Occupational Exposure
Mechanical vibration arising from powered processes or tools and entering the body at the fingers or the palm of the hands is called hand-transmitted vibration. Frequent synonyms for hand-transmitted vibration are hand-arm vibration and local or segmental vibration. Powered processes and tools which expose operators’ hands to vibration are widespread in several industrial activities. Occupational exposure to hand-transmitted vibration arises from hand-held powered tools used in manufacturing (e.g., percussive metal-working tools, grinders and other rotary tools, impact wrenches), quarrying, mining and construction (e.g., rock-drills, stone-hammers, pick-hammers, vibrocompactors), agriculture and forestry (e.g., chain saws, brush saws, barking machines) and public utilities (e.g., road and concrete breakers, drill-hammers, hand-held grinders). Exposure to hand-transmitted vibration can also occur from vibrating workpieces held in the hands of the operator as in pedestal grinding, and from hand-held vibrating controls as in operating lawn mowers or in controlling vibrating road compactors. It has been reported that the number of persons exposed to hand-transmitted vibration at work exceeds 150,000 in the Netherlands, 0.5 million in Great Britain, and 1.45 million in the United States. Excessive exposure to hand-transmitted vibration can cause disorders in the blood vessels, nerves, muscles, and bones and joints of the upper limbs. It has been estimated that 1.7 to 3.6% of the workers in European countries and the United States are exposed to potentially harmful hand-transmitted vibration (ISSA International Section for Research 1989). The term hand-arm vibration (HAV) syndrome is commonly used to refer to signs and symptoms associated with exposure to hand-transmitted vibration, which include:
- vascular disorders
- peripheral neurological disorders
- bone and joint disorders
- muscle disorders
- other disorders (whole body, central nervous system).
Leisure activities such as motorcycling or using domestic vibrating tools can occasionally expose the hands to vibration of high amplitude, but only long daily exposures may give rise to health problems (Griffin 1990).
The relationship between occupational exposure to hand-transmitted vibration and adverse health effects is far from simple. Table 1 lists some of the most important factors which concur to cause injuries in the upper limbs of vibration-exposed workers.
Table 1. Some factors potentially related to injurious effects during hand-transmitted vibration exposures
Vibration characteristics
- Magnitude (r.m.s., peak, weighted/unweighted)
- Frequency (spectra, dominant frequencies)
- Direction (x-, y-, z- axes)
Tools or processes
- Tool design (portable, fixed)
- Tool type (percussive, rotary, rotating percussive)
- Condition
- Operation
- Material being worked
Exposure conditions
- Duration (daily, yearly exposures)
- Pattern of exposure (continuous, intermittent, rest periods)
- Cumulative exposure duration
Environmental conditions
- Ambient temperature
- Airflow
- Humidity
- Noise
- Dynamic response of the finger-hand-arm system
- Mechanical impedance
- Vibration transmissibility
- Absorbed energy
Individual characteristics
- Method of working (grip force, push force, hand-arm posture, body position)
- Health
- Training
- Skill
- Use of gloves
- Individual susceptibility to injury
Biodynamics
It may be presumed that factors influencing the transmission of vibration into the finger-hand-arm system play a relevant role in the genesis of vibration injury. The transmission of vibration depends on both the physical characteristics of vibration (magnitude, frequency, direction) and the dynamic response of the hand (Griffin 1990).
Transmissibility and impedance
Experimental results indicate that the mechanical behaviour of the human upper limb is complex, as the impedance of the hand-arm system—that is, its resistance to vibrate—shows pronounced variations with the change in vibration amplitude, frequency and direction, applied forces, and orientation of the hand and arm with respect to the axis of the stimulus. Impedance is also influenced by body constitution and structural differences of the various parts of the upper limb (e.g., the mechanical impedance of the fingers is much lower than that of the palm of the hand). In general, higher vibration levels, as well as tighter hand-grips, result in greater impedance. However, the change in impedance has been found to be highly dependent on the frequency and direction of the vibration stimulus and various sources of both intra- and inter-subject variability. A resonance region for the finger-hand-arm system in the frequency range between 80 and 300 Hz has been reported in several studies.
Measurements of the transmission of vibration through the human arm have shown that lower frequency vibration (>50 Hz) is transmitted with little attenuation along the hand and forearm. The attenuation at the elbow is dependent on the arm posture, as the transmission of vibration tends to decrease with the increase of the flexion angle at the elbow joint. For higher frequencies (>50 Hz), the transmission of vibration progressively decreases with increasing frequency, and above 150 to 200 Hz most of the vibrational energy is dissipated in the tissues of the hand and fingers. From transmissibility measurements it has been inferred that in the high-frequency region vibration may be responsible for damage to the soft structures of the fingers and hands, while low-frequency vibration of high amplitude (e.g., from percussive tools) might be associated with injuries to the wrist, elbow and shoulder.
Factors influencing finger and hand dynamics
The adverse effects from vibration exposure may be assumed to be related to the energy dissipated in the upper limbs. Energy absorption is highly dependent on factors affecting the coupling of the finger-hand system to the vibration source. Variations in grip pressure, static force and posture modify the dynamic response of the finger, hand and arm, and, consequently, the amount of energy transmitted and absorbed. For instance, grip pressure has a considerable influence on energy absorption and, in general, the higher the hand grip the greater the force transmitted to the hand-arm system. Dynamic response data can provide relevant information to assess the injury potential of tool vibration and to assist in the development of anti-vibration devices such as hand-grips and gloves.
Acute Effects
Subjective discomfort
Vibration is sensed by various skin mechanoreceptors, which are located in the (epi)dermal and subcutaneous tissues of the smooth and bare (glabrous) skin of the fingers and hands. They are classified into two categories—slow and fast adapting—according to their adaptation and receptive field properties. Merkel discs and Ruffini endings are found in the slow-adapting mechanoreceptive units, which respond to static pressure and slow changes in pressure and are excited at low frequency (<16 Hz). Fast-adapting units have Meissner’s corpuscles and Pacinian corpuscles, which respond to rapid changes in stimulus and are responsible for vibratory sensation in the frequency range between 8 and 400 Hz. The subjective response to hand-transmitted vibration has been used in several studies to obtain threshold values, contours of equivalent sensation and unpleasant or tolerance limits for vibratory stimuli at different frequencies (Griffin 1990). Experimental results indicate that human sensitivity to vibration decreases with increasing frequency for both comfort and annoyance vibration levels. Vertical vibration appears to cause more discomfort than vibration in other directions. Subjective discomfort has also been found to be a function of the spectral composition of vibration and the grip force exerted on the vibrating handle.
Activity interference
Acute exposure to hand-transmitted vibration can cause a temporary increase in vibrotactile thresholds due to a depression of the excitability of the skin mechanoreceptors. The magnitude of the temporary threshold shift as well as the time for recovery is influenced by several variables, such as the characteristics of the stimulus (frequency, amplitude, duration), temperature as well as the worker’s age and previous exposure to vibration. Exposure to cold aggravates the tactile depression induced by vibration, because low temperature has a vasoconstrictive effect on digital circulation and reduces finger skin temperature. In vibration-exposed workers who often operate in a cold environment, repeated episodes of acute impairment of tactile sensitivity can lead to permanent reduction in sensory perception and loss of manipulative dexterity, which, in turn, can interfere with work activity, increasing the risk for acute injuries due to accidents.
Non-Vascular Effects
Skeletal
Vibration-induced bone and joint injuries are a controversial matter. Various authors consider that disorders of bones and joints in workers using hand-held vibrating tools are not specific in character and similar to those due to the ageing process and to heavy manual work. On the other hand, some investigators have reported that characteristic skeletal changes in the hands, the wrists and the elbows can result from prolonged exposure to hand-transmitted vibration. Early x-ray investigations had revealed a high prevalence of bone vacuoles and cysts in the hands and wrists of vibration-exposed workers, but more recent studies have shown no significant increase with respect to control groups made up of manual workers. Excess prevalence of wrist osteoarthrosis and elbow arthrosis and osteophytosis has been reported in coal miners, road construction workers and metal-working operators exposed to shocks and low frequency vibration of high amplitude from pneumatic percussive tools. On the contrary, there is little evidence for an increased prevalence of degenerative bone and joint disorders in the upper limbs of workers exposed to mid- or high-frequency vibrations arising from chain saws or grinding machines. Heavy physical effort, forceful gripping and other biomechanical factors can account for the higher occurrence of skeletal injuries found in workers operating percussive tools. Local pain, swelling, and joint stiffness and deformities may be associated with radiological findings of bone and joint degeneration. In a few countries (including France, Germany, Italy), bone and joint disorders occurring in workers using hand-held vibrating tools are considered to be an occupational disease, and the affected workers are compensated.
Neurological
Workers handling vibrating tools may experience tingling and numbness in their fingers and hands. If vibration exposure continues, these symptoms tend to worsen and can interfere with work capacity and life activities. Vibration-exposed workers may exhibit increased vibratory, thermal and tactile thresholds in clinical examinations. It has been suggested that continuous vibration exposure can not only depress the excitability of skin receptors but also induce pathological changes in the digital nerves such as perineural oedema, followed by fibrosis and nerve fibre loss. Epidemiological surveys of vibration-exposed workers show that the prevalence of peripheral neurological disorders varies from a few per cent to more than 80 per cent, and that sensory loss affects users of a wide range of tool types. It seems that vibration neuropathy develops independently of other vibration-induced disorders. A scale of the neurological component of the HAV syndrome was proposed at the Stockholm Workshop 86 (1987), consisting of three stages according to the symptoms and the results of clinical examination and objective tests (table 2).
Table 2. Sensorineural stages of the Stockholm Workshop scale for the hand-arm vibration syndrome
|
Stage |
Signs and symptoms |
|
0SN |
Exposed to vibration but no symptoms |
|
1SN |
Intermittent numbness, with or without tingling |
|
2SN |
Intermittent or persistent numbness, reduced sensory perception |
|
3SN |
Intermittent or persistent numbness, reduced tactile discrimination and/or |
Source: Stockholm Workshop 86 1987.
Careful differential diagnosis is required to distinguish vibration neuropathy from entrapment neuropathies, such as carpal tunnel syndrome (CTS), a disorder due to compression of the median nerve as it passes through an anatomical tunnel in the wrist. CTS seems to be a common disorder in some occupational groups using vibrating tools, such as rock-drillers, platers and forestry workers. It is believed that ergonomic stressors acting on the hand and wrist (repetitive movements, forceful gripping, awkward postures), in addition to vibration, can cause CTS in workers handling vibrating tools. Electroneuromyography measuring sensory and motor nerve velocities has proven to be useful to differentiate CTS from other neurological disorders.
Muscular
Vibration-exposed workers may complain of muscle weakness and pain in the hands and arms. In some individuals muscle fatigue can cause disability. A decrease in hand-grip strength has been reported in follow-up studies of lumberjacks. Direct mechanical injury or peripheral nerve damage have been suggested as possible aetiological factors for muscle symptoms. Other work-related disorders have been reported in vibration-exposed workers, such as tendinitis and tenosynovitis in the upper limbs, and Dupuytren’s contracture, a disease of the fascial tissue of the palm of the hand. These disorders seem to be related to ergonomic stress factors arising from heavy manual work, and the association with hand-transmitted vibration is not conclusive.
Vascular Disorders
Raynaud’s phenomenon
Giovanni Loriga, an Italian physician, first reported in 1911 that stone cutters using pneumatic hammers on marble and stone blocks at some yards in Rome suffered from finger blanching attacks, resembling the digital vasospastic response to cold or emotional stress described by Maurice Raynaud in 1862. Similar observations were made by Alice Hamilton (1918) among stone cutters in the United States, and later by several other investigators. In the literature various synonyms have been used to describe vibration-induced vascular disorders: dead or white finger, Raynaud’s phenomenon of occupational origin, traumatic vasospastic disease, and, more recently, vibration-induced white finger (VWF). Clinically, VWF is characterized by episodes of white or pale fingers caused by spastic closure of the digital arteries. The attacks are usually triggered by cold and last from 5 to 30 to 40 minutes. A complete loss of tactile sensitivity may be experienced during an attack. In the recovery phase, commonly accelerated by warmth or local massage, redness may appear in the affected fingers as a result of a reactive increase of blood flow in the cutaneous vessels. In the rare advanced cases, repeated and severe digital vasospastic attacks can lead to trophic changes (ulceration or gangrene) in the skin of the fingertips. To explain cold-induced Raynaud’s phenomenon in vibration-exposed workers, some researchers invoke an exaggerated central sympathetic vasoconstrictor reflex caused by prolonged exposure to harmful vibration, while others tend to emphasize the role of vibration-induced local changes in the digital vessels (e.g., thickening of the muscular wall, endothelial damage, functional receptor changes). A grading scale for the classification of VWF has been proposed at the Stockholm Workshop 86 (1987), (table 3). A numerical system for VWF symptoms developed by Griffin and based on scores for the blanching of different phalanges is also available (Griffin 1990). Several laboratory tests are used to diagnose VWF objectively. Most of these tests are based on cold provocation and the measurement of finger skin temperature or digital blood flow and pressure before and after cooling of fingers and hands.
Table 3. The Stockholm Workshop scale for staging cold-induced Raynaud’s phenomenon in the hand-arm vibration syndrome
|
Stage |
Grade |
Symptoms |
|
0 |
— |
No attacks |
|
1 |
Mild |
Occasional attacks affecting only the tips of one or more fingers |
|
2 |
Moderate |
Occasional attacks affecting distal and middle (rarely also |
|
3 |
Severe |
Frequent attacks affecting all phalanges of most fingers |
|
4 |
Very severe |
As in stage 3, with trophic skin changes in the finger tips |
Source: Stockholm Workshop 86 1987.
Epidemiological studies have pointed out that the prevalence of VWF is very wide, from less than 1 to 100 per cent. VWF has been found to be associated with the use of percussive metal-working tools, grinders and other rotary tools, percussive hammers and drills used in excavation, vibrating machinery used in the forest, and other powered tools and processes. VWF is recognized as an occupational disease in many countries. Since 1975–80 a decrease in the incidence of new cases of VWF has been reported among forestry workers in both Europe and Japan after the introduction of anti-vibration chain saws and administrative measures curtailing saw usage time. Similar findings are not yet available for tools of other types.
Other Disorders
Some studies indicate that in workers affected with VWF hearing loss is greater than that expected on the basis of ageing and noise exposure from the use of vibrating tools. It has been suggested that VWF subjects may have an additional risk of hearing impairment due to vibration-induced reflex sympathetic vasoconstriction of the blood vessels supplying the inner ear. In addition to peripheral disorders, other adverse health effects involving the endocrine and central nervous system of vibration-exposed workers have been reported by some Russian and Japanese schools of occupational medicine (Griffin 1990). The clinical picture, called “vibration disease,” includes signs and symptoms related to dysfunction of the autonomic centres of the brain (e.g., persistent fatigue, headache, irritability, sleep disturbances, impotence, electroencephalographic abnormalities). These findings should be interpreted with caution and further carefully designed epidemiological and clinical research work is needed to confirm the hypothesis of an association between disorders of the central nervous system and exposure to hand-transmitted vibration.
Standards
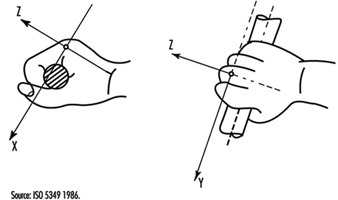
Several countries have adopted standards or guidelines for hand-transmitted vibration exposure. Most of them are based on the International Standard 5349 (ISO 1986). To measure hand-transmitted vibration ISO 5349 recommends the use of a frequency-weighting curve which approximates the frequency-dependent sensitivity of the hand to vibration stimuli. The frequency-weighted acceleration of vibration (ah,w) is obtained with an appropriate weighting-filter or by summation of weighted acceleration values measured in octave or one-third octave bands along an orthogonal coordinate system (xh, yh, zh), (figure 1). In ISO 5349 the daily exposure to vibration is expressed in terms of energy-equivalent frequency-weighted acceleration for a period of four hours ((ah,w)eq(4) in m/s2 r.m.s), according to the following equation:
(ah,w)eq(4)=(T/4)½(ah,w)eq(T)
where T is the daily exposure time expressed in hours and (ah,w)eq(T) is the energy-equivalent frequency-weighted acceleration for the daily exposure time T. The standard provides guidance to calculate (ah,w)eq(T) if a typical work-day is characterized by several exposures of different magnitudes and durations. Annex A to ISO 5349 (which does not form part of the standard) proposes a dose-effect relationship between (ah,w)eq(4) and VWF, which can be approximated by the equation:
C=[(ah,w)eq(4) TF/95]2 x 100
where C is the percentile of exposed workers expected to show VWF (in the range 10 to 50%), and TF is the exposure time before finger blanching among the affected workers (in the range 1 to 25 years). The dominant, single-axis component of vibration directed into the hand is used to calculate (ah,w)eq(4), which should not be in excess of 50 m/s2. According to the ISO dose-effect relationship, VWF may be expected to occur in about 10% of workers with daily vibration exposure to 3 m/s2 for ten years.
Figure 1. Basicentric coordinate system for the measurement of hand-transmitted vibration
In order to minimize the risk of vibration-induced adverse health effects, action levels and threshold limit values (TLVs) for vibration exposure have been proposed by other committees or organizations. The American Conference of Government Industrial Hygienists (ACGIH) has published TLVs for hand-transmitted vibration measured according to the ISO frequency-weighting procedure (American Conference of Governmental Industrial Hygienists 1992), (table 4). According to ACGIH, the proposal TLVs concern vibration exposure to which “nearly all workers may be exposed repeatedly without progressing beyond Stage 1 of the Stockholm Workshop Classification System for VWF”. More recently, exposure levels for hand-transmitted vibration have been presented by the Commission of the European Communities within a proposal of a Directive for the protection of workers against the risks arising from physical agents (Council of the European Union 1994), (table 5). In the proposed Directive the quantity used for the assessment of vibration hazard is expressed in terms of an eight-hour energy-equivalent frequency-weighted acceleration, A(8)=(T/8)½ (ah,w)eq(T), by using the vector sum of weighted accelerations determined in orthogonal coordinates asum=(ax,h,w2+ay,h,w2+az,h,w2)½ on the vibrating tool handle or workpiece. The methods of measurement and assessment of vibration exposure reported in the Directive are basically derived from the British Standard (BS) 6842 (BSI 1987a). The BS standard, however, does not recommend exposure limits, but provides an informative appendix on the state of knowledge of the dose-effect relationship for hand-transmitted vibration. The estimated frequency-weighted acceleration magnitudes liable to cause VWF in 10% of workers exposed to vibration according to the BS standard are reported in table 6.
___________________________________________________________________________
Table 4. Threshold limit values for hand-transmitted vibration
|
Total daily exposure (hours) |
Frequency-weighted r.m.s. acceleration in the dominant direction that should not be exceeded |
|
|
|
|
g* |
|
4-8 |
4 |
0.40 |
|
2-4 |
6 |
0.61 |
|
1-2 |
8 |
0.81 |
|
1 |
12 |
1.22 |
* 1 g = 9.81 ![]() .
.
Source: According to the American Conference of Government Industrial Hygienists 1992.
___________________________________________________________________________
Table 5. Proposal of the Council of the European Union for a Council Directive on physical agents: Annex II A. Hand-transmitted vibration (1994)
|
Levels ( |
A(8)* |
Definitions |
|
Threshold |
1 |
The exposure value below which continuous and/or repetitive exposure has no adverse effect on health and safety of workers |
|
Action |
2.5 |
The value above which one or more of the measures** specified in the relevant Annexes must be undertaken |
|
Exposure limit value |
5 |
The exposure value above which an unprotected person is exposed to unacceptable risks. Exceeding this level is prohibited and must be prevented through the implementation of the provisions of the Directive*** |
* A(8) = 8 h energy-equivalent frequency-weighted acceleration.
** Information, training, technical measures, health surveillance.
*** Appropriate measures for the protection of health and safety.
___________________________________________________________________________
Table 6. Frequency-weighted vibration acceleration magnitudes (![]() r.m.s.) which may be expected to produce finger blanching in 10% of persons exposed*
r.m.s.) which may be expected to produce finger blanching in 10% of persons exposed*
|
Daily exposure (hours) |
Life-time exposure (years) |
|||||
|
|
0.5 |
1 |
2 |
4 |
8 |
16 |
|
0.25 |
256.0 |
128.0 |
64.0 |
32.0 |
16.0 |
8.0 |
|
0.5 |
179.2 |
89.6 |
44.8 |
22.4 |
11.2 |
5.6 |
|
1 |
128.0 |
64.0 |
32.0 |
16.0 |
8.0 |
4.0 |
|
2 |
89.6 |
44.8 |
22.4 |
11.2 |
5.6 |
2.8 |
|
4 |
64.0 |
32.0 |
16.0 |
8.0 |
4.0 |
2.0 |
|
8 |
44.8 |
22.4 |
11.2 |
5.6 |
2.8 |
1.4 |
* With short duration exposure the magnitudes are high and vascular disorders may not be the first adverse symptom to develop.
Source: According to British Standard 6842. 1987, BSI 1987a.
___________________________________________________________________________
Measurement and Evaluation of Exposure
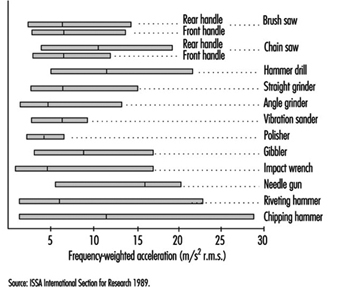
Vibration measurements are made to provide assistance for the development of new tools, to check vibration of tools at purchase, to verify maintenance conditions, and to assess human exposure to vibration at the workplace. Vibration-measuring equipment generally consists of a transducer (usually an accelerometer), an amplifying device, filter (bandpass filter and/or frequency-weighting network), and amplitude or level indicator or recorder. Vibration measurements should be made on the tool handle or workpiece close to the surface of the hand(s) where the vibration enters the body. Careful selection of the accelerometers (e.g., type, mass, sensitivity) and appropriate methods of mounting the accelerometer on the vibrating surface are required to obtain accurate results. Vibration transmitted to the hand should be measured and reported in the appropriate directions of an orthogonal coordinate system (figure 1). The measurement should be made over a frequency range of at least 5 to 1,500 Hz, and the acceleration frequency content of vibration in one or more axes can be presented in octave bands with centre frequencies from 8 to 1,000 Hz or in one-third octave bands with centre frequencies from 6.3 to 1,250 Hz. Acceleration can also be expressed as frequency-weighted acceleration by using a weighting network which complies with the characteristics specified in ISO 5349 or BS 6842. Measurements at the workplace show that different vibration magnitudes and frequency spectra can occur on tools of the same type or when the same tool is operated in a different manner. Figure 2 reports the mean value and the range of distribution of weighted accelerations measured in the dominant axis of power-driven tools used in forestry and industry (ISSA International Section for Research 1989). In several standards hand-transmitted vibration exposure is assessed in terms of four-hour or eight-hour energy-equivalent frequency-weighted acceleration calculated by means of the equations above. The method for obtaining energy-equivalent acceleration assumes that the daily exposure time required to produce adverse health effects is inversely proportional to the square of frequency-weighted acceleration (e.g., if the vibration magnitude is halved then exposure time may be increased by a factor of four). This time dependency is considered to be reasonable for standardization purposes and is convenient for instrumentation, but it should be noted that it is not fully substantiated by epidemiological data (Griffin 1990).
Figure 2. Mean values and range of distribution of frequency-weighted r.m.s. acceleration in the dominant axis measured on the handle(s) of some power tools used in forestry and industry
Prevention
The prevention of injuries or disorders caused by hand-transmitted vibration requires the implementation of administrative, technical and medical procedures (ISO 1986; BSI 1987a). Appropriate advice to the manufacturers and users of vibrating tools should also be given. Administrative measures should include adequate information and training to instruct the operators of vibrating machinery to adopt safe and correct work practices. Since continuous exposure to vibration is believed to increase vibration hazard, work schedules should be arranged to include rest periods. Technical measures should include the choice of tools with the lowest vibration and with appropriate ergonomic design. According to the EC Directive for the safety of machinery (Council of the European Communities 1989), the manufacturer shall make public whether the frequency-weighted acceleration of hand-transmitted vibration exceeds 2.5 m/s2, as determined by suitable test codes such as indicated in the International Standard ISO 8662/1 and its companion documents for specific tools (ISO 1988). Tool maintenance conditions should be carefully checked by periodic vibration measurements. Pre-employment medical screening and subsequent clinical examinations at regular intervals should be performed on vibration-exposed workers. The aims of medical surveillance are to inform the worker of the potential risk associated with vibration exposure, to assess health status and to diagnose vibration-induced disorders at the early stage. At the first screening examination particular attention should be paid to any condition which may be aggravated by exposure to vibration (e.g., constitutional tendency to white finger, some forms of secondary Raynaud’s phenomenon, past injuries to the upper limbs, neurological disorders). Avoidance or reduction of vibration exposure for the affected worker should be decided after considering both the severity of symptoms and the characteristics of the entire working process. The worker should be advised to wear adequate clothing to keep the entire body warm, and to avoid or minimize the smoking of tobacco and the use of some drugs which can affect peripheral circulation. Gloves may be useful to protect the fingers and hands from traumas and to keep them warm. So-called anti-vibration gloves may provide some isolation of the high frequency components of vibration arising from some tools.