred to the new enterprise from the original one, and the transfer should be reported by both enterprises to their local OHIs for record-keeping and further follow-up purposes.
If the diagnosis of an occupational disease is made after the worker has moved to a new enterprise, all the compensation or benefits should be paid by the new enterprise where the worker is currently working, regardless of whether or not the affliction is connected with the present working conditions. For a contracted worker or temporarily employed worker, if the occupational disease is diagnosed during unemployed periods and there is evidence proving exposure to related hazardous working environments when he or she was hired by any enterprise, the compensation and medical care should be paid by the enterprise (MOPH 1987).
Achievements in Occupational Disease Prevention and Control
Improvement of working environments
The concentration or intensity of occupational hazards in the workplace has declined significantly. The statistics of working environmental monitoring as supplied from the NCOHR showed that the proportion of worksites in compliance with national standards has increased 15% from 1986 to 1993 (NCOHR 1994). This is particularly true for state-owned and urban collective-owned industrial enterprises, of whose working environments nearly 70% had met the national standards. The situation in rural industrial enterprises is also improving. The compliance rate for occupational hazards increased from 42.5% in 1986 to 54.8% in 1993 (table 4). It is important to note that the estimation of the compliance rates of township industries might be higher than the actual situation, because this routine report can cover only about 15% of the rural industries every year, and most of them are located near cities which have well-developed health service facilities.
Table 4. Results of environmental monitoring for hazards in the workplace
|
Year* |
State-owned industry |
Rural industry |
||
|
No. of environmental locales monitored |
Proportion of locales up to standards (%) |
No. of environmental locales monitored |
Proportion of locales up to standards (%) |
|
|
1986 |
417,395 |
51.40 |
53,798 |
42.50 |
|
1987 |
458,898 |
57.20 |
50,348 |
42.60 |
|
1988 |
566,465 |
55.40 |
68,739 |
38.50 |
|
1989 |
614,428 |
63.10 |
74,989 |
53.50 |
|
1990 |
606,519 |
66.40 |
75,398 |
50.30 |
|
1991 |
668,373 |
68.45 |
68,344 |
54.00 |
|
1992 |
646,452 |
69.50 |
89,462 |
54.90 |
|
1993 |
611,049 |
67.50 |
104,035 |
54.80 |
* Exclusive of data from 1988: Yunnan, Xinjiang; 1989: Tibet, Taiwan; 1990: Tibet, Taiwan; 1991: Tibet, Taiwan; 1992: Tibet, Taiwan; 1993: Neimeng, Tibet, Taiwan.
The prevalence of some serious occupational diseases andthe implementation of comprehensive preventive measures
The national occupational health report data indicated that the prevalence of compensable occupational diseases maintained itself at a rate of 0.4 to 0.6%, although industries developed very quickly in recent years. Silicosis, for example, has been controlled for years in some large state-owned industrial or mining enterprises. Tables 5 and 6illustrate the success of Yiao Gang Xian Tungsten Mine and Anshan Steel Company in controlling silicosis (Zhu 1990).
Table 5. Dust exposure and prevalences of silicosis in Yiao Gang Xian Tungsten Mine
|
Year |
Dust concentrations ( mg/m3 ) |
Detected rates of silicosis (%) |
|
1956 |
66 |
25.8 |
|
1960 |
3.5 |
18.6 |
|
1965 |
2.7 |
2.6 |
|
1970 |
5.1 |
0.3 |
|
1975 |
1.6 |
1.2 |
|
1980 |
0.7 |
2.1 |
|
1983 |
1.1 |
1.6 |
Table 6. Detection rate of silicosis in Anshan Steel Company
|
Year |
No. of examinations |
Cases |
Rate (%) |
Compliance rate of dust (%) |
|
1950s |
6,980 |
1,269 |
18.21 |
23.60 |
|
1960s |
48,929 |
1,454 |
2.97 |
29.70 |
|
1970s |
79,422 |
863 |
1.08 |
28.70 |
|
1980s |
33,786 |
420 |
1.24 |
64.10 |
The nationwide epidemiological survey of pneumoconiosis in 1987-90 has also shown that the average working time of patients from their first exposure to silica dust to the appearance of signs of pneumoconiosis had been significantly prolonged, from 9.54 years in the 1950s to 26.25 years in the 1980s for those with silicosis, and 16.24 years to 24.72 years for those with coal worker’s pneumoconiosis in the same period of time. The average age of patients suffering from silicosis at death had also been increased from 36.64 years to 60.64, and for patients with coal pneumoconiosis from 44.80 years to 61.43 years (MOPH 1992). These improvements could be partly attributed to the successful occupational health policies and interventions of governmental policies as well as to the great efforts of occupational health professionals.
Promoting occupational health programmes in small-scale industries
Facing the continuing rapid development of small-scale industries, especially of township industries, and the growing gap between occupational health services and practical needs, the Ministry of Public Health decided to conduct a further comprehensive intervention field study. This study is important not only for helping to solve occupational health problems in rural industries, but also for exploring approaches to reform the occupational health service system in state-owned enterprises in order to match the changing requirements of the market economic system that is being established. Therefore, in December 1992, the Expert Group for the Field Study of Occupational Health Service Policies for Small-scale Industries was set up in the Department of Health Inspection, Ministry of Public Health. The Group was formed to support provinces in developing occupational health service programmes and approaches to effective intervention in hazardous situations. As the first step, the Group has drafted a “Recommended National Field Study Program” for provincial governments, which was approved and issued by the MOPH in 1992. The primary strategy of the programme is described as follows:
The enterprise, the provider of occupational health and the local government are the three key parts of the programme. The programme focuses on readjusting the relationship among the three parts to establish a new model of development. The basic objectives of the programme are to strengthen the regulatory control of government, to change the attitudes to health and the behaviours of the productive and operation functions of enterprises and to enlarge the coverage of minimum occupational health service while improving working conditions with appropriate technological measures (figure 4). Four counties (or districts) have been selected by the MOPH as national trial areas prior to the nationwide implementation of the programme, which include the Zhangdian district in Zibo municipality, Shandong province; the Baoshan District in Shanghai municipality; Jinhua County in Zhejiang province; and the Yuhong District in Shenyang municipality, Liaoning province.
Figure 4. The strategy of the pilot study on OHS in township enterprises
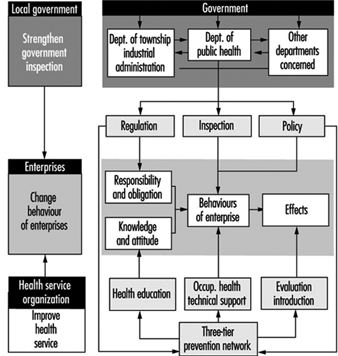
Seven spheres of policy interventions have been emphasized in the programme:
- strengthening the supervision and inspection provided by local governments of the occupational health of small-scale industries
- exploring how to integrate occupational health services for rural industries, with the goal “Health for All by the Year 2000” in China
- improving grass roots health organization networks to deliver occupational health services, management and supervision to the enterprises
- exploring practical approaches to enforce and implement occupational health inspection and service for township enterprises
- searching for and recommending appropriate technology for hazard control and personal protection for township enterprises
- implementing occupational health education programmes in township industries
- developing occupational health manpower and improving occupational health service working conditions to strengthen the occupational health service network, especially at the township and county levels.
Some preliminary results have been obtained in these four trial areas, and the basic ideas of the programme are being introduced to other areas in China and was scheduled for final evaluation in 1996.
The author thanks Prof. F. S. He for her assistance in reviewing this article.
Labour Protection in the Russian Federation: Law and Practice
The organization of labour protection that was inherited by the Russian Federation from previous times represented a hierarchical structure that had been built up under the former society and functioned under rigorous administrative control accompanied by planning and allocation of resources. Recent changes in the country’s economic and social systems caused by the transition to a market economy have necessitated both the revision of the existing labour legislation and the reorganization of the whole system of labour protection and particularly the provision of occupational health services to the working population.
Labour Legislation
Labour protection in Russia is recognized as a complex system for ensuring safe and healthy working conditions, which includes legal, socio-economic, organizational, preventive, safety, hygienic, technical and other measures.
Labour legislation in the Russian Federation comprises certain provisions of the Russian Constitution, the Labour Code, the Basic Law on Labour Protection, and enabling legislation, which consists of the relevant legal acts, regulations and directives, as well as guidelines, instructions, state standards and various standards approved by the appropriate authorities of the Russian Federation and those of the republics in the territory of Russia.
Article 37 of the Constitution of the Russian Federation stipulates that each citizen has the right to work in an environment that meets occupational safety and health requirements, to remuneration for work that is paid without any discrimination at a rate that is not less than the minimum established by the federal government, and to be protected from unemployment.
The Basic Law on Labour Protection, adopted in August 1993, contains provisions ensuring workers’ rights to protection of their health. It also regulates labour relations between employers and workers in all branches of the economy regardless of the forms of property. According to Article 4 of this Law, workers have the right to:
- safe and healthy working conditions
- workplaces that are protected against occupational hazards that may cause occupational accidents or diseases or decrease working capacity
- compensation for occupational injuries and occupational diseases
- information on existing occupational hazards and health risks and the measures undertaken by the employer to control them
- provision of personal protective equipment at the expense of the employer.
Article 9 of the Basic Law on Labour Protection makes management responsible for ensuring safe and healthy working conditions, while Article 16 specifies economic penalties for allowing unsafe and unhealthy working conditions, as well as for the impairment of workers’ health resulting from occupational exposures, injuries or diseases.
Chapter 10 of the Labour Code of the Russian Federation concerns occupational safety and health in industry. Article 139 stipulates the responsibility of management for the provision of safe and healthy working conditions through the introduction of up-to-date safety procedures and accident prevention measures that will ensure appropriate hazard control and the prevention of occupational accidents and diseases.
Article 143 of the Labour Code requires management to equip worksites with safe machinery and equipment and create safe working conditions in conformity with technical and hygienic standards as well as inter-industry and sectoral regulations on occupational safety and health that have been developed and adopted in accordance with the existing labour legislation.
The inter-industry occupational safety and health regulations cover all branches of industry. They consist of legal requirements applicable to all enterprises regardless of the types of their economic activity (e.g., hygienic norms SN 245-71 for the design of industrial enterprises). The inter-industry regulations are adopted by the Council of Ministries of the Russian Federation, or by other appropriate authorities if requested by the Council of Ministers.
The sectoral occupational safety and health regulations define requirements for diverse industrial processes, types of works and equipment specific for particular branches of industry (e.g., regulations on safety rules for welding operations in construction, or for the operation of loading cranes in dockworks). They take into account specific characteristics of particular branches of the economy and are adopted by respective ministries, state committees, state supervision bodies and other appropriate authorities.
Ministries also issue safety and health guidelines, instructions and technical standards for their respective fields of economic activities. Other instructions such as those that oblige employers to organize in-plant safety and health training for workers or those that oblige workers to comply with safety requirements are subject to consultations with employers’ and workers’ organizations.
Employers have the obligation to provide workers with proper clothing or uniforms and personal and collective protective equipment as specified by the regulations. They are also responsible for the organization of periodic health examinations for certain specific categories of workers, such as those doing heavy work or in hazardous occupations, transport workers and some others.
Along with the duties and responsibilities of the employers (when the state owns the property, the management of the enterprise represents the employer), labour legislation makes workers responsible for complying with the occupational safety and health requirements specified by relevant regulations and instructions. For example, they are required to participate in occupational safety and health training, properly maintain and use personal protective equipment, be trained in fire prevention, maintain the machinery and equipment they use and keep their workplaces clean.
At the enterprise level, everyday supervision of occupational safety and health standards and requirements is the responsibility of the occupational safety and health bureau, which is an integral unit of the enterprise, and enjoys an independent status. Its main functions include evaluation of occupational hazards, risk assessment, recommendation of safety and control measures, prevention of industrial accidents, analysis of the causes of occupational accidents, cooperation with other units of the enterprise in preventing work accidents and injuries, control of machinery and equipment and the implementation of safety programmes. The bureau has the authority to halt the operation of certain machinery or processes or the performance of jobs that may endanger workers’ life and health.
Small-scale enterprises are usually not in a position to organize an occupational safety and health bureau (see “Occupational health services in small-scale enterprises”). Article 8 of the Basic Law on Labour Protection gives them the right to consult external occupational safety and health specialists and to employ them on a contract basis.
In order to make the regulations covering the protection of workers in the Russian Federation more effective, there exists a system for establishing state standards on occupational safety and health (GOST). The state standards have the force of law and appropriate state authorities enforce their implementation.
In all, there are now more than 2,000 regulations, directives, instructions, hygienic norms and state standards on occupational safety and health, most of which had been developed by the various ministries, state committees and other authorities of the former USSR. These rules and regulations are still in effect, even though 700 had been established before 1981 and were intended to be applicable for a period of only five years. Most of them need reconsideration and modification in the light of the new economic situation.
As part of the reorganization of the system of labour protection in Russia, the Presidential Decree of 4 May 1994 created the Federal Labour Inspectorate (Rostrudinspekcija) under the Ministry of Labour and made it responsible for enforcing labour legislation in all territories of the Russian Federation. This established the system of state control and supervision in the field of labour protection. (Before this, the enforcement of labour legislation was the responsibility of trade union inspectors.) Regional Inspectorates with a networking structure are to be set up in all constituent regions of the Russian Federation to complete the organizational structure of the Federal Labour Inspectorate.
Health Legislation
Health legislation of the Russian Federation represents an instrument for the realization of the state policy on public health and epidemiological welfare. The Federal Hygienic and Epidemiological Service of the Russian Federation performs its activities in accordance with health legislation and plays an important role in activities aimed at the promotion of safety and health at work and public health in general.
Health legislation consists of the Hygienic and Epidemiological Welfare of the Population Act, adopted on 13 April 1992 by the Supreme Council of the Russian Federation, and of relevant directives and regulations adopted by respective competent authorities by virtue of this Act.
Article 1 of the Act defines the term hygienic and epidemiological welfare as “such a state of public health and the environment under which there is no hazardous influence of environmental factors on the health of the populations and there exist favourable conditions for creative activities.”
Health legislation establishes hygienic standards for enterprises, new types of machinery and equipment, and new technological processes and materials. It also stipulates the enforcement of existing norms and standards.
State hygienic supervision has two forms:
- Preventive hygienic supervision includes the enforcement of hygienic standards in the design, construction and reconstruction of enterprises, introduction of new technologies, manufacturing of machinery and equipment, and monitoring the environment.
- Routine hygienic supervision involves regular surveillance of the working environment of the enterprises using hygienic methods of exposure monitoring, sampling and analysis. It also includes control of the application of hygienic standards in the operation of machinery and equipment and the maintenance of the enterprise in general.
Article 9 of the Act requires enterprises to comply with health legislation by complying with established hygienic standards and by exercising control over their industrial environment. They are required to prevent environmental pollution and to develop and implement safety and health programmes that are aimed at the improvement of the working environment and the prevention of work accidents and injuries.
Chapter 4 of the Act determines the various degrees of liability for infringement of the Russian health legislation. Persons responsible for breaking the law may be prosecuted either under civil or criminal law (Article 27) of the Russian Federation.
Chapter 5 of the Act stipulates functions of the state hygienic and epidemiological supervision. It includes:
- assessment and prognosis of environmental health for the public
- identification of occurrences of communicable diseases, wide-spread non-communicable diseases and poisonings, and their causes
- development of mandatory measures to ensure hygienic and epidemiological welfare of the population
- supervision of the compliance of enterprises with health legislation and hygienic standards
- prosecution of organizations and persons for non-compliance with health legislation and hygienic standards
- compiling statistics on communicable diseases, occupational diseases, widespread non-communicable diseases and poisonings resulting from adverse environmental factors.
As a result of the structural changes taking place in employment patterns, the Act, for the first time, places obligation for the observance of health legislation, hygienic standards, hygienic quality of products and the prevention of environmental pollution not only on management and workers but also on self-employed persons who are involved in full-time employment (Article 34).
According to Article 32 of the Act, the Federal Hygienic and Epidemiological Service of the Russian Federation is assigned responsibility for enforcement of the health legislation. In addition, the Council of Ministers of the Russian Federation approved Directive No. 375, which reorganized the former hygienic and epidemiological stations into Centres for State Hygienic and Epidemiological Supervision (CSHES), operating in all territories of the Russian Federation.
The new health legislation is a crucial development in the legal regulation of the hygienic and epidemiological welfare of the population, as is the radical restructuring of the Federal Hygienic and Epidemiological Service of the Russian Federation to implement it. The Service has recently received the status of a Federal Service and is now included in the federal bodies of state control. As a result, the Federal Committee of the Russian Federation for Hygienic and Epidemiological Supervision has been established to provide overall supervision of this Service.
The Federal Hygienic and Epidemiological Service of the Russian Federation is made up of the following bodies:
- The Federal Committee of the Russian Federation for Hygienic and Epidemiological Supervision
- Centres for State Hygienic and Epidemiological Supervision (CSHES) at the republic, regional, municipal, district and local levels
- linear CSHES in water and air transport
- Information and Analytical Centre of the Russian Federation
- medical institutes and specialized training centres for the education and training of specialists to staff the CSHES
- research institutes specializing in occupational hygiene and epidemiology
- specialized medical establishments producing vaccines
- disinfection centres.
As defined in Directive No. 375, the main functions of the Federal Hygienic and Epidemiological Service include:
- enforcement of health legislation
- development of hygienic norms and standards
- elaboration of federal, republic, regional and local programmes for health protection and health promotion
- provision of technical information to appropriate authorities, enterprises, employers’ and workers’ organizations and other institutions involved in occupational safety and health activities, including information about hygienic and epidemiological conditions in the country, statistics on population morbidity and interpretation of legal documents relating to health legislation
- coordination of the activities of enterprises, employers’ and workers’ organizations, scientific associations and other institutions and organizations with respect to both the development and implementation of hygienic standards.
CSHES specialists have the right to visit and inspect enterprises in order to enforce health legislation. They investigate causes of occupational diseases and identify potential environmental and occupational hazards that may give rise to work-related diseases, injuries and poisonings. Ideally, where necessary, they cooperate with the occupational physicians and nurses staffing the occupational health services.
CSHES funds are provided directly from the federal budget of the Russian Federation. In addition, the CSHES may provide specialized services and advice under contract to enterprises and any others who may need their expertise. The list of specialized services provided by CSHES is approved by the Federal Committee for Hygienic and Epidemiological Supervision.
Health legislation is enforced through the application of relevant directives, regulations, instructions, norms and standards and legal requirements. These include:
- hygienic regulations, hygienic standards and requirements intended to create safe and healthy working conditions, protect the environment and promote public health in general
- hygienic standards establishing occupational exposure limits and maximum permissible levels for potential hazards encountered in workplaces and the environment
- hygienic norms establishing criteria for specific factors that may affect the health of future generations
- uniform hygienic regulations that combine different norms and standards.
Protection of workers’ health
Article 41 of the Constitution of the Russian Federation states that each citizen has the right to health protection and medical care. New legal acts provide for the development of municipal and private health care systems to supplement the state health care system. Health care in the state and municipal medical settings is provided without charge to patients, the costs being met by federal and local budgetary funds, health insurance funds and other sources.
The Hygienic and Epidemiological Welfare of the Population Act includes the following provisions aimed at the protection of workers’ health:
- Workers at enterprises shall undergo pre-placement and periodic health examinations.
- Pre-placement and periodic health examinations shall be required for all workers exposed to specific occupational hazards and hazardous types of work included in a list approved by the Federal Committee for Hygienic and Epidemiological Supervision and the Ministry of Health of the Russian Federation in consultation with representative organizations of employers and workers.
- Enterprises shall undertake all necessary measures to provide health examinations for workers.
A feature of the country’s health care system is the introduction, in 1991, of compulsory health insurance, which was amended in 1993. The Health Insurance of the Citizens of the Russian Federation Law encompasses a new insurance model under which employers contribute premiums amounting to 3.6% of their total payrolls to local administrations to meet health insurance needs. In 1996, about 40 million workers were covered by the Federal Compulsory Health Insurance Fund of the Russian Federation.
The main aim of the introduction of the compulsory health insurance was to ensure the financing of health care in the post-Soviet economic system based on insurance principles, using funds contributed through compulsory and voluntary dues. Compulsory health insurance introduced two types of public relationships into the health care system of the Russian Federation that had not existed before: the involvement of insurers, represented by local authorities that are responsible for the health insurance covering public employees and the unemployed; and the involvement of industrial insurers represented by the employers and enterprises that are responsible for the coverage of workers. According to Article 23, Health and Epidemiological Welfare of the Population Act health examinations of workers are included in the list of services covered by the compulsory health insurance.
In accordance with the Basic Law on the Health Protection of the Citizens of the Russian Federation, adopted by the Supreme Council of the Russian Federation on 22 July 1993, the basic principles of health protection are:
- observance of human rights in the field of health protection that are guaranteed by the government
- priority of prevention in health protection
- universal access to social and medical care
- social protection of workers in case of disability
- responsibility of the state, appropriate authorities, enterprises regardless of their forms of property, and the management of institutions and organizations for the protection and promotion of workers’ health.
The Basic Law specifies the relationships with respect to health protection and health promotion between the working population and the appropriate authorities, state enterprises, private sector establishments, and the state, municipal and private medical settings providing health care services.
In practice, occupational health services are provided to workers by public health care settings (hospitals and polyclinics) that are located near their residences, and by the specialized occupational health services located for the most part in large enterprises. The objective of this arrangement is to bring qualified health care services as close as possible to the workers and their workplaces.
Occupational health services are normally organized at large enterprises employing over 4,000 workers and in chemical, petrochemical, mining and quarrying industries with over 2,000 employees. An in-plant unit staffed by an occupational physician and an occupational nurse is required for all enterprises with more than 800 workers; those with 300 to 800 workers are required to have only an occupational nurse; the minimal number for enterprises with chemical, petrochemical, mining and quarrying operations is 200 employees. These in-plant units are part of the public health care system.
Small-scale enterprises rely for occupational health services on the hospitals and polyclinics of the public health care system, which are expected to provide an occupational physician to perform the health examinations of workers.
The occupational health service at very large enterprises usually includes a hospital providing inpatient services, a polyclinic providing outpatient services, occupational nursing services and a dispensary. Its services may be “closed” (i.e., limited to individuals working in the enterprise), or “open” (i.e., also providing services to workers’ families and, sometimes, to individuals living in the neighbourhood of the plant).
Conclusions
Significant transformations in Russia’s economic and social systems reflect the transition to a market economy, the appearance of various forms of property, the granting of economic independence to enterprises and the abolition of state administrative control, all of which have resulted in a great many changes in the society.
The system of labour protection in the Russian Federation described above, while preserving its general features, is still undergoing major reorganization to conform with changing realities and to be able to respond effectively to emerging issues. Although well under way, this process is also just beginning.
The provision of occupational health services to the working populations needs special attention because of the partial disintegration of the old network of occupational health services resulting from well-known economic problems, and also because of such innovations as the appearance of a private sector, the introduction of compulsory health insurance, and the integration of private medical settings into the country’s health care system.
Although some progress has been made in reducing the numbers of work accidents and the incidence of occupational injuries and diseases, the rates remain unacceptably high, which may have serious consequences in terms of the deterioration of workers’ health and its resultant impact on the economy. The improvement of working conditions and the working environment and the protection and promotion of workers’ health consequently command a high priority in revising the social policy of the state. Active participation of knowledgeable occupational safety and health professionals in this process is critical.
Some prerequisites for the improvement of the system of labour protection in Russia include:
- creation of economic stimuli for the improvement of working conditions and the working environment
- formulation of a coherent national policy on occupational health, occupational safety and the working environment
- revision of existing labour legislation and the establishment of a solid legislative basis for occupational safety and health practice
- effective enforcement of labour legislation
- wider cooperation of employers and workers on matters related to occupational safety and health
- authorizing state control bodies to close down enterprises with unsafe and unhealthy working conditions, as well as those polluting the environment
- emphasizing the improvement of working environment together with the protection of the general environment
- detailed analysis and prognosis of possible effects of the design and construction of new enterprises on workers’ health and the environment
- providing more options for workers in the procurement of occupational health services and increasing professional independence of occupational health professionals
- providing access to a “standard” package of health care services for all workers
- establishing comprehensive, multidisciplinary occupational health services at large-scale enterprises that are capable of providing a full range of services, including treatment and rehabilitation, to workers and their families
- upgrading the technical facilities of occupational health services and CSHES and enhancing the levels of the expertise of their staff
- organizing and deploying health centres to provide occupational health services for small-scale enterprises
- providing recommended types of health examinations to all workers, including workers in agriculture and the informal sector, through the most efficient use of various medical settings
- upgrading the education and training of occupational health professionals
- emphasizing workers’ education and training in occupational safety and health.
Occupational Health Services in Japan
Policy and Legislation
In Japan, the sole administrative body of occupational health is the Ministry of Labour, and the core law is the Industrial Safety and Health Law enacted in 1972 (this law will be termed “the Health Law” for the purposes of this article). The Health Law and its enforcement orders specify the employer’s responsibility to provide occupational safety and health services, including the appointment of an occupational health physician (OP), according to the size of the workplace. It is a requirement that all workplaces employing 50 or more workers appoint an OP (a full-time OP for workplaces that employ 1,000 or more workers). In addition, all workplaces, regardless of employee number, are mandated to provide health examinations for their workers. The mandatory health examinations include pre-employment and periodic general health examinations for full-time workers and specific health examinations for full-time workers engaged in activity described as “harmful work”. Compliance with the above legal requirements is generally good, although a gradient in compliance rate exists according to workplace size.
Organization and Service Provision Models
Organization and service provision models vary considerably according to the size of the workplace. Large-scale workplaces often embody full-size occupational health units, such as a health administration department, a department of health promotion or a clinic/hospital on the premises. These functional units may take the form of independent institutions, especially if they emphasize curative activities, but many are units subordinate to departments such as the labour department or the general affairs department. In some cases, the occupational health unit is run by a corporate health insurance union. The full-time OP is very often appointed to a directorial position of the unit, sometimes nominally matching a managerial post within the corporate hierarchy. The co-medical staff may consist of a variable combination of general nurses, occupational health nurses and x-ray and/or medical technologists.
In contrast, many small-scale workplaces lack the human and facility resources to carry out occupational health functions. In this sector, part-time OPs are recruited from among private general practitioners, hospital- or university-affiliated physicians and independent or non-independent occupational health practitioners. The part-time OPs engage in a variable range of occupational health activities depending on the needs of the workplace and the physician’s expertise. An occupational health organization (OHO), which is defined as an organization delivering occupational health services on a profit-earning basis, have played an essential role in the provision of occupational health services to small-scale workplaces. Services purchasable from OHOs cover provision and follow-up of various health examinations, implementation of environmental measurements and even the dispatch of OPs and nurses. Many small-scale workplaces appoint a part-time OP and contract with an OHO to meet specific legal requirements imposed on the workplace.
Activities and Content
Nationwide questionnaire surveys focusing on the activities of full-time and part-time OPs have been conducted periodically by the Occupational Health Promotion Foundation, an auxiliary non-profit-making organization of the Ministry of Labour. According to the 1991 survey, to which 620 full-time OPs responded, average time allocation was longest for curative activities (495 hours/year) followed by periodic health examinations (136) and health consultations (107). Time allocation to workplace patrols averaged 26.5 hours/year. In the survey, 340 part-time OPs also responded; the average time allocated by part-time OPs was proportionately less than that of full-time OPs. However, a detailed observation reveals that the activities of part-time OPs vary widely in quantity and quality, depending on several inter-related factors:
- size and characteristics of the workplace
- main job and other appointments of the physician
- work commitment.
Personnel Resources
There are no legal provisions on the qualifications of the OP: simply stated, the OP (whether full-time or part-time) can be appointed “from among physicians” (the Health Law). As of 1995, the total number of physicians is estimated to be 225,000, with an annual increase of about 5,000 (i.e., an increase of 7,000 qualifying from graduates of 80 medical schools in Japan and a decrease of 2,000 due to death). The estimated number of OPs as of 1991 was about 34,000 (2,000 full-time and 32,000 part-time), which was equivalent to 16.6% of the total number of physicians (205,000). In addition, an estimated several thousand nurses across the nation play an active part in the field of occupational health, although there is no legal definition of an occupational health nurse. A health supervisor, which is defined by the Health Law as a person who takes charge of technical matters related to health, is recruited from among the workers. The OP interacts closely with the health supervisor, to whom the OP may “give guidance or advice” under the Health Law.
Administration
Within the Ministry of Labour, occupational health is administered directly by the Industrial Safety and Health Department, which is subordinate to the Labour Standards Bureau. The Bureau’s functional units at the local level include the Prefectural Labour Standards Offices (of which there are 47) and the Labour Standards Inspection Offices (there are 347 of these) distributed nationwide and staffed by a total of about 3,200 “Labour Standards Inspectors”, 390 “Industrial Safety Expert Officers” and 300 “Industrial Health Expert Officers”.
The Ministry of Labour has been implementing consecutive five-year plans for the prevention of industrial accidents; the most recent of these (the eighth) was associated with the slogan “realizing a healthier and safer working life on both mental and physical aspects”. Accordingly, the Ministry is pursuing a Total Health Promotion (THP) plan. Under the THP plan, the OP prescribes an exercise menu for each worker based on health measurement data. Training programmes accommodating company representatives are organized by the government to develop necessary skills. The government also gives recognition to OHOs that are capable of providing services related to THP implementation.
Financing Systems
When occupational health services are provided on the premises, as is the case in large-scale workplaces, they will often take the form of an intracorporate department and will thus be placed under the financial constraints of the employer. Another variation involves the presence of an affiliated but self-supporting unit (clinic, hospital or OHO) which employs an occupational health staff. In some cases, the unit is run by a corporate health insurance union. Many small-scale workplaces, lacking the human, facility and financial resources, but under the requirement to appoint a part-time OP, will often do so by contracting with general practitioners, hospital- or university-affiliated physicians and others. As stated previously, the part-time OP will engage in a variable range of occupational health activities depending on the needs of the workplace and the physician’s expertise. The requirements imposed on the workplace, such as provision of periodic health examinations to all employees, often exceed the time capacity and/or the willingness of the contracted physician. This creates a demand-supply gap which is often filled by OHOs.
Research
The Japan Society for Occupational Health (JSOH) is an academic society comprising OPs, occupational health nurses and researchers. Its present membership exceeds 6,000 and is increasing at a rapid rate. The JSOH holds annual scientific meetings at national and regional levels and recently started publishing an English scientific periodical entitled Journal of Occupational Health. Some core research institutes are the National Institute of Industrial Health (periodical: Industrial Health, biannual, English), the Institute for Science of Labour (periodical: Journal of Science of Labour, monthly, Japanese and English), the Japan Industrial Safety and Health Association (publications: Industrial Safety Yearbook and so on) and the Institute of the Industrial Ecological Sciences of the University of Occupational and Environmental Health, Japan (periodical: Journal of UOEH, bimonthly, Japanese and English).
Future Developments
The Ministry of Labour recently launched a comprehensive plan aimed at disease prevention and health promotion for the nation’s workers. It plans to establish government-subsidized occupational health centres (OHCs) at prefectural and regional levels throughout the country within an eight-year plan. Prefectural OHCs are planned to be established for each of the 47 prefectures, and each will be staffed by about 15 personnel, including one administrative full-time physician and three or four part-time physicians. Their primary function will be the provision of training and dissemination of information to OPs working within the vicinity. Regional OHCs are planned for 347 sites nationwide in affiliation with the local divisions of the Japan Medical Association (JMA). They will focus on providing occupational health services to the under-served sector, that is, workers in small-scale industries. The initial budget for the fiscal year 1993 was 2.3 billion yen ($US20 million) for the establishment of six prefectural and 50 regional OHCs. The prefectural and regional OHCs will function interactively as well as with the administration, the JMA, the workers’ hospitals and so on. Collaboration between these various institutions will be the key to the success of this plan.
Academic-Based Occupational Health Services in the United States
During the 1980s and 1990s, academic occupational and environmental medicine clinics have emerged as a small, yet important source of occupational health services in the United States. These clinics are affiliated with academic medical centres, schools of medicine or schools of public health. The physician staff is composed primarily of faculty members of the academic programmes with principal teaching and research interests in occupational medicine. The main activity of these clinics is to provide diagnostic medical evaluations of potential occupational and environmental diseases, although many clinics also provide routine occupational health services. These clinics play an important role in occupational health in the United States by serving as an independent source of medical expertise on occupational diseases. The clinics are also major training sites for specialists in occupational medicine and recently for primary care physicians.
The Setting
Independent sources of medical expertise on occupational diseases are needed in the United States because employers are legally responsible for providing medical care and lost wages only if it can be demonstrated that an injury or illness is related to work. As noted in previous articles of this chapter, the vast majority of medical care for injured workers is provided by employers either directly by the employer or indirectly through contracts with private physicians, clinics, immediate care facilities and hospital-based programmes. This system of care is quite adequate for workers with acute injuries or diseases because the role of work in causing these conditions is clear. Therefore, it is in the employer’s interest to provide timely and effective medical treatment so that the employee returns to work as quickly as possible. However, the workers’ compensation systems in the United States do not function well for workers with chronic injuries and occupational diseases because employers are not required to pay for medical care unless it can be proved that the worker’s job was responsible for the condition. If an employer contests a compensation claim, the employee or workers’ compensation officials must seek an independent evaluation to determine whether the condition is work-related. Academic medical clinics have served as regional consultation programmes to provide this independent source of medical expertise.
Academic occupational medicine clinics have been able to maintain an independent perspective because few of them depend on employer contracts or similar financial incentives which could represent a conflict of interest in evaluating workers’ illnesses. These clinics typically operate as non-profit-making programmes that absorb some of the cost of medical evaluations as part of their teaching and service mission, since complex diagnostic evaluations are rarely cost-effective to undertake without employer support.
The growth of academic-based occupational and environmental medicine clinics has also come about as a consequence of the growth of academic occupational and environmental medicine programmes in schools of medicine and academic medical centres. Until recently, there was a small number of occupational health programmes in the United States, and virtually all of these were based in schools of public health, emphasizing disciplines such as industrial hygiene, toxicology and epidemiology. The number of academic occupational and environmental medicine programmes in schools of medicine increased substantially during the 1980s and 1990s.
This growth occurred for several reasons. The Occupational Safety and Health Act passed in 1970 created the National Institute for Occupational Safety and Health (NIOSH), which implemented a grant programme to support occupational medicine residency training. Many programmes were developed in schools of medicine and were able to provide residency training with the aid of NIOSH grant support. Another reason for the growth of residency programmes is that the professional accreditation organization for occupational medicine in the United States aimed to increase the field’s stature by making completion of a formal training programme (rather than only experience working in the field), a requirement for certification as an occupational medicine specialist. Residency programmes were also established in response to reports by prestigious professional organizations, such as the Institute of Medicine (IOM), documenting the severe shortage of qualified medical practitioners in the field of occupational and environmental medicine (IOM 1993). Many of the new residency programmes established clinics as training sites for the residency programmes. A large proportion of future specialists in the United States will receive their clinical training in the academic-based occupational and environmental medicine clinics.
Organizational Support for the Clinics
The academic-based clinics typically do not provide profitable, routine employee health services like those of the contract providers, so that institutional support has been essential in sustaining these programmes. Several governmental agencies have played an important role in supporting the clinics. As mentioned above, NIOSH has provided support for occupational medicine residency programmes; this support was supplied through the interdisciplinary Educational Resource Centre training consortiums and later through occupational medicine residency training grants. The National Institute for Environmental Health Sciences (NIEHS) has provided research and training support for academic occupational medicine programmes. Many of the most well-established clinics are affiliated with environmental health research centres supported by NIEHS. The clinics support the mission of the centres by identifying populations for clinical and epidemiological research. NIEHS also established the Environmental and Occupational Medicine Academic Award grant programme in the late 1980s to provide support to medical schools for faculty development in the field. This grant programme has now provided support to faculty in a substantial proportion of medical schools with academic-based clinics. The Agency for Toxic Substances and Disease Registry (ATSDR) which was established by the Comprehensive Environmental Response, Compensation, and Liability Act (Superfund) in 1980 to perform environmental health assessments and enhance professional training for evaluating hazardous substances has given essential support for programme development and related professional educational activities as many of the clinics have begun to address environmental as well as occupational health issues.
Several states have programmes to support occupational health services. The largest programme is the University of California Centres for Occupational and Environmental Health. These centres were established in five University campuses and include multidisciplinary research, training and clinical service programmes. Several other states (e.g., New Jersey, Oregon, Michigan and Washington) also support programmes through state schools of medicine or schools of public health. New York State created a statewide network of occupational and environmental health clinics, most of which are affiliated with academic medical centres. This network of clinics is able to evaluate persons with potential environmental or occupational medical problems even if they are not able to pay for these services. The clinics developed a common database system so that the network can serve as an occupational disease surveillance system for the state.
Professional associations have also provided critical support for the growth of academic clinics. Members of the American Public Health Association (APHA) provided an early focus for communication among the emerging clinics. The support of the APHA served to strengthen the public health and prevention orientation of the clinics. In 1987, members of the APHA occupational medicine clinic committee formed a new organization, the Association of Occupational and Environmental Clinics (AOEC), as a “network of clinical facilities dedicated to research and education, as well as the prevention and treatment of occupational and environmental diseases” (AOEC 1995). The AOEC has developed into a national network of more than 50 clinics, most of which are academic-based clinics. Most of the well-established academic-based clinics are members of the AOEC. The Association enhances communication among the clinics, establishes guidelines for quality of care and patient’s rights, seeks funding support for professional and educational activities and is developing a database system so that information from clinics can be systematically collected and analysed.
Programme Characteristics
As mentioned above, the clinics’ principal activity is to identify work-related and environmental diseases, rather than to provide routine employee health services. Because of this focus, the clinics are different from clinical programmes which provide employer-contracted services (Rosenstock 1982). Professionals in the academic clinics relate to potentially affected workers and community members as their primary clients, rather than the employers. The physicians participate in the medical, social, economic and legal aspects of patient problems. The patient-to-provider ratio is low: the clinics, focusing on relatively low-volume but complex medical cases call for longer and more thorough visits that engage the efforts of physician and patient beyond normal clinic hours.
Because of research and teaching responsibilities, the academic clinics usually are part-time, offering up to several sessions per week. A directory of 41 academic clinic members of the AOEC reported a range of one to 13 physicians per clinic, with 85% of the clinics having two to six physicians (AOEC 1995). Another characteristic is that the clinics use multidisciplinary teams of professionals to improve exposure and toxicity evaluation and to provide prevention and education services. For example, of 41 academic clinics in an AOEC directory, most had industrial hygienists (32), while approximately one-half had toxicologists (22), social workers (19) health educators (19) and epidemiologists (24) on the professional staff (AOEC 1995).
The clinics emphasize a community-oriented service perspective. Most clinics establish professional and community outreach programmes, both to establish a referral network for identifying patients and to provide education to health professionals, workers and community residents. Many clinics establish a worker and community advisory committee in order to provide oversight of clinic activities.
Many clinics maintain computer databases so that the experiences of the clinics can be retrieved and analysed. The databases include patient referral source, occupation and industry code of all jobs (or at least current and/or most important jobs), employer name, exposures, work-related diagnoses, assessment of link between exposures and diagnoses, and demographics (Rosenstock, Daniell and Barnhart 1992). So far data collected by the clinics has not been well coordinated, but the AOEC has developed a common database system so this information should be collected more systematically in the future.
Services
The mix of patients seen in academic clinics varies depending on types of employers and community hazards in the region, even more so than among the contract occupational services, which tend to develop in response to employer needs. The clinics may offer specialized diagnostic services depending on the expertise and research interests of the faculty. Patients may go to the clinics based on the expertise and reputation of the academic programme. A patient will usually present with either an actual disease, wanting to know if his or her job or an environmental exposure was responsible, or with a history of a potentially toxic exposure, wanting to know if adverse consequences will result from the exposure.
The most common occupational diagnoses seen in the clinics, as reported in a recent AOEC directory, were as follows (AOEC 1995): asthma, asbestos-related pulmonary diseases and other pulmonary conditions; carpal tunnel syndrome, repetitive strain, musculoskeletal conditions; and dermatological conditions. Few clinics reported neurological problems as a common diagnosis, and very few saw patients with acute injuries. The most common occupational exposure problems reported involved asbestos, lead or other heavy metals, chemicals and solvents.
The distribution of common environmental diagnoses was different from that typifying occupational problems. The most commonly reported diagnoses were determinations of multiple chemical sensitivity syndrome and “sick building syndrome”, or symptoms due to indoor air quality problems. The most common environmental exposure problems reported involved pesticides, lead, chemicals and hazardous waste in communities.
Patients are referred from a variety of sources—they may be self-referred or have been sent by employers, unions, public health agencies, physicians, lawyers and the workers’ compensation systems. Some referrals are made to the programmes because patients want an independent, high-quality medical assessment. Other referrals concern specific practitioners—often faculty members—who have recognized expertise. Choices leading to these latter referrals may be the outcome of a search that is national or even international in scope.
Academic clinics offer services in addition to evaluation of occupational and environmental diseases. Many clinics perform medical screenings for workers at the request of employers, unions or groups of workers who are concerned about a certain exposure, such as lead or asbestos. The clinics also provide medical surveillance examinations mandated by OSHA or state laws. Most clinics serve as regional resources by providing clinical consultations to workers, community residents and physicians, typically via telephone.
In addition to clinical services, the multidisciplinary staff of the academic clinics provide workplace and community hazard evaluations, sometimes including exposure monitoring. Virtually all of the clinics offer health education and prevention training for individuals, communities and health professionals.
The Future
The future of academic clinics in the United States may be affected by overall changes in the workers’ compensation and medical care systems. The need for independent medical evaluations of occupational and environmental problems will continue, but many states have implemented or are considering changes in workers’ compensation laws to restrict the freedom of workers independently to make their own choices regarding a medical evaluation. There is also a trend to integrate medical care for occupational and non-occupational conditions by a single managed care provider. The clinics will need to respond to the growth of managed care in the occupational health field because the independent approach used by these clinics may be largely excluded from a more managed workers’ compensation system.
To respond to these changes in the medical care system, some academic clinics are establishing affiliations with employer contracted programmes so that the clinics function as a speciality referral programme while the other programmes handle routine cases and medical treatment. Academic clinics may also need to establish affiliations with medical centres supplying primary care, urgent care, rehabilitation services and other specialities in order to lend greater comprehensiveness to the services that will be integrally provided by occupational health care and other medical care. This approach will be taken to increase financial stability through the use of contracts in addition to charging fees for service, and to provide training experiences for physicians, many of whom will practise in those settings.
The challenge for academic clinics will be to maintain their independent perspective while functioning in an integrated, managed care system largely financed by employers. The option of independent consultations will be maintained to some degree because of the regional and national referral patterns based on a clinic’s reputation. Clinical practitioners will also continue to provide expert consultations to individuals and lawyers under the tort system, which is also evolving in the United States, albeit more slowly than is the medical care system. However, even with these sources of support, academic clinics in the United States will continue to need support from governmental agencies and professional organizations to continue their role as independent sources of medical consultation, research and training. The future of many of the academic clinics will depend on whether the federal and state governments continue to support these programmes.
Labour Union-Based Activities in the United States
In 1995, the US Department of Labor, Bureau of Labor Statistics, published a report indicating that 18.8 million workers, or approximately 16% of the United States workforce, are either union members or workers who report no union affiliation but are covered by a union contract (US Department of Labor 1995). Table 1 draws upon this report to characterize the unionized workforce by industry. Most of these workers are represented by labour unions affiliated with the American Federation of Labour and Congress of Industrial Organizations (AFL-CIO), which comprises 86 national and international unions (Statistical Abstract of the United States 1994). Labour unions are typically organized into international or national headquarters, regional and district offices and local unions.
Table 1. 1994 distribution of the US unionized workforce according to industry
|
Occupation |
Total employed |
Members of unions* |
Represented by unions** |
||
|
Employed |
Total (%) |
Employed |
Total (%) |
||
|
Agricultural wage |
1,487 |
34 |
2.3 |
42 |
2.8 |
|
Private nonagricultural wage and salary workers |
88,163 |
9,620 |
10.9 |
10,612 |
12 |
|
Mining |
652 |
102 |
15.7 |
111 |
17.1 |
|
Construction |
4,866 |
916 |
18.8 |
966 |
19.9 |
|
Manufacturing |
19,267 |
3,514 |
18.2 |
3,787 |
19.7 |
|
Durable goods |
11,285 |
2,153 |
19.1 |
2,327 |
20.6 |
|
Nondurable goods |
7,983 |
1,361 |
17 |
1,460 |
18.3 |
|
Transportation and public utilities |
6,512 |
1,848 |
28.4 |
1,997 |
30.7 |
|
Transportation |
3,925 |
1,090 |
27.8 |
1,152 |
29.3 |
|
Communications and public utilities |
2,587 |
758 |
29.3 |
846 |
32.7 |
|
Wholesale and retail trade |
22,319 |
1,379 |
6.2 |
1,524 |
6.8 |
|
Wholesale trade |
3,991 |
260 |
6.5 |
289 |
7.2 |
|
Retail trade |
18,328 |
1,120 |
6.1 |
1,236 |
6.7 |
|
Finance, insurance and real estate |
6,897 |
156 |
2.3 |
215 |
3.1 |
|
Services |
27,649 |
1,704 |
6.2 |
2,012 |
7.3 |
|
Government workers |
18,339 |
7,094 |
38.7 |
8,195 |
44.7 |
* Data refer to members of a labour union or an employee association similar to a union.
** Data refer to members of a labour union or an employee association similar to a union, as well as to workers who report no union affiliation but whose jobs are covered by a union or an employee association contract.
Note: Data refer to the sole or principal job of full- or part-time workers. Excluded are self-employed workers whose businesses are incorporated although they technically qualify as wage and salary workers. Data for 1994 are not directly comparable with data for 1993 and earlier years. For additional information, see “Revisions in the current population survey effective January 1994”, in the February 1994 issue of Employment and Earnings.
Labour unions provide comprehensive safety and health services to workers who are members of unions. Through the development of collective bargaining agreements and by providing technical and related services, unions address the needs and concerns of their members.
On the national and international levels, union officers and staff members (safety and health professionals, attorneys, lobbyists and others) work to influence elected officials to pass safety and health laws and rules which protect workers. Union representatives also develop and negotiate collective bargaining agreements with employers containing legally binding safety and health contract language.
Labour unions ensure that workers have safe, healthful work environments through collective bargaining agreements. Ideally these agreements also provide workers with a means of addressing safety and health issues or of resolving safety and health disputes that may arise at the workplace.
Technical Assistance
At the central office, labour unions often employ or contract professional industrial hygienists, ergonomists, occupational physicians, engineers and other safety and health professionals to furnish technical assistance to workers. These professionals provide such services as conducting complaint investigations; carrying out job-site safety and health evaluations; and interpreting and translating environmental monitoring data, medical results and other technical information into language understandable by the average worker.
Safety and health complaint investigations are routinely conducted by labour union professional staff or consultants. Working in conjunction with designated employee representatives from the affected local union, these professionals address issues such as workers’ exposure to chemical or physical hazards, musculoskeletal illnesses and injuries, and non-compliance with applicable safety and health regulations.
In addition, unions may become involved in accident investigations in situations where the employer’s investigation results are disputed by the affected employees.
Labour union representatives may use the information obtained during such investigations to resolve safety and health complaints by working with the employer through the collective bargaining process. Unions may utilize the grievance procedure or specific safety and health contract language to protect workers. However, the union may elect to contact a federal or state regulatory agency if the employer is not in compliance with established laws, rules or regulations.
Union-based safety and health professionals and/or trained designated union workplace representatives—for example, local union safety and health committee members or shop stewards —conduct job-site surveys to evaluate the work environment for hazards.
During the surveys, the manufacturing processes or other operations within the job-site are evaluated. Safety and health records (for instance, OSHA 200 Logs, Department of Transportation (DOT) Accident Reports, environmental monitoring results and written programmes) are reviewed to determine compliance with collective bargaining agreements and governmental standards and regulations. The results of the surveys are documented and any problems are resolved through collective bargaining or by contacting a governmental regulatory agency.
Workers themselves often request technical or regulatory information and reports—for example, chemical fact sheets, environmental monitoring results, biological monitoring results, or federal or state safety and health regulations. Because of the technical nature of this information, the worker may require assistance in understanding the subject matter and how it applies to his or her workplace. Union-based safety and health staff can provide the workers with assistance in understanding technical information. The manner in which the assistance is provided is dependent upon the needs of the worker.
Labour unions also serve as a clearinghouse for specialized medical care or assistance for use in workers’ compensation hearings. Unions typically maintain lists of the names and addresses of reputable independent physicians to whom the worker may be referred, if necessary.
Legislative and Rulemaking Activities
Active involvement in safety and health governmental rulemaking is a very important concern of labour unions; they encourage their members to become involved in legislative and safety and health rulemaking activities on varying levels.
Unions seek to influence politicians to propose legislation to establish adequate workplace safety and health standards; to respond to proposed safety and health rulemaking submitted by governmental regulatory agencies; to influence the manner in which governmental regulatory agencies enforce workplace safety and health regulations; or to organize support for governmental regulatory agencies subject to budgetary reductions or operational changes by the US Congress.
Union lobbyists, technical professionals, research workers and legal staff members are the primary personnel involved in these activities. These staff members are responsible for collecting, analysing and organizing the data necessary to develop a union position on legislative or rulemaking activities. They also make the necessary contacts with agencies or individuals to ensure that the union’s position is presented to elected officials.
Union safety and health staff members may encounter a safety and health issue that affects workers but is not regulated by a governmental agency. In this instance, the union may develop written comments and/or oral testimony to be presented during public hearings. The intent of the comments or testimony is to educate the relevant officials and encourage them to draft legislation to resolve the issue.
Agencies that enforce safety and health regulations are, on occasion, targeted for budget reductions. Often these budget cuts are seen as being adverse to the protection of the safety and health of workers on the job. Labour unions develop and implement strategies to prevent such reductions. This may be done by working with union lobbyists to educate legislative and other officials on the adverse effects that the reductions will have on workers. In addition, there are “grassroots efforts” that include organizing and mobilizing workers to write letters to their elected officials highlighting their opposition to the proposed cuts.
In addition, unions are very involved in preparing and delivering written comments and oral testimony in response to proposed safety and health rulemaking promulgated by federal and state regulatory agencies. It is vitally important that workers have opportunities for meaningful participation in the rulemaking process. Labour unions are the means workers can use to participate fully in the rulemaking process.
Collective Bargaining Agreements
The collective bargaining agreement is the primary tool used by labour unions to implement services to the members. Labour unions use the technical expertise of industrial hygienists, ergonomists, engineers, occupational physicians and other safety and health professionals to collect and analyse safety and health information in order to prepare the union representatives who are responsible for negotiating collective bargaining agreements.
Labour unions utilize collective bargaining agreements as legal, binding documents to provide occupational safety and health protection to workers. The primary goals of the agreements are to provide protection to workers who are either not covered by federal or state workplace safety and health standards and regulations, or to provide protection to workers beyond the minimum state and federal standards.
To prepare for bargaining, unions collect information to document the safety and health issues affecting the membership. This may be accomplished by conducting membership surveys, working with technical staff and/or consultants to identify workplace hazards, reviewing information pertaining to safety and health complaints or investigations that may have been conducted, and by reviewing and evaluating workers’ compensation data, environmental monitoring surveys, or injury and illness logs.
In the final stages of preparation for bargaining, the negotiation committee prioritizes the safety and health issues and considers feasible solutions to the issues.
Worker Education and Training
Labour unions have a very important role in providing safety and health training and education to their members.
The type of training provided ranges from basic workplace safety rights (e.g., hazard communication) to extensive industry-specific training such as that provided to workers who are involved in hazardous waste remediation projects. This training is vitally important for workers who work in rapidly changing work environments.
Worker training provided by unions is usually funded through members’ dues, federal and state grants, and training funds established by employers as negotiated in collective bargaining agreements. Worker training and education courses are developed by professional staff and consultants along with extensive worker input. Often, train-the-trainer courses are provided to allow for peer training.
Research Efforts
Labour unions work with institutions such as universities and governmental agencies to conduct specific occupational safety and health research. The research efforts are typically funded by the union or the employers or through state or federal grants.
The unions use the results of the studies in the safety and health rulemaking process to negotiate contract language in order to eliminate or significantly reduce hazards in the workplace or, alternatively, to develop interventions to eliminate or significantly reduce excessive risk to the union members—for instance, to provide smoking cessation courses among asbestos-exposed workers. In addition, research results may be used to develop or modify various types of equipment used on the job.
The occupational safety and health services provided by labour unions are primarily preventive in nature and require the combined efforts of technical professionals, occupational physicians, lawyers, lobbyists and union members. By providing these services, labour unions are able effectively to ensure the safety and health of their members and of other workers in the workplace.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."