- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Cattle, sheep and goats
Material on hair-cutting and shearing was written with the assistance of J.F. Copplestone’s article on the subject in the 3rd edition of this Encyclopaedia.
Several animals convert high-fibre feeds, called roughage (over 18% fibre), into edible food that is consumed by humans. This ability comes from their four-stomach digestion system, which includes their largest stomach, the rumen (for which they gain the designation ruminants) (Gillespie 1997). Table 1 shows the various types of ruminant livestock that have been domesticated and their uses.
Table 1. Types of ruminants domesticated as livestock
|
Ruminant type |
Uses |
|
Cattle |
Meat, milk, draught |
|
Sheep |
Meat, wool |
|
Goats |
Meat, milk, mohair |
|
Camelids (llama, alpaca, dromedary and bactrian camels) |
Meat, milk, hair, draught |
|
Buffalo (water buffalo) |
Meat, draught |
|
Bison |
Meat |
|
Yaks |
Meat, milk, wool |
|
Reindeer |
Meat, milk, draught |
Production Processes
Processes for rearing ruminants vary from intensive, high-production operations such as raising beef cattle on large, 2,000-km2 ranches in Texas to communal grazing such as the nomadic herders of Kenya and the United Republic of Tanzania. Some farmers use their cattle as oxen for traction power in farm tasks such as ploughing. In humid areas, water buffalo serve the same purpose (Ker 1995). The trend is toward high-production, intensive systems (Gillespie 1997).
High-volume, intensive beef production depends on various interdependent operations. One is the cow-calf system, which involves keeping a herd of cows. The cows are bred by bulls or artificial insemination annually to produce calves, and, after weaning, the calves are sold to cattle feeders to raise for slaughter. Male calves are castrated for the slaughter market; a castrated calf is called a steer. Pure-bred breeders maintain the herds of breeding stock, including bulls, which are very dangerous animals.
Sheep are produced in either range or farm flocks. In range production, flocks of 1,000 to 1,500 ewes are common. In farm flocks, production is usually small and typically a secondary enterprise. Sheep are raised for their wool or as feeder lambs for the slaughter market. Lambs are docked, and most male lambs are castrated. Some enterprises specialize in raising rams for pure-bred breeding.
Goats are raised through either range or small-farm production for their mohair, milk and meat. Pure-bred breeders are small operations that raise rams for breeding does. Specific breeds exist for each of these products. The goats are dehorned, and most males are castrated. Goats browse on shoots, twigs and leaves of brush plants, and thus they may also be used to control brush on a ranch or farm.
Other major processes involved in rearing cattle, sheep and goats include feeding, disease and parasite control, hair clipping and fleece shearing. The milking process and livestock waste disposal are addressed in other articles in this chapter.
Cattle, sheep and goats are fed in several ways, including grazing or feeding hay and silage. Grazing is the least expensive way to deliver forage to animals. Animals typically graze on pastures, wild lands or crop residues, such as corn stalks, which remain in the field after crop harvests. Hay is harvested from the field and typically stored loose or in stacked bales. The feeding operation includes moving the hay from the stack to the open field or into mangers to feed the animals. Some crops such as corn are harvested and converted into silage. Silage is typically moved mechanically into mangers for feeding.
The control of diseases and parasites in cattle, sheep and goats is an integral part of the livestock-rearing process and requires animal contact. Routine visits to the herd by a veterinarian are an important part of this process, as is observing vital signs. Timely vaccination against diseases and quarantining diseased animals are also important.
External parasites include flies, lice, mange, mites and ticks. Chemicals are one control against these parasites. Pesticides are applied by spraying or through insecticide-impregnated ear tags. The heel fly lays eggs on the hair of cattle, and its larva, the cattle grub, burrows into the skin. A control for this grub is systemic pesticides (spread throughout the body through spray, dips or as a feed additive). Internal parasites, including roundworms or flatworms, are controlled with drugs, antibiotics or drenches (oral administration of a liquid medication). Sanitation is also a strategy for the control of infectious diseases and parasite infestations (Gillespie 1997).
The removal of hair from live animals helps to maintain their cleanliness or comfort and to prepare them for exhibitions. Hair may be sheared from live animals as a product, such as the fleece from sheep or mohair from goats. The sheep shearer catches the animal in a pen and drags it to a stand where it is laid on its back for the shearing operation. It is pinned by the shearer’s legs. Hair cutters and sheep shearers use a hand-operated scissors or motorized shears to clip the hair. The motorized shears are typically powered by electricity. Prior to shearing and also as part of gestation management, sheep are tagged and crutched (i.e., hair encrusted with faeces is removed). The cut fleece is manually trimmed according to the quality and staple of the hair. It is then compressed into packs for transportation using a hand-operated screw or hydraulic ram.
Facilities used for raising cattle, sheep and goats are generally considered to be either confined or unconfined. Confined facilities include confinement houses, feedlots, barns, corrals (holding, sorting and crowding pens), fences and working and loading chutes. Unconfined facilities refer to pasture or range operations. Feeding facilities include storage facilities (vertical and horizontal silos), feed grinding and mixing equipment, haystacks, conveying equipment (including augers and elevators), feed bunks, water fountains and mineral and salt feeders. In addition, sun protection may be provided by sheds, trees or overhead lattice work. Other facilities include back rubbers for parasite control, creep-feeders (allows feeder calves or lambs to feed without adults feeding), self-feeders, calf shelters, cattle-guard gates and cattle treatment stalls. Fencing may be used around pastures, and these include barbed wire and electric fences. Woven wire may be required to contain goats. Free-ranging animals would require herding to control their movement; goats may be tethered, but require shade. Dipping tanks are used for parasite control in large sheep flocks (Gillespie 1997).
Hazards
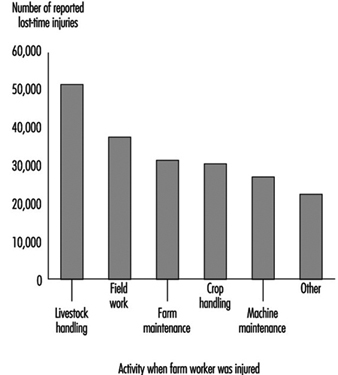
Table 2 shows several other processes of cattle, sheep and goat handling, with associated hazardous exposures. In a survey of farm workers in the United States (Meyers 1997), handling livestock represented 26% of lost-time injuries. This percentage was higher than any other farm activity, as shown in figure 1. These figures would be expected to be representative of the injury rate in other industrialized countries. In countries where draught animals are common, injury rates would be expected to be higher. Injuries from cattle usually occur in farm buildings or in the vicinity of buildings. Cattle inflict injuries when they kick or step on people or crush them against a hard surface such as the side of a pen. People may also be injured by falling when working with cattle, sheep and goats. Bulls inflict the most serious injuries. Most of the people injured are family members rather than hired workers. Fatigue can reduce judgement, and thus increase the chance of injury (Fretz 1989).
Table 2. Livestock rearing processes and potential hazards
|
Process |
Potential hazardous exposures |
|
Breeding, artificial inseminating |
Violent acts by bulls, rams or bucks; slips and falls; |
|
Feeding |
Organic dust; silo gas; machines; lifting; electricity |
|
Calving, lambing, kidding |
Lifting and pulling; animal behaviour |
|
Castrating, docking |
Animal behaviour; lifting; cuts from knives |
|
Dehorning |
Animal behaviour; cuts from trimmers; caustic |
|
Branding and marking |
Burns; animal behaviour |
|
Vaccinating |
Animal behaviour; needle sticks |
|
Spraying and dusting/drenching, worming |
Organophosphates |
|
Foot/hoof trimming |
Animal behaviour; awkward postures; tool-related |
|
Shearing, tagging and crutching, washing and clipping |
Awkward postures and lifting; animal behaviour; |
|
Loading and unloading |
Animal behaviour |
|
Manure handling |
Manure gases; slips and falls; lifting; machines |
Sources: Deere & Co. 1994; Fretz 1989; Gillespie 1997; NIOSH 1994.
Figure 1. Estimates of lost-time injury frequency by farm activity in the United States, 1993
Livestock exhibit behaviours that can lead to injuries of workers. The herding instinct is strong among animals such as cattle or sheep, and imposed limits such as isolation or overcrowding can lead to unusual behavioural patterns. Reflexive response is a common defensive behaviour among animals, and it can be predicted. Territorialism is another behaviour that is predictable. A reflexive escape struggle is apparent when an animal is removed from its normal quarters and placed in a confined environment. Animals that are restrained by chutes for loading for transportation will exhibit agitated reflex response behaviour.
Dangerous environments are numerous in cattle, sheep and goat production facilities. These include slippery floors, manure pits, corrals, dusty feed areas, silos, mechanized feeding equipment and animal confinement buildings. Confinement buildings may have manure storage pits, which can emit lethal gases (Gillespie 1997).
Heat exhaustion and stroke are potential hazards. Heavy physical labour, stress and strain, heat, high humidity and dehydration from lack of drinking water all contribute to these hazards.
Livestock handlers are at risk for developing respiratory illness from exposure to inhaled dusts. A common illness is organic dust toxic syndrome. This syndrome may follow exposures to heavy concentrations of organic dusts contaminated with micro-organisms. About 30 to 40% of workers who are exposed to organic dusts will develop this syndrome, which includes the conditions shown in table 3; this table also shows other respiratory conditions (NIOSH 1994).
Table 3. Respiratory illnesses from exposures on livestock farms
|
Organic dust toxic syndrome conditions |
|
Precipitin-negative farmer’s lung disease |
|
Pulmonary mycotoxicosis |
|
Silo unloader’s syndrome |
|
Grain fever in grain elevator workers |
|
Other important respiratory illnesses |
|
“Silo fillers’ disease” (acute toxic inflammation of the lung) |
|
“Farmer’s lung disease” (hypersensitivity pneumonitis) |
|
Bronchitis |
|
Asphyxiation (suffocation) |
|
Toxic gas inhalation (for example, manure pits) |
Hair cutters and sheep shearers face several hazards. Cuts and abrasions may result during the shearing operation. Animal hoofs and horns also present potential hazards. Slips and falls are an ever-present hazard while handling the animals. Power for the shears is sometimes transferred by belts, and guards must be maintained. Electrical hazards are also present. Shearers also face postural hazards, particularly to the back, as a result of catching and tipping the sheep. Constraining the animal between the shearer’s legs tends to strain the back, and torsional movements are common while shearing. Manual shearing usually results in tenosynovitis.
The control of insects on cattle, sheep and goats with pesticide spray or powder can expose workers to the pesticide. Sheep dips submerge the animal in a pesticide bath, and handling the animal or contact with the bath solution or contaminated wool can also expose workers to the pesticide (Gillespie 1997).
Common zoonoses include rabies, brucellosis, bovine tuberculosis, trichinosis, salmonella, leptospirosis, ringworm, tapeworm, orf virus disease, Q fever and spotted fever. Diseases that may be contracted while working with hair and fleece include tetanus, salmonellosis from tagging and crutching, leptospirosis, anthrax and parasitic diseases.
Animal faeces and urine also provide a mechanism for infection of workers. Cattle are a reservoir for cryptosporidosis, a disease that can be transmitted from cattle to humans through the faecal-oral route. Calves with diarrhoea (scours) may harbour this disease. Schistosomiasis, an infection by blood flukes, is found in cattle, water buffalo and other animals in several parts of the world; its life cycle goes from eggs excreted in urine and faeces, developing into larvae, which enter snails, then to free-swimming cercariae that attach to and penetrate human skin. Penetration can occur while workers are wading in water.
Some zoonoses are arthropod-borne viral diseases. The primary vectors for these diseases are mosquitoes, ticks and sandflies. These diseases include arboviral encephalitides transmitted by ticks and milk from sheep, babesiosis transmitted by ticks from cattle and Crimean-Congo haemorrhagic fever (Central Asian haemorrhagic fever) transmitted by mosquitoes and ticks from cattle, sheep and goats (as amplifying hosts) during epizootics (Benenson 1990; Mullan and Murthy 1991).
Preventive Action
The principal occupational hazards that occur in rearing ruminants include injuries, respiratory problems and zoonotic diseases. (See “A checklist for livestock rearing safety practices”.)
Stair steps should be maintained in good condition, and floors must be even to reduce fall hazards. Guards on belts, mechanical screws, compression rams and shear sharpening equipment should be maintained. Wiring should be maintained in good condition to prevent electrical shock. Ventilation should be assured wherever internal combustion engines are used in barns.
Training and experience in properly handling animals helps to prevent injuries related to the animals’ behaviour. Safe livestock handling requires understanding of both innate and acquired components of animal behaviour. Facilities should be designed so workers do not have to enter small or enclosed areas with animals. Lighting should be diffuse, since animals may become confused and balk around bright lights. Sudden noises or movements may startle cattle, causing them to crowd a person against hard surfaces. Even clothing hanging on fences flapping in the wind can startle cattle. They should be approached from the front so as not to surprise them. Avoid use of contrasting patterns in cattle facilities, because cattle will slow or stop when they see these patterns. Shadows across the floor should be avoided because cattle may refuse to cross over them (Gillespie 1997).
Risks of organic dust exposure can be minimized in several ways. Workers should be aware of the health effects of breathing organic dust and inform their physician about recent dust exposures when seeking help for respiratory illness. Minimizing spoilage of feed can minimize potential fungal spore exposures. To avoid such hazards, workers should use mechanized equipment to move decaying materials. Farm operators should use local exhaust ventilation and wet methods of dust suppression to minimize exposure. Appropriate respirators should be worn when organic dust exposure cannot be avoided (NIOSH 1994).
Preventing zoonoses depends upon maintaining clean livestock facilities, vaccinating the animals, quarantine of sick animals and avoiding exposure to sick animals. Rubber gloves should be worn when treating sick animals to avoid exposures through any cuts in the hands. Workers who become sick after contact with a sick animal should seek medical help (Gillespie 1997).
Postal Services
Although the social obligation of most postal administrations—domestic mail collection, sorting, delivery and international mail processing while preserving the security of mail—has remained unchanged over the last century, the methods by which this obligation is carried out have been transformed due to the rapid advances of technology and increases in mail volumes. Australia, France, Germany, Sweden, the United Kingdom and other industrialized countries each process billions of mail pieces each year. In 1994 the US Postal Service delivered almost two hundred billion pieces of mail, an increase in mail volume of 67% since 1980. Competition by private carriers entering the market, particularly for parcel delivery and express delivery service, as well as from other technological advancements, such as facsimile (fax) machines, computer modems, electronic mail, electronic transfer of funds and satellite systems, have also changed personal and business communications. Since private carriers carry out many of the same operations as postal services, their workers face many of the same hazards.
Most postal administrations are government-owned and operated, although this is changing. For example, Argentina, Australia, Canada, Germany, the Netherlands, Sweden, the United Kingdom and the United States have, to varying degrees, privatized their postal operations. The franchising or contracting of work and services is becoming increasingly common among the postal administrations in the industrialized world.
Postal administrations, especially in industrialized nations, are often one of the largest employers in the country; they employ up to several hundred thousand people in some countries. Although advances in technology have not dramatically changed how postal administrations are structured, they have altered the methods by which mail is sorted and delivered. As postal services have long been highly labour intensive (with wages and benefits accounting for up to 80% of total operating costs in some countries), efforts to reduce these costs as well as to improve productivity and increase operating efficiency have promoted technological advancement through capital investments. For many industrialized nations the objective is to fully automate the processing of mail up to the point of delivery.
Operations
Postal operations are divided into three main phases: collection, sorting and delivery. Administrative and maintenance services are also integral aspects of postal operations. The technological changes in operating methods, especially for the sorting phase, have led to a declining demand for workers. As a result, workers are more isolated because less staffing is required to operate the newer postal equipment. Enhanced technology has also led to a reduction of requisite skills in the workforce as computers have replaced such tasks as memorizing postal codes and performing diagnostic tests on mechanical equipment.
Shift work is still a common practice in postal operations as most mail is collected at the end of the day and then transported and sorted at night. Many postal administrations provide home and business mail delivery six days a week. The frequency of service requires most postal operations to run twenty-four hours a day, seven days a week. Consequently, the psychological and physical stress from shift work and night work still remain problems for many postal workers, particularly during the busy night shift in large processing centres.
Most postal administrations in the industrialized world are organized with large processing centres supporting small retail and delivery offices. Often several stories high and occupying several thousands of square metres, processing centres are equipped with large pieces of machinery, material handling equipment, motor vehicles and repair and paint shops similar to work environments in other industrial workplaces. Smaller retail offices, however, are generally cleaner and less noisy and more akin to office environments.
Hazards and Their Prevention
While technology has eliminated many dangerous and monotonous tasks performed by postal workers, different hazards have emerged that, if not properly addressed, may jeopardize the health and safety of postal workers.
Retail services
For employees who work at retail postal counters, job tasks depend on the size of the post office and the type of services offered by the postal administration. General duties of the retail employee include selling stamps and money orders, weighing and pricing letters and parcels and providing postal information to customers. Since retail personnel are directly involved in the exchange of money with the public, the risk of violent robbery is increased for these workers. For retail personnel who work alone, in proximity to high crime areas or late at night or early in the mornings, workplace violence can be a major occupational hazard if appropriate protective measures are not taken. The potential for such workplace violence also contributes to undue mental stress. Also, the day-to-day pressure from dealing with the public and the responsibility for relatively large amounts of money are contributing stress factors.
Environmental conditions and the physical layout of the retail employee’s workstation may also contribute to health and safety hazards. Indoor air quality problems, such as dust, the lack of fresh air and temperature variations may cause discomfort for the retail clerk. Poorly designed work stations that require the operator to work in awkward postures due to the placement of retail equipment (e.g., cash register, scale, mail and parcel containers), prolonged standing postures or sitting in uncomfortable and unadjustable chairs, and lifting heavy parcels can lead to musculoskeletal disorders.
Preventive measures that address these hazards include improving security by installing bright external and internal lighting, doors, windows and partitions of bullet proof glass and silent alarms, ensuring that clerks do not work alone, providing emergency and defensive response training and ensuring that the public has limited and controlled access to the facility. Ergonomic and indoor air quality assessments may also contribute to the improvement of the working conditions for retail personnel.
Sorting
The transition from manual operations to mechanized and automated systems has greatly affected the handling and sorting phase of postal operations. For example, whereas postal workers were once required to memorize various codes that corresponded to address delivery routes, that task is now computerized. Since the early 1980s, technology has improved so that many machines can now “read” an address and apply a code. In the industrialized countries, the task of sorting mail has shifted from humans to machines.
Material handling
Although technology has reduced the amount of manual letter and small parcel sorting, it has had less of an impact on the movement of containers, bundles and sacks of mail inside a postal facility. Mail that is transported by trucks, planes, rail or ship into large processing and sorting centres may be internally transferred to different sorting areas by complex conveyor or belt systems. Fork-lift trucks, mechanical dumpers and smaller conveyors assist postal employees in unloading and loading trucks and placing the mail onto the complex conveyor systems. Some material handling tasks, however, especially those performed in smaller postal facilities, must still be performed manually. Culling operations that separate mail to be processed by machine from mail that which must be sorted by hand is one task that has not been fully automated. Depending on the postal administration’s regulations or national health and safety regulations, limits on load weights may be imposed to prevent employees from having to lift and carry containers of mail and parcels that are too heavy (see figure 1).
Figure 1. Manual lifting of heavy parcels is a serious ergonomic hazard. Weight and size limits on parcels are necessary.

Material handling tasks also expose postal workers to electrical hazards and machine parts that may injure the body. Although paper dust is a nuisance to almost all postal workers, employees who primarily perform material handling tasks commonly inhale dust when they first open mailbags, containers and sacks. Material handling workers are also the first employees to come into contact with any biological or chemical materials that may have spilled during transport.
Efforts to reduce fatigue and back injuries include automating some of the manual lifting and carrying tasks. Transporting pallets of mail by forklifts, using rolling containers to transport mail inside a facility and installing automatic container unloaders are methods of automating material handling tasks. Some industrialized nations are utilizing robotics to assist in material handling tasks such as loading containers onto conveyors. Regulating the amount of weight workers lift and carry and training workers in proper lifting techniques may also help to reduce the incidence of back injury and pain.
To control exposure to chemicals and biological matter, some postal administrations place prohibitions on the type and amount of hazardous materials that can be sent by mail and also require these materials to be identifiable to postal workers. Since some mail will undoubtedly be sent without proper warnings affixed, workers should be trained in responding to releases of potentially hazardous materials.
Manual/mechanized
As sorting technology improves, manual letter sorting is rapidly being phased out. Some manual letter sorting, however, is still necessary in many postal administrations, particularly in the developing countries. Manual letter sorting involves workers placing individual letters into slots or “pigeon holes” in a case. The worker then bundles the mail from each slot and places the bundles into containers or mail bags for dispatch. Manual sorting is a repetitive activity that the worker performs while either standing or sitting on a stool.
Manual parcel sorting is also still performed by postal workers. Since parcels are generally larger in size and much heavier than letters, workers must often put the parcels into separate hampers or containers that are arranged around them. Workers who perform manual parcel sorting often are at risk for cumulative trauma disorders affecting the shoulders, arms and back.
Automation has addressed many of the ergonomic hazards associated with manual letter and parcel sorting. Where automation technology is not available, workers should have the opportunity to rotate to different tasks to relieve fatigue from one particular body area. Appropriate rest breaks should also be provided to workers performing repetitive tasks.
In modern, mechanized sorting systems, workers sit at a keyboard while letters are mechanically passed in front of them (figure 2). Coding desks are arranged either side-by-side or behind one another in a line. Operators must often memorize hundreds of codes that correspond to different zones and enter a code for each letter on a keyboard. Unless adjusted properly, the keyboards may require the operator to use more force to depress the keys than modern computer keyboards. Approximately fifty to sixty letters each minute are processed by the operator. Based upon the code entered by the operator, the letters are segregated into different bins and then removed, bundled and dispatched by the postal workers.
Figure 2. Coding desk operators sorting letters with the aid of computerized machines.

Ergonomic hazards that lead to musculoskeletal disorders, particularly tendinitis and carpal tunnel syndrome, are the biggest problem for mechanized sorting operators. Many of these machines were designed several decades ago when ergonomic principles were not applied with the same degree of diligence as they are today. Automated sorting equipment and VDUs are quickly replacing these mechanized sorting systems. In many postal administrations where mechanized sorting is still the primary system, workers may rotate to other positions and/or take breaks at regular intervals. Providing comfortable chairs and adjusting the keyboard force are other modifications that can improve the job. Although a nuisance and discomfort to the operator, noise and dust from the mail are generally not major hazards.
Visual display units
Visual display unit-based sorting terminals are beginning to replace mechanized sorters. Instead of the actual mail pieces being presented to the operator, enlarged images of the addresses appear on the screen. Much of the mail that is processed by VDU sorting has been previously rejected or culled as not machineable by the automatic sorters.
The advantage of VDU sorting is that it does not need to be located in close proximity to the mail. Computer modems can send the images to the VDUs that are located in another facility or even a different city. For the VDU operator, this means that the work environment is generally more comfortable, with no background noise from sorting machines or dust from mail. However, sorting with the VDU is a very visually demanding job and often involves only one task, keying from images of letters. As with most sorting tasks, the job is monotonous but at the same time requires intense concentration from the operator in order to maintain the required productivity levels.
Musculoskeletal discomfort and eye strain are the most common complaints of VDU operators. Steps to reduce physical, visual and mental fatigue include providing adjustable equipment, such as keyboards and chairs, maintaining adequate lighting to reduce glare and scheduling regular breaks. In addition, since VDU operators often work in an office-type environment, consideration should be given to indoor air quality complaints.
Automation
The most advanced type of sorting reduces the need for workers to be directly involved in the coding and segregation of individual mail pieces. Generally only 2 or 3 workers are required to operate an automatic sorter. At one end of the machine, a worker loads mail onto a mechanical belt that feeds each letter in front of an optical character reader (OCR). The letter is read or scanned by the OCR and a bar code is printed on it. The letters are then automatically segregated into dozens of bins located at the other end of the machine. Workers then remove the bundles of segregated mail from the bins and transport them to the next stage of the sorting process. Larger automated sorters can process between 30,000 and 40,000 pieces of mail per hour.
Although such automation no longer requires a keyboard to encode mail, workers are still exposed to monotonous, repetitive tasks that put them at risk for musculoskeletal disorders. Removing the bundles of segregated mail from the different bins and placing them into containers or other material handling equipment puts physical stress on the operator’s shoulders, back and arms. Operators also complain of wrist and hand problems from constantly grasping handfuls of mail. Dust exposure is sometimes more problematic for automated sorter workers than other postal employees because of the larger volume of mail processed.
Many postal administrations have only recently acquired automated sorting equipment. As complaints of musculoskeletal discomfort mount, equipment designers and engineers will be forced to incorporate ergonomic principles more thoroughly in their attempts to balance productivity needs with the well-being of employees. For example, in the United States, government safety and health officials have concluded that some of the automated mail-sorting equipment poses serious ergonomic deficiencies. While attempts can be made to modify either the equipment or work methods to reduce the risks of musculoskeletal discomfort, such modifications are not as effective as the proper design of equipment (and work methods) in the first place.
Another problem is the risk of injury during the clearing of jams or during maintenance and repair operations. Proper training and lockout/tagout procedures are needed for these operations.
Delivery
Postal operations rely upon many methods of transportation to distribute mail including air, rail, water and highway. For short distances and local delivery, mail is transported by motor vehicles. Mail travelling generally less than several hundred kilometres from large processing centres to smaller post offices is usually carried by trains or large trucks, while air and sea travel is reserved for the longer distances between large processing centres.
As the use of motor vehicles for delivery services has increased dramatically during the past two decades, accidents and injuries involving postal trucks, jeeps and automobiles have become for some postal administrations the biggest and most serious occupational safety and health problem. Vehicular accidents constitute the main cause of workplace fatalities. Additionally, while the increased use of motor vehicles for delivery and the installation of more street mail storage boxes have helped to reduce the amount of time letter carriers spend walking, musculoskeletal discomfort and back injuries still are problematic due to the heavy bags of mail that they must carry on their routes. Also, robberies and other violent attacks against letter carriers are on the rise. Injuries caused by slips, trips and falls, particularly during adverse weather conditions, and dog attacks are other serious hazards experienced by letter carriers. Unfortunately, other than increased awareness not much can be done to eliminate these particular hazards.
Steps designed to reduce the likelihood of vehicular accidents include installing anti-lock brakes and extra mirrors to improve visibility, increasing seat belt usage, improving driver training, conducting more frequent vehicle maintenance inspections and improving roadways and vehicle design. To address the ergonomic hazards associated with lifting and carrying mail, some postal administrations provide carts with wheels or specialized mail bags where the weight is more evenly distributed across the worker’s shoulders instead of concentrated on one side. To reduce the risk of workplace violence, letter carriers may carry two-way communication devices and their vehicles may be equipped with a tracking system. In addition, to address environmental concerns and concerns of exposure to diesel exhaust, some postal vehicles are powered by natural gas or electricity.
Repair and Maintenance
Workers that are responsible for the day-to-day upkeep, cleaning and repair of postal facilities and equipment, including motor vehicles, face similar hazards as maintenance employees in other industrial operations. Exposure to welding operations, electrical hazards, falls from scaffolding, chemicals found in cleaning fluids and machine lubricants, asbestos from brake linings and dust are examples of hazards associated with maintenance tasks.
Dairy
The dairy farmer is a livestock specialist whose aim is optimizing the health, nutrition and reproductive cycling of a herd of cows with the ultimate goal of maximal milk production. Major determinants of the farmer’s exposure to hazards are farm and herd size, labour pool, geography and degree of mechanization. A dairy farm may be a small family business milking 20 or fewer cows per day, or it may be a corporate operation using three shifts of workers to feed and milk thousands of cows around the clock. In regions of the world where the climate is quite mild, the cattle may be housed in open sheds with roofs and minimal walls. Alternatively, in some regions barns must be tightly closed to preserve sufficient heat to protect the animals and the watering and milking systems. All of these factors contribute variability to the risk profile of the dairy farmer. Nevertheless, there are a series of hazards which most people working in dairy farming around the world will encounter to at least some degree.
Hazards and Precautions
Noise
One potential hazard which clearly relates to the degree of mechanization is noise. In dairy farming, harmful noise levels are common and always related to some type of mechanical device. Leading offenders outside of the barn are tractors and chain-saws. Noise levels from these sources are often at or above the 90-100 dBA range. Within the barn, other noise sources include bedding choppers, small skid-steer loaders and milking pipeline vacuum pumps. Here again, sound pressures may exceed those levels generally considered to be damaging to the ear. Although the studies of noise-induced hearing loss in dairy farmers are limited in number, they combine to show a convincing pattern of hearing deficits affecting predominantly the higher frequencies. These losses can be quite substantial and occur considerably more frequently in farmers of all ages than in non-farm controls. In several of the studies, the losses were more notable in the left than the right ear—possibly because farmers spend much of their time with the left ear turned toward the engine and muffler when driving with an implement. Prevention of these losses may be accomplished by efforts directed at noise abatement and muffling, and institution of a hearing-conservation programme. Certainly, the habit of wearing hearing protective devices, either muffs or earplugs, may help substantially to reduce the next generation’s risk of noise-induced hearing loss.
Chemicals
The dairy farmer has contact with some chemicals which are commonly found in other types of agriculture, as well as some which are specific to the dairy industry, such as those used for cleaning the automated vacuum-powered milking pipeline system. This pipeline must be effectively cleaned before and after each use. Commonly this is done by first flushing the system with a very strong alkaline soap solution (typically 35% sodium hydroxide), followed by an acidic solution such as 22.5% phosphoric acid. A number of injuries have been observed in association with these chemicals. Spills have resulted in significant skin burns. Splatters may injure the cornea or conjunctivae of unprotected eyes. Tragic accidental ingestion—often by young children—which may occur when these materials are pumped into a cup and then briefly left unattended. These situations can be best prevented by the use of an automated, closed flush system. In the absence of an automated system, precautions must be taken to restrict access to these solutions. Measuring cups should be clearly labelled, reserved for only this purpose, never left unattended and rinsed thoroughly after each use.
Like others working with livestock, dairy farmers may have exposure to a variety of pharmaceutical agents ranging from antibiotics and progestational agents to prostaglandin inhibitors and hormones. Depending upon the country, dairy farmers also may use fertilizers, herbicides and insecticides with varying degrees of intensity. In general, the dairy farmer uses these agrochemicals less intensively than persons working in some other types of farming. However, the same care in mixing, applying and storing these materials is necessary. Appropriate application techniques and protective garb are as important for the dairy farmer as anyone else working with these compounds.
Ergonomic Risks
Although data on the prevalence of all musculoskeletal problems are currently incomplete, it is clear that dairy farmers have increased risk of arthritis of the hip and knee compared to nonfarmers. Similarly, their risk of back problems may also be elevated. Although not well studied, there is little question that ergonomics is a major problem. The farmer may routinely carry weights in excess of 40 kg—often in addition to considerable personal body weight. Tractor driving produces abundant vibration exposure. However, it is the portion of the job devoted to milking that seems most ergonomically significant. A farmer may bend or stoop 4 to 6 times in the milking of a single cow. These motions are repeated with each of a number of cows twice daily for decades. Carrying the milking equipment from stall to stall imposes an additional ergonomic load on the upper extremities. In countries where milking is less mechanized, the ergonomic load on the dairy farmer might be different, but still it is likely to reflect considerable repetitive strain. A potential solution in some countries is the shift to milking parlours. In this setting the farmer can milk a number of cows simultaneously while standing several feet below them in the central pit of the parlour. This eliminates the stooping and bending as well as the upper-extremity load of carrying equipment from stall to stall. The latter problem is also addressed by the overhead track systems being introduced in some Scandinavian countries. These support the weight of the milking equipment when moving between stalls, and can even provide a convenient seat for the milker. Even with these potential solutions, much remains to be learned about ergonomic problems and their resolution in dairy farming.
Dust
A closely linked problem is organic dust. This is a complex, often allergenic and generally ubiquitous material on dairy farms. The dust frequently has high concentrations of endotoxin and may contain beta-glucans, histamine and other biologically active materials (Olenchock et al. 1990). Levels of total and respirable dust may exceed 50 mg/m3 and 5 mg/m3, respectively, with certain operations. These most commonly involve work with microbially contaminated feed or bedding within a closed space such as a barn, hay loft, silo or grain bin. Exposure to these dust levels may result in acute problems such as ODTS or hypersensitivity pneumonitis (“farmer’s lung disease”). Chronic exposure may also play a role in asthma, farmer’s lung disease and chronic bronchitis, which seems to occur at twice the rate of a non-farm population (Rylander and Jacobs 1994). The prevalence rates of some of these problems are higher in settings where moisture levels in the feed are likely to be elevated and in areas where barns are more tightly closed because of climatic requirements. Various farming practices such as drying of the hay and shaking out of feed for the animals by hand, and the choice of bedding material, can be major determinants of the levels of both the dust and its associated illnesses. Farmers can often devise a number of techniques to minimize either the amount of microbial overgrowth or its subsequent aerosolization. Examples include the use of sawdust, newspapers and other alternative materials for bedding instead of moulded hay. If hay is used, the addition of a quart of water to the cut surface of the bale minimizes the dust generated by a mechanical bedding chopper. Capping vertical silos with plastic sheets or tarpaulins without additional feed on top of this layer minimizes the dust of subsequent uncapping. The use of small amounts of moisture and/or ventilation in situations where dust is likely to be generated is often possible. Finally, farmers must anticipate potential dust exposures and use appropriate respiratory protection in these situations.
Allergens
Allergens may represent a troublesome health challenge for some dairy farmers. Major allergens appear to be those encountered in the barns, typically animal danders and “storage mites” living in feed stored within the barns. One study has extended the storage mite problem beyond the barn, finding sizeable populations of these species living within farmhouses as well (van Hage-Hamsten, Johansson and Hogland 1985). Mite allergy has been confirmed as a problem in a number of parts of the world, often with differing species of mites. Reactivity to these mites, to cow dander and to multiple other less significant allergens, results in several allergic manifestations (Marx et al. 1993). These include immediate onset of nasal and eye irritation, allergic dermatitis and, of greatest concern, allergy-mediated occupational asthma. This can occur as either an immediate or delayed (up to 12 hours) reaction and may occur in individuals not previously known to be asthmatic. It is of concern because the dairy farmer’s involvement in barn activities is daily, intensive and lifelong. With this nearly continual allergic re-challenge, progressively more severe asthma is likely to be seen in some farmers. Prevention includes avoidance of dust, which is the most effective and, unfortunately, the most difficult intervention for most dairy farmers. The results of medical therapies, including allergy shots, topical steroids or other anti-inflammatory agents, and symptomatic relief with bronchodilators, have been mixed.
A Checklist for Livestock Rearing Safety Practices
Feeding
- Use proper ventilation in buildings and silos.
- Keep entrances to grain, feed and silage storage areas closed and locked.
- Post warning signs in feed and silage storage areas about the hazard of entrapment in flowing grain or feed.
- Maintain silo and bin ladders in good condition.
- Shield auger inlets to prevent contact with augers.
- Cover loading troughs on augers, elevators and conveyors with grating.
- Use caution when moving augers and elevators; check for overhead power lines.
- Assure that shields are in place for all feeding, grinding and other equipment.
- Be aware of health effects of breathing organic dust, and inform your doctor about recent dust exposure when seeking treatment for respiratory illness.
- Use automated or mechanized equipment to move decayed materials.
- Use source containment, local exhaust ventilation and wet methods to control organic dust.
- Use appropriate respiratory protection when dust exposure is unavoidable.
Handling
- Establish good sanitation, vaccination and inoculation programmes.
- When working with animals, plan an escape exit; have at least two ways out.
- Livestock handlers should have enough strength and experience for the job.
- Avoid working with animals when you are tired.
- Use caution when approaching animals so as not to startle them.
- Know the animals and be patient with them.
- Dehorn dangerous animals.
- Post warning signs where chemicals are stored; lock them in a room or cabinet.
- Mix all chemicals outside or in a well-ventilated area.
- Be careful when leading animals.
- Wear rubber gloves when treating sick animals.
- Vaccinate animals, and quarantine sick animals.
- Wash hands after contact with calves with diarrhoea (scours).
Containment and housing
- Make sure all pens, gates, loading chutes and fences are in good repair and strong enough to contain the animal.
- Do not allow tobacco smoking around farm buildings and fuel storage and refueling areas; post “no smoking” signs in these areas.
- Maintain fully charged ABC-type fire extinguishers in major farm buildings.
- Remove trash and debris around buildings to prevent fires and falls.
- Keep all buildings in good repair.
- Keep electrical wiring in good condition.
- Use adequate lighting in all buildings.
- Keep floors clean and free of broken concrete and slippery areas.
Waste disposal
- Correctly dispose of all chemical containers following directions on the label.
- Install vent pipes and exhaust fans in manure pits.
Inspection Services
National, state or provincial, municipal and other local government units employ inspectors in a variety of agencies to verify compliance with laws, ordinances and regulations intended to promote and protect the health and safety of both workers and the public. This is government’s traditional role of enacting laws to address socially unacceptable risks and then to assigning agencies to establish programmes to achieve conformance with the regulatory standards. The inspector or investigator is the key person on the front-line in enforcing regulatory standards.
An example of such a legislative mandate is the role of inspection of workplaces for health and safety practices. Worksite inspectors visit workplaces to verify compliance with regulations governing the workplace, potential occupational and environmental hazards, the tools, machines and equipment being used, and the way the work is done, including the use of personal protective equipment (PPE). The inspectors have the authority to initiate penalties (citations, monetary fines and, in egregious cases, criminal prosecution) when deficiencies are encountered. Under laws enacted in some localities, regional authorities share responsibilities for carrying out inspections with federal powers.
Other areas in which governmental agencies have inspection responsibilities include environmental protection, regulation of food and drugs, nuclear energy, interstate commerce and civil aviation, public health and consumer protection. Engineering and building inspections are generally organized at the local level.
Throughout the world the basic functions and protections addressed by inspection services are similar although the particular legislation and governmental structures vary. These are discussed elsewhere in this Encyclopaedia.
To protect workers and property, to avoid statutory penalties and the adverse publicity that accompanies them and to minimize legal liability and the costs of workers’ compensation benefits, private sector enterprises often conduct in-house inspections and audits to ensure that they are complying with the regulations. These self-audits may be conducted by appropriately qualified staff persons or outside consultants may be retained. A notable recent trend in the US and some other developed countries has been the proliferation of private consulting organizations and academic departments which offer occupational health and safety services to employers.
Hazards
In general, inspectors are faced by the very same hazards they are charged to identify and correct. For example, workplace health and safety inspectors may visit worksites that have toxic environments, harmful noise levels, infectious agents, radiation, fire or explosion hazards and unsafe buildings and equipment. Unlike workers in a fixed environment, the inspectors must anticipate the kinds of hazards they will encounter on a given day and make sure that they have the tools and PPE they might need. In each instance, they must prepare themselves for a worst-case scenario. For example, when entering a mine, inspectors must be prepared for an oxygen-deficient atmosphere, fires and explosions and cave-ins. Inspectors checking isolation units in health care facilities must protect themselves against contagious organisms.
Occupational stress is a prime hazard for inspectors. It stems from a number of factors:
- Work stress is increasing as fiscal retrenchments cause reductions in agency budgets, which often results in understaffing. This brings pressure to manage an increasing work load that inevitably affects the ability to maintain the quality and integrity of inspections.
- There is also the stress of having to enforce the minutiae of guidelines and regulations which the inspector may acknowledge to be unwarranted in particular situations. And, when circumstances do not allow them to be overlooked, the inspector may bear the brunt of abuse for enforcing unpopular rules and regulations.
- Employers, and sometimes the workers as well, may resent the “intrusion” of the inspector into the workplace and his or her need to maintain a high level of suspicion with respect to subterfuges and cover-ups. This often makes the job unpleasant and stressful for the inspector. This antagonism may escalate into threats and actual violence.
- The inspector may suffer from feelings of responsibility when neglected or unrecognized hazards in the workplace result in a worker’s loss of life or limb or, even worse, in disaster involving many individuals.
- Like many employees who work in the field on their own, inspectors may suffer from such bureaucratic ills as distant and/or inadequate supervision, lack of support, endless paperwork and separation from home, family and friends.
- The necessity of entering unsafe neighbourhoods may expose them to crime and violence.
- Finally, particularly when they are required to wear uniforms, they may be seen as enemies by those who bear a grudge against the particular agency or the government as a whole. This can culminate in abuse or even violent assaults. The 1996 bombing of the federal office building in Oklahoma City, Oklahoma, in the US is an indication of such hostility to government.
Agencies employing inspectors must have clearly written health and safety policies describing appropriate measures to protect the health and well-being of inspectors, particularly those working in the field. In the US, for example, OSHA includes such information in its compliance directives. In some instances, this agency requires inspectors to document their use of the appropriate protective equipment while performing an inspection. The integrity of the inspection may be compromised if the inspector himself or herself violates health and safety rules and procedures.
Education and training are the key to preparing inspectors to properly protect themselves. When new standards are promulgated and new initiatives or programmes undertaken, the inspectors should be trained in preventing illness and injury to themselves as well as being drilled in the new requirements and enforcement procedures. Unfortunately, such training is rarely offered.
As part of programmes for learning to cope with work stress, also rarely offered, inspectors should be trained in communication skills and contending with angry and abusive people.
Table 1 lists some of the categories of government inspectors and hazards to which they may be exposed. More detailed information about the recognition and control of such hazards is to be found elsewhere in this Encyclopaedia.
Table 1. Hazards of inspection services.
|
Occupations |
Tasks |
Associated hazards |
|
Occupational safety and health compliance officers |
Investigate and cite safety and health hazards |
A wide variety of safety and health hazards |
|
Agricultural inspectors |
Investigate agricultural and farmworker health and safety |
Agricultural equipment, chemicals, pesticides, biological agents and |
|
Environmental inspectors |
Investigate industrial and agricultural sites for contaminated air, water and soil |
Chemical, physical, biological and safety hazards |
|
Health inspectors |
Investigate nursing homes and hospitals for compliance with hospital safety and health standards |
Infectious, chemical, radioactive and safety hazards |
|
Food inspectors |
Investigate and cite food product safety and establishments |
Insects, vermin and associated microbiological agents; chemical agents; violence and dogs |
|
Engineering and building inspectors |
Investigate for compliance with building construction and fire operation and maintenance codes |
Unsafe structures, building and construction equipment and materials |
|
Customs inspectors |
Investigate for contraband and hazardous materials entering territorial boundaries |
Explosives, drugs, biological and chemical hazards |
A recent phenomenon in many countries that is disturbing to many is the trend toward deregulation and decreased emphasis on inspection as an enforcement mechanism. This has led to the under-financing, degrading and downsizing of agencies and erosion of their inspection services. There is a growing concern not only for the health and safety of the cadres of inspectors but also for the health and well-being of the workers and the public they are charged to protect.
Manure and Waste Handling
The importance of the management of waste has increased as the intensity of agricultural production on farms has increased. Waste from livestock production is dominated by manure, but also includes bedding and litter, wasted feed and water and soil. Table 1 lists some relevant characteristics of manure; human waste is included both for comparison and because it too must be treated on a farm. The high organic content of manure provides an excellent growth medium for bacteria. The metabolic activity of bacteria will consume oxygen and maintain bulk-stored manure in an anaerobic state. Anaerobic metabolic activity can produce a number of well-known toxic gaseous by-products, including carbon dioxide, methane, hydrogen sulphide and ammonia.
Table 1. Physical properties of manure as excreted per day per 1,000 lb of animal weight, excluding moisture.
|
Weight (lb) |
Volume (ft3) |
Volatiles (lb) |
Moisture (%) |
||
|
As excreted |
As stored |
||||
|
Dairy cow |
80–85 |
1.3 |
1.4–1.5 |
85–90 |
>98 |
|
Beef cow |
51–63 |
0.8–1.0 |
5.4–6.4 |
87–89 |
45–55 |
|
Pig (grower) |
63 |
1.0 |
5.4 |
90 |
91 |
|
Sow (gestation) |
27 |
0.44 |
2.1 |
91 |
97 |
|
Sow and piglets |
68 |
1.1 |
6.0 |
90 |
96 |
|
Laying hens |
60 |
0.93 |
10.8 |
75 |
50 |
|
Broilers |
80 |
1.3 |
15. |
75 |
24 |
|
Turkeys |
44 |
0.69 |
9.7 |
75 |
34 |
|
Lamb (sheep) |
40 |
0.63 |
8.3 |
75 |
— |
|
Human |
30 |
0.55 |
1.9 |
89 |
99.5 |
Source: USDA 1992.
Management Processes
The management of manure involves its collection, one or more transfer operations, storage or/and optional treatment and eventually utilization. The moisture content of manure as listed in table 1 determines its consistency. Wastes of different consistencies require different management techniques and therefore can present different health and safety hazards (USDA 1992). The reduced volume of solid or low-moisture manure generally permits lower equipment costs and energy requirements, but handling systems are not easily automated. The collection, transfer and any optional treatments of liquid waste are more easily automated and require less daily attention. Storage of manure becomes increasingly mandatory as the seasonal variability of the local crops increases; the storage method must be sized to meet the production rate and utilization schedule while preventing environmental damage, especially from water runoff. Options for utilization include use as plant nutrients, mulch, animal feed, bedding or a source to produce energy.
Manure Production
Dairy cows are typically raised on pastures, except when in holding areas for pre- and post-milking and during seasonal extremes. Water use for cleaning in milking operations can vary from 5 to 10 gallons per day per cow, where flushing of wastes is not practised, to 150 gallons per day per cow where it is. Therefore, the method used for cleaning has a strong influence on the method chosen for manure transport, storage and utilization. Because the management of beef cattle requires less water, beef manure is more often handled as a solid or semi-solid. Composting is a common storage and treatment method for such dry wastes. The local precipitation pattern also strongly influences the preferred waste management scheme. Excessively dry feedlots are apt to produce a downwind dust and odour problem.
The major problems for swine raised on traditional pastures are the control of runoff and soil erosion due to the gregarious nature of pigs. One alternative is the construction of semi-enclosed pig buildings with paved lots, which also facilitates the separation of solid and liquid wastes; solids require some manual transfer operations but liquids can be handled by gravity flow. Waste-handling systems for fully enclosed production buildings are designed to collect and store waste automatically in a largely liquid form. Livestock playing with their watering facilities can increase the volumes of swine waste. Manure storage is generally in anaerobic pits or lagoons.
Poultry facilities are generally divided into those for meat (turkeys and broilers) and egg (layers) production. The former are raised directly on prepared litter, which maintains the manure in a relatively dry state (25 to 35% moisture); the only transfer operation is mechanical removal, generally only once per year, and transport directly to the field. Layers are housed in stacked cages without litter; their manure can either be allowed to collect in deep stacks for infrequent mechanical removal or be automatically flushed or scraped in a liquid form much like swine manure.
The consistency of waste from most other animals, like sheep, goats and horses, is largely solid; the major exception is veal calves, because of their liquid diet. Waste from horses contains a high fraction of bedding and may contain internal parasites, which limits its utilization on pasture land. Waste from small animals, rodents and birds may contain disease organisms that can be transmitted to humans. However, studies have shown that faecal bacteria do not survive on forage (Bell, Wilson and Dew 1976).
Storage Hazards
Storage facilities for solid wastes must still control water runoff and leaching into surface and ground water. Thus, they should be paved pads or pits (that may be seasonal ponds) or covered enclosures.
Liquid and slurry storage is basically limited to ponds, lagoons, pits or tanks either below or above ground. Long-term storage is coincident with onsite treatment, usually by anaerobic digestion. Anaerobic digestion will reduce the volatile solids indicated in table 1, which also reduces odours emanating from eventual utilization. Unguarded below-surface holding facilities can lead to injuries or fatalities from accidental entry and falls (Knoblauch et al. 1996).
The transfer of liquid manure presents a highly variable hazard from mercaptans produced by anaerobic digestion. Mercaptans (sulphur-containing gases) have been shown to be major contributors to the odour of manure and are all quite toxic (Banwart and Brenner 1975). Perhaps the most dangerous of the effects from H2S shown in table 2 is its insidious capacity to paralyze the sense of smell in the 50- to 100-ppm range, removing the sensory capacity to detect higher, rapidly toxic levels. Liquid storage for as short as 1 week is enough to initiate the anaerobic production of toxic mercaptans. Major differences in long-term manure gas generation rates are thought to be due to uncontrolled variations in the chemical and physical differences within the stored manure, such as temperature, pH, ammonia and organic loading (Donham, Yeggy and Dauge 1985).
Table 2. Some important toxicologic benchmarks for hydrogen sulphide (H2S)
|
Physiological or regulatory benchmark |
Parts per million (ppm) |
|
Odour detection threshold (rotten-egg smell) |
.01–.1 |
|
Offensive odour |
3–5 |
|
TLV-TWA = recommended exposure limit |
10 |
|
TLV-STEL = recommended 15-minute exposure limit |
15 |
|
Olfactory paralysis (cannot be smelled) |
50–100 |
|
Bronchitis (dry cough) |
100–150 |
|
IDLH (pneumonitis and pulmonary oedema) |
100 |
|
Rapid respiratory arrest (death in 1–3 breaths) |
1,000–2,000 |
TLV-TWA = Threshold limit values–Time weighted average; STEL = Short-term exposure level; IDLH = Immediately dangerous to life and health.
The normally slow release of these gases during storage is greatly increased if the slurry is agitated to resuspend the sludge that accumulates at the bottom. H2S concentrations of 300 ppm have been reported (Panti and Clark 1991), and 1,500 ppm has been measured during the agitation of liquid manure. The rates of gas release during agitation are much too large to be controlled by ventilation. It is most important to realize that natural anaerobic digestion is uncontrolled and therefore highly variable. The frequency of serious and fatal over-exposures can be predicted statistically but not at any individual site or time. A survey of dairy farmers in Switzerland reported a frequency of about one manure gas accident per 1,000 person-years (Knoblauch et al. 1996). Safety precautions are necessary each time agitation is planned to avoid the unusually hazardous event. If the operator does not agitate, sludge will build up until it may have to be removed mechanically. Such sludge should be left to dry before someone physically enters an enclosed pit. There should be a written confined-space programme.
Rarely used alternatives to anaerobic ponds include an aerobic pond, a facultative pond (one using bacteria that can grow under both aerobic and anaerobic conditions), drying (dewatering), composting or an anaerobic digester for biogas (USDA 1992). Aerobic conditions can be created either by keeping the liquid depth no more than 60 to 150 cm or by mechanical aeration. Natural aeration takes more space; mechanical aeration is more costly, as are the circulating pumps of a facultative pond. Composting may be conducted in windrows (rows of manure which must be turned every 2 to 10 days), a static but aerated pile or a specially constructed vessel. The high nitrogen content of manure must be reduced by mixing a high carbon amendment that will support the thermophilic microbial growth necessary for composting to control odours and remove pathogens. Composting is an economical method of treating small carcasses, if local ordinances permit. See also the article “Waste disposal operations” elsewhere in this Encyclopaedia. If a rendering or disposal plant is not available, other options include incineration or burial. Their prompt treatment is important to control herd or flock disease. Swine and poultry wastes are particularly amenable to methane production, but this utilization technique is not widely adopted.
Thick crusts can form on top of liquid manure and appear solid. A worker may walk on this crust and break through and drown. Workers can also slip and fall into liquid manure and drown. It is important to keep rescue equipment near the liquid manure storage site and avoid working alone. Some manure gases, such as methane, are explosive, and “no smoking” signs should be posted in or around the manure storage building (Deere & Co. 1994).
Application Hazards
Transfer and utilization of dry manure can be by hand or with mechanical aids like a front-end loader, skid-steer loader and manure spreader, each of which presents a safety hazard. Manure is spread onto land as fertilizer. Manure spreaders are generally pulled behind a tractor and powered by a power-take-off (PTO) from the tractor. They are classified into one of four types: box-type with rear beaters, flail, V-tank with side discharge and closed tank. The first two are used to apply solid manure; the V-tank spreader is used to apply liquid, slurry or solid manure; and the closed tank spreader is used to apply liquid manure. The spreaders throw the manure over large areas either to the rear or sides. Hazards include the machinery, falling objects, dust and aerosols. Several safety procedures are listed in table 3.
Table 3. Some safety procedures related to manure spreaders
1. Only one person should operate the machine to avoid inadvertent activation by another person.
2. Keep workers clear of active power-take offs (PTOs), beaters, augers and expellers.
3. Maintain all guards and shields.
4. Keep persons clear of rear and sides of the spreader, which can project heavy objects mixed into the manure as far as 30 m.
5. Avoid dangerous unplugging operations by preventing spreader plugging:
- Keep stones, boards and other objects out of the spreader.
- In freezing weather, make sure flails and chains on flail-type spreaders are loose and unfrozen before operation.
- Keep chains and beaters on beater-type spreaders in good operating order by replacing stretched chains and avoiding dropping loads of frozen manure onto the spreader chains.
- Never get into an operating spreader to clean it.
- Maintain the unloading auger and discharge expeller on V-tank spreaders so they operate freely.
- In cold weather, clean the spreader insides so wet manure will not freeze the moving parts.
6. Use good tractor and PTO safety practices.
7. Make sure the relief valve on closed-tank spreaders is operative to avoid excessive pressures.
8. When unhooking the spreader from the tractor, make sure the jack that holds the weight of the spreader tongue is secure and locked to prevent the spreader from falling.
9. When the spreader is creating airborne dust or aerosols, use respiratory protection.
Source: Deere & Co. 1994.
Case Report: Violence and Urban Park Rangers in Ireland
Rangers in parks in large Irish cities are employed to “keep the peace”, to “liaise with the public” (i.e., discourage vandalism and respond to any complaints that might be made) and to perform “light cleaning duties” (i.e., cleaning up rubbish and garbage such as broken bottles, needles and syringes discarded by drug abusers and used condoms). Their hours are unsociable: they report around mid-day and remain on duty until dusk when they are supposed to lock the park gates. This means long hours in the summertime that are somewhat compensated for by the shorter days in winter.
The majority of the parks have only one ranger who works alone, although there may be other local authority employees doing landscaping, gardening and other jobs in the park. Usually the only building in the park is the depot where gardening equipment is kept and where the staff may go for shelter in very severe weather. To avoid spoiling the ambiance, the depots are usually located in sequestered areas out of the public view where they are subject to misuse by vandals and marauding gangs of youths.
The park rangers are frequently exposed to violence. An employment policy that favoured the hiring of individuals with mild disabilities as rangers was recently supplanted when it was realized that public knowledge of such problems made these rangers ready targets for violent assault. Public authorities were not covered by the Irish health and safety legislation which, until recently, was applicable only to factories, building sites, docks and other process industries. As a result, there were no formalized arrangements for dealing with violence against park workers who, unlike their counterparts in some other countries, were not provided with firearms or other weapons. Nor was there any access to post-violence counselling.
The tendency to assign rangers who lived in the immediate neighbourhood to a particular park meant that they were more likely to be able to identify the trouble-makers likely to have been the perpetrators of violent acts. However, this also increased the danger of reprisals to the ranger for having “fingered” the culprits, making him or her less inclined to make formal complaints against their assailants.
Lack of an adequate police presence in the parks and the very early release from prison of convicted perpetrators were often crushing blows to the morale of the victims of the violence.
The trade unions representing the rangers and other public authority personnel have been active in promoting efforts to deal with violence. They now include training in recognizing and preventing violence in the courses they sponsor for safety representatives.
Even though the Irish health and safety legislation now covers public authority workers, the creation of a national committee to deal with both the control of violence and the provision of aftercare for its victims would be beneficial. While guidelines on preventing violence are now available to assist those engaged in assessing the risks of violence in workplaces, their use should be made mandatory for all occupations where violence is a risk. Furthermore, increased resources for and enhanced coordination with the city’s police force are desirable for dealing with the problem of violence and assault in the public parks.
Training in how to deal with individuals and groups likely to be violent should be make available to all workers who face this risk in their jobs. Such training might include how to approach and deal with individuals presenting indications of violent assault as well as self-defence manoeuvres.
Improved communications for reporting problem situations and requesting help would also be helpful. Installing telephones in all park depots would be a useful first step while “walkie-talkie” radios and cellular telephones would be useful when away from the depot. Video camera systems for surveillance of sensitive areas, such as the park depots and sports facilities, might help to deter violence.
Occupational Health and Safety Hazards in Public and Governmental Services
Public and government services encompass a wide variety of industrial and occupational categories. For example, included are workers employed within telecommunications and postal services, inspection and field services, as well as sewage treatment, recycling, landfill and hazardous waste operations. Depending on the individual country, industrial categories such as telecommunications and postal services may be located within either the public or private sector.
Occupational and environmental safety and health hazards in public and government services include exposure to chemicals, ergonomics, blood-borne pathogens, tuberculosis, machinery hazards, violence, motor vehicles and flammable materials. In the future, as public and government services continue to grow and become more complex, it is anticipated that occupational safety and health hazards will increase and become more widespread. In turn, led by tripartite (labour, management and government) initiatives, improvements in occupational safety and health hazard recognition and control will provide improved resolution of identified hazards.
Health Problems and Disease Patterns
Patterns or identifiable trends of occupational health problems have been associated with the type of work (i.e., use of visual display units (VDUs) or chemicals), as well as where the work is performed (i.e., indoors or outdoors).
Indoor work
The primary hazards associated with indoor work are poor or inadequate physical and work organization ergonomics, inadequate indoor air quality or heating, ventilation and air conditioning systems, chemicals, asbestos, workplace violence and electromagnetic fields (low-level radiation).
Health symptoms and disorders or illnesses have been associated with exposure to these hazards. Since the mid-1980s, a large number of ergonomic-related upper extremity physical illnesses have been reported. Disorders include carpal tunnel syndrome, ulnar deviation, thoracic outlet syndrome and tendinitis. Many of these are related to the introduction of new technology, particularly VDUs, as well as the use of hand tools and equipment. Causes of identified illnesses include physical and work organization factors.
Since the engineering and construction of “tight-buildings” in the 1970s, a pattern of increasing incidence of upper respiratory and dermatological health symptoms and illnesses has been observed. Such health problems are associated with improper maintenance of the heating, ventilation and air conditioning systems; chemical contaminants and microbiological agents; and the inadequate provision of fresh air and air flow.
Exposure to chemicals in indoor work environments has been linked to upper respiratory and dermatological health symptoms and illnesses. A variety of different chemical contaminants are emitted from copying machines, furniture, carpets, cleaning materials (solvents) and the heating, ventilation and air conditioning system. One particular syndrome, multiple chemical sensitivity, has been associated with chemical exposures in indoor work environments.
Asbestos exposure may occur when building renovation and service work are performed and asbestos products or materials are deteriorated or damaged, thus causing asbestos fibres to become airborne.
Since the 1980s, workplace violence and associated safety and health problems have become increasingly widespread. Work environments where increasing rates of workplace violence have been documented are characterized as follows: handling money, working with the public, working alone, coming into contact with patients or clients who may be violent and dealing with customer or client complaints.
Health concerns include physical harm and death. For example, homicide was the second leading cause of death in the US workplace in 1992, accounting for 17% of all workplace deaths. In addition, from 1980 to 1989 homicide was the leading cause of death in the workplace for women, as discussed in more detail in the chapter Violence in this Encyclopaedia.
Work with and exposure to electronic equipment and related electromagnetic fields or non-ionizing radiation has become commonplace, as is exposure to high frequency non-ionizing radiation emitting products such as laser and microwave transmission equipment, radio-frequency heat sealers and electric tools and generation equipment. The relationship between such exposures and consequent health effects such as cancer, visual and skin disorders is not yet clear and much research is still needed. Several chapters in this Encyclopaedia are devoted to these areas.
Outdoor work
Outdoor work environment occupational hazards include exposure to chemicals, lead, hazardous and solid waste, environmental conditions, inadequate ergonomics, motor vehicles, electrical and mechanical equipment and electromagnetic field emissions.
Exposure to chemicals occurs in several identified occupational categories including waste disposal operations, water and sanitation services, sewage treatment, domestic waste collection, postal collection and technician jobs in telecommunications. Such exposure has been related to upper respiratory, dermatological, cardiovascular and central nervous system illnesses. Exposure to lead occurs among telecommunications workers while performing splicing operations with and removing lead telecommunications cables. Such exposure has been liked to a variety of health symptoms and illnesses, including anaemia, peripheral and central nervous system disorders, sterility, kidney damage and birth defects.
Hazardous work environments are common to waste disposal operations, water and sanitation services, sewage treatment and domestic waste collection. Occupational safety and health hazards include microbiological and medical waste, chemicals, inadequate ergonomics, motor vehicles, confined spaces and electrical and mechanical equipment. Identified health symptoms and illnesses include upper respiratory, dermatological, upper and lower extremity musculoskeletal, cardiovascular, central nervous system and visual problems. Additional concerns include lacerations, heat exhaustion and stroke.
Inadequately designed workplace tools and equipment are common to all outside public and government service occupations. Hazards comprise poorly designed hand and power tools, machinery and motor vehicles. Associated health problems include upper and lower extremity musculoskeletal symptoms and illnesses. Safety-related concerns include visual problems, strains, sprains and fractured and broken bones.
Hazards associated with motor vehicles include poorly designed equipment (e.g., hoppers, compaction boxes and aerial equipment), as well as improperly operating machinery and equipment. Associated health problems comprise musculoskeletal injuries and death. Motor vehicle accidents account for the greatest number of injuries and fatalities outdoors.
Hazards associated with electrical and mechanical equipment include poorly designed equipment, electrical shock and electrocution, as well as chemical exposures. Health problems include strains, sprains, broken bones, central nervous and cardiovascular system disorders, as well as upper respiratory and dermatological disorders and death.
Work with or in close proximity to electrical transmission equipment and the associated electromagnetic fields of non-ionizing radiation emissions has been linked with the occurrence of certain central nervous system symptoms and disorders as well as cancer. However, scientific and epidemiological research has, as of yet, not clearly defined the degree of harm posed by electromagnetic fields.
Outdoor public and government services activities present several environmental and public health problems. For example, chemicals, microbiological agents, sewage and domestic waste may be used and disposed of improperly, thus finding their way into the water table as well as streams, lakes and oceans, causing environmental contamination. In turn, such waste may lead to the contamination of public water supplies as well as the creation of toxic dumps or sites. Such contamination has been related to the deterioration and destruction of the environment as well as public health. Associated human health effects include dermatological, central nervous and cardiovascular system health symptoms and disorders, as well as certain types of cancer.
Case Study: Animal Behaviours
Understanding what influences animal behaviour can help make for a safer work environment. Genetics and learned responses (operant conditioning) influence the way an animal behaves. Certain breeds of bulls are generally more docile than others (genetic influence). An animal that has balked or refused to enter an area, and is successful at not doing so, will likely refuse to do so the next time. On repeated tries it will get more agitated and dangerous. Animals respond to the way in which they are treated, and draw upon past experiences when reacting to a situation. Animals that are chased, slapped, kicked, hit, yelled at, frightened and so on, will naturally have a sense of fear when a human is near. Thus, it is important to do everything possible to make movement of animals successful on the first attempt and as free of stress as possible for the animal.
Domesticated animals living under fairly uniform conditions develop habits which are based on doing the same thing each day at a specific time. Confining bulls in a paddock and feeding them allows them to get used to humans and can be utilized with bull-confinement mating systems. Habits are also caused by regular changes in environmental conditions, such as temperature or humidity fluctuations when daylight turns to darkness. Animals are most active at the time of greatest change, which is at dawn or dusk, and least active either in the middle of the day or the middle of the night. This factor can be used to advantage in the movement or working of animals.
Like animals in the wild, domesticated animals can protect territories. During feeding, this can appear as aggressive behaviour. Studies have shown that feed distributed in large, unpredictable patches eliminates territorial behaviour in livestock. When feed is distributed uniformly or in predictable patterns, it may result in fighting by animals to secure the feed and exclude others. Territorial protection may also occur when a bull is permitted to remain with the herd. The bull may view the herd and the range they cover as his territory, which means he will defend it against perceived and real threats, such as humans, dogs and other animals. Introducing a new or strange bull of breeding age into the herd almost always results in fighting to establish the dominant male.
Bulls, due to having their eyes on the side of their head, have panoramic vision and very little depth perception. This means they can see about 270° around them, leaving a blind spot directly behind them and right in front of their noses (see figure 1). Sudden or unexpected movements from behind can “spook” the animal because it cannot determine the proximity or seriousness of the perceived threat. This can cause a “flight or fight” response in the animal. Because cattle have poor depth perception, they can also be easily frightened by shadows and movements outside of working or holding areas. Shadows falling within the working area may appear as a hole to the animal, which can cause it to balk. Cattle are colour blind, but do perceive colours as different shades of black and white.
Many animals are sensitive to noise (compared with humans), especially at high frequencies. Loud, abrupt noises, such as metal gates clanging shut, head chutes latching and/or humans yelling can cause stress in the animals.
Figure 1. Panoramic vision of cattle

Animal Husbandry
Animal husbandry—the rearing and use of animals—involves a wide variety of activities, including breeding, feeding, moving animals from one location to another, basic care (e.g., hoof care, cleaning, vaccinations), care for injured animals (either by animal handlers or veterinarians) and activities associated with particular animals (e.g., milking of cows, shearing of sheep, working with draught animals).
Such handling of livestock is associated with a variety of injuries and illnesses among humans. These injuries and illnesses may be due to direct exposure or may be due to environmental contamination from animals. The risk of injury and illness is dependent largely on the type of livestock. The risk of injury also depends on the particulars of animal behaviour (see also the articles in this chapter on specific animals). In addition, persons associated with animal husbandry are often more likely to consume products from the animals. Finally, the specific exposures depend on methods of handling livestock, which have emerged from geographical and social factors that vary across human society.
Hazards and Precautions
Ergonomic Risks
Personnel who work with cattle often have to stand, reach, bend or exert physical effort in sustained or unusual positions. Livestock workers do have an increased risk of joint pain of the back, hips and knees. There are several activities that place the livestock worker at ergonomic risk. For example, assisting with birthing of a large animal may put the farmworker in an unusual and strained position, whereas with a small animal, the worker may be required to work or lie in an inclement environment. Further, the worker may be injured by assisting animals who are ill and whose behaviour cannot be anticipated. More commonly, joint and back pain have to do with a repetitive motion, such as milking, during which the worker may crouch or kneel repeatedly.
Other cumulative trauma diseases are recognized in farmworkers, particularly livestock workers. These may be due to repetitive motion or frequent small injuries.
Solutions to reduce ergonomic risk include intensified educational efforts focused upon appropriate handling of animals, as well as engineering efforts to redesign the work environment and its tasks to accommodate animal and human factors.
Injuries
Animals are commonly recognized as agents of injury in surveys of injuries associated with agriculture. There are several postulated explanations for these observations. Close association between the worker and the animal, which often has unpredictable behaviour, puts the livestock worker at risk. Many livestock have superior size and strength. Injuries are often due to direct trauma from kicking, biting or crushing against a structure and often involve the worker’s lower extremity. The behaviour of workers may also contribute to risk of injury. Workers who penetrate the “flight zone” of livestock or who position themselves in livestock “blind spots” are at increased risk of injury resulting from flight reaction, butting, kicking and crushing.
Figure 1. Panoramic vision of cattle
Women and children are over-represented among injured livestock workers. This may be due to societal factors resulting in women and children doing more of the animal-related work, or it may be due to exaggerated size differences between the animals and worker or, in the case of children, use of handling techniques to which livestock are unaccustomed.
Specific interventions to prevent animal-associated injuries include intense educational efforts, selecting animals that are more compatible with humans, selecting workers who are less likely to agitate animals and engineering approaches that decrease the risk of exposure of humans to animals.
Zoonotic Diseases
Livestock rearing requires close association of workers and animals. Humans may become infected by organisms normally present on animals, which are rarely human pathogens. In addition, the tissues and behaviour associated with infected animals may expose workers who would experience few, if any, exposures if they were working with healthy livestock.
The relevant zoonotic diseases include numerous viruses, bacteria, mycobacteria, fungi and parasites (see table 1). Many zoonotic diseases, such as anthrax, tinea capitis or orf, are associated with skin contamination. In addition, contamination resulting from exposure to a diseased animal is a risk factor for rabies and tularaemia. Because livestock workers often are more likely to ingest under-treated animal products, such workers are at risk of diseases such as Campylobacter, cryptosporidiosis, salmonellosis, trichinosis or tuberculosis.
Table 1. Zoonotic diseases of livestock handlers
|
Disease |
Agent |
Animal |
Exposure |
|
Anthrax |
Bacteria |
Goats, other herbivores |
Handling hair, bone or other tissues |
|
Brucellosis |
Bacteria |
Cattle, swine, goats, sheep |
Contact with placenta and other contaminated tissues |
|
Campylobacter |
Bacteria |
Poultry, cattle |
Ingestion of contaminated food, water, milk |
|
Cryptosporidiosis |
Parasite |
Poultry, cattle, sheep, small mammals |
Ingestion of animal faeces |
|
Leptospirosis |
Bacteria |
Wild animals, swine, cattle, dogs |
Contaminated water on open skin |
|
Orf |
Virus |
Sheep, goats |
Direct contact with mucous membranes |
|
Psittacosis |
Chlamydia |
Parakeets, poultry, pigeons |
Inhaled desiccated droppings |
|
Q fever |
Rickettsia |
Cattle, goats, sheep |
Inhaled dust from contaminated tissues |
|
Rabies |
Virus |
Wild carnivores, dogs, cats, livestock |
Exposure of virus-laden saliva to breaks in skin |
|
Salmonellosis |
Bacteria |
Poultry, swine, cattle |
Ingestion of food from contaminated organisms |
|
Tinea capitis |
Fungus |
Dogs, cats, cattle |
Direct contact |
|
Trichinosis |
Roundworm |
Swine, dogs, cats, horses |
Eating poorly cooked flesh |
|
Tuberculosis, bovine |
Mycobacteria |
Cattle, swine |
Ingestion of unpasteurized milk; inhalation of airborne droplets |
|
Tularaemia |
Bacteria |
Wild animals, swine, dogs |
Inoculation from contaminated water or flesh |
The control of zoonotic diseases must focus on the route and source of exposure. Elimination of the source and/or interruption of the route are essential to disease control. For example, there must be proper disposal of the carcasses of diseased animals. Often, the human disease can be prevented by eliminating the disease in animals. Additionally, there should be adequate processing of animal products or tissues before use in the human food chain.
Some zoonotic diseases are treated in the livestock worker with antibiotics. However, routine prophylactic antibiotic usage on livestock may cause emergence of resistant organisms of general public health concern.
Blacksmithing
Blacksmithing (farrier work) involves primarily musculoskeletal and environmental injury. The manipulation of metal to be used in animal care, such as for horseshoes, does demand heavy work requiring substantial muscle activity to prepare the metal and position animal legs or feet. Furthermore, applying the created product, such as a horseshoe, to the animal in farrier work is an additional source of injury (see figure 2).
Figure 2. Blacksmith shoeing a horse in Switzerland

Often, the heat required to bend metal involves exposure to noxious gases. A recognized syndrome, metal fume fever, has a clinical picture similar to pulmonary infection and results from inhalation of fumes of nickel, magnesium, copper or other metals.
Adverse health effects associated with blacksmithing can be alleviated by working with adequate respiratory protection. Such respiratory devices include respirators or powered air-purifying respirators with cartridges and pre-filters capable of filtering acid gas/organic vapours and metal fumes. If the farrier work occurs in a fixed location, local exhaust ventilation should be installed for the forge. Engineering controls, which place distance or barricades between the animal and the worker, will reduce the risk of injury.
Animal Allergies
All animals possess antigens which are non-human and could therefore serve as potential allergens. In addition, livestock are often hosts for mites. Since there are a large number of potential animal allergies, recognition of a specific allergen requires careful and thorough disease and occupational histories. Even with such data, recognition of a specific allergen may be difficult.
The clinical expression of animal allergies may include an anaphylaxis-type picture, with hives, swelling, nasal discharge and asthma. In some patients, itching and nasal discharge may be the only symptoms.
Controlling exposure to animal allergies is a formidable task. Improved practices in animal husbandry and changes in livestock facility ventilation systems may make it less likely that the livestock handler will be exposed. However, there may be little that can be done, other than desensitization, to prevent the formation of specific allergens. In general, desensitizing a worker can be performed only if the specific allergen is adequately characterized.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."