The hip joint is a ball-and-socket joint surrounded by ligaments, strong muscles and bursae. The joint is weight bearing and has both high intrinsic stability and a wide range of motion. In young people pain in the hip region usually originates in the muscles, tendon insertions or bursae, while in older people, osteoarthrosis is the predominant disorder causing hip pain.
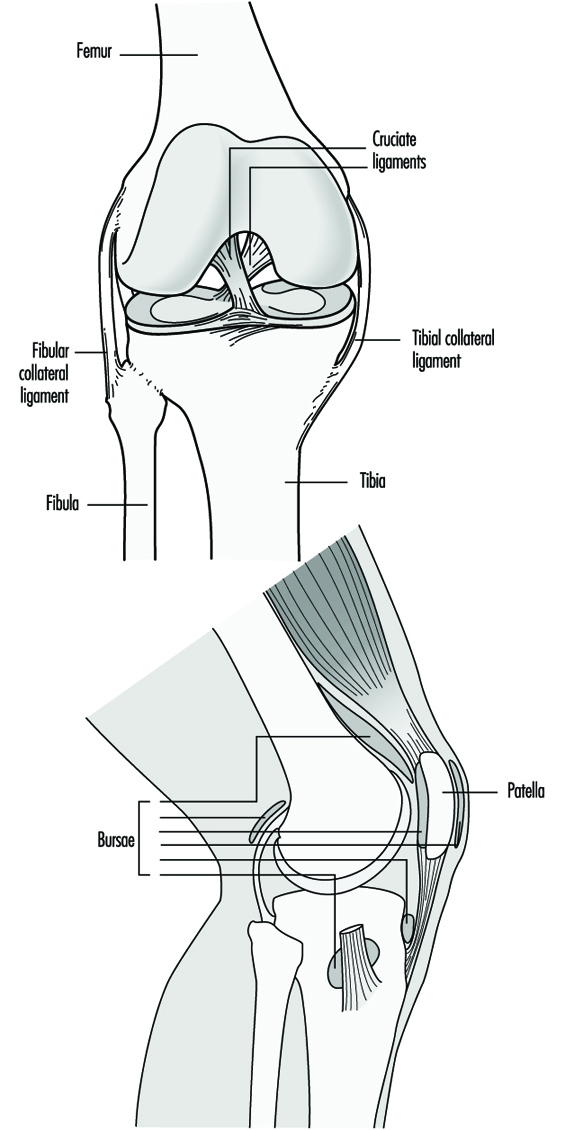
The knee is a weight-bearing joint that is important for walking, standing, bending, stooping and squatting. The knee is rather unstable and depends for support on ligaments and strong muscles as shown in figure 1. There are two joints in the knee, the femorotibial and the femoropatellar. On both inner and outer side of the joint there are strong ligaments, and in the centre of the femorotibial joint are the cruciate ligaments, which give stability and assist in the normal mechanical function of the knee. The menisci are curved, fibrocartilaginous structures that lie between the femoral (femoral condyles) and the tibial bones (tibial plateau). The knee joint is both stabilized and empowered by muscles that originate above the hip joint and at the shaft of the femur and are inserted upon bony structures below the knee joint. Around the knee joint there is a synovial capsule, and the joint is protected by several bursae.
Figure 1. The knee.
All these structures are easily hurt by trauma and overuse, and medical treatment for knee pain is rather common. Osteoarthrosis of the knee is a common disorder among the elderly, leading to pain and disability. In younger people, patellar bursitis and patellofemoral pain syndromes like a painful pes anserinus are rather common.
Osteoarthrosis
Osteoarthrosis (OA) is a common degenerative joint disorder in which the cartilage is more or less destroyed and the structure of the underlying bone is affected. Sometimes it is accompanied by few symptoms, but usually OA causes suffering, changes in ability to work and a decreased quality of life. Changes in the joint can be seen on x ray, and an OA sufferer usually seeks medical care because of pain, which is present even at rest, and a diminished range of motion. In severe cases, the joint may become totally stiff, and even destroyed. Surgery to replace a destroyed joint and replace it with a prosthesis is well developed today.
Studying the causes of osteoarthrosis of the hip is difficult. The onset of the disorder is usually hard to pinpoint; the development is usually slow and insidious (that is, one doesn’t necessarily know it is happening). The end point, for research purposes, can be different things, varying from slight changes in x rays to symptomatic disorders that require surgery. Indeed the end points used to identify the condition may differ because of different traditions in different countries, and even between different clinics in the same town. These factors cause problems in the interpretation of research studies.
Epidemiological research tries to identify associations between exposures such as physical load, and outcomes, such as osteo-arthrosis. When combined with other knowledge, it is possible to find associations that could be considered causal, but the cause-effect chain is complicated. Osteoarthrosis is common in every population, and one must remember that the disorder exists among persons with no known hazardous exposure, while there are healthy subjects in the group with high and well-known harmful exposure. Unknown paths between exposure and disorder, unknown health factors, genetics and selection forces may be a few of the contributors to that.
Individual risk factors
Age: The occurrence of arthrosis increases with age. X-ray investigations of osteoarthrosis of different joints, mainly the hip and the knee, have been made in different populations and the prevalences found to vary. The explanation might be ethnic differences or variations in investigation techniques and diagnostic criteria.
Congenital and developmental diseases and changes: Early changes in the joint, such as congenital malformations, those caused by infections and so on, lead to an earlier and faster progression of osteoarthrosis of the hip. Knock-knees (varus) and bandy-legs (valgus) put an uneven distribution of forces on the knee joint, for example, which can have some importance for arthrosis development.
Heredity: Hereditary factors are present for osteoarthrosis. For example, osteoarthrosis of the hip is a rare disease among people of Asian origin but more common among Caucasians, which suggests a hereditary factor. Osteoarthrosis in three or more joints is called generalized osteoarthrosis and has a hereditary pattern. The hereditary pathway for osteoarthrosis of the knee is not very well known.
Overweight: Overweight can probably cause osteoarthrosis of the knee and hip. The relationship between overweight and knee osteoarthrosis has been shown in large epidemiological studies of the general population, such as the National Health and Nutrition Examination Survey (NHANES) and Framingham study in the United States. The association was strongest for women but existed even for men (Anderson and Felson 1988; Felson et al. 1988).
Trauma: Accidents or causes of trauma or injury, especially those that interfere with the mechanics and circulation of the joint and ligament, can give rise to an early osteoarthrosis.
Sex and oestrogen use: Osteoarthrosis of the hip and knee seems to be equally distributed among men and women. From a study on female participants in the Framingham study, it was concluded that oestrogen use in women is associated with a modest but insignificant protective effect against osteoarthrosis of the knee (Hannan et al. 1990).
Mechanical load
Experimental studies in monkeys, rabbits, dogs and sheep have shown that compression forces on a joint, especially when it is held in an extreme position, with or without simultaneous shifting loads, can lead to changes in the cartilage and bone similar to those of osteoarthrosis in human beings.
Sports activities: Participation in sports can increase the load on different joints. The risk of trauma is also increased. On the other hand, however, good muscle function and coordination are developed at the same time. Few data are available as to whether participating in sports prevents trauma or is harmful to the joints. Data drawn from good scientific studies are very limited, and some are described here. Several studies of soccer players have shown that both professionals and amateurs have more osteoarthrosis of the hip and knee than the general male population. For example, one Swedish study of 50- to 70-year-old men with a severe osteoarthrosis who were compared with healthy men in the same age group, showed that the men with osteoarthrosis had been more heavily involved in sports activities in their youth. Track and field, racket sports, and soccer seemed to be most harmful (Vingård et al. 1993). In the scientific literature there are other studies that have not shown any differences between athletes and those who do not participate in sports. However most of them are performed on still active athletes and are thus not conclusive.
Workload factors
The aetiology of osteoarthrosis of the knee and hip is, as for all diseases, complex and multifactorial. Recent well-performed studies have shown that physical load on the joint from occupational exposures will play a role as a contributing cause for the development of premature osteoarthrosis.
Most epidemiological studies concerning physical workload are cross-sectional and carried out on occupational groups without making individual exposure assessments. These serious methodological problems make generalizing the results of such studies extremely difficult. Farmers have been found to have more osteoarthrosis of the hip than other occupational groups in several studies. In a Swedish study of 15,000 farmers, farmers’ wives and other farm workers were asked about past x-ray examinations in which the hip joint could be seen. Among the 565 men and 151 women who had been examined, hip joints were studied using the same criteria and the same investigator as in a population study from Sweden 1984. The distribution of osteoarthrosis of the hip among male farmers and the male population of Malmö is shown in table 1 (Axmacher and Lindberg 1993).
Table 1. Prevalence of primary osteoarthrosis of the hip among male farmers and population of different age groups in the city of Malmö.
|
Male farmers |
Male Malmö population |
|||||
|
Age group |
N |
Cases |
Prevalence |
N |
Cases |
Prevalence |
|
40–44 |
96 |
1 |
1.0% |
250 |
0 |
0.0% |
|
45–49 |
127 |
5 |
3.9% |
250 |
1 |
0.4% |
|
50–54 |
156 |
12 |
6.4% |
250 |
2 |
0.8% |
|
55–59 |
127 |
17 |
13.4% |
250 |
3 |
1.2% |
|
60–64 |
59 |
10 |
16.9% |
250 |
4 |
1.6% |
N = Number of men studied; cases = men with osteoarthrosis of the hip.
Source: Axmacher and Lindberg 1993.
In addition to farmers, construction workers, food-processing workers (grain-mill workers, butchers and meat preparers), firefighters, mail carriers, shipyard workers and professional ballet dancers have all been found to be at an increased risk of hip osteoarthrosis. It is important to realize that an occupational title alone does not adequately describe the stress on a joint—the same job type can mean different loads for different workers. Further, the load of interest in a study is the exact pressure placed on a joint. In a study from Sweden, physical workload has been quantified retrospectively through individual interviews (Vingård et al. 1991). Men with high physical load exposures due to their occupations up to the age of 49 had more than double the risk for developing osteoarthrosis of the hip compared to those with low exposure. Both dynamic exposures, such as heavy lifting, and static exposure, such as prolonged sitting in a twisted position, seemed to be equally harmful to the joint.
The risk of knee osteoarthrosis has been found to be increased in coal miners, dockers, shipyard workers, carpet and floor layers and other construction workers, firefighters, farmers and cleaners. Moderate to heavy physical demands at work, knee bending and traumatic injury increase the risk.
In another English study from 1968, dockers were found to have more osteoarthrosis of the knee than civil servants in sedentary occupations (Partridge and Duthie 1968).
In Sweden, Lindberg and Montgomery investigated workers in a shipyard and compared them to office workers and teachers (Lindberg and Montgomery 1987). Among shipyard workers 3.9% had gonarthrosis, compared to 1.5% among office workers and teachers.
In Finland, Wickström compared concrete reinforcement workers with painters, but no differences in disability from the knees were found (Wickström et al. 1983). In a later Finnish study, knee disorders in carpet and floor layers and painters were compared (Kivimäki, Riihimäki and Hänninen 1992). Knee pain, knee accidents, and treatment regimes for the knees, as well as osteophytes around the patella, were more common among carpet and floor layers than among the painters. The authors suggest that kneeling work increases the risk of knee disorders and that the changes observed in x rays might be an initial sign of knee degeneration.
In the United States, factors associated with osteoarthrosis of the knee in the first National Health and Nutrition Examination Survey (NHANES 1) were examined for a total of 5,193 men and women aged 35 to 74 years, 315 of whom had x-ray-diagnosed osteoarthrosis of the knee (Anderson 1988). In investigating occupational load the authors characterized the physical demands and knee-bending stress from occupational titles in US Department of Labor Dictionary of Occupational Titles. For both men and women, for those whose jobs were described as involving a lot of knee-bending, the risk for developing an osteoarthrosis of the knee was more than double that for those without such jobs. When controlling for age and weight in the statistical analysis, they found that 32% of the osteoarthrosis of the knee occurring in these workers was attributable to occupation.
In the Framingham study in the United States, subjects from Framingham, a town outside Boston, have been followed in an epidemiological study for more than 40 years (Felson 1990). Occupational status was reported for the years 1948–51 and 1958–61 and the results of x rays looking for radiographic osteo- arthrosis of the knee during the years 1983–85. Each subject’s job was characterized by its level of physical demand and whether the job was associated with knee-bending. This study also found that the risk for developing osteoarthrosis of the knee was doubled for those with a lot of knee bending and at least medium physical demands in their occupation.
In a study from California the roles of physical activity, obesity and knee injury on the development of severe osteoarthrosis of the knee was evaluated (Kohatsu and Schurman 1990). Forty-six people with gonarthrosis and 46 healthy people from the same community were studied. The persons with osteoarthrosis were two to three times more likely than the controls to have performed moderate to heavy work earlier in life and 3.5 times more likely to have been obese at the age of 20. They were almost five times more likely to have had a knee injury. There was no difference in the leisure time activities reported in the two groups.
In a register-based cohort study from Sweden (Vingärd et al. 1991) subjects born between 1905 and 1945, living in 13 of the 24 counties in Sweden in 1980 and reporting that they held the same blue-collar occupation in the censuses of 1960 and of 1970, were studied. The blue-collar occupations reported were then classified as to whether they were associated with high (more than average) or low (less than average) load on the lower extremity. During 1981, 1982 and 1983 it was determined whether the study population sought hospital care for osteoarthrosis of the knee. Firefighters, farmers and construction workers had an elevated relative risk among men to develop osteoarthrosis of the knee. Among women, cleaners were found to be at greater risk.
Chondromalacia patellae
A special case of osteoarthrosis is chondromalacia patellae, which often starts in the young. It is a degenerative change in the cartilage on the back of the patella bone. The symptom is pain in the knee, especially while bending it. Among sufferers, the patella is very tender when tapped, and especially if pressure is put on it. The treatment is quadriceps muscle training and, in severe cases, surgery. The connection to occupational activity is unclear.
Patellar bursitis
In the knee, there is a bursa between the skin and the patella. The bursa, which is a sac containing fluid, can be subject to mechanical pressure during kneeling and thus become inflamed. Symptoms are pain and swelling. A substantial amount of serous fluid can be aspirated from the bursa. This disorder is rather common among occupational groups that do a lot of kneeling. Kivimäki (1992) has investigated soft-tissue changes in the front of the knee using ultrasonography in two occupational groups. Among carpet and floor layers 49% had thickening of the prepatellar or superficial infrapatellar bursa, compared to 7% among painters.
Pes anserinus bursitis
The pes anserinus consists of the tendons of the sartorius, semimembranous and gracilis muscles at the inner aspect of the knee joint. Under the insertion point of these tendons, there is a bursa that can be inflamed. Pain is increased by forceful extension of the knee.
Trochanter bursitis
The hip has many bursae that surround it. The trochanteric bursa lies between the tendon of the gluteus maximus muscle and the posterolateral prominence of the greater trochanter (the other side of the hip). Pain in this area is usually called trochanter bursitis. Sometimes it is a true bursitis. The pain can radiate down the thigh and may simulate sciatic pain.
Theoretically it is possible that a special occupational posture can cause the disorder, but there are no scientific investigations.
Meralgia paresthetica
Meralgia paresthetica belongs to the entrapment disorders, and the cause is probably an entrapment of the nervus cutaneus femoris lateralis where the nerve comes out between muscles and fasciae above the edge of the pelvis (spina iliaca anterior superior). The sufferer will have pain along the front and lateral side of the thigh. The disorder can be rather tricky to cure. Different remedies, from pain killers to surgery, have been used with varying success. Since there are occupational exposures which cause pressure against the nerve, so this condition may be an occupational disorder. Anecdotal accounts of this exist, but there are no epidemiological investigations available that verify it.