- You are here:
-
Home

-
Part XVII. Services and Trade
-
Health Care Facilities and Services
- Chemicals in the Health Care Environment
Case Study: Occupational health and Safety Campaigns at the National Level in India
Background
This case study, which presents an example of a successful national safety campaign, is based on 24 years of experience organizing the annual National Safety Day (NSD) Campaign in India. The Campaign celebrates the foundation by the Government of India of the National Safety Council (NSC) in the Ministry of Labour on 4 March 1966 as an autonomous, non-political and non-profit-making organization at the national level to generate, develop and sustain a voluntary movement with respect to occupational safety and health (OSH). The NSC’s Board of Governors is broad-based, with representation from all the central organizations of employers and trade unions. Total membership was approximately 4,000 in April 1995, drawn predominantly from the industrial sector, although there also is some membership from non-industrial sectors. In 1966, industrial workplaces in India experienced a rising trend of accidents, and enforcement of safety and health statutes by government agencies alone was not sufficient to reverse this trend. The birth of the NSC as a voluntary body in such a national perspective therefore constituted an important milestone. For many years, the NSC mainly concerned itself with industrial safety; however, with the coverage of some non-industrial sectors in recent years, its scope has been expanded from industrial to occupational safety. The coverage of occupational health, however, is still in its infancy in India. As the idea found favour of commemorating the foundation day of the NSC in the form of a national awareness campaign, the first NSD Campaign was launched in 1972. NSD became an annual event, and even though the duration of the Campaign has been increased to a week, it continues to be known as the National Safety Day Campaign due to the popularity that the title has gained.
Objectives
The objectives of the NSD Campaign, which have been kept broad, general and flexible, include the following:
- to increase OSH standards throughout India
- to enlist the support and participation of all major participants in different sectors at different levels, such as the central and state governments and their regulatory agencies and institutions; district and local administrations; non-governmental organizations (NGOs); employers’ organizations; public, private and joint-sector undertakings; trade unions
- to promote the active participation of employers in the education of their employees to achieve OSH goals in their workplace through the use of local knowledge, experience and talent
- to foster development of need-based programmes and activities, self-compliance with statutory requirements, and strengthening of professional OSH management systems in undertakings
- to bring into the fold of the voluntary OSH movement certain sectors not so far covered by safety and health legislation in the country—for instance, the construction sector, the research and development sector, and small shops and establishments using hazardous machines, equipment and materials.
The above objectives are part of an overall goal of creating and strengthening OSH culture in workplaces and integrating it with the work culture. In a developing country, achievement of this goal continues to be a highly challenging task.
Methodology and Approach
The methodology and approach used to introduce and promote the Campaign initially comprised two elements: (1) issuing of letters of appeal to NSC member organizations to organize the Campaign; and (2) providing them with professionally designed promotional materials such as badges, copies of the NSD pledge (see box), cloth banners, posters, stickers and so on, and promotional-cum-utility items such as key chains, ball-point pens, and paperweights with OSH messages printed on them. These materials are centrally designed, produced and distributed by the NSC with the following three aims.
- to make it convenient for the participants to organize the Campaign without having to go through the time-consuming and costly process of designing and producing such materials in small quantities themselves
- to ensure that the Campaign materials are of professional quality with appealing messages reflecting national OSH issues
- to generate income to contribute to NSC’s financial self-reliance with respect to the fulfilment of the wider objective of strengthening the voluntary OSH movement in India.
Text of National Safety Day Pledge
On this day, I solemnly affirm that I will rededicate myself to the cause of safety, health and protection of environment and will do my best to observe rules, regulations and procedures and develop attitudes and habits conducive for achieving these objectives.
I fully realize that accidents and diseases are a drain on the national economy and may lead to disablement, death, damage to health and property, social suffering and general degradation of environment.
I will do everything possible for prevention of accidents and occupational diseases and protection of environment in the interest of self, my family, community and the nation at large.
(In some states, the above pledge has been administered by the Governor of State to state ministers, other government officials, executives and workers from industries, and the public participating in NSD functions. In private enterprise, it is usual for the chief executive or some other top executive to administer the pledge to all employees.)
In its initial years, the Campaign was confined to NSC members and grew gradually. After about a decade, the methodology and approach were widened in the following strategic ways:
- The Union Ministry of Labour, responsible for OSH in the workplace, was asked to extend support to the NSC’s efforts to approach the State Governments for aid in the organization of celebrations. Since then, the Union Labour Minister has requested that the State Labour Ministers organize celebrations by constituting Campaign Committees at the state and district levels; these committees would be comprised of representatives of industries, workers and officials of the concerned government departments, and would send reports to the Central Government. Such support has given the Campaign national stature.
- The electronic media (television and radio) under state control has been advised by the Government to cover the Campaign. Such coverage has made the Campaign highly visible.
- The NSC’s own journals, as well as newspapers and magazines published by employers and trade unions and the national and local press, have been involved more effectively.
- The duration of the Campaign has been increased to a week, and flexibility has been provided to participants to start or conclude the Campaign on any convenient date, taking care to include 4 March (NSC foundation day) in the week. This has increased the span of visible impact of the Campaign.
- The state chapters and district action centres of the NSC have actively involved the state governments and district administrations in the Campaign at the grass roots.
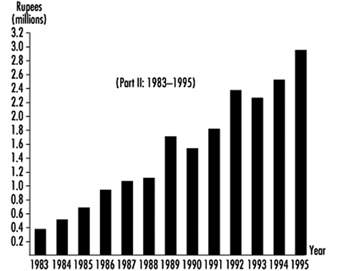
- The Campaign has grown over the years. Figure 1, figure 2 and figure 3 show this growth in terms of the persons reached for the pinning of the badge and the financial receipts from the sale of Campaign materials.
Figure 1. Growth of NSD campaign in terms of persons reached for pinning badge

Figure 2. Growth in terms of financial receipts from sale of NSD campaign materials (1972-1982)
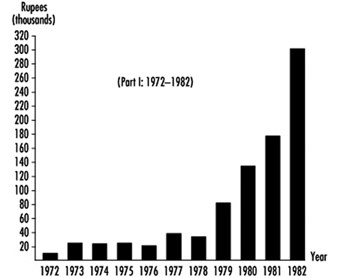
Figure 3. Growth in terms of financial receipts from sale of NSD campaign materials (1983-1995)
Participation at Different Levels
Participation by all stakeholders at the national, state, district and individual enterprise levels has been of vital importance to the success and effectiveness of the Campaign. However, the degree of involvement by various stakeholders has not been uniform. In the first instance, different stakeholders started participating in the Campaign in different years. Furthermore, their perceptions regarding their roles and needs vary greatly. For example, some governments, particularly those of industrialized states, have been organizing elaborate and purposeful activities, but in some other less industrialized states, they have been low-key. Similarly, while some industry associations have lent great support to the Campaign, others have yet to start participating. While activities at the national, state and district levels have dealt with broad issues, those at the individual enterprise/undertaking level have been more detailed and need-based.
Campaign Materials
The national OSH issues and messages to be projected through a particular year’s campaign materials produced by the NSC are identified by a core group of professionals from the NSC, industry and trade unions. The visuals for communicating them in a simple, humorous and effective way are designed by eminent cartoonists. In this way it is ensured that the campaign materials are original, attractive, appealing and rooted in Indian culture.
These materials fall into two broad categories: (1) purely promotional materials used for display and educational purposes; and (2) promotional-cum-utility materials which, besides promoting the OSH messages, are also good for day-to-day use. In the second category, most items are for the daily use of workers and are relatively inexpensive and affordable by managements of various enterprises for free distribution to all their employees. Some items appropriate for use of executives are also produced to give them a sense of involvement. To prevent the items from becoming monotonous, they are changed either completely or in style and appearance in different years.
As the Campaign has grown over the years and the demand for Campaign materials substantially increased, a number of private producers and suppliers have emerged who produce materials as per their own market research. This has been a welcome development. Individual enterprises also produce materials relevant to specific themes of their need-based campaigns. Many of these organize contests among their employees to generate ideas and then publicize the prize winners through their campaign materials.
Activities
At the national level, activities have taken the form of public functions, seminars, discussions and debates, the issuance of appeals and messages and the release of special films on national OSH issues. Participation of the Union Minister and top officials of the Ministry of Labour, Chairman and senior officials of NSC, senior executives from industry, national trade union leaders and eminent persons from institutions, NGOs and the public has imparted to these activities the desired level of impact. The national television and radio networks, the press and other print media have been involved in propagating these activities widely.
At the state level, activities vary from state to state but are generally of the same type as at the national level. The emphasis of these activities is on the projection of specific state issues through the medium of regional language. A welcome trend observed in state activities in recent years has been that an important government function, namely, distribution of state safety awards, is combined with the Campaign celebrations.
The activities at the individual enterprise level are more practical and varied. Generally, such activities are designed by the safety committee (if existing as per statutory requirements applicable to enterprises employing a certain minimum number of employees) or by a specially constituted task force set up by management. Some typical activities are contests among employees or among different departments for good housekeeping, lowest accident frequency rate, and accident-free work, safety posters, safety slogans, safety suggestions and so on, exhibitions, skits, dramas, one-act plays, songs, training programmes and seminars, lectures, screening of films, practical demonstrations, organizing of emergency drills, holding of functions, and so on. Experts from outside the enterprise are also invited as guest speakers.
Some of the most common and important approaches which have contributed to the effectiveness of activities at the enterprise level may be summarized as follows:
- The dramatizations and plays staged by employees of some enterprises have been of good professional quality and offer effective entertainment, communicating accident case histories with lessons to be learnt. Such plays have been video recorded for telecasting on state and national television networks, thereby increasing their impact.
- Qwaali, a popular form of song on the Indian subcontinent, has also been commonly used for communicating OSH messages while providing entertainment consistent with Indian cultural traditions.
- A number of large companies, in both the public and private sectors, have their own residential colonies and schools for the benefit of their employees. Many of these companies have designed activities including contests to involve families and students in safety and health; this has had a positive impact on the motivation of the employees. Even undertakings not having their own residential colony or school have used this approach to involve the families and school-age children of their employees with similar success.
- In the wake of the Bhopal disaster, many enterprises engaged in manufacture, storage or use of hazardous chemicals and having potential for major accidents have developed activities to create awareness of OSH in nearby communities. They invite members of these communities to visit their plants for exhibitions or functions during the Campaign. They also invite government authorities as guests of honour. This approach has been useful in building cooperation among industry, government and community, so important to ensure quick and effective response to chemical emergencies at the local level.
- Activities involving practical demonstrations of important safety-oriented resources such as the use of firefighting methods and personal protective equipment, the holding of emergency drills and the conducting of tailor-made in-plant training courses and seminars on specific needs have proved successful in creating enthusiasm and a supportive environment within enterprises.
The approaches listed are particularly suitable for OSH campaigns at the unit level.
Impact Achieved
The NSD Campaign has shown a positive impact on the trend of industrial injuries (reportable under the Factories Act) in India. As shown in table 1, the incidence rate of industrial injuries (injuries per 1,000 workers) decreased from 75.67 in 1971 to 26.54 in 1992 (the latest year for which published statistics are available), a reduction of about 65%. It should be noted that this reduction is due to the combined impact on OSH of government policy and legislation, enforcement, education and training, promotion, modernization of industrial processes and operations, and so on, as well as of NSD Campaign activities.
Table 1. Number of Indian working factories, estimated average daily employment, reportable injuries and their incidence rates
|
Year |
No. of working factories |
Estimated average daily |
Industrial injuries |
Rate of injuries per thousand employees in factories submitting returns |
||
|
Fatal |
Total |
Fatal |
Total |
|||
|
1971 |
81,078 |
5,085 |
635 |
325,180 |
0.15 |
75.67 |
|
1972 |
86,297 |
5,349 |
655 |
285,912 |
0.15 |
63.63 |
|
1973 |
91,055 |
5,500 |
666 |
286,010 |
0.15 |
62.58 |
|
1974 |
97,065 |
5,670 |
650 |
249,110 |
0.14 |
53.77 |
|
1975 |
104,374 |
5,771 |
660 |
242,352 |
0.14 |
50.86 |
|
1976 |
113,216 |
6,127 |
831 |
300,319 |
0.17 |
61.54 |
|
1977 |
119,715 |
6,311 |
690 |
316,273 |
0.14 |
63.95 |
|
1978 |
126,241 |
6,540 |
792 |
332,195 |
0.15 |
68.62 |
|
1979 |
135,173 |
6,802 |
829 |
318,380 |
0.16 |
62.19 |
|
1980 |
141,317 |
7,017 |
657 |
316,532 |
0.14 |
66.92 |
|
1981 |
149,285 |
7,240 |
687 |
333,572 |
0.16 |
76.73 |
|
1982(P) |
157,598 |
7,388 |
549 |
296,027 |
0.13 |
69.10 |
|
1983(P) |
163,040 |
7,444 |
456 |
213,160 |
0.13 |
55.63 |
|
1984(P)* |
167,541 |
7,603 |
824 |
302,726 |
0.10 |
36.72 |
|
1985(P)* |
175,316 |
7,691 |
807 |
279,126 |
0.23 |
58.70 |
|
1986(P) |
178,749 |
7,795 |
924 |
276,416 |
0.14 |
49.31 |
|
1987(P) |
183,586 |
7,835 |
895 |
236,596 |
0.14 |
41.54 |
|
1988(P) |
188,136 |
8,153 |
694 |
200,258 |
0.15 |
41.68 |
|
1989(P) |
193,258 |
8,330 |
706 |
162,037 |
0.16 |
35.11 |
|
1990(P) |
199,826 |
8,431 |
663 |
128,117 |
0.21 |
33.11 |
|
1991(P)* |
207,980 |
8,547 |
486 |
60,599 |
0.21 |
26.20 |
|
1992(P)* |
207,156 |
8,618 |
573 |
74,195 |
0.20 |
26.54 |
Key to Symbols: P = provisional; * = incomplete data.
Source: Labour Bureau.
The research and development sector under the Central Government, comprising 40 national laboratories located all over India and employing over 26,000 employees, including over 9,000 scientists, does not fall under the purview of any OSH legislation. For the last 3 years, the corporate level and the individual laboratories have started organizing NSD celebrations, have set up safety cells and are proceeding in a systematic way towards establishing a sound system of OSH management. This is a concrete example of the impact of the NSD Campaign in strengthening the voluntary OSH movement in India.
The organizations in charge of nuclear power stations, heavy water plants and research reactors, as well as other divisions in the Department of Atomic Energy (DAE) of the Government, have been organizing celebrations during the NSD Campaign. They have instituted interdepartmental contests and awards for achievements in the fields of safety, health and environmental protection. The enforcement of safety and health statutes in the above establishments is carried out by an independent agency under the control of DAE, but these units are not open to inspection by state regulating agencies covering other workplaces. Activities under the Campaign have served to create interaction between departmental and external regulatory agencies and between the NSC and other institutions, and have furthermore facilitated the dissemination of OSH information to the public.
Located on the west coast, Gujarat is one of the most industrialized states in India. The state has 525 medium and large factories manufacturing, storing or using one or more of 38 hazardous chemicals. All these factories have prepared and rehearsed emergency plans. As a part of the last NSD Campaign, each of these larger entities was requested by the Chief Inspector of Factories to impart practical training in the use of breathing apparatus and fire extinguishers to emergency-response workers from 10 small factories located in its neighbourhood. Six workers (two from each shift) were selected from each small unit, for a total of 31,500 workers from 5,250 units. This case is illustrative of the impact of the Campaign in making available practical emergency training to small units engaged in hazardous processes.
In conclusion, the most important contribution of the NSD Campaign may be summed up as creating awareness in business and industrial circles and the public that safety, health and environmental protection constitute a vital and integral part of the strategy for sustainable development. However, there is a long way to go before this strategy is translated into a greater reality. The NSD Campaign will no doubt have an increasing role to play in achieving this reality.
Safety Promotion
The aim of safety promotion is to induce employees to improve their own protective behaviour and that of their co-workers, and to support an organization’s stated safety goals. Safety promotion objectives include increasing safety awareness at all organizational levels and confirming the furtherance of employee safety as a top management priority.
The ultimate effectiveness of any promotion programme or activity depends directly on how well an organization manages its safety programme. Safety promotion can play an important contributory role in improving workplace safety when sound hazard management practice exists at all operational phases, including facilities planning, machine design, employee training and supervision, personal protective equipment, environmental maintenance, housekeeping, emergency response and rehabilitation.
No matter how intrinsically effective and efficient a safety promotion scheme is in changing employee attitudes and behaviour, it requires management support in the form of visible leadership and commitment. This condition is a prerequisite for a successful promotion, be it focused on production, product quality or employee safety and health. It is also the consistent characteristic that marks all successful safety programmes, no matter how much their specifics differ.
Employee Motivation
Safety promotion relates directly to the concept of motivation, which has been the subject of a great deal of research. There is controversy about how and why people are “motivated” either to adopt new behaviours or change old ones. A central issue concerns the relation between attitudes and behaviour. Must attitude change come before behaviour change? Can behaviour change exist without attitude change? Does attitude change predict behaviour change? Does behaviour change cause attitude change?
Answers to these questions are uncertain. There are those who insist that motivation is best achieved by changing external behaviour alone, while others feel that internal attitude or cognitive change must be part of the behaviour change process. Both of these viewpoints have influenced the conduct of safety promotion.
Although not directly observable, motivation can be inferred from changes in behaviour and attitudes. Three variables that define motivation are as follows:
- Direction of behaviour requires the specification of objectives and the provision of the necessary training or education to achieve them.
- Intensity of action involves the realization and strengthening of behaviour and attitude change primarily through reinforcement and feedback.
- Persistence of effort involves making the desired behaviour and attitude changes permanent in all facets of employee performance.
Safety Promotion Models
The safety literature describes a variety of safety promotion theories and methods that address each of the motivational variables; among these, two models have shown the capacity to improve safety performance. One, organization behaviour management (OBM), focuses on behaviour modification and the application of behaviour control methods developed by B.F. Skinner. The other, total quality management (TQM), focuses on process modification and the application of quality control principles developed by W.E. Demming.
Behaviour modification is founded on the premise that the causes of behaviour are environmental in nature. Accordingly, one can predict and control behaviour by studying the interaction between individuals and their environments. This knowledge requires the specification of three conditions:
- the antecedents of behaviour—that is, the occasion on which a response occurs
- the behaviour or action that occurs
- the consequences that reinforce the behaviour or action.
Quality improvement requires a “constancy of purpose” or commitment by both employees and management to make improved product and service quality a corporate priority. This attitude adjustment rests on a conscious management decision to do whatever it takes to make the quality improvement vision a reality. Quality improvement objectives are broader in scope and the methods for their achievement are less uniform than those of behaviour modification. They are more concerned with changing or even eliminating total processes than with modifying individual behaviours.
As shown in table 1, both models are responsive to the variables and supporting actions that motivation requires. The models differ, however, on the safety emphases used to motivate employees. As a result, they differ in terms of their efficiency in satisfying the requirements of the three motivational variables.
Table 1. OBM vs. TQM models of employee motivation
|
Motivational variable |
Supporting action |
Safety emphasis |
|
|
OBM |
TQM |
||
|
Direction of behaviour |
Specify objectives. |
Behaviour |
Attitudes/behaviour |
|
Intensity of action |
Give reinforcement. |
Behaviour occurrence |
Process improvement |
|
Persistence of effort |
Commit employee. |
Behaviour change |
Continuous improvement |
OBM Model
Direction of behaviour
OBM safety objectives are usually narrow in scope and focus on increasing the occurrence of specific safe behaviours, thereby decreasing the incidence of unsafe acts. The following sources can be used to select unsafe acts or behaviours as targets for observation and eventual reduction:
- analysis of incident investigations and related safety records
- interviews with employees at all levels to obtain data on unreported events, hazards and so forth
- observation of in-house safety inspections.
Based on information from these sources, employees are asked to assist in establishing a list of priority behaviours judged to be critical to improved safety performance. An observation system to track the occurrence of these critical behaviours is established, observers are trained and an observation schedule is set. The incidence of priority behaviours is then observed during a pre-intervention period. This phase of the problem definition process provides baseline data against which to measure the success of the behaviour modification process. These data also alert employees to the presence of unsafe behaviour in the workplace.
Employees are then exposed to training that covers the behaviours to be practised, offers safe behaviour performance guidelines, and allows for behavioural feedback. For example, workers are sometimes shown slides or videotapes of safe and unsafe practices, followed by discussion. At this time they are also shown baseline data and encouraged to improve their performance of critical safe behaviours. The data, often in chart form, are posted in the plant to prepare for the subsequent phases of the OBM programme. The activities of observation and recognition are performed on a continuing basis by supervisors or trained co-workers. As appropriate, new job safety performance elements are added to the training and become part of the programme.
Intensity of action
OBM uses both individual reinforcement and group feedback to modify behaviour. Reinforcement occurs at the individual employee level in the form of verbal praise or other sorts of recognition when a display of safety behaviour is seen in the workplace. Feedback about the level of safety behaviour exhibited by the group is also communicated throughout the programme.
Various types of rewards can be used to reinforce behaviour, such as the following:
- individual monetary incentives (e.g., cash awards and tokens for the purchase of consumer goods)
- praise and feedback (e.g., knowledge of results, congratulatory notes and positive comments)
- team competitions, which may involve the use of cash awards.
Rewards are often used in combination, so it is very difficult to isolate the impact of any individual type of reinforcement. Nevertheless, it is clear that positive responses to safe behaviour do increase its occurrence.
Reinforcement also includes group feedback about safety performance, which frequently takes the form of learning curves or bar charts tracking the percentage of safe behaviours that are observed during the intervention period. This information is displayed prominently so that the work group is aware of progress. This knowledge tends to maintain safe work group performance and stimulate future efforts at improvement.
In the OBM paradigm, reinforcement and feedback require a continuing programme of behavioural observation. This condition enables positive communication to occur on the spot when safe behaviours are seen or when unsafe practices require correction. Although behaviour modification emphasizes positive reinforcement rather than discipline, its proponents recognize that reprimands or other aversive actions may be necessary in certain situations. Whenever possible, however, these steps should be avoided because their effects are usually short-lived and may diminish employee commitment to the total programme.
Persistence of effort
OBM effectiveness in sustaining behaviour change depends on continuous observation and reinforcement of specific safe behaviours until they become self-reinforcing and a habitual part of an employee’s job activity. The strength of OBM rests in the creation of a measurement system that allows a company to continually monitor and control critical behaviours. To achieve long-term success, use of this measurement system must become part of an organization’s management style.
There is little doubt that the OBM approach produces positive results and does so relatively quickly. Most studies show that the use of positive reinforcement, in the form of incentives or feedback, enhances safety and/or reduces accidents in the workplace, at least over the short term. In contrast, longevity of behaviour change as produced by OBM procedures has not been fully demonstrated by research. In fact, most of the studies conducted are short-term in duration (less than one year). This situation has raised questions about the permanence of OBM treatment effects, although two studies of OBM techniques, one conducted in the United States and the other in Finland, have reported some long-term positive effects.
In the United States, the use of a trading stamp award system improved safety performance in two coal mines for more than ten years. In this study, employees earned stamps for working without lost-time injuries, for being in no lost-time injury work groups, for not being involved in equipment-damaging incidents, for making safety suggestions that were adopted, and for unusual incident or injury prevention behaviour. Besides the token award system, workers received extensive training during the baseline period, intended to prompt safe behaviour and to maintain safe work conditions. This training activity was regarded as very important to the improvements obtained.
In Finland, significant housekeeping improvements in a shipyard were achieved during a three-phase programme featuring feedback to foremen and workers following baseline measurement and employee training. These improvements, expressed as higher housekeeping indices, continued to be observed at the new high level throughout a two-year follow-up period during which no feedback was given. Significant accident reductions were also noted throughout the project’s duration. The long-term effects of this programme were attributed to reinforcement that concentrates on the outcome of behaviour and persists in the environment (as housekeeping changes do), rather than simply on a behaviour, which influences workers for only seconds.
These studies notwithstanding, it is difficult to determine the long-term efficacy of OBM approaches in maintaining safety performance improvements. In the US study, the use of tokens evidently became an accepted part of the mines’ management style, but there was also a strong emphasis on training. Learned feedback from environmental changes that are an outcome of behaviour, as reported in the Finnish study, looks promising. Here too, however, there is some indication that other factors may have been operative to influence shipyard employees during the follow-up “no feedback” period.
With these observations in mind, the bulk of research suggests that feedback must be maintained if OBM programmes are to achieve lasting success, and that this process must be accompanied by a management style that permits it. When these conditions are absent, positive behaviour change effects diminish rapidly and revert to previous levels. Where housekeeping improvements are involved, there is some evidence that the higher performance levels continue for a relatively long period, but the reasons for this remain to be determined.
TQM Model
Direction of behaviour
TQM goals are broad in scope and centre on creating improved processes. There is an emphasis on discovering and eliminating the conditions that cause or support the existence of unsafe behaviours, as opposed to a concentration on unsafe acts as the cause of injuries.
The TQM approach uses many of the same methods as OBM to uncover safety performance deficiencies that are to become targets for improvement. Additionally, it concentrates on the management systems and practices that contribute to these problems. These conditions may appear in all functions, from planning, through organizing and decision making, to evaluating cost-effectiveness. They also include the presence or absence of practices that incorporate employee safety considerations into everyday business processes such as the application of ergonomic principles to workplace and equipment design, review of purchasing specifications by safety and health professionals, and timely correction of reported hazards. Operational indicators such as the lattermost, combined with injury, downtime and employee absence records, provide baseline information on how well the management system supports the safety function.
Employee safety programme perception surveys have also become a popular tool for assessing the safety management system. Employees give their opinions about the effectiveness of the management practices and safety support activities that are present in their company. These data are gathered anonymously according to standard administrative procedures. Survey results help to set improvement priorities and provide another baseline against which to measure progress.
Just as TQM defines its performance objectives more broadly than OBM, it also makes a broader spectrum of training available to employees. TQM-based instruction teaches employees not only how to be safe but educates them about self-improvement and team-building methods that make possible ongoing contributions intended to increase safety throughout the organization.
The importance cannot be overstated of task planning at the systems level and providing sufficient safety training for employees whose jobs are expanded or enriched through process changes. There is some evidence indicating that as the number and variety of nonrepetitive tasks to which workers are exposed increases, so too does the frequency of accidents. It is not clear that this unwanted potential outcome has been recognized in the TQM literature.
Intensity of action
TQM uses various methods for reinforcing improved processes. These aim at creating an organizational culture that supports concerted employee effort to make process improvements. The mechanisms for behaviour change also incorporate reinforcement and feedback techniques to both recognize and reward performance improvement.
Several key conditions that support the development of improved processes are as follows:
- an open corporate climate with increased information sharing and removal of formal departmental barriers
- a focus on employee involvement, teamwork and training at all levels
- the removal of informal barriers to pride of workmanship
- a corporate culture that involves all employees in contributing to improvements
- follow-up to act upon or more fully develop new ideas for process improvement.
Adoption of these measures leads to higher employee morale and satisfaction that can increase the willingness to improve safety performance.
It should be noted that reinforcement at the employee level is regularly used in the TQM model. Rather than responding to specific critical behaviours, however, individuals receive praise for safe work at any phase of a process, with the goal being to encourage employees to internalize a process that incorporates improved safety performance.
Feedback about observed safety and health improvement results is also provided periodically through such media as meetings and newsletters, as well as through the conduct of follow-up surveys. These results are presented in the form of operating indicators. They may include such indices as lost workdays due to occupational injury and illness, number of safety and health improvement suggestions submitted, attendance levels, workers’ compensation costs and employee attitudes toward safety.
Persistence of behaviour
The long-term effectiveness of the TQM approach resides in its capacity to create or continuously improve processes that support safe job performance. These improvements require both attitude and behaviour change. They also must be endorsed at the deepest levels of management practice and philosophy if they are to last. That is, they must become part of an organization’s culture. For these reasons, positive results are not realized immediately. For example, successful users of TQM report an average of three years to achieve improved quality performance.
Evidence about the relationship between TQM and improved safety performance comes from two sources: the safety records of companies that have used TQM to successfully improve product and service quality, and the safety support processes used by companies with excellent safety records. Of 14 US companies receiving national recognition for excellence in quality management and achievement in the form of the Malcolm Baldrige National Quality Award, 12 had better lost-workday injury and illness rates than their industry average. Eleven of these companies also reported improved rates associated with the introduction of TQM practices, while only three companies had worse rates.
The efficacy of TQM techniques as applied to occupational safety is also exemplified by National Safety Council member companies with the most outstanding safety performance records in the United States. These successful programmes emphasize a “humanistic” approach to employee management, featuring less discipline, more active worker participation and better communication between workers and management.
Because TQM emphasizes employee involvement and empowerment in implementing system and process safety and health improvements, the potential for permanent change is maximized. Its emphasis on educating employees so that they are able to better contribute to future safety performance improvement also lays the groundwork for long-term effectiveness. Finally, TQM approaches visualize employees as active decision makers who are responsible for rather than simply responsive to the environment. These features make it highly likely that both employees and management will be committed to change produced through TQM on a long-term basis.
Comparison of OBM and TQM
OBM seeks to decrease specific unsafe practices and increase safe performance through a structured approach that defines critical behaviours, trains employees in safe/unsafe practices, establishes a system of behaviour observation, and uses a schedule of reinforcement and feedback to control employee behaviour. Its strengths are its emphasis on behaviour observation and results measurement, and the rapid production of positive results when the programme is present. Its weaknesses rest in its focus on specific behaviours that may not have been integrated with the need for management system changes, the use of an external control programme to maintain employee behaviour, and lack of demonstrated staying power.
TQM seeks to improve processes within the management system that affect employee safety and health. It stresses both attitude and behaviour changes and relies on a broad range of employee involvement and training programmes to define both safety and health improvement objectives and the means to achieve them. It uses reinforcement and feedback aimed at recognizing process improvements and employees’ contribution to them. Its strengths are in its emphasis on employee participation and internal control (facilitating and reinforcing both attitude and behaviour change), its capacity to sustain safety and health improvements, and its integration within an organization’s total management effort. Its weaknesses rest in its dependence on: (1) high levels of management/employee involvement that take time to develop and show improved results, (2) new process measurement systems, and (3) management’s willingness to allot the time and resources it takes to produce positive results.
Safety Promotion Programmes and Practices
In what follows, the interaction between wage systems and safety will first be considered. Wage systems have a critical effect on employee motivation in general and have the potential to influence worker safety attitudes and behaviour in the context of job performance. Incentives, including both monetary and non-monetary rewards, will be examined in light of their debated value as a safety promotion tactic. Finally, the role of communications and campaigns in safety promotions will be described.
Wage systems and safety
Wage systems can affect safety indirectly when incentive compensation, gain-sharing or bonuses are established to increase production, or when piece-work pay structures are in effect. Each of these arrangements may motivate workers to sidestep safe work procedures in an effort to increase earnings. Also, wage systems can be directly tied to safety considerations in the form of compensating wages that are paid for work that involves above-average risk.
Incentive wages
Incentive compensation or gain-sharing programmes can be established for productivity; for safety records; for scrap, rework and return rates; and for a variety of other performance criteria, alone or in combination. Such programmes have the potential to communicate management strategy and priorities to employees. For this reason, the performance criteria that an organization includes in its incentive wage system are critical. If safety performance and related factors are part of the package, than employees are likely to perceive them as being important to management. If they are not, then an opposite message is sent.
There are situations where work performance is introduced as a wage incentive criterion to induce workers to put up with dangerous conditions, or to fail to report accidents. Some commentators have noted the increased occurrence of this abuse, particularly in enterprise bargaining agreements and in efforts to reduce workers’ compensation premiums. Obviously, this practice not only sends employees the wrong message but is counterproductive and will ultimately increase employer costs.
Although the theory behind incentive compensation appears to be strong, in practice its influence on worker productivity is far from certain. Research on the effects of financial incentive schemes on productivity shows extreme variability of results, indicating that naive approaches to the planning and implementation of incentive compensation programmes can lead to problems. However, when applied correctly, these programmes can have very positive effects on productivity, especially output.
A US investigation of the effects of bonus plans on accidents and productivity in 72 mines yielded little evidence that they had any significant impact either on improving safety or increasing production. Some 39% of these plans included safety in bonus calculations, while the rest did not. Within the study sample there was wide variability in the bonus payout frequency. Although the modal payout period was monthly, in many cases miners earned productivity bonuses only once or twice a year, or even less often. In such cases, the effect on production was negligible and, as might be expected, safety performance was not affected. Even among mines that paid production bonuses more than 80% of the time, no significant negative effects upon miner safety (i.e., increased lost-time accident frequency rates) were found. Mines that had monetary bonus plans directed solely at safety also failed to produce accident rate reductions. Most of these used lost-time accidents and violations as performance criteria, and experienced the same low payout problem that plagued many of the productivity-based plans.
The failure to find a clear-cut relationship between incentive compensation and productivity or safety in this study highlights the complexity of trying to conduct successful wage incentive programmes. Although increased wages are important, the perceived value of money varies among workers. There are also many other factors that can influence whether monetary incentives will have the desired motivational effect. Incentive or gain-sharing programmes often fail to produce expected results when employees think the programme is unfair. Actions that can be taken to help prevent this from happening and reinforce the motivational properties of an incentive programme include the following:
- Set a performance standard that employees perceive to be reasonable.
- Make bonus earning intervals short.
- Use multiple performance criteria.
- Include only performance objectives that employees can control.
Controversy also surrounds the use of piece-rate pay. It is, perhaps, the most direct way to relate pay to performance. Even so, the literature is full of studies that describe adverse behaviour that piece-rate plans produce. Piece-rate plans often create adversarial relationships between employees and employers in matters that are inherent to productivity. These involve the determination of production rates, the establishment of informal limits on production, and the negotiation of off-standard piece-rate plans. In some situations, performance may decline in spite of higher rates of payment.
Unfortunately, the very existence of piece-rate plans, whether or not they have their intended effect in the form of increased productivity, creates an atmosphere that can be detrimental to safe job performance. For example, a study investigating the transition from piece-rate to time-based wages in the Swedish forestry industry found reduced accident frequency and severity. Following the wage system change, several hundred forestry workers were questioned about its effect on their job performance. They indicated three major reasons for the reduction, including:
- reduced pressure to work fast, take risks and ignore specific safety guidelines
- reduced stress, leading to fewer errors in judgement
- more time to consider safety matters, try new methods, and benefit from interactions with peers.
The Swedish experience was only partially corroborated by earlier research conducted in British Columbia in Canada. In this case, there were no differences in accident frequency between piece-work versus salaried “fallers” in the logging industry, although more severe accidents among piece-work fallers as compared with their salaried counterparts were reported.
In the final analysis, opinion remains divided as regards the potential uses and abuses of incentive wage systems, their contribution to increased productivity, and their effect on safety. Nevertheless, research supporting any of them is scarce, and what evidence exists certainly is not conclusive. Clearly, the effect of incentive compensation programmes on safety depends on their content, their mode of conduct, and the circumstances surrounding them.
Compensating wages
Economists have been studying the subject of extra pay for high-risk work in an effort to place an economic value on human life and to determine whether the marketplace already compensates for high-risk exposures. If so, it may be argued that government interventions to reduce risk in these areas are not cost-effective because workers are already being compensated for their exposure to increased hazards. Attempts to validate the compensatory wage theory have been made in the United States and England using available mortality estimates. At this time, it would appear that the compensatory wage theory has been supported to a degree in England but not in the United States.
Another problem that besets the compensatory wage theory is the fact that many workers are unaware of the true risks associated with their jobs, particularly occupational disease exposures. Surveys done in the United States suggest that large percentages of workers are not aware of their exposures to hazardous working conditions. Also, psychologically speaking, individuals have a tendency to minimize the importance of very low probabilities associated with their own death. As a result, even if workers were aware of the actual risks associated with their work, they would be willing to take those risks.
Although the issue of compensatory wages poses some intriguing theoretical questions which remain currently unresolved, the true danger of a compensatory wage structure relates to its underlying causes. When employers use extra pay in any form as an excuse for continuing a substandard safety and health programme, the practice is harmful and totally unacceptable.
Safety incentives
The term incentive can be defined as a reason for undertaking action with extra zeal in an effort to receive a reward. The use of incentives to motivate employees is a common practice throughout the world. Nevertheless, the value of incentive programmes is a subject of controversy among scientists and practitioners alike. Opinions range from the denial of any link between incentives and motivation to the contention that incentives are primary factors in the behaviour change process. Between these two extremes, there are those who see incentive programmes as a useful stimulus to improve productivity and those who see them as promoting the wrong sort of employee behaviour with results that are exactly the opposite of what is intended.
In the area of safety and health, opinions about the utility of incentive programmes are no less diverse. In some organizations, for example, management is reluctant to offer extra incentives for safety because it is already an integral part of job performance and needn’t be singled out for special emphasis. Another opinion suggests that offering incentives for improved safety performance diminishes the perceived intrinsic value of worker well-being on the job, which is, after all, the most important reason for emphasizing safety in the first place.
Along with the philosophical reasons for questioning the value of incentive programmes there are other issues that must be considered when discussing their merits or potential contributions as a safety promotion practice. These are problems related to the criteria upon which incentive programmes are based, the possibility for abuse of the programme by both employers and employees, and the maintenance of employee participation.
The criteria for awarding incentives are critical to the success of the programme. There are shortcomings attached to incentive programmes that are tied solely (1) to accumulating a certain number of safe days, (2) to lost-time injury rate (to workers’ compensation premium reduction), and (3) to some other accident-related measures. Accident criteria are not very sensitive. Success is measured negatively, by the reduction or non-occurrence of events. Because accidents are rare events, it can take a relatively long time for significant improvements to occur. Such indices do not assess an organization’s safety record but its reported accident record, which can be influenced by numerous factors not under the control of incentive programme participants.
Both employers and workers can abuse safety incentive programmes. Employers sometimes use incentive programmes as a substitute for the establishment of a legitimate safety and health management system or as a short-term cure for long-standing safety and health deficiencies that require much different and more fundamental treatment than can be rendered by a promotion effort. At the employee level, the principal form of abuse appears to be the failure to report an injury or incident for fear that either an individual or work group will not receive an award. The chance of this problem occurring appears to be increased when monetary incentives are at stake or financial incentive plans for improved safety performance are written into labour contracts or agreements.
The success of an incentive programme is heavily influenced by the nature of employee participation and their perceptions about its fairness. If goals are set too high or if employees cannot perceive how their personal efforts can affect reaching the goals, then the programme is not going to be effective. Also, the longer the distance between safe job performance and reward reception, the less influence the incentive system is likely to have. It is difficult to maintain worker motivation with an incentive programme that won’t pay off for several months or longer, and even then only if things go well for the entire period.
Clearly the pitfalls that have been described help to explain why many organizations hesitate to use incentive programmes as a safety promotion device. It is easy to design an incentive programme that doesn’t work. But, there is a good deal of evidence, both quasi-experimental and anecdotal, that documents the contributions of incentives to the successful operation of safety and health programmes. The use of incentives, awards and recognitions to motivate employees to perform safely is an accepted feature of both the OBM and the TQM models. In the OBM model, use of incentives to reinforce employee behaviour is critical to programme success. With TQM, rewards, promotions and other incentives are used to recognize individuals for contributions to process improvement. Also, at the group, team or company level, special days or other functions are used to celebrate achievement.
Broadly speaking, the use of incentives may be viewed to have a positive influence on employee attitudes and behaviour. When evaluation of safety and health performance is made part of the decisions to increase an employee’s pay, these factors take on added significance as important job-related requirements. As indicated above, accident rate and related measures present significant problems when they are established as the sole incentive criteria. In contrast, the use of positive safety performance measures in the form of behavioural or process improvements provide specificity for employee action and create an opportunity for frequent feedback and incentive distribution. The characteristics of successful incentive programmes appear to remedy some of the problems associated with performance criteria, programme abuse and the nature of employee participation. Although the research into these areas is far from complete, sufficient data are available to provide guidance for organizations that want to make incentive programmes part of their safety and health management system.
Employer and employee abuses are largely circumstantial in nature. The reasons that incentive programmes are used to remedy safety management deficiencies largely determine whether the abuse can be corrected. If management sees employee safety and health as a low-priority concern, then such abuse is likely to continue until circumstances force a change in policy. In contrast, if management is committed to making safety and health improvements, then the need for a comprehensive approach to solving problems will be understood and accepted, and the support role played by incentive programmes will be recognized and valued. Similarly, the problem of employees not reporting accidents can be substantially reduced by changing the criteria that govern how incentives are awarded.
Research has shown that, to be effective in holding employee interest, rewards must be both frequent and tied to improved performance. If possible, to stimulate the feeling of participation in an incentive programme, employees should be involved in the selection of safety performance priorities. In this regard, it is necessary to insure that attention to priority behaviours does not lead employees to neglect other important job functions. Specific criteria and means for successful job performance should be clearly communicated and frequent progress reports given to programme participants.
There is also some evidence that distinguishes between the effects of rewards that are perceived as “controlling” and those that are viewed as “informational”. Studies of these differences have found that rewards for achievement that recognize personal competence are stronger than those that simply provide positive performance feedback. One explanation for this finding is that employees perceive informational rewards, which recognize achievement and personal competence, to be under their own control, rather than in the hands of another person who gives or withholds rewards based on the performance being observed. Accordingly, the focus for control of informational rewards is within the employee, or intrinsic, as opposed to being outside the employee, or extrinsic, as is the case of controlling rewards.
In summary, the appropriate use of incentives can play an important helping role for organizations that use them wisely. They can increase employee interest in safety and can stimulate enhanced self-protective actions by workers.
Communication in safety promotions
Communications of various kinds are used to enhance the effectiveness of any safety promotion effort. The communication process can be summed up by the following question: “Who says what in which channel, to whom, with what effect?” Accordingly, communication programmes usually involve a source, message, medium, target and objectives.
Communications vary in terms of their coverage and impact. Safety posters, banners and other mass media are high in coverage, because they are easily exposed to large number of people over time. They are generally considered to be low in impact, because it is unlikely that every exposure will produce the desired effect. Mass media or one-way communications are most effective in increasing general awareness about safety and health topics, and giving directives or safety reminders. They can also be a useful vehicle for making employees aware of management’s general interest in their welfare. In contrast, person-to-person or two-way communication, either through group discussions or individual contacts, though low in coverage value, can be high in impact and lead to decisions to change behaviour.
Credibility of source is very important in safety and health communications. In the workplace, for example, knowledge of a task and its hazards and the setting of a good example are important to making supervisors credible sources of safety and health information.
With regard to communication content, the use of fear has been a topic of research and controversy for years. Fear messages are used to change attitudes about the risks involved in hazardous behaviours by frightening the target audience. The message goes on to reduce the fear it has instilled by providing methods to prevent the danger or lower the risk. Workplace examples include campaigns to promote the use of personal protective equipment, while non-workplace examples include anti-smoking campaigns and auto seat-belt programmes. The main argument against using fear messages is the contention that receivers block out or suppress the message. Reactions such as these are likely to occur when the highly threatening communications fail to reduce the fear and individuals feel personally or situationally unable to handle the danger.
If fear messages are used, the following precautions should be taken:
- The message should attempt to evoke a high level of concern, and stress the positive benefits of the action to be taken.
- The suggested preventive actions should be concrete, relatively detailed, and specific.
- The guidelines for risk reduction should be presented, at one time, immediately after the fear response is evoked.
- The suggested preventive actions must be understandable and perceived by the target audience to be effective in preventing danger.
- The source of the communication should have high credibility.
- Use of statistics or risk data should be specific to the workplace or situation.
Finally, safety and health communications should consider the target groups at which messages are aimed. For example, research has shown that fear messages are more effective with new employees than with seasoned employees, who can use their experiences to discount the message. Additionally, fear messages have been found to be especially effective in influencing employees who are not under direct supervision and are thus expected to comply with safety regulations on their own.
As an aid both to defining targets and establishing objectives, the use of employee surveys is recommended to assess prevailing levels of safety and health knowledge, attitudes toward safety management programmes and practices, and compliance with rules and procedures. Such measurements assist in pinpointing education and persuasion priorities, and set a baseline for later evaluations of the effectiveness of communication efforts.
Safety campaigns
Safety campaigns usually are conducted to focus employee attention on a specific accident problem and are frequently associated with a particular slogan or theme to maintain interest and visibility. They use mass media such as posters, banners, videotapes, booklets and a variety of written or oral communications. Campaigns may be aimed at increasing awareness, conveying information, and changing attitudes in an effort to produce behaviour change.
The intended effect of safety campaigns is the same as that of behaviour modification and other programmes that attempt to get employees, supervisors and managers to make safety an integral feature of proficient job performance. Compared with behaviour modification programmes, however, safety campaigns are much less precise in defining target behaviours and outcomes, and less rigorous in the reinforcement of these behaviours. Even so, the major objective of both approaches is to emphasize the importance of safe work practices with the expectation that they will become habitual in nature.
Unfortunately, few studies have examined the effectiveness of safety campaigns in occupational settings. Case histories of successful efforts are frequently described in occupational safety publications, but these reports are seldom accompanied by convincing empirical evidence. Research has been done on the behavioural effects of specific media, such as posters, which indicates some positive results and provides a basis for guiding campaign communications, but meaningful research on safety campaign effectiveness in industry is simply not available. Rather, most of the useful information on the effectiveness of safety campaigns comes from the field of highway safety, particularly as reported in the United States and Australia.
Among the general recommendations that flow from anecdotal reports, the study of media effectiveness, and experience with highway safety promotion, the following can increase the power of any safety campaign and deserve special emphasis:
- Conduct needs studies to select campaign targets, using employee feedback to supplement data gathered from other sources.
- Assure employee involvement in campaign planning and materials selection.
- Pilot test the campaign theme and materials on the intended target groups.
- Involve all levels of management in the campaign from the top person to the lowest line supervisor.
- Use emotional/persuasive themes more than rational/informative ones.
Safety campaigns are intended to support an organization’s total safety programme. For this reason, it is usually preferable to judge their effectiveness by how well they attain defined support objectives. These include maintaining interest in safety, expressing management’s concern for employee safety, generating employee participation in safety activities, increasing morale and reminding employees to take special precautions.
Attempts to use accident reduction criteria to measure the effectiveness of campaigns, though seemingly appropriate, are usually confounded by the effects of the existing safety programme. Also, because accidents and injuries occur rarely, they are relatively insensitive criteria for evaluating the effects of specific safety programme changes that deal with the human or behavioural components of the safety system.
Safety Incentive Programmes
Safety incentive programmes have their intended effect: a reduction in the loss due to accidents. They also have positive side-effects. For one thing, they are a profitable proposition in industry, as the savings usually exceed the costs. For another, they may lead to better company morale. Incentive programmes can help improve the general organizational climate and, therefore, make a positive contribution to productivity over and above the gain due to accident reduction. Group-based safety incentive programmes give workers a common cause with each other as well as with management. Reinforcing safe acts “removes the unwanted side effects with discipline and the use of penalties; it increases the employees’ job satisfaction; it enhances the relationship between the supervisor and employees” (McAfee and Winn 1989).
Cost-Effectiveness of Incentive Programmes
There have been many cases, in manufacturing, construction and other industries, in which the accident rate per employee was reduced by 50 to 80%. Sometimes the results are better still, as was the case in two mining companies in which the total lost days dropped by 89 and 98% respectively (Fox, Hopkins and Anger 1987). Sometimes the results are more modest. A cable plant reduced the accident costs per employee by 35%; a manufacturer of tobacco products by 31% (Stratton 1988); a grain processing and transportation company by 30%; a Pacific resort complex by 39%, and a manufacturer of food products by 10% (Bruening 1989).
These favourable effects continue to last over long periods of time. Incentive plans in two American mines were studied over periods of 11 and 12 years. In one mine the number of days lost due to accidents was reduced to about 11% of baseline and in another to about 2%. Benefit/cost ratios varied from year to year between 18 and 28 at one mine and between 13 and 21 at the other. There was no sign that the effectiveness of the incentive plans diminished over time at either mine (Fox et al. 1987). A high benefit/cost ratio—about 23 to 1—has also been observed for incentives for safety in the resort hotel business.
The ratios between benefits (savings due to accidents prevented) and programme costs (bonuses and administration) are usually greater than 2 to 1, meaning that companies can make money on such accident-prevention efforts. This is largely due to reduced fees to workers’ compensation boards and other insurance, as well as to increased production, reduced downtime and a lesser need for replacement workers.
Requirements for Effective Incentive Programming
Incentive programmes, when properly designed, carry the approval of the people to whom they are addressed, and in this respect they compare favourably with the other forms of safety motivation such as laws, rule books and policing, which are much less popular. To put it plainly: a small carrot is not only much better liked than a big stick, it is also much more effective. Only one negative side-effect has been noticed so far, and that is the tendency of people to under-report accidents when incentive programmes are in effect. Fortunately, such under-reporting has been found to occur with respect to minor accidents only (McAfee and Winn 1989).
Past experience with incentive programmes also shows that some programmes have had much greater effect than others. For instance, a German incentive plan which promised professional truck and van drivers a bonus of DM 350 for each half-year of driving without being at fault in an accident, produced a reduction in direct accident cost to less than one-third in the first year of application and remained at that level for over three decades (Gros 1989). In the California “good driver” experiment, where drivers in the general population were offered free extension of their driver’s licence by one year in return for each year of accident-free driving, the accident rate dropped by 22% in the first year of the programme (Harano and Hubert 1974).
An attempt has been made here to cull the ingredients of the most effective incentive plans from published reports. This has by necessity largely been based on inference, because to date there are no well-controlled experiments in which one particular incentive characteristic is being varied and all other factors are kept constant. For obvious reasons, such experiments are not likely to be forthcoming; industry is not in the business of running such experiments. Never the less, the items that appear in the checklist below would seem to make very good sense (Wilde 1988; McAfee and Winn 1989; Peters 1991).
Managerial vigour
The introduction and long-term maintenance of incentive programmes should be conducted with managerial vigour, commitment and coherence. Workers or drivers should not only be informed of the programme in existence, but they should also frequently be reminded of it in attention-catching ways. In order to motivate and to inform the relevant audience, those in charge of incentive programmes should provide clear and frequent knowledge of results to the audience (Komaki, Barwick and Scott 1978).
Rewarding the “bottom line”
Incentive programmes should reward the outcome variable (the fact of not having caused an accident), not some process variable like wearing safety glasses or seat-belts, being sober or obeying shop-floor safety rules. This is because rewarding specific behaviours does not necessarily strengthen the motivation towards safety. A potential safety benefit due to an increased frequency of one specific form of “safe” behaviour may simply be offset by road users less frequently displaying other forms of “safe” acting. “The risk is here that while the rewarded behaviour may improve, other related safe behaviours may deteriorate” (McAfee and Winn 1989).
Attractiveness of the reward
Incentive programmes can be expected to be more successful to the extent that they widen the difference between the perceived benefit of not having an accident and the perceived disadvantage of having an accident. Rewards for accident-free operation in industry have taken many different forms, ranging from cash to public commendation. They include trading stamps, lottery tickets, gift certificates, shares of company stock, extra holidays, promotions and other privileges. While the flexible use of money prevents satiation from occurring, merchandise, especially customized merchandise, may constitute a lasting reminder of the value of safety. Merchandise items also have a “value-added” component in the sense that they can be obtained at a lower price than the recipients would likely have to pay if they bought the items at retail. In the United States, a substantial industry has sprung up to provide the merchandise for safety prizes. Gift certificates hold a middle ground between cash and merchandise; they can be put to flexible use and yet be personalized and imprinted with a commemorative message. Drivers have been rewarded with cash, automobile insurance rebates and free licence renewal.
Awards do not have to be large to be effective. In fact, a case can be made for relatively small recognition awards, such as 1- and 5-year safe driving pins, these being preferable in some cases. Small awards make it possible to hand out awards more frequently, they are probably less conducive to under-reporting of accidents, and they may foster the internalization of pro-safety attitudes through the process of cognitive dissonance reduction (Geller 1990). When a small reward changes a person’s behaviour, that person may justify the change by reasoning that the change was for safety’s sake rather than due to the insignificant inducement. No such internalization of pro-safety attitudes is necessary when the external inducement is large, because in that case it fully justifies the behaviour change.
It should be noted, however, that the attitude-shaping effect of modest awards can take place only after the operators have changed their behaviour for whatever minor external inducement. So, the award should be desirable enough to achieve some behaviour change to begin with. Rewards should have “perceived value” in the minds of the recipients. In some cases, a small material reward might imply a major social reward because of its “symbolic function”. Safe behaviour may thus become the “right thing to do”. This might help explain why a modest incentive such as free licence renewal for one year produced a major reduction in the accident rate of California drivers. Moreover, analogous to earlier studies that found that accident rates in dangerous tasks (such as piece-work) were exponentially related (to the power of three) to higher wages, it may be suggested that relatively small increments in wages for having no accidents should reduce the accident rate by a larger amount (Starr 1969).
Progressive safety credits
The amount of the incentive should continue to grow progressively as the individual operator accumulates a larger number of uninterrupted accident-free periods; for example, the bonus for ten uninterrupted years of accident-free operation should be greater than ten times the bonus for one year of accident-free performance.
Programme rules
The operational rules of the programme should be kept simple, so that they are easily understood by all persons to whom the programme applies. It is of paramount importance that the incentive programme should be developed in cooperation and consultation with those people to whom it will be applied. People are more likely to actually strive for goals they have helped define themselves (Latham and Baldes 1975).
Perceived equity
The incentive programme should be perceived as equitable by those to whom it is addressed. The bonus should be such that it is viewed as a just reward for not causing an accident in a given time period. Similarly, incentive systems should be designed such that those workers who are not eligible for the (top) award do not resent the system, and that those who are rewarded will be seen by others as justly receiving the award. As chance plays a part in having or not having an accident, the actual receipt of the award may be made dependent on the additional requirement that the accident-free worker in question also maintains cleanliness and safety in his or her workstation. In the event that disincentives are used as well, it is necessary that the public view the penalty imposed as justified.
Perceived attainability
Programmes should be designed such that the bonus is viewed as within potential reach. This is of particular importance if the bonus is awarded in a lottery system. Lotteries make it possible to hand out greater awards, and this may enhance the attention-getting appeal of an incentive programme, but fewer among the people who have accumulated the safety credit will receive the bonus. This, in turn, may discourage some people from making an active attempt to accumulate the safety credit to begin with.
Short incubation period
The specified time period in which the individual has to remain accident-free in order to be eligible for the bonus should be kept relatively short. Delayed rewards and penalties tend to be discounted and are thus less effective in shaping behaviour than more immediate consequences. Periods as short as one month have been used. If longer periods apply, then monthly reminders, status reports and similar materials should be used. In the California experiment cited above, those drivers whose licenses were coming up for renewal within 1 year after being informed of the incentive programme showed a greater reduction in accident rate than was true for people whose licenses were not to be renewed until two or three years later.
Rewarding group as well as individual performance
Incentive programmes should be designed to strengthen peer pressure towards having no accident. Thus, the plan should not only stimulate each individual operator’s concern for his or her own safety, but also motivate them to influence peers so that their accident likelihood is also reduced. In industrial settings this is achieved by extending a bonus for accident-free performance of the particular work team in addition to the bonus for individual freedom of accidents. Team bonuses increase the competitive motivation towards winning the team award. They also have been found effective in isolation—that is, in the absence of awards for individual performance. A dual bonus plan (individual cum team) can be further strengthened by informing families of the safety award programme, the safety goals and the potential rewards.
Prevention of accident under-reporting
Thought should be given to the question of how to counteract operators’ tendency not to report the accidents they have. The possibility that incentive programmes may stimulate this tendency seems to be the only currently identified negative side-effect of such programmes (while occasionally moral objections have been raised against rewarding people for obtaining a goal they should aspire to on their own, without being “bribed into safety”). Some incentive programmes have clauses providing for deduction of safety credits in case accidents are not reported (Fox et al. 1987). Fortunately, only those accidents that are minor remain unreported at times, but the greater the safety bonus, the more frequent this phenomenon may become.
Reward all levels of the organization
Not only are shop-floor workers to be rewarded for safe performance, but their supervisors and middle management as well. This creates a more cohesive and pervasive safety orientation within a company (thus shaping a “safety culture”).
Whether or not to supplement rewards with safety training
Although educating towards safety is different from motivating towards safety, and a person’s ability to be safe should be clearly distinguished from that person’s willingness to be safe, some authors in the field of incentives in industrial settings feel that it may be helpful to safety if workers are told through what specific behaviours accidents can be avoided (e.g., Peters 1991).
Maximizing net savings versus maximizing benefit/cost
In the planning of an incentive programme, thought should be given to the question of what actually constitutes its primary goal: the greatest possible accident reduction, or a maximal benefit/cost ratio. Some programmes may reduce the accident frequency only slightly, but achieve this at a very low cost. The benefit/cost ratio may thus be higher than is true for another programme where the ratio between benefits and costs is lower, but which is capable of reducing the accident rate by a much greater degree. As distinct from the issue of the size of the benefit/cost ratio, the total amount of money saved may well be much greater in the latter case. Consider the following example: Safety programme A can save $700,000 at an implementation cost of $200,000. Programme B can save $900,000 at a cost of $300,000. In terms of benefit/cost, A’s ratio is 3.5, while B’s ratio equals 3.0. Thus, judged by the benefit/cost criterion, A is superior, but if net savings are considered, the picture is different. While programme A saves $700,000 minus $200,000, or $500,000, programme B saves $900,000 minus $300,000, or $600,000. In terms of net savings, the larger programme is to be preferred.
Concluding Comment
Like any other accident countermeasure, an incentive plan should not be introduced without evaluating its short-term and long-term feasibility and its best possible form, nor without provision for scientifically adequate evaluation of its implementation costs and its observed effectiveness in reducing the accident rate. Without such research the surprising effect of one particular reward programme would never have come to light. Although there seems little chance for a safety incentive to actually have a negative effect, there is one variation of a series of California reward/incentive programmes for the general driving public that did produce worse driving records. In this particular programme component, a benefit was given to drivers with no accidents on their records without their prior knowledge of that benefit. It took the form of an unexpected reward rather than an incentive, and this highlights the importance of the distinction for safety promotion. The term incentive refers to a pre-announced gratification or bonus extended to workers or drivers on the specific condition that they do not have an accident of their own fault within a specified future time period.
Successful Safety Programmes
The moral imperative of an enterprise to actively seek to reduce damages, pain and suffering in the workplace will be tempered by the ability of the organization to sustain such an effort. Most human activities have risk attached to them, and risks in the workplace vary widely, from those much lower than those associated with normal, non-occupational activities, to very significantly more hazardous ones. An essential part of an organization is its willingness to accept the risks of business which have the potential for producing financial losses and are based on the pain and suffering of employees that result from accidents. A successful safety programme is intended to control a portion of these losses by reducing the risks, particularly where such risks arise from unsafe conditions or unsafe acts. The safety programme, therefore, is simply another subsystem of management. Like other management programmes, the safety programme consists of complementary strategies, procedures and standards. Similarly, the measure of a safety programme is performance—that is, how well it reduces accidents and the consequent losses.
A safe workplace depends on the control of hazards and unsafe behaviours, and control such as this is the primary function of management. A safety programme should produce complementary benefits: a reduction in damages and pain and suffering in the workforce (from both acute and chronic injuries and illnesses) and a resultant reduction in the financial burden to the organization due to such accidents. To achieve such benefits, a successful safety programme will follow the general approach of all management tools by establishing goals, monitoring performance and correcting deviations. This approach will be applied to a rather wide range of organizational activities, including organizational design, the production processes and the behaviour of the workers.
Safety in the Enterprise
A safe workplace is the end product of a complex and interactive process, and each process is a characteristic of an individual organization. A typical process is described in figure 1. The successful programme will need to address the various aspects of such a system.
Figure 1. The management process and occupational safety
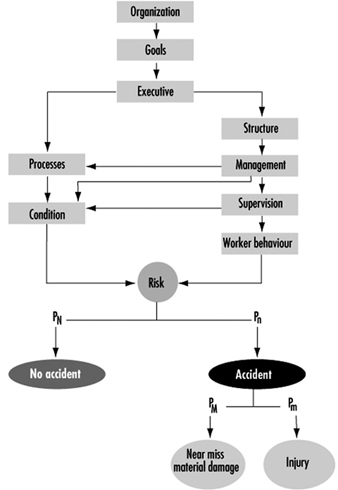
Safety is often seen as a worker/workplace issue, but figure 1 indicates the pivotal role of management in safety as it responds to the overall goals of the organization. This can be seen from management’s clear responsibility for the selection of the industrial processes utilized, the control of supervision, working conditions, and the attitudes and procedures of the worker, all of which are factors that establish the extent of a risk in a particular workplace. Usually there is a large probability that no accident will occur, and a small probability that there will be an accident leading to either material damage or injury to a worker. A safety programme is concerned with reducing that risk and also minimizing injuries that occur.
Understanding the Accident Process
There are several competing theories of accident causation, but the model first proposed by Frank Bird (1974) is particularly valuable, as it provides a ready analogy which is compatible with many management practices. Bird likened the process that leads to injury or damage to a row of dominoes, standing on edge (see figure 2). When any domino falls, it can disturb the others and a sequence is actuated which eventually leads to the fall of the final piece, corresponding to the occurrence of an injury. This analogy implies that if any one of the dominoes is removed from the sequence, or is robust enough to withstand the previous impact, then the chain of events will be broken and the ultimate event of injury or damage will not occur.
Figure 2. The Bird domino theory as modified by E. Adams
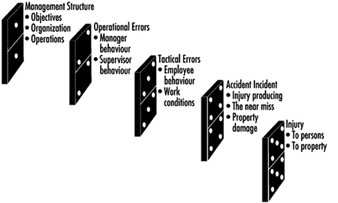
Despite more recent models, this approach is still valuable, for it clearly identifies the concept of interventions in the accident process and the role of the effective safety programme in introducing them to inhibit the process and prevent injury.
Organizational Goals
There is little disagreement among authors that the single most significant aspect of any safety programme is the visible continuous commitment of senior management. This commitment must be recognized and reflected by succeeding levels of management down through the supervisory ranks. Although executive management often believes its concern with safety is apparent to all in the enterprise, such clarity can be lost at the successive layers of management and supervision. In successful safety programmes, the executive management must demonstrate a clearly identified commitment to the concept that safety is a responsibility of all employees, from senior management to the temporary worker. Such a commitment should take the form of a brief written document, provided for everyone in the enterprise and utilized at the earliest possible stage for inducting new workers into the organization. Some organizations have recently extended this by introducing the concept that the commitment to a safe and healthy workplace for all its employees and customers is an explicit corporate value. Such corporations frequently express this point of view in written documents, together with more traditional corporate values, such as profitability, reliability, customer service and community commitment.
Clarity of communication is particularly important in large organizations, where the direct link between the owners of the enterprise and the workforce can easily be broken. One of the clearest ways to achieve this is by the development of a series of written policies and procedures, starting with senior management’s establishing objectives for the safety programme. These should be clear, concise, achievable, supportable and, above all, unambiguous. It is not sufficient for a manager to assume that everyone down the chain of command shares a similar background, understanding and perception of the safety programme. These aspects must be made perfectly explicit. Equally, in spelling out the terms of this written procedure, it is essential to have realistic goals.
Management Control
Developing effective safety programmes from this original commitment requires that the measurement of safety performance be an integral part of the annual performance review of all management and supervisory staff. In keeping with the philosophy that safety is only one measure, among many, of the manager’s control of the process, safety performance must be included along with output, cost per unit, and profitability of the department. Such a philosophy, insofar as accidents occur from a lack of control of the process, appears to be highly compatible with the contemporary emphasis on total quality management (TQM). Both procedures adopt the position that deviations from normal are minimized in order to provide more control in achieving the corporate objectives. Additionally, the TQM concept of year-by-year, incremental improvement, is particularly significant in the long-term management of safety programmes.
Training and Education
Training and education are major components of any safety programme. This begins with the dissemination from senior management not only of the programme’s objectives and goals, but also information on progress towards those goals, measured through record keeping and cost accounting. Education, by which is meant a more general understanding of the nature of a hazard and of approaches to risk reduction, appears to work well, particularly in circumstances where there is still doubt about individual risk factors. One example is the epidemic of upper extremity cumulative disorders in Australia, Europe and North America. These disorders have become more significant, especially given that broad agreement does not exist on criteria for control of these disorders. The cumulative nature of such disorders, however, makes control of this problem particularly amenable to education. An increased awareness of risks allows individual workers to avoid such conditions by recognizing their exposures and modifying them by changes to procedures. Similarly, an understanding of the mechanics of low-back stresses can prepare workers to avoid some potentially dangerous work practices and substitute safer methods of accomplishing tasks.
Training is as necessary for management and supervisors as it is for the workers, so that they develop an understanding of their responsibilities and duties and increase their awareness levels of hazard potential. Individual workers need to be provided with clear and unambiguous process-relevant procedures for safe working. They should have an understanding of the hazards involved in the particular operations, and the likely effects of exposures to both toxic and physical agents. Additionally, managers, supervisors and workers should be familiar with the procedures for minimizing losses once an accident has occurred.
Safe Behaviour
Philosophically, the twentieth century has seen several swings in which safety programmes have allocated varying amounts of responsibility for the behaviour of workers to the individual, the employer and society. However, it is clear that safe behaviour is an absolutely crucial part of the safety process. An example of the significance of such behaviour is the development of group ethics, or team norms, in which the assumption of a risk by an individual might be perceived negatively by other members of the group. The converse is true: the acceptance of dangerous practices can become accepted as “normal”. Such behaviours can be modified by specific procedures of training and reinforcement, as shown by the highly successful programmes that combated the spread of AIDS from careless needle use in the health care industry. The heightened emphasis by management, coupled with training and educational materials, fundamentally changed the procedures involved and reduced the incidence of this hazard.
Participation
Increasingly, societies are mandating worker participation in safety programmes. Although the validation of such participation tends to be somewhat variable, worker involvement can be valuable at several stages in the safety process. Undoubtedly the people who are exposed to the hazards are extremely valuable resources for identifying hazards, and frequently are aware of potential solutions for reducing them. When problems have been identified and solutions have been developed, implementation will be greatly facilitated if the workforce has been a partner in record keeping, identifying, developing and validating the proposed interventions. Finally, in terms of understanding management’s commitment and resource constraints, participation embodied in a safety programme is beneficial.
Incentives
Incentives have been widely promulgated in some countries for increasing safe behaviours. The evidence that these incentives work is far from convincing, although, as part of a comprehensive safety programme, they can be used to demonstrate management’s continuing concern with safety, and they can form a significant feedback of performance. Thus, those safety programmes in which a small financial award is mailed to a recipient are likely to be ineffective. The same award, made in public by senior management, and based on specific performance measures—for example, 2,500 hours of work without any accidents—is likely to form positive reinforcement. In practice, in many industries the reverse is true—there are considerable incentives that reward poor safety behaviours. For example, piece-rate payment systems clearly reward workers for cutting out any time-consuming elements in a work cycle, including any which may be related to safe working procedures. Enterprises using incentives are more likely to need engineering controls and active surveillance techniques if they are truly committed to protecting the health and safety of the workforce.
Measurement and Control
Information is the lifeblood of management, and record keeping is an essential part of management information. Without a good source of data, progress toward accident reduction will be unreliable, and management’s willingness to expend resources to reduce risks is likely to be impaired. In some countries, collection of such data is a legislative requirement, and clearly a successful safety programme must facilitate the gathering and collation of such data. Satisfaction of regulatory requirements may be necessary, but frequently is not sufficient for a successful safety programme. Local variations in such data requirements may occur—for example, between jurisdictions—with the result that the value of such data is obscured; this development is a particular problem in organizations with multiple locations located in different regional or national jurisdictions. Consequently, the standardization of, and approach to, data collection must be specifically established as part of the safety programme. Thus, each programme must first identify the information needed for compliance with regulations, but then determine the need for further collection and analysis necessary for accident reduction.
Costs of Accidents
An essential management aspect of the data system is the identification of the cost of losses. Loss source analysis—that is, the determination of the actual sources of losses—will include the measurement of the number of incidents, the severity of incidents and the direct costs of damages, injuries and illnesses. Such information is essential if management is to maintain its focus on the true problems in the workplace. In many countries, the compensation costs—whether borne directly by the employer, by a federation, or by a state organization—can be assumed to be proportional to the pain and suffering in the workplace. Thus, in identifying the source of loss, management is discharging its responsibility for providing safe working conditions for the workforce in a way that is highly compatible with the cost/benefit analysis approach used in other activities.
Direct costs are not the true financial costs from accidents and injuries borne by an enterprise. In many countries around the world, and with various degrees of rigour, attempts have been made to estimate indirect costs associated with accidents. These indirect costs include loss in supervisory time, loss of productive time during the accident investigation and cleanup, retraining of replacement workers, and the amount of overtime required to meet production schedules. These indirect costs have been found to exceed the direct costs substantially, often by factors estimated to be in a range of three to ten times those of the direct insurance losses.
Determining Costs
The measurement of losses normally involves passive surveillance, which requires that the preceding history be examined in terms of frequency and severity of accidents. Passive surveillance is not sufficient for certain situations, particularly those with very low probabilities of errors occurring, but large, uncontrolled potential damage in the case that they do occur. In such circumstances, particularly in complex process industries, it is necessary to perform an assessment of potential losses. It is clearly unacceptable that, simply because no process has yet claimed a victim, processes involving large amounts of energy or of toxic materials should not be analysed prior to such an accident. Thus, in some industries, it is wise to institute active surveillance, particularly where similar processes elsewhere have led to losses. Information from trade associations and from national and international labour and safety organizations is a valuable source that can be used to establish pre-incident estimates which are likely to be valid and valuable. Other techniques, including fault tree analysis and failure mode analysis, are discussed elsewhere in this Encyclopaedia. In circumstances such as those involving chemical exposures, active surveillance may include routine medical examinations of the worker. Such an approach is particularly significant where well-established limit values have been determined. This approach of estimating potential and actual losses highlights a feature that the successful safety programme should address, and that is the difference between day-to-day risk and the effect of a potential catastrophe.
Information Feedback
The use of information feedback has been shown to be crucial in a wide range of organizational activities, including safety programmes. The calculation of both incidence rates and severity rates will form the basis for rational deployment of resources by the enterprise and for measuring the success of the programme. This information is as valuable to management for evaluating the safety function as it is to workers in the execution of the programme. However, the presentation of such data should reflect the end user: aggregated data will allow management comparison of operating units; department-specific data and visual aids (such as thermometer charts indicating the number of safe work days at the shop-floor level) can enhance understanding of, and buy-in from, the whole spectrum of employees.
Field Observation
The information system is an off-line component of a successful safety programme, which must be complemented by a hands-on approach to safety in the workplace. Such an approach would involve the walk-through, in which an informed and trained observer subjectively identifies hazards in the workplace. In addition to identifying hazards, the walk-through is particularly suitable for detecting issues of non-compliance with both corporate and legislative requirements. For example, the reduction of hazards by machine guarding is ineffective if many of the machines have had the guards removed—a typical finding of a walk-through. As the walk-through is an open-ended and adaptive procedure, it is also the easiest way to detect deficiencies in the training of the worker, and possibly those of the supervisor.
Effective safety programmes should utilize this technique on a regular but random basis. The walk-through, however, is not the only way of identifying hazards. The workers themselves can provide essential information. In many cases, they have experience of “near misses” that have never been reported, and are consequently in a good position to discuss these with the safety officer during the walk-through. Workers in general should be encouraged by supervision to report safety defects both actual and potential.
Accident Investigation
All accidents must be investigated by the responsible supervisor. Accidents such as those in the process industry often require investigation by a team of knowledgeable persons representing diverse interests, possibly including an outside expert. Successful programmes frequently involve workers in such accident investigations. This involvement brings benefits in terms of better understanding of the incident and of rapid dissemination of recommendations throughout the workforce. From figure 1, it is clear that, in this context, accidents are not only those events that conclude in an injury to a worker, but rather, events that encompass damage to equipment or materials or even significant events that result in neither (known as “near accidents”). The figure indicates that such incidents should be subject to management investigation and control even if, fortuitously, no worker is injured. Avoidance of similar incidents in the future will reduce the risk that they will result in injury. Accident investigations that seek to lay blame appear to be less successful than those seeking methods to determine cause. In an investigation that is seen to be an attempt to blame a worker, peer pressure and other psychosocial behaviours can severely degrade the quality of information collected.
The essentials of an accident report will include a formalized process, involving written descriptions of the events that occurred before, during and after the accident as well as an assessment of the factors that led to the accident. The report should end with a clear recommendation for action. The recommendation could range from immediate modification of the work process or, in the case of complex situations, to the need for further, professional investigation. Such reports should be signed by the responsible supervisor or the leader of the investigation team, and forwarded to an appropriate level of management. Management review and acceptance of the recommendations is an essential part of the accident reporting process. The signature of the manager should indicate his or her endorsement or rejection of the proposed changes to prevent future accidents, and rejections should be accompanied by an explanation. Accident investigations that do not lead to an individual responsibility for action for the recommendations are likely to be ineffective, and rapidly become viewed by all involved as irrelevant. A successful safety programme seeks to ensure that lessons learned from a particular incident are shared elsewhere within the organization.
Hazard Control
The best intervention as regards hazard control will always be the removal of the hazard by engineering design, substitution or modification. If the hazard is removed (or, at second best, shielded or guarded), then irrespective of the human variability arising from training, individual differences of strength, attention, fatigue or diurnal rhythm, the operator will be protected.
Unfortunately, in some cases, the costs of achieving this engineering design can reach or exceed the limits of economic liability. Certain processes are inherently much riskier than others, and feasible engineering designs are only partial solutions. Construction projects carried out at elevated sites, deep coal mining, steel production and over-the-road driving all require exposure of employees to higher than “normal” risks. In such cases, administrative control and personal protective devices may be necessary. Administrative control may involve specific training and procedures to reduce risks: consider, for example, the prohibition against individual workers entering confined spaces, or the provision of lockout systems designed to isolate dangerous equipment and processes from the operator during the work cycle. These procedures can be effective, but require continual maintenance. In particular, work practices tend to move away from compliance with the necessary administrative procedures. This trend must be halted by the implementation of procedures for training, and refresher training as well, for all workers and supervisors involved in the system.
The final component in hazard control is the use of personal protective devices, which include respirators, protective gloves, whole-body harnesses and hard hats, to mention just a few. In general, it can be seen that such devices are valuable when the hazards have not been entirely removed from the workplace, nor controlled by administrative procedures. They are intended to reduce the effect of such hazards on the worker, and typically are subject to concerns of improper use, design limitations, inadequate supervisor oversight, and failure of maintenance.
First Aid
Despite the best attempts to reduce hazards, the successful safety programme must address the post-accident scenario. The development of first aid and emergency medical treatment capabilities can provide major benefits for the safety programme. A protocol must be established for medical treatment following an accident. Selected workers must be familiarized with the written instructions for summoning medical assistance to the worksite. Such assistance should be prearranged, for a delay can seriously affect the condition of an injured worker. For accidents producing minor injuries, the inherent losses can be reduced by the provision of point-of-incident medical treatment. In-plant treatment for minor cuts and bruises, contusions and so on, can reduce operators’ time away from their tasks.
The first aid capability must include acceptable levels of supplies, but more important, adequate medical/first aid training. Such training can directly affect the probability of survival in case of a potentially mortal injury, and can reduce the actual severity of a range of less serious accidents. First aid action such as cardiopulmonary resuscitation, or the stabilization of haemorrhaging, can make the difference between life and death to patients in need of major emergency treatment. Frequently, the provision of immediate first aid at the accident site provides the opportunity for subsequent major surgical interventions. Such a capability is even more significant in nonurban enterprises, where medical treatment may be delayed by a matter of hours.
First aid can also facilitate the efficient return to work of a worker involved in a minor injury. Such in-house intervention has been shown to reduce the need for lengthy medical visits outside the enterprise, and thus prevents a loss of productivity. Perhaps even more significant is the reduced chance of the medicalization of the injury, which is seen as an emerging problem in several countries.
Catastrophe Planning
Routinely, at least annually, a safety programme should identify potential causes of catastrophe. In some circumstances—for example, with the storage of large amounts of flammable or hazardous materials—the focus of attention is not too difficult. In other circumstances, great ingenuity may be required to make meaningful suggestions to plan for such catastrophes. By definition, catastrophes are rare, and it is unlikely that a particular enterprise would have suffered a similar catastrophe earlier. Definition of medical management, communication flows and managerial control of the catastrophe situation should form part of the safety programme. It is clear that in many enterprises such annual plans would be rather minimal, but the very exercise of developing them can be valuable in increasing the management’s awareness of some of the risks that the business assumes.
Conclusion
The successful safety programme is not a book, or a binder of notes, but a conceptual plan to reduce the risks of injury as measured on the basis of both incidents and severity. Like all other processes in an enterprise, the safety process is the responsibility of management rather than that of a safety engineer or an individual worker. Management is responsible for setting the goals, providing resources, establishing means of measuring progress towards those goals and taking corrective action when this progress is unsatisfactory. In order to do this, information is the key requirement, followed in importance by communication of the objectives at all levels within the enterprise. At each level, from executive through management supervisor to the individual worker, contributions to safe working conditions can be made. But at the same time, organizational, procedural and behavioural inadequacies may regrettably prevent such contributions from occurring. The successful safety programme is one which recognizes and utilizes such factors in developing an integrated approach to reducing the pain and suffering in the workplace which arises from injuries and disease.
Implementation of a Safety Programme
The implementation of a safety programme should reflect its nature as a normal, day-to-day concern of general management. The need for information for decision making at all stages and for communication between all levels of the enterprise form the basis for successful implementation of such a programme.
Executive Level
Initially, the introduction of a new or modified safety programme will require the agreement of senior management, who may regard it as a cost/benefit decision to be made in light of competition for resources from elsewhere in the enterprise. The desire to reduce damages, pain and suffering in the workplace through the implementation of a safety programme will be tempered by the organization’s ability to sustain such an effort. Informed management decisions will require three elements:
- an explicit description of the programme, which fully defines the proposed approach
- an assessment of the impact of the programme on the company operations
- an estimate of the costs of implementation with a prediction of the benefits that are likely to be produced.
The only exception to this will be when a safety programme is mandated by regulation and must be instituted in order to remain in business.
In the latter endeavour, it is useful to add an estimate of the true costs of the current safety record of the enterprise, as well as those costs covered by direct insurance or direct out-of-pocket expenses. The indirect costs are likely to be significant in all cases; estimates for serious incidents in the United Kingdom suggest that the real costs (borne by an enterprise as indirect costs) range from a factor of two to three up to a factor of ten times the actual, direct insurance costs. In those countries requiring compulsory insurance, the cost, and hence the savings, will vary widely depending on the social environment of each particular nation. Insurance costs in countries where the insurance carriers are required to cover full medical and rehabilitation costs, such as the United States, are likely to be higher than those in countries in which the treatment of the injured worker is part of the social contract. An ideal way to emphasize the significance of such losses is to identify the annual production required to generate revenue lost in paying for these losses. This is highly compatible with the concept that, while a business must necessarily assume the risk of doing business, it should be managing that risk in order to reduce the losses and improve its financial performance.
Management Level
Following acceptance at the senior management level, an implementation team should be formed to develop the strategy and the plan to introduce the programme of the roll-out plan. Such an approach is more likely to be effective than one that shifts the responsibility for safety to an individual designated as the safety engineer. The size and level of the involvement of this implementation team will vary widely, depending on the enterprise and the social environment. Nevertheless, input is essential from at least those with responsibility for operations, personnel, risk management and training, as well as key representatives of employee groups who will be affected by the programme. It is likely that a team of this composition will detect possible conflicts (for example, between production and safety) early on in the process, before attitudes and positions, as well as procedures, hardware and equipment, have become fixed. It is at this point that collaboration, rather than confrontation, is likely to provide a better opportunity for problem solving. The output of this team should be a document that identifies the corporate view of the programme, the key elements of the programme, the schedule for implementation and the responsibilities of those involved.
Care should be taken to ensure that the executive commitment is particularly evident to managers at the operational level at which the safety programme can be effected. Perhaps the most significant way of achieving this is to establish a form of chargeback, or allocation of the true costs of an accident directly to this level of management. The assumption of medical and indemnity costs (or their associated insurance costs) as a corporate overhead should be avoided by management. The unit manager, concerned with day-to-day financial control of the organization, should have the real costs of inadequate safety programmes appearing on the same balance sheet as the production and development costs. For example, a unit manager of an organization in which all the workers’ compensation costs are carried as a corporate overhead will be unable to justify expenditure of resources to remove a very serious hazard affecting a low number of workers. This difficulty can occur at the local level, despite the fact that such expenditures could produce major savings at the corporate level. It is essential that managers who are responsible for workplace design and operations bear the brunt, or reap the benefits, of the safety programme for which they are responsible.
Supervisor Level
The supervisor is responsible for understanding, transmitting and ensuring compliance with the managerial objectives of the safety programme. Successful safety programmes will address the question of educating and training supervisors in this responsibility. Although special safety trainers are sometimes used in educating workers, the supervisor should be responsible both for this training and for the attitudes of workers. In particular, informed supervisors see their responsibility as including the prevention of unsafe acts and exhibiting a high level of intolerance of unsafe conditions in the workplace. The control of the manufacturing process is accepted as the mainstream responsibility for supervisors; the application of such control will also produce benefits in the reduction of damages and unintentional injuries. Regardless of whether the safety function is staffed by safety officers, joint worker-management committees or consultants, the day-to-day responsibility for safe, error-free operation of the process should be a written component in the job description of supervisors.
Worker Level
At the beginning of the century, the primary emphasis for workers to perform safely was placed on negative reinforcement. Rules were set, workers were expected to follow those rules without question, and a transgression from the rules subjected the worker to disciplinary action. With increasingly complicated workplaces, flexible management systems and the rising social expectations of the workforce, the inadequacies and liabilities of such an approach have been revealed. It is not only in the military arena that flexibility and responsibility at the local level appears to be a vital component of high-performance units. This approach has led to an increasing reliance upon positive reinforcement and empowerment of the workforce, with the concomitant requirements for education and understanding. This thrust in safety mirrors the worldwide trend of labour to seek improvements in the quality of working life and the development of self-directed working groups.
Roll-out Plan
The key elements of the safety programme will identify the requirements for familiarization with the conceptual basis of the programme, the development of specific safety skills and the implementation of measurement tools. Responsibilities will be assigned to specific people within a phased programme at the point of introduction. The end of the roll-out process will be the establishment of a measurement system, or safety programme audit, in order to assess the continuing performance of the programme. Appropriate communication must be explicitly specified in the plan. In many cultures, multiple dialects and languages coexist in the workplace; and in certain cultures, a “managerial” dialect or language may normally not be used by the workforce. This problem includes the use of jargon and acronyms in communication between groups. Worker participation in the roll-out design may avert such shortcomings, and lead to solutions such as multilingual instructions and guidelines, a wider use of symbols and pictograms, and the selection of simple language. The wider approach to worker participation in the plan will produce benefits in terms of “buy-in” and acceptance of the plan’s goals and approaches.
The review process, or safety programme audit, should be repeated on a regular (annual) basis and will form the basis for 3-year rolling (or cyclical) plans. These plans will establish the future direction of the programme and provide the impetus for continual improvement, even in the face of changing production and process systems.
Continuous Improvement
Successful safety programmes do not remain static, but change to reflect changes in both corporate and social environments. Equally, successful programmes avoid dramatic but unachievable goals. Instead, a philosophy of continuous improvement and of continually rising standards is a key approach. The annual 3-year rolling plan is a good way to achieve that. Each year, the plan identifies broad goals and estimates with respect to likely costs and benefits that will develop over the next 3-year period. This will automatically provide for adaptation and continued improvement. As such plans are to be reviewed by management each year, an additional benefit will be that the objectives of the safety function are continuously aligned with corporate objectives.
Conclusion
The implementation of the safety programme must reflect its being an integral component of the management of the enterprise. Success would depend on clearly identifying the responsibilities of the various levels of management. The participation of workers in the implementation programme, and particularly the roll-out plan, is likely to produce benefits in the widespread adoption of the plan. The roll-out plan is a document which identifies the necessary activities, the timing of those activities and the responsibility for implementing each activity. The components of each activity—whether training, development of a working procedure or education—must be described in a way that is unambiguous to all levels of the enterprise. The final stage in the roll-out plan is to ensure that a continuous improvement cycle can occur by the installation of a safety programme audit on at least an annual basis.
Safety Services: Consultants
Occasionally, those responsible for safety in an organization—whether they be concerned with the behavioural system, the safety system or the physical environment—call upon external resources such as professional safety consultants for help. When this occurs, it is important to bear in mind that the responsibility for the successful completion of the task (as distinguished from the performance of the task itself) of analysing a given system and making improvements to it cannot be delegated to outside agencies. Internal analysts (as opposed to external consultants) studying a system can usually obtain more reliable data because of their close familiarity with the organization. Nevertheless, the help of an outside consultant who has a wide range of experience with analysing safety problems and suggesting appropriate remedies, can be invaluable.
Seeking Outside Help
If there is no one in an organization who is familiar with safety laws and standards on the national level, it might be helpful to call in a safety regulations expert for assistance. Often there is no one in the organizational structure who may be able to analyse the behavioural system, and in such an eventuality it would be advisable to obtain help from someone who can do so. Kenneth Albert (1978) suggests that there are six specific occasions when outside help should be obtained:
- when special expertise is essential
- for a politically sensitive issue
- when impartiality is necessary
- if time is critical and the internal resources are not immediately available
- if anonymity must be maintained
- when the prestige of an outsider would be helpful.
Although Albert’s remarks were not made in connection with safety, the above points seem valid in determining the need for an outside safety consultant. Often a safety problem is intertwined with managerial personalities and is extremely difficult to solve internally. In such a situation a solution may be acceptable to all parties involved just because it came from an outsider. If an organization needs an analysis in a hurry it often can be done faster by an outside consultant, and often the outsider’s recommendation will carry more weight than the insider’s. In the field of safety, it appears that outside help is needed by many organizations with behavioural system analysis, some with safety system analysis and a few with physical condition analysis. However, with regard to the availability of safety consultants, supply and demand are inversely related, as there seems to be an ample supply of physical condition consultants, whereas there are fewer safety system analysts, and safety behavioural analysis experts are almost non-existent.
Safety Consultants
While the types of external safety consultant help will vary by country, they might generally be classified into these categories:
- insurance company field safety engineers or consultants
- government safety consultants (national, state, provincial and local)
- private consulting firms and full-time professional safety consultants
- part-time private consultants
- safety council or safety association consultants
- industry association consultants.
Insurance consultants. Most of the safety consultants and safety engineers in the United States who do not work for government or industry are employed by insurance firms. Many other safety professionals started their careers working for insurance companies. Almost all companies, except the very large and self-insured, are helped routinely by insurance loss-control representatives.
Government consultants. The providers of government consulting services vary from country to country and as to their affiliation (national, state, provincial or local) and the sorts of tasks they are permitted and qualified to perform. In the United States, the stated goal of the onsite consultation programme offered by the Occupational Safety and Health Administration (OSHA) is to obtain “safe and healthful workplaces for employees”. Thus by stipulation, the consultations will pertain only to physical conditions. An organization seeking this kind of help should consider OSHA’s offering. If, however, consulting help is needed with the safety system or the behavioural system, OSHA is the wrong place to go.
The defined onsite responsibilities of OSHA consultants are as follows:
- to identify and properly classify hazards
- to recommend corrective measures (short of engineering assistance)
- to arrange abatement dates for serious hazards
- to report to their supervisors any serious hazards which the employer has not acted upon
- to follow up on employer actions.
It is obvious that there are some aspects of receiving OSHA consulting service by this route that are unusual. The purpose of the consultants is to help improve physical conditions, but in two instances the consultants have additional duties:
- In the case of serious violations of OSHA standards, they must set abatement dates and follow up on them.
- In the case of imminent violations of the OSHA standards, they must refer them to either their supervisors (and thence to the Department of Labor hierarchy) or to the organization’s compliance staff for their immediate action.
In other words, OSHA consulting is true consulting only when nothing seriously wrong is found. If anything serious or imminently hazardous is found, the “customer” loses control of the decision process as to how and when to correct it.
Private consulting firms. A third source of external help is the (full-time) private consultant or the private consulting firms, who can provide help in any area—behavioural systems, safety systems or physical conditions—with none of the special limitations mentioned above. The only difficulty is ensuring that a consultant has been selected who has the necessary skills and knowledge to provide the desired work product.
Part-time private consultation and others. The fourth place to locate a private consultant is among those individuals who consult on a part-time basis to supplement their incomes. These consultants are either retired safety professionals who remain active, or college or university professors who supplement their income and stay knowledgeable about the world outside the academy. Here again the problem is to locate these people and ensure that the person hired has the competencies needed. Additional sources include consultants who make themselves available through national or local safety councils, and consultants with trade associations.
Locating a Consultant
In the first two categories of external help listed above, government and insurance, finding a consultant is easy. For example, in the United States, one can contact the appropriate workers’ compensation insurance carrier or the local OSHA grant office and ask them to visit the organization. Many other countries provide similar governmental and insurance resources.
Finding a consultant in the second two categories, private individual consultants and consulting firms, is more difficult. In the United States, for instance, several organizations publish directories of consultants. As an example, the American Society of Safety Engineers (ASSE) publishes a national directory, which includes some 260 names of consultants. However, there seem to be considerable problems using this directory. An analysis of the 260 people on the list shows that 56% are individuals who indicate that they are for hire but who have not stated whether they work for companies and seek additional income or are full-time consultants or part-time retired safety consultants. An additional 32% were identified as being connected with consulting firms, 5% were connected with universities, 3% were insurance brokers, 3% were connected with manufacturing companies and 1% were associated with state governments. Actually, this directory, while advertised as a document which tells the reader “where the occupational safety/health experts are”, is really a roster of those people who have paid their dues and are members of the consultants division of the ASSE.
There is no easy way to find a consultant who has the expertise needed. Probably the best approaches other than insurance or government are to (1) network with other organizations with similar problems to see who they have used and whether they were satisfied with the results, (2) contact a professional organization at the national level, or (3) make use of professional directories such as the one above, keeping in mind the qualifications made concerning it.
Insurance Consulting
The most readily available of the outside consultants are insurance consultants. Since the beginning of the industrial safety movement, the insurance industry has been involved with safety. For many years. the only possible external help for most companies had been that available from the company’s insurance carrier. While this is no longer true, the insurance consultant is most often sought out.
The safety services departments of typical large insurance companies are charged with three specific functions:
- a sales assistance function
- an underwriting assistance function
- a customer service function.
Only the third of these is of value to the customer needing safety assistance. The underwriting assistance function is carried out by a field representative who is the “eyes and ears” of the insurance company, observing what is going on at the policyholder’s place of business and reporting back to the desk-bound underwriter. The third function consists of assisting customers to improve their loss prevention and safety programmes and reducing the likelihood of those customers having accidents and suffering financial loss. The assistance offered varies considerably from company to company.
Over the years, different philosophies have emerged which dictate the value of the service that the insurance company is able to provide. In some companies the safety services department is still very much a part of the underwriting function and their duties are to observe and report, while in others, the engineering department reports to the underwriting department. In some insurance companies, the loss-control department is independent, existing primarily to serve the customer and only secondarily to assist the sales and underwriting functions. When the primary mission of the service is to assist sales, customer service will suffer. If the loss-control department is part of underwriting, it may be difficult to get safety service from them, as they simply may not be staffed with trained, qualified people to provide that sort of service. If the loss-control department is not part of underwriting, then it may be able to provide good service to a customer. Conversely, it may also be quite ineffective, because numerous factors can intervene that can frustrate the effective provision of safety service.
When the service is an inspection-only service, as is very prevalent, the safety system and the behavioural system will be totally overlooked. When the service consists of the delivery of safety aids and materials, and nothing else, it is a virtually meaningless service. When the service consists primarily or totally of holding safety meetings for a customer, such as delivering the “canned” safety programme that the carrier’s home office has devised for use at all insured companies, or merely ensuring that physical conditions are up to code, it is also a weak service.
Depending upon the sort of philosophy that underlies the service of the carrier, additional services may be available over and beyond that provided by the representative that calls on the customer. Figure 1 outlines some typical additional services that can be particularly useful to customers, such as industrial hygiene, nursing and specialist (engineering and fire protection) services, depending upon the organization’s current needs. Training services are somewhat less common but are also valuable.
Figure 1. Additional services of consultants
Government Consultants
As with the insurance consultants, certain considerations, such as the following, must be weighed by a company before deciding whether or not to request the assistance of government consultants.
- whether the terms under which government assistance is offered are acceptable
- the competence of the people
- the limited scope of the consulting
- the inability to direct the consulting focus.
Probably the first consideration is whether or not a company wishes to become involved with a government at all. When using other kinds of consultants (either private or those provided by an insurance firm), whatever findings are obtained are strictly between the organization and the consultant. Whatever the company decides to do is a decision reserved to the company alone, which retains control over the disposition of the information. With government consultants this is not totally true. For example, if the consultants find one or both of two kinds of hazards—violations of the law and those immediately dangerous to life or health—the organization may not be able to retain the power of decision as to what to do about the hazard and when to do it.
Government consultants can provide assistance with determining whether or not an organization is in compliance with regulations and standards. This is an extremely narrow focus and has many weaknesses, as pointed out by Peters (1978) in his article “Why only a fool relies on safety standards”: “For those who know little about safety, it seems quite plausible and reasonable to expect that the existence of good safety standards and a sufficient conformance to those standards should be an adequate measure of safety assurance.” Peters suggests that not only is such an expectation in error, but also that reliance on standards will subvert professional activities that are needed to reduce loss.
Private Consulting
With the private consultant, whether an independent individual or an employee of a consulting firm, full or part time, there are no mandatory reporting requirements. The private consultant does not have to abide by the mandates of a required referral system; the relationship is strictly between the organization and the individual consultant. The scope of the consultation is limited, as the “customer” can very directly control the focus of the consultant’s activities. Thus the only thing the client has to worry about is whether or not the consultant is competent in the areas where help is needed and whether or not the fee is judged to be a fair one. Figure 2 lists some of the most basic functions of the management consultant.
Figure 2. Basic functions of the management consultant

G. Lippit (1969), who has written extensively on the consulting process, has identified eight specific consultant activities:
- helps management examine organizational problems (e.g., organizes a management meeting for problem identification in the problem relationships between home and field personnel)
- helps management examine the contribution of the proper dialogue to these problems (e.g., in relation to home and field office problems, explores with management how a conference on communication blocks might lead to problem solving)
- helps examine the long- and short-range objectives of the renewal action (e.g., involves management in refining objectives and in setting goals)
- explores, with management, alternatives to renewal plans
- develops, with management, the renewal plans (e.g., based on the objectives, works with a task force to develop a process with built-in evaluation rather than simply submitting an independently developed plan to management for approval)
- explores appropriate resources to implement renewal plans (e.g., provides management with a variety of resources both inside and outside the organization; the renewal stimulator must help management to understand what each resource can contribute to effective problem solving)
- provides consultation for management on evaluation and review of renewal process (e.g., evaluation must be in terms of problem solving; working with management; the renewal stimulator must assess the current status of the problem, rather than check whether or not certain activities have been conducted)
- explores with management the follow-up steps necessary to reinforce problem solving and outputs from the renewal process (e.g., encourages management to look at implications of the steps taken so far, and to assess the current status of the organization in terms of other actions that might be necessary to follow up on implementation of the renewal process).
Lippit (1969) has also identified five different positions which the consultants can adopt vis-à-vis their clients’ needs (Figure 3).
Figure 3. Five consultant approaches

Choosing a Consultant
When choosing a consultant, a process such as that given by figure 4 is suggested.
Figure 4. Choosing a consultant
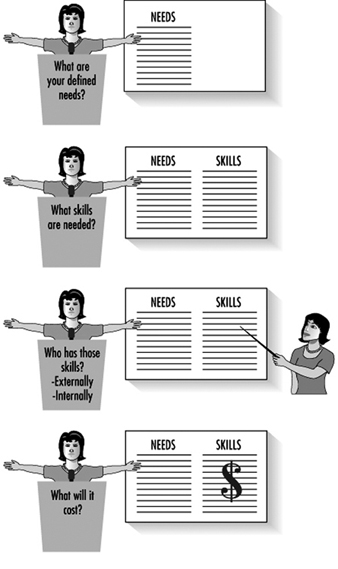
Whether or not to use a consultant, and which one to use, ought to be determined by the user’s defined needs and by what kinds of skills and knowledge the consultant must have to be of real help. Then, it would seem logical to look for individuals or groups that have those sorts of skills and knowledge. It may be determined that as a result of this process, the job can be done without external help; for example, to locate the needed skills internally and apply those skills to the defined safety problems. Conversely, it may be decided to go to the outside for the skills needed.
Evaluating the Consultant’s Performance
After having worked with consultants for a period of time, a company can judge their individual performance and worth to the organization much more accurately (figure 5). As a result of the analysis provided by the consultant, the conclusion may be made that perhaps the remainder of the job, or a similar job, can be done as well using internal resources. Many companies do this now, and more are turning to it, in both safety and nonsafety areas.
Figure 5. Evaluating the consultant's performance

Problem-Solving Approaches
K. Albert, in his book, How to Be Your Own Management Consultant (1978), suggests that there are four different types of internal management problem-solving approaches:
- to hire a full-time internal consultant
- to put someone on a special assignment on a temporary basis
- to create a task force to work on a problem
- collaboration between an outside consultant and an internal consultant.
Furthermore, Albert suggests that no matter which approach is chosen, these ground rules must be followed for success:
- Get total support of top management.
- Establish confidentiality.
- Earn the acceptance of operation units.
- Avoid company politics.
- Report to a high level.
- Start slowly and maintain objectivity.
Government Services
The establishment and control of acceptable standards of safety and health at work is universally regarded as a function of government, even though the legal responsibility for compliance rests with the employer. (It should be noted that in many countries, safety standards are established by consensus between manufactures, users, insurers, public and government and then adopted or referenced by government into regulations.) Government provides a range of safety services in order to discharge its function. In this context, government includes both national, regional and provincial authorities.
Legislative Framework
One of the most important services supporting safety in the workplace is the legislative framework within which it must operate, and the task of providing this framework is a vital function of government. Such legislation should be comprehensive in its scope and application, reflect international standards as well as national needs, give consideration to established, proven industry safe practices and provide for the means to carry its intentions into practical effect. Safety and health legislation which is based on extensive consultation with the social partners, industry and the community stands a much greater chance of being properly observed and respected, and therefore contributes significantly to sound standards of protection.
Compliance
The legislative framework, although important, must be effectively translated into practical action at the level of the enterprise. A vital government service is the creation of an effective inspectorate to carry the law into effect. Government must therefore establish an inspectorate, supply it with adequate resources in terms of finance and personnel, and provide it with sufficient powers to do its work.
Safety and Health Information
A key service is that of publicity for safety and health. This function is not of course exclusive to government; safety associations, employers’ groups, trade unions and consultants can all play a part in ensuring a greater awareness of legal requirements, of standards, of technical solutions and of new hazards and risk. Government may take a leading role in offering guidance on compliance with legislation and on compliance with standards governing safety practices, ranging from acceptable methods of machinery guarding to publicizing tables of exposure limits to hazardous substances.
Government should also provide the stimulus in identifying suitable topics for specific campaigns and initiatives. Such activities are usually carried out in cooperation with employers’ associations and trade unions, and are often derived from analysis of government, industry and association statistics relating to accidents and ill health. In considering its publicity and information strategy, government must ensure that it reaches not only the more sophisticated and developed industries but also those with very limited knowledge and awareness of safety and health matters. This is particularly important in developing countries and those with economies heavily dependent upon agriculture and upon the family as the unit of employment.
The collection, analysis and publication of statistics on safety and health is an important service. Statistics provide the inspectorates and their social partners with the raw material that enables them to identify emerging trends or shifting patterns in accident and ill-health causation and to assess, in measurable terms, the effectiveness of national policies, of specific campaigns and of standards of compliance. Statistics can also provide some degree of comparative standards and of achievement on an international basis.
The accuracy of the statistical information on accidents is clearly of prime importance. Some countries have an accident reporting system which is wholly separate from the social benefit or injury compensation system. Reliance is placed on a legal requirement that accidents be reported to the enforcing authority. Statistical studies have shown that there can be a significant shortfall in the reporting of accidents (other than fatalities) under this system. Up to 60% of accidents in some industries are not reported to the enforcing authorities. This shortfall can only devalue the statistics which are produced. The integrity and accuracy of accident and ill-health statistics must be a priority for government.
Safety Training
Safety training is another area in which service may be provided by government. Most safety and health legislation features requirements for adequate training. The extent to which government is directly involved in organizing and providing training varies considerably. At the highest levels of training—that is, for the safety professionals—the work is usually undertaken at universities and colleges of technology. Direct government input at this level is relatively uncommon although government scientists, lawyers and technologists from inspectorates often do contribute as lecturers and by providing funding and training materials.
A similar pattern exists at the lower level of skills training for safety. Educational courses for workers are often conducted by industry, trade or training associations with an input and funding from the inspectorates, as are courses which are designed to increase the safety awareness of workers. The function of government is less to conduct and direct training services, than to stimulate and encourage non-governmental organizations to do this work, and to contribute directly wherever appropriate. More direct assistance can be provided through government subsidies to assist in defraying the costs of training to companies. Much of the material on which safety training is based is provided by official government publications, notes of guidance and formally published standards.
Services for Small Businesses
The problem of furnishing service to small businesses is singularly complex. There is the very real need to provide sympathetic help and encouragement to an important element of the national and local economy. At the same time there is a need to ensure that this be done effectively without lowering the standards of protection for employees and possibly endangering their safety and their health. In attempting to address this complexity, the service provided by government plays a key role.
Many governments provide a particular service to small enterprises which includes the management of safety and health. This service is provided in a variety of ways, including, for example, special “start-up” packs of information which provide (1) details on means of complying in practical terms with legal requirements, (2) facts as to where to find sources of information and (3) a contact point with the inspectorates. Some inspectorates have staff dedicated to dealing with the particular needs of small businesses and, in conjunction with trade associations, provide seminars and meetings where safety and health issues can be constructively discussed in a nonconfrontational atmosphere.
Safety Research
Research is another service provided by government, either directly through supporting its own laboratories and research programmes on safety and health problems, or indirectly by providing grants to independent research organizations for specific projects. Health and safety research may be divided into two broad categories, as follows:
- forensic research, exemplified by the research that follows major accidents in order to determine their causes
- longer-term research which investigates, for example, exposure levels for potentially hazardous substances.
There is also laboratory service which provides facilities for such tests as the analysis of samples counts, and for approvals systems for protective equipment. This service is important both for the inspectorates and for the social partners concerned in validating health standards in enterprises. There is debate whether government should maintain laboratory and research facilities, or whether these functions might more properly be the responsibility of universities and independent research units. But these arguments are about means rather than about basic purpose. Few would dispute that the research function in its broadest sense is a vital government service to safety and health, whether the government acts through its own facilities or stimulates and provides resources to non-governmental organizations to do the work.
Safety Representation
Finally, the government provides a service via its representational role within the international community. Many safety and health problems are international in character and cannot be confined within national boundaries. Cooperation between governments, the establishment of internationally accepted standards for hazardous substances, the exchange of information between governments, support for international organizations dealing with safety and health—all these are the functions of government, and the effective discharge of these duties can only serve to enhance both the standing and the standards of safety and health nationally and internationally.
Occupational Safety Research: An Overview
Occupational safety research is the study of the incidence, characteristics, causes and prevention of workplace injury. Beginning with the pioneering work of John Gordon (1949) and William Haddon, Jr. (Haddon, Suchman and Klein 1964), and increasingly in the 1980s and 1990s, injury has been viewed as a public health problem to which the public health approach, historically successful against disease, could be applied. Epidemiology, the science of public health, has been applied to injury, including occupational injury. The epidemiological model describes the relationship between the agent (the environmental entity or phenomenon that is the necessary cause of the disease or injury), the host (the affected person) and the environment. Its adaptation to the study of workplace injury came largely through the insights of two seminal figures in injury research, James J. Gibson (1961) and later Haddon (Haddon, Suchman and Klein 1964). Haddon recognized that the various forms of energy—me-chanical, thermal, radiant, chemical or electrical—were the “agents” of injury, analogous to the micro-organisms that cause infectious illnesses. Researchers and practitioners from multiple disciplines—primarily epidemiology, engineering, ergonomics, biomechanics, behavioural psychology, safety management and industrial hygiene—are engaged in the study of the factors associated with the worker (the host); the environment; the type and source of energy involved (the agent); and the tools, machines and tasks (the vehicles) that combine to cause or contribute to workplace injury.
Two Complementary Approaches: Public Health and Safety Analysis
The public health approach is one model which provides a framework for occupational safety research. The public health approach involves:
- the identification, characterization and description of injury cases, hazards and exposures through surveillance
- the in-depth analysis of specified injury problems in specified worker populations in order to identify, quantify and compare risk and causal factors
- the identification and development of prevention strategies and interventions
- the evaluation of preventive strategies in laboratory and field experiments
- the communication of information on risk and the development of strategies and programmes for reducing risk and preventing injuries.
Ideally, workplace safety problems may be identified and solved systematically by means of this process.
Safety analysis is another relevant model for addressing workplace injury. Safety analysis has been defined as “a systematic examination of the structure and functions of a system aiming at identifying accident contributors, modelling potential accidents, and finding risk-reducing measures” (Suokas 1988). It is an engineering-oriented approach which involves the consideration of potential system failures (one outcome of which could be worker injury) during the design or evaluation of processes, equipment, tools, tasks and work environments. This model presupposes an ability to analyse and understand the interactions among components of workplace systems in order to predict possible modes of failure before the systems are implemented. Ideally, systems can be made safe at the design stage, rather than modified after injury or damage has already occurred.
The Public Health Approach to Occupational Safety Research
The field of occupational safety research is evolving as different approaches and perspectives, such as epidemiology and engineering, merge to create new methods for evaluating and documenting workplace hazards, and thereby identifying possible strategies for prevention This article discusses the public health approach to occupational safety research, and the areas where safety analysis fits into this approach in order to provide both a general overview of the field and some insight into future opportunities and challenges. A secondary intent is to discuss (1) the relationship of occupational safety research to safety management, regulation and technology transfer, and (2) the impact of advancing technology on occupational safety research and communication.
Surveillance
To solve occupational injury problems, specific problems faced by specific worker populations must be identified. Therefore, the public health approach to occupational safety research begins with epidemiological surveillance, which has been defined as “the ongoing systematic collection, analysis and the interpretation of health data in the process of describing and monitoring a health event” (CDC 1988). In safety research, this refers to the collection, analysis and interpretation of data on injuries, hazards, exposures, work processes and worker populations.
Surveillance answers the basic questions about occupational injury. Surveillance can provide information about injuries by various demographic categories, including the worker’s gender, ethnicity, age, occupation and industry, in addition to information relating to the time and place of injury and sometimes the circumstances surrounding the incident. With such basic case information and employment information to provide denominators for the calculation of rates, researchers have been able to describe risk in terms of (1) the frequency of injuries, which helps define the scope or extent of a problem, and (2) the rate of injury (expressed as the number of injuries or deaths per 100,000 workers), which helps define the relative risk faced by certain types of workers in certain circumstances. These analyses and comparisons are useful to researchers in identifying problems, including emerging or escalating problems; establishing priorities; formulating hypotheses for further research; and monitoring trends in order to evaluate the effectiveness of prevention programmes.Findings obtained from occupational injury and fatality surveillance have enabled researchers to plan and conduct in-depth research aimed at both identifying causes or contributing factors and ultimately developing preventive strategies. Additionally, the information gained from surveillance serves an important social function by raising awareness of risk among those at risk, risk managers, policy makers and the general public, and by pointing to problem areas in need of increased attention and resources for research and prevention.
Analytical Research
As major occupational injury problem areas become apparent through surveillance, researchers can devise studies to answer more detailed questions about the risks faced by target populations. Analytical epidemiology and engineering methods can be employed to look more closely at the circumstances and factors that may cause or contribute to injuries. Occupational injury surveillance generally does not provide data in sufficient detail to enable one to determine risk factors, those characteristics associated with workplace components (including workers) that can directly or indirectly cause injurious incidents. Without such detailed information, opportunities for prevention may not be discovered. This sort of information, which describes the circumstances surrounding an injurious event, is necessary to analyse the sequence of tasks; the interaction of factors associated with the victim, the coworkers, the tasks, the tools and the processes; the time phases of the event (from pre-event to post-event); the preventive strategies employed; and the organization and safety attitudes of the employer.
One method of collecting detailed information is through the investigation of occupational injuries or fatalities. Investigation generally relies on a formal methodology that combines information collection via interviewing, analysing case reports and other documentation, and onsite or laboratory-based engineering analysis and observation (i.e., forensic engineering) in the attempt to reconstruct the events and circumstances that led to the incident. Analytical epidemiological research techniques require various types of study designs such as case-control, prospective or retrospective designs to test hypotheses regarding specific risk factors and their relative contributions to specified outcomes. Safety analysis techniques such as hazard analysis, job/task analysis, fault-tree analysis and other systems safety engineering tools can also be used to define risks and causes, and to predict or assign probabilities to various failure modes that might eventuate in injury to workers. The future of occupational risk and causality research may well lie in a combination of these research modes that allows causation models based on analytical systems engineering methods to be validated by experience as documented through investigative and epidemiological research findings.
Developing Prevention Strategies and Interventions
As risk and causal factors are identified and characterized, and the relative importance of multiple risk factors are discerned, opportunities for prevention may become apparent. With insight into risk and causal factors, occupational safety researchers and practitioners can consider possible prevention strategies aimed at reducing risk, or consider interventions to interrupt the causal sequence of accidents. Currently, there are a wide range of protective technologies and strategies that have already been applied to worker protection, and might be more broadly applied with beneficial results. Similarly, technologies and strategies have been developed and applied in other fields which may have potential for worker protection. Finally, undiscovered technologies and strategies will be brought to light in the pursuit of improved worker protection. The goal of occupational safety research is the identification, development and implementation of effective preventive strategies to reduce the risk of injury to workers.
Haddon (1973) postulated ten basic, generalized strategies for reducing damage due to environmental or workplace hazards. The highest priority of occupational safety researchers studying preventive strategies is to identify, design and evaluate engineering controls that are well integrated into the workplace environment, equipment, tools or processes, and that provide protection automatically (“passive” controls), without any specific action or behaviour on the part of the worker. Of the three classes of prevention strategies—persuasion (via information and education), those that impose requirements (via laws and standards) (Robertson 1983) and those that provide automatic protection, it is the latter that is generally cited as the most effective and preferable. Examples of passive, or automatic, controls might include an interlock safety device on an electrical circuit that automatically de-energizes the circuit if safety barriers are removed or bypassed, or protective vehicle airbags that automatically deploy upon collision.
Evaluating and Demonstrating Prevention Strategies and Interventions
A crucial step that is often omitted from the safety research process is the formal evaluation of potential prevention strategies and interventions to ensure that they work in controlled laboratory settings and in actual workplace environments before they are widely or universally implemented. Sometimes, the well-intentioned introduction of a prevention strategy may have the effect of creating a new, unforeseen hazard. Even if there are compelling reasons to implement preventive strategies before they can be formally evaluated, evaluation should not be neglected altogether. Evaluation is important not just for engineering controls and modifications, but also for tasks, processes, procedures, regulations, training programmes and safety information products—that is, any strategy, intervention or modification aimed at eliminating or reducing risk.
Occupational Injury Risk and Prevention Information
When effective preventive strategies are identified or developed, they are the keys to implementing the strategies. Occupational safety research produces two types of information that are useful to individuals and organizations outside the research community: risk information and prevention information.
- Risk messages may include the notification that risk exists; information about the scope or nature of risk; information about the individuals or populations at risk; information about when, where, how and why the risk exists; and information about the factors that influence or contribute to risk and their relative importance. Risk information is a principal product of surveillance and analytical research.
- Prevention messages include information on methods of reducing risk and may cover a broad range of strategies and interventions.
The most important audiences for risk and prevention information are the populations at risk, and the various individuals and organizations that have the power to change or influence workplace risk through their decisions, programmes and policies. These audiences, which include the workers, employers, safety and health practitioners, regulators, insurers, legislators and policymakers, are targeted when researchers develop new information regarding the existence or scope of occupational injury problems, or recommendations aimed at reducing risk. Another key audience for both the methods and findings of research are peer scientists and scientists in government agencies, private sector organizations and academic institutions who are working to illuminate and solve the injury and illness problems besetting the workforce. Researchers must also cultivate the mass and regional media and continue to promote the ideas that occupational injuries and deaths constitute a significant public health problem and are preventable.
Communication
Research is needed into the diffusion and practical application of occupational safety research findings. The communication of safety information is rarely evaluated to determine what methods, messages, channels and formats are effective in given situations for specific groups. The growing need for communication of information related to health has given rise to several approaches applicable to the communication of safety information. Health education, health communication, health promotion, risk communication and social marketing are some of the areas where communication activities are being systematized and studied scientifically. Research into human behaviour, motivation, cognition and perception plays an obvious role in determining whether and how information and communication processes can produce safety awareness and safety behaviours in at-risk individuals and groups. Many of the customer-oriented techniques of commercial marketing have been adapted by “social” marketers to promote changes in behaviour and attitude that serve a social benefit, including those that can lead to improved safety, health and well-being among workers.
Relationship of Research Findings to Safety Management
Safety practitioners and managers must be aware of current research findings that have practical implications for workplace safety. New risk or prevention information may require review and modification of existing programmes and procedures. The following sections discuss the relationship of research to the regulation of workplaces and the transfer of technology—that is, the transferral of new, proven preventive strategies and technologies from their innovation sites to other, comparable workplaces where similar conditions and risks exist.
Research and regulation
Regulators—those who develop and enforce occupational safety standards—must be aware of current research findings that affect regulatory requirements. Regulatory safety requirements imposed on employers should be based on scientifically proven prevention strategies that have been sufficiently demonstrated to be effective in reducing the risk of injury. This requires a close relationship and effective communications between the occupational safety research and the regulatory communities. Whether the regulatory body is a government agency or a voluntary, industry-based organization, the safety standards that they promulgate should incorporate the best available research findings. It is incumbent on both the regulators and the researchers to ensure effective communications.
Research and technology transfer
Individual workers, supervisors, companies, safety specialists and researchers are solving safety problems every day through the development and implementation of prevention strategies and interventions. Unfortunately, however, there are too few mechanisms and incentives enabling and actuating individuals or companies to share effective prevention measures with others that may face similar safety problems. Industry and trade associations, labour unions, insurers and other organizations serve the function of collecting, organizing and distributing prevention information to their members and clients. However, a large potential benefit from the sharing of prevention information remains unrealized, particularly by small employers and underserved workers. Research findings in the diffusion of innovations, communications and information management may be useful in addressing this gap.
Research and technology
The advance of technology has expanded upon the ways in which research can be designed and conducted; harmful exposures can be detected, measured, recorded or displayed, and reduced; hazards can be controlled; and information can be presented and distributed. The most significant technologies for safety research are in the areas of sensors, materials and, perhaps most important, digital electronics; the processing power, storage capacity and networking of computers has set the stage for a new era of simulation, automation and global communications. The challenge for researchers and practitioners in the field of occupational safety is to utilize advanced technological tools for research and to improve the communication of hazard and hazard control information. Some technological tools can improve our ability to accomplish difficult or otherwise dangerous research—for example, through simulations that do not require destruction of costly equipment or tools, or exposure of human participants. Some tools can improve analysis or decision making—for example, through simulating human expertise—and thus command a scarce resource: knowledge of how to conduct occupational injury research and achieve injury prevention. Technological tools can improve our ability to distribute relevant hazard-related information to those who need it, and make it possible for them to actively seek out such information.
Research needs and trends
Occupational safety research should be prepared to take advantage of evolving technologies and expressions of increased social concern, to focus on areas where more research is needed, including the following:
- new scientific methods that incorporate and integrate epidemiology and engineering techniques and approaches in the study of occupational safety
- expanded and standardized surveillance to include systems for nonfatal injuries, “near miss” incidents, hazards and exposures
- increased attention to the role of organizational factors, as well as economic factors, in occupational safety; this would include study of the effects of management techniques and movements, such as the worldwide quality movement sparked by the work of W. Edwards Deming
- more emphasis on underserved, high-risk populations, including those in agriculture, logging, commercial fishing, construction and small businesses in all sectors; and on leading causes of death and serious injury that require more study, including those causes involved in work-related motor-vehicle transportation and violence (Veazie et al. 1994)
- evaluation and demonstration of engineering controls and other preventive strategies, including regulation, education and communications
- technology transfer: the use of technologies utilized for other purposes to address questions of occupational safety research and management, and the appropriate use of effective protective technologies or strategies implemented at one site or in a limited setting, to address similar risks in a wider area
- the role of psychosocial factors, including stress, on the incidence of occupational injury
- old and new technological approaches to passive methods of worker protection, including sensors, microprocessors, robotics, artificial intelligence, display and imaging technology, wireless telecommunications and interlocks.
Summary
Traditionally, public health researchers and practitioners have employed epidemiology, biostatistics, medicine, microbiology, toxicology, pharmacology, health education and other disciplines in the identification, evaluation and prevention of infectious and, more recently, chronic illnesses. Injuries and injury deaths, including those that occur at work, are serious public health problems too, and are often associated with specific causes and factors that contribute to their occurrence. Injuries and injury deaths are not random events, but result from cause-and-effect relationships, and are therefore predictable and preventable. These injury outcomes lend themselves to the same problem-solving approaches as have been used to identify, characterize and prevent illnesses.
One primary difference between the approaches to illness and injury outcomes lies in the nature of the preventive measures that can be taken. To prevent or reduce the risk of infectious and chronic diseases, health practitioners may recommend or use vaccines and pharmaceuticals, nutritional and lifestyle modifications, or environmental controls. To prevent or reduce the risk of occupational injuries, safety practitioners may recommend or use engineering controls, such as equipment guards, interlocks, and ergonomically designed tools and machines; or administrative controls, such as work practices, schedules and training; or personal protective equipment, such as respirators, hard hats or fall protective devices. This means that in injury prevention, epidemiologists, biostatisticians and health educators are joined by engineers, physicists, industrial hygienists and ergonomists. The problem-solving process is the same; some of the intervention approaches, and therefore the disciplines involved in identifying, developing and testing interventions, may be different.
The mechanism of occupational safety and health research is the public health approach, an integrated, multidisciplinary approach to identification through (1) surveillance and investigation, (2) epidemiological and safety analysis, (3) research and development leading to preventive technologies and strategies, (4) evaluation and demonstration to ensure that these technologies and strategies are effective, and (5) communication of risk information, research methods and findings, and effective technologies and strategies. The public health approach and the safety analysis approach are merging in the study of occupational safety. The principal disciplines of epidemiology and engineering are collaborating to bring new insight into injury causation and prevention. New and advancing technologies, particularly digital electronic computer technology, are being adapted to solve workplace safety problems.
Risk Acceptance
The concept of risk acceptance asks the question, “How safe is safe enough?” or, in more precise terms, “The conditional nature of risk assessment raises the question of which standard of risk we should accept against which to calibrate human biases” (Pidgeon 1991). This question takes importance in issues such as: (1) Should there be an additional containment shell around nuclear power plants? (2) Should schools containing asbestos be closed? or (3) Should one avoid all possible trouble, at least in the short run? Some of these questions are aimed at government or other regulatory bodies; others are aimed at the individual who must decide between certain actions and possible uncertain dangers.
The question whether to accept or reject risks is the result of decisions made to determine the optimal level of risk for a given situation. In many instances, these decisions will follow as an almost automatic result of the exercise of perceptions and habits acquired from experience and training. However, whenever a new situation arises or changes in seemingly familiar tasks occur, such as in performing non-routine or semi-routine tasks, decision making becomes more complex. To understand more about why people accept certain risks and reject others we shall need to define first what risk acceptance is. Next, the psychological processes that lead to either acceptance or rejection have to be explained, including influencing factors. Finally, methods to change too high or too low levels of risk acceptance will be addressed.
Understanding Risk
Generally speaking, whenever risk is not rejected, people have either voluntarily, thoughtlessly or habitually accepted it. Thus, for example, when people participate in traffic, they accept the danger of damage, injury, death and pollution for the opportunity of benefits resulting from increased mobility; when they decide to undergo surgery or not to undergo it, they decide that the costs and/or benefits of either decision are greater; and when they are investing money in the financial market or deciding to change business products, all decisions accepting certain financial dangers and opportunities are made with some degree of uncertainty. Finally, the decision to work in any job also has varying probabilities of suffering an injury or fatality, based on statistical accident history.
Defining risk acceptance by referring only to what has not been rejected leaves two important issues open; (1) what exactly is meant by the term risk, and (2) the often made assumption that risks are merely potential losses that have to be avoided, while in reality there is a difference between merely tolerating risks, fully accepting them, or even wishing for them to occur to enjoy thrill and excitement. These facets might all be expressed through the same behaviour (such as participating in traffic) but have different underlying cognitive, emotional and physiological processes. It seems obvious that a merely tolerated risk relates to a different level of commitment than if one even has the desire for a certain thrill, or “risky” sensation. Figure 1 summarizes facets of risk acceptance.
Figure 1. Facets of risk acceptance and risk rejection
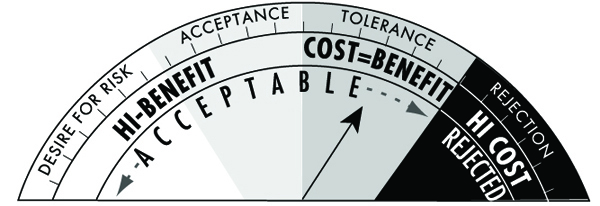
If one looks up the term risk in the dictionaries of several languages, it often has the double meaning of “chance, opportunity” on one hand and “danger, loss” (e.g., wej-ji in Chinese, Risiko in German, risico in Dutch and Italian, risque in French, etc.) on the other. The word risk was created and became popular in the sixteenth century as a consequence of a change in people’s perceptions, from being totally manipulated by “good and evil spirits,” towards the concept of the chance and danger of every free individual to influence his or her own future. (Probable origins of risk lie in the Greek word rhiza, meaning “root and/or cliff”, or the Arabic word rizq meaning “what God and fate provide for your life”.) Similarly, in our everyday language we use proverbs such as “Nothing ventured, nothing gained” or “God helps the brave”, thereby promoting risk taking and risk acceptance. The concept always related to risk is that of uncertainty. As there is almost always some uncertainty about success or failure, or about the probability and quantity of consequences, accepting risks always means accepting uncertainties (Schäfer 1978).
Safety research has largely reduced the meaning of risk to its dangerous aspects (Yates 1992b). Only lately have positive consequences of risk re-emerged with the increase in adventurous leisure time activities (bungee jumping, motorcycling, adventure travels, etc.) and with a deeper understanding of how people are motivated to accept and take risks (Trimpop 1994). It is argued that we can understand and influence risk acceptance and risk taking behaviour only if we take the positive aspects of risks into account as well as the negative.
Risk acceptance therefore refers to the behaviour of a person in a situation of uncertainty that results from the decision to engage in that behaviour (or not to engage in it), after weighing the estimated benefits as greater (or lesser) than the costs under the given circumstances. This process can be extremely quick and not even enter the conscious decision-making level in automatic or habitual behaviour, such as shifting gears when the noise of the engine rises. At the other extreme, it may take very long and involve deliberate thinking and debates among several people, such as when planning a hazardous operation such as a space flight.
One important aspect of this definition is that of perception. Because perception and subsequent evaluation is based on a person’s individual experiences, values and personality, the behavioural acceptance of risks is based more on subjective risk than on objective risk. Furthermore, as long as a risk is not perceived or considered, a person cannot respond to it, no matter how grave the hazard. Thus, the cognitive process leading to the acceptance of risk is an information-processing and evaluation procedure residing within each person that can be extremely quick.
A model describing the identification of risks as a cognitive process of identification, storage and retrieval was discussed by Yates and Stone (1992). Problems can arise at each stage of the process. For example, accuracy in the identification of risks is rather unreliable, especially in complex situations or for dangers such as radiation, poison or other not easily perceptible stimuli. Furthermore, the identification, storage and retrieval mechanisms underlie common psychological phenomena, such as primacy and recency effects, as well as familiarity habituation. That means that people familiar with a certain risk, such as driving at high speed, will get used to it, accept it as a given “normal” situation and estimate the risk at a far lower value than people not familiar with the activity. A simple formalization of the process is a model with the components of:
Stimulus → Perception → Evaluation → Decision → Behaviour → Feedback loop
For example, a slowly moving vehicle in front of a driver may be the stimulus to pass. Checking the road for traffic is perception. Estimating the time needed to pass, given the acceleration capabilities of one’s car, is evaluation. The value of saving time leads to the decision and following behaviour to pass the car or not. The degree of success or failure is noticed immediately and this feedback influences subsequent decisions about passing behaviour. At each step of this process, the final decision whether to accept or reject risks can be influenced. Costs and benefits are evaluated based on individual-, context- and object-related factors that have been identified in scientific research to be of importance for risk acceptance.
Which Factors Influence Risk Acceptance?
Fischhoff et al. (1981) identified the factors (1) individual perception, (2) time, (3) space and (4) context of behaviour, as important dimensions of risk taking that should be considered in studying risks. Other authors have used different categories and different labels for the factors and contexts influencing risk acceptance. The categories of properties of the task or risk object, individual factors and context factors have been used to structure this large number of influential factors, as summarized in figure 2.
Figure 2. Factors influencing risk acceptance

In normal models of risk acceptance, consequences of new technological risks (e.g., genetic research) were often described by quantitative summary measures (e.g., deaths, damage, injuries), and probability distributions over consequences were arrived at through estimation or simulation (Starr 1969). Results were compared to risks already “accepted” by the public, and thus offered a measure of acceptability of the new risk. Sometimes data were presented in a risk index to compare the different types of risk. The methods used most often were summarized by Fischhoff et al. (1981) as professional judgement by experts, statistical and historical information and formal analyses, such as fault tree analyses. The authors argued that properly conducted formal analyses have the highest “objectivity” as they separate facts from beliefs and take many influences into account. However, safety experts stated that the public and individual acceptance of risks may be based on biased value judgements and on opinions publicized by the media, and not on logical analyses.
It has been suggested that the general public is often misinformed by the media and political groups that produce statistics in favour of their arguments. Instead of relying on individual biases, only professional judgements based on expert knowledge should be used as a basis for accepting risks, and the general public should be excluded from such important decisions. This has drawn substantial criticism as it is viewed as a question of both democratic values (people should have a chance to decide issues that may have catastrophic consequences for their health and safety) and social values (does the technology or risky decision benefit receivers more than those who pay the costs). Fischhoff, Furby and Gregory (1987) suggested the use of either expressed preferences (interviews, questionnaires) or revealed preferences (observations) of the “relevant” public to determine the acceptability of risks. Jungermann and Rohrmann have pointed out the problems of identifying who is the “relevant public” for technologies such as nuclear power plants or genetic manipulations, as several nations or the world population may suffer or benefit from the consequences.
Problems with solely relying on expert judgements have also been discussed. Expert judgements based on normal models approach statistical estimations more closely than those of the public (Otway and von Winterfeldt 1982). However, when asked specifically to judge the probability or frequency of death or injuries related to a new technology, the public’s views are much more similar to the expert judgements and to the risk indices. Research also showed that although people do not change their first quick estimate when provided with data, they do change when realistic benefits or dangers are raised and discussed by experts. Furthermore, Haight (1986) pointed out that because expert judgements are subjective, and experts often disagree about risk estimates, that the public is sometimes more accurate in its estimate of riskiness, if judged after the accident has occurred (e.g., the catastrophe at Chernobyl). Thus, it is concluded that the public uses other dimensions of risk when making judgements than statistical number of deaths or injuries.
Another aspect that plays a role in accepting risks is whether the perceived effects of taking risks are judged positive, such as adrenaline high, “flow” experience or social praise as a hero. Machlis and Rosa (1990) discussed the concept of desired risk in contrast to tolerated or dreaded risk and concluded that in many situations increased risks function as an incentive, rather than as a deterrent. They found that people may behave not at all averse to risk in spite of media coverage stressing the dangers. For example, amusement park operators reported a ride becoming more popular when it reopened after a fatality. Also, after a Norwegian ferry sank and the passengers were set afloat on icebergs for 36 hours, the operating company experienced the greatest demand it had ever had for passage on its vessels. Researchers concluded that the concept of desired risk changes the perception and acceptance of risks, and demands different conceptual models to explain risk-taking behaviour. These assumptions were supported by research showing that for police officers on patrol the physical danger of being attacked or killed was ironically perceived as job enrichment, while for police officers engaged in administrative duties, the same risk was perceived as dreadful. Vlek and Stallen (1980) suggested the inclusion of more personal and intrinsic reward aspects in cost/benefit analyses to explain the processes of risk assessment and risk acceptance more completely.
Individual factors influencing risk acceptance
Jungermann and Slovic (1987) reported data showing individual differences in perception, evaluation and acceptance of “objectively” identical risks between students, technicians and environmental activists. Age, sex and level of education have been found to influence risk acceptance, with young, poorly educated males taking the highest risks (e.g., wars, traffic accidents). Zuckerman (1979) provided a number of examples for individual differences in risk acceptance and stated that they are most likely influenced by personality factors, such as sensation seeking, extroversion, overconfidence or experience seeking. Costs and benefits of risks also contribute to individual evaluation and decision processes. In judging the riskiness of a situation or action, different people reach a wide variety of verdicts. The variety can manifest itself in terms of calibration—for example, due to value-induced biases which let the preferred decision appear less risky so that overconfident people choose a different anchor value. Personality aspects, however, account for only 10 to 20% of the decision to accept a risk or to reject it. Other factors have to be identified to explain the remaining 80 to 90%.
Slovic, Fischhoff and Lichtenstein (1980) concluded from factor-analytical studies and interviews that non-experts assess risks qualitatively differently by including the dimensions of controllability, voluntariness, dreadfulness and whether the risk has been previously known. Voluntariness and perceived controllability were discussed in great detail by Fischhoff et al. (1981). It is estimated that voluntarily chosen risks (motorcycling, mountain climbing) have a level of acceptance which is about 1,000 times as high as that of involuntarily chosen, societal risks. Supporting the difference between societal and individual risks, the importance of voluntariness and controllability has been posited in a study by von Winterfeldt, John and Borcherding (1981). These authors reported lower perceived riskiness for motorcycling, stunt work and auto racing than for nuclear power and air traffic accidents. Renn (1981) reported a study on voluntariness and perceived negative effects. One group of subjects was allowed to choose between three types of pills, while the other group was administered these pills. Although all pills were identical, the voluntary group reported significantly fewer “side-effects” than the administered group.
When risks are individually perceived as having more dreadful consequences for many people, or even catastrophic consequences with a near zero probability of occurrence, these risks are often judged as unacceptable in spite of the knowledge that there have not been any or many fatal accidents. This holds even more true for risks previously unknown to the person judging. Research also shows that people use their personal knowledge and experience with the particular risk as the key anchor of judgement for accepting well-defined risks while previously unknown risks are judged more by levels of dread and severity. People are more likely to underestimate even high risks if they have been exposed for an extended period of time, such as people living below a power dam or in earthquake zones, or having jobs with a “habitually” high risk, such as in underground mining, logging or construction (Zimolong 1985). Furthermore, people seem to judge human-made risks very differently from natural risks, accepting natural ones more readily than self-constructed, human-made risks. The approach used by experts to base risks for new technologies within the low-end and high-end “objective risks” of already accepted or natural risks seems not to be perceived as adequate by the public. It can be argued that already “accepted risks” are merely tolerated, that new risks add on to the existing ones and that new dangers have not been experienced and coped with yet. Thus, expert statements are essentially viewed as promises. Finally, it is very hard to determine what has been truly accepted, as many people are seemingly unaware of many risks surrounding them.
Even if people are aware of the risks surrounding them, the problem of behavioural adaptation occurs. This process is well described in risk compensation and risk homeostasis theory (Wilde 1986), which states that people adjust their risk acceptance decision and their risk-taking behaviour towards their target level of perceived risk. That means that people will behave more cautiously and accept fewer risks when they feel threatened, and, conversely, they will behave more daringly and accept higher levels of risk when they feel safe and secure. Thus, it is very difficult for safety experts to design safety equipment, such as seat-belts, ski boots, helmets, wide roads, fully enclosed machinery and so on, without the user’s offsetting the possible safety benefit by some personal benefit, such as increased speed, comfort, decreased attention or other more “risky” behaviour.
Changing the accepted level of risk by increasing the value of safe behaviour may increase the motivation to accept the less dangerous alternative. This approach aims at changing individual values, norms and beliefs to motivate alternative risk acceptance and risk-taking behaviour. Among the factors that increase or decrease the likelihood of risk acceptance, are those such as whether the technology provides a benefit corresponding to present needs, increases the standard of living, creates new jobs, facilitates economic growth, enhances national prestige and independence, requires strict security measures, increases the power of big business, or leads to centralization of political and economic systems (Otway and von Winterfeldt 1982). Similar influences of situational frames on risk evaluations were reported by Kahneman and Tversky (1979 and 1984). They reported that if they phrased the outcome of a surgical or radiation therapy as 68% probability of survival, 44% of the subjects chose it. This can be compared to only 18% who chose the same surgical or radiation therapy, if the outcome was phrased as 32% probability of death, which is mathematically equivalent. Often subjects choose a personal anchor value (Lopes and Ekberg 1980) to judge the acceptability of risks, especially when dealing with cumulative risks over time.
The influence of “emotional frames” (affective context with induced emotions) on risk assessment and acceptance was shown by Johnson and Tversky (1983). In their frames, positive and negative emotions were induced through descriptions of events such as personal success or the death of a young man. They found that subjects with induced negative feelings judged the risks of accidental and violent fatality rates as significantly higher, regardless of other context variables, than subjects of the positive emotional group. Other factors influencing individual risk acceptance include group values, individual beliefs, societal norms, cultural values, the economic and political situation, and recent experiences, such as seeing an accident. Dake (1992) argued that risk is—apart from its physical component—a concept very much dependent on the respective system of beliefs and myths within a cultural frame. Yates and Stone (1992) listed the individual biases (figure 3) that have been found to influence the judgement and acceptance of risks.
Figure 3. Individual biases that influence risk evaluation and risk acceptance

Cultural factors influencing risk acceptance
Pidgeon (1991) defined culture as the collection of beliefs, norms, attitudes, roles and practices shared within a given social group or population. Differences in cultures lead to different levels of risk perception and acceptance, for example in comparing the work safety standards and accident rates in industrialized countries with those in developing countries. In spite of the differences, one of the most consistent findings across cultures and within cultures is that usually the same concepts of dreadfulness and unknown risks, and those of voluntariness and controllability emerge, but they receive different priorities (Kasperson 1986). Whether these priorities are solely culture dependent remains a question of debate. For example, in estimating the hazards of toxic and radioactive waste disposal, British people focus more on transportation risks; Hungarians more on operating risks; and Americans more on environmental risks. These differences are attributed to cultural differences, but may just as well be the consequence of a perceived population density in Britain, operating reliability in Hungary and the environmental concerns in the United States, which are situational factors. In another study, Kleinhesselink and Rosa (1991) found that Japanese perceive atomic power as a dreadful but not unknown risk, while for Americans atomic power is a predominantly unknown source of risk.
The authors attributed these differences to different exposure, such as to the atomic bombs dropped on Hiroshima and Nagasaki in 1945. However, similar differences were reported between Hispanic and White American residents of the San Francisco area. Thus, local cultural, knowledge and individual differences may play an equally important role in risk perception as general cultural biases do (Rohrmann 1992a).
These and similar discrepancies in conclusions and interpretations derived from identical facts led Johnson (1991) to formulate cautious warnings about the causal attribution of cultural differences to risk perception and risk acceptance. He worried about the widely spread differences in the definition of culture, which make it almost an all-encompassing label. Moreover, differences in opinions and behaviours of subpopulations or individual business organizations within a country add further problems to a clear-cut measurement of culture or its effects on risk perception and risk acceptance. Also, the samples studied are usually small and not representative of the cultures as a whole, and often causes and effects are not separated properly (Rohrmann 1995). Other cultural aspects examined were world views, such as individualism versus egalitarianism versus belief in hierarchies, and social, political, religious or economic factors.
Wilde (1994) reported, for example, that the number of accidents is inversely related to a country’s economic situation. In times of recession the number of traffic accidents drops, while in times of growth the number of accidents rises. Wilde attributed these findings to a number of factors, such as that in times of recession since more people are unemployed and gasoline and spare parts are more costly, people will consequently take more care to avoid accidents. On the other hand, Fischhoff et al. (1981) argued that in times of recession people are more willing to accept dangers and uncomfortable working conditions in order to keep a job or to get one.
The role of language and its use in mass media were discussed by Dake (1991), who cited a number of examples in which the same “facts” were worded such that they supported the political goals of specific groups, organizations or governments. For example, are worker complaints about suspected occupational hazards “legitimate concerns” or “narcissistic phobias”? Is hazard information available to the courts in personal injury cases “sound evidence” or “scientific flotsam”? Do we face ecological “nightmares” or simply “incidences” or “challenges”? Risk acceptance thus depends on the perceived situation and context of the risk to be judged, as well as on the perceived situation and context of the judges themselves (von Winterfeldt and Edwards 1984). As the previous examples show, risk perception and acceptance strongly depend on the way the basic “facts” are presented. The credibility of the source, the amount and type of media coverage—in short, risk communication—is a factor determining risk acceptance more often than the results of formal analyses or expert judgements would suggest. Risk communication is thus a context factor that is specifically used to change risk acceptance.
Changing Risk Acceptance
To best achieve a high degree of acceptance for a change, it has proven very successful to include those who are supposed to accept the change in the planning, decision and control process to bind them to support the decision. Based on successful project reports, figure 4 lists six steps that should be considered when dealing with risks.
Figure 4. Six steps for choosing, deciding upon and accepting optimal risks

Determining “optimal risks”
In steps 1 and 2, major problems occur in identifying the desirability and the “objective risk” of the objective. while in step 3, it seems to be difficult to eliminate the worst options. For individuals and organizations alike, large-scale societal, catastrophic or lethal dangers seem to be the most dreaded and least acceptable options. Perrow (1984) argued that most societal risks, such as DNA research, power plants, or the nuclear arms race, possess many closely coupled subsystems, meaning that if one error occurs in a subsystem, it can trigger many other errors. These consecutive errors may remain undetected, due to the nature of the initial error, such as a nonfunctioning warning sign. The risks of accidents happening due to interactive failures increases in complex technical systems. Thus, Perrow (1984) suggested that it would be advisable to leave societal risks loosely coupled (i.e., independently controllable) and to allow for independent assessment of and protection against risks and to consider very carefully the necessity for technologies with the potential for catastrophic consequences.
Communicating “optimal choices”
Steps 3 to 6 deal with accurate communication of risks, which is a necessary tool to develop adequate risk perception, risk estimation and optimal risk-taking behaviour. Risk communication is aimed at different audiences, such as residents, employees, patients and so on. Risk communication uses different channels such as newspapers, radio, television, verbal communication and all of these in different situations or “arenas”, such as training sessions, public hearings, articles, campaigns and personal communications. In spite of little research on the effectiveness of mass media communication in the area of health and safety, most authors agree that the quality of the communication largely determines the likelihood of attitudinal or behavioural changes in risk acceptance of the targeted audience. According to Rohrmann (1992a), risk communication also serves different purposes, some of which are listed in figure 5.
Figure 5. Purposes of risk communication

Risk communication is a complex issue, with its effectiveness seldom proven with scientific exactness. Rohrmann (1992a) listed necessary factors for evaluating risk communication and gave some advice about communicating effectively. Wilde (1993) separated the source, the message, the channel and the recipient and gave suggestions for each aspect of communication. He cited data that show, for example, that the likelihood of effective safety and health communication depends on issues such as those listed in figure 6.
Figure 6. Factors influencing the effectiveness of risk communication

Establishing a risk optimization culture
Pidgeon (1991) defined safety culture as a constructed system of meanings through which a given people or group understands the hazards of the world. This system specifies what is important and legitimate, and explains relationships to matters of life and death, work and danger. A safety culture is created and recreated as members of it repeatedly behave in ways that seem to be natural, obvious and unquestionable and as such will construct a particular version of risk, danger and safety. Such versions of the perils of the world also will embody explanatory schemata to describe the causation of accidents. Within an organization, such as a company or a country, the tacit and explicit rules and norms governing safety are at the heart of a safety culture. Major components are rules for handling hazards, attitudes toward safety, and reflexivity on safety practice.
Industrial organizations that already live an elaborate safety culture emphasize the importance of common visions, goals, standards and behaviours in risk taking and risk acceptance. As uncertainties are unavoidable within the context of work, an optimal balance of taking chances and control of hazards has to be stricken. Vlek and Cvetkovitch (1989) stated:
Adequate risk management is a matter of organizing and maintaining a sufficient degree of (dynamic) control over a technological activity, rather than continually, or just once, measuring accident probabilities and distributing the message that these are, and will be, “negligibly low”. Thus more often than not, “acceptable risk” means “sufficient control”.
Summary
When people perceive themselves to possess sufficient control over possible hazards, they are willing to accept the dangers to gain the benefits. Sufficient control, however, has to be based on sound information, assessment, perception, evaluation and finally an optimal decision in favour of or against the “risky objective”.
Risk Perception
In risk perception, two psychological processes may be distinguished: hazard perception and risk assessment. Saari (1976) defines the information processed during the accomplishment of a task in terms of the following two components: (1) the information required to execute a task (hazard perception) and (2) the information required to keep existing risks under control (risk assessment). For instance, when construction workers on the top of ladders who are drilling holes in a wall have to simultaneously keep their balance and automatically coordinate their body-hand movements, hazard perception is crucial to coordinate body movement to keep dangers under control, whereas conscious risk assessment plays only a minor role, if any. Human activities generally seem to be driven by automatic recognition of signals which trigger a flexible, yet stored hierarchy of action schemata. (The more deliberate process leading to the acceptance or rejection of risk is discussed in another article.)
Risk Perception
From a technical point of view, a hazard represents a source of energy with the potential of causing immediate injury to personnel and damage to equipment, environment or structure. Workers may also be exposed to diverse toxic substances, such as chemicals, gases or radioactivity, some of which cause health problems. Unlike hazardous energies, which have an immediate effect on the body, toxic substances have quite different temporal characteristics, ranging from immediate effects to delays over months and years. Often there is an accumulating effect of small doses of toxic substances which are imperceptible to the exposed workers.
Conversely, there may be no harm to persons from hazardous energy or toxic substances provided that no danger exists. Danger expresses the relative exposure to hazard. In fact there may be little danger in the presence of some hazards as a result of the provision of adequate precautions. There is voluminous literature pertaining to factors people use in the final assessment of whether a situation is determined hazardous, and, if so, how hazardous. This has become known as risk perception. (The word risk is being used in the same sense that danger is used in occupational safety literature; see Hoyos and Zimolong 1988.)
Risk perception deals with the understanding of perceptual realities and indicators of hazards and toxic substances—that is, the perception of objects, sounds, odorous or tactile sensations. Fire, heights, moving objects, loud noise and acid smells are some examples of the more obvious hazards which do not need to be interpreted. In some instances, people are similarly reactive in their responses to the sudden presence of imminent danger. The sudden occurrence of loud noise, loss of balance, and objects rapidly increasing in size (and so appearing about to strike one’s body), are fear stimuli, prompting automatic responses such as jumping, dodging, blinking and clutching. Other reflex reactions include rapidly withdrawing a hand which has touched a hot surface. Rachman (1974) concludes that the prepotent fear stimuli are those which have the attributes of novelty, abruptness and high intensity.
Probably most hazards and toxic substances are not directly perceptible to the human senses, but are inferred from indicators. Examples are electricity; colourless, odourless gases such as methane and carbon monoxide; x rays and radioactive subs-tances; and oxygen-deficient atmospheres. Their presence must be signalled by devices which translate the presence of the hazard into something which is recognizable. Electrical currents can be perceived with the help of a current checking device, such as may be used for signals on the gauges and meters in a control-room register that indicate normal and abnormal levels of temperature and pressure at a particular state of a chemical process. There are also situations where hazards exist which are not perceivable at all or cannot be made perceivable at a given time. One example is the danger of infection when one opens blood probes for medical tests. The knowledge that hazards exist must be deduced from one’s knowledge of the common principles of causality or acquired by experience.
Risk Assessment
The next step in information-processing is risk assessment, which refers to the decision process as it is applied to such issues as whether and to what extent a person will be exposed to danger. Consider, for instance, driving a car at high speed. From the perspective of the individual, such decisions have to be made only in unexpected circumstances such as emergencies. Most of the required driving behaviour is automatic and runs smoothly without continuous attentional control and conscious risk assessment.
Hacker (1987) and Rasmussen (1983) distinguished three levels of behaviour: (1) skill-based behaviour, which is almost entirely automatic; (2) rule-based behaviour, which operates through the application of consciously chosen but fully pre-programmed rules; and (3) knowledge-based behaviour, under which all sorts of conscious planning and problem solving are grouped. At the skill-based level, an incoming piece of information is connected directly to a stored response that is executed automatically and carried out without conscious deliberation or control. If there is no automatic response available or any extraordinary event occurring, the risk assessment process moves to the rule-based level, where the appropriate action is selected from a sample of procedures taken out of storage and then executed. Each of the steps involves a finely tuned perceptual-motor programme, and usually, no step in this organizational hierarchy involves any decisions based on risk considerations. Only at the transitions is a conditional check applied, just to verify whether the progress is according to plan. If not, automatic control is halted and the ensuing problem solved at a higher level.
Reason’s GEMS (1990) model describes how the transition from automatic control to conscious problem solving takes place when exceptional circumstances arise or novel situations are encountered. Risk assessment is absent at the bottom level, but may be fully present at the top level. At the middle level one can assume some sort of “quick-and-dirty” risk assessment, while Rasmussen excludes any type of assessment that is not incorporated in fixed rules. Much of the time there will be no conscious perception or consideration of hazards as such. “The lack of safety consciousness is both a normal and a healthy state of affairs, despite what has been said in countless books, articles and speeches. Being constantly conscious of danger is a reasonable definition of paranoia” (Hale and Glendon 1987). People doing their jobs on a routine basis rarely consider these hazards or accidents in advance: they run risks, but they do not take them.
Hazard Perception
Perception of hazards and toxic substances, in the sense of direct perception of shape and colour, loudness and pitch, odours and vibrations, is restricted by the capacity limitations of the perceptual senses, which can be temporarily impaired due to fatigue, illness, alcohol or drugs. Factors such as glare, brightness or fog can put heavy stress on perception, and dangers can fail to be detected because of distractions or insufficient alertness.
As has already been mentioned, not all hazards are directly perceptible to the human senses. Most toxic substances are not even visible. Ruppert (1987) found in his investigation of an iron and steel factory, of municipal garbage collecting and of medical laboratories, that from 2,230 hazard indicators named by 138 workers, only 42% were perceptible by the human senses. Twenty-two per cent of the indicators have to be inferred from comparisons with standards (e.g., noise levels). Hazard perception is based in 23% of cases on clearly perceptible events which have to be interpreted with respect to knowledge about hazardousness (e.g., a glossy surface of a wet floor indicates slippery). In 13% of reports, hazard indicators can be retrieved only from memory of proper steps to be taken (e.g., current in a wall socket can be made perceivable only by the proper checking device). These results demonstrate that the requirements of hazard perception range from pure detection and perception to elaborate cognitive inference processes of anticipation and assessment. Cause-and-effect relationships are sometimes unclear, scarcely detectable, or misinterpreted, and delayed or accumulating effects of hazards and toxic substances are likely to impose additional burdens on individuals.
Hoyos et al. (1991) have listed a comprehensive picture of hazard indicators, behavioural requirements and safety-relevant conditions in industry and public services. A Safety Diagnosis Questionnaire (SDQ) has been developed to provide a practical instrument to analyse hazards and dangers through observation (Hoyos and Ruppert 1993). More than 390 workplaces, and working and environmental conditions in 69 companies concerned with agriculture, industry, manual work and the service industries, have been assessed. Because the companies had accident rates greater than 30 accidents per 1,000 employees with a minimum of 3 lost working days per accident, there appears to be a bias in these studies towards dangerous worksites. Altogether 2,373 hazards have been reported by the observers using SDQ, indicating a detection rate of 6.1 hazards per workplace and between 7 and 18 hazards have been detected at approximately 40% of all workplaces surveyed. The surprisingly low mean rate of 6.1 hazards per workplace has to be interpreted with consideration toward the safety measures broadly introduced in industry and agriculture during the last 20 years. Hazards reported do not include those attributable to toxic substances, nor hazards controlled by technical safety devices and measures, and thus reflect the distribution of “residual hazards”.
In figure 1 an overview of requirements for perceptual processes of hazard detection and perception is presented. Observers had to assess all hazards at a particular workplace with respect to 13 requirements, as indicated in the figure. On the average, 5 requirements per hazard were identified, including visual recognition, selective attention, auditory recognition and vigilance. As expected, visual recognition dominates by comparison with auditory recognition (77.3% of the hazards were detected visually and only 21.2% by auditory detection). In 57% of all hazards observed, workers had to divide their attention between tasks and hazard control, and divided attention is a very strenuous mental achievement likely to contribute to errors. Accidents have frequently been traced back to failures in attention while performing dual tasks. Even more alarming is the finding that in 56% of all hazards, workers had to cope with rapid activities and responsiveness to avoid being hit and injured. Only 15.9% and 7.3% of all hazards were indicated by acoustical or optical warnings, respectively: consequently, hazard detection and perception was self-initiated.
Figure 1. Detection and perception of hazard indicators in industry
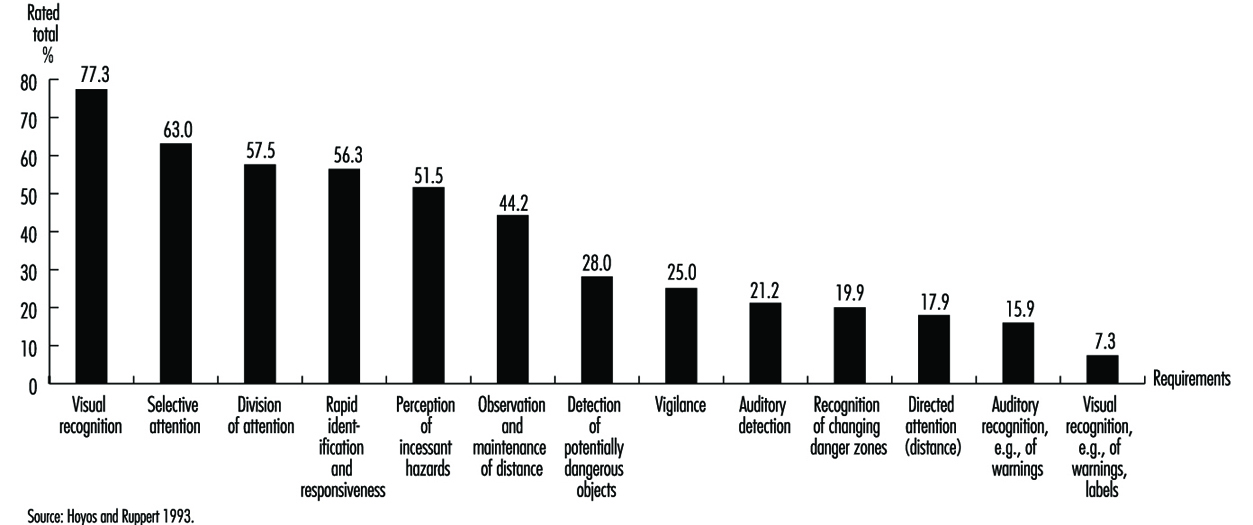
In some cases (16.1%) perception of hazards is supported by signs and warnings, but usually, workers rely on knowledge, training and work experience. Figure 2 shows the requirements of anticipation and assessment required to control hazards at the worksite. The core characteristic of all activities summarized in this figure is the need for knowledge and experience gained in the work process, including: technical knowledge about weight, forces and energies; training to identify defects and inadequacies of work tools and machinery; and experience to predict structural weaknesses of equipment, buildings and material. As Hoyos et al. (1991) have demonstrated, workers have little knowledge relating to hazards, safety rules and proper personal preventive behaviour. Only 60% of the construction workers and 61% of the auto-mechanics questioned knew the right solutions to the safety-related problems generally encountered at their workplaces.
Figure 2. Anticipation and assessment of hazard indicators
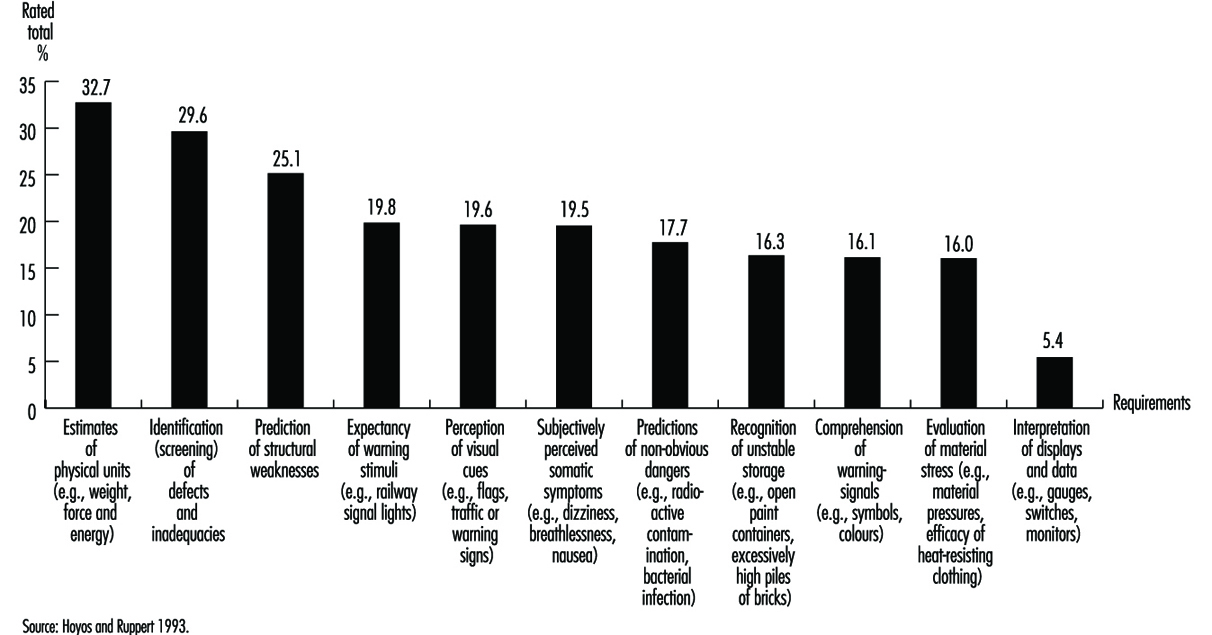
The analysis of hazard perception indicates that different cognitive processes are involved, such as visual recognition; selective and divided attention; rapid identification and responsiveness; estimates of technical parameters; and predictions of non-observable hazards and dangers. In fact, hazards and dangers are frequently unknown to job incumbents: they impose a heavy burden on people who have to cope sequentially with dozens of visual- and auditory-based requirements and are a source of proneness to error when work and hazard control is performed simultaneously. This requires much more emphasis to be placed on regular analysis and identification of hazards and dangers at the workplace. In several countries, formal risk assessments of workplaces are mandatory: for example, the health and safety Directives of the EEC require risk assessment of computer workplaces prior to commencing work in them, or when major alterations at work have been introduced; and the US Occupational Safety and Health Administration (OSHA) requires regular hazard risk analyses of process units.
Coordination of Work and Hazard Control
As Hoyos and Ruppert (1993) point out, (1) work and hazard control may require attention simultaneously; (2) they may be managed alternatively in sequential steps; or (3) prior to the commencement of work, precautionary measures may be taken (e.g., putting on a safety helmet).
In the case of simultaneously occurring requirements, hazard control is based on visual, auditory and tactile recognition. In fact, it is difficult to separate work and hazard control in routine tasks. For example, a source of constant danger is present when performing the task of cutting off threads from yarns in a cotton-mill factory—a task requiring a sharp knife. The only two types of protection against cuts are skill in wielding the knife and use of protective equipment. If either or both are to succeed, they must be totally incorporated into the worker’s action sequences. Habits such as cutting in a direction away from the hand which is holding the thread must be ingrained into the worker’s skills from the outset. In this example hazard control is fully integrated into task control; no separate process of hazard detection is required. Probably there is a continuum of integration into work, the degree depending on the skill of the worker and the requirements of the task. On the one hand, hazard perception and control is inherently integrated into work skills; on the other hand, task execution and hazard control are distinctly separate activities. Work and hazard control may be carried out alternatively, in sequential steps, when during the task, danger potential steadily increases or there is an abrupt, alerting danger signal. As a consequence, workers interrupt the task or process and take preventive measures. For example, the checking of a gauge is a typical example of a simple diagnostic test. A control room operator detects a deviation from standard level on a gauge which at first glance does not constitute a dramatic sign of danger, but which prompts the operator to search further on other gauges and meters. If there are other deviations present, a rapid series of scanning activities will be carried out at the rule-based level. If deviations on other meters do not fit into a familiar pattern, the diagnosis process shifts to the knowledge-based level. In most cases, guided by some strategies, signals and symptoms are actively looked for to locate causes of the deviations (Konradt 1994). The allocation of resources of the attentional control system is set to general monitoring. A sudden signal, such as a warning tone or, as in the case above, various deviations of pointers from a standard, shifts the attentional control system onto the specific topic of hazard control. It initiates an activity which seeks to identify the causes of the deviations on the rule-based level, or in case of misfortune, on the knowledge-based level (Reason 1990).
Preventive behaviour is the third type of coordination. It occurs prior to work, and the most prominent example is the use of personal protective equipment (PPE).
The Meanings of Risk
Definitions of risks and methods to assess risks in industry and society have been developed in economics, engineering, chemistry, safety sciences and ergonomics (Hoyos and Zimolong 1988). There is a wide variety of interpretations of the term risk. On the one hand, it is interpreted to mean “probability of an undesired event”. It is an expression of the likelihood that something unpleasant will happen. A more neutral definition of risk is used by Yates (1992a), who argues that risk should be perceived as a multidimensional concept that as a whole refers to the prospect of loss. Important contributions to our current understanding of risk assessment in society have come from geography, sociology, political science, anthropology and psychology. Research focused originally on understanding human behaviour in the face of natural hazards, but it has since broadened to incorporate technological hazards as well. Sociological research and anthropological studies have shown that assessment and acceptance of risks have their roots in social and cultural factors. Short (1984) argues that responses to hazards are mediated by social influences transmitted by friends, family, co-workers and respected public officials. Psychological research on risk assessment originated in empirical studies of probability assessment, utility assessment and decision-making processes (Edwards 1961).
Technical risk assessment usually focuses on the potential for loss, which includes the probability of the loss’s occurring and the magnitude of the given loss in terms of death, injury or damages. Risk is the probability that damage of a specified type will occur in a given system over a defined time period. Different assessment techniques are applied to meet the various requirements of industry and society. Formal analysis methods to estimate degrees of risk are derived from different kinds of fault tree analyses; by use of data banks comprising error probabilities such as THERP (Swain and Guttmann 1983); or on decomposition methods based on subjective ratings such as SLIM-Maud (Embrey et al. 1984). These techniques differ considerably in their potential to predict future events such as mishaps, errors or accidents. In terms of error prediction in industrial systems, experts attained the best results with THERP. In a simulation study, Zimolong (1992) found a close match between objectively derived error probabilities and their estimates derived with THERP. Zimolong and Trimpop (1994) argued that such formal analyses have the highest “objectivity” if conducted properly, as they separated facts from beliefs and took many of the judgemental biases into account.
The public’s sense of risk depends on more than the probability and magnitude of loss. It may depend on factors such as potential degree of damage, unfamiliarity with possible consequences, the involuntary nature of exposure to risk, the uncontrollability of damage, and possible biased media coverage. The feeling of control in a situation may be a particularly important factor. For many, flying seems very unsafe because one has no control over one’s fate once in the air. Rumar (1988) found that the perceived risk in driving a car is typically low, since in most situations the drivers believe in their own ability to achieve control and are accustomed to the risk. Other research has addressed emotional reactions to risky situations. The potential for serious loss generates a variety of emotional reactions, not all of which are necessarily unpleasant. There is a fine line between fear and excitement. Again, a major determinant of perceived risk and of affective reactions to risky situations seems to be a person’s feeling of control or lack thereof. As a consequence, for many people, risk may be nothing more than a feeling.
Decision Making under Risk
Risk taking may be the result of a deliberate decision process entailing several activities: identification of possible courses of action; identification of consequences; evaluation of the attractiveness and chances of the consequences; or deciding according to a combination of all the previous assessments. The overwhelming evidence that people often make poor choices in risky situations implies the potential to make better decisions. In 1738, Bernoulli defined the notion of a “best bet” as one which maximizes the expected utility (EU) of the decision. The EU concept of rationality asserts that people ought to make decisions by evaluating uncertainties and considering their choices, the possible consequences, and one’s preferences for them (von Neumann and Morgenstern 1947). Savage (1954) later generalized the theory to allow probability values to represent subjective or personal probabilities.
Subjective expected utility (SEU) is a normative theory which describes how people should proceed when making decisions. Slovic, Kunreuther and White (1974) stated, “Maximization of expected utility commands respect as a guideline for wise behaviour because it is deduced from axiomatic principles that presumably would be accepted by any rational man.” A good deal of debate and empirical research has centred around the question of whether this theory could also describe both the goals that motivate actual decision makers and the processes they employ when reaching their decisions. Simon (1959) criticized it as a theory of a person selecting among fixed and known alternatives, to each of which known consequences are attached. Some researchers have even questioned whether people should obey the principles of expected utility theory, and after decades of research, SEU applications remain controversial. Research has revealed that psychological factors play an important role in decision making and that many of these factors are not adequately captured by SEU models.
In particular, research on judgement and choice has shown that people have methodological deficiencies such as understanding probabilities, negligence of the effect of sample sizes, reliance on misleading personal experiences, holding judgements of fact with unwarranted confidence, and misjudging risks. People are more likely to underestimate risks if they have been voluntarily exposed to risks over a longer period, such as living in areas subject to floods or earthquakes. Similar results have been reported from industry (Zimolong 1985). Shunters, miners, and forest and construction workers all dramatically underestimate the riskiness of their most common work activities as compared to objective accident statistics; however, they tend to overestimate any obvious dangerous activities of fellow workers when required to rate them.
Unfortunately, experts’ judgements appear to be prone to many of the same biases as those of the public, particularly when experts are forced to go beyond the limits of available data and rely upon their intuitions (Kahneman, Slovic and Tversky 1982). Research further indicates that disagreements about risk should not disappear completely even when sufficient evidence is available. Strong initial views are resistant to change because they influence the way that subsequent information is interpreted. New evidence appears reliable and informative if it is consistent with one’s initial beliefs; contrary evidence tends to be dismissed as unreliable, erroneous or unrepresentative (Nisbett and Ross 1980). When people lack strong prior opinions, the opposite situation prevails—they are at the mercy of the formulation of the problem. Presenting the same information about risk in different ways (e.g., mortality rates as opposed to survival rates) alters their perspectives and their actions (Tversky and Kahneman 1981). The discovery of this set of mental strategies, or heuristics, that people implement in order to structure their world and predict their future courses of action, has led to a deeper understanding of decision making in risky situations. Although these rules are valid in many circumstances, in others they lead to large and persistent biases with serious implications for risk assessment.
Personal Risk Assessment
The most common approach in studying how people make risk assessments uses psychophysical scaling and multivariate analysis techniques to produce quantitative representations of risk attitudes and assessment (Slovic, Fischhoff and Lichtenstein 1980). Numerous studies have shown that risk assessment based on subjective judgements is quantifiable and predictable. They also have shown that the concept of risk means different things to different people. When experts judge risk and rely on personal experience, their responses correlate highly with technical estimates of annual fatalities. Laypeople’s judgements of risk are related more to other characteristics, such as catastrophic potential or threat to future generations; as a result, their estimates of loss probabilities tend to differ from those of experts.
Laypeople’s risk assessments of hazards can be grouped into two factors (Slovic 1987). One of the factors reflects the degree to which a risk is understood by people. Understanding a risk relates to the degree to which it is observable, is known to those exposed, and can be detected immediately. The other factor reflects the degree to which the risk evokes a feeling of dread. Dread is related to the degree of uncontrollability, of serious consequences, of exposure of high risks to future generations, and of involuntary increase of risk. The higher a hazard’s score on the latter factor, the higher its assessed risk, the more people want to see its current risks reduced, and the more they want to see strict regulation employed to achieve the desired reduction in risk. Consequently, many conflicts about risk may result from experts’ and laypeople’s views originating from different definitions of the concept. In such cases, expert citations of risk statistics or of the outcome of technical risk assessments will do little to change people’s attitudes and assessments (Slovic 1993).
The characterization of hazards in terms of “knowledge” and “threat” leads back to the previous discussion of hazard and danger signals in industry in this section, which were discussed in terms of “perceptibility”. Forty-two per cent of the hazard indicators in industry are directly perceptible by human senses, 45% of cases have to be inferred from comparisons with standards, and 3% from memory. Perceptibility, knowledge and the threats and thrills of hazards are dimensions which are closely related to people’s experience of hazards and perceived control; however, to understand and predict individual behaviour in the face of danger we have to gain a deeper understanding of their relationships with personality, requirements of tasks, and societal variables.
Psychometric techniques seem well-suited to identify similarities and differences among groups with regard to both personal habits of risk assessment and to attitudes. However, other psychometric methods such as multidimensional analysis of hazard similarity judgements, applied to quite different sets of hazards, produce different representations. The factor-analytical approach, while informative, by no means provides a universal representation of hazards. Another weakness of psychometric studies is that people face risk only in written statements, and divorce the assessment of risk from behaviour in actual risky situations. Factors that affect a person’s considered assessment of risk in a psychometric experiment may be trivial when confronted with an actual risk. Howarth (1988) suggests that such conscious verbal knowledge usually reflects social stereotypes. By contrast, risk-taking responses in traffic or work situations are controlled by the tacit knowledge that underlies skilled or routine behaviour.
Most of the personal risk decisions in everyday life are not conscious decisions at all. People are, by and large, not even aware of risk. In contrast, the underlying notion of psychometric experiments is presented as a theory of deliberate choice. Assessments of risks usually performed by means of a questionnaire are conducted deliberately in an “armchair” fashion. In many ways, however, a person’s responses to risky situations are more likely to result from learned habits that are automatic, and which are below the general level of awareness. People do not normally evaluate risks, and therefore it cannot be argued that their way of evaluating risk is inaccurate and needs to be improved. Most risk-related activities are necessarily executed at the bottom level of automated behaviour, where there is simply no room for consideration of risks. The notion that risks, identified after the occurrence of accidents, are accepted after a conscious analysis, may have emerged from a confusion between normative SEU and descriptive models (Wagenaar 1992). Less attention was paid to the conditions in which people will act automatically, follow their gut feeling, or accept the first choice that is offered. However, there is a widespread acceptance in society and among health and safety professionals that risk taking is a prime factor in causing mishaps and errors. In a representative sample of Swedes aged between 18 and 70 years, 90% agreed that risk taking is the major source of accidents (Hovden and Larsson 1987).
Preventive Behaviour
Individuals may deliberately take preventive measures to exclude hazards, to attenuate the energy of hazards or to protect themselves by precautionary measures (for instance, by wearing safety glasses and helmets). Often people are required by a company’s directives or even by law to comply with protective measures. For example, a roofer builds a scaffolding prior to working on a roof to prevent the eventuality of suffering a fall. This choice might be the result of a conscious risk assessment process of hazards and of one’s own coping skills, or, more simply, it may be the outcome of a habituation process, or it may be a requirement which is enforced by law. Often warnings are used to indicate mandatory preventive actions.
Several forms of preventive activities in industry have been analysed by Hoyos and Ruppert (1993). Some of them are shown in figure 3, together with their frequency of requirement. As indicated, preventive behaviour is partly self-controlled and partly enforced by the legal standards and requirements of the company. Preventive activities comprise some of the following measures: planning work procedures and steps ahead; use of PPE; application of safety work technique; selection of safe work procedures by means of proper material and tools; setting an appropriate work pace; and inspection of facilities, equipment, machinery and tools.
Figure 3. Typical examples of personal preventive behaviour in industry and frequency of preventive measure
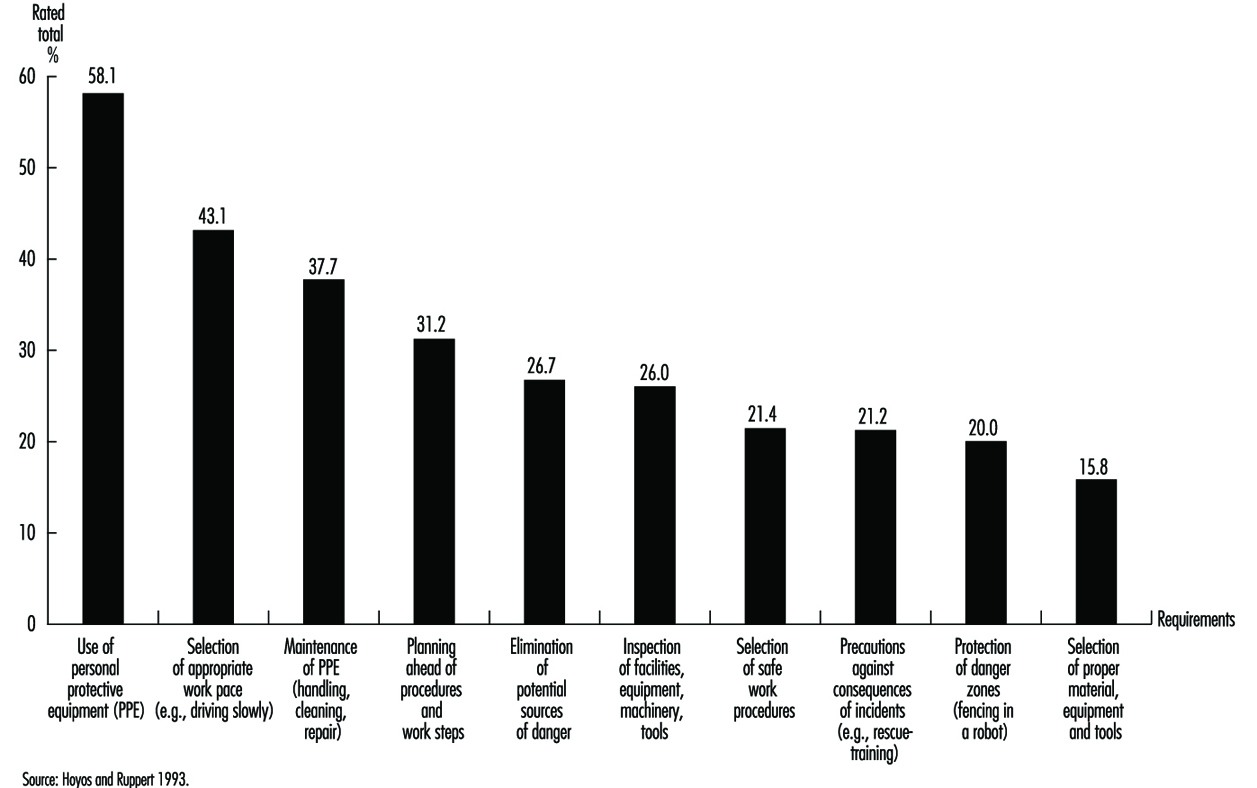
Personal Protective Equipment
The most frequent preventive measure required is the use of PPE. Together with correct handling and maintenance, it is by far the most common requirement in industry. There exist major differences in the usage of PPE between companies. In some of the best companies, mainly in chemical plants and petroleum refineries, the usage of PPE approaches 100%. In contrast, in the construction industry, safety officials have problems even in attempts to introduce particular PPE on a regular basis. It is doubtful that risk perception is the major factor which makes the difference. Some of the companies have successfully enforced the use of PPE which then becomes habitualized (e.g., the wearing of safety helmets) by establishing the “right safety culture” and subsequently altered personal risk assessment. Slovic (1987) in his short discussion on the usage of seat-belts shows that about 20% of road users wear seat-belts voluntarily, 50% would use them only if it were made mandatory by law, and beyond this number, only control and punishment will serve to improve automatic use.
Thus, it is important to understand what factors govern risk perception. However, it is equally important to know how to change behaviour and subsequently how to alter risk perception. It seems that many more precautionary measures need to be undertaken at the level of the organization, among the planners, designers, managers and those authorities that make decisions which have implications for many thousands of people. Up to now, there is little understanding at these levels as to which factors risk perception and assessment depend upon. If companies are seen as open systems, where different levels of organizations mutually influence each other and are in steady exchange with society, a systems approach may reveal those factors which constitute and influence risk perception and assessment.
Warning Labels
The use of labels and warnings to combat potential hazards is a controversial procedure for managing risks. Too often they are seen as a way for manufacturers to avoid responsibility for unreasonably risky products. Obviously, labels will be successful only if the information they contain is read and understood by members of the intended audience. Frantz and Rhoades (1993) found that 40% of clerical personnel filling a file cabinet noticed a warning label placed on the top drawer of the cabinet, 33% read part of it, and no one read the entire label. Contrary to expectation, 20% complied completely by not placing any material in the top drawer first. Obviously it is insufficient to scan the most important elements of the notice. Lehto and Papastavrou (1993) provided a thorough analysis of findings pertaining to warning signs and labels by examining receiver-, task-, product- and message-related factors. Furthermore, they provided a significant contribution to understanding the effectiveness of warnings by considering different levels of behaviour.
The discussion of skilled behaviour suggests that a warning notice will have little impact on the way people perform a familiar task, as it simply will not be read. Lehto and Papastavrou (1993) concluded from research findings that interrupting familiar task performance may effectively increase workers’ noticing warning signs or labels. In the experiment by Frantz and Rhoades (1993), noticing the warning labels on filing cabinets increased to 93% when the top drawer was sealed shut with a warning indicating that a label could be found within the drawer. The authors concluded, however, that ways of interrupting skill-based behaviour are not always available and that their effectiveness after initial use can diminish considerably.
At a rule-based level of performance, warning information should be integrated into the task (Lehto 1992) so that it can be easily mapped to immediate relevant actions. In other words, people should try to get the task executed following the directions of the warning label. Frantz (1992) found that 85% of subjects expressed the need for a requirement on the directions of use of a wood preservative or drain cleaner. On the negative side, studies of comprehension have revealed that people may poorly comprehend the symbols and text used in warning signs and labels. In particular, Koslowski and Zimolong (1992) found that chemical workers understood the meaning of only approximately 60% of the most important warning signs used in the chemical industry.
At a knowledge-based level of behaviour, people seem likely to notice warnings when they are actively looking for them. They expect to find warnings close to the product. Frantz (1992) found that subjects in unfamiliar settings complied with instructions 73% of the time if they read them, compared to only 9% when they did not read them. Once read, the label must be understood and recalled. Several studies of comprehension and memory also imply that people may have trouble remembering the information they read from either instruction or warning labels. In the United States, the National Research Council (1989) provides some assistance in designing warnings. They emphasize the importance of two-way communication in enhancing understanding. The communicator should facilitate information feedback and questions on the part of the recipient. The conclusions of the report are summarized in two checklists, one for use by managers, the other serving as a guide for the recipient of the information.
" DISCLAIMER: The ILO does not take responsibility for content presented on this web portal that is presented in any language other than English, which is the language used for the initial production and peer-review of original content. Certain statistics have not been updated since the production of the 4th edition of the Encyclopaedia (1998)."