- You are here:
-
Home

-
Part XVI. Construction
-
Construction
- Tools, Equipment and Materials
Armed Forces
Nations maintain military forces to deter aggression, discourage conflict and, should the need arise, to be prepared to fight and win their wars. Military forces are also used in non-combat roles that are referred to as “peacetime engagements” or “operations other than war”. These include: humanitarian missions such as emergency disaster assistance; peacemaking and peacekeeping operations; counter-drug and counter-terrorism work; and security assistance.
Men and women of the armed forces work under the sea, on surface ships, above the earth, on all kinds of terrain, in extremes of temperature and at high elevations. Many military jobs relate to maintaining the skills needed to operate equipment unique to the military (like submarines, fighter aircraft and tanks) in action against an armed enemy. The military also has a large number of uniformed people who perform maintenance, repair, administrative, medical and other functions to support those who fight battles.
All military people maintain proficiency in basic military skills, such as marksmanship, and a high level of physical fitness so that they may react appropriately if they become involved in warfare. Exercise programmes are used extensively to develop and maintain strength and aerobic fitness. If used in excess or poorly managed, these programmes may cause excessive injuries.
In addition to their job exposures, uniformed people are often at enhanced risk of acquiring infectious diseases. Basic training camp environments and close living spaces, as found on ships, may contribute to outbreaks of acute respiratory and other infectious diseases. Noise is a universal problem. Also, service in many parts of the world brings with it exposure to contaminated food and water, and to disease vectors carrying protozoan, viral and bacterial agents.
The armed forces rely on many civilian employees to do research and development and provide maintenance, administrative and other support services. Some civilians are paid by the military; others work for companies under contract to the military. In the past, civilian workers did not routinely accompany members of the armed forces into hostile areas. Recently, civilians have been performing many support functions in close proximity to deployed military forces, and may face similar occupational and environmental exposures.
The Fixed Workplace
In many fixed military facilities (such as repair depots, administrative offices and hospitals) uniformed members and civilians perform operations that are similar to those found in non-military workplaces. These include painting; degreasing; welding; grinding; chipping; electroplating; handling hydraulic fluids, fuels and cleaning agents; using microcomputers; and managing patients with infectious diseases. However, performing industrial operations in confined spaces in ships and submarines, or inside armoured vehicles, increases the risk of overexposure to toxicants. Additionally, some work must be done by divers at various depths.
In some fixed facilities, militarily unique items are developed, manufactured, serviced or stored. These items may include: nerve and mustard agent munitions; military explosives, propellants and special fuels, such as hydroxylammonium nitrate; laser range finders and target designators; microwave radiation sources in radar and communications equipment; and ionizing radiation from munitions, armour and nuclear power plants. Composite materials are not militarily unique but are common in military equipment. Where older military equipment is used, workers may be exposed to polychlorinated biphenyls in electrical systems, asbestos in the lagging around steam pipes and lead-based paints.
The Militarily Unique Workplace
People in the armed forces are always on duty, but commanders try to maintain acceptable work-rest cycles. However, battles are not fought on prearranged schedules, and military forces train as they expect to fight. During intense training, fatigue and sleep deprivation are common. The situation is worsened by quickly transporting military forces across time zones and having them perform their jobs immediately upon arrival. In all military operations, and particularly large operations that cover wide areas and involve air, land and sea forces from different countries, there is considerable pressure to maintain effective coordination and communication among the various elements to reduce the risk of accidents, such as placing weapons fire upon a friendly target. Stress is increased if operations result in long family separations, or if the possibility of hostile action exists.
Naval Vessels
On naval vessels, the tight spaces, multiple doors and ladders and narrow passageways close to operating equipment are hazardous. The confined spaces also restrict movement during work and contribute to ergonomic injuries (see figure 1). In submarines, air quality is a major concern that requires constant monitoring and the restriction of unnecessary contaminants. In all military environments where exposure to nuclear power plants, nuclear weapons or other radioactive material may occur, exposures are assessed, controls are implemented and monitoring is conducted as appropriate.
Figure 1. On aircraft carriers, naval flight deck personnel must work in extremely close proximity to operating fixed-wing jets and helicopters, and their associated safety hazards, exhaust combustion products and noise.

US Army
Aircraft
Flight operations in the aerospace environment involve a variety of fixed-wing and rotary-wing (helicopter) aircraft. Military air crews experience exposures that are different from those in the civilian environment. Many military aircraft are unique in their design, flight characteristics and mission performance. Air crew members are frequently at risk of exposure to excessive accelerative forces (centrifugal and gravitational), decompression sickness, circadian desynchrony resulting from long missions or night operations and spatial disorientation. Vibration originating from the aircraft and/or atmospheric turbulence may affect vision, result in motion sickness, produce fatigue and contribute to the development of disorders of the lumbar spine, particularly in helicopter pilots. Exposure to products of combustion from engine exhaust, overheating or burning of aircraft components may pose a toxic hazard if the aircraft is damaged during combat operations. Fatigue is a major concern when flight operations occur over extended periods of time, or involve long distances. Spatial disorientation and illusionary sensations of aircraft attitude and motion can be causes of mishaps, particularly when flights occur at high speeds in close proximity to the ground. Ground crews may be under considerable time pressure to perform maintenance and resupply (often with aircraft engines running) under difficult working conditions.
Helicopters are used extensively in the military as low-altitude weapons systems and observation platforms, and as medical evacuation and utility vehicles. These rotary-wing aircraft are associated with unique physical hazards, mission profiles and physiological implications for air crews. Helicopters have the ability to fly forward, sideward and rearward, but are inherently unstable flight platforms. Consequently, helicopter air crews must maintain constant concentration and have exceptional vision and muscle coordination to operate flight control systems and avoid collisions with terrain and other obstructions during low-level flight.
Fatigue is a serious concern for crew members involved in extended flights, large numbers of short missions and/or low-level, nap-of-the-earth (NOE) flights in which pilots fly as close to terrain contours as the speed and performance contours will allow. Low-level flights at night are particularly challenging. Night vision goggles are commonly used by helicopter pilots in military aviation and law enforcement; however, their use may restrict depth perception, field of view and colour differentiation. Engines, transmissions and rotors of helicopters produce unique vibration spectra which can adversely affect visual acuity and contribute to muscle strain and fatigue. These aircraft components also produce intense noise levels which can disrupt cockpit communications and contribute to hearing loss. Shrouds enclosing noisy components, acoustic blankets as insulation in cockpit/cabin areas and hearing protective devices are used to reduce the risk of hearing loss. Heat stress may be a special problem for helicopter air crews given the lower altitudes at which helicopters operate. Helicopter crashes tend to involve vertical impacts with the ground, often at relatively low forward speeds (in contrast to the longitudinal pattern of fixed-wing aircraft). Compression fractures of the spine and basilar skull fractures are common injuries in crash victims. Design features employed to prevent and control injuries include protective helmets, crash-worthy fuel systems, strengthened cockpit areas to prevent intrusion of the rotor system or transmission, and special seats and restraint systems utilizing shock-absorbing devices.
Ground Forces
Ground troops fire rifles, large guns and rockets, and ride in vehicles over rough terrain. At times they work under the cover of smokes produced from fog oil, diesel fuel or other chemicals (see figure 2). Exposures to noise, blast overpressure from large guns, vibration and propellant combustion products are common. Ballistic eye injuries occur but can be prevented by protective eyewear. The possibility of adverse health effects is increased when rockets and large guns are fired in enclosed areas, as in buildings. Armoured vehicle crew compartments are closed spaces where carbon monoxide concentrations may reach thousands of parts per million after weapons firing, and require effective ventilation systems. Heat stress in some vehicles may necessitate the use of cooling vests. Troops may also experience heat stress from wearing special clothing, hoods and masks to protect against chemical and biological agent attacks. These personal protective measures may contribute to accidents because of interference with vision and mobility. In field medical facilities, infection control practices and containment of waste anaesthetic gases may present unique challenges.
Figure 2. This mechanized smoke generator produces a curtain of fog oil smoke through heat evaporation; fog oil may cause a slipping hazard.
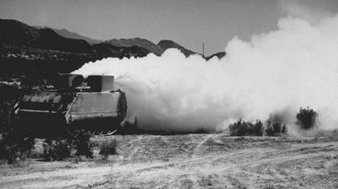
US Army
Military personnel face injury and illness from a variety of weapons. The more conventional weapons produce casualties using projectiles and fragments, blast effects (which may result in lung contusion trauma) and flame and incendiary devices, such as those containing napalm and phosphorus. Eye injuries from lasers may occur accidentally or when lasers are used as offensive weapons. Other weapons systems employ biological material, such as anthrax spores, or chemicals like anticholinesterase agents.
Extensive use of mines has caused concern because of the casualties that have occurred in civilian non-combatants. Narrowly defined, a mine is an explosive ordinance designed to be buried in the ground. In reality, a mine is any hidden explosive that lies in wait and may be detonated by enemy forces, friendly forces, non-combatants or animals. Mines may be employed against matériel or people. Anti-matériel mines are directed at military vehicles and may contain about 5 to 10 kg of explosive, but require 135 kg or more of compressive force to be activated. Antipersonnel mines are designed to maim rather than to kill. Less than 0.2 kg of explosive buried in the ground can blow off a foot. The dirt particles surrounding a mine become missiles that grossly contaminate wounds. The radius in which a mine can produce casualties was expanded with the development of the “pop-up mine”. In these mines a small explosive charge sends a canister about a metre into the air. The canister immediately detonates, spraying fragments to a distance of 35 m. Modern mine designs, like the “Claymore”, can be detonated electrically, by timed fuse or by a trip wire, and can send hundreds of steel spheres, each weighing 0.75 g, over a 60° arc for distances up to 250 m. Within 50 m, gross mutilation and lethal injuries are common.
A range of chemical agents have been employed in warfare. Herbicides (e.g., 2,4-D n-butyl ester mixed with 2,4,5-T n-butyl ester, also known as Agent Orange) were used in Vietnam to control terrain. Some chemicals (e.g., tear gas) have been used as incapacitating agents to produce transient physical or mental effects, or both. Other chemicals are extremely toxic and capable of producing serious injury or death. This category includes the anticholinesterase agents (e.g., Tabun and Sarin), the vesicants or blister agents (e.g., mustard and arsenicals), the lung-damaging or “choking” agents (e.g., phosgene and chlorine) and the blood agents that block the oxidative processes (e.g., hydrogen cyanide and cyanogen chloride).
In addition to armed conflict, other potential sources of exposure to chemical agents include: terrorist activities; storage sites for old military chemical stocks, where leaking containers may occur; sites where military chemical stocks are being destroyed through incineration or other means; and the accidental unearthing of old, forgotten chemical disposal sites.
The Medical Care System
Medical care for the armed forces and civilian workers is focused on prevention. Often, medical personnel study military vehicles and equipment during development to identify potential health hazards to users and maintainers so that these can be controlled. Training and user manuals and educational programmes address protection against hazards. Medical care includes initial medical screening, periodic medical assessment, health education and promotion, and disability evaluations, in addition to primary care and emergency services. Medical personnel also participate in accident investigations. When people deploy to areas presenting new health risks, medical risk assessments are used to identify threats and interventions like vaccines, prophylactic drugs, personnel protective measures and educational programmes.
Medical personnel who provide preventive and primary care to members of the armed forces must be knowledgeable about the characteristics of weapons used in training and on the battlefield to: predict and prepare for the casualties that may occur; take preventive actions that may reduce morbidity and/or mortality; and provide appropriate treatment when casualties do occur. Personal protective equipment is important in defending against chemical and biological agents and eye injuries from missiles and lasers. Other measures to be considered are vaccines and chemoprophylactic drugs for biological agents, and drug pre-treatment and antidotes for chemical agents. Training medical personnel in the early detection and management of illnesses and injuries caused by weapons is critical. Early recognition can result in rapid initiation of appropriate therapy and possibly a reduction in future morbidity and mortality. Also, military surgical staffs are better prepared to take care of their patients and themselves if they are knowledgeable about the wounds they are treating. For example: wounds made by high-velocity rifles often do not require extensive debridement for soft-tissue destruction; wounds made by fragmentation bullets may require extensive exploration; and wounds may contain unexploded munitions.
Security Guards: The Development and State of Occupational Safety in Germany
Growing security needs as a result of generally rising criminal activity, the opening of the borders to the East and within the European Union, as well as the accession of the former German Democratic Republic, have led to a disproportionate growth in the number of commercial guard and security companies as well as the number of employees of these companies in Germany.
At the start of 1995 the number of employees in the more than 1,200 guard and security companies stood at over 155,000. The mid-sized companies have mostly 20 to 200 employees. There are also companies, however, with fewer than 10 employees and others with several thousand. Company mergers are increasingly common.
The Administration Trade Organization is responsible for legal accident insurance for these companies and their employees.
Accident Prevention Regulations
Background of the accident prevention regulations and their scope of application
With the rising occurrence of accidents, the “Guard and Security Services” (VBG 68) Accident Prevention Regulation that had been in force since May 1964 in guard and security work became outdated. It has therefore been reworked and completely redrafted, with the participation of representatives of the affected employers, employees, accident insurance companies, manufacturers’ and trade organizations as well as representatives of the Federal Minister of Labour and Social Questions, the state industrial oversight authorities, the Federal Minister of Defence, the Federal Crime Office, the state police authorities, other institutions and a specialized committee. This committee is an organ of the central office of the Safety and Health Trade Organization of the industrial trade organizations, under the responsibility of the Administration Trade Organization.
The newly drafted accident regulation went into effect 1 October 1990, after several years of consultations. The regulation is the legal standard for all employers and employees in guard and security companies. It lays out duties and lines of authority upon which newly drafted governmental ordinances specific to each specialty are based.
Guard and security work to protect persons and valuables includes:
- private guard duty, such as gate-keepers and park watchmen
- security at construction sites and rail yards
- guarding private property, including factory guards
- guarding military installations and atomic power plants
- ranger and patrol duty on various properties
- security service for performances, trade fairs and expositions
- crowd control
- courier service
- investigative services
- money and valuables transport
- personal protection
- staffing alarm centres
- responding to alarms.
General responsibilities of the employer
The employer or his or her agent may employ only persons who are currently qualified and adequately instructed for the desired guard and security activity. These qualifications are set out in writing.
The conduct of the personnel, including notification of deficiencies and particular dangers, must be regulated with detailed service instructions.
If particular dangers result from guard and security work, adequate supervision of the personnel must be ensured.
Guard and security tasks should be taken on only when avoidable dangers in the working area have been eliminated or secured. To this end, the scope and course of the security, including known side activities, must be set out in writing.
The employer or his or her agent, independent of the client’s duties, must ensure that the property to be secured has been inspected for dangers. Records of these inspections must be kept. These inspections must take place on a regular basis and also immediately when the occasion warrants.
The employer or his or her agent must require of the client that avoidable dangers be eliminated or dangerous locations be secured. Until these security measures are implemented, regulations should be formulated that guarantee the safety of the guard and security personnel in another manner. Inadequately secured danger zones should be excluded from surveillance.
The guard and security personnel must be instructed on the property to be secured and its specific dangers during the time period when the guard and safety activity will take place.
The guard and security personnel must be supplied with all necessary facilities, equipment and resources, especially appropriate footwear, effective flashlights in darkness, as well as personal protective gear in good condition, as needed. The personnel must be adequately instructed in the use of such resources. Equipment and other resources that are worn must not unduly restrict freedom of movement, especially of the hands.
General duties of the employee
Employees must abide by all occupational safety measures and follow the service instructions. They should not accede to any directives from the client that contravene the safety instructions.
Deficiencies and dangers that are discovered, as well as corrective measures taken, must be reported to the employer or his or her agent.
The employees must use the equipment and resources provided appropriately. They may not use or enter installations if not authorized.
Employees must not use alcoholic beverages or other intoxicants while on duty. This also applies for an appropriate time period before work: the employee must start work sober.
Employees who must wear glasses to correct their vision during guard or security work must secure these against loss or bring a replacement pair. This also applies to contact lenses.
Use of dogs
In general, only dogs tested and approved by appropriately certified and competent dog handlers are to be used for guard and security work. Untested dogs should be used only for warning tasks when they are clearly under the control of their handler, but not for additional security tasks. Dogs that have vicious tendencies or that are no longer sufficiently competent must not be used.
Excessive demands should not be put on the dogs. Adequate education and training based on the results of research on animal behaviour must be provided. Proper limits for period of service, minimum rest times and total daily service times need to be set.
The competence of the dog handler must be regularly certified. If the handler is no longer adequately qualified, authorization to handle dogs should be withdrawn.
Regulations must be formulated to guarantee smooth and safe handling of dogs, contact with the dog, the taking over and turning over of the dog, leashing and unleashing, a uniform set of commands used by different handlers, the handling of the leash and conduct when third persons are encountered.
Minimal requirements are prescribed for dog kennels concerning condition and equipping as well as setting access authorization.
When transporting dogs, a separation between transport area and passenger area must be maintained. Car trunks are not suitable under any circumstances. Separate facilities for each dog must be provided.
Use of firearms
Employees must use firearms only on express instructions of the employer or his or her agent, in accordance with all legal requirements and only when the employee is appropriately reliable, suited and trained.
Those carrying firearms must regularly participate in target practice at authorized firing ranges and prove their skill and knowledge. Corresponding records must be kept. If an employee no longer fulfils the requirements, firearms must be withdrawn.
Only officially tested and approved firearms are to be used. The firearms should be tested by experts periodically, and also whenever an inadequacy is suspected; they must be repaired by trained and officially approved persons.
Guards and security personnel must not have or use blank- or gas-firing weapons. In confrontations with armed perpetrators, these weapons provide a false sense of security that leads to extreme danger without adequate possibility of self-defence.
Strict regulations guarantee the flawless and safe use, carrying, transfer, loading and unloading, and storage of firearms and ammunition.
Transporting money and valuables
Due to the high risk of robbery, at least two couriers must be employed for transporting money in publicly accessible areas. One of these must be exclusively occupied with security. This applies also to the couriers’ movements between money transport vehicles and the locations where the money is picked up or delivered.
Exceptions are permitted only if: (1) the money transport is not recognizable by outsiders as a transport of money either from the clothing or equipment of the personnel, or from the vehicle used, the route taken or the course of the transport; (2) the incentive for robbery is significantly reduced by technical equipment that must be clearly recognizable by outsiders; or (3) only coin is being transported, and this is clearly recognizable by outsiders from the conduct and course of the transport.
Technical equipment that considerably reduces the incentive for robbery includes, for example, devices that either constantly or during the entire transport are firmly attached to the money transport container and that, in the case of a forced conveyance or snatching during delivery, automatically either immediately or after a timed delay set off an optical alarm by means of a release of coloured smoke. Additional devices such as simultaneous acoustic alarms are advisable.
The design, form, size and weight of money transport containers must be adequately manageable for carrying. They must not be attached to the courier, as this poses an increased risk.
Money transport with vehicles should in general be carried out only in vehicles specially secured for this purpose. These vehicles are adequately secured when their construction and equipment meet the requirements of Accident Prevention Regulation “Vehicles” (VBG 12) and especially the “Safety Rules for Money Transport Vehicles” (ZH1/209).
Money transport in unsecured vehicles is permissible only when exclusively coin, clearly recognizable as such, is being transported, or it is completely unrecognizable as a transport of money. In this case neither the clothing nor equipment of the personnel, nor the construction, equipping or markings of the vehicle used should indicate that money is being transported.
Transport times and routes as well as loading and unloading locations needs to be varied. Money transport vehicles must also be constantly occupied by at least one person behind barred doors during loading and unloading in public areas.
Alarm centres and vaults
Alarm centres and vaults must be adequately secured against assault. The minimal requirements are the Accident Prevention Regulation “Tellers’ windows” (VBG 120), which governs securing and equipping credit and money-changing institutions that deal with cash.
Final Considerations
There are practical limits in all attempts to improve occupational safety. This is especially clear in guard and security work. Whereas in other areas, structural measures and improvements lead to success, these play only a secondary role in guard and security work. Significant improvements in this area ultimately can be achieved only by changing the company organizational structure and human conduct. The newly drafted Accident Prevention Regulation “Guard and Security Services” (VBG 68), which may seem exaggerated and too detailed on superficial viewing, nevertheless takes this basic knowledge into very particular consideration.
Thus it is not surprising that since regulations have taken effect, the reportable accidents and occupational diseases in commercial guard and security companies have declined by about 20%, despite the generally increasing crime rate. Some companies which have especially conscientiously implemented the Accident Prevention Regulation, and additionally have voluntarily applied supplementary security measures based on a criteria catalogue that is available, were able to register decreases in occurrences of accidents and occupational diseases of up to 50%. This was especially true in the use of dogs.
Furthermore, the totality of the measures taken led to a reduction in the mandatory premiums for legal accident insurance for commercial guard and security companies, despite rising costs.
Overall it is clear that secure conduct can be achieved in the long run only with precise norms and organizational regulations, as well as through constant training and checking.
Law Enforcement
Law enforcement is difficult, stressful, demanding work. There is evidence that much of the work is sedentary, but the small part of the work which is not sedentary is physically demanding. This is also the part of the work which is often the most critical. In this respect, police work has been likened to the work of a lifeguard at a swimming pool. Most of the time, the lifeguard is watching from the water’s edge, but when it is necessary to intervene the emotional and physical demands are extreme and there is usually no warning. Unlike the lifeguard, the police officer may be exposed to attack with a knife or a gun, and may be exposed to intentional violence from some members of the public. Routine activities include patrolling streets, subways, country roads, parks and many other areas. Patrols may be carried out on foot, in vehicles (such as automobiles, helicopters or snowmobiles) and sometimes on horseback. There is a need for constant vigilance and, in many parts of the world, there is the constant threat of violence. Police officers may be called upon to provide assistance to the public in cases of robbery, riot, assault or domestic disputes. They may be involved in crowd control, search and rescue, or assistance to the public in the event of natural disaster. There is an episodic need to chase criminals on foot or in a vehicle, to grapple with, tackle and control criminals and, occasionally, to resort to the use of a lethal weapon. Routine activities can escalate to life-threatening violence with little or no warning. Some police officers work undercover, sometimes for prolonged periods. Others, particularly forensic specialists, are exposed to toxic chemicals. Almost all are exposed to biohazard risk from blood and body fluids. Police officers usually work shifts. Often their shifts are extended by administrative work or court appearances. The actual physical demands of police work and the physical tasks of policing have been extensively studied and are remarkably similar in different police forces and different geographical locations. The question of whether any specific medical condition may be attributable to the occupation of policing is controversial.
Violence
Violence is, unfortunately, a reality of police work. In the United States the homicide rate for police is more than double that for the general population. Work-related violent assault is common among police officers. The particular activities that are likely to result in violent conflict have been the subject of much recent research. The notion that domestic dispute calls were particularly dangerous has been seriously questioned (Violanti, Vena and Marshall 1986). More recently, the activities most likely to result in the assault of a police officer were ranked as follows: First, arresting/controlling suspects; second, robbery in progress; and third, domestic dispute.
The type of violence to which police officers are exposed varies from one country to another. Firearms are more common in the United States than Britain or Western Europe. Countries where political unrest is recent may see police officers exposed to attack from large-calibre or automatic-fire weaponry of a military type. Knife wounds are encountered everywhere, but large-blade knives, particularly machetes, seem more common in tropical countries.
Police officers must maintain a high level of physical fitness. Police training must include training in the physical control of suspects where necessary, as well as training in the use of firearms and other types of tools such as CS gas, pepper spray or hand-held batons. Personal protective equipment such as the “bullet proof” vest is necessary in some communities. Similarly, a communication system that allows the police officer to summon assistance is often important. The most important training, however, must be in the prevention of violence. Current police theory underscores the idea of community policing, with the police officer an integral part of the community. It is to be hoped that as this approach replaces the philosophy of armed military incursion into the community, the need for weaponry and for armour will be reduced.
The sequelae of violence need not be physical. Violent encounters are exceedingly stressful. This stress is particularly likely if the incident has resulted in serious injury, bloodshed or death. Particularly important is the assessment for post-traumatic stress disorder (PTSD) after such incidents.
Emotional and Psychological Stress
It is apparent that police work is stressful. For many police officers the excess of paperwork, as opposed to active law enforcement, is seen as a major stressor. The combination of shiftwork and the uncertainty about what may happen during the shift provides a powerfully stressful situation. In times of fiscal restraint, these stressors are often dramatically amplified by inadequate staffing and inadequate equipment. Situations where there is a potential for violence are stressful in themselves; the stress is dramatically increased where staffing is such that there is inadequate back-up, or when the police officer is seriously overworked.
In addition, the high stress levels which may result from police work have been blamed for marital difficulties, alcohol abuse and suicides among police officers. Much of the data supporting such associations are variable from one geographic region to another. Nevertheless, these problems may well result from the occupation of police work in some cases.
The need for constant vigilance for evidence of stress-related problems or post-traumatic stress disorder cannot be overemphasized. Stress-related disease may manifest as behavioural problems, marital or family problems or, sometimes, as alcohol or substance abuse.
Atherosclerotic Heart Disease
There have been numerous studies suggesting that atherosclerotic disease is more common among police officers (Vena et al. 1986; Sparrow, Thomas and Weiss 1983); there are also studies suggesting that this is not the case. It has been suggested that the increase in the prevalence of heart disease among police officers was almost entirely due to the increased risk of acute myocardial infarction.
This is intuitively satisfying since it is well known that sudden exertion, in the face of underlying heart disease, is an important risk factor for sudden death. The functional job analysis for a general-duty constable clearly indicates that a police officer may be expected, in the course of duty, to go from the sedentary state to maximal exertion with little or no warning and with no preparation. Indeed, much police work is sedentary, but, when required, the police officer is expected to run and chase, to grapple and tackle, and to forcibly subdue a suspect. It is therefore not unexpected that even if the rate of underlying coronary disease is not much different among police officers than the rest of the population, the risk of suffering an acute myocardial infarction, because of the nature of the work, may well be higher (Franke and Anderson 1994).
The demographics of the police population must be considered when assessing the risks for heart disease. Heart disease is most commonly found among middle-aged men, and this group makes up a very large proportion of police officers. Women, who have a significantly lower rate of heart disease during their premenopausal years, are significantly under-represented in the demographics of most police forces.
If one is to effectively reduce the risk of cardiac disease in police officers, the regular assessment of the police officer, by a physician knowledgeable about police work and the potential cardiac risks that are associated with police work, is essential (Brown and Trottier 1995). The periodic health assessment must include health education and counselling about cardiac risk factors. There is good evidence that work-based health promotion programmes have a salutary effect on employee health and that the modification of cardiac risk factors reduces the risks of cardiac death. Smoking cessation programmes, nutritional advice, hypertension awareness and cholesterol monitoring and modification are all appropriate activities that will help modify risk factors for cardiac disease among police officers. Regular exercise may be particularly important in police work. The generation of a work environment that educates the worker about positive nutritional and lifestyle choices and that encourages such choices is likely to be beneficial.
Lung Disease in Police Work
The evidence suggests that the prevalence of lung disease in police work is lower than in the general population. There is, however, evidence of an increased rate of cancer of the respiratory system. The majority of police officers are not routinely exposed to inhaled toxins at a rate any greater than other residents of the communities they police. There are exceptions to this general rule, however, the most notable exception being police officers working in forensic identification. There is good evidence that these individuals may suffer from an increased prevalence of respiratory symptoms and, possibly, occupational asthma (Souter, van Netten and Brands 1992; Trottier, Brown and Wells 1994). Cyanoacrylate, used in uncovering latent fingerprints, is a known respiratory sensitizer. In addition to this, there are a large number of chemical carcinogens routinely used in this type of work. For these reasons it is recommended that police officers who work in forensic identification, particularly those who do fingerprint work, should undergo annual chest x ray and spirometry. Similarly, periodic health assessment of these officers must include a careful assessment of the respiratory system.
Even though the practice of smoking cigarettes is becoming less common, a significant number of police officers continue to smoke. This may be the reason why some studies have shown an increased risk of lung and laryngeal cancers among police officers. Smoking is, of course, a major risk factor for cardiac disease. It is also the leading cause of lung cancer. When a police officer gets lung cancer the question frequently asked is whether the cancer is due to occupational exposure, in particular to the carcinogens known to be present in fingerprint powders. If the police officer smokes, it will be impossible to confidently assign blame to any occupational exposure. In summary, respiratory disease is not normally an occupational hazard of police work except for forensic identification workers.
Cancer
There is some evidence that police officers suffer a somewhat higher risk of cancer than expected in the general population. In particular, the risk of digestive tract cancers such as cancer of the oesophagus, cancer of the stomach and cancer of the large bowel is reported to be elevated among police officers. There may be an increased risk of cancer of the lung and larynx. The risk of cancer among police officers working in forensic identification and forensic laboratory work has been briefly discussed above. The controversial issue of testicular cancer associated with the use of police “radar” to detect speeders must also be addressed.
The data suggesting an increase in the risk of cancer of the digestive tract among police officers is scant, but it is a question that must be seriously examined. In the case of lung and oesophageal cancer, it is difficult to see how the activities of police work would be expected to increase the risk. Smoking, of course, is known to increase the risk of both lung and oesophageal cancer, and significant numbers of police officers are known to continue to smoke cigarettes. Another substance known to increase the risk of oesophageal cancer is alcohol, particularly whisky. Police work is known to be exceedingly stressful, and there have been some studies that suggest police officers may sometimes use alcohol to relieve the tension and stress of their work.
The same research that demonstrated an increased risk of cancers of the digestive tract also demonstrated a peculiar increase in the incidence of cancers of the lymphatic and haemopoietic systems in some police officers. The increased risk was restricted to one group and the overall risk was not elevated. Given this very peculiar distribution, and the small numbers, this finding may well turn out to be a statistical aberration.
The risk of cancer among police officers involved in forensic identification work and forensic laboratory work has been discussed. The expected toxicities of chronic low-level exposure to various chemicals are determined by the level of exposure and the use of personal protective equipment. Based on these exposures a periodic health examination has been developed, performed annually and tailored to risks specific for these exposures.
Recent work has suggested a possible increase in the risk of skin cancer, including melanoma, among police officers. Whether this is due to the amount of sun exposure experienced by some police officers who work out of doors is purely speculative.
The question of cancer resulting from exposure to microwaves from “police radar” units has created much controversy. There is certainly some evidence that there may be clustering of certain kinds of cancers among police officers exposed (Davis and Mostofi 1993). The particular concern is about exposure from hand-held units. Alternatively, recent work with large populations refutes any risk of carcinogenicity from exposure to these units. Testicular cancer, in particular, has been reported to be associated with such exposure. The circumstance said to pose the greatest risk is that where the hand-held unit is turned on and resting on the lap of the police officer. This could result in considerable cumulative exposure of the testes over the long term. Whether such exposure causes cancer remains unproven. In the meantime it is recommended that police radar units be mounted outside the police car, be directed away from the police officer, not be used inside the car, be turned off when not in use and be tested regularly for microwave leakage. In addition the periodic examination of police officers should include careful palpation of the testes.
Back Pain
Low-back pain is a major cause of absenteeism throughout the Western world. It is a condition most common among middle-aged males. The factors which predispose to chronic low-back pain are multiple and some, such as the correlation to smoking, seem intuitively difficult to comprehend.
With respect to the occupation of driving, there is ample evidence that individuals who drive for a living are at a dramatically increased risk of low-back pain. This observation includes police officers for whom driving plays a significant part in their daily work. The majority of police cars continue to be equipped with the seats that were installed at the time of their manufacture. Various back supports and prosthetic devices are available which may improve the support of the lumbar spine, but the problem remains.
There is evidence that physical confrontation may play a role in the development of back pain. Motor vehicle accidents, particularly in police vehicles, may play a part. Some police equipment, such as thick leather belts festooned with heavy equipment, may also play a role.
It is important to remember that stress may precipitate or exacerbate back pain and that back pain, as a reason for sick-leave, may be perceived by some police officers as more acceptable than the need to recover from emotional trauma.
There is no doubt that specific exercises designed to maintain flexibility and strengthen the muscles of the back can significantly improve function and symptoms. Numerous classification systems of back pain have been promulgated. These different patterns of pain have distinct approaches of active intervention through specific muscle strengthening programmes. It is important that specific symptom patterns be sought out among police officers and that appropriate intervention and treatment be initiated. This requires periodic assessment by physicians knowledgeable in this clinical syndrome and capable of early effective intervention. It is equally important that a good level of overall fitness be maintained in order to avoid disability from this common chronic, costly syndrome.
Biohazard Risks
There are reports of police officers said to have contracted AIDS from their work. In May 1993 the US Federal Bureau of Investigations reported that there had been seven cases of police officers contacting AIDS through their work over 10 years (Bigbee 1993). Let us begin by noting that this is a surprisingly small number of cases over a 10-year period in the entire United States. Let us next observe that there was some controversy about whether these cases were all to be considered job-related. Nevertheless, it is clearly possible to become infected with HIV as a result of police work.
Since there is no cure for AIDS, and no vaccine that prevents the disease, the best defence a police officer has against this infection is prevention. Latex gloves should be worn, whenever possible, any time that contact with blood or blood-contaminated evidence is foreseen. This is especially important if there are any skin breaks on the hands.
Any open sores or cuts that a police officer has sustained must be kept covered with an occlusive dressing while on duty. Needles should be handled with extreme care, and needles or syringes must be transported in a sharps container that can effectively prevent the needle from penetrating through the container. Sharp edges must be avoided and sharp exhibits handled with extreme care, particularly when contaminated with fresh blood. Where possible, such exhibits should be picked up with instruments rather than by hand.
Latex gloves and a barrier mask should be used if resuscitation attempts are undertaken, and latex gloves must always be worn when rendering first aid. It is important to bear in mind, however, that the risk of becoming infected with HIV from resuscitation procedures is very remote.
There are also some traditional techniques in policing that must be avoided. “Pat down” searches are dangerous to the police officer. There are numerous cases of police officers suffering needle stick injuries from this type of procedure. Also dangerous is searching containers, bags or even pockets by rummaging through them. All containers must be emptied into a flat surface and their contents examined in plain view. Similarly sweep searches under car seats and between seats and backs of couches and chairs must not be performed. It is preferable to dismantle furniture rather than have police officers putting their hands blindly in places where needles and syringes may be hidden. Latex gloves do not protect from needlestick injury.
Eye protection and face masks may be appropriate in circumstances where spatter of body fluid such as saliva or blood can reasonably be foreseen. There must be a system in place for the safe disposal of personal protective equipment. There must be a facility for police officers to wash their hands. Given the fact that few patrol cars have running water and sinks, prepackaged washing solutions for cleaning skin should be provided. Lastly, the question of what should be done for a police officer who, in spite of all the best precautions, suffers a percutaneous exposure to HIV should be asked. After appropriate wound care the first step is to try to determine whether the source of the exposure is truly HIV positive. This is not always possible. Secondly, it is imperative that the police officer be educated about the true risks of infection. Many non-medical personnel assume that the risk is much higher than it really is. Thirdly, the police officer must be informed of the need to retest for at least six months and possibly nine months in order to ensure that the officer has not been infected. Steps must be taken to prevent potential infection of the officer’s sexual partner(s) for at least six months. Lastly, the question of post-exposure prophylaxis must be discussed. There is increasing evidence that prophylaxis with antiviral drugs may be helpful in reducing the risk of seroconversion after percutaneous exposure. These are discussed elsewhere in the Encyclopaedia. In addition, the area of prophylaxis is under intense research scrutiny so that current references must be consulted to assure the most appropriate approach.
There are numerous case reports of occupationally acquired hepatitis among law enforcement personnel. The quantitative risk is not dramatically high when compared to other occupations. Nevertheless it is a real risk and must be seen as a possible occupational disease. The preventive approach to HIV infection that was outlined above applies equally well to the blood-borne disease hepatitis B. Given the fact that hepatitis B is so much more contagious than AIDS, and more likely to cause disease or death in the short term, this disease ought to be an even more compelling reason for following universal precautions.
There is an effective vaccine against hepatitis B. All police officers regardless of whether they are involved in forensics or general-duty policing, should be vaccinated against hepatitis B. Other conditions, including hepatitis C, tuberculosis and airborne pathogens, may also be encountered by police officers.
Firefighting Hazards
We thank the Edmonton Fire-fighters’ Union for their interest and generous support of the development of this chapter. The “Edmonton Sun” and the “Edmonton Journal” graciously allowed their news photographs to be used in the articles on firefighting. Ms. Beverly Cann of the Manitoba Federation of Labour Occupational Health Centre contributed invaluable advice on the article on paramedical personnel and ambulance attendants.
Fire-brigade personnel may be engaged on a full-time, part-time, paid-on-call or unpaid, volunteer basis—or on a combination of these systems. The type of organization employed will, in most cases, depend on the size of the community, the value of the property to be protected, the types of fire risk and the number of calls typically answered. Cities of any appreciable size require regular fire brigades with full crews on duty equipped with the appropriate apparatus.
Smaller communities, residential districts and rural areas having few fire calls usually depend upon volunteer or paid-on-call fire-fighters for either full staffing of their firefighting apparatus or to assist a skeleton force of full-time regulars.
Although there are a great many efficient, well equipped volunteer fire departments, full-time, paid fire departments are essential in larger communities. A call or volunteer organization does not lend itself as readily to the continuous fire-prevention inspection work that is an essential activity of modern fire departments. Using volunteer and call systems, frequent alarms may call out workers who hold other jobs, causing a loss of time with seldom any direct benefit to employers. Where full-time fire-fighters are not employed, the volunteers must come to a central fire hall before response can be made to a call, causing a delay. Where there are only a few regulars, a supplementary group of well-trained call or volunteer fire-fighters should be provided. There should be a reserve arrangement that make assistance available for the response of neighbouring departments on a mutual-aid basis.
Firefighting is a highly unusual occupation, in that it is perceived of as dirty and dangerous but is indispensable and even prestigious. Fire-fighters enjoy public admiration for the essential work that they do. They are well aware of the hazards. Their work involves intermittent periods of exposure to extreme physical and psychological stress on the job. Fire-fighters are also exposed to serious chemical and physical hazards, to a degree unusual in the modern workforce.
Hazards
Occupational hazards experienced by fire-fighters may be categorized as physical (mostly unsafe conditions, thermal stress and ergonomic stress), chemical and psychological. The level of exposure to hazards that may be experienced by a fire-fighter in a given fire depends on what is burning, the combustion characteristics of the fire, the structure that is on fire, the presence of non-fuel chemicals, the measures taken to control the fire, the presence of victims that require rescue and the position or line of duty held by the fire-fighter while fighting the fire. The hazards and levels of exposure experienced by the first fire-fighter to enter a burning building are also different from those of the fire-fighters who enter later or who clean up after the flames are extinguished. There is usually rotation among the active firefighting jobs in each team or platoon, and a regular transfer of personnel between fire halls. Fire-fighters may also have special rank and duties. Captains accompany and direct the crews but are still actively involved in fighting the fire on site. Fire chiefs are the heads of the fire service and are called out only in the worst fires. Individual fire-fighters may still experience unusual exposures in particular incidents, of course.
Physical hazards
There are many physical dangers in firefighting that can lead to serious physical injury. Walls, ceilings and floors can collapse abruptly, trapping fire-fighters. Flashovers are explosive eruptions of flame in a confined space that occur as a result of the sudden ignition of flammable gas products driven out of burning or hot materials and combined with superheated air. Fire situations that lead to flashovers may engulf the fire-fighter or cut off escape routes. The extent and number of injuries can be minimized by intensive training, job experience, competency and good physical fitness. However, the nature of the job is such that fire-fighters may be placed in dangerous situations by miscalculation, circumstance or during rescues.
Some fire departments have compiled computerized databases on structures, materials and potential hazards likely to be encountered in the district. Quick access to these databases assists the crew in responding to known hazards and anticipating possibly dangerous situations.
Thermal hazards
Heat stress during firefighting may come from hot air, radiant heat, contact with hot surfaces or endogenous heat that is produced by the body during exercise but which cannot be cooled during the fire. Heat stress is compounded in firefighting by the insulating properties of the protective clothing and by physical exertion, which result in heat production within the body. Heat may result in local injury in the form of burns or generalized heat stress, with the risk of dehydration, heat stroke and cardiovascular collapse.
Hot air by itself is not usually a great hazard to the fire-fighter. Dry air does not have much capacity to retain heat. Steam or hot, wet air can cause serious burns because much more heat energy can be stored in water vapour than in dry air. Fortunately, steam burns are not common.
Radiant heat is often intense in a fire situation. Burns may occur from radiant heat alone. Fire-fighters may also show skin changes characteristic of prolonged exposure to heat.
Chemical hazards
Over 50% of fire-related fatalities are the result of exposure to smoke rather than burns. One of the major contributing factors to mortality and morbidity in fires is hypoxia because of oxygen depletion in the affected atmosphere, leading to loss of physical performance, confusion and inability to escape. The constituents of smoke, singly and in combination, are also toxic. Figure 1 shows a fire-fighter using self-contained breathing apparatus (SCBA) rescuing an unprotected fire-fighter who was trapped in a very smoky fire in a tire warehouse. (The fire-fighter being rescued ran out of air, took off his SCBA to breathe as best he could, and was fortunate enough to be rescued before it was too late.)
Figure 1. Fire-fighter rescuing another fire-fighter who was trapped in the toxic smoke from a fire in a tire warehouse.

All smoke, including that from simple wood fires, is hazardous and potentially lethal with concentrated inhalation. Smoke is a variable combination of compounds. The toxicity of smoke depends primarily on the fuel, the heat of the fire and whether or how much oxygen is available for combustion. Fire-fighters on the scene of a fire are frequently exposed to carbon monoxide, hydrogen cyanide, nitrogen dioxide, sulphur dioxide, hydrogen chloride, aldehydes and organic compounds such as benzene. Different gas combinations present different degrees of hazard. Only carbon monoxide and hydrogen cyanide are commonly produced in lethal concentrations in building fires.
Carbon monoxide is the most common, characteristic and serious acute hazard of firefighting. Carboxyhaemoglobin accumulates rapidly in the blood with duration of exposure, as a result of the affinity of carbon monoxide for haemoglobin. High levels of carboxyhaemoglobin may result, particularly when heavy exertion increases minute ventilation and therefore delivery to the lung during unprotected firefighting. There is no apparent correlation between the intensity of smoke and the amount of carbon monoxide in the air. Fire-fighters should particularly avoid cigarette smoking during the clean-up phase, when burning material is smouldering and therefore burning incompletely, as this adds to the already elevated levels of carbon monoxide in the blood. Hydrogen cyanide is formed from the lower temperature combustion of nitrogen-rich materials, including natural fibres such as wool and silk, as well as common synthetics such as polyurethane and polyacrylonitrile.
Light-molecular-weight hydrocarbons, aldehydes (such as formaldehyde) and organic acids may be formed when hydrocarbon fuels burn at lower temperatures. The oxides of nitrogen are also formed in quantity when temperatures are high, as a consequence of the oxidation of atmospheric nitrogen, and in lower temperature fires where the fuel contains significant nitrogen. When the fuel contains chlorine, hydrogen chloride is formed. Polymeric plastic materials pose particular hazards. These synthetic materials were introduced into building construction and furnishings in the 1950s and thereafter. They combust into particularly hazardous products. Acrolein, formaldehyde and volatile fatty acids are common in smouldering fires of several polymers, including polyethylene and natural cellulose. Cyanide levels increase with temperature when polyurethane or polyacrylonitriles are burned; acrylonitrile, acetonitrile pyridine and benzonitrile occur in quantity above 800 but below 1,000 °C. Polyvinyl chloride has been proposed as a desirable polymer for furnishings because of its self-extinguishing characteristics due to the high chlorine content. Unfortunately, the material produces large quantities of hydrochloric acid and, sometimes, dioxins when fires are prolonged.
Synthetic materials are most dangerous during smouldering conditions, not in conditions of high heat. Concrete retains heat very efficiently and may act as a “sponge” for trapped gases that are then released from the porous material, releasing hydrogen chloride or other toxic fumes long after a fire has been extinguished.
Psychological hazards
A fire-fighter enters a situation that others are fleeing, walking into immediate personal danger greater than in almost any other civilian occupation. There is much that can go wrong in any fire, and the course of a serious fire is often unpredictable. Besides personal security, the fire-fighter must be concerned with the safety of others threatened by the fire. Rescuing victims is an especially stressful activity.
The professional life of a fire-fighter is more than an endless round of anxious waiting punctuated by stressful crises, however. Fire-fighters enjoy the many positive aspects of their work. Few occupations are so respected by the community. Job security is largely assured in urban fire departments once a fire-fighter is hired, and the pay usually compares well with other jobs. Fire-fighters also enjoy a strong sense of team membership and group bonding. These positive aspects of the job offset the stressful aspects and tend to protect the fire-fighter against the emotional consequences of repeated stress.
At the sound of an alarm, a fire-fighter experiences a degree of immediate anxiety because of the inherent unpredictability of the situation he or she is about to encounter. The psychological stress experienced at this moment is as great and perhaps greater than any of the stresses that follow during the course of responding to an alarm. Physiological and biochemical indicators of stress have shown that fire-fighters on duty have sustained psychological stress that reflects subjectively perceived patterns of psychological stress and activity levels at the station.
Health Risks
The acute hazards of firefighting include trauma, thermal injury and smoke inhalation. The chronic health effects that follow recurrent exposure have not been so clear until recently. This uncertainty has led to a patchwork of employment and workers’ compensation board policies. The occupational risks of fire-fighters have received a great deal of attention because of their known exposure to toxic agents. A large body of literature has developed on the mortality experience of fire-fighters. This literature has grown with the addition of several substantial studies in recent years, and a sufficient database is now available to describe certain patterns in the literature.
The critical compensation issue is whether a general presumption of risk can be made for all fire-fighters. This means that one must decide whether all fire-fighters can be assumed to have an elevated risk of a particular disease or injury because of their occupation. To satisfy the usual compensation standard of proof that the occupational cause must be more likely than not responsible for the outcome (giving the benefit of the doubt to the claimant), a general presumption of risk requires a demonstration that the risk associated with occupation must be at least as great as the risk in the general population. This can be demonstrated if the usual measure of risk in epidemiological studies is at least double the expected risk, making allowances for uncertainty in the estimate. Arguments against presumption in the specific, individual case under consideration are called “rebuttal criteria”, because they can be used to question, or rebut, the application of the presumption in an individual case.
There are a number of unusual epidemiological characteristics that influence the interpretation of studies of fire-fighters and their occupational mortality and morbidity. Fire-fighters do not show a strong “healthy worker effect” in most cohort mortality studies. This may suggest an excess mortality from some causes compared to the rest of the healthy, fit workforce. There are two types of healthy worker effect that may conceal excess mortality. One healthy worker effect operates at the time of hire, when new workers are screened for firefighting duty. Because of the strenuous fitness requirements for duty, this effect is very strong and might be expected to have an effect of reducing mortality from cardiovascular disease, especially in the early years following hire, when few deaths would be expected anyway. The second healthy worker effect occurs when workers become unfit following employment due to obvious or subclinical illness and are reassigned to other duties or are lost to follow-up. Their relative high contribution to total risk is lost by undercount. The magnitude of this effect is not known but there is a strong evidence that this effect occurs among fire-fighters. This effect would not be apparent for cancer because, unlike cardiovascular disease, the risk of cancer has little to do with fitness at the time of hire.
Lung Cancer
Lung cancer has been the most difficult cancer site to evaluate in epidemiological studies of fire-fighters. A major issue is whether the large-scale introduction of synthetic polymers into building materials and furnishings after about 1950 increased the risk of cancer among fire-fighters because of exposure to the combustion products. Despite the obvious exposure to carcinogens inhaled in smoke, it has been difficult to document an excess in mortality from lung cancer big enough and consistent enough to be compatible with occupational exposure.
There is evidence that work as a fire-fighter contributes to risk of lung cancer. This is seen mostly among fire-fighters who had the highest exposure and who worked the longest time. The added risk may be superimposed on a greater risk from smoking.
Evidence for an association between firefighting and lung cancer suggests that the association is weak and does not attain the attributable risk required to conclude that a given association is “more likely than not” due to occupation. Certain cases with unusual characteristics may warrant this conclusion, such as cancer in a relatively young non-smoking fire-fighter.
Cancer at Other Sites
Other cancer sites have been shown recently to be more consistently associated with firefighting than lung cancer.
The evidence is strong for an association with genito-urinary cancers, including kidney, ureter and bladder. Except for bladder, these are rather uncommon cancers, and the risk among fire-fighters appears to be high, close to or in excess of a doubled relative risk. One could therefore consider any such cancer to be work-related in a fire-fighter unless there is a convincing reason to suspect otherwise. Among the reasons one might doubt (or rebut) the conclusion in an individual case would be heavy cigarette smoking, prior exposure to occupational carcinogens, schistosomiasis (a parasitic infection—this applies to bladder only), analgesic abuse, cancer chemotherapy and urologic conditions that result in stasis and prolonged residence time of urine in the urinary tract. These are all logical rebuttal criteria.
Cancer of the brain and central nervous system has shown highly variable findings in the extant literature, but this is not surprising since the numbers of cases in all reports are relatively small. It is unlikely that this association will be clarified any time soon. It is therefore reasonable to accept a presumption of risk for fire-fighters on the basis of current evidence.
The increased relative risks for lymphatic and haematopoietic cancers appear to be unusually high. However, the small numbers of these relatively rare cancers make it difficult to evaluate the significance of the association in these studies. Because they are individually rare, epidemiologists group them together in order to make statistical generalizations. The interpretation is even more difficult because grouping these very different cancers together makes little sense medically.
Heart Disease
There is no conclusive evidence for an increased risk of death overall from heart disease. Although a single large study has shown an excess of 11%, and a smaller study confined to ischemic heart disease suggested a significant excess of 52%, most studies cannot conclude that there is a consistently increased population risk. Even if the higher estimates are correct, the relative risk estimates still fall far short of what would be required to make a presumption of risk in the individual case.
There is some evidence, primarily from clinical studies, to suggest a risk of sudden cardiac decompensation and risk of a heart attack with sudden maximal exertion and following exposure to carbon monoxide. This does not seem to translate into an excess risk of fatal heart attacks later in life, but if a fire-fighter did have a heart attack during or within a day after a fire it would be reasonable to call it work-related. Each case must therefore be interpreted with a knowledge of individual characteristics, but the evidence does not suggest a generally elevated risk for all fire-fighters.
Aortic Aneurysm
Few studies have accumulated sufficient deaths among fire-fighters from this cause to achieve statistical significance. Although one study conducted in Toronto in 1993 suggests an association with work as a fire-fighter, it should be considered an unproven hypothesis at present. Should it be ultimately confirmed, the magnitude of risk suggests that it would merit acceptance on a schedule of occupational diseases. Rebuttal criteria would logically include severe atherosclerosis, connective tissue disease and associated vasculitis and a history of thoracic trauma.
Lung Disease
Unusual exposures, such as intense exposure to the fumes of burning plastics, can certainly cause severe lung toxicity and even permanent disability. Ordinary firefighting may be associated with short-term changes similar to asthma, resolving over days. This does not appear to result in an increased lifetime risk of dying from chronic lung disease unless there has been an unusually intense exposure (the risk of dying from the consequences of smoke inhalation) or smoke with unusual characteristics (particularly involving burning polyvinyl chloride (PVC)).
Chronic obstructive pulmonary disease has been extensively studied among fire-fighters. The evidence does not support an association with firefighting, and therefore there can be no presumption. An exception may be in rare cases when a chronic lung disease follows an unusual or severe acute exposure and there is a compatible history of medical complications.
A general presumption of risk is not easily or defensibly justified in situations of weak associations or when diseases are common in the general population. A more productive approach may be to take the claims on a case-by-case basis, examining individual risk factors and overall risk profile. A general presumption of risk is more easily applied to unusual disorders with high relative risks, particularly when they are unique to or characteristic of certain occupations. Table 1 presents a summary of specific recommendations, with criteria that could be used to rebut, or question, presumption in the individual case.
Table 1. Summary of recommendations, with rebuttal criteria and special considerations, for compensation decisions.
|
|
Risk estimate (approximate) |
Recommendations |
Rebuttal criteria |
|
Lung cancer |
150 |
A NP |
- Smoking, previous occupational carcinogens |
|
Cardiovascular disease |
<150 |
NA NP |
+ Acute event at or soon following exposure |
|
Aortic aneurysm |
200 |
A P |
- Atherosclerosis (advanced), connective tissue disorders, history of thoracic trauma |
|
Cancers of genitourinary tract
|
>200
|
A P |
+ Occupational carcinogens - Heavy cigarette smoking, previous occupational carcinogens, schistosomiasis (bladder only), analgesic abuse, cancer chemotherapy (chlornaphazine), conditions resulting in urinary stasis / Coffee consumption, artificial sweeteners |
|
Brain cancer |
200
|
A P |
- Heritable neoplasms (rare), previous vinyl chloride exposure, radiation to head / Trauma, family history, smoking |
|
Cancers of lymphatic and haematopoietic system |
200 |
A
P |
- Ionizing radiation, previous occupational carcinogens (benzene), immunosuppressed state, cancer chemotherapy + Hodgkin’s disease |
|
Cancer of colon and rectum |
A NP NA NP |
A NP |
+ Low risk profile - Familial syndromes, ulcerative colitis / Other occupational exposures |
|
Acute lung disease |
NE NE |
A P |
Circumstances of case |
|
Chronic lung disease (COPD) |
NE NE |
NA NP |
+ Sequela of severe acute exposure, followed by recovery - Smoking, protease deficiency |
A = epidemiological association but not sufficient for presumption of association with firefighting. NA = no consistent epidemiological evidence for association. NE = Not established. P = presumption of association with firefighting; risk exceeds doubling over general population. NP = no presumption; risk does not exceed doubling over general population. + = suggests increased risk due to firefighting. - = suggests increased risk due to exposures unrelated to firefighting. / = no likely contribution to risk.
Injuries
Injuries associated with firefighting are predictable: burns, falls and being struck by falling objects. Mortality from these causes is markedly increased among fire-fighters compared to other workers. Jobs in firefighting have a high risk of burns, especially, include those involving early entry and close-in firefighting, such as holding the nozzle. Burns are also more commonly associated with basement fires, recent injury before the incident and training outside the fire department of present employment. Falls tend to be associated with SCBA use and assignment to truck companies.
Ergonomics
Firefighting is a very strenuous occupation and is often performed under extreme environmental conditions. The demands of firefighting are sporadic and unpredictable, characterized by long periods of waiting between bouts of intense activity.
Fire-fighters maintain their level of exertion at a relatively constant, intense level once active firefighting begins. Any additional burden in the form of an encumbrance by protective equipment or victim rescue, however necessary for protection, reduces performance because fire-fighters are already exerting themselves to the maximum. The use of personal protection equipment has imposed new physiological demands on fire-fighters but has removed others by reducing exposure levels.
A great deal is known about the exertion characteristics of fire-fighters as a result of many careful studies on the ergonomics of firefighting. Fire-fighters adjust their levels of exertion in a characteristic pattern during simulated fire conditions, as reflected by heart rate. Initially, their heart rate increases rapidly to 70 to 80% of maximal within the first minute. As firefighting progresses, they maintain their heart rates at 85 to 100% maximal.
The energy requirements for firefighting are complicated by the severe conditions encountered in many inside fires. The metabolic demands of coping with retained body heat, heat from the fire and fluid loss through sweating add to the demands of physical exertion.
The most demanding activity known is building search and victim rescue by the “lead hand” (first fire-fighter to enter building), resulting in the highest average heart rate of 153 beats/minute and highest rise in rectal temperature of 1.3 °C. Serving as “secondary help” (entering a building at a later time to fight the fire or to conduct additional searches and rescues) is next most demanding, followed by exterior firefighting and serving as crew captain (directing the firefighting, usually at some distance from the fire). Other demanding tasks, in decreasing order of energy costs, are climbing ladders, dragging the fire hose, carrying a travelling ladder and raising a ladder.
During firefighting, core body temperature and heart rate follow a cycle over a period of minutes: they both increase slightly in response to work in preparation for entry, then both increase more as a result of environmental heat exposure and subsequently increase more steeply as a result of high work loads under conditions of heat stress. After 20 to 25 minutes, the usual length of time allowed for interior work by the SCBA used by fire-fighters, the physiological stress remains within limits tolerable by a healthy individual. However, in extended firefighting involving multiple re-entries, there is insufficient time between SCBA air bottle changes to cool off, leading to a cumulative rise in core temperature and an increasing risk of heat stress.
Personal Protection
Fire-fighters exert themselves to maximal levels while fighting fires. Under fire conditions, physical demands are complicated by the metabolic demands of coping with heat and loss of fluids. The combined effect of internally generated heat during work and of external heat from the fire may result in markedly increased body temperatures that climb to unusually high levels in an intense firefighting situation. Half-hour interval breaks to change SCBAs are not enough to arrest this climb in temperature, which can reach dangerous levels in prolonged firefighting. Although essential, personal protection, particularly SCBAs, imposes a considerable additional energy burden on the fire-fighter. The protective clothing also becomes much heavier when it gets wet.
The SCBA is an effective personal protection device that prevents exposure to the products of combustion when used properly. Unfortunately, it is often used only during the “knockdown” phase, when the fire is being actively fought, and not during the “overhaul” phase, when the fire is over but the debris is being examined and embers and smouldering flames are being extinguished.
Fire-fighters tend to judge the level of hazard they face by the intensity of smoke and decide whether to use an SCBA solely on the basis of what they see. This may be very misleading, after the flames are extinguished. While the fire scene may appear to be safe at this stage, it can still be dangerous.
The additional burden or energy cost of using personal protective equipment has been a major area of emphasis in occupational health research on firefighting. This undoubtedly reflects the degree to which firefighting is an extreme case of a matter of general interest, the implications for performance of using personal protection.
Although fire-fighters are obliged to use several forms of personal protection in their work, it is respiratory protection that is most problematic and which has received the most attention. A 20% decrement has been found in work performance imposed by carrying an SCBA, which is a substantial restraint under extreme and dangerous conditions. Investigations have identified several factors of importance in evaluating the physiological demands imposed by respirators in particular, among them the characteristics of the respirator, physiological characteristics of the user and the interactive effects with other personal protection and with environmental conditions.
The fire-fighter’s typical “turnout” gear may weigh 23 kg and imposes a high energy cost. Chemical protective clothing (17 kg), as used for clean-up of spills, is the next most demanding gear to wear, followed by the use of SCBA gear while wearing light clothing, which is only slightly more demanding than wearing light, flame-resistant clothing with a low-resistance mask. The firefighting apparatus has been associated with significantly greater retention of internally generated heat and rise in body temperature.
Fitness
Numerous studies have evaluated the physiological characteristics of fire-fighters, usually in the context of other studies to determine the response to firefighting-related demands.
Studies of the fitness of fire-fighters have shown fairly consistently that most fire-fighters are as or somewhat more fit than the general adult male population. They are not, however, necessarily fit to an athletically trained level. Fitness and health maintenance programmes have been developed for fire-fighters but have not been convincingly evaluated for their effectiveness.
The entrance of female applicants into firefighting has caused a re-evaluation of performance tests and studies comparing the sexes. In studies of trained individuals capable of achieving their potential maximum performance, rather than typical applicants, women demonstrated lower scores on average than men in all performance items, but a subgroup of women performed nearly as well in some tasks. The overall difference in performance was attributed primarily to lower absolute lean body weight, which correlated most strongly and consistently with performance differences. The most difficult tests for women were the stair-climbing exercises.
Firefighting Procedures
Firefighting is one of the world’s most honoured but hazardous operations. By becoming fire-fighters, people join an organization rich in heritage of dedication, unselfish sacrifice and inspired human action. The job of a fire-fighter is not comfortable or easy. It is one that requires a high sense of personal dedication, a genuine desire to help people and a devotion to a profession that requires a high level of skill. It is also a profession that exposes an individual to a high level of personal danger.
Whenever there is a disaster, the fire department is one of the first called to the scene. Because it is a disaster, the conditions will not always be favourable. There will be hard, fast work that will drain energy and test endurance. The situation will not always involve fire. There will be cave-ins, building collapses, auto accidents, aircraft crashes, tornadoes, dangerous-goods incidents, civil disturbances, rescue operations, explosions, water incidents and medical emergencies. The emergency list is unlimited.
All fire-fighters use the same tactics and strategies to combat a fire. The strategies are simple—fight this fire offensively or defensively. Regardless, the goal is the same—extinguishment of the fire. Urban firefighting deals with structural firefighting. (The management of forest fires is dealt with in the chapter Forestry). It includes dealing with hazardous goods, water and ice, as well as high-angle rescue and emergency medicine. Fire service personnel must respond day and night to emergencies.
The tactical priorities that fire-fighters engage in during the course of the fire are shown in figure 1. It is during these operations that hose lays using attack lines, back up lines and supply lines can be employed. Other commonly used equipment are ladders and pushing/pulling and striking tools like axes and pike poles. Specialty equipment includes tarps that are used for salvage or hydraulic tools used for a rescue. The fire-fighter must use and be familiar with all of them. See figure 1.
Figure 1. The tactical priorities of structural firefighting operations.

Figure 2 shows a fire-fighter with appropriate personal protection laying water on a structural fire with a fire hose.
Figure 2. Firefighter laying water on a structural fire.

These operations expose the fire-fighter to the greatest risks and injuries regardless of the tool used or the operation engaged in. Back injuries, sprains, fall-related injuries and heat stress commonly occur. Heart and lung diseases are quite common among fire-fighters, which is thought to be due, in part, to the toxic gases and the level of physical activity required on the fire ground. Therefore, many departments are aggressively pursuing the addition of fitness programmes within their departments’ overall safety programme. Many jurisdictions have programmes in place to deal with critical incident stress, because the fire-fighter faces incidents that can create severe emotional reactions. Such reactions are normal reactions in the face of very abnormal situations.
The mission of every fire department is the preservation of life and property; therefore, safety on the fire ground is of paramount importance. Many of the operations discussed here have an underlying goal of providing greater safety on the fire ground. Many of the dangers that exist on the fire ground are due to the nature of fire. Backdraft and flashover kill fire-fighters. Backdraft is caused by the introduction of air into a superheated oxygen-starved area. Flashover is the build-up of heat within an area until it suddenly ignites everything within that area. These two conditions reduce the level of safety and increase property damage. Ventilation is one method of control that fire-fighters use. Increasing ventilation can lead to much damage to property. The fire-fighter is often observed breaking windows or cutting holes in the roof and intensity of the fire appears to grow. This is because smoke and toxic gases are released from the fire area. But this is a necessary part of firefighting. Special attention must be paid to roof collapse, to establishing a quick means of egress and to back-up hose lines for protection of the personnel and property.
The fire-fighter must put safety first and must work with a safety-conscious attitude and within organizational environments that promote safety. In addition, proper protective clothing must be provided and maintained. Clothing should be designed for freedom of movement and protection from heat. The structural fire-fighter must be outfitted with heavy fire-resistant fibre suits and a self-contained breathing apparatus.
The type of clothing worn is generally specific to the types of hazards faced by the fire-fighter outside the fire area on the fire line; the urban fire-fighter is generally inside a structure where intense heat and toxic gases are present. Helmets, boots and gloves designed specifically for the hazard that is faced by the fire-fighter provide head, foot and hand protection. Fire crews need training to ensure that fire-fighters have the knowledge and skills necessary to perform safely and efficiently. Training is usually provided through an in-house training programme, which can consist of a combination of on-the-job training and a formalized theory programme. Most provincial and state governments have agencies that promote various types of training programmes.
North America leads the world in property loss and many North American departments engage in preventive programmes to reduce the life and property losses within their jurisdictions. Public education and enforcement programmes are aggressively pursued by the most pro-active departments because, according to available statistics, the cost of prevention is cheaper than the cost of rebuilding. Furthermore, only 10% of businesses that suffer a total fire loss successfully rebuild. Thus the costs of a fire loss to a community can be staggering, since in addition to the cost to rebuild, sources of tax revenue, jobs and lives may also be lost forever. It is important, therefore, that both the community and the fire service work together to ensure that lives and property are preserved.
Environmental and Public Health Issues
Educational institutions are responsible for ensuring that their facilities and practices are in conformity with environmental and public health legislation and comply with accepted standards of care towards their employees, students and the surrounding community. Students are not generally covered under occupational health and safety legislation, but educational institutions must exercise diligence towards their students to at least the same degree as is required by legislation designed to protect workers. In addition, teaching institutions have a moral responsibility to educate their students on matters of personal, public, occupational and environmental safety which relate to them and to their activities.
Colleges and Universities
Large institutions such as college and university campuses may be compared to large towns or small cities in terms of the size of the population, geographic area, type of basic services required and complexity of activities being carried out. In addition to the occupational health and safety hazards found within such institutions (covered in the chapter Public and government services), there is a vast range of other concerns, relating to large populations living, working and studying in a defined area, that need to be addressed.
Waste management on campus is often a complex challenge. Environmental legislation in many jurisdictions requires stringent control of water and gas emissions from teaching, research and service activities. In certain situations external community concerns may require public relations attention.
Chemical and solid waste disposal programmes must take into consideration occupational, environmental and community health concerns. Most large institutions have comprehensive programmes for the management of the wide variety of wastes produced: toxic chemicals, radioisotopes, lead, asbestos, biomedical waste as well as trash, wet garbage and construction materials. One problem is the coordination of waste management programmes on campuses due to the large number of different departments, which often have poor communication with each other.
Colleges and universities differ from industry in the amounts and types of hazardous waste produced. Campus laboratories, for example, usually produce small amounts of many different hazardous chemicals. Methods of hazardous waste control can include neutralization of acids and alkalis, small-scale solvent recovery by distillation and “lab” packing, where small containers of compatible hazardous chemicals are placed in drums and separated by sawdust or other packing materials to prevent breakage. Since campuses can generate large quantities of paper, glass, metal and plastic waste, recycling programmes can usually be implemented as a demonstration of community responsibility and as part of the educational mission.
A few institutions located within urban areas may rely heavily upon external community resources for essential services such as police, fire protection and emergency response. The vast majority of medium-size and larger institutions establish their own public safety services to service their campus communities, often working in close cooperation with external resources. In many college towns, the institution is the largest employer and consequently may be expected to provide protection to the population which supports it.
Colleges and universities are no longer entirely remote or separate from the communities in which they are located. Education has become more accessible to a larger sector of society: women, mature students and the disabled. The very nature of educational institutions puts them at particular risk: a vulnerable population where the exchange of ideas and differing opinions is valued, but where the concept of academic freedom may not always be balanced with professional responsibility. In recent years educational institutions have reported more acts of violence toward educational community members, coming from the external community or erupting from within. Acts of violence perpetrated against individual members of the educational community are no longer extremely rare events. Campuses are frequent sites for demonstrations, large public assemblies, political and sports events where public safety and crowd control need to be considered. The adequacy of security and public safety services and emergency response and disaster recovery plans and capabilities needs to be constantly evaluated and periodically updated to meet community needs. Hazard identification and controls must be taken into consideration for sports programmes, field trips and a variety of sponsored recreational activities. Emergency medical service needs to be available even for off-campus activities. Personal safety is best managed through hazard reporting and education programmes.
Public health issues associated with campus life, such as control of communicable diseases, sanitation of food services and residence facilities, provision of fresh water, clean air and uncontaminated soil, must be addressed. Programmes for inspection, evaluation and control are required. Education of students in this regard is usually the responsibility of student service personnel, but occupational health and safety professionals are often involved. Education regarding sexually transmitted diseases, drug and alcohol abuse, blood-borne pathogens, stress and mental illness is particularly important in a campus community, where risky behaviour may increase the probability of exposure to associated hazards. Medical and psychological services must be available.
Elementary and Secondary Schools
Grade schools have many of the same environmental and public health issues as colleges and universities, only on a smaller scale. Often, however, schools and school districts do not have effective waste management programmes. A serious problem faced by many schools is the disposal of explosive ether and picric acid that have been stored in school laboratories for many years (National Research Council 1993). Attempts to dispose of these materials by unqualified personnel have caused explosions in several instances. One problem is that school districts can have many schools separated by several miles. This can create difficulties in centralizing hazardous waste programmes by having to transport hazardous waste on public roads.
Health Problems and Disease Patterns
Teachers comprise a large and growing segment of the workforce in many countries. For example, over 4.2 million workers were classified as preschool through high school teachers in the United States in 1992. In addition to classroom teachers, other professional and technical workers are employed by schools, including custodial and maintenance workers, nurses, food service workers and mechanics.
Teaching has not traditionally been regarded as an occupation that entails exposure to hazardous substances. Consequently, few studies of occupationally related health problems have been carried out. Nevertheless, school teachers and other school personnel may be exposed to a wide variety of recognized physical, chemical, biological and other occupational hazards.
Indoor air pollution is an important cause of acute illnesses in teachers. A major source of indoor air pollution is inadequate maintenance of heating, ventilation and air conditioning systems (HVAC). Contamination of HVAC systems can cause acute respiratory and dermatological illnesses. Newly constructed or renovated school buildings release chemicals, dusts and vapours into the air. Other sources of indoor air pollution are roofing, insulation, carpets, drapes and furniture, paint, caulk and other chemicals. Unrepaired water damage, as from roof leakage, can lead to the growth of micro-organisms in building materials and ventilation systems and the release of bioaerosols that affect the respiratory systems of teachers and students alike. Contamination of school buildings by micro-organisms can cause severe health conditions such as pneumonia, upper respiratory infections, asthma and allergic rhinitis.
Teachers who specialize in certain technical fields may be exposed to specific occupational hazards. For example, arts and craft teachers frequently encounter a variety of chemicals, including organic solvents, pigments and dyes, metals and metal compounds, minerals and plastics (Rossol 1990). Other art materials cause allergic reactions. Exposure to many of these materials is strictly regulated in the industrial workplace but not in the classroom. Chemistry and biology teachers work with toxic chemicals such as formaldehyde and other biohazards in school laboratories. Shop teachers work in dusty environments and may be exposed to high levels of wood dust and cleaning materials, as well as high noise levels.
Teaching is an occupation that is often characterized by a high degree of stress, absenteeism and burnout. There are many sources of teacher stress, which may vary with grade level. They include administrative and curriculum concerns, career advancement, student motivation, class size, role conflict and job security. Stress may also arise from dealing with children’s misbehaviours and possibly violence and weapons in schools, in addition to physical or environmental hazards such as noise. For example, desirable classroom sound levels are 40 to 50 decibels (dB) (Silverstone 1981), whereas in one survey of several schools, classroom sound levels averaged between 59 and 65 dB (Orloske and Leddo 1981). Teachers who are employed in second jobs after work or during the summer may be exposed to additional workplace hazards that can affect performance and health. The fact that the majority of teachers are women (three-fourths of all teachers in the United States are women) raises the question of how the dual role of worker and mother may affect women’s health. However, despite perceived high levels of stress, the rate of cardiovascular disease mortality in teachers was lower than in other occupations in several studies (Herloff and Jarvholm 1989), which could be due to lower prevalence of smoking and less consumption of alcohol.
There is a growing concern that some school environments may include cancer-causing materials such as asbestos, electromagnetic fields (EMF), lead, pesticides, radon and indoor air pollution (Regents Advisory Committee on Environmental Quality in Schools 1994). Asbestos exposure is a special concern among custodial and maintenance workers. A high prevalence of abnormalities associated with asbestos-related diseases has been documented in school custodians and maintenance employees (Anderson et al. 1992). The airborne concentration of asbestos has been reported higher in certain schools than in other buildings (Lee et al. 1992).
Some school buildings were built near high-voltage transmission power lines, which are sources of EMF. Exposure to EMF also comes from video display units or exposed wiring. Excess exposure to EMF has been linked to the incidence of leukaemia as well as breast and brain cancers in some studies (Savitz 1993). Another source of concern is exposure to pesticides that are applied to control the spread of insect and vermin populations in schools. It has been hypothesized that pesticide residues measured in adipose tissue and serum of breast cancer patients may be related to the development of this disease (Wolff et al. 1993).
The large proportion of teachers who are women has led to concerns about possible breast cancer risks. Unexplained increased breast cancer rates have been found in several studies. Using death certificates collected in 23 states in the United States between 1979 and 1987, the proportionate mortality ratios (PMRs) for breast cancer were 162 for White teachers and 214 for Black teachers (Rubin et al. 1993). Increased PMRs for breast cancer were also reported among teachers in New Jersey and in the Portland-Vancouver area (Rosenman 1994; Morton 1995). While these increases in observed rates have so far not been linked either to specific environmental factors or to other known risk factors for breast cancer, they have given rise to heightened breast cancer awareness among some teachers’ organizations, resulting in screening and early detection campaigns.
Art Teaching
Health and safety problems in art programmes can be similar in educational institutions ranging from junior high schools to universities. Arts programmes are a special problem because their hazards are not often recognized and, especially at the college level, can be semi-industrial in scale. Hazards can include inhalation of airborne contaminants; ingestion or dermal absorption of toxins; injury from machinery and tools; slips, trips and falls; and repetitive strain and other musculoskeletal injuries. Precautions include the provision of adequate ventilation (both dilution and local exhaust), the safe handling and storage of chemicals, machine-guarding and competent maintenance of machinery, efficient clean-up, good housekeeping and adjustable work stations. A key precaution in avoiding occupational safety and health problems of all kinds is adequate and mandatory training.
Elementary and Secondary School Teachers
Hazards at the elementary and secondary school levels include practices such as spraying and unsafe use of solvents and other chemicals and poor ventilation of processes. There is frequently a lack of proper equipment and sufficient knowledge of materials to ensure a safe workplace. Precautions include efficient engineering controls, better knowledge of materials, the elimination of hazardous art supplies from schools and substitution with safer ones (see table 1). This will help protect not only teachers, technicians, maintenance workers and administrators, but also students.
Table 1. Hazards and precautions for particular classes.
|
Class |
Activity/Subject |
Hazards |
Precautions |
||||||
|
Elementary Classes |
|||||||||
|
Science |
Animal handling
Plants
Chemicals
Equipment
|
Bites and scratches, zoonoses, parasites
Allergies, poisonous plants
Skin and eye problems, toxic reactions, allergies
Electrical hazards, safety hazards |
Allow only live, healthy animals. Handle animals with heavy gloves. Avoid animals which can carry disease-transmitting insects and parasites.
Avoid plants which are known to be poisonous or cause allergic reaction.
Avoid using toxic chemicals with children. Wear proper personal protective equipment when doing teacher demonstrations with toxic chemicals.
Follow standard electrical safety procedures. Ensure all equipment is properly guarded. Store all equipment, tools, etc., properly. |
||||||
|
Art |
Painting and drawing
Photography
Textile and fibre arts
Printmaking
Woodworking
Ceramics |
Pigments, solvents
Photochemicals
Dyes
Acids, solvents
Cutting tools
Tools
Glues
Silica, toxic metals, heat, kiln fumes |
Use only non-toxic art materials. Avoid solvents, acids, alkalis, spray cans, chemical dyes, etc.
Use only children’s paints. Do not use pastels, dry pigments.
Do not do photoprocessing. Send out film for developing or use Polaroid cameras or blueprint paper and sunlight.
Avoid synthetic dyes; use natural dyes such as onion skins, tea, spinach, etc.
Use water-based block printing inks.
Use linoleum cuts instead of woodcuts.
Use soft woods and hand tools only.
Use water-based glues.
Use wet clay only, and wet mop. Paint pottery rather than using ceramic glazes. Do not fire kiln inside classroom.
|
||||||
|
Secondary Classes |
|||||||||
|
Chemistry |
General
Organic chemistry
Inorganic chemistry
Analytical chemistry
Storage |
Solvents
Peroxides and explosives
Acids and bases
Hydrogen sulphide
Incompatibilities
Flammability |
All school laboratories should have the following: laboratory hood if toxic, volatile chemicals are used; eyewash fountains; emergency showers (if concentrated acids, bases or other corrosive chemicals are present); first aid kits; proper fire extinguishers; protective goggles, gloves and lab coats; proper disposal receptacles and procedures; spill control kit. Avoid carcinogens, mutagens and highly toxic chemicals like mercury, lead, cadmium, chlorine gas, etc.
Use only in laboratory hood. Use least toxic solvents. Do semi-micro- or microscale experiments.
Do not use explosives or chemicals such as ether, which can form explosive peroxides.
Avoid concentrated acids and bases when possible.
Do not use hydrogen sulphide. Use substitutes.
Avoid alphabetical storage, which can place incompatible chemicals in close proximity. Store chemicals by compatible groups.
Store flammable and combustible liquids in approved flammable-storage cabinets. |
||||||
|
Biology |
Dissection
Anaesthetizing insects
Drawing of blood
Microscopy
Culturing bacteria |
Formaldehyde
Ether, cyanide
HIV, Hepatitis B
Stains
Pathogens |
Do not dissect specimens preserved in formaldehyde. Use smaller, freeze-dried animals, training films and videotapes, etc.
Use ethyl alcohol for anaesthetization of insects. Refrigerate insects for counting.
Avoid if possible. Use sterile lancets for blood typing under close supervision.
Avoid skin contact with iodine and gentian violet.
Use sterile technique with all bacteria, assuming there could be contamination by pathogenic bacteria. |
||||||
|
Physical sciences |
Radioisotopes
Electricity and magnetism
Lasers |
Ionizing radiation
Electrical hazards
Eye and skin damage, electrical hazards |
Use radioisotopes only in “exempt” quantities not requiring a license. Only trained teachers should use these. Develop a radiation safety programme.
Follow standard electrical safety procedures.
Use only low-power (Class I) lasers. Never look directly into a laser beam or pass the beam across face or body. Lasers should have a key lock. |
||||||
|
Earth sciences |
Geology
Water pollution
Atmosphere
Volcanoes
Solar observation |
Flying chips
Infection, toxic chemicals
Mercury manometers
Ammonium dichromate
Infrared radiation |
Crush rocks in canvas bag to prevent flying chips. Wear protective goggles.
Do not take sewage samples because of infection risk. Avoid hazardous chemicals in field testing of water pollution.
Use oil or water manometers. If mercury manometers are used for demonstration, have mercury spill control kit.
Do not use ammonium dichromate and magnesium to simulate volcanoes.
Never view sun directly with eyes or through lenses. |
||||||
|
Art and Industrial Arts |
All
Painting and drawing
Photography
Textile and fibre arts |
General
Pigments, solvents
Photochemicals, acids, sulphur dioxide
Dyes, dyeing assistants, wax fumes |
Avoid most dangerous chemicals and processes. Have proper ventilation. See also precautions under Chemistry
Avoid lead and cadmium pigments. Avoid oil paints unless cleanup is done with vegetable oil. Use spray fixatives outside.
Avoid colour processing and toning. Have dilution ventilation for darkroom. Have eyewash fountain. Use water instead of acetic acid for stop bath.
Use aqueous liquid dyes or mix dyes in glove box. Avoid dichromate mordants. Do not use solvents to remove wax in batik. Have ventilation if ironing out wax. |
||||||
|
|
Papermaking
Printmaking
Woodworking
Ceramics
Sculpture
Jewelry
|
Alkali, beaters
Solvents
Acids, potassium chlorate
Dichromates
Woods and wood dust
Machinery and tools
Noise
Glues
Paints and finishes
Lead, silica, toxic metals, kiln fumes
Silica, plastics resins, dust
Soldering fumes, acids |
Do not boil lye. Use rotten or mulched plant materials, or recycle paper and cardboard. Use large blender instead of more dangerous industrial beaters to prepare paper pulp.
Use water-based instead of solvent-based silk screen inks. Clean intaglio press beds nd inking slabs with vegetable oil and dishwashing liquid instead of solvents. Use cut paper stencils instead of lacquer stencils for silk screen printing.
Use ferric chloride to etch copper plates instead of Dutch mordant or nitric acid on zinc plates. If using nitric acid etching, have emergency shower and eyewash fountain and local exhaust ventilation.
Use diazo instead of dichromate photoemulsions. Use citric acid fountain solutions in lithography to replace dichromates.
Have dust collection system for woodworking machines. Avoid irritating and allergenic hardwoods, preserved woods (e.g., chromated copper arsenate treated).Clean up wood dust to remove fire hazards.
Have machine guards. Have key locks and panic button.
Reduce noise levels or wear hearing protectors.
Use water-based glues when possible. Avoid formaldehyde/resorcinol glues, solvent-based glues.
Use water-based paints and finishes. Use shellac based on ethyl alcohol rather than methyl alcohol.
Purchase wet clay. Do not use lead glazes. Buy prepared glazes rather than mixing dry glazes. Spray glazes only in spray booth. Fire kiln outside or have local exhaust ventilation. Wear infrared goggles when looking into hot kiln.
Use only hand tools for stone sculpture to reduce dust levels. Do not use sandstone, granite or soapstone, which might contain silica or asbestos. Do not use highly toxic polyester, epoxy or polyurethane resins. Have ventilation if heating plastics to remove decomposition products. Wet mop or vacuum dusts.
Avoid cadmium silver solders and fluoride fluxes. Use sodium hydrogen sulphate rather than sulphuric acid for pickling. Have local exhaust ventilation. |
||||||
|
|
Enameling
Lost wax casting
Stained glass
Welding
Commercial art |
Lead, burns, infrared radiation
Metal fumes, silica, infrared radiation, heat
Lead, acid fluxes
Metal fumes, ozone, nitrogen dioxide, electrical and fire hazards
Solvents, photochemicals, video display terminals |
Use only lead-free enamels. Ventilate enameling kiln. Have heat-protective gloves and clothing, and infrared goggles.
Use 50/50 30-mesh sand/plaster instead of cristobalite investments. Have local exhaust ventilation for wax burnout kiln and casting operation. Wear heat-pro tective clothing and gloves.
Use copper foil technique rather than lead came. Use lead- and antimony-free solders. Avoid lead glass paints. Use acid- and rosin-free soldering fluxes.
Do not weld metals coated with zinc, lead paints, or alloys with hazardous metals (nickel, chromium, etc.). Weld only metals of known composition.
Use double-sided tape instead of rubber cement. Use heptane-based, not hexane rubber cements. Have spray booths for air brushing. Use water-based or alcohol- based permanent markers instead of xylene types. See Photography section for photoprocesses. Have proper ergonomic chairs, lighting, etc., for computers. |
||||||
|
Performing Arts |
Theatre
Dance
Music |
Solvents, paints, welding fumes, isocyanates, safety, fire
Acute injuries Repetitive strain injuries
Musculoskeletal injuries (e.g., carpal tunnel syndrome)
Noise
Vocal strain |
Use water-based paints and dyes. Do not use polyurethane spray foams. Separate welding from other areas. Have safe rigging procedures. Avoid pyrotechnics, firearms, fog and smoke, and other hazardous special effects. Fireproof all stage scenery. Mark all trap doors, pits and elevations.
Have a proper dance floor. Avoid full schedules after period of inactivity. Assure proper warm-up before and cool-down after dance activity. Allow sufficient recovery time after injuries.
Use proper sized instruments. Have adequate instrument supports. Allow sufficient recovery time after injuries.
Keep sound levels at acceptable levels. Wear musician’s ear plugs if needed. Position speakers to minimize noise levels. Use sound-absorbing materials on walls.
Assure adequate warm-up. Provide proper vocal training and conditioning. |
||||||
|
Automotive Mechanics |
Brake drums
Degreasing
Car motors
Welding
Painting |
Asbestos
Solvents
Carbon monoxide
Solvents, pigments |
Do not clean brake drums unless approved equipment is used.
Use water-based detergents. Use parts cleaner
Have tailpipe exhaust.
See above.
Spray paint only in spray booth, or outdoors with respiratory protection.
|
||||||
|
Home Economics |
Food and nutrition |
Electrical hazards
Knives and other sharp utensils
Fire and burns
Cleaning products |
Follow standard electrical safety rules.
Always cut away from body. Keep knives sharpened.
Have stove hoods with grease filters that exhaust to outside. Wear protective gloves with hot objects.
Wear goggles, gloves and apron with acidic or basic cleaning products. |
||||||
College and University Teachers
Hazards at the college and university levels include, in addition to those mentioned above, the fact that students, teachers and technicians tend to be more experimental and tend to use more potentially dangerous materials and machinery. They also often work on a larger scale and for longer periods of time. Precautions must include education and training, the provision of engineering controls and personal protective equipment, written safety policies and procedures and insistence on compliance with these.
Artistic Freedom
Many art teachers and technicians are artists in their own right, resulting in multiple exposures to the hazards of art materials and processes which can significantly increase their health risks. When confronted with hazards in their field about which they have not known or which they have ignored, many teachers become defensive. Artists are experimental and frequently belong to an anti-establishment culture which encourages defiance of institutional rules. It is important, however, for the school administration to realize that the quest for artistic freedom is not a valid argument against working safely.
Liability and Training
In many jurisdictions teachers will be subject to both a personal and a school liability for the safety of their students, particularly the younger ones. “Because of the age, maturity, and experience limitations of most students, and because teachers stand in loco parentis (in the place of a parent), schools are expected to provide a safe environment and establish reasonable behaviour for the protection of students” (Qualley 1986).
Health and Safety Programmes
It is important that schools take the responsibility for training both art teachers and school administrators in the potential hazards of art materials and processes and in how to protect their students and themselves. A prudent school administration will ensure that there are in place written health and safety policies, procedures and programmes, compliance with these, regular safety training and a real interest in teaching how to create art safely.
Colleges and Universities
The large number and wide variety of operations and hazardous materials involved in teaching, research and support service activities present a challenge to health and safety management in colleges and universities. The very nature of research implies risk: challenging the limits of current knowledge and technology. Many research activities in science, engineering and medicine require sophisticated and expensive facilities, technology and equipment which may not be readily available or have yet to be developed. Research activities within existing facilities may also evolve and change without the facilities being modified to contain them safely. Many of the most hazardous activities are performed infrequently, periodically or on an experimental basis. Hazardous materials used in teaching and research often include some of the most dangerous substances and hazards with unavailable or poorly documented safety and toxicity data. These are commonly used in relatively small quantities under less than ideal conditions by poorly trained personnel. Health and safety hazards are not always easily recognized or readily acknowledged by highly educated academics with specialized fields of expertise who may have a poor regard for legislative or administrative controls when these are perceived to limit academic freedom.
Academic freedom is a sacred principle, fiercely guarded by academics, some of whom may be experts in their disciplines. Any legislative or institutional constraints which are perceived as encroaching on this principle will be fought and may even be disregarded. Methods for the identification and control of health and safety hazards associated with teaching and research activities cannot be readily imposed. Academics need to be persuaded that health and safety policies support and enhance the primary mission rather than confine it. Policies, where they exist, tend to protect the academic mission and the rights of individuals, rather than to conform with external regulations and standards. Liability and accountability issues affecting teachers and researchers directly may have more effect than rules.
Most health and safety legislation, standards and guidance criteria are developed for industry with large quantities of relatively few chemicals, well documented hazards, established procedures and a stable workforce within a well defined management system. The academic environment differs from industry in almost every aspect. In some jurisdictions academic institutions may even be exempt from health and safety legislation.
Academic institutions are generally hierarchical in their management systems, with academics at the top followed by non-academic professionals, technicians and support staff. Graduate students are often employed on a part-time basis to perform a variety of teaching and research functions. Academics are appointed to senior management positions for specific terms with little management experience or training. Frequent turn-over may result in a lack of continuity. Within this system, senior researchers, even within large institutions, are granted relative autonomy to manage their affairs. They are usually in control of their own budgets, facility design, purchasing, organization of work and hiring of personnel. Hazards may be overlooked or go unrecognized.
It is common practice for researchers in academic institutions to employ graduate students as research assistants in a master/apprentice relationship. These individuals are not always protected under health and safety laws. Even if covered by legislation, they are frequently reluctant to exercise their rights or to voice safety concerns to their supervisors who may also be responsible for evaluating their academic performance. Long hours under great pressure, overnight and weekend work with minimal supervision and skeleton support services are routine. Cost saving and energy conservation efforts may even reduce essential services such as security and ventilation during nights and weekends. Though students are not usually protected by health and safety legislation, due diligence requires that they are treated with the same level of care as is provided for employees.
Potential Hazards
The range of hazards can be extremely broad depending upon the size and nature of the institution, the type of academic programmes offered and the nature of research activities (see table 1). Small colleges offering only liberal arts programmes may have relatively few hazards while comprehensive universities with schools of medicine, engineering and fine arts and extensive research programmes may have a complete range, including some very serious hazards, such as toxic chemicals, biohazards, reproductive hazards, ionizing and non-ionizing radiations and various other physical agents.
Table 1. Summary of hazards in colleges and universities.
|
Type of hazard |
Sources |
Locations/activities |
|
Toxic chemicals (carcinogens, teratogens, caustics, heavy metals, asbestos, silica) |
Lab chemicals, solvents, degreasers, glues, art supplies, manometers, thermometers, photochemicals, dyes, hazardous waste |
Laboratories, art studios, workshops, health care facilities, maintenance operations, machine shops, theatres, darkrooms, engineering, hockey arenas |
|
Flammables and explosives |
Lab chemicals, cleaning agents, solvents, fuels |
Laboratories, maintenance operations, workshops, art studios, construction sites |
|
Pesticides |
Fumigation, rodent and pest control, disinfectants |
Housekeeping, groundskeeping, greenhouse, agriculture |
|
Biological agents |
Animal handling, cell and tissue cultures, blood and body fluids, diagnostic specimens, contaminated sharps, solid waste |
Animal care facilities, health care, housekeeping, laboratories |
|
Non-ionizing radiation |
Lasers, microwaves, magnets, electronics, ultraviolet light |
Laboratories, electrical operations, health care facilities, workshops, technical operations |
|
Ionizing radiation |
Radioisotopes, gas chromatography, x-rays, calibration, reactors, neutron generators, waste management |
Laboratories, medical facilities, engineering |
|
Ergonomics |
Materials handling, office work, computers |
Libraries, offices, maintenance operations, movers, truck drivers, food services |
|
Heat/cold |
Outdoor work, overexertion |
Groundskeeping, public safety, maintenance, field work, agriculture and forestry |
|
Noise |
Machinery, boilers and pressure vessels, computers, construction and maintenance, ventilation systems |
Boiler rooms, print shops, maintenance and grounds, construction operations, computer rooms, labs, machine shops, art studios |
|
Violence |
Internal community, external community, domestic disputes, civil disobedience |
Classrooms, places of assembly, accounts, stores, food service, personnel department, security operations |
|
Electrical |
Electrical equipment, construction and maintenance operations, amateur wiring jobs, special events |
Laboratories, workshops, maintenance shops, construction sites, electronic shops, residences, theatre, special events |
|
Compressed gases |
Laboratory equipment and operations, welding operations, coolants, ice-making equipment, construction |
Laboratories, metal shops, construction sites, machine shops, hockey arenas |
|
Machine hazards |
Materials handling, robots, maintenance and construction work |
Printing shops, maintenance and grounds operations, engineering, science and technical laboratories, machine shops |
|
Sharp objects |
Broken glass, cutting instruments, needles, lab vessels, test tubes |
Housekeeping, laboratories, health care, art studios, workshops |
Maintenance and groundskeeping, hazardous materials handling, machine and motor vehicle operations and office work are common to most institutions and comprise hazards which are covered elsewhere in this Encyclopaedia.
Workplace violence is an emerging issue of particular concern for teaching staff, front-line personnel, money handlers and security personnel.
Large institutions may be compared to small towns where a population lives and works. Issues of personal and community safety interface with occupational health and safety concerns.
Control of Hazards
Hazard identification through the usual processes of inspection and incident and injury investigation need to be preceded by careful review of proposed programmes and facilities prior to the start up of activities. The occupational and environmental risk aspects of new research projects and academic programmes should be taken into consideration in the earliest stages of the planning process. Researchers may not be aware of legislative requirements or safety standards applicable to their operations. For many projects, researchers and safety professionals need to work together to develop the safety procedures as the research proceeds and new hazards emerge.
Ideally the safety culture is incorporated into the academic mission - for example, through inclusion of relevant health and safety information into course curricula and laboratory and procedure manuals for students as well as specific health and safety information and training for employees. Hazard communication, training and supervision are critical.
In laboratories, art studios and workshops, general ventilation control needs to be augmented by local exhaust ventilation. Containment of biohazards and isolation or shielding of radioisotopes are necessary in certain cases. Personal protective equipment, while not a primary prevention method in most situation, may be the option of choice for temporary set-ups and some experimental conditions.
Hazardous materials and waste management programmes are usually required. Centralized purchasing and distribution of commonly used chemicals and micro-scale experiments in teaching prevent the storage of large volumes in individual laboratories, studios and workshops.
The maintenance of an emergency response and disaster recovery plan in anticipation of major events which overwhelm the normal response capabilities will mitigate the health and safety effects of a serious incident.
Vocational Training and Apprenticeships
The teaching of trades through the apprenticeship system dates at least as far back as the Roman Empire, and continues to this day in classic trades such as shoemaking, carpentry, stone masonry and so forth. Apprenticeships can be informal, where a person desiring to learn a trade finds a skilled employer willing to teach him or her in exchange for work. However, most apprenticeships are more formal and involve a written contract between the employer and the apprentice, who is bound to serve the employer for a given time in return for training. These formal apprenticeship programmes usually have standard rules regarding qualifications for completing the apprenticeship that are set by an institution such as a trade union, guild or employer organization. In some countries, trade unions and employer organizations run the apprenticeship programme directly; these programmes usually involve a combination of structured on-the-job training and classroom instruction.
In today’s technological world, however, there is a growing need for skilled labour in many areas, such as laboratory technicians, mechanics, machinists, cosmetologists, cooks, service trades and many more. The learning of these skilled trades usually takes place in vocational programmes in schools, vocational institutes, polytechnics, colleges with two-year programmes and similar institutions. These sometimes include internships in actual work settings.
Both the teachers and the students in these vocational programmes face occupational hazards from the chemicals, machinery, physical agents and other hazards associated with the particular trade or industry. In many vocational programmes, students are learning their skills using old machinery donated by industry. These machines often are not equipped with modern safety features such as proper machine guards, fast-acting brakes, noise-control measures and so forth. The teachers themselves often have not had adequate training in the hazards of the trade and appropriate precautions. Often, the schools do not have adequate ventilation and other precautions.
Apprentices often face high-risk situations because they are assigned the dirtiest and most hazardous tasks. Often they are used as a source of cheap labour. In these situations, it is even more likely that the apprentice’s employers have not had adequate training in the hazards and precautions of their trade. Informal apprenticeships are usually not regulated, and there is often no recourse for apprentices facing such exploitation or hazards.
Another common problem with both apprenticeship programmes and vocational training is age. Apprenticeship entry age is generally between 16 and 18 year of age. Vocational training can begin at elementary school. Studies have shown that young workers (aged 15 to 19 years) account for a disproportionate percentage of lost-time injury claims. In Ontario, Canada, for the year 1994, the largest proportion of injured young workers were employed in the service industry.
These statistics indicate that students entering these programmes may not understand the importance of health and safety training. Students also can have different attention spans and comprehension levels than adults, and this should be reflected in their training. Finally, extra attention is needed in sectors such as service industries, where health and safety has generally not received the attention found in other industries.
In any apprenticeship or vocational programme, there should be built-in safety and health training programmes, including hazard communication. The teachers or employers should be properly trained in the hazards and precautions, both to protect themselves and to teach the students properly. The work or training setting should have adequate precautions.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."