- You are here:
-
Home

-
Part XVI. Construction
-
Construction
- Major Sectors and Their Hazards
Contract Occupational Health Services in the United States
Setting
Employers in the United States have long provided medical care for injured workers through the use of private physicians, clinics, immediate-care facilities and hospital emergency departments. This care for the most part has been episodic and rarely coordinated, as only the largest corporations could provide in-house occupational health services.
A recent survey of 22,457 companies of fewer than 5,000 employees in a suburban area of Chicago found that 93% had less than 50 employees and only 1% employed more than 250 employees. Of this group, 52% utilized a specific provider for their work injuries, 24% did not utilize a specific provider and another 24% allowed the employee to seek his or her own provider. Only 1% of the companies utilized a medical director to provide care. These companies make up 99% of all employers in the surveyed area, representing over 524,000 employees (National Health Systems 1992).
Since the passage of the act which created the Occupational Safety and Health Administration in 1970, and with the accompanying changes in health care financing that have taken place since that time, the focus and priorities of care have changed. Insurance costs for workers’ compensation and group health care have risen from 14 to 26% annually from 1988 to 1991 (BNA 1991). In 1990, health care costs accounted for the single largest portion of the $53 billion spent in the United States for workers’ compensation benefits, and in 1995, medical benefits are expected to reach 50% of a total $100 billion price tag for workers’ compensation costs (Resnick 1992).
Premium costs vary by state because of differing workers’ compensation regulations. The Kiplinger Washington Letter of 9 September 1994 states, “In Montana, contractors pay an average of $35.29 in compensation insurance for every $100 of payroll. In Florida, it’s $21.99. Illinois, $19.48. Same coverage costs $5.55 in Indiana or $9.55 in South Carolina.” As the need for economical workers’ compensation care has evolved, employers are demanding more assistance from their health care providers.
The bulk of this medical care is rendered by independently owned medical facilities. Employers may contract for this care, develop a relationship with a provider or secure it on an as-needed basis. Most care is rendered on a fee-for-service basis, with the beginnings of capitation and direct contracting emerging during the later half of the 1990s.
Types of Services
Employers universally require that occupational health services include acute treatment of injuries and illnesses such as sprains, strains, back and eye injuries and lacerations. These make up the majority of acute cases seen in an occupational health programme.
Often, examinations are requested that are given pre-placement or after a job offer, to determine prospective employees’ ability to safely perform the work required without injury to themselves or others. These examinations must be evaluated consistently with US law as embodied in the Americans with Disabilities Act. This law forbids discrimination in hiring based on a disability that does not prevent an individual from performing the essential functions of the prospective job. The employer is further expected to make a “reasonable accommodation” to a disabled employee (EEOC and Department of Justice 1991).
Though required by law only for certain job categories, substance abuse testing for drugs and/or alcohol is now performed by 98% of the Fortune 200 companies in the United States. These tests may include measurements of urine, blood and breath for levels of illicit drugs or alcohol (BNA 1994).
In addition, an employer may require specialized services such as OSHA-mandated medical surveillance tests—for instance, respirator fitness examinations, based on a worker’s physical capacity and pulmonary function, assessing the worker’s ability to wear a respirator with safety; asbestos examinations and other chemical exposure tests, tailored to assess an individual’s health status with respect to possible exposure and long-term effects of a given agent on the person’s overall health.
In order to assess the health status of key employees, some companies contract for physical examinations for their executives. These examinations are generally preventive in nature and offer extensive health assessment, including laboratory testing, x rays, cardiac stress testing, cancer screening and lifestyle counselling. The frequency of these examinations is often based on age rather than type of work.
Periodic fitness examinations are often contracted for by municipalities to assess the health status of fire and police officers, who are generally tested to measure their physical ability to handle physically stressful situations and to determine whether exposures have occurred in the workplace.
An employer may also contract for rehabilitative services, including physical therapy, work hardening, workplace ergonomic assessments as well as vocational and occupational therapies.
More recently, as a benefit to employees and in an effort to decrease health care costs, employers are contracting for wellness programmes. These prevention-oriented screenings and educational programmes seek to assess health so that appropriate interventions might be offered to alter lifestyles that contribute to disease. Programmes include cholesterol screening, health risk appraisals, smoking cessation, stress management and nutrition education.
Programmes are being developed in all areas of health care to meet the needs of employees. The employee assistance program (EAP) is another recent programme developed to provide counselling and referral services to employees with substance abuse, emotional, family and/or financial problems which employers have determined have an effect on the employee’s ability to be productive.
A service that is relatively new to occupational health is case management. This service, usually provided by nurses or clerical personnel supervised by nurses, has effectively reduced costs while ensuring appropriate quality care for the injured worker. Insurance companies have long provided management of claims costs (the dollars spent on workers’ compensation cases) at a point when the injured worker has been off work for a specified length of time or when a certain dollar amount has been reached. Case management is a more proactive and concurrent process which may be applied from the first day of the injury. Case managers direct the patient to the appropriate level of care, interact with the treating physician to determine what types of modified work the patient is medically capable of performing, and work with the employer to ensure that the patient is performing work which will not worsen the injury. The case manager’s focus is to return the employee to a minimum of modified duty as quickly as possible as well as to identify good quality physicians whose results will best benefit the patient.
The Providers
Services are available through a variety of providers with varying degrees of expertise. The private physician’s office may offer pre-placement examinations and substance abuse testing as well as follow-up of acute injuries. The physician’s office generally requires appointments and has limited hours of service. If the capabilities exist, the private physician may also offer executive examinations or may refer the patient to a nearby hospital for extensive laboratory, x-ray and stress testing.
The industrial clinic generally offers acute care of injuries (including follow-up care), pre-placement examinations and substance abuse testing. They often have x-ray and laboratory capabilities and may have physicians who have experience in assessing the workplace. Again, their hours are generally limited to business hours so that employers with second- and third-shift operations may need to utilize an emergency department during evenings and weekends. The industrial clinic rarely treats the private patient, and it is generally perceived as the “company doctor”, since arrangements are usually made to bill the employer or the company’s insurance carrier directly.
Immediate care facilities are another alternative delivery site. These facilities are walk-in providers of general medical care and require no appointments. These facilities generally are equipped with x-ray and laboratory capabilities and physicians experienced in emergency medicine, internal medicine or family practice. The type of client ranges from the paediatrics patient to the adult with a sore throat. In addition to acute injury care and minor follow-up of injured employees, these facilities may perform pre-placement physicals and substance abuse testing. Those facilities which have developed an occupational health component often provide periodic exams and OSHA-mandated screenings, and may have contractual relationships with additional providers for services that they do not themselves offer.
The hospital emergency room is often the site of choice for treatment of acute injuries and has generally been capable of little else in terms of occupational health services. This has been the case although the hospital has had the resources to provide most of the required services with the exception of those offered by physicians with expertise in occupational medicine. Yet an emergency department alone lacks the managed care and return-to-work expertise now being demanded by industry.
Hospital-Based Programmes
Hospital administrations have become cognizant that they not only have the resources and technology available but that workers’ compensation was one of the last “insurance” programmes which would pay fees for service, thereby boosting revenues hurt by discounting arrangements that were made with managed care insurance companies such as HMOs and PPOs. These managed care companies, as well as the federally and state funded Medicare and Medicaid programmes for general health care, have demanded shorter lengths of stay and have imposed a payment system based on “diagnosis-related grouping” (DRG). These schemes have forced hospitals to lower costs by seeking improved coordination of care and new revenue-producing products. Fears arose that costs would be shifted from group health managed care to workers’ compensation; in many cases these fears were well-founded, with costs for treating an injured back under workers’ compensation two to three times the cost under group health plans. A 1990 Minnesota Department of Labour and Industry study reported that costs of treatment for sprains and strains were 1.95 times greater, and those for back injuries 2.3 times greater, under workers’ compensation than under group health insurance plans (Zaldman 1990).
Several different hospital delivery models have evolved. These include the hospital-owned clinic (either on campus or off), the emergency department, the “fast-track” (non-acute emergency department), and administratively managed occupational health services. The American Hospital Association reported that Ryan Associates and Occupational Health Research had studied 119 occupational health programmes in the United States (Newkirk 1993). They found that:
- 25.2% were hospital emergency department based
- 24.4% were hospital non-emergency department based
- 28.6% were hospital free-standing clinics
- 10.9% were independently owned free-standing clinics
- 10.9% were other types of programmes.
All of these programmes assessed costs on a fee-for-service basis and offered a variety of services which, in addition to treatment of acutely injured workers, included pre-placement examinations, drug and alcohol testing, rehabilitation, workplace consulting, OSHA-mandated medical surveillance, executive physicals and wellness programmes. In addition, some offered employee assistance programmes, onsite nursing, CPR, first aid and case management.
More often today hospital occupational health programmes are adding a nursing model of case management. Within such a model incorporating integrated medical management, total workers’ compensation costs can be lowered 50%, which is a significant incentive for the employer to utilize providers that afford this service (Tweed 1994). These cost reductions are generated by a strong focus on the need for early return to work and for consultation on modified work programmes. The nurses work with the specialists to help define medically acceptable work that an injured employee can perform safely and with restrictions.
In most states, US workers receive two-thirds of their salary while receiving temporary workers’ compensation for total disability. When they return to modified work, they continue to provide a service for their employers and maintain their self-esteem through work. Workers who have been off work six or more weeks frequently never return to their full employment and are often forced to perform lower-paying and less skilled jobs.
The ultimate goal of a hospital-based occupational health programme is to allow patients access to the hospital for work injury treatment and to continue with the hospital as their primary provider of all health care services. As the United States moves to a capitated health care system, the number of covered lives a hospital serves becomes the prime indicator of success.
Under this capitated form of health care financing, employers pay a per capita rate to providers for all health care services that their employees and their dependants may need. If the individuals covered under such a plan stay healthy, then the provider is able to profit. If the covered lives are high utilizers of services, the provider may not earn enough revenue from premiums to cover the costs of care and may therefore lose money. Several states in the United States are moving toward capitation for group health insurance and a few are piloting 24-hour coverage for all health care, including workers’ compensation medical benefits. Hospitals will no longer judge success on patient census but on a ratio of covered lives to costs.
Comprehensive hospital-based occupational health programmes are designed to fill a need for a high-quality comprehensive occupational medicine programme for the industrial and corporate community. The design is based on the premise that injury care and pre-placement physicals are important but alone do not constitute an occupational medicine programme. A hospital serving many companies can afford an occupational medicine physician to oversee medical services, and therefore, a broader occupational focus can be gained, allowing for toxicology consultations, worksite evaluations and OSHA-mandated examin-ations for such contaminants as asbestos or lead and for equipment such as respirators, in addition to the usual services of work injury treatment, physical examinations and drug screening. Hospitals also have the resources necessary to provide a compute-rized database and case management system.
By providing employers with a single full service centre for their employees’ health care needs, the occupational health programme can better ensure that the employee receives quality, compassionate health care in the most appropriate setting, at the same time reducing costs to the employer. Occupational health providers can monitor trends within a company or an industry and make recommendations to reduce workplace accidents and improve safety.
A comprehensive hospital-based occupational health programme allows the small employer to share the services of a corporate medical department. Such a programme provides prevention and wellness as well as acute care service and permits a sharper focus on promotion of health for US workers and their families.
Corporate Occupational Health Services in the United States: Services Provided Internally
Industrial medical programmes vary in both content and structure. It is a common conception that industrial medical programmes are supported only by large corporations and are comprehensive enough to evaluate all workers for all possible adverse effects. However, the programmes implemented by industries vary considerably in their scope. Some programmes offer only pre-placement screening, while others offer total medical surveillance, health promotion and other special services. In addition, the structures of programmes differ from one another, as do the members of the safety and health teams. Some programmes contract with an off-site physician to perform medical services, while others have a health unit at the site staffed by physicians and nursing personnel and backed by a staff of industrial hygienists, engineers, toxicologists and epidemiologists. The duties and responsibility of these members of the safety and health team will vary according to the industry and the risk involved.
Motivation for Industrial Medical Programmes
The medical monitoring of workers is motivated by multiple factors. First, there is the concern for the general safety and health of the employee. Second, a monetary benefit results from a surveillance effort through increased productivity of the employee and reduced medical care costs. Third, compliance with the Occupational Safety and Health Act (OSHA), with equal employment opportunity requirements (EEO), the Americans with Disabilities Act (ADA) and other statutory guidelines is mandatory. Finally, there is the spectre of civil and criminal litigation if adequate programmes are not established or are found to be inadequate (McCunney 1995; Bunn 1985).
Types of Occupational Health Servicesand Programmes
Occupational health services are determined through a needs assessment. Factors that affect which type of occupational health service is to be utilized include the potential risks of normal operations, the demographics of the workforce and management’s interest in occupational health. Health services are dependent on the type of industry, the physical, chemical or biological hazards present, and the methods used to prevent exposure, as well as government and industry standards, regulations and rulings.
Important general health services tasks include the following:
- evaluation of employees’ ability to perform their assigned duties in a safe manner (via pre-placement evaluations)
- recognition of early symptoms and signs of work-related health effects and appropriate intervention (medical surveillance examinations can reveal these)
- provision of treatment and rehabilitation for occupational injuries and illnesses and non-occupational disorders that affect work performance (work-related injuries)
- promotion and maintenance of employees’ health (wellness)
- evaluation of a person’s ability to work in light of a chronic medical disorder (an independent medical examination is required in such a case)
- supervision of policies and programmes related to worksite health and safety.
Location of Health Services Facilities
Onsite facilities
Delivery of occupational health services today is increasingly provided through contractors and local medical facilities. However, onsite services formed by employers were the traditional approach taken by industry. In settings with a substantial number of employees or certain health risks, onsite services are cost-effective and provide high-quality services. The extent of these programmes varies considerably, ranging from part-time nursing support to a fully-staffed medical facility with full-time physicians.
The need for onsite medical service is usually determined by the nature of the company’s business and the potential health hazards present in the workplace. For example, a company that uses benzene as a raw material or ingredient in its manufacturing process will probably need a medical surveillance programme. In addition, many other chemicals handled or produced by the same plant may be toxic. In these circumstances, it may be economically feasible as well as medically advisable to provide onsite medical services. Some onsite services provide occupa-tional nursing support during daytime working hours and may also cover second and third shifts or weekends.
Onsite services should be performed in plant areas compatible with the practice of medicine. The medical facility should be centrally located to be accessible to all employees. Heating and cooling needs should be considered to permit the most economical use of the facility. A rule of thumb that has been used in allocating floor space to an in-house medical unit is one square foot per employee for units servicing up to 1,000 employees; this figure should probably include a minimum of 300 square feet. The cost of space and several relevant design considerations have been described by specialists (McCunney 1995; Felton 1976).
For some manufacturing facilities located in rural or otherwise remote areas, services may usefully be provided in a mobile van. If such an installation is made available, the following recommendations may be made:
- Assistance should be furnished to companies whose in-house medical services are not fully equipped to cope with medical surveillance programmes that require the use of special equipment, such as audiometers, spirometers or x-ray machines.
- Medical surveillance programmes should be made available in remote geographical areas, especially to ensure uniformity in data collected for epidemiology studies. For example, to enhance the scientific accuracy of a study of occupational lung disorders, a similar spirometer should be used and the preparation of chest films should be performed according to appropriate international standards, such as those of the International Labour Organization (ILO).
- Data from different sites should be coordinated for entry into a computer software programme.
A company that relies on a mobile van service, however, will still require a physician to conduct pre-placement examinations and to assure the quality of the services provided by the mobile van company.
Services Most Commonly Performedin the In-house Facility
An onsite assessment is essential to determine the type of health services appropriate for a facility. The most common services provided in the occupational health setting are pre-placement evaluations, assessment of work-related injury or illness and medical surveillance examinations.
Pre-placement evaluations
The pre-placement examination is performed after a person has been given a conditional offer of a job. The ADA uses pre-employment to mean that the person is to be hired if he or she passes the physical examination.
The pre-placement examination should be performed with attention to the job duties, including physical and cognitive requirements (for safety sensitivity) and potential exposure to hazardous materials. The content of the examination depends on the job and the worksite assessment. For example, jobs that require use of personal protective equipment, such as a respirator, often include a pulmonary function study (breathing test) as part of the pre-placement examination. Those involved in the US Department of Transportation (DOT) activities usually require urinary drug testing. To avoid errors in either the content or the context of the examination, it is advisable to develop standard protocols to which the company and the examining physician agree.
After the examination, the physician provides a written opinion about the person’s suitability for performing the job without health or safety risk to self or others. Under usual circumstances, medical information is not to be divulged on this form, merely fitness for duty. This form of communication can be a standard form that should then be placed in the employee’s file. Specific medical records, however, remain at the health facility and are maintained only by a physician or nurse.
Work-related injuries and illnesses
Prompt, quality medical care is essential for the employee sustaining a work-related injury or occupational illness. The medical unit or contract physician should treat employees who are injured at work or who experience work-related symptoms. The company’s medical service has an important role to play in the management of workers’ compensation costs, especially in performing return-to-work assessments following absence due to an illness or injury. A major function of the medical professional is the coordination of rehabilitation services of such absentees to insure a smooth return to work. The most effective rehabilitation programmes make use of modified-duty or alternative assignments.
An important task of the company’s medical adviser is to determine the relationship between exposure to hazardous agents and illness, injury or impairment. In some states, the employee may choose his or her attending physician, whereas in other states the employer may direct or at least suggest evaluation by a specific physician or health care facility. The employer usually has the right to specify a physician to conduct a “second opinion” examination, especially in the context of a protracted recovery or serious medical disorder.
The nurse or physician advises management on the recordability of occupational injuries and illnesses in accordance with OSHA record-keeping requirements, and needs to be familiar with both OSHA and Bureau of Labor Statistics (BLS) guidelines. Management must assure that the health care provider is thoroughly familiar with these guidelines.
Medical surveillance examinations
Medical surveillance examinations are required by some OSHA standards for exposure to some substances (asbestos, lead and so on) and are recommended as being in accordance with good medical practice for exposure to others, such as solvents, metals and dusts such as silica. Employers must make these examinations, when required by OSHA standards, available at no cost to employees. Although the employee may decline to participate in an examination, the employer may specify that the examination is a condition of employment.
The purpose of medical surveillance is to prevent work-related illnesses through early recognition of problems, such as abnormal laboratory results that may be associated with the early stages of a disease. The employee is then re-evaluated at subsequent intervals. Consistency in the medical follow-up of abnormalities uncovered during medical surveillance examinations is essential. Although management should be apprised of any medical disorders related to work, medical conditions not arising from the workplace should remain confidential and be treated by the family physician. In all cases, employees should be informed of their results (McCunney 1995; Bunn 1985, 1995; Felton 1976).
Management Consultation
Although the occupational health physician and nurse are most readily recognized through their hands-on medical skills, they can also offer significant medical advice to any business. The health professional can develop procedures and practices for medical programmes including health promotion, substance abuse detection and training, and medical record-keeping.
For facilities with an in-house medical programme, a policy for the management of medical waste handling and related activities is necessary in accordance with the OSHA blood-borne pathogen standard. Training with respect to certain OSHA standards, such as the Hazard Communication Standard, the OSHA Standard on Access to Exposure and Medical Records, and OSHA record-keeping requirements, is an essential ingredient to a well-managed programme.
Emergency response procedures should be developed for any facility that is at increased risk of natural disaster or that handles, uses or manufactures potentially hazardous materials, in accordance with the Superfund Act Reauthorization Amendment (SARA). Principles of medical emergency response and disaster management should, with the assistance of the company’s physician, be incorporated in any site emergency response plan. Since the emergency procedures will differ depending on the hazard, the physician and nurse should be prepared to handle both physical hazards, such as those that occur in a radiation accident, and chemical hazards.
Health Promotion
Health promotion and wellness programmes to educate people on the adverse health effects of certain lifestyles (such as cigarette smoking, poor diet and lack of exercise) are becoming more common in industry. Although not essential to an occupational health programme, these services can be valuable to employees.
The incorporation of wellness and health promotion plans in the medical programme is recommended whenever feasible. The objectives of such a programme are a health-conscious, productive workforce. Health care costs can be reduced as a result of health promotion initiatives.
Substance Abuse Detection Programmes
Within the past few years, especially since the US Department of Transportation (DOT) Ruling on Drug Testing (1988), many organizations have developed drug testing programmes. In the chemical and other manufacturing industries, the most common type of urinary drug test is performed at the pre-placement evaluation. The DOT rulings on drug testing for interstate trucking, gas transmission operations (pipelines), and the railroad, coast guard and aviation industries are considerably broader and include periodic testing “for cause,” that is, for reasons of suspected substance abuse. Physicians are involved in drug screening programmes by reviewing results to assure that reasons other than illicit drug use are eliminated for individuals with positive tests. They must ensure the integrity of the testing process and confirm any positive test with the employee before releasing the results to management. An employee assistance programme and uniform company policy are essential.
Medical Records
Medical records are confidential documents which should be maintained by an occupational physician or nurse and stored in such a manner so as to protect their confidentiality. Some records, such as a letter indicating a person’s fitness for respirator use, should be kept onsite in the event of a regulatory audit. Specific medical test results, however, should be excluded from such files. Access to such records should be limited to the health professional, the employee and other persons designated by the employee. In some instances, such as the filing of a workers’ compensation claim, confidentiality is waived. The OSHA Access to Employee Exposure and Medical Records standard (29 CFR 1910.120) requires that employees be informed annually of their right of access to their medical records and of the location of such records.
Confidentiality of medical records must be preserved in accordance with legal, ethical and regulatory guidelines. Employees should be informed when medical information will be released to management. Ideally, an employee will be asked to sign a medical form that authorizes release of certain medical information, including laboratory tests or diagnostic material.
The first item in the American College of Occupational and Environmental Medicine Code of Ethics requires that “Physicians should accord the highest priority to the health and safety of individuals in both the workplace and the environment.” In the practice of occupational medicine, both employer and employee benefit if physicians are impartial and objective and apply sound medical, scientific and humanitarian principles.
International Programmes
In international occupational and environmental medicine, physicians working for US industries will have not only the traditional responsibilities of occupational and environmental physicians but will also have significant clinical management responsibilities. The responsibility of the medical department will include the clinical care of the employees and commonly the spouses and children of the employees. Servants, extended family and the community are often included in the clinical responsibilities. In addition, the occupational physician will also have responsibilities for occupational programmes related to workplace exposures and risks. Medical surveillance programmes, as well as pre-employment and periodic examinations are critical programme components.
Designing appropriate health promotion and prevention programmes is also a major responsibility. In the international arena, these prevention programmes will include issues in addition to those lifestyle issues commonly considered in the United States or Western Europe. Infectious diseases require a systematic approach to needed vaccination and chemoprophylaxis. Educational programmes for prevention must include attention to food-, water- and blood-borne pathogens and to general sanitation. Accident prevention program-mes must be considered in view of the high risk for traffic-related deaths in many developing countries. Special issues such as evacuation and emergency care must be given detailed scrutiny and appropriate programmes implemented. Environmental exposure to chemical, biological and physical hazards is often increased in developing countries. Environmental prevention programmes are based on multi-staged education plans with indicated biological testing. The clinical programmes to be developed internationally may include inpatient, outpatient, emergency and intensive care management of expatriates and national employees.
An ancillary programme for international occupational physicians is travel medicine. The safety of short-term rotational travellers or foreign residents requires special knowledge of the indicated vaccinations and other preventive measures on a global basis. In addition to recommended vaccinations, a knowledge of medical requirements for visas is imperative. Many countries require serologic testing or chest x rays, and some countries may take into account any significant medical condition in the decision to issue a visa for employment or as a residency requirement.
Employee assistance and marine and aviation programmes are also commonly included within the international occupational physician’s responsibilities. Emergency planning and the provision of appropriate medications and training in their use are challenging issues for sea and air vessels. Psychological support both of expatriate and national employees is often desirable and/or necessary. Employee assistance programmes may be extended to expatriates and special support given to family members. Drug and alcohol programmes should be considered within the social context of the given country (Bunn 1995).
Conclusion
In conclusion, the scope and organization of corporate occupational health programmes may vary widely. However, if appropriately discussed and implemented, these programmes are cost-effective, protect the company from legal liabilities and promote the occupational and general health of the workforce.
Governmental Occupational Health Agencies in the United States
The Occupational Safety and Health Administration(OSHA)
Purpose and organization
OSHA was created to encourage employers and workers to reduce workplace hazards and to implement effective safety and health programmes. This is accomplished by setting and enforcing standards, monitoring the performance of state OSHA programmes, requiring employers to maintain records of work-related injuries and illnesses, providing safety and health training for employers and employees and investigating complaints of workers who claim they have been discriminated against for reporting safety or health hazards.
OSHA is directed by an Assistant Secretary of Labor for Occupational Safety and Health, who reports to the Secretary of Labor. The OSHA headquarters is in Washington, DC, with ten regional offices and about 85 area offices. About half of the states administer their own state safety and health programmes, with federal OSHA responsible for enforcement in states without approved state programmes. The Occupational Safety and Health Act also requires that each federal government agency maintain a safety and health programme consistent with OSHA standards.
Programme and services
Standards form the basis of OSHA’s enforcement programme, setting out the requirements employers must meet to be in compliance. Proposed standards are published in the Federal Register with opportunities for public comment and hearings. Final standards are also published in the Federal Register and may be challenged in a US Court of Appeals.
In areas where OSHA has not established a standard, employers are required to follow the Occupational Safety and Health Act’s general duty clause, which states that each employer shall furnish “a place of employment which is free from recognized hazards that are causing or are likely to cause death or serious physical harm to his employees”.
OSHA has the right to enter the workplace to determine whether an employer is in compliance with requirements of the Act. OSHA places highest priority on investigating imminent danger situations, catastrophes and fatal accidents, employee complaints and scheduled inspections in highly hazardous industries.
If the employer refuses entry, the inspector can be required to obtain a search warrant from a US district judge or US magistrate. Both worker and employer representatives have a right to accompany OSHA inspectors on their plant visits. The inspector issues citations and proposed penalties for any violations found during the inspection and sets a deadline for correcting them.
The employer may contest the citation to the Occupational Safety and Health Review Commission, an independent body established to hear challenges to OSHA citations and proposed fines. The employer may also appeal an unfavourable Review Commission decision to a federal court.
Consultation assistance is available at no cost to employers who agree to correct any serious hazards identified by the consultant. Assistance can be given in developing safety and health programmes and training workers. This service, which is targeted toward smaller employers, is largely funded by OSHA and provided by state government agencies or universities.
OSHA has a voluntary protection programme (VPP), which exempts workplaces from scheduled inspections if they meet certain criteria and agree to develop their own comprehensive safety and health programmes. Such workplaces must have lower than average accident rates and written safety programmes, make injury and exposure records available to OSHA and notify workers about their rights.
Resources
In 1995, the OSHA budget was $312 million, with about 2,300 employees. These resources are intended to provide coverage for more than 90 million workers throughout the United States.
State OSHA Programmes
Purpose and organization
The Occupational Safety and Health Act of 1970 gave state governments the option of regulating workplace safety and health.
States conduct their own programmes for setting and enforcing safety and health standards by submitting a state plan to OSHA for approval. The state plan details how the state proposes to set and enforce standards that are “at least as effective” as OSHA’s and to assume jurisdiction over state, city and other (non-federal) public employees whom OSHA itself does not otherwise cover. In these states, the federal government gives up direct regulatory responsibilities, and instead provides partial funding to the state programmes, and monitors the state activities for conformance with the national standards.
Programme and services
Approximately half of the states have chosen to administer their own programmes. Two other states, New York and Connecticut, have elected to keep the federal jurisdiction in their states, but to add a state workplace safety and health system that provides protection for public employees.
State-run OSHA programmes allow states to tailor resources and target regulatory efforts to match special needs in their states. For example, logging is done differently in the eastern and western United States. North Carolina, which runs its own OSHA programme, was able to target its logging regulations, outreach, training and enforcement programmes to address the safety and health needs of loggers in that state.
Washington State, which has a large agricultural economic base, developed agriculture safety requirements that exceed the mandated national minimums and translated safety information into Spanish to meet the needs of Spanish-speaking farm workers.
In addition to developing programmes that meet their special needs, states are able to develop programmes and enact regulations for which there might not be sufficient support at the federal level. California, Utah, Vermont and Washington have restrictions on workplace exposure to environmental tobacco smoke; Washington State and Oregon require that each employer develop worksite-specific injury and illness prevention plans; Utah’s standard for oil and gas drilling and the manufacture of explosives exceeds federal OSHA standards.
State programmes are permitted to conduct consultation programmes that provide free assistance to employers in identifying and correcting workplace hazards. These consultations, which are made only at the request of the employer, are kept separate from enforcement programmes.
Resources
In 1993, state-administered programmes had a total of about 1,170 enforcement personnel, according to the Occupational Safety and Health State Plan Association. In addition, they had about 300 safety and health consultants and nearly 60 training and education coordinators. The majority of these programmes are in state labour departments.
Mine Safety and Health Administration (MSHA)
Purpose and organization
The Mine Safety and Health Administration (MSHA) sets and enforces standards to reduce injuries, illnesses and deaths in mines and mineral processing operations regardless of size, number of employees or method of extraction. MSHA is required to inspect every underground mine at least four times a year and every surface mine at least twice a year.
In addition to enforcement programmes, the Mine Safety and Health Act requires that the agency establish regulations on safety and health training for miners, upgrade and strengthen mine safety and health laws and encourage the participation of miners and their representatives in safety activities. MSHA also works with the mine operators to solve safety and health problems through education and training programmes and the development of engineering controls to reduce injuries.
Like OSHA, MSHA is directed by an Assistant Secretary of Labor. The coal mine safety and health activities are administered through ten district offices in the coal mining regions. The metal and non-metal mine safety and health activities are administered through six district offices in the mining areas of the country.
A number of staff offices that assist in administering the agency’s responsibilities are located at the headquarters in Arlington, Virginia. These include the Office of Standards, Regulations and Variances; the Office of Assessments; the Technical Support directorate; and the Office of Program Policy. In addition, the Educational Policy and Development Office oversees the agency’s training programme at the National Mine Health and Safety Academy in Beckley, West Virginia, which is the world’s largest institution devoted entirely to mine safety and health training.
Programme and services
Mining deaths and injuries have declined significantly during the last hundred years. From 1880 to 1910, thousands of coal miners were killed, with 3,242 dying in 1907 alone. Large numbers of miners were also killed in other sorts of mines. The average number of mining deaths has declined over the years to less than 100 per year today.
MSHA enforces the mine act provisions requiring mine operators to have an approved safety and health training plan which provides for 40 hours of basic training for new underground miners, 24 hours of training for new surface miners, 8 hours of annual refresher training for all miners and safety-related task training for miners assigned to new jobs. The National Mine Health and Safety Academy offers a wide variety of safety and health courses. MSHA provides special training programmes for managers and workers at small mining operations. MSHA training materials, including videotapes, films, publications and technical materials are available at the Academy and at district offices.
Resources
In 1995, MSHA had a budget of about $200 million and about 2,500 employees. These resources were responsible for ensuring the health and safety of about 113,000 coal miners and 197,000 miners in metal and non-metal mines.
The National Institute for Occupational Safety and Health (NIOSH)
Purpose and organization
The National Institute for Occupational Safety and Health (NIOSH) is the federal agency responsible for conducting research on occupational injuries and illnesses and transmitting recommended standards to OSHA. NIOSH funds education programmes for occupational safety and health professionals through Educational Resource Centres (ERCs) and training projects at universities throughout the United States. Under the Federal Mine Safety and Health Act of 1977, NIOSH also conducts research and health hazard evaluations, and recommends mine health standards to the Mine Safety and Health Administration.
The Director of NIOSH reports to the Director of the Centers for Disease Control and Prevention within the Department of Health and Human Services. The NIOSH headquarters is in Washington, DC, with administrative offices in Atlanta, Georgia, and laboratories in Cincinnati, Ohio, and Morgantown, West Virginia.
Programme and services
NIOSH research is conducted both in the field and in the laboratory. Surveillance programmes identify the occurrence of work-related injury and disease. These include targeted data collection directed toward specific conditions, such as high blood lead levels in adults or injuries among adolescent workers. NIOSH also links data collected by states and other federal agencies to make it increasingly practicable to obtain a national picture of the effects of occupational hazards.
Field research is conducted at workplaces throughout the United States. These studies make it possible to identify hazards, evaluate the extent of exposures and determine the effectiveness of preventive measures. The right of entry into the workplace is essential to the ability of the Institute to conduct this research. This field research results in articles in the scientific literature as well as recommendations for preventing hazards at specific worksites.
Working with state health departments, NIOSH investigates on-the-job fatalities from specific causes, including electrocutions, falls, machine-related incidents and confined space entry accidents. NIOSH has a special programme to assist small businesses by developing inexpensive and effective technologies to control hazardous exposures at the source.
NIOSH conducts laboratory research to study workplace hazards under controlled conditions. This research assists NIOSH in determining the causes and mechanisms of workplace illnesses and injuries, developing tools for measuring and monitoring exposures, and developing and evaluating control technology and personal protective equipment.
About 17% of the NIOSH budget is devoted to funding service activities. Many of these service activities are also research-based, such as the health hazard evaluation programme. NIOSH conducts hundreds of health hazard evaluations each year when requested by employers, workers or federal and state agencies. After evaluating the worksite, NIOSH provides workers and employers with recommendations to reduce exposures.
NIOSH also responds to requests for information through a toll-free telephone number. Through this number, callers can obtain occupational safety and health information, request a health hazard evaluation or obtain a NIOSH publication. The NIOSH Home Page on the World Wide Web is also a good source of information about NIOSH.
NIOSH maintains a number of databases, including NIOSHTIC, a bibliographic database of occupational safety and health literature, and the Registry of Toxic Effects of Chemical Substances (RTECS), which is a compendium of toxicological data extracted from the scientific literature which fulfils the NIOSH mandate to “list all known toxic substances and concentrations at which toxicity is known to occur”.
NIOSH also tests respirators and certifies that they meet established national standards. This assists employers and workers in choosing the most appropriate respirator for specific hazardous environments.
NIOSH funds programmes at universities throughout the United States to train occupational medicine physicians, occupational health nurses, industrial hygienists and safety professionals. NIOSH also funds programmes to introduce safety and health into business, engineering and vocational schools. These programmes, which are either multidisciplinary ERCs or single-discipline project training grants, have made a significant contribution to the development of occupational health as a discipline and to meeting the need for qualified safety and health professionals.
Resources
NIOSH had about 900 employees and a budget of $133 million in 1995. NIOSH is the only federal agency with statutory responsibility to conduct occupational safety and health research and professional training.
The Future of Occupational Safetyand Health Programmes
The future of these federal occupational safety and health programmes in the United States is very much in doubt in the anti-regulatory climate of the 1990s. There continue to be serious proposals from Congress that would drastically change how these programmes operate.
One proposal would require the regulatory agencies to focus more on education and consultation and less on standards setting and enforcement. Another would set up requirements for complex cost benefit analyses that must be conducted before standards could be established. NIOSH has been threatened with abolition or merger with OSHA. And all these agencies have been targeted for budget reductions.
If enacted, these proposals would greatly decrease the federal role in conducting research and in setting and enforcing uniform occupational safety and health standards throughout the United States.
Occupational Health Services in the United States: Introduction
History
Occupational health services in the United States have always been divided in function and control. The extent to which government at any level should make rules affecting working conditions has been a matter of continuing controversy. Furthermore, there has been an uneasy tension between the state and federal governments about which should take primary responsibility for preventive services based primarily upon laws governing workplace safety and health. Monetary compensation for workplace injury and illness has primarily been the responsibility of private insurance companies, and safety and health education, with only recent changes, has been left largely to unions and corporations.
It was at the state level that the first governmental effort to regulate working conditions took place. Occupational safety and health laws began to be enacted by states in the 1800s when increasing levels of industrial production began to be accompanied by high accident rates. Pennsylvania enacted the first coal mine inspection act in 1869, and Massachusetts was the first state to pass a factory inspection law in 1877.
By 1900 the more industrialized states had some laws in place regulating some workplace hazards. Early in the twentieth century, New York and Wisconsin led the nation in developing more comprehensive occupational safety and health programmes.
Most states adopted worker’s compensation laws mandating private no-fault insurance between 1910 and 1920. A few states, such as Washington, provide a state-run system allowing the collection of data and the targeting of research goals. The compensation laws varied widely from state to state, were generally not well enforced, and omitted many workers, such as agricultural workers, from coverage. Only railway, longshore and harbour workers, and federal employees have national worker’s compensation systems.
In the first decades of the twentieth century, the federal role in occupational safety and health was largely restricted to research and consultation. In 1910 the Federal Bureau of Mines was established in the Department of the Interior to investigate accidents; consult with industry; conduct safety and production research; and provide training in accident prevention, first aid and mine rescue. The Office of Industrial Hygiene and Sanitation was created in the Public Health Service in 1914 to conduct research and assist states in solving occupational safety and health problems. It was located in Pittsburgh because of its close association with the Bureau of Mines and its focus on injuries and illnesses in the mining and steel industries.
In 1913 a separate Department of Labor was established; the Bureau of Labor Standards and the Interdepartmental Safety Council were organized in 1934. In 1936, the Department of Labor began to assume a regulatory role under the Walsh-Healey Public Contracts Act, which required certain federal contractors to meet minimum safety and health standards. Enforcement of these standards was often carried out by the states with varying degrees of effectiveness, under cooperative agreements with the Department of Labor. There were many who felt that this patchwork of state and federal laws was not effective in preventing workplace injuries and illnesses.
The Modern Era
The first comprehensive federal occupational safety and health laws were passed in 1969 and 1970. In November 1968, an explosion in Farmington, West Virginia, killed 78 coalminers, providing impetus to the demands of the miners for tougher federal legislation. In 1969, the Federal Coal Mine Health and Safety Act was passed, which set mandatory health and safety standards for underground coal mines. The Federal Mine Safety and Health Act of 1977 combined and expanded the 1969 Coal Mine Act with other earlier mining laws and created the Mine Safety and Health Administration (MSHA) to establish and enforce safety and health standards for all mines in the United States.
It was not a single disaster, but a steady rise in injury rates during the 1960s that helped spur passage of the Occupational Safety and Health Act of 1970. An emerging environmental consciousness and a decade of progressive legislation secured the new omnibus act. The law covers the majority of workplaces in the United States. It established the Occupational Safety and Health Administration (OSHA) in the Department of Labor to set and enforce federal workplace safety and health standards. The law was not a complete break from the past in that it contained a mechanism by which states could administer their own OSHA programmes. The Act also established the National Institute for Occupational Safety and Health (NIOSH), in what is now the Department of Health and Human Services, to conduct research, train safety and health professionals and develop recommended safety and health standards.
In the United States today, occupational safety and health services are the divided responsibility of a number of different sectors. In large companies, services for treatment, prevention and education are primarily provided by corporate medical departments. In smaller companies, these services are usually provided by hospitals, clinics or physicians’ offices.
Toxicological and independent medical evaluations are provided by individual practitioners as well as academic and public sector clinics. Finally, governmental entities provide for the enforcement, research funding, education and standard setting mandated by occupational safety and health laws.
This complex system is described in the following articles. Drs. Bunn and McCunney from the Mobil Oil Corporation and the Massachusetts Institute of Technology, respectively, report on corporate services. Penny Higgins, RN, BS, of Northwest Community Healthcare in Arlington Heights, Illinois, delineates the hospital-based programmes. The academic clinic activities are reviewed by Dean Baker, MD, MPH, the Director of the University of California, Irvine’s Centre for Occupational and Environmental Health. Dr. Linda Rosenstock, Director of the National Institute for Occupational Safety and Health, and Sharon L. Morris, Assistant Chair for Community Outreach of the University of Washington’s Department of Environmental Health, summarize government activities at the federal, state and local levels. LaMont Byrd, the Director of Health and Safety for the International Brotherhood of Teamsters, AFL-CIO, describes the various activities provided to the membership of this international union by his office.
This division of responsibilities in occupational health often leads to overlapping, and in the case of workers’ compensation, inconsistent requirements and services. This pluralistic approach is both the strength and weakness of the system in the United States. It promotes multiple approaches to problems, but it can confuse all but the most sophisticated user. It is a system that often is in flux, with the balance of power shifting back and forth among the key players—private industry, labour unions, and state or federal governments.
Accident Insurance and Occupational Health Services in Germany
Every employer is contractually obligated to take precautions to guarantee the safety of his employees. The labour-related rules and regulations to which attention must be paid are of necessity just as various as the dangers present in the workplace. For this reason, the Occupational Safety Act (ASiG) of the Federal Republic of Germany includes among the duties of employers a legal obligation to consult specialist professionals on matters of occupational safety. This means that the employer is required to appoint not only specialist staff (particularly for technical solutions) but also company doctors for medical aspects of occupational safety.
The Occupational Safety Act has been in effect since December 1973. There were in the FRG at that time only about 500 doctors trained in what was called occupational medicine. The system of statutory accident insurance has played a decisive role in the development and construction of the present system, by means of which occupational medicine has established itself in companies in the persons of company doctors.
Dual Occupational Health and Safety System in the Federal Republic of Germany
As one of five branches of social insurance, the statutory accident insurance system makes a priority the task of taking all appropriate measures to ensure prevention of work accidents and occupational diseases through detection and elimination of work-related health hazards. In order to fulfil this legal mandate, legislators have granted extensive authority to a self-governing accident insurance system to enact its own rules and regulations concretizing and shaping the requisite preventive precautions. For this reason, the statutory accident insurance system has—within the bounds of existing public law—taken over the role of determining when an employer is required to take on a company doctor, what expert qualifications in occupational medicine the employer may demand of the company doctor and how much time the employer may estimate that the doctor will have to spend on the care of his employees.
The first draft of this accident prevention regulation dates from 1978. At that time, the number of available doctors with expertise in occupational medicine did not appear sufficient to provide all businesses with the care of company doctors. Thus the decision was made at first to establish concrete conditions for the larger businesses. At that time, to be sure, the businesses belonging to large-scale industry had often already made their own arrangements for company doctors, arrangements which already met or even exceeded the requirements stated in the accident prevention regulations.
Employment of a Company Doctor
The hours allocated in firms for the care of employees—called assignment times—are established by the statutory accident insurance system. Knowledge available to insurers concerning the existing risks to health in the various branches formed the basis for the calculation of the assignment times. The classification of firms with regard to particular insurers and the evaluation of possible health risks undertaken by them were thus the basis for the assignment of a company doctor.
Since the care rendered by company doctors is an occupational safety measure, the employer must cover the costs of assignment for such doctors. The number of employees within each of the several areas of hazard multiplied by the time allocated for care determine the sum of financial expenses. The result is a range of different forms of care, since it can pay—depending on the size of a firm—either to employ a doctor or doctors full-time, that is as the company’s own, or part-time, with services rendered on an hourly basis. This variety of requirements has led to a variety of organizational forms in which occupational medical services are offered.
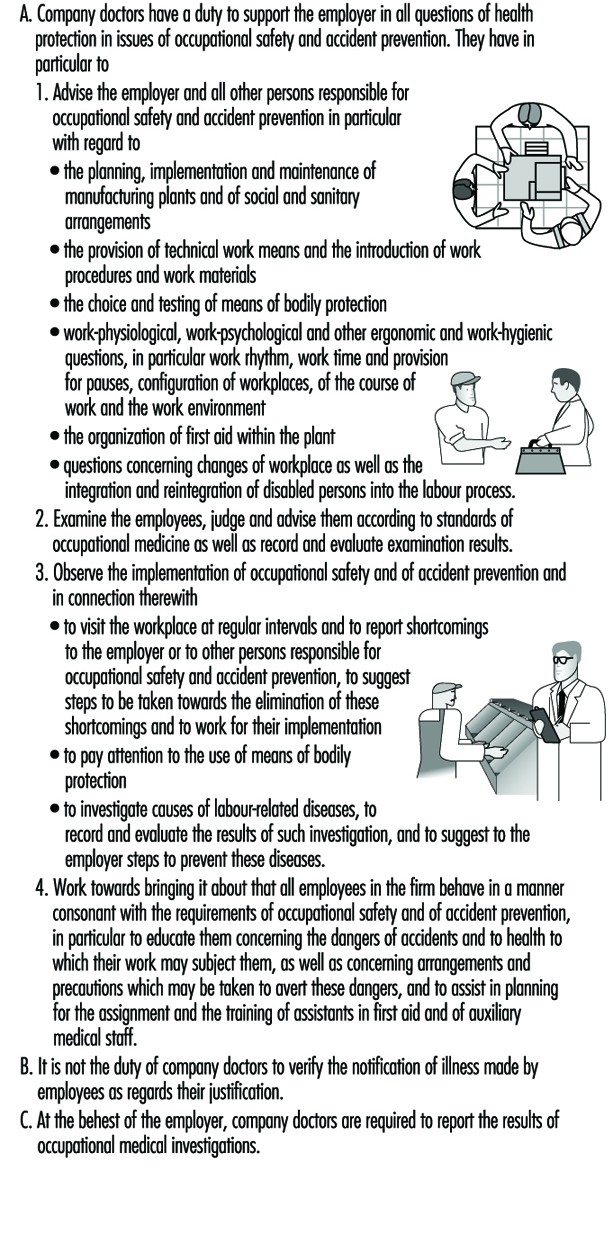
The Duties of a Company Doctor
In principle, a distinction should be made, for legal reasons, between the provisions made by companies to provide care for employees and the work done by the doctors in the public health system responsible for the general medical care of the population.
In order to differentiate clearly which services of occupational medicine employers are responsible for, which are given in figure 1, the Occupational Safety Act has already anchored in law a catalogue of duties for company doctors. The company doctor is not subject to the orders of the employer in the fulfilment of these tasks; still, company doctors have had to fight the image of an employer-appointed doctor up to the present day.
Figure 1. The duties of occupational physicians employed by companies in Germany
One of the essential duties of the company doctor is the occupational medical examination of employees. This examination can become necessary according to the specific features of a given concern, if particular working conditions exist which lead the company doctor to offer, of his own accord, an examination to the employees involved. He cannot, however, force an employee to allow himself to be examined by him, but must rather convince him through trust.
Special Preventive Checkups in Occupational Medicine
There exists, in addition to this kind of examination, the special preventive check-up, participation in which by the employee is expected by the employer on legal grounds. These special preventive checkups end in the issuance of a doctor’s certificate, in which the examining doctor certifies that, based on the examination conducted, he has no objection to the employee’s engaging in work at the workplace in question. The employer may assign the employee only once for each certificate issued.
Special preventive checkups in occupational medicine are legally prescribed if exposure to particular hazardous materials occurs in the workplace or if particular hazardous activities belong to job practice and such health risks cannot be excluded through appropriate occupational safety precautions. Only in exceptional circumstances—as is the case, for example, with radiation protection checkups—is the legal requirement that an examination be performed supplemented by legal regulations concerning what the doctor carrying out the examination must pay attention to, which methods he must apply, which criteria he must use to interpret the outcome of the examination and which criteria he must apply in judging health status with regard to work assignments.
This is why in 1972 the Berufsgenossenschaften, made up of commercial trade associations which provide the accident insurance for trade and industry, authorized a committee of experts to work out commensurate recommendations to doctors working in occupational medicine. Such recommendations have existed for more than 20 years. The Berufsgenossenschaften Guidelines for Special Preventive Checkups, listed in figure 2, now show a total of 43 examination procedures for the various health hazards which can be countered, on the grounds of present knowledge, with appropriate medical precautionary measures so as to prevent diseases from developing.
Figure 2. A summary information on external services of the Berufgenossenschaften in the German building industry

The Berufsgenossenschaften deduce the mandate to make available such recommendations from their duty to take all appropriate measures to prevent occupational diseases from arising. These Guidelines for Special Preventive Checkups are a standard work in the field of occupational medicine. They find application in all spheres of activity, not only in enterprises in the sphere of trade and industry.
In connection with the provision of such occupational medical recommendations, the Berufsgenossenschaften also took steps early on to ensure that in businesses lacking their own company doctor the employer would be required to arrange for these preventive checkups. Subject to certain basic requirements having to do primarily with the specialized knowledge of the doctor, but also with the facilities available in his or her practice, even doctors without expertise in occupational medicine can acquire the authority to offer companies their services in performing preventive checkups, contingent on a policy administered by the Berufsgenossenschaften. This was the precondition for the current availability of the total of 13,000 authorized doctors in Germany who perform the 3.8 million preventive checkups performed annually.
It was the supply of a sufficient number of doctors that also made it possible legally to require that employers initiate these special preventive checkups in complete independence of the question of whether or not the company employs a doctor prepared to do such checkups. In this way, it became possible to use the statutory accident insurance system to ensure enforcement of certain measures of health protection at work, even at the level of small businesses. The relevant legal regulations may be found in the Ordinance on Hazardous Substances and, comprehensively, in the accident prevention regulation, which regulates the rights and duties of the employer and the examined employee and the function of the licensed doctor.
Care Provided by Company Doctors
The statistics released annually by the Federal Board of Doctors (Bundesärztekammer) show that for the year 1994 more than 11,500 doctors fulfil the prerequisites, in the form of specialist knowledge in industrial medicine, to be company doctors (see table 1). In the Federal Republic of Germany, the organization Standesvertretung representing the medical profession regulates autonomously which qualifications must be met by doctors as regards study and subsequent professional development before they may become active as doctors in a given field of medicine.
Table 1. Doctors with specialist knowledge in occupational medicine
|
Number* |
Percentage* |
|
|
Field designation “occupational medicine” |
3,776 |
31.4 |
|
Additional designation “corporate medicine” |
5,732 |
47.6 |
|
Specialist knowledge in occupational medicine |
2,526 |
21.0 |
|
Total |
12,034 |
100 |
* As of 31 December 1995.
The satisfaction of these prerequisites for the activity of a company doctor represents either the attainment of the field designation “occupational medicine” or of the additional designation “corporate medicine”—that is, either four years’ further study after the licence to practice in order to be active exclusively as a work physician, or three years’ further study, after which activity as a company doctor is allowed only in so far as it is connected with medical activity in another field (e.g., as an internist). Doctors tend to prefer the second variant. This means, however, that they themselves see the chief emphasis of their professional work as physicians in a classical field of medical activity, not in occupational medical practice.
For these doctors, occupational medicine has the significance of an auxiliary source of income. This explains at the same time why the medical element of the examination by doctors continues to dominate the practical exercise of the profession of company doctor, although the legislature and the statutory accident insurance system themselves emphasize inspection of companies and medical advice given to employers and employees.
In addition, there still exists a group of doctors who, having acquired specialist knowledge in occupational medicine in earlier years, met different requirements at that time. Of particular significance in this regard are the standards which doctors in the former German Democratic Republic were required to meet in order to be allowed to practice as company doctors.
Organization of Care Provided by Company Doctors
In principle, it is left up to the employer to choose freely a company doctor for the firm from among those offering occupational medical services. Since this supply was not yet available subsequent to the establishment, in the early 1970s, of the relevant legal preconditions, the statutory accident insurance system took the initiative in regulating the market economy of supply and demand.
The Berufsgenossenschaften of the building industry instituted their own occupational medical services by engaging doctors with specialist knowledge in occupational medicine in contracts to provide care, as company doctors, to the firms affiliated with them. Via their statutes, the Berufsgenossenschaften arranged for each of their firms to be cared for by its own occupational medical service. The costs incurred were distributed among all the firms through appropriate forms of financing. A summary of information concerning external occupational medical services of the Berufsgenossenschaften of the building industry is given in table 2.
Table 2. Company medical care provided by external occupational medical services,1994
|
Doctors providing care as primary occupation |
Doctors providing care as secondary occupation |
Centres |
Employees cared for |
|
|
ARGE Bau1 |
221 |
83 mobile: 46 |
||
|
BAD2 |
485 |
72 |
175 mobile: 7 |
1.64 million |
|
IAS3 |
183 |
58 |
500,000 |
|
|
TÜV4 |
72 |
|||
|
AMD Würzburg5 |
60–70 |
30–35 |
1 ARGE Bau = Workers’ Community of the Berufgenossenschaften of Building Industry Trade Associations.
2 BAD = Occupational Medical Service of the Berufgenossenschaften.
3 IAS = Institute for Occupational and Social Medicine.
4 TÜV = Technical Control Association.
5 AMD Würzburg = Occupational Medical Service of the Berufgenossenschaften.
The Berufsgenossenschaften for the maritime industry and that for domestic shipping also founded their own occupational medical services for their businesses. It is a characteristic of all of them that the idiosyncrasies of the businesses in their trade—non-stationary enterprises with special vocational requirements—were a decisive factor in their taking the initiative to make clear to their companies the necessity for company doctors.
Similar considerations occasioned the remaining Berufsgenossenschaften to unite themselves in a confederation in order to found the Occupational Medical Service of the Berufsgenossenschaften (BAD). This service organization, which offers its services to every enterprise in the market, was enabled at an early stage by the financial collateral provided by the Berufsgenossenschaften to be present over the entire area of the Federal Republic of Germany. Its broad coverage, as far as representation goes, was meant to ensure that even those businesses located in the Federal states, or states of relatively poor economic activity, of the Federal Republic would have access to a company doctor in their area. This principle has been maintained up to the present time. The BAD is considered, meanwhile, the largest provider of occupational medical services. Nonetheless, it is forced by the market economy to assert itself against competition from other providers, particularly within urban agglomerations, by maintaining a high level of quality in what it provides.
The occupational medical services of the Technical Control Association (TÜV) and of the Institute for Occupational and Social Medicine (IAS) are the second- and third-largest transregional providers. There are in addition numerous smaller, regionally active enterprises in all of the Federated States of Germany.
Cooperation with Other Providers of Services in Occupational Health and Safety
The Occupational Safety Act, as a legal foundation for care provided to companies by company doctors, provides also for professional supervision of occupational safety, particularly in order to ensure that aspects of occupational safety be handled by personnel schooled in technical precautions. The requirements of industrial practice have changed meanwhile to such an extent that technical knowledge regarding questions of occupational safety must now be supplemented more and more by familiarity with questions of the toxicology of materials used. In addition, questions of ergonomic organization of work conditions and of the physiological effects of biological agents play an increasing role in evaluations of stresses in a place of work.
The requisite knowledge may be mustered only through interdisciplinary cooperation of experts in the field of health and safety at work. Therefore, the statutory accident insurance system supports particularly the development of forms of organization which take such interdisciplinary cooperation into account at the organizational stage, and creates within its own structure the preconditions for this cooperation by redesigning its administrative departments in a suitable fashion. What was once called the Technical Inspection Service of the statutory accident insurance system turns into a field of prevention, within which not only technical engineers but also chemists, biologists and, increasingly, physicians are active together in designing solutions for problems of labour safety.
This is one of the indispensable prerequisites for creating a basis for the type of organization of interdisciplinary cooperation—within businesses and between safety technology service organizations and company doctors—required for efficient solution of the immediate problems of occupational health and safety.
In addition, supervision in respect of safety technology should be advanced, in all companies, just as much as supervision by company doctors. Safety specialists are to be employed by businesses on the same legal basis—the Occupational Safety Act—or appropriately trained personnel affiliated with the industry are to be supplied by the businesses themselves. Just as in the case of the supervision provided by company doctors, the accident prevention regulation, Specialists for Occupational Safety (VBG 122), has formulated the requirements according to which businesses must employ safety specialists. In the case of safety-technical supervision of businesses as well, these requirements take all necessary precautions to incorporate each of the 2.6 million firms currently comprising the commercial economy as well as those in the public sector.
Around two million of these firms have fewer than 20 employees and are classed as small industry. With the full supervision of all enterprises, that is, including the smaller and smallest of businesses, the statutory accident insurance system creates for itself a platform for the establishment of occupational health and safety in all areas.
Occupational Health Services in Small-Scale Enterprises
The coverage of workers in small-scale enterprises (SSEs) is perhaps the most daunting challenge to systems for delivering occupational health services. In most countries, SSEs comprise the vast majority of the business and industrial undertakings—reaching as high as 90% in some of the developing and newly industrialized countries—and they are found in every sector of the economy. They employ on average nearly 40% of the workforce in the industrialized countries belonging to the Organization for Economic Cooperation and Development and up to 60% of the workforce in developing and newly industrialized countries. Although their workers are exposed to perhaps an even greater range of hazards than their counterparts in large enterprises (Reverente 1992; Hasle et al. 1986), they usually have little if any access to modern occupational health and safety services.
Defining Small-Scale Enterprises
Enterprises are categorized as small-scale on the basis of such characteristics as the size of their capital investment, the amount of their annual revenues or the number of their employees. Depending on the context, the number for the last category has ranged from one to 500 employees. In this article, the term SSE will be applied to enterprises having 50 or fewer employees, the most widely accepted definition (ILO 1986).
SSEs are gaining importance in national economies. They are employment-intensive, flexible in adapting to rapidly changing market situations, and provide job opportunities for many who would otherwise be unemployed. Their capital requirements are often low and they can produce goods and services near the consumer or client.
They also present disadvantages. Their lifetime is often brief, making their activities difficult to monitor and, frequently, their small margins of profits are achieved only at the expense of their workers (who are often also their owners) in terms of hours and intensity of workloads and exposure to occupational health risks.
The Workforce of SSEs
The workforce of SSEs is characterized by its diversity. In many instances, it comprises the manager as well as members of his or her family. SSEs provide entry to the world of work for young people and meaningful activities to elderly and redundant workers who have been separated from larger enterprises. As a result, they often expose such vulnerable groups as children, pregnant women and the elderly to occupational health risks. Further, since many SSEs are carried out in or near the home, they often expose family members and neighbours to the physical and chemical hazards of their workplaces and present public health problems through contamination of air or water or of food grown near the premises.
The educational level and socio-economic status of SSE workers vary widely but are often lower than the averages for the entire workforce. Of particular relevance is the fact that their owners/managers may have had little training in operation and management and even less in the recognition, prevention and control of occupational health risks. Even where appropriate educational resources are made available, they often lack the time, energy and financial resources to make use of them.
Occupational Hazards in SSEs and the Health Statusof their Workers
Like all other aspects of SSEs, their working conditions vary widely depending on the general nature of the enterprise, the type of production, the ownership and location. In general, the occupational health and safety hazards are much the same as those encountered in larger enterprises, but as noted above, the exposures to them are often substantially higher than in large enterprises. Occasionally, however, the working conditions in SSEs may be much better than those in larger enterprises with a similar type of production (Paoli 1992).
Although very few studies have been reported, it is not surprising that surveys of the health of workers in SSEs in such industrialized countries as Finland (Huuskonen and Rantala 1985) and Germany (Hauss 1992) have disclosed a relatively high incidence of health problems, many of which were associated with lowered capacity for work and/or were work-related in origin. In SSEs in developing countries an even higher prevalence of occupational diseases and work-related health problems has been reported (Reverente 1992).
Barriers to Occupational Health Services for SSEs
There are formidable structural, economic and psychological barriers to the provision of occupational health services to SSEs. They include the following:
- Traditionally, occupational safety and health legislation in most countries has exempted SSEs and is generally applicable only to manufacturing industries. The “informal sector” (this would include, say, the self-employed) and agriculture were not covered. Even where the legislation had wider coverage, it was not applicable to enterprises with small numbers of employees—500 employees was the usual lower limit. Re-cently, some countries (e.g., France, Belgium and the Nordic countries) have enacted legislation requiring the provision of occupational health service for all enterprises regardless of size or sector of the economy (Rantanen 1990).
- SSEs, as defined for this article, are too small to justify an in-plant occupational health service. Their wide diversity with respect to type of industry and methods of production as well as style of organization and operation, along with the fact that they are spread over wide geographic areas, makes it difficult to organize occupational health services that will meet all their needs.
- Economic barriers are substantial. Many SSEs hover on the edge of survival and just cannot afford any additions to their operating costs even though they may promise significant savings in the future. Further, they may not be able to afford education and training in hazard recognition, prevention and control for their owners/managers, much less their employees. Some countries have addressed the economic problem by providing subsidies either from governmental agencies or social security institutions (Rantanen 1994), or have included occupational health services in programmes promoting the general economic and social development of SSEs (Kogi, Phoon and Thurman 1988).
- Even when financial constraints are not inhibiting, there is often a disinclination among the owners/managers of SSEs to devote the time and energy needed to acquire the necessary basic understanding of the relationships between work and health. Once acquired, however, SSEs may be very successful in applying the information and abilities in their workplaces (Niemi and Notkola 1991; Niemi et al. 1991).
- Enterprises in the informal sector and small farming are seldom registered, and their formal links with official agencies may be weak or non-existent. Activities carried out as a business may be difficult to distinguish from those involving the private household and family. As a result, there may be concerns about privacy and resistance to interventions by “outsiders”. SSEs often resist becoming involved in trade associations and community organizations, and in perhaps the majority of instances their employees are not members of unions. To overcome such barriers, some countries have used extension organizations for the distribution of information, the creation of special training opportunities for the SSEs by official occupational safety and health agencies, and the adoption of the primary care model for the provision of occupational health services (Jeyaratnam 1992).
- Many SSEs are located in communities providing ready access to emergency and primary care services. However, the physicians’ and nurses’ lack of knowledge and experience with respect to occupational hazards and their effects often results in failure to recognize occupational diseases and, probably more important, loss of opportunities to install the necessary prevention and control measures.
International Instruments Covering OccupationalSafety and Health Services
In some countries, occupational safety and health activities are in the jurisdiction of labour ministries and are regulated by a special occupational safety and health authority; in others, this responsibility is shared by their ministries of labour, health and/or social affairs. In some countries, such as Italy, regulations covering occupational health services are embodied in health legislation or, as in Finland, in a special act. In the United States and in England, provision of occupational health services rests on a voluntary basis, while in Sweden, among others, it was once regulated by collective agreement.
The ILO Occupational Safety and Health Convention (No. 155) (ILO 1981a) requires governments to organize a policy for occupational safety and health to be applicable to all enterprises in all sectors of the economy that is to be implemented by a competent authority. This Convention stipulates the responsibilities of the authorities, employers and workers and, supplemented by the concomitant Recommendation No. 164, defines the key occupational safety and health activities of all relevant actors at both national and local levels.
The ILO supplemented these in 1985 by the International Convention No. 161 and Recommendation No. 171 on Occupational Health Services. These contain provisions on policy design, administration, inspection and collaboration of occupational health services, activities by occupational safety and health teams, conditions of operation, and responsibilities of employers and workers, and they furthermore offer guidelines for organizing occupational health services at the level of the enterprise. While they do not specify SSEs, they were developed with these in mind since no size limits were set for occupational health services and the necessary flexibility in their organization was emphasized.
Unfortunately, ratification of these ILO instruments has been limited, particularly in developing countries. On the basis of experience from the industrialized countries, it is likely that without special actions and support by government authorities, the implementation of the ILO principles will not take place in SSEs.
The WHO has been active in promoting the development of occupational health services. Examination of the legal requirements was carried out in a consultation in 1989 (WHO 1989a), and a series of about 20 technical documents on various aspects of occupational health services has been published by WHO headquarters. In 1985 and again in 1992, the WHO Regional Office in Europe carried out and reported surveys of occupational health services in Europe, while the Pan American Health Organization designated 1992 as a special year for occupational health by promoting occupational health activities in general and conducting a special programme in Central and South America.
The European Union has issued 16 directives concerning occupational safety and health, the most important of which is Directive 391/1989, which has been called the “Framework Directive” (CEC 1989). These contain provisions for specific measures such as requiring employers to organize health risk assessments of different technical facilities or to provide health examinations of workers exposed to special hazards. They also cover the protection of workers against physical, chemical and biological hazards including the handling of heavy loads and working at video display units.
While all of these international instruments and efforts were developed with SSEs in mind, the fact is that most of their provisions are practical only for larger enterprises. Effective models for organizing a similar level of occupational health services for SSEs remain to be developed.
Organizing Occupational Health Services for SSEs
As noted above, their small size, geographic dispersion and wide variation in types and conditions of work, coupled with great limitations in economic and human resources, make it difficult to efficiently organize occupational health services for SSEs. Only a few of the various models for delivering occupational health services described in detail in this chapter are adaptable to SSEs.
Perhaps the only exceptions are SSEs that are dispersed operating units of large enterprises. These usually are governed by policies established for the entire organization, participate in company-wide educational and training activities, and have access to a multidisciplinary team of specialists in occupational health located in a central occupational health service that is usually based at the headquarters of the enterprise. A major factor in the success of this model is having all of the costs of occupational safety and health activities covered by the central occupational health unit or the general corporate budget. When, as is increasingly common, the costs are allocated to the operating budget of the SSE, there may be difficulty in enlisting the full cooperation of its local manager, whose performance may be judged on the basis of the profitability of that particular enterprise.
Group services organized jointly by several small or medium-sized enterprises have been successfully implemented in several European countries—Finland, Sweden, Norway, Denmark, the Netherlands and France. In some other countries they have been experimented with, with the help of government subsidies or private foundations, but they have not survived after termination of subsidies.
An interesting modification of the group service model is the branch-oriented service, which provides services for a high number of enterprises operating all in the same type of industry, such as construction, forestry, agriculture, food industry and so on. The model enables the service units to specialize in the problems typical for the branch and thus accumulate high competence in the sector that they serve. A famous example of such a model is the Swedish Bygghälsan, which provides services for construction industries.
A notable exception is the arrangement organized by a trade union whose members are employed in widely scattered SSEs in a single industry (e.g., health care workers, meat cutters, office workers and garment workers). Usually organized under a collective agreement, they are financed by employers’ contributions but are usually governed by a board comprising representatives of both employers and workers. Some operate local health centres providing a broad range of primary and specialist clinical services not only for workers but often for their dependants as well.
In some instances, occupational health services are being provided by hospital outpatient clinics, private health centres and community primary care centres. They tend to focus on the treatment of acute work-related injuries and illnesses and, except perhaps for routine medical examinations, provide little in the way of preventive services. Their staffs often have a low level of sophistication in occupational safety and health, and the fact that they are usually paid on a fee-for-service basis provides no great incentive for their involvement in the surveillance, prevention and control of workplace hazards.
A particular disadvantage of these “external services” arrangements is that the customer or client relationship with those using them generally precludes the participation and collaboration of employers and workers in the planning and monitoring of these services that are stipulated in the ILO Conventions and the other international instruments created to guide occupational safety and health services.
Another variant is the “social security model”, in which occupational health services are provided by the same organization that is responsible for the cost of compensation for occupational diseases and injuries. This facilitates the availability of resources to finance the services in which, although curative and rehabilitative services are featured, preventive services are often prioritized.
An extensive study carried out in Finland (Kalimo et al. 1989), one of the very few attempts to evaluate occupational health services, showed that municipal health centres and private health centres were the dominant providers of occupational health services to SSEs, followed by the group or shared centres. The smaller the enterprise, the more likely it was to use the municipal health centre; up to 70% of SSEs with one to five workers were served by municipal health centres. Significant findings of the study included verification of the value of workplace visits by the personnel of the centres serving the SSEs to gain knowledge (1) of the working conditions and the particular occupational health problems of the client enterprises, and (2) of the need to provide them with special training in occupational safety and health before they undertake the provision of the services.
Types of Activities for Occupational Health Services for SSEs
The occupational health services designed for SSEs vary widely according to national laws and practices, the types of work and work environments involved, the characteristics and health status of the workers and the availability of resources (both in terms of the ability of the SSEs to afford the occupational health services and the availability of health care facilities and personnel in the locality). Based on the international instruments cited above and regional seminars and consultations, a list of activities for comprehensive occupational health services has been developed (Rantanen 1989; WHO 1989a, 1989b). A number of key activities that should always be found in an occupational health services programme, and that are relevant for SSEs, can be picked up from those reports. They include for example:
Assessment of occupational health needs of the enterprise
- preliminary analysis of the activities of the enterprise and identification of the health and safety hazards common to such workplaces
- inspection and surveillance of the workplace to identify and quantify the hazards actually present in the particular enterprise
- assessment of the extent of the risks they present and ranking them in order of their urgency and priority
- repeating the hazard assessment whenever there are changes in production methods, equipment and materials.
Prevention and control activities in the workplace
- communication of the results of the assessment to the owners/managers and the workers’ representatives
- identification of the prevention and control measures that are needed and available, assigning relative priority to them in terms of urgency and feasibility
- overseeing their installation and implementation
- monitoring their continuing effectiveness.
Preventive activities oriented to workers
- assessment and surveillance of workers’ health status by pre-placement, screening and periodic examinations which may be general as well as focused on the biological effects of particular hazards to which the workers may have been exposed
- adaptation of the job, the work station and the workplace environment to promote workers’ ongoing health and safety with special attention to such vulnerable groups as the very young, the elderly and those with acquired diseases and disabilities
- providing workers with health education and training in proper work practices
- providing education and training for owners/managers and supervisors that will inculcate awareness of the health needs of workers and motivation to initiate appropriate prevention and control measures.
Curative activities
- provide or arrange the delivery of the appropriate diagnostic, therapeutic and rehabilitative services for occupational injuries and diseases
- provide or arrange for early rehabilitation to obviate avoidable disability and encourage and oversee adjustments in the job that will permit early return to work
- provide education and training (and periodic retraining) in first aid and emergency procedures
- establish procedures and conduct training drills for coping with major emergencies such as spills, fires, explosions and so on
- provide or arrange for workers’ involvement in programmes that promote general health and well-being.
Record keeping and evaluation
- make and retain appropriate records on occupational accidents, injuries and diseases and if possible on exposure; evaluate the overall health and safety status of the enterprise on the basis of such data
- monitor the effectiveness of hazard prevention and control measures.
Implicit in the above list of core activities is the appropriate availability of advice and consultations in such occupational safety and health specialities as occupational hygiene, ergonomics, work physiology, safety engineering, occupational psychiatry and psychology and so on. Such specialists are not likely to be represented in the personnel of the facilities providing occupational health services to SSEs but, when needed, they can usually be provided by governmental agencies, universities and private consulting resources.
Because of their lack of sophistication and time, owners/managers of SSEs are forced to rely more heavily on the purveyors of safety equipment for the effectiveness and reliability of their products, and on the suppliers of chemicals and other production materials for complete and clear information (e.g., data sheets) about the hazards they may present and how these may be prevented or controlled. It is important, therefore, that there be national laws and regulations covering proper labelling, product quality and reliability, and the provision of easily understood information (in the local language) about equipment use and maintenance as well as product use and storage. As a backup, the trade and community organizations of which SSEs are often members should feature information about the prevention and control of potentially hazardous exposures in their newsletters and other communications.
Conclusions
In spite of their importance for the national economy and their role as employer of a majority of the nation’s workforce, SSEs, the self-employed and agriculture are sectors that are typically underserved by occupational health services. ILO Convention No. 161 and Recommendation No. 171 provide relevant guidelines for the development of such services for SSEs and should be ratified and implemented by all countries. National governments should develop the requisite legal, administrative and financial mechanisms to provide all workplaces with occupational safety and health services that will effectively identify, prevent and control exposures to potential hazards and promote the enhancement and maintenance of optimal levels of health status, well-being and productive capacity of all workers. Collaboration at international, regional and subregional levels, such as that provided by the ILO and the WHO, should be encouraged to foster the exchange of information and experience, the development of appropriate standards and guidelines and the undertaking of relevant training and research programmes.
SSEs may in many instances be reluctant to seek actively the services of occupational health units even though they might be the best beneficiaries of such services. Considering this, some governments and institutions, particularly in Nordic countries, have adopted a new strategy by starting wide-scale interventions for establishment or development of services. For instance the Finnish Institute of Occupational Health currently implements an Action Programme, for 600 SSEs employing 16,000 workers, aimed at the development of occupational health services, maintenance of work ability, prevention of environmental hazards in the neighbourhood and improving the competence of SSEs in occupational health and safety.
Medical Inspection of Workplaces and Workers in France
History
In the 1930s, the application in France of certain clauses of the labour code concerning occupational hygiene demonstrated the value of providing workplace inspectors with access to consulting physicians.
The laws of 17 July 1937 and 10 May 1946 (articles L 611-7 and R 611-4) empowered the Department of Workplace Inspection to order temporary medical interventions. Over time, these interventions, originally conceived of as intermittent, evolved into ongoing activities complementary to and conducted simultaneously with workplace inspection.
The promulgation of the law of 11 October 1946 concerning occupational medicine was soon followed by the establishment of a permanent technical framework for the medical inspection of workplaces and workers. The decree of 16 January 1947 established the context, pay scales, status and functions of medical inspectors of workplaces and workers.
Since 1947, however, technical development in this area has been irregular and sporadic, and the number of medical inspectors has sometimes failed to keep pace with the number of inspection tasks; the latter has also been true of workplace inspections. Thus, while medical departments created in accordance with the law of 11 October 1946 increased in prevalence and importance, the number of medical inspectors was gradually reduced from 44, the number originally called for in 1947, to 21. These contradictory trends partially explain some of the criticism the occupational medicine system has had to face.
However, since 1970, and particularly since 1975, there has been a significant effort to create a Department of Workplace Medical Inspection capable of responding to the needs of the approximately 6,000 physicians responsible for over 12 million workers. In 1980, inspection services were allocated 39 paid positions, of which 36 were actually filled. In 1995, 43 positions were available. Priority Action Plan Number 12 of the VIIth Plan provides for 45 medical inspectors; this will bring staffing levels up to the levels originally envisaged in 1947.
At the same time that French officials were recognizing the necessity of establishing a specialized inspection department responsible for the application of legislative and regulatory directives concerning occupational hygiene and medicine, identical conclusions were being drawn in other countries. In response to this growing consensus, the ILO, in collaboration with the WHO, convened an international colloquium on the medical inspection of workplaces, in Geneva in 1963. Among the noteworthy outcomes of the colloquium were the definition of the responsibilities, duties, and knowledge and training requirements of medical inspectors, and the techniques and methods of medical inspection.
General Organization
The central office of the Department of Workplace and Worker Medical Inspection is part of the Industrial Relations Department and reports directly to the Regional Director of Industrial Relations and Medical Inspection. The Regional Director, in turn, is part of the Regional Labour and Employment Board and reports directly to the Regional Director of Labour and Employment. The number of professionals and workers in France in 1995 were:
- 12.5 million workers benefiting from general coverage
- 6,337 physicians, of which 2,500 are full-time
- 4,000 nurses
- 1,500 medical departments
- 90% of workers are followed up by sectoral medical departments.
The number of medical inspectors in each region depends on the number of salaried occupational medicine positions in that region. In general, each regional medical inspector should be responsible for approximately 300,000 workers. This general rule is, however, subject to modification in either direction, depending on the size and geography of each region.
Mission
Although many of its clauses are no longer relevant or have lapsed, it is nevertheless useful to review the responsibilities of medical inspectors prescribed by the aforementioned decree of 16 January 1947.
The physician in charge of the department is responsible, among other things, for the coordination of all medical problems in the various departments of the Ministry of Labour and Social Security. His or her functions can be extended by decree.
The Medical Inspector of Workplaces and Workers will:
- maintain, with the Technical Committees of the Social Security Credit Unions, direct and permanent contact with the Workplace Inspection Department, and ensure the application of legislation concerning occupational hygiene and the protection of worker health
- carry out, on an ongoing basis, activities designed to protect worker health in the workplace; these activities will include, among other things, the supervision of the Occupational Medical Departments established by virtue of the law of 11 October 1946
- supervise, in close collaboration with psychotechnical departments, medical examinations aimed at determining workers’ fitness for work, and reclassifying and referring workers who are temporarily unfit for work or physically handicapped to rehabilitation centres
- supervise, in collaboration with the Technical Committees of the Social Security Credit Unions, the preparation, compilation and use of statistics concerning the physiopathological characteristics of the workforce.
The Medical Inspector of Workplaces will communicate information he or she possesses concerning the risk of occupational disease and accidents in different companies to the Technical Committees of the Social Security Credit Unions. The note of 15 September 1976 concerning the organization of Industrial Relations Departments assigns the following responsibilities to the Department of Workplace and Worker Medical Inspection:
- the investigation of technical aspects of occupational medicine, pathology, work physiology and ergonomics
- the investigation of questions related to the protection of wor-kers’ health and to work conditions
- the investigation of medical aspects of work
- the monitoring of progress in medicine, physiology and erg-onomics
- the coordination of regional information gathering.
Management of medical inspectors involves:
- the coordination of regional medical inspectors
- the development and application of reports, technical studies and research conducted regionally or transregionally, and ulti-mately, of specialized work groups
- the organization of meetings which provide members of the Department of Workplace and Worker Medical Inspection with an opportunity to compare experiences and define consistent approaches to new problems
- the preparation of recruitment and training procedures for medical inspectors of workplaces and workers
- the continuing education of all regional medical inspectors.
In addition to these core activities, the Department of Workplace and Worker Medical Inspection also collaborates with industrial relations and human resources departments in all cases involving medical aspects of work (especially those involving handicapped workers, candidates for continuing education and job applicants) and is responsible for managing, coordinating, recruiting and training regional medical inspectors and ensuring their continuing technical education. Finally, the central office of the Department also engages in consulting activities and is the government’s official representative in matters concerning occupational medicine.
The Department of Labour’s central or regional Departments of Workplace and Worker Medical Inspection may be called upon to intervene when other governmental departments without their own medical inspection services (most notably the Department of Health and Social Security) find themselves faced with problems related to the prevention or correction of occupational health hazards; these departments of the Department of Labour may also assist in the establishment of a department of medical prevention. Except in cases where the requesting party is another governmental work-inspection service, the Department’s role is usually limited to an advisory one.
From 7 to 10 June 1994, almost 1,500 people attended the XIIIth Journées nationales de médecine du travail (the 23rd National Occupational Medicine Conference) organized by the Société et l’Institut de médecine du travail et d’ergonomie de Franche-Comté (the Society and Institute of Occupational Medicine and Ergonomics of Franche-Comté). The following subjects were discussed:
- neurotoxicity of low-level solvent exposure
- health and the precariousness of health and work
- stress and strain of contemporary work—the role of the occup-ational physician.
The Department is the government’s representative in medicosocial, scientific and professional agencies or institutions in the field of occupational medicine. These include the Conseil National de l’Ordre des Médecins (the National Council of the Order of Physicians), le Haut Comité d’Études et d’Information contre l’alcoolisme (the High Commission for Alcoholism Research and Information) and various university and scientific institutions. In addition, the central Department of Workplace and Worker Medical Inspection is frequently called upon to present the French government’s position on medical questions to the European Economic Community, the WHO and the ILO. Regional departments have similar responsibilities, in accordance with Circular DRT No. 18-79, of 6 July 1979, on the role of cooperation between workplace inspectors and medical inspectors of workplaces in the prevention of occupational hazards. The circular identifies orientation, informational, supervisory, management and intervention activities to be carried out, as needed, in collaboration with the regional, departmental or local workplace inspection departments.
Although both workplace inspectors and medical inspectors share common goals—the prevention of occupational health ha-zards—their specific interventions may differ, depending on the technical expertise required. Other circumstances may, on the other hand, require their collaboration.
Proposed New Circular
A circular in preparation reiterates and updates the clauses of the circular of 6 July 1979. It should be noted that on 1 January 1995, the Departments of Occupational Training assumed the responsibilities of the regional Departments of Labour and Employment. The function, role and mission of medical inspectors of workplaces must therefore be reviewed.
In summary, we can say that by 1980, medical inspection departments had, for all intents and purposes, regained the role and functions originally foreseen for them in the period 1946-47. The most likely next step in medical inspection is towards increasing emphasis on promotion, management and research in workplaces. This evolution, it should be noted, parallels that of occupational medicine itself. Following a long period of development and implementation that may now be considered practically completed, occupational medicine must now embark upon a new era of qualitative improvement and scientific advance.
Occupational Health Services and Practice
Infrastructures, Practice and Approaches in Occupational Health
While much progress has been made since the 1980s towards a comprehensive approach in occupational health where the protection and promotion of workers’ health are pursued together with the maintenance and promotion of their working capacity, with a special emphasis on the establishment and maintenance of a safe and healthy working environment for all, there is much room for discussion as to the manner in which occupational health is actually implemented. The expression occupational health practice is currently used to cover the whole spectrum of activities undertaken by employers, workers and their organizations, designers and architects, manufacturers and suppliers, legislators and parliamentarians, labour and health inspectors, work analysts and work organization specialists, standardization organizations, universities and research institutions to protect health and to promote occupational safety and health.
The expression occupational health practice includes the contribution of occupational health professionals, but it is not limited to their practice of occupational health.
Confusion often occurs because the term occupational health services may be used to denote:
- the provision of occupational health services (i.e., the contribution of occupational health professionals to occupational safety and health)
- the institutionalized organizational arrangements to provide such services (i.e., the occupational health services which are part of the infrastructure to protect and promote workers’ health).
In order to overcome this difficulty and several other common causes of misunderstanding, the following wording was used for the second point on the agenda of the Twelfth Session of the Joint ILO/WHO Committee on Occupational Health: “Infrastructures for occupational health practice: options and models for national policies, primary health care approaches, strategies and programmes, and functions of occupational health services” (1995b) with the following understanding of the terms:
- Occupational health practice encompasses the activities of all those who contribute to the protection and promotion of workers’ health and to the improvement of working conditions and environment; these terms should not be understood as merely the practice of occupational health professionals.
- Occupational health approaches embodies a number of principles and approaches to guide action, such as the general principle of primary health care advocated by the WHO and the improvement of the working conditions and environment advocated by the ILO.
- Infrastructures for occupational health practice means the organizational arrangements to implement a national policy and to conduct action at the enterprise level; infrastructures may take the form of “institutionalized” occupational health services and include many other bodies such as national institutes for occupational safety and health.
The use of the key words infrastructures, practice and approaches permits the various actors and partners in prevention to play their individual roles in their respective fields of competence and to act jointly, as well.
Occupational health services contribute to the occupational health practice, which is intrinsically multidisciplinary and intersectoral and involves other specialists both in the enterprise and outside in addition to occupational health and safety professionals, as well as the appropriate governmental authorities, employers, workers and their representatives. Functionally, occupational health services must be considered both a part of country-level health infrastructures as well as of the infrastructures that exist for the implementation of relevant legislation on occupational safety and health. It is a national decision to determine whether such services should be under the supervision of the ministry of labour, the ministry of health, the social security institutions, a tripartite national committee or other bodies.
There are a large number of models for occupational health services. One of them enjoys the support of a large consensus at the international level: the model proposed by the ILO Occupational Health Services Convention (No. 161) and Recommendation (No. 171) adopted by the International Labour Conference in 1985. Countries should consider this model as an objective towards which progress should be made, taking into account, of course, local differences and the availability of specialized personnel and financial resources. A national policy should be adopted to develop progressively occupational health services for all workers, taking into account the specific risks of the undertakings. Such policy should be formulated, implemented and periodically reviewed in the light of national conditions and practice in consultation with the most representative organizations of employers and workers. Plans should be established indicating the steps which will be taken when occupational health services cannot be immediately established for all undertakings.
Multidisciplinary Cooperation and Intersectoral Collaboration: An Overall Perspective
The ILO and the WHO have a common definition of occupational health (see box), which was adopted by the Joint ILO/WHO Committee on Occupational Health at its first session (1950) and revised at its twelfth session (1995).
Governments, in collaboration with employers’ and workers’ organizations and professional organizations concerned, should design adequate and appropriate policies, programmes and plans of action for the development of occupational health with multidisciplinary content and comprehensive coverage. In each country, the scope and content of programmes should be adapted to national needs, should take into account local conditions and should be incorporated into national development plans. The Joint ILO/WHO Committee emphasized that the principles embodied in the ILO Conventions No. 155 and No. 161 and their accompanying Recommendations, as well as WHO resolutions, guidelines and approaches related to occupational health, provide a universally accepted guide for design of such policies and programmes (Joint ILO/WHO Committee on Occupational Health 1992).
Definition of occupational health adopted by the Joint
ILO/WHO Committee on Occupational Health (1950)
Occupational health should aim at the promotion and maintenance of the highest degree of physical, mental and social well-being of workers in all occupations; the prevention amongst workers of departures from health caused by their working conditions; the protection of workers in their employment from risks resulting from factors adverse to health; the placing and maintenance of the worker in an occupational environment adapted to his physiological and psychological capabilities and; to summarize: the adaptation of work to man and of each man to his job.
The main focus in occupational health is on three different objectives: (i) the maintenance and promotion of workers’ health and working capacity; (ii) the improvement of working environment and work to become conducive to safety and health and (iii) development of work organizations and working cultures in a direction which supports health and safety at work and in doing so also promotes a positive social climate and smooth operation and may enhance productivity of the undertakings. The concept of working culture is intended in this context to mean a reflection of the essential value systems adopted by the undertaking concerned. Such a culture is reflected in practice in the managerial systems, personnel policy, principles for participation, training policies and quality management of the undertaking.
There are similar features between the ILO strategy for the improvement of the working conditions and environment and the WHO general principle of primary health care. Both rest on similar technical, ethical and social considerations and they both:
- aim at all concerned, workers or the public
- define policies, strategies and means of action
- insist on the responsibility of each employer for the health and safety of the workers in his or her employment
- emphasize primary prevention and the control of risk at the source
- give special importance to information, health education and training
- indicate the need to develop an occupational health practice that is easily accessible to all and available at the workplace
- recognize the central place of participation, community participation in health programmes, inter-sectoral participation and workers’ participation in the improvement of the working conditions and the working environment
- highlight the interactions between health, environment and development, as well as between occupational safety and health and productive employment.
The main focus of ILO activity has been on the provision of international guidelines and a legal framework for the development of occupational health policies and infrastructures on a tripartite basis (including governments, employers and workers) and the practical support for improvement actions at the workplace, while the WHO has concentrated on the provision of scientific backgrounds, methodologies, technical support and on the training of health and related manpower for occupational health (Joint ILO/WHO Committee on Occupational Health 1992).
Multidisciplinary cooperation
For the WHO, occupational health includes safety at work. Hygiene is conceptualized as directed towards disease prevention while safety is thought of as the discipline that prevents bodily injuries due to accidents. For the ILO, occupational safety and health is considered as a discipline aiming at the prevention of work injuries (both occupational diseases and accidents) and at the improvement of working conditions and the environment. The terms occupational safety, occupational health, occupational medicine, occupational hygiene and occupational health nursing are used to acknowledge the contribution of different professions (e.g., engineers, physicians, nurses, hygienists) and in recognition of the fact that the organization of occupational safety and health at the enterprise level very often comprises separate occupational safety services and occupational health services, as well as safety and health committees.
To some extent, occupational safety and primary prevention are more directly linked to the technology which is used, to the process of production and to daily management than is occupational health, which focuses more on the relationships between work and health, in particular on the surveillance of the working environment and of workers’ health (secondary prevention), as well as on human factors and ergonomic aspects. Further, at the enterprise level, engineers are a necessary presence and are inte-gral to the management line (production engineers, maintenance, technicians and so on), while occupational health and hygiene requires the intervention of specialists in the health field who need not be present for the enterprise to function, but can be consultants or belong to an external occupational health service.
Whatever organizational arrangements and terminology are used, the most important thing is that occupational safety and health professionals work as a team. They need not necessarily be in the same unit or service, although this may be desirable where appropriate. The emphasis should not be on the structure of services but on the execution of their functions at the enterprise level in a sound manner (from a scientific, technical and ethical point of view). The emphasis should be on cooperation and coordination in the elaboration and implementation of a programme of action, as well as on the development of unifying concepts, such as “working cultures” (safety culture, labour protection culture, corporate culture) that are conducive to safety and health at work and “continuing quality improvement” of the working conditions and environment.
In 1992, the Joint ILO/WHO Committee emphasized that the scope of occupational health is very broad (as shown in table 1), encompassing disciplines such as occupational medicine, occupational nursing, occupational hygiene, occupational safety, ergonomics, engineering, toxicology, environmental hygiene, occupational psychology and personnel management. Collaboration and participation of employers and workers in occupational health programmes is an essential prerequisite for successful occupational health practice.
Table 1. Six principles and three levels for a sound occupational health practice
|
Principles |
|||||
|
Levels |
Prevention |
Protection |
Adaptation |
Promotion |
Mitigation |
|
Individuals (diversity) |
Accident prevention Industrial hygiene 1920s |
Industrial medicine Personal protective equipment 1930s |
Scientific organization of work Job analysis 1950s |
Employee assistance programmes 1950s |
Treatment compensation 1910s |
|
Groups (exposed groups, special needs) |
Safe and healthy working environment Built-in safety 1970s |
Occupational medicine Machine guarding 1940s |
Ergonomics including design 1950s |
Workers’ health promotion programmes 1980s |
Emergency planning and preparedness 1970s |
|
Society and all workers |
Control technologies Environmental health management 1970s |
Environmental health Epidemiology Preventive health care 1960s |
Appropriate technologies Consumers’ protection 1970s |
Health education and promotion programmes 1970s |
Curative health care 1920s |
Note: The times (1910, 1920, etc.) are arbitrary. Dates are merely given to provide an idea of the time scale for the progressive development of a comprehensive approach in occupational health. Dates will vary from country to country and may indicate the beginning or the full development of a discipline or the appearance of new terms or approaches for a practice which has been carried out for many years. This table does not intend to delineate exact disciplines involved in the process but to present in a concise manner their relationships within the framework of a mutlidisciplinary approach and intersectoral cooperation, towards a safe and healthy working environment and health for all, with a participatory approach and the objective of new forms of development which should be equitable if they are to be sustainable.
The definition of a common goal is one of the solutions to avoid the trap of an excessive compartmentalization of disciplines. Such compartmentalization of disciplines may sometimes be an asset since it allows for a specialized in-depth analysis of the problems. It may often be a negative factor, because it prevents the development of a multidisciplinary approach. There is a need to develop unifying concepts which open fields of cooperation. The new definition of occupational health adopted by the Joint Committee in 1995 serves this purpose.
Sometimes there can be heated arguments as to whether occupational health is a discipline in itself, or is part of labour protection, of environmental health or of public health. When the issue is more than academic and involves such decisions as which organization or ministry is competent for specific subject areas, the outcome can have significant consequences with regard to the allocation of funds and distribution of resources available in the form of expertise and equipment.
One of the solutions to such a problem is to advocate convergent approaches based on the same values with a common objective. The WHO approach of primary health care and the ILO approach of improving the working conditions and environment can serve this purpose. With common values of equity, solidarity, health and social justice in mind, these approaches can be translated into strategies (the WHO’s strategy of occupational health for all) and programmes (the ILO International Programme for the Improvement of Working Conditions and Environment) as well as into plans of action and activities implemented or carried out at the enterprise, national and international levels by all partners in prevention, protection and promotion of workers’ health, independently or jointly.
There are other possibilities. The International Social Security Association (ISSA) proposes the “concept of prevention” as a golden path to social security to address “safety worldwide” at work and at home, on the road and during leisure time. The International Commission on Occupational Health (ICOH) is developing an approach of ethics in occupational health and catalyses a rapprochement and cross-fertilization between occupational health and environment health. A similar trend can be seen in many countries where, for example, professional associations now get together occupational health and environmental health specialists.
Intersectoral collaboration
In 1984, the ILO’s annual International Labour Conference adopted a resolution concerning the improvement of working conditions and environment incorporating the concept that the improvement of the working conditions and environment is an element essential to the promotion of social justice. It stressed that improved working conditions and environment are a positive contribution to national development and represent a measure of success of any economic and social policy. It spelled out three fundamental principles:
- Work should take place in a safe and healthy environment.
- Conditions of work should be consistent with workers’ well-being and human dignity.
- Work should offer real possibilities for personal achievement, self-fulfilment and service to society.
During the 1980s a shift occurred from the concept of development towards the concept of “sustainable development”, which includes “the right to a healthy and productive life in harmony with nature” as indicated in the first principle of the Rio Declaration (United Nations Conference on Environment and Development—UNCED 1992). The objective of a safe and healthy environment has thus become an integral part of the concept of sustainable development, which also implies balancing environment protection with generation of opportunity for employment, improved livelihoods and health for all. Both environmental health and occupational health contribute to make development sustainable, equitable and sound not only from an economic but also from a human, social and ethical point of view. This paradigm shift is illustrated in figure 1.
Figure 1. A multidisciplinary approach towards a sustainable and equitable development

The purpose of this figure is to illustrate the interaction between occupational health and environmental health and their mutually supportive contribution to a sustainable development. It identifies an area which represents the integration of the economic and social objectives which can be met while at the same time taking account of the environment, employment and health.
The WHO Commission on Health and Environment has further recognized that “the kind of development needed to safeguard health and welfare will depend on many conditions, including respect for the environment, while development without regard for the environment would inevitably result in impairment of human health” (WHO 1992). In the same vein, occupational health should be recognized as an “added value”, that is, a positive contribution to national development and a condition of its sustainability.
Of particular significance to the work of the ILO and the WHO are the Declaration and Programme of Action adopted by the World Summit for Social Development held in Copenhagen in 1995. The Declaration commits the nations of the world to pursuing the goal of full, productive and freely chosen employment as a basic priority of their economic and social policies. The Summit clearly indicated that the goal must not be to create just any sort of jobs, but quality jobs that safeguard the basic rights and interests of workers. It made clear that the creation of good quality jobs must include measures to achieve a healthy and safe working environment, to eliminate environmental health hazards and provide for occupational health and safety. This is an indication that the future of occupational health may well be active partnership in reconciling employment, health and environment towards an equitable and sustainable development.
The primary health care approach emphasizes social equity, affordability and accessibility, participation and community involvement, as noted by the Joint ILO/WHO Committee on Occupational Health in 1995. These basic moral and ethical values are common to the ILO and the WHO. The primary health care approach is innovative because it applies social values to preventive and curative health care. This complementarity has not always been clearly understood; sometimes confusion is due to the interpretation of common words, which has led to a degree of misunderstanding in discussing actual roles and activities to be undertaken by the ILO and the WHO, which are complementary and mutually supportive.
Primary health care can be considered to be based on principles of social equity, self-reliance and community development. It may also be considered to be a strategy for reorienting health systems, in order to promote individual and community involvement and collaboration between all sectors concerned with health. A general principle should be that primary health care should incorporate an occupational health component and specialized occupational health services should apply the general principle of primary health care, regardless of the structural model in place.
There are many partners in prevention, sharing the philosophy of both the ILO and the WHO, who should provide the necessary inputs to implement a good occupational practice. The Joint ILO/WHO Committee has indicated that the ILO and the WHO should promote an inclusive approach to occupational health in their member countries. If such an approach is used, occupational health can be seen as a multidisciplinary and integrated subject. Taken in this light, activities of different organizations and ministries will not be competitive or contradictory but will be complementary and mutually supportive, working towards an equitable and sustainable development. The emphasis should be on common goals, unified concepts and basic values.
As pointed out by the Joint ILO/WHO Committee in 1995, there is a need to develop occupational health indicators for the promotion and monitoring of the progression towards health and sustainable development. Forms of development which jeopardize health cannot claim the quality of being equitable or sustainable. Indicators towards “sustainability” necessarily include health indicators, since UNCED emphasized that the commitment of “protecting and promoting human health” is a fundamental principle for sustainable development (Agenda 21, Chapter 6). The WHO has taken a leading role in developing both the concept and use of environmental health indicators, some of which concern health and the working environment.
The WHO and the ILO are expected to develop occupational health indicators which could help countries in the evaluation, both retrospective and prospective, of their occupational health practice, and assist them in monitoring the progress made towards the objectives set by national policies on occupational safety, occupational health and the working environment. The development of such indicators focusing on the interactions between work and health could also assist occupational health services in evaluating and guiding their programmes and their activities to improve the working conditions and environment (i.e., in monitoring the efficiency and the manner in which they carry out their functions).
Standards and Guidance
The ILO Conventions and Recommendations on occupational safety and health define the rights of the workers and allocate duties and responsibilities to appropriate authorities, to the employers, and to the workers in the field of occupational safety and health. The ILO Conventions and Recommendations adopted by the International Labour Conference, taken as a whole, constitute the International Labour Code which defines minimum standards in the labour field.
The ILO policy on occupational health and safety is essentially contained in two international Conventions and their accompanying Recommendations. The ILO Occupational Safety and Health Convention (No. 155) and its Recommendation (No. 164), 1981, provide for the adoption of a national occupational safety and health policy at the national level and describe the actions needed at the national and at the enterprise levels to promote occupational safety and health and to improve the working environment. The ILO Occupational Health Services Convention (No. 161) and its Recommendation (No. 171), 1985, provide for the establishment of occupational health services which will contribute to the implementation of the occupational safety and health policy and will perform their functions at the enterprise level.
These instruments provide for a comprehensive approach to occupational health that includes primary, secondary and tertiary prevention and is consistent with general principles of primary health care. They indicate the manner in which occupational health care should ideally be delivered to the working populations, and propose a model that channels towards the workplace organized activities which require expert staff in order to catalyse an interaction between various disciplines to promote cooperation between all partners in prevention. These instruments also provide an organizational framework wherein occupational health professionals can deliver efficiently quality services to ensure workers’ health protection and promotion and contribute to the health of enterprises.
Functions
Convention No. 161 defines occupational health services as services dedicated to essentially preventive functions and responsible for advising employers, workers and their representatives at the enterprise on the requirements for establishing and maintaining a safe and healthy working environment that will optimize physical and mental health in relation to work and on the adaptation of work to the capabilities of workers, taking into consideration their state of physical and mental health.
The Convention specifies that occupational health services should include those of the following functions that are adequate and appropriate to the occupational risks at the worksite:
- identification and assessment of the risks from health hazards in the workplace
- surveillance of the factors in the working environment and working practices which may affect workers’ health, including sanitary installations, canteens and housing where these facilities are provided by the employer
- advice on planning and organization of work, including the design of workplaces, on the choice, maintenance and condition of machinery and other equipment and on substances used in work
- participation in the development of programmes for the improvement of working practices, as well as testing and evaluation of health aspects of new equipment
- advice on occupational health, safety and hygiene and on ergonomics and individual and collective protective equipment
- surveillance of workers’ health in relation to work
- promoting the adaptation of work to the worker
- contributing to measures of vocational rehabilitation
- collaborating in providing information, training and education in the fields of occupational health and hygiene and ergonomics
- organizing first aid and emergency treatment
- participating in analysis of occupational accidents and occupational diseases.
The ILO Convention and Recommendation are very flexible with regard to the forms of organization of occupational health services. The establishment of occupational health services may be done by laws or regulations, by collective agreements, or in any other manner approved by the appropriate authority, after consultation with the representative organizations of concerned employers and workers. Occupational health services may be organized as a service for a single enterprise or as a service common to a number of enterprises. As far as possible, the occupational health services should be located near the place of employment or should be organized to ensure their proper functioning at the place of employment. They may be organized by the concerned enterprises, by the public authorities or official services, by social security institutions, by any other bodies authorized by the authorities or, indeed, by combination of any of these. This offers a large degree of flexibility and, even in the same country, several or all of these methods may be used, according to local conditions and practice.
The flexibility of the Convention demonstrates that the spirit of the ILO instruments on occupational health services is to place more emphasis on its objectives rather than on the administrative rules for achieving them. It is important to ensure occupational health to all workers, or at least to make progress towards this objective. Such progress is usually achievable by degrees but it is necessary to make some progress towards achieving these aims and to mobilize resources in the most efficient manner for this purpose.
Various methods of financing occupational health exist. In many countries the obligation of establishing and maintaining occupational health services rests with employers. In other countries they are part of national health schemes or public health services. Staffing, financing and training of personnel are not detailed in the Convention but are individual national approaches.
Many examples exist of occupational health services set up by social security institutions or financed by special workers’ insurance schemes. Sometimes their financing is governed by an arrangement agreed upon by the ministry of labour and the ministry of health or by the social security institutions. In some countries trade unions run occupational health services. There are also special arrangements wherein funds are collected from employers by a central institution or tripartite body and then disbursed to provide occupational health care or distributed to finance the functioning of occupational health services.
The sources of financing occupational health services may also vary according to their activities. For example, when they have curative activities, social security may contribute to their financing. If occupational health services take part in public health programmes and in health promotion or in research activities, other funding sources may be found or become available. Financing will depend not only on the structural model chosen to organize the occupational health services, but also on the value that society concedes to health protection and promotion and its willingness to invest in occupational health and in the prevention of occupational hazards.
Conditions of Operation
A special emphasis is placed on the conditions of operation of occupational health services. It is not only necessary for the occupational health services to execute a number of tasks but it is equally important that these tasks should be performed in an appropriate manner, taking into consideration technical and ethical aspects.
There are some basic requirements as regards the operation of occupational health services which are spelled out in the ILO Convention, and especially in the Recommendation on Occupational Health Services. These may be summarized as follows:
- The personnel in occupational health services should be qualified and benefit from a full professional independence.
- Confidentiality should be ensured.
- Workers should be informed of the activities of the services and of the results of their health assessments.
- Employers, workers and their representatives should participate in the operation of the services and in the design of their programmes.
Ethical dimensions of occupational health are increasingly taken into account, and emphasis is placed on the need for both quality and on-going evaluation of occupational health services. It is not only necessary to determine what should be done but also for which purpose and under which conditions. The ILO Recommendation on Occupational Health Services (No. 171) introduced a first set of principles in this respect. Further guidance is given by the International Code of Ethics for Occupational Health Professionals adopted by the International Commission on Occupational Health (ICOH 1992).
In 1995, the Joint ILO/WHO Committee on Occupational Health emphasized that “quality assurance of services must be an integral part of the occupational health services development. It is unethical to give poor quality of service”. The ICOH Code of Ethics prescribes that “occupational health professionals should institute a programme of professional audit of their own activities in order to ensure that appropriate standards have been set, that they are being met and that deficiencies, if any, are detected and corrected”.
Common Goals and Values
The role of institutionalized occupational health services should be seen within the broader framework of health and social policies and infrastructures. The functions of occupational health services contribute to the implementation of the national policies on occupational safety, occupational health and the working environment advocated by the ILO Occupational Safety and Health Convention (No. 155) and Recommendation (No. 164), 1981. Occupational health services contribute also to the attainment of the objectives embodied in the “Health For All” strategy advocated by the WHO as a policy for equity, solidarity and health.
There are signs of an increasing trend to mobilize expertise and resources within the framework of networking arrangements and joint ventures. At the international level, such is already the case for chemical safety, where there is an interorganization me-chanism for chemical safety: the Inter-Organization Programme for the Sound Management of Chemicals (IOMC). There are many other fields where new flexible forms of international cooperation among countries and international organizations are emerging or could be developed, such as radiation protection and biological safety.
Networking arrangements open new fields of cooperation which may be adapted in a flexible manner to the theme which is to be addressed, such as occupational stress, coordinating research or updating this Encyclopaedia. The emphasis is placed on interactions and not any more on vertical compartmentalization of disciplines. The concept of leadership gives way to active partnership. International networking for occupational safety and health is developing rapidly and could be further developed on the basis of existing structures which could be interconnected. The roles of the ILO and the WHO may well be to initiate international networks designed to fulfil the needs and demands of their constituents and to meet the common goal of protecting the people at work.
The social and ethical values agreed upon by the international community are incorporated into the ILO Conventions and Recommendations, as well as in the WHO policy on “Health For All”. Since the 1980s the concept of sustainable development has progressively emerged and, after the Rio Conference and the Social Summit in Copenhagen, now takes into account the interrelationships between employment, health and the environment. The common goal of a safe and healthy working environment for all will reinforce the determination of all those involved in occupational safety and health to better serve the health of workers and to contribute to a sustainable and equitable development for all. One of the main challenges in occupational health may well be to resolve the conflict between values such as the right to health and the right to work at the level both of the individual and all workers, with the aim of protecting health and allowing employment.
Standards, Principles and Approaches in Occupational Health Services
This article is based on the standards, principles and approaches embodied in the ILO Occupational Health Services Convention, 1985 (No. 161) and its accompanying Recommendation (No. 171); ILO Occupational Safety and Health Convention, 1981 (No. 155) and its accompanying Recommendation (No. 164); and the Working Document of the Twelfth Session of the Joint ILO/WHO Committee on Occupational Health, 5-7 April 1995.
The ILO Occupational Health Services Convention (No. 161) defines “occupational health services” as services entrusted with essentially preventive functions and responsible for advising the employer, the workers and their representatives in the undertaking on the requirements for establishing and maintaining a safe and healthy working environment which will facilitate optimal physical and mental health in relation to work and the adaptation of work to the capabilities of workers in the light of their state of physical and mental health.
Provision of occupational health services means carrying out activities in the workplace with the aim of protecting and promoting workers’ safety, health and well-being, as well as improving working conditions and the working environment. These services are provided by occupational health professionals functioning individually or as part of special service units of the enterprise or of external services.
Occupational health practice is broader and consists not only of the activities performed by the occupational health service. It is multidisciplinary and multisectoral activity involving in addition to occupational health and safety professionals other specialists both in the enterprise and outside, as well as competent authorities, the employers, workers and their representatives. Such involvement requires a well-developed and well-coordinated system at the workplace. The necessary infrastructure should comprise all the administrative, organizational and operative systems that are needed to conduct the occupational health practice successfully and ensure its systematic development and continuous improvement.
The most elaborate infrastructure for occupational health practice is described in the ILO Occupational Safety and Health Convention, 1981 (No. 155) and the Occupational Health Services Convention, 1985 (No. 161). The establishment of occupational health services according to the models advocated by the Convention No. 161 and its accompanying Recommendation No. 171 is one of the options. It is however evident that the most advanced occupational health services are in concordance with the ILO instruments. Other types of infrastructures may be used. Occupational medicine, occupational hygiene and occupational safety may be practised separately or together within the same occupational health service. The occupational health service may be a single integrated entity or a composite of different occupational health and safety units unified by a common concern for workers’ health and well-being.
Availability of Occupational Health Services
Occupational health services are unevenly distributed in the world (WHO 1995b). In the European Region, about half of the working population remains uncovered by competent occupational health services; the variation among countries is very wide, with coverage figures ranging between 5% and 90% of the workforce. The Central and Eastern European countries now in transition are having problems in providing services due to reorganization of their economic activities and the break-up of the large centralized industries into smaller units.
Lower coverage figures are found on other continents. Only a few countries (United States, Canada, Japan, Australia, Israel) show coverage figures comparable to those in Western Europe. In typical developing regions, the coverage by employee health services ranges from 5% to 10% at best, with services being found mainly in manufacturing enterprises, while some sectors of industry, agriculture, the self-employed, small-scale enterprises and the informal sector are usually not covered at all. Even in countries where coverage rates are high, there are gaps, with small-scale enterprises, certain mobile workers, construction, agriculture and the self-employed being underserved.
Thus, there is a universal need to increase the coverage of workers by occupational health services throughout the world. In a number of countries, intervention programmes to increase the coverage have demonstrated that it is possible to substantially improve the availability of occupational health services in a relatively short time and at a reasonable cost. Such interventions have been found to improve both the workers’ access to the services and the cost effectiveness of the services provided.
Policy Impact of International Instruments
The so-called work environment reform which took place in most of the industrialized countries in the 1970s and 1980s saw the production of important international instruments and guidelines. They reflected the responses of occupational health policies to the new needs of working life, and the achievement of an international consensus on the development of occupational safety and health.
The International Programme for the Improvement of Working Conditions and Environment (PIACT) was launched by the ILO in 1976 (Improving Working Conditions and Environment: An International Programme (PIACT) 1984; 71st Session of the International Labour Conference 1985). The ILO Occupational Safety and Health Convention, 1981 (No. 155), with its accompanying Recommendation (No. 164), and the ILO Occupational Health Services Convention, 1985 (No. 161) and its accompanying Recommendation (No. 171), amplified the impact of the ILO in the development of occupational safety and health. By 31 May 1995, 40 ratifications of these Conventions had been registered, but their practical impact was much wider than the number of ratifications, since many countries had implemented the principles embodied in these instruments, although they had not been able to ratify them.
Simultaneously, the WHO Global Strategy Health for All by the Year 2000 (HFA) (1981), first launched in 1979, was followed in the 1980s by introduction and implementation of regional and national HFA strategies in which workers’ health constituted an essential part. In 1987, WHO launched a Programme of Action for Workers’ Health, and in 1994 the WHO Collaborating Centres in Occupational Health developed the Global Strategy for Occupational Health for All (1995), which was endorsed by the WHO Executive Board (EB97.R6) and unanimously adopted by the World Health Assembly in May 1996 (WHA 49.12).
The most important features of the international consensus on occupational safety and health are:
- a focus on occupational health and safety for all workers irrespective of the sector of the economy, the type of employment (salaried worker or self-employed), the size of the enterprise or company (industry, public sector, services, agriculture and so on)
- the responsibility of governments for the establishment of appropriate infrastructures for occupational health practice through legislation, collective agreements or any other mechanism acceptable to the government after consultation with employers’ and workers’ representative organizations
- the liability of governments for the development and implementation of occupational safety and health policy in tripartite collaboration with employers’ and workers’ organizations
- the primary responsibility of the employer for the provision of occupational health services at the enterprise level, who must involve competent occupational health professionals to implement the provisions stipulated by the national legislation or the collective agreements
- the prevention of work accidents and occupational diseases and control of workplace hazards as well as the development of a work environment and work conducive to workers’ health are the main purpose of occupational health services.
The United Nations Summit on Environment and Development in Rio de Janeiro in 1993 touched on several aspects of human environment which have relevance to occupational health (WHO 1993). Its Agenda 21 contains elements on providing services for underserved workers and ensuring chemical safety at the workplace. The Rio Declaration emphasized peoples’ right to lead “healthy and productive lives in harmony with nature”, which would require work and working environment to meet certain minimum health and safety standards.
Such instruments and international programmes directly or indirectly stimulated the inclusion of the provision of occupational health services in the national Health for All by the Year 2000 programmes and other national development programmes. Thus, the international instruments have served as guidelines for the development of national legislation and programmes.
A significant role in the global development of occupational health has been played by the Joint ILO/WHO Committee on Occupational Health, which, in its twelve meetings held since 1950, has made important contributions toward the definition of concepts and their transfer into national and local practices.
Legislative Structures for Occupational Health Practice
Most countries have laws governing the provision of occupational health services, but the structure of the legislation, its content and the workers covered by it vary widely (Rantanen 1990; WHO 1989c). The more traditional laws consider occupational health services as a group of specialized and separate activities such as occupational health care, occupational safety and hygiene services, workplace health promotion programmes and so on. In many countries, instead of stipulating what might be regarded as programmes, the legislation stipulates the responsibility of employers to provide health risk assessments, health examinations of workers or other individual activities related to workers’ health and safety.
More recent laws reflecting international guidelines such as those contained in the ILO Convention on Occupational Health Services (No. 161) consider the occupational health service as an integrated, comprehensive, multidisciplinary team containing all the elements needed for the improvement of health at work, improvement of the working environment, promotion of workers’ health, and the overall development of the structural and managerial aspects of the workplace needed for health and safety.
The legislation usually delegates the authority to establish, implement and inspect occupational health services to such ministries or agencies as Labour, Health or Social Security (WHO 1990).
There are two main types of legislation regulating occupational health services:
One views the occupational health service as an integrated multidisciplinary service infrastructure and stipulates the objectives, activities, obligations and rights of the various partners, the conditions of operation, as well as the qualifications of its personnel. Examples include the European Union Framework Directive No. 89/391/EEC on Occupational Safety and Health (CEC 1989; Neal and Wright 1992), the Dutch ARBO Act (Kroon and Overeynder 1991) and the Finnish Act on Occupational Health Services (Translation of the Occupational Health Care Act and the Council of the State Decree No. 1009 1979). There are only a few examples of the organization of systems of occupational health services in the industrialized world that are in accord with this type of legislation, but their number is expected to grow with progressive implementation of the European Union Framework Directive (89/391/EEC).
The other type of legislation is found in most industrialized countries and is more fragmented. Instead of a single act stipulating the occupational health service as an entity, it involves a number of laws that simply oblige employers to carry out certain activities. These may be stipulated quite specifically or merely in general, leaving issues of their organization and conditions of operation open (WHO 1989c). In many developing countries, this legislation is applicable only to main industrial sectors, while large numbers of other sectors as well as agriculture, small-scale enterprises and the informal sector remain uncovered.
During the 1980s, particularly in industrialized countries, social and demographic developments such as ageing of the working population, increase in disability pensions and sickness absenteeism, and difficulty in controlling social security budgets led to some interesting reforms of national occupational health systems. These focused on the prevention of both short-term and long-term disability, preservation of working capacity, particularly of older workers, and reducing early retirement.
For example, the amendment of the Dutch ARBO Act (Kroon and Overeynder 1991) together with three other social laws aimed at the prevention of short- and long-term disability stipulated important new requirements for occupational health and safety services at the plant level. They included:
- minimum requirements for procedures, guidelines and facilities
- minimum requirements for the numbers, composition and competence of occupational health service teams, including such specialists as physicians with competence in occupational health, senior safety experts, occupational hygienists and management consultants
- requirements specifying the organization of services and their activities
- requirement of quality assurance systems, including appropriate audits
- requirement that the specialists working in the service be certified by appropriate authorities and that the service itself be certified on the basis of an external audit.
This new system will be implemented stepwise and should be mature before the end of the 1990s.
Amendments of the Finnish Act on Occupational Health Services in 1991 and 1994 introduced the maintenance of working capacity, particularly of ageing workers, as a new element in the legislation-based preventive activities of occupational health services. Implemented through the close collaboration of all the actors in the workplace (management, workers, health and safety services), it involves improvement and adaptation of work, working environment and equipment to the worker, improving and maintaining the physical and mental working capacity of the worker, and making the work organization more conducive to maintaining the work capacity of the worker. Currently, efforts are being directed at the development and evaluation of practical methods to achieve these goals.
The adoption in 1987 of the Single European Act gave new impetus to the occupational health and safety measures taken by the European Communities. This was the first time health and safety at work had been directly included in the EEC Treaty of 1957 and was done through the new Article 118a. Of significant importance to the level of protection is that directives adopted by the Member States under Article 118a lay down minimum requirements concerning health and safety at work. According to this principle, the Member States must raise their level of protection if it is lower than the minimum requirements set by the directives. Beyond this, they are entitled and encouraged to maintain and introduce more stringent protective measures than required by the directives.
June 1989 saw the adoption of the first and probably the most important Directive providing for minimum requirements concerning health and safety at work under Article 118a: Framework Directive 89/391/EEC on the introduction of measures to encourage improvements in the safety and health of workers at work. It is the core strategy on health and safety on which all subsequent directives will be built. The Framework Directive is to be supplemented by individual directives covering specific areas and also sets the general framework for future directives related to it.
The Framework Directive 89/391/EEC contains many features of the ILO Conventions Nos. 155 and 161 which the 15 countries of the European Union will implement in their national laws and practices. Main provisions that are relevant to occupational health practice include:
- the development of a coherent overall prevention policy at the enterprise level covering the working environment, technology, organization of work, working conditions and social relationships
- the responsibility of the employer to ensure the safety and health of workers in every aspect related to the work, including prevention of occupational hazards, provision of information and training, as well as provision of the necessary work organization, control measures and means that occupational health activities should be carried out in collaboration between employers and workers
- that workers should receive health surveillance adequate for the health risks they incur at work
- that workers have the right to receive all the necessary information concerning the safety and health risks as well as preventive and protective measures in respect of both the enterprise in general and each type of workstation and work practice
- that the planning and introduction of new technologies should be subject to consultation with the workers and/or their representatives, as regards the choice of equipment, working conditions and the working environment for the safety and health of workers
- that the general principles of prevention should include the elimination of occupational hazards; evaluation of hazards which cannot be avoided; combating the risks at the source; adapting the work to the individual, especially as regards the design of workplaces, the choice of equipment and working and production methods; adapting to technical progress; replacing dangerous substances by non-dangerous or less dangerous ones; giving collective protective measures priority over individual protective measures; giving appropriate instructions to the workers.
During the past years, a large amount of European Union legislation has been introduced, including a series of individual directives based on the principles formulated in the Framework Directive, some supplementing those which had been subject to technical harmonization measures in preparation, and others covering specific risks and high-risk sectors. Examples of the first group are directives concerning the minimum safety and health requirements for the workplace, for the use of work equipment by workers at work, for the use of personal protective equipment, for the manual handling of loads, for work with display screen equipment, for the provision of safety and health signs at work, and the implementation of the minimum safety and health requirements at temporary or mobile construction sites. The second group includes such directives as the protection of workers from the risks related to exposure to vinyl chloride monomer, metallic lead and its ionic compounds, asbestos at work, carcinogens at work, biological agents at work, the protection of workers by the banning of certain specified agents and/or certain work activities, and some others (Neal and Wright 1992; EC 1994).
Proposals have been made recently for the adoption of other directives (namely, the directives on physical agents, chemical agents, transport activities and workplaces, and work equipment) in order to consolidate some existing directives and rationalize the overall approach to the safety and health of workers in these fields (EC 1994).
Many new elements in the national legislation and practices respond to today’s emerging problems of working life and contain provisions for further development of occupational health infrastructures. This especially concerns programming, at the national and enterprise level, more comprehensive activities in respect of psychosocial, organizational and work capacity aspects and particular emphasis on the principle of participation. They also provide for the application of quality management systems, auditing and certification of both the competence of the experts and services to meet the requirements of occupational safety and health legislation. Thus, such national laws, by absorbing the substantive content of the ILO instruments, no matter whether the instruments are ratified or not, lead to the stepwise implementation of the objectives and principles embodied in the ILO Conventions Nos. 155 and 161 and in the WHO HFA Strategy.
Objectives of Occupational Health Practice
The objectives of occupational health practice that were originally defined in 1950 by the Joint ILO/WHO Committee on Occupational Health stated that:
Occupational health should aim at the promotion and maintenance of the highest degree of physical, mental and social well-being of workers in all occupations; the prevention amongst workers of departures from health caused by their working conditions; the protection of workers in their employment from risks resulting from factors adverse to health; the placing and maintenance of the worker in an occupational environment adapted to his physiological and psychological capabilities; and, to summarize: the adaptation of work to man and of each man to his job.
In 1959, based on discussions of the special ILO tripartite committee (representing governments, employers and workers), the Forty-third Session of the International Labour Conference adopted Recommendation No. 112 (ILO 1959) which defined an occupational health service as a service established in or near a place of employment for the purposes of:
- protecting the workers against any health hazard which may arise out of their work or the conditions in which it is carried on
- contributing towards the workers’ physical and mental adjustment, in particular by the adaptation of the work to the workers and their assignment to jobs for which they are suited
- contributing to the establishment and maintenance of the highest possible degree of physical and mental well-being of the workers.
In 1985, the ILO adopted new international instruments—the Occupational Health Services Convention (No. 161) and its accompanying Recommendation (No. 171) (ILO 1985a, 1985b)— which defined occupational health services as services entrusted with essentially preventive functions and responsible for advising the employer, the workers and their representatives in the undertaking on: the requirements for establishing and maintaining a safe and healthy working environment which will facilitate optimal physical and mental health in relation to work; and the adaptation of work to the capabilities of workers in light of their state of physical and mental health.
In 1980, the WHO/Euro Working Group on Evaluation of Occupational Health and Industrial Hygiene Services (WHO 1982) defined the ultimate goal of such services as “promoting conditions at work that guarantee the highest degree of quality of working life by protecting workers’ health, enhancing their physical, mental and social well-being, and preventing ill-health and accidents”.
The extensive survey of occupational health services in the 32 countries in the European Region carried out in 1985 by the WHO Regional Office for Europe (Rantanen 1990) identified the following principles as objectives of occupational health practice:
- protecting workers’ health against hazards at work (the protection and prevention principle)
- adapting work and the work environment to the capabilities of workers (the adaptation principle)
- enhancing the physical, mental and social well-being of workers (the health promotion principle)
- minimizing the consequences of occupational hazards, accidents and injuries, and occupational and work-related diseases (the cure and rehabilitation principle)
- providing general health care services for workers and their families, both curative and preventive, at the workplace or from nearby facilities (the general primary health care principle).
Such principles can still be considered to be relevant with respect to the new developments in countries’ policies and legislation. On the other hand, the formulation of objectives of occupational health practice as they stand on recent national laws and the development of new needs for working life seem to emphasize the following trends (WHO 1995a, 1995b; Rantanen, Lehtinen and Mikheev 1994):
- The scope of occupational health is expanding to cover not only health and safety but also psychological and social well-being and the ability to conduct socially and economically productive life.
- The full range of objectives extends beyond the scope of traditional occupational health and safety issues.
- The new principles go beyond the mere prevention and control of effects adverse to the health and safety of workers to the positive promotion of health, the improvement of the working environment and work organization.
Thus, there certainly exists a tendency for expansion of the scope of the objectives of occupational health practice towards new types of issues entailing social and economic consequences for workers.
Functions and Activities of Occupational Health Services
To protect and promote the health of workers, an occupational health service has to meet the special needs of the enterprise it serves and the workers employed in it. With the enormous range and scope of industrial, manufacturing, commercial, agricultural and other economic activities, it is not possible to lay down a detailed programme of activity or pattern of organization and conditions of operation for an occupational health service which should be suitable for all enterprises and in all circumstances. According to the ILO Occupational Safety and Health Convention (No. 155) and the ILO Occupational Health Services Convention (No. 161), the prime responsibility for health and safety of workers rests with the employers. The functions of an occupational health service are to protect and promote the health of workers, improve working conditions and the working environment and maintain the health of the enterprise as a whole by providing occupational health services to workers and expert advice to the employer on how to achieve the highest possible standards of health and safety in the interests of the particular working community of which it is a part.
ILO Convention No. 161 and its accompanying Recommendation No. 171 envisage occupational health services as multidisciplinary, comprehensive and, although essentially preventive, also allow for carrying out curative activities. The WHO documents calling for services for small-scale enterprises, the self-employed and agricultural workers encourage the provision of services by primary health care units (Rantanen, Lehtinen and Mikheev 1994). The documents described above and national laws and programmes recommend a stepwise implementation so that the occupational health activities can be adjusted to the national and local needs and the prevailing circumstances.
Ideally, an occupational health service should establish and act in accordance with a programme of activities adapted to the needs of the enterprise where it operates. Its functions should be adequate and appropriate to the occupational hazards and health risks of the enterprise it serves, with particular attention given to the problems specific to the branch of economic activity concerned. The following represent the basic functions and most typical activities of an occupational health service.
Preliminary orientation to the enterprise
If occupational health services have not been previously provided or when new occupational health service staff members are recruited, a preliminary orientation to the occupational safety and health situation of the enterprise is needed. This involves the following steps:
- Analysis of the type of production will indicate the types of hazards typical for the economic activity, work or occupation which therefore may be expected to be encountered in the enterprise and can help identify those that may call for special attention.
- Review of problems that have been identified by occupational health professionals, management, workers or other specialists, and occupational health measures that have previously been undertaken at the workplace will indicate the perception of the problems by the enterprise. This should include examination of reports of occupational health and safety activities, industrial hygiene measurements, biological monitoring data and so on.
- Review of the characteristics of the workforce (i.e., numbers by age, sex, ethnic background, family relations, occupational classifications, work history and, if available, related health issues) will help to identify vulnerable groups and those with special needs.
- Available data on occupational diseases and accidents and sickness absenteeism grouped, if possible, by department, occupation and type of work, causative factors and the type of injury or disease should be examined.
- Data on working methods, chemical substances handled at work, recent exposure measurements and the numbers of workers exposed to special hazards are needed for the identification of the priority problems.
- The knowledge by employees of occupational health problems, the extent of their training in emergency measures and first-aid, and the prospects for an effective occupational safety and health committee should be explored.
- Finally, pending plans for changes in production systems, installation of new facilities, machinery and equipment, introduction of new materials and changes in the organization of work should be examined as a basis for changing the occupational health practice in the future.
Surveillance of the working environment
The quality of the working environment through compliance with safety and health standards has to be ensured by surveillance at the workplace. According to ILO Convention No. 161, surveillance of the working environment is one of the main tasks of the occupational health services.
On the basis of the information obtained through the preliminary orientation to the enterprise, a walk-through survey of the workplace is conducted, preferably by a multidisciplinary occupational health team supplemented by employers’ and workers’ representatives. This should include interviews with managers, foremen and workers. When needed, special safety, hygiene, ergonomic or psychological checks can be performed.
Special checklists and guidelines are available and are recommended for such surveys. The observations may indicate a need for specific measurements or checks which should be performed by specialists in occupational hygiene, ergonomics, toxicology, safety engineering or psychology who may be members of the occupational health team of the enterprise or may have to be procured externally. Such special measurements or checks may be beyond the resources of small-scale enterprises, which would have to rely on observations made during the survey supplemented by qualitative or, in the best case, by semi-quantitative data as well.
As a basic checklist for the identification of potential health hazards, the List of Occupational Diseases (amended 1980) appended to the ILO Employment Injury Benefits Convention, 1964 (No. 121), may be recommended. It lists the major known causes of occupational diseases, and although its main purpose is to provide guidance for compensation of occupational diseases, it can also serve for their prevention. Hazards not mentioned in the list can be added according to national or local conditions.
The scope of surveillance of the working environment as defined by the ILO Occupational Health Services Recommendation (No. 171) is as follows:
- identification and evaluation of the environmental factors which may affect the workers’ health
- assessment of conditions of occupational hygiene and factors in the organization of work which may give rise to risks for the health of workers
- assessment of collective and personal protective equipment
- assessment where appropriate, by valid and generally accepted monitoring methods, of exposure of workers to hazardous agents
- assessment of control systems designed to eliminate or reduce exposure.
As a result of the walk-through survey a hazard inventory should be prepared, identifying each hazard inherent in the enterprise. This inventory is necessary for estimating a potential for exposure and suggesting control measures. For purposes of this inventory and to facilitate designing, implementing and evaluating of controls, hazards should be cross-classified by the risks they present for workers’ health with acute or chronic outcomes and by type of hazard (i.e., chemical, physical, biological, psychological or ergonomic).
The next step is a quantitative assessment of exposure, which is necessary for more exact health hazard evaluation. It consists of measuring the intensity or concentration, the variation in time, the total duration of exposure, as well as the number of workers exposed. Measurement and evaluation of exposure are usually conducted by occupational hygienists, ergonomists and specialists in injury control. They are based on the principles of environmental monitoring and should include, where necessary, ambient monitoring to collect data on exposure in a given working environment, and personal exposure monitoring of an individual worker or a group of workers (e.g., exposed to specific hazards). Measurement of exposure is necessary whenever hazards are suspected or reasonably predictable, and should be based on the completed hazard inventory combined with an assessment of work practices. Knowledge of potential effects caused by each hazard should be used to establish priorities for intervention.
The evaluation of health hazards in the workplace should be accomplished by considering the complete picture of exposures in comparison with established occupational exposure standards. Such standards are expressed in terms of permissible levels and exposure limits and are set up through numerous scientific studies correlating exposure with produced health effects. Some of them have become state standards and are legally enforceable according to national law and practice. Examples are Maximum Allowable Concentrations (MAKs in Germany, MACs in the East European countries) and Permissible Exposure Limits (PELs, United States). There are PELs for about 600 chemical substances commonly found in the workplace. There are also limits on time-weighted average exposure, short-term exposure limits (STELs), ceilings, and for some hard conditions that might result in skin absorption.
Surveillance in the working environment includes monitoring both the hazardous exposures and the health outcomes. If exposure to hazards is excessive, it should be controlled regardless of outcome, and the health of exposed workers should be evaluated. Exposure is considered excessive if it approaches or exceeds established limits such as those mentioned above.
Surveillance of the work environment provides information on the occupational health needs of the enterprise and indicates the priorities for preventive and control actions. Most of the instruments guiding occupational health services emphasize the need to carry out the surveillance before initiating services, periodically during the course of the activities, and always when substantial changes in work or the working environment have taken place.
The results obtained provide the necessary data to estimate whether preventive actions taken against health hazards are effective, as well as whether workers are placed in jobs adequate to their capacities. These data are also used by the occupational health service to ensure that reliable protection against exposures is maintained and to formulate advice on how to implement controls in order to improve the working environment. In addition, the accumulated information is used for epidemiological surveys, for the revision of permissible exposure levels, as well as for the evaluation of the effectiveness of the engineering control measures and other methods of various preventive programmes.
Informing employer, enterprise managementand workers about occupational health hazards
As information about potential workplace health hazards is obtained, it should be communicated to those responsible for implementing preventive and control measures as well as to the workers exposed to these hazards. The information should be as precise and quantitative as possible, describing the preventive measures being taken and explaining what the workers should do to ensure their effectiveness.
The ILO Occupational Health Services Recommendation, 1985 (No. 171) provides that in accordance with national law and practice, data resulting from surveillance of the working environ-ment should be recorded in an appropriate manner and be available to the employer, the workers and their representatives, or to the safety and health committee, where one exists. These data should be used on a confidential basis solely to provide guidance and advice on measures to improve the working en-vironment and the safety and health of workers. The competent authority should also have access to these data. They may be communicated to others by the occupational health service only with the agreement of the employer and the workers. Workers concerned should be informed in an adequate and appropriate manner of the results of the surveillance and should have the right to request the monitoring of the working environment.
Assessment of health risks
To assess occupational health risks, information from surveillance of the work environment is combined with information from other sources, such as epidemiological research on particular occupations and exposures, reference values like occupational exposure limits and available statistics. Qualitative (e.g., whether the substance is carcinogenic) and, where possible, quantitative (e.g., what is the degree of exposure) data may demonstrate that workers face health hazards and indicate a need for preventive and control measures.
The steps in an occupational health risk assessment include:
- identification of occupational health hazards (performed as a result of surveillance of the working environment)
- analysis of how the hazard may affect the worker (ways of entry and type of exposure, threshold limit values, dose-response relationships, adverse health effects it may cause and so on)
- identification of workers or group of workers exposed to specific hazards
- identification of individuals and groups with special vulnerabilities
- evaluation of available hazard prevention and control measures
- making conclusions and documenting the findings of the assessment
- periodic review and, if necessary, reassessment.
Surveillance of workers’ health
Due to limitations of a technological and economic nature, it is often not possible to eliminate all health hazards in the workplace. It is in these circumstances that surveillance of workers’ health plays a major role. It comprises many forms of medical evaluation of health effects developed as a result of workers’ exposure to occupational health hazards.
The main purposes of health examinations are to assess the fitness of a worker to carry out certain jobs, to assess any health impairment which may be related to the exposure to harmful agents inherent in the work process and to identify cases of occupational diseases in accordance with national legislation.
Health examinations cannot protect workers against health hazards and they cannot substitute for appropriate control measures, which have the first priority in the hierarchy of actions. Health examinations help to identify conditions which may make a worker more susceptible to the effects of hazardous agents or detect early signs of health impairment caused by these agents. They should be conducted in parallel with surveillance of the working environment, which provides information on potential exposure in the workplace and is used by occupational health professionals to assess results obtained through health surveillance of the exposed workers.
Health surveillance of workers may be passive and active
In case of passive health surveillance, ill or affected workers are required to consult occupational health professionals. Passive surveillance usually detects only symptomatic disease and requires that occupational health professionals be able to differentiate the effects of occupational exposures from the similar effects of non-occupational exposures.
In case of active health surveillance, occupational health professionals select and examine workers who are at high risk of work-related disease or injury. It may be conducted under many forms, including periodic medical examinations for all workers, medical examinations for workers exposed to specific health hazards, screening and biological monitoring of selected groups of workers. Specific forms of health surveillance depend largely upon possible health effects resulting from a particular occu-pational exposure. Active surveillance is more appropriate for workers with a history of multiple exposures and those at higher risk for disease or injury.
Details about health surveillance are given in the ILO Convention No. 161 and Recommendation No. 171. These instruments specify that surveillance of workers’ health should include, in the cases and under the conditions specified by the competent authority, all assessments necessary to protect the health of workers, which may include:
- health assessment of workers before their assignment to specific tasks which may involve a danger to their health or that of others
- health assessment at periodic intervals during employment which involves exposure to a particular hazard to health
- health assessment on resumption of work after a prolonged absence for health reasons, for the purposes of determining possible occupational causes, recommending appropriate action to protect the workers and determining the workers’ suitability for the job and needs for assignment and rehabilitation
- health assessment on and after termination of assignment involving hazards which might cause or contribute to future health impairment.
Evaluation of the health status of workers is of utmost importance when occupational health practice is initiated, when new workers are recruited, when new working practices are adopted, when new technologies are introduced, when special exposures are identified, and when individual workers display health characteristics that need follow-up. A number of countries have special regulations or guidelines specifying when and how health examinations should be carried out. Health examinations should be monitored and continuously developed to identify the work-related health effects at their earliest stage of development.
Pre-assignment (pre-employment) health examinations
This type of health assessment is carried out before the job placement of workers or their assignment to specific tasks which may involve a danger to their health or that of others. The purpose of this health assessment is to determine whether a person is physically and psychologically fit to perform a particular job and to ensure that his or her placement in this job will not represent a danger to his or her health or to the health of other workers. In most instances, a review of the medical history, a general physical examination and routine laboratory tests (e.g., simple blood count and urinalysis) will suffice, but in some cases the presence of a health problem or the unusual requirements of a particular job will require extensive functional examinations or diagnostic testing.
There are a number of health problems that may make a certain job hazardous for the worker or incur a risk for the public or other workers. For these reasons, it may be necessary, for example, to exclude workers with uncontrolled hypertension or unstable diabetes from certain hazardous jobs (e.g., air and sea pilots, drivers of public service and heavy goods vehicles, crane drivers). Colour blindness may justify an exclusion from jobs requiring colour discrimination for safety purpose (e.g., reading traffic signals). In jobs demanding a high standard of general fitness like deep-water diving, fire fighting, police service and aircraft piloting, only workers able to meet the performance requirements would be acceptable. A possibility that chronic diseases may be aggravated by the exposures involved in a particular job should also be considered. It is essential, therefore, that the examiner have a detailed knowledge of the job and the work environment and be aware that standardized job descriptions may be too superficial or even misleading.
After finishing a prescribed health assessment, the occupational physician should communicate the results in writing to both the worker and the employer. These conclusions communicated to the employer should contain no information of a medical nature. They should contain a conclusion about the fitness of the examined person for the proposed or held assignment and specify the kinds of jobs and the conditions of work which are medically contra-indicated either temporarily or permanently.
The pre-employment medical examination is important to the worker’s subsequent occupational history since it provides the necessary clinical information and laboratory data on the worker’s health status at the moment of entering the employment. It also represents an indispensable baseline for the subsequent evaluation of any changes in health status that may occur later on.
Periodic health examinations
These are performed at periodic intervals during employment which involves exposure to potential hazards that could not be entirely eliminated by preventive and control measures. The purpose of periodic health examinations is to monitor the health of workers during the course of their employment. It aims at verifying workers’ fitness in relation to their jobs and at detecting as early as possible any sign of ill-health which may be due to work. They are often supplemented by other examinations in accordance with the nature of hazards observed.
Their objectives include:
- identifying as early as possible any adverse health effects caused by work practices or exposures to potential hazards
- detecting the possible onset of an occupational disease
- verifying whether the health of an especially vulnerable or chronically ill worker is being adversely affected by the work or the work environment
- monitoring personal exposure with the help of biological monitoring
- checking the effectiveness of preventive and control measures
- identifying possible health effects of changes in the working practices, technology or substances used in the enterprise.
These objectives will determine the frequency, content and methods of the periodic health examinations, which may be conducted as frequently as every one to three months or every few years, depending on the nature of the exposure, the biological response expected, the opportunities for preventive measures and the feasibility of the examination method. They may be comprehensive or limited to just a few tests or determinations. Special guidelines on the purpose, frequency, content and methodology of these examinations are available in a number of countries.
Return-to-work health examinations
This type of health assessment is required to authorize the resumption of work after a long absence for health reasons. This health examination determines the workers’ suitability for the job, recommends appropriate actions to protect them against future exposures, and identifies whether there is a need for a reassignment or a special rehabilitation.
Similarly, when a worker changes jobs, the occupational physician is required to certify that the worker is fit to carry out the new duties. The objective of the examination, the need and the use of the results determine its content and methods and the context in which it is performed.
General health examinations
In many enterprises, general health examinations may be performed by the occupational health service. They are usually voluntary and may be available to the entire workforce or only to certain groups determined by age, length of employment, status in the organization and so on. They may be comprehensive or limited to screenings for particular diseases or health risks. Their objectives determine their frequency, contents and methods used.
Health examinations after the ending of service
This type of health assessment is performed after the termination of assignment involving hazards which could cause or contribute to future health impairment. The purpose of this health assessment is to make a final evaluation of workers’ health, compare it with previous medical examinations and to assess how the prior job assignments may have affected their health.
General observations
The general observations summarized below apply to all types of health examinations.
Health examinations of workers should be conducted by professionally qualified personnel trained in occupational health. These health professionals should be familiar with the exposures at work, physical requirements and other conditions of work in the enterprise and experienced in using appropriate medical examination techniques and instruments, as well as in keeping correct record forms.
The health examination is not a substitute for action to prevent or control hazardous exposures in the working environment. If prevention has been successful, fewer examinations are needed.
All data collected in connection with health examinations are confidential and should be recorded by the occupational health service in a personal confidential health files. Personal data relating to health assessments may be communicated to others only with the informed consent of the worker concerned. When the worker wishes the data to be forwarded to a personal physician, he or she provides formal permission for this.
Conclusions about the suitability of a worker for a particular job or about the health effects of the job should be communicated to the employer in a form that does not violate the principle of the confidentiality of personal health data.
Use of health examinations and their results for any kind of discrimination against workers cannot be tolerated and must be strictly prohibited.
Initiatives for preventive and control measures
Occupational health services are responsible not only for the identification and evaluation of potential risks for the health of workers but also for providing advice on preventive and control measures which will help to avoid risks.
After analysing the results of surveillance of the working environment, including where necessary workers’ personal exposure monitoring, and the results of workers’ health surveillance, including where necessary the results of biological monitoring, occupational health services should be in a position to assess possible connections between the exposure to occupational hazards and resulting health impairments and to propose appropriate control measures to protect workers’ health. These measures are recommended together with other technical services in the enterprise after consulting the enterprise management, employers, workers or their representatives.
Control measures should be adequate to prevent unnecessary exposure during normal operating conditions as well as during accident and emergencies. Planned modifications in work processes should also be taken into account, and recommendations should be adaptable to future needs.
Measures of control of health hazards are used to eliminate occupational exposure, minimize or in any case reduce it to permissible limits. They include primarily engineering, engineering controls in the work environment, changes in technology, substances and materials and as secondary preventive measures, human behaviour controls, personal protective equipment, integrated control and others.
The formulation of recommendations for control measures is a complicated process that includes the analysis of information on existing health risks in the enterprise and the consideration of occupational safety and health requirements and needs. For analysis of feasibility and costs versus benefits one should consider the fact that the investments made for health and safety may pay back during long periods in the future, but not necessarily immediately.
The ILO instruments include a requirement that the employers, workers and their representatives should cooperate and participate in the implementation of such recommendations. They are usually discussed by the safety and health committee at large-scale enterprises, or in smaller enterprises by the representatives of the employers and workers. It is important to document the proposed recommendations so that there can be a follow-up of their implementation. Such documentation should emphasize the responsibility of management for preventive and control actions at the enterprise.
Advisory role
Occupational health services have an important task to perform by providing advice to the enterprise management, the employers, the workers, and health and safety committees in their collective as well as individual capacities. This needs to be recognized and used in the decision-making processes as it often happens that occupational health professionals are not directly involved in the decision-making.
The ILO Occupational Health Services Convention (No. 161) and Recommendation (No. 171) promote the advisory role of occupational health professionals in the enterprise. To promote the adaptation of work to the workers and improve working conditions and environment, occupational health services should act as advisers on occupational health, hygiene, ergonomics, collective and individual protective equipment to the employers, the workers and their representatives in the enterprise, and to the safety and health committee, and should collaborate with other services already operating as advisers in these fields. They should advise on the planning and organization of work, the design of workplaces, on the choice, maintenance and condition of machinery and other equipment, as well as on the substances and materials used in the enterprise. They should also participate in the development of programmes for the improvement of working practices, as well as in the testing and evaluation of health aspects of new equipment.
Occupational health services should provide workers with personal advice concerning their health in relation to work.
Another important task is to provide advice and information related to the integration of workers who have been victims of work accidents or diseases in order to help them in their rapid rehabilitation, protect their working capacity, reduce absenteeism and restore a good psychosocial climate in the enterprise.
Educational and training activities are closely linked to the advisory task that occupational health professionals perform vis-à-vis the employers and workers. They are of particular importance when the modification of existing installations or the introduction of new equipment are envisaged, or when there may be changes in the layout of workplaces, workstations and in the organization of work. Such activities have an advantage when started at the right time because they provide for better consideration of human factors and ergonomic principles in the improvement of working conditions and environment.
Technical advisory services at the workplace constitute an important preventive function of occupational health services. They should give priority to the awareness of occupational hazards and to the involvement of the employers and workers in hazard control and the improvement of the working environment.
First aid services and emergency preparedness
The organization of first aid and emergency treatment is a tradi-tional responsibility of occupational health services. ILO Convention No. 161 and Recommendation No. 171 stipulate that the occupational health service should provide first aid and emergency treatment in cases of accident or indisposition of workers at the workplace and should collaborate in the organization of first aid.
This covers preparedness for accidents and acute health conditions in individual workers, as well as readiness for response in collaboration with other emergency services in cases of serious accidents affecting the entire enterprise. Training in first aid is a primary duty of occupational health services, and the personnel of these services are among the first to respond.
The occupational health service should make appropriate preliminary arrangements for ambulance services and with community fire, police and rescue units and local hospitals in order to avoid delays and confusion that may threaten the survival of critically injured or affected workers. These arrangements, supplemented by drills when feasible, are particularly important in preparing for major emergencies such as fire, explosions, toxic emissions and other catastrophes that may involve many individuals in the enterprise as well as in the neighbourhood and may result in a number of casualties.
Occupational health care, general preventiveand curative health services
Occupational health services may be involved in the diagnosis, treatment and rehabilitation of occupational injuries and diseases. The knowledge of occupational diseases and injuries coupled with the knowledge of the job, the working environment and occupational exposures present in the workplace enable the occupational health professionals to play a key role in the management of work-related health problems.
According to the scope of activities and as required by national legislation or based on national practice, occupational health services fall into three main categories:
- occupational health services with essentially preventive functions, including mainly workplace visits, health examinations and the provision of first-aid
- occupational health services with preventive functions supplemented by selective curative and general health care services
- occupational health services with a wide range of activities including both preventive and comprehensive curative and rehabilitation activities.
The ILO Occupational Health Services Recommendation (No. 171) promotes the provision of curative and general health care services as functions of occupational health services where they are found to be appropriate. Based on national legislation and practice, the occupational health service may undertake or participate in one or more of the following curative activities with regard to occupational illnesses:
- treatment of workers who have not stopped work or who have resumed work after an absence
- treatment of workers with occupational diseases or health impairments aggravated by work
- treatment of victims of occupational accidents and injuries
- medical aspects of vocational re-education and rehabilitation.
The provision of general preventive and curative health care services includes the prevention and treatment of non-occupational illnesses and other relevant primary health care services. Usually, general preventive health care services include immunizations, maternity and child care, general hygiene and sanitary services, whereas general curative health care services include conventional general-practitioner-level practice. Here, ILO Recommendation No. 171 prescribes that the occupational health service may, taking into account the organization of preventive medicine at the national level, fulfil the following functions:
- carry out immunizations in respect of biological hazards in the working environment
- take part in campaigns aimed at the protection of workers’ health
- collaborate with the health authorities within the framework of public health programmes.
Occupational health services set up by large enterprises, as well as those operating in remote or medically underserved areas, may be called upon to provide general non-occupational health care not only for workers but for their families as well. The extension of such services depends on the infrastructure of the health services in the community and on the capacity of the enterprises. When industrial enterprises are established in poorly developed areas, it may even be expedient to provide such services together with occupational health care.
In some countries, occupational health services provide ambulatory treatment during working hours which is normally provided by a general practitioner. It usually concerns simple forms of treatment, or it may be more comprehensive medical care if the enterprise has an agreement with the social security or other insurance institutions providing reimbursement of the cost of workers’ treatment.
Rehabilitation
The participation of occupational health services is particularly crucial in guiding workers’ rehabilitation and their return to work. This is becoming more and more important owing to a large number of occupational accidents in developing countries and the ageing of the working populations in industrialized societies. Rehabilitation services are usually provided by external units which may be free-standing or hospital-based and staffed by rehabilitation specialists, occupational therapists, vocational counsellors and so on.
There are some important aspects concerning the participation of occupational health services in the rehabilitation of injured workers.
First, the occupational health service may play an important role in seeing that workers recovering from injury or disease are referred to them promptly. It is greatly preferable, when practicable, for a worker to return to his or her original place of employment, and it is an important function of the occupational health service to maintain contact during the period of incapacity with those responsible for treatment during the acute stages in order to identify the time when a return to work can be envisaged.
Second, the occupational health service can facilitate an early return to work by collaborating with the rehabilitation unit in planning. Its knowledge of the job and work environment will be helpful in exploring the possibilities of modifying the original job (e.g., changes in work assignment, limited hours, rest periods, special equipment and so on) or arranging an alternative temporary substitute.
Finally, by following the worker’s progress, the occupational health service can keep management informed of the probable duration of absence or limited capacity, or the extent of any residual disability, so that arrangements for alternative staffing may be made with minimal impact on production schedules. On the other hand, the occupational health service maintains a link with the workers and often with their families, facilitating and better preparing their return to work.
Adaptation of work to the workers
To facilitate the adaptation of work to the workers and improve the working conditions and environment, occupational health services should advise the employer, the workers and the safety and health committee in the enterprise on matters of occupational health, occupational hygiene and ergonomics. Recommendations may include modifications of the job, the equipment and the working environment that will allow the worker to perform effectively and safely. This may involve reducing the physical workload for an ageing worker, providing special equipment for workers with sensory or locomotor impairments or fitting equipment or work practices to the anthropometric dimensions of the worker. The adaptations may be required temporarily in the case of workers recovering from an injury or disease. A number of countries have legal provisions requiring workplace adaptations.
Protection of vulnerable groups
The occupational health service is responsible for recommendations that will protect vulnerable groups of workers, such as those with hypersensitivities or chronic diseases and those with certain disabilities. This may include selection of a job that minimizes adverse effects, provision of special equipment or protective devices, prescription of sick leave and so on. The recommendations must be feasible in the light of the circumstances in a particular workplace, and workers may be required to undertake special training in appropriate working practices and the use of personal protective equipment.
Information, education and training
Occupational health services should play an active role in providing relevant information and organizing education and training in relation to work.
The ILO Occupational Health Services Convention (No. 161) and Recommendation (No. 171) provide for the participation of occupational health services in designing and implementing programmes of information, education and training in the field of occupational safety and health for the personnel of the enterprise. They should participate in the progressive and continuing training of all workers in the enterprise who contribute to occupational safety and health.
Occupational health professionals can help increase workers’ awareness of occupational hazards to which they are exposed, discuss with them existing health risks and advise workers on the protection of their health, including protective measures and proper use of personal protective equipment. Every contact with workers offers an opportunity to provide useful information and to encourage healthful behaviour in the workplace.
Occupational health services should provide all information on occupational hazards present in the enterprise as well as on safety and health standards relevant to the local situation. This information should be written in language understandable by the workers. It should be provided on a periodic basis and especially when new substances or equipment are being introduced or changes are being made in the working environment.
Education and training can play a key role in the improvement of working conditions and environment. Efforts to improve safety, health and welfare at work are often substantially limited due to lack of awareness, technical expertise and know-how. Education and training in specific fields of occupational safety and health and working conditions can facilitate both the diagnosis of problems and the implementation of solutions, and can therefore help overcome these limitations.
ILO Conventions Nos. 155 and 161 and their accompanying Recommendations emphasize the key role of education and training in the enterprise. Training is essential to fulfil the obligations of both the employers and the workers. Employers are responsible for the organization of in-plant occupational safety and health training, and workers and their representatives in the enterprise should fully cooperate with them in this respect.
Training in occupational safety and health should be organized as an integral part of the overall efforts for improving working conditions and environment, and occupational health services should play a major role in this respect. It should aim at solving various problems affecting the physical and mental well-being of workers and should address adaptation to technology and equipment, improvement of working environment, ergonomics, working time arrangements, the organization of work, job content and workers’ welfare.
Health promotion activities
There is some tendency, particularly in North America, to incorporate wellness promotion activities in the form of occupational health programmes. These programmes are, however, essentially general health promotion programmes that may include such elements as health education, stress management and assessment of health risks. They usually aim at changing personal health practices such as alcohol and drug abuse, smoking, diet and physical exercise, with a view to improving overall health status and reducing absenteeism. Although such programmes are supposed to improve productivity and reduce health care costs, they have not been properly evaluated so far. These programmes, designed as health promotion programmes, though valuable as such are not usually considered as occupational health programmes, but as public health services delivered in the workplace, because they focus attention and resources on personal health habits rather than on protection of workers against occupational hazards.
It should be recognized that the implementation of health promotion programmes is an important factor contributing to the improvement of the health of workers in the enterprise. In some countries, “health promotion in the workplace” is regarded as a separate discipline on its own and is carried out by completely independent groups of health workers other than occupational health professionals. In this case, their activities should be coordinated with the activities of the occupational health service, whose staff can ensure their relevance, feasibility and sustainable effect. The participation of occupational health services in the realization of health promotion programmes should not limit the performance of their main functions as specialized health services created to protect workers against harmful exposures and unhealthy working conditions in the workplace.
A very recent development in some countries (e.g., the Netherlands, Finland) is the establishment of occupational health promotion activity within occupational health services. Such activities aim at promotion and maintenance of work ability of workers by targeting early prevention and promotion actions to workers and their health, to work environment, and to work organization. The results of such activities are found to be highly positive.
Data collection and record-keeping
It is important that all medical contacts, evaluations, assessments and surveys be properly documented and the records safely stored so that, if necessary for follow-up health examinations, legal or research purposes, they may be retrieved years and even decades later.
The ILO Occupational Health Services Recommendation (No. 171) provides that occupational health services should record data on workers’ health in personal confidential files. These files should also contain information on jobs held by the workers, on exposure to occupational hazards involved in their work, and on the results of any assessment of workers’ exposure to these hazards. Personal data relating to health assessments may be communicated to others only with the informed consent of the worker concerned.
The conditions under which and time during which records containing workers’ health data should be kept, communicated or transferred, and the measures necessary to keep them confidential, especially when these data are computerized, are usually prescribed by national laws or regulations or by the competent authority, and governed by recognized ethical guidelines.
Research
According to the ILO Occupational Health Services Recommendation (No. 171), occupational health services, in consultation with the employers’ and workers’ representatives, should contribute to research within the limits of their resources by participating in studies in the enterprise or in the relevant branch of economic activity (e.g., to collect data for epidemiological purposes or participate in national research programmes). Occupational physicians involved in the implementation of research projects will therefore be bound by the ethical considerations applied to such projects by the World Medical Association (WMA) and the Council for International Organizations of Medical Sciences (CIOMS). Research in the working environment may involve healthy “volunteers”, and the occupational health service should fully inform them about the purpose and the nature of the research. Each participant should give individual consent to the participation in the project. The collective consent provided by the workers’ trade union in the enterprise is not enough. Workers must feel free to withdraw from the investigation at any time and the occupational health service should be responsible that they will not be subjected to undue pressure to remain within the project against their will.
Liaison and Communications
A successful occupational health service is necessarily involved in communications of many kinds.
Internal collaboration
The occupational health service is an integral part of the productive apparatus of the enterprise. It must closely coordinate its activities with occupational hygiene, occupational safety, health education and health promotion, and other services directly related to workers’ health, when these operate separately. In addition, it must collaborate with all services in the operation in the enterprise: personnel administration, finance, employee relations, planning and design, production engineering, plant maintenance and so on. There should be no obstacles in reaching out to any department in the enterprise when issues of worker health and safety are involved. At the same time, the occupational health service should be responsive to the needs and sensitive to the constraints of all other departments. And, if it does not report to a most senior executive, it must have the privilege of direct access to top management in cases when important recommendations relating to workers’ health are denied appropriate consideration.
In order to function effectively, the occupational health service needs the support of the enterprise management, the employer, workers and their representatives. The ILO instruments (ILO 1981a, 1981b, 1985a, 1985b) require the employer and the workers to cooperate and participate in the implementation of the organizational and other measures relating to occupational health services on an equitable basis.
The employer should collaborate with the occupational health service in achieving its objectives particularly by:
- providing general information about occupational health and safety in the enterprise
- providing information on any known or suspected factors that might affect the workers’ health
- providing the occupational health service with adequate resources in terms of facilities, equipment and supplies, and qualified staff
- providing appropriate authority to enable the occupational health service to perform its functions
- allowing free access to all parts and facilities of the enterprise (including separate plants and field units) and providing information about plans for changes in production equipment and supplies, as well as work processes and the organization of work, so that preventive measures can be taken before workers are exposed to any potential hazards
- giving prompt consideration to any recommendations made by the occupational health service for the control of occupational hazards and the protection of workers’ health, and ensuring their implementation
- safeguarding the professional independence of occupational health professionals, encouraging and, where possible, subsidizing their continuing education and training.
Where a special plant-level programme for occupational health activities is required, the collaboration between the employer and the occupational health service is crucial in the preparation of such a programme and the activity report.
Occupational health services are established to protect and promote workers’ health by preventing work injuries and occupational diseases. Many functions of occupational health services cannot be carried out without cooperation with workers. According to the ILO instruments, workers and their organizations should cooperate with occupational health services and provide support to these services in the execution of their duties (ILO, 1981a, 1981b, 1985a, 1985b). The workers should cooperate with occupational health services in particular by:
- informing the occupational health service about any known or suspected factors in the work and the work environment that may have adverse effects on their health
- assisting occupational health staff in performing their duties in the workplace
- participating in health examinations, surveys and other activities conducted by the occupational health service
- obeying health and safety rules and regulations
- maintaining safety equipment and personal protective devices as well as first aid supplies and emergency equipment, and learning to use them properly
- participating in health education and safety training exercises in the workplace
- reporting on the effectiveness of occupational safety and health measures
- participating in the organization, planning, implementation and evaluation of activities of occupational health services.
The ILO instruments recommend the collaboration between the employers and workers on matters of occupational safety and health (ILO 1981a,1981b,1985a,1985b). This collaboration is carried out in the occupational safety and health committee of the enterprises, which comprises the representatives of workers and the employer and constitutes a forum for the discussion of matters relating to occupational health and safety. The establishment of such a committee may be prescribed by legislation or collective agreements in enterprises with 50 or more workers. In smaller enterprises, its functions are intended to be fulfilled by less formal discussions between the workers’ safety delegates and the employer.
The committee has a broad range of functions (ILO 1981b) which may include:
- participating in decisions regarding the establishment, organization, staffing and operation of the occupational health service
- contributing to the occupational health and safety programme of the enterprise
- providing support to the occupational health service in the performance of its duties
- participating in the evaluation of the activities of the occupational health service and contributing to its reports submitted to subsidizing bodies, enterprise management and external authorities
- facilitating the communication of information on occupational health and safety matters between different services in the enterprise
- providing a forum for discussions and decisions on collaborative actions in the enterprise regarding matters of occupational safety and health
- evaluating the overall status of occupational health and safety in the enterprise.
The principle of workers’ participation in decisions concerning their own health and safety, on changes in jobs and working environments, and on safety and health activities is emphasized in recent guidelines on occupational health practice. It also requires that workers should have access to information on the activities of the enterprise concerning occupational safety and health and on any potential health hazard that they may encounter at the workplace. Accordingly, the principle of “right to know” and transparency principles have been established or strengthened by legislation in many countries.
External collaboration
Occupational health services should establish close relations with external services and institutions. Foremost among these are relationships with the public health care system of the country as a whole and the institutions and facilities in the local communities. This starts at the level of primary health care units and extends to the level of hospital-based specialized services, some of which may also be providing occupational health services. Such relationships are important when it is necessary to refer workers to specialized health services for appropriate evaluation and treatment of occupational injuries and diseases, and also to provide opportunities for mitigating the possible adverse effects of non-occupational health problems on attendance and work performance. Collaboration with public health as well as environmental health services is important. Inviting general practitioners and other health professionals to visit the occupational health service and familiarize themselves with the demands made on their patients by occupations or the hazards to which they are exposed will not only help to establish friendly relations, but also provide an opportunity to sensitize them to the particulars of occupational health issues that ordinarily would be ignored in their treatment of workers for whom they provide general health care services.
Rehabilitation institutes are a frequent collaborative partner, particularly in the case of workers with handicaps or chronic disabilities who may require special efforts to enhance and maintain their work capacities. Such collaboration is especially important in recommending temporary job modifications that will accelerate and facilitate the return to work of individuals recovering from serious injuries or illnesses, with occupational or non-occupational aetiology.
Emergency response organizations and first aid providers such as ambulance services, hospital outpatient and emergency clinics, poison control centres, police and fire brigades, and civic rescue organizations can ensure the expeditious treatment of acute injuries and illnesses and assist in planning for and response to major emergencies.
Appropriate links with social security and health insurance institutions can facilitate the administration of benefits and functioning of the workers’ compensation system.
The competent safety and health authorities and labour inspectorates are key collaborative partners for the occupational health services. In addition to expediting formal inspections, appropriate relationships may provide support for internal occupational health and safety activities and offer opportunities to input to the formulation of regulations and methods of enforcement.
Participation in professional societies and in activities of educational/training institutes and universities is valuable for arranging continuing education for professional staff members. Ideally, the time and expenses should be subsidized by the enterprise. In addition, the collegial contacts with occupational health professionals serving other enterprises can provide strategic information and insights and may lead to partnerships for meaningful data collection and research.
The kinds of collaboration described above should be initiated from the very beginning of the operation of the occupational health service and be continued and expanded as appropriate. They may not only facilitate achievement of the objectives of the occupational health service, but may also contribute to the community and public relations efforts of the enterprise.
Infrastructures for Occupational Health Services
Infrastructures for the provision of occupational health services are insufficiently developed in most parts of the world, including developed and developing countries. The need for occupational health services is particularly acute in the developing and newly industrialized countries, which contain eight out of ten of the world’s workers. If organized appropriately and effectively, such services would contribute significantly not only to workers’ health, but also to the overall socio-economic development, productivity, environmental health, and the well-being of countries, communities and families (WHO 1995b; Jeyaratnam and Chia 1994). Effective occupational health services can not only reduce avoidable-sickness absenteeism and work disability, but also help to control the costs of health care and social security. Thus, the development of the occupational health services covering all workers is fully justified with regard to both workers’ health and the economy.
Infrastructures for the provision of occupational health services should permit effective implementation of activities needed to meet the objectives of occupational health (ILO 1985a, 1985b; Rantanen, Lehtinen and Mikheev 1994; WHO 1989b). To allow the necessary flexibility, Article 7 of ILO Convention No. 161 provides that occupational health services may be organized as a service for a single undertaking or as a service common to a number of undertakings. Or, in accordance with national conditions and practice, occupational health services may be organized by the undertakings or groups of undertakings concerned, public authorities or official services, social security institutions, any other bodies authorized by the competent authority, or any combination of the above.
Some countries have regulations relating the organization of occupational health services to the size of the enterprise. For example, larger enterprises have to establish their own in-plant occupational health service while medium-sized and small enterprises are required to join group services. As a rule, legislation allows flexibility in the choice of structural models of occupational health services in order to meet local conditions and practices.
Models of Occupational Health Services
To meet the occupational health needs of enterprises which vary widely with respect to type of industry, size, type of activity, structure and so on, a number of different models of occupational health services have been developed (Rantanen, Lehtinen and Mikheev 1994; WHO 1989). In developing and newly industrialized countries, for example, where health care for the general population may be deficient, the occupational health service may provide primary non-occupational health care to the employees and their families as well. This has also been successfully implemented in Finland, Sweden and Italy (Rantanen 1990; WHO 1990). On the other hand, the high level of worker coverage in Finland has been made possible by organizing municipal health centres (PHC units) providing occupational health services for workers in small-scale enterprises, the self-employed and even small worksites operated by large enterprises that are scattered throughout the country.
In-plant (in-company) model
Many large industrial and non-industrial enterprises in both the private and public sectors have an integrated, comprehensive occupational health service on their premises that not only provides a full range of occupational health services, but may also provide non-occupational health services to workers and their families, and may carry out research. These units usually have multidisciplinary staff that may include not only occupational physicians and nurses, but also occupational hygienists, ergonomists, toxicologists, occupational physiologists, laboratory and x-ray technicians, and possibly physiotherapists, social workers, health educators, counsellors and industrial psychologists. Occupational hygiene and safety services may be provided by the staff of the occupational health service or by separate units of the enterprise. Such multidisciplinary units are usually afforded only by large (often multinational) enterprises and their quality of services and impact on health and safety is most convincing.
Smaller enterprises may have an in-plant unit that is staffed by one or more occupational health nurses and a part-time occupational physician who visits the unit for several hours a day or several times a week. A variant is the unit staffed by one or more occupational health nurses with an “on-call” physician who visits the unit only when summoned and usually provides “standing orders” which authorize the nurse to perform procedures and dispense medications that are normally the prerogative of licensed physicians only. In some instances in the United States and England, these units are operated and supervised by an external contractor such as a local hospital or a private entrepreneurial organization.
Due to various reasons, the occupational health staff may sometimes become more and more separated from the central operating structure of the enterprise, and, as result, the range of services it provides tends to shrink to first aid and treatment of acute occupational injuries and illnesses and the performance of routine medical examinations. Part-time and particularly on-call physicians often do not acquire the necessary familiarity with details of the kinds of jobs being performed or the working environment, and may not have enough contact with managers and the safety committee or do not have enough authority to effectively recommend appropriate preventive measures.
As part of the reductions in workforce seen at times of recession, some large enterprises are shrinking their occupational health services and, in some instances, eliminating them entirely. The latter may occur when an enterprise with an established occupational health service is acquired by an enterprise that had not maintained one. In such cases, the enterprise may contract with external resources to operate the in-plant facility and employ consultants on an ad hoc basis to provide such specialized services as occupational hygiene, toxicology and safety engineering. Some enterprises choose to retain an expert in occupational and environmental health to serve as an in-house medical director or manager to coordinate the services of the external providers, monitor their performance, and provide advice to top management on matters relating to employee health and safety and environmental concerns.
Group or inter-enterprise model
Sharing of occupational health services by groups of small or medium-sized enterprises has been widely used in industrialized countries such as Sweden, Norway, Finland, Denmark, the Netherlands, France and Belgium. This enables enterprises that are individually too small to have their own services, to enjoy the advantages of a well-staffed, well-equipped comprehensive service. The Slough Plan, organized some decades ago in an industrial community in England, pioneered this type of arrangement. In the 1980s, interesting experiments with regional occupational health centres organized in Sweden were found to be feasible and particularly useful for mid-sized enterprises, and some countries, such as Denmark, have made efforts to increase the size of the shared units to allow them to provide a broader range of services instead of splitting them into smaller monodisciplinary units.
A frequently encountered disadvantage of the group model compared to the in-plant model of larger enterprises is the distance between the worksite and the occupational health service. This is important not only in cases requiring first aid for more serious injuries (it is sometime more prudent to send such cases directly to a local hospital, bypassing the occupational health unit) but because more time is usually lost when workers are forced to go off the premises when seeking health services during working hours. Another problem arises when the participating enterprises are unable to contribute sufficient funds to sustain the unit which is forced to close down when the government or private foundation grants that may have subsidized its start-up are no longer available.
Industry-oriented (branch-specific) model
A variant of the group model is the joint use of an occupational health service by a number of enterprises in the same industry, trade or economic activity. Construction, food, agriculture, banking and insurance are examples of sectors that have made such arrangements in Europe; such models are found in Sweden, the Netherlands and France. The advantage of this model is the opportunity for the occupational health service to concentrate on the particular industry and accumulate special competence in addressing its problems. Such a model for the construction industry in Sweden provides sophisticated, high-quality, multidisciplinary services for the entire country and has been able to conduct research and develop programmes dealing with problems specific to that industry.
Hospital outpatient clinics
Hospital outpatient clinics and emergency rooms have traditionally provided services to injured or sick workers who seek care. A notable disadvantage is the lack of familiarity with occupational diseases on the part of the usual staff and attending physicians. In some instances, as noted above, occupational health services have made arrangements with local hospitals to provide certain specialized services and fill the gap either by collaborating in the care or educating the hospital staff about the kinds of cases that may be referred to them.
More recently, hospitals have begun to operate special occupational health clinics or services that are compared favourably to the large in-plant or group services described above. They are staffed by physicians specialized in occupational health who may also conduct research involving the kinds of problems they see. In Sweden, for example, there are eight regional clinics of occupational medicine, several of which are affiliated with a university or medical college, each providing services to enterprises in several communities. Several have a special unit to serve small enterprises.
A significant difference between the group services and the hospital-based activity is that in the case of the former, the participating enterprises usually share ownership of the occupational health service and have the decision-making authority over how it operates, while the latter operates as a private or public polyclinic that has a provider-customer relationship with the client enterprises. This limits, for example, the extent to which participation and collaboration between employers and workers can influence the operation of the unit.
Private health centres
The private health centre model is a unit usually organized by a group of physicians (it may be organized by a private entrepreneurial organization that employs the physicians) to provide several types of outpatient and sometimes also hospital-based health services. The larger centres often have a multidisciplinary staff and may offer occupational hygiene and physiotherapy services, while smaller units usually supply only medical services. As in the hospital clinic model, the provider-client relationship with participating enterprises may hinder implementation of the principle of employer and worker involvement in formulating policies and procedures.
In some countries, private health centres have been criticized for being too much oriented to curative clinical services provided by the physicians. Such criticism is justified in the case of smaller centres where the services are provided by general practitioners instead of health professionals experienced in occupational health practice.
Primary health care units
Primary health care units are usually organized by municipal or other local authorities or by the national health service, and usually provide both preventive services and primary health care. This is the model strongly recommended by the WHO as a means of providing services to small-scale enterprises and, particularly, to agricultural enterprises, the informal sector and the self-employed. Since general physicians and nurses usually lack specialization and experience in occupational health, the success of this model critically depends on how much training in occupational health and occupational medicine can be arranged for the health professionals.
An advantage of this model is its good coverage of the country and its location in the communities where the people it serves work and live. This is a particular advantage in serving agricul-tural workers and the self-employed.
A weakness is its concentration on general curative health services and treatment of emergencies with only limited ability to carry out surveillance of the working environment and to institute preventive measures needed in the workplace. Experience in Finland, where large primary health care units employ teams of trained specialists to provide occupational health services is, however, highly positive. Interesting new models for providing occupational health services by primary health care units have been tried in the Shanghai area of China.
Social security model
In Israel, Mexico, Spain and some African countries, for example, occupational health services are provided by special units organized and operated by the social security system. In Israel, this model is essentially similar in structure and operation to the group model, while elsewhere it is usually oriented more to curative health care. The specific feature of this model is that it is operated by the organization responsible for workers’ compensation for occupational injuries and diseases. While curative and rehabilitative services are provided, the emphasis on controlling social security costs has led to priority being given to preventive services.
Selecting a Model for Occupational Health Services
The primary decision of whether or not to have an occupational health service may be determined by law, by a labour-management contract, or by management’s concerns about employees’ health and safety. While many enterprises are motivated toward a positive decision by awareness of the value of an occupational health service in maintaining their productive apparatus, others are impelled by such economic considerations as controlling the costs of workers’ compensation benefits, avoidable sickness absenteeism and disability, early retirement for health reasons, regulatory penalties, litigation and so on.
The model for providing occupational health services may be dictated by laws or regulations which may be general or applicable only to certain industries. This is generally the case with the social security model, in which the client enterprises have no other option.
In most instances, the model selected is determined by such factors as the size of the workforce and its demographic characteristics, the kinds of work they do and the workplace hazards they encounter, the location of the worksite(s), the kind and quality of health services available in the community and, perhaps most important, the affluence of the enterprise and its ability to provide the requisite financial support. Sometimes, an enterprise will launch a minimal unit and enlarge and expand its activities as it proves its worth and earns the acceptance of the workers. Only a few comparative studies have been conducted so far on the operation of various models of occupational health services in different situations.
Occupational hygiene services
International instruments and guidelines strongly recommend the inclusion of occupational hygiene services in the multidisciplinary occupational health service. In some countries, however, occupational hygiene is traditionally carried out as a separate and independent activity. Under such circumstances, collaboration with other services involved in occupational safety and health activities is necessary.
Safety services
Safety services are traditionally carried out as a separate activity either by safety officers or safety engineers who are employees of the enterprise (ILO 1981a; Bird and Germain 1990) or by some form of consulting arrangement. In the in-plant safety service, the safety officer is often also the chief responsible for safety in the enterprise and represents the employer in such matters. Again, the modern trend is to integrate safety along with occupational hygiene and occupational health and other services involved in occupational health activities in order to form a multidisciplinary entity.
Where safety activities are carried out in parallel with those of occupational health and occupational hygiene, the collaboration is necessary particularly as regards the identification of accident hazards, risk assessment, planning and implementation of preventive and control measures, education and training of managers, supervisors and workers, and collecting, maintaining and registering records of accidents, and the operation of any control measures that are instituted.
Staffing of the Occupational Health Service
Traditionally, the occupational health service is staffed by an occupational health physician only, or a physician and a nurse who, perhaps with the addition of an industrial hygienist, may be designated as the “core” staff. The most recent provisions, however, require that whenever possible the occupational health staff should be multidisciplinary in composition.
The staff may be enlarged to a full multidisciplinary team depending on the model of the service, the nature of the industry and the types of work involved, the availability of the various specialists or of programmes for training them, and the extent of the available financial resources. When not actually on the staff, the supplementary staff positions may be filled in by external support services (WHO 1989a, 1989b). They may include safety engineers, mental health specialists (e.g., psychologists, counsellors), work physiologists, ergonomists, physiotherapists, toxicologists, epidemiologists and health educators. Most of these are rarely included in the full-time staff of the occupational health service and are involved on a part-time or an “as needed” basis (Rantanen 1990).
Since quantitative needs for occupational health staff vary widely depending on the enterprise in question, the organization model and the services provided by the occupational health service, as well as on the availability of support and parallel services, it is not possible to be categorical about the numerical size of the staff (Rantanen 1990; Rantanen, Lehtinen and Mikheev 1994). For example, 3,000 workers in one large enterprise require a smaller staff than would be needed to provide a similar range of services for 300 workplaces with 10 employees each. It has been noted, however, that at present in Europe, the usual proportion is one physician and two nurses to serve from 2,000 to 3,000 workers. The variation is wide, ranging from 1 per 500 to 1 per 5,000. In some countries, decisions on the staffing of the occupational health service is made by the employer on the basis of the kinds and volume of services provided, whereas in a number of countries the number and composition of occupational health staff are stipulated by legislation. For example, recent legislation in the Netherlands requires that the occupational health team must consist at least of a physician, a hygienist, a safety engineer and an expert in labour/organization relations (Ministerial Order on the Certification of SHW Services and Expertise Requirements for SHW Services 1993).
Many countries have formulated official or semi-official competence criteria for occupational physicians and nurses, but those for the other disciplines have not been established. The new European Union principles call for confirmation of the competence of all occupational health specialists, and some countries have established certification systems for them (CEC 1989; Ministerial Order on the Certification of SHW Services and Expertise Requirements for SHW Services 1993).
Training curricula for occupational health specialists are not well developed, apart from those for occupational physicians, nurses and, in some countries, occupational hygienists (Rantanen 1990). The establishment of curricula at all levels for all of the specialist categories, including programmes for basic, postgraduate and continuing education, has been encouraged. It is also deemed desirable to include training elements of occupational health at the level of basic education, not only in medical schools but also in other institutions such as technical universities, faculties of science and so on. In addition to the background in science and practical skills needed for occupational health practice, the training should include development of appropriate attitudes towards protection of workers’ health. Training in collaboration with specialists in other disciplines would enable a multidisciplinary approach. Training in collaboration with competent authorities and employers is also deemed necessary.
The professional identity of occupational health specialists needs to be supported on an equitable basis among the various disciplines. Strengthening their professional independence is crucial for efficient performance of their duties and may increase interest of other health professionals in developing lifelong careers in occupational health. It is important that the training curricula be reorganized while countries are developing new competence and certification criteria for occupational health specialists.
Infrastructures for Support Services
The majority of enterprises cannot afford the comprehensive multidisciplinary occupational health service needed for their occupational health and safety programmes. In addition to basic services provided for the enterprise, the occupational health service itself may need technical expertise in such areas as (Kroon and Overeynder 1991; CEC 1989; Rantanen, Lehtinen and Mikheev 1994):
- occupational hygiene (measurement and analysis)
- ergonomics
- information and advice about new problems and approaches to their solution
- organizational development
- psychology and stress management
- newer developments in control measures and equipment
- research support.
Countries have used different approaches to the organization of such services. For example, Finland has an Institute of Occupational Health with six regional institutes to supply expert support for front-line occupational health services. Most of the industrialized countries have such a national institute or a comparable structure with research, training, information and consultation services as its main functions; they are rare in the developing countries. Where such an institute does not exist, these services may be provided by university research groups, social security institutions, national health service systems, governmental occupational health and safety authorities and private consultants.
Experiences from industrialized countries have demonstrated the advisability of creating in each industrializing and newly developing country a special centre for occupational health research and development that can:
- provide support for policy development, evaluation and monitoring
- provide continuous scientific support for setting standards and occupational exposure limits
- develop and implement criteria for evaluating competence in the various occupational health disciplines
- provide and promote the creation of educational and training programmes to increase the number and competence of occupational health specialists
- provide information and advice on occupational health matters not only to those in the field but also to managers, labour unions, government agencies and the general public
- conduct or commission needed research in occupational health and safety.
When an individual institute is not able to supply all of the needed services, networking among several service units such as universities, research institutions and other such organizations may be needed.
Financing of Occupational Health Services
According to the ILO instruments, the primary responsibility for financing occupational health and safety services rests with the employer, with no charge being made to the workers. In some countries, however, there are modifications of these principles. For example, costs for the provision of occupational health services may be substantially subsidized by the social security institution. A case in point is Finland, where the primary financial responsibility is on the employer but 50% of the costs will be reimbursed by the social insurance institution provided there is evidence of compliance with the occupational health and safety regulations and the occupational safety and health committee of the enterprise confirms that the occupational health services have been properly provided.
In most countries, such national systems of reimbursement are available. In the community health centre model for the delivery of occupational health services, the start-up costs for facilities, equipment and personnel are met by the community, but operating costs are met by collecting fees from employers and from the self-employed.
The reimbursement or subsidy systems are intended to encourage the availability of services to enterprises with economic constraints, and particularly to small-scale enterprises which rarely can command adequate resources. The effectiveness of such a system is shown by the experience in Sweden in the 1980s, in which the allocation of substantial amounts of government financing to subsidize occupational health service for enterprises in general and particularly for small-scale enterprises increased the proportion of covered workers from 60% to over 80%.
Quality Systems and Evaluation of OccupationalHealth Services
The occupational health service should continually evaluate for itself its objectives, activities and results achieved as regards the protection of workers’ health and the improvement of the working environment. Many enterprises have arrangements for periodic independent audits by specialists in the organization or by external consultants. In some countries, there are governmental or private mechanisms for periodic recertification based on formal audit protocols. In some enterprises, periodic employee surveys provide useful indications of workers’ regard for the occupational health service and their satisfaction with the services it provides. To be truly valuable, there must be a feedback of the results of such surveys to participating employees, and evidence that appropriate actions are being taken to address any problems they disclose.
Many of the industrialized countries (e.g., the Netherlands and Finland) have initiated the use of the ISO 9000 series standards in developing quality systems for health services in general as well as for occupational health services. This is particularly appropriate because many client enterprises are applying such standards to their production processes. Some enterprises which have included their occupational health services in the application of Total Quality Management (also known as Continuous Quality Improvement) throughout their organizations have reported a positive experience in terms of improved quality and smoother operation of services.
In practice, the application of a programme of continuous quality improvement means that each department or unit of the enterprise analyses its functions and performance, and institutes any changes needed to bring their quality to an optimal level. The occupational health service should not only be a willing participant in this effort but should make itself available to ensure that considerations of workers’ health and safety are not overlooked in this process.
Evaluation of the quality of occupational health services not only serves the interests of the employers, workers and the competent authorities, but also the interests of the providers of the services as well. Several schemes for such evaluation have been developed in a number of countries. For practical purposes, the self-evaluation by the occupational health service staff itself may be the most practical, particularly when there is a health and safety committee to assess the results of such evaluation.
There is a growing interest in examining the economic aspects of occupational health and safety services and validating their cost-effectiveness, but few such studies have yet been reported.
Stepwise Development of Occupational Health Services
The ILO Occupational Health Services Convention, 1985 (No. 161) and its accompanying Recommendation (No. 171) encourage countries to develop progressively occupational health services for all workers, in all branches of economic activity and in all undertakings, including those in the public sector and the members of production cooperatives. Some countries have already developed well-organized services based on provisions stipulated by their legislation.
Starting with established services, there are three strategies for further development: extending the full spectrum of activities to cover more enterprises and more workers; expanding the content of occupational health services offering only core services; and stepwise expansion of both the content and the coverage.
There have been discussions of the minimum activities that should be provided by an occupational health service. In some countries, they are limited to health examinations conducted by specially authorized physicians. In 1989, the WHO/European Consultation on Occupational Health Services (WHO 1989b) proposed that the minimum should comprise the following core activities:
- assessment of occupational health needs
- preventive and control actions directed to the work environment
- preventive activities directed to the worker
- curative activities limited to first aid, diagnosis of occupational diseases, rehabilitation on return to work
- follow-up and evaluation of statistics of occupational injuries and diseases.
In practice, there exist a large number of workplaces around the world that have not yet been able to provide any services to their workers. Consequently, the first step for a national programme may be limited just to establishing occupational health services providing these core activities for those most in need.
Future Perspectives for Occupational Health Services Development
The future development of occupational health services depends on a number of factors in the world of work and on national economies and policies as well. The most important trends in industrialized countries include ageing of the workforce, increase of irregular employment patterns and working schedules, distant work (telework), mobile workplaces and the steady increase in small-scale enterprises and the self-employed. New technologies are introduced, new substances and materials are used, and new forms of work organization appear. There is pressure for simultaneously increasing productivity and quality, resulting in the need to maintain strong motivation for work in the face of the increasing tempo of change, and the need to learn new work practices and methods grows apace.
While measures to combat traditional occupational hazards have been successful, particularly in industrialized countries, these hazards are not likely to totally disappear in the near future and they will still represent danger even though for smaller populations of workers. Psychological and psychosocial problems are becoming dominant occupational hazards. The globalization of the world economy, the regionalization and the growth of multinational economies and enterprises are creating an internationally mobile workforce and resulting in the exportation of occupational hazards to areas in which protective regulations and constraints are weak or non-existent.
In response to these trends, the Second Meeting of the WHO Collaborating Centres in Occupational Health (the Network of 52 National Institutes of Occupational Health) held in October 1994 developed the Global Strategy on Occupational Health for All with particular relevance to future development of occupational health practice. With regard to further development of occupational health services, the following emerging issues will have to be met in the future:
- universal development of occupational health for all in order to equalize the conditions of work and health in all parts of the world
- developing better predictive methods for assessing in advance health risks of exposures and providing health and safety criteria for industrial planners, designers and engineers
- improving the integration of occupational health services with other services of the enterprise
- developing improved systems for providing occupational health services to small enterprises, agricultural workers and the self-employed
- accelerating and improving the assessment of the potential hazards introduced by new technologies, materials and substances
- strengthening the strategies and methodologies applicable in dealing with the psychosocial aspects of work, with special attention to controlling hazards and preventing their adverse effects
- improving the capability for preventing and controlling musculoskeletal disorders, cumulative strain injuries and occupational stress
- increasing attention to the needs of ageing workers and improving the methods for their adaptation to work and the maintenance of work capacities
- developing and enhancing programmes for maintaining the work capacities of the unemployed and facilitating their re-employment
- increasing the numbers and competence of professionals in many disciplines involved in occupational health and safety and recognizing the need for involvement of such new disciplines as the science of work organization, quality management and health economics.
To summarize, occupational health services will face formidable challenges during the next decade and beyond in addition to the economic, political and social pressures inherent in changing national and industrial configurations. They include the occupational health problems linked with new information technologies and automation, new chemical substances and new forms of physical energy, the hazards of new biotechnologies, relocation and international transfer of hazardous technologies, ageing of the workforce, the special problems of such vulnerable groups as the chronically ill and the handicapped, as well as the unemployment and relocations forced by job-seeking, and the appearance of new and hitherto unrecognized diseases that may affect the workforce.
Conclusions
Occupational health infrastructures are insufficiently developed to meet the needs of workers in all parts of the world. The need for effective occupational health services is growing rather than decreasing. The ILO instruments on occupational health services and the parallel WHO strategies provide a valid basis for the significant development of occupational health services, and should be used by each country as it sets policy objectives to ensure the health and safety of workers in the country.
The developing and newly industrialized countries contain approximately 8 out of 10 of the world’s workers, and no more than 5 to 10% of this working population has access to adequate occupational health services. In many industrialized countries this proportion rises to no higher than 20 to 50%. If such services could be organized and provided for all workers it would not only favourably influence workers’ health, but also have a positive influence on the well-being and economic status of the countries, their communities and their whole populations. This would also help to control the costs of avoidable sickness absenteeism and disability and restrain the escalation of health care and social security costs.
International guidelines for effective occupational health policies and programmes are available but insufficiently applied on national and local levels. Collaboration between countries and the international organizations and among the countries themselves should be fostered to provide the necessary financial, technical and professional support needed to increase access to occupational health services.
The range and quantity of occupational health services required by an enterprise vary widely depending on conditions in the country and the community, the nature of the industry and the processes and materials used, as well as on the characteristics of the workforce. Preventive services should be given highest priority and an acceptable level of quality should be ensured.
A variety of models are available for organizing occupational health services and creating the associated infrastructures. The choice should be determined by the characteristics of the enterprise, the available resources in terms of finances, facilities, qualified personnel, the kinds of problems anticipated, and what is available in the community. Further research on the suitability of various models in different situations is needed.
Providing high-quality occupational health services often requires the involvement of a broad range of occupational health and safety, general health and psychosocial disciplines. The ideal service is staffed by a multidisciplinary team in which a number of these specialities are represented. However, even such services must turn to external sources when infrequently used specialists are required. To meet the growing need for such specialists, adequate numbers must be recruited, trained and provided with the specialization in occupational health needed for optimal effectiveness in the world of work. International collaboration should be encouraged in the collection of available information and design of its application under varied circumstances, and its dissemination through already established networks widely promoted.
Research activities in occupational health have traditionally been focused on such areas as toxicology, epidemiology and the diagnosis and treatment of health problems. More research is needed on the effectiveness of various models and mechanisms for delivering occupational health services, on their cost-effectiveness and their adaptability to different circumstances.
There are a number of goals and objectives of occupational health services, some of which may need to be reconsidered because of the constantly changing world of work. These should be reviewed and revised by the most authoritative international bodies in the light of new and emerging problems of occupational health and safety and the new modes of promoting and protecting the health of workers.
The ILO Occupational Health and Safety Conventions and Recommendations, approaches and standards embodied in them, the WHO strategies and resolutions, as well as international programmes of both organizations constitute a solid basis for national work and wide international cooperation in the further development and improvement of occupational health services and practice. Such instruments and their due implementation are particularly needed throughout the world in times of rapidly changing working life; in implementation of new technologies; and under the growing risk of setting the short-term economic and material objectives ahead of the health and safety values.
Outplacement
Outplacement is a professional consulting service that helps organizations plan and implement individual terminations or reductions in their workforces so as to minimize disruptions and avoid legal liability, and counsels terminated employees in order to minimize the trauma of separation while orienting them towards seeking alternative employment or new careers.
The economic downturn of the 1980s, which continues in the 1990s, has been characterized by a virtual pandemic of job terminations reflecting the closing down of obsolescent or unprofitable units, plants and businesses, the elimination of redundancies created by mergers, takeovers, consolidations and reorganizations, and the trimming of staff to reduce operating costs and produce a “lean and mean” workforce. Although less striking than in private industry thanks to the protection of civil service regulations and political pressures, the same phenomenon has also been seen in government organizations struggling to cope with budget deficits and a philosophy that less government is desirable.
For the terminated employees, job loss is a potent stressor and source of trauma, especially when the manner of dismissal is sudden and brutal. It generates anger, anxiety and depression and may cause decompensation in persons with marginal adjustment to chronic mental illness. Rarely, the anger may express itself in sabotage or violence aimed at the supervisors and managers responsible for the termination. Sometimes, the violence is directed at spouses and family members.
The trauma of job loss has also been associated with physical ailments ranging from headaches, gastrointestinal disturbances and other functional complaints to stress-related disorders such as heart attacks, bleeding peptic ulcers and colitis.
In addition to the financial impact of loss of earnings and, in the United States, loss of employer-sponsored health insurance, job loss also affects the health and well-being of the families of the terminated employees.
Employees who are not terminated are also affected. Despite employers’ reassurances, there often is concern over the possibility of additional layoffs (threatened job loss has been found to be an even more potent stressor than actual loss of the job). In addition, there is the stress of adjusting to changes in work load and job content as relationships with co-workers are reshuffled. “Downsizing”, or reduction in the size of a workforce, may also be traumatic to the employer. It may take significant time and effort to smooth out the resultant organizational disruptions and achieve the desired productive efficiency. Valuable employees not scheduled for termination may leave for other, ostensibly more secure jobs and better-organized firms. There is also the potential of legal liability stemming from discharged employees’ allegations of breach of contract or unlawful discrimination.
Outplacement—A Preventive Approach
Outplacement is a professional service offered to prevent, or at least minimize, the trauma of staff reduction for terminated employees, those who remain and the employer.
Not all discharged employees require assistance. For some, the termination precipitates an opportunity to seek new work that might provide welcome relief from a job that had become stultifying and offered little hope of advancement. For most, however, professional counselling in working through the almost inevitable disappointment and anger of dismissed employees and help in finding new jobs can facilitate the restoration of their sense of self-worth and their well-being. Even those who accept the lure of the “golden handshake” (a package of enhanced severance and retirement benefits) and leave voluntarily may benefit from help in making the necessary readjustments.
It is generally agreed that outplacement services are most inexpensively provided by in-house staff. However, even a large organization with a competent and well-functioning staff may not have had much experience with the sensitive work of downsizing and may be too busy planning the restructuring of the organization following the exodus to attend to the niceties that may be involved. Even hardened executives often find it difficult to deal with their erstwhile co-workers. Furthermore, the departing employees are more likely to give credibility to advice from a “neutral” resource.
Accordingly, the vast majority of organizations find it expedient to contract with an outplacement consultant or consulting firm. This neutrality is reinforced by having all possible outplacement contacts located offsite in separate quarters occupied even temporarily by the consultant(s).
Outplacement Process
The outplacement process for terminated employees needs to be individualized depending on their attitudes, capabilities and circumstances, and the nature of the job market locally or in other regions. For non-exempt production workers and first-line supervisors, it involves an inventory of the worker’s skills and, where there is a market for them, assistance in placement. Where no suitable jobs exist, it involves assessment of the potential for retraining, referral for retraining, and assistance in marketing the new skills. An unfortunate complication that is difficult to overcome arises when the pay scales for the available new jobs do not measure up to the earnings of the former employment.
For employees in managerial and “creative” positions, the process generally involves a number of phases that are frequently overlapping. These phases are considered under the following heads.
Leaving the past employer.
The object is to help the candidate through the stages of reaction, understanding and acceptance of his or her predicament. Occasionally, this may require the intervention of a mental health professional.
This usually involves a reevaluation of the termination event. To earn the candidate’s confidence and assist in establishing a desirable rapport, the consultant generally reviews the circumstances of the termination and makes certain that the candidate understands them and, furthermore, has received all of the monetary and other benefits to which he or she may be entitled.
This phase concludes when the candidate is able to deal constructively with the immediate problems and responsibilities and is ready to start preparing for the future with a positive attitude. Ideally, some measure of reconciliation has been established with the past employer and the candidate is willing to accept whatever support may be offered. Such support may include temporary use of an office with a business address and telephone, supplemented by the services of a secretary who can provide typing and photocopying services, take messages, confirm appointments, etc. Most candidates function more effectively from an business-like office environment than from their own homes. Also, the consultant helps formulate a mutually satisfactory reason for the termination and arrange a mutually acceptable response to requests for references from potential employers.
Preparation for new employment.
This phase is intended to provide the focus and structure for positive thinking and action. It involves a start of the recovery of self-confidence (which continues throughout the process) by building a personal data base of the candidate’s skills, abilities, knowledge and experience, and learning to communicate it in clear, functional terms. Simultaneously, the candidate begins to identify and confirm suitable job objectives and to consider the nature of the jobs for which his or her background might be particularly suitable. Through it all, the candidate acquires the knack of accumulating and organizing information that will highlight the range and depth of his or her experience and level of competence.
Résumé writing.
Here, the candidate learns to develop a flexible tool that will present his or her objectives, qualifications, and background, arouse the interest of potential employers, help obtain interviews, and serve as an aid during job interviews. Rather than being restricted to a fixed format, the résumé is varied to “package” skills and experiences to make them most attractive for particular job opportunities.
Assessing job opportunities.
The consultant guides the candidate to an assessment of the availability of potential jobs that might be suitable. This includes a survey of different industries, the job market in different localities, opportunities for growth and advancement, and likely earning potential. Experience indicates that about 80% of job opportunities are “hidden,” that is, they are not readily apparent on the basis of industry designation or job title. Where appropriate, the assessment also includes an appraisal of the potential of self-employment.
Job-hunting campaign.
This involves identifying and exploring existing and potential opportunities through direct approaches to potential employers and developing and making use of contacts and intermediaries. The campaign entails obtaining interviews with the “right” people on a right basis, and using letters both to obtain interviews and as a follow-up to interviews.
The consultant will, as part of enhancing the candidate’s job-hunting skills, improve his or her writing and interview techniques. Practice in letter writing is aimed at polishing a communication skill that is uniquely helpful in defining job opportunities, in identifying the “right” people and developing contacts with them, obtaining interviews with them and in following up on interviews. The candidate is further trained by interview coaching, which involves role playing and critiquing videotapes of practice interviews in order to maximize the effectiveness with which his or her personality, experience and desires are presented. The candidate’s chances of coming away from an interview, with, at least, an appointment for the next interview, if not an actual job offer, are by this means enhanced.
Negotiating compensation.
The consultant will help candidates overcome their dislike or even fear of discussing compensation in negotiating a potential position so that they can obtain the best compensation package possible under the existing circumstances, avoiding the possibility of over-selling or under-selling themselves or antagonizing the interviewer.
Control.
Within the limits of the consulting contract, regular contact with the candidate is maintained until a new position is maintained. This involves gathering and organizing information to track how the campaign is progressing and to ensure optimal use of time and effort. It will help the candidate to avoid errors of omission and provide a signal to correct errors of commission.
Following through.
When a new position is obtained, the candidate notifies the consultant and the old employer as well as other prospective employers with whom he or she may have been negotiating.
Follow-up.
Again, within the limits of the contract, the consultant maintains contact to assist the candidate’s adjustment to the new position to aid in overcoming any adverse factors and to encourage continuing career growth and development. Finally, at the close of the programme, the consultant provides the employer with an aggregate report of the results (personal and/or sensitive information is usually held confidential).
The organization
It is rare for the outplacement consultant to be involved in designating specifically which employees are to be separated and which will remain — that is a decision usually made by the organization’s top management, often in consultation with department heads and line supervisors and in the light of the structure envisioned for the revised organization. The consultant, however, does provide guidance on the planning, timing and staging of the downsizing process and on the communications with both those who will leave and those who will remain. Since the “grapevine” (i.e., rumors circulating in the workforce) is usually active, it is imperative that these communications be timely, complete and accurate. Proper communications will also help address potential allegations of discrimination. The consultant also often assists with public relations communications to the industry, customers and the community.
Caveats
The extent of downsizing during the last decade, at least in the United States, has given impetus to development of a veritable industry of outplacement consultants and firms. A number of search firms devoted to identifying candidates for job vacancies have taken up outplacement as a side-line. A variety of semiprofessionals, including former personnel directors, have become outplacement counsellors.
Until recently, there was no formally adopted code of practice and ethical standards. However, in 1992, the International Association of Outplacement Professionals (IAOP) sponsored the creation of the Outplacement Institute, membership in which requires meeting a set of criteria based on educational background and personal experience, evidence of continuing participation in programs of personal and professional development, and a commitment to uphold and observe the published IAOP Standards for Ethical Practice.
Conclusion
Reduction in the size of a workforce is, at best, a trying experience for the employees being terminated or forced into retirement, and for those remaining and for the organization as a whole. It is invariably traumatic. Outplacement is a professional consulting service designed to prevent or minimize the potential adverse effects and promote the health and well-being of those involved.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."