Pain and discomfort in the neck are some of the most common symptoms associated with work. They occur in heavy, manual work as well as in seated, sedentary work, and the symptoms often last for prolonged periods of time—in fact, in some cases, over the whole lifetime. It follows that disorders of the neck are difficult to cure once they have arisen, and therefore much emphasis should be put into primary prevention. There are three main reasons why neck disorders are common in working life:
- The load on the neck structures is maintained for prolonged periods of time, due to high visual demands of the job and to the need of stabilization of the neck-shoulder region in working with the arms.
- Psychologically demanding jobs with high demands on concentration and on quality and quantity of work output are common, and induce an increased activity in neck muscles. This tension increases further if the job in general is psychologically stressful, due to, for example, poor industrial relations, little influence on the organization of work and so on.
- The discs and joints of the neck are frequently the site of degenerative changes, which increase in prevalence with age. This reduces the capacity to withstand occupational workloads. It is also likely that the rate of degeneration increases as the result of physical demands of the job.
Anatomy and Biomechanics of the Neck
The musculoskeletal part of the neck consists of seven vertebral bodies, six intervertabral discs (consisting of cartilage), ligaments to hold these together and linking them to the skull and to the thoracic spine, and muscles surrounding the spine. Although each joint of the cervical spine has a very limited range of motion, the neck can be bent, extended, twisted and tilted with a relatively large range of motion (see table 1). In a normal upright posture and looking straight forward, the centre of gravity of the head and neck is actually situated in front of the centre of support, and therefore needs to be balanced by the dorsal muscles, that is, those situated behind the vertebral bodies. When the head is tilted forward more muscle force is needed to balance the head, and when forward tilt of the head is maintained for prolonged periods of time a substantial muscle fatigue can develop. In addition to muscle fatigue, tilting and bending the head leads to increased compression of the inter-vertebral discs, which may accelerate degenerative processes.
Table 1. Normal and permissible for prolonged driving range of motion (ROM) in degrees, for head.
|
Normal1 |
Permissible2 for prolonged driving |
|
|
Lateral bend |
45 |
– |
|
Twist |
60 |
0 – 15 |
|
Flexion |
45 |
0 – 25 |
|
Extension |
–45 |
0 – –5 |
1 American Academy of Orthopedic Surgeons 1988.
2 Hansson 1987
The muscles surrounding the neck are also active in arm work, in order to stabilize the shoulder/arm complex. The trapezius and several other muscles originate on the cervical spine and extend downwards/outwards to insert on the shoulder. These muscles are commonly the site of dysfunction and disorders, especially in static or repetitive work tasks where the arms are elevated and the vision is fixed.
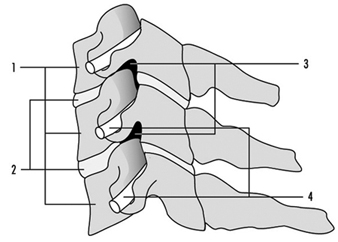
The structures stabilizing the neck are very robust, which serves to protect the nervous tissue inside the spinal canal and the nerves emerging from the intervertebral openings and supplying the neck, upper extremity and upper part of the thorax. The intervertebral discs, the adjoining parts of the vertebral bodies and the facet joints of the intervertebral foramina are often the site of degenerative changes, which can exert pressure on the nerves and narrow their space. (See figure 1).
Figure 1. Schematic drawing of a cross-section of three of the lower cervical vertebral bodies (1) with intervertebral discs; (2) intervertebral foramina; (3) and nerve roots; (4) seen from the side.
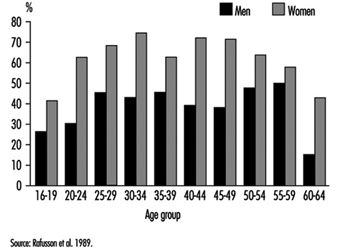
As mentioned in the introduction, symptoms like pain, ache and discomfort in the neck are very common. Depending on the criteria used and the method of investigation, the prevalence rates for neck disorders vary. If a postal enquiry or an interview focusing on musculoskeletal disorders is used, the prevalence of disorders is usually higher than in a thorough investigation also including a physical examination. Thus comparisons between groups should be made only when the same investigation technique has been employed. Figure 2 gives one-year prevalence figures for a representative sample of the Icelandic population who answered a postal enquiry, the so-called “Nordic” questionnaire on musculo- skeletal disorders (Kuorinka et al. 1987). Neck trouble (pain, ache or discomfort) was the third most common (38% average for the whole sample), after shoulder (43%), and low-back (56%) problems. Neck trouble among women was more common than among men, and there was an increase in prevalence up to age 25 to 30, when the rates stabilized; they again went down somewhat at age 50 to 55. In a representative sample of 200 men and women from Stockholm, aged 16 to 65 years, the 12-month prevalence was about 30% among the men and 60% among women. The experience of recent pain in the neck with a duration of at least one month, was found among 22% of a population sample in Gothenburg, Sweden—again rated third most common after shoulder and low-back pain.
Figure 2. Twelve-month prevalence of symptoms of neck trouble of a random sample of the Icelandic population (n=1000)
Risk Factors at Work
Neck disorders are considerably more prevalent in certain occupational groups. Using the Nordic questionnaire (Kuorinka et al. 1987), Swedish occupational health services have compiled data from several occupations. The results indicate that the risk of neck trouble (pain, ache or discomfort) is very high among visual display unit (VDU) operators, sewing machine operators, seamstresses and electronic assembly workers, with a 12-month period prevalence greater than 60%. In addition, up to one-third of those who report disorders also state that the problems have an impact on their working lives, either causing them to take sick-leave, or necessitating a change of job or work tasks.
Epidemiological studies of neck and shoulder disorders have been reviewed, and the different studies have been pooled by type of exposure (repetitive work and work above shoulder level, respectively). Soft-tissue disorders of the neck, such as tension neck and other myalgias, were considerably increased in a number of occupational tasks like data entry, typing, scissors manufacturing, lamp assembly and film rolling.
Degenerative disorders of the intervertebral discs of the neck are more common among coal-miners, dentists and meat industry workers (Hagberg and Wegman 1987).
Posture
Prolonged flexion, extension, lateral bending and twisting of the neck induce muscle fatigue, and may lead to chronic muscle injuries and degenerative changes of the cervical spine. The muscle activity needed to counteract the weight of the head in forward flexion of the neck increases with the flexion angle, as shown in figure 3. Fatigue and pain are common in neck flexion if prolonged work is performed. When the head is tilted forward to the extreme of its range of motion, the main load is transferred from muscles to ligaments and joint capsules surrounding the cervical spine. It has been calculated that if the entire cervical spine is flexed maximally, the torque exerted by the head and neck on the disc between the seventh cervical and the first thoracic vertebral body is increased by a factor of 3.6. Such postures lead to pain within only about 15 minutes, and usually the posture has to be normalized within 15 to 60 minutes because of intense pain. Postures where the neck is bent forward for prolonged periods of time—several hours—are common in assembly work in industry, in VDT work and in packaging and inspection tasks where the work stations are poorly designed. Such postures are frequently caused by a compromise between the need to perform work with the hands, without elevating the arms, and the simultaneous need for visual control. For a review of the mechanisms leading from muscle fatigue to injury, see the accompanying article “Muscles”.
Figure 3. Percentage of maximal neck extension strength required at increasing neck inclination (flexion).

Extension of the neck for prolonged periods, as in overhead work in the building industry, can be very tiring for the muscles in front of the cervical spine. Especially when carrying heavy protective equipment like safety helmets, the torque tilting the head backwards can be high.
Repetitive movements
Repetitive movements performed by the hands increase the demands on stabilization of the neck and shoulder region, and thereby increase the risk of neck complaints. Factors like high demands on speed and precision of movements, as well as high demands on force exerted by the hands, imply even larger demands on stabilization of the proximal body regions. Repetitive movements of the head are less common. Rapid and repeated changes between visual targets are usually accomplished through eye movements, unless the distance between the objects observed is fairly large. This may occur for example at large computerized work stations.
Vibration
Local vibration of the hands, such as working with drills and other vibrating hand-held machines, is transferred along the arm but the fraction transferred up to the shoulder-neck region is negligible. However, the holding of a vibrating tool may induce muscle contractions in the proximal shoulder-neck muscles in order to stabilize the hand and the tool, and may thereby exert a tiring effect on the neck. The mechanisms and the prevalence of such vibration-induced complaints are not well known.
Work organization
Work organization in this context is defined as the distribution of work tasks over time and between workers, the duration of work tasks, and the duration and distribution of rest periods and breaks. The duration of work and rest periods has a profound effect on tissue fatigue and recovery. Few specific studies on the effect of work organization on neck disorders have been performed. In a large epidemiological study in Sweden, it was found that VDU work exceeding four hours per day was associated with elevated rates of neck symptoms (Aronsson, Bergkvist and Almers 1992). These findings have subsequently been confirmed in other studies.
Psychological and social factors
Associations between psychological and social factors at work and disorders of the neck region have been demonstrated in several studies. Especially factors such as perceived psychological stress, poor control of work organization, poor relations with management and work mates and high demands on accuracy and speed of work have been highlighted. These factors have been associated with an increased risk (up to twofold) of disorders in cross-sectional studies. The mechanism is likely to be an increase of tension in the trapezius and other muscles surrounding the neck, as part of a general “stress” reaction. Since well-controlled longitudinal studies are scarce, it is still uncertain whether these factors are causal or aggravating. Moreover, poor psychological and social conditions often occur in jobs also characterized by prolonged awkward postures.
Individual factors
Individual characteristics like age, sex, muscle strength and endurance, physical fitness, body size, personality, intelligence, leisure time habits (physical activity, smoking, alcohol, diet) and previous musculoskeletal disorders have been discussed as factors which might modify the response to physical and psychosocial exposures. Age as a risk factor is discussed above and is illustrated in figure 2.
Females usually report a higher prevalence of neck symptoms than males. The most likely explanation is that exposure to both physical and psychosocial risk factors is higher in women than among men, such as in work with VDUs, assembly of small components and machine sewing.
Studies of muscle groups other than those of the neck do not consistently indicate that a low static strength implies an elevated risk of development of disorders. No data are available concerning neck muscles. In a recent study of a random population of Stockholm, low endurance at neck extension was weakly associated with later development of neck disorders (Schüldt et al. 1993). Similar results have been reported for low-back disorders.
In a longitudinal study in Sweden, personality type was a risk factor for development of shoulder-neck disorders (Hägg, Suurküla and Kilbom 1990). Those employees who had a type A personality (e.g., were ambitious and impatient) developed more serious problems than others, and these associations were not related to individual productivity.
Little is known of the association between other individual characteristics and neck disorders.
Prevention
Work station design
The work station should be organized so that the head is not statically bent, extended or twisted beyond the limits given for the permissible range of motion given for prolonged driving in table 1. Now and then, movements that are within the limits for normal range of motion are acceptable, as well as the occasional movement to the individual extremes. Experimental studies have shown that the load of the neck muscles is lower with a slightly backward tilted trunk than with a straight upright posture, which in turn is better than a forward tilted trunk (Schüldt 1988).
The set-up of the workstation and the positioning of the work object requires a careful consideration and a trade-off between the demands for optimal head and shoulder-arm posture. Usually the work object is positioned somewhat below elbow height, which may however induce a high strain on the neck muscles (e.g., in assembly work). This requires individually adjustable work stations.
Visual strain will increase the tension of the neck muscles, and therefore attention should be given to the lighting and contrasts of the work station and to readability of information given on VDUs and on printed material. For VDU work the viewing distance should be optimized to about 45 to 50 cm and the viewing angle to 10 to 20 degrees. The vision of the worker should be optimized with the aid of glasses.
Work organization
In work with static loads on the neck, such as in assembly and data entry VDU work, frequent breaks should be introduced to provide recovery from fatigue. Recommendations to introduce one break of about 10 minutes per hour and to limit VDU work to a maximum of four hours per day have been issued in some localities. As pointed out above, the scientific basis for these recommendations with regard to the neck is relatively weak.
Clinical Characteristics and Treatmentof Neck Disorders
Painful soft-tissue disorders
Tension neck and other myalgias
The most common localization for neck tension and other myalgias is in the upper part of the trapezius muscle, but other muscles originating in the neck are often affected simultaneously. Symptoms are stiffness of the neck and ache at work and at rest. Frequently, excessive muscle fatigue is perceived, even during short-lasting and low-level periods of work. The muscles are tender, and often “tender points” can be found on palpation. Tension neck is common in jobs with prolonged static loads on neck and shoulders. Microscopic examination of the tissue has shown changes in the muscle morphology, but the mechanisms are incompletely understood and are likely to involve both the blood circulation and the nervous regulation.
Acute torticollis
This state of acute pain and stiffness of the neck can be provoked by sudden twisting of the head and extension of the opposite arm. Sometimes no provoking event can be identified. Acute torticollis is believed to be caused by strain and partial ruptures of the ligaments of the neck. Usually the pain and stiffness subsides within a week following rest, external support of the neck (collar) and muscle-relaxing medication.
Degenerative disorders
Acute disorder (disc herniation)
Degeneration of the cervical spine involves the discs, which lose some of their resistance to even mild stresses. Herniation of the disc with extrusion of its contents, or bulging of it, can compromise nervous tissue and blood vessels laterally and posteriorly to the disc. One acute degenerative disorder of the disc is compression of the nerve roots extending from the spinal cord and supplying the neck, arms and upper thorax. Depending on the level of compression (disc between second and third cervical vertebrae, third and fourth, and so on), acute sensory and motor symptoms arise from the regions supplied by the nerves. The investigation of acute symptoms of the neck and arms includes a thorough neurological examination in order to identify the level of a possible disc prolapse and plain x-ray examination, usually supplemented with CT scanning and MRI.
Chronic disorders (Cervical spondylosisand cervical syndrome)
Degeneration of the cervical spine involves narrowing of the disc, formation of new bone (so-called osteophytes) extending from the edges of the cervical vertebra, and thickening of the ligaments as in acute disorder. When osteophytes extend into the foramina, they may compress the nerve roots. Spondylosis is the term used for the radiological changes in the neck. Sometimes these changes are associated with chronic local symptoms. Radiological changes may be advanced without serious symptoms and vice versa. Symptoms are usually ache and pain in the neck, sometimes extending to the head and the shoulder region, and reduced mobility. Whenever nerve roots are compressed, the diagnosis cervical syndrome is used. Symptoms of cervical syndrome are ache and pain in the neck, reduced mobility of the neck, and sensory and motor symptoms from the side of the compressed nerve root. Symptoms like reduced sensitivity to touch, numbness, tingling and reduced strength are common in the hand and arm. Thus symptoms are similar to those arising from acute disc prolapse, but usually the onset is more gradual and the severity may fluctuate depending on the external workload. Both cervical spondylosis and cervical syndrome are common in the general population, particularly among aged persons. The risk of cervical spondylosis is elevated in occupational groups with a sustained, high biomechanical load on the neck structures, like coal-miners, dentists and meat industry workers.
Traumatic disorders (whiplash injuries)
In rear-end car accidents, the head (if not restricted by support from behind) is tilted backward at high speed and with great force. In less severe accidents only partial muscle ruptures may occur, whereas severe accidents may seriously damage the muscles and ligaments in front of the cervical spine and also damage nerve roots. The most serious cases occur when the cervical vertebrae are dislocated. Whiplash injuries need careful examination and treatment, as long-lasting symptoms such as headaches may persist if the injury is not cared for properly.