- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
System Design in Diamond Manufacturing
The author acknowledges the assistance of Mr. E. Messer and Prof. W. Laurig for their contribution to the biomechanical and design aspects, and to Prof. H. Stein and Dr. R. Langer for their help with the physiological aspects of the polishing process. The research was supported by a grant from the Committee for Research and Prevention in Occupational Safety and Health, Ministry of Labor and Social Affairs, Israel.
The design of manually operated work benches and working methods in the diamond polishing industry has not changed for hundreds of years. Occupational health studies of diamond polishers have identified high rates of musculoskeletal disorders of the hands and arms, specifically, ulnar neuropathy at the elbow. These are due to the high musculoskeletal demands placed on the upper body in the practice of this manually intensive profession. A study conducted at the Technion Israel Institute of Technology addressed itself to the investigation of the ergonomic aspects and occupational diseases relating to safety issues among craftsmen in the diamond polishing industry. The tasks in this industry, with its high demands for manipulative movements, include movements that require frequent, rapid hand exertions. An epidemiological review conducted during the years 1989-1992 in the Israeli diamond industry has pointed out that the manipulative movements experienced in diamond polishing very often cause serious health problems to the worker in the upper extremities and in the upper and lower back. When such occupational hazards affect workers, it produces a chain reaction that eventually affects the industry’s economy as well.
For thousands of years, diamonds have been objects of fascination, beauty, richness and capital value. Skillful craftsmen and artists have tried, through the ages, to create beauty by enhancing the shape and values of this unique form of hard carbon crystal formation. In contrast to the continuing achievements of artistic creation with the native stone and the emergence of a great international industry, very little has been done to improve some questionable working conditions. A survey of the diamond museums in England, South Africa and Israel allows one to draw the historical conclusion that the traditional polishing workplace has not changed for hundreds of years. The typical diamond polishing tools, working bench and work processes are described by Vleeschdrager (1986), and they have been found to be universally common to all polishing setups.
Ergonomic evaluation performed at diamond manufacturing setups points to a great lack of engineering design of the polishing workstation, which causes back pain and neck and arm stress due to working posture. A micromotion study and biomechanical analysis of motion patterns involved in the diamond polishing profession indicate extremely intense hand and arm movements that involve high acceleration, rapid movement and a great degree of repetitiveness in short-period cycles. A symptom survey of diamond polishers indicated that 45% of the polishers were younger than 40 years of age, and although they represent a young and healthy population, 64% reported pain in the shoulders, 36% pain in the upper arm and 27% pain in the lower arm. The act of polishing is performed under an extensive amount of “hand on tool” pressure which is applied to a vibrating polishing disk.
The first known description of a diamond polishing workstation was given in 1568 by the Italian goldsmith, Benvenuto Cellini, who wrote: “One diamond is rubbed against another until by mutual abrasion both take a form which the skilled polisher wishes to achieve.” Cellini’s description could have been written today: the role of the human operator has not changed over these 400 years. If one examines the working routines, hand tools and the nature of the decisions involved in the process one can see that the user-machine relationship has also hardly changed. This situation is unique among most industries where enormous changes have occurred with the entry of automation, robotics and computer systems; these have completely changed the role of the worker in the world today. Yet the polishing work cycle has been found to be very similar, not only in Europe where the polishing craft started, but in most industries all over the globe, whether in advanced facilities in the United States, Belgium or Israel—which specialize in fancy geometry and higher-value diamond products—or the facilities in India, China and Thailand, which generally produce popular shapes and mid-value products.
The polishing process is based on grinding the fixed rough diamond over diamond dust bonded to the polishing disk’s surface. Owing to its hardness, only grinding by friction against similar carbon material is effective in manipulating the diamond’s shape to its geometric and brilliant finish. The workstation hardware is composed of two basic groups of elements: workstation mechanisms and hand-held tools. The first group includes an electric motor, which rotates a polishing disk on a vertical cylindrical shaft, perhaps by a single direct drive; a solid flat table which surrounds the polishing disk; a bench seat and a source of light. The hand-held operating tools consist of a diamond holder (or tang) which houses the rough stone during all polishing phases and is usually held in the left palm. The work is magnified with a convex lens which is held between the first, second and third fingers of the right hand and viewed with the left eye. This method of operation is imposed by a strict training process which in most cases does not take handedness into account. During work the polisher assumes a reclining posture, pressing the holder to the grinding disk. This posture requires the support of the arms on the working table in order to stabilize the hands. As a result, the ulnar nerve is vulnerable to external lesions due to its anatomical position. Such an injury is common among diamond polishers and has been accepted as an occupational disease since the 1950s. The number of polishers worldwide today is around 450,000, of whom approximately 75% are located in the Far East, primarily India, which has dramatically expanded its diamond industry in the last two decades. The act of polishing is done manually, with each of the diamond facets being produced by polishers who are trained and skilled with respect to a certain part of the stone’s geometry. The polishers are a clear majority of the diamond craft force, composing about 80% of the overall industry’s workforce. Therefore, most of the occupational risks of this industry can be addressed through improving the operation of the diamond polishing workstation.
Analysis of the motion patterns involved in polishing shows that the polishing routine consists of two subroutines: a simpler routine called the polish cycle, which represents the basic diamond polishing operation, and a more important one called the facet cycle, which involves a final inspection and a change of the stone’s position in the holder. The overall procedure includes four basic work elements:
- Polishing. This is simply the actual polishing operation.
- Inspection. Every few seconds the operator, using a magnifying glass, visually inspects the progress made on the polished facet.
- Dop adjustment. An angular adjustment is made to the diamond holder’s head (dop).
- Stone change. The act of changing facets, which is done by turning the diamond through a predetermined angle. It takes about 25 repetitions of these four elements to polish a diamond’s facet. The number of such repetitions depends upon such aspects as operator’s age, stone hardness and characteristics, time of day (owing to operator fatigue), and so on. On average, each repetition takes about four seconds. A micromotion study as performed on the polishing process and the methodology used is given by Gilad (1993).
Two of the elements—polishing and inspection—are performed in relatively static working postures while so-called “hand to polish” (H to P) and “hand to inspect” (H to I) actions require short and fast movements of the shoulder, elbow and wrist. Most of the actual movements of both hands are performed by flexion and extension of the elbow and pronation and supination of the elbow. Body posture (back and neck) and all other movements except wrist deviation are relatively unchanged during normal work. The stone holder, which is constructed of a square cross-sectional steel rod, is held so that it presses on blood vessels and bone, which can result in a reduction of blood flow to the ring and little fingers. The right hand holds the magnifying glass all during the polishing cycle, exerting isometric pressure on the three first fingers. For most of the time the right and left hands follow parallel movement patterns, while in the “hand to grind” movement the left hand leads and the right hand starts moving after a short delay, and in the “hand to inspect” movement the order is reversed. Right-hand tasks involve either holding the magnifying glass to the inspecting left eye while supporting the left hand (elbow flexion), or by putting pressure on the diamond holder head for better grinding (elbow extension). These fast movements result in rapid accelerations and decelerations that end up in a very precise placing of the stone on the grinding disk, which requires a high level of manual dexterity. It should be noted that it takes long years to become proficient to the point where work movements are almost embedded reflexes executed automatically.
On the face of it, diamond polishing is a simple straightforward task, and in a way it is, but it requires much skill and experience. In contrast to all other industries, where raw and processed material is controlled and manufactured according to exact specifications, the diamond in the rough is not homogeneous and each diamond crystal, large or small, has to be checked, categorized and treated individually. Apart from the needed manual skill, the polisher has to make operational decisions at every polishing phase. As a result of the visual inspection, decisions must be made on such factors as angular spatial correction—a three-dimensional judgment—amount and duration of pressure to be applied, angular positioning of the stone, contact point on the grinding disk, among others. Many points of significance have to be considered, all in the average time of four seconds. it is important to understand this decision-making process when improvements are designed.
Before one can advance to the stage at which motion analysis can be used for setting better ergonomic design and engineering criteria for a polishing workstation, one has to be aware of yet further aspects involved in this unique user-machine system. In this post-automation age, we still find the production part of the successful and expanding diamond industry almost untouched by the enormous technological advances made in the last few decades. While almost all other sectors of industry have undergone continuing technology change that defined not only production methods but the products themselves, the diamond industry has remained virtually static. A plausible reason for this stability may be the fact that neither the product nor the market have changed through the ages. The design and shapes of diamonds have in practice remained almost unchanged. From the business point of view, there was no reason to change the product or the methods. Furthermore, since most of the polishing work is done by subcontracting to individual workers, the industry had no problem in regulating the labour force, adjusting the flow of work and the supply of rough diamonds according to market fluctuations. As long as the production methods do not change, the product will not change either. Once the use of more advanced technology and automation are adopted by the diamond industry, the product will change, with a greater variety of forms available in the market. But a diamond still has a mystic quality that sets it apart from other products, a value that may well decrease when it comes to be regarded as merely another mass-produced item. Recently though, market pressures and the arrival of new production centres, mainly in the Far East, are challenging the old established European centres. These are forcing the industry to examine new methods and production systems and the role of the human operator.
When considering improving the polishing workstation, one must look upon it as part of a user-machine system that is governed by three main factors: the human factor, the technology factor and the business factor. A new design that takes account of ergonomic principles will provide a springboard to a better production cell in the broad sense of the term, meaning comfort over long working hours, a better quality product and higher production rates. Two different design approaches have been considered. One involves a redesign of the existing workstation, with the worker given the same tasks to perform. The second approach is to look at the polishing task in an unbiased manner, aiming at an optimal, total station and task design. A total design should not be based on the present workstation as input but on the future polishing task, generating design solutions that integrate and optimize the needs of the three above-mentioned system factors.
At present, the human operator performs most of the tasks involved in the polishing act. These human-performed tasks rely on “filling” and working experience. This is a complex psychophysiological process, only partially conscious, based on trial and error input which enables an operator to execute complex operations with a good prediction of the outcome. During periodic daily work cycles of thousands of identical movements, “filling” manifests itself in the human-automatic operation of motor memory executed with great precision. For each of these automatic motions, tiny corrections are made in response to feedback received from the human sensors, like the eyes, and the pressure sensors. In any future diamond polishing workstation these tasks will continue to be performed in a different way. As to the material itself, in the diamond industry, by contrast with most other industries, the relative value of the raw material is very high. This fact explains the importance of making maximal use of the rough diamond’s volume (or stone weight) in order to get the largest net stone possible after polishing. This emphasis is paramount throughout all the stages of diamond processing. Productivity and efficiency are not measured by reference to time only, but also by the size and precision achieved.
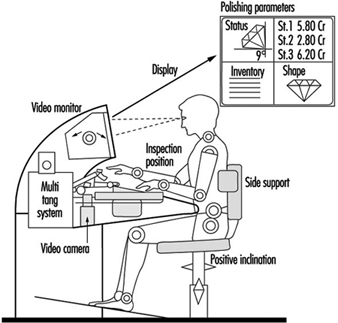
The four repetitive work elements—“polish”, “hand to inspect”, “inspect” and “hand to polish”—as performed in the polishing act, can be classified under the three main task categories: motor tasks for motion elements, visual tasks as sensing elements, and control and management as decision-content elements. Gilad and Messer (1992) discuss design considerations for an ergonomic workstation. Figure 1 presents an outline of an advanced polishing-cell. Only the general construction is indicated, since the details of such a design are guarded as a professionally restricted “know-how”. The term polishing cell is used since this user-machine system includes a totally different approach to polishing diamonds. In addition to ergonomic improvements, the system consists of mechanical and optoelectronic devices that enable the manufacture of three to five stones at the same time. Parts of visual and control tasks have been transferred to technical operators and management of the production cell is mediated via a display unit that provides momentary information about geometry, weight and optional operation moves in order to support optimal operating acts. Such a design takes the polishing workstation a few steps ahead into modernization, incorporating an expert system and a visual control system to replace the human eye in all routine work. Operators will still be able to intervene at any point, set up data and make human judgements on machine performance. The mechanical manipulator and the expert system will form a closed-loop system capable of performing all polishing tasks. Material handling, quality control and final approval will still reside with the operator. At this stage of an advanced system, it would be appropriate to consider the employment of higher technology such as a laser polisher. At present, lasers are being used extensively to saw and cut diamonds. Using a technologically advanced system will radically change the human task description. The need for skilled polishers will diminish until they will deal only with polishing larger, top-valued diamonds, probably with supervision.
Figure 1. Schematic presentation of a polishing-cell
Workers with Special Needs
Designing for Disabled Persons is Designing for Everyone
There are so many products on the market that readily reveal their unfitness for the general population of users. What evaluation should one make of a doorway too narrow to comfortably accommodate a stout person or pregnant woman? Shall its physical design be faulted if it satisfies all relevant tests of mechanical function? Certainly such users cannot be regarded as disabled in any physical sense, since they may be in a state of perfect health. Some products need considerable handling before one can force them to perform as desired—certain inexpensive can openers come, not altogether trivially, to mind. Yet a healthy person who may experience difficulty operating such devices need not be considered disabled. A designer who successfully incorporates considerations of human interaction with the product enhances the functional utility of his or her design. In the absence of good functional design, people with a minor disability may find themselves in the position of being severely hampered. It is thus the user-machine interface that determines the value of design for all users.
It is a truism to remind oneself that technology exists to serve human beings; its use is to enlarge their own capabilities. For disabled persons, this enlargement has to be taken some steps further. For instance in the 1980s, a good deal of attention was paid to the design of kitchens for disabled people. The experience gained in this work penetrated design features for “normal” kitchens; the disabled person in this sense may be considered a pioneer. Occupationally-induced impairments and disabilities—one has but to consider the musculoskeletal and other complaints suffered by those confined to sedentary tasks so common in the new workplace—similarly call for design efforts aimed not only also preventing the recurrence of such conditions, but at the development of user-compatible technology adapted to the needs of workers already affected by work-related disorders.
The Broader Average Person
The designer should not focus on a small, unrepresentative population. Among certain groups it is most unwise to entertain assumptions concerning similarities among them. For example, a worker injured in a certain way as an adult may not necessarily be anthropometrically quite so different from an otherwise comparable, healthy person, and may be considered as part of the broad average. A young child so injured will display a considerably different anthropometry as an adult since his muscular and mechanical development will be steadily and sequentially influenced by preceding growth stages. (No conclusions as to comparability as adults ought to be ventured as regards the two cases. They must be regarded as two distinct, specific groups, only the one being included among the broad average.) But as one strives for a design suitable for, say, 90% of the population, one should exert fractionally greater pains to increase this margin to, say, 95%, the point being that in this way the need for design for specific groups can be reduced.
Another way to approach design for the broader average population is to produce two products, each one designed roughly to fit the two percentile extremes of human differences. Two sizes of chair, for instance, might be built, the one with brackets allowing it to be adjusted in height from 38 to 46 cm, and the other one from 46 to 54 cm; two sizes of pliers already exist, one fitting larger and average sizes of men’s hands and the other fitting average women’s hands and hands of smaller men.
It would be a well-advised company policy to reserve annually a modest amount of money to have worksites analysed and made more suitable for workers, a move that would prevent illness and disability due to excessive physical load. It also increases the motivation of workers when they understand that management is actively trying to improve their work environment, and more impressively so when elaborate measures sometimes have to be undertaken: thorough work analysis, the construction of mock-ups, anthropometrical measurements, and even the specific design of units for the workers. In a certain company, in fact, the conclusion was that the units should be redesigned at every worksite because they caused physical overload in the form of too much standing, there were unsuitable dimensions associated with the seated positions, and there were other deficiencies as well.
Costs, Benefits and Usability of Design
Cost/benefit analyses are developed by ergonomists in order to gain insight into the results of ergonomic policies other than those that are economic. In the present day, evaluation in the industrial and commercial realms includes the negative or positive impact of a policy on the worker.
Methods of evaluating quality and usability are currently the subject of active research. The Rehabilitation Technology Useability Model (RTUM), as shown in figure 1, can be utilized as a model for evaluating the usability of a product within rehabilitation technology and to illuminate the various aspects of the product which determine its usability.
Figure 1. The Rehabilitation Technology Useability Model (RTUM)
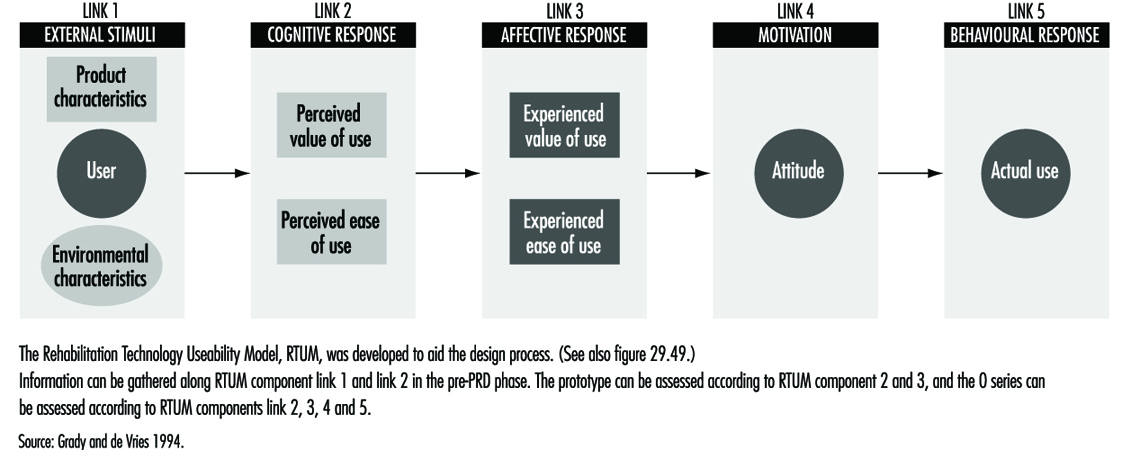
From the strictly economic point of view, the costs of creating a system in which a given task can be performed or in which a certain product can be made can be specified; it scarcely needs mentioning that in these terms each company is interested in a maximum return on its investment. But how can the real costs of task performance and product manufacturing in relation to financial investment be determined when one takes into account the varying exertions of workers’ physical, cognitive and mental systems? In fact, the judging of human performance itself is, among other factors, based on the workers’ perception of what has to be done, their view of their own value in doing it, and their opinion of the company. It is actually the intrinsic satisfaction with work that is the norm of value in this context, and this satisfaction, together with the aims of the company, constitute one’s reason for performing. Worker well-being and performance are thus based on a wide spectrum of experiences, associations and perceptions that determine attitudes towards work and the ultimate quality of performance—an understanding upon which the RTUM model is predicated.
If one does not accept this view, it becomes necessary to regard investment only in relation to doubtful and unspecified results. If ergonomists and physicians wish to improve the work environment of disabled people—to produce more from machine operations and enhance the usability of the tools used—they will encounter difficulties in finding ways to justify the financial investment. Typically, such justification has been sought in savings realized by prevention of injury and illness due to work. But if the costs of illness have been borne not by the company but by the state, they become financially invisible, so to speak, and are not seen as work-related.
Nevertheless, the awareness that investment in a healthy working environment is money well spent has been growing with the recognition that the “social” costs of incapacities are translatable in terms of ultimate costs to a country’s economy, and that value is lost when a potential worker is sitting about at home making no contribution to society. Investing in a workplace (in terms of adapting a work station or providing special tools or perhaps even help in personal hygiene) can not only reward a person with job satisfaction but can help make him or her self-sufficient and independent of social assistance.
Cost/benefit analyses can be carried out in order to determine whether special intervention in the workplace is justified for disabled persons. The following factors represent sources of data that would form the object of such analyses:
1. Personnel
- Absence. Will the disabled worker have a satisfactory attendance record?
- Is it likely that extra costs may be incurred for special task instruction?
- Are personnel changes called for? Their costs must be considered also.
- Can accident compensation rates be expected to increase?
2. Safety
- Will the job being considered for the disabled worker involve safety regulations?
- Will special safety regulations be involved?
- Is the work characterized by a considerable frequency of accidents or near accidents?
3. Medical
- As regards the worker whose disability is being examined with a view to his or her re-entry into the workplace, the nature and seriousness of the incapacity must be assessed.
- The extent of the disabled worker’s absence must also be taken into account.
- What is the character and frequency of the worker’s “minor” symptoms, and how are they to be dealt with? Can the future development of related “minor” illnesses capable of hampering the worker’s efficiency be foreseen?
As concerns time lost from work, these calculations can be made in terms of wages, overhead, compensation and lost production. The sort of analyses just described represents a rational approach by which an organization can arrive at an informed decision as to whether a disabled worker is better off back on the job and whether the organization itself will gain by his or her return to work.
In the preceding discussion, designing for the broader population has received a focus of attention heightened by emphasis on specific design in relation to usability and the costs and benefits of such design. It is still a difficult task to make the needed calculations, including all relevant factors, but at present, research efforts are continuing that incorporate modelling methods in their techniques. In some countries, for example the Netherlands and Germany, government policy is making companies more responsible for job-related personal harm; fundamental changes in regulatory policies and insurance structures are, clearly, to be expected to result from trends of this sort. It has already become a more or less settled policy in these countries that a worker who suffers a disabling accident at work should be provided with an adapted work station or be able to perform other work within the company, a policy that has made the treatment of the disabled a genuine achievement in the humane treatment of the worker.
Workers with Limited Functional Capacity
Whether design is aimed at the disabled or at the broader average, it is hindered by a scarcity of research data. Handicapped people have been the subjects of virtually no research efforts. Therefore, in order to set up a product requirements document, or PRD, a specific empirical research study will have to be undertaken in order to gather that data by observation and measurement.
In gathering the information needed about the disabled worker or user it is necessary to consider not only the current functional status of the disabled person, but to make the attempt to foresee whatever changes might be the result of the progression of a chronic condition. This kind of information can, in fact, be elicited from the worker directly, or a medical specialist can supply it.
In designing, for instance, a work action to which data about the worker’s physical strength is relevant, the designer will not choose as a specification the maximum strength which the disabled person can exert, but will take into account any possible diminution in strength that a progression in the worker’s condition might bring about. Thus the worker will be enabled to continue to use the machines and tools adapted or designed for him or at the work station.
Furthermore, designers should avoid designs that involve manipulations of the human body at the far extremes of, say, the range of motion of a body part, but should accommodate their designs to the middle ranges. A simple but very common illustration of this principle follows. A very common part of the drawers of kitchen and office cabinets and desks is a handle that has the form of a little shelf under which one places the fingers, exerting upward and forward force to open the drawer. This manoeuvre requires 180 degrees of supination (with the palm of the hand up) in the wrist—the maximum point for the range of this sort of motion of the wrist. This state of affairs may present no difficulty for a healthy person, provided that the drawer can be opened with a light force and is not awkwardly situated, but makes for strain when the action of the drawer is tight or when the full 180-degree supination is not possible, and is a needless burden on a disabled person. A simple solution—a vertically placed handle—would be mechanically far more efficient and more easily manipulated by a larger portion of the population.
Physical Functioning Ability
In what follows, the three chief areas of limitation in physical functional ability, as defined by the locomotion system, the neurological system and the energy system, will be discussed. Designers will gain some insight into the nature of user/worker constraints in considering the following basic principles of bodily functions.
The locomotion system. This consists of the bones, joints, connective tissues and muscles. The nature of the joint structure determines the range of motion possible. A knee joint, for example, shows a different degree of movement and stability than the joint of the hip or the shoulder. These varying joint characteristics determine the actions possible to the arms, hands, feet, and so on. There are also different types of muscle; it is the type of muscle, whether the muscle passes over one or two joints, and the location of the muscle that determines, for a given body part, the direction of its movement, its speed, and the strength which it is capable of exerting.
The fact that this direction, speed and strength can be characterized and calculated is of great importance in design. For disabled people, one has to take it into account that the “normal” locations of muscles have been disturbed and that the range of motion in joints has been changed. In an amputation, for instance, a muscle may function only partly, or its location may have changed, so that one has to examine the physical ability of the patient carefully to establish what functions remain and how reliable they may be. A case history follows.
A 40-year-old carpenter lost his thumb and the third finger of his right hand in an accident. In an effort to restore the carpenter’s capacity for work, a surgeon removed one of the patient’s great toes and he replaced the missing thumb with it. After a period of rehabilitation, the carpenter returned to work but found it impossible to do sustained work for more than three to four hours. His tools were studied and found to be unfitted to the “abnormal” structure of his hand. The rehabilitation specialist, examining the “redesigned” hand from the point of view of its new functional ability and form was able to have new tools designed that were more appropriate and usable with respect to the altered hand. The load on the worker’s hand, previously too heavy, was now within a usable range, and he regained his ability to continue work for a longer time.
The neurological system. The neurological system can be compared to a very sophisticated control room, complete with data collectors, whose purpose it is to initiate and govern one’s movements and actions by interpreting information relating to those aspects of the body’s components relating to position and mechanical, chemical and other states. This system incorporates not only a feedback system (e.g., pain) that provides for corrective measures, but a “feed-forward” capability which expresses itself anticipatorily so as to maintain a state of equilibrium. Consider the case of a worker who reflexively acts so as to restore a posture in order to protect himself from a fall or from contact with dangerous machine parts.
In disabled persons, the physiological processing of information can be impaired. Both the feedback and the feed-forward mechanisms of visually impaired people are weakened or absent, and the same is true, on an acoustic level, among the hearing-impaired. Furthermore the important governing circuits are interactive. Sound signals have an effect on the equilibrium of a person in conjunction with proprioceptive circuits that situate our bodies in space, so to speak, via data gathered from muscles and joints, with the further help of visual signals. The brain can function to overcome quite drastic deficiencies in these systems, correcting for errors in the coding of information and “filling in” missing information. Beyond certain limits, to be sure, incapacity supervenes. Two case histories follow.
Case 1. A 36-year-old woman suffered a lesion of the spinal cord due to an automobile accident. She is able to sit up without assistance and can move a wheelchair manually. Her trunk is stable. The feeling in her legs is gone, however; this defect includes an inability to sense temperature changes.
She has a sitting workplace at home (the kitchen is designed to allow her to work in a seated position). The safety measure has been taken of installing a sink in a position sufficiently isolated that the risk of burning her legs with hot water is minimized, since her inability to process temperature information in the legs leaves her vulnerable to being unaware of being burned.
Case 2. A five-year-old boy whose left side was paralysed was being bathed by his mother. The doorbell rang, the mother left the boy alone to go to the front door, and the boy, turning on the hot-water tap, suffered burns. For safety reasons, the bath should have been equipped with a thermostat (preferably one that the boy could not have overridden).
The energy system. When the human body has to perform physical labour, physiological changes, notably in the form of interactions in the muscle cells, take place, albeit relatively inefficiently. The human “motor” converts only about 25% of its energy supply to mechanical activity, the remainder of the energy representing thermal losses. The human body is therefore not especially suited to heavy physical labour. Exhaustion sets in after a certain time, and if heavy labour has to be performed, reserve energy sources are drawn upon. These sources of reserve energy are always used whenever work is carried out very rapidly, is started suddenly (without a warm-up period) or involves heavy exertion.
The human organism obtains energy aerobically (via oxygen in the bloodstream) and anaerobically (after depleting aerobic oxygen, it calls upon small, but important reserve units of energy stored in muscle tissue). The need for fresh air supplies in the workplace naturally draws the focus of discussion of oxygen usage toward the aerobic side, working conditions that are strenuous enough to call forth anaerobic processes on a regular basis being extraordinarily uncommon in most workplaces, at least in the developed countries. The availability of atmospheric oxygen, which relates so directly to human aerobic functioning, is a function of several conditions:
- Ambient air pressure (approximately 760 torr, or 21.33 kPa at sea level). High-altitude task performance can be profoundly affected by oxygen deficiency and is a prime consideration for workers in such conditions.
- For workers doing heavy labour, ventilation is necessary to ensure refreshment of the air supply, allowing the volume of air respired per minute to be increased.
- Ambient oxygen makes its way into the bloodstream via the alveoli by diffusion. At higher blood pressures, the diffusion surface is enlarged and thereby the oxygen capacity of the blood.
- An increase in oxygen diffusion to the tissues causes an increase of the diffusion surface and consequently of the oxygen level.
- People with certain heart problems suffer when, with increased cardiac output (together with the oxygen level), the blood circulation changes in favour of the muscles.
- By contrast with oxygen, because of the large reserves of glucose, and especially fat, the energy source (“fuel”) need not be continuously delivered from the outside. In heavy labour, it is merely glucose, with its high energy value, that is used. With lighter work, fat is called upon, at a rate varying with the individual. A brief, general case history follows.
A person suffering from asthma or bronchitis, both of which are diseases affecting the lungs, causes the worker severe limitation in his or her work. The work assignment of this worker should be analysed with respect to factors such as physical load. The environment should be analysed as well: clean ambient air will contribute substantially to workers’ well-being. Furthermore, the workload should be balanced through the day, avoiding peak loads.
Specific Design
In some cases, however, there is still a need for specific design, or design for very small groups. Such a need arises when the tasks to be performed and the difficulties a disabled person is experiencing are excessively large. If the needed specific requirements cannot be made with the available products on the market (even with adaptations), specific design is the answer. Whether this sort of solution may be costly or cheap (and aside from humanitarian issues) it must be nonetheless regarded in the light of workability and support to the firm’s viability. A specially designed worksite is worthwhile economically only when the disabled worker can look forward to working there for years and when the work he or she does is, in production terms, an asset to the company. When this is not the case, although the worker may indeed insist upon his or her right to the job, a sense of realism should prevail. Such touchy problems should be approached in a spirit of seeking a solution by cooperative endeavours at communication.
The advantages of specific design are as follows:
- The design is custom made: it fits the problems to be solved to perfection.
- The worker so served can return to work and a life of social participation.
- The worker can be self-sufficient, independent of welfare.
- The costs of any personnel changes that the alternative might involve are avoided.
The disadvantages of specific design are:
- The design is unlikely to be used for even one other person, let alone a larger group.
- Specific design is often costly.
- Specifically designed products must often be handmade; savings owing to mass methods are most often not realizable.
Case 1. For example, there is the case of a receptionist in a wheelchair who had a speech problem. Her speech difficulty made for rather slow conversations. While the firm remained small, no problems arose and she continued to work there for years. But when the firm enlarged, her disabilities began to make themselves problematic. She had to speak more rapidly and to move about considerably faster; she could not cope with the new demands. However, solutions to her troubles were sought and reduced themselves to two alternatives: special technical equipment might be installed so that the deficiencies that degraded the quality of some of her tasks could be compensated for, or she could simply choose a set of tasks involving a more desk-bound workload. She chose the latter course and still works for the same company.
Case 2. A young man, whose profession was the production of technical drawings, suffered a high level spinal cord lesion due to diving in shallow waters. His injury is severe enough for him to require help with all his daily activities. Nevertheless, with the help of a computer-aided design (CAD) software, he continues to be able make his living at technical drawing and lives, financially independent, with his partner. His work space is a study adapted for his needs and he works for a firm with which he communicates by computer, phone and fax. To operate his personal computer, he had to have certain adaptations made to the keyboard. But with these technical assets he can earn a living and provide for himself.
The approach for specific design is not different from other design as described above. The only insurmountable problem that may arise during a design project is that the design objective cannot be achieved on purely technical grounds—in other words, it can’t be done. For example, a person suffering from Parkinson’s disease is prone, at a certain stage in the progression of his or her condition, to fall over backwards. An aid which would prevent such an eventuality would of course represent the desired solution, but the state of the art is not such that such a device can yet be built.
System Ergonomic Design and Workers with Special Physical Needs
One can treat bodily impairment by medically intervening to restore the damaged function, but the treatment of a disability, or deficiency in the ability to perform tasks, can involve measures far less developed in comparison with medical expertise. As far as the necessity of treating a disability is concerned, the severity of the handicap strongly influences such a decision. But given that treatment is called for, however, the following means, taken singly or in combination, form the choices available to the designer or manager:
- leaving out a task
- compensating for a worker’s deficiency in performing a task element by using a machine or another person’s help
- differentiation of the task order, that is, dividing the task into more manageable subtasks
- modification of the tools used in the task
- special design of tools and machines.
From the specific ergonomic point of view, treatment of a disability includes the following:
- modification of the task
- modification of a tool
- design of new tools or new machines.
The issue of efficacy is always the point of departure in the modification of tools or machines, and is often related to the costs devoted to the modification in question, the technical features to be addressed, and the functional changes to be embodied in the new design. Comfort and attractiveness are qualities that by no means deserve to be neglected among these other characteristics.
The next consideration relating to design changes to be made to a tool or machine is whether the device is one already designed for general use (in which case, modifications will be made to a pre-existing product) or is to be designed with an individual type of disability in mind. In the latter case, specific ergonomic considerations must be devoted to each aspect of the worker’s disability. For example, given a worker suffering from limitations in brain function after a stroke, impairments such as aphasia (difficulty in communication), a paralysed right arm, and a spastic paresis of the leg preventing its being moved upwards might require the following adjustments:
- a personal computer or other device enabling the worker to communicate
- tools that can be operated with the remaining useful arm
- a prosthetic system that would serve to restore the function of the impaired foot as well as to compensate for the patient’s loss of ability to walk.
Is there any general answer to the question of how to design for the disabled worker? The system ergonomic design (SED) approach is an eminently suitable one for this task. Research related to the work situation or to the kind of product at issue requires a design team for the purpose of gathering special information relating either to a special group of disabled workers or to the unique case of an individual user disabled in a particular way. The design team will, by virtue of including a diversity of qualified people, be in possession of expertise beyond the technical sort expected of a designer alone; the medical and ergonomic knowledge shared among them will be as fully applicable as the strictly technical.
Design constraints determined by assembling data related to disabled users are treated with the same objectivity and in the same analytical spirit as are counterpart data relating to healthy users. Just as for the latter, one has to determine for disabled persons their personal patterns of behavioural response, their anthropometrical profiles, biomechanical data (as to reach, strength, range of motion, handling space used, physical load and so forth), ergonomic standards and safety regulations. But one is most regretfully obliged to concede that very little research indeed is done on behalf of disabled workers. There exist a few studies on anthropometry, somewhat more on biomechanics in the field of prostheses and orthoses, but hardly any studies have been carried on physical load capabilities. (The reader will find references to such material in the “Other relevant reading” list at the end of this chapter.) And while it is sometimes easy to gather and apply such data, frequently enough the task is difficult, and in fact, impossible. To be sure, one must obtain objective data, however strenuous the effort and unlikely the chances of doing so, given that the numbers of disabled persons available for research is small. But they are quite often more than willing to participate in whatever research they are offered the opportunity of sharing in, since there is great consciousness of the importance of such a contribution towards design and research in this field. It thus represents an investment not only for themselves but for the larger community of disabled people.
Elderly Workers
The status of ageing workers varies according to their functional condition, which itself is influenced by their past working history. Their status also depends on the work post that they occupy, and the social, cultural and economic situation of the country in which they live.
Thus, workers who have to perform much physical labour are also, most often, those who have had the least schooling and the least occupational training. They are subject to exhausting work conditions, which can cause disease, and they are exposed to the risk of accidents. In this context, their physical capacity is very likely to decline towards the end of their active life, a fact that makes them more vulnerable at work.
Conversely, workers who have had the advantage of lengthy schooling, followed by occupational training that equips them for their work, in general practise trades where they can put to use the knowledge thus acquired and progressively widen their experience. Often they do not work in the most harmful occupational environments and their skills are recognized and valued as they grow older.
During a period of economic expansion and shortage of labour, ageing workers are recognized as having the qualities of “occupational conscientiousness”, being regular in their work, and being able to keep up their know-how. In a period of recession and unemployment, there will be greater emphasis on the fact that their work performance falls short of that of younger people and on their lower capacity to adapt to changes in work techniques and organization.
Depending on the countries concerned, their cultural traditions and their mode and level of economic development, consideration for ageing workers and solidarity with them will be more or less evident, and their protection will be more or less assured.
The time dimensions of the age/work relationship
The relationship between ageing and work covers a great diversity of situations, which can be considered from two points of view: on the one hand, work appears to be a transformation factor for the worker throughout his or her active life, the transformations being either negative (e.g., wear and tear, decline in skills, illnesses and accidents) or positive (e.g., acquisition of knowledge and experience); on the other hand, work reveals the changes connected with age, and this results in marginalization and even exclusion from the production system for older workers exposed to demands at work that are too great for their declining capacity, or on the contrary allows for progress in their working career if the content of the work is such that a high value is placed on experience.
Advancing age therefore plays the role of a “vector” on which events in life are registered chronologically, both at and outside work. Around this axis are hinged processes of decline and building, which are very variable from one worker to another. In order to take into account the problems of ageing workers in the design of work situations, it is necessary to take into account both the dynamic characteristics of changes connected with age and the variability of these changes among individuals.
The age/work relationship can be considered in the light of a threefold evolution:
- Work evolves. Techniques change; mechanization, automation, computerization and methods of information transfer, among other factors, tend or will tend to become more generalized. New products make their appearance, others disappear. New risks are revealed or extended (e.g., radiation and chemical products), others become less prominent. Work organization, labour management, the distribution of tasks and the work schedules are transformed. Some production sectors develop, while others decline. From one generation to another, the work situations encountered during the active life of the worker, the demands that they make and the skills that they require are not the same.
- Working populations change. Age structures are modified in accordance with demographic changes, the means of entering or retiring from work and attitudes towards employment. Women’s share in the working population continues to evolve. Genuine upheavals are occurring in the field of education, occupational training and access to the health system. All these transformations are at the same time producing generation-related and period-related effects which obviously influence the age/work relationship and which can to a certain extent be anticipated.
- Finally—a point that deserves emphasis—individual changes are in progress throughout one’s working life, and the adjustment between the characteristics of particular work and those of the people who carry it out is therefore frequently called into question.
Some processes of organic ageing and their relationship to work
The main organic functions involved in work decline in an observable way from the ages of 40 or 50, after some of them have undergone development up to the ages of 20 or 25.
In particular, a decline with age is observed in maximum muscular strength and range of joint movement. The reduction in strength is in the order of 15 to 20% between the ages of 20 and 60. But this is only an overall trend, and the variability among individuals is considerable. Moreover, these are maximum capacities; the decline is much less for more moderate physical demands.
One function that is very sensitive to age is regulation of posture. This difficulty is not very apparent for common and stable working positions (standing or sitting) but it becomes obvious in situations of disequilibrium that require precise adjustments, strong muscular contraction or joint movements at extreme angles. These problems become more severe when the work has to be carried out on unstable or slippery supports, or when the worker suffers a shock or unexpected jolt. The result is that accidents due to loss of balance become more frequent with age.
Sleep regulation becomes less reliable from the ages of 40 to 45 onwards. It is more sensitive to changes in working schedules (such as night work or shift work) and to disturbing environments (e.g., noise or lighting). Changes in the length and quality of sleep follow.
Thermoregulation also becomes more difficult with age, and this causes older workers to have specific problems with regard to work in heat, particularly when physically intense work has to be carried out.
Sensory functions begin to be affected very early, but the resulting deficiencies are rarely marked before the ages of 40 to 45. Visual function as a whole is affected: there is a reduction in the amplitude of accommodation (which can be corrected with appropriate lenses), and also in the peripheral visual field, perception of depth, resistance to glare and light transmission through the crystalline lens. The resulting inconvenience is noticeable only in particular conditions: in poor lighting, near sources of glare, with objects or texts of very small size or badly presented, and so on.
The decline in auditory function affects the hearing threshold for high frequencies (high-pitched sounds), but it reveals itself particularly as difficulty in discriminating sound signals in a noisy environment. Thus, the intelligibility of the spoken word becomes more difficult in the presence of ambient noise or strong reverberation.
The other sensory functions are, in general, little affected at this time of life.
It can be seen that, in a general way, organic decline with age is noticeable particularly in extreme situations, which should in any case be modified to avoid difficulties even for young workers. Moreover, ageing workers can compensate for their deficiencies by means of particular strategies, often acquired with experience, when the work conditions and organization permit: the use of additional supports for unbalanced postures, lifting and carrying loads in such a way as to reduce extreme effort, organizing visual scanning so as to pinpoint useful information, among other means.
Cognitive ageing: slowing down and learning
As regards cognitive functions, the first thing to note is that work activity brings into play basic mechanisms for receiving and processing information on the one hand, and on the other, knowledge acquired throughout life. This knowledge concerns mainly the meaning of objects, signals, words and situations (“declarative” knowledge), and ways of doing things (“procedural” knowledge).
Short-term memory allows us to retain, for some dozens of seconds or for some minutes, useful information that has been detected. Processing of this information is carried out by comparing it with knowledge that has been memorized on a permanent basis. Ageing acts on these mechanisms in various ways: (1) by virtue of experience, it enriches knowledge, the capacity to select in the best way both useful knowledge and the method of processing it, especially in tasks that are carried out fairly frequently, but (2) the time taken to process this information is lengthened owing both to ageing of the central nervous system, and to more fragile short-term memory.
These cognitive functions depend very much on the environment in which the workers have lived, and therefore on their past history, their training, and the work situations which they have had to face. The changes that occur with age are therefore manifested in extremely varied combinations of phenomena of decline and reconstruction, in which each of these two factors may be more or less accentuated.
If in the course of their working lives workers have received only brief training, and if they have had to carry out relatively simple and repetitive tasks, their knowledge will be limited and they have difficulties when confronted with new or relatively unfamiliar tasks. If, moreover, they have to perform work under marked time constraints, the changes that have occurred in their sensory functions and the slowing down of their information processing will handicap them. If, on the other hand, they have had lengthy schooling and training, and if they have had to carry out a variety of tasks, they will thereby have been able to enhance their skills so that the sensory or cognitive deficiencies associated with age will be largely compensated for.
It is therefore easy to understand the role played by continued training in the work situation of ageing workers. Changes in work make it necessary more and more often to have recourse to periodic training, but older workers rarely receive it. Firms frequently do not consider it worthwhile to give training to a worker nearing the end of his or her active life, particularly as learning difficulties are thought to increase with age. And the workers themselves hesitate to undergo training, fearing that they will not succeed, and not always seeing very clearly the benefits that they could derive from training.
In fact, with age, the manner of learning is modified. Whereas a young person records the knowledge transmitted to him, an older person needs to understand how this knowledge is organized in relation to what he or she already knows, what is its logic, and what is its justification for work. He or she also needs time to learn. Therefore one response to the problem of training older workers is, in the first place, to use different teaching methods, according to each person’s age, knowledge and experience, with, in particular, a longer training period for older people.
Ageing of men and women at work
Age differences between men and women are found at two different levels. At the organic level, life expectancy is generally greater for women than for men, but what is called life expectancy without disability is very close for the two sexes—up to 65 to 70 years. Beyond that age, women are generally at a disadvantage. Moreover, women’s maximum physical capacity is on average 30% less than men’s, and this difference tends to persist with advancing age, but the variability in the two groups is wide, with some overlap between the two distributions.
At the level of the working career there are great differences. On average, women have received less training for work than men when they start their working life, they most often occupy posts for which fewer qualifications are needed, and their working careers are less rewarding. With age they, therefore, occupy posts with considerable constraints, such as time constraints and repetitiveness of the work. No sexual difference in the development of cognitive capacity with age can be established without reference to this social context of work.
If the design of work situations is to take account of these gender differences, action must be taken especially in favour of the initial and continuing vocational training of women and constructing work careers that increase women’s experiences and enhance their value. This action must, therefore, be taken well before the end of their active lives.
Ageing of working populations: the usefulness of collective data
There are at least two reasons for adopting collective and quantitative approaches with respect to the ageing of the working population. The first reason is that such data will be necessary in order to evaluate and foresee the effects of ageing in a workshop, a service, a firm, a sector or a country. The second reason is that the main components of ageing are themselves phenomena subject to probability: all workers do not age in the same way or at the same rate. It is therefore by means of statistical tools that various aspects of ageing will sometimes be revealed, confirmed or assessed.
The simplest instrument in this field is the description of age structures and of their evolution, expressed in ways relevant to work: economic sector, trade, group of jobs, and so on.
For example, when we observe that the age structure of a population in a workplace remains stable and young, we may ask which characteristics of the work could play a selective role in terms of age. If, on the contrary, this structure is stable and older, the workplace has the function of receiving people from other sectors of the firm; the reasons for these movements are worth studying, and we should equally verify whether the work in this workplace is suited to the characteristics of an ageing workforce. If, finally, the age structure shifts regularly, simply reflecting recruitment levels from one year to another, we probably have a situation where people “grow old on site”; this sometimes requires special study, particularly if the annual number of recruitments is tending to decline, which will shift the overall structure towards higher age groups.
Our understanding of these phenomena can be enhanced if we have quantitative data on working conditions, on the posts currently occupied by the workers and (if possible) on the posts that they no longer occupy. The work schedules, the repetitiveness of work, the nature of the physical demands, the work environment, and even certain cognitive components, can be the subject of queries (to be asked of the workers) or of evaluations (by experts). It is then possible to establish a connection between the characteristics of the present work and of past work, and the age of the workers concerned, and so to elucidate the selection mechanisms to which the work conditions can give rise at certain ages.
These investigations can be further improved by also obtaining information on the health status of the workers. This information can be derived from objective indicators such as the work accident rate or sickness absence rate. But these indicators often require considerable care as regards methodology, because although they do indeed reflect health conditions that may be work-related, they also reflect the strategy of all those concerned with occupational accidents and absence due to illness: the workers themselves, the management and the physicians can have various strategies in this regard, and there is no guarantee that these strategies are independent of the worker’s age. Comparisons of these indicators between ages are therefore often complex.
Recourse will therefore be had, when possible, to data arising from self-evaluation of health by the workers, or obtained during medical examinations. These data may relate to diseases whose variable prevalence with age needs to be better known for purposes of anticipation and prevention. But the study of ageing will rely above all on the appreciation of conditions that have not reached the disease stage, such as certain types of functional deterioration: (e. g., of the joints—pain and limitation of sight and hearing, of the respiratory system) or else certain kinds of difficulty or even incapacity (e. g. in mounting a high step, making a precise movement, maintaining equilibrium in an awkward position).
Relating data concerning age, work and health is therefore at the same time a useful and complex matter. Their use permits various types of connections to be revealed (or their existence to be presumed). It may be a case of simple causal relationships, with some requirement of the work accelerating a type of decline in the functional state as age advances. But this is not the most frequent case. Very often, we shall be led to appreciate simultaneously the effect of an accumulation of constraints on the a set of health characteristics, and at the same time the effect of selection mechanisms in accordance with which workers whose health has declined may find that they are excluded from certain kinds of work (what the epidemiologists call the “healthy worker effect”).
In this way we can evaluate the soundness of this collection of relationships, confirm certain fundamental knowledge in the sphere of psychophysiology, and above all obtain information that is useful for devising preventive strategies as regards ageing at work.
Some types of action
Action to be undertaken to maintain ageing workers in employment, without negative consequences for them, must follow several general lines:
- One must not consider this age group as a category apart, but must instead consider age as one factor of diversity among others in the active population; protective measures that are too targeted or too accentuated tend to marginalize and weaken the position of the populations concerned.
- One should anticipate individual and collective changes related to age, as well as changes in work techniques and organization. The management of human resources can be effectively carried out only over time, so as to prepare appropriate adjustments in work careers and training. The design of work situations can then take account at the same time of the available technical and organizational solutions and the characteristics of the (future) population concerned.
- The diversity of individual development throughout working life should be taken into consideration, so as to create conditions of equivalent diversity in work careers and situations.
- Attention should be devoted to favouring the process of building up skills and attenuating the process of decline.
On the basis of these few principles, several types of immediate action can first be defined. The highest priority of action will concern working conditions that are capable of posing particularly acute problems for older workers. As mentioned earlier, postural stresses, extreme exertion, strict time constraints (e.g., as with assembly-line work or the imposition of higher output goals), harmful environments (temperature, noise) or unsuitable environments (lighting conditions), night work and shift work are examples.
Systematic pinpointing of these constraints in posts that are (or may be) occupied by older workers allows an inventory to be drawn up and priorities to be established for action. This pinpointing can be carried out by means of empirical inspection checklists. Of equal use will be analysis of worker activity, which will permit observation of their behaviour to be linked with the explanations that they give of their difficulties. In these two cases, measures of effort or of environmental parameters may complete the observations.
Beyond this pinpointing, the action to be taken cannot be described here, since it will obviously be specific to each work situation. The use of standards may sometimes be useful, but few standards take account of specific aspects of ageing, and each one is concerned with a particular domain, which tends to give rise to thinking in an isolated fashion about each component of the activity under study.
Apart from the immediate measures, taking ageing into account implies longer-range thinking directed towards working out the widest possible flexibility in the design of work situations.
Such flexibility must first be sought in the design of work situations and equipment. Restricted space, nonadjustable tools, rigid software, in short, all the characteristics of the situation that limit the expression of human diversity in the carrying out of the task are very likely to penalize a considerable proportion of older workers. The same is true of the more constraining types of organization: a completely predetermined distribution of tasks, frequent and urgent deadlines, or too numerous or too strict orders (these, of course, must be tolerated when there are essential requirements relating to the quality of production or the safety of an installation). The search for such flexibility is, therefore, the search for varied individual and collective adjustments that can facilitate the successful integration of ageing workers into the production system. One of the conditions for the success of these adjustments is obviously the establishment of work training programmes, provided for workers of all ages and geared to their specific needs.
Taking ageing into account in the design of work situations thus entails a series of coordinated actions (overall reduction in extreme stresses, using all possible strategies for work organization, and continuous efforts to increase skills), which are all the more efficient and all the less expensive when they are taken over the long term and are carefully thought out in advance. The ageing of the population is a sufficiently slow and foreseeable phenomenon for appropriate preventive action to be perfectly feasible.
Cultural Differences
Culture and technology are interdependent. While culture is indeed an important aspect in technology design, development and utilization, the relationship between culture and technology is, however, extremely complex. It needs to be analysed from several perspectives in order to be considered in the design and application of technology. Based on his work in Zambia, Kingsley (1983) divides technological adaptation into changes and adjustments at three levels: that of the individual, of the social organization and of the cultural value system of the society. Each level possesses strong cultural dimensions which require special design considerations.
At the same time, technology itself is an inseparable part of culture. It is built, wholly or in part, around the cultural values of a particular society. And as part of culture, technology becomes an expression of that society’s way of life and thinking. Thus, in order for technology to be accepted, utilized and acknowledged by a society as its own, it must be congruent to the overall image of that society’s culture. Technology must complement culture, not antagonize it.
This article will deal with some of the intricacies concerning cultural considerations in technology designs, examining the current issues and problems, as well as the prevailing concepts and principles, and how they can be applied.
Definition of Culture
The definition of the term culture has been debated at length amongst sociologists and anthropologists for many decades. Culture can be defined in many terms. Kroeber and Kluckhohn (1952) reviewed over a hundred definitions of culture. Williams (1976) mentioned culture as one of the most complicated words in the English language. Culture has even been defined as the entire way of life of people. As such, it includes their technology and material artefacts—anything one would need to know to become a functioning member of the society (Geertz 1973). It may even be described as “publicly available symbolic forms through which people experience and express meaning” (Keesing 1974). Summing it up, Elzinga and Jamison (1981) put it aptly when they said that “the word culture has different meanings in different intellectual disciplines and systems of thought”.
Technology: Part and Product of Culture
Technology can be considered both as part of culture and its product. More than 60 years ago the noted sociologist Malinowsky included technology as part of the culture and gave the following definition: “culture comprises inherited artefacts, goods, technical processes, ideas, habits and values.” Later, Leach (1965) considered technology as a cultural product and mentioned “artefacts, goods and technical processes” as “products of culture”.
In the technological realm, “culture” as an important issue in the design, development and utilization of technical products or systems has been largely neglected by many suppliers as well as receivers of technology. One major reason for this neglect is the absence of basic information on cultural differences.
In the past, technological changes have led to significant changes in social life and organization and in people’s value systems. Industrialization has made deep and enduring changes in the traditional lifestyles of many previously agricultural societies since such lifestyles were largely regarded as incompatible with the way industrial work should be organized. In situations of large cultural diversity, this has led to various negative socio-economic outcomes (Shahnavaz 1991). It is now a well-established fact that simply to impose a technology on a society and believe that it will be absorbed and utilized through extensive training is wishful thinking (Martin et al. 1991).
It is the responsibility of the technology designer to consider the direct and indirect effects of the culture and to make the product compatible with the cultural value system of the user and with its intended operating environment.
The impact of technology for many “industrially developing countries” (IDCs) has been much more than improvement in efficiency. Industrialization was not just modernization of the production and service sectors, but to some extent Westernization of the society. Technology transfer is, thus, also cultural transfer.
Culture, in addition to religion, tradition and language, which are important parameters for technology design and utilization, encompasses other aspects, such as specific attitudes towards certain products and tasks, rules of appropriate behaviour, rules of etiquette, taboos, habits and customs. All these must be equally considered for optimum design.
It is said that people are also products of their distinctive cultures. Nevertheless, the fact remains that world cultures are very much interwoven due to human migration throughout history. It is small wonder that there exist more cultural than national variations in the world. Nevertheless, some very broad distinctions can be made regarding societal, organizational and professional culture-based differences that could influence design in general.
Constraining Influences of Culture
There is very little information on both theoretical and empirical analyses of the constraining influences of culture on technology and how this issue should be incorporated in the design of hardware and software technology. Even though the influence of culture on technology has been recognized (Shahnavaz 1991; Abeysekera, Shahnavaz and Chapman 1990; Alvares 1980; Baranson 1969), very little information is available on the theoretical analysis of cultural differences with regard to technology design and utilization. There are even fewer empirical studies that quantify the importance of cultural variations and provide recommendations on how cultural factors should be considered in the design of product or system (Kedia and Bhagat 1988). Nevertheless, culture and technology can still be studied with some degree of clarity when viewed from different sociological viewpoints.
Culture and Technology: Compatibility and Preference
Proper application of a technology depends, to a large extent, on the compatibility of the user’s culture with the design specifications. Compatibility must exist at all levels of culture—at the societal, organizational and professional levels. In turn, cultural compatibility can have strong influence on a people’s preferences and aptness to utilize a technology. This question involves preferences relating to a product or system; to concepts of productivity and relative efficiency; to change, achievement and authority; as well as to the manner of technology utilization. Cultural values can thus affect people’s willingness and ability to select, to use and to control technology. They have to be compatible in order to be preferred.
Societal culture
As all technologies are inevitably associated with sociocultural values, the cultural receptivity of the society is a very important issue for the proper functioning of a given technological design (Hosni 1988). National or societal culture, which contributes to the formation of a collective mental model of people, influences the entire process of technology design and application, which ranges from planning, goal setting and defining design specifications, to production, management and maintenance systems, training and evaluation. Technology design of both hardware and software should, therefore, reflect society-based cultural variations for maximum benefit. However, defining such society-based cultural factors for consideration in the design of technology is a very complicated task. Hofstede (1980) has proposed four dimensional framework variations of national-based culture.
- Weak versus strong uncertainty avoidance. This concerns a people’s desire to avoid ambiguous situations and to what extent their society has developed formal means (such as rules and regulations) to serve this purpose. Hofstede (1980) gave, for example, high uncertainty avoidance scores to countries like Japan and Greece, and low scores to Hong Kong and Scandinavia.
- Individualism versus collectivism. This pertains to the relationship between individuals and organizations in the society. In individualistic societies, the orientation is such that each person is expected to look after his or her own interests. In contrast, in a collectivist culture, social ties between people are very strong. Some examples of individualistic countries are the United States and Great Britain while Colombia and Venezuela can be considered as having collectivist cultures.
- Small versus large power distance. A large “power distance” characterizes those cultures where the less powerful individuals accept the unequal distribution of power in a culture, as well as the hierarchies in the society and its organizations. Examples of large power distance countries are India and the Philippines. Small power distances are typical of countries like Sweden and Austria.
- Masculinity versus femininity. Cultures that put more emphasis on material achievements are regarded as belonging to the former category. Those giving more value to quality of life and other less tangible outcomes belong to the latter.
Glenn and Glenn (1981) have also distinguished between “abstractive” and “associative” tendencies in a given national culture. It is argued that when people of an associative culture (like those from Asia) approach a cognitive problem, they put more emphasis on context, adapt a global thinking approach and try to utilize association among various events. Whereas in the Western societies, a more abstractive culture of rational thinking predominates. Based on these cultural dimensions, Kedia and Bhagat (1988) have developed a conceptual model for understanding cultural constraints on technology transfer. They have developed various descriptive “propositions” which provide information on different countries’ cultural variations and their receptivity with regard to technology. Certainly many cultures are moderately inclined to one or the other of these categories and contain some mixed features.
Consumers’ as well as producers’ perspectives upon technological design and utilization are directly influenced by the societal culture. Product safety standards for safeguarding consumers as well as work-environment regulations, inspection and enforcement systems for protecting the producers are to a large extent the reflection of the societal culture and value system.
Organizational culture
A company’s organization, its structure, value system, function, behaviour, and so on, are largely cultural products of the society in which it operates. This means that what happens within an organization is mostly a direct reflection of what is happening in the outside society (Hofstede 1983). The prevailing organizations of many companies operating in the IDCs are influenced both by the characteristics of the technology producer country as well as those of the technology recipient environment. However, the reflection of the societal culture in a given organization can vary. Organizations interpret the society in terms of their own culture, and their degree of control depends, among other factors, on the modes of technology transfer.
Given the changing nature of organization today, plus a multicultural, diverse workforce, adapting a proper organizational programme is more important than ever before to a successful operation (an example of a workforce diversity management programme is described in Solomon (1989)).
Professional culture
People belonging to a certain professional category may use a piece of technology in a specific fashion. Wikström et al. (1991), in a project aimed to develop hand tools, have noted that despite the designers’ assumption of how plate shares are to be held and used (i.e., with a forward holding grip and the tool moving away from one’s own body), the professional tinsmiths were holding and using the plate share in a reversed manner, as shown in figure 1. They concluded that tools should be studied in the actual field conditions of the user population itself in order to acquire relevant information on the tools characteristics.
Figure 1. The use of plate share tools by professional tinsmiths in practice (the reversed grip)
Using Cultural Features for Optimum Design
As implied by the foregoing considerations, culture provides identity and confidence. It forms opinions about the objectives and characteristics of a “human-technology system” and how it should operate in a given environment. And in any culture, there are always some features that are valuable with regard to technological progress. If these features are considered in the design of software and hardware technology, they can act as the driving force for technology absorption in the society. One good example is the culture of some southeast Asian countries largely influenced by Confucianism and Buddhism. The former emphasizes, among other things, learning and loyalty, and considers it a virtue to be able to absorb new concepts. The latter teaches the importance of harmony and respect for fellow human beings. It is said that these unique cultural features have contributed to the provision of the right environment for the absorption and implementation of advanced hardware and organizational technology furnished by the Japanese (Matthews 1982).
A clever strategy would thus make the best use of the positive features of a society’s culture in promoting ergonomic ideas and principles. According to McWhinney (1990) “the events, to be understood and thus used effectively in projection, must be embedded in stories. One must go to varying depths to unleash founding energy, to free society or organization from inhibiting traits, to find the paths along which it might naturally flow. . . . Neither planning nor change can be effective without embedding it consciously in a narrative.”
A good example of cultural appreciation in designing management strategy is the implementation of the “seven tools” technique for quality assurance in Japan. The “seven tools” are the minimum weapons a samurai warrior had to carry with him whenever he went out to fight. The pioneers of “quality control circles”, adapting their nine recommendations to a Japanese setting, reduced this number in order to take advantage of a familiar term—“the seven tools”—so as to encourage the involvement of all employees in their quality work strategy (Lillrank and Kano 1989).
However, other cultural features may not be beneficial to technological development. Discrimination against women, the strict observation of a caste system, racial or other prejudice, or considering some tasks as degrading, are a few examples that can have a negative influence on technology development. In some traditional cultures, men are expected to be the primary wage-earners. They become accustomed to regarding the role of women as equal employees, not to mention as supervisors, with insensitivity or even hostility. Withholding equal employment opportunity from women and questioning the legitimacy of women’s authority is not appropriate to the current needs of organizations, which require optimum utilization of human resources.
With regard to task design and job content, some cultures consider tasks like manual labour and service as degrading. This may be attributed to past experiences linked to colonial times regarding “master-slave relationships”. In some other cultures, strong biases exist against tasks or occupations associated with “dirty hands”. These attitudes are also reflected in lower-than-average pay scales for these occupations. In turn, these have contributed to shortages of technicians or inadequate maintenance resources (Sinaiko 1975).
Since it usually takes many generations to change cultural values with respect to a new technology, it would be more cost-effective to fit the technology to the technology recipient’s culture, taking cultural differences into consideration in the design of hardware and software.
Cultural Considerations in Product and System Designing
By now it is obvious that technology consists both of hardware and software. Hardware components include capital and intermediary goods, such as industrial products, machinery, equipment, buildings, workplaces and physical layouts, most of which chiefly concern the micro-ergonomics domain. Software pertains to programming and planning, management and organizational techniques, administration, maintenance, training and education, documentation and services. All these concerns fall under the heading of macro-ergonomics.
A few examples of cultural influences that require special design consideration from the micro- and macro-ergonomic point of view are given below.
Micro-ergonomic issues
Micro-ergonomics is concerned with the design of a product or system with the objective of creating a “usable” user-machine-environment interface. The major concept of product design is usability. This concept involves not only the functionality and reliability of the product, but issues of safety, comfort and enjoyment as well.
The user’s internal model (i.e., his or her cognitive or mental model) plays an important role in usability design. To operate or control a system efficiently and safely, the user must have an accurate representative cognitive model of the system in use. Wisner (1983) has stated that “industrialization would thus more or less require a new kind of mental model.” In this view, formal education and technical training, experience as well as culture are important factors in determining the formation of an adequate cognitive model.
Meshkati (1989), in studying the micro- and macro-ergonomic factors of the 1984 Union Carbide Bhopal accident, highlighted the importance of culture on the Indian operators’ inadequate mental model of the plant operation. He stated that part of the problem may have been due to “the performance of poorly trained Third World operators using advanced technological systems designed by other humans with much different educational backgrounds, as well as cultural and psychosocial attributes.” Indeed, many design usability aspects at the micro-interface level are influenced by the user’s culture. Careful analyses of the user’s perception, behaviour and preferences would lead to a better understanding of the user’s needs and requirements for designing a product or system that is both effective and acceptable.
Some of these culture-related micro-ergonomic aspects are the following:
- Interface design. Human emotion is an essential element of product design. It is concerned in such factors as colour and shape (Kwon, Lee and Ahn 1993; Nagamachi 1992). Colour is regarded as the most important factor to do with human emotions with regard to product design. The product’s colour treatment reflects the psychological and sentimental dispositions of the users, which differ from country to country. The symbolism of colour may also differ. For example, the colour red, which indicates danger in Western countries, is an auspicious token in India (Sen 1984) and symbolizes joy or happiness in China.
- Pictorial signs and symbols that are used in many different applications for public accommodations are strongly culture related. Western pictorial information, for example, is difficult to interpret by non-Western people (Daftuar 1975; Fuglesang 1982).
- Control/display compatibility. Compatibility is a measure of how well spatial movements of control, display behaviour or conceptual relationships meet human expectations (Staramler 1993). It refers to the user’s expectation of the stimulus-response relationship, which is a fundamental ergonomic issue for safe and efficient operation of a product or system. A compatible system is one which considers people’s common perceptual-motor behaviour (i.e., their population-stereotype). However, like other human behaviour, perceptual-motor behaviour may also be influenced by culture. Hsu and Peng (1993) compared American and Chinese subjects regarding control/burner relationships in a four-burner stove. Different population-stereotype patterns were observed. They conclude that population stereotypes regarding control/burner linkages were culturally different, probably as a result of differences in reading or scanning habits.
- Workplace design. An industrial workstation design aims to eliminate harmful postures and improve user performance in relation to the user’s biological needs, preferences and task requirements. People from different cultures may prefer different types of sitting posture and work heights. In Western countries, work heights are set near the seated elbow height for maximum comfort and efficiency. However, in many parts of the world people sit on the floor. Indian workers, for example, prefer squatting or sitting cross-legged to standing or to sitting on a chair. In fact it has been observed that even when chairs are provided, the operators still prefer to squat or sit cross-legged on the seats. Daftuar (1975) and Sen (1984) have studied the merits and implications of the Indian sitting posture. After describing the various advantages of sitting on the floor, Sen stated that “as a large population of the world market covers societies where squatting or sitting on the ground predominate, it is unfortunate that up to now no modern machines have been designed to be used in this way.” Thus, variations in preferred posture should be considered in machine and workplace design in order to improve the operator’s efficiency and comfort.
- Design of protective equipment. There exist both psychological and physical constraints with regard to wearing protective clothing. In some cultures, for example, jobs requiring the use of protective wear may be regarded as common labour, suitable only for unskilled workers. Consequently, protective equipment is usually not worn by engineers at workplaces in such settings. Regarding physical constraints, some religious groups, obliged by their religion to wear a head covering (like the turbans of Indian Sikhs or the head covers of Muslim women) find it difficult to wear, for example, protective helmets. Therefore, special designs of protective wear are needed to cope with such cultural variations in protecting people against work-environmental hazards.
Macro-ergonomic issues
The term macro-ergonomics refers to the design of software technology. It concerns the proper design of organizations and management systems. Evidence exists showing that because of differences in culture, sociopolitical conditions and educational levels, many successful managerial and organizational methods developed in industrialized countries cannot be successfully applied to developing countries (Negandhi 1975). In most IDCs, an organizational hierarchy characterized by a down-flow of authority structure within the organization is a common practice. It has little concern for Western values such as democracy or power sharing in decision-making, which are regarded as key issues in modern management, being essential for proper utilization of human resources as regards intelligence, creativity, problem solving potential and ingenuity.
The feudal system of social hierarchy and its value system are also widely practised in most industrial workplaces in the developing countries. These make a participatory management approach (which is essential for the new production mode of flexible specialization and the motivation of the workforce) a difficult endeavour. However, there are reports confirming the desirability of introducing autonomous work systems even in these cultures Ketchum 1984).
- Participatory ergonomics. Participatory ergonomics is a useful macro-ergonomics approach for solving various work-related problems (Shahnavaz, Abeysekera and Johansson 1993; Noro and Imada 1991; Wilson 1991). This approach, mostly used in industrialized countries, has been applied in different forms depending on the organizational culture in which it has been implemented. In a study, Liker, Nagamachi and Lifshitz (1988) compared participatory ergonomics programmes in two US and two Japanese manufacturing plants which were aiming to reduce physical stress on workers. They concluded that an “effective participatory ergonomics programme can take many forms. The best programme for any plant in any culture may depend on its own unique history, structure and culture.”
- Software systems. Societal and organizational culture-based differences should be considered in designing a new software system or introducing a change in the organization. With respect to information technology, De Lisi (1990) indicates that networking capabilities will not be realized unless the networks fit the existing organizational culture.
- Work organization and management. In some cultures, the family is so important an institution that it plays a prominent role in work organization. For example, among some communities in India, a job is generally regarded as a family responsibility and is collectively performed by all family members (Chapanis 1975).
- Maintenance system. Design of maintenance programmes (both preventive and regular) as well as housekeeping are other examples of areas in which work organization should be adapted to cultural constraints. The traditional culture among the sort of agricultural societies predominant in many IDCs is generally not compatible with the requirements of industrial work and how activities are organized. Traditional agricultural activity does not require, for example, formal maintenance programming and precision work. It is for the most part not carried out under time pressure. In the field, it is usually left to the recycling process of nature to take care of maintenance and housekeeping work. The design of maintenance programmes and housekeeping manuals for industrial activities should thus take these cultural constraints into account and provide for adequate training and supervision.
Zhang and Tyler (1990), in a case study related to the successful establishment of a modern telephone cable production facility in China supplied by a US firm (the Essex Company) stated that “both parties realize, however, that the direct application of American or Essex management practices was not always practical nor desirable due to cultural, philosophical, and political differences. Thus the information and instructions provided by Essex was often modified by the Chinese partner to be compatible with the conditions existing in China.” They also argued that the key to their success, despite cultural, economic and political differences, was both parties’ dedication and commitment to a common goal as well as the mutual respect, trust, and friendship which transcended any differences between them.
Design of shift and work schedules are other examples of work organization. In most IDCs there are certain sociocultural problems associated with shift work. These include poor general living and housing conditions, lack of support services, a noisy home environment and other factors, which require the design of special shift programmes. Furthermore, for female workers, a working day is usually much longer than eight hours; it consists of not only the actual time spent working, but also the time spent on travelling, working at home and taking care of children and elderly relatives. In view of the prevailing culture, shift and other work design requires special work-rest schedules for effective operation.
Flexibility in work schedules to allow cultural variances such as an after-lunch nap for Chinese workers and religious activities for Muslims are further cultural aspects of work organization. In the Islamic culture, people are required to break from work a few times a day to pray, and to fast for one month each year from sunrise to sunset. All these cultural constraints require special work organizational considerations.
Thus, many macro-ergonomic design features are closely influenced by culture. These features should be considered in the design of software systems for effective operation.
Conclusion: Cultural Differences in Design
Designing a usable product or system is not an easy task. There exists no absolute quality of suitability. It is the designer’s task to create an optimum and harmonic interaction between the four basic components of the human-technology system: the user, the task, the technological system and the operating environment. A system may be fully usable for one combination of user, task and environmental conditions but totally unsuitable for another. One design aspect which can greatly contribute to the design’s usability, whether it is a case of a single product or a complex system, is the consideration of cultural aspects which have a profound influence on both the user and the operating environment.
Even if a conscientious engineer designs a proper human-machine interface for use in a given environment, the designer is often unable to foresee the effects of a different culture on the product’s usability. It is difficult to prevent possible negative cultural effects when a product is used in an environment different from that for which it was designed. And since there exist almost no quantitative data regarding cultural constraints, the only way the engineer can make the design compatible with regard to cultural factors is to actively integrate the user population in the design process.
The best way to consider cultural aspects in design is for the designer to adapt a user-centred design approach. True enough, the design approach adapted by the designer is the essential factor that will instantly influence the usability of the designed system. The importance of this basic concept must be recognized and implemented by the product or system designer at the very beginning of the design life cycle. The basic principles of user-centred design can thus be summarized as follows (Gould and Lewis 1985; Shackel 1986; Gould et al. 1987; Gould 1988; Wang 1992):
- Early and continual focus on user. The user should be an active member of the design team throughout the whole product development life cycle (i.e., predesign, detail design, production, verification and product improvement phase).
- Integrated design. The system should be considered as a whole, ensuring a holistic design approach. This means that all aspects of the system’s usability should be evolved in parallel by the design team.
- Early and continuous user testing. User reaction should be tested using prototypes or simulations while carrying out real work in the real environment from early development stage to the final product.
- Iterative design. Designing, testing and redesigning are repeated in regular cycles until satisfactory usability results are achieved.
In the case of designing a product on a global scale, the designer has to consider the needs of consumers around the world. In such a case, access to all actual users and operating environments may not be possible for the purpose of adopting a user-centred design approach. The designer has to use a broad range of information, both formal and informal, such as literature reference material, standards, guidelines, and practical principles and experience in making an analytical evaluation of the design and has to provide sufficient adjustability and flexibility in the product in order to satisfy the needs of a wider user population.
Another point to consider is the fact that designers can never be all-knowing. They need input from not only the users but also other parties involved in the project, including managers, technicians, and repair and maintenance workers. In a participatory process, people involved should share their knowledge and experiences in developing a usable product or system and accept collective responsibility for its functionality and safety. After all, everyone involved has something at stake.
Designing for Specific Groups
In designing a product or an industrial process, one focuses on the “average” and “healthy” worker. Information regarding human abilities in terms of muscular strength, bodily flexibility, length of reach, and many other characteristics is for the most part derived from empirical studies carried out by military recruitment agencies, and reflects measured values valid for the typical young male in his twenties. But working populations, to be sure, consist of people of both sexes and a broad range of ages, to say nothing of a variety of physical types and abilities, levels of fitness and health, and functional capacities. A classification of the varieties of functional limitation among people as outlined by the World Health Organization is given in the accompanying article "Case Study: The International Classifcation of Functional Limitation in People." At present, industrial design for the most part takes insufficient account of the general abilities (or inabilities, for that matter) of workers at large, and should take as its point of departure a broader human average as a basis for design. Clearly, a suitable physical load for a 20-year-old may exceed the capacity to manage of a 15-year-old or a 60-year-old. It is the business of the designer to consider such differences not only from the point of view of efficiency, but with a eye to the prevention of job-related injury and illness.
The progress of technology has brought about the state of affairs that, of all the workplaces in Europe and North America, 60% involve the seated position. The physical load in work situations is now on average far less than before, but many worksites, nonetheless, call for physical loads that cannot be sufficiently reduced to fit human physical capabilities; in some developing countries, the resources of current technology are simply not available to relieve the human physical burden to any appreciable extent. And in technologically advanced countries, it is still a common problem that a designer will adapt his or her approach to constraints imposed by product specifications or production processes, either slighting or leaving out human factors related to disability and the prevention of harm due to the workload. With respect to these aims, designers have to be educated to devote attention to all such human factors, expressing the results of their study in a product requirements document (PRD). The PRD contains the system of demands which the designer has to meet in order to achieve both the expected product quality level and the satisfaction of human capability needs in the production process. While it is unrealistic to demand a product that matches a PRD in every respect, given the need of unavoidable compromises, the design method suited to the closest approach to this goal is the system ergonomic design (SED) method, to be discussed following a consideration of two alternative design approaches.
Creative Design
This design approach is characteristic of artists and others involved in the production of work of a high order of originality. The essence of this design process is that a concept is worked out intuitively and through “inspiration”, allowing problems to be dealt with as they arise, without conscious deliberation beforehand. Sometimes, the outcome will not resemble the initial concept, but nonetheless represents what the creator regards as his or her authentic product. Not seldom, too, the design is a failure. Figure 1 illustrates the route of creative design.
System design arose from the need to predetermine the steps in design in a logical order. As design becomes complex, it has to be subdivided into subtasks. Designers or subtask teams thus become interdependent, and design becomes the job of a design team rather than an individual designer. Complementary expertise is distributed through the team, and design assumes an interdisciplinary character.
System design is oriented to the optimal realization of complex and well-defined product functions through the selection of the most appropriate technology; it is costly, but the risks of failure are considerably reduced as compared with less organized approaches. The efficacy of the design is measured against the goals formulated in the PRD.
The way in which the specifications formulated in the PRD are of the first importance. Figure 2 illustrates the relationship between the PRD and other parts of the system design process.
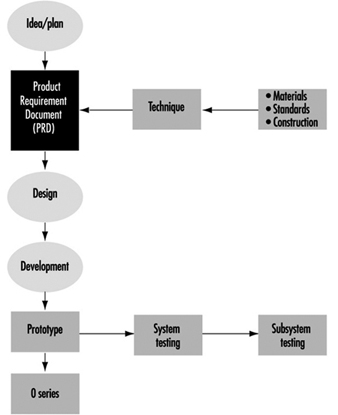
As this scheme shows, the input of the user is neglected. Only at the end of the design process can the user criticize the design. This is unhelpful to both producer and user, since one has to wait for the next design cycle (if there is one) before errors can be corrected and modifications made. Furthermore, user feedback is seldom systematized and imported into a new PRD as a design influence.
System ergonomic design (SED)
SED is a version of system design adapted to ensure that the human factor is accounted for in the design process. Figure 3 illustrates the flow of user input into the PRD.
Figure 3. System ergonomic design
 In system ergonomic design, the human being is considered part of the system: design specification changes are, in fact, made in consideration of the worker’s abilities with respect to cognitive, physical and mental aspects, and the method lends itself as an efficient design approach for any technical system where human operators are employed.
In system ergonomic design, the human being is considered part of the system: design specification changes are, in fact, made in consideration of the worker’s abilities with respect to cognitive, physical and mental aspects, and the method lends itself as an efficient design approach for any technical system where human operators are employed.
For example, to examine the implications of the worker’s physical abilities, task-allocation in the design of the process will call for a careful selection of tasks to be performed by the human operator or by the machine, each task being studied for its aptness to machine or human treatment. Clearly, the human worker will be more effective at interpreting incomplete information; machines however calculate much more rapidly with prepared data; a machine is the choice for lifting heavy loads; and so forth. Furthermore, since the user-machine interface can be tested at the prototype phase, one can eliminate design errors that would otherwise untimely manifest themselves at the phase of technical functioning.
Methods in User Research
No “best” method exists, nor any source of formulae and sure and certain guidelines, according to which design for disabled workers ought to be undertaken. It is a rather a common-sense business of making as exhaustive search of all obtainable knowledge relevant to the problem and of implementing it to its most evident best effect.
Information can be assembled from sources such as the following:
- The literature of research results.
- Direct observation of the disabled person at work and description of his or her particular work difficulties. Such observation should be made at a point in the worker’s schedule when he or she can be expected to be subject to fatigue—the end of a work shift, perhaps. The point is that any design solutions should be adapted to the most arduous phase of the work process, or else such phases may fail to be performed adequately (or at all) owing to the worker’s capacity having been physically exceeded.
- The interview. One has to be aware of the possibly subjective responses which the interview per se may have the effect of eliciting. It is a far better approach that the interview technique be combined with observation. Disabled persons sometimes hesitate to discuss their difficulties, but when workers are aware that the investigator is willing to exert special thoroughness on their behalf, their reticence will diminish. This technique is time-consuming, but quite worthwhile.
- Questionnaires. An advantage of the questionnaire is that it can be distributed to large groups of respondents and at the same time gather data of as specific a sort as one wishes to provide for. The questionnaire must, however, be constructed upon the basis of representative information pertaining to the group to which it will be administered. This means that the type of information to be sought must be obtained on the basis of interviews and observations carried out among a sample of workers and specialists that ought to be reasonably restricted as to size. In the case of disabled persons, it is sensible to include among such a sample the physicians and therapists who are involved with prescribing special aids for disabled persons and have examined them regarding their physical capabilities.
- Physical measurements. Measurements obtained from instruments in the field of bio-instrumentation (e.g., the activity level of muscles, or the amount of oxygen consumed in a given task) and by anthropometrical methods (e.g., the linear dimensions of body elements, the range of motion of limbs, muscular strength) are of indispensable value in human-oriented work designs.
The methods described above are some of the various ways of gathering data about people. Methods exist, too, to evaluate user-machine systems. One of these—simulation—is to construct a realistic physical copy. The development of a more or less abstract symbolic representation of a system is an example of modelling. Such expedients, of course, are both useful and necessary when the actual system or product is not in existence or not accessible to experimental manipulation. Simulation is more often used for training purposes and modelling for research. A mock-up is a full-size, three-dimensional copy of the designed workplace composed, where necessary, of improvised materials, and is of great use in testing design possibilities with the proposed disabled worker: in fact, the majority of design problems can be identified with the aid of such a device. Another advantage to this approach is that the motivation of the worker grows as he or she participates in the design of his or her own future workstation.
Analysis of Tasks
In the analysis of tasks, different aspects of a defined job are subject to analytical observation. These manifold aspects include posture, routing of work manipulations, interactions with other workers, handling tools and operating machines, the logical order of subtasks, the efficiency of operations, static conditions (a worker may have to perform tasks in the same posture over a long time or with high frequency), dynamic conditions (calling for numerous varying physical conditions), material environmental conditions (as in a cold slaughterhouse) or non-material conditions (as with stressful work surroundings or the organization of the work itself).
Work design for the disabled person has, then, to be founded on a thorough task analysis as well as a full examination of the functional abilities of the disabled person. The basic design approach is a crucial issue: it is more efficient to elaborate all possible solutions for the problem in hand without prejudice than to produce a single design concept or a limited number of concepts. In design terminology, this approach is called making a morphological overview. Given the multiplicity of original design concepts, one can proceed to an analysis of the pro and con features of each possibility with respect to material use, construction method, technical production features, ease of manipulation, and so on. It is not unprecedented that more than one solution reaches the prototype stage and that a final decision is made at a relatively late phase in the design process.
Although this may seem a time-consuming way to realize design projects, in fact the extra work it entails is compensated for in terms of fewer problems encountered in the developmental stage, to say nothing that the result—a new workstation or product—will have embodied a better balance between the needs of the disabled worker and the exigencies of the working environment. Unfortunately, the latter benefit rarely if ever reaches the designer in terms of feedback.
Product Requirements Document (PRD) and Disability
After all information relating to a product has been assembled, it should be transformed into a description not only of the product but of all those demands which may be made of it, regardless of source or nature. These demands may of course be divided along various lines. The PRD should include demands relating to user-operator data (physical measurements, range of motion, range of muscular strength, etc.), technical data (materials, construction, production technique, safety standards, etc.), and even conclusions arising out of market feasibility studies.
The PRD forms the designer’s framework, and some designers regard it as an unwelcome restriction of their creativity rather than as a salutary challenge. In view of the difficulties at times accompanying the execution of a PRD, it should always be borne steadily in mind that a design failure causes distress for the disabled person, who may relinquish his or her efforts to succeed in the employment arena (or else fall helpless victim to the progress of the disabling condition), and additional costs for redesign as well. To this end, technical designers should not operate alone in their design work for the disabled, but should cooperate with whatever disciplines are needed for securing the medical and functional information to set up an integrated PRD as a framework for the design.
Prototype Testing
When a prototype is built, it should be tested for errors. Error testing should be carried out not only from the point of view of the technical system and subsystems, but also with a view to its usability in combination with the user. When the user is a disabled person, extra precautions have to be taken. An error to which an unimpaired worker may successfully respond in safety may not afford the disabled worker the opportunity of avoiding harm.
Prototype testing should be carried out on a small number of disabled workers (except in the case of a unique design) according to a protocol matched to the PRD. Only by such empirical testing can the degree to which the design meets the demands of the PRD be adequately judged. Although results on small numbers of subjects may not be generalizable to all cases, they do supply valuable information for the designer’s use in either the final design or in future designs.
Evaluation
The evaluation of a technical system (a work situation, machine or tool) should be judged on its PRD, not by questioning the user or even by attempting comparisons of alternative designs with respect to physical performance. For instance, the designer of a specific knee brace, basing his or her design on research results that show unstable knee joints to exhibit a delayed hamstring reaction, will create a product that compensates for this delay. But another brace may have different design aims. Yet present evaluation methods show no insight as to when to prescribe what kind of knee brace to which patients under what conditions—precisely the sort of insight a health professional needs when prescribing technical aids in the treatment of disabilities.
Current research aims at making this sort of insight possible. A model used to obtain insight into those factors which actually determine whether or not a technical aid ought to be used, or whether or not a worksite is well designed and equipped for the disabled worker is the Rehabilitation Technology Useability Model (RTUM). The RTUM model offers a framework to use in evaluations of existing products, tools or machines, but can also be used in combination with the design process as shown in figure 4.
Figure 4. Rehabilitation Technology Useability Model (RTUM) in combination with the system ergonomic design approach

Evaluations of existing products reveal that as regards technical aids and worksites, the quality of PRDs is very poor. At some times, the product requirements are not recorded properly; at others they are not developed to a useful extent. Designers simply must learn to start documenting their product requirements, including those relevant to disabled users. Note that, as figure 4 shows, RTUM, in conjunction with SED, offers a framework that includes the requirements of disabled users. Agencies responsible for prescribing products for their users must request industry to evaluate those products before marketing them, a task in essence impossible in the absence of product requirement specifications; figure 4 also shows how provision can be made to ensure that the end result can be evaluated as it should (on a PRD) with the help of the disabled person or group for whom the product is intended. It is up to national health organizations to stimulate designers to abide by such design standards and to formulate appropriate regulations.
Information Processing and Design
In designing equipment it is of the utmost importance to take full account of the fact that a human operator has both capabilities and limitations in processing information, which are of a varying nature and which are found on various levels. Performance in actual work conditions strongly depends on the extent to which a design has either attended to or ignored these potentials and their limits. In the following a brief sketch will be offered of some of the chief issues. Reference will be made to other contributions of this volume, where an issue will be discussed in greater detail.
It is common to distinguish three main levels in the analysis of human information processing, namely, the perceptual level, the decision level and the motor level. The perceptual level is subdivided into three further levels, relating to sensory processing, feature extraction and identification of the percept. On the decision level, the operator receives perceptual information and chooses a reaction to it which is finally programmed and actualized on the motor level. This describes only the information flow in the simplest case of a choice reaction. It is evident, though, that perceptual information may accumulate and be combined and diagnosed before eliciting an action. Again, there may arise a need for selecting information in view of perceptual overload. Finally, choosing an appropriate action becomes more of a problem when there are several options some of which may be more appropriate than others. In the present discussion, the emphasis will be on the perceptual and decisional factors of information processing.
Perceptual Capabilities and Limits
Sensory limits
The first category of processing limits is sensory. Their relevance to information processing is obvious since processing becomes less reliable as information approaches threshold limits. This may seem a fairly trivial statement, but nonetheless, sensory problems are not always clearly recognized in designs. For example, alphanumerical characters in sign posting systems should be sufficiently large to be legible at a distance consistent with the need for appropriate action. Legibility, in turn, depends not only on the absolute size of the alphanumericals but also on contrast and—in view of lateral inhibition—also on the total amount of information on the sign. In particular, in conditions of low visibility (e.g., rain or fog during driving or flying) legibility is a considerable problem requiring additional measures. More recently developed traffic signposts and road markers are usually well designed, but signposts near and within buildings are often illegible. Visual display units are another example in which sensory limits of size, contrast and amount of information play an important role. In the auditory domain some main sensory problems are related to understanding speech in noisy environments or in poor quality audio transmission systems.
Feature extraction
Provided sufficient sensory information, the next set of information processing issues relates to extracting features from the information presented. Most recent research has shown ample evidence that an analysis of features precedes the perception of meaningful wholes. Feature analysis is particularly useful in locating a special deviant object amidst many others. For instance, an essential value on a display containing many values may be represented by a single deviant colour or size, which feature then draws immediate attention or “pops out”. Theoretically, there is the common assumption of “feature maps” for different colours, sizes, forms and other physical features. The attention value of a feature depends on the difference in activation of the feature maps that belong to the same class, for example, colour. Thus, the activation of a feature map depends on the discriminability of the deviant features. This means that when there are a few instances of many colours on a screen, most colour feature maps are about equally activated, which has the effect that none of the colours pops out.
In the same way a single moving advertisement pops out, but this effect disappears altogether when there are several moving stimuli in the field of view. The principle of the different activation of feature maps is also applied when aligning pointers that indicate ideal parameter values. A deviation of a pointer is indicated by a deviant slope which is rapidly detected. If this is impossible to realize, a dangerous deviation might be indicated by a change in colour. Thus, the general rule for design is to use only a very few deviant features on a screen and to reserve them only for the most essential information. Searching for relevant information becomes cumbersome in the case of conjunctions of features. For example, it is hard to locate a large red object amidst small red objects and large and small green objects. If possible, conjunctions should be avoided when trying to design for efficient search.
Separable versus integral dimensions
Features are separable when they can be changed without affecting the perception of other features of an object. Line lengths of histograms are a case in point. On the other hand, integral features refer to features which, when changed, change the total appearance of the object. For instance, one cannot change features of the mouth in a schematic drawing of a face without altering the total appearance of the picture. Again, colour and brightness are integral in the sense that one cannot change a colour without altering the brightness impression at the same time. The principles of separable and integral features, and of emergent properties evolving from changes of single features of an object, are applied in so-called integrated or diagnostic displays. The rationale of these displays is that, rather than displaying individual parameters, different parameters are integrated into a single display, the total composition of which indicates what may be actually wrong with a system.
Data presentation in control rooms is still often dominated by the philosophy that each individual measure should have its own indicator. Piecemeal presentation of the measures means that the operator has the task of integrating the evidence from the various individual displays so as to diagnose a potential problem. At the time of the problems in the Three Mile Island nuclear power plant in the United States some forty to fifty displays were registering some form of disorder. Thus, the operator had the task of diagnosing what was actually wrong by integrating the information from that myriad of displays. Integral displays may be helpful in diagnosing the kind of error, since they combine various measures into a single pattern. Different patterns of the integrated display, then, may be diagnostic with regard to specific errors.
A classical example of a diagnostic display, which has been proposed for nuclear control rooms, is shown in figure 1. It displays a number of measures as spokes of equal length so that a regular polygon always represents normal conditions, while different distortions may be connected with different types of problems in the process.
Figure 1. In the normal situation all parameter values are equal, creating a hexagon. In the deviation, some of the values have changed creating a specific distortion.
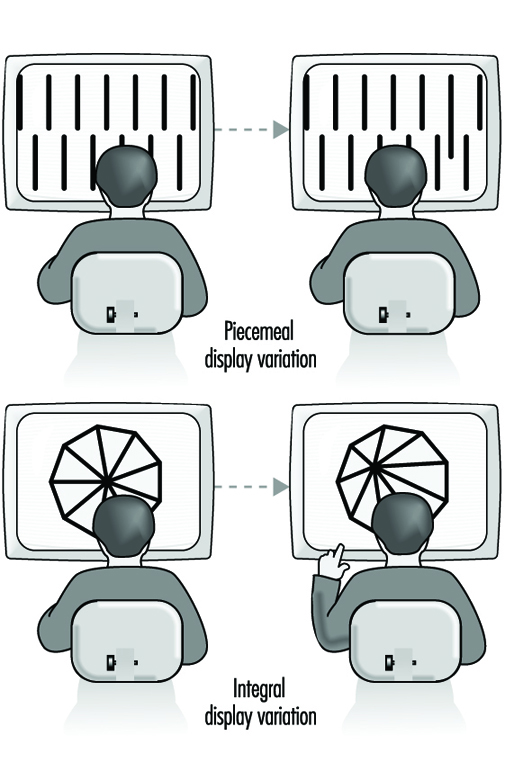 Not all integral displays are equally discriminable. To illustrate the issue, a positive correlation between the two dimensions of a rectangle creates differences in surface, while maintaining an equal shape. Alternatively, a negative correlation creates differences in shape while maintaining an equal surface. The case in which variation of integral dimensions creates a new shape has been referred to as revealing an emergent property of the patterning, which adds to the operator’s ability to discriminate the patterns. Emergent properties depend upon the identity and arrangement of parts but are not identifiable with any single part.
Not all integral displays are equally discriminable. To illustrate the issue, a positive correlation between the two dimensions of a rectangle creates differences in surface, while maintaining an equal shape. Alternatively, a negative correlation creates differences in shape while maintaining an equal surface. The case in which variation of integral dimensions creates a new shape has been referred to as revealing an emergent property of the patterning, which adds to the operator’s ability to discriminate the patterns. Emergent properties depend upon the identity and arrangement of parts but are not identifiable with any single part.
Object and configural displays are not always beneficial. The very fact that they are integral means that the characteristics of the individual variables are harder to perceive. The point is that, by definition, integral dimensions are mutually dependent, thus clouding their individual constituents. There may be circumstances in which this is unacceptable, while one may still wish to profit from the diagnostic patternlike properties, which are typical for the object display. One compromise might be a traditional bar graph display. On the one hand, bar graphs are quite separable. Yet, when positioned in sufficiently close vicinity, the differential lengths of the bars may together constitute an object-like pattern which may well serve a diagnostic aim.
Some diagnostic displays are better than others. Their quality depends on the extent that the display corresponds to the mental model of the task. For example, fault diagnosis on the basis of distortions of a regular polygon, as in figure 1, may still bear little relationship to the domain semantics or to the concept of the operator of the processes in a power plant. Thus, various types of deviations of the polygon do not obviously refer to a specific problem in the plant. Therefore, the design of the most suitable configural display is one that corresponds to the specific mental model of the task. Thus it should be emphasized that the surface of a rectangle is only a useful object display when the product of length and width is the variable of interest!
Interesting object displays stem from three-dimensional representations. For instance, a three-dimensional representation of air traffic—rather than the traditional two-dimensional radar representation—may provide the pilot with a greater “situational awareness” of other traffic. The three-dimensional display has been shown to be much superior to a two-dimensional one since its symbols indicate whether another aircraft is above or below one’s own.
Degraded conditions
Degraded viewing occurs under a variety of conditions. For some purposes, as with camouflage, objects are intentionally degraded so as to prevent their identification. On other occasions, for example in brightness amplification, features may become too blurred to allow one to identify the object. One research issue has concerned the minimal number of “lines” required on a screen or “the amount of detail” needed in order to avoid degradation. Unfortunately, this approach to image quality has not led to unequivocal results. The problem is that identifying degraded stimuli (e.g., a camouflaged armoured vehicle) depends too much on the presence or absence of minor object-specific details. The consequence is that no general prescription about line density can be formulated, except for the trivial statement that degradation decreases as the density increases.
Features of alphanumeric symbols
A major issue in the process of feature extraction concerns the actual number of features which together define a stimulus. Thus, the legibility of ornate characters like Gothic letters is poor because of the many redundant curves. In order to avoid confusion, the difference between letters with very similar features—like the i and the l, and the c and the e—should be accentuated. For the same reason, it is recommended to make the stroke and tail length of ascenders and descenders at least 40% of the total letter height.
It is evident that discrimination among letters is mainly determined by the number of features which they do not share. These mainly consist of straight line and circular segments which may have horizontal, vertical and oblique orientation and which may differ in size, as in lower- and upper-case letters.
It is obvious that, even when alphanumericals are well discriminable, they may easily lose that property in combination with other items. Thus, the digits 4 and 7 share only a few features but they do not do well in the context of larger otherwise identical groups (e.g., 384 versus 387) There is unanimous evidence that reading text in lower case is faster than in capitals. This is usually ascribed to the fact that lower case letters have more distinct features (e.g., dog, cat versus DOG, CAT). The superiority of lower case letters has not only been established for reading text but also for road signs such as those used for indicating towns at the exits of motorways.
Identification
The final perceptual process is concerned with identification and interpretation of percepts. Human limits arising on this level are usually related to discrimination and finding the appropriate interpretation of the percept. The applications of research on visual discrimination are manifold, relating to alphanumerical patterns as well as to more general stimulus identification. The design of brake lights in cars will serve as an example of the last category. Rear-end accidents account for a considerable proportion of traffic accidents, and are due in part to the fact that the traditional location of the brake light next to the rear lights makes it poorly discriminable and therefore extends the driver’s reaction time. As an alternative, a single light has been developed which appears to reduce the accident rate. It is mounted in the centre of the rear window at approximately eye level. In experimental studies on the road, the effect of the central braking light appears to be less when subjects are aware of the aim of the study, suggesting that stimulus identification in the traditional configuration improves when subjects focus on the task. Despite the positive effect of the isolated brake light, its identification might still be further improved by making the brake light more meaningful, giving it the form of an exclamation mark, “!”, or even an icon.
Absolute judgement
Very strict and often counterintuitive performance limits arise in cases of absolute judgement of physical dimensions. Examples occur in connection with colour coding of objects and the use of tones in auditory call systems. The point is that relative judgement is far superior to absolute judgement. The problem with absolute judgement is that the code has to be translated into another category. Thus a specific colour may be linked with an electrical resistance value or a specific tone may be intended for a person for which an ensuing message is meant. In fact, therefore, the problem is not one of perceptual identification but rather of response choice, which will be discussed later in this article. At this point it suffices to remark that one should not use more than four or five colours or pitches so as to avoid errors. When more alternatives are needed one may add extra dimensions, like loudness, duration and components of tones.
Word reading
The relevance of reading separate word units in traditional print is demonstrated by various widely experienced evidence, such as the fact that reading is very much hampered when spaces are omitted, printing errors remain often undetected, and it is very hard to read words in alternating cases (e.g., ALTeRnAtInG). Some investigators have emphasized the role of word shape in reading word units and suggested that spatial frequency analysers may be relevant in identifying word shape. In this view meaning would be derived from total word shape rather than by letter-by-letter analysis. Yet, the contribution of word shape analysis is probably limited to small common words—articles and endings—which is consistent with the finding that printing errors in small words and endings have a relatively low probability of detection.
Text in lower case has an advantage over upper case which is due to a loss of features in the upper case. Yet, the advantage of lower case words is absent or may even be reversed when searching for a single word. It could be that factors of letter size and letter case are confounded in searching: Larger-sized letters are detected more rapidly, which may offset the disadvantage of less distinctive features. Thus, a single word may be about equally legible in upper case as in lower case, while continuous text is read faster in lower case. Detecting a SINGLE capital word amidst many lower case words is very efficient, since it evokes pop-out. An even more efficient fast detection can be achieved by printing a single lower case word in bold, in which case the advantages of pop-out and of more distinctive features are combined.
The role of encoding features in reading is also clear from the impaired legibility of older low-resolution visual display unit screens, which consisted of fairly rough dot matrices and could portray alphanumericals only as straight lines. The common finding was that reading text or searching from a low-resolution monitor was considerably slower than from a paper-printed copy. The problem has largely disappeared with the present-day higher-resolution screens. Besides letter form there are a number of additional differences between reading from paper and reading from a screen. The spacing of the lines, the size of the characters, the type face, the contrast ratio between characters and background, the viewing distance, the amount of flicker and the fact that changing pages on a screen is done by scrolling are some examples. The common finding that reading is slower from computer screens—although comprehension seems about equal—may be due to some combination of these factors. Present-day text processors usually offer a variety of options in font, size, colour, format and style; such choices could give the false impression that personal taste is the major reason.
Icons versus words
In some studies the time taken by a subject in naming a printed word was found to be faster than that for a corresponding icon, while both times were about equally fast in other studies. It has been suggested that words are read faster than icons since they are less ambiguous. Even a fairly simple icon, like a house, may still elicit different responses among subjects, resulting in response conflict and, hence, a decrease in reaction speed. If response conflict is avoided by using really unambiguous icons the difference in response speed is likely to disappear. It is interesting to note that as traffic signs, icons are usually much superior to words, even in the case where the issue of understanding language is not seen as a problem. This paradox may be due to the fact that the legibility of traffic signs is largely a matter of the distance at which a sign can be identified. If properly designed, this distance is larger for symbols than for words, since pictures can provide considerably larger differences in shape and contain less fine details than words. The advantage of pictures, then, arises from the fact that discrimination of letters requires some ten to twelve minutes of arc and that feature detection is the initial prerequisite for discrimination. At the same time it is clear that the superiority of symbols is only guaranteed when (1) they do indeed contain little detail, (2) they are sufficiently distinct in shape and (3) they are unambiguous.
Capabilities and Limits for Decision
Once a precept has been identified and interpreted it may call for an action. In this context the discussion will be limited to deterministic stimulus-response relations, or, in other words, to conditions in which each stimulus has its own fixed response. In that case the major problems for equipment design arise from issues of compatibility, that is, the extent to which the identified stimulus and its related response have a “natural” or well-practised relationship. There are conditions in which an optimal relation is intentionally aborted, as in the case of abbreviations. Usually a contraction like abrvtin is much worse than a truncation like abbrev. Theoretically, this is due to the increasing redundancy of successive letters in a word, which allows “filling out” final letters on the basis of earlier ones; a truncated word can profit from this principle while a contracted one cannot.
Mental models and compatibility
In most compatibility problems there are stereotypical responses derived from generalized mental models. Choosing the null position in a circular display is a case in point. The 12 o’clock and 9 o’clock positions appear to be corrected faster than the 6 o’clock and 3 o’clock positions. The reason may be that a clockwise deviation and a movement in the upper part in the display are experienced as “increases” requiring a response that reduces the value. In the 3 and 6 o’clock positions both principles conflict and they may therefore be handled less efficiently. A similar stereotype is found in locking or opening the rear door of a car. Most people act on the stereotype that locking requires a clockwise movement. If the lock is designed in the opposite way, continuous errors and frustration in trying to lock the door are the most likely result.
With respect to control movements the well-known Warrick’s principle on compatibility describes the relation between the location of a control knob and the direction of the movement on a display. If the control knob is located to the right of the display, a clockwise movement is supposed to move the scale marker up. Or consider moving window displays. According to most people’s mental model, the upward direction of a moving display suggests that the values go up in the same way in which a rising temperature in a thermometer is indicated by a higher mercury column. There are problems in implementing this principle with a “fixed pointer-moving scale” indicator. When the scale in such an indicator moves down, its value is intended to increasing. Thus a conflict with the common stereotype occurs. If the values are inverted, the low values are on the top of the scale, which is also contrary to most stereotypes.
The term proximity compatibility refers to the correspondence of symbolic representations to people’s mental models of functional or even spatial relationships within a system. Issues of proximity compatibility are more pressing as the mental model of a situation is more primitive, global or distorted. Thus, a flow diagram of a complex automated industrial process is often displayed on the basis of a technical model which may not correspond at all with the mental model of the process. In particular, when the mental model of a process is incomplete or distorted, a technical representation of the progress adds little to develop or correct it. A daily-life example of poor proximity compatibility is an architectural map of a building that is intended for viewer orientation or for showing fire escape routes. These maps are usually entirely inadequate—full of irrelevant details—in particular for people who have only a global mental model of the building. Such convergence between map reading and orientation comes close to what has been called “situational awareness”, which is particularly relevant in three-dimensional space during an air flight. There have been interesting recent developments in three-dimensional object displays, representing attempts to achieve optimal proximity compatibility in this domain.
Stimulus-response compatibility
An example of stimulus-response (S-R) compatibility is typically found in the case of most text processing programs, which assume that operators know how commands correspond to specific key combinations. The problem is that a command and its corresponding key combination usually fail to have any pre-existing relation, which means that the S-R relations must be learned by a painstaking process of paired-associate learning. The result is that, even after the skill has been acquired, the task remains error-prone. The internal model of the program remains incomplete since less practised operations are liable to be forgotten, so that the operator can simply not come up with the appropriate response. Also, the text produced on the screen usually does not correspond in all respects to what finally appears on the printed page, which is another example of inferior proximity compatibility. Only a few programs utilize a stereotypical spatial internal model in connection with stimulus-response relations for controlling commands.
It has been correctly argued that there are much better pre-existing relations between spatial stimuli and manual responses—like the relation between a pointing response and a spatial location, or like that between verbal stimuli and vocal responses. There is ample evidence that spatial and verbal representations are relatively separate cognitive categories with little mutual interference but also with little mutual correspondence. Hence, a spatial task, like formatting a text, is most easily performed by spatial mouse-type movement, thus leaving the keyboard for verbal commands.
This does not mean that the keyboard is ideal for carrying out verbal commands. Typing remains a matter of manually operating arbitrary spatial locations which are basically incompatible with processing letters. It is actually another example of a highly incompatible task which is only mastered by extensive practise, and the skill is easily lost without continuous practice. A similar argument can be made for shorthand writing, which also consists of connecting arbitrary written symbols to verbal stimuli. An interesting example of an alternative method of keyboard operation is a chording keyboard.
The operator handles two keyboards (one for the left and one for the right hand) both consisting of six keys. Each letter of the alphabet corresponds to a chording response, that is, a combination of keys. The results of studies on such a keyboard showed striking savings in the time needed for acquiring typing skills. Motor limitations limited the maximal speed of the chording technique but, still, once learned, operator performance approached the speed of the conventional technique quite closely.
A classical example of a spatial compatibility effect concerns the traditional arrangements of stove burner controls: four burners in a 2 ´ 2 matrix, with the controls in a horizontal row. In this configuration, the relations between burner and control are not obvious and are poorly learned. However, despite many errors, the problem of lighting the stove, given time, can usually be solved. The situation is worse when one is faced with undefined display-control relations. Other examples of poor S-R compatibility are found in the display-control relations of video cameras, video recorders and television sets. The effect is that many options are never used or must be studied anew at each new trial. The claim that “it is all explained in the manual”, while true, is not useful since, in practice, most manuals are incomprehensible to the average user, in particular when they attempt to describe actions using incompatible verbal terms.
Stimulus-stimulus (S-S) and response-response (R-R) compatibility
Originally S-S and R-R compatibility were distinguished from S-R compatibility. A classical illustration of S-S compatibility concerns attempts in the late forties to support auditory sonar by a visual display in an effort to enhance signal detection. One solution was sought in a horizontal light beam with vertical perturbations travelling from left to right and reflecting a visual translation of the auditory background noise and potential signal. A signal consisted of a slightly larger vertical perturbation. The experiments showed that a combination of the auditory and visual displays did not do better than the single auditory display. The reason was sought in a poor S-S compatibility: the auditory signal is perceived as a loudness change; hence visual support should correspond most when provided in the form of a brightness change, since that is the compatible visual analogue of a loudness change.
It is of interest that the degree of S-S compatibility corresponds directly to how skilled subjects are in cross-modality matching. In a cross-modality match, subjects may be asked to indicate which auditory loudness corresponds to a certain brightness or to a certain weight; this approach has been popular in research on scaling sensory dimensions, since it allows one to avoid mapping sensory stimuli to numerals. R-R compatibility refers to correspondence of simultaneous and also of successive movements. Some movements are more easily coordinated than others, which provides clear constraints for the way a succession of actions—for example, successive operation of controls—is most efficiently done.
The above examples show clearly how compatibility issues pervade all user-machine interfaces. The problem is that the effects of poor compatibility are often softened by extended practice and so may remain unnoticed or underestimated. Yet, even when incompatible display-control relations are well-practised and do not seem to affect performance, there remains the point of a larger error probability. The incorrect compatible response remains a competitor for the correct incompatible one and is likely to come through on occasion, with the obvious risk of an accident. In addition, the amount of practice required for mastering incompatible S-R relations is formidable and a waste of time.
Limits of Motor Programming and Execution
One limit in motor programming was already briefly touched upon in the remarks on R-R compatibility. The human operator has clear problems in carrying out incongruent movement sequences, and in particular, changing from the one to another incongruent sequence is hard to accomplish. The results of studies on motor coordination are relevant to the design of controls in which both hands are active. Yet, practice can overcome much in this regard, as is clear from the surprising levels of acrobatic skills.
Many common principles in the design of controls derive from motor programming. They include the incorporation of resistance in a control and the provision of feedback indicating that it has been properly operated. A preparatory motor state is a highly relevant determinant of reaction time. Reacting to an unexpected sudden stimulus may take an additional second or so, which is considerable when a fast reaction is needed—as in reacting to a lead car’s brake light. Unprepared reactions are probably a main cause of chain collisions. Early warning signals are beneficial in preventing such collisions. A major application of research on movement execution concerns Fitt’s law, which relates movement, distance and the size of the target that is aimed at. This law appears to be quite general, applying equally to an operating lever, a joystick, a mouse or a light pen. Among others, it has been applied to estimate the time needed to make corrections on computer screens.
There is obviously much more to say than the above sketchy remarks. For instance, the discussion has been almost fully limited to issues of information flow on the level of a simple choice reaction. Issues beyond choice reactions have not been touched upon, nor problems of feedback and feed forward in the ongoing monitoring of information and motor activity. Many of the issues mentioned bear a strong relation to problems of memory and of planning of behaviour, which have not been addressed either. More extensive discussions are found in Wickens (1992), for example.
Controls, Indicators and Panels
Karl H. E. Kroemer
In what follows, three of the most important concerns of ergonomic design will be examined: first, that of controls, devices to transfer energy or signals from the operator to a piece of machinery; second, indicators or displays, which provide visual information to the operator about the status of the machinery; and third, the combination of controls and displays in a panel or console.
Designing for the Sitting Operator
Sitting is a more stable and less energy-consuming posture than standing, but it restricts the working space, particularly of the feet, more than standing. However, it is much easier to operate foot controls when sitting, as compared to standing, because little body weight must be transferred by the feet to the ground. Furthermore, if the direction of the force exerted by the foot is partly or largely forward, provision of a seat with a backrest allows the exertion of rather large forces. (A typical example of this arrangement is the location of pedals in an automobile, which are located in front of the driver, more or less below seat height.) Figure 1 shows schematically the locations in which pedals may be located for a seated operator. Note that the specific dimensions of that space depend on the anthropometry of the actual operators.
Figure 1. Preferred and regular workspace for feet (in centimetres)
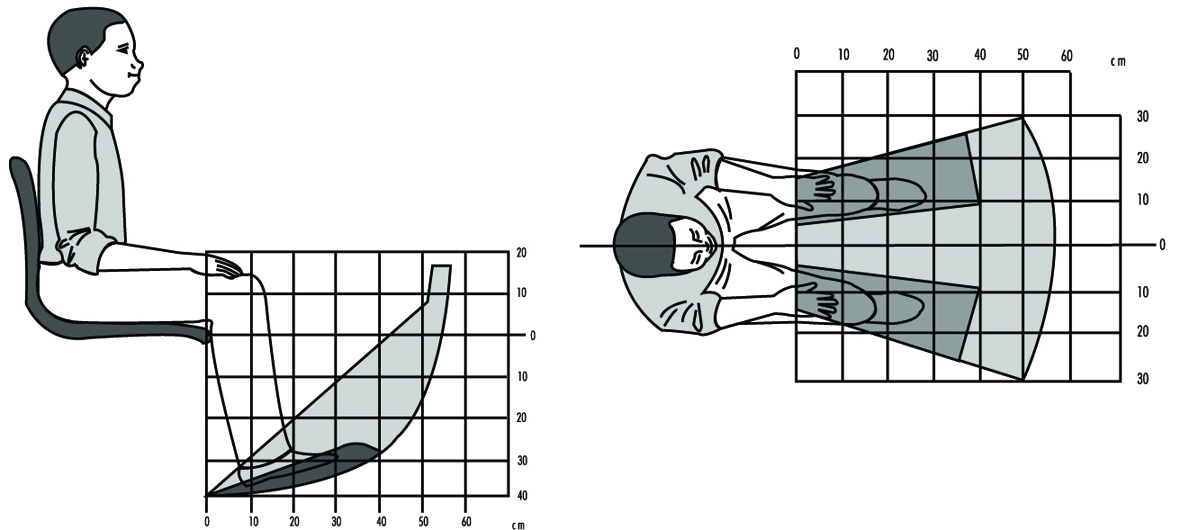
The space for the positioning of hand-operated controls is primarily located in front of the body, within a roughly spherical contour that is centred at either the elbow, at the shoulder, or somewhere between those two body joints. Figure 2 shows schematically that space for the location of controls. Of course, the specific dimensions depend on the anthropometry of the operators.
Figure 2. Preferred and regular workspace for hands (in centimetres)
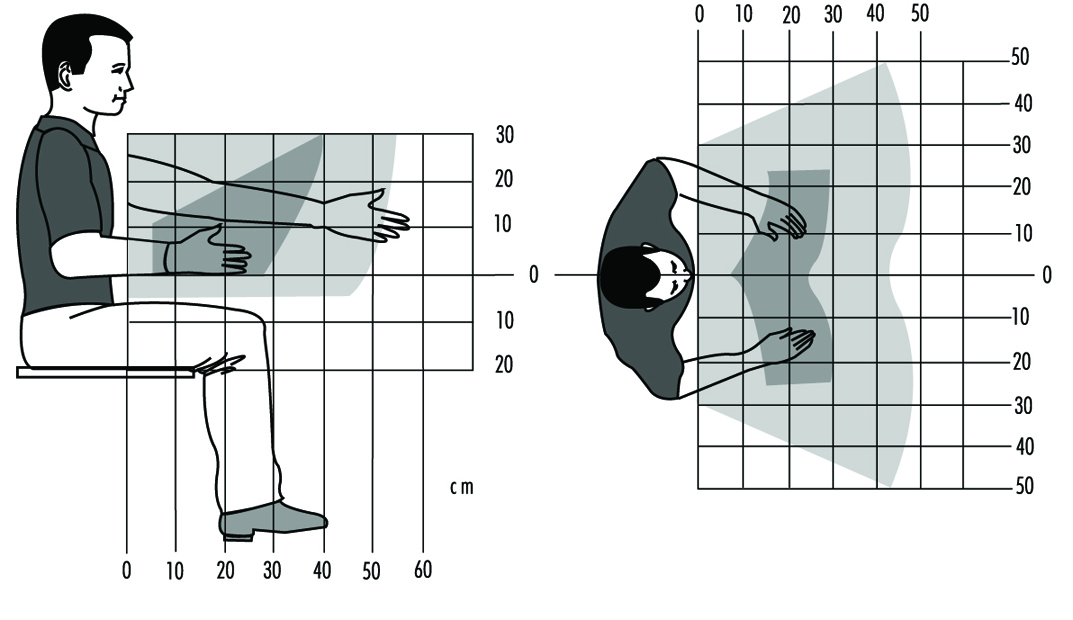
The space for displays and for controls that must be looked at is bounded by the periphery of a partial sphere in front of the eyes and centred at the eyes. Thus, the reference height for such displays and controls depends on the eye height of the seated operator and on his or her trunk and neck postures. The preferred location for visual targets closer than about one metre is distinctly below the height of the eye, and depends on the closeness of the target and on the posture of the head. The closer the target, the lower it should be located, and it should be in or near the medial (mid-sagittal) plane of the operator.
It is convenient to describe the posture of the head by using the “ear-eye line” (Kroemer 1994a) which, in the side view, runs through the right ear hole and the juncture of the lids of the right eye, while the head is not tilted to either side (the pupils are at the same horizontal level in the frontal view). One usually calls the head position “erect” or “upright” when the pitch angle P (see figure 3) between the ear-eye line and the horizon is about 15°, with the eyes above the height of the ear. The preferred location for visual targets is 25°–65° below the ear-eye line (LOSEE in figure 3), with the lower values preferred by most people for close targets that must be kept in focus. Even though there are large variations in the preferred angles of the line of sight, most subjects, particularly as they become older, prefer to focus on close targets with large LOSEE angles.

Designing for the Standing Operator
Pedal operation by a standing operator should be seldom required, because otherwise the person must spend too much time standing on one foot while the other foot operates the control. Obviously, simultaneous operation of two pedals by a standing operator is practically impossible. While the operator is standing still, the room for the location of foot controls is limited to a small area below the trunk and slightly in front of it. Walking about would provide more room to place pedals, but that is highly impractical in most cases because of the walking distances involved.
The location for hand-operated controls of a standing operator includes about the same area as for a seated operator, roughly a half sphere in front of the body, with its centre near the shoulders of the operator. For repeated control operations, the preferred part of that half sphere would be its lower section. The area for the location of displays is also similar to the one suited to a seated operator, again roughly a half sphere centred near the operator’s eyes, with the preferred locations in the lower section of that half sphere. The exact locations for displays, and also for controls that must be seen, depends on the posture of the head, as discussed above.
The height of controls is appropriately referenced to the height of the elbow of the operator while the upper arm is hanging from the shoulder. The height of displays and controls that must be looked at is referred to the eye height of the operator. Both depend on the operator’s anthropometry, which may be rather different for short and tall persons, for men and women, and for people of different ethnic origins.
Foot-operated Controls
Two kinds of controls should be distinguished: one is used to transfer large energy or forces to a piece of machinery. Examples of this are the pedals on a bicycle or the brake pedal in a heavier vehicle that does not have a power-assist feature. A foot-operated control, such as an on-off switch, in which a control signal is conveyed to the machinery, usually requires only a small quantity of force or energy. While it is convenient to consider these two extremes of pedals, there are various intermediate forms, and it is the task of the designer to determine which of the following design recommendations apply best among them.
As mentioned above, repeated or continual pedal operation should be required only from a seated operator. For controls meant to transmit large energies and forces, the following rules apply:
- Locate pedals underneath the body, slightly in front, so that they can be operated with the leg in a comfortable position. The total horizontal displacement of a reciprocating pedal should normally not exceed about 0.15 m. For rotating pedals, the radius should also be about 0.15 m. The linear displacement of a switch-type pedal may be minimal and should not exceed about 0.15 m.
- Pedals should be so designed that the direction of travel and the foot force are approximately in the line extending from the hip through the ankle joint of the operator.
- Pedals that are operated by flexion and extension of the foot in the ankle joint should be so arranged that in the normal position the angle between the lower leg and the foot is approximately 90°; during operation, that angle may be increased to about 120°.
- Foot-operated controls that simply provide signals to the machinery should normally have two discrete positions, such as ON or OFF. Note, however, that tactile distinction between the two positions may be difficult with the foot.
Selection of Controls
Selection among different sorts of controls must be made according to the following needs or conditions:
- Operation by hand or foot
- Amounts of energies and forces transmitted
- Applying “continuous” inputs, such as steering an automobile
- Performing “discrete actions,” for example, (a) activating or shutting down equipment, (b) selecting one of several distinct adjustments, such as switching from one TV or radio channel to another, or (c) carrying out data entry, as with a keyboard.
The functional usefulness of controls also determines selection procedures. The main criteria are as follows:
- The control type shall be compatible with stereotypical or common expectations (for instance, using a push-button or toggle switch to turn on an electric light, not a rotary knob).
- Size and motion characteristics of the control shall be compatible with stereotypical experience and past practice (for instance, providing a large steering wheel for the two-handed operation of an automobile, not a lever).
- The direction of operation of a control shall be compatible with stereotypical or common expectations (for instance, an ON control is pushed or pulled, not turned to the left).
- Hand operation is used for controls that require small force and fine adjustment, while foot operation is suitable for gross adjustments and large forces (however, consider the common use of pedals, particularly accelerator pedals, in automobiles, which does not comply with this principle).
- The control shall be “safe” in that it cannot be operated inadvertently nor in ways that are excessive or inconsistent with its intended purpose.
Table 1. Control movements and expected effects
|
Direction of control movement |
||||||||||||
|
Function |
Up |
Right |
Forward |
Clockwise |
Press, |
Down |
Left |
Rearward |
Back |
Counter- |
Pull1 |
Push2 |
|
On |
+3 |
+ |
+ |
+ |
– |
+3 |
+ |
|||||
|
Off |
+ |
– |
– |
+ |
– |
|||||||
|
Right |
+ |
– |
||||||||||
|
Left |
+ |
– |
||||||||||
|
Raise |
+ |
– |
||||||||||
|
Lower |
– |
+ |
||||||||||
|
Retract |
– |
+ |
– |
|||||||||
|
Extend |
+ |
– |
– |
|||||||||
|
Increase |
– |
– |
+ |
– |
||||||||
|
Decrease |
– |
– |
+ |
– |
||||||||
|
Open Value |
– |
+ |
||||||||||
|
Close Value |
+ |
– |
||||||||||
Blank: Not applicable; + Most preferred; – less preferred. 1 With trigger-type control. 2 With push-pull switch. 3 Up in the United States, down in Europe.
Source: Modified from Kroemer 1995.
Table 1 and table 2 help in the selection of proper controls. However, note that there are few “natural” rules for selection and design of controls. Most current recommendations are purely empirical and apply to existing devices and Western stereotypes.
Table 2. Control-effect relations of common hand controls
|
Effect |
Key- |
Toggle |
Push- |
Bar |
Round |
Thumbwheel |
Thumbwheel |
Crank |
Rocker switch |
Lever |
Joystick |
Legend |
Slide1 |
|
Select ON/OFF |
+ |
+ |
+ |
= |
+ |
+ |
+ |
||||||
|
Select ON/STANDBY/OFF |
– |
+ |
+ |
+ |
+ |
+ |
|||||||
|
Select OFF/MODE1/MODE2 |
= |
– |
+ |
+ |
+ |
+ |
|||||||
|
Select one function of several related functions |
– |
+ |
– |
= |
|||||||||
|
Select one of three or more discrete alternatives |
+ |
+ |
|||||||||||
|
Select operating condition |
+ |
+ |
– |
+ |
+ |
– |
|||||||
|
Engage or disengage |
+ |
||||||||||||
|
Select one of mutually |
+ |
+ |
|||||||||||
|
Set value on scale |
+ |
– |
= |
= |
= |
+ |
|||||||
|
Select value in discrete steps |
+ |
+ |
+ |
+ |
Blank: Not applicable; +: Most preferred; –: Less preferred; = Least preferred. 1 Estimated (no experiments known).
Source: Modified from Kroemer 1995.
Figure 4 presents examples of “detent” controls, characterized by discrete detents or stops in which the control comes to rest. It also depicts typical “continuous” controls where the control operation may take place anywhere within the adjustment range, without the need to be set in any given position.
Figure 4. Some examples of "detent" and "continuous" controls

The sizing of controls is largely a matter of past experiences with various control types, often guided by the desire to minimize the needed space in a control panel, and either to allow simultaneous operations of adjacent controls or to avoid inadvertent concurrent activation. Furthermore, the choice of design characteristics will be influenced by such considerations as whether the controls are to be located outdoors or in sheltered environments, in stationary equipment or moving vehicles, or may involve the use of bare hands or of gloves and mittens. For these conditions, consult readings at the end of the chapter.
Several operational rules govern the arrangement and grouping of controls. These are listed in table 3. For more details, check the references listed at the end of this section and Kroemer, Kroemer and Kroemer-Elbert (1994).
Table 3. Rules for arrangement of controls
|
Locate for the |
Controls shall be oriented with respect to the operator. If the |
|
Primary controls |
The most important controls shall have the most advantageous |
|
Group related |
Controls that are operated in sequence, that are related to a |
|
Arrange for |
If operation of controls follows a given pattern, controls shall |
|
Be consistent |
The arrangement of functionally identical or similar controls |
|
Dead-operator |
If the operator becomes incapacitated and either lets go of a |
|
Select codes |
There are numerous ways to help identify controls, to indicate |
Source: Modified from Kroemer, Kroemer and Kroemer-Elbert 1994.
Reproduced by permission of Prentice-Hall. All rights reserved.
Preventing Accidental Operation
The following are the most important means to guard against inadvertent activation of controls, some of which may be combined:
- Locate and orient the control so that the operator is unlikely to strike it or move it accidentally in the normal sequence of control operations.
- Recess, shield or surround the control by physical barriers.
- Cover the control or guard it by providing a pin, a lock or other means that must be removed or broken before the control can be operated.
- Provide extra resistance (by viscous or coulomb friction, by spring-loading or by inertia) so that an unusual effort is required for actuation.
- Provide a “delaying” means so that the control must pass through a critical position with an unusual movement (such as in the gear shift mechanism of an automobile).
- Provide interlocking between controls so that prior operation of a related control is required before the critical control can be activated.
Note that these designs usually slow the operation of controls, which may be detrimental in case of an emergency.
Data Entry Devices
Nearly all controls can be used to enter data on a computer or other data storage device. However, we are most used to the practice of using a keyboard with push-buttons. On the original typewriter keyboard, which has become the standard even for computer keyboards, the keys were arranged in a basically alphabetic sequence, which has been modified for various, often obscure, reasons. In some cases, letters which frequently follow each other in common text were spaced apart so that the original mechanical type bars might not entangle if struck in rapid sequence. “Columns” of keys run in roughly straight lines, as do the “rows” of keys. However, the fingertips are not aligned in such manners, and do not move in this way when digits of the hand are flexed or extended, or moved sideways.
Many attempts have been made over the last hundred years to improve keying performance by changing the keyboard layout. These include relocating keys within the standard layout, or changing the keyboard layout altogether. The keyboard has been divided into separate sections, and sets of keys (such as numerical pads) have been added. Arrangements of adjacent keys may be changed by altering spacing, offset from each other or from reference lines. The keyboard may be divided into sections for the left and right hand, and those sections may be laterally tilted and sloped and slanted.
The dynamics of the operation of push-button keys are important for the user, but are difficult to measure in operation. Thus, the force-displacement characteristics of keys are commonly described for static testing, which is not indicative of actual operation. By current practise, keys on computer keyboards have fairly little displacement (about 2 mm) and display a “snap-back” resistance, that is, a decrease in operation force at the point when actuation of the key has been achieved. Instead of separate single keys, some keyboards consist of a membrane with switches underneath which, when pressed in the correct location, generate the desired input with little or no displacement felt. The major advantage of the membrane is that dust or fluids cannot penetrate it; however, many users dislike it.
There are alternatives to the “one key-one character” principle; instead, one can generate inputs by various combinatory means. One is “chording”, meaning that two or more controls are operated simultaneously to generate one character. This poses demands on the memory capabilities of the operator, but requires the use of only very few keys. Other developments utilize controls other than the binary tapped push button, replacing it by levers, toggles or special sensors (such as an instrumented glove) which respond to movements of the digits of the hand.
By tradition, typing and computer entry have been made by mechanical interaction between the operator’s fingers and such devices as keyboard, mouse, track ball or light pen. Yet there are many other means to generate inputs. Voice recognition appears one promising technique, but other methods can be employed. They might utilize, for example, pointing, gestures, facial expressions, body movements, looking (directing one’s gaze), movements of the tongue, breathing or sign language to transmit information and to generate inputs to a computer. Technical development in this area is very much in flux, and as the many nontraditional input devices used for computer games indicate, acceptance of devices other than the traditional binary tap-down keyboard is entirely feasible within the near future. Discussions of current keyboard devices have been provided, for example, by Kroemer (1994b) and McIntosh (1994).
Displays
Displays provide information about the status of equipment. Displays may apply to the operator’s visual sense (lights, scales, counters, cathode-ray tubes, flat panel electronics, etc.), to the auditory sense (bells, horns, recorded voice messages, electronically generated sounds, etc.) or to the sense of touch (shaped controls, Braille, etc.). Labels, written instructions, warnings or symbols (“icons”) may be considered special kinds of displays.
The four “cardinal rules” for displays are:
- Display only that information which is essential for adequate job performance.
- Display information only as accurately as is required for the operator’s decisions and actions.
- Present information in the most direct, simple, understandable and usable form.
- Present information in such a way that failure or malfunction of the display itself will be immediately obvious.
The selection of either an auditory or visual display depends on the prevailing conditions and purposes. The objective of the display may be to provide:
- historical information about the past state of the system, such as the course run by a ship
- status information about the current state of the system, such as the text already input into a word processor or the current position of an airplane
- predictive information, such as on the future position of a ship, given certain steering settings
- instructions or commands telling the operator what to do, and possibly how to do it.
A visual display is most appropriate if the environment is noisy, the operator stays in place, the message is long and complex, and especially if it deals with the spatial location of an object. An auditory display is appropriate if the workplace must be kept dark, the operator moves around, and the message is short and simple, requires immediate attention, and deals with events and time.
Visual Displays
There are three basic types of visual displays: (1)The check display indicates whether or not a given condition exists (for example a green light indicates normal function). (2)The qualitative display indicates the status of a changing variable or its approximate value, or its trend of change (for example, a pointer moves within a “normal” range). (3) The quantitative display shows exact information that must be ascertained (for example, to find a location on a map, to read text or to draw on a computer monitor), or it may indicate an exact numerical value that must be read by the operator (for example, a time or a temperature).
Design guidelines for visual displays are:
- Arrange displays so that the operator can locate and identify them easily without unnecessary searching. (This usually means that the displays should be in or near the medial plane of the operator, and below or at eye height.)
- Group displays functionally or sequentially so that the operator can use them easily.
- Make sure that all displays are properly illuminated or illuminant, coded and labelled according to their function.
- Use lights, often coloured, to indicate the status of a system (such as ON or OFF) or to alert the operator that the system, or a subsystem, is inoperative and that special action must be taken. Common meanings of light colours are listed in figure 5. Flashing red indicates an emergency condition that requires immediate action. An emergency signal is most effective when it combines sounds with a flashing red light.
Figure 5. Colour coding of indicator lights
For more complex and detailed information, especially quantitative information, one of four different kinds of displays are traditionally used: (1) a moving pointer (with fixed scale), (2) a moving scale (with fixed pointer), (3) counters or (4) “pictorial” displays, especially computer-generated on a display monitor. Figure 6 lists the major characteristics of these display types.
Figure 6. Characteristics of displays
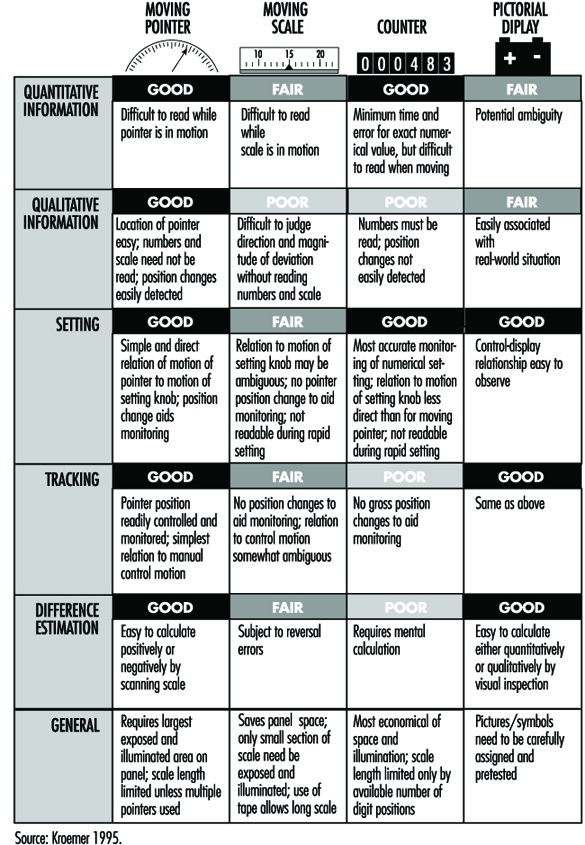
It is usually preferable to use a moving pointer rather than a moving scale, with the scale either straight (horizontally or vertically arranged), curved or circular. Scales should be simple and uncluttered, with graduation and numbering so designed that correct readings can be taken quickly. Numerals should be located outside the scale markings so that they are not obscured by the pointer. The pointer should end with its tip directly at the marking. The scale should mark divisions only so finely as the operator must read. All major marks should be numbered. Progressions are best marked with intervals of one, five or ten units between major marks. Numbers should increase left to right, bottom to top or clockwise. For details of dimensions of scales refer to standards such as those listed by Cushman and Rosenberg 1991 or Kroemer 1994a.
Starting in the 1980s, mechanical displays with pointers and printed scales were increasingly replaced by “electronic” displays with computer-generated images, or solid-state devices using light-emitting diodes (see Snyder 1985a). The displayed information may be coded by the following means:
- shapes, such as straight or circular
- alphanumeric, that is, letters, numbers, words, abbreviations
- figures, pictures, pictorials, icons, symbols, in various levels of abstraction, such as the outline of an airplane against the horizon
- shades of black, white or gray
- colours.
Unfortunately, many electronically generated displays have been fuzzy, often overly complex and colourful, hard to read, and required exact focusing and close attention, which may distract from the main task, for example, driving a car. In these cases the first three of the four “cardinal rules” listed above were often violated. Furthermore, many electronically generated pointers, markings and alphanumerics did not comply with established ergonomic design guidelines, especially when generated by line segments, scan lines or dot matrices. Although some of these defective designs were tolerated by the users, rapid innovation and improving display techniques allows many better solutions. However, the same rapid development leads to the fact that printed statements (even if current and comprehensive when they appear) are becoming obsolete quickly. Therefore, none are given in this text. Compilations have been published by Cushman and Rosenberg (1991), Kinney and Huey (1990), and Woodson, Tillman and Tillman (1991).
The overall quality of electronic displays is often wanting. One measure used to assess the image quality is the modulation transfer function (MTF) (Snyder 1985b). It describes the resolution of the display using a special sine-wave test signal; yet, readers have many criteria regarding the preference of displays (Dillon 1992).
Monochrome displays have only one colour, usually either green, yellow, amber, orange or white (achromatic). If several colours appear on the same chromatic display, they should be easily discriminated. It is best to display not more than three or four colours simultaneously (with preference being given to red, green, yellow or orange, and cyan or purple). All should strongly contrast with the background. In fact, a suitable rule is to design first by contrast, that is, in terms of black and white, and then to add colours sparingly.
In spite of the many variables that, singly and interacting with each other, affect the use of complex colour display, Cushman and Rosenberg (1991) compiled guidelines for use of colour in displays; these are listed in figure 7.
Figure 7. Guidelines for use of colours in displays

Other suggestions are as follows:
- Blue (preferably desaturated) is a good colour for backgrounds and large shapes. However, blue should not be used for text, thin lines or small shapes.
- The colour of alphanumeric characters should contrast with that of the background.
- When using colour, use shape as a redundant cue (e.g., all yellow symbols are triangles, all green symbols are circles, all red symbols are squares). Redundant coding makes the display much more acceptable for users who have colour-vision deficiencies.
- As the number of colours is increased, the sizes of the colour-coded objects should also be increased.
- Red and green should not be used for small symbols and small shapes in peripheral areas of large displays.
- Using opponent colours (red and green, yellow and blue) adjacent to one another or in an object/background relationship is sometimes beneficial and sometimes detrimental. No general guidelines can be given; a solution should be determined for each case.
- Avoid displaying several highly saturated, spectrally extreme colours at the same time.
Panels of Controls and Displays
Displays as well as controls should be arranged in panels so they are in front of the operator, that is, close to the person’s medial plane. As discussed earlier, controls should be near elbow height, and displays below or at eye height, whether the operator is sitting or standing. Infrequently operated controls, or less important displays, can be located further to the sides, or higher.
Often, information on the result of control operation is displayed on an instrument. In this case, the display should be located close to the control so that the control setting can be done without error, quickly and conveniently. The assignment is usually clearest when the control is directly below or to the right of the display. Care must be taken that the hand does not cover the display when operating the control.
Popular expectancies of control-display relations exist, but they are often learned, they may depend on the user’s cultural background and experience, and these relationships are often not strong. Expected movement relationships are influenced by the type of control and display. When both are either linear or rotary, the stereotypical expectation is that they move in corresponding directions, such as both up or both clockwise. When the movements are incongruent, in general the following rules apply:
- Clockwise for increase. Turning the control clockwise causes an increase in the displayed value.
- Warrick’s gear-slide rule. A display (pointer) is expected to move in the same direction as does the side of the control close to (i.e., geared with) the display.
The ratio of control and display displacement (C/D ratio or D/C gain) describes how much a control must be moved to adjust a display. If much control movement produces only a small display motion, once speaks of a high C/D ratio, and of the control as having low sensitivity. Often, two distinct movements are involved in making a setting: first a fast primary (“slewing”) motion to an approximate location, then a fine adjustment to the exact setting. In some cases, one takes as the optimal C/D ratio that which minimizes the sum of these two movements. However, the most suitable ratio depends on the given circumstances; it must be determined for each application.
Labels and Warnings
Labels
Ideally, no label should be required on equipment or on a control to explain its use. Often, however, it is necessary to use labels so that one may locate, identify, read or manipulate controls, displays or other equipment items. Labelling must be done so that the information is provided accurately and rapidly. For this, the guidelines in table 4 apply.
Table 4. Guidelines for labels
|
Orientation |
A label and the information printed on it shall be oriented |
|
Location |
A label shall be placed on or very near the item that it |
|
Standardization |
Placement of all labels shall be consistent throughout the |
|
Equipment |
A label shall primarily describe the function (“what does it |
|
Abbreviations |
Common abbreviations may be used. If a new abbreviation is |
|
Brevity |
The label inscription shall be as concise as possible without |
|
Familiarity |
Words shall be chosen, if possible, that are familiar to the |
|
Visibility and |
The operator shall be able to be read easily and accurately at |
|
Font and size |
Typography determines the legibility of written information; |
Source: Modified from Kroemer, Kroemer and Kroemer-Elbert 1994
(reproduced by permission of Prentice-Hall; all rights reserved).
Font (typeface) should be simple, bold and vertical, such as Futura, Helvetica, Namel, Tempo and Vega. Note that most electronically generated fonts (formed by LED, LCD or dot matrix) are generally inferior to printed fonts; thus, special attention must be paid to making these as legible as possible.
- The height of characters depends on the viewing distance:
viewing distance 35 cm, suggested height 22 mm
viewing distance 70 cm, suggested height 50 mm
viewing distance 1 m, suggested height 70 mm
viewing distance 1.5 m, suggested height at least 1 cm.
- The ratio of strokewidth to character height should be between 1:8 to 1:6 for black letters on white background, and 1:10 to 1:8 for white letters on black background.
- The ratio of character width to character height should be about 3:5.
- The space between letters should be at least one stroke width.
- The space between words should be at least one character width.
- For continuous text, mix upper- and lower-case letters; for labels, use upper-case letters only.
Warnings
Ideally, all devices should be safe to use. In reality, often this cannot be achieved through design. In this case, one must warn users of the dangers associated with product use and provide instructions for safe use to prevent injury or damage.
It is preferable to have an “active” warning, usually consisting of a sensor that notices inappropriate use, combined with an alerting device that warns the human of an impending danger. Yet, in most cases, “passive” warnings are used, usually consisting of a label attached to the product and of instructions for safe use in the user manual. Such passive warnings rely completely on the human user to recognize an existing or potential dangerous situation, to remember the warning, and to behave prudently.
Labels and signs for passive warnings must be carefully designed by following the most recent government laws and regulations, national and international standards, and the best applicable human engineering information. Warning labels and placards may contain text, graphics, and pictures—often graphics with redundant text. Graphics, particularly pictures and pictograms, can be used by persons with different cultural and language backgrounds, if these depictions are selected carefully. However, users with different ages, experiences, and ethnic and educational backgrounds, may have rather different perceptions of dangers and warnings. Therefore, design of a safe product is much preferable to applying warnings to an inferior product.
Tools
Commonly a tool comprises a head and a handle, with sometimes a shaft, or, in the case of the power tool, a body. Since the tool must meet the requirements of multiple users, basic conflicts can arise which may have to be met with compromise. Some of these conflicts derive from limitations in the capacities of the user, and some are intrinsic to the tool itself. It should be remembered, however, that human limitations are inherent and largely immutable, while the form and function of the tool are subject to a certain amount of modification. Thus, in order to effect desirable change, attention must be directed primarily to the form of the tool, and, in particular, to the interface between the user and the tool, namely the handle.
The Nature of Grip
The widely accepted characteristics of grip have been defined in terms of a power grip, a precision grip and a hook grip, by which virtually all human manual activities can be accomplished.
In a power grip, such as is used in hammering nails, the tool is held in a clamp formed by the partially flexed fingers and the palm, with counterpressure being applied by the thumb. In a precision grip, such as one uses when adjusting a set screw, the tool is pinched between the flexor aspects of the fingers and the opposing thumb. A modification of the precision grip is the pencil grip, which is self-explanatory and is used for intricate work. A precision grip provides only 20% of the strength of a power grip.
A hook grip is used where there is no requirement for anything other than holding. In the hook grip the object is suspended from the flexed fingers, with or without the support of the thumb. Heavy tools should be designed so that they can be carried in a hook grip.
Grip Thickness
For precision grips, recommended thicknesses have varied from 8 to 16 millimetres (mm) for screwdrivers, and 13 to 30 mm for pens. For power grips applied around a more or less cylindrical object, the fingers should surround more than half the circumference, but the fingers and thumb should not meet. Recommended diameters have ranged from as low as 25 mm to as much as 85 mm. The optimum, varying with hand size, is probably around 55 to 65 mm for males, and 50 to 60 mm for females. Persons with small hands should not perform repetitive actions in power grips of diameter greater than 60 mm.
Grip Strength and Hand Span
The use of a tool requires strength. Other than for holding, the greatest requirement for hand strength is found in the use of cross-lever action tools such as pliers and crushing tools. The effective force in crushing is a function of the grip strength and the required span of the tool. The maximum functional span between the end of the thumb and the ends of the grasping fingers averages about 145 mm for men and 125 mm for women, with ethnic variations. For an optimal span, which ranges from 45 to 55 mm for both men and women, the grip strength available for a single short-term action ranges from about 450 to 500 newtons for men and 250 to 300 newtons for women, but for repetitive action the recommended requirement is probably closer to 90 to 100 newtons for men, and 50 to 60 newtons for women. Many commonly used clamps or pliers are beyond the capacity of one-handed use, particularly in women.
When a handle is that of a screwdriver or similar tool the available torque is determined by the user’s ability to transmit force to the handle, and thus is determined by both the coefficient of friction between hand and handle and the diameter of the handle. Irregularities in the shape of the handle make little or no difference to the ability to apply torque, although sharp edges can cause discomfort and eventual tissue damage. The diameter of a cylindrical handle that allows the greatest application of torque is 50 to 65 mm, while that for a sphere is 65 to 75 mm.
Handles
Shape of handle
The shape of a handle should maximize contact between skin and handle. It should be generalized and basic, commonly of flattened cylindrical or elliptical section, with long curves and flat planes, or a sector of a sphere, put together in such a manner as to conform to the general contours of the grasping hand. Because of its attachment to the body of a tool, the handle may also take the form of a stirrup, a T-shape or an L-shape, but the portion that contacts the hand will be in the basic form.
The space enclosed by the fingers is, of course, complex. The use of simple curves is a compromise intended to meet the variations represented by different hands and different degrees of flexion. In this regard, it is undesirable to introduce any contour matching of flexed fingers into the handle in the form of ridges and valleys, flutings and indentations, since, in fact, these modifications would not fit a significant number of hands and might indeed, over a prolonged period, cause pressure injury to the soft tissues. In particular, recesses of greater that 3 mm are not recommended.
A modification of the cylindrical section is the hexagonal section, which is of particular value in the design of small calibre tools or instruments. It is easier to maintain a stable grip on a hexagonal section of small calibre than on a cylinder. Triangular and square sections have also been used with varying degrees of success. In these cases, the edges must be rounded to avert pressure injury.
Grip Surface and Texture
It is not by accident that for millennia wood has been the material of choice for tool handles other than those for crushing tools like pliers or clamps. In addition to its aesthetic appeal, wood has been readily available and easily worked by unskilled workers, and has qualities of elasticity, thermal conductivity, frictional resistance and relative lightness in relation to bulk that have made it very acceptable for this and other uses.
In recent years, metal and plastic handles have become more common for many tools, the latter in particular for use with light hammers or screwdrivers. A metal handle, however, transmits more force to the hand, and preferably should be encased in a rubber or plastic sheath. The grip surface should be slightly compressible, where feasible, nonconductive and smooth, and the surface area should be maximized to ensure pressure distribution over as large an area as possible. A foam rubber grip has been used to reduce the perception of hand fatigue and tenderness.
The frictional characteristics of the tool surface vary with the pressure exerted by the hand, with the nature of the surface and contamination by oil or sweat. A small amount of sweat increases the coefficient of friction.
Length of handle
The length of the handle is determined by the critical dimensions of the hand and the nature of the tool. For a hammer to be used by one hand in a power grip, for example, the ideal length ranges from a minimum of about 100 mm to a maximum of about 125 mm. Short handles are unsuitable for a power grip, while a handle shorter than 19 mm cannot be properly grasped between thumb and forefinger and is unsuitable for any tool.
Ideally, for a power tool, or a hand saw other than a coping or fret saw, the handle should accommodate at the 97.5th percentile level the width of the closed hand thrust into it, namely 90 to 100 mm in the long axis and 35 to 40 mm in the short.
Weight and Balance
Weight is not a problem with precision tools. For heavy hammers and power tools a weight between 0.9 kg and 1.5 kg is acceptable, with a maximum of about 2.3 kg. For weights greater than recommended, the tool should be supported by mechanical means.
In the case of a percussion tool such as a hammer, it is desirable to reduce the weight of the handle to the minimum compatible with structural strength and have as much weight as possible in the head. In other tools, the balance should be evenly distributed where possible. In tools with small heads and bulky handles this may not be possible, but the handle should then be made progressively lighter as the bulk increases relative to the size of the head and shaft.
Significance of Gloves
It is sometimes overlooked by tool designers that tools are not always held and operated by bare hands. Gloves are commonly worn for safety and comfort. Safety gloves are seldom bulky, but gloves worn in cold climates may be very heavy, interfering not only with sensory feedback but also with the ability to grasp and hold. The wearing of woollen or leather gloves can add 5 mm to hand thickness and 8 mm to hand breadth at the thumb, while heavy mittens can add as much as 25 to 40 mm respectively.
Handedness
The majority of the population in the western hemisphere favours the use of the right hand. A few are functionally ambidextrous, and all persons can learn to operate with greater or less efficiency with either hand.
Although the number of left-handed persons is small, wherever feasible the fitting of handles to tools should make the tool workable by either left-handed or right-handed persons (examples would include the positioning of the secondary handle in a power tool or the finger loops in scissors or clamps) unless it is clearly inefficient to do so, as in the case of screw-type fasteners which are designed to take advantage of the powerful supinating muscles of the forearm in a right-handed person while precluding the left-hander from using them with equal effectiveness. This sort of limitation has to be accepted since the provision of left-hand threads is not an acceptable solution.
Significance of Gender
In general, women tend to have smaller hand dimensions, smaller grasp and some 50 to 70% less strength than men, although of course a few women at the higher percentile end have larger hands and greater strength than some men at the lower percentile end. As a result there exists a significant although undetermined number of persons, mostly female, who have difficulty in manipulating various hand tools which have been designed with male use in mind, including in particular heavy hammers and heavy pliers, as well as metal cutting, crimping and clamping tools and wire strippers. The use of these tools by women may require an undesirable two-handed instead of single-handed function. In a mixed-gender workplace it is therefore essential to ensure that tools of suitable size are available not only to meet the requirements of women, but also to meet those of men who are at the low percentile end of hand dimensions.
Special considerations
The orientation of a tool handle, where feasible, should allow the operating hand to conform to the natural functional position of the arm and hand, namely with the wrist more than half-supinated, abducted about 15° and slightly dorsiflexed, with the little finger in almost full flexion, the others less so and the thumb adducted and slightly flexed, a posture sometimes erroneously called the handshake position. (In a handshake the wrist is not more than half-supinated.) The combination of adduction and dorsiflexion at the wrist with varying flexion of the fingers and thumb generates an angle of grasp comprising about 80° between the long axis of the arm and a line passing through the centre point of the loop created by the thumb and index finger, that is, the transverse axis of the fist.
Forcing the hand into a position of ulnar deviation, that is, with the hand bent towards the little finger, as is found in using a standard pliers, generates pressure on the tendons, nerves and blood vessels within the wrist structure and can give rise to the disabling conditions of tenosynovitis, carpal tunnel syndrome and the like. By bending the handle and keeping the wrist straight, (that is, by bending the tool and not the hand) compression of nerves, soft tissues and blood vessels can be avoided. While this principle has been long recognized, it has not been widely accepted by tool manufacturers or the using public. It has particular application in the design of cross-lever action tools such as pliers, as well as knives and hammers.
Pliers and cross-lever tools
Special consideration must be given to the shape of the handles of pliers and similar devices. Traditionally pliers have had curved handles of equal length, the upper curve approximating the curve of the palm of the hand and the lower curve approximating the curve of the flexed fingers. When the tool is held in the hand, the axis between the handles is in line with the axis of the jaws of the pliers. Consequently, in operation, it is necessary to hold the wrist in extreme ulnar deviation, that is, bent towards the little finger, while it is being repeatedly rotated. In this position the use of the hand-wrist-arm segment of the body is extremely inefficient and very stressful on the tendons and joint structures. If the action is repetitive it may give rise to various manifestations of overuse injury.
To counter this problem a new and ergonomically more suitable version of pliers has appeared in recent years. In these pliers the axis of the handles is bent through approximately 45° relative to the axis of the jaws. The handles are thickened to allow a better grasp with less localized pressure on the soft tissues. The upper handle is proportionately longer with a shape that fits into, and around the ulnar side of, the palm. The forward end of the handle incorporates a thumb support. The lower handle is shorter, with a tang, or rounded projection, at the forward end and a curve conforming to the flexed fingers.
While the foregoing is a somewhat radical change, several ergonomically sound improvements can be made in pliers relatively easily. Perhaps the most important, where a power grip is required, is in the thickening and slight flattening of the handles, with a thumb support at the head-end of the handle and a slight flare at the other end. If not integral to the design, this modification can be achieved by encasing the basic metal handle with a fixed or detachable non-conductive sheath made of rubber or an appropriate synthetic material, and perhaps bluntly roughened to improve the tactile quality. Indentation of the handles for fingers is undesirable. For repetitive use it may be desirable to incorporate a light spring into the handle to open it after closing.
The same principles apply to other cross-lever tools, particularly with respect to change in the thickness and flattening of the handles.
Knives
For a general purpose knife, that is, one that is not used in a dagger grasp, it is desirable to include a 15° angle between handle and blade to reduce the stress on joint tissues. The size and shape of handles should conform in general to that for other tools, but to allow for different hand sizes it has been suggested that two sizes of knife handle should be supplied, namely one to fit the 50th to 95th percentile user, and one for the 5th to 50th percentile. To allow the hand to exert force as close to the blade as possible the top surface of the handle should incorporate a raised thumb rest.
A knife guard is required to prevent the hand from slipping forward onto the blade. The guard may take several forms, such as a tang, or curved projection, about 10 to 15 mm in length, protruding downwards from the handle, or at right angles to the handle, or a bail guard comprising a heavy metal loop from front to rear of the handle. The thumb rest also acts to prevent slippage.
The handle should conform to general ergonomic guidelines, with a yielding surface resistant to grease.
Hammers
The requirements for hammers have been largely considered above, with the exception of that relating to bending the handle. As noted above, forced and repetitive bending of the wrist may cause tissue damage. By bending the tool instead of the wrist this damage may be reduced. With respect to hammers various angles have been examined, but it would appear that bending the head downward between 10° and 20° may improve comfort, if it does not actually improve performance.
Screwdrivers and scraping tools
The handles of screwdrivers and other tools held in a somewhat similar manner, such as scrapers, files, hand chisels and so on, have some special requirements. Each at one time or another is used with a precision grip or a power grip. Each relies on the functions of the fingers and the palm of the hand for stabilization and the transmission of force.
The general requirements of handles have already been considered. The most common effective shape of a screwdriver handle has been found to be that of a modified cylinder, dome-shaped at the end to receive the palm, and slightly flared where it meets the shaft to provide support to the ends of the fingers. In this manner, torque is applied largely by way of the palm, which is maintained in contact with the handle by way of pressure applied from the arm and the frictional resistance at the skin. The fingers, although transmitting some force, occupy more of a stabilizing role, which is less fatiguing since less power is required. Thus the dome of the head becomes very important in handle design. If there are sharp edges or ridges on the dome or where the dome meets the handle, then either the hand becomes callused and injured, or the transmission of force is transferred towards the less efficient and more readily fatigued fingers and thumb. The shaft is commonly cylindrical, but a triangular shaft has been introduced which provides better support for the fingers, although its use may be more fatiguing.
Where the use of a screwdriver or other fastener is so repetitive as to comprise an overuse injury hazard the manual driver should be replaced with a powered driver slung from an overhead harness in such a manner as to be readily accessible without obstructing the work.
Saws and power tools
Hand saws, with the exception of fret saws and light hacksaws, where a handle like that of a screwdriver is most appropriate, commonly have a handle which takes the form of a closed pistol grip attached to the blade of the saw.
The handle essentially comprises a loop into which the fingers are placed. The loop is effectively a rectangle with curved ends. To allow for gloves it should have internal dimensions of approximately 90 to 100 mm in the long diameter and 35 to 40 mm in the short. The handle in contact with the palm should have the flattened cylindrical shape already mentioned, with compound curves to reasonably fit the palm and the flexed fingers. The width from outer curve to inner curve should be about 35 mm, and the thickness not more than 25 mm.
Curiously, the function of grasping and holding a power tool is very similar to that of holding a saw, and consequently a somewhat similar type of handle is effective. The pistol grip common in power tools is akin to an open saw handle with the sides being curved instead of being flattened.
Most power tools comprise a handle, a body and a head. Placement of the handle is significant. Ideally handle, body and head should be in line so that the handle is attached at the rear of the body and the head protrudes from the front. The line of action is the line of the extended index finger, so that the head is eccentric to the central axis of the body. The centre of mass of the tool, however, is in front of the handle, while the torque is such as to create a turning movement of the body which the hand must overcome. Consequently it would be more appropriate to place the primary handle directly under the centre of mass in such a way that, if necessary, the body juts out behind the handle as well as in front. Alternatively, particularly in a heavy drill, a secondary handle can be placed underneath the drill in such a manner that the drill can be operated with either hand. Power tools are normally operated by a trigger incorporated into the upper front end of the handle and operated by the index finger. The trigger should be designed to be operated by either hand and should incorporate an easily reset latching mechanism to hold the power on when required.
Workstations
An Integrated Approach in the Design of Workstations
In ergonomics, the design of workstations is a critical task. There is general agreement that in any work setting, whether blue-collar or white-collar, a well-designed workstation furthers not only the health and well-being of the workers, but also productivity and the quality of the products. Conversely, the poorly designed workstation is likely to cause or contribute to the development of health complaints or chronic occupational diseases, as well as to problems with keeping product quality and productivity at a prescribed level.
To every ergonomist, the above statement may seem trivial. It is also recognized by every ergonomist that working life worldwide is full of not only ergonomic shortcomings, but blatant violations of basic ergonomic principles. It is clearly evident that there is a widespread unawareness with respect to the importance of workstation design among those responsible: production engineers, supervisors and managers.
It is noteworthy that there is an international trend with respect to industrial work which would seem to underline the importance of ergonomic factors: the increasing demand for improved product quality, flexibility and product delivery precision. These demands are not compatible with a conservative view regarding the design of work and workplaces.
Although in the present context it is the physical factors of workplace design that are of chief concern, it should be borne in mind that the physical design of the workstation cannot in practice be separated from the organization of work. This principle will be made evident in the design process described in what follows. The quality of the end result of the process relies on three supports: ergonomic knowledge, integration with productivity and quality demands, and participation. The process of implementation of a new workstation must cater to this integration, and it is the main focus of this article.
Design considerations
Workstations are meant for work. It must be recognized that the point of departure in the workstation design process is that a certain production goal has to be achieved. The designer—often a production engineer or other person at middle-management level—develops internally a vision of the workplace, and starts to implement that vision through his or her planning media. The process is iterative: from a crude first attempt, the solutions become gradually more and more refined. It is essential that ergonomic aspects be taken into account in each iteration as the work progresses.
It should be noted that ergonomic design of workstations is closely related to ergonomic assessment of workstations. In fact, the structure to be followed here applies equally to the cases where the workstation already exists or when it is in a planning stage.
In the design process, there is a need for a structure which ensures that all relevant aspects be considered. The traditional way to handle this is to use checklists containing a series of those variables which should be taken into account. However, general purpose checklists tend to be voluminous and difficult to use, since in a particular design situation only a fraction of the checklist may be relevant. Furthermore, in a practical design situation, some variables stand out as being more important than others. A methodology to consider these factors jointly in a design situation is required. Such a methodology will be proposed in this article.
Recommendations for workstation design must be based on a relevant set of demands. It should be noted that it is in general not enough to take into account threshold limit values for individual variables. A recognized combined goal of productivity and conservation of health makes it necessary to be more ambitious than in a traditional design situation. In particular, the question of musculoskeletal complaints is a major aspect in many industrial situations, although this category of problems is by no means limited to the industrial environment.
A Workstation Design Process
Steps in the process
In the workstation design and implementation process, there is always an initial need to inform users and to organize the project so as to allow for full user participation and in order to increase the chance of full employee acceptance of the final result. A treatment of this goal is not within the scope of the present treatise, which concentrates on the problem of arriving at an optimal solution for the physical design of the workstation, but the design process nonetheless allows the integration of such a goal. In this process, the following steps should always be considered:
- collection of user-specified demands
- prioritizing of demands
- transfer of demands into (a) technical specifications and (b) specifications in user terms
- iterative development of the workstation’s physical layout
- physical implementation
- trial period of production
- full production
- evaluation and identification of rest problems.
The focus here is on steps one through five. Many times, only a subset of all these steps is actually included in the design of workstations. There may be various reasons for this. If the workstation is a standard design, such as in some VDU working situations, some steps may duly be excluded. However, in most cases the exclusion of some of the steps listed would lead to a workstation of lower quality than what can be considered acceptable. This can be the case when economic or time constraints are too severe, or when there is sheer neglect due to lack of knowledge or insight at management level.
Collection of user-specified demands
It is essential to identify the user of the workplace as any member of the production organization who may be able to contribute qualified views on its design. Users may include, for instance, the workers, the supervisors, the production planners and production engineers, as well as the safety steward. Experience shows clearly that these actors all have their unique knowledge which should be made use of in the process.
The collection of the user-specified demands should meet a number of criteria:
- Openness. There should be no filter applied in the initial stage of the process. All points of view should be noted without voiced criticism.
- Non-discrimination. Viewpoints from every category should be treated equally at this stage of the process. Special consideration should be given to the fact that some persons may be more outspoken than others, and that there is a risk that they may silence some of the other actors.
- Development through dialogue. There should be an opportunity to adjust and develop the demands through a dialogue between participants of different backgrounds. Prioritizing should be addressed as part of the process.
- Versatility. The process of collection of user-specified demands should be reasonably economical and not require the involvement of specialist consultants or extensive time demands on the part of the participants.
The above set of criteria may be met by using a methodology based on quality function deployment (QFD) according to Sullivan (1986). Here, the user demands may be collected in a session where a mixed group of actors (not more than eight to ten people) is present. All participants are given a pad of removable self-sticking notes. They are asked to write down all workplace demands which they find relevant, each one on a separate slip of paper. Aspects relating to work environment and safety, productivity and quality should be covered. This activity may continue for as long as found necessary, typically ten to fifteen minutes. After this session, one after the other of the participants is asked to read out his or her demands and to stick the notes on a board in the room where everyone in the group can see them. The demands are grouped into natural categories such as lighting, lifting aids, production equipment, reaching requirements and flexibility demands. After the completion of the round, the group is given the opportunity to discuss and to comment on the set of demands, one category at a time, with respect to relevance and priority.
The set of user-specified demands collected in a process such as the one described in the above forms one of the bases for the development of the demand specification. Additional information in the process may be produced by other categories of actors, for example, product designers, quality engineers, or economists; however, it is vital to realize the potential contribution that the users can make in this context.
Prioritizing and demand specification
With respect to the specification process, it is essential that the different types of demands be given consideration according to their respective importance; otherwise, all aspects that have been taken into account will have to be considered in parallel, which may tend to make the design situation complex and difficult to handle. This is why checklists, which need to be elaborate if they are to serve the purpose, tend to be difficult to manage in a particular design situation.
It may be difficult to devise a priority scheme which serves all types of workstations equally well. However, on the assumption that manual handling of materials, tools or products is an essential aspect of the work to be carried out in the workstation, there is a high probability that aspects associated with musculoskeletal load will be at the top of the priority list. The validity of this assumption may be checked in the user demand collection stage of the process. Relevant user demands may be, for instance, associated with muscular strain and fatigue, reaching, seeing, or ease of manipulation.
It is essential to realize that it may not be possible to transform all user-specified demands into technical demand specifications. Although such demands may relate to more subtle aspects such as comfort, they may nevertheless be of high relevance and should be considered in the process.
Musculoskeletal load variables
In line with the above reasoning, we shall here apply the view that there is a set of basic ergonomic variables relating to musculoskeletal load which need to be taken into account as a priority in the design process, in order to eliminate the risk of work-related musculosketal disorders (WRMDs). This type of disorder is a pain syndrome, localized in the musculoskeletal system, which develops over long periods of time as a result of repeated stresses on a particular body part (Putz-Anderson 1988). The essential variables are (e.g., Corlett 1988):
- muscular force demand
- working posture demand
- time demand.
With respect to muscular force, criteria setting may be based on a combination of biomechanical, physiological and psychological factors. This is a variable that is operationalized through measurement of output force demands, in terms of handled mass or required force for, say, the operation of handles. Also, peak loads in connection with highly dynamic work may have to be taken into account.
Working posture demands may be evaluated by mapping (a) situations where the joint structures are stretched beyond the natural range of movement, and (b) certain particularly awkward situations, such as kneeling, twisting, or stooped postures, or work with the hand held above shoulder level.
Time demands may be evaluated on the basis of mapping (a) short-cycle, repetitive work, and (b) static work. It should be noted that static work evaluation may not exclusively concern maintaining a working posture or producing a constant output force over lengthy periods of time; from the point of view of the stabilizing muscles, particularly in the shoulder joint, seemingly dynamic work may have a static character. It may thus be necessary to consider lengthy periods of joint mobilization.
The acceptability of a situation is of course based in practice on the demands on the part of the body that is under the highest strain.
It is important to note that these variables should not be considered one at a time but jointly. For instance, high force demands may be acceptable if they occur only occasionally; lifting the arm above shoulder level once in a while is not normally a risk factor. But combinations among such basic variables must be considered. This tends to make criteria setting difficult and involved.
In the Revised NIOSH equation for the design and evaluation of manual handling tasks (Waters et al. 1993), this problem is addressed by devising an equation for recommended weight limits which takes into account the following mediating factors: horizontal distance, vertical lifting height, lifting asymmetry, handle coupling and lifting frequency. In this way, the 23-kilogram acceptable load limit based on biomechanical, physiological and psychological criteria under ideal conditions, may be modified substantially upon taking into account the specifics of the working situation. The NIOSH equation provides a base for evaluation of work and workplaces involving lifting tasks. However, there are severe limitations as to the usability of the NIOSH equation: for instance, only two-handed lifts may be analysed; scientific evidence for analysis of one-handed lifts is still inconclusive. This illustrates the problem of applying scientific evidence exclusively as a basis for work and workplace design: in practice, scientific evidence must be merged with educated views of persons who have direct or indirect experience of the type of work considered.
The cube model
Ergonomic evaluation of workplaces, taking into account the complex set of variables which need to be considered, is to a large extent a communications problem. Based on the prioritizing discussion described above, a cube model for ergonomic evaluation of workplaces was developed (Kadefors 1993). Here the prime goal was to develop a didactic tool for communication purposes, based on the assumption that output force, posture and time measures in a great majority of situations constitute interrelated, prioritized basic variables.
For each one of the basic variables, it is recognized that the demands may be grouped with respect to severity. Here, it is proposed that such a grouping may be made in three classes: (1) low demands, (2) medium demands or (3) high demands. The demand levels may be set either by using whatever scientific evidence is available or by taking a consensus approach with a panel of users. These two alternatives are of course not mutually exclusive, and may well entail similar results, but probably with different degrees of generality.
As noted above, combinations of the basic variables determine to a large extent the risk level with respect to the development of musculoskeletal complaints and cumulative trauma disorders. For instance, high time demands may render a working situation unacceptable in cases where there are also at least medium level demands with respect to force and posture. It is essential in the design and assessment of workplaces that the most important variables be considered jointly. Here a cube model for such evaluation purposes is proposed. The basic variables—force, posture and time—constitute the three axes of the cube. For each combination of demands a subcube may be defined; in all, the model incorporates 27 such subcubes (see figure 1).
Figure 1. The "cube model" for ergonomics assessment. Each cube represents a combination of demands relating to force, posture and time. Light: acceptable combination; gray: conditionally acceptable; black: unacceptable
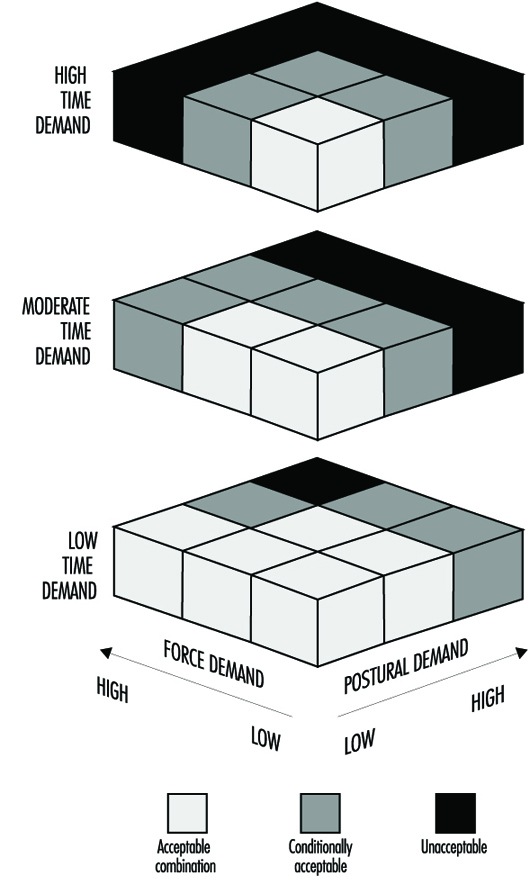
An essential aspect of the model is the degree of acceptability of the demand combinations. In the model, a three-zone classification scheme is proposed for acceptability: (1) the situation is acceptable, (2) the situation is conditionally acceptable or (3) the situation is unacceptable. For didactic purposes, each subcube may be given a certain texture or colour (say, green-yellow-red). Again, the assessment may be user-based or based on scientific evidence. The conditionally acceptable (yellow) zone means that “there exists a risk of disease or injury that cannot be neglected, for the whole or a part of the operator population in question” (CEN 1994).
In order to develop this approach, it is useful to consider a case: the evaluation of load on the shoulder in moderately paced one-handed materials handling. This is a good example, since in this type of situation, it is normally the shoulder structures that are under the heaviest strain.
With respect to the force variable, classification may be based in this case on handled mass. Here, low force demand is identified as levels below 10% of maximal voluntary lifting capacity (MVLC), which amounts to approximately 1.6 kg in an optimal working zone. High force demand requires more than 30% MVLC, approximately 4.8 kg. Medium force demand falls in between these limits. Low postural strain is when the upper arm is close to the thorax. High postural strain is when humeral abduction or flexion exceeds 45°. Medium postural strain is when the abduction/flexion angle is between 15° and 45°. Low time demand is when the handling occupies less than one hour per working day on and off, or continuously for less than 10 minutes per day. High time demand is when the handling takes place for more than four hours per working day, or continuously for more than 30 minutes (sustained or repetitively). Medium time demand is when the exposure falls between these limits.
In figure 1, degrees of acceptability have been assigned to combinations of demands. For instance, it is seen that high time demands may only be combined with combined low force and postural demands. Moving from unacceptable to acceptable may be undertaken by reducing demands in either dimension, but reduction in time demands is the most efficient way in many cases. In other words, in some cases workplace design should be altered, in other cases it may be more efficient to change the organization of work.
Using a consensus panel with a set of users for definition of demand levels and classification of degree of acceptability may enhance the workstation design process considerably, as considered below.
Additional variables
In addition to the basic variables considered above, a set of variables and factors characterizing the workplace from an ergonomics point of view has to be taken into account, depending upon the particular conditions of the situation to be analysed. They include:
- precautions to reduce risks for accidents
- specific environmental factors such as noise, lighting and ventilation
- exposure to climatic factors
- exposure to vibration (from hand-held tools or whole body)
- ease of meeting productivity and quality demands.
To a large extent these factors may be considered one at a time; hence the checklist approach may be useful. Grandjean (1988) in his textbook covers the essential aspects that usually need to be taken into account in this context. Konz (1990) in his guidelines provides for workstation organization and design a set of leading questions focusing on worker-machine interfacing in manufacturing systems.
In the design process followed here, the checklist should be read in conjunction with the user-specified demands.
A Workstation Design Example: Manual Welding
As an illustrative (hypothetical) example, the design process leading to implementation of a workstation for manual welding (Sundin et al. 1994) is described here. Welding is an activity frequently combining high demands for muscular force with high demands for manual precision. The work has a static character. The welder is often doing welding exclusively. The welding work environment is generally hostile, with a combination of exposure to high noise levels, welding smoke and optical radiation.
The task was to devise a workplace for manual MIG (metal inert gas) welding of medium size objects (up to 300 kg) in a workshop environment. The workstation had to be flexible since there was a variety of objects to be manufactured. There were high demands for productivity and quality.
A QFD process was carried out in order to provide a set of workstation demands in user terms. Welders, production engineers and product designers were involved. User demands, which are not listed here, covered a wide range of aspects including ergonomics, safety, productivity and quality.
Using the cube model approach, the panel identified, by consensus, limits between high, moderate and low load:
- Force variable. Less than 1 kg handled mass is termed a low load, whereas more than 3 kg is considered a high load.
- Postural strain variable. Working positions implying high strain are those involving elevated arms, twisted or deep forward-flexed positions, and kneeling positions, and also include situations where the wrist is held in extreme flexion/extension or deviation. Low strain occurs where the posture is straight upright standing or sitting and where hands are in optimal working zones.
- Time variable. Less than 10% of the working time devoted to welding is considered low demand, whereas more than 40% of total working time is termed high demand. Medium demands occur when the variable falls between the limits given above, or when the situation is unclear.
It was clear from assessment using the cube model (figure 1) that high time demands could not be accepted if there were concurrent high or moderate demands in terms of force and postural strain. In order to reduce these demands, mechanized object handling and tool suspension was deemed a necessity. There was consensus developed around this conclusion. Using a simple computer-aided design (CAD) program (ROOMER), an equipment library was created. Various workplace station layouts could be developed very easily and modified in close interaction with the users. This design approach has significant advantages compared with merely looking at plans. It gives the user an immediate vision of what the intended workplace may look like.
Figure 2. A CAD version of a workstation for manual welding, arrived at in the design process

Figure 2 shows the welding workstation arrived at using the CAD system. It is a workplace which reduces the force and posture demands, and which meets nearly all the residual user demands put forward.
Figure 3. The welding workstation implemented

On the basis of the results of the first stages of the design process, a welding workplace (figure 3) was implemented. Assets of this workplace include:
- Work in the optimized zone is facilitated using a computerized handling device for welding objects. There is an overhead hoist for transportation purposes. As an alternative, a balanced lifting device is supplied for easy object handling.
- The welding gun and grinding machine are suspended, thus reducing force demands. They can be positioned anywhere around the welding object. A welding chair is supplied.
- All media come from above, which means that there are no cables on the floor.
- The workstation has lighting at three levels: general, workplace and process. The workplace lighting comes from ramps above the wall elements. The process lighting is integrated in the welding smoke ventilation arm.
- The workstation has ventilation at three levels: general displacement ventilation, workplace ventilation using a movable arm, and integrated ventilation in the MIG welding gun. The workplace ventilation is controlled from the welding gun.
- There are noise-absorbing wall elements on three sides of the workplace. A transparent welding curtain covers the fourth wall. This makes it possible for the welder to keep informed of what happens in the workshop environment.
In a real design situation, compromises of various kinds may have to be made, due to economic, space and other constraints. It should be noted, however, that licensed welders are hard to come by for the welding industry around the world, and they represent a considerable investment. Nearly no welders go into normal retirement as active welders. Keeping the skilled welder on the job is beneficial for all parties involved: welder, company and society. For instance, there are very good reasons why equipment for object handling and positioning should be an integral constituent of many welding workplaces.
Data for Workstation Design
In order to be able to design a workplace properly, extensive sets of basic information may be needed. Such information includes anthropometric data of user categories, lifting strength and other output force capacity data of male and female populations, specifications of what constitutes optimal working zones and so forth. In the present article, references to some key papers are given.
The most complete treatment of virtually all aspects of work and workstation design is probably still the textbook by Grandjean (1988). Information on a wide range of anthropometric aspects relevant to workstation design is presented by Pheasant (1986). Large amounts of biomechanical and anthropometric data are given by Chaffin and Andersson (1984). Konz (1990) has presented a practical guide to workstation design, including many useful rules of thumb. Evaluation criteria for the upper limb, particularly with reference to cumulative trauma disorders, have been presented by Putz-Anderson (1988). An assessment model for work with hand tools was given by Sperling et al. (1993). With respect to manual lifting, Waters and co-workers have developed the revised NIOSH equation, summarizing existing scientific knowledge on the subject (Waters et al. 1993). Specification of functional anthropometry and optimal working zones have been presented by, for example, Rebiffé, Zayana and Tarrière (1969) and Das and Grady (1983a, 1983b). Mital and Karwowski (1991) have edited a useful book reviewing various aspects relating in particular to the design of industrial workplaces.
The large amount of data needed to design workstations properly, taking all relevant aspects into account, will make necessary the use of modern information technology by production engineers and other responsible people. It is likely that various types of decision-support systems will be made available in the near future, for instance in the form of knowledge-based or expert systems. Reports on such developments have been given by, for example, DeGreve and Ayoub (1987), Laurig and Rombach (1989), and Pham and Onder (1992). However, it is an extremely difficult task to devise a system making it possible for the end-user to have easy access to all relevant data needed in a specific design situation.
Sleep Deprivation
Healthy individuals regularly sleep for several hours every day. Normally they sleep during the night hours. They find it most difficult to remain awake during the hours between midnight and early morning, when they normally sleep. If an individual has to remain awake during these hours either totally or partially, the individual comes to a state of forced sleep loss, or sleep deprivation, that is usually perceived as tiredness. A need for sleep, with fluctuating degrees of sleepiness, is felt which continues until sufficient sleep is taken. This is the reason why periods of sleep deprivation are often said to cause a person to incur sleep deficit or sleep debt.
Sleep deprivation presents a particular problem for workers who cannot take sufficient sleep periods because of work schedules (e.g., working at night) or, for that matter, prolonged free-time activities. A worker on a night shift remains sleep-deprived until the opportunity for a sleep period becomes available at the end of the shift. Since sleep taken during daytime hours is usually shorter than needed, the worker cannot recover from the condition of sleep loss sufficiently until a long sleep period, most likely a night sleep, is taken. Until then, the person accumulates a sleep deficit. (A similar condition—jet lag—arises after travelling between time zones that differ by a few hours or more. The traveller tends to be sleep-deprived as the activity periods in the new time zone correspond more clearly to the normal sleep period in the originating place.) During the periods of sleep loss, workers feel tired and their performance is affected in various ways. Thus various degrees of sleep deprivation are incorporated into the daily life of workers having to work irregular hours and it is important to take measures to cope with unfavourable effects of such sleep deficit. The main conditions of irregular working hours that contribute to sleep deprivation are shown in table 1.
Table 1. Main conditions of irregular working hours which contribute to sleep deprivation of various degrees
|
Irregular working hours |
Conditions leading to sleep deprivation |
|
Night duty |
No or shortened night-time sleep |
|
Early morning or late evening duty |
Shortened sleep, disrupted sleep |
|
Long hours of work or working two shifts together |
Phase displacement of sleep |
|
Straight night or early morning shifts |
Consecutive phase displacement of sleep |
|
Short between-shift period |
Short and disrupted sleep |
|
Long interval between days off |
Accumulation of sleep shortages |
|
Work in a different time zone |
No or shortened sleep during the “night” hours in the originating place (jet lag) |
|
Unbalanced free time periods |
Phase displacement of sleep, short sleep |
In extreme conditions, sleep deprivation may last for more than a day. Then sleepiness and performance changes increase as the period of sleep deprivation is prolonged. Workers, however, normally take some form of sleep before sleep deprivation becomes too protracted. If the sleep thus taken is not sufficient, the effects of sleep shortage still continue. Thus, it is important to know not only the effects of sleep deprivation in various forms but also the ways in which workers can recover from it.
Figure 1. Perfomance, sleep ratings and physiological variables of a group of subjects exposed to two nights of sleep deprivation
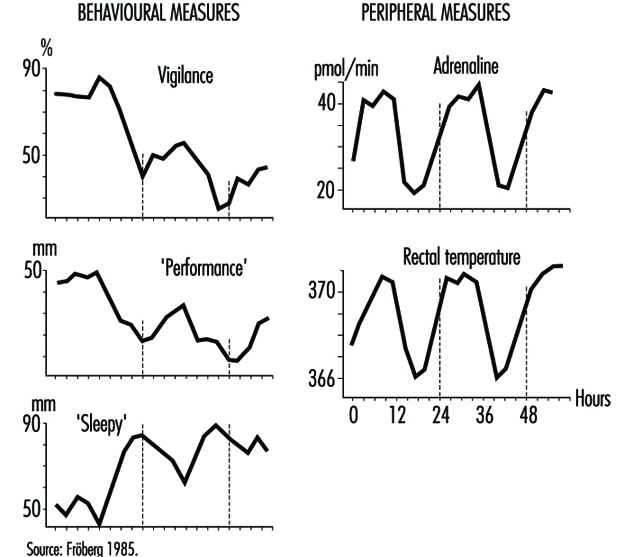
The complex nature of sleep deprivation is shown by figure 1, which depicts data from laboratory studies on the effects of two days of sleep deprivation (Fröberg 1985). The data show three basic changes resulting from prolonged sleep deprivation:
- There is a general decreasing trend in both objective performance and subjective ratings of performance efficiency.
- The decline in performance is influenced by the time of day. This cycling decline is correlated with those physiological variables which have a circadian cycling period. Performance is better in the normal activity phase when, for example, adrenaline excretion and body temperature are higher than those in the period originally assigned to a normal night’s sleep, when the physiological measures are low.
- Self-ratings of sleepiness increase with time of continuous sleep deprivation, with a clear cyclic component associated with time of day.
The fact that the effects of sleep deprivation are correlated with physiological circadian rhythms helps us to understand its complex nature (Folkard and Akerstedt 1992). These effects should be viewed as a result of a phase shift of the sleep-wakefulness cycle in one’s daily life.
The effects of continuous work or sleep deprivation thus include not only a reduction in alertness but decreased performance capabilities, increased probability of falling asleep, lowered well-being and morale and impaired safety. When such periods of sleep deprivation are repeated, as in the case of shift workers, their health may be affected (Rutenfranz 1982; Koller 1983; Costa et al. 1990). An important aim of research is thus to determine to what extent sleep deprivation damages the well-being of individuals and how we can best use the recovery function of sleep in reducing such effects.
Effects of Sleep Deprivation
During and after a night of sleep deprivation, the physiological circadian rhythms of the human body seem to remain sustained. For example, the body temperature curve during the first day’s work among night-shift workers tends to keep its basic circadian pattern. During the night hours, the temperature declines towards early morning hours, rebounds to rise during the subsequent daytime and falls again after an afternoon peak. The physiological rhythms are known to get “adjusted” to the reversed sleep-wakefulness cycles of night-shift workers only gradually in the course of several days of repeated night shifts. This means that the effects on performance and sleepiness are more significant during night hours than in the daytime. The effects of sleep deprivation are therefore variably associated with the original circadian rhythms seen in physiological and psychological functions.
The effects of sleep deprivation on performance depend on the type of the task to be performed. Different characteristics of the task influence the effects (Fröberg 1985; Folkard and Monk 1985; Folkard and Akerstedt 1992). Generally, a complex task is more vulnerable than a simpler task. Performance of a task involving an increasing number of digits or a more complex coding deteriorates more during three days of sleep loss (Fröberg 1985; Wilkinson 1964). Paced tasks that need to be responded to within a certain interval deteriorate more than self-paced tasks. Practical examples of vulnerable tasks include serial reactions to defined stimulations, simple sorting operations, the recording of coded messages, copy typing, display monitoring and continuous inspection. Effects of sleep deprivation on strenuous physical performance are also known. Typical effects of prolonged sleep deprivation on performance (on a visual task) is shown in figure 2 (Dinges 1992). The effects are more pronounced after two nights of sleep loss (40-56 hours) than after one night of sleep loss (16-40 hours).
Figure 2. Regression lines fit to response speed (the reciprocal of response times) on a 10-minute simple, unprepared visual task administered repeatedly to healthy young adults during no sleep loss (5-16 hours), one night of sleep loss (16-40 hours) and two nights of sleep loss (40-56 hours)
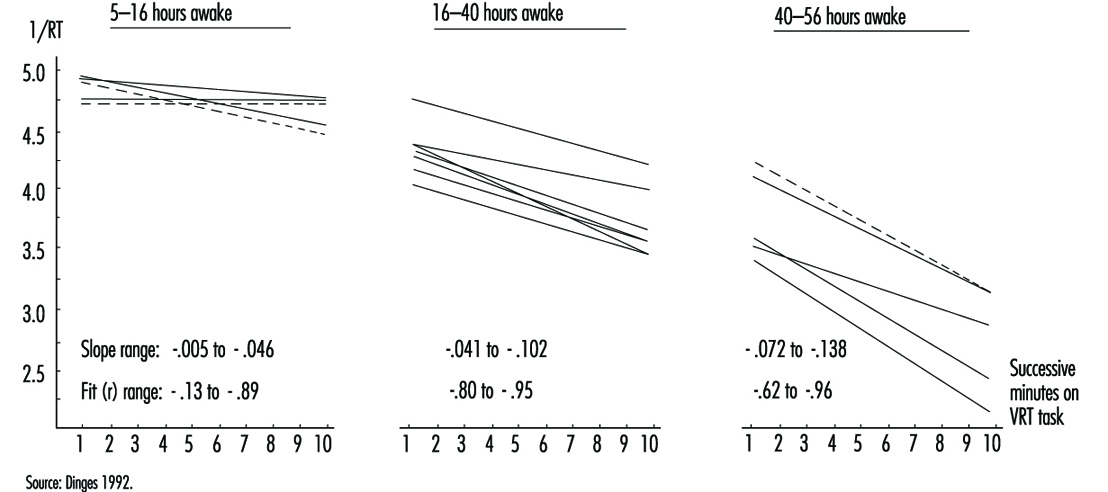
The degree to which the performance of tasks is affected also appears to depend on how it is influenced by the “masking” components of the circadian rhythms. For example, some measures of performance, such as five-target memory search tasks, are found to adjust to night work considerably more quickly than serial reaction time tasks, and hence they may be relatively unimpaired on rapidly rotating shift systems (Folkard et al. 1993). Such differences in the effects of endogenous physiological body clock rhythms and their masking components must be taken into account in considering the safety and accuracy of performance under the influence of sleep deprivation.
One particular effect of sleep deprivation on performance efficiency is the appearance of frequent “lapses” or periods of no response (Wilkinson 1964; Empson 1993). These performance lapses are short periods of lowered alertness or light sleep. This can be traced in records of videotaped performance, eye movements or electroencephalograms (EEGs). A prolonged task (one-half hour or more), especially when the task is replicated, can more easily lead to such lapses. Monotonous tasks such as repetitions of simple reactions or monitoring of infrequent signals are very sensitive in this regard. On the other hand, a novel task is less affected. Performance in changing work situations is also resistant.
While there is evidence of a gradual arousal decrease in sleep deprivation, one would expect less affected performance levels between lapses. This explains why results of some performance tests show little influence of sleep loss when the tests are done in a short period of time. In a simple reaction time task, lapses would lead to very long response times whereas the rest of the measured times would remain unchanged. Caution is thus needed in interpreting test results concerning sleep loss effects in actual situations.
Changes in sleepiness during sleep deprivation obviously relate to physiological circadian rhythms as well as to such lapse periods. Sleepiness sharply increases with time of the first period of night-shift work, but decreases during subsequent daytime hours. If sleep deprivation continues to the second night sleepiness becomes very advanced during the night hours (Costa et al. 1990; Matsumoto and Harada 1994). There are moments when the need for sleep is felt to be almost irresistible; these moments correspond to the appearance of lapses, as well as to the appearance of interruptions in the cerebral functions as evidenced by EEG records. After a while, sleepiness is felt to be reduced, but there follows another period of lapse effects. If workers are questioned about various fatigue feelings, however, they usually mention increasing levels of fatigue and general tiredness persisting throughout the sleep deprivation period and between-lapse periods. A slight recovery of subjective fatigue levels is seen during the daytime following a night of sleep deprivation, but fatigue feelings are remarkably advanced in the second and subsequent nights of continued sleep deprivation.
During sleep deprivation, sleep pressure from the interaction of prior wakefulness and circadian phase may always be present to some degree, but the lability of state in sleepy subjects is also modulated by context effects (Dinges 1992). Sleepiness is influenced by the amount and type of stimulation, the interest afforded by the environment and the meaning of the stimulation to the subject. Monotonous stimulation or that requiring sustained attention can more easily lead to vigilance decrement and lapses. The greater the physiological sleepiness due to sleep loss, the more the subject is vulnerable to environmental monotony. Motivation and incentive can help override this environmental effect, but only for a limited period.
Effects of Partial Sleep Deprivation and Accumulated Sleep Shortages
If a subject works continuously for a whole night without sleep, many performance functions will have definitely deteriorated. If the subject goes to the second night shift without getting any sleep, the performance decline is far advanced. After the third or fourth night of total sleep deprivation, very few people can stay awake and perform tasks even if highly motivated. In actual life, however, such conditions of total sleep loss rarely occur. Usually people take some sleep during subsequent night shifts. But reports from various countries show that sleep taken during daytime is almost always insufficient to recover from the sleep debt incurred by night work (Knauth and Rutenfranz 1981; Kogi 1981; ILO 1990). As a result, sleep shortages accumulate as shift workers repeat night shifts. Similar sleep shortages also result when sleep periods are reduced on account of the need to follow shift schedules. Even if night sleep can be taken, sleep restriction of as little as two hours each night is known to lead to an insufficient amount of sleep for most persons. Such sleep reduction can lead to impaired performance and alertness (Monk 1991).
Examples of conditions in shift systems which contribute to accumulation of sleep shortages, or partial sleep deprivation, are given in table 1. In addition to continued night work for two or more days, short between-shift periods, repetition of an early start of morning shifts, frequent night shifts and inappropriate holiday allotment accelerate the accumulation of sleep shortages.
The poor quality of daytime sleep or shortened sleep is important, too. Daytime sleep is accompanied by an increased frequency of awakenings, less deep and slow-wave sleep and a distribution of REM sleep different from that of normal night-time sleep (Torsvall, Akerstedt and Gillberg 1981; Folkard and Monk 1985; Empson 1993). Thus a daytime sleep may not be as sound as a night sleep even in a favourable environment.
This difficulty of taking good quality sleep due to different timing of sleep in a shift system is illustrated by figure 3 which shows the duration of sleep as a function of the time of sleep onset for German and Japanese workers based on diary records (Knauth and Rutenfranz 1981; Kogi 1985). Due to circadian influence, daytime sleep is forced to be short. Many workers may have split sleep during the daytime and often add some sleep in the evening where possible.
Figure 3. Mean sleep length as a function of the time of sleep onset. Comparison of data from German and Japanese shift workers.
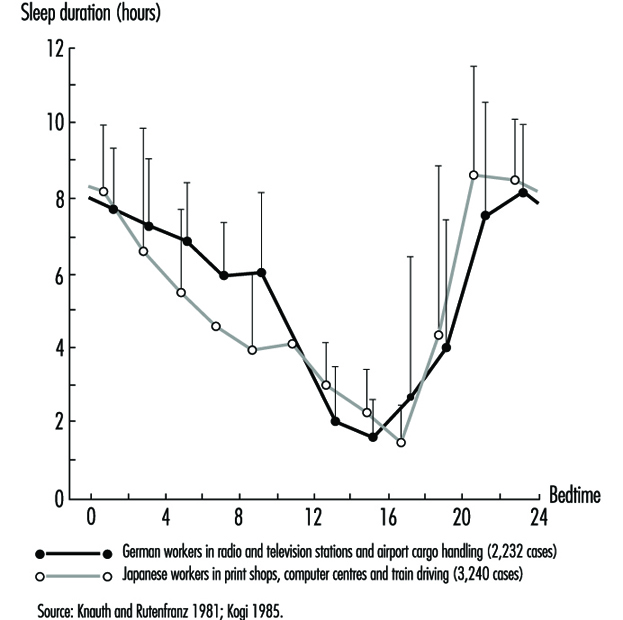
In real-life settings, shift workers take a variety of measures to cope with such accumulation of sleep shortages (Wedderburn 1991). For example, many of them try to sleep in advance before a night shift or have a long sleep after it. Although such efforts are by no means entirely effective to offset the effects of sleep deficit, they are made quite deliberately. Social and cultural activities may be restricted as part of coping measures. Outgoing free-time activities, for example, are undertaken less frequently between two night shifts. Sleep timing and duration as well as the actual accumulation of sleep deficit thus depend on both job-related and social circumstances.
Recovery from Sleep Deprivation and Health Measures
The only effective means of recovering from sleep deprivation is to sleep. This restorative effect of sleep is well known (Kogi 1982). As recovery by sleep may differ according to its timing and duration (Costa et al. 1990), it is essential to know when and for how long people should sleep. In normal daily life, it is always the best to take a full night’s sleep to accelerate the recovery from sleep deficit but efforts are usually made to minimize sleep deficit by taking sleep at different occasions as replacements of normal night sleeps of which one has been deprived. Aspects of such replacement sleeps are shown in table 2.
Table 2. Aspects of advance, anchor & retard sleeps taken as replacement of normal night sleep
|
Aspect |
Advance sleep |
Anchor sleep |
Retard sleep |
|
Occasion |
Before a night shift |
Intermittent night |
After a night shift |
|
Duration |
Usually short |
Short by definition |
Usually short but |
|
Quality |
Longer latency of |
Short latency |
Shorter latency for |
|
Interaction with |
Disrupted rhythms; |
Conducive to |
Disrupted rhythms; |
To offset night sleep deficit, the usual effort made is to take daytime sleep in “advance” and “retard” phases (i.e., before and after night-shift work). Such a sleep coincides with the circadian activity phase. Thus the sleep is characterized by longer latency, shortened slow-wave sleep, disrupted REM sleep and disturbances of one’s social life. Social and environmental factors are important in determining the recuperative effect of a sleep. That a complete conversion of circadian rhythms is impossible for a shift worker in a real-life situation should be borne in mind in considering the effectiveness of the recovery functions of sleep.
In this respect, interesting features of a short “anchor sleep” have been reported (Minors and Waterhouse 1981; Kogi 1982; Matsumoto and Harada 1994). When part of the customary daily sleep is taken during the normal night sleep period and the rest at irregular times, the circadian rhythms of rectal temperature and urinary secretion of several electrolytes can retain a 24-hour period. This means that a short night-time sleep taken during the night sleep period can help preserve the original circadian rhythms in subsequent periods.
We may assume that sleeps taken at different periods of the day could have certain complementary effects in view of the different recovery functions of these sleeps. An interesting approach for night-shift workers is the use of a night-time nap which usually lasts up to a few hours. Surveys show this short sleep taken during a night shift is common among some groups of workers. This anchor-sleep type sleep is effective in reducing night work fatigue (Kogi 1982) and may reduce the need of recovery sleep. Figure 4 compares the subjective feelings of fatigue during two consecutive night shifts and the off-duty recovery period between the nap-taking group and the non-nap group (Matsumoto and Harada 1994). The positive effects of a night-time nap in reducing fatigue was obvious. These effects continued for a large part of the recovery period following night work. Between these two groups, no significant difference was found upon comparing the length of the day sleep of the non-nap group with the total sleeping time (night-time nap plus subsequent day sleep) of the nap group. Therefore a night-time nap enables part of the essential sleep to be taken in advance of the day sleep following night work. It can therefore be suggested that naps taken during night work can to a certain extent aid recovery from the fatigue caused by that work and accompanying sleep deprivation (Sakai et al. 1984; Saito and Matsumoto 1988).
Figure 4. Mean scores for subjective feelings of fatigue during two consecutive night shifts and the off-duty recovery period for nap and no-nap groups
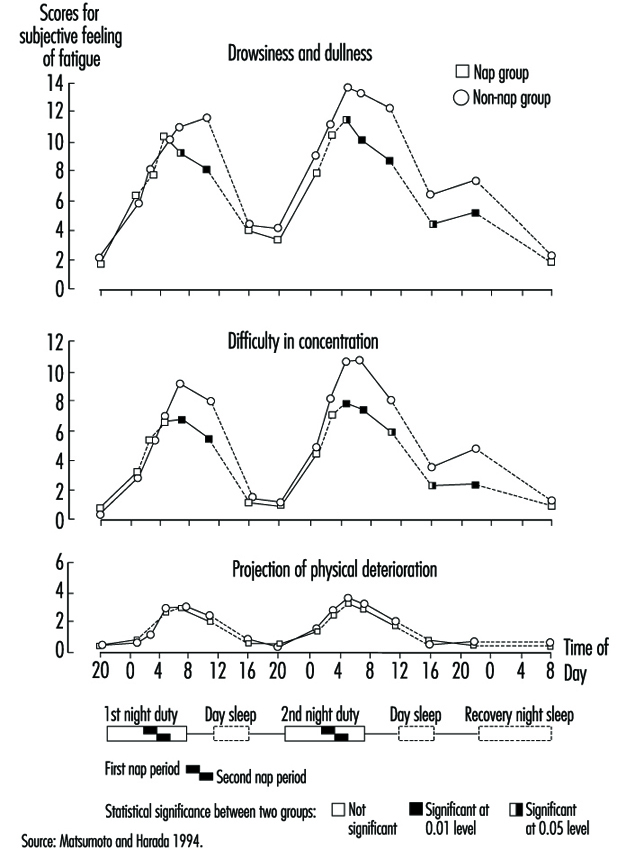
It must be admitted, however, that it is not possible to work out optimal strategies that each worker suffering from sleep deficit can apply. This is demonstrated in the development of international labour standards for night work that recommend a set of measures for workers doing frequent night work (Kogi and Thurman 1993). The varied nature of these measures and the trend towards increasing flexibility in shift systems clearly reflect an effort to develop flexible sleep strategies (Kogi 1991). Age, physical fitness, sleep habits and other individual differences in tolerance may play important roles (Folkard and Monk 1985; Costa et al. 1990; Härmä 1993). Increasing flexibility in work schedules in combination with better job design is useful in this regard (Kogi 1991).
Sleep strategies against sleep deprivation should be dependent on type of working life and be flexible enough to meet individual situations (Knauth, Rohmert and Rutenfranz 1979; Rutenfranz, Knauth and Angersbach 1981; Wedderburn 1991; Monk 1991). A general conclusion is that we should minimize night sleep deprivation by selecting appropriate work schedules and facilitate recovery by encouraging individually suitable sleeps, including replacement sleeps and a sound night-time sleep in the early periods after sleep deprivation. It is important to prevent the accumulation of sleep deficit. The period of night work which deprives workers of sleep in the normal night sleep period should be as short as possible. Between-shift intervals should be long enough to allow a sleep of sufficient length. A better sleep environment and measures to cope with social needs are also useful. Thus, social support is essential in designing working time arrangements, job design and individual coping strategies in promoting the health of workers faced with frequent sleep deficit.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."