Diet, physical activity and other lifestyle practices such as not smoking cigarettes and reduction of stress are important in the prevention of chronic diseases. Proper nutrition and other healthy lifestyle practices also aid in maintaining individual well-being and productivity. The worksite is an ideal place to teach people about good health habits, including sound nutrition, weight control and exercise practices. It is an excellent forum for efficiently disseminating information and monitoring and reinforcing changes that have been made (Kaplan and Brinkman-Kaplan 1994). Nutrition programs rank among the most commonly included activities in wellness programs sponsored by employers, labor unions and, sometimes, jointly. In addition to formal classes and programs, other supportive educational efforts such as newsletters, memos, payroll inserts, posters, bulletin boards, and electronic mail (e-mail) can be offered. Nutrition education materials can also reach employees’ dependants through mailings to the home and making classes and seminars available to homemakers who are the gatekeepers of their families’ food intake practices and habits. These approaches provide useful information that can be applied easily both at the worksite and elsewhere and can help reinforce formal instruction and encourage workers to enroll in programs or make informed and profitable use of worksite facilities (such as the cafeteria). Moreover, carefully targeted materials and classes can have a very significant impact on many people, including the families of workers, especially their children, who can learn and adopt good nutrition practices that will last a lifetime and be passed on to future generations.
Successful worksite intervention programs require a supportive environment that enables workers to act on nutrition messages. In this context, it is essential that employees have access to appropriate foods in cafeterias and vending machines that facilitate adherence to a recommended diet. For those whose lunches depend on “brown bags” or lunch boxes, worksite arrangements for storing the lunch bags or boxes are part of a supportive environment. In addition, employer-provided or entrepreneurial lunch wagons can offer nourishing food on the spot at field worksites remote from feeding facilities. Facilities for light personal washing before eating are also important. These employer-sponsored activities express a strong commitment to the health and well-being of their employees.
In-plant Catering Programs, Vending Machines, and Coffee and Tea Breaks
Many employers subsidize in-plant food services partially or totally, making them attractive as well as convenient. Even where there is only one shift, many cafeterias serve breakfasts and dinners as well as lunches and refreshments at breaks; this is of particular value to those who live alone or whose food preparation in the home may be less than adequate. Some worksite cafeterias are open to employees’ friends and families to encourage “lunching-in” rather than using more expensive and often less nutritionally desirable facilities in the community.
Modifying foods that are offered at the worksite provides support and encouragement of healthy eating patterns (Glanz and Mullis 1988). In fact, cafeteria interventions are one of the most popular worksite nutrition programs as they allow point-of-choice nutrition information to be readily made available (Glanz and Rogers 1994). Other interventions include modifying menu choices to provide low-fat, low-calorie and high-fiber foods or to highlight “heart healthy” foods (Richmond 1986). Worksites also can implement healthy catering policies and offer nutrient-dense foods that are low in fat, cholesterol and sodium (American Dietetic Association 1994). Negotiations can be conducted with food service vendors to also provide low-fat food items, including fruit, in vending machines. One such program resulted in a greater selection by employees of low-calorie foods (Wilber 1983). Food service management, caterers and vendors may realize greater sales and increased participation in the food service activities at the worksite especially when tasty, attractive, healthy foods are served (American Dietetic Association 1994).
Coffee and tea breaks with nutrient-dense snack foods available can help employees meet nutritional needs. Many “lunch hours” are only 30 or 40 minutes long and because some employees use that time for shopping, socializing or personal business, they skip eating. A supportive environment may require lengthening the lunch period. Moreover, maintaining proper hygiene in the in-plant catering facility and ensuring the health and proper training of all food service personnel (even when the facility is operated under contract with an outside vendor) demonstrates the worksite’s commitment to employee health, thereby increasing workers’ interest in supporting the onsite food service establishments as well as other programs.
General Nutrition Guidance
The basic dietary recommendations that have been issued by government agencies of different countries encourage health promotion and the prevention of diet-related, noncommunicable diseases (FAO and WHO 1992). The dietary guidelines adopted include the following principles:
- Adjust energy intake to meet energy expenditure in order to achieve and maintain desirable body weight.
- Avoid excessive fat intake and, especially, intake of saturated fat and cholesterol.
- Increase intake of complex carbohydrates and dietary fibre and limit sugar intake to moderate levels.
- Limit salt intake to a moderate level.
- Limit alcohol intake.
- Offer a variety of foods from all food groups.
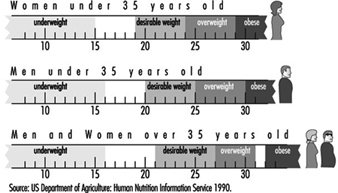
There is compelling scientific evidence to support these dietary recommendations. Not only is abnormal body weight a risk factor for many chronic diseases, but fat distribution is also important to health (Bray 1989). Android obesity, or excess fat in the abdomen, is a greater health risk than gynoid obesity, the presence of excess weight below the waist (i.e., in the hips and thighs). A waist-to-hip ratio close to or above one is associated with a greater risk of hypertension, hyperlipidaemia, diabetes and insulin resistance (Seidell 1992). Thus, both body mass index (BMI)—that is, body weight (kilograms) divided by height (meters) squared—and the waist-to-hip ratio are useful in assessing weight status and the need to lose weight. Figure 1 presents BMI classifications of underweight, desirable weight, overweight and obesity.
Figure 1. Body mass index (BMI) classifications.
Essentially everyone, even individuals who are at an ideal body weight, would benefit from nutrition guidance aimed at preventing the weight gain that typically occurs with ageing. An effective weight control program integrates nutrition, exercise, and behavior modification principles and techniques.
A diet that provides less than 30% of calories from fat, less than 10% of calories from saturated fat, and less than 300 milligrams of cholesterol daily is typically recommended to help maintain a desirable blood cholesterol level (i.e., <200 mg/dl) (National Institutes of Health 1993b). Saturated fat and cholesterol raise blood cholesterol levels. A diet relatively low in total fat facilitates achieving the saturated fat recommendation. A 2,000-calorie diet can include 67 grams of total fat and less than 22 grams of saturated fat per day. A diet low in total fat also facilitates reducing calories for weight management and may be implemented by including a variety of foods in the diet so that nutrient needs are met without exceeding calorie needs.
Diets high in complex carbohydrates (the sort of carbohydrate found in grains, legumes, vegetables, and, to some extent, fruits) are also high in many other nutrients (including B vitamins, vitamins A and C, zinc and iron) and low in fat. The recommendation to use sugar in moderation has been made because sugar, despite being a source of energy, has limited nutrient value. Thus, for persons with low calorie needs, sugar should be used sparingly. In contrast, sugar can be used as a source of calories, in moderation, in higher calorie (nutritionally adequate) diets. Although sugar promotes dental caries, it is less cariogenic when consumed with meals than when consumed in frequent between-meal snacks.
Because of the association between sodium intake and systolic hypertension, dietary salt and sodium are recommended only in moderation. A diet that provides not more than 2,400 milligrams of sodium daily is recommended for the prevention of hypertension (National Institutes of Health 1993a). A high-sodium diet also has been shown to promote calcium excretion and, thus, may contribute to the development of osteoporosis, a female-predominant risk (Anderson 1992). The major sources of sodium in the diet include processed foods and salt (or high-sodium condiments such as soy sauce) added to food during cooking or at the table.
If alcohol is consumed, it should be used in moderation. This is because excessive alcohol consumption may cause liver and pancreatic disease, hypertension and damage to the brain and heart. Further adverse consequences associated with heavy alcohol consumption include addiction, increased risk of accidents and impaired job performance.
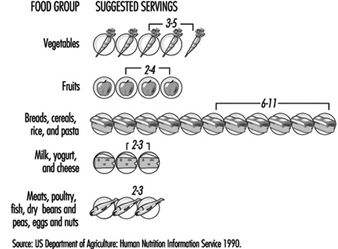
Another common recommendation is to consume a variety of foods from all food groups. More than 40 different nutrients are required for good health. Since no single food provides all nutrients, including a variety of foods facilitates achieving a nutritionally adequate diet. A typical food guide provides recommendations for the number of “servings” of foods from the different food groups (figure 2). The range of servings listed represents the minimum that should be consumed daily. As energy needs increase, the range should increase correspondingly.
Figure 2. Example of a good daily nutrition guide.
Other specific dietary recommendations have been made by different countries. Some countries recommend water fluoridation, breastfeeding, and iodine supplementation. Many also recommend that protein intake be adequate but that excess protein be avoided. Some have guidelines for the relative proportion of animal to vegetable protein in the diet. Others have emphasized vitamin C and calcium intake. Implicit to these country-specific recommendations is that they are targeted to the special needs identified for a particular area. Other nutritional issues that are important and relevant to individuals worldwide include those relating to calcium, hydration, and antioxidant vitamins and minerals.
An adequate calcium intake is important throughout life to build a strong skeleton and achieve a maximum peak bone mass (bone mass peaks between the ages of 18 and 30) and help retard age-associated bone mass loss that often leads to osteoporosis. At least 800 milligrams of calcium daily is recommended from age one year through old age. For adolescents, when bones are growing rapidly, 1,200 milligrams of calcium per day are recommended. Some authorities believe that young adults, postmenopausal women and men over 65 years of age need 1,500 milligrams of calcium per day and that the diet of all other adults should provide 1,000 milligrams. Pregnant and lactating women need 1,200 milligrams of calcium per day. Dairy products are rich sources of calcium. Low fat dairy products are recommended to control blood cholesterol levels.
Maintaining adequate hydration is essential for achieving maximal work performance. One serious consequence of dehydration is an inability to dissipate heat effectively, with a consequent increase in body temperature. Thirst usually is a good indicator of hydration status, except during heavy physical exertion. Workers always should respond to thirst and drink fluids liberally. Cool, dilute fluids replace water losses fastest. Laborers also should drink fluids liberally; for every 0.5 kilogram of weight lost per day due to exertion, one-half liter of water is recommended to replace the water lost via sweat.
Antioxidants have received a great deal of attention lately because of the growing evidence that suggests they may protect against the development of cancer, heart disease, cataracts and even slow the ageing process. The antioxidant vitamins are beta-carotene and vitamins A, E, and C. The mineral selenium also is an antioxidant. Antioxidants are thought to prevent the formation of harmful free radicals which destroy cell structures over time in a process that leads to the development of various diseases. The evidence to date suggests that antioxidants may protect against the development of cancer, heart disease and cataracts, although a causal relationship has not been established. Food sources of beta-carotene and vitamin A include green leafy vegetables, and red, orange and yellow fruits and vegetables. Grains and fish are significant sources of selenium. Citrus fruits are important sources of vitamin C, and vitamin E is found in sources of polyunsaturated fat, including nuts, seeds, vegetable oil and wheat germ.
The remarkable similarity in the dietary recommendations made by different countries underscores the consensus among nutritionists about the ideal diet for promoting health and well being. The challenge that lies before the nutrition community now is to implement these population-based dietary recommendations and assure proper nutrition globally. This will require not only providing a safe and adequate food supply to all persons everywhere, but also necessitates developing and implementing nutrition education programs worldwide that will teach virtually everyone the principles of a healthy diet.
Cultural and Ethnic Approaches to Foods and Diet
Effective nutrition education approaches must address cultural issues and ethnic food habits. Cultural sensitivity is important in planning nutrition intervention programs and in eliminating barriers to effective communication in individual counseling, as well. Given the current emphasis on cultural diversity, exposure to different cultures in the worksite, and a keen interest among individuals to learn about other cultures, pace-setting nutrition programs that embrace cultural differences should be well received.
Societies have vastly different beliefs about the prevention, cause, and treatment of disease. The value placed on good health and nutrition is highly variable. Helping people adopt healthy nutrition and lifestyle practices requires an understanding of their beliefs, culture and values (US Department of Health and Human Services 1990). Nutrition messages must be targeted to the specific practices of an ethnic population or group. Moreover, the intervention approach must be planned to address widely held beliefs about health and nutrition practices. For example, some cultures disapprove of alcohol whereas others consider it to be an essential part of the diet even when taken with meals eaten at the worksite. Thus, nutrition interventions must be specialized not only to meet the particular needs of a target group, but to embrace the values and beliefs that are unique to their culture.
Overweight
The key environmental factors that contribute to the development of overweight and obesity are principally caloric excess and lack of physical activity.
Overweight and obesity are most often classified on the basis of BMI, which is correlated with body composition (r = 0.7–0.8). Weight status classifications according to BMI for men and women less than 35 and greater than 35 years of age are presented in Figure 10. The health risks associated with overweight and obesity are clear. Data from a number of studies have shown a J-shape relationship between body weight and all-cause mortality. Although the mortality rate increases when BMI exceeds 25, there is a pronounced increase when BMI is greater than 30. Interestingly, underweight also increases risk of mortality, albeit not to the extent as does overweight. Whereas overweight and obese individuals are at higher risk of death due to cardiovascular disease, gallbladder disease and diabetes mellitus, underweight persons are at higher risk for the development of digestive and pulmonary diseases (Lew and Garfinkel 1979). The incidence of overweight and obesity in some developed countries may be as high as 25 to 30% of the population; it is even higher in certain ethnic groups and in groups of low socioeconomic status.
A low caloric diet that leads to a weight loss of 0.2 to 0.9 kilograms (0.5 to 2 pounds) per week is recommended for weight reduction. A low-fat diet (about 30% of calories from fat or lower) that is also high in fiber (15 grams per 1000 calories) is recommended to facilitate decreasing calories and providing bulk for satiety. A weight loss program should include both exercise and behavior modification. A slow, steady weight loss is recommended to successfully modify eating behaviors in order to maintain weight loss. Guidelines for a sound weight-reduction program appear in figure 3.
Figure 3. Guidelines for a sound weight-reduction programme.

A random-digit telephone survey of 60,589 adults across the United States revealed that approximately 38% of women and 24% of men were actively trying to lose weight. Reflecting the marketing efforts of what has become a veritable weight-reduction industry, the methods employed ranged from periodic fasting, participating in organized weight-reduction programs, often with commercially prepared foods and special supplements, and taking diet pills. Only half of those trying to lose weight reported using the recommended method of calorie restriction combined with exercise demonstrating the importance of worksite nutrition education programs (Serdula, Williamson et al. 1994).
Weight loss in overweight or obese persons beneficially affects various chronic disease risk factors (NIH 1993a). Weight loss leads to reductions in blood pressure, plasma lipids and lipoproteins (i.e., total cholesterol, low-density lipoprotein (LDL) cholesterol, and triglycerides) and increases high density lipoprotein (HDL) cholesterol, all of which are major risk factors for coronary heart disease (figure 4). Furthermore, blood glucose, insulin and glycosylated haemoglobin levels are favorably affected. With weight losses as modest as about four kilograms, even when some excess weight is regained, improvements in these parameters have been observed.
Figure 4. Major coronary heart-disease risk factors.

Weight control is essential for reducing chronic disease morbidity and mortality. This has formed the basis of the dietary recommendations of many groups worldwide to achieve and maintain a healthy body weight. These recommendations have been made mainly for developed countries where overweight and obesity are major public health concerns. While diet, exercise, and behavior modification are recommended for weight loss, the key to reducing the incidence of overweight and obesity is to implement effective prevention programs.
Underweight
Underweight (defined as a body weight of 15 to 20% or more below accepted weight standards) is a serious condition that results in a loss of energy and an increased susceptibility to injury and infection. It is caused by an insufficient food intake, excessive activity, malabsorption and poor utilization of food, wasting diseases or psychological stress. High-energy diets are recommended for a gradual, steady weight gain. A diet that provides 30 to 35% of calories from fat and an additional 500 to 1,000 calories per day is recommended. Underweight persons can be encouraged to eat calorie-dense meals and snacks at the worksite by offering them access to a wide variety of palatable, popular foods.
Special Diets
Special diets are prescribed for the treatment of certain diseases and conditions. In addition, dietary modifications should accompany preventive lifestyle and nutrition programs and should be implemented during various stages of the life cycle, such as during pregnancy and lactation. An important aspect of successfully implementing special diets is recognizing that a number of different strategies can be utilized to achieve the nutrient specifications of the special diet. Thus, individualizing diet plans to meet the unique needs of persons is essential for attaining long-term dietary adherence and, thereby, realizing the health benefits of the diet.
Low-fat, low-saturated fat, low-cholesterol diet
The recommended diets for the treatment of an elevated blood cholesterol level are the Step-One diet (<30% of calories from fat, 8 to 10% of calories from saturated fat and <300 milligrams of cholesterol) and the Step-Two diet (<30% of calories from fat, <7% of calories from saturated fat, and <200 milligrams of cholesterol) (NIH 1993b). These diets are designed to progressively reduce intake of saturated fat and cholesterol and to decrease total fat intake. The major sources of fat in the diet are meat, poultry; full-fat dairy products and fats and oils. In general, for most persons in developed countries, adherence to a Step-One diet requires reducing total fat and saturated fat by about 20 to 25%, whereas following a Step-Two diet requires decreasing total fat similarly but decreasing saturated fat by approximately 50%. A Step-One diet can be achieved rather easily by applying one or more fat reduction strategies to the diet, such as substituting lean meat, poultry and fish for higher-fat varieties, substituting low-fat and skim milk products for full-fat dairy products, using less fat in food preparation and adding less fat to food prior to consumption (e.g., butter, margarine or salad dressing) (Smith-Schneider, Sigman-Grant and Kris-Etherton 1992). A Step-Two diet requires more careful diet planning and the intensive nutrition education efforts of a qualified nutritionist.
Very low-fat diet
A diet that provides 20% or less of calories from fat is recommended by some nutritionists for the prevention of certain cancers that have been associated with diets high in fat (Henderson, Ross and Pike 1991). This diet is rich in fruits and vegetables, grains, cereals, legumes and skim milk dairy products. Red meat can be used sparingly, as can fats and oils. Foods are prepared with little or no added fat and are cooked by baking, steaming, boiling or poaching.
A diet that provides minimal amounts of saturated fat (3% of calories) and total fat (10% of calories), together with major lifestyle changes (smoking cessation, exercise and meditation) has been shown to result in the regression of atherosclerosis (Ornish et al. 1990). This particular diet requires major lifestyle changes (i.e., a change in habitual cuisine), including adopting a largely vegetarian diet and using meat, fish and poultry as a condiment, if at all, and emphasizing grains, legumes, fruits, vegetables, and skim milk dairy products. Adherence to this diet can require the purchase of special foods (fat-free products) while avoiding most commercially prepared foods. While this regimen is an option for some persons at high risk for cardiovascular disease, especially as an alternative to drug therapy, it requires a very high level of motivation and commitment.
Diet for workers with diabetes
An individually developed dietary prescription based on metabolic, nutrition, and lifestyle requirements is recommended (American Dietetic Association 1994). In general, dietary protein provides 10 to 20% of calories. Saturated fat should account for less than 10% of total caloric intake. The distribution of remaining energy from carbohydrate and fat varies according to the patient’s condition and reflects the specific glucose, lipid and weight outcomes chosen for him or her. For those who are at or close to ideal weight, 30% of calories from fat is recommended. For overweight persons, a reduction in total fat facilitates reducing calories, resulting in a corresponding weight loss. For persons who have an elevated triglyceride level, a diet higher in total fat, and, in particular, monounsaturated fat is recommended, together with close supervision; the higher-fat diet may perpetuate or aggravate obesity. The new model for the medical nutrition therapy for diabetes includes assessment of the individual’s metabolic and lifestyle parameters, an intervention plan and monitoring therapeutic outcomes.
Diet for pregnancy and lactation
Pregnancy and lactation represent periods when both energy and nutrient demands are high. For pregnancy, a diet should provide sufficient calories for adequate weight gain (National Research Council 1989). The calories and nutrients needed to maximally support pregnancy and lactation for as long as several years during multiple pregnancies and lengthy lactation periods can be obtained from a diet that includes the basic food groups. Other recommendations for both pregnant and lactating women include selecting a variety of foods from each food group, consuming regular meals and snacks, and including ample dietary fiber and fluid. Alcoholic beverages should be avoided or at least markedly restricted by pregnant and lactating women. Salt to taste is also recommended for pregnant women. An adequate diet during pregnancy and lactation is essential to assure normal fetal and infant growth and development and maternal health and well-being, and should be emphasized in worksite nutrition education programs and catering facilities.
Lactose Intolerance and Gluten Sensitivity
Many adults, especially those of certain ethnic groups, must restrict lactose in their diet due to a lactase deficiency. The major source of lactose in the diet is dairy products and foods prepared with them. It is important to note that the excipient in many medications is lactose, a circumstance that could pose problems to those who take a number of medications. For the small number of people who have a gluten sensitivity (coeliac disease), foods containing gluten must be eliminated from the diet. Sources of gluten in the diet include wheat, rye, barley and oats. Whereas many individuals with a lactose intolerance can tolerate small amounts of lactose, especially when eaten with foods that do not contain lactose, persons with a gluten sensitivity must avoid any food that contains gluten. Worksite catering facilities should have appropriate foods available if there are employees with these special conditions.
Summary
The worksite is an ideal setting for implementing nutrition programs aimed at teaching the principles of good nutrition and their application. There is a variety of programs that can be developed for the worksite. In addition to providing classes and nutrition education materials for all employees, special programs can be targeted to workers at high risk for different chronic diseases or for selected groups based on ethnic or demographic characteristics. Chronic disease risk reduction requires a long-term commitment by both workers and their employers. Effective worksite nutrition programs are beneficial in reducing the risk of chronic diseases in countries worldwide.