Motion sickness, or kinetosis, is not a pathological condition, but is a normal response to certain motion stimuli with which the individual is unfamiliar and to which he or she is, therefore, unadapted; only those without a functioning vestibular apparatus of the inner ear are truly immune.
Motions producing sickness
There are many different types of provocative motion that induce the motion sickness syndrome. Most are associated with aids to locomotion—in particular, ships, hovercraft, aircraft, automobiles and trains; less commonly, elephants and camels. The complex accelerations generated by fairground amusements, such as swings, roundabouts (merry-go-rounds), roller-coasters and so on, can be highly provocative. In addition, many astronauts/cosmonauts suffer from motion sickness (space-motion sickness) when they first make head movements in the abnormal force environment (weightlessness) of orbital flight. The motion sickness syndrome is also produced by certain moving visual stimuli, without any physical motion of the observer; the external visual world display of fixed-base simulators (simulator sickness) or a large-screen projection of scenes taken from a moving vehicle (Cinerama or IMAX sickness) are examples.
Aetiology
The essential characteristics of stimuli that induce motion sickness is that they generate discordant information from the sensory systems that provide the brain with information about the spatial orientation and motion of the body. The principal feature of this discord is a mismatch between the signals provided, principally, by the eyes and inner ear, and those that the central nervous system “expects” to receive and to be correlated.
Several categories of mismatch can be identified. Most important is the mismatch of signals from the vestibular apparatus (labyrinth) of the inner ear, in which the semicircular canals (the specialized receptors of angular accelerations) and the otolith organs (the specialized receptors of translational accelerations) do not provide concordant information. For example, when a head movement is made in a car or aircraft which is turning, both the semicircular canals and the otoliths are stimulated in an atypical manner and provide erroneous and incompatible information, information that differs substantially from that generated by the same head movement in a stable, 1-G gravity environment. Likewise, low-frequency (below 0.5 Hz) linear accelerations, such as occur aboard ship in rough seas or in an aircraft during flight through turbulent air, also generate conflicting vestibular signals and, hence, are a potent cause of motion sickness.
The mismatch of visual and vestibular information can also be an important contributory factor. The occupant of a moving vehicle who cannot see out is more likely to suffer from motion sickness than one who has a good external visual reference. The passenger below deck or in an aircraft cabin senses motion of the vehicle by vestibular cues, but he or she receives visual information only of his or her relative movement within the vehicle. The absence of an “expected” and concordant signal in a particular sensory modality is also considered to be the essential feature of visually induced motion sickness, because the visual motion cues are not accompanied by the vestibular signals that the individual “expects” to occur when subjected to the motion indicated by the visual display.
Signs and symptoms
On exposure to provocative motion, the signs and symptoms of motion sickness develop in a definite sequence, the time scale being dependent upon the intensity of the motion stimuli and the susceptibility of the individual. There are, however, considerable differences among individuals not only in susceptibility, but also in the order in which particular signs and symptoms develop, or whether they are experienced at all. Typically, the earliest symptom is epigastric discomfort (“stomach awareness”); this is followed by nausea, pallor and sweating, and is likely to be accompanied by a feeling of bodily warmth, increased salivation and eructation (belching). These symptoms commonly develop relatively slowly, but with continuing exposure to the motion, there is a rapid deterioration in well-being, the nausea increases in severity and culminates in vomiting or retching. Vomiting may bring relief, but this is likely to be short-lived unless the motion ceases.
There are other more variable features of the motion sickness syndrome. Alteration of respiratory rhythm with sighing and yawning may be an early symptom, and hyperventilation may occur, particularly in those who are anxious about the cause or consequence of their disability. Headache, tinnitus and dizziness are reported, while in those with severe malaise, apathy and depression are not uncommon, and may be of such severity that personal safety and survival are neglected. A feeling of lethargy and somnolence may be dominant following the cessation of provocative motion, and these may be the only symptoms in situations where adaptation to unfamiliar motion takes place without malaise.
Adaptation
With continued or repeated exposure to a particular provocative motion, most individuals show a decrease in the severity of symptoms; typically after three or four days of continuous exposure (as aboard ship or in a space vehicle) they have adapted to the motion and can carry out their normal duties without disability. In terms of the “mismatch” model, this adaptation or habituation represents the establishment of a new set of “expectations” in the central nervous system. However, on return to a familiar environment, these will no longer be appropriate and symptoms of motion sickness can recur (mal de débarquement) until readaptation occurs. Individuals differ considerably in the rate at which they adapt, the way they retain adaptation and the degree to which they can generalize protective adaptation from one motion environment to another. Unfortunately, a small proportion of the population (probably about 5%) do not adapt, or adapt so slowly that they continue to experience symptoms throughout the period of exposure to provocative motion.
Incidence
The incidence of sickness in a particular motion environment is governed by a number of factors, notably:
- the physical characteristics of the motion (its intensity, frequency and direction of action)
- the duration of exposure
- the intrinsic susceptibility of the individual
- the task being performed
- other environmental factors (e.g., odour).
Not surprisingly, the occurrence of sickness varies widely in different motion environments. For example: nearly all the occupants of life rafts in rough seas will vomit; 60% of student aircrew members suffer from air sickness at some time during training, which in 15%is sufficiently severe to interfere with training; in contrast, less than 0.5% of passengers in civil transport aircraft are affected, although the incidence is higher in small commuter aircraft flying at low altitude in turbulent air.
Laboratory and field studies have shown that for vertical translational oscillatory motion (appropriately called heave), oscillation at a frequency of about 0.2 Hz is the most provocative (figure 1). For a given intensity (peak acceleration) of oscillation, the incidence of sickness falls quite rapidly with an increase in frequency above 0.2 Hz; motion at 1 Hz is less than one-tenth as provocative as that at 0.2 Hz. Likewise, for motion at frequencies below 0.2 Hz, although the relationship between incidence and frequency is not well defined because of a lack of experimental data; certainly, a stable, zero frequency, 1-G environment is not provocative.
Figure 1. Motion sickness incidence as a function of wave frequency and acceleration for 2 hour exposure to vertical sinusoidal motion
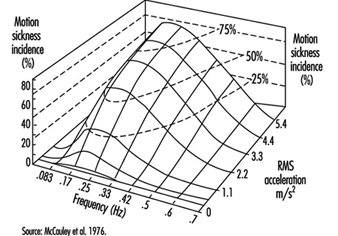
Relationships established between the incidence of symptoms of motion sickness and the frequency, magnitude and duration of heave (z-axis) motion have led to the development of simple formulae that can be used to predict incidence when the physical parameters of the motion are known. The concept, embodied in British Standard 6841 (BSI 1987b) and in ISO Draft International Standard 2631-1, is that the incidence of symptoms is proportional to the Motion Sickness Dose Value (MSDVz). The MSDVz (in m/s1.5) is defined:
MSDVz=(a2t)½
where a is the root-mean-square (r.m.s.) value of the frequency-weighted acceleration (in m/s2) determined by linear integration over the duration, t (in seconds), of exposure to the motion.
The frequency weighting to be applied to the stimulus acceleration is a filter having a centre frequency and attenuation characteristics similar to those depicted in figure 1. The weighting function is defined precisely in the standards.
The percentage of an unadapted adult population (P) who are likely to vomit is given by:
P =1/3 MSDVz
Furthermore, the MSDVz may also be used to predict the level of malaise. On a four-point scale of zero (I felt all right) to three (I felt absolutely dreadful) an “illness rating” (I) is given by:
I =0.02MSDVz
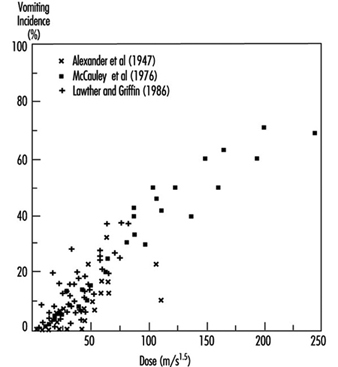
Given the large differences among individuals in their susceptibility to motion sickness, the relationship between MSDVz and the occurrence of vomiting in laboratory experiments and in sea trials (figure 2) is acceptable. It should be noted that the formulae were developed from data acquired on exposures lasting from about 20 minutes to six hours with vomiting occurring in up to 70% of individuals (mostly seated) exposed to vertical, heave, motion.
Figure 2. Relationship between incidence of vomiting and stimulus dose (MSDV2), calculated by the procedure described in the text. Data from laboratory experiments volving vertical oscillation (x) and sea trials (+)
Knowledge about the effectiveness of translational oscillation acting in other body axes and other than in a vertical direction is fragmentary. There is some evidence from laboratory experiments on small groups of subjects that translational oscillation in a horizontal plane is more provocative, by a factor of about two, than the same intensity and frequency of vertical oscillation for seated subjects, but is less provocative, also by a factor of two, when the subject is supine and the stimulus acts in the longitudinal (z) body axis. Application of formulae and weighting characteristics embodied in standards to the prediction of sickness incidence should, therefore, be made with caution and due concern for the constraints noted above.
The considerable variability between individuals in their response to provocative motion is an important feature of motion sickness. Differences in susceptibility can, in part, be related to constitutional factors. Infants much below the age of about two years are rarely affected, but with maturation, susceptibility increases rapidly to reach a peak between four and ten years. Thereafter, susceptibility falls progressively so that the elderly are less likely to be affected, but are not immune. In any age group, females are more sensitive than males, the incidence data suggesting a ratio of approximately 1.7:1. Certain dimensions of personality, such as neuroticism, introversion and perceptual style have also been shown to be correlated, albeit weakly, with susceptibility. Motion sickness can also be a conditioned response and a manifestation of phobic anxiety.
Preventive measures
Procedures which minimize the provocative stimulus or increase the tolerance are available. These may prevent sickness in a proportion of the population, but none, other than withdrawal from the motion environment, is 100%effective. In the design of a vehicle, attention to factors which raise the frequency and reduce the magnitude of the oscillations (see figure 1) experienced by occupants during normal operation is beneficial. The provision of head support and body restraint to minimize the unnecessary head movements is advantageous, and is further aided if the occupant can assume a reclined or supine position. Sickness is less if the occupant can be given a view of the horizon; for those deprived of an external visual reference, closing the eyes reduces visual/vestibular conflict. Involvement in a task, particularly control of the vehicle, is also helpful. These measures can be of immediate benefit, but in the longer term the development of protective adaptation is of the greatest value. This is achieved by continued and repeated exposure to the motion environment, though it can be facilitated by ground-based exercises in which provocative stimuli are generated by making head movements whilst rotating on a spin table (desensitization therapy).
There are several drugs which increase tolerance, though all have side-effects (in particular, sedation), so that they should not be taken by those in primary control of a vehicle or when optimum performance is mandatory. For short-term (less than four hours) prophylaxis, 0.3 to 0.6 mg hyoscine hydrobromide (scopolamine) is recommended; longer acting are the antihistaminics, promethazine hydrochloride (25 mg), meclozine hydrochloride (50 mg), dimenhydrinate (50 mg) and cinnarizine (30 mg). The combination of either hyoscine or promethazine with 25 mg ephedrine sulphate increases prophylactic potency with some reduction of side-effects. Prophylaxis for up to 48 hours can be achieved using a scopolamine patch, which allows the drug to be slowly absorbed through the skin at a controlled rate. Effective concentrations of the drug in the body are not achieved until six to eight hours after application of the patch, so the need for this type of therapy must be anticipated.
Treatment
Those suffering from established motion sickness with vomiting should, when practicable, be placed in a position where the motion stimulus is minimized, and be given an anti–motion sickness drug, preferably promethazine by injection. Should vomiting be prolonged and repeated, intravenous replacement of fluid and electrolytes may be necessary.